 Xinfeng Tang
Xinfeng Tang Qiwen Liu2
Qiwen Liu2 Suqin Tang
Suqin Tang
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychol. , 22 August 2022
Sec. Cultural Psychology
Volume 13 - 2022 | https://doi.org/10.3389/fpsyg.2022.792356
The objective of the study is to provide a reliable estimate of the pooled prevalence of social anxiety disorder (SAD) and social anxiety symptoms (SAS) among children, adolescents, and young adults (CAYA) in China. Meta-analysis is used to provide pooled-prevalence rate of SAD and SAS. Literature searches were conducted in both English and Chinese databases from the database's inception to April 2019. Eleven studies were identified for SAD, and 17 were included for SAS. The results revealed a pooled prevalence of SAD of 2.1% (95% CI: 1.2–3.8%) with high between-studies heterogeneity (Q = 1,055.2, I2 = 99.1%, p < 0.001). The pooled prevalence estimate of SAS was 23.5% (95% CI: 18.6–29.3%), also with significant heterogeneity (Q = 1,019.3, I2 = 98.4%, p < 0.001). Different diagnostic tools or self-report scales reported significant different prevalence of SAD or SAS. Further analysis stratified by gender, age, sampling methods, economic status, and risk of bias were performed. Limitations include the high level of heterogeneity between studies, inadequate number of the studies, and significant differences in prevalence caused by measurements.
Systematic review registration: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020149591, identifier: PROSPERO CRD42020149591.
Social anxiety disorder (SAD) is quite common among young people, with a lifetime prevalence rate ranging from 3.5 to 9.1% aged 10-24 in western countries such as the United State, Germany and Austria (Stein et al., 2001; Burstein et al., 2011; Knappe et al., 2011; Wagner et al., 2017). The core features of SAD are excessive fear of scrutiny by others and avoidance of social situations in which embarrassment or humiliation might occur (American Psychiatric Association., 2013). Social anxiety brings a series of problems such as impaired academic and global functioning (Ranta et al., 2009; Edlund et al., 2018; Finsaas et al., 2020), loneliness (Bernstein et al., 2008; Eres et al., 2021), low level of social support from classmates (Coyle and Malecki, 2018), poor social skills (Scharfstein et al., 2011; Lau et al., 2022), and high rates of sickness absence and unemployment (Amin et al., 2019). The onset of SAD is early, with a median age of 13 years in epidemiological studies (Kessler et al., 2005), and there are few new cases after 25 years of age (Wittchen and Fehm, 2003; Stein et al., 2017). In clinical samples, SAD is the most chronic anxiety disorder, with a 37–56% remission rate (Bruce et al., 2005; Springer et al., 2018).
Due to its significant negative consequences, SAD has received much research and clinical attention. However, significant social anxiety symptoms (SAS) should not be ignored because social anxiety is on a continuous spectrum from absence of social fear through normal anxiety and shyness to SAD (McNeil, 2001). Studies have shown that even subthreshold social anxiety (≥one social phobia symptoms in DSM-IV plus avoidance) brings significant psychosocial impairment and elevated rates of other psychiatric disorders (Crum and Pratt, 2001; Merikangas et al., 2002; Filho et al., 2010). In the present study, SAD refers to a type of an anxiety disorder that meet the DSM-5 or ICD-11 diagnosis. SAS, on the other hand, refers to the symptoms and manifestations of social anxiety which is measured by valid self-report scales.
Epidemiological surveys revealed significant cultural differences in the prevalence of social anxiety symptoms and disorder. A review shows that the prevalence of SAD among adults in Asian countries is significantly lower than that in Europe and the United States (Hofmann et al., 2010). For example, Asian countries such as China, South Korea, and Japan had 12-month prevalence rates of 0.2% (Shen et al., 2006), 0.2% (Cho et al., 2007), and 0.8% (Kawakami et al., 2005), respectively. Meanwhile, the prevalence of SAD in some European and American countries such as the United States, the Netherlands, and Australia ranged between 4.2 and 7.1% (Bijl et al., 1998; Ruscio et al., 2008; Crome et al., 2015). Interestingly, the phenomenon is reversed in self-report measurement. A meta-analysis found that individuals of Asian heritage had higher self-reported social anxiety scores than those of European heritage in 28 out of 32 independent studies and yielded a mean effect size of d = 0.36 (Krieg and Xu, 2015). One possible reason for this difference is that Asian individuals belong to collectivism and are more likely to feel embarrassment and anxiety in social interactions, and therefore have higher social anxiety symptoms. However, Asian culture acquiesces or even appreciates social shyness and anxiety. Individuals with high social anxiety symptoms do not necessarily bring about impairment in social functioning in Asian societies, and therefore exhibit lower prevalence of social anxiety disorder (Heinrichs et al., 2006).
It is not clear whether a similar phenomenon exists in children and adolescent populations. There is a lack of large-scale epidemiological surveys or meta-analyses to report the prevalence of SAD or SAS among Chinese children, adolescents, and young adults (CAYA). Some studies found that the point prevalence of SAD in primary and secondary schools was as low as 0.6% (Ye et al., 2013), while others reported a prevalence rate of 2.7% (Su et al., 2006). The findings of SAS prevalence were also inconsistent. One previous study found that 6.9% of Chinese primary school students experienced severe social anxiety symptoms as measured by the Social Anxiety Scale for Children (SASC; Cai, 1998). However, with the same assessment tool and cutoff point, one more recent study reported a rate of 26.3% in a similar population (Gao et al., 2013). These inconsistencies might be due to the use of different age groups of CAYA, sampling frames, sampling methods, and other factors.
Compared with depression, PTSD, and other mental health issues, people have less knowledge and poorer recognition of social anxiety (Katzelnick et al., 2001; Coles et al., 2016). The public's underestimate of the severity of social anxiety could be due to the inaccurate estimates of the prevalence of social anxiety, which might further hinder the clinicians' detection and recognition of social anxiety and provide treatment to people who are in need.
Therefore, a meta-analysis focusing on the prevalence of social anxiety among Chinese CAYA is warranted. The purpose of the current study was to combine the prevalence rates in existing surveys to provide a more reliable prevalence estimate of SAD and its symptoms in Chinese CAYA. For social anxiety disorder, the prevalence refers to the proportion of individuals who are positive on a certain diagnostic tool. For social anxiety symptoms, the prevalence is the proportion of individuals who exceed a cutoff on a self-rated scale. The most appropriate test cutoff value is determined with a compromise between sensitivity and specificity based on receiver operating characteristic (ROC) analysis (Habibzadeh et al., 2016). Although there are some drawbacks to using a dichotomous approach for a psychological disorder which lies on a continuum, this approach is simple to understand and can be of great value to the public and to clinical practice, especially in China where relevant data are lacking.
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA; Liberati et al., 2009) and Meta-Analysis of Observational Studies in Epidemiology (MOOSE; Stroup et al., 2000) guidelines throughout this meta-analysis. This review has been registered at PROSPERO (Registration Number: CRD42020149591).
We searched the following online English-language databases: MEDLINE, PsycINFO, EMBASE, and Web of Science. Chinese databases were also searched including the China National Knowledge Infrastructure Database (CNKI), the Wanfang database and the Chinese Scientific Journal Database (VIP Database). Reference lists of relevant review articles and all included articles, as well as papers citing these relevant studies in Google Scholar or CNKI, were searched by hand for additional studies. The review examined all journal articles published until July 2020. The search was restricted to English and Chinese language articles. The search terms can be seen in Supplementary material 1.
The following inclusion criteria were applied: (1) CAYA aged 6–25; (2) original studies that reported the prevalence rate of SAD or symptoms; and (3) the use of a standardized assessment procedure deriving diagnosis of SAD or valid measures with good psychometric properties to assess social anxiety symptoms (Leffler et al., 2015; Wong et al., 2016; Hunsley and Mash, 2018); diagnostic and self-report instruments are listed in Supplementary material 2; (4) Most studies only reported point prevalence of SAD in Chinese CAYA. Therefore, we only included studies which reported point prevalence of SAD in the current meta-analysis. (5) For SAS, the scales in the included studies must contain a definite cutoff which is supported by empirial research.
The following studies were excluded from this meta-analysis: (1) reviews, case reports, comments, letters, or editorials; (2) studies that only focused on a specific population such as CAYA who were obese, bullied, or experienced physical (e.g., stuttering) or mental illness (e.g., depression); and (3) articles that could not be retrieved in full-text form through online databases, library requests, or email correspondence with the authors of the studies.
Two reviewers (FC and QL) screened the title and/or abstracts independently and then retrieved the full texts and independently assessed them based on the inclusion and exclusion criteria. They used a standardized form to extract information such as authors, publication year, participants and setting, assessment tools, sample size, prevalence rate, and other subgroup data (e.g., gender). If the study was carried out at multiple time points, then data from the first time point were used because there might have been missing participants in the follow-ups. If multiple studies were based on the same dataset, the study with a larger sample size was included. Interrater reliability was calculated for continuous variables (e.g., prevalence, sample size) using intraclass correlation coefficients (ICC) and for categorical moderators (e.g., gender, sampling method) using Cohen's kappa. Interrater reliability was high (ICC = 0.99 and κ = 0.87 for continuous and categorical variables, respectively), and discrepancies were resolved through discussion. If a consensus could not be reached, other reviewers (ST and XT) discussed until they reached a consensus. Missing or additional data were requested from the original authors.
We assessed the quality of each study according to the Risk of Bias Tool for Prevalence Studies developed by Hoy et al. (2012). The tool has 10 items including external validity and internal validity subscales. The external validity subscale has four items including representation of the national population, sampling frame, random sampling, and nonresponse bias. The internal validity subscale has six items: data collected directly from the participants or a proxy, case definition, quality of instruments, consistency of data collection mode, duration of the prevalence period, and calculation of prevalence (see Supplementary material 3). Each item was assigned a score of 1 (low risk of bias) or 0 (high risk of bias). The sum of these items was the total score ranging from 1–10. Consistent with previous studies (Aminde et al., 2016), each study was classified as having a low (≥ 8), moderate (6–7), or high (≤5) risk of bias. Two investigators (XS and HT) independently rated the included studies, and inconsistencies were resolved by consensus or by the decision of other authors (ST and XT).
Due to the between-studies heterogeneity in the current review, a random effects model was used to combine prevalence estimates from multiple studies (Borenstein et al., 2010). It gave an overall estimate of prevalence rates across studies weighted by sample size. The I2 statistic was chosen as an indicator of heterogeneity. I2 values of 25, 50, and 75% are generally interpreted as mild, moderate, and high degrees of heterogeneity, respectively. An I2 <50% is considered acceptable (Higgins et al., 2003).
We performed subgroup analyses stratified by scales, gender, age group, sampling method, sample size, economic status, risk of bias, etc. Publication bias was assessed using funnel plots and Egger's tests (Egger et al., 1997; Sterne and Egger, 2001). We also calculated the “fail-safe N” to evaluate how many additional studies with zero effect would be needed to nullify the overall effect size. A fail-safe N greater than or equal to five times the number of observations plus 10 indicates a robust result (Rosenthal, 1979). Comprehensive Meta-Analysis (V2.0, Biostat, Englewood, NJ, USA) was used to perform the meta-analyses.
Figure 1 depicts the screening process. According to the search terms, a total of 2,747 unique records were found. Among these, 2,558 were excluded by screening titles and abstracts. A total of 189 full texts were retrieved for further assessment of eligibility. After the full-text screening, 17 articles met the inclusion criteria for social anxiety symptoms, and 11 were included for SAD (the full list of articles is shown in Supplementary material 4). Of the 161 articles that were excluded, 73 did not provide prevalence, 53 did not use valid measures for social anxiety, 16 did not focused on social anxiety, six did not provide a cutoff, five studies were not Chinese participants, and the rest were excluded due to duplicates (n = 4) not focusing on CAYA (n = 2), or focusing on specific groups (n = 1).
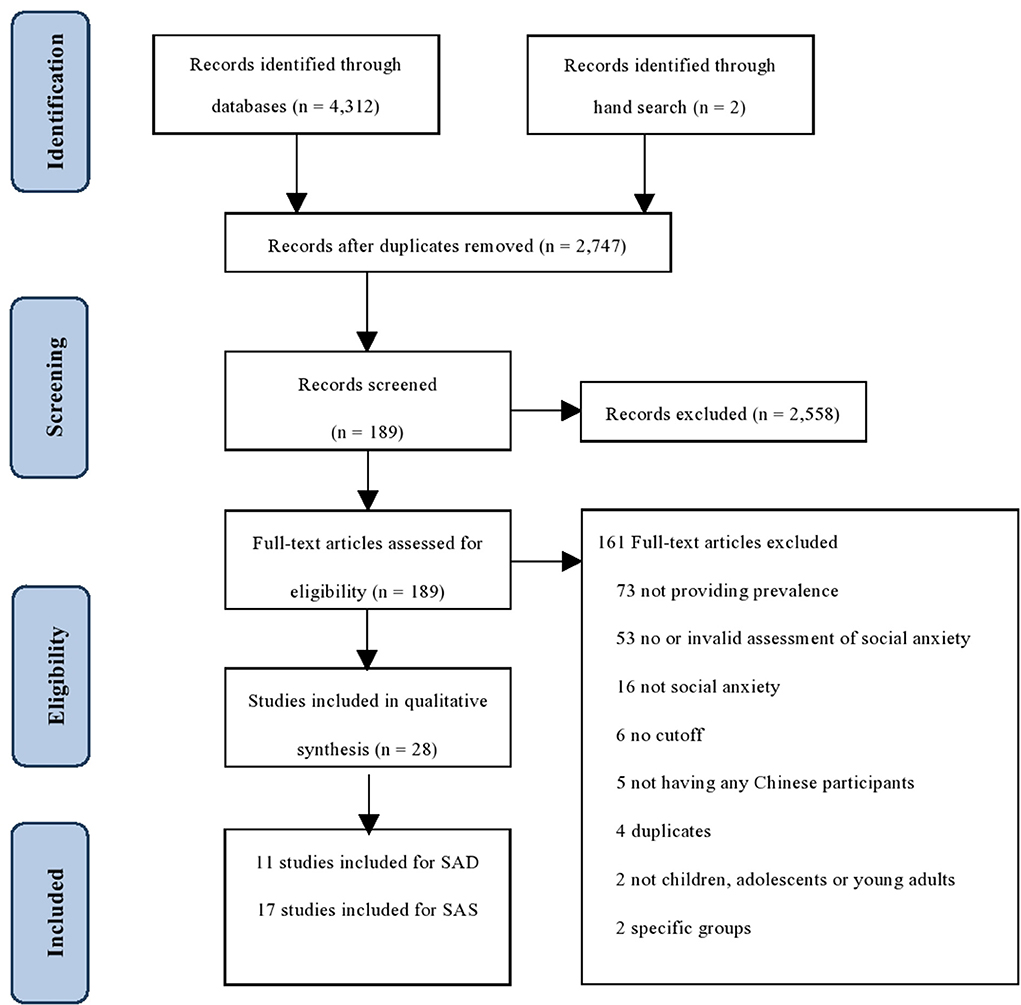
Figure 1. PRISMA flowchart of study selection.
Table 1 shows the characteristics of the included studies on SAD. Eleven independent studies were eligible for the meta-analysis, including a total of 60,921 participants. Six diagnostic instruments were used to identify SAD: the Structured Clinical Interview for DSM-IV (SCID-IV; n = 3), the Kiddie Schedule for Affective Disorders and Schizophrenia (K-SADS; n = 2), the Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-KID; n = 2), the Chinese Classification of Mental Disorders Version 3 (CCMD-3; n = 2), the Development and Wellbeing Assessment (DAWBA; n = 1), and the Composite International Diagnostic Interview Version 3.0 (CIDI 3.0; n = 1).
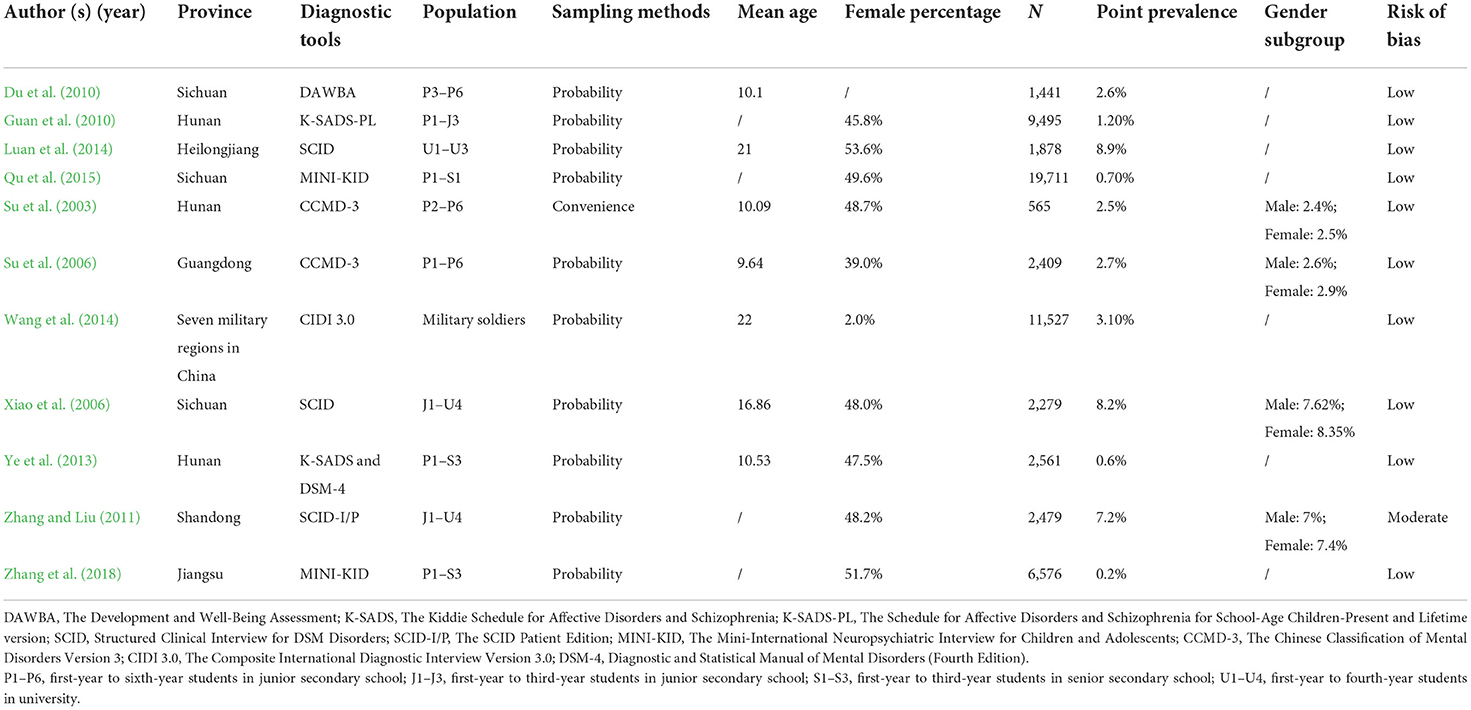
Table 1. Social anxiety disorder: study characteristics of the included studies.
The characteristics of studies on SAS is presented in Table 2. Seventeen studies were included involving a total of 17,677 participants. These studies had sample sizes ranging from 137 to 5,162 and covered nine provinces in China. Of the 17 included studies, 14 studies used convenience sampling, and only 3 studies used probability sampling. All studies were conducted in school settings, from primary schools to universities. Three self-report measures with different cutoffs were used to screen SAS: the Social Anxiety Scale for Children (SASC; cutoff ≥ 8, n = 5; cutoff ≥ 10, n = 6), the Liebowitz Social Anxiety Scale-Self Report (LSAS-SR; cutoff ≥ 38, n = 4), and the Social Phobia Inventory (SPIN; cutoff ≥ 20, n = 1; cutoff ≥ 25, n = 1).
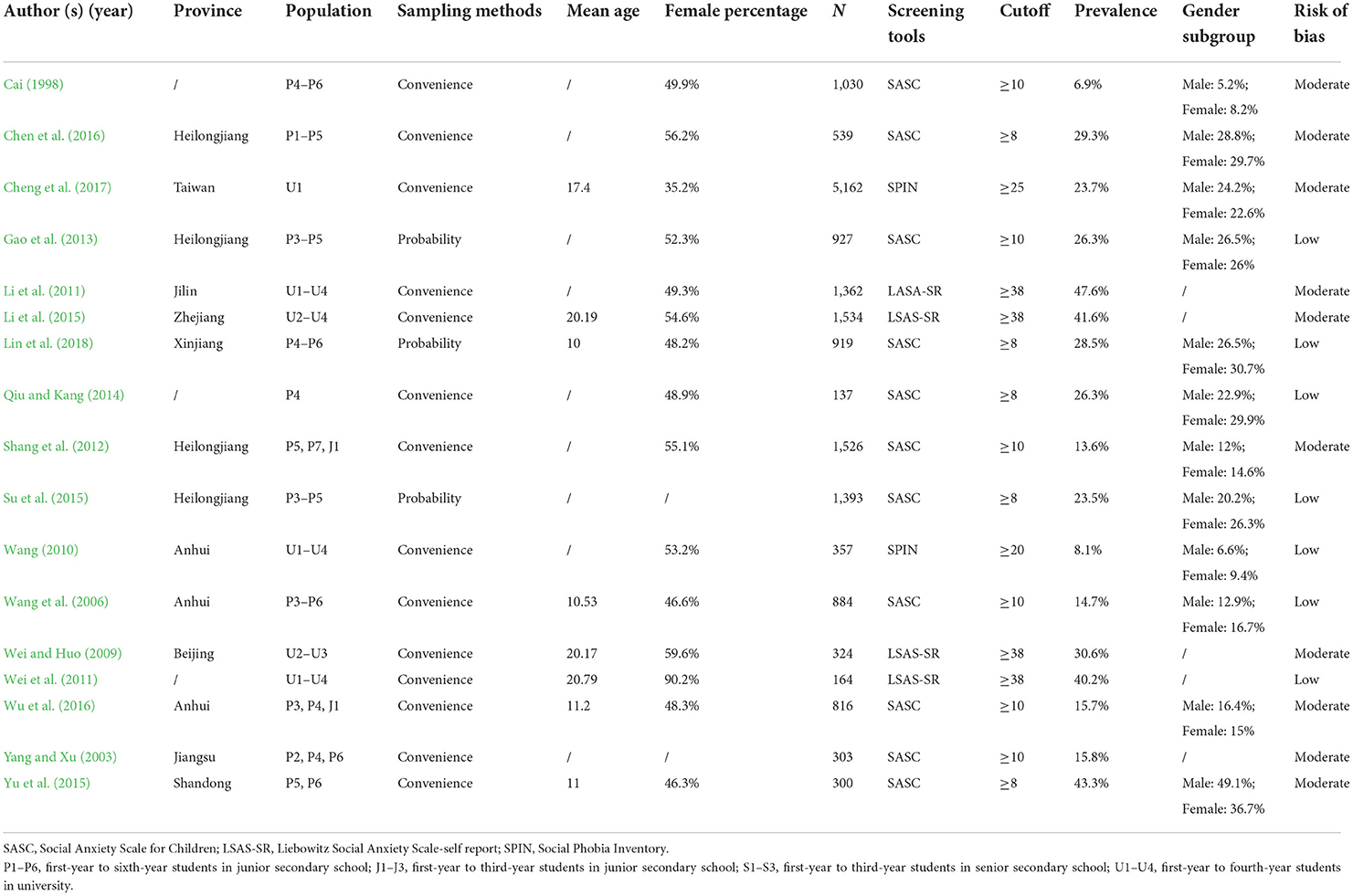
Table 2. Social anxiety symptoms: study characteristics of the included studies.
The overall point prevalence of SAD among Chinese CAYA was 2.1% (95% CI: 1.2–3.8%) with significant heterogeneity (Q = 1,055.2, I2 = 99.1%, p < 0.001; see Supplementary material 5). The overall pooled prevalence estimates of SAS yielded a crude summary prevalence of 23.5% (95% CI: 18.6–29.3%) with significant heterogeneity present (Q = 1019.3, I2 = 98.4%, p < 0.001; see Supplementary material 6).
The results of subgroup analysis of SAD are presented in Table 3. There were substantial differences in prevalence of SAD between different diagnostic instruments. Studies that employed SCID to identify SAD had the highest prevalence (8.1%; 95% CI: 6.1–10.6%) compared with studies that used CCMD-3 (2.6%; 95% CI: 1.7–4.1%), K-SADS (0.9%; 95% CI: 0.6–1.4%), and MINI-KID (0.4%; 95% CI: 0.3–0.7%; p < 0.001). CAYA above 15 years old (6.4%; 95% CI: 3.7–10.9%) had a higher prevalence of SAD than those below 15 years old (1.8%; 95% CI: 1–3.4%; p = 0.003). There were no significant differences in prevalence estimates between different economic statuses or genders.
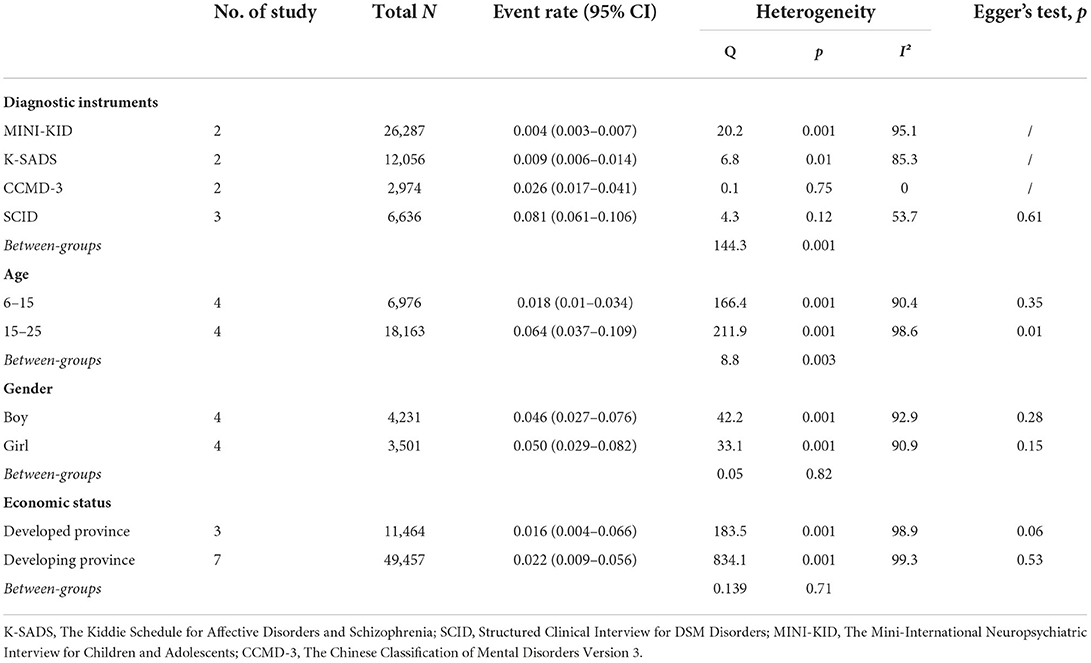
Table 3. Pooled event rates of social anxiety disorder grouped by moderators.
Table 4 shows the subgroup analysis of SAS studies. A significant difference in the prevalence of SAS was also observed between different self-reports with different cutoffs. The pooled prevalence was the highest with LSAS-SR with a cutoff of 38 (40%; 95% CI: 31.4–49.3%), followed by SASC with a cutoff of 8 (29.8%; 95% CI: 23.2%−37.3%) and SASC with a cutoff of 10 (14.7%; 95% CI: 11.2–19%; p < 0.001). When stratified by the economic status of location where the studies were conducted, participants from developed areas had higher combined prevalence estimates (32.8%; 95% CI: 21.4–42.8%) than those from developing areas (18.9%; 95% CI: 13.9–25.3%). CAYA aged 15–25 had a slightly higher prevalence of SAS (29.8%; 95% CI, 20.9–40.6%) than those aged 6–15 (20.6%; 95% CI, 15.4–26.9%). However, the difference was not significant (p = 0.100). Gender, sampling methods, and risk of bias were not significant moderators.
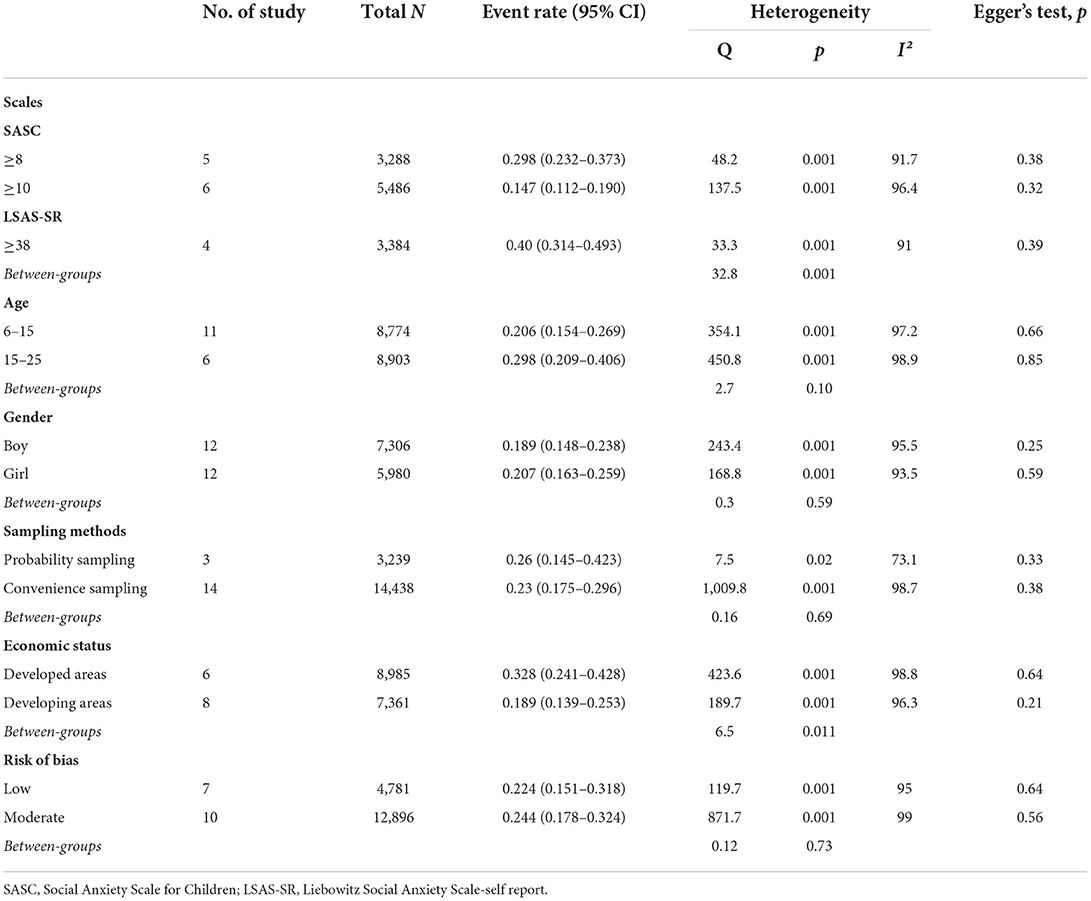
Table 4. Pooled event rates of social anxiety symptoms grouped by moderators.
For SAD, the majority (10 of 11) of the included studies were assessed as having low risk of bias, and only one study had a moderate risk of bias. The funnel plot (see Supplementary material 7) or Egger test (p = 0.28) did not find significant publication bias. The fail-safe N analysis suggested that an additional number of 5,182 studies with non-significant results would be required to reduce the overall effect size to a trivial level at p = 0.05, which indicated that the result was robust.
For SAS, seven of 17 studies were rated as having low risk of bias, while the other 10 studies had a moderate risk of bias. Publication bias in the prevalence of SAS was not detected in the funnel plot (see Supplementary material 8) or Egger test (p = 0.340). The fail-safe N calculation revealed that 2,627 additional studies with non-significant results would be needed to substantially change the overall effect to a trivial level at p = 0.05.
To our knowledge, this review is the first meta-analysis that provides prevalence estimates of SAD and its symptoms in Chinese CAYA.
The review showed that the point prevalence of SAD among Chinese CAYA was 2.1%. Direct comparisons are difficult to conduct because most studies in other countries tend to report 12-month or lifetime prevalence (Burstein et al., 2011; Knappe et al., 2011; Jefferies and Ungar, 2020; Mohammadi et al., 2020). However, there are some studies providing point prevalence rates in countries such as Spain (3.4%; Canals et al., 2019) and Austria (3.5%; Wagner et al., 2017), which had a higher prevalence than Chinese CAYA. This observation is consistent with Hofmann's review, which found that the prevalence of SAD is lower in Asian cultures than in European cultures (Hofmann et al., 2010). Meanwhile, the current study showed that the proportion of Chinese CAYA experiencing SAS was 23.5%. This prevalence estimate is comparable to the prevalence of CAYA in many other countries such as the United Kingdom (28.5%; Fahy et al., 2016), Italy (23.5%; Di Blasi et al., 2015), Spain (25.8%; Calvete, 2014), India (22.9%; Yuvaraj et al., 2018), and Saudi Arabia (25.8%; Hakami et al., 2017).
Our review was partially consistent with the findings of Krieg and Xu (2015)—that is, Chinese CAYA have a lower prevalence of SAD than their western counterparts, however, the prevalence of SAS is similar to their western counterparts.
The similar prevalence of SAS may be due to the fact that Chinese and Western CAYA are exposed to the same risk factors, such as low self-acceptance, negative self-evaluation, and fear of negative evaluation (Li et al., 2019; Peng et al., 2019; Liu et al., 2020). On the other hand, factors specific to Chinese culture, such as shame, may only provoke more social anxiety in early adulthood or in an older population (Zhong et al., 2008; Lau et al., 2009), with no additional effect in social anxiety in younger groups.
It might be true that Chinese CAYA experience a considerable amount of SAS, but this does not necessarily imply that they have a corresponding rate of SAD as their western counterparts did. A criterion of SAD is impairment in social functioning (American Psychiatric Association., 2013). Several cultural factors might reduce the possibility of social dysfunction in the Chinese population. First, in many individualistic cultures, fear and avoidance of social situations are regarded as problematic and might impair social functioning. However, collectivist cultures have greater acceptance of socially reticent behavior (Schreier et al., 2010). Studies have found that in Canadian children, reticent behavior was associated with peer rejection such as overt refusal and disagreement, but the same behavior was associated with positive responses such as approval in a Chinese sample (Chen et al., 2006). In addition, life interference was found to have a stronger relationship with social anxiety in Western youths than in East Asia (Rapee et al., 2011). Second, interpersonal harmony is highly valued in East Asian countries, especially in China (Zhang et al., 2005; Wei and Li, 2013). People might even maintain interpersonal harmony by suppressing their negative emotions (Wei et al., 2013). It is likely for individuals in western cultures to “express appropriate disagreement or disapproval to people they don't know very well” as listed in the LSAS scale (Fresco et al., 2001), whereas Chinese youth might display more fear and avoidance, which reduce the occurrence of social conflicts or dysfunction. Some studies have provided indirect support for this argument. Although Chinese youths feel relatively high levels of anxiety in social situations, they tend not to undermine social norms and interpersonal harmony. It is therefore less likely for them to experience social dysfunction, which is a necessary diagnostic criterion for SAD. However, the cultural factors need to be interpreted with caution. For example, interpersonal harmony may also put more social stress on the individual. In order to maintain interpersonal harmony, individuals may need to compromise and be more attentive to the impact of their behavior on others, which may in turn be a risk factor for social anxiety. More cross-cultural studies may need to be done in the future to explore the reasons for the manifestation of SAS and SAD in China.
The study showed that the prevalence of social anxiety disorder in older CAYA (i.e., aged 15–25) was significantly higher than that of younger CAYA (i.e., 6–15), whereas there was no difference in the prevalence of social anxiety symptoms between the two groups. These finding about the SAD aligns with the existing literature, which suggests that prevalence of SAD is still at a relatively low level in childhood and has a significant increase after early adolescence (Kim et al., 2010; Burstein et al., 2011; Spence et al., 2018). In contrast, the prevalence of SAS remains stable or even decrease from early adolescence to late adolescence (Inderbitzen-Nolan and Walters, 2000; Ranta et al., 2009, 2012). Rapee and Spence (2004) provided a possible explanation that the transition from high social anxiety symptoms to social anxiety disorder depends on the age at which the individual encounters social impairment. From childhood to young adulthood, their perceived social anxiety distress remains unchanged or even decreases, but their social functioning impairment increases when they enter the adolescence. Adolescents usually have to be faced with changes in school environments, physical development, and peer relationships (Simmons, 2017). They might confront more challenges in social aspects, tend to experience impairment in social functioning and therefore are more likely to suffer from SAD.
Although the study showed that the prevalence of SAS and SAD were slightly higher in girls than boys (SAS: 20.7% vs. 18.9; SAD: 5 vs. 4.6%), the differences were not significant (p >0.05). This result was in contrast with most of the existing literature, which suggests that females have a higher prevalence of social anxiety than males worldwide and that gender differences are larger in adolescents (Caballo et al., 2014; Asher et al., 2017; Asher and Aderka, 2018). Self-construal, again, might be one reason that explains the non-significant gender differences in the Chinese population. In western culture, men tend to construct and maintain an independent self-construal, whereas women tend to construct and keep an interdependent self-construal (Cross and Madson, 1997). Women's sense of self being more dependent on relationships with others could make them more prone to social anxiety. However, as mentioned above, all individuals in East Asian culture generally have a higher interdependent social construal (Krieg and Xu, 2018). This could make the gender difference in social anxiety among Chinese CAYA relatively small or non-significant. However, the lack of significant gender differences may be due to the broad age range of the study. Research showed that gender differences in social anxiety were more pronounced in mid- and late-adolescence than in childhood and early adolescence (Beesdo et al., 2009). As age increases into adulthood, the gender differences gradually decline (Espinosa et al., 2008). Therefore, combining data from these different age groups may have resulted in an insignificant gender difference.
It is worth noting that there are significant differences in the prevalence estimates between different self-report scales as well as diagnostic tools. For example, the pooled prevalence of SAS assessed by LSAS-SR is significantly higher than SASC, and the prevalence of SAD diagnosed by SCID is significantly higher than MINI-KID. The difference in diagnostic algorithms and the stringency with which these criteria are applied between measurement tools might be one possible factor that leads to differences in the pooled prevalence estimates (Pélissolo et al., 2000).
Strengths of the current meta-analysis include performing a thorough literature search in both English and Chinese databases and estimating prevalence for both SAS and SAD. However, the study has several limitations. First, there is high heterogeneity between studies that has not yet been explained by the hypothesized moderators (e.g., gender, sampling methods, measures). Second, relative to the large population of China, the numbers of studies and participants included in this meta-analysis are still inadequate and underrepresented. The results of this study could provide a reference for researchers and practitioners and cannot replace national, large-scale epidemiological surveys. Third, there was significant heterogeneity across the included studies. One important reason is that different studies used different measurement tools, that is, the prevalence estimates of SAS and SAD assessed by different self-report scales and diagnostic tools significantly differ. Other possible sources of heterogeneity may include differences in the geographic location of the sample, age, and sex ratio. Fourth, the present study included a wide age range (e.g., 6–25). There may be considerable heterogeneity in the prevalence of social anxiety across age groups and a combination of them may be misleading. In addition, studies on children (mean age between 6 and 10 years old) are very few in this meta-analysis, so the findings may be problematic when generalizing to this population. In sum, we need to be cautious when interpreting and applying these results.
Overall, our findings revealed that Chinese CAYA frequently experience SAS and SAD. It is hoped that more large-scale epidemiological surveys that use consistent screening and diagnostic tools will be conducted in the future to identify the accurate prevalence of social anxiety in this population. In addition, more culturally sensitive screening and diagnostic tools might need to be developed to identify SAS and SAD. If SAS constantly lead to psychological distress in the Chinese population, the criteria of SAD might need further revision. Finally, prevention and intervention programs to reduce social anxiety in Chinese CAYA are still scarce, and more rigorous randomized controlled trials are needed in the future.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
XT and ST contributed to the conception and design of the meta-analysis, contributed to the manuscript writing, revision, and approved the submitted version. QL, FC, HT, and XS conducted the coding of studies. All authors listed have made a substantial, direct, and intellectual contribution to the work, and approved it for publication.
This work was supported by the Renmin University of China New Faculty Start-Up Grant [22XNKJ27], the Guangdong Planning Office of Philosophy and Social Science [Grant Number GD20YSH06], and the Shenzhen University Natural Science Research Grant [Grant Number 860-000002110172].
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2022.792356/full#supplementary-material
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders (DSM-5®). Washington, DC: American Psychiatric Pub.
Amin, R., Svedberg, P., and Narusyte, J. (2019). Associations between adolescent social phobia, sickness absence and unemployment: a prospective study of twins in Sweden. Eur. J. Public Health 29, 931–936. doi: 10.1093/eurpub/ckz033
Aminde, L. N., Dzudie, A., and Kengne, A. P. (2016). Prevalent diabetes mellitus in patients with heart failure and disease determinants in sub-Saharan Africans having diabetes with heart failure: a protocol for a systematic review and meta-analysis. BMJ Open 6, e010097. doi: 10.1136/bmjopen-2015-010097
Asher, M., and Aderka, I. M. (2018). Gender differences in social anxiety disorder. J. Clin. Psychol. 74, 1730–1741. doi: 10.1002/jclp.22624
Asher, M., Asnaani, A., and Aderka, I. M. (2017). Gender differences in social anxiety disorder: A review. Clin. Psychol. Rev. 56, 1–12. doi: 10.1016/j.cpr.2017.05.004
Beesdo, K., Knappe, S., and Pine, D. S. (2009). Anxiety and anxiety disorders in children and adolescents: developmental issues and implications for DSM-V. Psychiatr. Clin. 32, 483–524. doi: 10.1016/j.psc.2009.06.002
Bernstein, G. A., Bernat, D. H., Davis, A. A., and Layne, A. E. (2008). Symptom presentation and classroom functioning in a nonclinical sample of children with social phobia. Depress. Anxiety 25, 752–760. doi: 10.1002/da.20315
Bijl, R. V., Ravelli, A., and Van Zessen, G. (1998). Prevalence of psychiatric disorder in the general population: results of The Netherlands Mental Health Survey and Incidence Study (NEMESIS). Soc. Psychiatry Psychiatr. Epidemiol. 33, 587–595. doi: 10.1007/s001270050098
Borenstein, M., Hedges, L. V., Higgins, J., and Rothstein, H. R. (2010). A basic introduction to fixed-effect and random-effects models for meta-analysis. Res. Synth. Methods 1, 97–111. doi: 10.1002/jrsm.12
Bruce, S. E., Yonkers, K. A., Otto, M. W., Eisen, J. L., Weisberg, R. B., Pagano, M., et al. (2005). Influence of psychiatric comorbidity on recovery and recurrence in generalized anxiety disorder, social phobia, and panic disorder: a 12-year prospective study. Am. J. Psychiatry 162, 1179–1187. doi: 10.1176/appi.ajp.162.6.1179
Burstein, M., He, J.-P., Kattan, G., Albano, A. M., Avenevoli, S., and Merikangas, K. R. (2011). Social phobia and subtypes in the National Comorbidity Survey–Adolescent Supplement: prevalence, correlates, and comorbidity. J. Am. Acad. Child Adolesc. Psychiatry 50, 870–880. doi: 10.1016/j.jaac.2011.06.005
Caballo, V. E., Salazar, I. C., Irurtia, M. J., Arias, B., Hofmann, S. G., and Team, C.-A. R. (2014). Differences in social anxiety between men and women across 18 countries. Pers. Individ. Dif. 64, 35–40. doi: 10.1016/j.paid.2014.02.013
Cai, L. (1998). Survey of Social Situations in 1030 Elementary School Students. Chin. J. School Doctor. 12, 32–33.
Calvete, E. (2014). Emotional abuse as a predictor of early maladaptive schemas in adolescents: Contributions to the development of depressive and social anxiety symptoms. Child Abuse and Neglect 38, 735–746. doi: 10.1016/j.chiabu.2013.10.014
Canals, J., Voltas, N., Hernández-Martínez, C., Cosi, S., and Arija, V. (2019). Prevalence of DSM-5 anxiety disorders, comorbidity, and persistence of symptoms in Spanish early adolescents. Eur. Child Adol. Psychiat. 28, 131–143. doi: 10.1007/s00787-018-1207-z
Chen, F., Li, H., Ren, X., Su, S., Xin, Z., and Wang, Y. (2016). A 2-year follow-up investigation of social anxiety and its maternal influencing factors of peasant- worker's children in Harbin. Chin. J. behave. Med. Brain Sci. 25, 467–471.
Chen, X., DeSouza, A. T., Chen, H., and Wang, L. (2006). Reticent behavior and experiences in peer interactions in Chinese and Canadian children. Dev. Psychol. 42, 656–665. doi: 10.1037/0012-1649.42.4.656
Cheng, S. H., Sun, Z. J., Lee, I. H., Lee, C. T., Chen, K. C., Tsai, C. H., et al. (2017). Factors related to self-reported social anxiety symptoms among incoming university students. Early Intervent. Psychiatry. 11, 314–321. doi: 10.1111/eip.12247
Cho, M. J., Kim, J.-K., Jeon, H. J., Suh, T., Chung, I.-W., Hong, J. P., et al. (2007). Lifetime and 12-month prevalence of DSM-IV psychiatric disorders among Korean adults. J. Nerv. Ment. Dis. 195, 203–210. doi: 10.1097/01.nmd.0000243826.40732.45
Coles, M. E., Ravid, A., Gibb, B., George-Denn, D., Bronstein, L. R., and McLeod, S. (2016). Adolescent mental health literacy: young people's knowledge of depression and social anxiety disorder. Journal of Adolescent Health 58, 57–62. doi: 10.1016/j.jadohealth.2015.09.017
Coyle, S., and Malecki, C. K. (2018). The association between social anxiety and perceived frequency and value of classmate and close friend social support. School Psych. Rev. 47, 209–225. doi: 10.17105/SPR-2017-0067.V47-3
Crome, E., Grove, R., Baillie, A. J., Sunderland, M., Teesson, M., and Slade, T. (2015). DSM-IV and DSM-5 social anxiety disorder in the Australian community. Aust. N. Z. J. Psychiatry 49, 227–235. doi: 10.1177/0004867414546699
Cross, S. E., and Madson, L. (1997). Models of the self: self-construals and gender. Psychol. Bull. 122, 5–37. doi: 10.1037/0033-2909.122.1.5
Crum, R. M., and Pratt, L. A. (2001). Risk of heavy drinking and alcohol use disorders in social phobia: a prospective analysis. Am. J. Psychiatry 158, 1693–1700. doi: 10.1176/appi.ajp.158.10.1693
Di Blasi, M., Pavia, L., Cavani, P., Lo Verso, G., and Schimmenti, A. (2015). Cannabis use and social anxiety in adolescence: the role of facilitation expectancies. J. Child Adolesc. Subst. Abuse 24, 397–404. doi: 10.1080/1067828X.2013.872066
Du, Q., Li, S., Dong, Z., Qiu, C., Liu, K., Meng, Y., et al. (2010). The analysis of social anxiety disorder prevalence rates and influencing factors of Chengdu primary school students. Chin. J. Behav. Med. Brain Sci. 19, 964–966.
Edlund, M. J., Wang, J., Brown, K. G., Forman-Hoffman, V. L., Calvin, S. L., Hedden, S. L., et al. (2018). Which mental disorders are associated with the greatest impairment in functioning? Soc. Psychiatry Psychiatr. Epidemiol. 53, 1265–1276. doi: 10.1007/s00127-018-1554-6
Egger, M., Smith, G. D., Schneider, M., and Minder, C. (1997). Bias in meta-analysis detected by a simple, graphical test. BMJ. 315, 629–634.
Eres, R., Lim, M. H., Lanham, S., Jillard, C., and Bates, G. (2021). Loneliness and emotion regulation: Implications of having social anxiety disorder. Aust. J. Psychol. 73, 46–56. doi: 10.1080/00049530.2021.1904498
Espinosa, X. P., Caballo, V. E., Salazar-Torres, I. C., Irurtia, M. J., Arias, B., Hofmann, S. G., et al. (2008). Social anxiety in 18 nations: sex and age differences. Psicología Conductual 16, 163–187.
Fahy, A. E., Stansfeld, S. A., Smuk, M., Smith, N. R., Cummins, S., and Clark, C. (2016). Longitudinal associations between cyberbullying involvement and adolescent mental health. J. Adolesc. Health 59, 502–509. doi: 10.1016/j.jadohealth.2016.06.006
Filho, A., Hetem, L., Ferrari, M., Trzesniak, C., Martín-Santos, R., Borduqui, T., et al. (2010). Social anxiety disorder: what are we losing with the current diagnostic criteria? Acta Psychiatr. Scand. 121, 216–226. doi: 10.1111/j.1600-0447.2009.01459.x
Finsaas, M. C., Kessel, E. M., Dougherty, L. R., Bufferd, S. J., Danzig, A. P., Davila, J., et al. (2020). Early childhood psychopathology prospectively predicts social functioning in early adolescence. J. Clin. Child Adolesc. Psychol. 49, 353–364. doi: 10.1080/15374416.2018.1504298
Fresco, D., Coles, M., Heimberg, R. G., Liebowitz, M., Hami, S., Stein, M. B., et al. (2001). The Liebowitz Social Anxiety Scale: a comparison of the psychometric properties of self-report and clinician-administered formats. Psychol. Med. 31, 1025–1035. doi: 10.1017/S0033291701004056
Gao, P., Shang, J., He, L., Ren, X., and Wang, Y. (2013). Survery of social anxiety and related influence factors of 3-5 grades studentgs in China. Chin. J. Child Health Care 21, 90–92.
Guan, B., Luo, X., Deng, Y., Wei, Z., Ye, H., Yuan, X., et al. (2010). Prevalence of psychiatric disorders in primary and middle school students in Hunan Province. Chin. J. Contemp. Pediatr. 12, 123–127.
Habibzadeh, F., Habibzadeh, P., and Yadollahie, M. (2016). On determining the most appropriate test cut-off value: the case of tests with continuous results. Biochem. Med. 26, 297–307. doi: 10.11613/BM.2016.034
Hakami, R. M., Mahfouz, M. S., Adawi, A. M., Mahha, A. J., Athathi, A. J., Daghreeri, H. H., et al. (2017). Social anxiety disorder and its impact in undergraduate students at Jazan University, Saudi Arabia. Ment. Ill. 9, 42–47. doi: 10.1108/mi.2017.7274
Heinrichs, N., Rapee, R. M., Alden, L. A., Bögels, S., Hofmann, S. G., Oh, K. J., et al. (2006). Cultural differences in perceived social norms and social anxiety. Behav. Res. Ther. 44, 1187–1197. doi: 10.1016/j.brat.2005.09.006
Higgins, J. P., Thompson, S. G., Deeks, J. J., and Altman, D. G. (2003). Measuring inconsistency in meta-analyses. BMJ 327, 557. doi: 10.1136/bmj.327.7414.557
Hofmann, S. G., Anu Asnaani, M., and Hinton, D. E. (2010). Cultural aspects in social anxiety and social anxiety disorder. Depress. Anxiety 27, 1117–1127. doi: 10.1002/da.20759
Hoy, D., Brooks, P., Woolf, A., Blyth, F., March, L., Bain, C., et al. (2012). Assessing risk of bias in prevalence studies: modification of an existing tool and evidence of interrater agreement. J. Clin. Epidemiol. 65, 934–939. doi: 10.1016/j.jclinepi.2011.11.014
Hunsley, J., and Mash, E. J. (2018). A Guide to Assessments That Work. 2nd ed. New York, NY: Oxford University Press.
Inderbitzen-Nolan, H. M., and Walters, K. S. (2000). Social Anxiety Scale for Adolescents: Normative data and further evidence of construct validity. J. Clin. Child Psychol. 29, 360–371. doi: 10.1207/S15374424JCCP2903_7
Jefferies, P., and Ungar, M. (2020). Social anxiety in young people: a prevalence study in seven countries. PLoS ONE 15, e0239133. doi: 10.1371/journal.pone.0239133
Katzelnick, D. J., Kobak, K. A., DeLeire, T., Henk, H. J., Greist, J. H., Davidson, J. R., et al. (2001). Impact of generalized social anxiety disorder in managed care. Am. J. Psychiatry 158, 1999–2007. doi: 10.1176/appi.ajp.158.12.1999
Kawakami, N., Takeshima, T., Ono, Y., Uda, H., Hata, Y., Nakane, Y., et al. (2005). Twelve-month prevalence, severity, and treatment of common mental disorders in communities in Japan: preliminary finding from the World Mental Health Japan Survey 2002–2003. Psychiatry Clin. Neurosci. 59, 441–452. doi: 10.1111/j.1440-1819.2005.01397.x
Kessler, R. C., Berglund, P., Demler, O., Jin, R., Merikangas, K. R., and Walters, E. E. (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 62, 593–602. doi: 10.1001/archpsyc.62.6.593
Kim, S.-J., Kim, B.-N., Cho, S.-C., Kim, J.-W., Shin, M.-S., Yoo, H.-J., et al. (2010). The prevalence of specific phobia and associated co-morbid features in children and adolescents. J. Anxiety Disord. 24, 629–634. doi: 10.1016/j.janxdis.2010.04.004
Knappe, S., Beesdo-Baum, K., Fehm, L., Stein, M. B., Lieb, R., and Wittchen, H.-U. (2011). Social fear and social phobia types among community youth: differential clinical features and vulnerability factors. J. Psychiatr. Res. 45, 111–120. doi: 10.1016/j.jpsychires.2010.05.002
Krieg, A., and Xu, Y. (2015). Ethnic differences in social anxiety between individuals of Asian heritage and European heritage: a meta-analytic review. Asian Am. J. Psychol. 6, 66–80. doi: 10.1037/a0036993
Krieg, A., and Xu, Y. (2018). From self-construal to threat appraisal: understanding cultural differences in social anxiety between Asian Americans and European Americans. Cult. Divers. Ethnic Minor. Psychol. 24, 1–12. doi: 10.1037/cdp0000194
Lau, A. S., Fung, J., Wang, S.-,w., and Kang, S.-M. (2009). Explaining elevated social anxiety among Asian Americans: Emotional attunement and a cultural double bind. Cult. Diver. Ethnic Minority Psychol. 15, 77–85. doi: 10.1037/a0012819
Lau, N., Zhou, A. M., Yuan, A., Parigoris, R., Rosenberg, A. R., and Weisz, J. R. (2022). Social skills deficits and self-appraisal biases in children with social anxiety disorder. J. Child Fam. Stud. 1–12. doi: 10.1007/s10826-021-02194-w
Leffler, J. M., Riebel, J., and Hughes, H. M. (2015). A review of child and adolescent diagnostic interviews for clinical practitioners. Assessment 22, 690–703. doi: 10.1177/1073191114561253
Li, J., Liu, Y., Wan, H., and Mei, S. (2011). Correlation between social anxiety and psychological traits among university students. Chin. J. Public Health. 27, 1073–1075. doi: 10.11847/zgggws2011-27-09-01
Li, M., Tang, G., Zhou, L., Yu, Z., and Mao, H. (2015). Association between social anxiety and excessive daytime sleepiness among college students. Chin. J. Public Health. 36, 1675–1677.
Li, Z., Li, C., Cao, J., Su, H., and Yu, H. (2019). Investigation on the prevalence and influencing factors of social anxiety among secondary vocational school students in Daqing. J. Neurosci. Mental Health 19, 12–16.
Liberati, A., Altman, D. G., Tetzlaff, J., Mulrow, C., Gøtzsche, P. C., Ioannidis, J. P., et al. (2009). The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 6, e1000100. doi: 10.1371/journal.pmed.1000100
Lin, S., Wang, D., Xian, Y., Yang, J., and Wu, P. (2018). Current status of social anxiety and depression among primary school students in Urumqi, China. Chin. J. Contemp. Pediatr. 20, 670–674. doi: 10.7499/j.issn.1008-8830.2018.08.013
Liu, X., Yang, Y., Wu, H., Kong, X., and Cui, L. (2020). The roles of fear of negative evaluation and social anxiety in the relationship between self-compassion and loneliness: a serial mediation model. Curr. Psychol. 1–9. doi: 10.1007/s12144-020-01001-x
Luan, Y., Cao, J., Zhou, Y., Yang, J., and Yang, J. (2014). The prevalence rate and growth environmental factors of social anxiety disorder among Daqing college students. Chin. J Behav. Med. Brain Sci. 23, 793–796.
McNeil, D. W. (2001). Terminology and evolution of constructs related to social phobia. In: Hofmann S. G., DiBartolo P. M., editors. Social Phobia and Social Anxiety: An Integration Needham Heights, MA: Allyn and Bacon. p. 8–19.
Merikangas, K. R., Avenevoli, S., Acharyya, S., Zhang, H., and Angst, J. (2002). The spectrum of social phobia in the Zurich cohort study of young adults. Biol. Psychiatry 51, 81–91. doi: 10.1016/S0006-3223(01)01309-9
Mohammadi, M. R., Salehi, M., Khaleghi, A., Hooshyari, Z., Mostafavi, S. A., Ahmadi, N., et al. (2020). Social anxiety disorder among children and adolescents: A nationwide survey of prevalence, socio-demographic characteristics, risk factors and co-morbidities. J. Affect. Disord. 263, 450–457. doi: 10.1016/j.jad.2019.12.015
Pélissolo, A., Andr,é, C., Moutard-Martin, F., Wittchen, H., and Lépine, J. (2000). Social phobia in the community: relationship between diagnostic threshold and prevalence. European Psychiatry 15, 25–28. doi: 10.1016/S0924-9338(00)00214-5
Peng, S., Wang, X., Niu, G., Zhang, H., and Hu, X. (2019). Fear of negative evaluation on social anxiety: base on cognitive behavioral model of social anxiety disorder. Psychol. Dev. Edu. 35, 121–128. doi: 10.16187/j.cnki.issn1001-4918.2019.01.14
Qiu, W., and Kang, K. (2014). Social anxiety of rural children in the fourth grade of a primary school. J. Campus Life Ment. Health. 12, 247–248.
Qu, Y., Jiang, H. Y., Zhang, N., Wang, D. H., and Guo, L. T. (2015). Prevalence of Mental Disorders in 6-16-Year-Old Students in Sichuan Province, China. Int. J. Environ. Res. Public Health. 12, 5090–5107. doi: 10.3390/ijerph120505090
Ranta, K., Junttila, N., Laakkonen, E., Uhmavaara, A., La Greca, A. M., and Niemi, P. M. (2012). Social Anxiety Scale for Adolescents (SAS-A): measuring social anxiety among Finnish adolescents. Child Psychiatry Hum. Dev. 43, 574–591. doi: 10.1007/s10578-012-0285-2
Ranta, K., Kaltiala-Heino, R., Rantanen, P., and Marttunen, M. (2009). Social phobia in Finnish general adolescent population: prevalence, comorbidity, individual and family correlates, and service use. Depress. Anxiety 26, 528–536. doi: 10.1002/da.20422
Rapee, R. M., Kim, J., Wang, J., Liu, X., Hofmann, S. G., Chen, J., et al. (2011). Perceived impact of socially anxious behaviors on individuals' lives in Western and East Asian countries. Behav. Ther. 42, 485–492. doi: 10.1016/j.beth.2010.11.004
Rapee, R. M., and Spence, S. H. (2004). The etiology of social phobia: Empirical evidence and an initial model. Clin. Psychol. Rev. 24, 737–767. doi: 10.1016/j.cpr.2004.06.004
Rosenthal, R. (1979). The file drawer problem and tolerance for null results. Psychol. Bull. 86, 638–641. doi: 10.1037/0033-2909.86.3.638
Ruscio, A. M., Brown, T. A., Chiu, W. T., Sareen, J., Stein, M. B., and Kessler, R. C. (2008). Social fears and social phobia in the USA: results from the National Comorbidity Survey Replication. Psychol. Med. 38, 15–28. doi: 10.1017/S0033291707001699
Scharfstein, L. A., Beidel, D. C., Sims, V. K., and Finnell, L. R. (2011). Social skills deficits and vocal characteristics of children with social phobia or Asperger's disorder: a comparative study. J. Abnorm. Child Psychol. 39, 865–875. doi: 10.1007/s10802-011-9498-2
Schreier, S. S., Heinrichs, N., Alden, L., Rapee, R. M., Hofmann, S. G., Chen, J., et al. (2010). Social anxiety and social norms in individualistic and collectivistic countries. Depress. Anxiety 27, 1128–1134. doi: 10.1002/da.20746
Shang, J., Chen, X., He, L., Ren, X., and Wang, Y. (2012). Effect of maternal anxiety, depression, acceptance and psychological control on students? social anxiety. Chin. J Behav. Med. Brain Sci. 21, 778–780.
Shen, Y.-C., Zhang, M.-Y., Huang, Y.-Q., He, Y.-L., Liu, Z.-R., Cheng, H., et al. (2006). Twelve-month prevalence, severity, and unmet need for treatment of mental disorders in metropolitan China. Psychol. Med. 36, 257–267. doi: 10.1017/S0033291705006367
Simmons, R. G. (2017). Moving Into Adolescence: The Impact of Pubertal Change and School Context. Milton Park: Routledge.
Spence, S. H., Zubrick, S. R., and Lawrence, D. (2018). A profile of social, separation and generalized anxiety disorders in an Australian nationally representative sample of children and adolescents: Prevalence, comorbidity and correlates. Aust. N. Z. J. Psychiatry 52, 446–460. doi: 10.1177/0004867417741981
Springer, K. S., Levy, H. C., and Tolin, D. F. (2018). Remission in CBT for adult anxiety disorders: a meta-analysis. Clin. Psychol. Rev. 61, 1–8. doi: 10.1016/j.cpr.2018.03.002
Stein, D. J., Lim, C. C., Roest, A. M., De Jonge, P., Aguilar-Gaxiola, S., Al-Hamzawi, A., et al. (2017). The cross-national epidemiology of social anxiety disorder: data from the World Mental Health Survey Initiative. BMC Med. 15, 143. doi: 10.1186/s12916-017-0889-2
Stein, M. B., Fuetsch, M., Müller, N., Höfler, M., Lieb, R., and Wittchen, H.-U. (2001). Social anxiety disorder and the risk of depression: a prospective community study of adolescents and young adults. Arch. Gen. Psychiatry 58, 251–256. doi: 10.1001/archpsyc.58.3.251
Sterne, J.A., and Egger, M. (2001). Funnel plots for detecting bias in meta-analysis: guidelines on choice of axis. J. Clin. Epidemiol. 54, 1046–1055.
Stroup, D. F., Berlin, J. A., Morton, S. C., Olkin, I., Williamson, G. D., Rennie, D., et al. (2000). Meta-analysis of observational studies in epidemiology: a proposal for reporting. JAMA 283, 2008–2012. doi: 10.1001/jama.283.15.2008
Su, C., Huang, G., HU, L., Zhang, X., Ni, S., Lin, J., et al. (2006). Epidemiological Survey of Social Anxiety Disorder in Pupils of Zhanjiang Urban Districts. Chin. Ment. Health J. 20, 736–739. doi: 10.3321/j.issn:1000-6729.2006.11.013
Su, L., Yin, Q., Wang, K., Zhu, Y., Tang, J., and Luo, X. (2003). Anxiety disorders in Chinese elementary school pupils. Chin. J. Nerv. Ment. Dis. 29, 330–333.
Su, S., Ren, X., Chen, F., Li, H., and Wang, Y. (2015). Study on 4-year follow-up of the students' social anxiety detection about 684 students in Harbin. Chin. J. Child Health Care. 23, 465–467.
Wagner, G., Zeiler, M., Waldherr, K., Philipp, J., Truttmann, S., Dür, W., et al. (2017). Mental health problems in Austrian adolescents: a nationwide, two-stage epidemiological study applying DSM-5 criteria. Eur. Child Adolesc. Psychiatry 26, 1483–1499. doi: 10.1007/s00787-017-0999-6
Wang, H., Zhang, R., Chen, Y., Wang, H., Zhang, Y., Gan, J., et al. (2014). Social anxiety disorder in the Chinese military: prevalence, comorbidities, impairment, and treatment-seeking. Psychiatry Res. 220, 903–908.
Wang, J. (2010). Relationship between social anxiety and type of temperament in college students. Chin. J. School Doctor. 24, 500–501.
Wang, L., Zhang, S., Sun, Y., and Zhang, X. (2006). Social anxiety and the influencing factors among pupils in rural area in Anhui. Chin. J. School Health. 27, 853–855.
Wei, M., Su, J. C., Carrera, S., Lin, S.-P., and Yi, F. (2013). Suppression and interpersonal harmony: A cross-cultural comparison between Chinese and European Americans. J. Couns. Psychol. 60, 625–633. doi: 10.1037/a0033413
Wei, X., and Li, Q. (2013). The Confucian value of harmony and its influence on Chinese social interaction. Cross Cult. Commun. 9, 60–66. doi: 10.3968/j.ccc.1923670020130901.12018
Wei, Z., and Huo, L. (2009). Study on the relationship between social anxiety and adult attachment styles of college students. Chin. J. Health Psychol. 17, 954–957.
Wei, Z., Sun, H., and Huo, L. (2011). Study on the relationship between social anxiety and adult attachment styles among junior college nursing students. J. Nurs. Admin. 11, 554–556.
Wittchen, H. U., and Fehm, L. (2003). Epidemiology and natural course of social fears and social phobia. Acta Psychiatr. Scand. 108, 4–18. doi: 10.1034/j.1600-0447.108.s417.1.x
Wong, Q. J., Gregory, B., and McLellan, L. F. (2016). A review of scales to measure social anxiety disorder in clinical and epidemiological studies. Curr. Psychiatry Rep. 18, 38. doi: 10.1007/s11920-016-0677-2
Wu, Y. -L., Zhao, X., Li, Y. -F., Ding, X. -X., Yang, H. -Y., Bi, P., et al. (2016). The risk and protective factors in the development of childhood social anxiety symptoms among Chinese children. Psychiatry Res. 240, 103–109.
Xiao, R., Wu, W., Hu, J., Qiu, C., Qiang, W., Geng, W., et al. (2006). Prevalence and risk factors of social anxiety disorder in high schools and universities in Chengdu. J. Sichuan Univ. Med. Sci. Edn. 37, 636–640.
Yang, H., and Xu, H. (2003). A survery and treatment of primary school students' social anxiety. J. Chin. Soc. Educ. 2, 46–47.
Ye, H., Luo, X., Yuan, X., Wei, Z., Guan, B., and Ning, Z. (2013). Epidemiological investigation of anxiety disorders in primary and middle school students in Changsha area. J. Xinxiang Med. Univ. 30, 814–816.
Yu, X., Zhu, X., Zheng, H., Zhao, Y., Ma, H., and Cheng, S. (2015). Relationship of parents' upbringing mode, type of temperament and children's social anxiety. J. Hebei Unit. Univ. 17, 46–49.
Yuvaraj, K., Kumar, G. D., Priyan, S., Yamini, M., Kumar, S. G., and Subitha, L. (2018). Prevalence and associated factors for social phobia among school-going adolescents in a rural area of Puducherry, South India. Int. J. Adolesc. Med. Health. 33. doi: 10.1515/ijamh-2018-0037
Zhang, J., Zhao, B., Yao, H., Sun, X., and Zhang, C. (2018). Prevalence of mental disorders in 6-16-year-old students in Zhenjiang, Jiangsu Province. J. Neurosci. Ment. Health. 18, 718–722.
Zhang, Q., and Liu, C. (2011). An epidemiological survey of social anxiety disorders among college students in Qingzhou. J. Chin. Trad. Chin. Med. Infm. 3, 43.
Zhang, Y. B., Lin, M.-C., Nonaka, A., and Beom, K. (2005). Harmony, hierarchy and conservatism: A cross-cultural comparison of Confucian values in China, Korea, Japan, and Taiwan. Commun. Res. Rep. 22, 107–115. doi: 10.1080/00036810500130539
Keywords: children, adolescents, young adults, China, prevalence, social anxiety
Citation: Tang X, Liu Q, Cai F, Tian H, Shi X and Tang S (2022) Prevalence of social anxiety disorder and symptoms among Chinese children, adolescents and young adults: A systematic review and meta-analysis. Front. Psychol. 13:792356. doi: 10.3389/fpsyg.2022.792356
Received: 16 November 2021; Accepted: 28 July 2022;
Published: 22 August 2022.
Edited by:
Seth Oppong, University of Botswana, BotswanaReviewed by:
Peter Jonathan Cooper, University of Reading, United KingdomCopyright © 2022 Tang, Liu, Cai, Tian, Shi and Tang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Suqin Tang, amFzbWluZXRzcUBob3RtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.