
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol., 05 July 2022
Sec. Health Psychology
Volume 13 - 2022 | https://doi.org/10.3389/fpsyg.2022.907939
This article is part of the Research TopicThe Psychological Challenges of Respiratory DiseaseView all 10 articles
 Ingeborg Farver-Vestergaard1*
Ingeborg Farver-Vestergaard1* Sandra Rubio-Rask1Signe Timm2,3
Sandra Rubio-Rask1Signe Timm2,3 Camilla Fischer Christiansen1Ole Hilberg1,3Anders Løkke1,3
Camilla Fischer Christiansen1Ole Hilberg1,3Anders Løkke1,3Background: Commonly applied measures of symptoms of anxiety are not sensitive to disease-specific anxiety in patients with chronic obstructive pulmonary disease (COPD). There is a need for validated instruments measuring COPD-specific anxiety. Therefore, we translated the COPD-Anxiety Questionnaire (CAF) into Danish (CAF-R-DK) and performed an initial validation of the psychometric properties in a sample of patients with COPD.
Materials and Methods: Translation procedures followed the World Health Organization guidelines. Participants with COPD completed questionnaires measuring COPD-specific anxiety (CAF-R-DK), general psychological distress (Hospital Anxiety and Depression Scale) as well as variables related to COPD (COPD Assessment Test; modified Medical Research Council dyspnea scale), quality of life (the 12-item Short Form survey, SF12), and socio-demography.
Results: A total of 260 patients with COPD (mean age: 65.0, 69% female) completed questionnaires. The Danish version of CAF-R-DK demonstrated acceptable Cronbach’s α values that were comparable with those of the original CAF. As expected, the CAF-R-DK showed positive correlations with convergent constructs (CAT; HADS) and negative correlations with discriminant constructs (SF-12). However, the results for specific subdomains of the CAF-R-DK indicated inconsistency in the underlying concept of disease-specific anxiety, which was also suggested based on the subsequent confirmatory and exploratory factor analyzes.
Conclusion: The CAF could serve as an important supplement to generic psychological distress screening of patients with COPD in somatic health care settings, and the questionnaire is now available in Danish. Translation into other languages is needed with the purpose of obtaining data for further testing the psychometric properties of the questionnaire.
Living with breathlessness, reduced mobility, and uncertainty related to chronic obstructive pulmonary disease (COPD) is associated with high levels of anxiety for many patients (Willgoss and Yohannes, 2013; von Leupoldt, 2017). Anxiety is a natural psychophysiological response to a perceived threat, which for most patients occur as passing emotional states in relation to external events (e.g., exacerbations of symptoms, hospitalization, or receiving messages with negative contents related to health and/or treatment options) or internal events (e.g., bodily sensations or intrusive thoughts or memories). However, for a considerable proportion of patients with COPD, symptoms of anxiety are persistent over a longer period of time and can be associated with behavioral avoidance of activities that are expected to trigger dyspnea (Holas et al., 2017; Stoeckel et al., 2018; Hanania and O’Donnell, 2019). Hence, symptoms of anxiety can aggravate daily functioning and quality of life, and are related to increased healthcare utilization, morbidity, and mortality in COPD (Eisner et al., 2010).
General symptoms of anxiety can be assessed with questionnaires such as the Beck Anxiety Inventory (BAI) (Fydrich et al., 1992), the General Anxiety Disorder-7 (GAD-7) (Spitzer et al., 2006), and the Hospital Anxiety and Depression Scale (HADS) (Zigmond and Snaith, 1983). In COPD, the HADS is most commonly applied (Smid et al., 2017b; Larsen et al., 2021), and was initially developed for use in somatic disease populations to avoid ceiling effects due to overlap between physical symptoms from the somatic disease and the psychological condition, respectively. Routine screening for general symptoms of anxiety and depression are important with the purpose of detecting potential psychological comorbidities in COPD, but the existing instruments has been criticized for suboptimal screening accuracy against diagnostic interviews (Baker et al., 2018). Moreover, recent studies differentiates general from disease-specific symptoms of anxiety in COPD, and stress the importance of assessing both aspects in COPD care (von Leupoldt and Janssens, 2016; Reijnders et al., 2019). Reijnders et al. (2019) showed that greater reductions in COPD-specific anxiety were associated with greater improvements in exercise capacity, quality of life, and health status as well as a more pronounced decrease in depression over the course of a pulmonary rehabilitation program – independent of general anxiety levels. Moreover, Keil et al. (2014) showed that COPD-specific anxiety contributed independently to disease-specific disability after statistically controlling for disease severity, sociodemographic variables, and general anxiety.
While several instruments measuring general symptoms of anxiety exist, fewer disease-specific anxiety measures are available for use in respiratory disease populations. The Anxiety Inventory for Respiratory Disease (Willgoss et al., 2013) was developed according to the same principles as the HADS, where somatic symptoms are excluded. This increases the specificity of the questionnaire, which means that the risk of identifying false positive cases is lowered, but at the same time it reduces the sensitivity, which leads to an increased risk of overseeing true positive cases (Trevethan, 2017; Baker et al., 2018). The Interpretation of Breathing Problems Questionnaire (Sutton et al., 1999) and the Breathlessness Catastrophizing Questionnaire (Solomon et al., 2015) are examples of questionnaires designed to measure dyspnea-related anxiety in respiratory illness, and they are therefore not sensitive toward other aspects of COPD-specific anxiety.
The COPD-Anxiety Questionnaire (CAF) was developed in Germany in 2011 to assess COPD-specific anxiety (Kühl et al., 2011). The original, German-language scale consists of 27 general items and 8 conditional items for patients with a partner and/or who receive oxygen treatment. The items cover the five subdomains of Fear of dyspnea (FD), Fear of physical activity (FPA, Fear of progression (FP), Fear of social exclusion (FSE), and Sleep-related worries (SRW). A shorted, 20-item version (CAF-R) was validated in 2014 (Keil et al., 2014). While questionnaires assessing general symptoms of anxiety have long been available in multiple languages, measurement instruments of disease-specific anxiety were developed relatively recently, and have therefore not yet been translated and validated more broadly.
On this background, the present study aimed to translate the CAF-R into Danish, and to validate the Danish version of the questionnaire (CAF-R-DK) in a sample of patients with COPD, including an initial evaluation of different response formats, i.e., electronic and paper-version.
The translation and initial validation strategy was based on the World Health Organization’s (WHO) guidelines for the process of translation and adaptation of instruments1 and is described in detail below.
The initial translation of the CAF from German into Danish language was performed by the second author (SRR) who is a nurse with considerable experience within respiratory medicine. The translator is knowledgeable of the German-speaking culture and her mother tongue is Danish. The initial translation was based on a conceptual rather than literal approach, aiming at the conceptual equivalent of a given word or phrase rather than a word-by-word translation. Use of technical terms, colloquialism, idioms, or vernacular terms was avoided. Back-translation was performed by two independent native German translators, who had no prior knowledge of the questionnaire. Discrepancies were discussed until an agreement was reached.
An expert panel of researchers from different relevant disciplines (i.e., psychology, respiratory medicine, pulmonary rehabilitation) discussed the Danish translation of the CAF-R. Relevant adjustments of the CAF-R-DK were made on the basis of the suggestions from the panel.
Five pre-test respondents with a diagnosis of COPD were recruited from the pulmonary outpatient clinic at the Department of Medicine, Lillebaelt Hospital, Vejle, Denmark. Each respondent completed the questionnaire individually and immediately thereafter participated in a debriefing asking (1) whether they could repeat the question in their own words, (2) what came to their mind when they heard a particular phrase or term, and (3) explain how they choose their answer. The questions were repeated for each item in the questionnaire. Hereafter, the cognitive interviewing was based on understanding potential conflicts in verbal answers and questionnaire-answers with the purpose of reaching consistency. Relevant adjustments of the CAF-R-DK were made on the basis of the interview material to ensure face validity.
A questionnaire package was distributed electronically via the webpage and social media platforms of the Danish Lung Association. Furthermore, a paper-version of the questionnaire package was distributed among COPD outpatients at the Department of Medicine, Lillebaelt Hospital, Vejle, Denmark. The questionnaire package consisted of the following questionnaires.
The Danish version of the COPD-Anxiety Questionnaire 20-item version (CAF-R-DK) (Keil et al., 2014) was applied to measure COPD-specific anxiety. The questionnaire consists of 20 item each rated on a Likert scale from 0 = “never” to 4 = “always.” The items cover the domains of Fear of dyspnea (“When I become short of breath, I get scared”), Fear of physical activity (“I avoid physical exertion”), Fear of progression (“I fear that someday I will become a burden for others because of my illness”), Fear of social exclusion (“I feel left alone with my illness”), and Sleep-related worries (“I wake up at night because of my breathing”). The original CAF-questionnaire has good internal consistency, with Cronbach’s α of domain scales ranging from α = 0.78 (SRW) to α = 0.87 (FSE, FP) (Keil et al., 2014). The Danish version of the questionnaire can be obtained from the authors upon request.
The COPD Assessment Test (CAT) (Jones et al., 2009) was included with the purpose of measuring COPD-specific disability, or health status, and consists of 8 items that are rated on a semantic differential scale from 0 (e.g., “I am not limited doing any activities at home”) to 5 (e.g., “I am very limited doing activities at home”). The CAT is commonly applied in COPD research and clinical practice and shows good psychometric properties, e.g., Cronbach’s α = 0.88 (Jones et al., 2009, 2011; Kon et al., 2014; Smid et al., 2017a).
The modified Medical Research Council dyspnea scale (mMRC) (Williams, 2017) was applied to measure the degree of dyspnea on a Likert scale from 0 = “I only get breathless with strenuous exercise” to 4 = “I am too breathless to leave the house or I am breathless when getting dressed.” The scale is recommended for baseline assessment of dyspnea in the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines (GOLD, 2017).
The Hospital Anxiety and Depression Scale (HADS) was used to measure symptoms of anxiety and depression. The scale consists of 14 items, including 7 for symptoms of depression (e.g., “I feel as if I am slowed down”) and 7 for general symptoms of anxiety (e.g., “I feel tense or ‘wound up”). Items are rated on a semantic differential scale from 0 (e.g., “Not at all”) to 3 (e.g., “Most of the time”). The scale is commonly used as a screening tool in COPD, with a Cronbach’s α of 0.87 (Baker et al., 2018).
The 12-item Short Form survey (SF-12) (Ware et al., 1996) was applied to measure quality of life by addressing different aspects of emotional states and daily activities (e.g., “Have you felt down-hearted and blue?”; “Have you accomplished less than you would like as a result of your physical health?”). Total scores for the physical components score (PCS) and the mental component score (MCS), respectively, are calculated based on population norms (score range from 0–100), with higher scores indicating better health. The SF-12 demonstrates good sensitivity to change and discriminative values in grades of COPD (Menn et al., 2010).
All analyzes were performed using Stata 17 software (StataCorp. 2021. Stata Statistical Software: Release 17. College Station, TX, United States: StataCorp. LLC). For all analyzes, p-values of ≤ 0.05 were considered statistically significant. Correlation coefficients of 0.20, 0.40, 0.60, and 0.80 were considered weak, moderate, strong, and very strong, respectively. Missing data were imputed by mean substitution, except from the SF-12, where missing data were handled according to the scoring descriptions (Ware et al., 1995) (the full description can be found in Supplementary Material 1). For the CAF-R-DK, missing data on individual items were explored with the purpose of identifying whether particular items in the CAF-R-DK indicated problems in understanding the content (Primdahl et al., 2021).
Convergent validity was tested with Spearman’s rank correlation coefficients. We expected positive correlations with all convergent variables (i.e., CAT, HADS-Anxiety, and HADS-Depression) and negative correlations with discriminant variables (i.e., SF-12 PCS and SF-12 MCS). Reliability was assessed by computing Cronbach’s α. A confirmatory factor analysis was conducted to evaluate whether the factor structure of the CAF-R-DK corresponded to the original CAF-R. If a less than acceptable fit was obtained, a supplementary exploratory factor analysis was performed to evaluate the number of latent variables/subdomains of the CAF-R-DK, and whether individual items belonged to subdomains other than those hypothesized by the original CAF-R. Bartlett’s test of sphericity (Bartlett, 1951) and Kaiser-Meyer-Olkin (KMO) sampling adequacy (Kaiser, 1974) were calculated to ensure that factor analysis was appropriate.
In the period from May to September 2020 a total of 260 participants completed the questionnaire package. Respondents for electronic and paper-based completion were recruited in parallel. A total number of 333 individuals opened the link to the online questionnaire, resulting in 238 (71.5%) completed electronic responses. The remaining responses (n = 22) were paper-based. See Table 1 for an overview of participant characteristics.
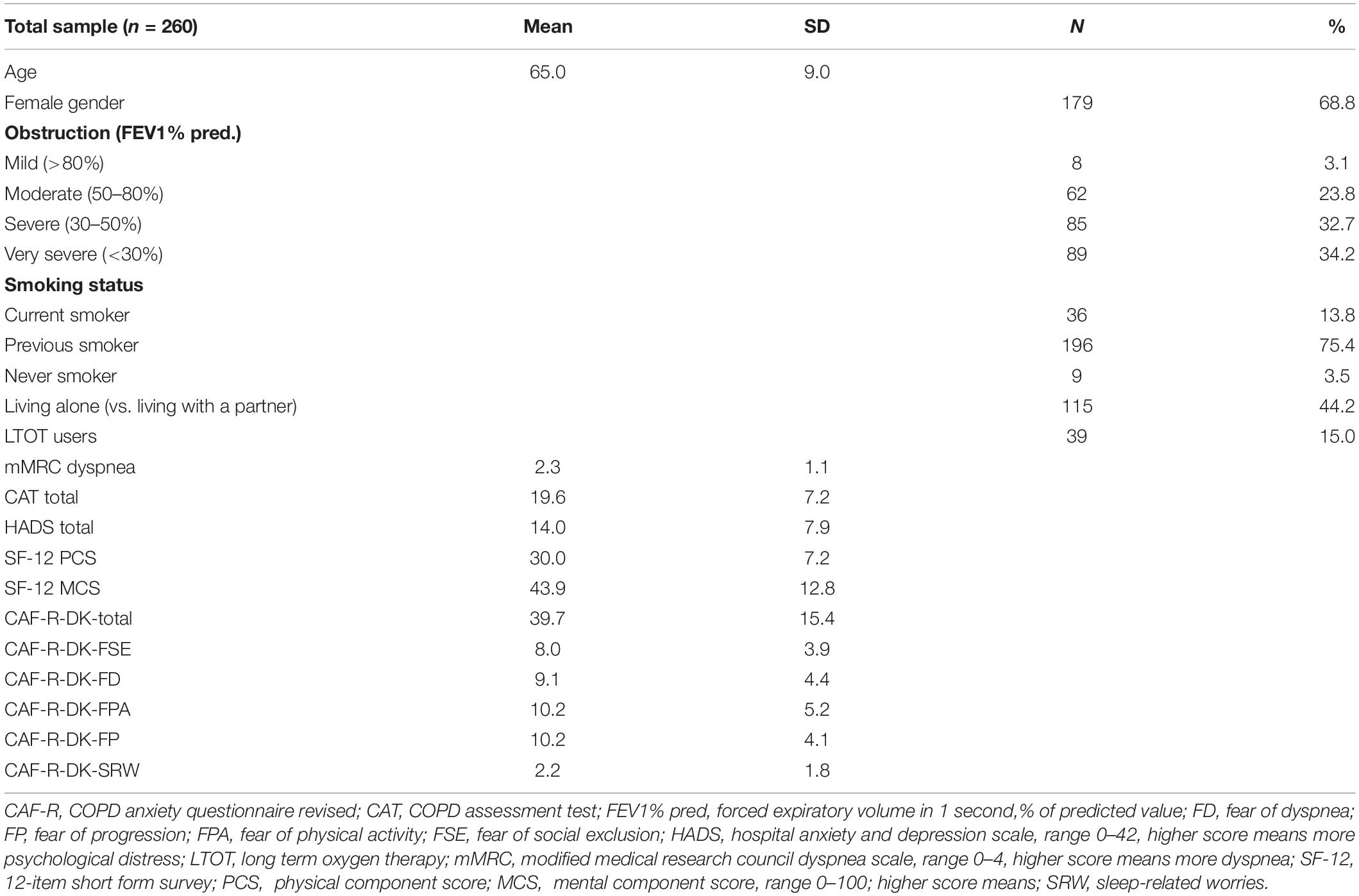
Table 1. Participant characteristics.
Correlation coefficients of all validity and reliability analyzes can be found in Table 2. The CAF-R-DK total score and all individual domain scores showed acceptable to excellent reliability with Cronbach’s α ranging from 0.77 to 0.89. All convergent and discriminant construct showed the expected direction of the correlations (positive correlations for convergent constructs versus negative correlations for discriminant constructs). Correlations with convergent constructs were all moderate to strong (r = 0.39–0.69). The discriminant construct of SF-12 PCS was weakly correlated with the CAF, compared to the SF-12 MCS (PCS r = −0.04 to −0.30; MCS r = −0.43 to −0.67).
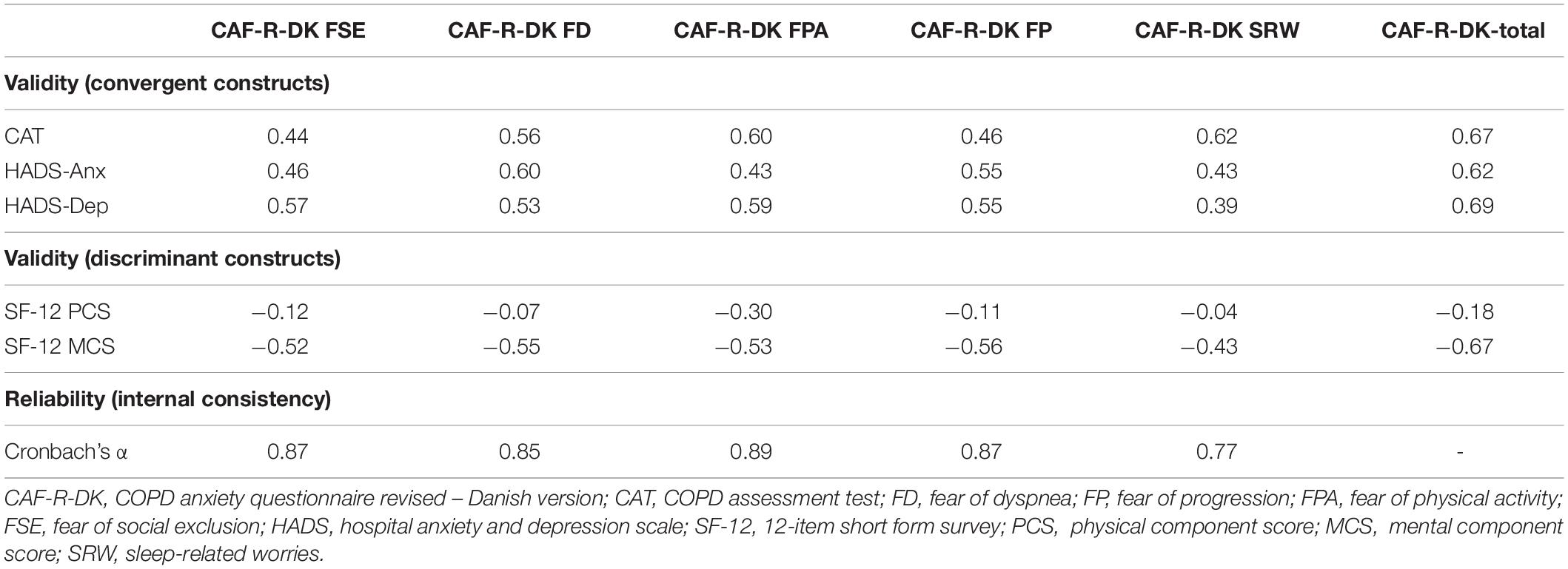
Table 2. Validity and reliability of the chronic obstructive pulmonary disease-anxiety questionnaire revised – Danish version (CAF-R-DK).
The p-value for Bartlett’s test of sphericity was < 0.001 and the KMO measure of sampling adequacy was 0.907, which were both sufficient for conducting factor analysis (Bartlett, 1951; Kaiser, 1974).
A confirmatory factor analysis was conducted to test whether the structure of the CAF-R-DK corresponded to the original version of the questionnaire. The root mean square error of approximation was 0.087 (CIs: 0.077–0.097; p = 0.000), the Comparative Fit Index was 0.911, and the Tucker-Lewis index was 0.894, which altogether indicate a less than acceptable fit (Fan et al., 1999).
Hence, a polychoric exploratory factor analysis with oblique rotation was conducted with the purpose of exploring whether the number of latent variables in the CAF-R-DK was different from those identified in the original version of questionnaire, or whether the individual items loaded on different latent variables than described. Horn’s parallel analysis (Dinno, 2009), together with a scree plot, was conducted with the purpose of assessing the number of latent variables, and the existence of five factors in the questionnaire was confirmed (see graph in Supplementary Material 2). Table 3 shows the factor loadings for each individual item in the CAF-R-DK. For factors 2–5, the loading of the individual items of the CAF-R-DK were comparable to those of the original questionnaire. However, items originally belonging to the subscales of Fear of dyspnea (e.g., “When I get short of breath I am afraid that I will suffocate”), Fear of physical activity (i.e., “I plan the route in detail before I go for a walk”), and Fear of progression (i.e., “I am afraid that my breathing problems will become worse”) all loaded on the same factor (factor 1) in the present dataset.
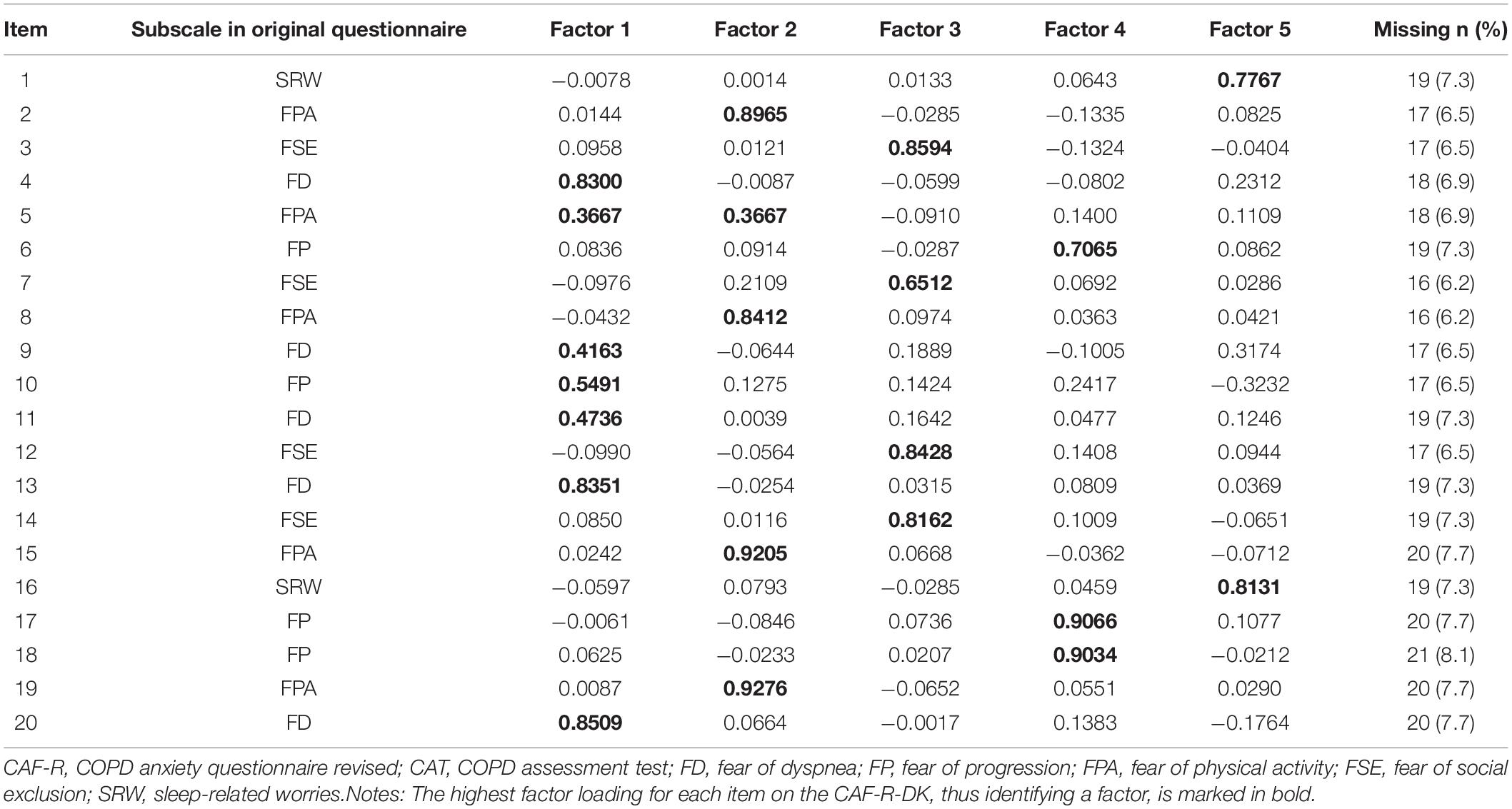
Table 3. Factor loadings of items from the chronic obstructive pulmonary disease-anxiety questionnaire revised – Danish version (CAF-R-DK).
An overview of missing values per item can be found in Table 3. Number of missing values for each item in the CAF-R-DK varied from 16 (6.2%) on Item 8 (“I avoid activities that make me sweat”) to 21 (8.1%) on Item 18 (“I fear that I will eventually become dependent of care from others because of my illness”). Compared to electronic questionnaire responses, paper-based responses had a very low number of missing items, with only one participant missing one item (Item 1).
It has been proposed that many patients with COPD are living with unrecognized symptoms of anxiety due to the poor availability of instruments measuring disease-specific anxiety in this population (Yohannes and Lavoie, 2013; Breland et al., 2015; Larsen et al., 2021). The COPD Anxiety Questionnaire (CAF) is an example of a COPD-specific anxiety instrument that has been developed in German language, but is still not available in multiple languages. For the purpose of the present study, we translated the short version of the CAF (CAF-R) into Danish (CAF-R-DK) and performed an initial validation of its psychometric properties in a sample of 260 patients with COPD across all degrees of obstructive lung function impairment (mild, moderate, severe, and very severe).
The results of the present study indicated that the CAF-R-DK showed acceptable to excellent reliability with Cronbach’s α scores of subscales ranging from 0.77 to 0.89, which are also comparable with reliability scores of the original questionnaire (Cronbach’s α of subscales: 0.78–0.87 (Keil et al., 2014).
With respect to construct validity, the CAF-R-DK showed positive correlations with converging constructs [COPD-symptoms level (CAT), general symptoms of anxiety (HADS-Anxiety), symptoms of depression (HADS-Depression)] and negative correlations with discriminant constructs [physical quality of life (SF-12 PCS), mental quality of life (SF-12 MCS)], as expected. Concerning the individual converging constructs, the total score of the CAF-R-DK showed higher correlations with the HADS-depression scale (r = 0.69), compared to the HADS-anxiety scale (r = 0.62). This is surprising, as the construct of disease-specific anxiety was expected to correlate relatively more with general symptoms of anxiety, compared with symptoms of depression. A possible explanation could be that the correlation with symptoms of depression are driven by the specific CAF-subdomains Fear of social exclusion (r = 0.57) and Fear of physical activity (r = 0.59), which include items such as “I feel let alone with my illness” and “I avoid all kinds of physical activity”. Such items could be interpreted as expressions of hopelessness and lethargy, respectively, which are characteristic of depressive states (Osler, 2021). Moreover, the converging construct of COPD symptoms, measured with the CAT, also showed a relatively higher correlation (r = 0.67) with the CAF-R-DK total score, than the HADS-Anxiety. This was especially the case for the CAF-subdomains of Fear of physical activity (r = 0.60) and Sleep-related worries (r = 0.62), the latter consisting of items such as “The sound of my breathing or coughing wake me up at night”. The wording of such items could be more indicative of physical symptom level than of anxious symptom interpretation, which may explain the higher correlation of the CAF-R-DK with COPD symptom level than with general symptoms of anxiety. On the other hand, when inspecting correlations of the CAF-R-DK with the discriminant constructs of physical and mental quality of life, all subdomains of the CAF-R-DK showed considerably stronger correlations with the mental component score of the SF-12 (r = −0.67), compared with the physical component score (r = −0.18). This finding supports CAF-R-DK as measuring the predominantly psychological, not physical, construct of disease-specific anxiety. Taken together, the present study results indicate that disease-specific anxiety in COPD can be understood as a psychophysiological construct, including and correlating strongly with physical symptoms and sensations (O’Donnell et al., 2007; Ora et al., 2010; Hanania and O’Donnell, 2019). However, the results could also be indicative of relatively poor construct validity and wording of individual items in the CAF, which should be kept in mind when applying the questionnaire and interpreting its results in future studies and clinical practice. As the present study did not perform a direct comparison between the original version and the Danish translation of the questionnaire, it is unknown whether these findings are true only for the CAF-R-DK, or whether they could be extrapolated to the CAF more generally. However, the developers of the original version of the CAF (Kühl et al., 2011) appear to have collected relatively limited data for the conceptualization of disease-specific anxiety prior to designing the questionnaire, i.e., five patient interviews and items from the Cardiac Anxiety Questionnaire (Eifert et al., 2000), which may have compromised the construct validity of the questionnaire. In addition to cardiac-related anxiety, the construct of disease-specific anxiety in COPD may also share features with anxiety in asthma, measured with the Asthma-Related Anxiety Scale (Bruzzese et al., 2011). Moreover, in other to determine the specific characteristics of anxiety in COPD in the future, a mapping of shared and distinctive features of anxiety in COPD, asthma, cardiac disease, multiple sclerosis and other diseases that are characterized by chronic impairment and a high risk of acute symptom worsening (i.e., exacerbations; attacks) is needed (Murray et al., 2005).
Furthermore, concerning the internal consistency of the CAF-R-DK, the initial confirmatory factor analysis of the structure of the original version of the questionnaire did not result in a good fit to the data in the present study. In the subsequent exploratory factor analysis, the five-factor structure of the questionnaire was confirmed, but individual items that belonged to the Fear of physical activity (i.e., “I plan the route in detail before I go for a walk”) and Fear of disease progression (i.e., “I am afraid that my breathing problems will become worse”) subscales in the original version of the questionnaire loaded on the Fear of dyspnea scale (e.g., “When I get short of breath I am afraid that I will suffocate”) in the present study. The results do not allow for any conclusions as to whether these differences stem from language- or cultural differences between the German and Danish version of the questionnaire or whether they are resulting from a suboptimal scale construction of the original version of the CAF. However, researchers and clinicians should be aware that it can be difficult to differentiate certain latent variables of disease-specific anxiety, and there may be significant overlap between the experience of fear of dyspnea, fear of physical activity, and fear of disease progression.
When inspecting the number of missing answers for the items in CAF-R-DK, there was a relatively high proportion of missing values across all items (6.2–8.1%). As 16 respondents (6.2%) missed the entire CAF-R-DK, the missing responses are less likely to be a result of poor understanding of individual items. Missing values were predominantly observed for the electronic responses, while only one participant missed one item in the paper-based responses. This may speak to an increased feasibility of the paper-version of the CAF-R, but it also stands in contrast to other studies, showing a higher number of missing in paper-based responses (Palen et al., 2008; Shih and Fan, 2009), and the feasibility of electronic vs. paper-based questionnaire formats appears to depend on the specific respondent population (Shih and Fan, 2009). Hence, the relatively high missing rates in the electronic responses of the present study should not prevent researchers from using the electronic format in future studies. However, “forced responding” in the electronic version of the CAF could be considered (Nayak and Narayan, 2019).
The results of the present study expand the availability of instruments for the assessment of disease-specific anxiety in COPD, which is relevant for psychological screening in routine care, e.g., rehabilitation clinics, general practice, and outpatient hospital visits. In a study by Hardy et al. (2014), primary care nurses were trained in following a systematic psychological screening and intervention pathway during the annual review of 35 patients with COPD. The results of their evaluation showed that 75% of the patients felt pleased about being asked questions regarding depression and anxiety, while the remaining patients reported that they had no particular feelings. Moreover, 91% reported that they felt more motivated to manage their symptoms after the screening and consultation with the nurse. On the other hand, screening and assessment of anxiety in clinical practice can be obstructed by certain barriers among healthcare professionals. In an editorial, Heslop-Marshall and Burns (2019) present three important barriers: (1) Clinicians may not recognize the scale of the problem, assuming that the symptoms of anxiety is a natural part of the ‘psychological makeup’ of the patient with COPD; (2) Clinicians may consider psychological symptoms to be outside their professional remit; (3) Access to appropriate therapy and availability of trained therapists are scarce, and clinicians may therefore consider identification of psychological symptoms pointless. The results of the present study do not allow for conclusions it terms of (barriers to) the practical use of the CAF-R-DK, and it is therefore important to address such barriers in future research with the purpose of achieving and optimal implementation of psychological screening procedures in clinical practice.
Moreover, when applying instruments such as the CAF, clinicians should be aware that a high CAF-score is not necessarily equal to high level of general symptoms of anxiety or to the presence of a mental disorder, e.g., panic disorder, generalized anxiety disorder, social phobia, and post-traumatic stress disorder, for all of which a high prevalence rate has been demonstrated in COPD (Yohannes et al., 2010; Willgoss and Yohannes, 2013; Ouellette and Lavoie, 2017). Disease-specific anxiety and accompanying, maladaptive avoidance or safety behaviors could potentially increase the risk of developing an anxiety disorder, but future studies, including diagnostic interviews, are needed to confirm the relationship between disease-specific anxiety and the development of anxiety disorders and other mental disorders in COPD.
The present study has several strengths. First, owing to the electronic participation option, the study is based on a large sample of patients with COPD with all degrees of obstructive lung function impairment (mild, moderate, severe, and very severe), including a considerable proportion of long-term oxygen therapy users (15%) who can be difficult to reach for research purposes. Second, the translation of the CAF-R into Danish is based on a comprehensive and systematic approach, which ensures a high-quality version of the questionnaire ready for application in the Nordic countries. Third, taking a comprehensive approach to measurement, the questionnaire package of the present study includes several relevant scales that allows for assessment of associations with both convergent and discriminant constructs.
However, a number of limitations should also be noted. First, the questionnaire format, i.e., electronically versus paper-based, were applied in two different recruitment setups, i.e., patient organization versus outpatient clinic, and a direct comparison of the response formats could therefore not be performed. Studies using random assignment to electronic versus paper versions of the questionnaire are needed to test whether the response format impacts the validity of the questionnaire. Second, due to recruitment anonymity for online respondents, and with the purpose of limiting participation burden for patients in the present study, the single measurement design did not allow for assessment of test-retest reliability of the questionnaire. A more comprehensive testing of the psychometric properties of the CAF-R-DK is needed to confirm longitudinal, predictive validity and reliability. Third, while the CAF is currently the only existing instrument measuring COPD-specific anxiety beyond fear of dyspnea, the quality of the questionnaire can be criticized: (a) The initial conceptualization of the construct of COPD-specific anxiety was based on five patient interviews (Kühl et al., 2011), which can be considered as a relatively restricted database (de Vet et al., 2011). (b) The developers of the questionnaire (Kühl et al., 2011) claim that the wording of the items was based on the Cardiac Anxiety Questionnaire (Eifert et al., 2000). But very few similarities between the wording of the two questionnaires can be found, and several items of the CAF does not adhere to suggested standards for item wording (e.g., avoiding negative wording; items should be specific) (de Vet et al., 2011). (c) The questionnaire has not been translated into English, leading to relatively limited application and testing of the questionnaire worldwide. Lastly, due to the experiential nature of the construct of anxiety, it is not possible to validate the scale against a “gold standard,” objective measurement method, which prevents the analyzes of predictive validity as well as the determination of a clinically significant cut-point. Future studies could benefit from performing a direct comparison between CAF scores and diagnostic interviewing by a mental health specialist.
A Danish version of the COPD-Anxiety Questionnaire (CAF-R-DK) is now available for the assessment of disease-specific anxiety in Danish-speaking patients with COPD. The CAF should not be used as an alternative to screening for symptoms of anxiety in general, but can be applied as an important supplement to the Hospital Anxiety and Depression Scale (HADS) (as an example) with the purpose of identifying relevant areas of disease-specific anxiety that might act as barriers for outcomes of rehabilitation programs. There might be general inconsistencies in the construct validity of the CAF-R-DK and/or the CAF in general. In the future, there is a need for translation of the questionnaire into other languages with the purpose of obtaining clinical and research-based data on the psychometric properties and practical application of the CAF. Moreover, there is a need for studies that aim to test measures of disease-specific anxiety against general anxiety questionnaires and diagnostic interviews in COPD.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
IF-V had a leading role in the conception and design of the present study as well as in the data analysis and drafting of the present manuscript. SR-R had a leading role in data acquisition. ST contributed to the statistical analysis. SR-R, ST, CFC, OH, and AL contributed to the conception and interpretation of data for the work and to revising the contents of the present manuscript. All authors provided approval for publication of the content of the present manuscript and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
The Innovation Fund at Lillebaelt Hospital, the Danish Regions’ prevention research fund (grant number: EMN-2019-00852 1357604) and the Health Foundation (www.helsefonden.dk) (grant number: 20A0122) provided funding for the present study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank Theresa Htrewneets and Britta Japp for assisting with the translation of the questionnaire. We thank the staff in the pulmonary outpatient clinic at the Department of Medicine, Lillebaelt Hospital, and Vejle for assistance in distributing questionnaires. We also thank the Danish Lung Association for assistance in distributing the survey link.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2022.907939/full#supplementary-material
Baker, A. M., Holbrook, J. T., Yohannes, A. M., Eakin, M. N., Sugar, E. A., Henderson, R. J., et al. (2018). Test performance characteristics of the AIR, GAD-7, and HADS-anxiety screening questionnaires for anxiety in chronic obstructive pulmonary disease. Ann. Am. Thorac. Soc. 15, 926–934. doi: 10.1513/AnnalsATS.201708-631OC
Bartlett, M. S. (1951). The effct of standardization on a Chi-aquare approximation in factor analysis. Biometrika 38, 337–344.
Breland, J. Y., Hundt, N. E., Barrera, T. L., Mignogna, J., Petersen, N. J., Stanley, M. A., et al. (2015). Identification of Anxiety Symptom Clusters in Patients with COPD: implications for Assessment and Treatment. Int. J. Behav. Med. 22, 590–596. doi: 10.1007/s12529-014-9450-2
Bruzzese, J. M., Unikel, L. H., Shrout, P. E., and Klein, R. G. (2011). Youth and parent versions of the asthma-related anxiety scale: development and initial testing. Pediatr. Allergy Immunol. Pulmonol. 24, 95–105. doi: 10.1089/ped.2011.0076
de Vet, H. C. W., Mokkink, L. B., Knol, D. L., and Terwee, C. B. (2011). Measurement in Medicine: A Practical Guide. Cambridge: Cambridge University Press.
Dinno, A. (2009). Implementing Horn’s parallel analysis for principal component analysis and factor analysis. Stata J. 9, 291–298. doi: 10.1177/1536867x0900900207
Eifert, G. H., Thompson, R. N., Zvolensky, M. J., Edwards, K., Frazer, N. L., Haddad, J. W., et al. (2000). The Cardiac Anxiety Questionnaire: development and preliminary validity. Behav. Res. Ther. 38, 1039–1053. doi: 10.1016/S0005-7967(99)00132-1
Eisner, M. D., Blanc, P. D., Yelin, E. H., Katz, P. P., Sanchez, G., Iribarren, C., et al. (2010). Influence of anxiety on health outcomes in COPD. Thorax 65, 229–234. doi: 10.1136/thx.2009.126201
Fan, X., Thompson, B., and Wang, L. (1999). Effects of sample size, estimation method, and model specification on structural equation modeling fit indexes. Struct. Equ. Model. 6, 56–83.
Fydrich, T., Dowdall, D., and Chambless, D. L. (1992). Reliability and validity of the beck anxiety inventory. J. Anxiety Disord. 6, 55–61. doi: 10.1016/0887-6185(92)90026-4
GOLD (2017). Global Initiative for Chronic Obstructive Lung A Guide for Health Care Professionals Global Initiative for Chronic Obstructive Disease. Available online at: www.goldcopd.org (accessed June 24, 2022).
Hanania, N. A., and O’Donnell, D. E. (2019). Activity-related dyspnea in chronic obstructive pulmonary disease: physical and psychological consequences, unmet needs, and future directions. Int. J. COPD 14, 1127–1138. doi: 10.2147/COPD.S188141
Hardy, S., Smart, D., Scanlan, M., and Rogers, S. (2014). Integrating psychological screening into reviews of patients with COPD. Br. J. Nurs. 23, 832–836. doi: 10.12968/bjon.2014.23.15.832
Heslop-Marshall, K., and Burns, G. (2019). The role of cognitive behavioural therapy in living well with COPD. Breathe 15, 95–97. doi: 10.1183/20734735.0119-2019
Holas, P., Michałowski, J., Gaweda, Ł, and Domagała-Kulawik, J. (2017). Agoraphobic avoidance predicts emotional distress and increased physical concerns in chronic obstructive pulmonary disease. Respir. Med. 128, 7–12. doi: 10.1016/j.rmed.2017.04.011
Jones, P., Harding, G., Berry, P., Wiklund, I., Chen, W.-H., and Kline Leidy, N. (2009). Development and first validation of the COPD Assessment Test. Eur. Respir. J. 34, 648–654. doi: 10.1183/09031936.00102509
Jones, P. W., Brusselle, G., Dal Negro, R. W., Ferrer, M., Kardos, P., Levy, M. L., et al. (2011). Properties of the COPD assessment test in a cross-sectional European study. Eur. Respir. J. 38, 29–35. doi: 10.1183/09031936.00177210
Keil, D. C., Stenzel, N. M., Kühl, K., Vaske, I., Mewes, R., Rief, W., et al. (2014). The impact of chronic obstructive pulmonary disease-related fears on disease-specific disability. Chron. Respir. Dis. 11, 31–40. doi: 10.1177/1479972313516881
Kon, S. S. C., Canavan, J. L., Jones, S. E., Nolan, C. M., Clark, A. L., Dickson, M. J., et al. (2014). Minimum clinically important difference for the COPD Assessment Test: a prospective analysis. Lancet Respir. Med. 2, 195–203. doi: 10.1016/S2213-2600(14)70001-3
Kühl, K., Kuhn, C., Kenn, K., and Rief, W. (2011). [The COPD-Anxiety-Questionnaire (CAF): a new instrument to assess illness specific anxiety in COPD patients]. Psychother. Psychosom. Med. Psychol. 61, e1–e9. doi: 10.1055/s-0030-1248281
Larsen, C. H., Bendstrup, E., and Neergaard, M. A. (2021). Screening Tools for Depression and Anxiety in Patients with Chronic Obstructive Pulmonary Disease–A Systematic Review. COPD J. Chronic Obstr. Pulm. Dis. 18, 683–689. doi: 10.1080/15412555.2021.1972091
Menn, P., Weber, N., and Holle, R. (2010). Health-related quality of life in patients with severe COPD hospitalized for exacerbations - comparing EQ-5D, SF-12 and SGRQ. Health Qual. Life Outcomes 8:39. doi: 10.1186/1477-7525-8-39
Murray, S. A., Kendall, M., Boyd, K., and Sheikh, A. (2005). Illness trajectories and palliative care. BMJ 330, 1007–1011. doi: 10.1136/bmj.330.7498.1007
Nayak, M., and Narayan, K. A. (2019). Strengths and weakness of online surveys. IOSR J. Humanit. Soc. Sci. 24, 31–38. doi: 10.9790/0837-2405053138
O’Donnell, D. E., Banzett, R. B., Carrieri-Kohlman, V., Casaburi, R., Davenport, P. W., Gandevia, S. C., et al. (2007). Pathophysiology of dyspnea in chronic obstructive pulmonary disease. Proc. Am. Thorac. Soc. 4, 145–168. doi: 10.1513/pats.200611-159CC
Ora, J., Jensen, D., and O’Donnell, D. E. (2010). Exertional dyspnea in chronic obstructive pulmonary disease: mechanisms and treatment approaches. Curr. Opin. Pulm. Med. 16, 144–149. doi: 10.1097/MCP.0b013e328334a728
Osler, L. (2021). Bodily saturation and social disconnectedness in depression. Phenomenol. Mind 21, 48–61.
Ouellette, D. R., and Lavoie, K. L. (2017). Recognition, diagnosis, and treatment of cognitive and psychiatric disorders in patients with COPD. Int. J. COPD 12, 639–650.
Palen, L. A., Graham, J. W., Smith, E. A., Caldwell, L. L., Mathews, C., and Flisher, A. J. (2008). Rates of missing responses in Personal Digital Assistant (PDA) versus paper assessments. Eval. Rev. 32, 257–272. doi: 10.1177/0193841X07307829
Primdahl, J., Esbensen, B. A., Pedersen, A. K., Bech, B., and de Thurah, A. (2021). Validation of the Danish versions of the Bristol Rheumatoid Arthritis Fatigue Multi-Dimensional Questionnaires (BRAFs). Scand. J. Rheumatol. 50, 351–359. doi: 10.1080/03009742.2020.1869301
Reijnders, T., Schuler, M., Wittmann, M., Jelusic, D., Troosters, T., Janssens, W., et al. (2019). The impact of disease-specific fears on outcome measures of pulmonary rehabilitation in patients with COPD. Respir. Med. 146, 87–95. doi: 10.1016/j.rmed.2018.12.004
Shih, T.-H., and Fan, X. (2009). Comparing response rates in e-mail and paper surveys: a meta-analysis. Educ. Res. Rev. 4, 26–40.
Smid, D. E., Franssen, F. M. E., Houben-Wilke, S., Vanfleteren, L. E. G. W., Janssen, D. J. A., Wouters, E. F. M., et al. (2017b). Responsiveness and MCID Estimates for CAT, CCQ, and HADS in Patients With COPD Undergoing Pulmonary Rehabilitation: a Prospective Analysis. J. Am. Med. Dir. Assoc. 18, 53–58. doi: 10.1016/j.jamda.2016.08.002
Smid, D. E., Franssen, F. M. E., Gonik, M., Miravitlles, M., Casanova, C., Cosio, B. G., et al. (2017a). Redefining Cut-Points for High Symptom Burden of the Global Initiative for Chronic Obstructive Lung Disease Classification in 18,577 Patients With Chronic Obstructive Pulmonary Disease. J. Am. Med. Dir. Assoc. 18, 1097.e11–1097.e24. doi: 10.1016/j.jamda.2017.09.003
Solomon, B. K., Wilson, K. G., Henderson, P. R., Poulin, P. A., Kowal, J., and McKim, D. A. (2015). A Breathlessness Catastrophizing Scale for chronic obstructive pulmonary disease. J. Psychosom. Res. 79, 62–68. doi: 10.1016/j.jpsychores.2014.11.020
Spitzer, R. L., Kroenke, K., Williams, J. B. W., and Löwe, B. (2006). A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch. Intern. Med. 166, 1092–1097. doi: 10.1001/archinte.166.10.1092
Stoeckel, M. C., Esser, R. W., Gamer, M., Büchel, C., and von Leupoldt, A. (2018). Dyspnea catastrophizing and neural activations during the anticipation and perception of dyspnea. Psychophysiology 55:e13004. doi: 10.1111/psyp.13004
Sutton, K., Cooper, M., Pimm, J., and Wallace, L. (1999). Anxiety in Chronic Obstructive Pulmonary Disease: the Role of Illness Specific Catastrophic Thoughts. Cognit. Ther. Res. 23, 573–585.
Trevethan, R. (2017). Sensitivity, Specificity, and Predictive Values: foundations, Pliabilities, and Pitfalls in Research and Practice. Front. Public Health 5:307. doi: 10.3389/fpubh.2017.00307
von Leupoldt, A. (2017). Treating anxious expectations can improve dyspnoea in patients with COPD. Eur. Respir. J. 50:1701352. doi: 10.1183/13993003.01352-2017
von Leupoldt, A., and Janssens, T. (2016). Could targeting disease specific fear and anxiety improve COPD outcomes? Expert Rev. Respir. Med. 10, 835–837. doi: 10.1080/17476348.2016.1198697
Ware, J. E., Kosinski, M., and Keller, S. D. (1995). SF-12: How to Score the SF-12 Physical and Mental Health Summary Scales. Boston, MA: The Helath Institute.
Ware, J. E., Kosinski, M., and Keller, S. D. (1996). A 12-Item short-form health survey: construction of scales and preliminary tests of reliability and validity. Med. Care 34, 220–233. doi: 10.1097/00005650-199603000-00003
Willgoss, T. G., Goldbart, J., Fatoye, F., and Yohannes, A. M. (2013). The development and validation of the anxiety inventory for respiratory disease. Chest 144, 1587–1596. doi: 10.1378/chest.13-0168
Willgoss, T. G., and Yohannes, A. M. (2013). Anxiety disorders in patients with COPD: a systematic review. Respir. Care 58, 858–866. doi: 10.4187/respcare.01862
Williams, N. (2017). The MRC breathlessness scale. Occup. Med. 67, 496–497. doi: 10.1093/occmed/kqx086
Yohannes, A. M., and Lavoie, K. L. (2013). Overseeing anxiety and depression in patients with physical illness. Chest 144, 726–728. doi: 10.1378/chest.13-0511
Yohannes, A. M., Willgoss, T. G., Baldwin, R. C., and Connolly, M. J. (2010). Depression and anxiety in chronic heart failure and chronic obstructive pulmonary disease: prevalence, relevance, clinical implications and management principles. Int. J. Geriatr. Psychiatry 25, 1209–1221. doi: 10.1002/gps.2463
Keywords: disease-specific fear, respiratory illness/disease, psychological distress, assessment, measurement, Danish translation
Citation: Farver-Vestergaard I, Rubio-Rask S, Timm S, Christiansen CF, Hilberg O and Løkke A (2022) Disease-Specific Anxiety in Chronic Obstructive Pulmonary Disease: Translation and Initial Validation of a Questionnaire. Front. Psychol. 13:907939. doi: 10.3389/fpsyg.2022.907939
Received: 30 March 2022; Accepted: 20 June 2022;
Published: 05 July 2022.
Edited by:
Paolo Innocente Banfi, Fondazione Don Carlo Gnocchi Onlus (IRCCS), ItalyReviewed by:
Qaisar Khalid Mahmood, International Islamic University, PakistanCopyright © 2022 Farver-Vestergaard, Rubio-Rask, Timm, Christiansen, Hilberg and Løkke. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ingeborg Farver-Vestergaard, aW5nZWJvcmcuZmFydmVyQHJzeWQuZGs=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.