 Kaja Teraz
Kaja Teraz Luka Šlosar
Luka Šlosar Armin H. Paravlić
Armin H. Paravlić Eling D. de Bruin
Eling D. de Bruin Uros Marusic1,6
Uros Marusic1,6
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychol., 16 June 2022
Sec. Movement Science
Volume 13 - 2022 | https://doi.org/10.3389/fpsyg.2022.837710
This article is part of the Research TopicHuman Movement and Motor Control in the Natural EnvironmentView all 18 articles
Background: Efficient performance of most daily activities requires intact and simultaneous execution of motor and cognitive tasks. To mitigate age-related functional decline, various combinations of motor and cognitive training have shown promising results. The aim of this systematic review and meta-analysis of randomized controlled trials (RCTs) was to evaluate the efficacy of different types of motor-cognitive training interventions (e.g., sequential and simultaneous) on selected functional outcomes in healthy older adults.
Methods: Six online academic databases were used to retrieve eligible RCTs up to April 2021, following PRISMA guidelines and PICO criteria. A random-effects model was used for all meta-analyses conducted on selected functional outcomes: single- and dual-task gait speed, the Timed Up and Go Test (TUG), and Berg Balance Scale (BBS) score. Effect size (ES) was calculated as Hedges' g and interpreted as: trivial: <0.20, small: 0.20–0.60, moderate: 0.61–1.20, large: 1.21–2.00, very large: 2.01–4.00 or extremely large >4.00.
Results: From 2,546 retrieved records, 91 RCTs were included for meta-analysis (n = 3,745 participants; 64.7–86.9 years). The motor-cognitive interventions included differed according to the type of training (e.g., sequential, simultaneous with additional cognitive task or exergame training. The results showed that motor-cognitive interventions can improve gait speed under single-task conditions (small ES = 0.34, P = 0.003). The effect of the intervention was moderated by the type of control group (Q = 6.203, P = 0.013): passive (moderate ES = 0.941, P = 0.001) vs. active controls (trivial ES = 0.153, P = 0.180). No significant effect was found for dual-task walking outcomes (P = 0.063). Motor-cognitive intervention had a positive effect on TUG (small ES = 0.42, P < 0.001), where the effect of intervention was moderated by control group [passive (moderate ES = 0.73, P = 0.001) vs. active (small ES = 0.20, P = 0.020)], but not by the type of training (P = 0.064). Finally, BBS scores were positively affected by motor-cognitive interventions (small ES = 0.59, P < 0.001) with however no significant differences between type of control group (P = 0.529) or intervention modality (P = 0.585).
Conclusions: This study provides evidence for the effectiveness of various types of motor-cognitive interventions on performance-based measures of functional mobility in healthy older adults. With respect to significant effects, gait speed under single-task condition was improved by motor-cognitive interventions, but the evidence shows that this type of intervention is not necessarily more beneficial than motor training alone. On the other hand, motor-cognitive interventions are better at improving multicomponent tasks of dynamic balance and mobility function, as measured by the TUG. Because of substantial heterogeneity and the current limited availability of different types of interventions, the conclusions should be interpreted with caution.
Aging leads to a decline in physical and cognitive abilities, which has been associated with an increased incidence of falls (Lord et al., 1999; Masud and Robert, 2001; Ambrose et al., 2013). Falls occur when everyday tasks become too difficult (either physically or cognitively) and can lead to various injuries that later affect functioning in old age (Masud and Robert, 2001; Tinetti, 2003; Ambrose et al., 2013). Older adults typically struggle with tasks that must be performed simultaneously, such as using a cell phone and walking down the stairs or simultaneously observing the traffic and stepping off the sidewalk at the same time (Beurskens and Bock, 2012; MacPherson, 2018). This “ability to perform two tasks simultaneously” (MacPherson, 2018) is defined as dual-tasking. Dual-tasking is often challenging for older adults, but the underlying mechanism is not yet clear. Older people engage more cognitive control in mobility tasks (Marusic and Grosprêtre, 2018). This is partly due to age-related sensory impairments and partly due to lower automated motor and cognitive performance (Baltes and Lindenberger, 1997; Li and Lindenberger, 2002; Heuninckx et al., 2005; Wollesen and Voelcker-Rehage, 2014). Human attention is limited (Jiang and Kanwisher, 2003) and both physical and cognitive changes that occur in the brain during aging impair executive functions (Peters, 2006).
Appropriate training, whether motor or cognitive training, can slow down the decline of motor and cognitive functions (Allen et al., 2011; Schoene et al., 2013; Smith et al., 2015; Hortobágyi et al., 2016). Studies are describing different types of exercise for older people to improve mobility-related outcomes; motor training (Allen et al., 2011; Hortobágyi et al., 2016), cognitive training (e.g., Smith et al., 2015), and motor-cognitive dual-task training (e.g., Schoene et al., 2013). Recent systematic reviews have shown that motor (for a review see Plummer et al., 2015) and cognitive training (for a review see Marusic et al., 2018b) can have positive effects on mobility in older adults.
In 2010, two research groups conducted two separate pilot studies that indicated extensive transfer from cognitive training to mobility domain (Li et al., 2010; Verghese et al., 2010). After these two pilot trials, there were many other studies that confirmed this effect, which was also summarized in a meta-analysis (for review see Marusic et al., 2018b). In addition, the various types of non-physical interventions (e.g., cognitive training, motor imagery and action observation) can improve motor-related outcomes (Marusic et al., 2018a; Paravlic et al., 2018, 2019). The potential mechanisms of improved mobility performance after non-physical training sessions have been suggested by intertwined neural circuits and brain substrates involved in both cognitive (executive functions) and mobility processes (Marusic et al., 2018b).
The so-called motor-cognitive training is a type of dual-task training, i.e., it involves two different tasks (the motor task and the cognitive task) that can be performed simultaneously or sequentially (Herold et al., 2018), where one of the tasks specifically challenges motor functions and the other task challenges cognitive functions. In sequential training, the motor task (e.g., walking) and the cognitive task (e.g., solving tasks while sitting at a table and using a desktop computer) are separated (Herold et al., 2018). In simultaneous motor-cognitive training, both motor and cognitive exercises are executed at the same time (Lauenroth et al., 2016; Herold et al., 2018). This type of training can be divided into two types: (i) motor training with cognitive exercises that tend to be unrelated to motor task performance, and (ii) motor training in which successful physical task performance depends on cognitive ability (Herold et al., 2018). If the cognitive exercise appears to be more of a distractor, a simultaneous motor-cognitive training is performed with an additional cognitive task (e.g., cycling while counting backwards from 50 and subtracting 4 s). Conversely, simultaneous motor-cognitive training with a built-in cognitive task (e.g., exergame/exergaming or learning to dance) is conducted when the cognitive exercise fits the content of the intervention as a necessary task to successfully complete the training (Schott, 2015; Manser et al., 2021). Exergaming is defined as technology-based physical activities, such as playing video games, that require participants to be physically active or move in order to play the game. These games require the user to move their entire body to participate in virtual sports, group fitness exercises, or other interactive physical activities (American College of Sports Medicine., 2013).
The different types of motor-cognitive training (sequential, simultaneous with additional or incorporated cognitive task) have not been studied. Therefore, the combination of motor and cognitive intervention has recently gained scientific interest. Several reviews and intervention studies have already reported positive effects of motor-cognitive interventions on single- and dual-task walking and balance in both healthy and cognitively impaired older adults (Law et al., 2014; Fritz et al., 2015; Lauenroth et al., 2016; Zhu et al., 2016; Levin et al., 2017; Raichlen et al., 2020; Chen et al., 2021). However, a systematic investigation on the most effective of all motor-cognitive interventions (sequential, simultaneous with an additional or incorporated cognitive task) effecting gait and balance is not available. Our aim was to identify, summarize, and compare randomized controlled trials (RCTs) examining motor-cognitive intervention approaches vs. single or no training interventions in older adults on selected gait and balance functions.
We performed a systematic literature search in six bibliographic databases, i.e., PubMed, Pedro, Cinahl, SportDiscus, and Scopus. In addition, we performed a literature search on Google Scholar. The search strategy included only terms related to or describing the intervention. Terms were combined with the Cochrane MEDLINE filter for controlled trials of interventions. Our search syntax was: (“motor-cognitive intervention” OR “dual-task” OR “motor-cognitive training” OR “physical-cognitive intervention” OR “motor-cognitive exercise” OR “exergames” OR “serious game” OR “active video game”) AND (“gait” OR “walk” OR “walking” OR “mobility” OR “balance” OR “posture”) AND (“elderly” OR “old” OR “older” OR “older adult” OR “older adults” OR “aging” OR “elder adults” OR “elders” OR “old-olds”). Search terms were adapted for use with other bibliographic databases in combination with database-specific filters for controlled trials, where these are available. Database searches were supplemented by the review of the authors files. We additionally reviewed the reference list of each included article. We included only studies published in English. When searching for articles, we did not set a time frame for publication. Nevertheless, all articles that met our inclusion criteria were published between 2009 and 2021. The searches were performed again just before the final analysis and additional studies were selected for inclusion. Titles and abstracts that did not meet the inclusion criteria were excluded from the list. The remaining full texts were screened by 3 reviewers (UM, KT, and LŠ). Ultimately, only randomized controlled trials that met the listed inclusion criteria were included.
The strategy for the literature search followed the PRISMA (The Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. This is an evidence-based minimum set of items for reporting in systematic reviews and meta-analyses. PRISMA is used as the basis for reporting systematic reviews with objectives. In addition, we included the Problem/Population, Intervention, Comparison, and Outcome (PICO) framework; it can help formulate the search strategy with set of key questions to efficiently find high- quality evidence:
Population: healthy and diseased1 older adults; the mean age of subjects was over 60 years.
Intervention: motor-cognitive approaches (sequential, simultaneous distractor, simultaneous incorporated).
Comparison: either passive control (neither cognitive nor motor training performed) or motor training groups.
Outcome measures: Gait speed under (m/s) a single- and a dual-task condition, balance performance as measured with Timed Up and Go test (sec) and Berg Balance Scale (points).
We included only randomized controlled trials (RCTs). The inclusion criteria were: (1) the type of outcome measure was gait speed under a single- and/or a dual-task, the Up and Go test and/or the Berg Balance Scale, (2) subjects who performed motor-cognitive interventions were compared with those who performed only motor interventions or subjects who were in the passive control group; (3) the mean age of subjects was greater than 60 years (4) studies in which the effect of interventions was of interest if data were available.
Initially, we included subjects classified as “healthy” older adults with no specific diseases diagnosed and individuals with different diseases such as Parkinson's disease, balance impairment, mild cognitive impairment, osteoporosis, dementia, diabetes mellitus, Alzheimer's disease, and studies, that included either patients after stroke or hospitalized patients or patients with a history of falls, or osteoarthritic patients with balance impairment or older adults who were classified as frail or adults with various motor and cognitive deficits or residents of long-term-care facilities or patients with severe neurocognitive disorders. Because we found a high degree of heterogeneity within the groups diagnosed with a particular deficit, we decided to exclude from further analysis all studies that included diseased individuals. However, we have left a summary of all studies included in the original analysis in Supplementary Tables 1–4.
Three independent authors (KT, UM, and LŠ) conducted the search for available studies on a selected topic. The screening was performed in four steps. First, the titles were screened by the reviewers to determine whether they were suitable for our meta-analysis. Then, abstracts were assessed to determine whether the study topic met the selected inclusion and exclusion criteria. The inclusion criteria were selected as follows (as mentioned above) and are described in Table 1: the mean age of the participants was 60 years or more, the type of intervention was a motor-cognitive intervention, the comparison group was either passive or with included motor intervention, the outcomes of the studies were gait speed under a single- or a dual-task condition, TUG and BBS test and the study design was a RCT. The exclusion criteria were: no control group, irrelevant outcomes, unsuitable measurement of gait (e.g., measures were performed on a treadmill), inadequate results and unsuitable measurement of balance (e.g., measures were performed on a force plate). Third, the full text articles were read, the required information was selected and included (if appropriate) in the meta-analysis. Finally, the references of the included studies were reviewed for possible inclusion. If the full text of any paper was unavailable or the data of the study were incomprehensible (certain data on results were missing, e.g., standard deviation, or we were unable to deduce the value of the results from the reported data, e.g., data were reported in graphs), the corresponding author was contacted by email. Disagreements about the inclusion/exclusion of certain RCT were resolved by discussion or by a third person when no consensus could be reached (EdB, AP).
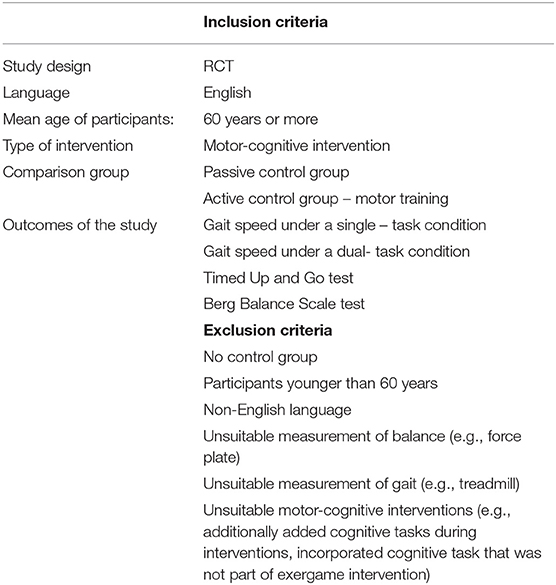
Table 1. Inclusion and exclusion criteria.
The Physiotherapy Evidence Database (PEDro) scale was used to assess the risk of bias and quality of included studies (Maher et al., 2003). This scale helps the reader to quickly assess whether a clinical trial presents reliable and meaningful results for use in clinical practice. Points are awarded only when a criterion is clearly met. In addition, points are awarded according to the specifics of the article and if the article meets those specifics (eligibility criteria were specified, subjects were randomly assigned to groups, assignment was concealed, the groups were similar at baseline regarding the most important prognostic indicators, there was blinding of all subjects, there was blinding of all therapist who administered the therapy, there was blinding of all assessors who measured at least one key outcome, measures of at least one key outcome were obtained from more than 85% of the subjects initially allocated to groups, all subjects from whom outcome measures were available received the treatment or control condition as allocated or, where this was not the case, data for at least one key outcome was analyzed by “intention to treat”, the results of between group statistical comparisons are reported for at least one key outcome). The quality assessment score was interpreted as follows: studies scoring 6–10 points on PEDro quality assessment were of “high quality”, studies scoring 4–5 of “fair quality” and studies scoring 0–3 of “poor quality”. The evaluation of the studies is available in Table 2.
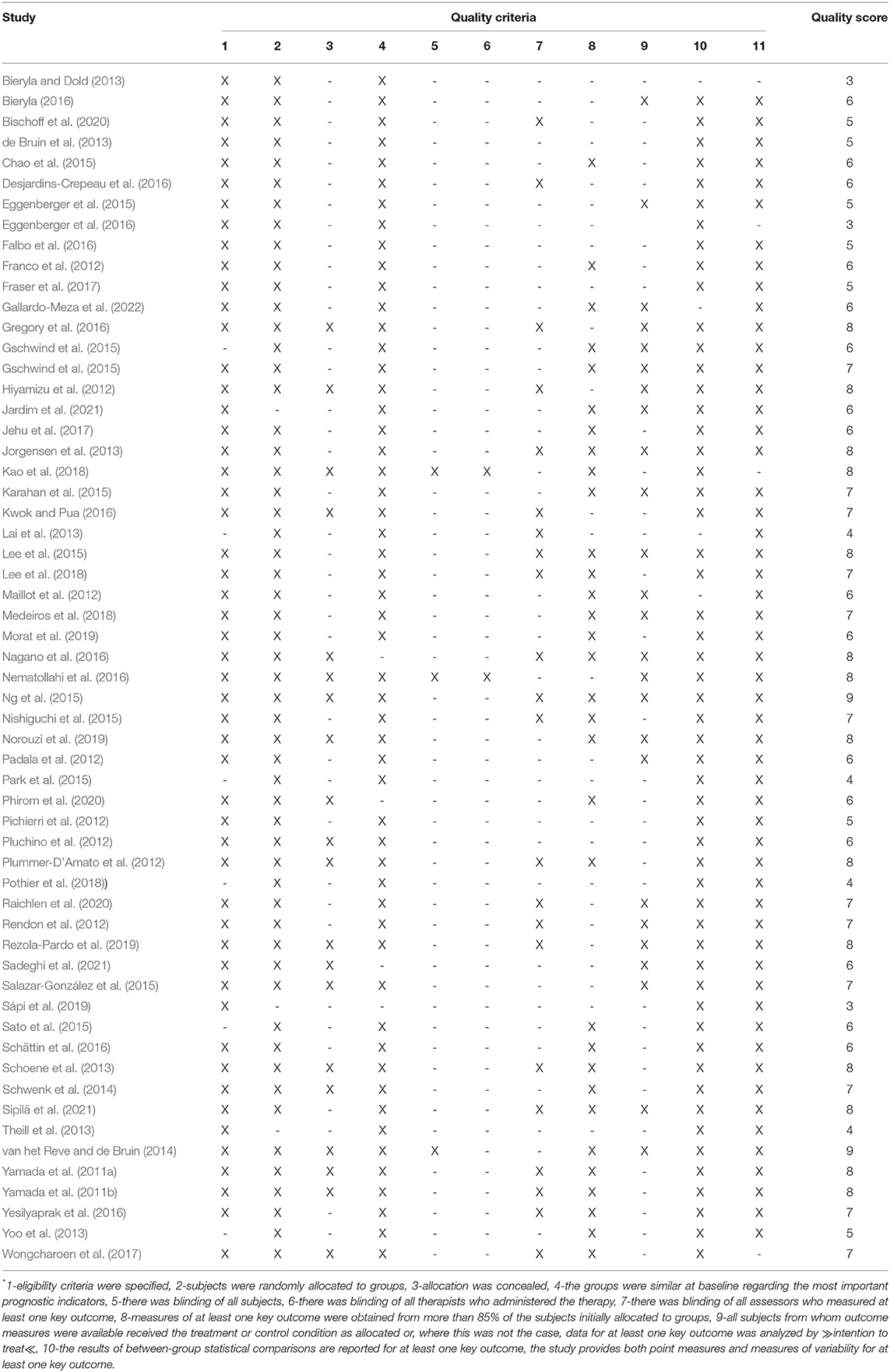
Table 2. Quality assessment of included studies with healthy older adults according to PEDro scale.
All included studies were divided into three groups (Tables 3–5) according to the type of dual-task intervention they performed. According to Herold's definition (Herold et al., 2018), we divided the studies into those that can be performed simultaneously or sequentially. Furthermore, studies that included training with a dual-task performed simultaneously were further divided into studies that performed simultaneous motor-cognitive training with additional cognitive task or those who performed simultaneous motor-cognitive training with incorporated cognitive task. In the category of simultaneous motor-cognitive training with an incorporated cognitive task, there were very few studies that did not use exergaming. We excluded the studies that did not meet the definition of exergaming and formed a group with exergaming studies only. The third group is therefore called exergaming.
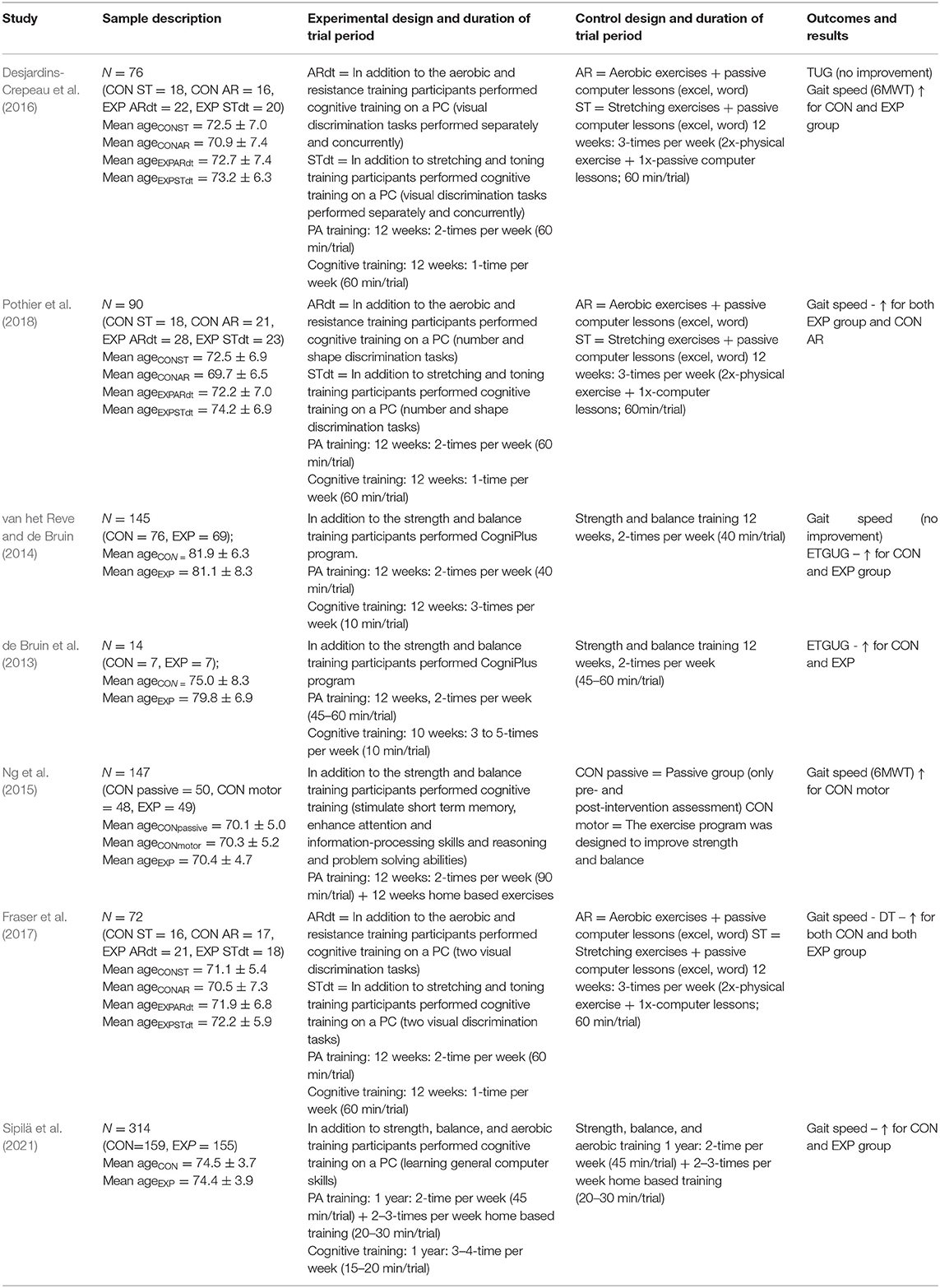
Table 3. Sequential motor-cognitive training.
The meta-analyses were performed using Comprehensive Meta-analysis software (version 3.0; Biostat Inc., Englewood, NJ, USA). The mean differences and 95% confidence intervals (Cls) were calculated for the included studies. We applied the random-effects model of the meta-analysis in all comparisons to determine the effect of the motor-cognitive intervention on gait and balance. Due to the high heterogeneity of the measured variables, the effect sizes were reported in Hedges-‘g. To calculate each effect size we used reported mean value of selected parameter, their standard deviation and sample size of the included study. The following established criteria were used to interpret the magnitude of motor-cognitive intervention for gait and balance improvements: trivial (<0.20), small (0.21–0.60), moderate (0.61–1.20), large (1.21–2.00), very large (2.01–4.00) and extremely large (>4.00) changes (Hopkins et al., 2009; Fraser et al., 2017; Wongcharoen et al., 2017; Laatar et al., 2018). Heterogeneity across studies was assessed using the I2 statistics, which is a measure of inconsistency used to quantify between-study variability. A value of 25% is recommended to represent low statistical heterogeneity, 50% moderate and 75% high statistical heterogeneity (Higgins, 2003). In addition, the sensitivity analysis excluded studies with poor methodological quality, i.e., the study's PEDro score was 3 or less. The publication bias was assessed by examining the asymmetry of the funnel plots using Egger's test (Egger et al., 1997; Sterne et al., 2011). Significant publication bias was considered if the p - value was < 0.10.
The Egger's test was performed to provide statistical evidence of funnel plot asymmetry (see Supplementary Figures 2A–D). The results indicated publication bias for TUG only (P = 0.003).
The initial search yielded 6,314 results. After duplicates were removed, 2,546 articles remained to be considered. After screening titles and abstracts, 890 records were excluded. Full-text reading of 351 articles revealed that 262 articles did not meet our inclusion criteria. We excluded 262 articles with the following reasons: no matched control group in the study (n = 44), unsuitable protocol (e.g., only intervention group, without control group) (n = 20), irrelevant outcomes (n = 32), unsuitable motor-cognitive interventions (e.g., additionally added cognitive tasks during interventions, incorporated cognitive task that was not part of exergame intervention) (n = 81), unsuitable measurement of gait (e.g., measures were performed on a treadmill) (n = 11), inadequate outcomes (n = 20), and unsuitable measurement of balance (e.g., measures were performed on a force plate) (n = 6) and not randomized controlled trials (n = 48). After excluding studies that included diseased older adults, there were 58 studies that we included in the quantitative synthesis. Details of the study selection process are presented in Supplementary Figure 1.
Based on the quality assessment, 44 out of 58 studies were high quality, 11 of fair quality and only 3 of low quality (Table 2). The intervention characteristics, including the type of intervention, a description of the motor and cognitive components and the frequency and dose of training described in the included studies are summarized in Tables 3–5. To facilitate the review of included studies, we have subdivided all studies according to the type of training performed by the experimental group (sequential motor-cognitive training, simultaneous motor cognitive training with additional cognitive task and exergaming).
We included 7 studies with sequential motor-cognitive training (presented in Table 3). These studies included samples ranging from 14 to 147 participants (range of age 69.7–81.9 years). The most common training approach (N = 6) was a combination of aerobic/resistance/strength/balance training and performing cognitive tasks on the PC.
There were 19 studies with simultaneous motor-cognitive training with an additional cognitive task (presented in Table 4). Studies included samples ranging from 17 to 286 participants, with the age of participants in both groups (experimental and control group) varying from 64.7 to 85.3 years. The most common training approach used was a combination of balance training while simultaneously performing different cognitive tasks (the number of studies with that type of training is 9).
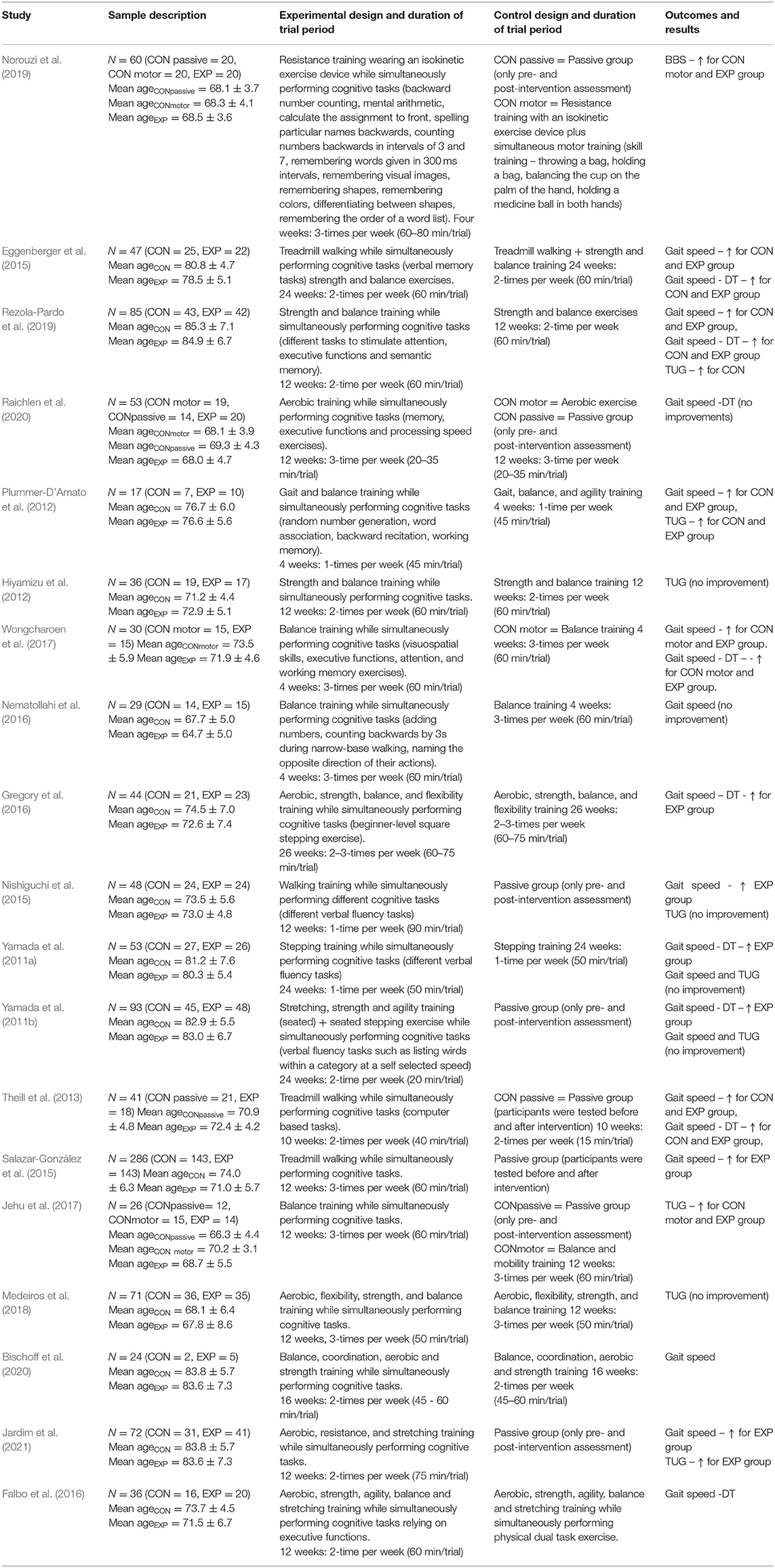
Table 4. Simultaneous motor-cognitive training with additional cognitive task.
We included 33 studies that performed exergaming (Table 5). Studies included samples ranging from 9 to 153 participants. The age range of participants in both groups (experimental and control) was between 65.2 and 86.9 years. The training approach in the studies included different types of interventions using PC and consoles with game controls, e.g., Nintendo Wii and Xbox Kinect, as one form of exergaming training offered to the participants.
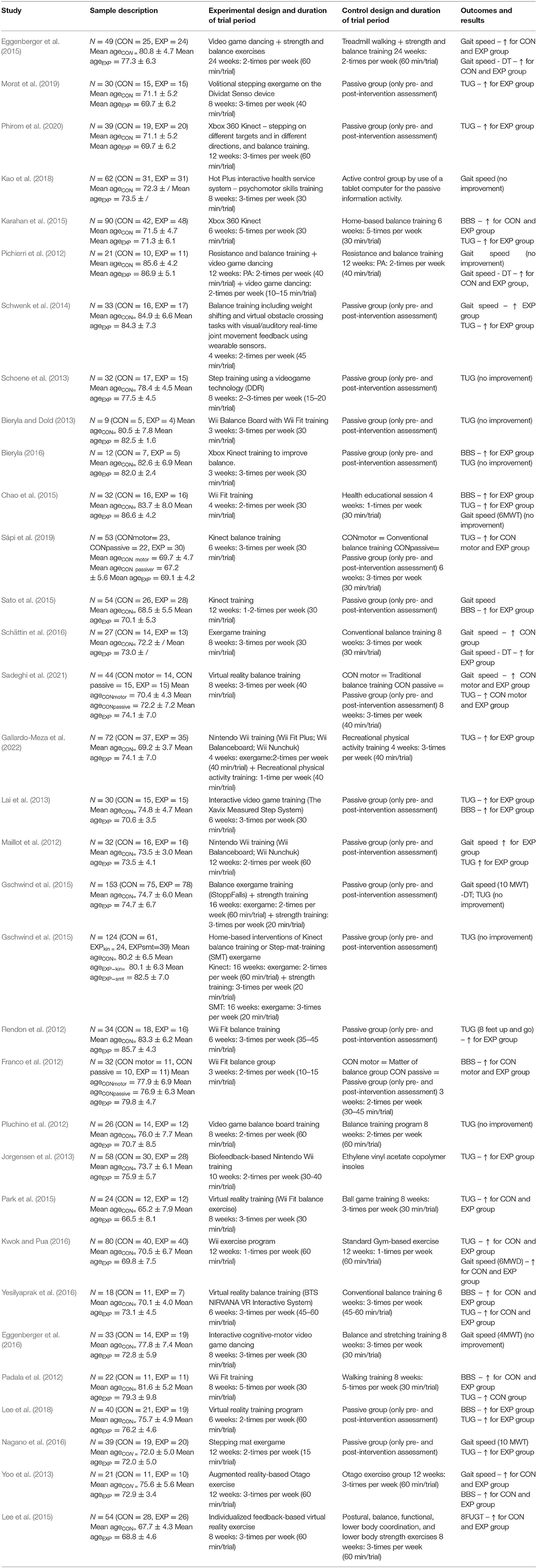
Table 5. Exergaming.
Forty-one studies (41 ESs) were included to assess the effect of motor-cognitive intervention on gait speed under a single-task condition. The results showed that the motor-cognitive intervention has a small positive effect on gait speed under a single-task condition (ES = 0.34, 95% Cl 0.12 to 0.57, P = 0.003). The effect of the intervention was moderated by the control group (Q = 6.203, P = 0.013); i.e., passive (ES = 0.941, 95% Cl 0.36 to 1.52, P = 0.001) vs. active (ES = 0.153, 95% Cl −0.07 to 0.38, P = 0.180). The type of intervention did not bring significant differences where additional, incorporated, and sequential intervention had the same effect on gait speed under a single task (Q = 0.668; P = 0.716). Even after excluding the study (Eggenberger et al., 2016) that had a low PEDro score (PEDro score = 3), the results showed a small positive effect of the motor-cognitive intervention on a gait speed under a single-task condition (ES = 0.35, 95% Cl 0.12 to 0.58, P = 0.003) and the effect of the intervention was moderated by the control group (Q = 6.067, P = 0.014); i.e., passive (ES = 0.941, 95% Cl 0.36 to 1.52, P = 0.001) vs. active (ES = 0.159, 95% Cl −0.07 to 0.39, P = 0.177). Moreover, once again the type of intervention did not bring significant difference on a gait speed under a single task (Q = 0.799; P = 0.671).
Twenty studies (20 ESs) were included to assess the effect of motor-cognitive intervention on gait speed under a dual-task condition. The results showed that the motor-cognitive intervention has no significant effect on gait speed under a dual-task condition (ES = 0.22, 95% Cl −0.01 to 0.44, P = 0.063). There was no significant difference between different control groups (Q = 0.003; P = 0.957) nor the type of intervention (Q = 0.213; P = 0.899).
Forty-one studies (41 ESs) were included to assess the effect of motor-cognitive intervention on TUG test. The results showed that the motor-cognitive intervention has a small positive effect on TUG (ES = 0.42, 95% Cl 0.21 to 0.63, P < 0.001). The effect of the intervention was moderated by the control group (Q = 4.92; P = 0.027); i.e., passive (ES = 0.73, 95% Cl 0.30 to 1.15, P = 0.001) vs. active (ES = 0.20, 95% Cl 0.03 to 0.38, P = 0.020), but not by the type of training (Q = 5.51; P = 0.064). After conducting sensitivity analysis by excluding two studies with low PEDro score (Bieryla and Dold, 2013; Sápi et al., 2019), the results still showed a small positive effect of the motor-cognitive intervention on TUG results (ES = 0.35, 95% Cl 0.15 to 0.55, P = 0.001) and the effect of the intervention was still moderated by the control group (Q = 4.280, P = 0.039); i.e., passive (ES = 0.619, 95% Cl 0.22 to 1.02, P = 0.003) vs. active (ES = 0.160, 95% Cl 0.001 to 0.320, P = 0.048). There was no significant difference between different types of intervention after excluding low quality studies.
Eleven studies (11 ESs) were included to assess the effect of motor-cognitive intervention on BBS score. The results showed that the motor-cognitive intervention has a small positive effect on BBS (ES = 0.59, 95% Cl 0.39 to 0.79, P < 0.001). There was no difference between active or passive control group (Q = 0.397; P = 0.529) and no difference between the type of intervention (Q = 0.299; P = 0.585).
The aim of the present systematic review and meta-analysis was to investigate whether motor-cognitive interventions can have a positive impact on selected gait and balance parameters in older adults. We contrasted the effects of passive and active control groups as well as three different types of motor-cognitive training. We focused on motor-cognitive interventions such as dual-task training and included studies with healthy older adults. Because of high heterogeneity in the studies performed in diseased older adults, we excluded them and performed the analysis only on healthy older people. To increase sensitivity, we additionally excluded three studies from the analysis that were of poor quality according to the PEDro assessment.
Overall, we found evidence that motor-cognitive interventions can improve gait speed under single-task condition, and measures of functional balance, but they have no significant effects on dual-task walking outcomes. However, motor-cognitive intervention does not necessarily have a better effect on gait speed under single-task improvement than active control group, which in this case is conventional motor training. On the other hand, there was a small but significant effect in favor of motor-cognitive interventions compared with other conventional motor interventions for TUG. Finally, we found that most studies conducted motor-cognitive training with additional cognitive tasks (n = 53), fewer studies conducted exergaming training (48). The least research has been conducted with sequential motor-cognitive training (n = 8). However, the studies differed in terms of intervention protocol, frequency, dosage of training, and sample size. Therefore, considerable heterogeneity was found among the included studies in terms of the methodology used. In the next sections we discuss the results per outcomes of interest in some more detail.
Our meta-analysis showed that motor-cognitive intervention can improve gait speed under single-task conditions. There was a small but significant effect that suggests that motor-cognitive interventions for this specific gait parameter may be beneficial for healthy older adults. However, further analysis showed that such interventions are no more effective than other conventional interventions in improving gait speed under a single-task conditions and that the type of motor-cognitive intervention is not a moderating factor for a positive effect.
Although walking was considered a fairly simple task until recently, it requires a large amount of higher-level cognitive input (Mirelman et al., 2018). For this reason, we hypothesized that motor-cognitive interventions would be more beneficial compared to motor training alone. The fact that motor-cognitive training does not contribute more to gait improvement in the active comparison groups than conventional forms of motor training alone is an important point to discuss. The finding is in line with one other systematic review (Gavelin et al., 2021) showing that the addition of cognitive training to physical exercise does not reduce physical efficacy of the training, and exergaming was only superior to passive control for both physical and cognitive outcomes. However, this review also found that motor-cognitive training is likely to be most effective for cognition.
The effect size of the overall improvement in gait speed under a single-task conditions was small, with high statistical heterogeneity between studies. Because of the great heterogeneity in the methods and measurements of the studies, more studies within each subgroup would be needed to draw definitive conclusions. When planning future motor-cognitive interventions, overall effectiveness is important and a deeper understanding of causation is needed (e.g., type and design of intervention, quality of research conducted). There were 27 studies in which motor-cognitive intervention had a positive effect and 14 studies in which motor-cognitive intervention had a negative effect. Among the studies with the positive effect, the highest effect of intervention had the study by Sadeghi et al. (2021) (quality score = 6/11, see Table 2). The experimental design of this study involved a motor-cognitive intervention with visual context displayed on a PC, a confirmed human-computer interaction with tasks performed dynamically. The effect of an intervention study conducted by Jardim et al. (2021) (quality score = 6/11), in which participants performed aerobic, resistance, and stretching training while simultaneously solving cognitive tasks, was similarly high. The third largest effect was in the study by Pothier et al. (2018) (quality score = 4/11), where participants in addition to the aerobic and resistance training, performed cognitive training on a PC. Taken together, analysis of studies with larger effect sizes did not identify any pure trends that could currently provide an answer to the most effective designs of motor-cognitive interventions.
Finally, an additional analysis was performed excluding the study by Eggenberger et al. (2016) due to poor quality (PEDro score ≤ 3). The exclusion of the study did not affect the final conclusion of the results, as the additional calculations only confirmed the results reported above.
We included twenty studies in the meta-analysis to evaluate the effect of a motor-cognitive intervention on gait speed under dual-task conditions, which yielded a non-significant effect. Regarding the quality (assessed by the PEDro scale) of the included studies, 6 studies were of “good quality” and 5 studies were of “fair quality”. Heterogeneity was moderate (82%), and the dual-task assessment methods varied considerably. When interpreting our non-significant results on gait speed under dual-task conditions, it should also be considered that dual-task walking used different cognitive tasks and were combined into one effect size (e.g., walking with n-back task, verbal fluency task, backward couniting, Go/No Go task). Therefore, future studies should investigate this effect considering different subcategories of cognition as a secondary task.
We found that motor-cognitive intervention has a small positive effect on TUG performance for healthy individuals. Moreover, our analysis showed that motor-cognitive intervention is more effective than other conventional interventions in improving the TUG test, but the type of motor-cognitive intervention is not a moderating factor for a positive effect.
The overall effect size was small, with the majority of included studies showing a positive effect of motor-cognitive intervention on TUG test. We included 41 studies, of which 33 had a positive effect size and 8 had a negative effect size. The three interventions related to TUG performance with high effect sizes differed in the type of motor-cognitive intervention as well as in the study quality ratings; one study conducted motor-cognitive training with an additional cognitive task (Jardim et al., 2021; quality score = 6/11). The experimental design included the simultaneous performance of aerobic, resistance, and stretching training, in addition to the performance of various cognitive tasks. Two studies conducted motor-cognitive training with an incorporated cognitive task (Sápi et al., 2019, quality score = 3/11, Kinect balance training; Sadeghi et al., 2021, quality score = 6/11, balance training in virtual reality). On the other hand, the highest negative effect was found by Medeiros et al. (2018) (quality score = 7/11), but it was still only a small negative effect. In the latter study, participants in the experimental group performed a combination of aerobic, flexibility, strength, and balance training while completing a cognitive task. The authors explained the negative effect by the type of the sample (participants had exercised before the intervention) and the relatively short duration of the intervention (12 weeks). Similar to gait speed under a single-task condition, no clear trend for the most effective design of motor-cognitive intervention can be derived for the TUG test.
In addition, the type of control group (passive vs. active) moderated the effects of motor-cognitive interventions, suggesting that motor-cognitive interventions are better able to improve multicomponent tasks of dynamic balance and mobility function as measured by the TUG. Indeed, both the passive and active control groups had a significant effect on the results. The effect of the passive control group was moderate, while the effect of the active control group was smaller, as expected (ES = small), but still statistically significant. Since TUG is a multicomponent test that examines balance, gait speed, and functional ability (Beauchet et al., 2011), it achieves higher ecological validity compared with less complex straight-line walking without an additional task. Motor-cognitive interventions could therefore be a promising strategy to improve dynamic balance and mobility in older adults. When performing a sub-analysis of different types of motor-cognitive interventions (although there was only a non-significant trend with P = 0.064), both the additional and incorporated interventions had a positive effect on TUG, but the sequential intervention did not. One possible explanation is that performing motor and cognitive tasks at different times (sequential motor-cognitive training) may not be as stimulating for improving complex movement tasks as performing these tasks simultaneously. In addition, Prosperini et al. (2021) conducted a meta-analysis in which they found that exergaming interventions can have a positive impact on the balance of people with neurological disorders. This study (Prosperini et al., 2021) was performed on a group of diseased older adults, and we cannot directly confirm our findings with the above-mentioned study, but related results may help us draw meaningful conclusions on this topic. That is, a motor-cognitive intervention with incorporated cognitive task or exergaming has already been shown to have a positive effect on the selected population.
In addition, our results were also confirmed by the exclusion of two studies that were considered to be of poor quality by the PEDro assessment (Bieryla and Dold, 2013; Sápi et al., 2019). Reanalysis confirmed a small but positive effect of motor-cognitive intervention on TUG scores and the effect of the intervention was still moderated by the control group.
The 11 studies included in our meta-analysis showed a positive but small effect on Berg Balance Scale scores (BBS). Thus, motor-cognitive intervention may be beneficial for healthy older adults while improving BBS score, but no differences were found between control groups or type of intervention. All included studies had a positive effect on BBS. The highest effect of the intervention was found in the studies by Karahan et al. (2015) (quality score = 7/11) and Norouzi et al. (2019) (quality score = 8/11). Participants in the experimental group in the study by Karahan et al. (2015) performed exergaming training, where they exercised on the Xbox 360 Kinect. The control group participated in balance training at home. On the other hand, participants in the experimental group in the study by Norouzi et al. (2019) performed resistance training using an isokinetic training device while performing cognitive tasks. Considering that BBS evaluates static and dynamic balance, the possible explanation for the results in favor of the control group could be the implementation of conventional physical therapy, that is motor training. The conventional motor training may have a better effect on balance parameters (BBS) than walking or playing video games. In addition, the existing literature summarizing the effect of simultaneous motor-cognitive training with incorporated cognitive task is inconsistent; Howes et al. (2017) and Pacheco et al. (2020) concluded that exergaming can improve static balance measured with BBS, whereas Chen et al. (2021) did not reach this conclusion.
There are also some limitations as well as future directions that should be mentioned. First, despite a high heterogeneity among motor-cognitive approaches in terms of the selected cognitive or motor task, duration, and frequency, we pooled and summarized the data for the meta-analysis. Second, our meta-analysis included participants with a mean age of 60 years, allowing for the possibility that some individuals in the studies were younger than this age. Third, the results of publication bias indicated the presence of bias in TUG and BBS outcomes. Future studies should focus on other aspects of functional mobility and examine the effectiveness of such motor-cognitive interventions on activities of daily living, such as navigating parks and grocery stores, ability to drive, and others. Finally, the current scarcity of literature on motor-cognitive interventions in specific disease populations may open new avenues of discussion for the implementation of such training. For example, technology-driven exergames with forms of extended reality (XR) that combine real and virtual environments and relate to human-machine interactions generated by computers and wearable technologies will provide services for remote monitoring, training, and telerehabilitation (Meulenberg et al., 2022). The nature of engagement in XR allows training and/or rehabilitation exercises to feel similar to physically performed actions, while seemingly being more engaging, motivating, and stimulating than conventional practice.
This systematic review and meta-analysis shows that conventional motor-cognitive interventions and technology-based exergames can improve performance-based measures of functional mobility in older adults. Our results show that motor-cognitive interventions can be effective, particularly in the multicomponent daily tasks that older adults encounter and that resemble the TUG test-mobility tasks of transferring from sitting to standing and walking, as well as balance tasks during walking, stopping, and turning. Because of substantial heterogeneity and the current limited availability of different types of interventions, conclusions should be drawn with caution. Further dose-response studies should be conducted to determine the appropriate training dose for this specific population. New insights into training design, as well as recent advances in immersive and wearable technology, offer a new perspective for implementing motor-cognitive interventions as more comprehensive training tools to improve functional mobility in the elderly and increase their effectiveness.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
KT and UM designed the research. KT, LŠ, and AP performed the data extraction and performed the meta-analysis. KT, EB, and UM drafted the manuscript. KT, LŠ, EB, AP, and UM edited and revised the manuscript. All authors approved the final version of the manuscript.
The authors acknowledge the financial support from the Slovenian Research Agency (research core funding No. P5-0381). This study was also supported by the European Union's Horizon 2020 research and innovation programme under grant agreement no. 952401 (TwinBrain – TWINning the BRAIN with machine learning for neuro-muscular efficiency).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank all the contacted corresponding authors of the manuscripts who provided feedback and raw data for the calculation of effect sizes.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2022.837710/full#supplementary-material
1. ^We found a high degree of heterogeneity within the groups diagnosed with a particular deficit, so we decided to exclude all studies that included diseased individuals from further analysis. However, we have left a summary of all studies included in the original analysis in Supplementary Tables 1–4.
Allen, N. E., Sherrington, C., Paul, S. S., and Canning, C. G. (2011). Balance and falls in Parkinson's disease: A meta-analysis of the effect of exercise and motor training: exercise and motor training for balance in PD. Movem. Diso. 26, 1605–1615. doi: 10.1002/mds.23790
Ambrose, A. F., Paul, G., and Hausdorff, J. M. (2013). Risk factors for falls among older adults: a review of the literature. Maturitas 75, 51–61. doi: 10.1016/j.maturitas.2013.02.009
American College of Sports Medicine. (2013). Exergaming. Available online at: http://healthysd.gov/wp-content/uploads/2014/11/exergaming.pdf (accessed April 30 2022).
Baltes, P. B., and Lindenberger, U. (1997). Emergence of a powerful connection between sensory and cognitive functions across the adult life span: a new window to the study of cognitive aging? Psychol. Aging. 12, 12–21. doi: 10.1037/0882-7974.12.1.12
Beauchet, O., Fantino, B., Allali, G., Muir, S. W., Montero-Odasso, M., and Annweiler, C. (2011). Timed up and go test and risk of falls in older adults: A systematic review. J. Nutr. Health Aging 15, 933–938. doi: 10.1007/s12603-011-0062-0
Beurskens, R., and Bock, O. (2012). Age-related deficits of dual-task walking: a review. Neural Plast. 2012, 1–9. doi: 10.1155/2012/131608
Bieryla, K., and Dold, N. (2013). Feasibility of Wii Fit training to improve clinical measures of balance in older adults. Clin. Intervent. Aging. 775. doi: 10.2147/CIA.S46164
Bieryla, K. A. (2016). Xbox Kinect training to improve clinical measures of balance in older adults: a pilot study. Aging Clin. Exper. Res. 28, 451–457. doi: 10.1007/s40520-015-0452-y
Bischoff, L. L., Cordes, T., Meixner, C., Schoene, D., Voelcker-Rehage, C., and Wollesen, B. (2020). Can cognitive-motor training improve physical functioning and psychosocial wellbeing in nursing home residents? A randomized controlled feasibility study as part of the PROCARE project. Aging Clin. Exper. Res. 33, 943–56. doi: 10.1007/s40520-020-01615-y
Chao, Y.-Y., Scherer, Y. K., Montgomery, C. A., Wu, Y.-W., and Lucke, K. T. (2015). Physical and psychosocial effects of wii fit exergames use in assisted living residents: a pilot study. Clin. Nurs. Res. 24, 589–603. doi: 10.1177/1054773814562880
Chen, Y., Zhang, Y., Guo, Z., Bao, D., and Zhou, J. (2021). Comparison between the effects of exergame intervention and traditional physical training on improving balance and fall prevention in healthy older adults: A systematic review and meta-analysis. J. NeuroEng. Rehabilit. 18, 164. doi: 10.1186/s12984-021-00917-0
de Bruin, E. D., van het Reve, E., and Murer, K. (2013). A randomized controlled pilot study assessing the feasibility of combined motor–cognitive training and its effect on gait characteristics in the elderly. Clin. Rehabil. 27, 215–225. doi: 10.1177/0269215512453352
Desjardins-Crepeau, L., Berryman, N., Fraser, S., Vu, T. T. M., Kergoat, M.-J., Li, K., et al. (2016). Effects of combined physical and cognitive training on fitness and neuropsychological outcomes in healthy older adults. Clin. Interv. Ag. 11, 1287–1299. doi: 10.2147/CIA.S115711
Eggenberger, P., Theill, N., Holenstein, S., Schumacher, V., and de Bruin, E. (2015). Multicomponent physical exercise with simultaneous cognitive training to enhance dual-task walking of older adults: A secondary analysis of a 6-month randomized controlled trial with 1-year follow-up. Clin. Interv. Ag. 1711. doi: 10.2147/CIA.S91997
Eggenberger, P., Wolf, M., Schumann, M., and de Bruin, E. D. (2016). Exergame and balance training modulate prefrontal brain activity during walking and enhance executive function in older adults. Front. Aging Neurosci. 8. doi: 10.3389/fnagi.2016.00066
Egger, M., Smith, G. D., Schneider, M., and Minder, C. (1997). Bias in meta-analysis detected by a simple, graphical test. BMJ. 315, 629–634. doi: 10.1136/bmj.315.7109.629
Falbo, S., Condello, G., Capranica, L., Forte, R., and Pesce, C. (2016). Effects of physical-cognitive dual task training on executive function and gait performance in older adults: a randomized controlled trial. BioMed. Res. Int. 2016, 1–12. doi: 10.1155/2016/5812092
Franco, J. R., Jacobs, K., Inzerillo, C., and Kluzik, J. (2012). The effect of the Nintendo Wii Fit and exercise in improving balance and quality of life in community dwelling elders. Technol. Health Care. 20, 95–115. doi: 10.3233/THC-2011-0661
Fraser, S. A., Li, K. Z.-H., Berryman, N., Desjardins-Crépeau, L., Lussier, M., Vadaga, K., et al. (2017). Does combined physical and cognitive training improve dual-task balance and gait outcomes in sedentary older adults? Front. Human Neurosci. 10. doi: 10.3389/fnhum.2016.00688
Fritz, N. E., Cheek, F. M., and Nichols-Larsen, D. S. (2015). Motor-cognitive dual-task training in persons with neurologic disorders: a systematic review. J. Neurol. Phys. Ther. 39, 142–153. doi: 10.1097/NPT.0000000000000090
Gallardo-Meza, C., Simon, K., Bustamante-Ara, N., Ramirez-Campillo, R., García-Pinillos, F., Keogh, J. W. L., et al. (2022). Effects of 4 weeks of active exergames training on muscular fitness in elderly women. J. Strength Condition. Res. 36, 427–432. doi: 10.1519/JSC.0000000000003560
Gavelin, H. M., Dong, C., Minkov, R., Bahar-Fuchs, A., Ellis, K. A., Lautenschlager, N. T., et al. (2021). Combined physical and cognitive training for older adults with and without cognitive impairment: a systematic review and network meta-analysis of randomized controlled trials. Age. Res. Rev. 66, 101232. doi: 10.1016/j.arr.2020.101232
Gregory, M. A., Gill, D. P., Zou, G., Liu-Ambrose, T., Shigematsu, R., Fitzgerald, C., et al. (2016). Group-based exercise combined with dual-task training improves gait but not vascular health in active older adults without dementia. Arch. Gerontol. Geriatr. 63, 18–27. doi: 10.1016/j.archger.2015.11.008
Gschwind, Y. J., Schoene, D., Lord, S. R., Ejupi, A., Valenzuela, T., Aal, K., et al. (2015). The effect of sensor-based exercise at home on functional performance associated with fall risk in older people – a comparison of two exergame interventions. Eur. Rev. Aging Phys. Activ. 12, 11. doi: 10.1186/s11556-015-0156-5
Herold, F., Hamacher, D., Schega, L., and Müller, N. G. (2018). Thinking while moving or moving while thinking – concepts of motor-cognitive training for cognitive performance enhancement. Front. Age. Neurosci. 10, 228. doi: 10.3389/fnagi.2018.00228
Heuninckx, S., Wenderoth, N., Debaere, F., Peeters, R., and Swinnen, S. P. (2005). Neural basis of aging: the penetration of cognition into action control. J. Neurosci. 25, 6787–6796. doi: 10.1523/JNEUROSCI.1263-05.2005
Higgins, J. P. T. (2003). Measuring inconsistency in meta-analyses. BMJ 327, 557–560. doi: 10.1136/bmj.327.7414.557
Hiyamizu, M., Morioka, S., Shomoto, K., and Shimada, T. (2012). Effects of dual task balance training on dual task performance in elderly people: A randomized controlled trial. Clin. Rehabil. 26, 58–67. doi: 10.1177/0269215510394222
Hopkins, W. G., Marshall, S. W., Batterham, A. M., and Hanin, J. (2009). Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exer. 41, 3–13. doi: 10.1249/MSS.0b013e31818cb278
Hortobágyi, T., Lesinski, M., Gäbler, M., VanSwearingen, J. M., Malatesta, D., and Granacher, U. (2016). Erratum to: effects of three types of exercise interventions on healthy old adults' gait speed: a systematic review and meta-analysis. Sports Med. 46, 453–453. doi: 10.1007/s40279-016-0498-9
Howes, S. C., Charles, D. K., Marley, J., Pedlow, K., and McDonough, S. M. (2017). Gaming for health: systematic review and meta-analysis of the physical and cognitive effects of active computer gaming in older adults. Phys. Ther. 97, 1122–1137. doi: 10.1093/ptj/pzx088
Jardim, N. Y. V., Bento-Torres, N. V. O., Costa, V. O., Carvalho, J. P. R., Pontes, H. T. S., Tomás, A. M., et al. (2021). Dual-task exercise to improve cognition and functional capacity of healthy older adults. Front. Age. Neurosci. 13, 589299. doi: 10.3389/fnagi.2021.589299
Jehu, D. A., Paquet, N., and Lajoie, Y. (2017). Balance and mobility training with or without concurrent cognitive training improves the timed up and go (TUG), TUG cognitive, and TUG manual in healthy older adults: an exploratory study. Aging Clin. Exper. Res. 29, 711–720. doi: 10.1007/s40520-016-0618-2
Jiang, Y., and Kanwisher, N. (2003). Common neural mechanisms for response selection and perceptual processing. J. Cogn. Neurosci. 15, 1095–1110. doi: 10.1162/089892903322598076
Jorgensen, M. G., Laessoe, U., Hendriksen, C., Nielsen, O. B. F., and Aagaard, P. (2013). Efficacy of nintendo wii training on mechanical leg muscle function and postural balance in community-dwelling older adults: a randomized controlled trial. J. Gerontol. A. 68, 845–852. doi: 10.1093/gerona/gls222
Kao, C.-C., Chiu, H.-L., Liu, D., Chan, P.-T., Tseng, I.-J., Chen, R., et al. (2018). Effect of interactive cognitive motor training on gait and balance among older adults: A randomized controlled trial. Int. J. Nurs. Stud. 82, 121–128. doi: 10.1016/j.ijnurstu.2018.03.015
Karahan, A. Y., Tok, F., Taşkin, H., Küçüksara,ç, S., Başaran, A., and Yildirim, P. (2015). Effects of exergames on balance, functional mobility, and quality of life of geriatrics versus home exercise programme: randomized controlled study. Central Eur. J. Public Health. 23, S14–S18. doi: 10.21101/cejph.a4081
Kwok, B. C., and Pua, Y. H. (2016). Effects of WiiActive exercises on fear of falling and functional outcomes in community-dwelling older adults: A randomised control trial. Age Age. 45, 621–627. doi: 10.1093/ageing/afw108
Laatar, R., Kachouri, H., Borji, R., Rebai, H., and Sahli, S. (2018). Combined physical-cognitive training enhances postural performances during daily life tasks in older adults. Exper. Gerontol. 107, 91–97. doi: 10.1016/j.exger.2017.09.004
Lai, C.-H., Peng, C.-W., Chen, Y.-L., Huang, C.-P., Hsiao, Y.-L., and Chen, S.-C. (2013). Effects of interactive video-game based system exercise on the balance of the elderly. Gait Posture 37, 511–515. doi: 10.1016/j.gaitpost.2012.09.003
Lauenroth, A., Ioannidis, A. E., and Teichmann, B. (2016). Influence of combined physical and cognitive training on cognition: a systematic review. BMC Geriatr. 16, 141. doi: 10.1186/s12877-016-0315-1
Law, L. L. F., Barnett, F., Yau, M. K., and Gray, M. A. (2014). Effects of combined cognitive and exercise interventions on cognition in older adults with and without cognitive impairment: a systematic review. Age. Res. Rev. 15, 61–75. doi: 10.1016/j.arr.2014.02.008
Lee, M., Son, J., Kim, J., and Yoon, B. (2015). Individualized feedback-based virtual reality exercise improves older women's self-perceived health: A randomized controlled trial. Arch. Gerontol. Geriatr. 61, 154–160. doi: 10.1016/j.archger.2015.06.010
Lee, S.-Y., Tung, H.-H., Liu, C.-Y., and Chen, L.-K. (2018). Physical activity and sarcopenia in the geriatric population: a systematic review. J. Am. Med. Direct. Assoc. 19, 378–383. doi: 10.1016/j.jamda.2018.02.003
Levin, O., Netz, Y., and Ziv, G. (2017). The beneficial effects of different types of exercise interventions on motor and cognitive functions in older age: a systematic review. Eur. Rev. Aging Phys. Activ. 14, 20. doi: 10.1186/s11556-017-0189-z
Li, K. Z. H., and Lindenberger, U. (2002). Relations between aging sensory/sensorimotor and cognitive functions. Neurosci. Biobehav. Rev. 26, 777–783. doi: 10.1016/S0149-7634(02)00073-8
Li, K. Z. H., Roudaia, E., Lussier, M., Bherer, L., Leroux, A., and McKinley, P. A. (2010). Benefits of cognitive dual-task training on balance performance in healthy older adults. J. Gerontol. A Biol. Sci. Med. Sci. 65A, 1344–1352. doi: 10.1093/gerona/glq151
Lord, S. R., Rogers, M. W., Howland, A., and Fitzpatrick, R. (1999). Lateral Stability, Sensorimotor Function and Falls in Older People. J. Am. Geriatr. Soc. 47, 1077–1081. doi: 10.1111/j.1532-5415.1999.tb05230.x
MacPherson, S. E. (2018). Definition: dual-tasking and multitasking. Cortex. 106, 313–314. doi: 10.1016/j.cortex.2018.06.009
Maher, C. G., Sherrington, C., Herbert, R. D., Moseley, A. M., and Elkins, M. (2003). Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 83, 713–721. doi: 10.1093/ptj/83.8.713
Maillot, P., Perrot, A., and Hartley, A. (2012). Effects of interactive physical-activity video-game training on physical and cognitive function in older adults. Psychol. Aging 27, 589–600. doi: 10.1037/a0026268
Manser, P., Thalmann, M., Adcock, M., Knols, R. H., and de Bruin, E. D. (2021). Can reactivity of heart rate variability be a potential biomarker and monitoring tool to promote healthy aging? a systematic review with meta-analyses. Front. Physiol. 12, 686129. doi: 10.3389/fphys.2021.686129
Marusic, U., and Grosprêtre, S. (2018). Non-physical approaches to counteract age-related functional deterioration: Applications for rehabilitation and neural mechanisms. Eur. J. Sport Sci. 18, 639–649. doi: 10.1080/17461391.2018.1447018
Marusic, U., Grosprêtre, S., Paravlic, A., Kova,č, S., Pišot, R., and Taube, W. (2018a). Motor imagery during action observation of locomotor tasks improves rehabilitation outcome in older adults after total hip arthroplasty. Neural Plast. 2018, 1–9. doi: 10.1155/2018/5651391
Marusic, U., Verghese, J., and Mahoney, J. R. (2018b). Cognitive-based interventions to improve mobility: a systematic review and meta-analysis. J. Am. Med. Direct. Assoc. 19, 484–491.e3. doi: 10.1016/j.jamda.2018.02.002
Masud, T., and Robert, O. M. (2001). Epidemiology of falls. Age Age. 30, 3–7. doi: 10.1093/ageing/30.suppl_4.3
Medeiros, L. B., Ansai, J. H., Buto, M. S., de, S., Barroso, V. D. V., Farche, A. C. S., et al. (2018). Impact of a dual task intervention on physical performance of older adults who practice physical exercise. Brazil. J. Kinanthropom. Human Perform. 20, 10–19. doi: 10.5007/1980-0037.2018v20n1p10
Meulenberg, C. J., de Bruin, E. D., and Marusic, U. (2022). A perspective on implementation of technology-driven exergames for adults as telerehabilitation services. Front. Psychol. 767. doi: 10.3389/fpsyg.2022.840863
Mirelman, A., Shema, S., Maidan, I., and Hausdorff, J. M. (2018). Gait. Handb. Clin. Neurol. 159, 119–134. doi: 10.1016/B978-0-444-63916-5.00007-0
Morat, M., Bakker, J., Hammes, V., Morat, T., Giannouli, E., Zijlstra, W., et al. (2019). Effects of stepping exergames under stable versus unstable conditions on balance and strength in healthy community-dwelling older adults: a three-armed randomized controlled trial. Exper. Gerontol. 127, 110719. doi: 10.1016/j.exger.2019.110719
Nagano, Y., Ishida, K., Tani, T., Kawasaki, M., and Ikeuchi, M. (2016). Short and long-term effects of exergaming for the elderly. SpringerPlus 5, 793. doi: 10.1186/s40064-016-2379-y
Nematollahi, A., Kamali, F., Ghanbari, A., Etminan, Z., and Sobhani, S. (2016). Improving balance in older people: a double-blind randomized clinical trial of three modes of balance training. J. Aging Phys. Activ. 24, 189–195. doi: 10.1123/japa.2014-0286
Ng, T. P., Feng, L., Nyunt, M. S. Z., Feng, L., Niti, M., Tan, B. Y., et al. (2015). Nutritional, physical, cognitive, and combination interventions and frailty reversal among older adults: a randomized controlled trial. Am. J. Med. 128, 1225–1236.e1. doi: 10.1016/j.amjmed.2015.06.017
Nishiguchi, S., Yamada, M., Tanigawa, T., Sekiyama, K., Kawagoe, T., Suzuki, M., et al. (2015). A 12-week physical and cognitive exercise program can improve cognitive function and neural efficiency in community-dwelling older adults: a randomized controlled trial. J. Am. Geriatr. Soc. 63, 1355–1363. doi: 10.1111/jgs.13481
Norouzi, E., Vaezmosavi, M., Gerber, M., Pühse, U., and Brand, S. (2019). Dual-task training on cognition and resistance training improved both balance and working memory in older people. Phys. Sportsmed. 47, 471–478. doi: 10.1080/00913847.2019.1623996
Pacheco, T. B. F., de Medeiros, C. S. P., de Oliveira, V. H. B., Vieira, E. R., and de Cavalcanti, F. A. C. (2020). Effectiveness of exergames for improving mobility and balance in older adults: a systematic review and meta-analysis. System. Rev. 9, 163. doi: 10.1186/s13643-020-01421-7
Padala, K. P., Padala, P. R., Malloy, T. R., Geske, J. A., Dubbert, P. M., Dennis, R. A., et al. (2012). Wii-fit for improving gait and balance in an assisted living facility: A pilot study. J. Aging Res. 2012:597573. doi: 10.1155/2012/597573
Paravlic, A. H., Pisot, R., and Marusic, U. (2019). Specific and general adaptations following motor imagery practice focused on muscle strength in total knee arthroplasty rehabilitation: a randomized controlled trial. PLOS ONE 14, e0221089. doi: 10.1371/journal.pone.0221089
Paravlic, A. H., Slimani, M., Tod, D., Marusic, U., Milanovic, Z., and Pisot, R. (2018). Effects and dose–response relationships of motor imagery practice on strength development in healthy adult populations: a systematic review and meta-analysis. Sports Med. 48, 1165–1187. doi: 10.1007/s40279-018-0874-8
Park, E.-C., Kim, S.-G., and Lee, C.-W. (2015). The effects of virtual reality game exercise on balance and gait of the elderly. J. Phys. Ther. Sci. 27, 1157–1159. doi: 10.1589/jpts.27.1157
Phirom, K., Kamnardsiri, T., and Sungkarat, S. (2020). Beneficial effects of interactive physical-cognitive game-based training on fall risk and cognitive performance of older adults. Int. J. Environ. Res. Public Health. 17, 6079. doi: 10.3390/ijerph17176079
Pichierri, G., Murer, K., and de Bruin, E. D. (2012). A cognitive-motor intervention using a dance video game to enhance foot placement accuracy and gait under dual task conditions in older adults: a randomized controlled trial. BMC Geriatr. 12, 74. doi: 10.1186/1471-2318-12-74
Pluchino, A., Lee, S. Y., Asfour, S., Roos, B. A., and Signorile, J. F. (2012). Pilot study comparing changes in postural control after training using a video game balance board program and 2 standard activity-based balance intervention programs. Arch. Phys. Med. Rehabil. 93, 1138–1146. doi: 10.1016/j.apmr.2012.01.023
Plummer, P., Zukowski, L. A., Giuliani, C., Hall, A. M., and Zurakowski, D. (2015). Effects of physical exercise interventions on gait-related dual-task interference in older adults: a systematic review and meta-analysis. Gerontology. 62, 94–117. doi: 10.1159/000371577
Plummer-D'Amato, P., Cohen, Z., Daee, N. A., Lawson, S. E., Lizotte, M. R., and Padilla, A. (2012). Effects of once weekly dual-task training in older adults: a pilot randomized controlled trial: Dual-task training in older adults. Geriatr. Gerontol. Int. 12, 622–629. doi: 10.1111/j.1447-0594.2011.00825.x
Pothier, K., Gagnon, C., Fraser, S. A., Lussier, M., Desjardins-Crépeau, L., Berryman, N., et al. (2018). A comparison of the impact of physical exercise, cognitive training and combined intervention on spontaneous walking speed in older adults. Aging Clin. Exper. Res. 30, 921–925. doi: 10.1007/s40520-017-0878-5
Prosperini, L., Tomassini, V., Castelli, L., Tacchino, A., Brichetto, G., Cattaneo, D., et al. (2021). Exergames for balance dysfunction in neurological disability: A meta-analysis with meta-regression. J. Neurol. 268, 3223–3237. doi: 10.1007/s00415-020-09918-w
Raichlen, D. A., Klimentidis, Y. C., Bharadwaj, P. K., and Alexander, G. E. (2020). Differential associations of engagement in physical activity and estimated cardiorespiratory fitness with brain volume in middle-aged to older adults. Brain Imaging Behav. 14, 1994–2003. doi: 10.1007/s11682-019-00148-x
Rendon, A. A., Lohman, E. B., Thorpe, D., Johnson, E. G., Medina, E., and Bradley, B. (2012). The effect of virtual reality gaming on dynamic balance in older adults. Age Age. 41, 549–552. doi: 10.1093/ageing/afs053
Rezola-Pardo, C., Arrieta, H., Gil, S. M., Zarrazquin, I., Yanguas, J. J., López, M. A., et al. (2019). Comparison between multicomponent and simultaneous dual-task exercise interventions in long-term nursing home residents: The Ageing-ONDUAL-TASK randomized controlled study. Age Age. 48, 817–823. doi: 10.1093/ageing/afz105
Sadeghi, H., Jehu, D. A., Daneshjoo, A., Shakoor, E., Razeghi, M., Amani, A., et al. (2021). Effects of 8 weeks of balance training, virtual reality training, and combined exercise on lower limb muscle strength, balance, and functional mobility among older men: A randomized controlled trial. Sports Health. 13, 606–612. doi: 10.1177/1941738120986803
Salazar-González, B. C., Cruz-Quevedo, J. E., Gallegos-Cabriales, E. C., Villarreal-Reyna, M. L. A., Ceballos-Gurrola, O., Hernandez-Cortez., et al. (2015). A physical-cognitive intervention to enhance gait speed in older mexican adults. Am. J. Health Promot. 30, 77–84. doi: 10.4278/ajhp.130625-QUAN-329
Sápi, M., Domjan, A., Kiss, A. F., and Pinter, S. (2019). Is kinect training superior to conventional balance training for healthy older adults to improve postural control?. Games Health J. 8, 41–48. doi: 10.1089/g4h.2018.0027
Sato, K., Kuroki, K., Saiki, S., and Nagatomi, R. (2015). Improving walking, muscle strength, and balance in the elderly with an exergame using kinect: A randomized controlled trial. Games Health J. 4, 161–167. doi: 10.1089/g4h.2014.0057
Schättin, A., Arner, R., Gennro, F., and de Bruin, E. D. (2016). Adaptations of prefrontal brain activity, executive functions, and gait in healthy elderly following exergame and balance training: A randomized-controlled study. Front. Aging Neurosi. 8:278. doi: 10.3389/fnagi.2016.00278
Schoene, D., Lord, S. R., Delbaere, K., Severino, C., Davies, T. A., and Smith, S. T. (2013). A randomized controlled pilot study of home-based step training in older people using videogame technology. PLoS ONE 8:e57734. doi: 10.1371/journal.pone.0057734
Schott, N. (2015). Trail Walking Test zur Erfassung der motorisch-kognitiven Interferenz bei älteren Erwachsenen: Entwicklung und Überprüfung der psychometrischen Eigenschaften des Verfahrens. Zeitschrift für Gerontol. Geriatr. 48, 722–733. doi: 10.1007/s00391-015-0866-3
Schwenk, M., Grewal, G. S., Honarver, B., Schwenk, S., Mohler, J., Khalsa, D. S., et al. (2014). Interactive balance training integrating sensor-based visual feedback of movement performance: A pilot study in older adults. J. Neuroeng. Rehabil 11:164. doi: 10.1186/1743-0003-11-164
Sipilä, S., Tirkkonen, A., Savikangas, T., Hanninen, T., Laukkanen, P., Alen, M., et al. (2021). Effects of physical and cognitive training on gait speed and cognition in older adults: A randomized controlled trial. Scand. J. Med. Sci. Sports 31, 1518–1533. doi: 10.1111/sms.13960
Smith, L., Gardner, B., Fisher, A., and Hamer, M. (2015). Patterns and correlates of physical activity behaviour over 10 years in older adults: prospective analyses from the English Longitudinal Study of Ageing. BMJ Open. 5, e007423. doi: 10.1136/bmjopen-2014-007423
Sterne, J. A. C., Sutton, A. J., Ioannidis, J. P. A., Terrin, N., Jones, D. R., Lau, J., et al. (2011). Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ. 343, d4002–d4002. doi: 10.1136/bmj.d4002
Theill, N., Schumacher, V., Adelsberger, R., Martin, M., and Jancke, L. (2013). Effects of simultaneously performed cognitive and physical training in older adults. BMC Neurosci. 14:103. doi: 10.1186/1471-2202-14-103
Tinetti, M. E. (2003). Preventing falls in elderly persons. New Engl. J. Med. 348, 42–49. doi: 10.1056/NEJMcp020719
van het Reve, E., and de Bruin, E. D. (2014). Strength-balance supplemented with computerized cognitive training to improve dual task gait and divided attention in older adults: a multicenter randomized-controlled trial. BMC Geriatr. 14:134. doi: 10.1186/1471-2318-14-134
Verghese, J., Mahoney, J., Ambrose, A. F., Wang, C., and Holtzer, R. (2010). Effect of cognitive remediation on gait in sedentary seniors. J. Gerontol. A Biol. Sci. Med. Sci. 65A, 1338–1343. doi: 10.1093/gerona/glq127
Wollesen, B., and Voelcker-Rehage, C. (2014). Training effects on motor-cognitive dual-task performance in older adults: A systematic review. Eur. Rev. Aging Phys Activ. 11, 5–24. doi: 10.1007/s11556-013-0122-z
Wongcharoen, S., Sungkarat, S., Munkhetvit, P., Lugade, V., and Silsupadol, P. (2017). Home-based interventions improve trained, but not novel, dual-task balance performance in older adults: a randomized controlled trial. Gait Posture 52, 147–152. doi: 10.1016/j.gaitpost.2016.11.036
Yamada, M., Aoyama, T., Hikita, Y., Takamura, M., Tanaka, Y., Kajiwara, Y., et al. (2011b). Effects of a DVD-based seated dual-task stepping exercise on the fall risk factors among community-dwelling elderly adults. Telemed. J. E. Health 17, 768–772. doi: 10.1089/tmj.2011.0054
Yamada, M., Aoyama, T., Tanaka, B., Nagai, K., and Ichihashi, N. (2011a). Seated stepping exercise in a dual-task condition improves ambulatory function with a secondary task: a randomized controlled trial. Aging Clin. Exp. Res. 23, 386–392. doi: 10.1007/BF03337763
Yesilyaprak, S. S., Yildirim, M. S., Tomruk, M., Ertekin, O., and Algun, Z. C. (2016). Comparison of the effects of virtual reality-based balance exercises and conventional exercises on balance and fall risk in older adults living in nursing homes in Turkey. Physiother. Theory Pract. 32, 191–201. doi: 10.3109/09593985.2015.1138009
Yoo, H., Chung, E., and Lee, B. -H. (2013). The effects of augmented reality-based otago exercise on balance, gait, and falls efficacy of elderly women. J. Phys. Ther. Sci. 25, 797–801. doi: 10.1589/jpts.25.797
Keywords: motor-cognitive intervention, dual-task, elderly, mobility, postural control
Citation: Teraz K, Šlosar L, Paravlić AH, de Bruin ED and Marusic U (2022) Impact of Motor-Cognitive Interventions on Selected Gait and Balance Outcomes in Older Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front. Psychol. 13:837710. doi: 10.3389/fpsyg.2022.837710
Received: 16 December 2021; Accepted: 25 April 2022;
Published: 16 June 2022.
Edited by:
Maurice Mohr, University of Innsbruck, AustriaReviewed by:
Alan Hartley, Scripps College, United StatesCopyright © 2022 Teraz, Šlosar, Paravlić, de Bruin and Marusic. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Eling D. de Bruin, ZWxpbmcuZGVicnVpbkBoZXN0LmV0aHouY2g=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.