 Paulina Buffle
Paulina Buffle Edouard Gentaz
Edouard Gentaz Giacomo Vivanti3
Giacomo Vivanti3
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol., 23 June 2022
Sec. Psychology for Clinical Settings
Volume 13 - 2022 | https://doi.org/10.3389/fpsyg.2022.915817
This article is part of the Research TopicImproving The Quality of Life of Autistic People and Their Caregivers From Diverse Backgrounds: Methods and ApproachesView all 7 articles
The identification and diagnosis of children with autism currently rely on behavioral presentation and developmental history. Cultural norms and other socio-demographic factors can influence what is expected or non-expected behaviors in a developing child. Perceptions, beliefs, and causal attribution of early signs can influence families’ help-search behaviors. Lack of recognition of autism’s first manifestations can critically delay the age of diagnosis, the provision of informed guidance to families, and the implementation of adapted interventions during the critical period of early development. Furthermore, a lack of understanding of early signs as the manifestations of a developmental condition may increase stigma and non-conventional explanations. Still, cultural and socio-demographic factors are largely understudied, particularly in low-and middle-income settings. Based on the hypothesis that non-specialists such as family members and friends are one of the first sources of referral in Latin American contexts, we aimed to study the general population’s perceptions and the explanatory causes of autism’s early signs. One-hundred-and-eighty-three Ecuadorian adults responded to a questionnaire developed for this study, describing sixteen ASD-related behaviors. Results indicated that, with the exemption of language impairment and self-injurious behaviors, a substantial proportion of participants did not endorse many behaviors as “concerning and requiring professional attention.” Also, language impairment was the only behavior identified as related to a developmental disorder. Additionally, most participants attributed the majority of behaviors listed in the questionnaire to causes unrelated to ASD, such as child personality. We discuss the impact of those findings in clinical practice and on awareness programs.
Autism Spectrum Disorder (ASD) refers to a group of neurodevelopmental conditions characterized by difficulties in social communication, and unusually restricted or repetitive behavior and interests (American Psychiatric Association, 2013). Although support at any age is essential, younger children may benefit most from intervention due to early brain plasticity (Dawson et al., 2010; Vivanti et al., 2016). However, access to services may not be granted in all socioeconomic contexts (Durkin et al., 2015; Tekola et al., 2016). At least one in one hundred children in the world develops with a form of autism (Elsabbagh et al., 2012; Maenner et al., 2020), and around 6 million individuals live with this condition in Latin America (Paula et al., 2020).
Studies conducted in high-resource settings have reported several barriers to ASD-targeted diagnostic services, such as reduced availability of specialized services, lack of familiarity with tools, and perceptions of ASD as a not well-defined condition (Dosreis et al., 2006; Daniels and Mandell, 2013; Fenikilé et al., 2015). Additionally, socio-demographic and culturally determined factors, such as the knowledge the general population possesses about developmental milestones (Ratto et al., 2016), caregivers’ ability to recognize early emerging symptoms (Mandell and Novak, 2005), and misconceptions about signs, symptoms, and etiology (Rahbar et al., 2011) can play a role in trajectories toward identification. For instance, a study performed in the United States with mothers from a Latin-American origin reported significantly fewer developmental concerns and fewer ASD symptoms in children diagnosed with ASD in this group, compared to Anglo-American mothers, possibly due to lower ASD awareness, parental practices, or the presence of perceptions concealing the recognition of symptoms (Blacher et al., 2019). Another United States study with families of Mexican heritage reported that parents expect children to show respect for their elders by not speaking to them unless they are spoken to, suggesting that in this context, a lower level of communication might not be acknowledged as concerning (Bridges et al., 2012).
Similarly, a lack of response to parents’ directions might be interpreted as “willfulness” or be related to a child’s personality (Ratto et al., 2016). A reduced frequency of social initiations can be understood as a sign of politeness (“bien educado”), as has been reported in a study involving Mexican American children (Bridges et al., 2012). The same perception of a “good child” has been described in an Indian study, which has also documented that parents notice something atypical about their child six to ten months later than parents in the United States, suggesting that in this context, misleading causal attribution can impact on families’ help-seeking actions (Daley, 2004).
A low degree of concern and unconventional causal explanations may also impact the nature and quantity of information that caregivers provide to clinicians and professionals’ interpretation of this information (Mandell and Novak, 2005). Besides, these factors could also influence the choice of treatment. For example, a United States study suggested that non-conventional causal attributions result in parents seeking non-conventional treatments (Harrington et al., 2006). Another study has indicated that parents who believe food allergies are the explanatory cause of their child’s ASD symptoms may be more likely to use dietary modification and vitamins (Dardennes et al., 2011), and parents attributing those symptoms to vaccines are more likely to use detoxification therapy (Shyu et al., 2010). Hispanic parents in the United States have been reported to be less likely to endorse causal attributions that lead to help-seeking actions than non-Hispanic white American parents (Yeh et al., 2004). Similarly, non-white, publicly insured parents and parents with lower socioeconomic status have been reported to be less likely than others to interpret their child’s unusual behaviors as being caused by genetic factors, which possibly impact families’ help-seeking actions (Zuckerman et al., 2016).
These studies suggest that a better understanding of contextual factors, including perceptions of typical and atypical behaviors and culturally influenced explicative causes, is critical to inform awareness and mental health literacy programs supporting early diagnosis and intervention. However, most studies have been performed on causal explanations parents provide to their child’s autism (Hebert and Koulouglioti, 2010), and limited information is available on the perception of autism early behaviors among the general population, particularly in contexts different from those where the concepts and tools related to their identification have been developed.
Ecuador is an upper-middle-income country with a population under 18 years old, estimated at 6,298,788 in 2018 (National Institute of Statistics and Censuses of Ecuador, 2010). As preliminary evidence, a study aiming to estimate attendance of children with an autism diagnosis at schools in Quito found a proportion of 0.11% among 453 pupils, ages 5 to 15, in 161 regular schools (Dekkers et al., 2015). Health authorities estimate a prevalence of 0.28% (0.18%–0.41%) in children aged five years old or less, and 1266 people diagnosed with ASD were reported in official registers (Ministry of Public Health, 2017, p. p. 11). The reason why estimates of ASD prevalence in Ecuador are remarkably lower than those reported in Western Countries (Elsabbagh et al., 2012; Zeidan et al., 2022) remains unclear.
As has been the case in many countries, parent associations in Ecuador have contributed to increasing the understanding of the needs of the autism spectrum community through public conferences and participation in the development of social policies (Buffle, 2020). In 2012, the Ministry of Public Health recognized autism as a disability (Ministry of Public Health, 2012), a status that grants specific rights to individuals with a diagnosis. The same year, a law on disabilities was adopted, aiming to ensure the prevention, detection, treatment, and rehabilitation and to assure that the rights of people with disabilities are guaranteed (National Assembly of the Republic of Ecuador, 2012). An agreement intending to ensure access to special education was enacted in 2013 (Ministry of Education, 2013).
More recent efforts include the publication of an official guide that provides information on identification and treatment in clinical practices (Ministry of Public Health, 2017) and the definition of a National Agenda 2017–2021 aiming to support the autonomy and productivity of people with disabilities (National Council for Equality in Disabilities, 2017). Universities offer postgraduate education in pediatrics; however, the specific pedo-psychiatric and neuro-pediatric fields rely on interns trained in other countries who return to work in Ecuador. In the pediatric sector, professionals may face many challenges in ASD case-identification and case-management, such as access to training and available resources to refer families (Buffle et al., 2022). The public health system has two pediatric hospitals in two main cities, and several community centers around the county and units providing specific ASD services of identification and treatment are currently being developed.
Understanding the general population’s perceptions and interpretation of symptoms in this context is essential to inform both educational programs for specialists and local awareness programs. This understanding is particularly relevant in low-to-middle income contexts, where toddlers may not be seen systematically for well-being child visits, and child-health programs may focus predominantly on life-threatening issues with less attention to developmental disabilities (Elsabbagh et al., 2012). Moreover, in the Latin American context, non-specialists in health or education, such as family members and friends, are reported to be one of the first sources of referral for children with autistic symptoms (Talero-Gutiérrez et al., 2012), and the Internet is reported as one of the primary sources of information for families of individuals with ASD (Paula et al., 2020).
To the best of our knowledge, perceptions and causal attribution of ASD symptoms in young children have not been documented in Latin American countries. In the current study, we used a questionnaire with items about social communication, play, and disruptive behaviors described in the literature presented to a group of adults from the general population. Based on the hypothesis that in Ecuador, as in many other countries, awareness of ASD symptoms is limited, we expected that a minority of ASD characteristic behaviors would be identified as “concerning and requiring professional attention” and that a minority of behaviors would be understood as the manifestation of a developmental condition. We also examined the types of explanations provided for each behavior. Finally, we examined whether demographic factors influenced participants’ endorsement of ASD-related behaviors as “concerning” and as manifestations of a neurodevelopmental disorder.
The description of behaviors presented in the questionnaire was inspired by 18 behaviors related to social communication and play described in the literature (Barbaro and Dissanayake, 2009; Robins et al., 2009; Barbaro et al., 2011) and available in Spanish (Albores-Gallo et al., 2012). In order to present a wide range of autism-related behaviors, the questionnaire also included one item related to expressive language delay, reported as one of the first signs alerting parents in different cultures (De Giacomo and Fombonne, 1998; Daley, 2004). Two questions about challenging behaviors that can be present in some young children developing with ASD (Matson et al., 2010, 2011) were also included.
A group of ten local advisors (five parents of toddlers and school-age children, two kindergarten teachers, two pediatricians, and one anthropologist) was required to verify each of the 21 items in terms of understandability and adaptability to an Ecuadorian context. Five advisors perceived five items (four related to social and communication behaviors and one related to make-believe play) as “abstract” and “difficult to understand for adults who are not familiar with children” or “difficult to understand without actually seeing the behavior,” These behaviors were excluded from the questionnaire.
The sixteen behaviors described in the questionnaire included: three joint attention behaviors, nine social communication behaviors (including expressive, receptive language), two idiosyncratic responses to sensory stimuli and unusual motor patterns, one behavior related to play and two challenging behaviors.
Considering the variability of the onset of symptoms during the first years of life (American Psychiatric Association, 2013) and aiming to assure a more precise mental representation of the items described, the questionnaire specified that the first eight items concerned children between 18 and 24 months; the remaining items concerned children aged between 24 and 36 months (Barbaro and Dissanayake, 2009; Robins et al., 2009; Boyd et al., 2010; Barbaro et al., 2011).
As an essential aim in the first section of the questionnaire was to capture the intensity of concerns elicited by the depicted behaviors, participants were required to select one of three options: (a) the behavior depicted corresponds to what is “expected at that age,” (b) the behavior is “peculiar, but it does not need for professional attention,” or (c) the behavior is “concerning and requiring professional attention.” The second section of the questionnaire aimed to collect participants’ causal attribution for each behavior through an open-ended question.
One hundred eighty-three adults (107 female) between 18 and 79 years old (Mage = 36.63, age-range = 18–79) from different socioeconomic statuses, professional and educational backgrounds, reporting to be born or raised in Ecuador, were enrolled through face to face recruitment (Table 1).
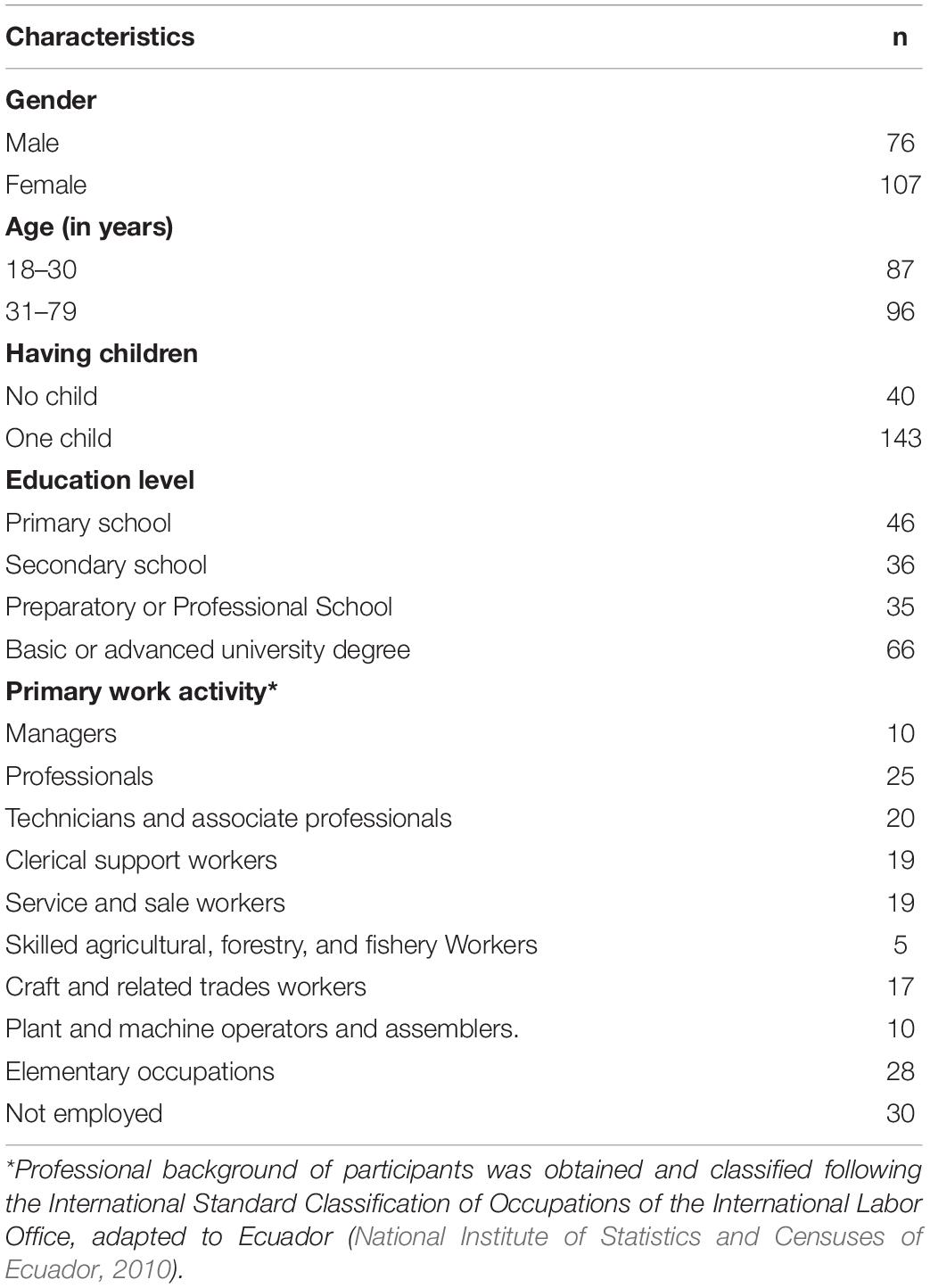
Table 1. Sample characteristics (n = 183).
In order to increase variability in the population, a list of popular markets attended by lower-middle to low-income classes was downloaded from a government agency,1 and a list of supermarkets attended by the upper-middle-income class was established. Five sites of each category were selected in 4 different towns, including the capital city, Quito, and permission to display information and proceed to interviews was obtained.
Participants were individually invited to participate and received information on the aim and procedure of the study. The information provided avoided using terms related to autism to exclude bias. Approximately 5% of individuals who approached the researchers for information declined the invitation to participate after receiving the information. Participants who accepted to participate provided written consent and were interviewed in Spanish by the author or by a graduate student in anthropology, both fluent in the language and familiar with Ecuadorian culture.
The 16-items were orally presented to avoid situations where participants could not read. Each autistic-related behavior was described to the participants, who were given enough time to produce a mental image of the situation described. Then, the two questions were read to the same participant. The researcher wrote down the option chosen for the first question (degree of concern) and the response to the open-ended question (causal attribution of the behaviors). The question related to the degree of concern and the question related to the explanatory cause were identical for each of the sixteen behaviors; participants responded in approximatively 30–35 min to the entire questionnaire. Participants also responded to a short demographic questionnaire. The research ethics committee of the first author provided approval for the study.
The responses to 16 open-ended questions were transcribed verbatim and classified using content analysis, a valuable method to identify emerging categories or themes from participants’ responses (Elo and Kyngäs, 2008; Kvale, 2008). The principal researcher, fluent in Spanish, read transcripts several times, aiming to identify regional and colloquial expressions. Local expressions were clarified by a local assistant (a nurse student). Each response was then introduced into an Excel sheet with responses in one column and the categories in the next column, and a code was assigned for each pattern identified. Constructed categories corresponded to ideas or expressions common among the participants’ responses.
In a second phase, the first researcher and a Spanish-speaker postgraduate student in anthropology independently verified that each response was assigned to at least one of the different constructed categories. Aiming to ensure reliability, a medical resident fluent in Spanish and blind to hypotheses independently reviewed by double-checking the constructed categories. Conflict situations (8% of responses) were resolved after discussion.
Eight categories were defined during the process of coding. (1) Personality Attitudes and Preferences; (2) Developmental Problems; (3) Physical or Sensory Issues; (4) Psychological Problems; (5) Rearing/Parenting; (6) Unspecified Causes; (7) Immaturity; (8) Does Not Know. Finally, frequencies of responses were calculated for all closed-ended and open-ended questions for each of the 16 behaviors.
As shown in Table 2, the two behaviors most frequently endorsed as “concerning and requiring professional attention” were Doesn’t Speak – Only Produce Sounds, and Hits his Head with Hands or Objects. Key social communication behaviors, such as Doesn’t Respond to Name, Doesn’t have Interest in Other Children, Doesn’t Understanding Emotions, and Doesn’t Understand Instructions, also received a high endorsement as “concerning” behaviors. The behavior that attracted less concern was Play Concentrates on Specific Toy Parts.
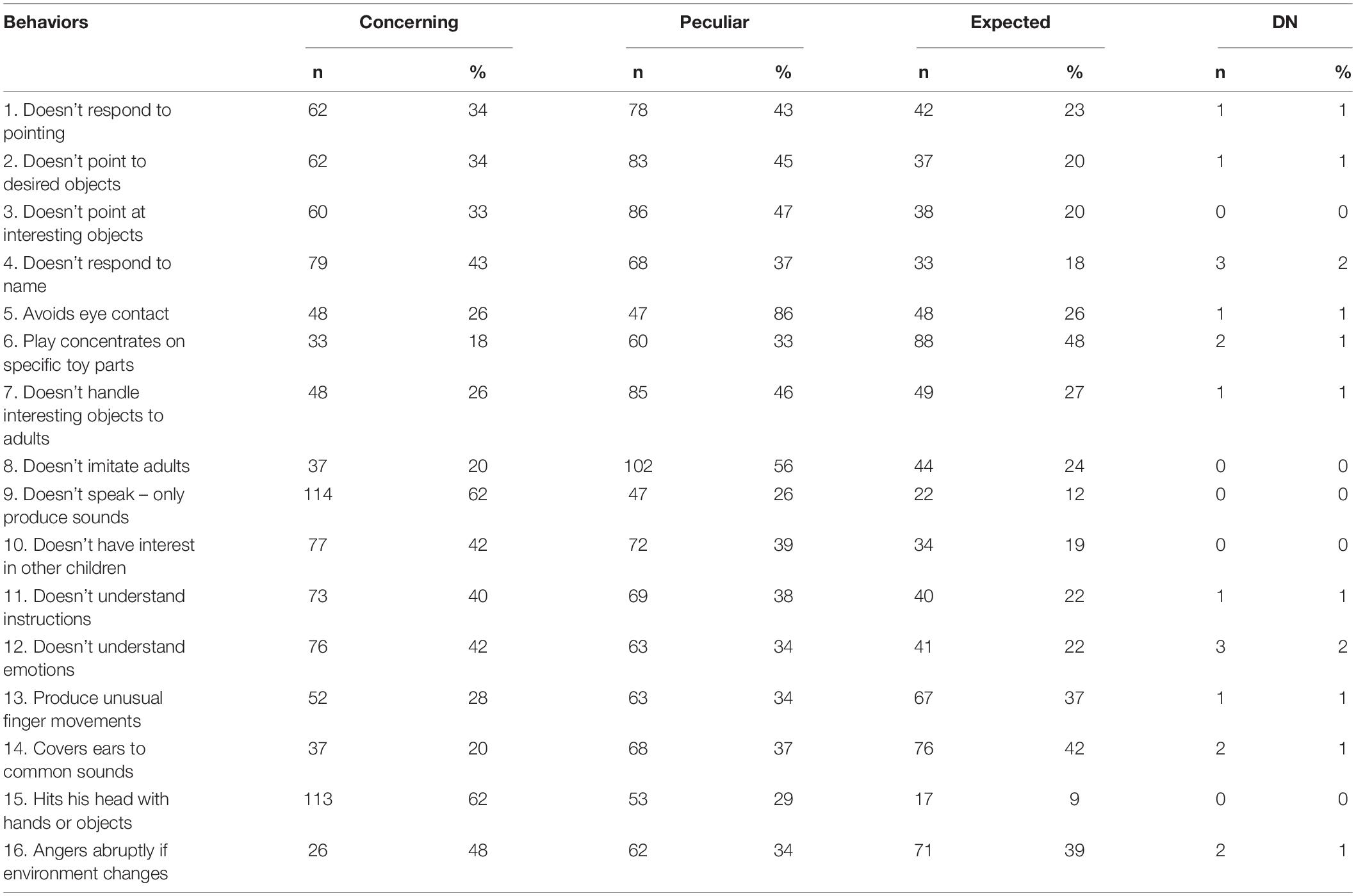
Table 2. Perception of the degree of concern by 183 adults in % in function of 16 behaviors.
The three joint attention behaviors presented, Doesn’t Respond to Pointing, Doesn’t Point at Desired Objects, and Doesn’t Point at Interesting Objects, were considered by most respondents as peculiar but not sufficiently alarming to search for professional advice. Two other behaviors related to social-communicative difficulties that were also considered peculiar are Doesn’t Imitate, Avoids Eye Contact, and Doesn’t Show Interesting Objects to Adults. Finally, the behaviors mostly considered “expected” were Play Concentrates on Specific Toy Parts, Covers Ears to Common Sounds, Angers Abruptly if Environment Changes, and Produce Unusual Finger Movements.
The explanatory cause most commonly cited (ten out of sixteen behaviors) was Personality, Attitude, or Preferences (Table 3). Some examples include “Es caprichoso” [He is spoiled] or “Es de temperamento” [He is temperamental]. The category Developmental Problems was the leading explanatory cause for only one of the sixteen behaviors, namely Doesn’t Speak – Only Produce Sounds. In this case, the specificity of the participant’s responses ranged from “Está atrazado” [His development is delayed] to precise answers such as “Tiene un trastorno del desarrollo” [He has a developmental disorder]. To a lesser extent, Hits his Head with Hands or Objects, Doesn’t Respond to Pointing, and Doesn’t Understand Emotions were understood as a sign of special needs situation: “Es una situación de necesidades especiales.”
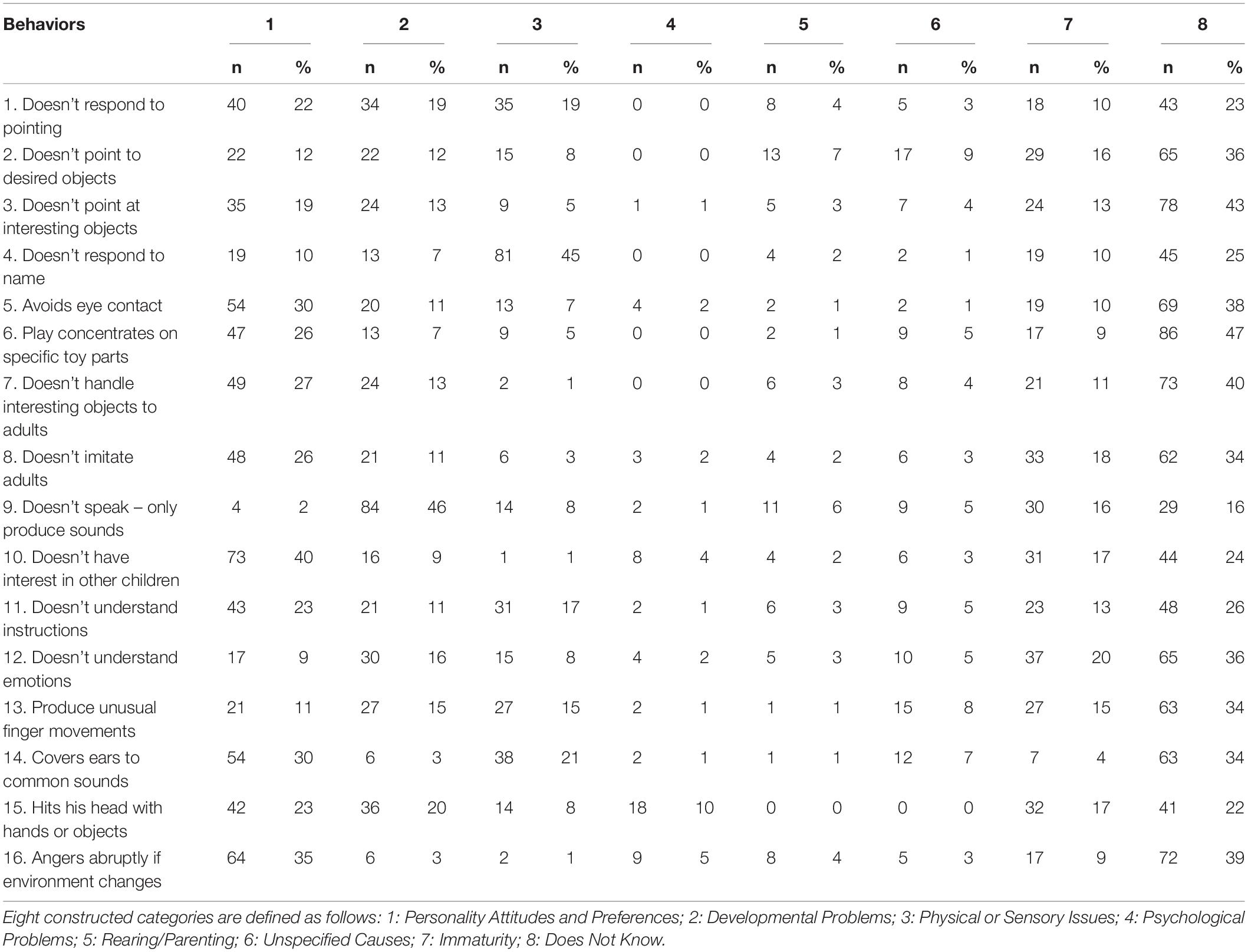
Table 3. Causal attributions repartition in eight categories by 183 adults in % in function of 16 behaviors.
Physical or Sensory Issues explanations such as, “No oye bien” [He doesn’t hear properly], were mainly associated with Doesn’t Respond to Name and Cover Ears in Response to Common Sounds. Scarce explanations were provided for the category Psychological Problems; examples included “Está traumado” [He is traumatized] or “Está estresado” [He is stressed] and were mainly associated with Hits his Head with Hands or Objects. Scarce explanations were also provided in the category Parenting; for example, “Sus padres no le han enseñado” [His parents haven’t taught him] was provided to the behavior Doesn’t Point to Desired Objects. The category Unspecified Reasons assembled responses that acknowledge a behavior as unusual but did not provide an explanatory cause, such as “Algo le pasa” [Something is happening to him], “Algo hay” [There is something]. Supranatural explanatory causes were provided by less than 1% of participants and were also included in this category. Explanatory causes related to the category Immaturity, such as “Todavía es chiquito” [He is still young], were provided by a small proportion of participants for all the behavior presented. Finally, an important rate of responses was associated to the category I don’t know and was provided to most of the behaviors presented.
We also aimed to study if the level of education, age, and parental status influenced the identification of behaviors as “concerning and requiring professional attention” and the explanatory causes related to a developmental condition.
In order to explore the effect of these factors, participants were classified by age (group 1 = 18–30 years old; group 2 = 31–79 years old), parenthood status (group 1 = parents; group 2 = no parents), and level of education (group 1 = primary and secondary education; group 2 = university and post-degree). The data was coded and entered into Statistica (Tibco) to analyze the differences between proportions testing the following hypotheses H0:PO = PY.
H1: PO > PY with a level of significance of 5%. Z-value equals the observed difference between proportions (p1-p2) divided by the standard error:
Classification under age indicated a significant impact on the perception as “concerning” among older participants on the following behaviors: Avoids Eye Contact, Doesn’t Handle Interesting Objects to Adults, Doesn’t Have Interest in Other Children, Doesn’t Understand Instructions, Doesn’t Understand Emotions. Parental status had a significant impact on the perception as “concernin” among older participants only on Avoids Eye Contact. The level of education was not found to have an effect on the perception of any of the behaviors as “concerning” (Table 4).
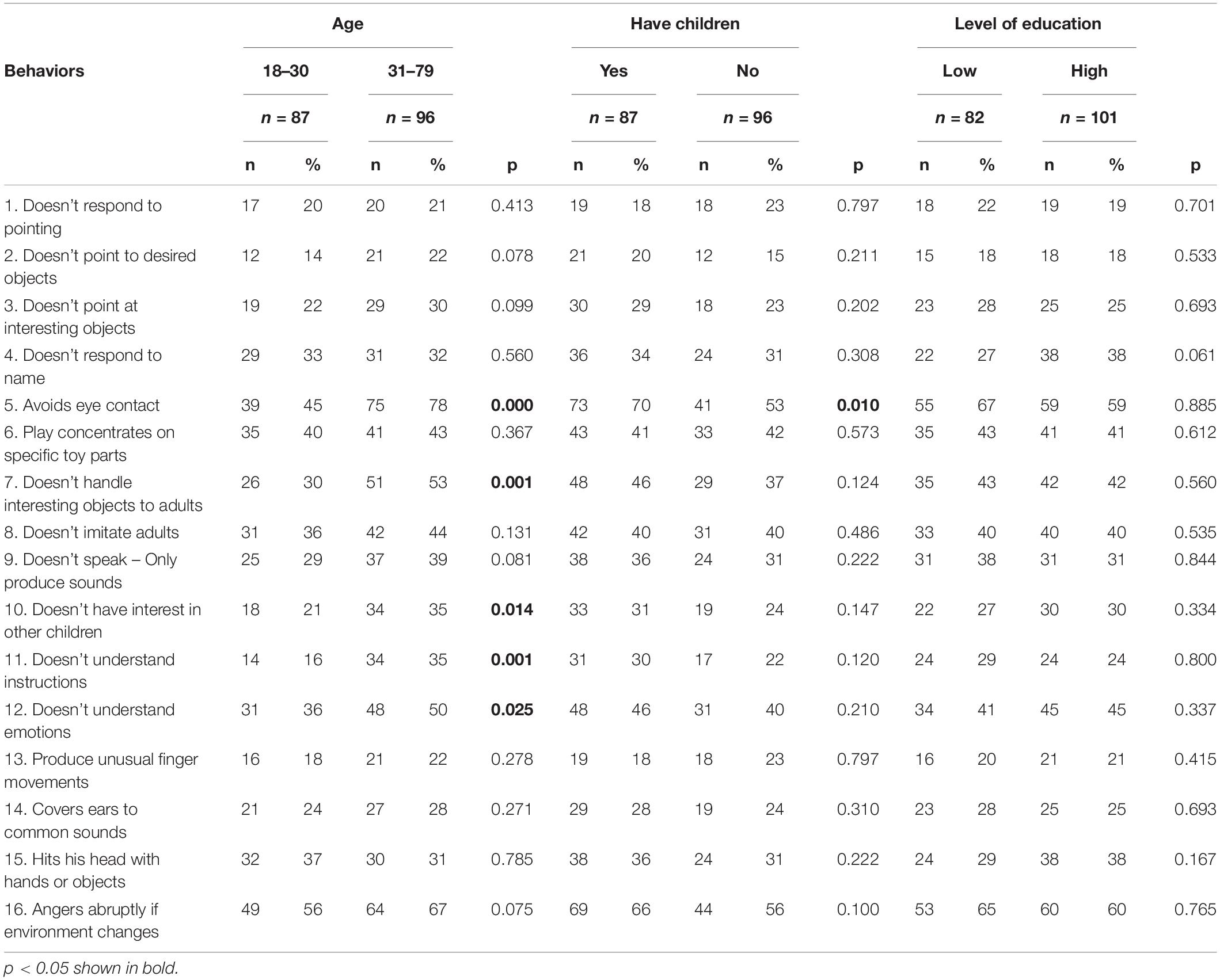
Table 4. Differences of proportions of participants that identified the 16 behaviors as “concerning” as a function of age, parenthood, and level of education.
Results also indicated that the age of the participants had a significant influence on the recognition of five behaviors as a sign of a developmental disorder: Avoids Eye Contact and Doesn’t Handle Interesting Objects to Adults, with older participants more often endorsing these behaviors as “concerning.” Participants with children provided a developmental explanatory cause to Covers Ears to Common Sounds and Doesn’t Handle Interesting Objects more often. Participants with a higher level of education provided a developmental explanatory cause to Produce Unusual Finger Movements more often. The level of education seemed to have no impact on understanding any of the behaviors as a symptom of a developmental disorder (Table 5). The results of this exploratory analysis should be interpreted with caution, considering the sample size.
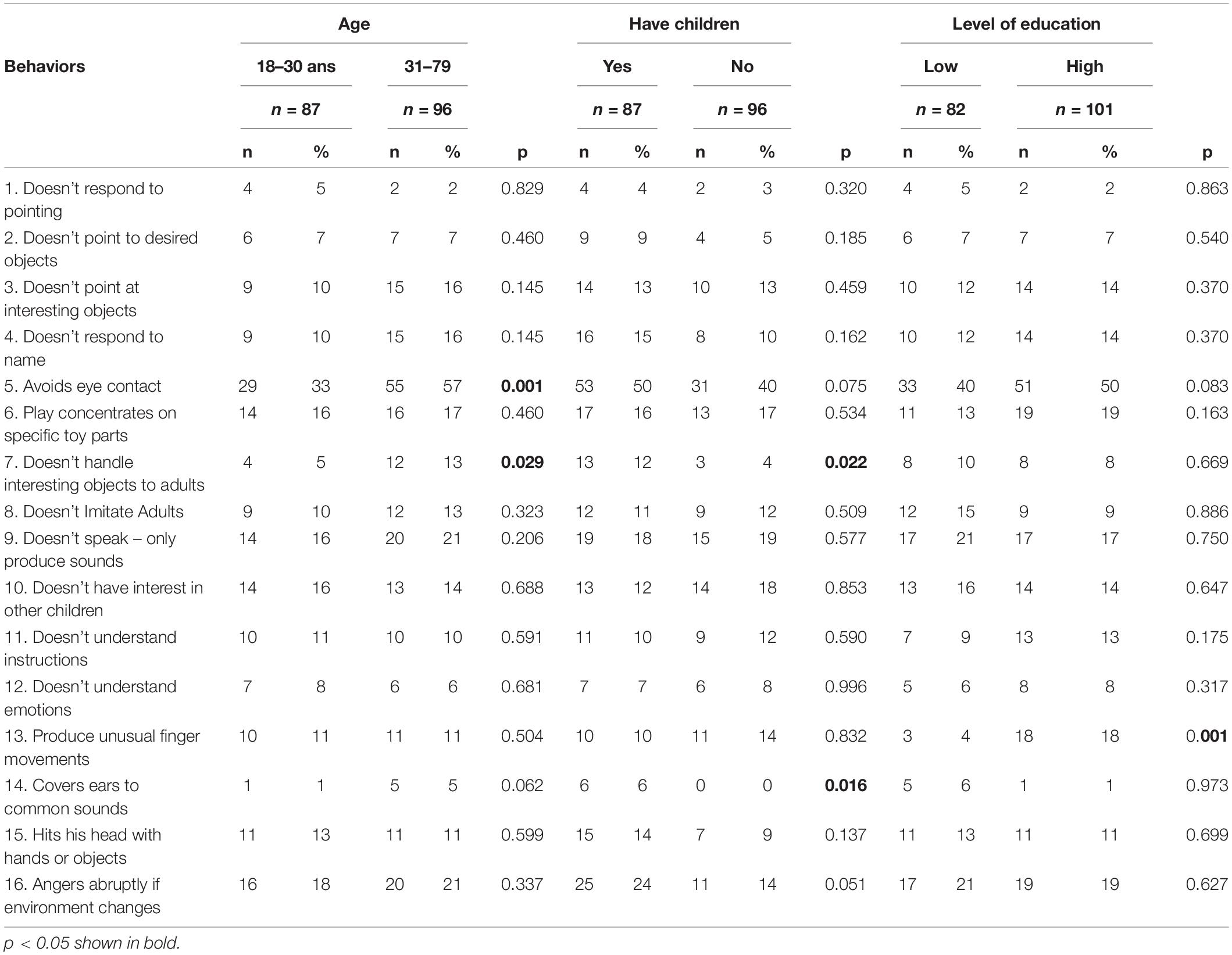
Table 5. Differences of proportions of participants identifying 16 behaviors as a symptom of a developmental disorder, as a function of age, parenthood, and level of education.
This study was designed to identify the perceptions of ASD early markers and the type of causal explanations the general adult population attributes to those behaviors. Several early ASD symptoms described in our questionnaire were perceived as “peculiar” although not “concerning” by at least one-third of the participants. These findings suggest that some common early signs could be overlooked by caregivers and adults surrounding a child. They are consistent with previous findings from Latin American communities in the United States reporting that mothers of children with ASD tend to normalize their child’s early behavior compared to non-Latin American mothers, which can negatively influence help-seeking actions (Zuckerman et al., 2014).
Our results also denote that participants did not perceive most of the behaviors presented in the questionnaire as potential manifestations of a developmental disorder, which is also consistent with previous studies on causal attribution of developmental difficulties (Zuckerman et al., 2016). For instance, in our sample, most of the participants could not provide a causal attribution to common autism-related behaviors, such as Avoids Eye Contact and Doesn’t Handle Interesting Objects to Adults. When an explicatory cause was provided, it was mainly related to the child’s personality. Interestingly, these two core symptoms have been reported among the first parental concerns in other low-and-middle-resources settings (Daley, 2004); however, in our sample, they were mainly endorsed as non-concerning. Those findings suggest that subtle behaviors associated with autism might pass unnoticed to adults in Ecuador and that pediatric providers should not assume that parents can spontaneously report them as a concern.
Similarly, the three joint attention behaviors (Doesn’t Respond to Pointing, Doesn’t Point at Desired Objects, and Doesn’t Point at Interesting Objects) were not considered “concerning,” and, as in the former example, most of the responders could not provide an explanatory cause or attributed it to a child’s personality. Those findings have a critical implication for clinical practice considering that they are commonly present in children who will receive a diagnosis. Furthermore, attribution of autistic symptoms to a child’s personality as “timidity,” “independence,” or “strong character” may have at least two potential impacts. Firstly, if caregivers and family friends underscore those behaviors parental help-seeking actions could be delayed. Secondly, rearing style can be affected, for example, if parents understand those behaviors as their child not wanting to cooperate or is voluntarily ignoring them. The same conclusion could be drawn for the items Doesn’t Have Interest in Other Children and Doesn’t Understand Instructions, which are considered “concerning” but mainly explained as the manifestation of a child’s personality.
Lack of response to name was identified as “concerning” by many participants but was primarily related to a hearing impairment, a type of explanation that may be pertinent in some cases and requires a differential diagnosis; however, in ASD cases, it has been associated with an increase in the age of diagnosis in the United States (Mandell et al., 2005). This finding points to the importance of continuous education for all pediatric health allies and in all levels of attention as children displaying atypical behaviors may be referred in the first instance to sensory examinations. Equally acknowledged as “concerning,” self-injurious behaviors were not identified as signs of a developmental disorder but rather as a personality problem. These perceptions could lead caregivers not to seek professional advice even though emerging self-injurious behavior can be associated with unfavorable outcomes and can be addressed through intervention.
The item Play Concentrates on Specific Toy Parts, which in the United States has been associated with a decrease in the age of diagnosis (Mandell et al., 2005), was considered by our sample as the least concerning behavior suggesting that interpretation of play-related behaviors may be under the contextual influence. The item Covers Ears to Common Sounds, Angers Abruptly if Environment Changes, was mainly perceived as expected and principally explained by personality. In the case of Unusual Finger Movements, participants provided several reasons unrelated to a developmental disorder, such as boredom, and it was mainly expected in typical development. Interestingly, these three behaviors are not related to social communicative abilities but rather to repetitive behaviors and sensory issues. It is difficult, at this stage, to know if the Ecuadorian population tends to identify non-social communicative ASD markers as less problematic and if those results reflect more tolerance of diversity in repetitive play and sensory issues. Further research is also needed to understand if identifying behaviors as problematic can help children and families in Ecuador access services or whether there is a risk of pathologizing certain behaviors in children that could otherwise be accepted and adjusted within their communities. A higher level of concern elicited by the social communicative markers is also consistent with the findings of a study performed in a group of Latin American countries, where more than half of the parents reported communication and social interaction deficits as the main challenges for their child with ASD (Paula et al., 2020).
Expressive language delay, as anticipated, was mainly endorsed as “concerning” and attributed to a developmental disorder suggesting that this difficulty could prompt families to seek professional consultation. However, because many children with ASD do not have a language delay, the presence of language could be a factor of late referral.
A very modest rate of supranatural explanations was found in our sample and was classified as unspecified causes. This finding is congruent with recent research. For example, a Canadian study found that the most common causal attribution provided by Latin American parents of children diagnosed with ASD was not related to religious explanations (Millau et al., 2018), and a study in the Philippines indicated that parents tend to disagree with previous myths about the etiology of ASD, such as parental sins and curses (Quilendrino et al., 2015).
Preliminary analyses did not suggest a clear association of perception of behaviors as “concerning” or as a sign of a developmental disorder and socio-demographic factors. Although the sample size limits these results, they suggest that awareness of ASD symptoms may be needed across all segments of the population in Ecuador, without distinction of age, parental status, or education. Community awareness remains an essential concern for families in Latin America despite significant recent efforts deployed (Paula et al., 2020). Awareness of the condition and its early manifestations is critical for the process of detection; it might also influence attitudes toward individuals with ASD and contribute to avoiding stigma.
These results suggest that parent education programs remain necessary, even if retrospective studies have shown that parents recognize signs of autism far earlier than it is diagnosed, particularly when they have an older child with autism (Ozonoff et al., 2009). Education aiming to inform parents about what to expect from their developing children during their early months and years could also help them identify when a child fails to reach certain milestones. Parents’ knowledge and understanding of early markers as the signs of a developmental condition can also influence their trust in diagnostic and willingness to comply with adapted early interventions (Mire et al., 2017). Finally, our results can inform professionals in pediatric settings about behaviors that caregivers may not consider “concerning and requiring professional attention,” which can impact the type of information parents transmit spontaneously during a consultation.
Generalizing those findings to other Latin American cultural contexts requires more extensive and more diversified participation. Although Latin American individuals share a language and many cultural references, they belong to a range of cultural sub-groups resulting from a complex interplay of self-perceived identities, socioeconomic factors, and level of education.
This study also presents methodological limitations related to some items, for example, Produce Unusual Finger Movement, which might be difficult to understand or visualize by non-specialists. This is an important point for the cross-cultural validity of parent-addressed checklists. As those instruments are essentially based on the description of behaviors, the understandability of such descriptions in various populations may need further study. Also, the questionnaire describes behaviors that could be present in other conditions, such as sensory impairments, receptive language disorder, or epilepsy (Wadhera, 2021), which could impact participants’ responses. Finally, it is important to notice that the behaviors presented in our questionnaire correspond to symptoms that have been defined as a “male stereotype” (Frazier et al., 2014).
Furthermore, all questions were related to behaviors that can be displayed in “un niño,” a masculine noun used as a generic for “a child” in Spanish, that could produce a gender bias as participants visualize these symptoms only in young boys. Further studies will need to be conducted to observe if the description of these behaviors elicits different degrees of concern and other causal explanations if applied to young girls. Further studies are also needed to determine if the concern elicited by certain behaviors, the type of explanation provided, or the presence of certain demographic traits could predict families’ help-seeking actions.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Ethical Committee of the Faculty of Psychology and Education at Geneva University approved this study. The patients/participants provided their written informed consent to participate in this study.
PB and EG designed the study and analyzed the data. PB acquired the data. PB and GV wrote the article’s first draft. All authors have approved the final manuscript.
PB received financial support from the Foundation Ernst et Lucie Schmidheiny, Switzerland. Open access funding was provided by the University of Geneva.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We are particularly grateful to Rosa Hoekstra, King’s College, United Kingdom, for her valuable advice in the conception of this project, Georgina Granero and Carmen Paredes for contributing to data collection and coding, and Lisa Madera for editing the manuscript and Thalia Cavadini for advice on data analysis. We are also grateful to parents, teachers, and medical doctors who provided advice on the development of the questionnaire.
Albores-Gallo, L., Roldán-Ceballos, O., Villarreal-Valdes, G., Betanzos-Cruz, B. X., Santos-Sánchez, C., Martínez-Jaime, M. M., et al. (2012). M-CHAT Mexican version validity and reliability and some cultural considerations. ISRN Neurol. 2012:408694. doi: 10.5402/2012/408694
American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders (DSM-5). Washington, DC: American Psychiatric Association.
Barbaro, J., and Dissanayake, C. (2009). Autism spectrum disorders in infancy and toddlerhood: a review of the evidence on early signs, early identification tools, and early diagnosis. J. Dev. Behav. Pediatr. 30, 447–459. doi: 10.1097/DBP.0b013e3181ba0f9f
Barbaro, J., Ridgway, L., and Dissanayake, C. (2011). Developmental surveillance of infants and toddlers by maternal and child health nurses in an Australian community-based setting: promoting the early identification of autism spectrum disorders. J. Pediatr. Nurs. 26, 334–347. doi: 10.1016/j.pedn.2010.04.007
Blacher, J., Stavropoulos, K., and Bolourian, Y. (2019). Anglo-Latino differences in parental concerns and service inequities for children at risk of autism spectrum disorder. Autism 23, 1554–1562. doi: 10.1177/1362361318818327
Boyd, B. A., Odom, S. L., Humphreys, B. P., and Sam, A. M. (2010). Infants and toddlers with autism spectrum disorder: early identification and early intervention. J. Early Interv. 32, 75–98. doi: 10.1177/1053815110362690
Bridges, M., Cohen, S. R., McGuire, L. W., Yamada, H., Fuller, B., Mireles, L., et al. (2012). Bien Educado: measuring the social behaviors of Mexican American children. Early Child. Res. Q. 27, 555–567. doi: 10.1016/j.ecresq.2012.01.005
Buffle, P. (2020). “Autism in ecuador,” in The Encyclopaedia of Autism, ed. F. R. Volkmar (Berlin: Springer).
Buffle, P., Naranjo, A., Gentaz, E., and Vivanti, G. (2022). Experiences and Attitudes on early identification practices of autism: a preliminary survey of pediatric professionals in ecuador. Children 9:123. doi: 10.3390/children9020123
Daley, T. C. (2004). From symptom recognition to diagnosis: children with autism in urban India. Soc. Sci. Med. 58, 1323–1335. doi: 10.1016/S0277-9536(03)00330-7
Daniels, A. M., and Mandell, D. S. (2013). Children’s compliance with american academy of pediatrics’ well-child care visit guidelines and the early detection of autism. J. Autism Dev. Disord. 43, 2844–2854. doi: 10.1007/s10803-013-1831-x
Dardennes, R. M., Al Anbar, N. N., Prado-Netto, A., Kaye, K., Contejean, Y., and Al Anbar, N. N. (2011). Treating the cause of illness rather than the symptoms: parental causal beliefs and treatment choices in autism spectrum disorder. Res. Dev. Disabil. 32, 1137–1146. doi: 10.1016/j.ridd.2011.01.010
Dawson, G., Rogers, S., Munson, J., Smith, M., Winter, J., Greenson, J., et al. (2010). Randomized, controlled trial of an intervention for toddlers with autism: the early start denver model. Pediatrics 125:e17. doi: 10.1542/peds.2009-0958
De Giacomo, A., and Fombonne, E. (1998). Parental recognition of developmental abnormalities in autism. Eur. Child Adolesc. Psychiatry 7, 131–136. doi: 10.1007/s007870050058
Dekkers, L. M. S., Groot, N. A., Díaz Mosquera, E. N., Andrade Zúñiga, I. P., and Delfos, M. F. (2015). Prevalence of autism spectrum disorders in ecuador: a pilot study in Quito. J. Autism Dev. Disord. 45, 4165–4173. doi: 10.1007/s10803-015-2559-6
Dosreis, S., Weiner, C. L., Johnson, L., and Newschaffer, C. J. (2006). Autism spectrum disorder screening and management practices among general pediatric providers. J. Dev. Behav. Pediatr. 27, S88–S94. doi: 10.1097/00004703-200604002-00006
Durkin, M. S., Elsabbagh, M., Barbaro, J., Gladstone, M., Happe, F., Hoekstra, R. A., et al. (2015). Autism screening and diagnosis in low resource settings: challenges and opportunities to enhance research and services worldwide. Autism Res. 8, 473–476. doi: 10.1002/aur.1575
Elo, S., and Kyngäs, H. (2008). The qualitative content analysis process. J. Adv. Nurs. 62, 107–115. doi: 10.1111/j.1365-2648.2007.04569.x
Elsabbagh, M., Divan, G., Koh, Y.-J., Kim, Y. S., Kauchali, S., Marcín, C., et al. (2012). Global prevalence of autism and other pervasive developmental disorders. Autism Res. 5, 160–179. doi: 10.1002/aur.239
Fenikilé, T. S., Ellerbeck, K., Filippi, M. K., and Daley, C. M. (2015). Barriers to autism screening in family medicine practice: a qualitative study. Prim Health Care Res Dev. 16, 356–366. doi: 10.1017/S1463423614000449
Frazier, T. W., Georgiades, S., Bishop, S. L., and Hardan, A. Y. (2014). Behavioral and cognitive characteristics of females and males with autism in the simons simplex collection. J. Am. Acad. Child Adolesc. Psychiatry 53:329–40.e1-3. doi: 10.1016/j.jaac.2013.12.004
Harrington, J. W., Patrick, P. A., Edwards, K. S., and Brand, D. A. (2006). Parental beliefs about autism: implications for the treating physician. Autism 10, 452–462. doi: 10.1177/1362361306066609
Hebert, E. B., and Koulouglioti, C. (2010). Parental beliefs about cause and course of their child’s autism and outcomes of their beliefs: a review of the literature. Issues Compr. Pediatr. Nurs. 33, 149–163. doi: 10.3109/01460862.2010.498331
Maenner, M. J., Shaw, K. A., Baio, J., Washington, A., Patrick, M., DiRienzo, M., et al. (2020). Prevalence of autism spectrum disorder among children aged 8 years – autism and developmental disabilities monitoring Network, 11 Sites, United States, 2016. MMWR Surveill Summ. 69, 1–12. doi: 10.15585/mmwr.ss6904a1
Mandell, D. S., and Novak, M. (2005). The role of culture in families’ treatment decisions for children with autism spectrum disorders. Ment. Retard. Dev. Disabil. Res. Rev. 11, 110–115. doi: 10.1002/mrdd.20061
Mandell, D. S., Novak, M. M., and Zubritsky, C. D. (2005). Factors associated with age of diagnosis among children with autism spectrum disorders. Pediatrics 116:1480. doi: 10.1542/peds.2005-0185
Matson, J. L., Boisjoli, J. A., Hess, J. A., and Wilkins, J. (2010). Factor structure and diagnostic fidelity of the baby and Infant Screen for children with aUtIsm traits–Part 1 (BISCUIT–Part 1). Dev. Neurorehabil. 13, 72–79. doi: 10.3109/17518420903213576
Matson, J. L., Boisjoli, J. A., Hess, J. A., and Wilkins, J. (2011). Comorbid psychopathology factor structure on the baby and infant screen for children with aUtIsm Traits-Part 2 (BISCUIT-Part 2). Res. Autism Spectr. Disord. 5, 426–432.
Millau, M., Rivard, M., and Mello, C. (2018). Immigrant families’ perception of the causes, first manifestations, and treatment of autism spectrum disorder. J. Child Fam. Stud. 27, 3468–3481. doi: 10.1007/s10826-018-1180-7
Ministry of Education (2013). Acuerdo 295–13 Para Estudiantes con Necesidades Educativas Especiales. London: Ministry of Education.
Ministry of Public Health (2012). Acuerdo Ministerial 1829. Emiìtense los Criterios de Inclusioìn de Enfermedades Consideradas Catastroìficas, Raras y Hueìrfanas Para Beneficiarios del Bono Joaquiìn Gallegos Lara Minsterial. Doha: Ministry of Public Health.
Ministry of Public Health (2017). Guiìa Praìctica Cliìnica. Trastornos del Espectro Autista en NinÞos y Adolescentes: Deteccioìn, Diagnoìstico, Tratamiento, Rehabilitacioìn y Seguimiento. Doha: Ministry of Public Health.
Mire, S. S., Gealy, W., Kubiszyn, T., Burridge, A. B., and Goin-Kochel, R. P. (2017). Parent perceptions about autism spectrum disorder influence treatment choices. Focus Autism Other Dev. Disabil. 32, 305–318.
National Assembly of the Republic of Ecuador (2012). Ley Orgaìnica de Discapacidades. Quit: National Assembly of the Republic of Ecuador.
National Council for Equality in Disabilities (2017). Agenda Nacional para la Igualdad de Discapacidades 2017–2021. Washington, DC: National Council for Equality in Disabilities.
National Institute of Statistics and Censuses of Ecuador (2010). Results form 2010. Población y Demografía. Quito: National Institute of Statistics and Censuses of Ecuador.
Ozonoff, S., Young, G. S., Steinfeld, M. B., Hill, M. M., Cook, I., Hutman, T., et al. (2009). How early do parent concerns predict later autism diagnosis? J Dev. Behav. Pediatr. 30:367. doi: 10.1097/dbp.0b013e3181ba0fcf
Paula, C. S., Cukier, S., Cunha, G. R., Irarrázaval, M., Montiel-Nava, C., Garcia, R., et al. (2020). Challenges, priorities, barriers to care, and stigma in families of people with autism: similarities and differences among six Latin American countries. Autism 24, 2228–2242. doi: 10.1177/1362361320940073
Quilendrino, M. I. O., Castor, M. A. R., Mendoza, N. R. N. P., Vea, J. R., and Castillo-Carandang, N. T. (2015). Parents’ perceptions of autism and their health-seeking behaviors. Clin. Epidemiol. Glob. Health. 3, S10–S15. doi: 10.1016/j.cegh.2015.11.003
Rahbar, M. H., Ibrahim, K., and Assassi, P. (2011). Knowledge and attitude of general practitioners regarding autism in Karachi, Pakistan. J. Autism Dev. Disord. 41, 465–474. doi: 10.1007/s10803-010-1068-x
Ratto, A. B., Reznick, J. S., and Turner-Brown, L. (2016). Cultural effects on the diagnosis of autism spectrum disorder among Latinos. Focus Autism Other Dev. Disabil. 31, 275–283. doi: 10.1177/1088357615587501
Robins, D. L., Fein, D., and Barton, M. (2009). Modified Checklist for Autism in Toddlers, Revised, with Follow-Up (M-CHAT-R/F) TM. Salt Lake City, UT: LineageN.
Shyu, Y.-I. L., Tsai, J.-L., and Tsai, W.-C. (2010). Explaining and selecting treatments for autism: parental explanatory models in Taiwan. J. Autism Dev. Disord. 40, 1323–1331. doi: 10.1007/s10803-010-0991-1
Talero-Gutiérrez, C., Rodríguez, M., De La Rosa, D., Morales, G., and Vélez-Van-Meerbeke, A. (2012). Profile of children and adolescents with autism spectrum disorders in an institution in Bogota, Colombia. Neurología (English Edn) 27, 90–96. doi: 10.1016/j.nrl.2011.03.005
Tekola, B., Baheretibeb, Y., Roth, I., Tilahun, D., Fekadu, A., Hanlon, C., et al. (2016). Challenges and opportunities to improve autism services in low-income countries: lessons from a situational analysis in Ethiopia. Glob. Ment. Health 3:e21. doi: 10.1017/gmh.2016.17
Vivanti, G., Dissanayake, C., and The Victorian, A. T. (2016). Outcome for children receiving the early start denver model before and after 48 months. J. Autism Dev. Disord. 46, 2441–2449. doi: 10.1007/s10803-016-2777-6
Wadhera, T. (2021). Brain network topology unraveling epilepsy and ASD association: automated EEG-based diagnostic model. Exp. Syst. Appl. 186:115762.
Yeh, M., Hough, R. L., McCabe, K., Lau, A., and Garland, A. (2004). Parental beliefs about the causes of child problems: exploring racial/ethnic patterns. J. Am. Acad. Child Adolesc. Psychiatry 43, 605–612. doi: 10.1097/00004583-200405000-00014
Zeidan, J., Fombonne, E., Scorah, J., Ibrahim, A., Durkin, M. S., Saxena, S., et al. (2022). Global prevalence of autism: a systematic review update. Autism Res. 15, 778–790.
Zuckerman, K. E., Lindly, O. J., and Sinche, B. (2016). Parent beliefs about the causes of learning and developmental problems among children with autism spectrum disorder: results from a national survey. Am. J. Intellect. Dev. Disabil. 121, 432–447. doi: 10.1352/1944-7558-121.5.432
Keywords: autism, early signs, perceptions, causal attributions, culturally-sensitive practice, underrepresented groups, low-and middle-resource settings
Citation: Buffle P, Gentaz E and Vivanti G (2022) Perception, Beliefs, and Causal Attribution of Autism Early Signs in Ecuadorian General Population. Front. Psychol. 13:915817. doi: 10.3389/fpsyg.2022.915817
Received: 08 April 2022; Accepted: 06 June 2022;
Published: 23 June 2022.
Edited by:
Georgitta Joseph Valiyamattam, Gandhi Institute of Technology and Management (GITAM), IndiaReviewed by:
Tanu Wadhera, Thapar Institute of Engineering & Technology, IndiaCopyright © 2022 Buffle, Gentaz and Vivanti. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Paulina Buffle, cGF1bGluYS5idWZmbGVAdW5pZ2UuY2g=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.