 Yuewei Wang1†
Yuewei Wang1† Zhili Liu
Zhili Liu- 1Central Sterile Supply Department (CSSD), The First Affiliated Hospital of Shantou University Medical College, Shantou, China
- 2Cardiac Care Unit (CCU), The First Affiliated Hospital of Shantou University Medical College, Shantou, China
- 3Department of Neurology, The First Affiliated Hospital of Shantou University Medical College, Shantou, China
Objective: This article explores the effect of preoperative health education, in the form of animation videos, on postoperative self-reported pain levels and anxiety in femoral fractures.
Methods: Ninety cases of femoral fracture were divided at random into the oral instruction group, the recorded video group, and the animation video group, with 30 cases in each group. Sociodemographic data were collected the day before surgery. Health education was then offered in one of three ways: orally, using a recorded video, or using an animation video. On days 2, 4, and 7 after surgery, the state-trait anxiety inventory (STAI) and the visual analog scale (VAS) were used to assess postoperative anxiety and pain levels, respectively, in the participants.
Results: At different time points during the evaluation, total anxiety scores in the animation and recorded video groups were significantly lower than in the oral instruction group (P < 0.01), and the pairwise comparisons indicated statistically significant differences (F = 11.04, 10.06, 10.37, P < 0.01). However, the levels of postoperative pain in the animation and recorded video groups were not significantly different (P > 0.05). STAI scores in the three groups were found to have significant interactions with the measurement time (F = 6.74, P < 0.01). However, there were no apparent interactions between the VAS score and the measurement time (F = 1.31, P > 0.05) in the three groups.
Conclusion: Preoperative health education with the aid of multimedia is more effective than oral instruction in lowering patients’ postoperative anxiety and pain levels. In addition, animation videos are superior to recorded videos in mitigating postoperative anxiety. Whether the two approaches differ in reducing postoperative pain in bone fractures remains to be further tested.
Introduction
Patients scheduled to undergo surgery for a femoral fracture might experience preoperative anxiety due to a sense of uncertainty about the prognosis (Huang et al., 2005). In the case of postoperative adverse events, the patients will likely suffer from postoperative anxiety and pain (Ma et al., 2021). Pain is an experience in which psychological factors play a key role (Varallo et al., 2021). Among these, in postoperative pain, anxiety plays a significant role (Zhang et al., 2021). Therefore, health education interventions aimed at reducing anxiety could also have an impact on pain (Kuo et al., 2021). In China, the overall incidence of preoperative anxiety in adult patients ranges from 11 to 80%, Anxiety in most patients started days to hours before surgery, and 82.4% had anxiety on the day of surgery (Gong and Zhao, 2018). Surgery-related anxiety and postoperative pain may cause sleep disorders, and other psychological and physiological complications (Li et al., 2021). If any of these conditions occur, postoperative recovery will be delayed and hospitalization length may be prolonged. This also adds to the health-related financial burden for both patients and society as a whole. According to health data published in China, 15 million people suffer from surgery-related anxiety every year, and 22.50 million report postoperative pain. For every extra day spent in the hospital, the total annual increase in hospitalization expenditure will be 13.13 billion RMB (Weiser et al., 2008; National Bureau of Statistics of the People’s Republic of China, 2011; Ministry of Health of the People’s Republic of China, 2012).
Evidence suggested that preoperative health education might be effective in reducing the incidence (Ayyadhah Alanazi, 2014). Effective preoperative health education not only enables patients to acquire relevant knowledge of the disease, but also enables the patient to actively cooperate with the doctor’s treatment, which is conducive to the recovery of the disease and reduces the occurrence of postoperative complications such as anxiety and postoperative pain in surgical patients, promote recovery, shorten hospital stays, and reduce medical costs (Wong et al., 2010). Therefore, the significance and role of health education are becoming more and more important. Medical staff do this work seriously and implement effective education content according to the needs of patients. At the same time, attention should also be paid to the health education of patients. At present, the research on the effect of preoperative education on anxiety and pain after femoral fracture is not enough to support its clinical application. In view of this, to examine the impact of three different preoperative guidance on postoperative complications in surgical patients in order to provide strong evidence for clinical application. In this study, we use three preoperative health education approaches (animation video, recorded video, and oral instruction) among patients with femoral fractures and measure the effects of these methods on postoperative anxiety and pain.
Subjects
Inclusion Criteria
Ninety patients, hospitalized between October 2012 and June 2013 in the Department of Orthopedics of a hospital, were included in our analysis, in accordance with the following criteria: (a) having undergone surgery for femoral fracture at the Department of Orthopedics, (b) aged over 18 years, (c) no auditory and visual disabilities, (d) awake consciousness and no psychological impairments, (e) able to speak and understand Mandarin, (f) agreed not to use analgesics after surgery, and (g) willing to participate in this experiment give their informed consent. Patient exclusion criteria for the study were as follows: cases not hospitalized in the Department of Orthopedics, or not receiving surgery for the first time, or for reasons other than femoral fracture.
Grouping
A quasi-experimental design and three-group pre–post tests were adopted, with 30 cases in each group. Data from cases that met the exclusion criteria or who asked to leave the study were eliminated. To compensate for excluded participants, another case that met the inclusion criteria was selected. The study was approved by the Medical Ethics Committee of our hospital. In this experiment, the cases were equally divided into the animation group (who were instructed by watching an animated video), the recorded video group, and the control group (instructed orally). The case information was collected by the most convenient method possible. In order to avoid interference between patients, data from the control group were collected first, followed by data from the recorded video group and, finally, from the animation group. The preoperative data collection was performed 1 day before surgery, and consent was obtained from the patients. The informed consent for the three groups is listed in Table 1.
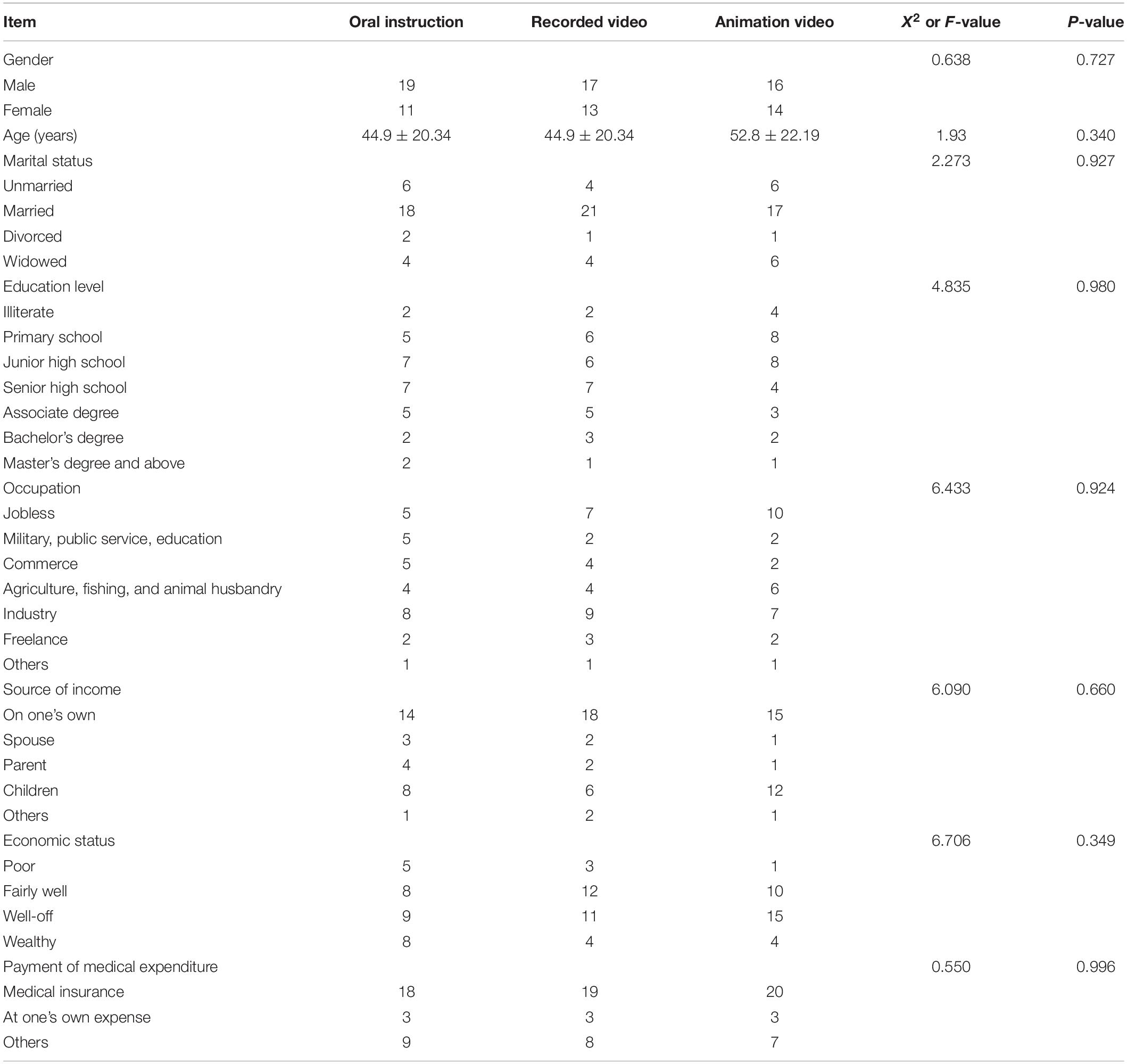
Table 1. General data from the three groups.
Materials and Methods
Approaches Toward Preoperative Health Education
The pre-intervention data were collected from all three groups. The measurement time points, the form of preoperative health education, and the specific content of preoperative health education are shown in Tables 2–4, respectively. In the 10-min health education, the video time is 3.5 min, the animation group will watch the animation video for 3.5 min, and the video group will watch the recorded video for 3.5 min. The content includes: fasting after 10:00, resting early, taking a bath if the condition allows, and the next day at 7:30 a.m., the family members will arrive at the ward and go to the operating room with the patient to introduce the general steps of the operation and the operating room environment.

Table 2. Time points of measurement.
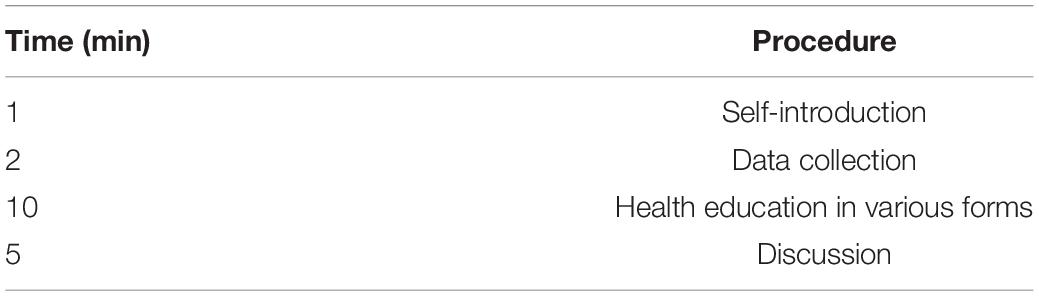
Table 3. Procedures of pre-operative health education.
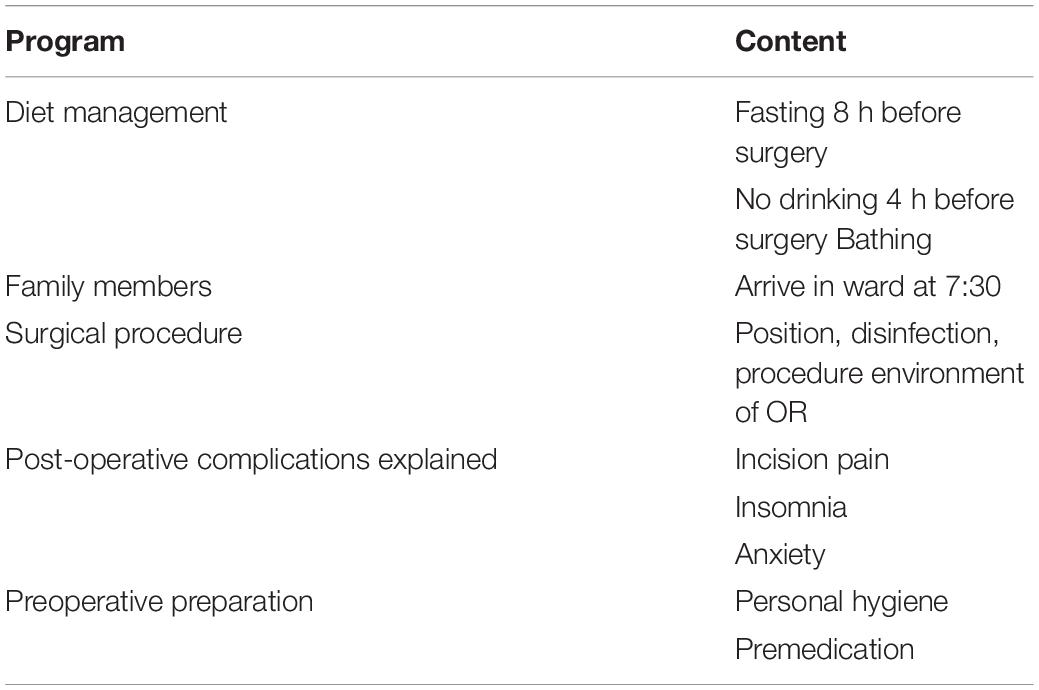
Table 4. Preoperative health education program.
Evaluation
Evaluation of Anxiety Levels
The Chinese version of the state-trait anxiety inventory (STAI) was administered to the patients in the three groups. This scale can distinguish between state (temporary) and trait (stable) anxiety and applies extensively to adults with anxiety disorders (Zhang, 2005).
Questions 1–20, corresponding to state anxiety, determined how the patients felt during the recent or perioperative period and assessed such feelings as fear, tension, worry, and nervousness. Questions 21–40, corresponding to trait anxiety, measured the frequency of anxiety. The cumulative scores of the state and trait anxiety scales were calculated, and the allowable range was 20–80 points. The higher the score, the higher the level of the specified type of anxiety.
Evaluation of the Pain Level
Postoperative pain was measured using visual analog scale (VAS) on a horizontal 10 cm-long straight line. A score of 0 indicated no pain, while a score of 10 indicated severe pain. The higher the score, the greater the degree of postoperative pain.
The author of this scale declared that the scale might be used for free without authorization. In addition, the scales used in this paper had good validity (Reips and Funke, 2008).
Quality Control
To create content for the preoperative health education methods, patients, operating room medical staff, and ward employees were interviewed before surgery and asked what subject matter should be included. These interview results were integrated with the experience of the researchers and their knowledge of evidence-based medicine. A pilot experiment was carried out using the produced video program, 10 patients with femoral fracture were selected to watch the video, and the length of the video was adjusted according to the experimental results of the patients to make it more concise and suitable for repeated viewing. Patient sampling was carried out using conventional methods, and patient groups were restricted from conferring with each other. Patients within groups were encouraged to learn from each other, and patients were rewarded with a small gift to increase their level of attention and participation in the study.
Statistical Processing
Data were statistically analyzed using SPSS 20.0 software. The measurement data were expressed as . The data of the three groups before and after surgery were compared using repeated-measures analysis of variance. Enumeration data were analyzed by the Chi-square test or Fisher’s exact test. P < 0.05 was considered statistically significant.
Results
Anxiety Levels of the Three Groups at Different Time Points
As seen from Table 5 and Figure 1, the preoperative STAI scores were not significantly different among the three groups (P > 0.05). All the STAI scores in the animation video group were much lower than those of the recorded video group on days 2, 4, and 7 after surgery. The STAI scores of the latter were markedly lower than those of the oral instruction group (P < 0.01). The STAI scores of the three groups varied in different ways throughout the duration of the study, which suggested an interaction with the factor of time (F = 6.74, P < 0.01, Table 6). The anxiety level was lowest in the animation video group and highest in the control group.

Table 5. Anxiety levels in the three groups.
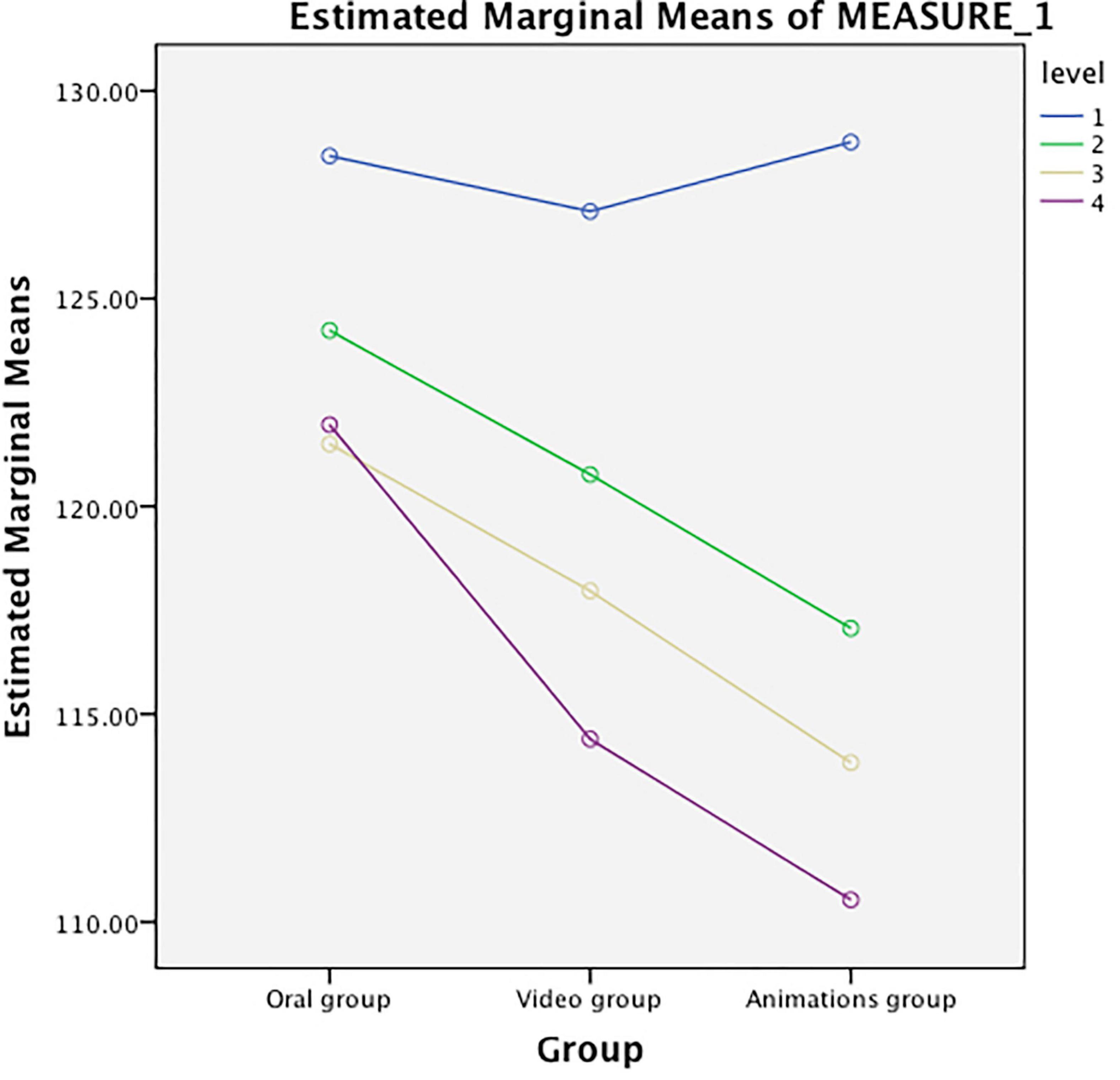
Figure 1. Intergroup differences in the anxiety levels between the three groups.

Table 6. Interaction between anxiety level and time.
Pain Levels in the Three Groups at Different Time Points
As shown in Table 7 and Figure 2, the three groups did not differ significantly from each other in terms of the VAS scores before surgery (P > 0.05). On days 2, 4, and 7 after surgery, the VAS scores in the animation video group showed no distinct differences from those in the recorded video group (P > 0.05). In these two groups, the VAS scores were considerably lower than those in the oral instruction group (P < 0.01). The trend variations in the VAS scores in the three groups were consistent over time, indicating no apparent interaction with the factor of time (F = 1.31, P > 0.05), as seen in Table 8. Pain levels in the animation video group and the recorded video group were lower compared with the oral instruction group.
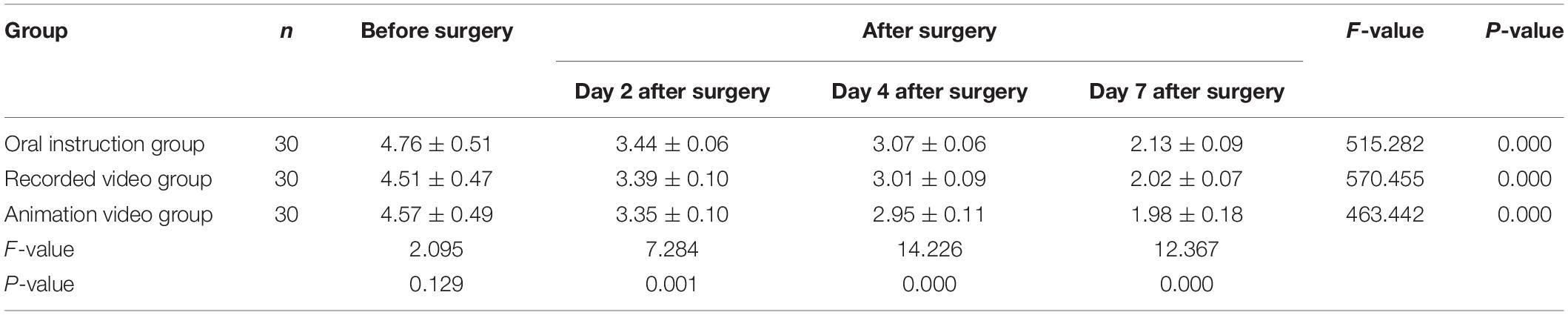
Table 7. Pain levels in the three groups.
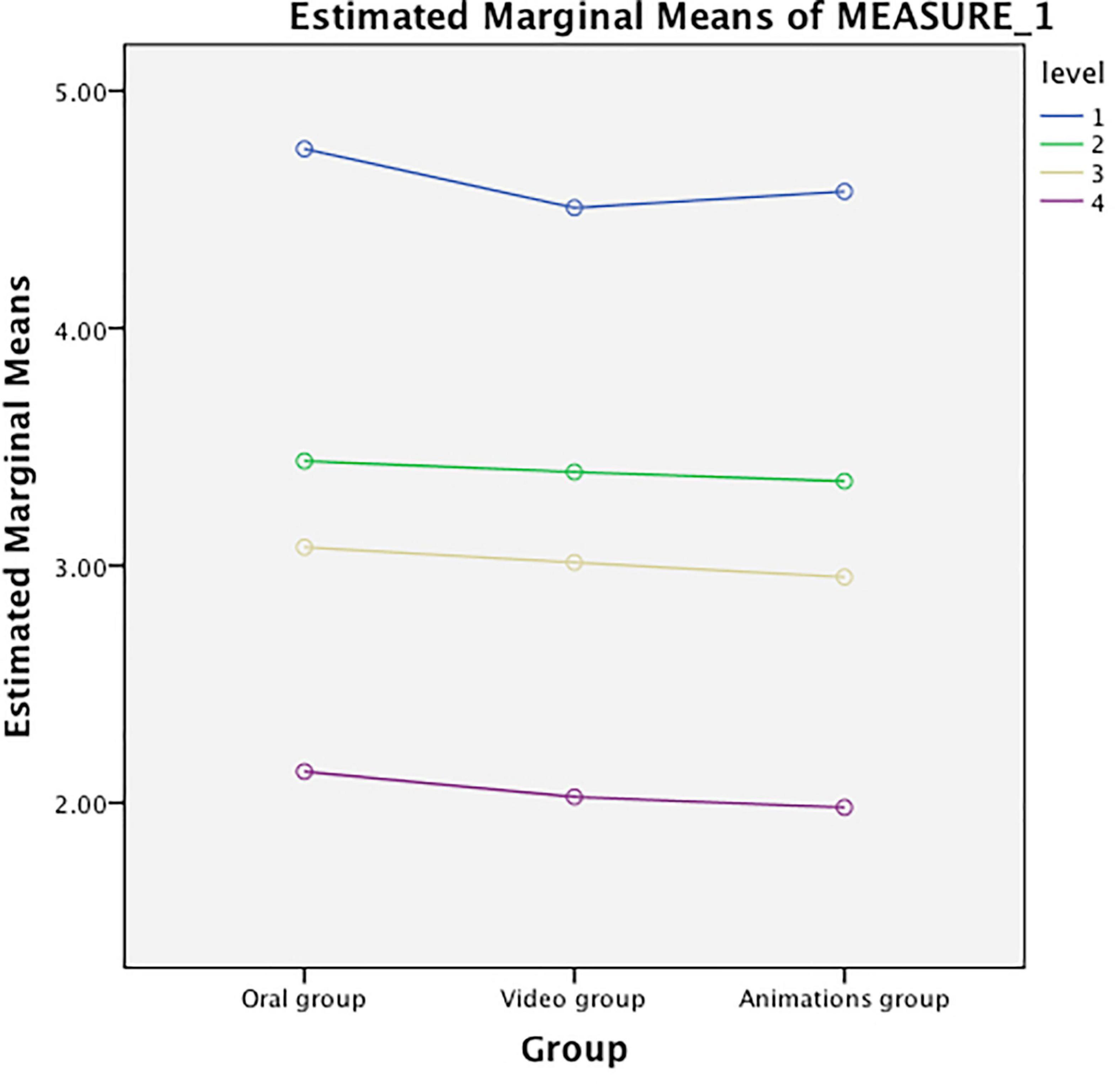
Figure 2. Intergroup differences in the pain levels between the three groups.

Table 8. Interaction between pain level and time.
Discussion
The Importance of Preoperative Health Education
Health knowledge and information are the basis for establishing positive health beliefs and attitudes and subsequent health behaviors. Health education is of great significance to patients since it not only helps them to understand their condition and take appropriate health behaviors to promote treatment and rehabilitation but also reduces fear and anxiety caused by the unknown.
Anxiety is the experience of an adverse emotional reaction to a potential threat, whereas fear leads to avoidance behavior, whereas anxiety is associated with uncontrollable or inevitable events (Michael et al., 2000). Surgery-related anxiety is very prevalent among patients, regardless of the type of surgery to be performed. However, the degree of anxiety affects the coping ability of surgical patients during the perioperative period, as they are prone to worrying about possible complications, recovery, and adverse events following surgery (Eijlers et al., 2019; Kuner and Kuner, 2021).
Surgery can cause damage to the body and can cause a sympathetic nervous system response. Tissue damage triggers the production of histamine and other inflammatory cytokines, and nociceptors are stimulated and produce pain signals that are transmitted to the brain, producing postoperative pain (Alattas et al., 2017). About 80% of surgical patients worldwide suffer from severe postoperative pain, which, if left untreated, will affect their quality of sleep and impede postoperative recovery. As a consequence, hospitalization will be prolonged (Alattas et al., 2017). This not only increases the economic burden for patients and society but also lowers patient satisfaction (Rabah et al., 2020; Small and Laycock, 2020; Dieu et al., 2021; Michael, 2021; Moghalu et al., 2021).
Preoperative health education is highly important for all surgical patients. Steves and Scafide (2021) found that preoperative health education shortened the hospital stay and saved on medical expenditure. Salibian et al. (2021) showed that the levels of anxiety and postoperative pain in women with breast cancer were much lower after the implementation of preoperative health education. Research by Wong et al. (2010) also indicated that patients benefited from health education, as pain and anxiety levels were lowered and self-efficacy was improved. Gholami et al. (2020), Sorel et al. (2020), and Rai et al. (2021) demonstrated that preoperative health education, when fully individualized and carried out correctly, can significantly reduce the level of postoperative anxiety and pain in surgical patients.
Importance of Preoperative Health Education in the Form of an Animation Video
As a measure to boost postoperative recovery, preoperative health education may be traditionally performed by oral instruction or group teaching, and it can rely on two-dimensional printed materials or multimedia. The traditional form of preoperative education, due to its common form and small impact, cannot achieve the effect expected by doctors. Recorded videos are often overloaded with educational content, and scenes depicting surgical bleeding and tissue incision may aggravate anxiety. Animation videos allow a lively representation of the contents of health education, which systematically instructs patients and their relatives on the surgery that they are going to undergo and the matters that require attention. If necessary, patients can watch the video repeatedly before surgery, and the risk of cross-infection caused by distributing and reading pamphlets does not exist. The use of videos for preoperative health education also reduces the workload of healthcare workers and its associated costs, as they otherwise would have to go from bed to bed to instruct patients orally.
With advances in multimedia technology, modes of health education in hospitals are constantly changing, and many medical organizations in China have carried out multimedia video-based health education activities (Yang et al., 2021). Animated health education videos based on multimedia broadcasting mitigate faults in traditional oral and educational manuals. With the help of rich and easy-to-understand animated videos, patients and their families can increase their understanding of health-related content through both sound and images, which meets the learning needs of patients of different ages and educational levels. Educational videos can be watched repeatedly so that patients may master increased knowledge. In addition, through animation video health education, and the joint efforts of relevant health educators in various nursing units, the hospital’s nursing level can be improved.
The Role of Preoperative Health Education, in the Form of Animation Videos, in Alleviating Postoperative Anxiety and Pain
In recent years, medical disputes caused by insufficient health education have occurred frequently, and, therefore, the provision of adequate health education plays an important role in medicine today. Animation videos can be applied as a useful tool, not only to promote a better and transparent doctors-patients relationship but also to reduce preoperative anxiety among children and adults (Michalski et al., 2016; Platto et al., 2019; Nair et al., 2021).
In this study, it was found that postoperative anxiety levels in patients with femoral fractures were lowered considerably after watching an animation video. The smallest reduction in anxiety was found with oral instruction (P < 0.01). The STAI score was significantly lower in the early period after surgery (day 2) in the animation video group than in the other two groups (P < 0.01). At each time point after surgery, the STAI scores of all three groups significantly decreased compared with those before surgery (P < 0.01). This suggests that the anxiety levels of patients declined rapidly with time following sufficient health education. The pain levels of the three groups varied consistently over time. The animation video group and recorded video group showed significant differences in the effectiveness of alleviating pain compared with the oral instruction group as the control (P < 0.01), the difference between the animation group and the oral information group is that the difference before and after watching the animation video group is greater than the difference before and after oral instruction group, but the two experimental groups did not differ significantly (P > 0.05). Although all three approaches toward preoperative health education were effective to some extent, the animation video provided the greatest benefit in alleviating either postoperative anxiety or postoperative pain. However, the use of an animation video did not achieve a significantly prominent effect in pain relief compared with the recorded video. The reason may be the similarity between the content taught by the two types of media and the fact that the recorded video contains few elements that may affect patient pain levels. The patients in our group generally agreed on the importance of animation videos as a preoperative health education tool, and therefore this method deserves further investigation.
In addition to enhancing patient understanding, animation videos convey additional benefits over other forms of preoperative health education, such as oral instruction and printed materials. For example, the method of playing the video can be adapted according to the specific conditions, such as the hardware facilities available at the hospital. The contents of the video to be played can be determined by the patients themselves or by their relatives, depending on their learning ability and individual needs. Thus, multimedia health education using animation videos meets the demands of a more diverse group of patients and achieves higher learning effectiveness. In addition, the patients and their relatives are offered a complete set of health education programs suitable for repeated viewing.
To sum up, preoperative health education in the form of animation videos can reduce the levels of postoperative anxiety and pain in patients with femoral fractures. Compared with the recorded video and oral instruction groups, the use of animation videos facilitated knowledge assimilation related to surgery and recovery, strengthened patients’ coping abilities, and lowered postoperative anxiety and pain levels. Therefore, it is worth popularizing this approach to preoperative health education in medical practices. However, since this study is affected by limitations, such as a small sample size and a lack of randomization, further investigations are required to confirm the conclusions reached in this paper.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by the First Affiliated Hospital of Shantou University Medical College. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
YW conceived of the study. XH participated in its design and coordination. ZL helped to draft the manuscript. All authors read and approved the final manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Alattas, S. A., Smith, T., Bhatti, M., Wilson-Nunn, D., and Donell, S. (2017). Greater pre-operative anxiety, pain and poorer function predict a worse outcome of a total knee arthroplasty. Knee Surg Sports Traumatol. Arthrosci. 25, 3403–3410. doi: 10.1007/s00167-016-4314-8
Ayyadhah Alanazi, A. (2014). Reducing anxiety in preoperative patients: a systematic review. Br. J. Nurs. 23, 387–393. doi: 10.12968/bjon.2014.23.7.387
Dieu, A., Huynen, P., Lavand’homme, P., Beloeil, H., Freys, S. M., Pogatzki-Zahn, E. M., et al. (2021). PROSPECT working group of the european society of regional anaesthesia and pain therapy (ESRA). pain management after open liver resection: procedure-specific postoperative pain management (PROSPECT) recommendations. Reg. Anesth Pain Med. 46, 433–445. doi: 10.1136/rapm-2020-101933
Eijlers, R., Dierckx, B., Staals, L. M., Berghmans, J. M., van der Schroeff, M. P., Strabbing, E. M., et al. (2019). Virtual reality exposure before elective day care surgery to reduce anxiety and pain in children: a randomised controlled trial. Eur. J. Anaesthesiol. 36, 728–737. doi: 10.1097/EJA.0000000000001059
Gholami, S., Mojen, L. K., Rassouli, M., Pahlavanzade, B., and Farahani, A. S. (2020). The predictors of postoperative pain among children based on the theory of unpleasant symptoms: a descriptive-correlational study. J. Pediatr. Nurs. 55, 141–146. doi: 10.1016/j.pedn.2020.08.006
Gong, R. S., and Zhao, J. (2018). Research progress of perioperative anxiety. Beijing Med. Sci. 40, 572–574. doi: 10.15932/j.0253-9713.2018.06.026
Huang, G. Q., Wu, X., and Liang, Z. (2005). Correlation of pre-operative and post-operative anxiety level to the sense of uncertanty in orthopedic patients. J. Rehabili. Med. Assoc. 33, 1–10.
Kuner, R., and Kuner, T. (2021). Cellular circuits in the brain and their modulation in acute and chronic pain. Physiol. Rev. 101, 213–258. doi: 10.1152/physrev.00040.2019
Kuo, C. P., Li, P. C., Chuang, H. L., Lee, S. H., Liao, W. C., and Lee, M. S. (2021). The effect of multimedia health education on pain and anxiety in women undergoing mammography in taiwan. Taiwan J. Obstet. Gynecol. 60, 1084–1089. doi: 10.1016/j.tjog.2021.09.021
Li, X. R., Zhang, W. H., and Williams, J. P. (2021). A multicenter survey of perioperative anxiety in china: pre- and postoperative associations. J. Psychosom Res. 147:110528. doi: 10.1016/j.jpsychores.2021.110528
Ma, Y., Wu, H., Wang, Y., and Guo, L. (2021). A feasibility study of modified self-efficacy for the improvement of adverse emotions and quality of life in traumatic fracture patients. Am. J. Trans. Res. 13, 6507–6515.
Michael, A. E. R. (2021). Analgesia in acute post-operative pain. Br. Dent J. 231:748. doi: 10.1038/s41415-021-3790-5
Michael, L., Jeannette, M., and Haviland, J. (2000). Handbook of Emotions, 2nd Edn. New York: Guilford Press, 720.
Michalski, A., Stopa, M., and Miśkowiak, B. (2016). Use of multimedia technology in the doctor-patient relationship for obtaining patient informed consent. Med. Sci. Monit. 22, 3994–3999. doi: 10.12659/msm.894147
Ministry of Health of the People’s Republic of China (2012). Chinese Health Statistical Digest 2012.
Moghalu, O., Stoffel, J. T., Elliott, S., Welk, B., Lenherr, S., Herrick, J., et al. (2021). Neurogenic bladder research group. psychosocial aspects of health-related quality of life and the association with patient-reported bladder symptoms and satisfaction after spinal cord injury. Spinal Cord. 59, 987–996. doi: 10.1038/s41393-020-00609-x
Nair, T., Choo, C. S. C., Abdullah, N. S., Lee, S., Teo, L. L. E., Chen, Y., et al. (2021). Home-initiated-programme-to-prepare-for-operation: evaluating the effect of an animation video on peri-operative anxiety in children: a randomised controlled trial. Eur. J. Anaesthesio. 38, 880–887. doi: 10.1097/EJA.0000000000001385
National Bureau of Statistics of the People’s Republic of China (2011). The Sixth National Population Census In 2010 The Main Data Bulletin (No. First). Beijing Weekly: English version. Available online at: http://www.gov.cn/test/2012-04/20/content_2118413.htm
Platto, J. F., Maarouf, M., Hendricks, A., Kurtzman, D. J., and Shi, V. Y. (2019). Animated video consultation for reducing pre-operative anxiety in dermatologic surgery. Dermatol. Online J. 25:13030.
Rabah, N. M., Levin, J. M., Winkelman, R. D., Mroz, T. E., and Steinmetz, M. P. (2020). The association between physicians’ communication and patient-reported outcomes in spine surgery. Spine 45, 1073–1080. doi: 10.1097/BRS.0000000000003458
Rai, A., Khan, H., and Baheer, Y. (2021). Effect of preoperative patient education on opioid consumption and well-being in breast augmentation. Plast Reconstr. Surg. 147, 340e–341e.
Reips, U. D., and Funke, F. (2008). Interval-level measurement with visual analogue scales in internet-based research: VAS generator. Behav. Res. Methods 40, 699–704. doi: 10.3758/brm.40.3.699
Salibian, A. A., Axelrod, D. M., Smith, J. A., Fischer, B. A., Agarwal, C., and Bluebond-Langner, R. (2021). Oncologic considerations for safe gender-affirming mastectomy: preoperative imaging, pathologic evaluation, counseling, and long-term screening. Plast Reconstr Surg. 147, 213e–221e. doi: 10.1097/PRS.0000000000007589
Sorel, J. C., Overvliet, G. M., Gademan, M. G. J., den Haan, C., Honig, A., and Poolman, R. W. (2020). The influence of perioperative interventions targeting psychological distress on clinical outcome after total knee arthroplasty. Rheumatol. Int. 40, 1961–1986. doi: 10.1007/s00296-020-04644-y
Steves, S. L., and Scafide, K. N. (2021). Multimedia in preoperative patient education for adults undergoing cancer surgery: a systematic review. Eur. J. Oncol. Nurs. 52:101981. doi: 10.1016/j.ejon.2021.101981
Varallo, G., Scarpina, F., Giusti, E. M., Cattivelli, R., Guerrini Usubini, A., Capodaglio, P., et al. (2021). Does kinesiophobia mediate the relationship between pain intensity and disability in individuals with chronic low-back pain and obesity? Brain Sci. 11:684. doi: 10.3390/brainsci11060684
Weiser, T. G., Regenbogen, S. E., and Thompson, K. D. (2008). An estimation of the global volume of surgery: a modelling strategy based on available data. Lancet 372, 139–144. doi: 10.1016/S0140-6736(08)60878-8
Wong, E. M., Chan, S. W., and Chair, S. Y. (2010). Effectiveness of an educational intervention on levels of pain, anxiety and self-efficacy for patients with musculoskeletal trauma. J. Adv. Nurs. 66, 1120–1131. doi: 10.1111/j.1365-2648.2010.05273.x
Yang, Q., Wu, Z., Xie, Y., Xiao, X., Wu, J., Sang, T., et al. (2021). The impact of health education videos on general public’s mental health and behavior during COVID-19. Glob Health Res. Policy. 6:37. doi: 10.1186/s41256-021-00211-5
Zhang, L., Hao, L. J., Hou, X. L., Wu, Y. L., Jing, L. S., and Sun, R. N. (2021). Preoperative anxiety and postoperative pain in patients with laparoscopic hysterectomy. Front. Psychol. 12:727250. doi: 10.3389/fpsyg.2021.727250
Keywords: surgical patient, animation videos, health education, anxiety, postoperative pain
Citation: Wang Y, Huang X and Liu Z (2022) The Effect of Preoperative Health Education, Delivered as Animation Videos, on Postoperative Anxiety and Pain in Femoral Fractures. Front. Psychol. 13:881799. doi: 10.3389/fpsyg.2022.881799
Received: 24 February 2022; Accepted: 12 April 2022;
Published: 06 May 2022.
Edited by:
Gema T. Ruiz-Parraga, University of Malaga, SpainReviewed by:
Giorgia Varallo, Italian Auxological Institute (IRCCS), ItalyNurcan Özyazıcıoğlu, Bursa Uludag University, Turkey
Copyright © 2022 Wang, Huang and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zhili Liu, bGl1ejU1NmlAMTI2LmNvbQ==
†These authors have contributed equally to this work