 Mit Vachhrajani
Mit Vachhrajani Sushanta Kumar Mishra
Sushanta Kumar Mishra Himanshu Rai1
Himanshu Rai1
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
HYPOTHESIS AND THEORY article
Front. Psychol. , 11 October 2022
Sec. Personality and Social Psychology
Volume 13 - 2022 | https://doi.org/10.3389/fpsyg.2022.947887
Healthcare professionals such as nurses faced a tough time during the pandemic. Despite the personal and professional challenges, they contributed immensely during the pandemic. However, there were variations in nurses’ work engagement during the pandemic. One reason could be their personality, especially neuroticism. Neuroticism represents individuals’ proneness to distress in stressful situations, such as COVID-19. Hence, understanding how and in which conditions neuroticism influences work engagement is crucial. We used the Job Demand-Resource (JD-R) model to test the association between neuroticism and work engagement. As neuroticism represents the stress-proneness of an individual, we further investigated if stress mediates the neuroticism-work engagement link. For the nurses, patient interaction is an integral part of their job. Based on the data collected from the nurses, we tested if contact with patients (i.e., beneficiary contact) alleviates the adverse effect of neuroticism on work engagement. During COVID-19, there was an intense need for nursing support. Hence, avoiding duty when society is looking for support might induce a fear of stigmatization among the nurses. We examined if the perceived stigma of duty avoidance would affect the neuroticism-engagement relationship. Our results indicated that higher patient contact alleviated the adverse effect of neuroticism on work engagement. On the other hand, higher fear of stigma exacerbated the adverse effect of neuroticism on work engagement. We further checked the combined effect of beneficiary contact and fear of stigma on neuroticism-work engagement relationships. The findings highlighted the importance of societal factors and policymakers in enhancing nurses’ work engagement.
Nurses play a critical role in providing quality care to COVID patients (Villar et al., 2021), preventing the collapse of healthcare systems. Apart from providing healthcare services, they helped in contact tracing, served quarantined clients in community care services, and worked toward preventing and handling the pandemic (Zhang, 2021). Their responsibilities included educating people on COVID-19 prevention and reducing misinformation about the virus (Choi et al., 2020). Nurses were expected to maintain a high standard of hygiene while providing support and care to patients (Hoogendoorn et al., 2021). Thus, nurses played a significant role in battling COVID-19 (Allobaney et al., 2022). However, long working hours in quarantine areas with inadequate and insufficient resources took a heavy toll on the nurses.
Further, due to changing policies and increased work hours, nurses face tremendous challenges personally and professionally (Wierenga and Moore, 2020). It was also due to an increased number of patients and higher absences among the health care workers due to sickness or quarantine protocols (Bernburg et al., 2021). Moreover, the fear of catching and passing the infection to family members created psychological challenges. These challenges increased nurses’ anxiety, depression, stress, and burnout. Scholars have highlighted the possibility that post-traumatic stress disorder among nurses (Mealer et al., 2009) might have harmful consequences in the long run. Thus, the pandemic exposed nurses to physical, psychological, and social challenges. Despite the odds, the nurses contributed to the society in battling the pandemic.
In the present study, we focused on work engagement for the following reasons. Work engagement is “a positive, fulfilling work-related state of mind that is characterized by vigor, dedication, and absorption” (Schaufeli et al., 2006, p. 702). For example, engaged employees achieve higher output and contribute toward team effectiveness (Turner, 2020). Engaged nurses are likely to inspire and keep up spirits in the wards, particularly during critical and low morale periods, improving patient care (Allisey et al., 2016). Further work engagement promotes employees’ psychological and physical health (Bakker and Demerouti, 2008). Scholars have attributed many factors that impact nurses ‘work engagement during the pandemic. For example, individual factors such as resilience, self-efficacy (Badu et al., 2020), feeling of belongingness, and societal factors such as support from the society (González-Sanguino et al., 2020) impact nurses’ work engagement. Improving our understanding of other factors that facilitate nurses’ work engagement during COVID-19 might help nurses, organizations, and policymakers to initiate necessary measures.
Since the nurses’ response during the pandemic was not uniform, this study aims to understand the role of personality concerning work engagement. In the present study, we focused on neuroticism, a personality dimension. Neuroticism is defined as “relatively stable individual differences in the tendency to experience negative affect (e.g., anxiety, sadness), to more readily perceive situations as threatening or stressful, and to respond quickly and strongly to such situations with greater negative affect” (Wrzus et al., 2021, p. 692). Highly neurotic individuals are likely to experience negative emotions (Eysenck, 1967), leading to extreme adverse reactions (Anicich et al., 2020). It makes individuals overly sensitive to threats, thereby susceptible to high stress (Gunthert et al., 1999), making it an essential predictor of individual health (Friedman et al., 2010). Neurotic individuals tend to convert ordinary situations into threatening situations (Widiger and Oltmanns, 2017) and react to stressful situations with distress (Swagler and Jome, 2005). This becomes a bigger problem in the COVID-19 scenario when the job of healthcare professionals is highly demanding. Nursing is a demanding occupation, and nurses experience intense emotions, such as stress and loneliness, in their workplace (Anand and Mishra, 2021).
Further, nurses would likely experience physical and mental health challenges during the COVID pandemic. The present study examined the direct and indirect effect (through perceived stress) of neuroticism on work engagement during COVID-19. Compared to an objective measure of stress, perceived stress captures the level of stress experienced by an individual; hence, it is a better predictor of employee outcomes (Cohen et al., 1983).
Moreover, patients are the beneficiaries of nurses’ work. The degree to which employees interact with the people who are touched by their work is termed beneficiary contact (Grant, 2007). It allows employees to witness the immediate effects of their work. Hence, we investigated if patient contact (termed beneficiary contact) ameliorates the adverse effect of neuroticism on work engagement. During the pandemic, healthcare employees, especially nurses, are expected to help humanity in whatever way possible. Hence, nurses abstaining from duty in this trying time are likely to get stigmatized by others. Fear of stigma denotes individuals’ perception of stigmatizing attitudes of others toward themselves (Berger et al., 2001). It involves distinguishing characteristics that devalue a person (Goffman, 1963). Therefore, it is an opposing force that might push the nurses to do their work. Hence, we further examined if the fear of stigmatization could impact neuroticism-work engagement linkage.
We draw from the job demand-resource (JD-R) model to argue the linkage between neuroticism and work engagement. The JD-R framework classifies job characteristics into two broad categories: job demands and job resources (Bakker and Demerouti, 2007). Job demands are the “physical, psychological, social, or organizational aspects of the job that require sustained physical and/or psychological (cognitive and emotional) effort or skills and are therefore associated with certain physiological and/or psychological costs” (Bakker and Demerouti, 2007, p. 312). On the other hand, job resources promote motivation and, thus, “are functional in achieving work goals; reduce job demands and the associated physiological and psychological costs; and stimulate personal growth, learning and development” (Bakker and Demerouti, 2007, p. 312).
Neuroticism describes an individual as anxious, fearful, tense, nervous, defensive, and moody (Costa and McCrae, 1992). According to Eysenck (1967), the limbic system of neurotic individuals gets overwhelmed by stressful stimuli. As a result, neurotic individuals usually convert ordinary situations into threatening situations (Widiger and Oltmanns, 2017), as they are susceptible to anxiety-inducing environmental cues and possess a pessimistic worldview (Spector et al., 2000), leading to adverse perceptions of work situations. Scholars found a positive relationship between neuroticism and job demand (Bakker et al., 2010). During the pandemic, the nurses worked under intense job demands, such as a lack of critical care resources, ICU beds and PPE suits, and the absence of a definite cure (Nathan et al., 2020). Unlike others, neurotic nurses are likely to experience these work situations as more demanding. For example, neurotic individuals are likely to experience higher fear of COVID-19 (Caci et al., 2020). As job demands include physical, psychological, social, or organizational features of a job, it strains individuals. To cope with the strain, individuals distance themselves from stain-inducing work (Connor-Smith and Flachsbart, 2007). As work engagement represents vigor, dedication, and absorption to work, we propose that during COVID-19, neurotic nurses will display reduced work engagement.
Hypothesis 1: Neuroticism is negatively related to work engagement.
According to the JD-R model, Job demands impose physiological and psychological costs (Bakker and Demerouti, 2007). COVID-19 has increased nurses’ workload due to an increased patient flow and the absence of colleagues owing to contracting COVID-19 and self-isolation due to close contact with an infected individual (Turale et al., 2020). Scholars suggest that neuroticism increases stress in two ways (Specter and Ferrari, 2000). First, neurotic individuals are more vulnerable to harmful stimuli. Scholars argue that neurotic individuals pay more attention to COVID-19-related information and are more concerned about the pandemic’s repercussions, showing higher stress levels (Liu et al., 2021). Thus, neurotic individuals respond to these events with negative emotions, further depleting their resources, and hence they indulge in ineffective behaviors (Van Jaarsveld et al., 2019). As a result, neuroticism is likely to enhance psychological strain, causing energy depletion (Penney et al., 2011).
Second, neurotic individuals tend to perceive ordinary situations as threatening. Neurotic individuals are more reactive to daily stressors (Suls et al., 1998) and react to stressful situations with intense distress (Swagler and Jome, 2005). It became a more significant problem during COVID-19 as the neurotic nurses perceived the job as highly demanding. Consequently, neuroticism is associated with negative views about self and others (Watson and Clark, 1984), leading to a wide range of adverse outcomes such as emotional exhaustion (Zellars et al., 2004) and health impairment (Bakker et al., 2010). In a highly stressful situation, individuals reduce unpleasant arousal by distancing themselves from stressors or related activities (Connor-Smith and Flachsbart, 2007), leading to disengagement (Bouchard, 2003). Hence, we posit that neurotic nurses experience enhanced stress leading to reduced work engagement.
Hypothesis 2: Perceived stress mediates the relationship between neuroticism and work engagement.
According to the JD-R model, job demands cost energy (Bakker, 2015), whereas job resources help individuals deal with these demands (Bakker and Demerouti, 2007). Moreover, the JD-R theory proposes that the interaction of job demands and resources shapes employees’ work and work outcomes. One critical job resource is contact with the beneficiaries.
Contact with beneficiaries increases task significance (Humphrey et al., 2007), interpersonal liking (Schoenrade et al., 1986), and employee motivation. Thus, beneficiary contact is a relational aspect of the job that provides employees with resources to strive for organizational goals (Vittal et al., 2022). When nurses have direct contact with the patients and can observe the effects of their work on health outcomes, they are likely to realize the criticality of their work. Extant research (Cohen and Rodgers, 2020) suggests that when the nurses were not allowed to remain in touch with their patients or could not see the changes in patient health during the pandemic, the quality of their care and engagement levels suffered. Nurses’ realization of the importance of their work is a positive resource. Thus, beneficiary contact is likely to buffer the adverse effect of neuroticism on employee engagement. On the other hand, neurotic nurses fail to realize the importance of their work and are likely to experience reduced work engagement. Based on the above discussion, we propose the following hypothesis.
Hypothesis 3: Beneficiary contact moderates the negative relationship between neuroticism and work engagement, such that the relationship is more negative when beneficiary contact is low.
The social context of work influences individuals’ perceptions of the job they perform (Gergen, 2009). The pandemic made the nurses indispensable. The nurses contributed to society in an acute resource constraint environment. Due to the patient interface, they expose themselves to the virus infection leading to significant risk to their life and threat of contagion to family members. However, being a nurse and not contributing during the pandemic was devalued in society. A stigma is an “attribute or a characteristic that conveys a social identity that is devalued in a particular context, which includes being the target of negative stereotypes, being rejected socially, being discriminated against” (Crocker et al., 1998, p.505). Studies about the stigma against health care providers, such as the nurses during COVID-19, are minimal (Nashwan et al., 2022). Though there are many drivers of stigma, the absence of nurses from their job during the pandemic is a stigma worth exploring. As stigma represents social rejection, nurses are likely to experience the fear of stigma. It involves a distinguishing characteristic that induces the fear of being devalued in a social context (Goffman, 1963). Drawing from the JD-R model, Barbier et al. (2013) argued that stigmatization is a kind of demand like job demand. Hence, in the workplace, the fear of stigma is likely to increase job demand impacting individuals’ attachment, attitude to work (Shantz and Booth, 2014), and turnover intention (Pinel and Paulin, 2005).
Similarly, in a society, nurses are likely to experience the fear of stigma. The nurses are likely to experience more negative interpersonal treatments (Singletary and Hebl, 2009) due to avoiding their duty when there is an intense need. Major and O’Brien (2005) suggested that stigma elicits voluntary (e.g., coping efforts) and involuntary (e.g., anxiety, working memory load) responses threatening one’s identity. Neurotic individuals are likely to experience enhanced fear of stigma (Cyders and Smith, 2008). The fear of stigma may push the neurotic nurses to their workplace, but it is unlikely to engage them with their work due to perceived job demand and its adverse impact on mental and physical well-being (Barbier et al., 2013). Further, studies found that nurses who treat COVID-19 patients experience an adverse impact on their professional self-concept (Allobaney et al., 2022), which would have negatively impacted their work engagement and patient care (Randle and Arthur, 2007).
Hypothesis 4: The fear of stigma moderates the relationship between neuroticism and work engagement, such that the relationship is more negative when the fear of stigma is high.
The hypothesized model is presented in Figure 1.
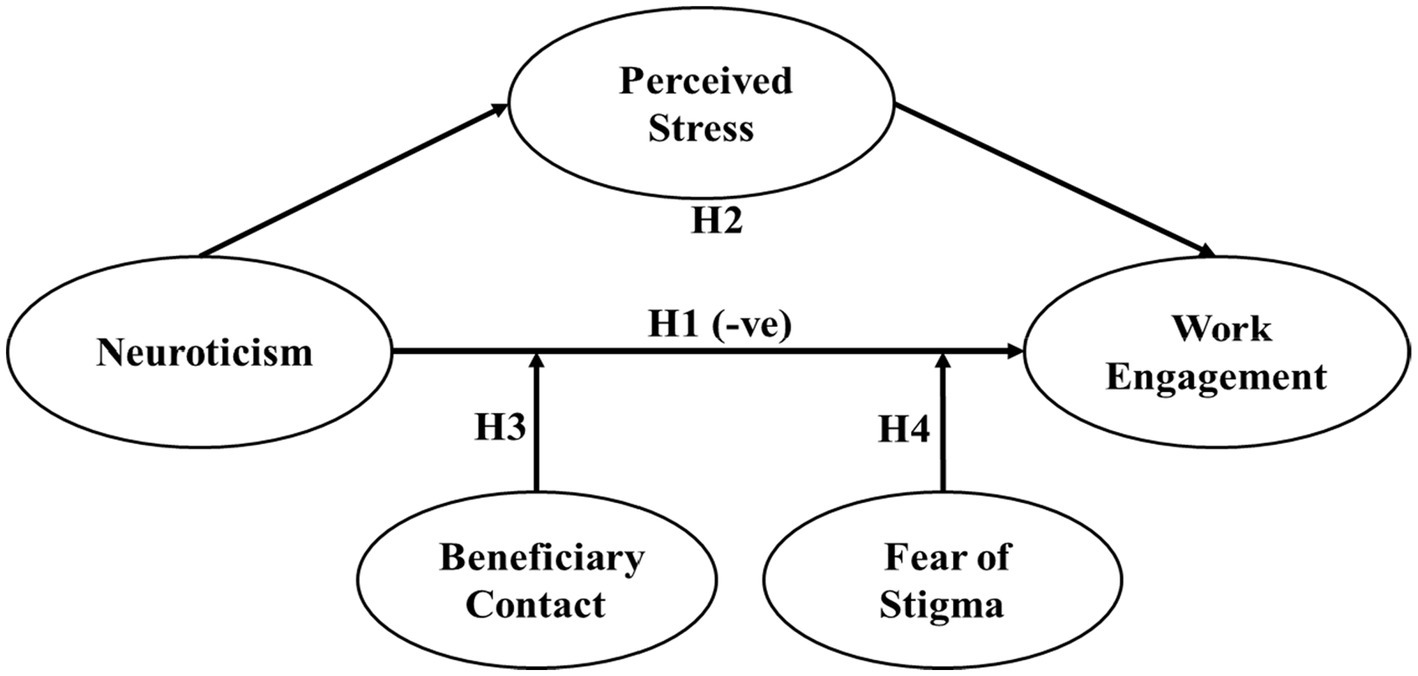
Figure 1. Hypothesized model. H1 indicates a negative relationship between neuroticism and work engagement; H2 indicates the indirect effect of neuroticism on work engagement through perceived stress. H3 and H4 indicate the moderation effect of beneficiary contact and fear of stigma, respectively, on the negative relationship between neuroticism and work engagement.
We collected the data after getting approval from the institutional review board. All the participants of the study provided oral consent before answering the questionnaire. We contacted 900 nurses, of which 790 agreed to participate in the study. Finally, we received 752 forms from the nurses. We contacted the nurses during their non-work time with prior appointments. Hence, there was no need to give reminders. After data cleaning, we included 657 usable responses from the nurses in the study. Of the 657 respondents, 445 were females and 212 were males. We denied the participation of some nurses in the survey as they had gone through some personal tragedy in the said period, so participating in the survey would have been emotionally exhausting for them. The required number of participants for performing linear regression using six predictors was observed to be 242 (effect size = 0.15, α = 0.01, power = 0.90) using GPower 3.1.9.4 (Faul et al., 2007).
We defined three explicit inclusion and exclusion criteria. First, we included only those nurses who had worked |in the COVID-19 ward during the second wave in India (March–June 2021). During this period, India reported at least 50,000 cases daily, with a peak of over 400,000 cases in May. We excluded the nurses from the study who did not serve in the COVID ward. Second, the nurses should be full-time practicing nurses and not student apprentices in their respective hospitals. Third, the hospitals should be in bigger cities, as bigger cities were the most affected in the country and faced a shortage of beds and medical facilities. We collected data from the nurses working in different hospitals in Delhi, Bangalore, Kolkata, Chennai, Ahmedabad, Mumbai, Pune, Hyderabad, and Lucknow.
In survey-based research, scholars have proposed multiple approaches to control the possibility of common method variance (Podsakoff et al., 2003). Maintaining a temporal separation while collecting the data is one of the powerful approaches. However, there is no specific accepted time interval between different phases of data collection (Cole and Maxwell, 2003). However, in recent scholarly work, researchers have maintained a temporal separation of 2 weeks to control the common method bias without losing the effect of the predictor on the outcome (Raja et al., 2018; Liekefett et al., 2022). Consistent with the existing practice, we followed a temporal separation of 2 weeks in our data collection. In phase 1, we captured age, gender, marital status, type of work, work experience, the city of work, neuroticism, and fear of stigma. In phase 2, we captured work experience, prosocial motivation, work engagement, beneficiary contact, and perceived stress. We used the respondent’s name, mobile number, and experience to match phase 1 data with phase 2. We collected the responses on a five-point scale ranging from 1 (Never/Strongly Disagree) to 5 (Always/Strongly Agree).
We used the eight-item scale of the Big-5 inventory to capture neuroticism (John and Srivastava, 1999). A sample item is “I am neither relaxed nor can handle stress well.” Studies have used this scale to measure neuroticism in the Indian context (Srivastava and Bajpai, 2020).
We adapted four items from the measures developed by Grant (2012). A sample item reads, “My job involves a great deal of interaction with the patients.” Studies have used this scale in the Indian context (Vittal et al., 2022).
We wanted to measure the fear of the stigma associated with not going to work during COVID-19. Hence, we measured the fear of stigma by adapting the items of the occupational stigma scale (Schaubroeck et al., 2018). A sample item reads, “Most people would have disrespected me if I had not gone to work during the pandemic.”
We measured perceived stress using the scale developed by Cohen et al. (1983). The items were adapted to fit into our context. A sample item is “In the last week, how often have you found that you could not cope with all the things that you had to do?.” The scale was used and validated in the Indian context (see Grover et al., 2020).
We used the 9-item Utrecht Work Engagement Scale (version-9) to measure work engagement (Schaufeli et al., 2006). The scale has three dimensions, namely visor, dedication, and absorption. A sample item is “At my work, I feel bursting with energy.” Studies have used this scale in the Indian context (see Alok, 2013).
We controlled for age, gender, marital status, type of work, work experience, city, and prosocial motivation as they are related to work engagement (Othman and Nasurdin, 2013; Goštautaitė and Bučiūnienė, 2015).
Before running the analyzes, we checked for convergent and discriminant validity. We conducted confirmatory factor analysis using structural equation modeling. The fit indices for a five-factor model were robust (CFI = 0.933, IFI = 0.933, TLI = 0.921, SRMR = 0.06, RMSEA = 0.040, & CMIN/df = 2) and better than the one factor, two factor, three factor and four factor models. For convergent validity, we relied on the Composite reliability (CR) scores following the recommendations by Fornell and Larcker (1981). Extant research (e.g., Lam, 2012) suggests that composite reliability scores higher than 0.70 is sufficient to establish convergent validity. The composite reliability for all the scales was greater than 0.80, establishing convergent validity. We further found that the AVE (average variance extracted) scores were greater than the square of the bivariate correlations, establishing discriminant validity (Fornell and Larcker, 1981). Apart from collecting the data at two time periods, we used an established marker variable (i.e., attitude toward blue color) to minimize common method variance (Miller and Simmering, 2022).
Table 1 presents the mean, standard deviation, bivariate correlations, and reliability scores of the study variables. We found a negative correlation between neuroticism and work engagement (r = −0.17, p < 0.001). Further, we found that neuroticism is positively related to perceived stress (r = 0.28, p < 0.001).
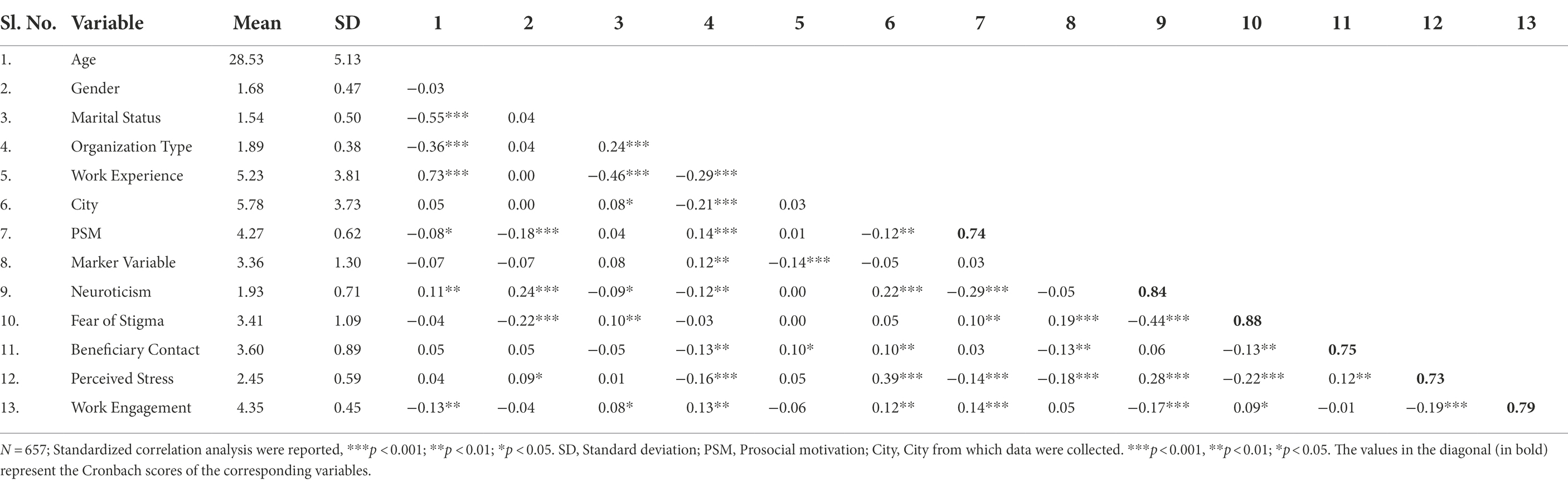
Table 1. Means, standard deviations, and zero-order correlations among the study variables.
We eliminated the effect of control variables and the marker variable while regressing work engagement with neuroticism (see Table 2). We found a significant negative relationship (β = 0.16, p < 0.001, ΔR2 = 0.02). Hence, hypothesis 1 was supported.
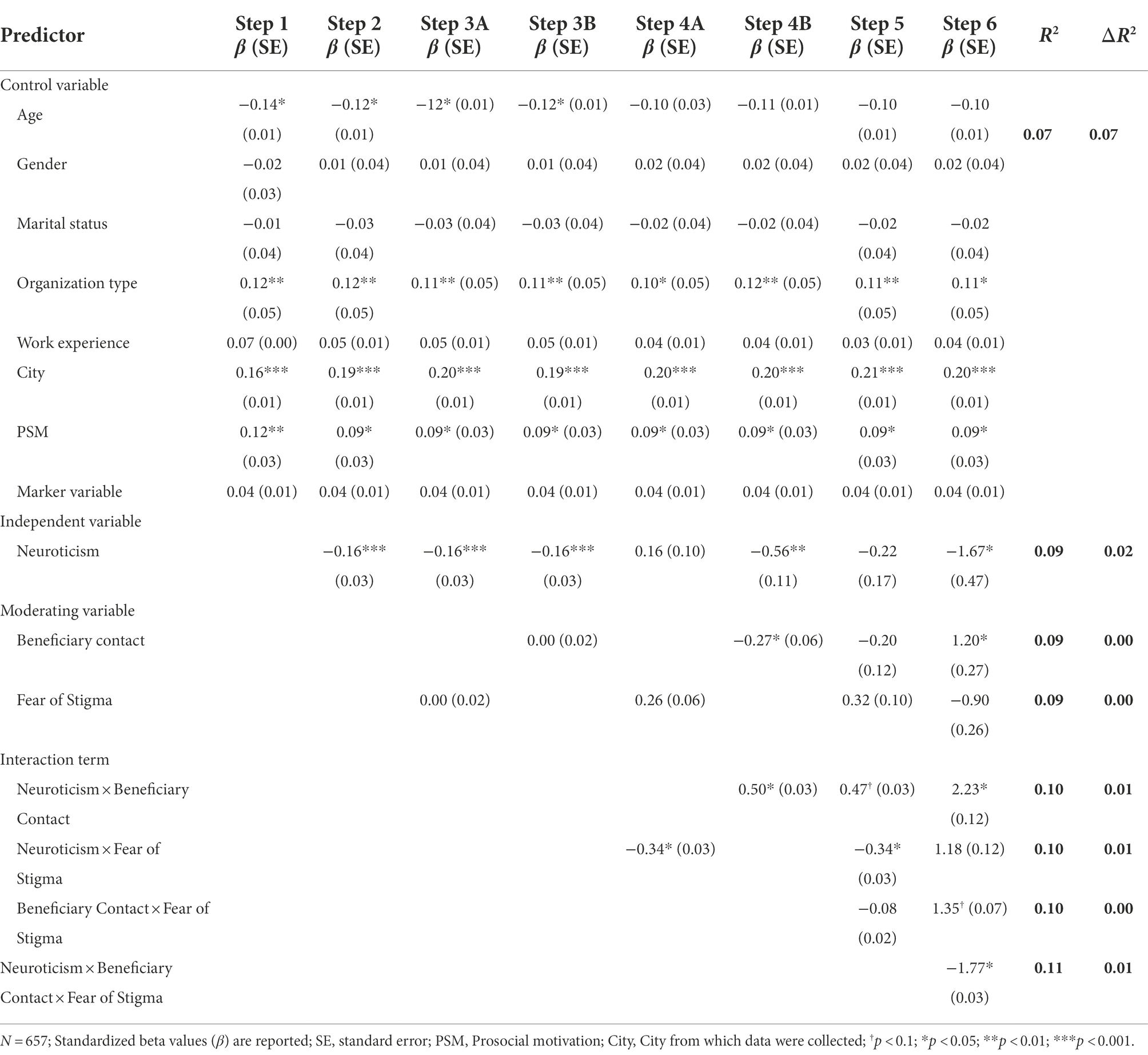
Table 2. Moderation effect of fear of stigma and beneficiary contact on neuroticism-work engagement relationship.
We tested for the mediation effect of perceived stress on the relationship between neuroticism and work engagement using Model-4 of PROCESS Macro (Preacher and Hayes, 2008). The indirect effect of neuroticism on work engagement was statistically significant based on 5,000 bootstrap samples (see Table 3). The bootstrapping at 95% confidence intervals does not include zero (−0.04, −0.02). We further conducted structural equation modeling to test the model fit of the mediation effect. The fit indices indicate the robustness of the model (GFI = 0.926, IFI = 0.939, TLI = 0.924, SRMR = 0.06, RMSEA = 0.043, & CMIN/df = 2.2). Hence hypothesis 2 was supported.
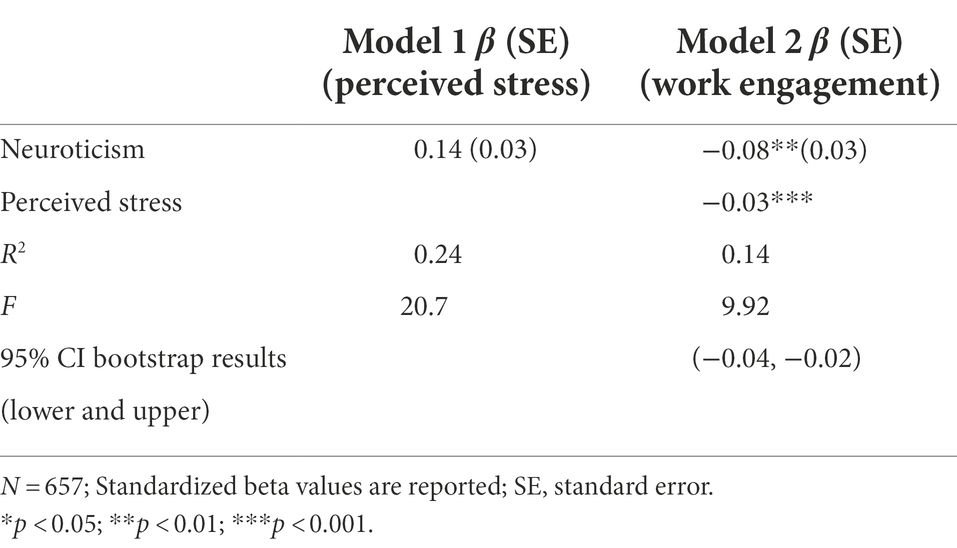
Table 3. Mediation effect of perceived stress on neuroticism-work engagement relationship.
We conducted a regression analysis to test the moderation effect of beneficiary contact on the neuroticism-work engagement relationship. Our results (see Table 2) indicated a significant positive effect of the interaction term (neuroticism*beneficiary contact) on work engagement (β = 0.50, p < 0.05, ΔR2 = 0.01). The interaction effect explained an additional 1 % variance after controlling the effect of control variables, marker variable, independent variable, and moderator. We plotted the relationship between neuroticism and work engagement for high and low values of beneficiary contact (see the graph in Figure 2).
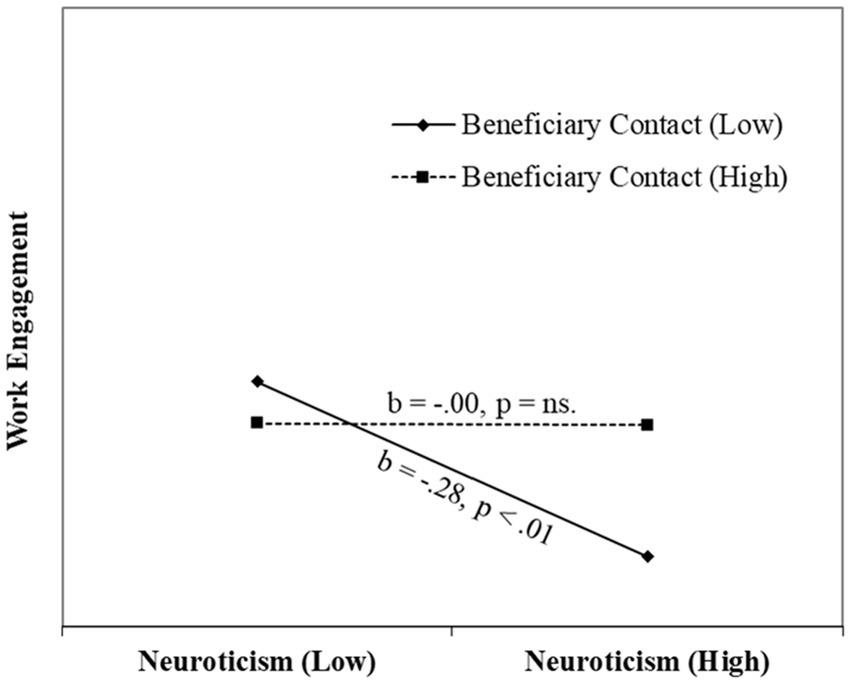
Figure 2. Interaction effect of beneficiary contact on Neuroticism–Work Engagement relationship.
The graph indicates the slope of the regression line is more negative when beneficiary contact is low. Thus, hypothesis 3 was supported. We repeated the above analysis to test the moderation effect of fear of stigma on the above relationship. As shown in Table 2, our results indicated that the fear of stigma has a significant moderation effect (β = −0.34, p < 0.05, ΔR2 = 0.01) on the relationship between neuroticism and work engagement. We plotted the relationship between neuroticism and work engagement for high and low values of perceived stigma (see the graph in Figure 3).

Figure 3. Interaction effect of perceived stigma on Neuroticism–Work Engagement relationship.
The graph indicates the slope of the regression line is more negative when fear of stigma is high. Hence, hypothesis 4 was supported.
We conducted three additional analyzes to test the robustness of our findings. One, we conducted the analyzes without the control variables. We found consistent results. Second, we conducted the moderated mediation analysis, and the findings support our hypotheses. Third, we conducted the effect of both moderators on the relationship between neuroticism and work engagement. The analysis is provided in Table 3 (see Steps 5 and 6). We found that the interaction term (i.e., the interaction of neuroticism, beneficiary contact, and the fear of stigma) is significantly related to work engagement (p < 0.05; ΔR2 = 0.01) after controlling the effect of other relevant variables. We further presented the 3-way interaction graph in Figure 4.
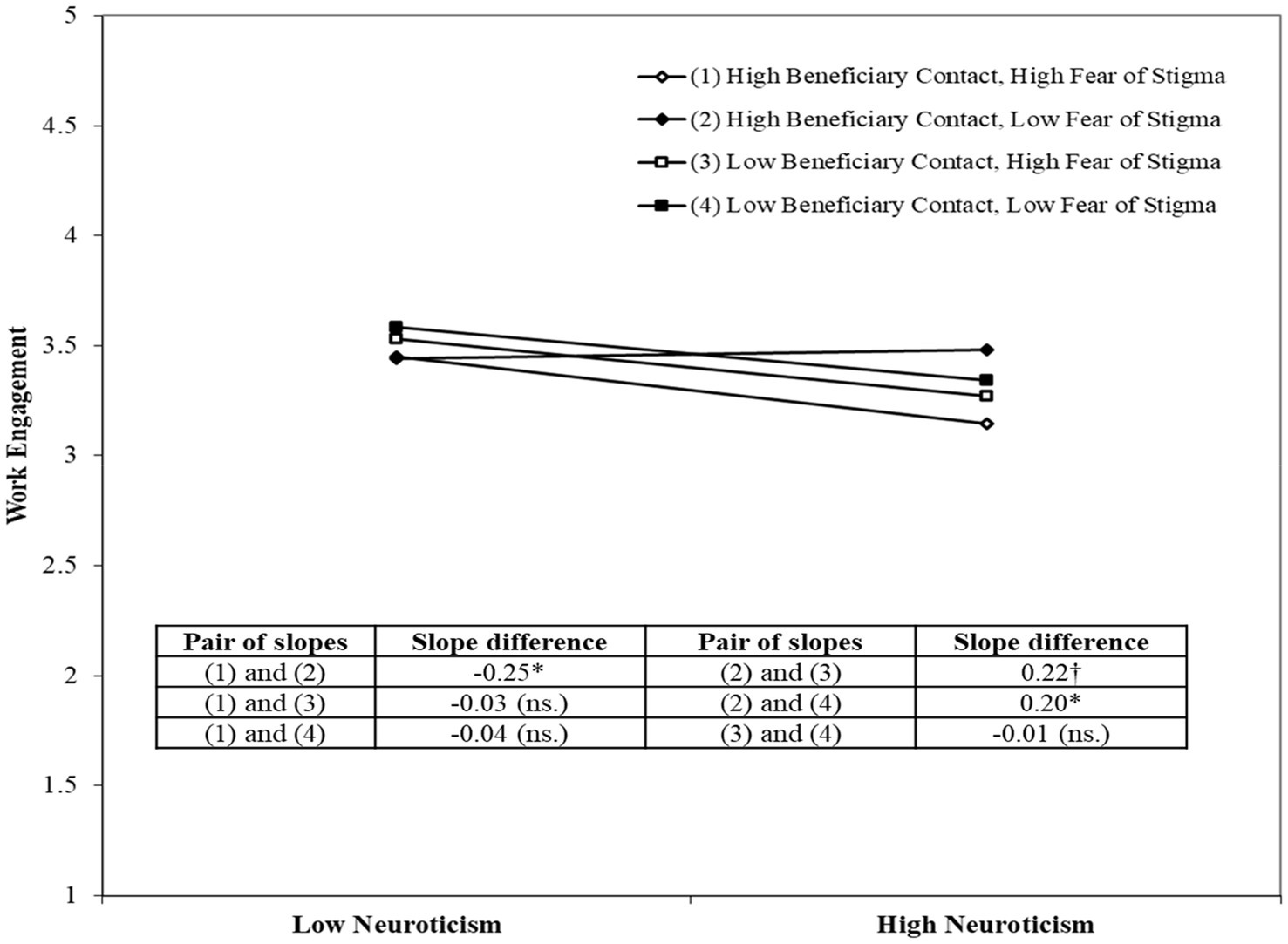
Figure 4. Interaction effect of beneficiary contact and fear of stigma on Neuroticism–Work Engagement relationship.
We analyzed the linkage between neuroticism and work engagement by comparing responses having high beneficiary contact (and low fear of stigma) with low beneficiary contact (and high fear of stigma). We found the neuroticism-engagement linkage is more negative for low beneficiary contact (with high fear of stigma) compared to the reverse scenario (Slope difference: 0.22, p < 0.1). The finding is consistent with our arguments for hypotheses 3 and 4. We further compared the above linkage for respondents with low fear of stigma (and having high and low beneficiary contact). The findings indicate that in situations of low fear of stigma, the high beneficiary contact nullifies the adverse consequence of neuroticism on engagement (slope difference: 0.20, p < 0.05). The finding supports hypothesis 3. However, in situations of high fear of stigma, the negative effect of neuroticism on engagement does not get impacted by high or low beneficiary contact (slope difference: −0.03, p = ns.).
We further checked the impact of fear of stigma on the neuroticism-engagement relationship for respondents having high beneficiary contact. Our findings indicate that in situations of high beneficiary contact, the neuroticism-engagement linkage becomes more negative for high fear of stigma (slope change: −0.25, p < 0.05). However, in situations of low beneficiary contact, the fear of stigma (irrespective of high or low) does not impact the neuroticism-engagement linkage (slope difference: −0.01, p = ns.). The findings provide an additional layer of interpretation to hypothesis 4 by providing the situation when fear of stigma becomes critical. Finally, we checked the linkage between neuroticism and engagement when both fear of stigma and beneficiary contact are high compared to the situation when both are low. We found the slope difference is insignificant (slope difference: −0.04, p = ns.). The findings support complementarity, i.e., the adverse effect of high fear of stigma is complemented by high beneficiary contact.
The health crisis due to the pandemic poses threats to individual lives and society at large. Scholars have argued that along with contextual conditions, individual dispositions such as neuroticism could be a source of adverse outcomes during the pandemic (Caci et al., 2020). Our study brings two contradictory aspects to explain the work engagement of nurses. On the one hand, nurses as trained to help patients recover from medical ailments. Hence, nurses are likely to come forward to contribute to healthcare services during the pandemic.
On the other hand, neurotic individuals experience negative affect (Kroencke et al., 2020), fear responses (Sep et al., 2019), and undergo stressful life experiences (Penley and Tomaka, 2002). As a result, they are likely to disengage from stressful situations, such as attending the COVID-19 patients. Hence, it is crucial to understand the approach of neurotic nurses to their work during the pandemic. Though studies explain the effect of neuroticism on individual outcomes, such as stress, loneliness, and boredom during the pandemic (Caci et al., 2020; Ikizer et al., 2022), we focused on organizational outcomes such as work engagement. Nurses’ work engagement has societal implications and was critical during the pandemic. We found that neurotic nurses display reduced engagement in their work directly and indirectly through increased stress perception. Our results indicate a negative association between stress and work engagement among Indian nurses, which is in line with the research undertaken in other countries like Germany (Bernburg et al., 2021), China (Zhang et al., 2021), and Spain (Allande-Cussó et al., 2021). These findings highlight the importance of keeping stress low among employees to increase their work engagement, irrespective of the context or culture.
Further, we selected beneficiary contact and the fear of stigma (for not attending the job) as moderators of the above relationship. We selected the above two factors for the following reason. Beneficiary contact might pull (motivate) the nurses toward the job, whereas the fear of stigma for not attending the job might push (force) them to work but disengage from work itself. We found beneficiary contact reduces the negative linkage between neuroticism and work engagement. Further, the fear of stigma increases the negative relationship between neuroticism and work engagement. The results reveal that neurotic people are more likely to disengage from work due to their personality traits, i.e., the tendency to focus on negative aspects during the pandemic. In the additional analysis we further tested the relative importance of push (fear of stigma) and pull (beneficiary contact) factors in explaining the neuroticism-work engagement relationship. Our findings highlighted the importance of both the factors. Firstly, we found that in cases of low fear stigma, high beneficiary contact nullifies the negative effect of personality trait of neuroticism on work engagement, and thus increases work engagement. Studies so far (e.g., Cernasev et al., 2021) have highlighted the importance of organizational policies and peer support in reducing stigma (push factor) to improve patient care. Our study highlights the additional advantage of beneficiary contact (pull factor) even in absence of push factors. Secondly, we found the negative effect of low beneficiary contact was offset by low fear of stigma and vice versa in the neuroticism-work engagement relationship. Thus, our study provides support in favor of complementarity of both push and pull factors. This is consistent with extant research highlighting that push and pull factors co-exist among healthcare employees (Mano-Negrin and Kirschenbaum, 1999).
Studies in psychology have examined the adverse impact of neuroticism during the pandemic. However, studies on neuroticism in nurses are sparse. We examined the effect of neuroticism on their work engagement during the pandemic. Extant research (Hashish and Ashour, 2020) emphasized the importance of the push-pull factors in studies relating to nurses. Our study highlights the individual and combined influence of push (fear of stigma) and pull (beneficiary contact) factors on the relationship of neuroticism with work engagement during the pandemic. The stigma literature is well developed both within and outside the organization. However, the interplay of outside stigma on employee behavior is relatively unaddressed. We extended the stigma literature by constructing a new concept, fear of stigma. We focused on the stigma associated with not going to work rather than the stigma associated with work. Our study highlighted that the fear of stigma is a more potent force pushing nurses toward their work.
Our study demonstrated both the pull and push factors and their impact on nurses’ work and work. The pull factor (beneficiary contact) has a positive effect: it minimizes the adverse effect of neuroticism on work engagement. The push factor (fear of stigma) has an adverse effect. The fear pushes the nurses to do their work but reduces their work engagement. We further analyzed the interaction of push and pull factors to explain the neuroticism-work engagement relationship. We found that in situations of low fear of stigma, the high beneficiary contact nullifies the adverse consequence of neuroticism on engagement. But the positive effect of beneficiary contact does not hold when the fear of stigma is high.
Further, we found that in situations of high beneficiary contact, the neuroticism-engagement linkage becomes more negative for high fear of stigma. But in situations of low beneficiary contact, the fear of stigma loses its effect. Our study thus provides evidence of the complementarity of beneficiary contact (pull factor) and the fear of stigma (push factor). Our study further highlights the importance of fear of stigma in patient interface occupations. Traditionally the literature has focused on the factors within the organization. To understand their interplay with neuroticism in predicting work engagement, we have considered two factors outside the organization: positive (beneficiary contact) and negative (the fear of stigma). Though scholars have highlighted the social aspects of the job (Grant, 2012), the literature has predominantly focused on the positive aspects of the job. Our findings extend the job characteristics model by highlighting the job’s positive and negative social aspects.
Our study proposes several inputs to the practitioners and policymakers. One, the study indicates that mere contact with beneficiaries mitigates the negative effect of neuroticism on work engagement. Organizations may find out suitable mechanisms to facilitate beneficiary contact with their nurses. Our findings indicated that pull factors are better than push factors in reducing the adverse effect of personality factors on work engagement. Organizations may find ways to motivate nurses rather than induce fear for their work engagement. Our recommendation to organizations is to focus on improving working conditions, and professional situations as these would improve the quality of nurses’ lives and their work engagement (Giménez-Espert et al., 2020).
Our study found that factors beyond the organization, i.e., societal factors, can influence employee engagement. Hence, policymakers can play a significant role in enhancing employee engagement. Communicating to people about the contributions of nurses and recognizing their efforts would transform the fear of stigma (push factor) into a call of duty (pull factor). Our study thus raises an important question. Why the responsibility for employee engagement lies within the organization? Policymakers may communicate many factors related to nurses’ work, such as the challenging work conditions (e.g., acute resource constraints), the threat of contamination, and long working hours, especially during critical times. It might bring dignity to their work (e.g., nursing is considered dirty work). The policymakers may find ways to pull the organizations for a societal cause rather than push them to deliver.
Our study has limitations. We conducted the study on a sample of Indian nurses. Unlike India, nurses in developed countries enjoy better pay and higher status. Hence, the findings may be helpful in countries having similar economic and social backgrounds. The literature supports that organizational systems and processes drive employee engagement. Future studies may explore if reward and recognition minimize the negative effect of neuroticism on work engagement. Studies have argued that in addition to beneficial contact, prosocial impact and worth of work influence frontline employees (Grant, 2012). Future studies might extend our study to examine the interplay of prosocial motivation with neuroticism in explaining work engagement in critical situations. Our findings indicate that females are more prone to the fear of stigma. Future studies may examine our model for the gender groups. We collected the data in two time periods during the pandemic. Though we have a solid theoretical underpinning, given the study’s cross-sectional nature, unequivocal causality cannot be established.
The present study is one of the initial studies that explained neuroticism’s direct and indirect effects on nurses’ work engagement. We identified two critical factors (pull and push) that influenced the neuroticism-work engagement relationship. Our work highlighted an essential yet neglected issue: the role of societal factors on employee engagement. Our study demonstrated the criticality of social aspects of work on nurses’ work engagement. By demonstrating the criticality of organizational actions (fostering beneficiary contact) and the broader social fabric (minimizing the fear of stigma), our study brings the nurses to the center of the discussion.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Institutional Review Board, IIM Indore. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
MV, SM, and HR: conceptualization, methodology, validation, software, formal analysis, writing—original draft, and writing—review and editing. AP: review and editing. All authors contributed to the article and approved the submitted version.
The authors declare that this study received funding from GIZ, GmbH, India. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Allande-Cussó, R., García-Iglesias, J. J., Ruiz-Frutos, C., Domínguez-Salas, S., Rodríguez-Domínguez, C., and Gómez-Salgado, J. (2021). Work engagement in nurses during the COVID-19 pandemic: A cross-sectional study. Healthcare 9, 253–263.
Allisey, A., Rodwell, J., and Noblet, A. (2016). An application of an extended effort-reward imbalance model to police absenteeism behaviour. Pers. Rev. 45, 663–680. doi: 10.1108/PR-06-2014-0125
Allobaney, N. F., Eshah, N. F., Abujaber, A. A., and Nashwan, A. J. J. (2022). Professional self-concept and self-confidence for nurses dealing with COVID-19 patients. J. Pers. Med. 12, 134–147. doi: 10.3390/jpm12020134
Alok, K. (2013). Work engagement in India: a factorial validation study of UWES-9 scales. Manage. Labour Stud. 38, 53–62. doi: 10.1177/0258042X13491478
Anand, P., and Mishra, S. K. (2021). Linking core self-evaluation and emotional exhaustion with workplace loneliness: does high LMX make the consequence worse? Int. J. Hum. Resour. Manag. 32, 2124–2149. doi: 10.1080/09585192.2019.1570308
Anicich, E. M., Foulk, T. A., Osborne, M. R., Gale, J., and Schaerer, M. (2020). Getting back to the “new normal”: autonomy restoration during a global pandemic. J. Appl. Psychol. 105, 931–943. doi: 10.1037/apl0000655
Badu, E., O’Brien, A. P., Mitchell, R., Rubin, M., James, C., McNeil, K., et al. (2020). Workplace stress and resilience in the Australian nursing workforce: a comprehensive integrative review. Int. J. Ment. Health Nurs. 29, 5–34. doi: 10.1111/inm.12662
Bakker, A. B. (2015). A job demands-resources approach to public service motivation. Public Adm. Rev. 75, 723–732. doi: 10.1111/puar.12388
Bakker, A. B., Boyd, C. M., Dollard, M., Gillespie, N., Winefield, A. H., and Stough, C. (2010). The role of personality in the job demands-resources model: a study of Australian academic staff. Career Dev. Int. 15, 622–636. doi: 10.1108/13620431011094050
Bakker, A. B., and Demerouti, E. (2007). The job demands-resources model: state of the art. J. Manag. Psychol. 22, 309–328. doi: 10.1108/02683940710733115
Bakker, A. B., and Demerouti, E. (2008). Towards a model of work engagement. Career Dev. Int. 13, 209–223. doi: 10.1108/13620430810870476
Barbier, M., Dardenne, B., and Hansez, I. (2013). A longitudinal test of the job demands-resources model using perceived stigma and social identity. Eur. J. Work Organ. Psy. 22, 532–546. doi: 10.1080/1359432X.2012.698056
Berger, B. E., Ferrans, C. E., and Lashley, F. R. (2001). Measuring stigma in people with HIV: psychometric assessment of the HIV stigma scale. Res. Nurs. Health 24, 518–529. doi: 10.1002/nur.10011
Bernburg, M., Hetzmann, M. S., Mojtahedzadeh, N., Neumann, F. A., Augustin, M., Harth, V., et al. (2021). Stress perception, sleep quality and work engagement of German outpatient nurses during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 19, 313–336. doi: 10.3390/ijerph19010313
Bouchard, G. (2003). Cognitive appraisals, neuroticism, and openness as correlates of coping strategies: an integrative model of adaptation to marital difficulties. Can. J. Behav. Sci. 35, 1–12. doi: 10.1037/h0087181
Caci, B., Miceli, S., Scrima, F., and Cardaci, M. (2020). Neuroticism and fear of COVID-19. The interplay between boredom, fantasy engagement, and perceived control over time. Front. Psychol. 11:574393. doi: 10.3389/fpsyg.2020.574393
Cernasev, A., Desselle, S., Hohmeier, K. C., Canedo, J., Tran, B., and Wheeler, J. (2021). Pharmacy technicians, stigma, and compassion fatigue: front-line perspectives of pharmacy and the US opioid epidemic. Int. J. Environ. Res. Public Health 18, 6231–6241. doi: 10.3390/ijerph18126231
Choi, K. R., Skrine Jeffers, K., and Cynthia Logsdon, M. (2020). Nursing and the novel coronavirus: risks and responsibilities in a global outbreak. J. Adv. Nurs. 76, 1486–1487. doi: 10.1111/jan.14369
Cohen, S., Kamarck, T., and Mermelstein, R. (1983). A global measure of perceived stress. J. Health Soc. Behav. 24, 385–396. doi: 10.2307/2136404
Cohen, J., and Rodgers, Y. (2020). Contributing factors to personal protective equipment shortages during the COVID-19 pandemic. Prev. Med. 141:106263. doi: 10.1016/j.ypmed.2020.106263
Cole, D. A., and Maxwell, S. E. (2003). Testing mediational models with longitudinal data: questions and tips in the use of structural equation modeling. J. Abnorm. Psychol. 112, 558–577. doi: 10.1037/0021-843X.112.4.558
Connor-Smith, J. K., and Flachsbart, C. (2007). Relations between personality and coping: a meta-analysis. J. Pers. Soc. Psychol. 93, 1080–1107. doi: 10.1037/0022-3514.93.6.1080
Costa, P. T., and McCrae, R. R. (1992). The five-factor model of personality and its relevance to personality disorders. J. Personal. Disord. 6, 343–359. doi: 10.1521/pedi.1992.6.4.343
Crocker, J., Major, B., and Steele, C. (1998). “Social stigma,” in Handbook of Social Psychology. eds. D. Gilbert, S. T. Fiske, and G. Lindzey. 4th Edn. (Boston: McGraw-Hill), 504–553.
Cyders, M. A., and Smith, G. T. (2008). Emotion-based dispositions to rash action: positive and negative urgency. Psychol. Bull. 134, 807–828. doi: 10.1037/a0013341
Faul, F., Erdfelder, E., Lang, A.-G., and Buchner, A. (2007). G⁎power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 39, 175–191. doi: 10.3758/BF03193146
Fornell, C., and Larcker, D. F. (1981). Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 18, 39–50. doi: 10.1177/002224378101800104
Friedman, H. S., Kern, M. L., and Reynolds, C. A. (2010). Personality and health, subjective well-being, and longevity. J. Pers. 78, 179–216. doi: 10.1111/j.1467-6494.2009.00613.x
Gergen, K. J. (2009). Realities and relationships: Soundings in social constructionism. Cambridge, UK: Harvard University Press.
Giménez-Espert, M. C., Prado-Gascó, V., and Soto-Rubio, A. (2020). Psychosocial risks, work engagement, and job satisfaction of nurses during COVID-19 pandemic. Front. Public Health 8:566896. doi: 10.3389/fpubh.2020.566896
González-Sanguino, C., Ausín, B., Castellanos, M. Á., Saiz, J., López-Gómez, A., Ugidos, C., et al. (2020). Mental health consequences during the initial stage of the 2020 coronavirus pandemic (COVID-19) in Spain. Brain Behav. Immunity 87, 172–176. doi: 10.1016/j.bbi.2020.05.040
Goštautaitė, B., and Bučiūnienė, I. (2015). Work engagement during lifespan: the role of interaction outside the organization and task significance. J. Vocat. Behav. 89, 109–119. doi: 10.1016/j.jvb.2015.05.001
Grant, A. M. (2007). Relational job design and the motivation to make a prosocial difference. Acad. Manag. Rev. 32, 393–417. doi: 10.2307/20159308
Grant, A. M. (2012). Leading with meaning: beneficiary contact, prosocial impact, and the performance effects of transformational leadership. Acad. Manag. J. 55, 458–476. doi: 10.5465/amj.2010.0588
Grover, S., Sahoo, S., Mehra, A., Avasthi, A., Tripathi, A., Subramanyan, A., et al. (2020). Psychological impact of COVID-19 lockdown: an online survey from India. Indian J. Psychiatry 62, 354–362. doi: 10.4103/psychiatry.IndianJPsychiatry_427_20
Gunthert, K. C., Cohen, L. H., and Armeli, S. (1999). The role of neuroticism in daily stress and coping. J. Pers. Soc. Psychol. 77, 1087–1100. doi: 10.1037/0022-3514.77.5.1087
Hashish, E. A., and Ashour, H. M. (2020). Determinants and mitigating factors of the brain drain among Egyptian nurses: a mixed-methods study. J. Res. Nurs. 25, 699–719. doi: 10.1177/1744987120940381
Hoogendoorn, M. E., Brinkman, S., Bosman, R. J., Haringman, J., de Keizer, N. F., and Spijkstra, J. J. (2021). The impact of COVID-19 on nursing workload and planning of nursing staff on the intensive care: a prospective descriptive multicenter study. Int. J. Nurs. Stud. 121:104005. doi: 10.1016/j.ijnurstu.2021.104005
Humphrey, S. E., Nahrgang, J. D., and Morgeson, F. P. (2007). Integrating motivational, social, and contextual work design features: a meta-analytic summary and theoretical extension of the work design literature. J. Appl. Psychol. 92, 1332–1356. doi: 10.1037/0021-9010.92.5.1332
Ikizer, G., Kowal, M., Aldemir, İ. D., Jeftić, A., Memisoglu-Sanli, A., Najmussaqib, A., et al. (2022). Big five traits predict stress and loneliness during the COVID-19 pandemic: evidence for the role of neuroticism. Personal. Individ. Differ. 190:111531. doi: 10.1016/j.paid.2022.111531
John, O. P., and Srivastava, S. (1999). “The big five trait taxonomy: history, measurement, and theoretical perspectives,” in Handbook of Personality: Theory and Research (2nd Edn). eds. L. Pervin and O. P. John (New York: Guilford), 102–138.
Kroencke, L., Geukes, K., Utesch, T., Kuper, N., and Back, M. D. (2020). Neuroticism and emotional risk during the COVID-19 pandemic. J. Res. Pers. 89:104038. doi: 10.1016/j.jrp.2020.104038
Lam, L. W. (2012). Impact of competitiveness on ‘salespeople’s commitment and performance. J. Bus. Res. 65, 1328–1334. doi: 10.1016/j.jbusres.2011.10.026
Liekefett, L., Christ, O., and Becker, J. C. (2022). Can conspiracy beliefs be beneficial? Longitudinal linkages between conspiracy beliefs, anxiety, uncertainty aversion, and existential threat. Personal. Soc. Psychol. Bull. 14616722110609. doi: 10.1177/01461672211060965
Liu, S., Lithopoulos, A., Zhang, C. Q., Garcia-Barrera, M. A., and Rhodes, R. E. (2021). Personality and perceived stress during COVID-19 pandemic: testing the mediating role of perceived threat and efficacy. Personal. Individ. Differ. 168:110351. doi: 10.1016/j.paid.2020.110351
Major, B., and O’Brien, L. T. (2005). The social psychology of stigma. Annu. Rev. Psychol. 56, 393–421. doi: 10.1146/annurev.psych.56.091103.070137
Mano-Negrin, R., and Kirschenbaum, A. (1999). Push and pull factors in medical employees turnover decisions: the effect of a careerist approach and organizational benefits on the decision to leave the job. Int. J. Hum. Resour. Manag. 10, 689–702. doi: 10.1080/095851999340341
Mealer, M., Burnham, E. L., Goode, C. J., Rothbaum, B., and Moss, M. (2009). The prevalence and impact of post-traumatic stress disorder and burnout syndrome in nurses. Depress. Anxiety 26, 1118–1126. doi: 10.1002/da.20631
Miller, B. K., and Simmering, M. J. (2022). Attitude toward the color blue: an ideal marker variable. Organ. Res. Methods, 109442812210753. doi: 10.1177/10944281221075361
Nashwan, A. J., Valdez, G. F. D., al-Fayyadh, S., al-Najjar, H., Elamir, H., Barakat, M., et al. (2022). Stigma towards health care providers taking care of COVID-19 patients: a multi-country study. Heliyon 8:e09300. doi: 10.1016/j.heliyon.2022.e09300
Nathan, N., Prevost, B., and Corvol, H. (2020). Atypical presentation of COVID-19 in young infants. Lancet 395, 1481–1483. doi: 10.1016/S0140-6736(20)30980-6
Othman, N., and Nasurdin, A. M. (2013). Social support and work engagement: a study of Malaysian nurses. J. Nurs. Manag. 21, 1083–1090. doi: 10.1111/j.1365-2834.2012.01448.x
Penley, J. A., and Tomaka, J. (2002). Associations among the big five, emotional responses, and coping with acute stress. Personal. Individ. Differ. 32, 1215–1228. doi: 10.1016/S0191-8869(01)00087-3
Penney, L. M., Hunter, E. M., and Perry, S. J. (2011). Personality and counterproductive work behaviour: using conservation of resources theory to narrow the profile of deviant employees. J. Occup. Organ. Psychol. 84, 58–77. doi: 10.1111/j.2044-8325.2010.02007.x
Pinel, E. C., and Paulin, N. (2005). Stigma consciousness at work. Basic Appl. Soc. Psychol. 27, 345–352. doi: 10.1207/s15324834basp2704_7
Podsakoff, P. M., MacKenzie, S. B., Lee, J. Y., and Podsakoff, N. P. (2003). Common method bias in behavioral research: A critical review of the literature and recommended remedies. J. Appl. Psychol. 88, 879–903.
Preacher, K. J., and Hayes, A. F. (2008). Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav. Res. Methods 40, 879–891. doi: 10.3758/BRM.40.3.879
Raja, U., Javed, Y., and Abbas, M. (2018). A time lagged study of burnout as a mediator in the relationship between workplace bullying and work–family conflict. Int. J. Stress. Manag. 25, 377–390. doi: 10.1037/str0000080
Randle, J., and Arthur, D. (2007). The professional self-concept of nurses: a review of the literature from 1992-2006. Aust. J. Adv. Nurs. 24, 60–64. doi: 10.3316/informit.403000570176504
Schaubroeck, J. M., Lam, L. W., Lai, J. Y. M., Lennard, A. C., Peng, A. C., and Chan, K. W. (2018). Changing experiences of work dirtiness, occupational disidentification, and employee withdrawal. J. Appl. Psychol. 103, 1086–1100. doi: 10.1037/apl0000330
Schaufeli, W. B., Bakker, A. B., and Salanova, M. (2006). The measurement of work engagement with a short questionnaire: a cross-national study. Educ. Psychol. Meas. 66, 701–716. doi: 10.1177/0013164405282471
Schoenrade, P. A., Batson, C. D., Brandt, J. R., and Loud, R. E. (1986). Attachment, accountability, and motivation to benefit another not in distress. J. Pers. Soc. Psychol. 51, 557–563. doi: 10.1037/0022-3514.51.3.557
Sep, M. S. C., Steenmeijer, A., and Kennis, M. (2019). The relation between anxious personality traits and fear generalization in healthy subjects: a systematic review and meta-analysis. Neurosci. Biobehav. Rev. 107, 320–328. doi: 10.1016/j.neubiorev.2019.09.029
Shantz, A., and Booth, J. E. (2014). Service employees and self-verification: the roles of occupational stigma consciousness and core self-evaluations. Hum. Relat. 67, 1439–1465. doi: 10.1177/0018726713519280
Singletary, S. L., and Hebl, M. R. (2009). Compensatory strategies for reducing interpersonal discrimination: the effectiveness of acknowledgments, increased positivity, and individuating information. J. Appl. Psychol. 94, 797–805. doi: 10.1037/a0014185
Specter, M. H., and Ferrari, J. R. (2000). Time orientations of procrastinators: focusing on the past, present, or future? J. Soc. Behav. Pers. 15, 197–202.
Spector, P. E., Zapf, D., Chen, P. Y., and Frese, M. (2000). Why negative affectivity should not be controlled in job stress research: Don’t throw out the baby with the bath water. J. Organ. Behav. 21, 79–95.
Srivastava, S., and Bajpai, L. (2020). Linking conservation of resource perspective to personal growth initiative and intention to leave: role of mediating variables. Pers. Rev. 50, 686–708. doi: 10.1108/PR-10-2019-0548
Suls, J., Green, P., and Hillis, S. (1998). Emotional reactivity to everyday problems, affective inertia, and neuroticism. Personal. Soc. Psychol. Bull. 24, 127–136. doi: 10.1177/0146167298242002
Swagler, M. A., and Jome, L. R. M. (2005). The effects of personality and acculturation on the adjustment of north American sojourners in Taiwan. J. Couns. Psychol. 52, 527–536. doi: 10.1037/0022-0167.52.4.527
Turale, S., Meechamnan, C., and Kunaviktikul, W. (2020). Challenging times: ethics, nursing, and the COVID-19 pandemic. Int. Nurs. Rev. 67, 164–167. doi: 10.1111/inr.12598
Turner, P. (2020). “Employee Engagement and the Employee Experience,” in Employee Engagement in Contemporary Organizations: Maintaining High Productivity and Sustained Competitiveness. ed. P. Turner (Cham: Palgrave Macmillan).
Van Jaarsveld, D., Walker, D., Restubog, S., Skarlicki, D., Chen, Y., and Frické, P. H. (2019). Unpacking the relationship between customer (in)justice and employee turnover outcomes: can fair supervisor treatment reduce employees’ emotional turmoil? J. Serv. Res. 24, 301–319. doi: 10.1177/1094670519883949
Villar, R. C., Nashwan, A. J., Mathew, R. G., Mohamed, A. S., Munirathinam, S., Abujaber, A. A., et al. (2021). The lived experiences of frontline nurses during the coronavirus disease 2019 (COVID-19) pandemic in Qatar: a qualitative study. Nurs. Open 8, 3516–3526. doi: 10.1002/nop2.901
Vittal, R. S., Mishra, S. K., and Varma, A. (2022). Direct and indirect effects of beneficiary contact and supervisor support on service performance: Does perceived externalprestige matter? Br. J. Manag. 1–16. doi: 10.1111/1467-8551.12606
Watson, D., and Clark, L. A. (1984). Negative affectivity: the disposition to experience aversive emotional states. Psychol. Bull. 96, 465–490. doi: 10.1037/0033-2909.96.3.465
Widiger, T. A., and Oltmanns, J. R. (2017). Neuroticism is a fundamental domain of personality with enormous public health implications. World Psychiatry 16, 144–145. doi: 10.1002/wps.20411
Wierenga, K. L., and Moore, S. E. (2020). Adapting to uncertainty. J. Cardiovasc. Nurs. 35, 322–323. doi: 10.1097/jcn.0000000000000712
Wrzus, C., Luong, G., Wagner, G. G., and Riediger, M. (2021). Longitudinal coupling of momentary stress reactivity and trait neuroticism: specificity of states, traits, and age period. J. Pers. Soc. Psychol. 121, 691–706. doi: 10.1037/pspp0000308
Zellars, K. L., Hochwarter, W. A., Perrewé, P. L., Hoffman, N., and Ford, E. W. (2004). Experiencing job burnout: the roles of positive and negative traits and states. J. Appl. Soc. Psychol. 34, 887–911. doi: 10.1111/j.1559-1816.2004.tb02576.x
Zhang, Y. (2021). Strengthening the power of nurses in combating COVID-19. J. Nurs. Manag. 29, 357–359. doi: 10.1111/jonm.13023
Keywords: neuroticism, work engagement, beneficiary contact, fear of stigma, nurses, COVID-19
Citation: Vachhrajani M, Mishra SK, Rai H and Paliwal A (2022) The direct and indirect effect of neuroticism on work engagement of nurses during COVID-19: A temporal analysis. Front. Psychol. 13:947887. doi: 10.3389/fpsyg.2022.947887
Edited by:
Muhammed Elhadi, University of Tripoli, LibyaReviewed by:
Abdulqadir J. Nashwan, Hamad Medical Corporation, QatarCopyright © 2022 Vachhrajani, Mishra, Rai and Paliwal. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mit Vachhrajani, bWl0dkBpaW1pZHIuYWMuaW4=; Sushanta Kumar Mishrac3VzaGFudGFtQGlpbWIuYWMuaW4=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.