 Tomas Frymann
Tomas Frymann Sophie Whitney
Sophie Whitney David B. Yaden
David B. Yaden Joshua Lipson
Joshua Lipson- 1Psychology and Spirituality Lab, Department of Counseling and Clinical Psychology, Teachers College, Columbia University, New York, NY, United States
- 2Depth and Clinical Psychology, Pacifica Graduate University, Carpinteria, CA, United States
- 3Department of Psychiatry and Behavioral Sciences, Center for Psychedelic and Consciousness Research, Johns Hopkins University School of Medicine, Baltimore, MD, United States
In this study, we describe the development and initial validation of two psychometric scales for measuring psychedelic integration. Psychedelic integration refers to the post-acute period of time following psychedelic drug administration. We created the Integration Engagement Scale (IES) to capture positive behavioral engagement with integration and the Experienced Integration Scale (EIS) to capture internal aspects of feeling integrated. These scales were developed to measure post-acute psychedelic administration dynamics in order to inform the creation of enhanced integration support and to help refine a general conceptual understanding of the construct of psychedelic integration. The scales are brief and face valid instruments designed for practical use in applied and research settings. Scale items were generated and refined using the Iterative Process Model of scale development, with input from psychedelics experts and clinicians. Content validity, internal structure, and reliability were assessed via expert surveys, content validity analysis, cognitive interviewing, convergent validity analysis, exploratory factor analysis, and confirmatory factor analysis. The data indicates the scales are valid and reliable measurements of the behavioral and experiential forms of Psychedelic Integration.
Introduction
Classic psychedelics (e.g., psilocybin and LSD; Nichols, 2016) can occasion effects spanning self-dissolution, the experience of intense emotions, distortion of sensory awareness, and even a sense of death and rebirth (Griffiths et al., 2006, 2008, 2011, 2016, 2018; Johnson et al., 2008; Cook, 2014; Hendricks et al., 2015; Carhart-Harris et al., 2016; Richards, 2016; Yaden and Griffiths, 2020). Such experiences often result in a lasting sense of improved life quality (Griffiths et al., 2006, 2008, 2011, 2016, 2018; Carhart-Harris et al., 2016). However, psychedelic experiences can also be challenging, confusing, and destabilizing, as they can catalyze radical changes, in both immediate states of consciousness and lasting aspects of life (Strassman, 1984; Barrett et al., 2016; Dos Santos et al., 2016). While enhanced wellbeing is a common result of psychedelic use, the psychological changes they induce can range from positive to negative, depending on how they are contextualized and supported (Carbonaro et al., 2016; Gorman et al., 2021). Psychedelic integration, which we define in this article as “The process by which a psychedelic experience translates into positive changes in daily life,” can help to ensure that change resulting from psychedelic experiences happens as beneficially, sustainably, and smoothly as possible, and that risks associated with use are minimized (Tupper et al., 2015).
Psychedelics are currently utilized in a variety of contexts, spanning psychiatric treatment at medical clinics, clinical trials at university research centers, healing ceremonies at retreat centers, guided journeys with underground guides, and recreational use within a diverse range of settings (Rucker et al., 2019; Yaden et al., 2021, 2022). Interest in the field continues to grow exponentially, as research continues to highlight the potential for psychedelics to contribute to lasting improvements in overall wellbeing and high rates of remission for treatment-resistant mental health symptoms (Mahr and Sweigart, 2020). As of 2013, there were 30 million lifetime users of psychedelics in the United States, a number poised to increase with the passing of decriminalization laws and the establishment of medically licensed clinics offering access to psychedelic treatments (Krebs and Johansen, 2013; Pilecki et al., 2021). However, psychedelic integration remains empirically understudied. As stated in the Yale Handbook for Psilocybin-Assisted Therapy, “While psychedelic integration has become a buzzword in psychedelic communities, it remains somewhat vaguely conceived, undertheorized, and, in general, longs for an operational relationship to the problem being treated” (Guss et al., 2020).
The importance of psychedelic integration became apparent at a cultural level in the wake of widespread LSD use in the United States during the 1960s and 70s. Timothy Leary’s slogan, “turn on, tune in, drop out,” captured the zeitgeist of the time—a strong message to split off from society and generally disconnect from social structures, roles, and responsibilities (Riley et al., 2010; Wesson, 2011). This message of encouraged disconnecting was at odds with healthy and adaptive forms of integration. In the aftermath of the festive free love movement, which placed psychedelic culture in opposition to being an engaged member of society, problems related to a reckless approach to life and substance use arose, including young adults falling into homelessness and using addictive drugs, such as methamphetamine, an increase in STD rates, and children being born without resources to be cared for (Wesson, 2011; Belouin and Henningfield, 2018). At the same time, the therapeutic potential of LSD was well documented (Wesson, 2011). Situated within a milieu that did not adequately support the importance of integration, however, cases of misuse and abuse continued and led to the association of psychedelics with risky and irresponsible behaviors (Tanne, 2004; Nichols, 2016). Today, we are in what has been described as a “psychedelic renaissance,” with rates of usage among adults increasing steadily along with the revival of psychedelic research (Krebs and Johansen, 2013; Kelly et al., 2019; Aday et al., 2020; Yockey et al., 2020; Killion et al., 2021; Palamar et al., 2021), warranting caution for both researchers and clinicians (Yaden et al., 2021).
An understanding of the domain of psychedelic integration begins with the meaning of the individual terms, “psychedelic” and “integration.” In the present article, we propose a definition of psychedelic integration that is congruent with the broader meaning of the term “integration,” as it applies to psychedelic experiences. The term “psychedelic” stems from two Ancient Greek words, psyche (mind or soul) and delos (to reveal, manifest, or make visible)—translating to mind-manifesting (Nichols, 2016). Neurobiologist Daniel Siegel (2016, p. 125) defines integration as “Unifying or connecting previously disconnected parts”. With “integration” as applied to “psychedelics,” the different elements brought into union are the non-ordinary experience occasioned by a psychedelic, on one hand, and the ordinary experience of daily life, on the other.
With the individual terms in mind, for the purpose of this research, we define psychedelic integration as: the process by which a psychedelic experience translates into positive changes in daily life. This definition describes integration as (1) Ongoing (a “process” which takes place over time); (2) Connection-Oriented (the “translation” of non-ordinary awareness into changes in ordinary life); (3) Helpful (“positive changes” identified as the natural output of applied insight); and (4) Embodied (“daily life” implying enacted changes in everyday behaviors). Our proposed definition aligns with scientific literature, including the Psychedelic Harm Reduction and Integration model (PHRI; Gorman et al., 2021, p. 8), which states “The goal of integration is to merge the psychedelic experience with the patient’s daily life in a way that helps the patient live a fuller life with less distress”. It also considers aspects of psychedelic integration described in the Yale Manual for Psilocybin Assisted Treatment of Depression, which states that integration is “a means of both making sense and meaning out of the experience, and helping positive changes and insights carry forth into day-to-day life” (Guss et al., 2020, p. 10). Similarly, the proposed definition of integration fits with Gandy et al. (2020, p. 8) description of therapeutic integration sessions as being “intended to support the participant in fully understanding any insights discovered during the session, and applying them to their life going forward”.
The Present Study
Overview of the Domain and Subdomains of Psychedelic Integration
To measure psychedelic integration, two distinct integration scales were developed, the Integration Engagement Scale (IES) and the Experienced Integration Scale (EIS). The IES focuses on behavioral engagement with integration, while the EIS focuses on the intrapsychic experience of integration. These scales aim to capture the distinct behavioral and experiential aspects of psychedelic integration, which may or may not co-occur. We developed the scales so that they may either be used individually or in tandem, when contextually appropriate, according to the needs of the investigator. The scales are designed to be used on an ongoing basis, given that psychedelic integration is an ongoing process. The final scale items and instructions are included in Figure 1.
We developed the Psychedelic Integration Scales following the Iterative Process Model, a generalized model of scale development formulated by Chatterji (2003). This approach emphasizes the importance of considering both a theoretical delineation of the measured construct as well as feedback from clinicians and experts, in an iterative process of item revision. The iterative development process of the Psychedelic Integration Scales began with the construction of the Integration Engagement Scale, and after expert feedback subsequently led to the development of a complementary Experienced Integration Scale. Our final aim was to create two brief psychedelic integration scales that would be valid and reliable tools for predicting beneficial outcomes from psychedelic experiences in clinical and non-clinical settings.
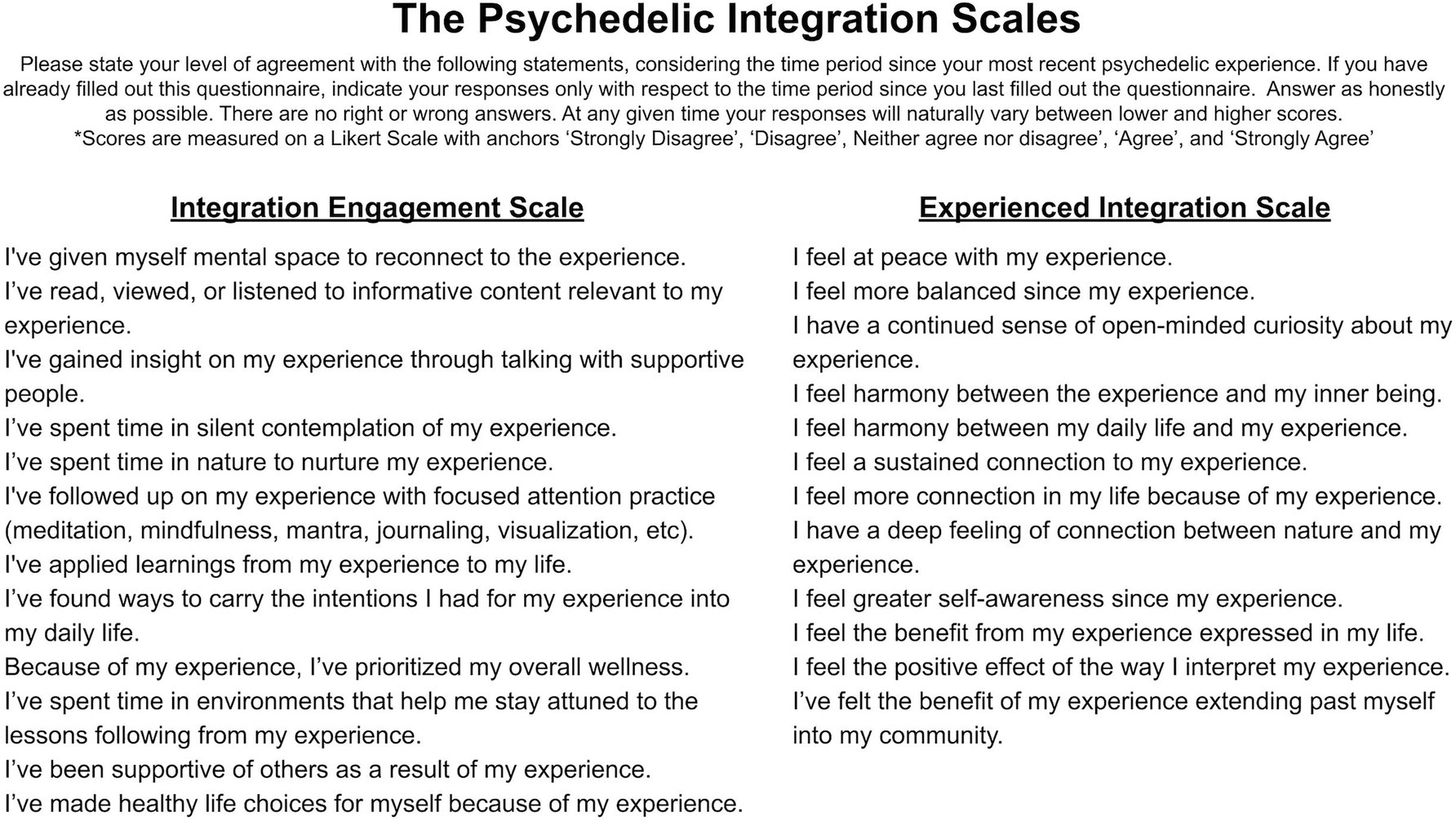
Figure 1. Psychedelic Integration Scales final items.
We conducted five studies in order to provide initial validity and reliability evidence on two scales. Pacifica Graduate Institute IRB approved all of these procedures. Figure 2 shows the sequence of developmental steps that were carried out for the Psychedelic Integration Scale.
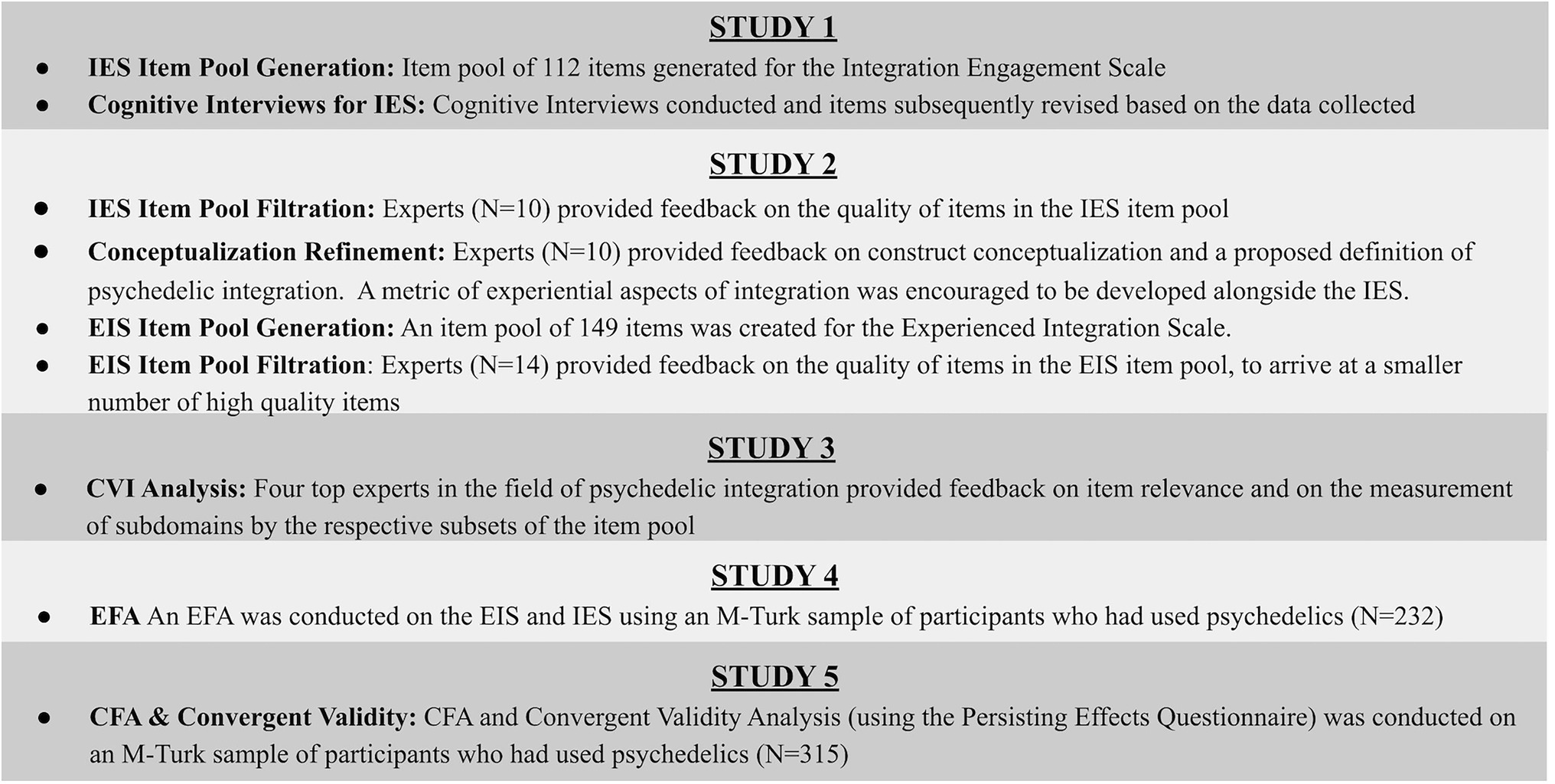
Figure 2. Psychedelic integration scales developmental process outline.
We delineated the subdomains of psychedelic integration based on a survey of the relevant literature, consultation with experts in the field of psychedelics administration and integration, and a factor analysis. In Study 1, we defined the behavioral domain of “Integration Engagement” as consisting of (A) Reflection (contemplative attention given to the experience) and (B) Application (behaviors in daily life resulting from awareness gained through the experience). In Study 2, we defined the intrapersonal domain of “Experienced Integration” as feeling (A) Settled (at peace with the experience) (B) Harmonized (a sense of life alignment with the experience) (C) Improved (experiencing tangible benefits). Below is a description of each of the identified subdomains of psychedelic integration.
Engagement With Integration
Reflection
In the aftermath of acute psychedelic experiences, a period of reflection is generally important for making sense of symbolic, emotional, psychological, and spiritual content, and adjusting to potentially radically different ways of understanding the nature of self and reality (Gandy et al., 2020, p. 9; Timmermann et al., 2021). Through reflection, connections are made between aspects of the psychedelic experience and the individual’s life—such as between sudden insights and their life implications, emotional experiences and their psychological underpinnings, or symbolic visions and their personal significance (Gorman et al., 2021). The reflection process may occur through both individual and interpersonal means.
In guided psychedelic experiences the reflection process is usually actively supported. Participants are often encouraged to retrospectively consider and make connections between the intentions that were set pre-session, what unfolded during the session, and how takeaways from the experience could be implemented and sustained in their daily life (Fadiman, 2011; Bourzat and Hunter, 2019; Gorman et al., 2021). Bourzat and Hunter (2019) states, “it is the guide’s role to notice how the intention relates to the content of an experience, reflect these connections, expand the elements that have emerged, and along with the journeyer, track apparent themes,” (p.180). The reflection process is best supported by guides or therapists who are deeply familiar with the effect of the psychedelic used by the participant, who have an empathetic presence, self-awareness, and integrity, and who can support, rather than directly influence, the reflection process (Mithoefer et al., 2016; Phelps, 2017). When the psychedelic experience is held in a group context, reflection may also be supported through structured and informal sharing between group participants.
In addition to reflection supported by guides or therapists, personal reflection can occur through a variety of individual means, such as journaling, silent contemplation, time in nature, reading books, watching videos, or any other means that help further illuminate the experience (Bourzat and Hunter, 2019). While trained guides or therapists may prompt helpful questions and novel perspectives, periods of solitary reflection are inherently suited to the individual attuning their own internal experience and wisdom (Phelps, 2017).
As a whole, the reflection process may be likened to the formation of an internal map for personal growth (Sloshower et al., 2020). In this analogy, the “map” is created through developing self-awareness, which grows and coalesces in the post-experience reflection stage (spanning topics as diverse as childhood experiences, values, personal health, relationships, metaphysics, etc.; Phelps, 2017; Guss et al., 2020). This analogy builds on Payne et al.’s (2021) proposal that psychedelics can, in many cases, serve as a “Compass” on an individual’s mental health journey, initiating, motivating, and steering the course of personal growth. The compass-like function of a psychedelic experience may be primarily related to the experiential content of the journey—the emotions, epiphanies, symbols, etc. that act as “amplifiers of psychotherapeutic practices and processes,” and set the mind in an aligned direction (Gandy et al., 2020, p. 7). While the raw experience may seem to provide a broad compass-like direction for personal growth, the reflection stage is critical to filling in the details for a well-informed path forward on the life journey. In turn, using this analogy, the “application” process can be likened to taking actual steps on the path.
Application
“Application,” as used in the present research, refers to putting insights gained from a psychedelic experience into action. Application may be expressed through ongoing daily life choices (such as selection of healthy environments, prioritizing supportive relationships, leaving abusive situations, extending forgiveness, expressing gratitude, and spending time in nature), as well as commitment to a range of different intentional practices (such as meditation, yoga, qi-gong, breathwork, exercise, mindful eating, and prayer; Büssing et al., 2005; Kettner et al., 2019; Guss et al., 2020; Gorman et al., 2021).
Staying connected to the unique intentions set for a psychedelic journey is an important starting point for applying the experience to daily life (Haijen et al., 2018). It may be useful to create intention statements for the psychedelic experience that capture personal values and to engage with values-congruent actions in the aftermath of the experience as a means of integration (Guss et al., 2020). For example, when individuals partake in a psychedelic for the purpose of addiction cessation, translating sobriety-related intentions into a range of supportive actions (such as being selective of keeping company with non-using friends) is an important factor predicting successful recovery (Johnson et al., 2017; Nielson et al., 2018). Overarchingly, the principle of having clear personalized intentions, and connecting those intentions to daily life actions is a broadly relevant and encouraged facet of integration (Sloshower et al., 2020).
In addition to cultivating values by staying connected to intentions and making values-aligned life choices, committed practices or exercises can also support integration and personal growth. Depending on the particular intentions of each individual and the unique nature of their experience, the best-suited practices may vary. For example, loving-kindness meditation may be particularly suited to an individual who has the intention to be more loving, while a practice like dance may be suited to an individual who has the intention to be more embodied and expressive.
Though a variety of practices may be supportive of integration, mindfulness practice has particularly strong empirical support as a beneficial form of psychedelic integration engagement (Sampedro et al., 2017; Griffiths et al., 2018; Walsh and Thiessen, 2018; Smigielski et al., 2019; Heuschkel and Kuypers, 2020; Payne et al., 2021; Radakovic et al., 2021). While Payne et al. (2021) liken psychedelic experiences to a compass for personal growth, they describe mindfulness practice as a vehicle for growth. For the purpose of the current research, we might liken the broad idea of a vehicle for growth to the more general concept of application, with mindfulness practice being a particularly well-built vehicle. Payne et al. identify mindfulness as being particularly effective because of its proficiency in helping to deepen and generalize insights, defuse maladaptive thoughts and behaviors, revitalize values and commitments, and maintain present-mindedness. Generally, each of these aspects of mindfulness practice is helpful in promoting psychedelic integration, regardless of the particular intentions of the individual.
Experienced Integration
Feeling Settled
The dramatic changes in consciousness produced by a psychedelic can be accompanied by the surfacing of repressed psychological content, intensified emotions (fear, confusion, paranoia, awe, gratitude, joy, etc), sudden changes in core beliefs, ego death or ego inflation, unprecedented stillness or invigorated motivation, and other amplified emotional and behavioral changes (Carhart-Harris, 2013; Ortigo and Richards, 2021; Timmermann et al., 2021). The dissipation of emotional extremes and return to internal stability and a feeling of settledness naturally tends to occur as the acute effects of a psychedelic subside, though in some cases imbalances may persist (Carhart-Harris and Friston, 2019). The stabilization of potential emotional imbalances or disturbances is an internal indicator of successful integration.
Intrapsychic imbalances can occur following both extreme negative or positive experiences. On the negative end of the spectrum, Barrett et al. (2016) identified seven dimensions characteristic of so-called “bad trips”: fear, grief, death, insanity, isolation, physical distress, and paranoia. When internal resistance is applied to strong negative emotions the unpleasant state often continues, as captured by the maxim “what you resist persists” (Hayes, 2005; Guss et al., 2020). On the other hand, by constructing a narrative which makes sense of challenging experiences, the accompanying emotions tend to resolve more quickly, and the experience takes on a sense of meaning (Dyck and Elcock, 2020; Gashi et al., 2021).
With euphoric or transcendent experiences, the risk of poor integration may pertain to imbalances in ego-centrism (Anderson et al., 2020). Ortigo and Richards (2021, p. 237) note that “A sense of grandiosity and overconfidence may be a temporary side effect of especially profound and sudden apotheosis,” and caution users about the potential to be “The person who after his first powerful journey, suddenly proclaims themselves to be a messiah or a “shaman”. Achieving settledness in regards to potentially ego-inflating experiences involves accessing a sense of humility (Ortigo and Richards, 2021).
Feeling Harmonized
In a broad sense, integration refers to the process of uniting different things. The successful uniting of different states of consciousness is of particular importance in regards to psychedelics use because of the radically non-ordinary states they can occasion, and the consequent change in personal belief structures that may result (Lebedev et al., 2016). The magnitude of change in consciousness is evidenced by brain scan studies of individuals under the influence of psychedelics (Dos Santos et al., 2016; Preller et al., 2019). According to Carhart-Harris’ Relaxed Beliefs Under Psychedelics Model, these changes in brain states tend to increase entropy and decrease the rigidity of beliefs, paving the way for change in belief structures (Carhart-Harris and Friston, 2019).
The beliefs that may flex as a result of psychedelics can be as fundamental as beliefs about the core nature of reality, beliefs upon which many other facets of life rest (Timmermann et al., 2021). Change in such beliefs can initially be jarring—though may also open individuals to unconsidered potentials (Shipley, 2021). The successful formation of novel intrapsychic connections has been postulated to be a core factor underlying positive mental health change following psychedelics use (Siegel, 2009; Carhart-Harris et al., 2018). As a whole, “feeling harmonized” is a sign that an individual has successfully engaged psychological flexibility in the integration process and aligned internal shifts with external behaviors (Sloshower et al., 2020).
Feeling Improved
The experience of improvements in wellbeing is inherent to successful integration. Yet psychedelic experiences often entail initial discomfort during the session and integration phase before improvements are felt (Gorman et al., 2021). This may be because of the tendency for psychedelics to elicit the surfacing of repressed content related to the root causes of psychological ill-being (Sloshower, 2018). In general, avoidance, minimization, dismissal, or psychological distancing are common strategies used to temporarily reduce or manage discomfort and are often maladaptive. As delineated in the ACT framework, sustained avoidance eventually contributes to worsening psychological tension, as the root causes of the tension remain unresolved (Kangas and McDonald, 2009; Payne et al., 2021). Such strategies of avoidance are associated with psychological rigidity, which in turn is associated with ill-being (Morris and Mansell, 2018). When psychedelics induce a state in which an individual is unavoidably confronted with the causes of their ill-being, it minimizes the potential for sustained avoidance. If resistance to the repressed content persists, the experience may become increasingly challenging, and the resolution of root causes delayed. On the other hand, adopting the psychological flexibility to confront such content, despite discomfort or unfamiliarity, and contextualize its meaning within one’s life is indicative of integration (Carbonaro et al., 2016; Gashi et al., 2021). The eventual result of such integration is the resolution of the causes previously underlying ill-being and the experience of improved wellbeing.
Psychedelic experiences can also be predominantly enjoyable, with positive feelings pervading most or all of the experience. When it comes to pleasant experiences, successful integration may entail sustaining a connection to that experience, and the qualities underlying the positive emotions (Guss et al., 2020). For example, if universal love is felt strongly during a psychedelic experience, the integration of that experience could involve identifying what was associated with the feeling (perhaps forgiveness, cosmic unity, or inner stillness), and finding ways to connect to those components in daily life.
Notable shifts in personality induced by psychedelics may also lead to various forms of felt life improvement. Findings suggest that psychedelics use can lead to increased openness (MacLean et al., 2011; Erritzoe et al., 2018). Erritzoe et al. (2018) identified two types of openness, both influenced by psychedelic experiences. First, openness to actions, which pertains to not being set in one’s way and willing to try and do new things. Second, openness to values, which involves embodying qualities, such as permissiveness, open-mindedness, and tolerance. Both facets of openness are components of psychological flexibility, which is strongly associated with psychological wellbeing (Wersebe et al., 2018).
The acute post-experience period of improved wellbeing that can follow after a psychedelic experience is often referred to as the “psychedelic afterglow” (Sampedro et al., 2017). The “afterglow” has been described in various ways; “I felt free, carefree, re-energized” (Watts et al., 2017); “The concrete coat had come off” (Watts et al., 2017); “All that day and well into the next, a high pressure system of wellbeing dominated my psychological weather” (Pollan, 2018, p. 254). In some cases, elevated afterglow states can be the result of having addressed and processed difficult unconscious blocks and emotions previously too uncomfortable to approach. The afterglow period has been suggested to offer a window of increased therapeutic potential, in which open and vulnerable reflection is readily available and positive changes can be reified (Murphy-Beiner and Soar, 2020). The occurrence of peak experiences under psychedelics is predictive of long-term positive changes in psychological wellbeing (Roseman et al., 2018). Particular long-term improvements documented include increases in positive mood, prosocial behaviors, empathy, cognitive flexibility, creativity, value alignment, nature-relatedness, spirituality, self-transcendence, and enhanced mindfulness (Griffiths et al., 2006, 2008, 2011, 2016, 2018; Elsey, 2017; Carhart-Harris et al., 2018; Carhart-Harris and Friston, 2019; Kettner et al., 2019; Luoma et al., 2020; Payne et al., 2021). The reification of change through integration practice can transform the afterglow from a fleeting state to a lasting change. Whether through sustaining connection to an already positive state or through growing from facing a challenge, improved wellbeing is a characteristic of openly and mindfully integrating all facets of the psychedelic experience into life (Siegel, 2016, p. 127).
Study 1
In this study, we identified subdomains and created a list of indicators and sub-indicators for the IES, based on a literature review, preliminary consultations with researchers and clinicians with expertise on psychedelic experiences, and on perusal of personal accounts and case studies of psychedelic integration. We then generated a pool of 112 items for the IES based on the sub-indicators. We subsequently conducted cognitive interviews with a convenience sample of individuals known to have had psychedelic experiences, with the aim of verifying which items were interpreted in a manner congruent with the intent of the question, as well as discovering any potential problems with item wording. At the time of study one, the authors had not yet intended to create a second scale measuring the experiential aspect of psychedelic integration. As such, cognitive interviewing feedback was only gathered for the IES item pool.
The following indicators and sub-indicators were used as a basis for the generation of the item pool for the Psychedelic Integration Scales (Figure 3).
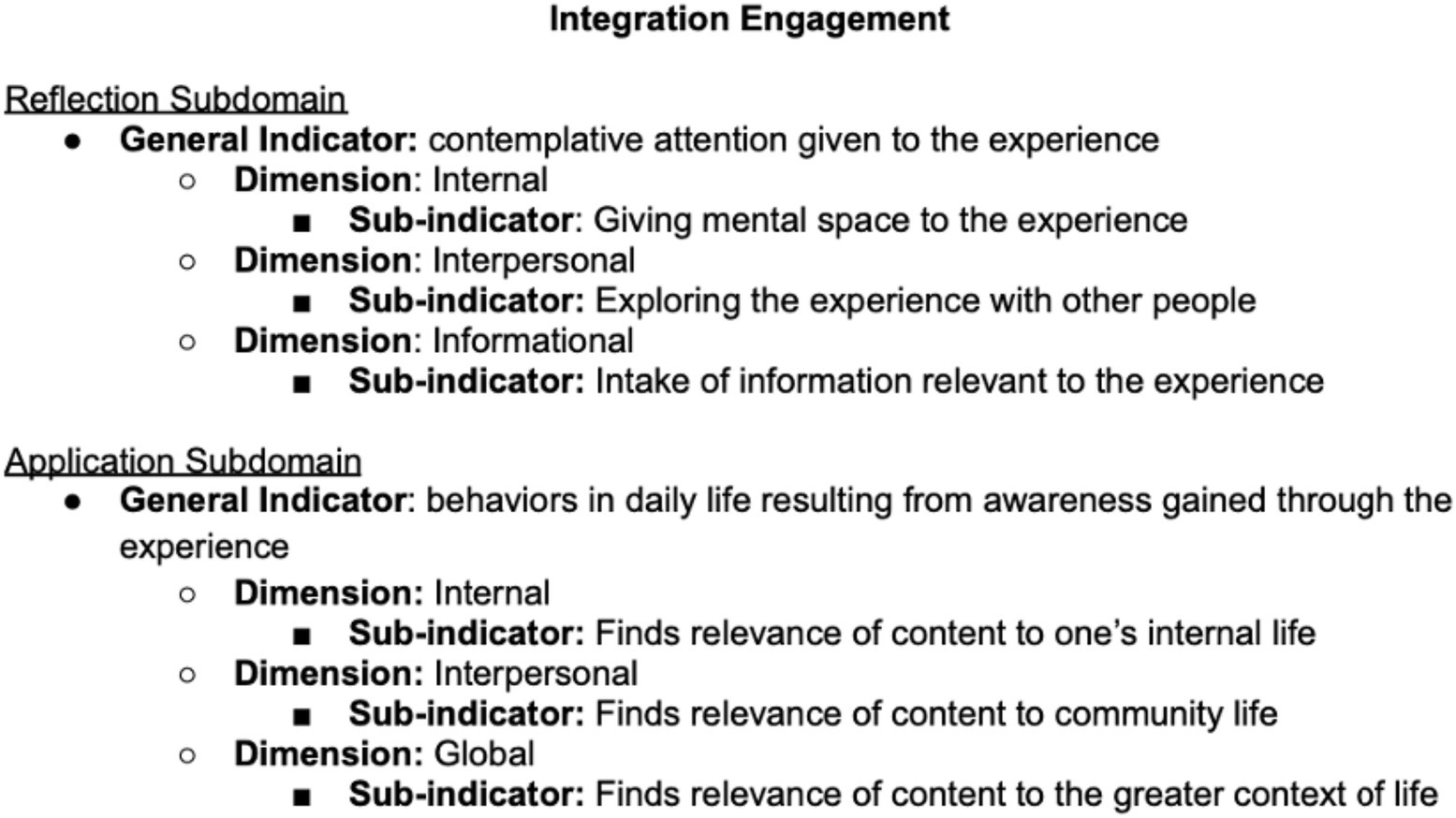
Figure 3. Subdomains, indicators, and sub-indicators for the integration engagement scale (IES).
Participants
A convenience sample of participants known by the authors who’d had psychedelic experiences was recruited either in-person or via a phone call (N = 13). Participants were adults between the ages of 27 and 58, drawn from the US and were predominantly White (92.3%, n = 12; Brazilian 7.7%, n = 1), educated (all were high school-educated, and 84.6%, n = 11 had bachelor degree or higher), and male (Male = 69.3%, n = 9; Female = 30.7%, N = 4).
Method
Participants were read the scale instructions and told, “Please describe your thought process when responding to the items.” Participants were encouraged to provide more information about relevant aspects of their thought process, using the prompt, “Can you please say more about that?” Responses were transcribed for later analysis.
Results
Items were judged and then revised based on the qualitative feedback. 56 revisions were made to the pool of 112 items. Sample changes are listed below (Table 1).
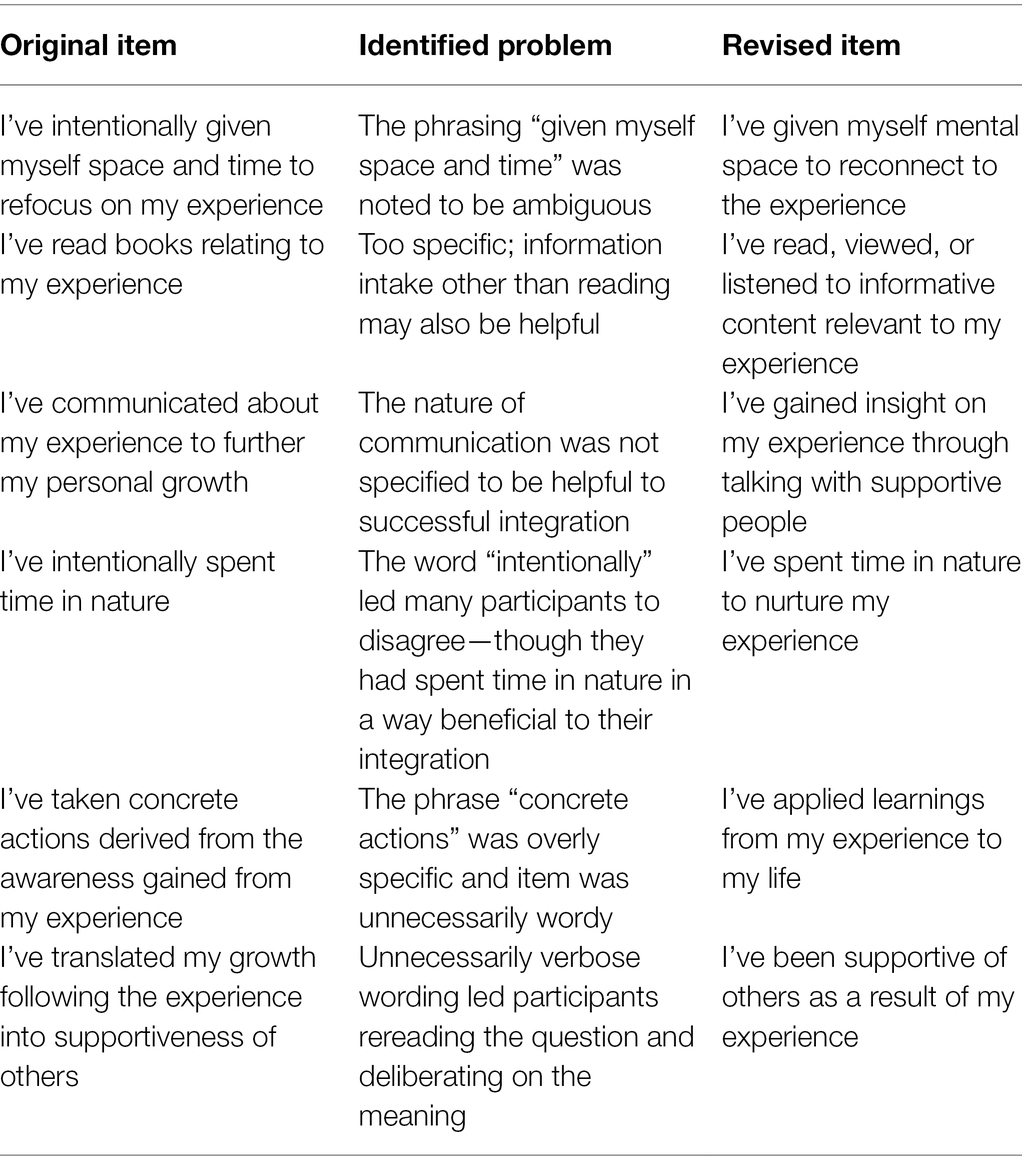
Table 1. Item revisions to IES scale items based on cognitive interviewing feedback.
Discussion
Revisions were made to items that were identified as vague or poetic, to phrasings with interpretations that differed highly between participants, to double-barrelled items, to items that very few individuals agreed with because of a qualifying word, and to items that did not reflect the indicators which they were intended to measure.
Study 2
In this study, we requested feedback on a proposed definition of psychedelic integration, and administered items to researchers and clinicians with expertise in psychedelic experiences (N = 10). Our aim was to improve upon the proposed definition and conceptualization and to arrive at a smaller number of high-quality items to increase construct validity and reduce participant burden. Experts gave feedback on the Integration Engagement Scale items, and also encouraged the construction of a tool to measure the experiential aspects of psychedelic integration. We subsequently identified subdomains and created a list of indicators and sub-indicators for the EIS, based on a literature review, preliminary consultations with researchers and clinicians with expertise on psychedelic experiences, and on perusal of personal accounts and case studies of psychedelic integration. We then created a new item pool of 149 items, which served as the basis of the Experienced Psychedelic Integration Scale (EU = IS). We then reached out to the same set of experts, as well as four additional experts, for feedback on item quality of the newly generated EIS items (N = 14; Figure 4).
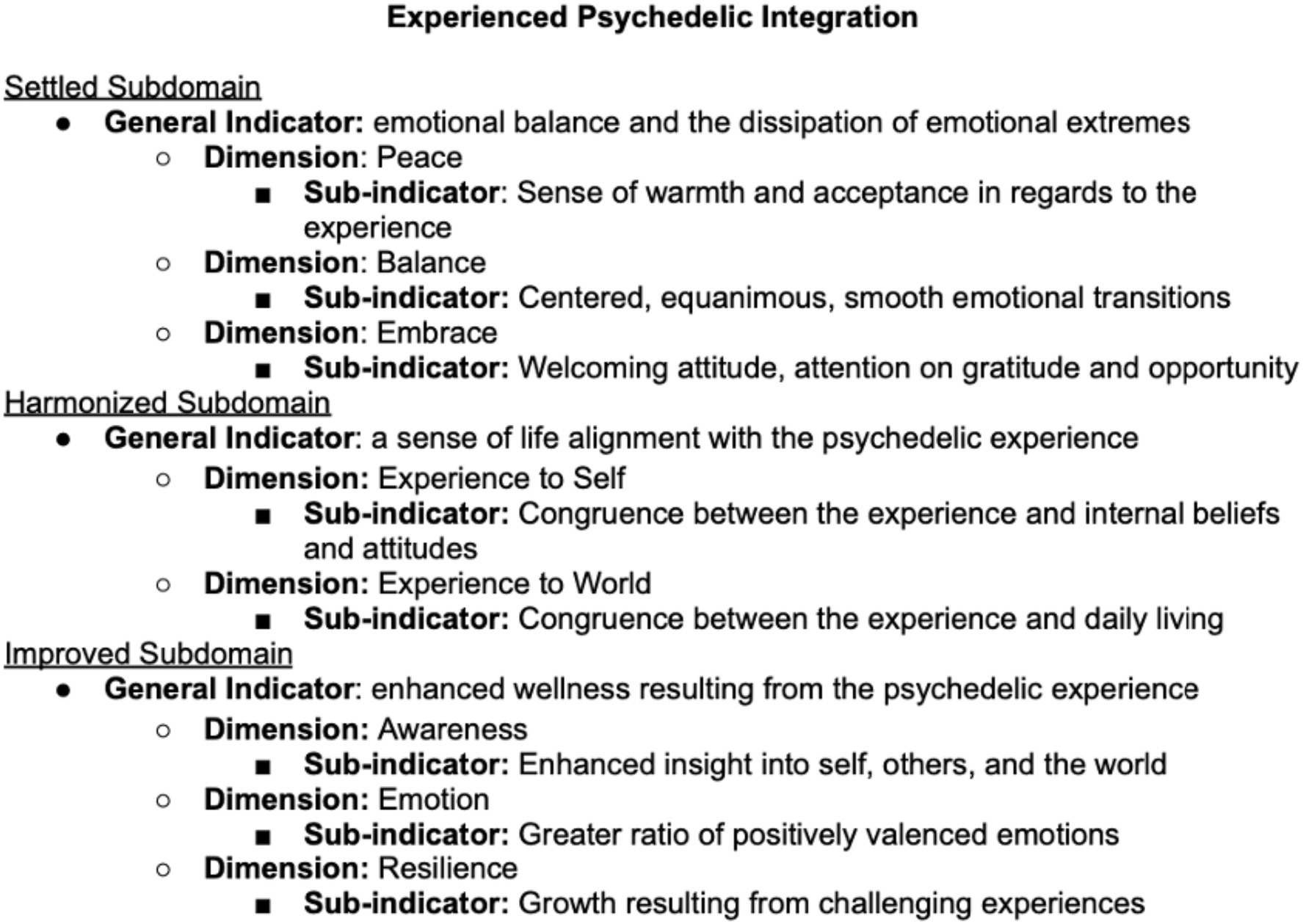
Figure 4. Subdomains, indicators, and sub-indicators for the experience of integration scale (EIS).
Participants
We recruited researchers and clinicians with expertise on psychedelic integration, reaching out to authors who had published in the field, as well as specialists at psychedelic treatment centers (N = 13). Participants were recruited via an email message, inviting them to participate in the study.
Method
Feedback on definition quality was indicated on a four-point Likert scale, with anchors “Way off,” “Near target,” “On target,” and “Exactly on target,” as well as via an open-ended response requesting written feedback on the definition. Feedback on item quality was indicated on a nine-point scale, with anchors “Worthless item,” “Nearly worthless item,” “Very poor item,” “Poor item,” “Mediocre item,” “Good item,” “Great item,” “Excellent item,” and “Perfect item.” Experts were given the instructions “Please indicate whether the following statements is overall a good item to include in the psychedelic integration scale (taking into account the IMPORTANCE, CLARITY, and CONCISENESS of each item). IMPORTANCE: how significant is the aspect of integration captured by this item. CLARITY: how interpretable is this item by a wide range of audiences. CONCISENESS: how succinctly an item is worded.” Items were presented in a single undivided item pool (so that quality could be assessed relative to the overall construct).
Results
The definition of psychedelic integration originally proposed was “The intentional application of psychedelic derived awareness into daily life.” Assessment of definition quality indicated an average definition rating of 2.70, falling in between the anchors “Near Target” and “On Target.” Assessment of item quality of the IES item pool indicated an overall average item quality score of 6.80, falling in between the anchors “Good item” and “Great item.” Assessment of item quality of the EIS item pool indicated an overall average item quality score of 7.24, falling in between the anchors “Great item” and “Excellent item.”
Discussion
Qualitative feedback regarding the proposed definition of psychedelic integration included encouragements to emphasize: (1) that integration is a process; (2) that intentionality may be a part of the process, but is not a necessary component of all aspects of integration; (3) that the term “application” suggests an overly external view of integration; and (4) that helpful change is inherent to the occurrence of integration. Considerations of the feedback led to the revised definition of psychedelic integration proposed: “The process by which a psychedelic experience translates into positive changes in daily life.”
31 items of the IES item pool had average item quality scores above seven—the anchor corresponding to “Great item.” These items were retained for further analysis. 101 items of the EIS item pool had average item quality scores above seven and were retained for further analysis. Of the 101 items, those that measured the same sub-indicator as another remaining item but had inferior item quality were then eliminated, leaving 31 items in the EIS item pool.
Study 3
In this study, four top experts in the psychedelic integration field were recruited to provide feedback on the remaining 31 items of the IES item pool and 31 items of the EIS item pool for a content validity index (CVI) assessment. They assessed item relevance, as well as the representativeness of the subsets of the item pool to the measurement of their respective subdomains (Reflection, Application, Settled, Harmonized, and Improved).
Participants
Top experts in the field of psychedelic integration were recruited through email requests. Experts consisted of a clinician at Johns Hopkins University, a researcher at New York University, an author who published a book on psychedelic integration, and a psychiatrist at Bristol University.
Methods
The relevance of each item to the measurement of psychedelic integration was assessed on a four-point scale, with the anchors “Not relevant,” “Somewhat relevant,” “Quite relevant,” and “Highly relevant.” Item CVI (I-CVI) scores were computed as the number of experts giving the item a 3 or a 4 divided by the total number of experts (Zamanzadeh et al., 2015). The scale CVI (S-CVI) was computed as the overall average of the I-CVI scores for each scale (Zamanzadeh et al., 2015). Representativeness of the collective pool of items measuring each subdomain was measured on a four-point scale with anchors of “Not representative,” “Somewhat representative,” “Quite representative,” “Highly representative.” A subdomain representativeness index was computed as the number of experts giving the item pool a 3 or a 4, divided by the total number of experts. The scale representativeness index was computed as the average of the subdomain representativeness index scores.
Results
The final IES demonstrated an S-CVI of 0.96 and a representativeness index of 1.0. The final EIS demonstrated an S-CVI of 0.92 and a representativeness index of 1.0 (Tables 2–5).
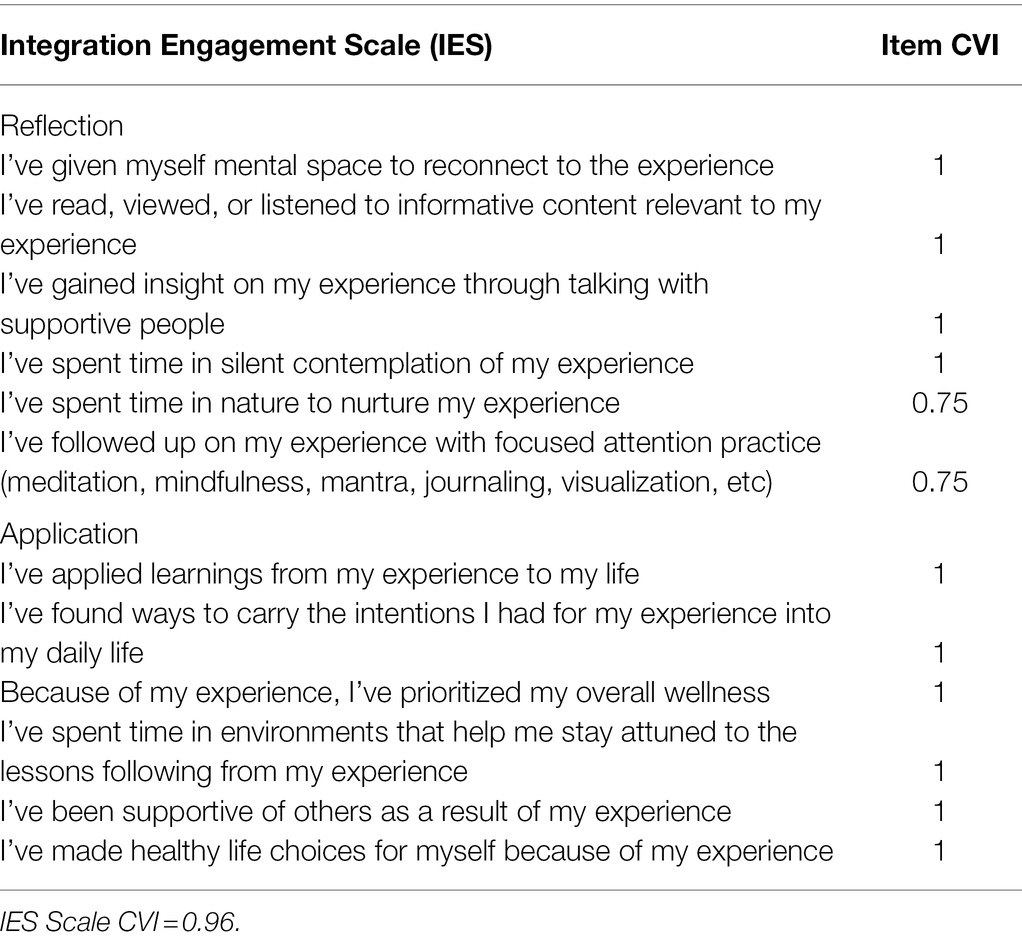
Table 2. Integration engagement scale CVI results for final scale items.
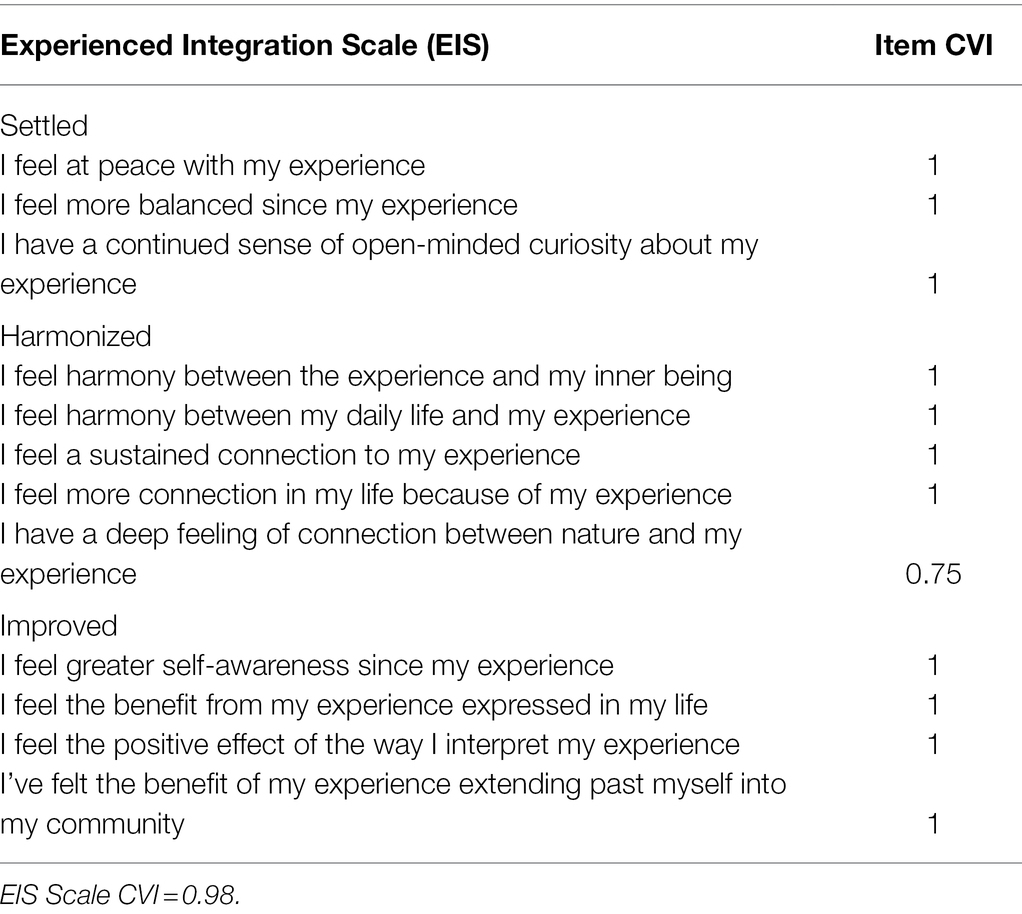
Table 3. Experienced integration scale CVI results.
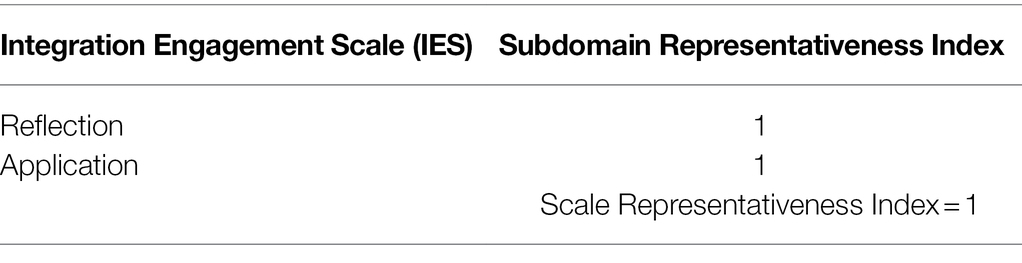
Table 4. Integration engagement scale representativeness index.
Table 5. Experienced integration scale representativeness index.
CVI scores for items that were not retained, along with the reason for their elimination, are listed in Study 4, Table 6.
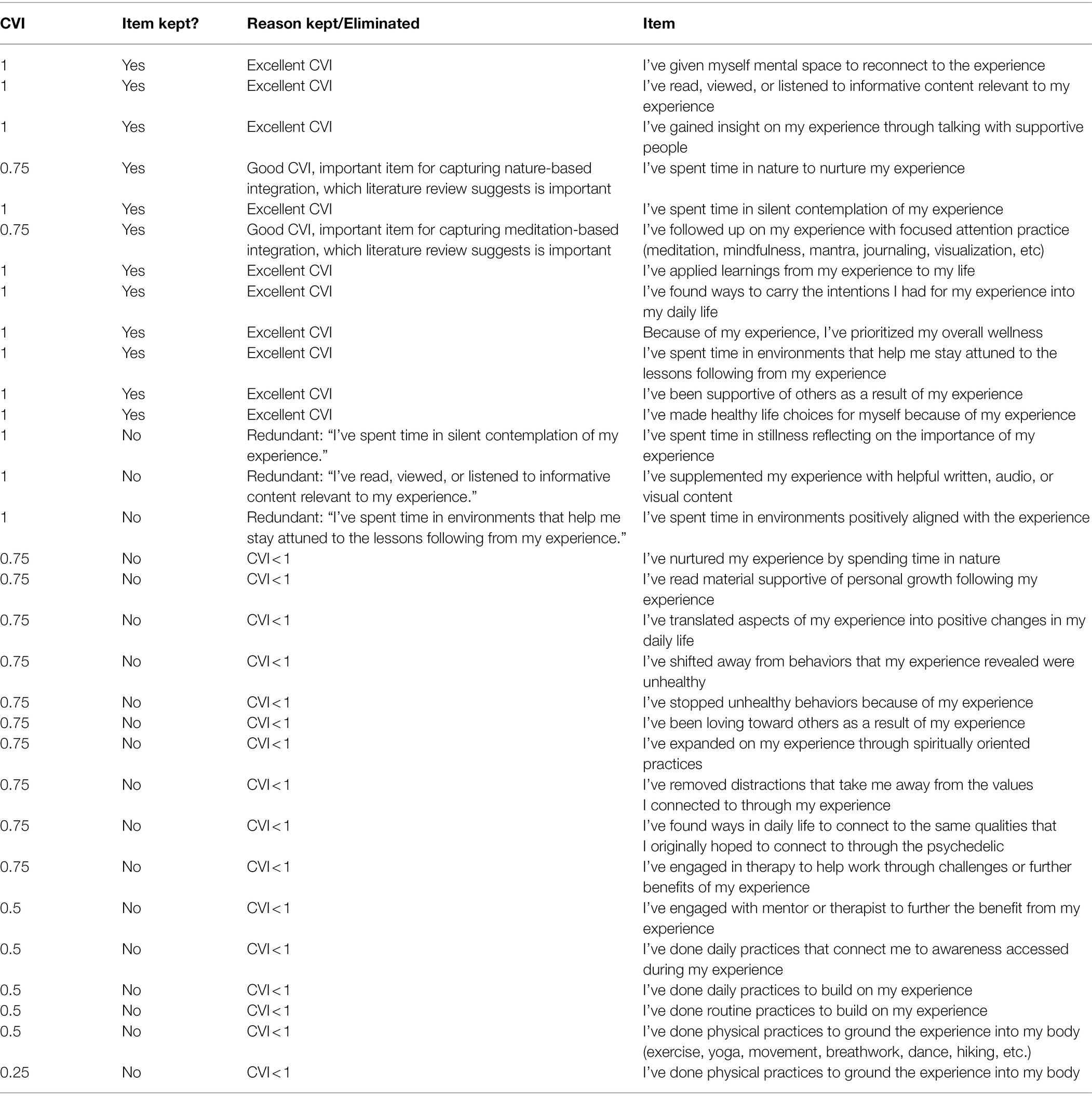
Table 6. Item filtration for the integration engagement scale item pool.
Discussion
Overall, the item and scale CVI scores and the representativeness indexes are excellent. The representativeness index of 1.0 for both scales evidenced that experts were in complete agreement that the set of items capturing each subdomain was highly representative of the subdomain intended to be measured. The content validity index scores indicate that experts were in nearly complete agreement that each of the final items was highly relevant to the measurement of psychedelic integration, with the exception of three items that were rated as “somewhat relevant” by a single expert. Two of those items had to do with nature-based integration, and the third with applied practices. The three lower ratings may have been a reflection of that particular expert’s opinion on the wording of those items, or a lesser priority given to nature-based integration and particular forms of applied integration practice.
Study 4
In this study, we administered the same 31 items from the IES and 31 items from the EIS item used in the CVI analysis to a sample from the normal population who indicated that they had taken psychedelics. We performed exploratory factor analysis and established initial reliability estimates.
Participants
Participants (N = 232) were adults (over 18) drawn from the US and were mostly White (79.7%, n = 185; Black 11.2%, n = 26; Asian 7.7%, n = 18), educated (all but one were at least high school-educated; 59.1%, n = 137 had bachelor degree or higher), and balanced between females and males (Male = 53.4%, n = 124; Female = 46.6%, 108).
Method
We collected a sample from M-Turk (an online platform hosted by Amazon Web Services which connects a paid population of respondents with research surveys), using the following language (“Questionnaire for Those Who’ve Had a Psychedelic Experience”). In order to be eligible, our sample of participants needed to have used psychedelics at least once, which was assessed with the question, “Have you ever used a psychedelic substance?” After deleting participants who had not used a psychedelic substance or who failed the attention check (N = 129), our final sample was 232. Participants agreed to an informed consent document and confirmed that they were over 18 years of age. Participants were compensated about one dollar for their participation. The survey was administered using Qualtrics, a secure online survey distribution and data collection program.
Participants were asked to consider their most recent psychedelic experience. Specifically, the instructions read: “The following statements have to do with the follow-up to your most recent psychedelic experience. Please indicate the level to which you agree with each statement—considering only the time period since your most recent psychedelic experience. There are no right or wrong answers. Answer as honestly as possible.” Participants were asked specifically to answer regarding the most recent psychedelic experience they had had. Each item was rated on a 7-point scale (1 = Strongly Disagree, 2 = Moderately Disagree, 3 = Somewhat Disagree, 4 = Neutral, 5 = Somewhat Agree, 6 = Moderately Agree, 7 = Strongly Agree).
Participants responded to 31 items from the IES item pool and 31 items from the EIS item pool. The goal was to create a brief scale suited to clinical use. To arrive at a succinct scale with high-quality items, only items with I-CVI scores of 1 were selected from the item pool to be used in the final EFA, with the exceptions of an IES item relating to nature-based integration practice, an IES item relating to focused awareness practices, and an EIS item relating to nature-related integration experience. These items had I-CVI scores of 0.75 but were included in the EFA analysis because they were the only items left in the item pools that captured statements relating to meditation and nature-based integration, both of which were identified in the literature review as particularly important forms of integration engagement. After filtering out items with I-CVI scores below 0.75, items that had CVI scores of 1 but were deemed by the authors to be overly redundant were dropped. The list of the items that were dropped and retained is described in Tables 6 and 7. After item filtration, 12 items remained for both the IES and EIS.
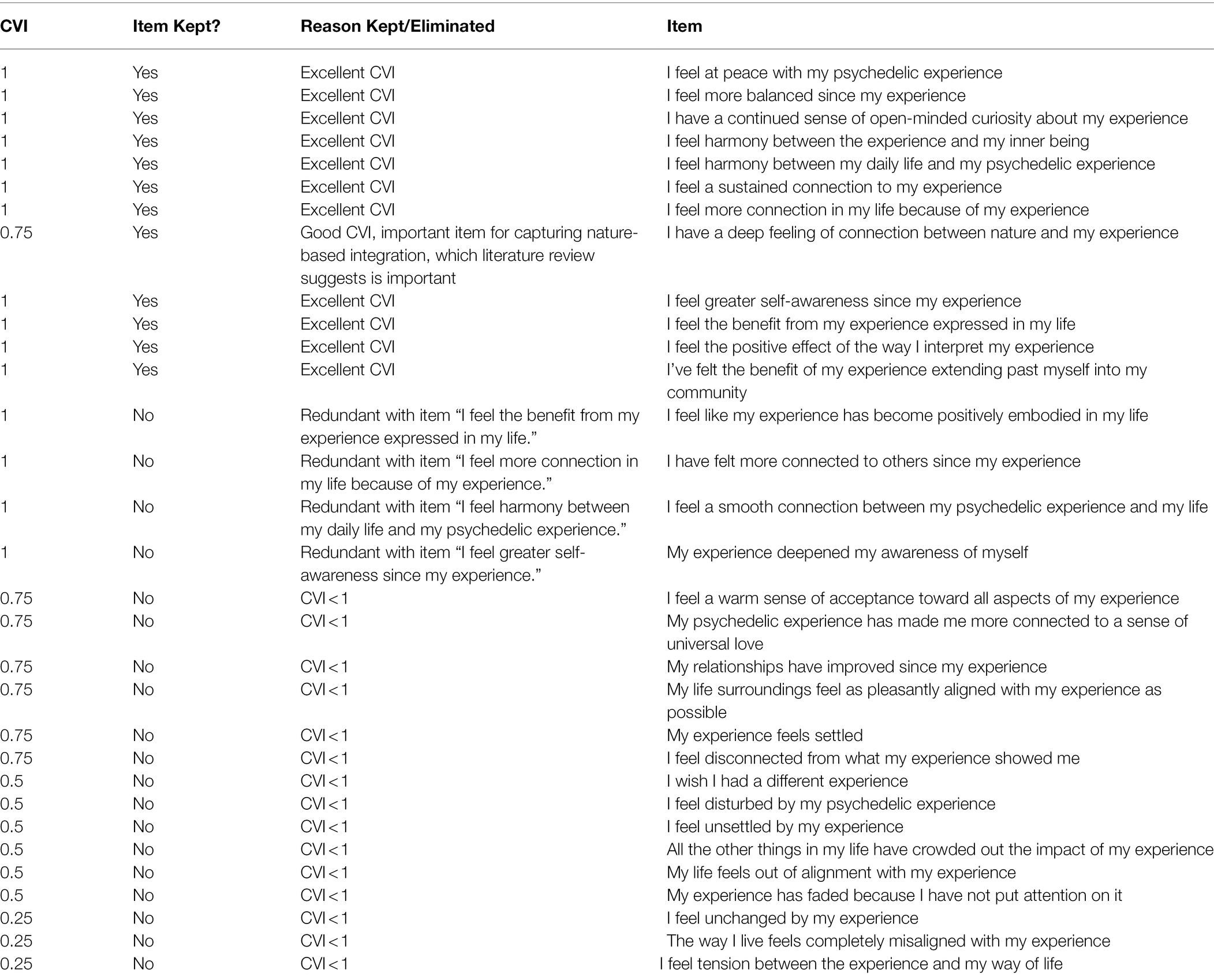
Table 7. Item filtration for the experienced integration scale item pool.
An EFA was run on these items via an M-Turk sample, filtering for only individuals who responded “yes” to the prompting question “Have you ever had a psychedelic experience?” (N = 232). Factor solutions were generated using SPSS with a Promax rotation. The oblique promax rotation method was chosen due to the assumption that factors would significantly positively correlate with one another. Parallel Analysis (PA; Horn, 1965), Minimum Average Partialing (MAP; Velicer, 1976), and Scree tests (Cattell, 1966) were used in order to estimate the number of factors, and standards of stability and reliability were applied to drop error factors, and arrive at an adequate factor solution.
Results
12 items each remained for both the IES and EIS. Promax rotation of the IES revealed a single-factor model. Scree plots, parallel analysis, and Minimum Average Partialing also pointed to a single-factor model. Promax rotation of the EIS revealed a two-factor model, with the second factor consisting of a single item with a factor loading of above 0.8, “I feel at peace with my experience.” However, Parallel Analysis and Minimum Average Partialing supported a single-factor solution for the EIS. As such, the final Promax rotation was run with the constraint to produce a single-factor solution.
For the IES, a single factor emerged, which accounted for 50.87 percent of the total variance (KMO = 0.932, Bartlett’s sig 0.000). For the EIS, a single factor emerged, which accounted for 56.13% of the total variance (KMO = 0.947, Bartlett’s sig 0.000).
Factor loadings were good (Tables 1 and 2), as all were between 0.6 and 0.8, with the exception of two items from the EIS, which were high (0.817 and 0.814). However, these two items describe two distinct aspects of positive feeling: “I feel the positive effect of the way I interpret my experience” represents the internal expression of positivity, while “I feel the benefit from my experience expressed in my life” represents its external expression (Tables 8 and 9).
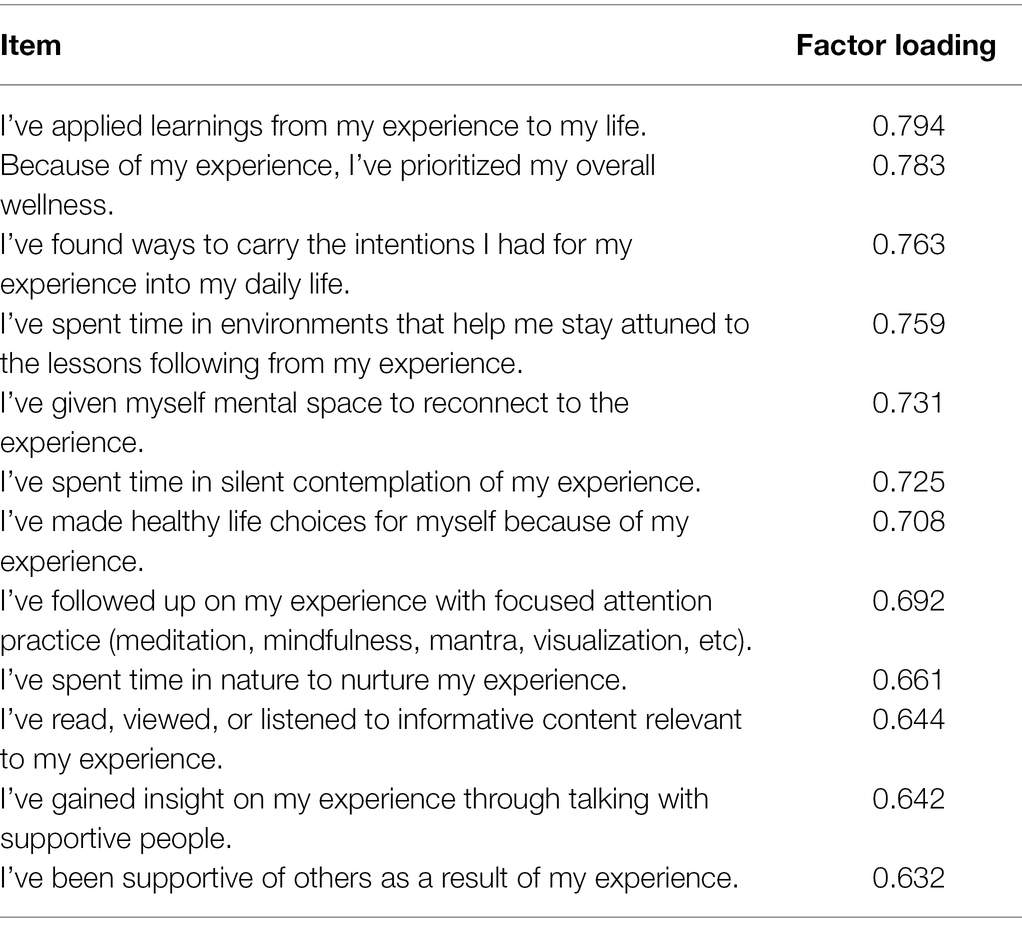
Table 8. EFA component matrix for the integration engagement scale.
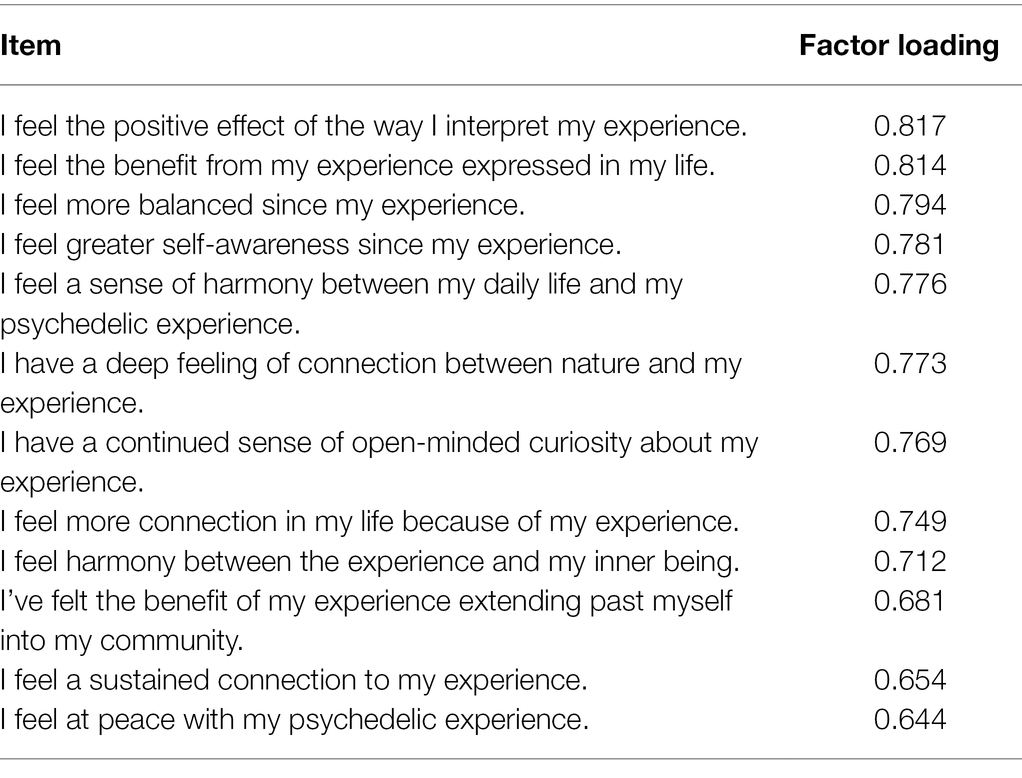
Table 9. EFA component matrix for the experienced integration scale.
Cronbach’s alpha for the Integration Engagement Scale was 0.90, and Cronbach’s alpha for the Experienced Integration Scale was 0.92.
Discussion
Due to an intention to make the scale succinct and practical for use in applied settings, a high constraint was put on redundancy and quality of items. This constraint was likely accountable for the single-factor solution we found in our analysis. Within the single-factor solution of our final scales, the items demonstrated factor scores indicating that each item was pertinent to measurement of the construct, and not overly redundant. Cronbach’s alpha scores demonstrated excellent internal consistency for both scales.
Study 5
In this study, we administered the IES and the EIS to N = 600 participants who reported having had a psychedelic experience in order to assess the convergent and divergent validity of these measures, as well as to conduct confirmatory factor analysis (CFA) to follow up on the results of Study 4’s exploratory factor analysis, which suggested single-factor structures for both the IES and the EIS. We also aimed to assess the convergent validity of the IES and EIS as measures of integration, namely, by measuring their correlation with a 6-item subset of the Persisting Effects Questionnaire (PEQ), an instrument devised by Griffiths et al. (2006) to study the long-term effects of psilocybin. Convergent validity analysis demonstrated strong positive associations with the PEQ item subset, MEQ item subset, and Awe Scale. Divergent validity was supported by a medium correlation with the Satisfaction with Life Scale. Discriminant validity was assessed by comparing the correlation between the EIS and IES and the square root of the AVE. The high correlation between the scales relative to the square root of the AVE did not indicate discriminant validity between the scales.
Participants
We collected a sample from M-Turk, under a survey titled Questionnaire for Those Who’ve Had a Psychedelic Experience. Our sample of participants needed to have used psychedelics, which was assessed with the question “Have you ever used a psychedelic substance?” After deleting participants who had not used a psychedelic substance, who failed the attention check, or who wrote incoherent responses to a verbal prompt, our final sample included 315 individuals. Participants agreed to an informed consent document and confirmed that they were over 18 years of age. Participants were compensated $1.25 for their participation. The survey was administered using Qualtrics, a secure online survey distribution and data collection program. The Institutional Review Board at Pacifica Graduate Institute approved this study.
Participants (N = 315) were adults (over 18) drawn from the US and were mostly White (80.6%, n = 254; Black 12.7%, n = 40; Asian 4.4%, n = 14), educated (all were at least high school-educated; 70.5%, n = 229 had bachelor degree or higher), and broadly balanced between males and females (Male = 58.4%, n = 184; Female = 41.6%, n = 131). Participants were asked which psychedelic they had most recently used. The majority had most recently used mushrooms (50.2%, n = 158), followed by LSD (20.8%, n = 66), MDMA (9.0%, n = 28), DMT (9.0%, n = 28), Ketamine (2.8%, n = 9), Ayahuasca (7.0%, n = 22), Other (0.6%, n = 2), and Iboga (0.4%, n = 1). Participants responded to a prompt asking when their most recent psychedelic experience had been, using anchors of 1 = “In the past week,” (23.2%, n = 73), 2 = “In the past month” (35.6%, n = 112), 3 = “In the past year,” (22.9%, n = 72), 4 = “in the past 5 years” (7.6%, n = 24), and 5 = “More than 5 years ago” (10.8%, n = 34).
Methods
To separately test the fit of the 12-item 1-factor models for the IES and the EIS respectively, we used SPSS AMOS structural equation modeling software to compute model chi-square, Comparative Fit Index (CFI), and Root Mean-Square Error of Approximation (RMSEA), all indices of model fit.
Given that a 1-factor model is the simplest CFA model, and serves as the null hypothesis or comparator in factor analyses involving multiple proposed factors, our 1-factor CFAs of the IES and EIS did not require the use of a comparator.
Convergent and divergent validity correlations were assessed between the IES and EIS and items from the PEQ, MEQ, Awe Scale, and Life Satisfaction Scale (Diener et al., 1985; Griffiths et al., 2006; Yaden et al., 2019). To reduce participant burden a subset of items of the PEQ and MEQ were used, rather than the full scales. Six items of the PEQ were selected a priori, each from a different domain of the scale, chosen by the authors as items that would at face value be relevant to the measurement of convergent validity. The six items of the PEQ chosen included “Your appreciation for life has increased,” “You feel more personal integration,” “You now feel more love and openheartedness,” “You have a more positive relationship with others,” “Your behavior has changed in ways you would consider positive since the experience,” and “Spirituality has become a more central part of your life.” Similarly, eight Items of the MEQ were chosen by the authors. These items included “Feeling that you experienced something profoundly sacred and holy,” “Experience of unity with ultimate reality,” “Experience of amazement,” “Feelings of joy,” “Experience of timelessness,” “Being in a realm with no space boundaries,” “Sense that the experience cannot be described adequately in words,” and “Feeling that you could not do justice to your experience by describing it in words.” These items were derived from the MEQ domains of Positive Mood, Sense of Sacredness, Internal Unity, Transcendence of Time and Space, and Ineffability and Paradoxicality. The shortened AWE-S was used, which includes the items “I sensed things momentarily slow down,” “I felt that my sense of self was diminished,” “I had the sense of being connected to everything,” “I felt that I was in the presence of something grand,” “I felt my jaw drop,” and “I felt challenged to mentally process what I was experiencing.”
To assess divergent validity the five-item Satisfaction with Life Scale was used, which includes the items “In most ways my life is close to my ideal,” “The conditions of my life are excellent,” “I am satisfied with life,” “So far I have gotten the important things I want in life,” and “If I could live my life over, I would change almost nothing.”
Results
For the IES, CFI was good (0.969) and RMSEA was good (0.032), with 90% confidence intervals of 0 and 0.05. In addition, the chi-square value obtained (71.0) was less than twice the degrees of freedom (54) of the model, further evidence of good fit. Overall, the 1-factor model of the IES demonstrated robust and superior fit.
For the EIS, CFI was good (0.958) and RMSEA was good (0.037), with 90% confidence intervals of 0.014 and 0.054. In addition, the chi-square value obtained (76.7) was less than twice the degrees of freedom (54) of the model, further evidence of good fit. Therefore, the 1-factor model of the EIS demonstrated robust and superior fit.
Moreover, a strong positive association was demonstrated between the PEQ item subset and both the IES (r = 0.76, p < 0.001) and the EIS (r = 0.73, p < 0.001), between the MEQ item subset and both the IES (r = 0.65, p < 0.001) and the EIS (r = 0.73, p < 0.001), and between the AWE-S and both the IES (r = 0.66, p < 0.001) and the EIS (r = 0.70, p < 0.001), indicating robust convergent validity. Divergent validity was demonstrated by correlations between the Satisfaction with Life Scale and the IES (r = 0.47, p < 0.001) and the EIS (r = 0.42, p < 0.001).
The correlation between the two scales was 0.83 (p < 0.001). The average variance extracted (AVE) for the IES was 0.51, and the square root of the AVE for the IES was 0.71. The AVE for the EIS was 0.56, and the square root of the AVE for the EIS was 0.75 (Tables 10–14).
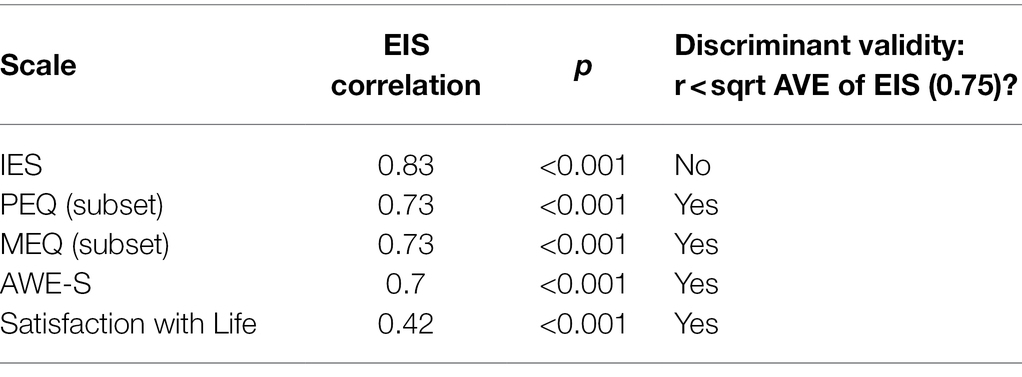
Table 10. Correlation matrix of EIS with related scales.
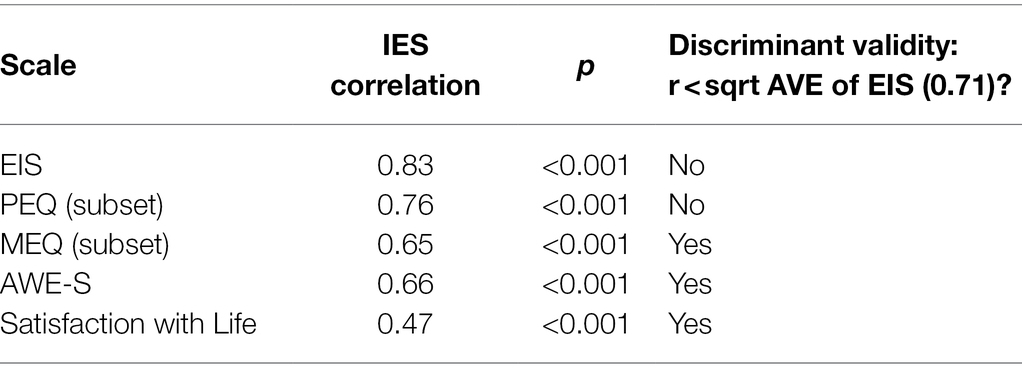
Table 11. Correlation matrix of IES with related scales.
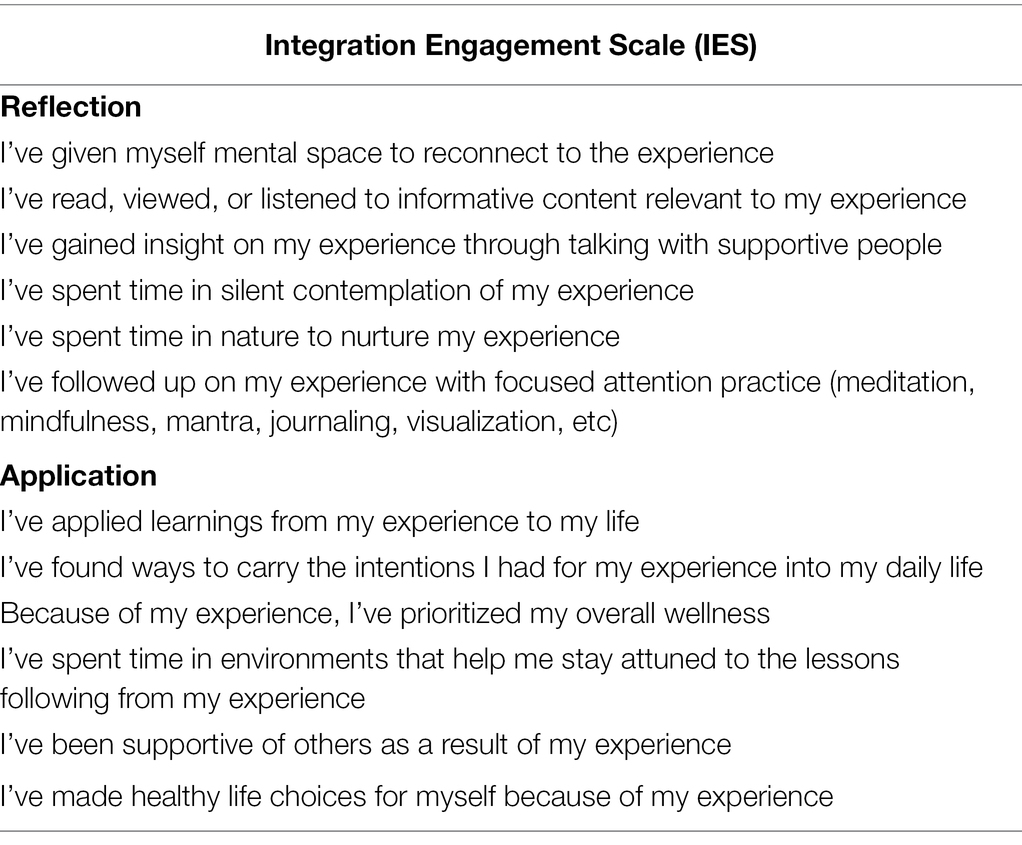
Table 12. The integration engagement scale.
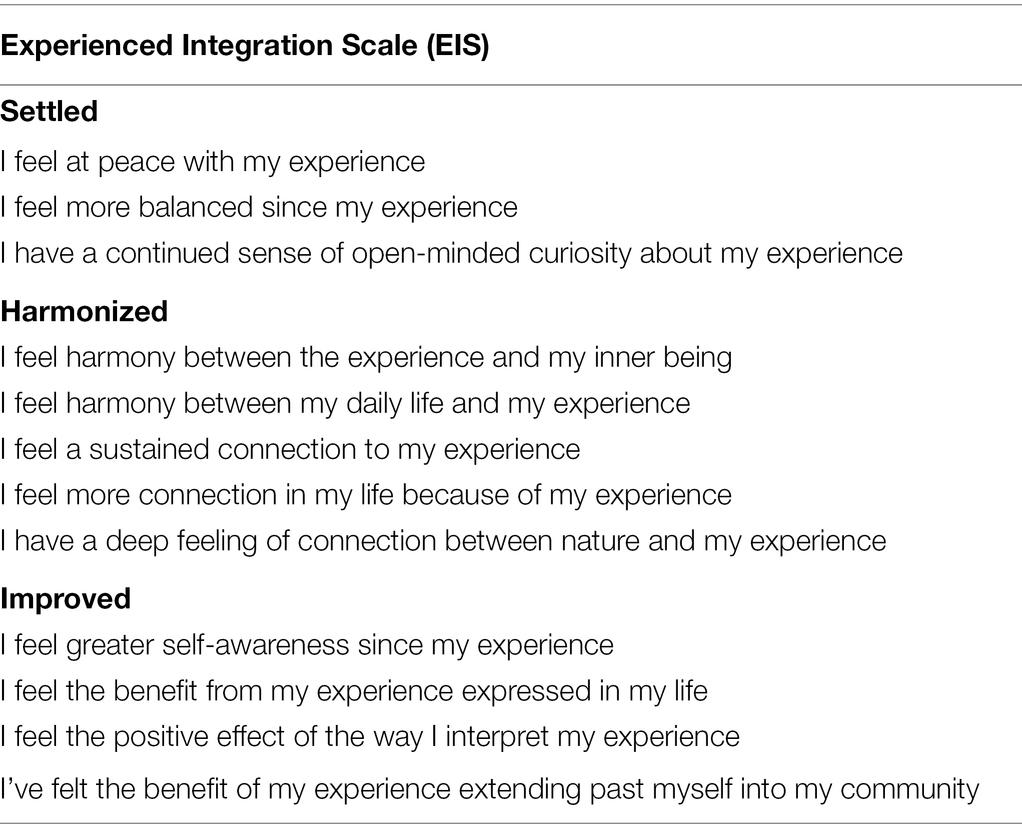
Table 13. The experience integration scale.
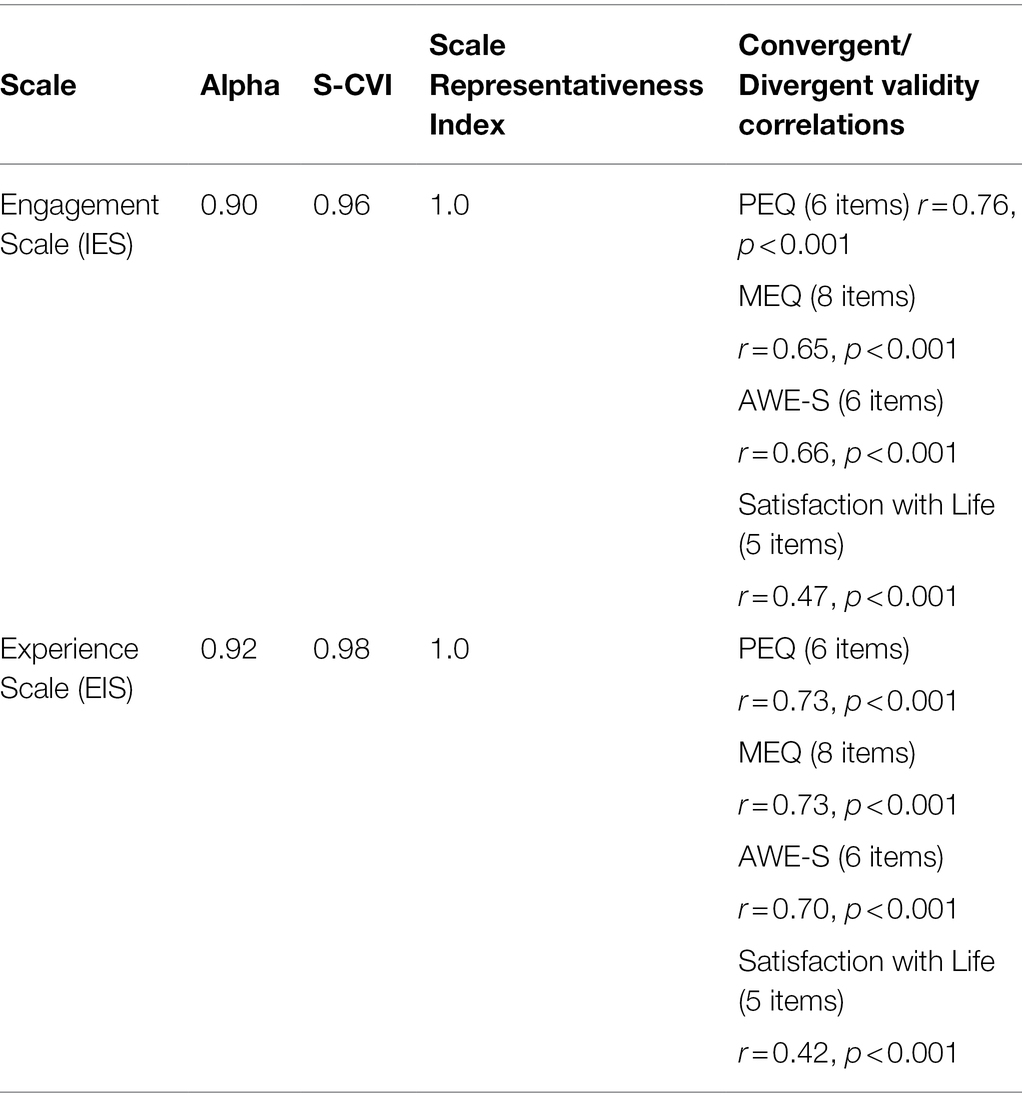
Table 14. Summary of scale statistics.
Discussion
CFA supported the results of Study 4’s EFA, yielding a single-factor structure for the IES, as well as a single-factor structure for the EIS. Convergent validity analysis demonstrated strong positive associations with PEQ, MEQ, and AWE-S items. Divergent validity was evidenced by moderate associations with the Satisfaction with Life Scale.
The high correlation of 0.83 between the IES and EIS, which was greater than the square root of the AVE for either scale, indicates a lack of discriminant validity between the two scales (Fornell and Larcker, 1981). In other words, the construct of engaging with integration and feeling integrated were highly similar in this sample. The correlation between the two scales may have been particularly high due to the length of time since participant’s most recent use of a psychedelic (on average participant’s most recent use fell just between the anchors of “In the last month” and “In the last year”). Integration engagement is hypothesized to eventually lead to the experience of integration. As such, over time it would be expected that scores on the two scales might converge. In future studies, divergent validity may be supported by an analysis of scores on the two scales at points closer in time to the participant’s recent psychedelic experience. Additionally, the authors hypothesize that divergent validity would be particularly pronounced with first time or novice users of psychedelics (particularly with high dose experiences), for whom the novelty and unfamiliarity of the experience would tend to be greater. In such cases, the experience of integration might be expected to be particularly low soon after the experience (given a stance that integration is often a process that takes time), while engagement would optimally be high (given the stance that engagement would support a novice user in adjusting to the potentially highly unfamiliar experience). Furthermore, discriminant validity may have been impacted by the item selection process. The selection process, which led to a small number of relatively diverse items, may have resulted in relatively lower factor loadings, and in turn a relatively lower AVE. This may have in part accounted for a square root of AVE which was lower than the correlation between the scales.
The Psychedelic Integration Scales items are all worded in a positive direction, with higher scores indicating greater integration. The scales are intended to be helpful tools for facilitators and clinicians to gain a sense of the status of a participant’s integration process. The utility of the scales will be improved as data are collected in clinical trials, indicating participant’s levels of integration and corresponding mental health outcomes. With such data, future research may be able to identify meaningful cutoff scores for levels of integration engagement and experience associated with mental health outcomes. Currently, practical interpretation of integration scales scores is limited to the clinician’s interpretation of scale scores relative to the anchor values. For example, a sum score of 72 on the IES would indicate an average level of “Agree” with each of the statements (suggesting a relatively high degree of integration engagement), while a sum score of 24 on the IES would indicate an average response of “Somewhat Disagree” (suggesting a relatively low degree of integration engagement).
Different facets of integration are expected to be accomplished at different rates, depending on factors, such as the strength of dose administered or the degree of challenging content addressed during the psychedelic experience. As such, a single sum score taken at one time point should be interpreted with caution. Furthermore, integration may be most robustly evidenced when it persists over time. For example, if universal love arose as a core quality of a psychedelic experience, integration would be most robustly indicated if an individual continued to act in accordance with qualities of universal love many months after the session. Given these considerations, we suggest administering the Psychedelic Integration Scales at multiple time points, beginning shortly after the acute stage of the psychedelic experience.
Overall Discussion
The purpose of our research is to validate a pair of scales measuring psychedelic integration. The definition of psychedelic integration set forth in this article is “The process by which a psychedelic experience translates into positive changes in daily life.” This definition characterizes psychedelic integration as ongoing, helpful, embodied, and oriented toward building connection. The two scales constructed in this article, the Integration Engagement Scale (IES) and Experienced Integration Scale (EIS), respectively measure the behavioral and intrapsychic aspects of integration. “Reflection” and “Application” are identified as the core features of integration engagement. The internal qualities of feeling “Settled,” “Harmonized,” and “Improved” are identified as the experiential hallmarks of integration.
Given that psychedelic experiences can have a very powerful psychological impact involving non-ordinary states of mind, the integration of these experiences is particularly important. As psychedelics use is on the rise, the construction of these scales is both significant and timely. As of 2022, the first legalization of therapeutic psychedelic use occurred in Oregon, and based on FDA designation of psychedelics as a “breakthrough treatment” legalization is predicted to expand over the coming years (Nutt and Carhart-Harris, 2021). In 2013 there were 30 million lifetime users of psychedelics in the United States alone (Krebs and Johansen, 2013). That number has been increasing at an accelerating rate with a shift in popular culture, current clinical trials, and new research publications that highlight the healing properties of psychedelics and plant medicines (Nutt and Carhart-Harris, 2021).
Given that extensive training is required to be a qualified provider of psychedelics, it is unlikely that the supply of sufficiently good facilitators will keep up with the public demand for psychedelics use. As such, it is reasonable to predict that many unintegrated experiences will result from the hundreds of millions of total psychedelic journeys that will likely occur in the coming years. Within Western and urban cultural containers that have individualistic, consumerist, and performance-oriented values and social structures, the challenges of integrating profound psychedelic experiences may be particularly acute (Diament et al., 2021). It is imperative that the scientific community better understands the processing of these powerful experiences in their aftermath, so that facilitators and users may both maximize the sustainable benefits of psychedelic experiences and minimize irresponsible harm (see Yaden et al., 2021) caused by inducing these experiences without a sufficiently supportive frame.
The psychedelic integration scales have the potential to support both benefit maximization and harm reduction related to psychedelics use. Because addiction to psychedelics is extremely rare, and they are physically safe, the form of harm that may result from their use is primarily psychological—most often related to reactions to the profound changes in consciousness which psychedelics can occasion (Müller and Schumann, 2011; Shalit et al., 2019). In order to improve harm reduction for individuals who choose to have a psychedelic experience, we must better understand how individuals may be supported in embracing the process of change and discovering positive potential within their experiences. “Set and Setting” are proposed to be two fundamental aspects of creating a positive environment conducive to harm reduction and benefit maximization during the experience. We propose that “Reflection and Application” are analogously two fundamental aspects of creating a situation conducive to benefit maximization and harm reduction in the aftermath—with the resulting qualities of feeling “Settled, Harmonized, and Improved” as testaments to successful integration.
The practical utility of the integration scales will grow with data collection. Future research may contribute to the identification of cutoff scores indicating beneficial or concerning levels of post-acute psychedelic integration, an optimal frequency and time scale during which to administer the scales, a sense of the importance of different aspects of integration given the use of different substances, doses, or intentions, and the relevance of the scales to the integration of psychedelic experiences which may have occurred in the past. An initial suggestion for helpful administration of the scales is to administer the EIS within 48 h of the initial experience, followed by administration of the EIS and IES once per week for 8 to 12 weeks. Item answers of “Somewhat Disagree” or below could be flagged as potential areas of concern related to integration. Response to scale items could be used by facilitators or clinicians as a segue into integration therapy or coaching topics.
The framework for understanding and measuring psychedelic integration proposed in this article is intended to help inform the formation of high-quality contexts for the facilitation of psychedelics. Psychedelics are proposed to be treatments which “address the root cause” of mental health issues, and present hopeful alternatives to other forms of medical treatment which may temporarily relieve symptoms but ultimately prove ineffective at causing sustainable positive shifts in mental health (Wheeler and Dyer, 2020). While traditional psychiatric medication often neutralizes symptoms at the expense of grave side effects, psychedelic medicines present opportunities to address symptom causes and pave the way for positive feedback loops of change to occur—with potentially far fewer lasting adverse side effects. However, the actualization of sustainable positive change resulting from psychedelics use depends on the integration of the psychedelic experience into daily life (Payne et al., 2021). For these substances to be used at their full potential—as catalysts of profound improvement—it is necessary that we augment their use with informed integration support.
In current psychedelic research trials, therapy is an integral part of the treatment design. Therapy can be an important part of the integration process; however, psychedelic integration extends beyond just therapy. Important aspects of integration identified include engagement with nature, supportive communities, seasoned psychedelic guides, personal contemplation, and physical and spiritual practices—all of which extend beyond the boundaries of traditional therapy. Each of these important components of psychedelic integration has been present in the ways of life and ceremony seen in indigenous tribes around the world, who have used psychedelics as sacraments for hundreds to thousands of years (Sessa, 2014; Trope et al., 2019; George et al., 2020). It is also important to acknowledge the historical and ongoing occurrence of misappropriation of psychedelic substances and traditions from indigenous communities (George et al., 2019). To continue to ethically research the healing potential of plant medicines we have a responsibility to honor the cultures and sources through which they have arrived in Western culture and to protect the ceremonial and sacred uses of these substances (Sloshower, 2018; Charcuna Institute, 2019).
Limitations
Different psychedelics have different properties, may be used in different dosages, and evoke different types of experience. Furthermore, each individual’s character, stage of life, and cultural context is unique. As a consequence, the optimal integration of each particular psychedelic experience will vary drastically. In this study, we only assessed the generalized qualities associated with good integration. We also recognize that integration is an unfolding process that takes time.
As such, a sum score derived from the scales should be interpreted with caution. A small dose experience, for example, may demand less intensive engagement with the integration process. An individual who scores low on the engagement scale after taking a small dose should not interpret that result as a testament that they are not practicing good psychedelic integration. Likewise, a large dose may naturally result in temporarily feeling unsettled or out of alignment, as profound changes continue to reverberate in the aftermath of the experience. An individual who initially scores low on items relating to feeling settled or harmonized should not interpret the score as a failure to integrate the experience. Further research will be needed to identify how optimal integration unfolds in the context of unique personalities, conditions, dosages, timeframes, psychedelic substances, and cultural contexts.
There are also limitations pertaining to the data source used in our study. All data was gathered via M-Turk users based in the United States, who indicated that they had had a psychedelic experience. M-Turk has been shown to be a credible source of data collection, and an attention check filter was used to increase data quality (Mortensen and Hughes, 2018). However, the pool of participants used is culturally and demographically limited. As such, conclusions regarding the validity of the scales are likewise limited. Furthermore, the CFA indicated that the majority of the M-Turk participants had most recently used classic psychedelics (predominantly mushrooms, LSD, MDMA, DMT, and Ayahuasca). While the authors postulate that the general principles of psychedelic integration would also apply to less commonly used psychedelic substances, the data are most relevant to the use of classic psychedelics. Another limitation pertaining to the data source includes the lack of demographic information regarding experts in studies two and three. Such information would be pertinent to assessing potential biases in the item rating process.
An additional limitation pertains to the theoretical rather than statistically supported nature of the subdomains. The authors prioritized arriving at succinct scale with conceptually diverse items. As such, a strong CVI and redundancy filter was applied to the set of items prior to EFA, potentially contributing to the finding of a single-factor model for both scales (rather than a multifactor model supporting the delineation of the subdomains). The face value assessment of redundancy implemented by the authors may also have introduced bias into the item selection process. Furthermore, the IES and EIS both showed correlations with each other that exceeded the square root of AVE, statistically indicating a lack of discriminant validity (Fornell and Larcker, 1981). This result may reflect a merging over time of integration engagement and experienced integration. Future studies may be employed to discern whether discriminant validity is supported to a greater degree closer in time to a psychedelic experience, or with novice users. The PEQ item subset and the IES also did not evidence discriminant validity, which may have resulted from selection bias in choosing the subset of PEQ items. The a priori selection of PEQ and MEQ item subsets based on face value relevance of the items to convergent validity analysis also may have influenced convergent validity correlation results. To gain a more robust metric of convergent validity, the full PEQ and MEQ scales could be used. Lastly, a more robust analysis of convergent validity would be supported by use of the scales in conjunction with the full PEQ, MEQ, and Awe scales.
Conclusion
We hope that the formation of the integration scales may be one step further in the direction of psychedelics being used in a responsible and beneficial manner. With enhanced value placed on integration, there is greater potential for psychedelic experiences to translate into the beneficial lived actions of psychedelic users, opening the door for a sense of respect and appreciation from others.
The Psychedelic Integration Scales
A full list of the final IES and EIS scale items, along with instructions, can be found in Figure 1. A five-point Likert scale is used to measure responses, with the anchors “strongly disagree,” “disagree,” “neither agree nor disagree,” “agree,” and “strongly agree.”
The following prompt is used to orient participants to the task:
“Please state your level of agreement with the following statements, considering the time period since your most recent psychedelic experience. If you have already filled out this questionnaire, indicate your responses only with respect to the time period since you last filled out the questionnaire. Answer as honestly as possible. There are no right or wrong answers. At any given time your responses will naturally vary between lower and higher scores.”
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Pacifica Graduate Institute IRB. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
TF and SW jointly conceived of the presented idea, conducted the literature review, scale item pool generation, domain and subdomain specifications, cognitive interviewing data collection and analysis, the expert validation recruitment, data collection, and analysis, and content validity index data collection and analysis. TF wrote the majority of the article, and conducted the exploratory factor analysis. SW wrote a minority of the article. DY provided edits to the writing and suggestions for data analysis and experimental design. JL provided edits to the writing and conducted the confirmatory factor analysis and convergent validity analysis. All authors contributed to the article and approved the submitted version.
Funding
Personal funding sourced by TF and SW.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors acknowledge the mentorship, guidance, and support of William A. Richards, Francoise Bourzat, Jennifer Sandoval, Matthew Watherston, Austin Mallard, Jim Whitney, Publio Valle, and Ingmar Gorman.
References
Aday, J. S., Bloesch, E. K., and Davoli, C. C. (2020). 2019: A year of expansion in psychedelic research, industry, and deregulation. Drug Sci. Policy Law 6:205032452097448. doi: 10.1177/2050324520974484
Anderson, B. T., Danforth, A., Daroff, P. R., Stauffer, C., Ekman, E., Agin-Liebes, G., et al. (2020). Psilocybin-assisted group therapy for demoralized older long-term AIDS survivor men: An open-label safety and feasibility pilot study. E Clin. Med. 27:100538. doi: 10.1016/j.eclinm.2020.100538
Barrett, F. S., Bradstreet, M. P., Leoutsakos, J. M. S., Johnson, M. W., and Griffiths, R. R. (2016). The challenging experience questionnaire: characterization of challenging experiences with psilocybin mushrooms. J. Psychopharmacol. 30, 1279–1295. doi: 10.1177/0269881116678781
Belouin, S., and Henningfield, J. (2018). Psychedelics: where we are now, why we got here, what we must do. Neuropharmacology 142, 7–19. doi: 10.1016/j.neuropharm.2018.02.018
Bourzat, F., and Hunter, K. (2019). Consciousness Medicine: Indigenous Wisdom, Entheogens, and Expanded States of Consciousness for Healing and Growth. United States: North Atlantic Books.
Büssing, A., Matthiessen, P. F., and Ostermann, T. (2005). Engagement of patients in religious and spiritual practices: confirmatory results with the SpREUK-P 1.1 questionnaire as a tool of quality of life research. Health Qual. Life Outcomes 3, 1–11. doi: 10.1186/1477-7525-3-53
Carbonaro, T. M., Bradstreet, M. P., Barrett, F. S., MacLean, K. A., Jesse, R., Johnson, M. W., et al. (2016). Survey study of challenging experiences after ingesting psilocybin mushrooms: acute and enduring positive and negative consequences. J. Psychopharmacol. 30, 1268–1278. doi: 10.1177/0269881116662634
Carhart-Harris, R. (2013). Psychedelic drugs, magical thinking and psychosis. J. Neurol. Neurosurg. Psychiatry 84:e1. doi: 10.1136/jnnp-2013-306103.17
Carhart-Harris, R. L., Bolstridge, M., Rucker, J., Day, C. M., Erritzoe, D., Kaelen, M., et al. (2016). Psilocybin with psychological support for treatment-resistant depression: an open-label feasibility study. Lancet Psychiatry 3, 619–627. doi: 10.1016/S2215-0366(16)30065-7
Carhart-Harris, R. L., Erritzoe, D., Haijen, E., Kaelen, M., and Watts, R. (2018). Psychedelics and connectedness. Psychopharmacology 235, 547–550. doi: 10.1007/s00213-017-4701-y
Carhart-Harris, R. L., and Friston, K. (2019). REBUS and the anarchic brain: toward a unified model of the brain action of psychedelics. Pharmacol. Rev. 71, 316–344. doi: 10.1124/pr.118.017160
Cattell, R. B. (1966). The screen test for the number of factors. Multivar. Behav. Res. 1, 245–276. doi: 10.1207/s15327906mbr0102_10
Charcuna Institute (2019). Council for the Protection of Sacred Plants. Available at: https://chacruna.net/council-for-the-protection-of-sacred-plants/ (Accessed December 18, 2021).
Cook, L. (2014). Empathetic reform and the psychedelic aesthetic: women’s accounts of LSD therapy. Configurations 22, 79–111. doi: 10.1353/con.2014.0002
Diament, M., Gomes, B. R., and Tófoli, L. F. (2021). “Ayahuasca and psychotherapy: beyond integration” in Ayahuasca Healing and Science. ed. C. Cavnar (Cham: Springer), 63–79.
Diener, E. D., Emmons, R. A., Larsen, R. J., and Griffin, S. (1985). The satisfaction with life scale. J. Pers. Assess. 49, 71–75. doi: 10.1207/s15327752jpa4901_13
Dos Santos, R. G., Osório, F. L., Crippa, J., and Hallak, J. (2016). Classical hallucinogens and neuroimaging: A systematic review of human studies: hallucinogens and neuroimaging. Neurosci. Biobehav. Rev. 71, 715–728. doi: 10.1016/j.neubiorev.2016.10.026
Dyck, E., and Elcock, C. (2020). Reframing bummer trips: scientific and cultural explanations to adverse reactions to psychedelic drug use. Soc. History Alcohol Drugs 34, 271–296. doi: 10.1086/707512
Elsey, J. W. (2017). Psychedelic drug use in healthy individuals: A review of benefits, costs, and implications for drug policy. Drug Sci. Policy Law 3:205032451772323. doi: 10.1177/2050324517723232
Erritzoe, D., Roseman, L., Nour, M. M., MacLean, K., Kaelen, M., Nutt, D. J., et al. (2018). Effects of psilocybin therapy on personality structure. Acta Psychiatr. Scand. 138, 368–378. doi: 10.1111/acps.12904
Fadiman, J. (2011). The Psychedelic explorer’s Guide: Safe, Therapeutic, and Sacred Journeys. United States: Simon and Schuster.
Fornell, C., and Larcker, D. F. (1981). Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 18, 39–50. doi: 10.1177/002224378101800104
Gandy, S., Forstmann, M., Carhart-Harris, R. L., Timmermann, C., Luke, D., and Watts, R. (2020). The potential synergistic effects between psychedelic administration and nature contact for the improvement of mental health. Health Psychol. 7:205510292097812. doi: 10.1177/2055102920978123
Gashi, L., Sandberg, S., and Pedersen, W. (2021). Making “bad trips” good: how users of psychedelics narratively transform challenging trips into valuable experiences. Int. J. Drug Policy 87:102997. doi: 10.1016/j.drugpo.2020.102997
George, J. R., Michaels, T. I., Sevelius, J., and Williams, M. T. (2019). The psychedelic renaissance and the limitations of a White-dominant medical framework: A call for indigenous and ethnic minority inclusion. J. Psychedelic Stu. [Advance online publication] doi: 10.1556/2054.2019.015
George, J. R., Michaels, T. I., Sevelius, J., and Williams, M. T. (2020). The psychedelic renaissance and the limitations of a white-dominant medical framework: A call for indigenous and ethnic minority inclusion. J. Psychedelic Stu. 4, 4–15. doi: 10.1556/2054.2019.015
Gorman, I., Nielson, E. M., Molinar, A., Cassidy, K., and Sabbagh, J. (2021). Psychedelic harm reduction and integration: a transtheoretical model for clinical practice. Front. Psychol. 12:645246. doi: 10.3389/fpsyg.2021.645246
Griffiths, R. R., Johnson, M. W., Carducci, M. A., Umbricht, A., Richards, W. A., Richards, B. D., et al. (2016). Psilocybin produces substantial and sustained decreases in depression and anxiety in patients with life-threatening cancer: A randomized double-blind trial. J. Psychopharmacol. 30, 1181–1197. doi: 10.1177/0269881116675513
Griffiths, R. R., Johnson, M. W., Richards, W. A., Richards, B. D., Jesse, R., MacLean, K. A., et al. (2018). Psilocybin-occasioned mystical-type experience in combination with meditation and other spiritual practices produces enduring positive changes in psychological functioning and in trait measures of prosocial attitudes and behaviors. J. Psychopharmacol. 32, 49–69. doi: 10.1177/0269881117731279
Griffiths, R. R., Johnson, M. W., Richards, W. A., Richards, B. D., McCann, U., and Jesse, R. (2011). Psilocybin occasioned mystical-type experiences: immediate and persisting dose-related effects. Psychopharmacology 218, 649–665. doi: 10.1007/s00213-011-2358-5
Griffiths, R., Richards, W., Johnson, M., McCann, U., and Jesse, R. (2008). Mystical-type experiences occasioned by psilocybin mediate the attribution of personal meaning and spiritual significance 14 months later. J. Psychopharmacol. 22, 621–632. doi: 10.1177/0269881108094300
Griffiths, R. R., Richards, W. A., McCann, U., and Jesse, R. (2006). Psilocybin can occasion mystical-type experiences having substantial and sustained personal meaning and spiritual significance. Psychopharmacology 187, 268–283. doi: 10.1007/s00213-006-0457-5
Guss, J., Krause, R., and Sloshower, J. (2020). The Yale manual for psilocybin-assisted therapy of depression (using acceptance and commitment therapy as a therapeutic frame). PsyarXiv. doi: 10.31234/osf.io/u6v9y, [Epub Ahead of Print]
Haijen, E. C., Kaelen, M., Roseman, L., Timmermann, C., Kettner, H., Russ, S., et al. (2018). Predicting responses to psychedelics: a prospective study. Front. Pharmacol. 9:897. doi: 10.3389/fphar.2018.00897
Hayes, S. C. (2005). Get out of your Mind and into your Life: The New Acceptance and Commitment Therapy. United States: New Harbinger Publications.
Hendricks, P. S., Thorne, C. B., Clark, C. B., Coombs, D. W., and Johnson, M. W. (2015). Classic psychedelic use is associated with reduced psychological distress and suicidality in the United States adult population. J. Psychopharmacol. 29, 280–288.
Heuschkel, K., and Kuypers, K. P. (2020). Depression, mindfulness, and psilocybin: possible complementary effects of mindfulness meditation and psilocybin in the treatment of depression. A review. Front. Psychiatry 11:224. doi: 10.3389/fpsyt.2020.00224
Horn, J. (1965). A rationale and test for the number of factors in factor analysis. Psychometrika 30, 179–185. doi: 10.1007/bf02289447
Johnson, M. W., Garcia-Romeu, A., Johnson, P. S., and Griffiths, R. R. (2017). An online survey of tobacco smoking cessation associated with naturalistic psychedelic use. J. Psychopharmacol. 31, 841–850. doi: 10.1177/0269881116684335
Johnson, M., Richards, W., and Griffiths, R. (2008). Human hallucinogen research: guidelines for safety. J. Psychopharmacol. 22, 603–620. doi: 10.1177/0269881108093587
Kangas, M., and McDonald, S. (2009). Is it time to act? The potential of acceptance and commitment therapy for psychological problems following acquired brain injury. Neuropsychol. Rehabil. 21, 250–276. doi: 10.1080/09602011.2010.540920
Kelly, J. R., Baker, A., Babiker, M., Burke, L., Brennan, C., and O’Keane, V. (2019). The psychedelic renaissance: the next trip for psychiatry? Ir. J. Psychol. Med., 1–5. doi: 10.1017/ipm.2019.39 [Epub Ahead of Print]
Kettner, H., Gandy, S., Haijen, E. C., and Carhart-Harris, R. L. (2019). From egoism to ecoism: psychedelics increase nature relatedness in a state-mediated and context-dependent manner. Int. J. Environ. Res. Public Health 16:5147. doi: 10.3390/ijerph16245147
Killion, B., Hai, A. H., Alsolami, A., Vaughn, M. G., Oh, P. S., and Salas-Wright, C. P. (2021). LSD use in the United States: trends, correlates, and a typology of us. Drug Alcohol Depend. 223:108715. doi: 10.1016/j.drugalcdep.2021.108715
Krebs, T. S., and Johansen, P. Ø. (2013). Over 30 million psychedelic users in the United States. F1000 Res. 2:98. doi: 10.12688/f1000research.2-98.v1
Lebedev, A. V., Kaelen, M., Lövdén, M., Nilsson, J., Feilding, A., Nutt, D. J., et al. (2016). LSD-induced entropic brain activity predicts subsequent personality change. Hum. Brain Mapp. 37, 3203–3213. doi: 10.1002/hbm.23234
Luoma, J. B., Chwyl, C., Bathje, G. J., Davis, A. K., and Lancelotta, R. (2020). A meta-analysis of placebo-controlled trials of psychedelic-assisted therapy. J. Psychoactive Drugs 52, 289–299. doi: 10.1080/02791072.2020.1769878
MacLean, K. A., Johnson, M. W., and Griffiths, R. R. (2011). Mystical experiences occasioned by the hallucinogen psilocybin lead to increases in the personality domain of openness. J. Psychopharmacol. 25, 1453–1461. doi: 10.1177/0269881111420188
Mahr, G., and Sweigart, J. (2020). Psychedelic drugs and Jungian therapy. J. Jungian Sch. Stud. 15, 86–98.
Mithoefer, M. C., Grob, C. S., and Brewerton, T. D. (2016). Novel psychopharmacological therapies for psychiatric disorders: psilocybin and MDMA. Lancet Psychiatry 3, 481–488. doi: 10.1016/S2215-0366(15)00576-3
Morris, L., and Mansell, W. (2018). A systematic review of the relationship between rigidity/flexibility and transdiagnostic cognitive and behavioral processes that maintain psychopathology. J. Exp. Psychopathol. 9:204380871877943. doi: 10.1177/2043808723279431
Mortensen, K., and Hughes, T. L. (2018). Comparing Amazon’s mechanical Turk platform to conventional data collection methods in the health and medical research literature. J. Gen. Intern. Med. 33, 533–538. doi: 10.1007/s11606-017-4246-0
Müller, C., and Schumann, G. (2011). To use or not to use: expanding the view on non-addictive psychoactive drug consumption and its implications. Behav. Brain Sci. 34, 328–347. doi: 10.1017/S0140525X1100135X
Murphy-Beiner, A., and Soar, K. (2020). Ayahuasca’s ‘afterglow’: improved mindfulness and cognitive flexibility in ayahuasca drinkers. Psychopharmacology 237, 1161–1169. doi: 10.1007/s00213-019-05445-3
Nielson, E. M., May, D. G., Forcehimes, A. A., and Bogenschutz, M. P. (2018). The psychedelic debriefing in alcohol dependence treatment: illustrating key change phenomena through qualitative content analysis of clinical sessions. Front. Pharmacol. 9:132. doi: 10.3389/fphar.2018.00132
Nutt, D., and Carhart-Harris, R. (2021). The current status of psychedelics in psychiatry. JAMA Psychiatry 78, 121–122. doi: 10.1001/jamapsychiatry.2020.2171
Ortigo, K. M., andamp; Richards, W. A. (2021). Beyond the Narrow Life: A Guide for Psychedelic Integration and Existential Exploration. United States: Synergetic Press.
Palamar, J. J., Rutherford, C., and Keyes, K. M. (2021). Trends in ketamine use, exposures, and seizures in the United States up to 2019. Am. J. Public Health 111, 2046–2049. doi: 10.2105/AJPH.2021.306486
Payne, J., Chambers, R., and Liknaitzky, P. (2021). Combining psychedelic and mindfulness interventions: synergies to inform clinical practice. ACS Pharmacol. Trans. Sci. 4, 416–423. doi: 10.1021/acsptsci.1c00034
Phelps, J. (2017). Developing guidelines and competencies for the training of psychedelic therapists. J. Humanist. Psychol. 57, 450–487. doi: 10.1177/0022167817711304
Pilecki, B., Luoma, J. B., Bathje, G. J., Rhea, J., and Narloch, V. F. (2021). Ethical and legal issues in psychedelic harm reduction and integration therapy. Harm Reduct. J. 18, 40–14. doi: 10.1186/s12954-021-00489-1
Pollan, M. (2018). How to Change Your Mind: What the New Science of Psychedelics Teaches us About Consciousness, Dying, Addiction, Depression, and Transcendence. United States: Penguin Books.
Preller, K. H., Razi, A., Zeidman, P., Stämpfli, P., Friston, K. J., and Vollenweider, F. X. (2019). Effective connectivity changes in LSD-induced altered states of consciousness in humans. Proc. Natl. Acad. Sci. 116, 2743–2748. doi: 10.1073/pnas.1815129116
Radakovic, C., Radakovic, R., Peryer, G., and Geere, J. A. (2021). Psychedelics and mindfulness: A systematic review and meta-analysis. PsyArXiv [Preprint]. doi: 10.31234/osf.io/yu7jf
Richards, W. A. (2016). Sacred Knowledge: Psychedelics and Religious Experiences. United States: Columbia University Press.
Riley, S., Thompson, J., and Griffin, C. (2010). Turn on, tune in, but don’t drop out: The impact of neo-liberalism on magic mushroom users’ (in)ability to imagine collectivist social worlds. Int. J. Drug Policy 21, 445–451. doi: 10.1016/j.drugpo.2010.07.001
Roseman, L., Nutt, D. J., and Carhart-Harris, R. L. (2018). Quality of acute psychedelic experience predicts therapeutic efficacy of psilocybin for treatment-resistant depression. Front. Pharmacol. 8:974. doi: 10.3389/fphar.2017.00974
Rucker, J., Iliff, J., and Nutt, D. (2019). Psychiatry and the psychedelic drugs. Past, present and future. Neuropharmacology 142, 200–218. doi: 10.1016/j.neuropharm.2017.12.040
Sampedro, F., de la Fuente Revenga, M., Valle, M., Roberto, N., Domínguez-Clavé, E., Elices, M., et al. (2017). Assessing the psychedelic “after-glow” in ayahuasca users: post-acute neurometabolic and functional connectivity changes are associated with enhanced mindfulness capacities. Int. J. Neuropsychopharmacol. 20, 698–711. doi: 10.1093/ijnp/pyx036
Sessa, B. (2014). Why psychiatry needs psychedelics and psychedelics need psychiatry. J. Psychoactive Drugs 46, 57–62. doi: 10.1080/02791072.2014.877322
Shalit, N., Rehm, J., and Lev-Ran, S. (2019). Epidemiology of hallucinogen use in the US results from the national epidemiologic survey on alcohol and related conditions III. Addict. Behav. 89, 35–43. doi: 10.1016/j.addbeh.2018.09.020
Shipley, M. (2021). “Alan Watts, psychedelic Buddhism, and religious play in postwar America,” in The Relevance of Alan Watts in Contemporary Culture. ed. P. J. Columbus (United States: Routledge), 79–91.
Siegel, D. J. (2009). Mindful awareness, mindsight, and neural integration. Humanist. Psychol. 37, 137–158. doi: 10.1080/08873260902892220
Siegel, D. J. (2016). Mind: A Journey to the Heart of Being Human. New York: W.W. Norton and Company.
Sloshower, J. (2018). “Integrating psychedelic medicines and psychiatry: theory and methods of a model clinic,” in Plant Medicines. eds. B. Labate and C. Cavnar (Springer Cham: Healing and Psychedelic Science).
Sloshower, J., Guss, J., Krause, R., Wallace, R. M., Williams, M. T., Reed, S., et al. (2020). Psilocybin-assisted therapy of major depressive disorder using acceptance and commitment therapy as a therapeutic frame. J. Contextual Behav. Sci. 15, 12–19. doi: 10.1016/j.jcbs.2019.11.002
Smigielski, L., Kometer, M., Scheidegger, M., Krähenmann, R., Huber, T., and Vollenweider, F. X. (2019). Characterization and prediction of acute and sustained response to psychedelic psilocybin in a mindfulness group retreat. Sci. Rep. 9:14914. doi: 10.1038/s41598-019-50612-3
Strassman, R. J. (1984). Adverse reactions to psychedelic drugs. A review of the literature. J. Nerv. Ment. Dis., 172, 577–595. doi:10.1097/00005053-198410000-00001
Timmermann, C., Kettner, H., Letheby, C., Roseman, L., Rosas, F. E., and Carhart-Harris, R. L. (2021). Psychedelics alter metaphysical beliefs. Sci. Rep. 11, 1–13. doi: 10.1038/s41598-021-01209-2
Trope, A., Anderson, B. T., Hooker, A. R., Glick, G., Stauffer, C., and Woolley, J. D. (2019). Psychedelic-assisted group therapy: A systematic review. J. Psychoactive Drugs 51, 174–188. doi: 10.1080/02791072.2019.1593559
Tupper, K. W., Wood, E., Yensen, R., and Johnson, M. W. (2015). Psychedelic medicine: a re-emerging therapeutic paradigm. CMAJ 187, 1054–1059. doi: 10.1503/cmaj.141124
Velicer, W. F. (1976). Determining the number of components from the matrix of partial correlations. Psychometrika 41, 321–327. doi: 10.1007/BF02293557
Walsh, Z., and Thiessen, M. S. (2018). Psychedelics and the new behaviourism: considering the integration of third-wave behaviour therapies with psychedelic-assisted therapy. Int. Rev. Psychiatry 30, 343–349. doi: 10.1080/09540261.2018.1474088
Watts, R., Day, C., Krzanowski, J., Nutt, D., and Carhart-Harris, R. (2017). Patients’ accounts of increased “connectedness” and “acceptance” after psilocybin for treatment-resistant depression. J. Humanist. Psychol. 57, 520–564. doi: 10.1177/0022167817709585
Wersebe, H., Lieb, R., Meyer, A. H., Hofer, P., and Gloster, A. T. (2018). The link between stress, well-being, and psychological flexibility during an acceptance and commitment therapy self-help intervention. Int. J. Clin. Health Psychol. 18, 60–68. doi: 10.1016/j.ijchp.2017.09.002
Wesson, D. R. (2011). Psychedelic drugs, hippie counterculture, speed and phenobarbital treatment of sedative-hypnotic dependence: a journey to the Haight Ashbury in the sixties. J. Psychoactive Drugs 43, 153–164. doi: 10.1080/02791072.2011.587708
Wheeler, S. W., and Dyer, N. L. (2020). A systematic review of psychedelic-assisted psychotherapy for mental health: An evaluation of the current wave of research and suggestions for the future. Psychol. Conscious. Theory Res. Pract. 7, 279–315. doi: 10.1037/cns0000237
Yaden, D. B., Berghella, A. P., Regier, P. S., Garcia-Romeu, A., Johnson, M. W., and Hendricks, P. S. (2021). Classic psychedelics in the treatment of substance use disorder: potential synergies with twelve-step programs. Int. J. Drug Policy 98:103380. doi: 10.1016/j.drugpo.2021.103380
Yaden, D. B., and Griffiths, R. R. (2020). The subjective effects of psychedelics are necessary for their enduring therapeutic effects. ACS Pharmacol. Trans. Sci. 4, 568–572. doi: 10.1021/acsptsci.0c00194
Yaden, D. B., Kaufman, S. B., Hyde, E., Chirico, A., Gaggioli, A., Zhang, J. W., et al. (2019). The development of the AWE experience scale (AWE-S): A multifactorial measure for a complex emotion. J. Posit. Psychol. 14, 474–488. doi: 10.1080/17439760.2018.1484940
Yaden, D. B., Nayak, S. M., Gukasyan, N., Anderson, B. T., and Griffiths, R. R. (2022). The potential of psychedelics for end of life and palliative care. Curr. Topics Behav. Neurosci. doi: 10.1007/7854_2021_278
Yaden, D. B., Yaden, M. E., and Griffiths, R. R. (2021). Psychedelics in psychiatry—keeping the renaissance from going off the rails. JAMA Psychiat. 78, 469–470. doi: 10.1001/jamapsychiatry.2020.3672
Yates, D. (2018). Three arguments for humility. Philos. Stud. 175, 461–481. doi: 10.1007/s11098-017-0877-6
Yockey, R. A., Vidourek, R. A., and King, K. A. (2020). Trends in LSD use among US adults: 2015–2018. Drug Alcohol Depend. 212:108071. doi: 10.1016/j.drugalcdep.2020.108071
Keywords: psychedelics, integration, psilocybin, psychedelic integration, harm reduction, psychotherapy, psychedelic, psychedelic therapy
Citation: Frymann T, Whitney S, Yaden DB and Lipson J (2022) The Psychedelic Integration Scales: Tools for Measuring Psychedelic Integration Behaviors and Experiences. Front. Psychol. 13:863247. doi: 10.3389/fpsyg.2022.863247
Edited by:
Sina Hafizi, University of Manitoba, CanadaReviewed by:
Brian Barnett, Cleveland Clinic, United StatesHannes Simon Kettner, Imperial College London, United Kingdom
Copyright © 2022 Frymann, Whitney, Yaden and Lipson. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tomas Frymann, dGFmMjEyNUB0Yy5jb2x1bWJpYS5lZHU=; Sophie Whitney, c29waGllandoaXRuZXlAZ21haWwuY29t; David B. Yaden, ZHlhZGVuMUBqaG1pLmVkdQ==; Joshua Lipson, amw1NzIxQHRjLmNvbHVtYmlhLmVkdQ==