 Shelly J. Lane
Shelly J. Lane Marco A. Leão
Marco A. Leão Virginia Spielmann
Virginia Spielmann
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Psychol. , 17 May 2022
Sec. Perception Science
Volume 13 - 2022 | https://doi.org/10.3389/fpsyg.2022.877527
This article is part of the Research Topic Meaningful Participation and Sensory Processing View all 15 articles
The prevalence of sleep dysfunction is considerably higher in the autistic population than in the non-autistic. Similarly, the incidence of sensory reactivity differences in autism exceeds that in the neurotypical population. The basis of sleep disorders in autism is multifactorial, but sensory integration/processing concerns may play a role. Research that investigates this interplay for autistic individuals is limited but vital. In this scoping review, we examined literature addressing the following research question: What is the relationship between sleep and sensory integration/processing in autism? We included articles if they were peer-reviewed, English or Spanish, purposefully addressed sensory integration/processing differences, were sleep focused and included autism as the primary diagnosis or population. Articles were excluded if the language was not English or Spanish, research was conducted with animals, they were non-peer-reviewed, the primary population was not autistic, the sensory focus reflected a specific sensorineural loss (e.g., blindness, or deafness), there was not a clear inclusion of sensory integration/processing or sleep. We searched six databases and included all citations from the inception of each database through June 2021. The search strategy identified 397 documents that were reduced to 24 included articles after exclusion criteria were applied. The majority of studies we identified characterized the relation between sleep and sensory integration/processing differences in autism. Investigators found multiple sleep concerns such as bedtime resistance, sleep anxiety, delayed sleep onset, night awaking, and short sleep duration in autistic individuals. Identified sensory concerns focused on reactivity, finding hyper- and hypo-reactivity as well as sensory seeking across sensory domains. Co-existence of sleep concerns and sensory integration/processing differences was frequently reported. Few intervention studies showed a clear sensory focus; those that did emphasized pressure, movement, touch, and individual sensory preferences/needs. Swimming programs and massage showed promising results. No studies were of high quality. At a minimum, there is a co-existence of sensory reactivity differences and sleep concerns in autistic children, and possibly autistic adults. The relationship between poor sleep and sensory integration/processing differences is complex and multi-faceted, requiring additional research. Interventions that purposefully include a central sensory component have not been well studied in autistic children or adults. Overall studies with greater rigor and purposeful use of sensation and sensorimotor supports as a component of intervention are needed. This study was not funded.
Sleep is a critical occupation for adequate neural function and maturation. Inadequate sleep has been linked to disruptions in attention, memory, mood, and behavior (cf. Souders et al., 2017; Tester and Foss, 2018), all of which influence participation across occupations. While many neurotypical children experience sleep difficulties, the incidence in autistic children1 is reported to be substantially higher; sleep disorders have been identified in as many as 50% of autistic adults and 80% of autistic children (Hirata et al., 2016; Souders et al., 2017; Deliens and Peigneux, 2019; Hohn et al., 2019). Reported sleep difficulties vary and may differ across the life span. However, the most often reported sleep concerns include reduced total sleep time, prolonged sleep latency, poor sleep efficiency, and wake after sleep onset; the literature is highly variable in both incidence and characteristics of sleep concerns (Malow et al., 2006; Miano et al., 2007; Goldman et al., 2012; Morgan et al., 2020).
Sensory reactivity differences are ubiquitous in autism and include sensory hyper-reactivity, sensory hypo-reactivity, and unusual sensory interests (Tomchek and Dunn, 2007; Crane et al., 2009; Marco et al., 2011; Puts et al., 2014; Tavassoli et al., 2014b; Taylor et al., 2020). Unusual sensory interests may be expressed as sensory seeking or craving (such as extensive smelling or touching of objects) and, along with reactivity differences, may be seen across the range of sensory domains (Schaaf and Lane, 2015). Importantly, investigators have indicated that sensory differences can negatively impact participation in autistic children (Little et al., 2015) and adults (Tavassoli et al., 2014b; Robertson and Simmons, 2015; Clince et al., 2016; Syu and Lin, 2018). More specifically, sensory integration/processing differences in autistic children have been associated with participation differences during mealtimes (Zobel-Lachiusa et al., 2015), in the classroom (Ashburner et al., 2008), during sleep (Reynolds et al., 2011), and with social participation (Watson et al., 2011). In addition, researchers such as Hochhauser and Engel-Yeger (2010) indicate that the choice of and setting for engagement in leisure is influenced by sensory seeking and sensory sensitivity. In autistic adults, sensory integration/processing differences have been shown to impact participation in higher education, and at least indirectly, social interactions (Robertson and Simmons, 2015; Syu and Lin, 2018), and other daily life activities (Tavassoli et al., 2014b). While there has been a great deal of research conducted on many of these associated occupational divergences, particularly in autistic children, the relationship between sensory integration/processing differences and the occupation of sleep has received only limited attention.
Importantly, both sensory reactivity differences and sleep concerns interfere with occupation and participation in activities of daily life (Roley et al., 2015; Dunn et al., 2016; Medic et al., 2017; Silverman and Tyszka, 2017; Berkley, 2021; Neufield et al., 2021). Clinically, understanding the range of these differences, as well as their inter-relatedness, has the potential to support more focused intervention. Deliens and Peigneux (2019) suggested that sensory reactivity and unusual sensory interests might play a role in sleep disturbances in autistic individuals. Drawing from the literature on neurotypical children (Tzchishinsky et al., 2008; Shochat et al., 2009), Deliens and Peigneux (2019) suggested that difficulty in the ability to filter out environmental sensation could interfere with sleep. Consistent with this suggestion, Hollway et al. (2013) indicated that to fall asleep and stay asleep individuals must be able to filter out sensation from the environment; as sensory reactivity differences are core to autism, this ability is heavily implicated.
Endeavoring to explain the link between historically perceived core characteristics2 associated with autism (e.g., differences in social communication challenges, insistence on sameness, and resistance to change) and sleep difficulties, Hollway et al. (2013) suggested that autistic children may interpret external cues around bedtime to be stressors, leading to sleep difficulties. These bedtime challenges may result in hyperarousal and difficulty falling asleep (Deliens and Peigneux, 2019). Hollway and colleagues also indicate that the relationship between sleep challenges and autism may be bidirectional such that poor sleep exacerbates features of autism, which in turn leads to sleep challenges. Other investigators (Schreck et al., 2004; Hundley et al., 2016; Cohen et al., 2018) have also indicated that poor sleepers have more significant autism features. However, the bidirectional relationship between sleep and features of autism is not universally accepted (Deliens and Peigneux, 2019). For instance, and admittedly with some inconsistency, investigators have found that sleep problems in individuals with a range of autism features correlate with IQ (Gabriels et al., 2005; Bruni et al., 2007; Giannotti et al., 2008), and challenging behaviors in both children and adults (Limoges et al., 2005; Allik et al., 2006; Bruni et al., 2007). In addition, Hundley et al. (2016) indicated that sleep challenges do not correlate universally with what are considered challenging behaviors. Instead, they found that poor sleep correlates with high rates of repetitive sensory-motor behaviors but not insistence-on-sameness. These investigators indicated that intervention for the myriad sleep challenges needs to be multifaceted and should consider sensory aspects of the environment (Hundley et al., 2016).
We are faced with challenges. First, there is inconsistency in research relative to the relationship between sleep difficulties and sensory integration/processing differences. Second, there remains some uncertainty about the impact of poor sleep and sensory integration/processing differences on occupation and participation in autistic individuals. Together these factors make for challenges in appreciating this interplay and lead to difficulties in providing appropriate intervention services. Further, investigations looking at this interconnectedness focus primarily on children with very limited information available for autistic adults. In this review, we examined how this relationship is characterized and defined by current research and looked at the interventions that have been used. Due to the broad nature of this aim, we determined that a scoping review was the most appropriate approach.
In conducting our review we considered both the National Institute of Mental Health Research Domain Criteria (RDoC) framework3 and the Diagnostic and Statistics Manual V (DSM-V; American Psychiatric Association [APA], 2013) to examine the interplay between the dimensions of sleep and sensory integration/processing. The RDoC is a framework designed to guide understanding of mental health as well as illness, in psychological and biological systems. The RDoC addresses the construct of Sleep/Wakefulness within the domain of Arousal and Regulatory Systems. Sensory reactivity, of interest in this review, is arguably also included under arousal in the domain of Arousal and Regulatory Systems: ‘‘sensitivity of the organism to stimuli, both external and internal.’’4 Sensorimotor systems are represented as a separate domain and include constructs of motor actions, agency and ownership, habit–sensorimotor, and innate motor patterns. In addition, sensory systems are embedded within the Cognitive Systems domain under the construct of perception (visual, auditory, olfactory, somatosensory, and multimodal). While the inclusion of both sleep and sensory reactivity within the Arousal and Regulatory system domain supports our examination of this interaction, the multiple representations of sensory integration/processing across other domains present challenges for examining the interaction of these constructs. In addition, there have been notable calls to include sensory processing as a unique domain in the RDoC (Harrison et al., 2019), and leading theorists are recognizing the importance of sensory integration/processing across disciplines (Bogdashina, 2016; Robertson and Baron-Cohen, 2017; Sinclair et al., 2017; Mueller and Tronick, 2020). These positions closely support our perspective on the centrality of sensory integration/processing to the development of health, wellness, occupation, and participation, providing support for this review. Within the DSM-V the foundational importance of sensory integration/processing to wellbeing finds some additional support, although it comes from the perspective of dysfunction. Within this framework, sensory reactivity differences are associated with autistic core characteristics and included under the “restricted, repetitive patterns of behaviors, interests, or activities” diagnostic feature. While no direct link is made to sleep concerns, they are considered either a reflection of underlying anxiety or depression, or a concomitant feature of autism.
This scoping review was structured based on the framework developed by Arksey and O’Malley (2005) and guidelines from the Joanna Briggs Institute (Peters et al., 2020), and utilized the PRISMA-ScR checklist (Tricco et al., 2018). This project was registered with Prospero, CRD42020209872.
Our intention in this review was to examine literature that investigated the relations between sensory integration/processing differences and sleep challenges in autistic individuals, across the life span. Our research question was: What is the relationship between sleep and sensory integration/processing in autism?
We conducted an initial search in CINAHL, Pubmed, PsychINFO, Academic Search Premier, Web of Science, and Embase databases, and included all citations from the inception of each database through November 2020. A sample search strategy comprised the terms: [sleep OR “sleep-wake disorders” OR “sleep dysfunction” OR “sleep disorder” OR “sleep problems” for Sleep; [“sensory processing” OR “sensory processing disorder*” OR “sensory integration” OR “sensory integration dysfunction*” OR “sensory integration dysfunction” OR “sensory processing disorder” OR “sensation disorder” OR “sensory over responsivity” OR “sensory reactivity” OR vestibular OR propriocept* OR interocept* OR tactile OR touch OR somatosensory OR “somatosensory” OR Postur* OR “multi sensory” OR multisensory OR sensorimotor] for sensory integration/processing; and [“autism spectrum disorder” OR “autistic disorder” OR asperger OR autism OR autistic] for autism. The search terms were entered into the databases with an “AND” term between each of them.
In June 2021, we conducted a follow-up search in the same databases to check for newer articles. We hand searched the reference lists from included articles (August 2021) to ensure that all appropriate articles were comprised.
Based on our research question, we set the inclusion criteria to be as follows: (1) peer-reviewed articles (qualitative or quantitative research papers), written in English or Spanish; (2) sensory integration/processing differences purposefully included (3); sleep focused and (4) autism as the primary diagnosis or population. We detailed the exclusion criteria in the following hierarchical order: (1) articles written in a language other than English or Spanish; (2) articles conducted with animals; (3) presentations, conference proceedings, non–peer-reviewed research literature, dissertations, and theses; (4) primary focus on populations other than autism; (5) sensory focus on a specific sensorineural loss (e.g., blindness, or deafness); (6) no clear inclusion of sensory integration/processing or sleep.
Initial and follow-up searches resulted in a total of 397 references. Of these, 114 duplicate articles were removed. A total of 283 abstracts were screened by title and abstract by two reviewers; conflicts were resolved by a third reviewer or through discussion and 179 articles were excluded. Two reviewers conducted full-text reviews of the remaining 104 potential articles; 82 additional articles were excluded for the following reasons: one study was conducted with animals rather than humans; 32 articles were not peer reviewed, seven articles collected data from populations other than autism; 40 studies did not include a clear definition of sensory integration/processing or sleep; one article was an additional duplicate and one full text was not available. Per hand search of reference lists in all included articles, we identified and added two additional articles (Table 1). Figure 1 shows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA-ScR; Tricco et al., 2018) flow diagram of the search strategy. The search strategy used for Web of Science is available as a Supplementary Table.
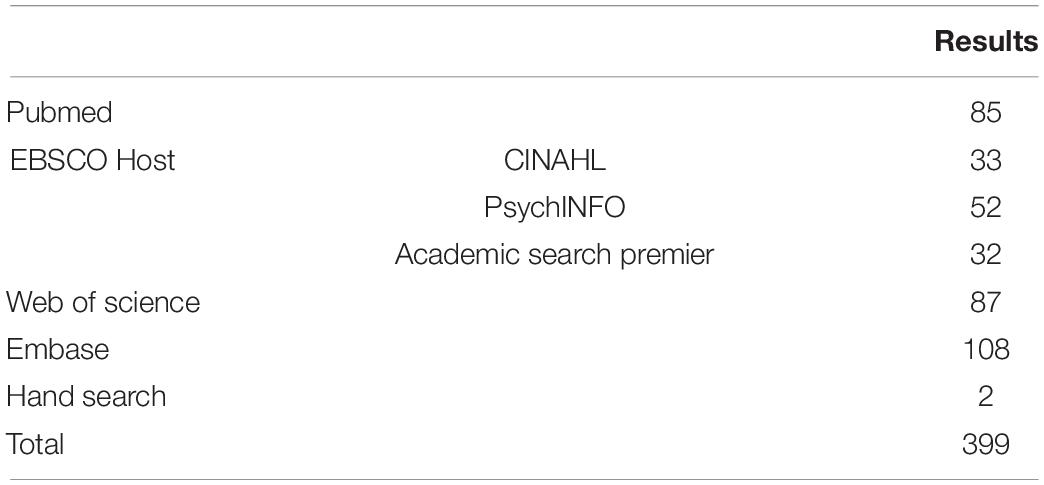
Table 1. Results per database.
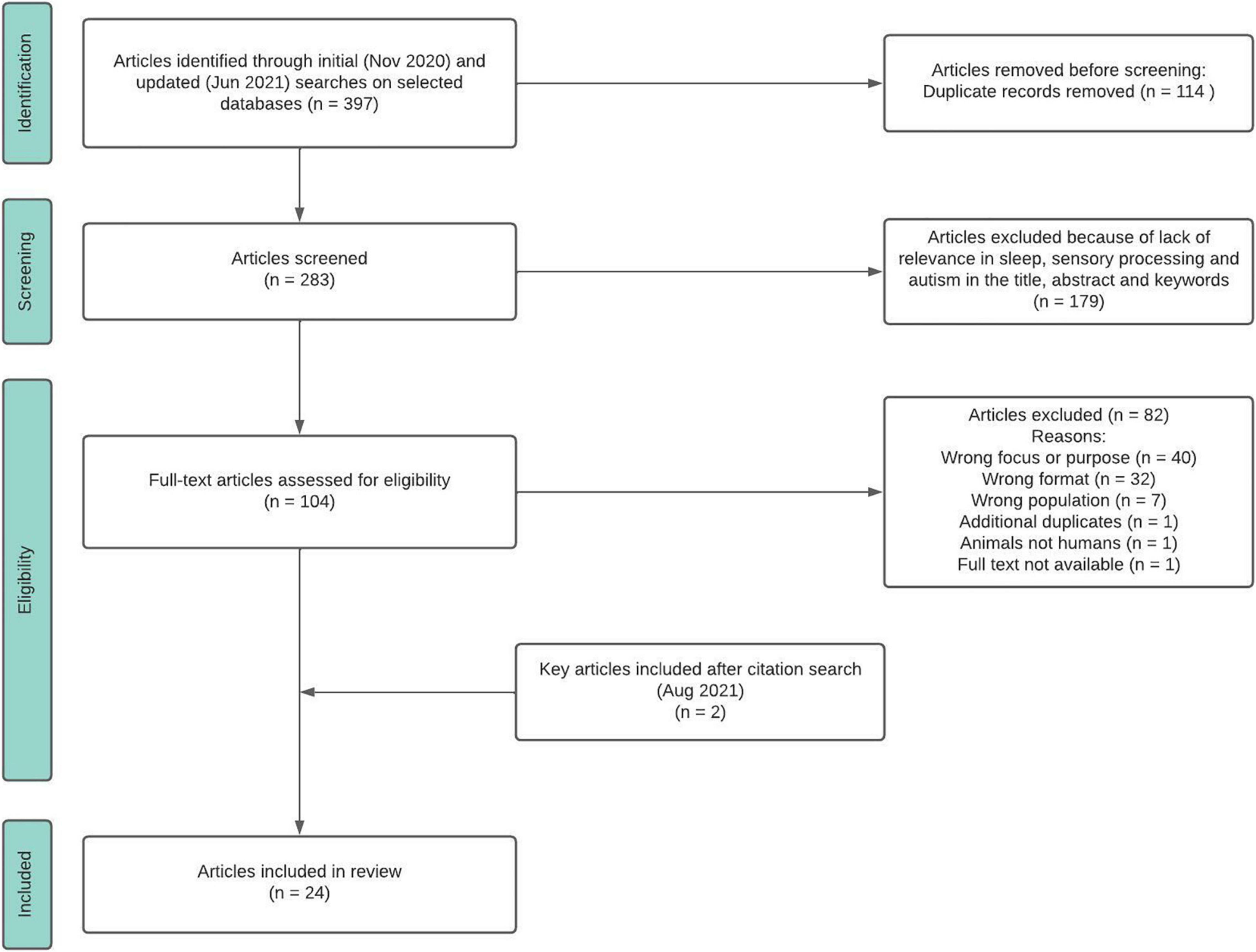
Figure 1. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA- ScR).
A total of 24 articles met the inclusion criteria and were included in the final review (Figure 1). Data extraction was conducted using these fields: title, authors, year, journal, source country, study design, research question, sample size, and characteristics, inclusion and exclusion criteria, diagnostic tools, measures of sensory integration/processing, sleep and other characteristics, intervention, quantitative and qualitative findings, identified relationships between sensory integration/processing and sleep, and authors conclusions.
We collated and summarized the data from the extraction table and determined there were two broad categories into which studies fell: characterization and intervention. We present results based on these categories.
A total of 24 articles were included in the data extraction. Of these, 17 articles offered information characterizing a relation between sleep concerns and sensory integration/processing differences (Table 2), and seven articles were intervention studies using approaches with a clear sensory focus (Table 3). We considered these interventions sensory-based if consideration of the sensory components was a focal point, or sensory incidental when the intervention provided sensory input, but the inclusion of sensation was not the primary focus.
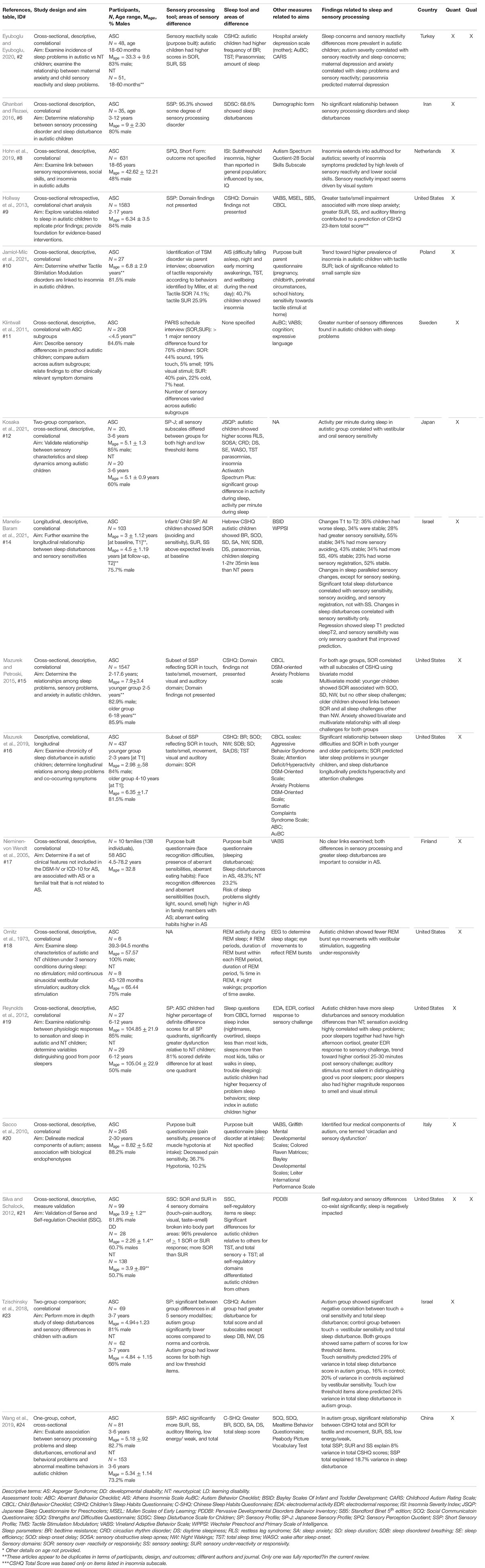
Table 2. Characterizing sleep/sensory processing relations.
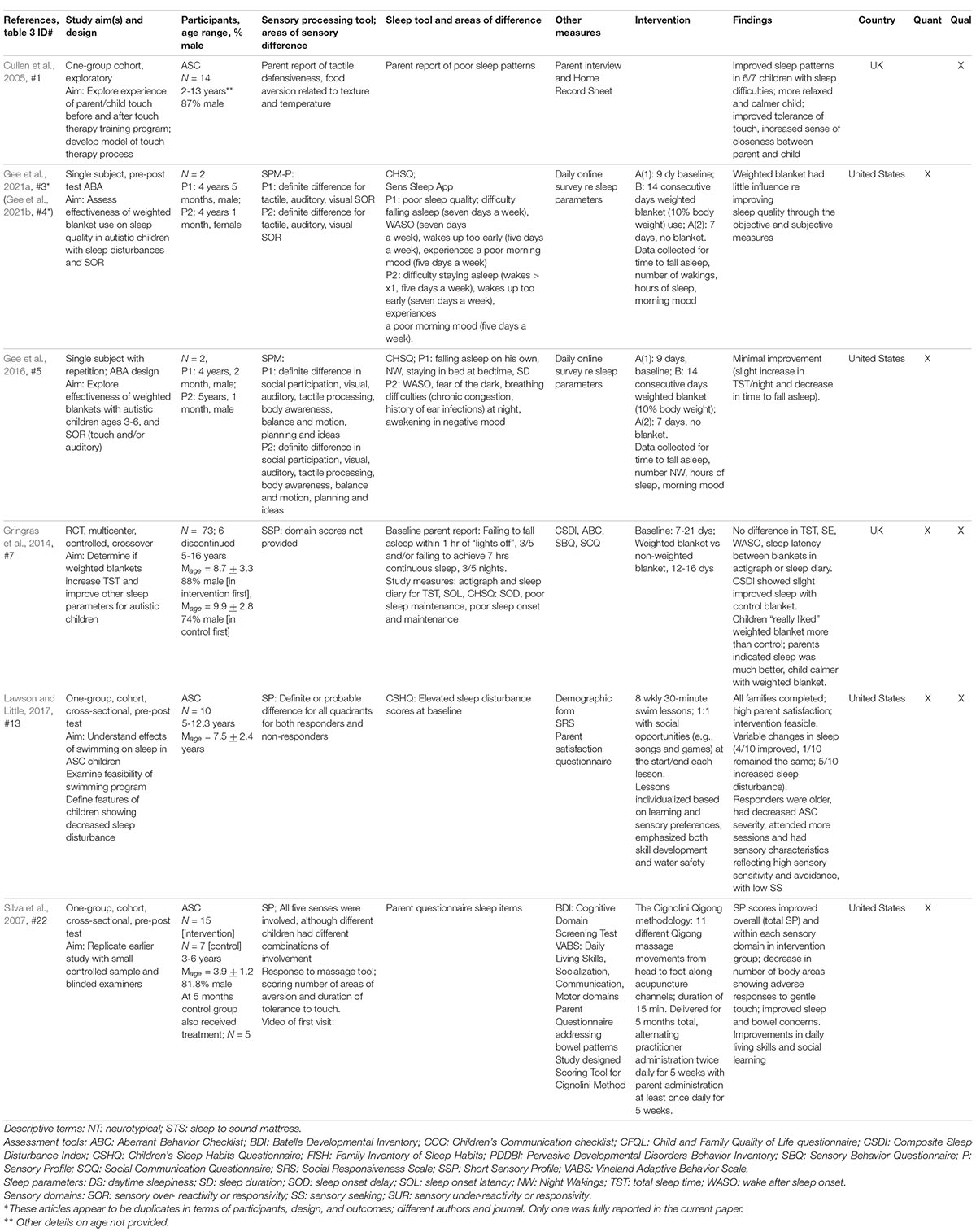
Table 3. Interventions addressing sleep and sensory processing.
The most commonly reported tool used to reflect sleep concerns was the Children’s Sleep Habits Questionnaire (CSHQ; Owens et al., 2000). This screening tool asks parents to reflect on their child’s sleep characteristics over a typical recent week. Subscales include bedtime resistance, sleep onset delay, sleep duration, sleep anxiety, night wakings, sleep disorder breathing, parasomnias, and daytime sleepiness. A total sleep score is also generated (Owens et al., 2000). The original version of this tool had 45 questions [CSHQ (45)]; the authors created a 33-item revised version to reduce redundancy and ambiguity [CSHQ (33)]. The CSHQ, or a version of it, was used to define sleep concerns in seven of the 17 articles that characterized a relationship between poor sleep and sensory reactivity differences (Table 2, studies #2, #9,#14, #15, #16,#23,#24) and one of the seven articles that utilized sensory-based interventions (Table 3, study #13). A variety of other means of determining sleep concerns, including both published tools and those purpose-built for individual studies, were used by other authors (Tables 2, 3). In some studies, sleep concerns were identified using both subjective measures based on parent report, and more objective measures such as actigraph (Table 2, study #12; Table 3, study #7). Sleep concerns of autistic children were multifaceted and included concerns in all domains tapped by the CSHQ, along with wake after sleep onset. Hohn et al. (2019), the only study found addressing adults, reported that autistic adults experienced an elevated incidence of insomnia.
Sensory integration/processing was assessed using a variety of tools, although some form of the Sensory Profile ([SP]; Dunn, 1999) or Short Sensory Profile ([SSP]; McIntosh et al., 1999) were used most commonly (Table 2, studies #6, #9, #12, #14, #15, #16, #19, #23, #24; Table 3, studies #7, #13, #22). In the SP and the SSP the authors consider the interface between neurological threshold and self-regulation in response to sensation, defining sensory processing patterns across four quadrants: poor sensory registration, sensory seeking, sensory avoiding, and sensory sensitivity. With the SP, Dunn also identifies reactivity differences within each sensory domain (sensory section scores) along a continuum from hyper- to hypo-reactivity, and within behavioral domains (behavioral section scores); this finer delineation is not available to users of the SSP. Thus, in these identified studies, the focus of sensory integration/processing differences was on sensory reactivity rather than perception or discrimination. There was variability in examining and reporting sensory differences across the studies. However, overall findings can be generalized to reflect sensory hyper-reactivity (which includes both sensory avoiding and sensory sensitivity), hypo-reactivity, and sensory seeking. Often a combination of these sensory processing differences was identified. While some investigators reported differences within specific sensory domains, we did not find consistency across studies; investigators variously reported sensory processing differences within visual, tactile, auditory, taste-smell, and vestibular sensory domains.
Most investigators agreed that there was, at minimum, a co-existence of sensory reactivity differences and sleep concerns. This finding was clearly stated by Silva and Schalock (2012): sleep and sensory processing differences co-exist in autism, and disordered sensory processing has a negative impact on sleep. In a family-based study, Nieminen-von Wendt et al. (2005) set out to examine familial traits of Asperger Syndrome not included in specific diagnostic criteria (DSM-IV or ICD-10). While they did not delineate a specific relationship between sleep concerns and sensory differences, they did find that these concerns and differences co-existed in their participants. These investigators suggested that sensory processing differences might be considered in the diagnostic criteria for Asperger Syndrome. Other investigators indicated that the combination of sleep concerns and sensory reactivity differences in autistic children exceeded that found in neurotypical children (Nieminen-von Wendt et al., 2005; Reynolds et al., 2012; Tzischinsky et al., 2018; Wang et al., 2019; Eyuboglu and Eyuboglu, 2020) and that a greater number of sensory integration/processing differences could be seen in autistic children with sleep concerns (Klintwall et al., 2011). Jamioł-Milc et al. (2021), investigating tactile modulation differences in autistic children through parent interview and observation, identified a potential relationship between tactile hypo-responsivity and insomnia but no relation between tactile hyper-responsivity or sensory seeking and insomnia. Interestingly, Ghanbari and Rezaei (2016) found no relationship between sensory processing differences and sleep concerns.
Using a Hebrew version of the CSHQ (45) (Tzchishinsky et al., 2008) and a version of the Infant-Child Sensory Profile (Neuman et al., 2004; Dunn, 2014) that had been validated in Israel, Manelis-Baram et al. (2021) examined the relationship between sleep and sensory reactivity at ages 3 (time 1) and 4.47 (time 2) years. Looking first at time 1, investigators indicated that sensory sensitivity was the only reliable indicator of sleep disturbance when controlling for scores in other sensory quadrants on the SP. Sensory sensitivity showed a strong relationship with both nighttime and total sleep time (including naps). Looking at change over time, these investigators found that more than 50% of their participants showed considerable changes (positive or negative) in either sleep severity or sensory reactivity. Hierarchical regression modeling, using age at time 1, time between assessments, time 1 sleep score, and the change in sensory sensitivity between times 1 and 2, investigators strongly predicted sleep disturbance at time 2; no other measure of sensory reactivity contributed to this prediction. They concluded that sleep disturbance and sensory reactivity severity were coupled and possibly rooted in a common physiological mechanism.
With a somewhat different focus, Mazurek and Petroski (2015) and Mazurek et al. (2019) drew items from the SP that reflected only sensory hyper-reactivity. Mazurek and Petroski (2015) grouped children with autism into younger (2–5 yrs.) and older (6–18 yrs.) subsets and found sensory hyper-reactivity to significantly correlate with all CSHQ (45) subscales. Applying a path analysis, they found sensory hyper-reactivity to be associated only with sleep onset delay, sleep duration, and night waking for the younger group. In contrast, sensory hyper-reactivity was related to all CSHQ (45) subscales except night waking for the older children. In a later study, Mazurek et al. (2019) identified a relationship between sensory hyper-reactivity and all subscales of the CSHQ (45) in both preschool and school-aged children. These investigators further indicated that sensory hyper-reactivity in preschoolers predicted sleep challenges at school age.
Looking within specific sensory systems, Tzischinsky et al. (2018) used the Hebrew version of the SP (Neuman et al., 2004) and found that while tactile and oral sensitivity differences were related to total sleep disturbances [Hebrew CSHQ (45)], tactile hyper-reactivity explained 24% of the variance in total sleep disturbance scores in autistic children. Jamioł-Milc et al. (2021) investigated tactile modulation disorders (either hyper- or hypo-reactivity) and poor-quality sleep in autistic children using their own tools. While they did not find significant relationships because of small sample size, they suggested that insomnia in autistic children could be related to tactile hypo-reactivity. Ornitz et al. (1973) investigated auditory and vestibular input and the relationship to aspects of REM sleep. These investigators found fewer REM burst eye movements in the autistic children who slept on a custom-made mattress that delivered continuous sinusoidal vestibular input, compared to the non-autistic group. One suggested conclusion from this study was that the vestibular system might be hypo-responsive during sleep in young autistic children.
Hohn et al. (2019) examined the relationship between sleep concerns, measured using the Insomnia Severity Index (ISI; Morin, 1993), and sensory processing differences, using the Sensory Perception Quotient (SPQ; Tavassoli et al., 2014a) in autistic adults, along with a link to social skills. They predicted that findings would parallel those in autistic children, and might vary relative to the sensory domain addressed. Overall, they found subthreshold insomnia in their population, although it was higher than that in a neurotypical population. The severity of insomnia was predicted, and potentially driven by, high levels of visual reactivity (neither proprioception nor vestibular modulation were assessed), but also related to increased difficulty engaging in neurotypical social skills as measured by the Autism Spectrum Quotient short form (ASQ; Hoekstra et al., 2011). Sacco et al. (2010) included adults and children in their study, seeking to define factors that contribute to autistic traits using statistical methods. Using a purpose-built survey based on clinical features of autism, participant and family features, and supporting assessments, these investigators completed a complex principal components analysis resulting in the identification of four components that they hypothesized may allow for categorization of autistic endophenotype subgroups with some homogeneity. One such component was, “circadian and sensory dysfunction” which was linked to sleep disorders, self-injurious behavior, hyperactivity, decreased pain sensitivity, and differences and delays in language development. Authors suggest that sleep challenges and sensory differences could be connected in a complex manner.
We found relatively few studies we considered sensory-based, having a primary sensory intervention focus. Gee and colleagues (Gee et al., 2016, 2021a, 2021b5), as well as Gringras et al. (2014), investigated the use of weighted blankets in improving sleep for autistic children. Based on existing theory, they reasoned that the provision of deep touch pressure might release endorphins and serotonin, leading to a sense of calm. In each of the investigative reports by Gee et al. (2021a,b) a single subject ABA design with replication was used (N = 2 in each study). These investigators collected data across a 9-day baseline, 14-day intervention, and 7-day intervention withdrawal period in all studies. Outcomes reflected no meaningful improvement in CSHQ (33) sleep quality either subjectively or objectively. Gringras et al. (2014) conducted a more rigorous randomized control study with crossover, and a much larger sample size (N = 73). Based on the actigraph sleep measure used, the weighted blanket (used for 12–16 days) failed to lead to improved quantitative sleep scores, although parents perceived their child slept better and was calmer after using the weighted blanket. In addition, parents reported that their child liked sleeping under the weighted blanket.
Lawson and Little (2017) investigated a sensory-enhanced swim program for autistic children. In this pre/post single group study autistic children with sensory integration/processing concerns identified using the SP, participated in 8 weekly 1:1 swim lessons, each 30 min in length. There was also the opportunity for social interaction. The sensory enhancements to swimming were based on sensory strengths and needs, as identified on the sensory profile, along with visual schedules, communication strategies, physical supports, and modeling. They found the intervention to be feasible, with high parent satisfaction. Looking at sleep outcomes reflected on the CSHQ (33), 40% of the children showed reduced sleep disturbance, and 50% showed increased sleep disturbance. Of the 40% showing improvements in sleep, children were older, autism severity scores were lower, the children attended more swim sessions, and baseline sensory differences reflected sensory hyper-reactivity but low sensory seeking. Investigators concluded that children with sensory hyper-reactivity may be the best candidates for this intervention; they hypothesized that engagement in the intervention provided proprioceptive and tactile inputs that helped the children regulate their arousal. Johnson et al. (2021) also utilized a swimming intervention, provided in 12-sessions over a 3-week timeframe. Although the focus of this study was on child challenging behavior and parent wellbeing, parent report indicated improved sleep on the days of swim lessons.
Cullen et al. (2005) trained parents to implement a touch therapy (massage) program, titled “Training and Support Programme” (TSP). Parents received 8 weekly training sessions with the therapist and their child. In addition, they received written information which included instructions, diagrams, and photographs to guide the touch interactions with their child. Parents completed home record sheets and engaged in an interview 16 weeks from baseline. The home record sheets indicated that touch therapy sessions lead to calm, relaxation, and sleepiness in five of seven children, and improved sleep patterns for six of the seven children reported to have sleep difficulties. Other benefits were also noted, including an increased feeling of closeness between parent and child.
Silva et al. (2007) examined the effect of providing Cignolini Qigong massage to autistic children, determining if they could replicate outcomes from an earlier case series (Silva and Cignolini, 2005). Using a two-group design (treatment and control), trained practitioners initially provided massage (11 massage movements delivered in approximately 15 min) twice weekly for 5 weeks. Parents were given written and verbal instruction during initial sessions and demonstrated their ability to provide intervention during later sessions. For the next 5 weeks, the parent provided the massage at least once daily. Practitioner and parent interventions then alternated in 5-week blocks for the 5-month intervention. At the 5-month time, investigators offered intervention to the control group, based on improvements in the intervention group. Silva et al. (2007) reported global improvement in sensory processing scores on the Sensory Profile following the intervention, and a worsening of sensory concerns in the control group prior to being switched to intervention. Sleep improvements were reported by parents in areas including going to sleep at a typical time, faster sleep onset time and sleeping through the night.
While there is a body of literature addressing the sensory differences experienced by autistic individuals (cf. Crane et al., 2009; Elwin et al., 2017; Feldman et al., 2020) and another addressing sleep concerns (cf. Malow et al., 2006; Goldman et al., 2012; Morgan et al., 2020), the interplay between these constructs has not received the same degree of consideration. We report evidence indicating, at minimum, a co-existence of sensory integration/processing differences and sleep concerns in autistic children, and to some extent, autistic adults (Nieminen-von Wendt et al., 2005; Klintwall et al., 2011; Reynolds et al., 2012; Silva and Schalock, 2012; Tzischinsky et al., 2018; Wang et al., 2019; Eyuboglu and Eyuboglu, 2020; Kosaka et al., 2021). In some instances the relationship was predictive (Hohn et al., 2019; Mazurek et al., 2019). Some narrative reviews, however, have suggested a causal relationship between sensory sensitivity and difficulties with sleep in autism (cf. Cortesi et al., 2010; Reynolds and Malow, 2011). A handful of investigators have begun to examine interventions that are sensory-based or sensory incidental in nature, with some having a positive, or partially positive, impact on sleep (Cullen et al., 2005; Silva and Schalock, 2012; Lawson and Little, 2017). However, there are few intervention studies, and they are hampered by small sample sizes and often no comparison groups.
Of note, the vast majority of literature we identified was on children and teens; only Hohn et al. (2019) focused on adults, and results indicated that insomnia in autistic adults was predicted by high levels of sensory reactivity differences, along with decreased social skills as defined in neurotypical individuals, as measured by the ASQ. Approaching this data dimensionally—per the RDoC framework—Hohn and colleagues suggest that these relations indicate a cyclical influence between quality of sleep, sensory responsivity and the resources autistic adults have available to navigate neurotypical social interactions.
While Sacco et al. (2010) included adults in their sample, the mean age in this study was 8.82 ± 5.62 years. They did identify a component of autism characterized by circadian and sensory integration/processing differences, linking sensory integration/processing differences and sleep concerns across several life stages. Thus, while we have some insight into the relationship between sleep concerns and sensory integration/processing differences in autistic adults, this connection requires further investigation.
Sleep concerns in autistics run the full gamut; bedtime resistance, sleep onset delay, short sleep duration, sleep anxiety, night wakings, sleep disorder breathing, parasomnias, daytime sleepiness; and shortened total sleep have all been reported. Investigators have variably found that sleep in autistics may or may not be influenced by age (Tzischinsky et al., 2018), autism severity (Hollway and Aman, 2011), behavioral differences (Hollway and Aman, 2011), medications, (Hollway et al., 2013; Tzischinsky et al., 2018) and intellectual ability (Hollway et al., 2013). Similarly, sensory integration/processing differences encompass a range of findings, including hyper- and hypo-reactivity and sensory seeking, with investigators also reporting a variety of specific sensory domain differences. The outcomes related to specific sensory domains are somewhat conflicting. Hohn et al. (2019) suggested that visual sensory sensitivity is a driver for insomnia in autistic adults. In children, investigators report poor auditory filtering and taste/smell differences (Hollway et al., 2013), tactile hypo-reactivity (Wang et al., 2019; Jamioł-Milc et al., 2021), vestibular and oral hyper-reactivity (Kosaka et al., 2021), vestibular hypo-reactivity (Ornitz et al., 1973; Wang et al., 2019), and touch and oral hyper-reactivity (Tzischinsky et al., 2018).
As might be expected, the relationship between poor sleep and sensory integration/processing differences is often described as complex and multi-faceted. The inconsistencies noted by these investigators are likely related, in part, to the assessment and outcome tools used. As noted, investigators often used the CSHQ or a version of it. Other investigators used sleep diaries, or purpose-built tools, all relying on parent report. While literature reports consistency between parent report and objective measures of some domains of sleep (Malow et al., 2006), other sleep concerns may be under-estimated (e.g., night wakings) or over-estimated (e.g., total sleep duration) (Goodwin et al., 2007) by parents. The intervention study conducted by Gringras et al. (2014), and the characterization study by Kosaka et al. (2021) coupled parent report tools with an objective measure of sleep such as actigraphy. To optimally measure sleep challenges many investigators recommended the use of actigraphy, polysomnography or activity trackers to enhance accuracy.
A variety of frameworks and models have been proposed to describe sensory reactivity differences, and, while there is some overlap between the models, there is no current consensus regarding typology. Most of the studies examined in this review relied on the model derived from the Sensory Profile (SP; Dunn, 1999), the Short Sensory Profile (SSP; McIntosh et al., 1999), and the Sensory Profile 2 (Dunn, 2014). As noted earlier, in this model Dunn considers the interface between neurological threshold and self-regulation in response to sensation, and identifies patterns across four quadrants (poor sensory registration, sensory seeking, sensory avoiding, and sensory sensitivity). Reactivity differences within each sensory domain (sensory section scores) can be identified along a continuum from hyper- to hypo-reactivity, and within behavioral domains (behavioral section scores). Other models of sensory processing differences have also been developed, but few were used in the studies included in our review. Thus, our review findings regarding sensory processing differences are informed more by the SP, or a derivative of it, than any other model or tool. Furthermore, the selection of these tools emphasizes differences in sensory modulation and omits sensory discrimination and the sensory-based motor differences of posture and motor planning defined in a recent model of sensory integration (Bundy and Lane, 2020). Expansion of research to include these dimensions would enable investigators to explore the dynamic interactions among constructs that contribute to health and illness.
Sleep is a universal and core occupation throughout the lifespan. Inadequate sleep can interfere with synaptic development and brain maturation, attention, memory, mood regulation, behavior, and other aspects of daytime function (Killgore, 2010; Beebe, 2011), leading to restrictions in occupation and participation. While sleep difficulties are not uncommon in the neurotypical population, sleep disorders have been reported in up to 80% of autistic individuals (Richdale and Schreck, 2009; Souders et al., 2009; Cortesi et al., 2010; Morgan et al., 2020). Souders and colleagues suggested that autism alone may predispose individuals to sleep problems. Alternatively, being autistic in a neurotypical world may itself predispose individuals to sleep problems.
Differences in neural synaptic pruning and neural organization, circadian function, and melatonin production, and arousal and sensory processing have been identified in autistic individuals, and are putative causes of insomnia. The potential connection with sensory integration/processing and establishing supportive circadian rhythm cannot be overlooked. Verhoeff et al. (2018) suggest that sleep concerns are part of the overall picture of autism. They indicate that sleep problems in autistics increase as children age, and contrast this with the decrease in sleep problems across ages seen in the neurotypical population. The effect of sleep deprivation, the high incidence of sleep concerns in autistics, and the possibility that sleep concerns may worsen during childhood, make it critical to consider effective interventions. In addition, and importantly, sleep challenges for autistic children also have a negative impact on the sleep of their parents (Lopez-Wagner et al., 2008).
Therapeutic supports have been suggested. A recent review and meta-synthesis of sleep interventions for autistic children indicated that intervention fell into five broad approaches: pharmacological, melatonin (which is sometimes included in the pharmacological category), behavioral, parent education, and alternative therapies (Cuomo et al., 2017). In terms of pharmacological interventions, melatonin appears to have the strongest level of support, especially for sleep duration and latency to sleep onset. A major drawback relative to melatonin is that it may stop working after its initial success (Bruni et al., 2007). In addition, Esposito et al. (2020) indicated that parents of autistic children often prefer non-pharmacological interventions.
There is some evidence suggesting that behavioral interventions, which include a wide array of approaches ranging from extinction, to developing sleep hygiene, may have positive effects. Practice Guidelines from the American Academy of Neurology (Buckley et al., 2020) support trying behavioral interventions initially, and offering melatonin as a second line of defense. Esposito et al. (2020) suggested that behavioral interventions will not be a good fit for all families; such interventions should be guided by a knowledgeable clinician and utilized by motivated caregivers. They further indicated that approaches such as sleep hygiene and behavioral interventions are not well utilized or understood by parents, and are not well researched.
Parent education programs show some effectiveness, although it appears to be relatively weak (Cuomo et al., 2017). The Autism Treatment Network6 provides a parent guide and sleep tool kit for parents that addresses sleep setting and aspects of sleep hygiene; it also includes a supplemental calming module, addressing internal factors including sensory and arousal dysregulation that threaten sleep. However, Adkins et al. (2012) have suggested that written material alone is not sufficient support for parents. Both Cullen et al. (2005) and Silva et al. (2007) provided written materials and one-to-one training in their investigations of different forms of massage. Cullen and colleagues noted that, while some of the child participants initially found touch therapy (massage) unsettling, the majority accommodated over the course of the program. Cullen et al. (2005) indicated that parents reported positive changes in many behaviors; of the seven children with sleep concerns, six showed improvements in sleep. This investigation did not include a comparison group. Silva and colleagues also report improved sleep following a Cignolini Qigong intervention, along with positive changes in sensory processing, adaptive and social skills. While still a relatively small study (total n = 15), a comparison group was included, adding some rigor.
Alternative interventions, including types of massage described above, have been noted to have some positive outcomes. In conducting this review we identified studies that we interpreted as sensory incidental, delivering sensation as an important component of the intervention. Two were yoga-based interventions, which would have incorporated proprioception and vestibular inputs as well as addressing sensorimotor differences like posture and bilateral coordination. In a pilot and follow-up study Narasingharao et al. (2017a,b) provided yoga to autistic children, delivered by a trained yoga teacher; parents were encouraged to practice asanas at home with their child. Investigators documented changes in all aspects of sleep measured by a purpose-built questionnaire in both studies; parent report indicated uninterrupted and longer duration nighttime sleep, and a reduction in daytime sleeping. Sleep disordered breathing also improved. Sensory changes noted included better body balance and body awareness, although there was no clear measure of sensory differences. Frazier et al. (2017) examined the effectiveness and tolerability of the “Sleep-to-Sound” mattress. This mattress technology allows users to hear any audio file, feel vibration, or have both stimuli coming through the mattress; the intensity of both sensations could be set by the user. In this study, a baseline period was followed by a 2-week intervention (mattress either on or off) with immediate crossover. Findings indicated overall tolerability, and improvement in sleep parameters including sleep duration and efficiency, as determined by actigraphy. In addition, parent-completed sleep diaries indicated improved sleep quality and ease of falling asleep. Unfortunately, because neither of these studies included a measure of sensory integration/processing they were not included in our review. Further, Cuomo et al. (2017) point out that the available studies using alternative interventions are of low quality. The guidelines from the American Academy of Neurology (Buckley et al., 2020) indicate that there is no evidence for the efficacy of interventions such as weighted blankets or specialized mattresses, much as we reported in this review.
Overall, the range of potential interventions coupled with limited research to support most described interventions points to a large gap in existing literature. In fact, Cuomo and colleagues concluded that of the available interventions, no single approach was effective across all domains of sleep concerns. Further, noted interventions failed to adequately address pre-sleep concerns (e.g., sleep anxiety). Given the clear relation between sleep concerns and sensory integration/processing differences (including modulation, discrimination and sensorimotor dimensions) identified in this review, we suggest that future investigations consider the inclusion of tools to address sensory differences within sleep focused interventions may provide a missing piece to the sleep intervention puzzle. This is supported in a case report by Souders et al. (2017), in which pre-sleep calming was based on sensory needs, along with anxiety, interests, and preferences, with positive outcomes for both sleep and anxiety.
We limited our search to articles published in English and Spanish. As such we may have missed pertinent articles. In addition, there is considerable variability in terminology around sensory integration/processing; we may have missed some articles due to variability in keyword use. We did not restrict our review to studies with high rigor, thus some of the reported findings require replication. Some studies lacked detail, and this along with the variability in assessment tools and terminology made it challenging to summarize across studies.
There is an established relationship between sleep concerns and sensory integration/processing differences in autistic children. In contrast, there is insufficient evidence to make this determination for autistic adults. Overall, research examining sensory and sleep differences in autistic individuals warrants future investigation. While the number of studies examining characteristics of this relationship exceeded those examining intervention, there is still much that is unclear. Intervention studies are few in number, and generally of low quality. This is an area ripe for future research.
SJL participated in developing search terms, initial abstract and title review, full-text review, and data extraction, was responsible for writing the initial draft, doing, and overseeing edits, and was first and primary author of the manuscript. MAL participated in developing search terms, running the search, de-duplicating, initial abstract, title review, full text review, and data extraction and assisted in manuscript development and editing. VS participated in full text review and data extraction, and contributed to the editing process. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Adkins, K., Molloy, C., Weiss, S., Reynolds, A., Goldman, S., Burnette, C., et al. (2012). Effects of a standardized pamphlet on insomnia in children with autism spectrum disorders. Pediatrics 130, S139–S144. doi: 10.1542/peds.2012-0900K
Allik, H., Larsson, J., and Smedje, H. (2006). Insomnia in school-age children with Asperger’s syndrome or high-functioning autism. BMC Psychiatr. 28, 6–18. doi: 10.1186/1471-244X-6-18
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders (DSM-5), 5th Edn. Washington, D.C: American Psychiatric Publishing.
Arksey, H., and O’Malley, L. (2005). Scoping studies: towards a methodological framework. Int. J. Soc. Res. Methodol. 8, 19–32. doi: 10.1080/1364557032000119616
Ashburner, J., Ziviani, J., and Rodger, S. (2008). Sensory processing and classroom emotional, behavioral, and educational outcomes in children with autism spectrum disorder. Am. J. Occup. Ther. 62, 564–573. doi: 10.5014/ajot.62.5.564
Beebe, D. W. (2011). Cognitive, behavioral, and functional consequences of inadequate sleep in children and adolescents. Pediatr. Clin. North Am. 58, 649–665. doi: 10.1016/j.pcl.2011.03.002
Berkley, A. S. (2021). Sleep, aging, and daily functioning. Nurs. Clin. North Am. 56, 287–298. doi: 10.1016/j.cnur.2021.02.007
Bogdashina, O. (2016). Sensory Perceptual Issues in Autism and Asperger Syndrome: Different Sensory Experiences-Different Perceptual Worlds. Philadelphia, PA: Jessica Kingsley Publishers.
Bruni, O., Ferri, R., Vittori, E., Novelli, L., Vignati, M., Porfirio, M. C., et al. (2007). Sleep architecture and NREM alterations in children and adolescents with Asperger’s syndrome. Sleep 30, 1577–1585. doi: 10.1093/sleep/30.11.1577
Buckley, A. W., Hirtz, D., Oskoui, M., Armstrong, M. J., Batra, A., Bridgemohan, C., et al. (2020). Practice guideline: Treatment for insomnia and disrupted sleep behavior in children and adolescents with autism spectrum disorder. Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology 94, 392–404. doi: 10.1212/WNL.0000000000009033
Bundy, A. C., and Lane, S. J. (2020). “Sensory integration: A. Jean Ayres’ theory revisited,” in Sensory Integration Theory and Practice, 3rd Edn, eds A. C. Bundy and S. J. Lane (Philadelphia: F.A. Davis) 2–55.
Clince, M., Connolly, L., and Nolan, C. (2016). Comparing and exploring the sensory processing patterns of higher education students with attention deficit hyperactivity disorder and autism spectrum disorder. Am. J. Occup. Ther. 70, 7002250010p1–9. doi: 10.5014/ajot.2016.016816
Cohen, S., Fulcher, B. D., Rajaratnam, S. M. W., Conduit, R., Sullivan, J. P., St Hilaire, M. A., et al. (2018). Sleep patterns predictive of daytime challenging behavior in individuals with low-functioning autism. Autism Res. 11, 391–403. doi: 10.1002/aur.1899
Cortesi, F., Giannotti, F., Ivanenko, A., and Johnson, K. (2010). Sleep in children with autistic spectrum disorder. Sleep Med. 11, 659–664. doi: 10.1016/j.sleep.2010.01.010
Crane, L., Goddard, L., and Pring, L. (2009). Sensory processing in adults with autism spectrum disorders. Autism 13, 215–228. doi: 10.1177/1362361309103794
Cullen, L. A., Barlow, J. H., and Cushway, D. (2005). Positive touch, the implications for parents and their children with autism: an exploratory study. Compl. Ther. Clin. Pract. 11, 182–189. doi: 10.1016/j.ctcp.2004.12.004
Cuomo, B. M., Vaz, S., Lee, E., Thompson, C., Rogerson, J. M., and Falkmer, T. (2017). Effectiveness of sleep-based interventions for children with autism spectrum disorder: a meta-synthesis. Pharmacotherapy 37, 555–578. doi: 10.1002/phar.1920
Deliens, G., and Peigneux, P. (2019). Sleep–behaviour relationship in children with autism spectrum disorder: methodological pitfalls and insights from cognition and sensory processing. Dev. Med. Child Neurol. 61, 1368–1376. doi: 10.1111/dmcn.14235
Dunn, W., Little, L., Dean, E., Robertson, S., and Evans, B. (2016). The state of the science on sensory factors and their impact on daily life for children: a scoping review. OTJR 36, 3S–26S. doi: 10.1177/1539449215617923
Elwin, M., Schröder, A., Ek, L., Wallsten, T., and Kjellin, L. (2017). Sensory clusters of adults with and without autism spectrum conditions. J. Autism Dev. Dis. 47, 579–589. doi: 10.1007/s10803-016-2976-1
Esposito, D., Belli, A., Ferri, R., and Bruni, O. (2020). Sleeping without prescription: Management of sleep disorders in children with autism with non-pharmacological interventions and over-the-counter treatments. Brain Sci. 10:441. doi: 10.3390/brainsci10070441
Eyuboglu, M., and Eyuboglu, D. (2020). Sensory reactivity and sleep problems in toddlers with autism spectrum disorder and anxiety/depression symptoms in their mothers: are they related? Early Child Dev. Care 190, 1791–1801. doi: 10.1080/03004430.2018.1550750
Feldman, J. I., Cassidy, M., Liu, Y., Kirby, A. V., Wallace, M. T., and Woynaroski, T. G. (2020). Relations between sensory responsiveness and features of autism in children. Brain Sci. 10:775. doi: 10.3390/brainsci10110775
Frazier, T. W., Krishna, J., Klingemier, E., Beukemann, M., Nawabit, R., and Ibrahim, S. (2017). A randomized, crossover trial of a novel sound-to-sleep mattress technology in children with autism and sleep difficulties. J. Clin. Sleep Med. 13, 95–104. doi: 10.5664/jcsm.6398
Gabriels, R. L., Cuccaro, M. L., Hill, D. E., Ivers, B. J., and Goldson, E. (2005). Repetitive behaviors in autism: relationships with associated clinical features. Res. Dev. Disabil. 26, 169–181. doi: 10.1016/j.ridd.2004.05.003
Gee, B. M., Peterson, T. G., Buck, A., and Lloyd, K. (2016). Improving sleep quality using weighted blankets among young children with an autism spectrum disorder. Int. J. Ther. Rehabil. 23, 173–181. doi: 10.12968/ijtr.2016.23.4.173
Gee, B. M., Lloyd, K., Sutton, J., and McOmber, T. (2021a). Weighted blankets and sleep quality in children with autism spectrum disorders: a single-subject design. Children 8:10. doi: 10.3390/children8010010
Gee, B. M., Scharp, V., and Williams, A. (2021b). Weighted blankets and sleep quality in children with autism spectrum disorders: a single-subject design. Open J. Occup. Ther. 9:10. doi: 10.15453/2168-6408.1704
Ghanbari, S., and Rezaei, A. (2016). The relationship between sensory-processing disorders and sleep disturbances in school-aged autistic children in shiraz. Jundishapur. J. Chronic. Dis. Care 5:e32337. doi: 10.17795/jjcdc-32337 [Epub ahead of print].
Giannotti, F., Cortesi, F., Cerquiglini, A., Miraglia, D., Vagnoni, C., Sebastiani, T., et al. (2008). An investigation of sleep characteristics, EEG abnormalities and epilepsy in developmentally regressed and non-regressed children with autism. J. Autism Dev. Dis. 38, 1888–1897. doi: 10.1007/s10803-008-0584-4
Goldman, S. E., Richdale, A. L., Clemons, T., and Malow, B. A. (2012). Parental sleep concerns in autism spectrum disorders: variations from childhood to adolescence. J. Autism Dev. Dis. 42, 531–538. doi: 10.1007/s10803-011-1270-5
Goodwin, J. L., Silva, G. E., Kaemingk, K. L., Sherrill, D. L., Morgan, W. J., and Quan, S. F. (2007). Comparison between reported and recorded total sleep time and sleep latency in 6- to 11-year-old children: the Tucson Children’s Assessment of Sleep Apnea Study (TuCASA). Sleep Breath. 11, 85–92. doi: 10.1007/s11325-006-0086-6
Gringras, P., Green, D., Wright, B., Rush, C., Sparrowhawk, M., Pratt, K., et al. (2014). Weighted blankets and sleep in autistic children - a randomized controlled trial. Pediatrics 134, 298–306. doi: 10.1542/peds.2013-4285
Harrison, L. A., Kats, A., Williams, M. E., and Aziz-Zadeh, L. (2019). The importance of sensory processing in mental health: A proposed addition to the Research Domain Criteria (RDoC) and suggestions for RDoC 2.0. Front. Psychol. 10:103. doi: 10.3389/fpsyg.2019.00103
Hirata, I., Mohri, I., Kato-Nishimura, K., Tachibana, M., Kuwada, A., Kagitani-Shimono, K., et al. (2016). Sleep problems are more frequent and associated with problematic behaviors in preschoolers with autism spectrum disorder. Res. Dev. Disabil. 4, 86–99. doi: 10.1016/j.ridd.2015.11.002
Hochhauser, M., and Engel-Yeger, B. (2010). Sensory processing abilities and their relation to participation in leisure activities among children with high-functioning autism spectrum disorder (HFASD). Res. Autism Spectr. Dis. 4, 746–754. doi: 10.1016/j.rasd.2010.01.015
Hoekstra, R. A., Vinkhuyzen, A. A., Wheelwright, S., Bartels, M., Boomsma, D. I., Baron-Cohen, S., et al. (2011). The construction and validation of an abridged version of the Autism-Spectrum Quotient (AQ-Short). J. Autism Dev. Dis. 41, 589–596. doi: 10.1007/s10803-010-1073-0
Hohn, V. D., de Veld, D. M. J., Mataw, K. J. S., van Someren, E. J. W., and Begeer, S. (2019). Insomnia severity in adults with autism spectrum disorder is associated with sensory hyper-reactivity and social skill impairment. J. Autism Dev. Dis. 49, 2146–2155. doi: 10.1007/s10803-019-03891-8
Hollway, J. A., and Aman, M. G. (2011). Sleep correlates of pervasive developmental disorders: a review of the literature. Res. Dev. Dis. 32, 1399–1421. doi: 10.1016/j.ridd.2011.04.001
Hollway, J. A., Aman, M. G., and Butter, E. (2013). Correlates and risk markers for sleep disturbance in participants of the Autism Treatment Network. J. Autism Dev. Dis. 43, 2830–2843. doi: 10.1007/s10803-013-1830-y
Hundley, R. J., Shui, A., and Malow, B. A. (2016). Relationship between subtypes of restricted and repetitive behaviors and sleep disturbance in autism spectrum disorder. J. Autism Dev. Dis. 46, 3448–3457. doi: 10.1007/s10803-016-2884-4
Jamioł-Milc, D., Bloch, M., Liput, M., Stachowska, L., and Skonieczna-Żydecka, K. (2021). Tactile processing and quality of sleep in autism spectrum disorders. Brain Sci. 11:362. doi: 10.3390/brainsci11030362
Johnson, N. L., Bekhet, A. K., Karenke, T., and Garnier-Villarreal, M. (2021). Swim program pilot for children with autism: impact on behaviors and health. West J. Nurs. Res. 43, 356–363. doi: 10.1177/0193945920948867
Killgore, W. D. (2010). Effects of sleep deprivation on cognition. Prog. Brain Res. 185, 105–129. doi: 10.1016/B978-0-444-53702-7.00007-5
Klintwall, L., Holm, A., Eriksson, M., Carlsson, L. H., Olsson, M. B., Hedvall, A., et al. (2011). Sensory abnormalities in autism. A brief report. Res. Dev. Disabil. 32, 795–800. doi: 10.1016/j.ridd.2010.10.021
Kosaka, T., Kawatani, M., Ohta, G., Mizuno, Y., Takiguchi, S., Kumano, A., et al. (2021). Low threshold to vestibular and oral sensory stimuli might affect quality of sleep among children with autism spectrum disorder. Brain Dev. 43, 55–62. doi: 10.1016/j.braindev.2020.07.01
Lafrance, M. N., and McKenzie-Mohr, S. (2013). The DSM and its lure of legitimacy. Fem. Psychol. 23, 119–140. doi: 10.1177/0959353512467974
Lawson, L. M., and Little, L. (2017). Feasibility of a swimming intervention to improve sleep behaviors of children with autism spectrum disorder. Ther. Recreat. J. 51, 97–108. doi: 10.18666/TRJ-2017-V51-I2-7899
Limoges, E., Mottron, L., Bolduc, C., Berthiaume, C., and Godbout, R. (2005). Atypical sleep architecture and the autism phenotype. Brain 128, 1049–1061. doi: 10.1093/brain/awh425
Little, L. M., Ausderau, K., Sideris, J., and Baranek, G. T. (2015). Activity participation and sensory features among children with autism spectrum disorders. J. Autism. Dev. Dis. 45, 2981–2990. doi: 10.1007/s10803-015-2460-3
Lopez-Wagner, M. C., Hoffman, C. D., Sweeney, D. P., Hodge, D., and Gilliam, J. E. (2008). Sleep problems of parents of typically developing children and parents of children with autism. J. Genet. Psychol. 169, 245–259. doi: 10.3200/GNTP.169.3.245-260
Malow, B. A., Marzec, M. L., McGrew, S. G., Wang, L., Henderson, L. M., and Stone, W. L. (2006). Characterizing sleep in children with autism spectrum disorders: a multidimensional approach. Sleep 29, 1563–1571. doi: 10.1093/sleep/29.12.1563
Manelis-Baram, L., Meiri, G., Ilan, M., Faroy, M., Michaelovski, A., Flusser, H., et al. (2021). Sleep disturbances and sensory sensitivities co-vary in a longitudinal manner in pre-school children with autism spectrum disorders. J. Autism Dev. Disord. 52, 923–937. doi: 10.1007/s10803-021-04973-2
Marco, E. J., Hinkley, L. B., Hill, S. S., and Nagarajan, S. S. (2011). Sensory processing in autism: a review of neurophysiologic findings. Pediatric. Res. 69, 48R–54R. doi: 10.1203/pdr.0b013e3182130c54
Mazurek, M. O., Dovgan, K., Neumeyer, A. M., and Malow, B. A. (2019). Course and predictors of sleep and co-occurring problems in children with autism spectrum disorder. J. Autism Dev. Dis. 49, 2101–2115. doi: 10.1007/s10803-019-03894-5
Mazurek, M. O., and Petroski, G. F. (2015). Sleep problems in children with autism spectrum disorder: examining the contributions of sensory over-responsivity and anxiety. Sleep Med. 16, 270–279. doi: 10.1016/j.sleep.2014.11.006
McIntosh, D. N., Miller, L. J., Shru, V., and Dunn, W. (1999). “Overview of the Short Sensory Profile,” in Sensory Profile, ed. W. Dunn (San Antonio, TX: Psychological Corporation), 59–75.
Medic, G., Wille, M., and Hemels, M. E. (2017). Short- and long-term health consequences of sleep disruption. Nat. Sci. Sleep 9, 151–161. doi: 10.2147/NSS.S134864
Miano, S., Bruni, O., Elia, M., Trovato, A., Smerieri, A., Verrillo, E., et al. (2007). Sleep in children with autistic spectrum disorder: a questionnaire and polysomnographic study. Sleep Med. 9, 64–70. doi: 10.1016/j.sleep.2007.01.014
Miller, L. J., Anzalone, M. E., Lane, S. J., Cermak, S. A., and Osten, E. T. (2007). Concept evolution in sensory integration: a proposed nosology for diagnosis. Am. J. Occup. Ther. 61, 135–140.
Morgan, B., Nageye, F., Masi, G., and Cortese, S. (2020). Sleep in adults with autism spectrum disorder: systematic review and meta-analysis of subjective and objective studies. Sleep Med. 65, 113e20. doi: 10.1016/j.sleep.2019.07.019
Mueller, I., and Tronick, E. (2020). “Sensory processing and meaning making in autism spectrum disorder,” in Autism 360°, 1st Edn, eds U. N. Das, N. Papaneophytou, and E. El-Kour (Cambridge, MA: Academic Press).
Narasingharao, K., Pradhan, B., and Navaneetham, J. (2017a). Efficacy of structured yoga intervention for sleep, gastrointestinal and behaviour problems of ASD children: an exploratory study. J. Clin. Diagn. Res. 11, VC01–VC06. doi: 10.7860/jcdr/2017/25894.9502
Narasingharao, K., Pradhan, B., and Navaneetham, J. (2017b). Feasibility of parent-based yoga intervention for group of autism spectrum disorder children in special schools: a pilot study. Int. J. Res. Ayurveda. Pharm. 8, 56–60. doi: 10.7897/2277-4343.08263
Neufield, J., Eriksson, L. H., Hammarsten, R., Remnelius, K. L., Tillmann, J., Isaksson, J., et al. (2021). The impact of atypical sensory processing on adaptive functioning within and beyond autism: the role of familial factors. Autism 25, 2341–2355. doi: 10.1177/13623613211019852
Neuman, A., Greenberg, D. F., Labovitz, D. R., and Suzuki, L. A. (2004). Cross-cultural adaptation of the Sensory Profile: Establishing linguistic equivalency of the Hebrew version. Occup. Ther. Int. 11, 112–130. doi: 10.1002/oti.201
Nieminen-von Wendt, T., Paavonen, J. E., Ylisaukko-Oja, T., Sarenius, S., Kallman, T., Jarvela, I., et al. (2005). Subjective face recognition difficulties, aberrant sensibility, sleeping disturbances and aberrant eating habits in families with Asperger syndrome. BMC Psychiatr. 5:20. doi: 10.1186/1471-244X-5-20
O’Reilly, M., Lester, J. N., and Kiyimba, N. (2020). “Autism in the twentieth century: An evolution of a controversial condition,” in Healthy minds in the twentieth century, eds S. J. Taylor and A. Brumby (London: Palgrave Macmillan), 137–165. doi: 10.1007/978-3-030-27275-3_7
Ornitz, E. M., Forsythe, A. B., and de la Pena, A. (1973). Effect of vestibular and auditory stimulation on the REMs of REM sleep in autistic children. Arch. Gen. Psychiatr. 29, 786–791. doi: 10.1001/archpsyc.1973.04200060062009
Owens, J. A., Spirito, A., and McGuinn, M. (2000). The Children’s Sleep Habits Questionnaire (CSHQ): psychometric properties of a survey instrument for school-aged children. Sleep 23, 1043–1051.
Peters, M. D. J., Godfrey, C., McInerney, P., Munn, Z., Tricco, A. C., and Khalil, H. (2020). “Scoping reviews,” in JBI Manual for Evidence Synthesis, Chap. 11, eds E. Aromataris and Z. Munn .
Puts, N. A., Wodka, E. L., Tommerdahl, M., Mostofsky, S. H., and Edden, R. A. (2014). Impaired tactile processing in children with autism spectrum disorder. J. Neurophysiol. 111, 1803–1811. doi: 10.1152/jn.00890.2013
Reynolds, A. M., and Malow, B. A. (2011). Sleep and Autism Spectrum Disorders. Pediatr. Clin. N. Am. 58, 685–698. doi: 10.1016/j.pcl.2011.03.009
Reynolds, S., Bendixen, R. M., Lawrence, T., and Lane, S. J. (2011). A pilot study examining activity participation, sensory responsiveness, and competence in children with high functioning autism spectrum disorder. J. Autism. Dev. Dis. 41, 1496–1506. doi: 10.1007/s10803-010-1173-x
Reynolds, S., Lane, S. J., and Thacker, L. (2012). Sensory processing, physiological stress, and sleep behaviors in children with and without autism spectrum disorders. OTJR 32, 246–257. doi: 10.1186/s12868-016-0283-6
Richdale, A. L., and Schreck, K. A. (2009). Sleep problems in autism spectrum disorders: prevalence, nature, & possible biopsychosocial aetiologies. Sleep Med. Rev. 13, 403–411. doi: 10.1016/j.smrv.2009.02.003
Robertson, C. E., and Baron-Cohen, S. (2017). Sensory perception in autism. Nat. Rev. Neurosci. 18, 671–684. doi: 10.1038/nrn.2017.112
Robertson, A. E., and Simmons, R. D. R. (2015). The sensory experiences of adults with autism spectrum disorder: a qualitative analysis. Perception 44, 569–586. doi: 10.1068/p7833
Roley, S. S., Mailloux, Z., Parham, L. D., Schaaf, R. C., Lane, C. J., and Cermak, S. (2015). Sensory integration and praxis patterns in children with autism. Am. J. Occup. Ther. 69:6901220010. doi: 10.5014/ajot.2015.012476
Sacco, R., Curatolo, P., Manzi, B., Militerni, R., Bravaccio, C., Frolli, A., et al. (2010). Principal pathogenetic components and biological endophenotypes in autism spectrum disorders. Autism Res. 3, 237–252. doi: 10.1002/aur.151
Schaaf, R. C., and Lane, A. E. (2015). Toward a best-practice protocol for assessment of sensory features in ASD. J. Autism Dev. Dis. 45, 1380–1395. doi: 10.1007/s10803-014-2299-z
Schreck, K. A., Mulick, J. A., and Smith, A. F. (2004). Sleep problems as possible predictors of intensified symptoms of autism. Res. Dev. Disabil. 25, 57–66. doi: 10.1016/j.ridd.2003.04.007
Shochat, T., Tzchishinsky, O., and Engel-Yeger, B. (2009). Sensory hypersensitivity as a contributing factor in the relation between sleep and behavioral disorders in normal schoolchildren. Behav. Sleep Med. 7, 53–62. doi: 10.1080/15402000802577777
Silva, L., and Cignolini, A. (2005). A medical qigong methodology for early intervention in autism spectrum disorder: A case series. Am. J. Chin. Med. 33, 315–327. doi: 10.1142/S0192415X05002837
Silva, L. M., Cignolini, A., Warren, R., Budden, S., and Skowron-Gooch, A. (2007). Improvement in sensory impairment and social interaction in young children with autism following treatment with an original Qigong massage methodology. Am. J. Chin. Med. 35, 393–406. doi: 10.1142/S0192415X07004916
Silva, L. M. T., and Schalock, M. (2012). Sense and self-regulation checklist, a measure of comorbid autism symptoms: initial psychometric evidence. Am. J. Occup. Ther. 66, 177–186. doi: 10.5014/ajot.2012.001578
Silverman, F., and Tyszka, A. C. (2017). Supporting participation for children with sensory processing needs and their families: community-based action research. Am. J. Occup. Ther. 71, 7104100010p1–7104100010p9.
Sinclair, D., Oranje, B., Razak, K. A., Siegel, S. J., and Schmid, S. (2017). Sensory processing in autism spectrum disorders and Fragile X syndrome-From the clinic to animal models. Neurosci. Biobehav. Rev. 76, 235–253. doi: 10.1016/j.neubiorev.2016.05.029
Souders, M., Mason, T., Valladares, O., Bucan, M., Levy, S., Mandell, D., et al. (2009). Sleep behaviors and sleep quality in children with autism spectrum disorders. Sleep 32, 1566–1578. doi: 10.1093/sleep/32.12.1566
Souders, M. C., Zavodny, S., Eriksen, W., Sinko, R., Connell, J., Kerns, C., et al. (2017). Sleep in children with Autism Spectrum Disorder. Cur. Psychiatr. Rep. 19:34. doi: 10.1007/s11920-017-0782-x
Sweet, P. L., and Decoteau, C. L. (2017). Contesting normal: The DSM-5 and psychiatric subjectivation. BioSocieties 13, 103–122. doi: 10.1057/s41292-017-0056-1
Syu, Y. A., and Lin, L.-Y. (2018). Sensory overresponsivity, loneliness, and anxiety in Taiwanese adults with autism spectrum disorder. Occup. Ther. Int. 2018, 9165978. doi: 10.1155/2018/9165978
Tavassoli, T., Hoekstra, R. A., and Baron-Cohen, S. (2014a). The Sensory Perception Quotient (SPQ): Development and validation of a new sensory questionnaire for adults with and without autism. Mol. Autism 5:29. doi: 10.1186/2040-2392-5-29
Tavassoli, T., Miller, L. J., Schoen, S. A., Nielsen, D. M., and Baron-Cohen, S. (2014b). Sensory over-responsivity in adults with autism spectrum conditions. Autism 18, 428–432. doi: 10.1177/1362361313477246
Taylor, E., Holt, R., Tavassoli, T., Ashwin, C., and Baron-Cohen, S. (2020). Revised scored Sensory Perception Quotient reveals sensory hypersensitivity in women with autism. Mol. Autism 11:18. doi: 10.1186/s13229-019-0289-x
Tester, N. J., and Foss, J. J. (2018). Sleep as an occupational need. Am. J. Occup. Ther. 72, 7201347010p1–7201347010p4. doi: 10.5014/ajot.2018.020651
Tomchek, S. D., and Dunn, W. (2007). Sensory processing in children with and without autism: a comparative study using the Short Sensory Profile. Am. J. Occup. Ther. 61, 190–200. doi: 10.5014/ajot.61.2.190
Tricco, A. C., Lillie, E., Zarin, W., O’Brien, K. K., Colquhoun, H., Levac, D., et al. (2018). PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann. Int. Med. 169, 467–473. doi: 10.7326/M18-0850
Tzchishinsky, O., Lufi, D., and Shochat, T. (2008). Reliability of the Children’s Sleep Habits Questionnaire Hebrew translation and cross cultural comparison of the psychometric properties. Sleep Diagnosis. Ther. 3, 30–34.
Tzischinsky, O., Meiri, G., Manelis, L., Bar-Sinai, A., Flusser, H., Michaelovski, A., et al. (2018). Sleep disturbances are associated with specific sensory sensitivities in children with autism. Mol. Autism. 9:22. doi: 10.1186/s13229-018-0206-8
Verhoeff, M. E., Blanken, L., Kocevska, D., Mileva-Seitz, V. R., Jaddoe, V., White, T., et al. (2018). The bidirectional association between sleep problems and autism spectrum disorder: a population-based cohort study. Mol. Autism. 9:8. doi: 10.1186/s13229-018-0194-8
Wang, G. F., Li, W. L., Han, Y., Gao, L., Dai, W., Su, Y. Y., et al. (2019). Sensory processing problems and comorbidities in Chinese preschool children with autism spectrum disorders. J. Autism. Dev. Dis. 49, 4097–4108. doi: 10.1007/s10803-019-04125-7
Watson, L. R., Patten, E., Baranek, G. T., Poe, M., Boyd, B. A., Freuler, A., et al. (2011). Differential associations between sensory response patterns and language, social, and communication measures in children with autism or other developmental disabilities. J. Speech Lang. Hear. Res. 54, 1562–1576. doi: 10.1044/1092-4388(2011/10-0029)
Keywords: autism spectrum disorder, sleep disturbances, sensory processing/integration, sensory reactivity, children, adults, insomnia
Citation: Lane SJ, Leão MA and Spielmann V (2022) Sleep, Sensory Integration/Processing, and Autism: A Scoping Review. Front. Psychol. 13:877527. doi: 10.3389/fpsyg.2022.877527
Received: 16 February 2022; Accepted: 15 April 2022;
Published: 17 May 2022.
Edited by:
Catana Brown, Midwestern University, United StatesReviewed by:
Angeles F. Estévez, University of Almería, SpainCopyright © 2022 Lane, Leão and Spielmann. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shelly J. Lane, c2hlbGx5LmxhbmVAY29sb3N0YXRlLmVkdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.