 Víctor Manuel López-Guerra
Víctor Manuel López-Guerra Carla López-Núñez
Carla López-Núñez Silvia L. Vaca-Gallegos
Silvia L. Vaca-Gallegos Pablo V. Torres-Carrión
Pablo V. Torres-Carrión
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol., 29 April 2022
Sec. Quantitative Psychology and Measurement
Volume 13 - 2022 | https://doi.org/10.3389/fpsyg.2022.813894
Background: The Patient Health Questionnaire-9 (PHQ-9) is the most well-known self-report measure to screen for depressive symptomatology, although discerning which is the factor structure that represents the best fit remains a challenge.
Objective: The aim of this study was to analyze the psychometric properties and factorial structure of the Spanish version of the PHQ-9 in a large sample of Ecuadorian college students.
Methods: A total of 5,394 students (M = 22.03 years; SD = 3.05; 54.8% female) from three Ecuadorian universities were surveyed using a computerized questionnaire within a 4-week assessment period. The PHQ-9 was tested for factorial structure, reliability, and correlations with other mental health-related measures.
Results: The hierarchical model that included a general factor and three nested factors had a better fit, and such a hierarchical structure remained invariant across sex and age. Total omega value (ω) was 0.90 for the total scale and hierarchical omega values (ωh) were 0.68 for the general factor, as well as 0.34, 0.38, and 0.44 for the respective nested factors (somatic, cognitive/affective, concentration/motor). Moreover, PHQ-9 scores were significantly higher among women, although effect sizes of comparison of those sex differences were very small. Finally, the PHQ-9 scores correlated with multiple mental health indicators (psychological inflexibility, loneliness, stress, and satisfaction with life).
Discussion: The Spanish version of the PHQ-9 showed good psychometric properties among Ecuadorian college students. The hierarchical structure showed the best fit for the data, including not only a dominant general factor, but also the somatic, cognitive/affective and concentration/motor subcomponents. In conclusion, the PHQ-9 tool seems to represent an easy-to-implement screening questionnaire to design preventive programs for those Ecuadorian college students at risk of developing depressive disorders.
Depression is a common psychological disorder affecting more than 280 million people worldwide, as well as a leading cause of disability and overall global burden of disease (World Health Organization, 2021). In particular, unipolar depression represents the fifth leading cause of illness and death in low- and middle-income countries (LMICs) (Lopez and Mathers, 2013; Schantz et al., 2017). Latin America is one of the regions with the highest rates of depression, including Ecuador (Pan American Health Organization, 2018), a country where previous research has already highlighted high rates of moderate and severe symptoms within its specific cultural context (Yusim et al., 2009; Kohn et al., 2018). Overall, this impairing mental health condition is the source of immense human suffering (Adewuya et al., 2006; World Health Organization, 2021), and persons with major depression have a greater chance of dying prematurely than the general population due to unattended physical health problems and suicide (World Health Organization, 2013, 2021). Therefore, treating depression through integrated mental health and social care services in community-based settings represents a key global target (World Health Organization, 2013).
Entering university represents a critical period for developing depression as moving from high school to college means a difficult and stressful life transition, as these “emerging adults” (Thomas et al., 2017) could face new challenges such as leaving their homes, living with other students, loneliness, as well as economic and social problems (Weitzman, 2004; Cleary et al., 2011). Therefore, psychological distress and maladaptive adjustment to college could lead to the emergence of several mental health problems, mainly anxiety and depression disorders (e.g., Eisenberg et al., 2007; Vanstone and Hicks, 2019). In particular, it seems that college students usually meet higher rates of depression in comparison to the general population (Ibrahim et al., 2013), leading to academic and social disadvantages (e.g., Harrington et al., 1993; Adewuya et al., 2006).
A recent systematic review and meta-analysis (Akhtar et al., 2020) highlighted the high prevalence of depression among college students in LMICs. In Ecuador, transition to university may be especially challenging due to some cultural factors such as moving from rural areas to cities for the first time, adaptating to new values and cultural practices (especially among Indigenous populations; Martín-Díaz, 2017) or poverty, among others. In this context, previous research has also shown that there is a high prevalence of depressive symptomatology among college students in Ecuador that predicts in turn other health problems such as substance use and abuse (Ruisoto et al., 2016; Torres et al., 2017).
Despite the fact that there are effective psychological and pharmacological treatments for moderate and severe depression (World Health Organization, 2021), mental health practitioners need validated instruments in all socio-cultural contexts to effectively detect such symptomatology across the population (including college students). Previous research has shown that 76–85% of people in LMICs receive no treatment for their disorder (Wang et al., 2007; Evans-Lacko et al., 2018; World Health Organization, 2021), and one of the major barriers to effective care include inaccurate assessment. In this line, World Health Organization (2021) states that people who are depressed are often not correctly diagnosed, and others who do not have such disorder are misdiagnosed and prescribed antidepressants. This concern is also common in the Ecuadorian cultural context, where there is a lack of validated tools to both measure mental health (in general) and depression (in particular) among adult populations.
Overall, screening and proper identification of depression are necessary to address this public health problem in Ecuador. As previous authors recommend (Schantz et al., 2017), resource-limited settings (as Ecuador) should rely on self-report screening tools that are easier to implement than other time intensive and costly diagnostic interviews. Among different validated self-report tools, the Patient Health Questionnaire-9 (PHQ-9) is one of the most widely used measures for the screening of depression worldwide, in both primary care settings and research studies (Mitchell et al., 2016; Lamela et al., 2020). The PHQ-9 represents an easy-to-implement 9-item depression screening tool (Kroenke et al., 2001) based on the DSM-IV (Diagnostic and Statistical Manual of Mental Disorders IV-TR; American Psychiatric Association, 2000) criteria for Major Depressive Disorder (MDD). This self-report questionnaire allows one to establish depressive disorder diagnoses and also grade the severity of depressive symptoms, from minimal to severe depression (Kroenke et al., 2001). Therefore, the PHQ-9 represents an efficient instrument that requires much less time of clinicians than the original PRIME-MD (Primary Care Evaluation of Mental Disorders) interviews (Spitzer et al., 1994, 1999).
The PHQ-9 not only has been used through clinical care settings and practice (e.g., Diez-Quevedo et al., 2001; Kroenke et al., 2001; Petersen et al., 2015; Beard et al., 2016; Guo et al., 2017; González-Blanch et al., 2018) but also among research studies with non-clinical populations (e.g., Familiar et al., 2015; Boothroyd et al., 2019; Patel et al., 2019; Villarreal-Zegarra et al., 2019; Arnold et al., 2020; Shin et al., 2020), including college student subsamples (e.g., Adewuya et al., 2006; Granillo, 2012; Cassiani-Miranda et al., 2017; Keum et al., 2018; Miranda and Scoppetta, 2018; Kim and Lee, 2019; Huarcaya-Victoria et al., 2020). The Spanish version of the PHQ-9 instrument has previously been validated across several contexts and countries, such as Chile (Baader et al., 2012; Borghero et al., 2018; Saldivia et al., 2019), Honduras (Wulsin et al., 2002), Mexico (Familiar et al., 2015), Puerto Rico (González-Rivera, 2019), Peru (Huarcaya-Victoria et al., 2020), or Spain (Diez-Quevedo et al., 2001; Pinto-Meza et al., 2005; González-Blanch et al., 2018). Moreover, some studies have found good reliability and validity of the PHQ-9 when applied to Spanish-speaking Latinos in the United States (e.g., Huang et al., 2006; Donlan and Lee, 2010; Merz et al., 2011; Granillo, 2012).
Despite the fact that the PHQ-9 represents a useful instrument for the screening of depressive symptomatology among both clinical and non-clinical samples, there is a lack of consensus in previous studies regarding its factor structure and measurement invariance (Doi et al., 2018). Firstly, preceding research has highlighted a unidimensional factor structure (e.g., Hansson et al., 2009; Patel et al., 2019; Villarreal-Zegarra et al., 2019), but other studies found a bifactorial structure (somatic and cognitive/affective factors) (e.g., Chilcot et al., 2013; Petersen et al., 2015; Beard et al., 2016; Guo et al., 2017; Arnold et al., 2020; Shin et al., 2020). This controversy is also present in studies carried out with college students, as some authors (e.g., Keum et al., 2018; Kim and Lee, 2019) found a clear unidimensional structure, whereas other researchers (Granillo, 2012; Cassiani-Miranda et al., 2017; Miranda and Scoppetta, 2018) described a two-dimensional factor structure. On the other hand, PHQ-9 measurement invariance is supported across different studies (Lamela et al., 2020), however, there are scarce studies regarding the sex measurement invariance of this scale, especially among college student subsamples (e.g., Keum et al., 2018). In this regard, it should be noted that Spanish versions of the PHQ-9 have also shown disparate data regarding the factor structure and measurement invariance across different Spanish cultural contexts. While a one-factor structure predominates in Argentina (Urtasun et al., 2019), Chile (Baader et al., 2012; Borghero et al., 2018; Saldivia et al., 2019), Honduras (Wulsin et al., 2002), Mexico (Familiar et al., 2015), Puerto Rico (González-Rivera, 2019), Spain (Diez-Quevedo et al., 2001; González-Blanch et al., 2018), and Latino communities in the United States (Huang et al., 2006; Donlan and Lee, 2010; Merz et al., 2011), other studies support a two-factor structure, as is the case in Colombia (Miranda and Scoppetta, 2018), Peru (Huarcaya-Victoria et al., 2020), and the United States (for Latin female college students; Granillo, 2012). Of these studies, only four assessed measurement invariance across the following variables: gender (González-Blanch et al., 2018; Miranda and Scoppetta, 2018); age, marital status, education level, and employment situation over time (González-Blanch et al., 2018); English and Spanish-speaking groups (Merz et al., 2011); and Latinas and non-Latina White female groups (Granillo, 2012). Due to this, it is necessary to increase awareness of the measurement invariance of the PHQ-9 across some key clinical and sociodemographic variables (such as sex or age).
Due to its clinical importance, the PHQ-9 could represent a useful screening tool to early detect those college students at risk of developing depressive disorders, as previous authors have already highlighted through non-clinical college populations (e.g., Adewuya et al., 2006; Granillo, 2012). Nonetheless, studies in Ecuador are scarce and no validated screening tools in the country allow researchers and clinicians to reliably measure depression among college students. Moreover, following international guidelines for adapting tests across different cultures (Hambleton and Zenisky, 2011; Muñiz et al., 2013), it is necessary to examine both the factor structure and sex measurement invariance of the PHQ-9 in the specific Ecuadorian cultural context. With the purpose of overcoming these gaps in the literature, the aim of this study was to evaluate the psychometric properties and factor structure of the PHQ-9 for the assessment of depressive symptomatology among a non-clinical subsample of Ecuadorian college students.
College students from three universities in Ecuador were invited via email to participate in the study, and they then completed a computerized survey within the 4-week assessment period. The initial sample was made up of 5,996 students and 602 questionnaires were discarded due to being filled in randomly or being incomplete. The final sample included 5,394 participants who completed the entire questionnaire as well as reported a full academic year at any of the three institutions included (average response rate across universities was 47.80%, ranging from 39.10 to 56.10%). Mean age was 22.03 years (SD = 3.05; range from 17 to 58 years old), and 54.8% were women. Additionally, 50.9% of the participants included in the final sample came from public universities, 94.5% were single, and 78.9% were full-time students. Moreover, 90% of participants were mestizo (that is, mixed-raced), 5% were Indigenous, 1.7% were Afro-Ecuadorian, and 1.5% were White.
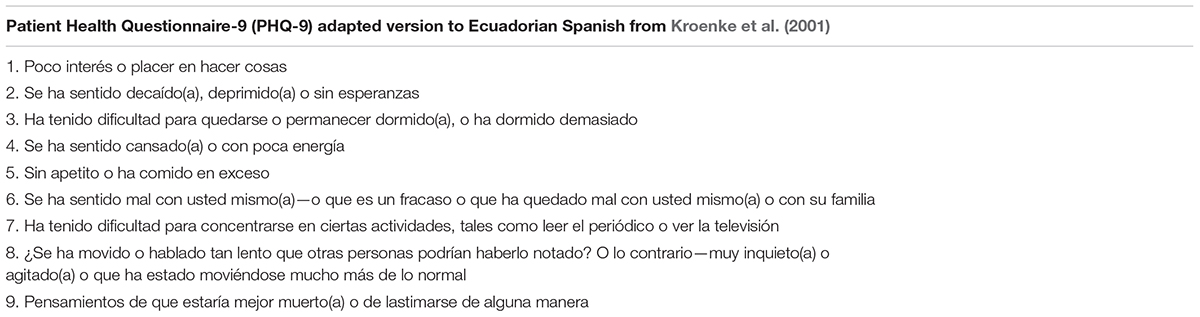
A descriptive cross-sectional study was conducted within the framework of a broader project of prediction of drug consumption among college students (CEPRA XII-2018-05) from three of the main universities in Ecuador: Universidad Técnica Particular de Loja (UTPL), Universidad Técnica del Norte (UTN), and Universidad Politécnica Salesiana (UPS). The study was approved by the Ethics Committee for Research in Human Beings (Comite de Ética de Investigación en Seres Humanos, UTPL-CEISH, March 6, 2019) of the UTPL Ecuador (UTPL-DIS-2019-0088-O) and was conducted according to the principles expressed in the Declaration of Helsinki (World Medical Association, 2013). Digital informed consent was obtained from all participants, who received personalized feedback on the results of their assessment. Prior to the final application of the online survey, the linguistic and cultural adaptation of the original PHQ-9 instrument into Ecuadorian Spanish language was tested on 30 participants as a pilot trial to test for the clarity and comprehensiveness of the questionnaire (see Appendix A). Overall, translation and adaptation processes of the scale were developed following the International Test Commission Guidelines—Second Edition (Hambleton and Zenisky, 2011; Muñiz et al., 2013).
Patient Health Questionnaire-9 (PHQ-9; Kroenke et al., 2001). This self-reported version of the PHQ is a 9-item depression module from the full PHQ (Spitzer et al., 1999) that assesses depressive symptomatology according to the DSM-IV criteria for Major Depressive Disorder (MDD). Participants had to fill out the questionnaire following the instruction of how they felt in the preceding 2 weeks with regards to different areas [anhedonia, sleep disturbance, fatigue, depressed mood, low self-esteem, concentration problems, psychomotor problems, appetite changes, and suicidal ideation; e.g., see Lamela et al. (2020)]. The PHQ-9 includes a 4-point scale (0 = “not at all”; 1 = “several days”; 2 = “more than half the days”; 3 = “nearly every day”) to measure severity of depression and its score ranges from 0 to 27. The global assessment of this scale represents the sum of the nine items’ scores and a higher score indicates a greater depression symptomatology. According to the authors of the original scale (Kroenke et al., 2001), scores can be used as a continuous assessment or as a diagnosis of major depression if 5 or more symptoms have been reported in the past 2 weeks at least “more than half the days,” and one of the symptoms is “anhedonia” or “depressed mood.” Besides, the authors recommend diagnosing other depression if 2–4 symptoms have occurred at least “more than half the days” in the past 2 weeks, and if “depressed mood” or “anhedonia” symptoms are selected. An example item is “Trouble falling or staying asleep, or sleeping too much.”
Acceptance and Commitment Questionnaire—II (AAQ-II; Bond et al., 2011). It is the most widely used general measure of psychological inflexibility and includes 7 items, to which participants must respond in a 7-point Likert-type scale, ranging from 1 = “never” to 7 = “always.” Scores of this scale range from 7 to 49, and higher scores indicate a tendency to act under the need to control or avoid aversive thoughts, memories, or feelings. The Spanish version of the AAQ-II (see Paladines-Costa et al., 2021) is characterized by a unifactorial structure that explains 66.87–70.03% of the total variance of the scale responses, a good internal consistency (α = 0.919 and ω = 0.928) and significant correlation with multiple health indicators (e.g., perceived stress). An example item would be “It seems like most people are handling their lives better than I am.” Medium to strong positive correlations were expected between the PHQ-9 and AAQ-II scores.
Loneliness Scale Revised- Short (UCLA-3; Hughes et al., 2004). This scale consists of a brief 3-item scale assessing the subjective feeling of loneliness, understood as the perception of less social support being available than desired. Scores range from 0 to 9, and participants should answer to a series of statements with 1 to 3 points (1 = “hardly ever,” 2 = “some of the time,” and 3 = “often”). Overall, higher scores indicate a greater feeling of loneliness or lack of social support. The internal consistency was good for both men (α = 0.75) and women (α = 0.84). The following item represents an example of this scale: “How often do you feel isolated from others?” Medium to strong positive correlations were expected between the PHQ-9 and UCLA-3 scores.
Perceived Stress Scale [PSS-10; Cohen et al., 1983; short version developed by Remor (2006)]. This 10-item scale evaluates the degree to which people perceive a lack of control in their daily lives. Scores range from 0 to 40 points, and participants should respond to a 5-point Likert-type scale, ranging from 0 (“never”) to 4 (“very often”). Higher scores indicate higher levels of psychological stress. This scale was both linguistic and culturally adapted in Ecuador by Ruisoto et al. (2020), finding good reliability (α = 0.85 and ω = 0.87), a bifactorial structure (which explains 56.99% of the total variance), as well as a satisfactory convergent validity with multiple health indicators (e.g., psychological inflexibility). An example item would be “In the last month, how often have you felt that you were unable to control important things in your life?” Medium to strong positive correlations were expected between the PHQ-9 and PSS-10.
Satisfaction with Life Scale [SWLS; Diener et al., 1985; Spanish adaptation conducted by Atienza et al. (2000)]. This 5-item instrument is aimed at assessing global cognitive judgments of one’s life satisfaction (not tapping related theoretical constructs such as positive affect or loneliness). The SWLS includes a 7-point Likert-type scale where answers range from 1 = “strongly disagree” to 7 = “strongly agree.” Overall ratings range from 5 to 35, and higher values indicate an increased satisfaction with one’s life. According to the authors of the original scale (Diener et al., 1985) some cut-offs could be followed as benchmarks: 5–9 = “extremely dissatisfied”; 10–14 = “dissatisfied”; 15–19 = “slightly dissatisfied”; 20 = “neutral”; 21–25 = “slightly satisfied”; 26–30 = “satisfied”; 31–35 = “extremely satisfied.” The psychometric properties of this unidimensional scale are adequate, being the internal consistency of the Spanish adaptation good (α = 0.84). An example item is: “So far I have gotten the important things I want in life.” Medium to strong negative correlations were expected between the PHQ-9 and SWLS scores.
The statistical analyses were carried out using the IBM Statistical Package for the Social Sciences (SPSS) software (IBM Inc., Chicago, IL, United States; version 26.0), AMOS version 25.0 (IBM Inc., Armonk, NY, United States) and Bifactor Indices Calculator: A Microsoft Excel-Based Tool to Calculate Various Indices Relevant to Bifactor CFA Models (Dueber, 2017).
Firstly, Kolmogorov–Smirnov normality and Levene’s homoscedasticity tests were conducted to test basic assumptions. Based on the distribution of the scores, a multivariate analysis of variance (MANOVA) test was also developed, offering the advantage of reducing type I error by assessing the sex differences of all items in the same analysis. Effect sizes of principal comparisons of sex differences were calculated using eta squared (η2), taking into account values for small (0.01–0.05), medium (0.06–0.13) and large (0.14) effects (Cohen, 1988).
Secondly, the factorial structure was analyzed by performing a confirmatory factor analysis (CFA), using the maximum likelihood method. The estimators of the goodness-of-fit were the Bentler comparative fit index (CFI), the Tucker–Lewis index (TLI), the root mean square error of approximation (RMSEA), the standardized root mean squared residual (SRMR), the chi ratio squared (χ2) by degrees of freedom (CMIN/DF), the Akaike information criterion (AIC), and the Bayesian information criterion (BIC). Good fitness of the model was considered if CFI and TLI ≥ 0.95, RMSEA ≤ 0.06, SRMR ≤ 0.08, and CMIN/DF ≤ 3. AIC and BIC were used to evaluate alternative models with the smaller value in each case indicating the best fitting model.
According to precedent literature using a CFA approach, we compared in our study the fit of six distinct and possible models of the Ecuadorian version of PHQ-9 (see Figure 1): Model 1, a unidimensional structure where each item is represented by a one-factor, therefore including the nine items assessed within a unique general factor (e.g., Baas et al., 2011; Yu et al., 2012; Bélanger et al., 2019); Model 2, a bidimensional model where the items are grouped into two-factors: somatic (includes three items, 3 = sleep difficulties, 4 = fatigue, 5 = appetite changes) and cognitive/affective (includes six items, 1 = anhedonia, 2 = depressed mood, 6 = feeling of worthlessness, 7 = concentration problems, 8 = moving or speaking slowly, 9 = suicidal ideation) (e.g., Patel et al., 2019; Lamela et al., 2020); Model 3 also represents a two-factor model but eliminates items 7 and 8 (that is, the cognitive/affective dimension only includes the remaining four items) (see Granillo, 2012); Model 4 represents a hierarchical structure that combines Models 1 and 2 as it includes two different nested factors (somatic and cognitive/affective) and a general factor that results from the sum of all item scores (see Doi et al., 2018); Model 5 also represents a hierarchical structure, by combining Models 1 and 3, and removing items 7 and 8; and finally Model 6, a hierarchical structure that combines a general factor and three nested factors (somatic, cognitive/affective, and concentration/motor). It should be noted that loadings of the two-item factor concentration/motor have been constrained to be equal prior to standardization in order to achieve identifiability.
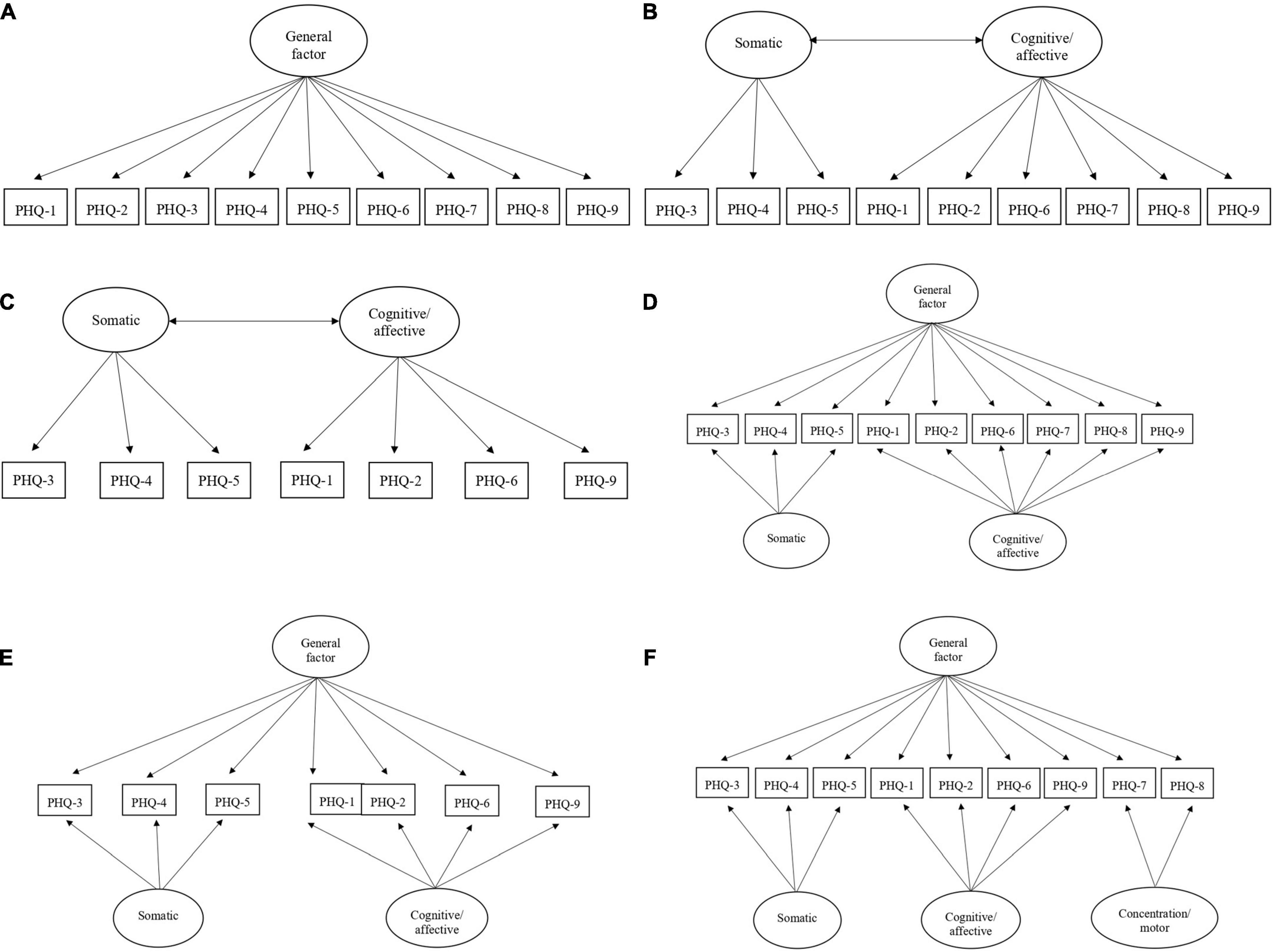
Figure 1. Tested models of the Ecuadorian version of PHQ-9. (A) Model 1. One-factor. (B) Model 2. Two-factors (somatic and cognitive/affective). (C) Model 3. Two-factors [somatic and cognitive/affective, but eliminating items 7 and 8; see Granillo (2012)]. (D) Model 4. Hierarchical structure that combines Models 1 and 2, including a general factor and two nested factors (somatic and cognitive/affective) (see Doi et al., 2018). (E) Model 5. Hierarchical structure that combines Models 1 and 3, eliminating items 7 and 8. (F) Model 6. Hierarchical structure that combines a general factor and three nested factors (somatic, cognitive/affective, and concentration/motor). PHQ-1, anhedonia; PHQ-2, depressed mood; PHQ-3, sleep difficulties; PHQ-4, fatigue; PHQ-5, appetite; PHQ-6, feeling of worthlessness; PHQ-7, concentration problems; PHQ-8, moving or speaking slowly; PHQ-9, suicidal ideation.
With the aim of assessing the hierarchical models, additional statistics such as ECV (Explained Common Variance), PUC (Percentage of Uncontaminated Correlations), replicability construct using H coefficient, omega coefficient (ω), and hierarchical omega coefficient (ωh) should be considered. Values greater than 0.70 for ECV and PUC support an essentially unidimensional structure of the PHQ-9 scale (Raykov and Hancock, 2005; Rodriguez et al., 2016). On the other hand, values included in the range 0.30–0.70 in ωh, H and ECV indexes reflect a substantive contribution of the factors or dimensions in explaining the construct variance; those values ≤ 0.30 indicate a poor contribution; and those values ≥ 0.70 indicate an excessive contribution (Moral et al., 2021).
Thirdly, we assessed the factorial invariance of the PHQ-9 across the total sample, taking into account the following models: configural invariance (Model configural, MC), which indicates a factorial structure without restrictions (baseline); metric invariance (Model metric, MM), where equivalence restrictions are established between factor loads; scalar invariance (Model Scalar, SC), that is, load and intercept equivalence restrictions; and strict invariance (Model Strict, ST), taking into account the equivalence restrictions of factor loads, intercepts, and residuals. Invariance tests for gender and age (<21 or >21 years old, that is, the median of the sample) were only planned for the best fitting model. We assessed the measurement invariance and its levels in accordance with the recommendations of Cheung and Rensvold (2002): ΔCFI ≤ 0.01 and ΔRMSEA ≤ 0.015.
Fourthly, internal consistency was analyzed based on omega coefficient (ω) and hierarchical omega coefficient (ωh), considering values ≥ 0.70 and 0.30 as satisfactory for ω and ωh, respectively. Finally, convergent and divergent validities were analyzed based on Pearson’s correlation (r) between the PHQ-9 scores and those scale’s ratings corresponding to different well-established psychological health indicators (psychological inflexibility, loneliness, perceived stress, and satisfaction with life). The size of Pearson’s correlation (r) values can range from 0.10 to 0.29 (small), 0.30 to 0.49 (medium), and 0.50 to 1.0 (large) (Cohen, 1988). In particular, r = 0.50–0.69 represents a strong value, r = 0.70–0.89 represents a very strong value, and ≥0.90 means that the relationship between the variables is perfect (Byrne, 2016).
Firstly, we assessed whether the PHQ-9 scores differed by sex. Overall, female participants reported significantly higher scores for depression (M = 6.86; SD = 5.92) than male ones (M = 5.81; SD = 5.42) on the total score (F = 45.515; p < 0.001; η2 = 0.008). Such statistically significant differences were also found throughout most PHQ-9 items, except for items 8 (referring to “moving or speaking slowly”) and 9 (referring to “suicidal ideation”). Nonetheless, effect sizes of comparison of such sex differences were very small and insignificant (see Table 1).
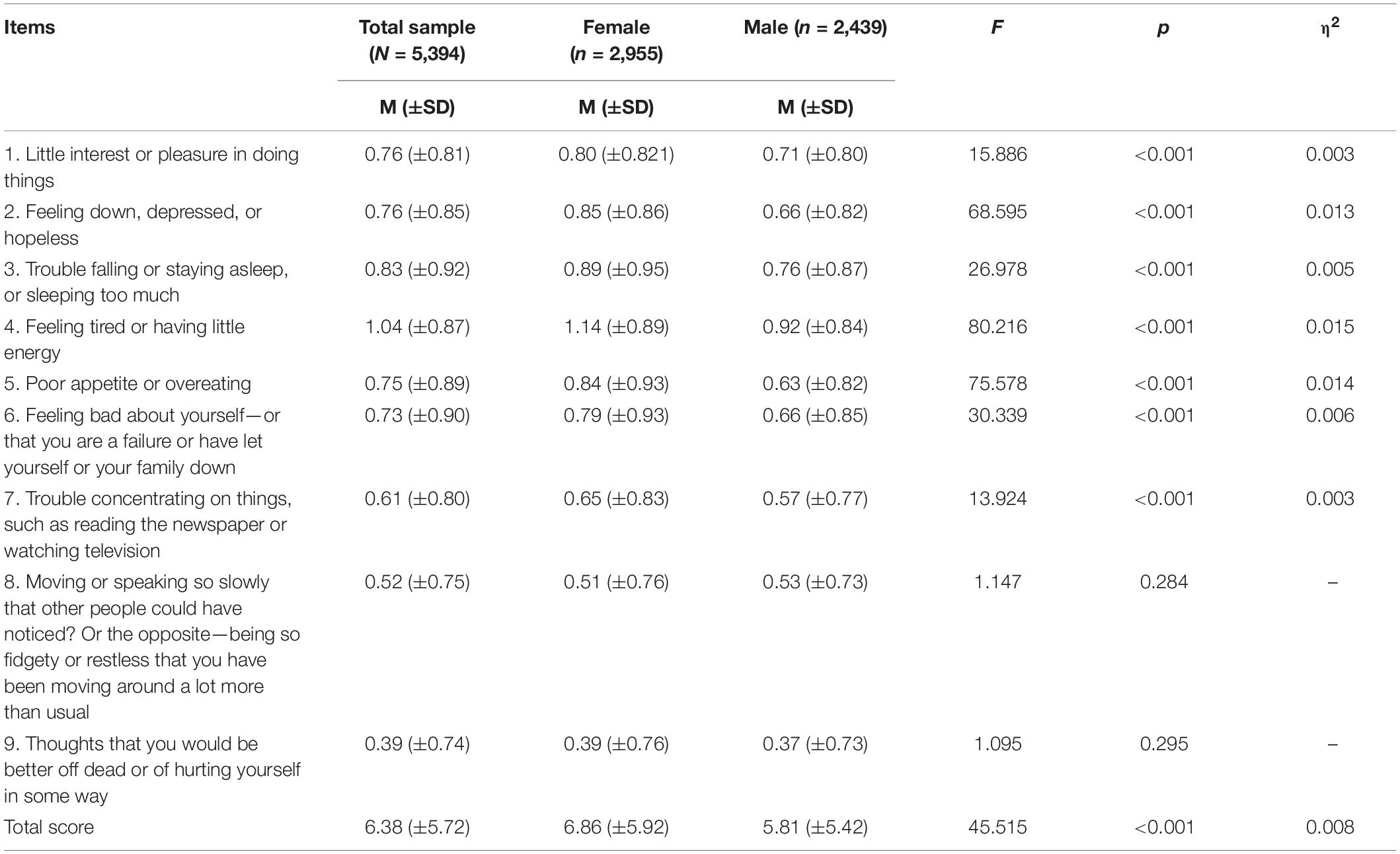
Table 1. Sex differences in Patient Health Questionnaire-9 (PHQ-9) scores (item by item).
With the aim of determining the PHQ-9 factor structure, we compared the goodness-of-fit indexes of six distinct factor models of the Ecuadorian Spanish version of the scale (see Figure 1): one-factor structure (Model 1); bi-factor structure (somatic and cognitive/affective dimensions; Model 2); bi-factor structure (somatic and cognitive/affective dimensions) without items 7 and 8 (Model 3); hierarchical structure that combines Models 1 and 2 (Model 4); hierarchical structure that combines Models 1 and 3, and removing items 7 and 8 (Model 5); and hierarchical structure that combines a general factor and three nested factors (somatic, cognitive/affective, and concentration/motor) (Model 6).
The CFI, TIL, RMSEA, SRMR, and CMIN/DF goodness-of-fit indexes of Models 1–5 were not as adequate as those presented by Model 6 (CFI = 0.996; TLI = 0.947; RMSEA = 0.036; SRMR = 0.008 CMIN/DF = 8.185; AIC = 182.721; BIC = 380.562) (see Table 2), although that model showed higher values for both AIC and BIC indicators when compared to Model 5 (AIC = 167.037; BIC = 167.102). Nevertheless, it is well-known that the AIC y BIC have explicit penalties for model complexity, and, in our analyses, Model 6 was definitely more complex that Model 5.
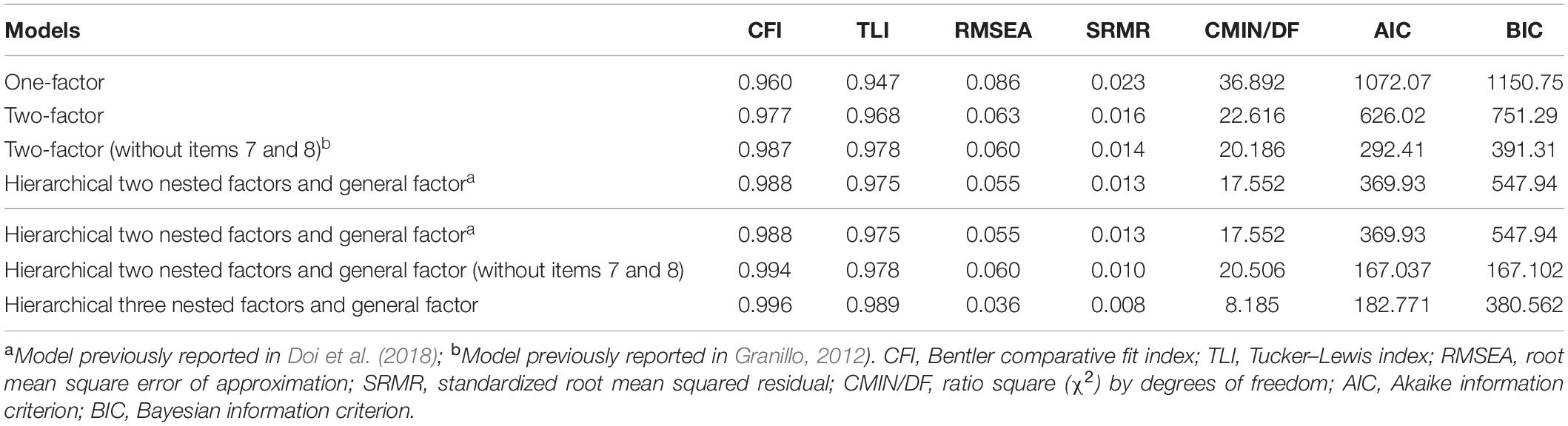
Table 2. Goodness-of-fit indexes for the confirmatory factor analysis (n = 5,394).
On the other hand, the additional assessment of the hierarchical models revealed that all factor loadings of Model 6 were greater than 0.30 and positive, in contrast to Models 4 and 5 (see Figure 2). The ECV values of the general and specific factors (see Table 3) suggested that Model 4 is essentially unidimensional, progressively increasing such multidimensionality in hierarchical solutions 5 and 6. That is, the percentage of the variance explained by the nested factors increased and the one explained by the general factor decreased. Specifically, the general factor of Model 6 explained the 52.8% of variance of depressive symptoms, and the three nested factors explained the 13.6, 21, and 12.6%, respectively. Model 6 also showed satisfactory ωh and H indexes (ranging in the interval 0.30–0.70), suggesting a substantive contribution not only of the general factor but also of the nested factors in explaining the variance of depression. In addition, the increase in PUC (>0.70) in Model 6 indicates that structural coefficients are relatively unbiased.
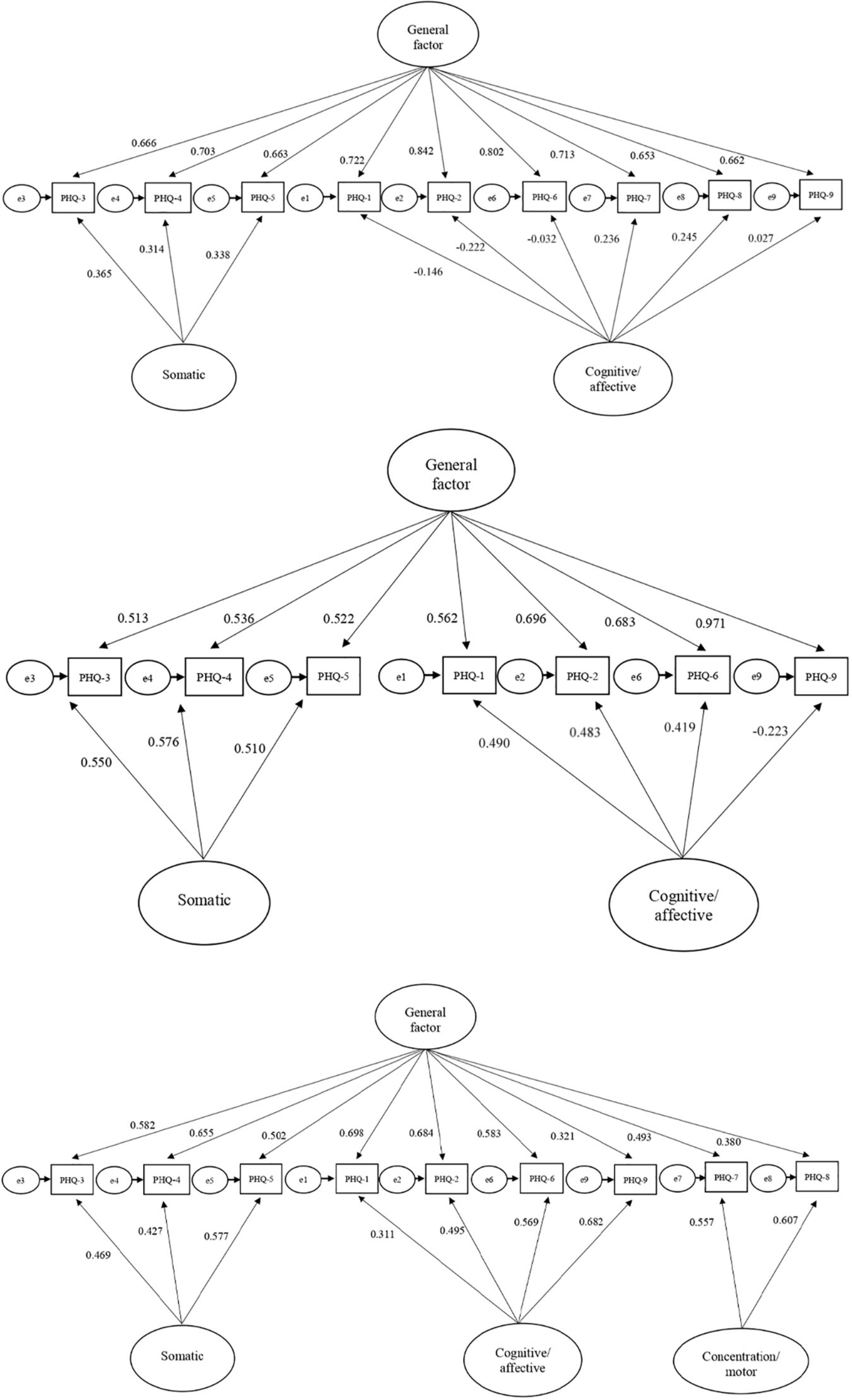
Figure 2. Patient Health Questionnaire-9 (PHQ-9) hierarchical models (Model 4, Model 5, and Model 6). Model 4. Hierarchical structure that combines Models 1 and 2, including two nested factors (somatic, cognitive/affective) and a general factor that results from the sum of all item scores (see Doi et al., 2018). Model 5. Hierarchical structure that combines Models 1 and 3, eliminating items 7 and 8. Model 6. Hierarchical structure that combines a general factor and three nested factors (somatic, cognitive/affective, and concentration/motor). PHQ-1, anhedonia; PHQ-2, depressed mood; PHQ-3, sleep difficulties; PHQ-4, fatigue; PHQ-5, appetite; PHQ-6, feeling of worthlessness; PHQ-7, concentration problems; PHQ-8, moving or speaking slowly; PHQ-9, suicidal ideation.
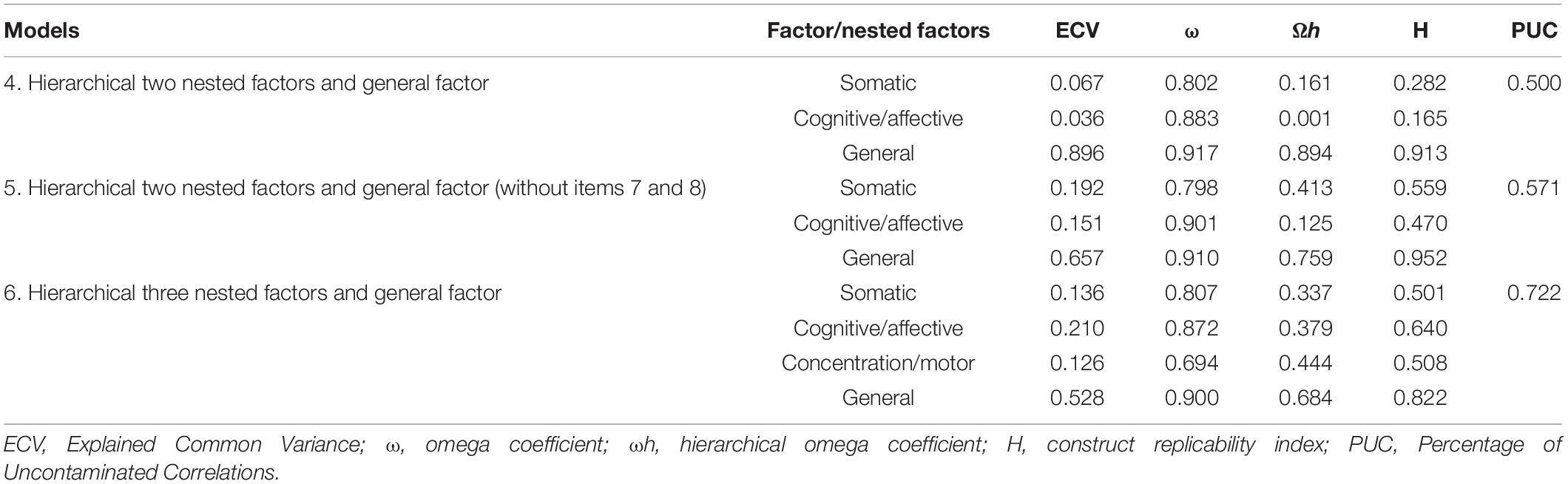
Table 3. Hierarchical model indexes (n = 5,394).
The adjustment indexes of the hierarchical Model 6 (for both the total sample and separated by sex) are presented in Table 4, showing an adequate fit in each of them. On the one hand, the configural invariance (MC) presented good fit indicators (χ2(30) = 140.521; CFI = 0.995 and RMSEA = 0.026 [0.022–0.031]). Similarly, the metric invariance (MM) resulted on good fit indexes (χ2(44) = 182.527; CFI = 0.994; RMSEA = 0.024 [0.021–0.028]), being similar to the MC values since they showed minimal differences (ΔCFI = 0.001 and ΔRMSEA = −0.002). These results indicate that the factorial loads are invariant between the subsamples of men and women and, therefore, the covariances can be compared. On the other hand, the scalar invariance (SC) demonstrated indexes equal to the previous model (χ2(51) = 420.468; CFI = 0.993; RMSEA = 0.025 [0.022–0.028]) without minimal differences (ΔCFI = 0.001 and ΔRMSEA = 0.001), assuming the invariance between the different thresholds. Finally, the strict invariance (ST) reflects a good fit (χ2(60) = 262.937; CFI = 0.992; RMSEA = 0.025 [0.022–0.028]), showing no differences (ΔCFI = −0.001 and ΔRMSEA = 0) and verifying the invariance of the residuals. Overall, the combined results demonstrated the factorial invariance of the Ecuadorian version of the PHQ-9 across sex (both male and female college students) as well as across age (see Table 5).
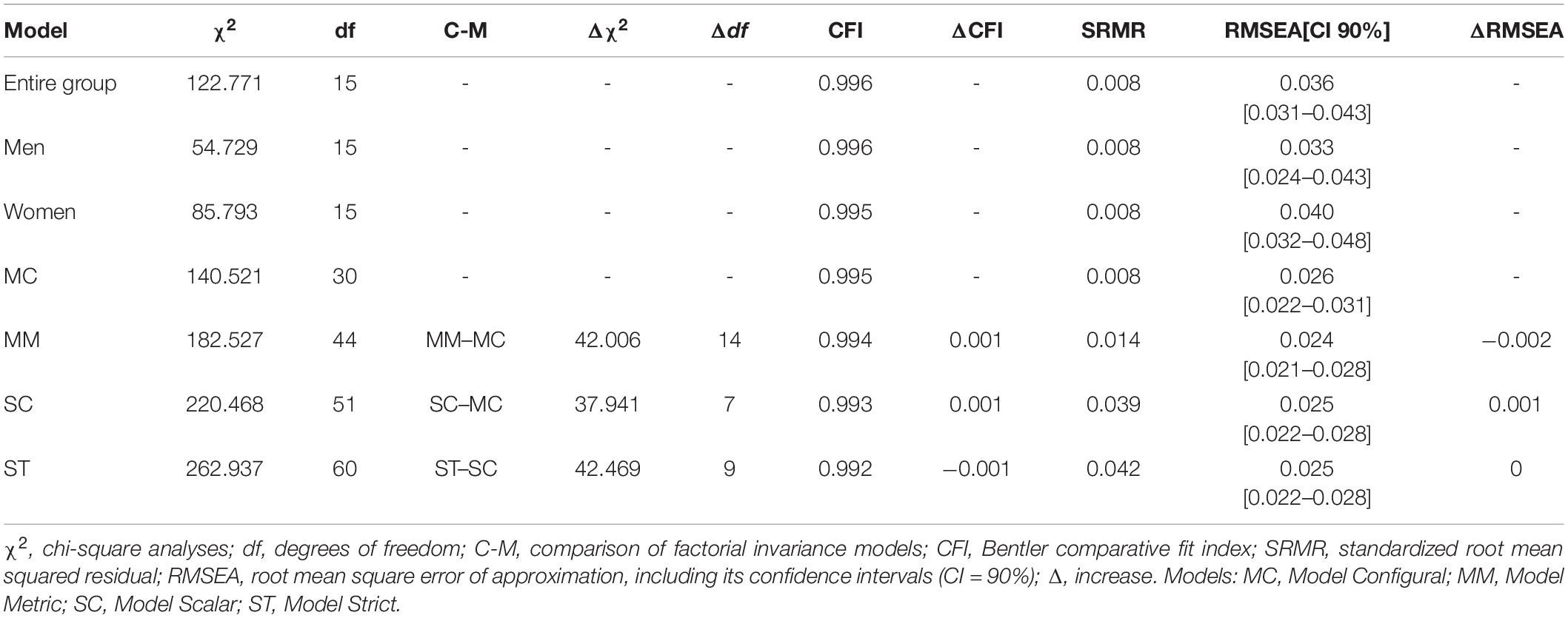
Table 4. PQH-9 factorial invariance for the total sample and by sex.
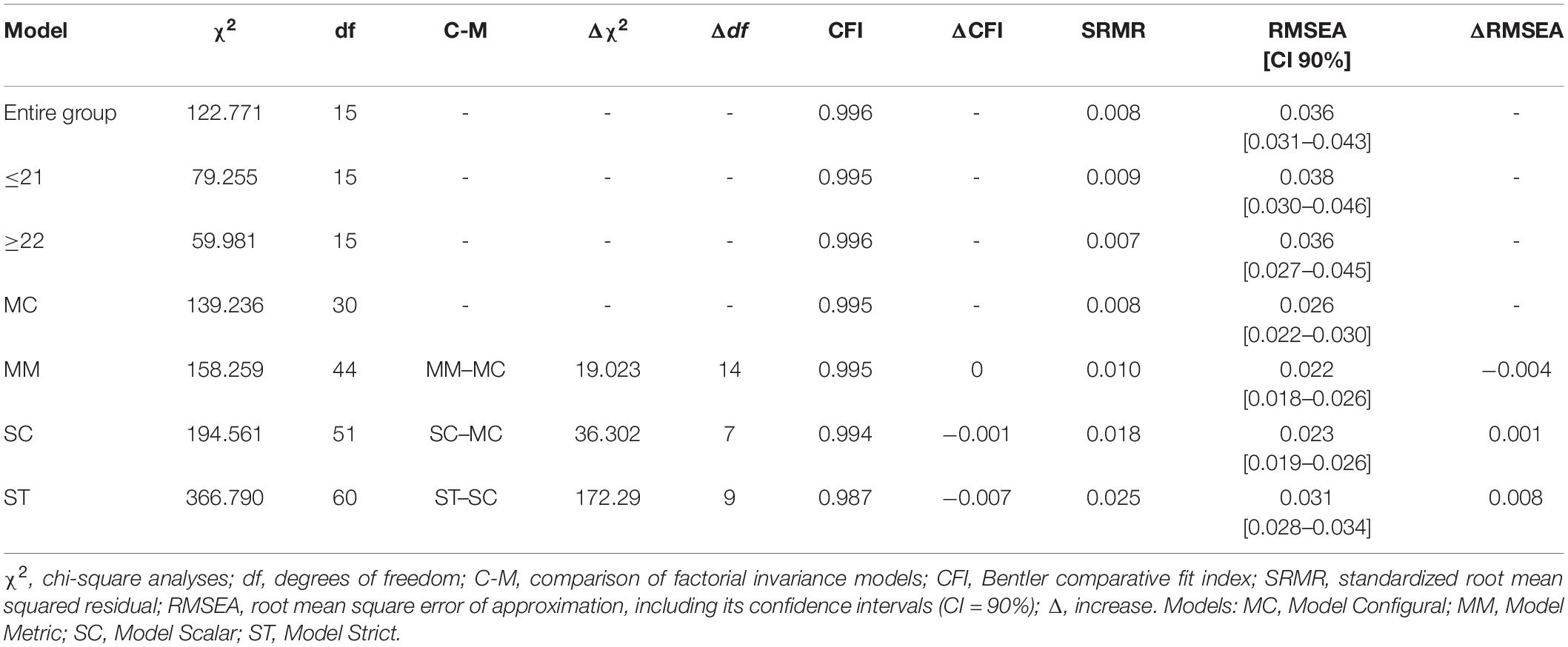
Table 5. PQH-9 factorial invariance for the total sample and by age.
The internal consistency of the hierarchical Model 6 of the PHQ-9 scale showed satisfactory outcomes for both the total scale (ω = 0.90, ωh = 0.68) and its three nested factors: somatic (ω = 0.81, ωh = 0.34), cognitive/affective (ω = 0.87, ωh = 0.38) and concentration/motor (ω = 0.69, ωh = 0.44). Regarding convergent validity, we conducted correlation analyses between PHQ-9 scores and some of the most relevant mental health factors. The main results (see Table 6) showed positive and statistically significant relationships between depressive symptomatology scores and psychological inflexibility, loneliness, and perceived stress (p < 0.01). Convergent validity analyses also demonstrated negative and statistically significant associations between PHQ-9 scores and satisfaction with life (p < 0.01). Most of the effect sizes of PHQ-9 on the mental health indicators were moderate or large (r > 0.50).

Table 6. Correlation matrix between Patient Health Questionnaire-9 (PHQ-9) scores and other psychological health-related measures.
The main goal of the present study was to analyze the psychometric properties and factor structure of the PHQ-9 for the assessment of depression among a non-clinical subsample of Ecuadorian college students. To our knowledge, no research had previously evaluated both the psychometric properties and factor structure in the Ecuadorian culture. Overall, results showed the adequate psychometric properties of the Ecuadorian Spanish version of the scale and demonstrated that the bifactorial model had a better fit than the unidimensional did. Specifically, our findings not only support the presence of a dominant general factor but also suggest the existence of two distinct subcomponents (somatic and a cognitive/affective), remaining such a structure invariant across sex.
Firstly, results regarding depressive symptomatology across the sample showed low-to-middle scores, with females obtaining significantly higher scores compared to males. Previous studies have already highlighted that youth in LMICs are vulnerable to mental health issues (Pan American Health Organization, 2018; Akhtar et al., 2020) and Latin America is one of the regions with elevated rates of depressive symptomatology, including Ecuador among the top five countries that show higher rates of disability due to depression (Yusim et al., 2009; Pan American Health Organization, 2018). Moreover, our findings are in line with precedent research (e.g., Kuehner, 2017; World Health Organization, 2017; Tibubos et al., 2021) showing that depressive symptomatology is higher among females when compare to males, not only among the general population (e.g., Hyde et al., 2008; Parker and Brotchie, 2010; Salk et al., 2017) but also within the university context (Adewuya et al., 2006; Bitsika et al., 2010; Torres et al., 2017). In particular, depressive symptomatology in males could be related to violence, drug use and an increased risk of suffering somatic diseases, while women could express symptoms such as negative emotions, anhedonia or guilt, among others (Tibubos et al., 2021). In this vein, our results support precedent research since rates in females are significantly higher for most of the items of the PHQ-9 when compared to men (except for items 8 and 9). Nonetheless, it should be noted that effect sizes of such sex differences were very small in our study, although it is not strange considering that prevalence of depression not always differs between male and female students from LMICs (Akhtar et al., 2020). This result could be related to some barriers that female students are successfully overcoming, as their educational opportunities and rates of enrollment are gradually increasing (Akhtar et al., 2020). Beyond such small effect sizes, our results are important when taking into account that depression among college students is related to self-stigma (Waqas et al., 2014; Akhtar et al., 2020), poor academic performance (Adewuya et al., 2006; Akhtar et al., 2020), social disadvantages (Harrington et al., 1993), and financial difficulties (Andrews and Wilding, 2004), among others.
As previously reported in some studies (e.g., Huarcaya-Victoria et al., 2020), we did not find a good fit when considering a unique general factor (that is, a unidimensional structure) of the PHQ-9 scale. Due to this, other theoretical proposals (e.g., Granillo, 2012; Doi et al., 2018; Patel et al., 2019; Lamela et al., 2020) were empirically contrasted, showing that the hierarchical Model 6 had the best fit to the data. In this sense, the Ecuadorian version of the PHQ-9 replicates previous results that supported a multidimensional structure of the scale, by including not only a general factor but also three nested factors (somatic, cognitive/affective, and concentration/motor) that allow researchers and clinicians to assess depressive symptomatology more accurately without disregarding a total score. In their recent systematic review of the PHQ-9 factor structure and measurement invariance, Lamela et al. (2020) stressed that there is no consensus on the factorial structure of this scale, ranging from one-factor to three-factor structures. In our study, the PHQ-9 scale clearly showed a higher hierarchical structure that contains three nested factors, as Marcos-Nájera et al. (2018) found among Spanish women in their first semester of pregnancy (cognitive-affective, somatic, and pregnancy-related), although it should be noted that not under a hierarchical model. In particular, the Ecuadorian version also showed a third nested factor by including items 7 and 8 as a separate entity (that is, concentration problems and psychomotor disturbances). We believe that such items are a separate dimension because they might have a different meaning for Ecuadorian college students. In this vein, Granillo (2012) excluded items 7 and 8 in her analyses and explained that some characteristics of college students (age, context) could lead to different interpretations of the activity levels and ability to focus on some tasks. This is not our case, as the best fit to the data occurred when both items were included and as separate entities. However, these results demonstrate that items 7 and 8 should be interpreted with caution when PHQ-9 is applied to college students, as the meaning of such items should be contextualized to their daily activities carried out within their role as students. For example, several studies have highlighted that, among college students, the decreased ability to concentrate symptom could be genuinely associated with higher levels of smartphone use, especially across campus spaces such as libraries, study rooms, etc. (Demirci et al., 2015; Wang et al., 2018).
Overall, while other studies offered no evidence for the necessity of using a multidimensional approach (e.g., Boothroyd et al., 2019), we believe that this multifactorial approach is relevant among Ecuadorian college students, as precedent studies have supported with both college students (Granillo, 2012; Cassiani-Miranda et al., 2017; Miranda and Scoppetta, 2018) and other subgroups of the population (Chilcot et al., 2013; Petersen et al., 2015; Beard et al., 2016; Guo et al., 2017; Doi et al., 2018; Arnold et al., 2020; Shin et al., 2020). This conclusion is important when taking into consideration culturally specific manifestations of depression and the social factors that influence them (Yusim et al., 2009). For example, somatic manifestations of depression seem important in previous research conducted in Latin American culture (Muñoz et al., 2005), and specifically in the Andean highlands of Ecuador (Yusim et al., 2009). These findings are similar to other studies where affective and somatic symptoms among Latino college students represent different subscales because the appearance of somatic symptomatology is considered the norm rather than the exception (e.g., Granillo, 2012).
Regarding measurement invariance, results of our study showed that the hierarchical structure remained invariant across men and women, supporting the idea that gender differences in the scores of the Ecuadorian version of the PHQ-9 are related to classical gender disparities in depression (Hyde et al., 2008; Parker and Brotchie, 2010; Salk et al., 2017) rather than the existence of bias in the measurement itself. Thus, we can conclude that the PHQ-9 scale can be equally administered across Ecuadorian female and male college students and, furthermore, it represents a sensitive assessment tool to existing gender differences in depressive symptomatology within an Ecuadorian context. Moreover, the symptoms assessed by the PHQ-9 scale are equivalent across different age groups. These findings are relevant as they allow us to compare male and female PHQ-9 scores as well as those results from groups of different ages, therefore replicating measurement invariance obtained in precedent research (e.g., Keum et al., 2018; Miranda and Scoppetta, 2018; Patel et al., 2019; Lamela et al., 2020; Tibubos et al., 2021). Overall, having a screening tool that is invariant across sex and different age groups will allow researchers and clinicians to develop both preventive and treatment programs of depression for both female and male college students in Ecuador.
On the other hand, our analyses revealed good internal consistency, not only for the total score but also for somatic, cognitive/affective, and concentration/motor scores. Such good reliability is similar to those results reported in precedent analyses of different PHQ-9 versions (e.g., Kroenke et al., 2001; Hansson et al., 2009; Doi et al., 2018; Huarcaya-Victoria et al., 2020; Lamela et al., 2020). Furthermore, the convergent and divergent validities of the Ecuadorian Spanish PHQ-9 showed that this depressive symptomatology correlated positively with other transdiagnostic health-related measures, such as psychological inflexibility (experiential avoidance or the tendency to suppress internal experiences; Hayes et al., 1996), loneliness (perceived social isolation; Cacioppo et al., 2006; Hawkley and Cacioppo, 2010), and perceived stress (perception of lack of control over the results of our behavior; Cohen et al., 1983); and negatively with satisfaction with life (global cognitive judgments of one’s life satisfaction; Diener et al., 1985). These findings were also consistent with previous studies, in which PHQ-9 scores were positively correlated with psychological inflexibility (Gilbert et al., 2019; Kato, 2020; McCracken et al., 2021; Paladines-Costa et al., 2021), psychological stress (Ruisoto et al., 2020), and perception of loneliness (Liu et al., 2020); and negatively correlated with satisfaction with life (Mei et al., 2021). The evidence of such associations is relevant as it supports the role of the PHQ-9 scale as a tool for the comprehensive assessment of mental health along with other key transdiagnostic variables.
Several limitations of this study merit mention. Firstly, our results should be considered with caution, since the sample only corresponds to college students. Precedent studies analyzing the factor structure of this scale did not have the limitation of only including college students and, in pursuit of overcoming this shortcoming, future research should further explore the psychometric properties and factor structure of the Ecuadorian Spanish version of PHQ-9 among other non-clinical and clinical populations as well as other age groups. Secondly, we only tested the measurement invariance among sex and different age subgroups, and it was not possible to assess other variables. For example, we were unable to evaluate measurement invariance across different ethnic groups, as most of the students were mestizos (that is, mixed-race). On the other hand, the range of ages has been limited, so future studies should analyze such measurement invariance across a wider age range as well as across other sociodemographic and clinical variables. Thirdly, this represents a cross-sectional study so measurement invariance, internal consistency as well as convergent and divergent validities should be replicated in future longitudinal designs. Finally, the use of a self-report tool (as the PHQ-9 scale) may be subject to some inaccuracies in data collection because of memory bias.
In spite of these shortcomings, our findings highlight the necessity of early identification of those Ecuadorian young people at risk of developing a serious psychological problem, as well as reveal that the PQH-9 could be a useful tool for the screening of depression among Ecuadorian college students. The analyses conducted clearly emphasize good psychometric properties of the Ecuadorian Spanish version of this scale and support a hierarchical model that includes not only a general factor but also three distinct nested factors (somatic, cognitive/affective, and concentration/motor), preserving measurement invariance across sex and age. Moreover, PHQ-9 scores correlate with other relevant transdiagnostic indicators of mental health, such as psychological inflexibility, loneliness, perceived stress, and satisfaction with life. These results are important as PHQ-9 represents an easy-to-implement screening questionnaire and a useful tool to develop preventive programs (Lamela et al., 2020), now including the Ecuadorian university context.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethics Committee for Research in Human Beings (Comité de Ética de Investigación en Seres Humanos, UTPL-CEISH, March 6, 2019) of the UTPL Ecuador (UTPL-DIS-2019-0088-O). Written informed consent from the participants’ legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
VL-G, CL-N, and SV-G: conceptualization, writing—original draft preparation, and writing—review and editing. VL-G: methodology, formal analysis, investigation, and data curation. VL-G and PT-C: supervision. PT-C and SV-G: project administration and funding acquisition. All authors have read and agreed to the published version of the manuscript.
This study was financially supported by the Particular Technical University of Loja (Ecuador) and developed under the project “Automatic processing techniques applied to the analysis and prediction of drug use” (Técnicas de procesamiento automático aplicadas al análisis y predicción del consumo de drogas), funded by the National Research and Education Network of Ecuador called RedCEDIA (Red Nacional de Investigación y Educación del Ecuador; COP-AL-23-18, CEPRA XII-2018-05).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We would like to thank the three universities that participated in this study (Universidad Técnica Particular de Loja, UTPL; Universidad Técnica del Norte, UTN; Universidad Politécnica Salesiana, UPS) and the National Research and Education Network of Ecuador (Red Nacional de Investigación y Educación del Ecuador, RedCEDIA).
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2022.813894/full#supplementary-material
Adewuya, A. O., Ola, B. A., Aloba, O. O., Mapayi, B. M., and Oginni, O. O. (2006). Depression amongst Nigerian university students. Soc. Psychiatry Psychiatr. Epidemiol. 41, 674–678. doi: 10.1007/s00127-006-0068-9
Akhtar, P., Ma, L., Waqas, A., Naveed, S., Li, Y., Rahman, A., et al. (2020). Prevalence of depression among university students in low and middle income countries (LMICs): a systematic review and meta-analysis. J. Affect. Disord. 274, 911–919. doi: 10.1016/j.jad.2020.03.183
American Psychiatric Association (2000). Diagnostic and Statistical Manual of Mental Disorders, 4th Edn. Washington, DC: American Psychiatric Association.
Andrews, B., and Wilding, J. M. (2004). The relation of depression and anxiety to life-stress and achievement in students. Br. J. Psychol. 95, 509–521. doi: 10.1348/0007126042369802
Arnold, S. R. C., Uljarević, M., Hwang, Y. I., Richdale, A. L., Trollor, J. N., and Lawson, L. P. (2020). Brief report: psychometric properties of the patient health questionaire-9 (PHQ-9) in Autistic adults. J. Autism Dev. Disord. 50, 2217–2225. doi: 10.1007/s10803-019-03947-9
Atienza, F. L., Pons, D., Balaguer, I., and Garciìa-Merita, M. L. (2000). Psychometric properties of the satisfaction with life scale in adolescents. Psicothema 12, 331–336.
Baader, T., Molina, J. L., Venezian, S., Rojas, C., Farías, R., and Fierro-Freixenet, C. (2012). Validación y utilidad de la encuesta PHQ-9 (Patient Health Questionnaire) en el diagnóstico de depresión en pacientes usuarios de atención primaria en Chile. Rev. Chil. Neuro Psiquiatr. 50, 10–22. doi: 10.4067/S0717-92272012000100002
Baas, K. D., Cramer, A. O. J., Koeter, M. W. J., van de Lisdonk, E. H., van Weert, H. C., and Schene, A. H. (2011). Measurement invariance with respect to ethnicity of the Patient Health Questionnaire-9 (PHQ-9). J. Affect. Disord. 129, 229–235. doi: 10.1016/J.JAD.2010.08.026
Beard, C., Hsu, K. J., Rifkin, L. S., Busch, A. B., and Björgvinsson, T. (2016). Validation of the PHQ-9 in a psychiatric sample. J. Affect. Disord. 193, 267–273. doi: 10.1016/j.jad.2015.12.075
Bélanger, E., Thomas, K. S., Jones, R. N., Epstein-Lubow, G., and Mor, V. (2019). Measurement validity of the Patient-Health Questionnaire-9 in US nursing home residents. Int. J. Geriatr. Psychiatry 34, 700–708. doi: 10.1002/gps.5074
Bitsika, V., Sharpley, C. F., and Melham, T. C. (2010). Gender differences in factor scores of anxiety and depression among Australian university students: implications for counselling interventions. Can. J. Couns. 44, 51–64.
Bond, F. W., Hayes, S. C., Baer, R. A., Carpenter, K. M., Guenole, N., Orcutt, H. K., et al. (2011). Preliminary psychometric properties of the Acceptance and Action Questionnaire–II: a revised measure of psychological inflexibility and experiential avoidance. Behav. Ther. 42, 676–688. doi: 10.1016/j.beth.2011.03.007
Boothroyd, L., Dagnan, D., and Muncer, S. (2019). PHQ-9: one factor or two? Psychiatry Res. 271, 532–534. doi: 10.1016/j.psychres.2018.12.048
Borghero, F., Martínez, V., Zitko, P., Vöhringer, P. A., Cavada, G., and Rojas, G. (2018). Screening depressive episodes in adolescents. Validation of the Patient Health Questionnaire-9 (PHQ-9). Rev. Med. Chil. 146, 479–486. doi: 10.4067/s0034-98872018000400479
Cacioppo, J. T., Hughes, M. E., Waite, L. J., Hawkley, L. C., and Thisted, R. A. (2006). Loneliness as a specific risk factor for depressive symptoms: cross-sectional and longitudinal analyses. Psychol. Aging 21, 140–151. doi: 10.1037/0882-7974.21.1.140
Cassiani-Miranda, C. A., Vargas-Hernández, M. C., Pérez-Anibal, E., Herazo-Bustos, M. I., and Hernández-Carrillo, M. (2017). Reliability and dimensionality of PHQ-9 in screening depression symptoms among health science students in Cartagena, 2014. Biomedica 37, 112–120. doi: 10.7705/biomedica.v37i0.3221
Cheung, G. W., and Rensvold, R. B. (2002). Evaluating goodness-of-fit indexes for testing measurement invariance. Model. Struct. Equat. 9, 233–255. doi: 10.1207/S15328007SEM0902_5
Chilcot, J., Rayner, L., Lee, W., Price, A., Goodwin, L., Monroe, B., et al. (2013). The factor structure of the PHQ-9 in palliative care. J. Psychosom. Res. 75, 60–64. doi: 10.1016/j.jpsychores.2012.12.012
Cleary, M., Walter, G., and Jackson, D. (2011). “Not always smooth sailing”: mental health issues associated with the transition from high school to college. Issues Ment. Health Nurs. 32, 250–254. doi: 10.1111/j.1525-1497.2005.0144.x
Cohen, S., Kamarck, T., and Mermelstein, R. (1983). A global measure of perceived stress. J. Health Soc. Behav. 24, 385–396. doi: 10.2307/2136404
Demirci, K., Akgönül, M., and Akpinar, A. (2015). Relationship of smartphone use severity with sleep quality, depression, and anxiety in university students. J. Behav. Addict. 4, 85–92. doi: 10.1556/2006.4.2015.01
Diener, E., Emmons, R. A., Larsen, R. J., and Griffin, S. (1985). The satisfaction with life scale. J. Pers. Assess. 49, 71–75. doi: 10.1207/s15327752jpa4901_13
Diez-Quevedo, C., Rangil, T., Sanchez-Planell, L., Kroenke, K., and Spitzer, R. L. (2001). Validation and utility of the patient health questionnaire in diagnosing mental disorders in 1003 general hospital Spanish inpatients. Psychosom. Med. 63, 679–686. doi: 10.1097/00006842-200107000-00021
Doi, S., Ito, M., Takebayashi, Y., Muramatsu, K., and Horikoshi, M. (2018). Factorial validity and invariance of the Patient Health Questionnaire (PHQ)-9 among clinical and non-clinical populations. PLoS One 13:e0199235. doi: 10.1371/journal.pone.0199235
Donlan, W., and Lee, J. (2010). Screening for depression among indigenous Mexican migrant farmworkers using the Patient Health Questionnaire-9. Psychol. Rep. 106, 419–432.
Dueber, D. M. (2017). Bifactor Indices Calculator: a Microsoft Excel-Based Tool to Calculate Various Indices Relevant to Bifactor CFA Models. Kentucky: University of Kentucky. doi: 10.13023/edp.tool.01
Eisenberg, D., Gollust, S. E., Golberstein, E., and Hefner, J. L. (2007). Prevalence and correlates of depression, anxiety, and suicidality among university students. Am. J. Orthopsychiatry 77, 534–542. doi: 10.1037/0002-9432.77.4.534
Evans-Lacko, S., Aguilar-Gaxiola, S., Al-Hamzawi, A., Alonso, J., Benjet, C., Bruffaerts, R., et al. (2018). Socio-economic variations in the mental health treatment gap for people with anxiety, mood, and substance use disorders: results from the WHO World Mental Health (WMH) surveys. Psychol. Med. 48, 1560–1571. doi: 10.1017/S0033291717003336
Familiar, I., Ortiz-Panozo, E., Hall, B., Vieitez, I., Romieu, I., Lopez-Ridaura, R., et al. (2015). Factor structure of the Spanish version of the Patient Health Questionnaire-9 in Mexican women. Int. J. Methods Psychiatr. Res. 24, 74–82. doi: 10.1002/mpr.1461
Gilbert, K. E., Tonge, N. A., and Thompson, R. J. (2019). Associations between depression, anxious arousal and manifestations of psychological inflexibility. J. Behav. Ther. Exp. Psychiatry 62, 88–96. doi: 10.1016/j.jbtep.2018.09.006
González-Blanch, C., Medrano, L. A., Muñoz-Navarro, R., Ruíz-Rodríguez, P., Moriana, J. A., Limonero, J. T., et al. (2018). Factor structure and measurement invariance across various demographic groups and over time for the PHQ-9 in primary care patients in Spain. PLoS One 13:e0193356. doi: 10.1371/journal.pone.0193356
González-Rivera, J. A. (2019). Validation and dimensionality of Patient Health Questionnaire for Depression (PHQ-8 and PHQ-9) in Hispanic LGBT+ community. Int. J. Recent Sci. Res. 10, 36670–36676. doi: 10.24327/ijrsr.2019.1012.4970
Granillo, M. T. (2012). Structure and function of the patient health questionnaire-9 among latina and non-latina white female college students. J. Soc. Soc. Work Res. 3, 80–93. doi: 10.5243/jsswr.2012.6
Guo, B., Kaylor-Hughes, C., Garland, A., Nixon, N., Sweeney, T., Simpson, S., et al. (2017). Factor structure and longitudinal measurement invariance of PHQ-9 for specialist mental health care patients with persistent major depressive disorder: exploratory structural equation modelling. J. Affect. Disord. 219, 1–8. doi: 10.1016/j.jad.2017.05.020
Hambleton, R. K., and Zenisky, A. L. (2011). “Translating and adapting tests for cross-cultural assessments,” in Cross-Cultural Research Methods in Psychology, eds D. Matsumoto and F. J. R. van de Vijver (Nueva York: Cambridge University Press), 46–70.
Hansson, M., Chotai, J., Nordstöm, A., and Bodlund, O. (2009). Comparison of two self-rating scales to detect depression: HADS and PHQ-9. Br. J. Gen. Pract. 59, e283–e288. doi: 10.3399/bjgp09X454070
Harrington, R. C., Fudge, H., Rutter, M. L., Bredenkamp, D., Groothues, C., and Pridham, J. (1993). Child and adult depression: a test of continuities with data from a family study. Br. J. Psychiatry 162, 627–633. doi: 10.1192/bjp.162.5.627
Hawkley, L. C., and Cacioppo, J. T. (2010). Loneliness matters: a theoretical and empirical review of consequences and mechanisms. Ann. Behav. Med. 40, 218–227. doi: 10.1007/s12160-010-9210-8
Hayes, S. C., Wilson, K. G., Gifford, E. V., Follette, V. M., and Strosahl, K. (1996). Experiential avoidance and behavioral disorders: a functional dimensional approach to diagnosis and treatment. J. Consult. Clin. Psychol. 64, 1152–1168. doi: 10.1037/0022-006X.64.6.1152
Huang, F. Y., Chung, H., Kroenke, K., Delucchi, K. L., and Spitzer, R. L. (2006). Using the Patient Health Questionnaire-9 to measure depression among racially and ethnically diverse primary care patients. J. Gen. Intern. Med. 21, 547–552. doi: 10.1111/j.1525-1497.2006.00409.x
Huarcaya-Victoria, J., De-Lama-Morán, R., Quiros, M., Bazán, J., López, K., and Lora, D. (2020). Propiedades psicométricas del Patient Health Questionnaire (PHQ-9) en estudiantes de medicina en Lima. Perú. Rev. Neuropsiquiatr. 83, 72–78. doi: 10.20453/rnp.v83i2.3749
Hughes, M. E., Waite, L. J., Hawkley, L. C., and Cacioppo, J. T. (2004). A short scale for measuring loneliness in large surveys: results from two population-based studies. Res. Aging 26, 655–672. doi: 10.1177/0164027504268574
Hyde, J. S., Mezulis, A. H., and Abramson, L. Y. (2008). The ABCs of depression: integrating affective, biological, and cognitive models to explain the emergence of the gender difference in depression. Psychol. Rev. 115, 291–313. doi: 10.1037/0033-295X.115.2.291
Ibrahim, A. K., Kelly, S. J., Adams, C. E., and Glazebrook, C. (2013). A systematic review of studies of depression prevalence in university students. J. Psychiatr. Res. 47, 391–400. doi: 10.1016/j.jpsychires.2012.11.015
Kato, T. (2020). Effect of psychological inflexibility on depressive symptoms and sleep disturbance among japanese young women with chronic pain. Int. J. Environ. Res. Public Health 17:7426. doi: 10.3390/ijerph17207426
Keum, B. T., Miller, M. J., and Inkelas, K. K. (2018). Testing the factor structure and measurement invariance of the PHQ-9 across racially diverse US college students. Psychol. Assess. 30, 1096–1106. doi: 10.1037/pas0000550
Kim, Y. E., and Lee, B. (2019). The psychometric properties of the patient health questionnaire-9 in a sample of Korean university students. Psychiatry Investig. 16, 904–910. doi: 10.30773/pi.2019.0226
Kohn, R., Ali, A. A., Puac-Polanco, V., Figueroa, C., López-Soto, V., Morgan, K., et al. (2018). Mental health in the Americas: an overview of the treatment gap. Rev. Panam. Salud Publica 42:e165. doi: 10.26633/RPSP.2018.165
Kroenke, K., Spitzer, R. L., and Williams, J. B. W. (2001). The PHQ-9: validity of a brief depression severity measure. J. Gen. Intern. Med. 16, 606–613. doi: 10.1046/j.1525-1497.2001.016009606.x
Kuehner, C. (2017). Why is depression more common among women than among men? Lancet Psychiatry 4, 146–158. doi: 10.1016/S2215-0366(16)30263-2
Lamela, D., Soreira, C., Matos, P., and Morais, A. (2020). Systematic review of the factor structure and measurement invariance of the patient health questionnaire-9 (PHQ-9) and validation of the Portuguese version in community settings. J. Affect. Disord. 276, 220–233. doi: 10.1016/j.jad.2020.06.066
Liu, T., Lu, S., Leung, D. K. Y., Sze, L. C. Y., Kwok, W. W., Tang, J. Y. M., et al. (2020). Adapting the UCLA 3-item loneliness scale for community-based depressive symptoms screening interview among older Chinese: a cross-sectional study. BMJ Open 10:e041921. doi: 10.1136/bmjopen-2020-041921
Lopez, A. D., and Mathers, C. D. (2013). Measuring the global burden of disease and epidemiological transitions: 2002–2030. Ann. Trop. Med. Parasitol. 100, 481–499. doi: 10.1179/136485906X97417
Marcos-Nájera, R., Le, H. N., Rodríguez-Muñoz, M. F., Olivares-Crespo, M. E., and Izquierdo-Mendez, N. (2018). The structure of the Patient Health Questionnaire-9 in pregnant women in Spain. Midwifery 62, 36–41. doi: 10.1016/j.midw.2018.03.011
Martín-Díaz, E. (2017). Are universities ready for interculturality? The case of the Intercultural University ‘Amawtay Wasi’(Ecuador). J. Lat. Am. Cult. Stud. 26, 73–90. doi: 10.1080/13569325.2016.1272443
McCracken, L. M., Badinlou, F., Buhrman, M., and Brocki, K. C. (2021). The role of psychological flexibility in the context of COVID-19: associations with depression, anxiety, and insomnia. J. Contextual Behav. Sci. 19, 28–35. doi: 10.1016/j.jcbs.2020.11.003
Mei, S., Qin, Z., Yang, Y., Gao, T., Ren, H., Hu, Y., et al. (2021). Influence of life satisfaction on quality of life: mediating roles of depression and anxiety among cardiovascular disease patients. Clin. Nurs. Res. 30, 215–224. doi: 10.1177/1054773820947984
Merz, E. L., Malcarne, V. L., Roesch, S. C., Riley, N., and Sadler, G. R. (2011). A multigroup confirmatory factor analysis of the Patient Health Questionnaire-9 among English-and Spanish-speaking Latinas. Cult. Divers Ethnic Minor Psychol. 17, 309–316. doi: 10.1037/a0023883
Miranda, C. A. C., and Scoppetta, O. (2018). Factorial structure of the Patient Health Questionnaire-9 as a depression screening instrument for university students in Cartagena, Colombia. Psychiatry Res. 269, 425–429. doi: 10.1016/j.psychres.2018.08.071
Mitchell, A. J., Yadegarfar, M., Gill, J., and Stubbs, B. (2016). Case finding and screening clinical utility of the Patient Health Questionnaire (PHQ-9 and PHQ-2) for depression in primary care: a diagnostic meta-analysis of 40 studies. BJPsych Open 2, 127–138. doi: 10.1192/bjpo.bp.115.001685
Moral, J., González, M., Landero, R., and Quezada, L. (2021). Validation of the five-factor model of the attitude scale towards statistics in mexican psychology students. Interdisciplinaria 38, 133–148. doi: 10.16888/interd.2021.38.1.9
Muñiz, J., Elosua, P., and Hambleton, R. K. (2013). Directrices para la traducción y adaptación de los tests: segunda edición. Psicothema 25, 151–157. doi: 10.7334/psicothema2013.24
Muñoz, R. A., McBride, M. E., Brnabic, A. J., López, C. J., Hetem, L. A. B., Secin, R., et al. (2005). Major depressive disorder in Latin America: the relationship between depression severity, painful somatic symptoms, and quality of life. J. Affect. Disord. 86, 93–98. doi: 10.1016/j.jad.2004.12.012
Paladines-Costa, B., López-Guerra, V., Ruisoto, P., Vaca-Gallegos, S., and Cacho, R. (2021). Psychometric properties and factor structure of the spanish version of the acceptance and action questionnaire-II (AAQ-II) in ecuador. Int. J. Environ. Res. Public Health 18:2944. doi: 10.3390/ijerph18062944
Pan American Health Organization (2018). The Burden of Mental Disorders in the Region of the Americas. Available online at: https://iris.paho.org/handle/10665.2/49578 [accessed on October 19, 2021].
Parker, G., and Brotchie, H. (2010). Gender differences in depression. Int. Rev. Psychiatry 22, 429–436. doi: 10.3109/09540261.2010.492391
Patel, J. S., Oh, Y., Rand, K. L., Wu, W., Cyders, M. A., Kroenke, K., et al. (2019). Measurement invariance of the patient health questionnaire-9 (PHQ-9) depression screener in U.S. adults across sex, race/ethnicity, and education level: NHANES 2005–2016. Depress Anxiety 36, 813–823. doi: 10.1002/da.22940
Petersen, J. J., Paulitsch, M. A., Hartig, J., Mergenthal, K., Gerlach, F. M., and Gensichen, J. (2015). Factor structure and measurement invariance of the Patient Health Questionnaire-9 for female and male primary care patients with major depression in Germany. J. Affect. Disord. 170, 138–142. doi: 10.1016/j.jad.2014.08.053
Pinto-Meza, A., Serrano-Blanco, A., Peñarrubia, M. T., Blanco, E., and Haro, J. M. (2005). Assessing depression in primary care with the PHQ-9: can it be carried out over the telephone? J. Gen. Intern. Med. 20, 738–742.
Raykov, T., and Hancock, G. R. (2005). Examining change in maximal reliability for multiple-component measuring instruments. Br. J. Math. Stat. Psychol. 58, 65–82. doi: 10.1348/000711005X38753
Remor, E. (2006). Psychometric properties of a European Spanish version of the Perceived Stress Scale (PSS). Span. J. Psychol. 9, 86–93. doi: 10.1017/s1138741600006004
Rodriguez, A., Reise, S. P., and Haviland, M. G. (2016). Evaluating bifactor models: calculating and interpreting statistical indices. Psychol. Methods 21, 137–150. doi: 10.1037/met0000045
Ruisoto, P., Cacho, R., López-Goñi, J. J., Vaca, S., and Jiménez, M. (2016). Prevalence and profile of alcohol consumption among university students in Ecuador. Gac. Sanit. 30, 370–374. doi: 10.1016/j.gaceta.2016.02.008
Ruisoto, P., López-Guerra, V. M., Paladines-Costa, M. B., Vaca, S. L., and Cacho, R. (2020). Psychometric properties of the three versions of the Perceived Stress Scale in Ecuador. Physiol. Behav. 224:113045. doi: 10.1016/j.physbeh.2020.113045
Saldivia, S., Aslan, J., Cova, F., Vicente, B., Inostroza, C., and Rincón, P. (2019). Propiedades psicométricas del PHQ-9 (Patient Health Questionnaire) en centros de atención primaria de Chile. Rev. Med. Chil. 147, 53–60. doi: 10.4067/S0034-98872019000100053
Salk, R. H., Hyde, J. S., and Abramson, L. Y. (2017). Gender differences in depression in representative national samples: meta-analyses of diagnoses and symptoms. Psychol. Bull. 143, 783–822. doi: 10.1037/bul0000102
Schantz, K., Reighard, C., Aikens, J. E., Aruquipa, A., Pinto, B., Valverde, H., et al. (2017). Screening for depression in Andean Latin America: factor structure and reliability of the CES-D short form and the PHQ-8 among Bolivian public hospital patients. Int. J. Psychiatry Med. 52, 315–327. doi: 10.1177/0091217417738934
Shin, C., Ko, Y. H., An, H., Yoon, H. K., and Han, C. (2020). Normative data and psychometric properties of the Patient Health Questionnaire-9 in a nationally representative Korean population. BMC Psychiatry 20:194. doi: 10.1186/s12888-020-02613-0
Spitzer, R. L., Kroenke, K., Williams, J. B., and The Patient Health Questionnaire Primary Care Study Group (1999). Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. JAMA 282, 1737–1744. doi: 10.1001/jama.282.18.1737
Spitzer, R. L., Williams, J. B., Kroenke, K., Linzer, M., deGruy, F. V., Hahn, S. R., et al. (1994). Utility of a new procedure for diagnosing mental disorders in primary care: the PRIME-MD 1000 study. JAMA 272, 1749–1756. doi: 10.1001/jama.1994.03520220043029
Thomas, L., Briggs, P., Hart, A., and Kerrigan, F. (2017). Understanding social media and identity work in young people transitioning to university. Comput. Hum. Behav. 76, 541–553. doi: 10.1016/j.chb.2017.08.021
Tibubos, A. N., Otten, D., Zöller, D., Binder, H., Wild, P. S., Fleischer, T., et al. (2021). Bidimensional structure and measurement equivalence of the Patient Health Questionnaire-9: sex-sensitive assessment of depressive symptoms in three representative German cohort studies. BMC Psychiatry 21:238. doi: 10.1186/s12888-021-03234-x
Torres, C., Otero, P., Bustamante, B., Blanco, V., Díaz, O., and Vázquez, F. L. (2017). Mental health problems and related factors in Ecuadorian college students. Int. J. Environ. Res. Public Health. 14:530. doi: 10.3390/ijerph14050530
Urtasun, M., Daray, F. M., Teti, G. L., Coppolillo, F., Herlax, G., Saba, G., et al. (2019). Validation and calibration of the patient health questionnaire (PHQ-9) in Argentina. BMC Psychiatry 19:291. doi: 10.1186/s12888-019-2262-9
Vanstone, D. M., and Hicks, R. E. (2019). Transitioning to university: coping styles as mediators between adaptive-maladaptive perfectionism and test anxiety. Pers. Individ. Dif. 141, 68–75. doi: 10.1016/j.paid.2018.12.026
Villarreal-Zegarra, D., Copez-Lonzoy, A., Bernabé-Ortiz, A., Melendez-Torres, G. J., and Bazo-Alvarez, J. C. (2019). Valid group comparisons can be made with the Patient Health Questionnaire (PHQ-9): a measurement invariance study across groups by demographic characteristics. PLoS One 14:e0221717. doi: 10.1371/journal.pone.0221717
Wang, P. S., Aguilar-Gaxiola, S., Alonso, J., Angermeyer, M. C., Borges, G., Bromet, E. J., et al. (2007). Use of mental health services for anxiety, mood, and substance disorders in 17 countries in the WHO world mental health surveys. Lancet 370, 841–850. doi: 10.1016/S0140-6736(07)61414-7
Wang, R., Wang, W., DaSilva, A., Huckins, J. F., Kelley, W. M., Heatherton, T. F., et al. (2018). Tracking depression dynamics in college students using mobile phone and wearable sensing. Proc. ACM Interact. Mob. Wearable Ubiquit. Technol. 2, 1–26. doi: 10.1145/3191775
Waqas, A., Zubair, M., Ghulam, H., Ullah, M. W., and Tariq, M. Z. (2014). Public stigma associated with mental illnesses in Pakistani university students: a cross sectional survey. PeerJ 2, e698. doi: 10.7717/peerj.698
Weitzman, E. R. (2004). Poor mental health, depression, and associations with alcohol consumption, harm, and abuse in a national sample of young adults in college. J. Nerv. Ment. Dis. 192, 269–277. doi: 10.1097/01.nmd.0000120885.17362.94
World Health Organization (2013). Mental Health. Action Plan 2013-2020. Available online at: https://apps.who.int/iris/bitstream/handle/10665/89966/9789241506021_eng.pdf [accessed on October 19, 2021].
World Health Organization (2017). Depression and other Common Mental Disorders. Global Health Estimates. Available online at: https://apps.who.int/iris/bitstream/handle/10665/254610/WHO-MSD-MER-2017.2-eng.pdf?sequence=1 [accessed on October 31, 2021].
World Health Organization (2021). Depression (fact sheet). Available online at: https://www.who.int/news-room/fact-sheets/detail/depression [accessed on October 31, 2021].
World Medical Association (2013). World medical association declaration of helsinki: 564 ethical principles for medical research involving human subjects. JAMA 310, 2191–2194. doi: 10.1001/jama.2013.281053
Wulsin, L., Somoza, E., and Heck, J. (2002). The feasibility of using the Spanish PHQ-9 to screen for depression in primary Care in Honduras. Prim. Care Companion J. Clin. Psychiatry 4, 191–195. doi: 10.4088/pcc.v04n0504
Yu, X., Tam, W. W., Wong, P. T., Lam, T. H., and Stewart, S. (2012). The Patient Health Questionnaire-9 for measuring depressive symptoms among the general population in Hong Kong. Compr. Psychiatr. 53, 95–102. doi: 10.1016/j.comppsych.2010.11.002
Yusim, A., Anbarasan, D., Hall, B., Goetz, R., Neugebauer, R., and Ruiz, P. (2009). Somatic and cognitive domains of depression in an underserved region of Ecuador: some cultural considerations. World Psychiatry 8, 178–180. doi: 10.1002/j.2051-5545.2009.tb00247.x
Keywords: psychometric properties, factor structure, Patient Health Questionnaire-9 (PHQ-9), depression, college students, Ecuador
Citation: López-Guerra VM, López-Núñez C, Vaca-Gallegos SL and Torres-Carrión PV (2022) Psychometric Properties and Factor Structure of the Patient Health Questionnaire-9 as a Screening Tool for Depression Among Ecuadorian College Students. Front. Psychol. 13:813894. doi: 10.3389/fpsyg.2022.813894
Received: 12 November 2021; Accepted: 12 April 2022;
Published: 29 April 2022.
Edited by:
Laura Galiana, University of Valencia, SpainReviewed by:
Juliane Burghardt, Karl Landsteiner University of Health Sciences, AustriaCopyright © 2022 López-Guerra, López-Núñez, Vaca-Gallegos and Torres-Carrión. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Carla López-Núñez, Y2xudW5lekB1cy5lcw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.