 Nicolaas Cornelis Verhoef
Nicolaas Cornelis Verhoef Robert Jan Blomme
Robert Jan Blomme
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychol. , 15 December 2022
Sec. Organizational Psychology
Volume 13 - 2022 | https://doi.org/10.3389/fpsyg.2022.1064889
This article is part of the Research Topic Healthcare Management: Challenges for Improving Performance and Quality of Patient Services View all 8 articles
Burnout is a major social and economic problem, specifically among general practitioners (GPs). The amount of literature on generic determinants of burnout is impressive. However, the size of the library on occupation-specific determinants of burnout among GPs are minimal. With the present study, we aim to gain insight into the existing academic literature on generic and occupation-specific determinants of burnout among GPs. Moreover, we aim to contribute to the ecological validity of this study by emphasizing occupation-specific determinants. We conducted a systematic quantitative literature review in which we followed the PRISMA statement and performed quality assessments according to the AXIS, CASP, MMAT, and 3-MIN procedures. Furthermore, we assessed frequency effect sizes (FES) and intensity effect sizes (IES). By performing Fisher’s exact tests, we investigated whether the quality of the studies influenced the outcomes. An extensive literature search revealed 60 eligible studies among which 28 strong studies, 29 moderate studies, and 3 weak studies were identified. Analyzing those studies delivered 75 determinants of burnout, of which 33 were occupation-specific for GPs. According to the average FES, occupation-specific determinants play a significant role in acquiring burnout compared to the generic determinants. The results of the Fisher exact tests provided evidence that the quality of the 60 studies did not affect the outcomes. We conclude that it is surprising that a profession with such an important social position and such a high risk of burnout has been so little researched.
In the general working population, burnout is considered a significant social and economic problem (Collier, 2017). In contrast to many other professions, relatively little is known about the causes of burnout among general practitioners (GPs).
Burnout is a psychological syndrome characterized by the three core symptoms of emotional exhaustion, depersonalization, and diminished personal effectiveness (Freudenberger and Richelson, 1980; Maslach et al., 2001). Since the introduction of the concept of burnout in the 1970s by Herbert Freudenberger, many studies have passed, attempting to explain this intriguing phenomenon (Freudenberger, 1974). Indeed, after introducing the Maslach Burnout Inventory (MBI) (Maslach and Jackson, 1981), a psychological assessment tool to measure the three dimensions of burnout, the research on this subject exploded (Maslach et al., 1996). Not surprisingly, considering the background of Freudenberger, the initial researchers found burnout exclusively related to human services, such as social work, healthcare, and teaching (Maslach and Schaufeli, 1993). However, the historical imperfection of exclusively relating burnout to human services, has been corrected abundantly in the past two decennia given a large amount of literature outside the human service sectors (Maslach and Schaufeli, 1993). Moreover, there was no theoretical argument to limit burnout to the human service professions (Maslach and Leiter, 1997). Moreover, there is enough evidence that shows that stressors leading to burnout in human services can be found in other non-human service professions as well (Buunk et al., 1998). Therefore, there appears to be sufficient theoretical arguments for releasing the initial conventional definition, restricting burnout to the human service professions. To meet this shortcoming of the Maslach Burnout Inventory-Human Services Survey (MBI-HSS), the Maslach Burnout Inventory–General Survey (MBI-GS) was developed, which was suitable for all workers, including those without intensive contact with recipients of services. One of the main differences between the two versions of the MBI was that the depersonalization scale from the MBI-HSS was transformed into the cynicism scale in the MBI-GS. Both scales reflect the social perception of distancing, distancing from people in the case of depersonalization and distancing from things in the case of cynicism (Schaufeli and Leiter, 1996). Simultaneously, the Oldenburg Burnout Inventory (OLBI) was developed, which consists of two dimensions: emotional exhaustion and disengagement from work (Demerouti, 1999). Despite their strengths and weaknesses, the MBI-HSS, the MBI-GS, and the OLBI are all widely practised.
According to Schaufeli and Taris (2005), burnout should be conceptualized, primarily as a work-related syndrome with at least emotional exhaustion and depersonalization as dimensions. One of the criticisms of the MBI is that depersonalization is a coping strategy under certain circumstances and should be better studied along with other coping strategies (Tipa et al., 2019). Furthermore, diminished personal efficiency, one of the three burnout dimensions of the MBI, should be perceived as one of the many consequences of long-term stress (Kristensen et al., 2005). These and other objections are amply and dignifiedly refuted by Schaufeli and Taris (2005). To address these concerns, the OLBI (Demerouti et al., 2003) was developed. One of the limitations of the OLBI is its limited construct validity (Halbesleben, 2003). However, a detailed discussion of this debate is beyond the scope of this study. Despite all the criticism, both the OLBI and the MBI are still widely used measurement tools today.
It is remarkable and as yet not easy to explain why the MBI is still so popular, despite all the criticism.
In response to the many well-documented objections to the MBI, a new Burnout Assessment Tool (BAT) has been developed (Schaufeli et al., 2019, 2020). The BAT comprises four core dimensions: exhaustion, mental distance, and emotional and cognitive impairment. Moreover, three secondary dimensions emerged: depressed mood, psychological distress, and psychosomatic complaints.
To classify the determinants of burnout globally, this study distinguished between job demands, job resources, and personal resources. Job demands are defined as those physical, social or organizational aspects of the job that require sustained physical or mental effort and are therefore associated with maintaining physiological and psychological costs (Demerouti et al., 2001). Examples of generic job demands are work overload and interpersonal conflict. Job resources were defined as those physical, social or organizational aspects of the job that may do any of the following: (a) be functional in achieving work goals; (b) reduce job demands and the associated physiological and psychological costs; (c) stimulate personal growth and development (Demerouti et al., 2001). Examples of generic job resources are feedback and social support. Personal resources are defined as the psychological characteristics or aspects of the self that are generally associated with resiliency and that refer to the ability to control and impact one’s environment successfully (Schaufeli and Taris, 2014). Examples of personal resources are self-efficacy and optimism. Extensive overviews of generic job demands, generic job resources and personal resources have been published by, among others, Lee and Ashforth (1996) and Schaufeli and Taris (2014).
Common theories in this regard are the job demands resources (JDR) theory and the conservation of resources (COR) theory. The JDR theory states that a balance between all possible work demands and all possible resources leads to the health and wellbeing of the worker (Demerouti et al., 2001; Schaufeli and Taris, 2014). The JDR model distinguishes two underlying processes, namely the health-limiting or energetic process and the motivational process (Demerouti et al., 2001). The health-limiting process arises at work demands and is mainly focused on exhaustion. The motivational process arises at work resources and is mainly focused on depersonalization. The JDR theory explains that there is an interaction between job demands and work resources, but the theory does not explain why, this requires additional psychological theories, such as the COR theory (Hobfoll, 2002). The central assumption of the COR theory is that people strive to preserve and protect the things they value, the resources. According to the COR theory, stress then arises when critical resources are threatened with loss, when they are lost, or when they are insufficiently regained after intensive effort (Hobfoll, 2002).
To empirically assess occupational stress, researchers usually study the effect of work demands and work resources on, for example, burnout. This research is usually done through questionnaires with generic job demands and job resources (Brough et al., 2009). The use of generic job demands and job resources is primarily driven by the wide range of occupations to which they apply so that the outcomes of studies can be compared between themselves but also with normative data (Brough et al., 2009).
The inclusion of occupation-specific job demands and job resources focuses on the assessment of the specific work context. This not only increases the ecological validity of the assessment but also improves the description of the work environment (e.g., Brough and Frame, 2004). The assessment of occupation-specific job demands and job resources is also beneficial for the development of targeted interventions (e.g., O’Driscoll et al., 2009). Finally, it is often overlooked by researchers that examining occupation-specific job demands and job resources simultaneously, yields additional explained variance over the generic job demands and job resources (e.g., Kop et al., 1999).
Occupational job demands and job resources have now been examined for various professions, for example, police officers (Juniper et al., 2010), teachers (Van der Doef and Maes, 2002; Bakker et al., 2007), firefighters (Tuckey and Hayward, 2011), prison staff (Brough and Biggs, 2015), nurses (Sundin et al., 2011), dentists (Hakanen et al., 2005), and GPs (Bakker et al., 2000a; Cathebras et al., 2004).
Traditionally, stressors or job demands of GPs have been related to the emotionally charged doctor-patient relationship. The demanding nature of the doctor-patient relationship has once been considered the root cause of burnout (Maslach, 1978). In the meantime, other than emotionally bound occupation-specific job demands for GPs have been identified, for example, high workload, and administrative job demands but also conflicts with social work (Cathebras et al., 2004).
Given the above-described added value of research into occupation-specific job demands and job resources, and the importance for a society of a well-functioning and healthy primary healthcare system, in particular for GPs, it is surprising that so little is known about occupation-specific job demands and job resources of GPs. The amount of academic literature on the determinants of burnout is impressive. However, the amount of literature on the determinants of burnout among GPs is much less. The amount of literature on occupation-specific determinants of burnout among GPs is very limited.
Therefore, the present study aims to gain insight into the existing academic literature on generic and occupation-specific determinants of burnout among GPs. We aim to contribute insight into and knowledge of the determinants that govern the mental energy household of GPs and that often lead to burnout. Moreover, by emphasizing occupation-specific determinants, we want to contribute to the ecological validity of this study.
We propose the following research question for the present study:
What is the current state of knowledge regarding the generic and occupation-specific determinants of burnout among GPs?
In the present study, we used the systematic quantitative literature review (Pickering and Byrne, 2014). The method is systematic because of how studies are initially identified for inclusion, i.e., explicit and reproducible. The method quantifies where there is research but also where there are gaps. The technique can be used for all types of studies, qualitative, quantitative and mixed-method. The method bridges the gap between traditional narrative review methods and meta-analyses (Pickering and Byrne, 2014).
The present study was conducted in four phases. First, the literature search was conducted over the period 1970–2021. In the first phase, existing literature on determinants of burnout among GPs was collected. The beginning of the search marks a period when the term burnout was introduced in the scientific literature by Freudenberger (1974) and Maslach (1976). The search was performed with the search terms “burnout,” “general practice,” “GP,” “family practitioner,” “family doctor,” “family physician,” “primary care,” “primary care practitioner,” “primary care doctor,” “primary care physician,” and combinations of these search terms. The following search engines were used: Open University digital library interface, including Web of Science, Embase, PsycINFO, Google Scholar, PubMed, and Mendeley.
The following inclusion criteria were used in the second phase, the screening phase, to narrow the natural result. An abstract of an identified study must be available for screening purposes, and the language of the study must be Dutch or English. Type of study means any study that addresses the nature of a determinant and its relationship with burnout, i.e., no intervention studies. In 2016, a comparative study on GPs was published by Schäfer et al. (2016), which included 34 nationalities because they have comparable and well-documented primary care. It concerns 31 European countries, Canada, Australia, and New Zealand. The inclusion criterion “Nationality” in the present study is based on the said study by Schäfer et al. (2016), i.e., we used the 34 nationalities as a “Nationality” inclusion criterion. A separate inclusion criterion, the “Language” criterion, which is separate from the “Nationality” criterion, is the language in which the study is published and must be English or Dutch.
The USA is a rich source of scientific literature on primary care. This literature has provided evidence that a well-developed primary healthcare system offers benefits in terms of better coordination, continuity of care and possibilities for cost control. However, part of this research has limited relevance to the European situation (Kringos et al., 2010). Therefore, in the current study, we have limited ourselves to the European situation, and a comparable situation, i.e., the 34 nationalities mentioned in the study by Schäfer et al. (2016).
After identifying duplicate studies and screening on title and abstract with the above inclusion criteria, phase three followed.
In the third phase, the full text of the remaining studies was reviewed and assessed against the same inclusion criteria as in the previous screening phase. Naturally, the full text of the study had to be available. The remaining studies were used for further analysis in the next phase.
In the fourth and final phase, the remaining studies were coded according to a range of variables: authors, year of publication, source journal, area of focus of the journal, study location, type of study, psychological theories used, and outcomes of the studies. Finally, the results of the studies were ranked according to generic and occupation-specific job demands and job resources, job characteristics, socio-demographic data, personal characteristics and a group of miscellaneous. The miscellaneous group consists of determinants that cannot be classified into other categories.
At several points in the procedure, decisions have to be made that are open to discussion. Making those decisions by only one reviewer increases the risk of selection bias. For example concerning the inclusion criteria or the distinction between generic and occupation-specific work demands and resources. Concerning the latter, the distinction between generic and occupation-specific work demands and resources is made by several authors who have used a profession-specific measurement scale, for example, Bakker et al. (2007) concerning teachers and Hakanen et al. (2005) concerning dentists. Therefore, in the present study, we have taken the measurement scale for job-specific work demands and resources from our previous study (Verhoef et al., 2021) as a starting point and the categories in the current study have been adjusted accordingly.
To better compare and interpret the results, two effect sizes were calculated, namely, the frequency effect size (FES) and the intensity effect size (IES) (Onwuegbuzie, 2003; Sandelowski et al., 2007). The FES is used to determine the relative magnitude of the abstracted findings and is calculated by dividing the number of studies that found a result by the total number of studies. The IES represents the impact of a study and is calculated by dividing the number of findings in that study by the total number of results in all studies.
As part of a systematic review, a formal assessment of the quality of studies indicates the strength of the evidence on which conclusions are based. This makes it possible to compare studies based on the risk of bias (Whiting et al., 2017). Following the PRISMA statement, the present study established the quality of our identified studies (Page et al., 2021). The quality of the quantitative studies was assessed according to the AXIS procedure (Downes et al., 2016); the quality of the qualitative studies to the CASP procedure for qualitative studies (Long et al., 2020); the quality of the mixed methods studies according to MMAT procedure (Hong et al., 2018); the quality of the meta-analysis according to the 3-MIN procedure (Hussain et al., 2011) and the quality of the systematic review according to the CASP procedure for systematic reviews (Nadelson and Nadelson, 2014).
It is a conventional view that research questions should guide decisions about the design and methodology of a research project (Bryman, 2007). Therefore, it is an essential element of quantitative, qualitative and mixed-method studies (Haynes, 2006). Furthermore, there are various methods to construct a good research question, for example, the Picot criteria (Haynes, 2006) and the Finer criteria (Hulley, 2007).
A hypothesis is a proposed explanation of a phenomenon and is used to answer the research question. As usual, a hypothesis is based on both the theoretical expectation about how things work and on the pre-existing empirical evidence. Finally, hypotheses are tested using the collected data (Haynes, 2006; Hulley, 2007).
Thorough increase and improvement of knowledge are of the utmost importance in any scientific discipline. Therefore, it is also crucial to investigate the quality of a study, and whether a research question, a theoretical foundation, and hypotheses are present in that study. Since the quality assessments used in this literature review, namely the AXIS procedure, the CASP procedure, the MMAT procedure, and the 3-MIN procedure, do not explicitly ask for research questions, theoretical underpinnings and hypotheses, additional attention has been paid to this. Moreover, we investigated whether the outcomes in this study, especially the FES, are influenced by the quality of the studies. We did this by using the Fisher exact test to test the null hypothesis that there is no difference between the FES in the strong studies (n = 30) and the moderate studies (n = 30) (see Tables 2–7) (Freeman and Julious, 2007).
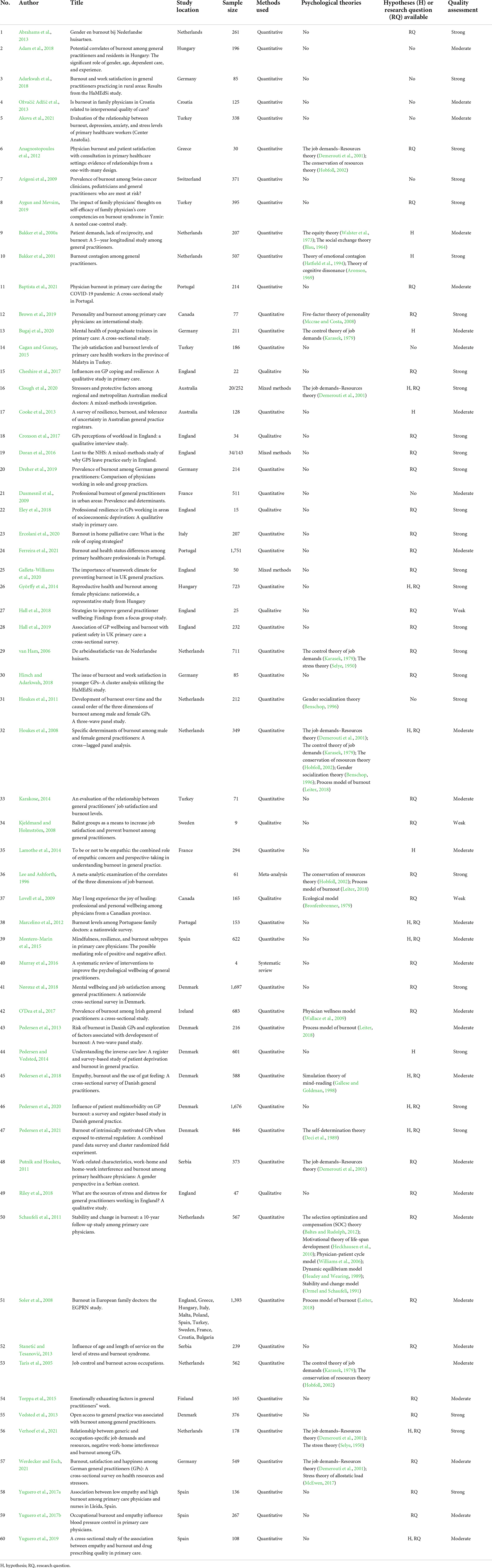
Table 1. Results of the systematic quantitative literature review (details of documents included in the data analysis).
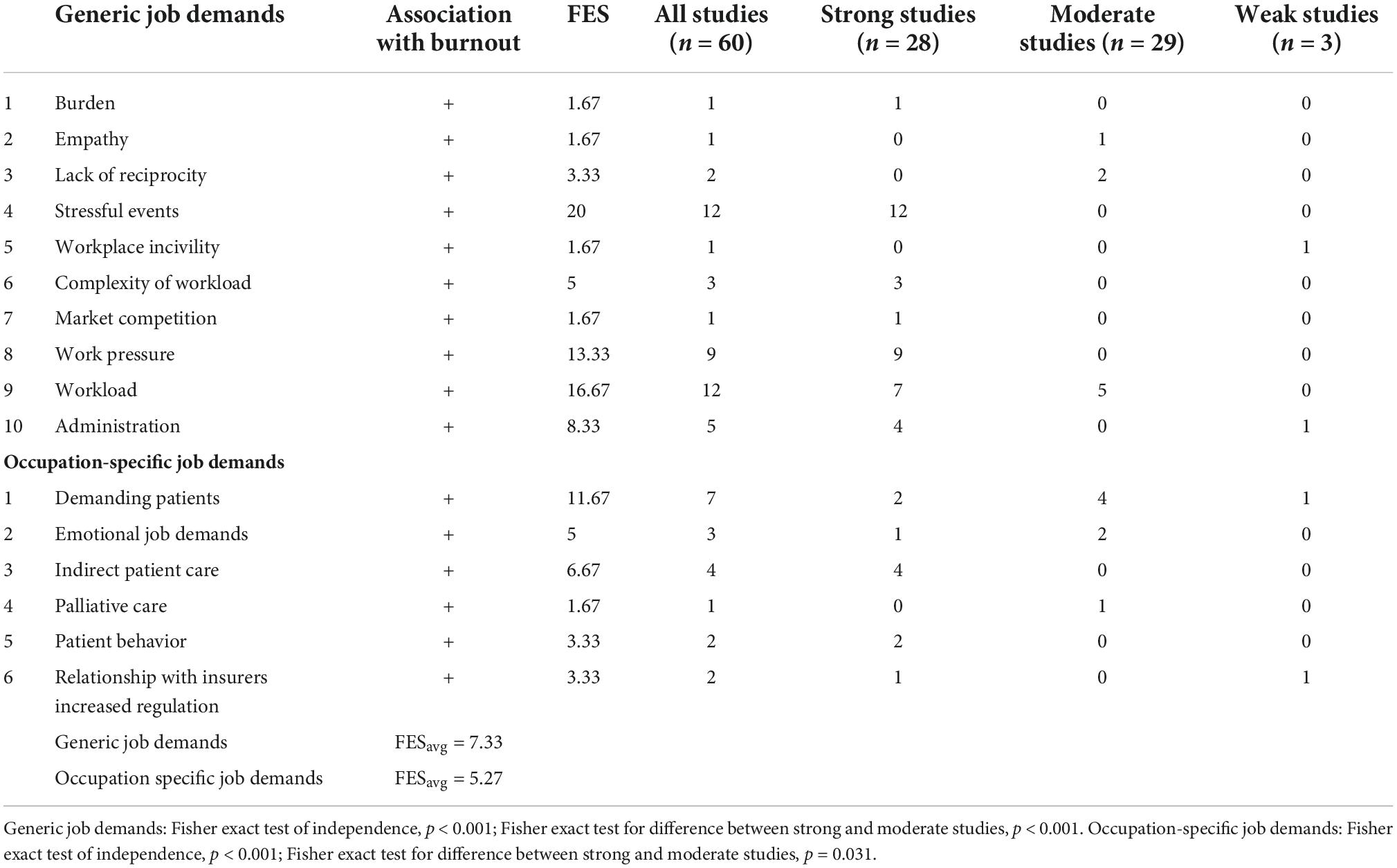
Table 2. Study outcomes job demands.
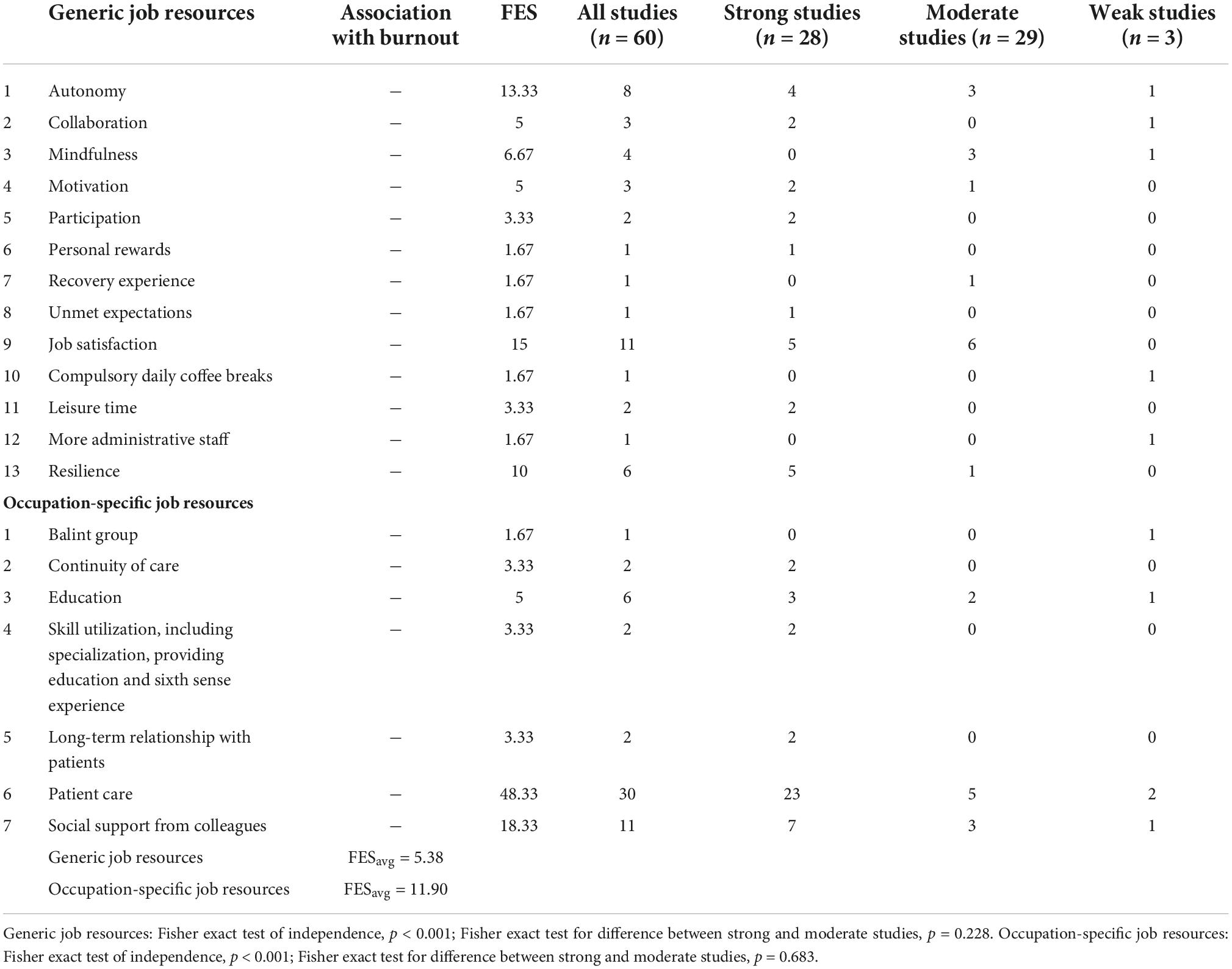
Table 3. Study outcomes job resources.
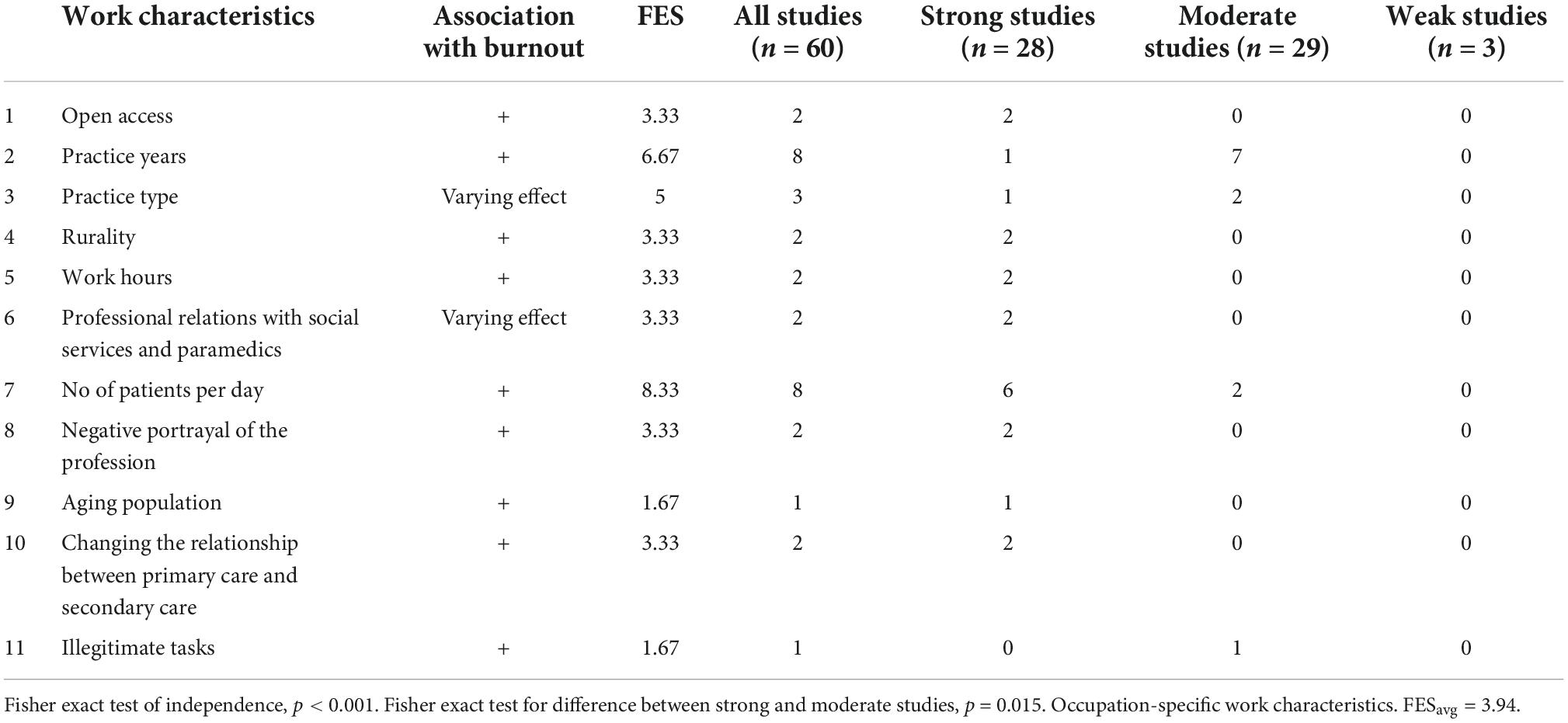
Table 4. Study outcomes work characteristics.
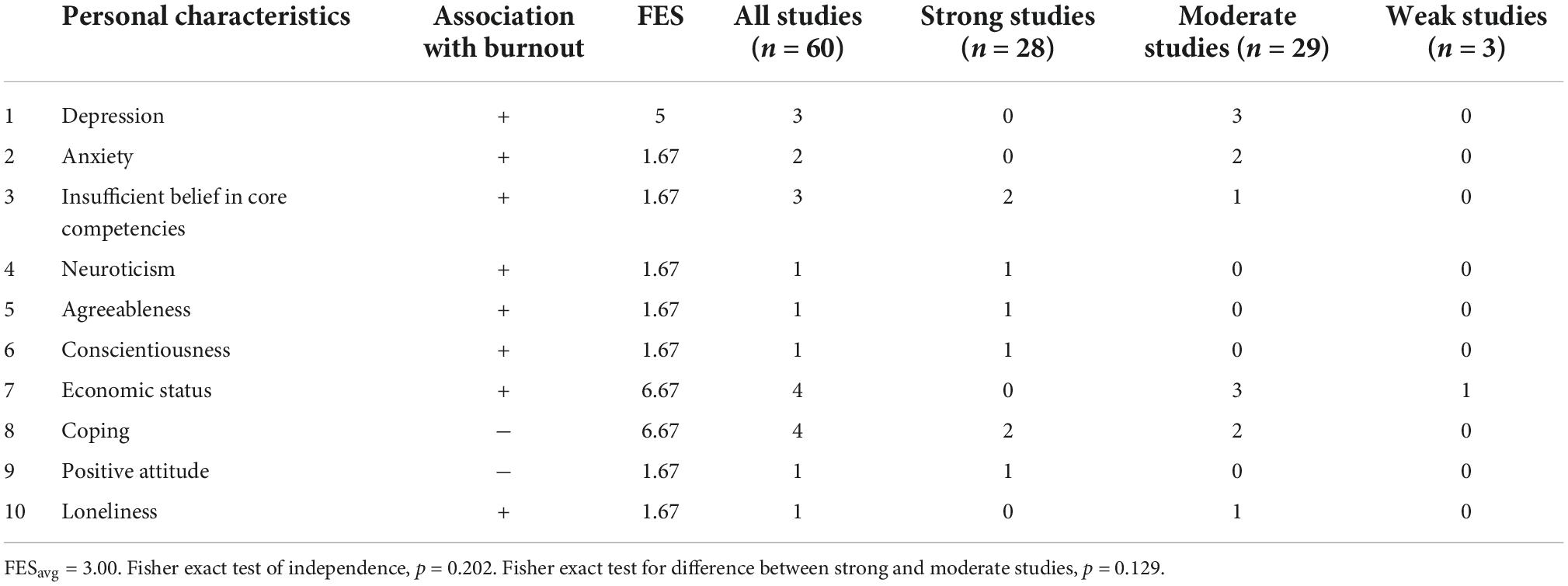
Table 5. Study outcomes personal characteristics [p-values are calculated according to Fisher exact (Freeman and Julious, 2007)].
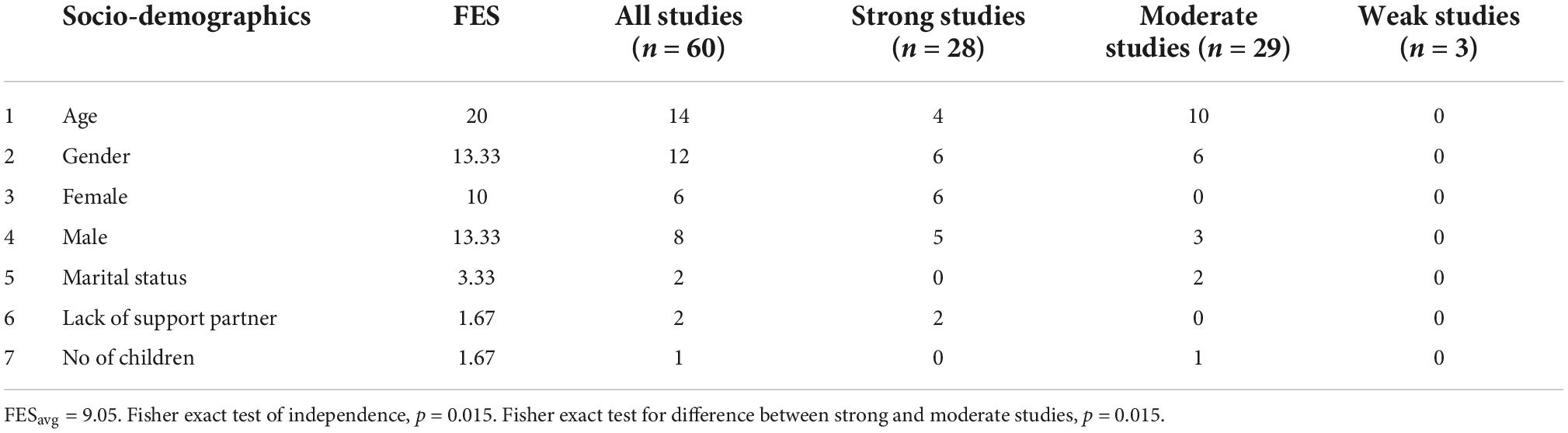
Table 6. Study outcomes socio-demographics [p-values are calculated according to Fisher exact (Freeman and Julious, 2007)].
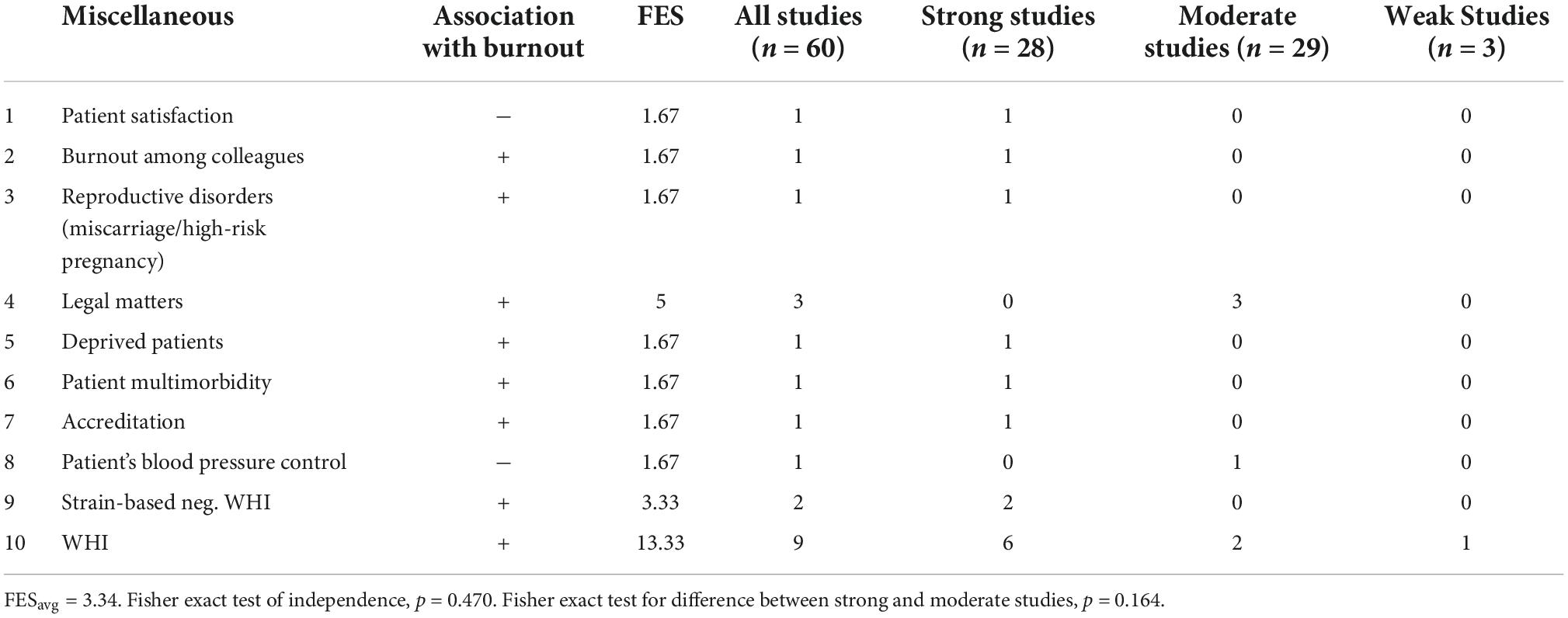
Table 7. Study outcomes miscellaneous category [p-values are calculated according to Fisher exact (Freeman and Julious, 2007)].
The outcomes of the four screening phases are indicated in the process diagram in Figure 1. The first rough search identified 9,508 studies, of which 60 studies ultimately remained for further analysis. The bibliographical details of these studies (authors and journals) are presented in Table 1. The methodological details of these studies are presented in Table 1. The outcomes of the quality assessments of all studies are presented in Table 1 and are denoted as strong, moderate or weak.
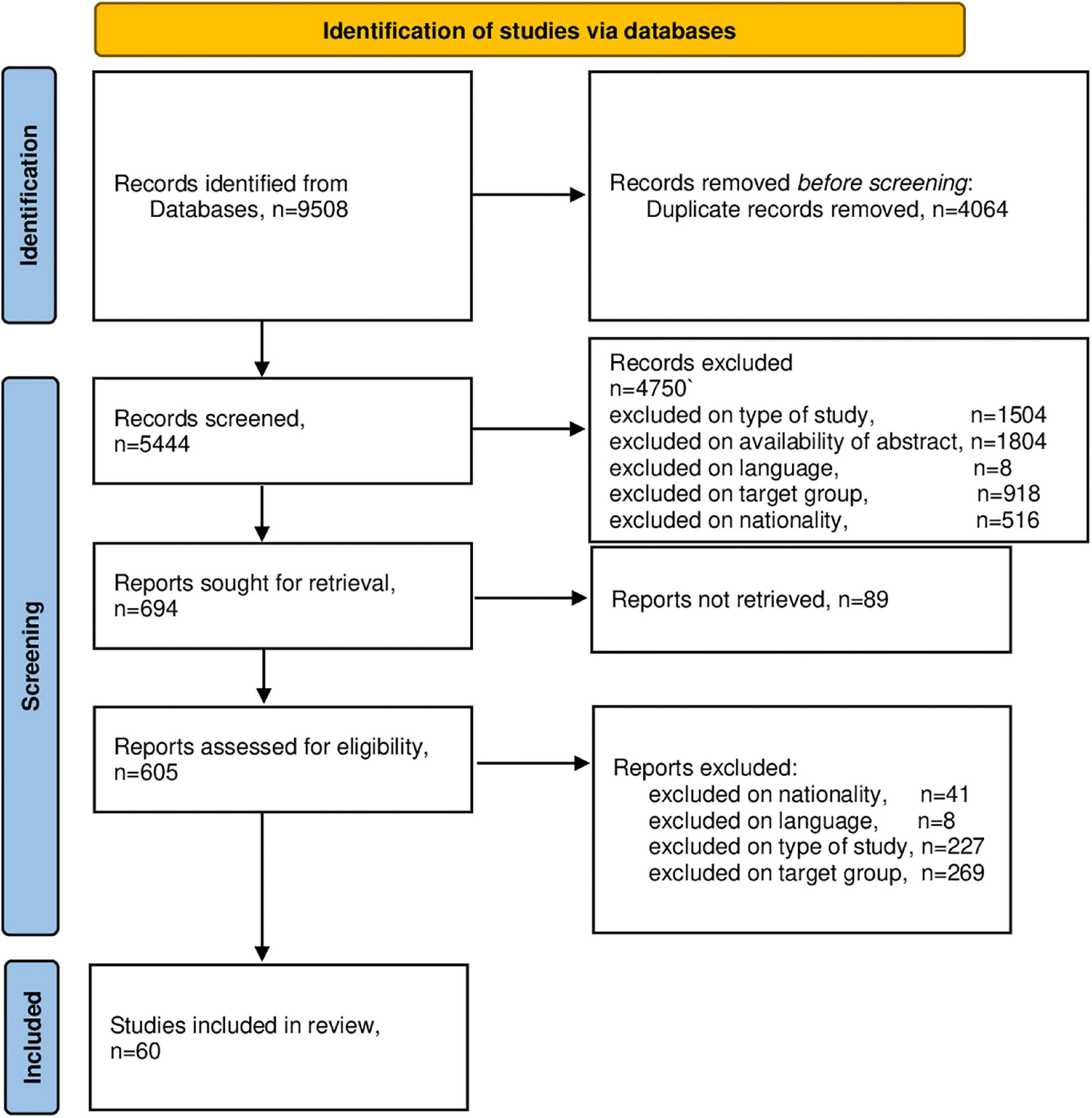
Figure 1. PRISMA 2020 flow diagram. From: Page et al. (2021).
The findings study is explained in detail, including the FES, in Tables 2–8. Table 1 lists the locations of the 60 studies reviewed. Of the 22 different nationalities, the Netherlands and England produced the highest number of studies, namely 9. The psychological theories used for the theoretical underpinning in the studies examined indicate a study’s solidity. Note, that the limited space in a journal can also cause the absence of a theory! Several methodological parameters have been identified and included in Table 1. Of the 24 distinct psychological theories, the COR theory (Hobfoll, 2002) and the JDR theory (Demerouti et al., 2001) have the highest frequencies with 7 (29.1%) and 6 (25%), respectively. Of the 60 studies examined, 65% do not appear to use a supporting psychological theory (see Table 1). Furthermore, of the 60 studies examined, only 10% appear to have formulated and tested a hypothesis and 55% a research question that guides the research.
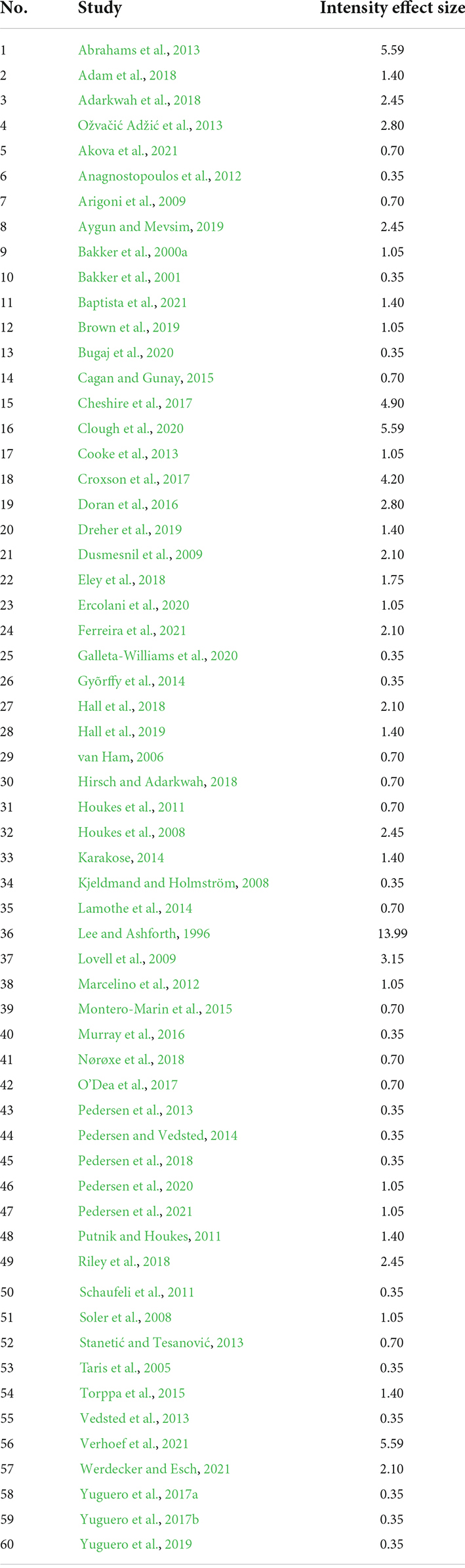
Table 8. Intensity effect size (IES) of all studies.
The results of an additional critical appraisal of the quality of the studies are presented as part of Table 1. The impact of a study is represented by its IES and is shown in Table 8 for all 60 studies examined. The mean IES = 1.99 (range 0.35–13.99). This parameter shows that the meta-analysis of Lee and Ashforth (1996) showed an IES = 13.99 and had thus the greatest impact on the current study. In addition, the qualitative study by Clough et al. (2020) (IES = 5.59) has a major impact on the results of the current study.
Finally, a Fisher exact test was conducted to test the null hypothesis that there is no difference between the FES in the strong studies (n = 30) and the moderate studies (n = 30) (see Tables 2–6) (Freeman and Julious, 2007). Tables 2–7 demonstrate that of the 75 items in total, only two had a significant p-value. Those items were Stressful events, Table 2, Job demands, had a p-value of 0.0001, and the other item was Patient care, Table 3, Job resources, had a p-value of 0.0007.
It is essential to gain a good understanding of the nature and strength of generic work requirements and resources. However, to increase ecological validity, it is also important to identify and further explore occupationally specific work demands and resources (Sundin et al., 2011; Brough and Biggs, 2015).
In the present study, we identified a substantial number of generic and some occupation-specific job requirements and resources for GPs (see Tables 2, 3). To better evaluate the results of a systematic review and the studies used for it, we used two effect measures. The FES of a finding, for example, a job requirement, is considered a measure of the strength of evidence for that finding (Sandelowski et al., 2007). The IES is regarded as a measure of the influence of the study in question on the final result of the ongoing study (see Table 8). For example, a study with an IES of 10 had much more influence on the final result of the ongoing study than a study with an IES of 2. In the current study, we selected 4 studies with relatively high IES, from Table 8, that is, Abrahams et al. (2013) (IES = 5.59), Clough et al. (2020) (IES = 5.59), Croxson et al. (2017) (IES = 4.90), and Cheshire et al. (2017) (IES = 4.90).
The quantitative study by Abrahams et al. (2013) aimed to investigate sex and gender differences in the prevalence and determinants of burnout among 349 Dutch GPs. The authors conclude that there is a relationship between gender and burnout that is mediated by work pressure, social support from the partner and a depressive response pattern. While these are highly recognizable work requirements and resources, they are all generic.
The mixed methods study by Clough et al. (2020) aimed to compare stressors leading to burnout and protective factors among 252 Australian GPs. The authors found 12 stressors (e.g., workload and time management) and nine protective factors (e.g., clinical interest). Except for this last resource, clinical interest, the other stressors and protective factors (resources) mentioned are generic.
The qualitative study by Croxson et al. (2017) aimed to investigate perceptions and attitudes toward workload among 34 UK GPs. The reasons cited for an increased workload are increased needs and expectations of patients, a changed relationship between primary and secondary healthcare and bureaucracy. It is primarily the workload balance within the practice that erodes the resource continuity of care. They, therefore, conclude that management of patient expectations and reduction of bureaucracy should be a high priority. It is the increased expectations of patients and the changed relationship between primary and secondary healthcare that can be regarded as occupation-specific work demands and continuity of care as a profession-specific resource.
Finally, the qualitative study by Cheshire et al. (2017) among 22 British GPs aimed to explore experiences with workplace challenges, stressors and coping. It was experienced as very stressful by the participants to feel bound by the moral implications of good doctors, resulting in anxiety, sleep disorders and stress. As individuals, they felt powerless to do anything about it. Various generic work requirements are mentioned (e.g., administration, workload, complexity of the work) as well as occupation-specific work requirements (e.g., demanding patients). Continuity of care is mentioned as an important occupational resource.
All in all, it is mainly generic work demands and resources that are mentioned in the results of the above four studies and relatively few profession-specific work demands and resources. Moreover, the generic job demands with an FESavg of 7.33 seem more important than the occupation-specific job demands with an FESavg of 5.27 (see Table 2). Further exploration of job-specific job demands and resources among GPs seems highly desirable. The situation is reversed for the resources, the generic resources with an FESavg = 5.38 seem much less important than the profession-specific resources with a much higher FESavg = 11.90 (see Table 3).
The fact that the share of England with nine studies and the Netherlands with nine studies have the largest share in the current study may mean that primary healthcare is changing in both countries.
Finally, Table 1, containing several methodological parameters, raises concerns about the methodological quality of studies. That only 35% of the studies use a supportive psychological theory is low. That only 10% of the studies generate a hypothesis is too low. That 55% of the studies use a directional research question seems average. However, to overcome this concern, we paid additional attention to the presence of the research question, supporting theory and hypotheses in the included studies and whether the quality assessments accounted for these items. Subsequently, we performed Fisher exact tests. From the results, we learned that only two out of 75 p-values were significant. We concluded that there was insufficient evidence to reject the null hypothesis. In other words, the quality of the studies did not affect the outcomes of the present study. We consider this finding a strength of this study.
GPs are independent healthcare professionals in small-scale working-groups outside the hospital. As a medical specialist, the GP has a broad medical knowledge of many diseases and disorders and is the first contact for people with various physical or mental complaints (Verstappen and Hobma, 2002). GPs are considered gatekeepers for hospital access (Van der Zee et al., 2004). The GP can also offer a solution if you have problems at home, school, or work. At least as necessary is GP care for the elderly in an aging society (Verlee et al., 2017; Grol et al., 2022). It is essential that a GP knows their patients and has time for a good conversation (van Ballegooijen et al., 2021). Fewer referrals to hospitals and less medication are also crucial for better health, to which the GP can make an excellent contribution (Gillam, 2022). During the current COVID-19 pandemic, the importance of good primary care has become apparent, as we can also learn from UK experiences (Mitchell et al., 2021). Some GPs vaccinate but also motivate people to get vaccinated. By taking over hospital care by the GP, patients can be discharged earlier and thus reduce the pressure on hospitals (Kloos, 2020; Cals et al., 2021).
If GPs are so important and valuable and have such a high risk of burnout (Bakker et al., 2000b; Soler et al., 2008), why is research into the causes and consequences of burnout among GPs so limited in size? The answer to this question, while partly obscure, is likely to be pluralistic. For example, recruitment problems for participants in research projects in primary healthcare have been reported (Bower et al., 2009; Graffy et al., 2009). But also, understaffed academic institutes for primary healthcare, with too few researchers, contribute to the limited literature (Campbell et al., 2015). Therefore, the urgent call in the current study to stimulate and initiate more research into burnout among GPs requires an ultimate effort that is worth it.
A significant limitation of the current study is that only one researcher conducted the study. Several researchers, at least two, preferably assess the many studies studied in a systematic review. Bias is a systematic error that leads to the acceptance of results and conclusions of a study that can be misleading. Selection bias in a systematic review can be reduced by conducting the study with multiple reviewers (Cooper et al., 2019).
Given the results of the present study, it is vital to conduct more qualitative studies to identify and further explore occupation-specific determinants of burnout among GPs. At the same time, this implies that the results of qualitative studies should be generalized by performing quantitative studies. However, given the recruitment constraints and understaffing of academic primary care research institutes, as discussed in the conclusion of the current study, more research will require an extra effort that is well worth it.
The original contributions presented in this study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
RB supervised this project. NV wrote the main body of the manuscript and carried out selection procedures. Both authors carried out extraction and synthesis procedures, read and approved the final manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
*Abrahams, H., Houkes, I., Winants, Y. H., Twellaar, M., and Verdonk, P. (2013). Gender en burnout bij Nederlandse huisartsen. Tijdschrift voor gezondheidswetenschappen 91, 225–233. doi: 10.1007/s12508-013-0079-3
*Adam, S., Mohos, A., Kalabay, L., and Torzsa, P. (2018). Potential correlates of burnout among general practitioners and residents in Hungary: The significant role of gender, age, dependant care and experience. BMC Fam. Prac. 19:193. doi: 10.1186/s12875-018-0886-3
*Adarkwah, C. C., Schwaffertz, A., Labenz, J., Becker, A., and Hirsch, O. (2018). Burnout and work satisfaction in general practitioners practicing in rural areas: Results from the HaMEdSi study. Psychol. Res. Behav. Manag. 11, 483–494. doi: 10.2147/PRBM.S179503
*Akova, I., Hasdemir, Ö, and Kiliç, E. (2021). Evaluation of the relationship between burnout, depression, anxiety, and stress levels of primary health-care workers (Center Anatolia). Alexandria J. Med. 57, 52–60. doi: 10.1080/20905068.2021.1874632
*Anagnostopoulos, F., Liolios, E., Persefonis, G., Slater, J., Kafetsios, K., and Niakas, D. (2012). Physician burnout and patient satisfaction with consultation in primary health care settings: Evidence of relationships from a one-with-many design. J. Clin. Psychol. Med. Sett. 19, 401–410. doi: 10.1007/s10880-011-9278-8
*Arigoni, F., Bovier, P., Mermillod, B., Waltz, P., and Sappino, A.-P. (2009). Prevalence of burnout among Swiss cancer clinicians, paediatricians and general practitioners: Who are most at risk? Support. Care Cancer 17, 75–81. doi: 10.1007/s00520-008-0465-6
Aronson, E. (1969). The theory of cognitive dissonance: A current perspective. Adv. Exp. Soc. Psychol. 4, 1–34.
*Aygun, O., and Mevsim, V. (2019). The impact of family physicians’ thoughts on self-efficacy of family physician’s core competencies on burnout syndrome in Ýzmir: A nested case–control study. Niger. J. Clin. Pract. 22:167.
Bakker, A. B., Hakanen, J. J., Demerouti, E., and Xanthopoulou, D. (2007). Job resources boost work engagement, particularly when job demands are high. J. Educ. Psychol. 99:274. doi: 10.1037/0022-0663.99.2.274
*Bakker, A. B., Schaufeli, W. B., Sixma, H. J., and Bosveld, W. (2001). Burnout contagion among general practitioners. J. Soc. Clin Psychol. 20, 82–98. doi: 10.1521/jscp.20.1.82.22251
Bakker, A., Schaufeli, W., and Van Dierendonck, D. (2000b). “Burnout: Prevalentie, risicogroepen en risicofactoren,” in Psychische vermoeidheid en werk, eds I. Houtman, W. Schaufeli, and T. Taris (Alphen a/d Rijn: Samsom), 65–82.
*Bakker, A., Schaufeli, W., Sixma, H., Bosveld, W., and Van Dierendonck, D. (2000a). Patient demands, lack of reciprocity, and burnout: A five-year longitudinal study among general practitioners. J. Organ. Behav. 21, 425–441. doi: 10.1002/(SICI)1099-1379(200006)21:4<425::AID-JOB21>3.0.CO;2-#
Baltes, B. B., and Rudolph, C. W. (2012). “The theory of selection, optimization, and compensation,” in The Oxford Handbook of Retirement, ed. M. Wang (New York, NY: Oxford University Press), 88–101.
*Baptista, S., Teixeira, A., Castro, L., Cunha, M., Serrão, C., Rodrigues, A., et al. (2021). Physician burnout in primary care during the COVID-19 pandemic: A cross-sectional study in portugal. J. Prim. Care Commun. Health 12, 1–9. doi: 10.1177/21501327211008437
Benschop, Y. (1996). Covered by equality: Gender in organizations. Nijmegen: Katholieke universiteit Nijmegen.
Bower, P., Wallace, P., Ward, E., Graffy, J., Miller, J., Delaney, B., et al. (2009). Improving recruitment to health research in primary care. Fam. Pract. 26, 391–397. doi: 10.1093/fampra/cmp037
Bronfenbrenner, U. (1979). The ecology of human development: Experiments by nature and design. Cambridge, MA: Harvard university press.
Brough, P., and Biggs, A. (2015). Job demands× job control interaction effects: Do occupation-specific job demands increase their occurrence? Stress Health 31, 138–149. doi: 10.1002/smi.2537
Brough, P., and Frame, R. (2004). Predicting police job satisfaction and turnover intentions: The role of social support and police organisational variables. N Z. J. Psychol. 33, 8–18.
Brough, P., O’Driscoll, M., Kalliath, T., Cooper, C. L., and Poelmans, S. A. (2009). Workplace psychological health: Current research and practice. Cheltenham: Edward Elgar Publishing. doi: 10.4337/9781781952672
*Brown, P. A., Slater, M., and Lofters, A. (2019). Personality and burnout among primary care physicians: An international study. Psychol. Res. Behav. Manag. 12, 169–177. doi: 10.2147/PRBM.S195633
Bryman, A. (2007). The research question in social research: What is its role? Int. J. Soc. Res. Methodol. 10, 5–20. doi: 10.1080/13645570600655282
*Bugaj, T. J., Krug, K., Rentschler, A., Nikendei, C., Szecsenyi, J., and Schwill, S. (2020). Mental health of postgraduate trainees in primary care: A cross-sectional study. BMC Fam. Pract. 21:123. doi: 10.1186/s12875-020-01199-6
Buunk, B., De Jonge, J., Ybema, J., and De Wolff, C. (1998). “Psychosocial aspects of occupational stress,” in Work Psychology, Handbook of Work and Organizational Psychology, 2nd Edn, eds P. J. D. Drenth, H. Thierry, and C. J. de Wolff (Hove: Psychology Press, Ltd).
*Cagan, O., and Gunay, O. (2015). The job satisfaction and burnout levels of primary care health workers in the province of Malatya in Turkey. Pak. J. Med. Sci. 31, 543–547. doi: 10.12669/pjms.313.6795
Cals, J., Derckx, R., and Blanker, M. (2021). Intensieve en palliatieve covid-19-zorg door huisarts: Landelijke registratie door Consortium Onderzoek Huisartsgeneeskunde (Intensive and palliative covid-19 care by GP: National registration by Consortium Research General Practice). Nederlands Tijdschrift voor Geneeskunde 164:D5616.
Campbell, J., Hobbs, F. R., Irish, B., Nicholson, S., Pringle, M., Reeve, J., et al. (2015). UK academic general practice and primary care. BMJ 351:h4164. doi: 10.1136/bmj.h4164
Cathebras, P., Begon, A., Laporte, S., Bois, C., and Truchot, D. (2004). Burn out among french general practitioners. Presse. Med. 33, 1569–1574. doi: 10.1016/S0755-4982(04)98994-4
*Cheshire, A., Ridge, D., Hughes, J., Peters, D., Panagioti, M., Simon, C., et al. (2017). Influences on GP coping and resilience: A qualitative study in primary care. Br. J. Gen. Pract. 67, e428–e436. doi: 10.3399/bjgp17X690893
*Clough, B. A., Ireland, M. J., Leane, S., and March, S. (2020). Stressors and protective factors among regional and metropolitan Australian medical doctors: A mixed methods investigation. J. Clin. Psychol. 76, 1362–1389. doi: 10.1002/jclp.22940
Collier, R. (2017). Physician burnout a major concern. CMAJ 189, E1236–E1237. doi: 10.1503/cmaj.1095496
*Cooke, P. E. G., Doust Jenny, A., and Steele Michael, C. (2013). A survey of resilience, burnout, and tolerance of uncertainty in Australian general practice registrars. BMC Med. Educ. 13:2. doi: 10.1186/1472-6920-13-2
Cooper, H., Hedges, L. V., and Valentine, J. C. (2019). The handbook of research synthesis and meta-analysis. New York, NY: Russell Sage Foundation. doi: 10.7758/9781610448864
*Croxson, C. H., Ashdown, H., and Hobbs, F. D. R. (2017). GPs’ perceptions of workload in England: A qualitative interview study. Br. J. Gen. Pract. 67, e138–e147. doi: 10.3399/bjgp17X688849
Deci, E. L., Connell, J. P., and Ryan, R. M. (1989). Self-determination in a work organization. J. Appl. Psychol. 74, 580–590. doi: 10.1037/0021-9010.74.4.580
Demerouti, E. (1999). Burnout: A consequence of specific working conditions among human service and production tasks. Frankfurt: Lang.
Demerouti, E., Bakker, A. B., Nachreiner, F., and Schaufeli, W. B. (2001). The job demands-resources model of burnout. J. Appl. Psychol. 86, 499–512. doi: 10.1037/0021-9010.86.3.499
Demerouti, E., Bakker, A. B., Vardakou, I., and Kantas, A. (2003). The convergent validity of two burnout instruments: A multitrait-multimethod analysis. Eur. J. Psychol. Assess. 19, 12–23. doi: 10.1027//1015-5759.19.1.12
*Doran, N., Fox, F., Rodham, K., Taylor, G., and Harris, M. (2016). Lost to the NHS: A mixed methods study of why GPS leave practice early in England. Br. J. Gen. Pract. 66, e128–e135. doi: 10.3399/bjgp16X683425
Downes, M. J., Brennan, M. L., Williams, H. C., and Dean, R. S. (2016). Development of a critical appraisal tool to assess the quality of cross-sectional studies (AXIS). BMJ Open 6:e011458. doi: 10.1136/bmjopen-2016-011458
*Dreher, A., Theune, M., Kersting, C., Geiser, F., and Weltermann, B. (2019). Prevalence of burnout among german general practitioners: Comparison of physicians working in solo and group practices. PLoS One 14:e0211223. doi: 10.1371/journal.pone.0211223
*Dusmesnil, H., Serre Bérengère, S., Régi Jean, C., Leopold, Y., and Verger, P. (2009). Professional burn-out of general practitioners in urban areas: Prevalence and determinants. Sante Publique 21, 355–364. doi: 10.3917/spub.094.0355
*Eley, E., Jackson, B., Burton, C., and Walton, E. (2018). Professional resilience in GPs working in areas of socioeconomic deprivation: A qualitative study in primary care. Br. J. Gen. Pract. 68, e819–e825. doi: 10.3399/bjgp18X699401
*Ercolani, G., Varani, S., Peghetti, B., Franchini, L., Malerba Maria, B., Messana, R., et al. (2020). Burnout in home palliative care: What is the role of coping strategies? J. Palliat. Care 35, 46–52. doi: 10.1177/0825859719827591
*Ferreira, P. L., Raposo, V., Tavares Aida, I., and Pinto, A. (2021). Burnout and health status differences among primary healthcare professionals in Portugal. BMC Fam. Pract. 22:81. doi: 10.1186/s12875-021-01425-9
Freudenberger, H. J. (1974). Staff burn-out. J. Soc. Issues 30, 159–165. doi: 10.1111/j.1540-4560.1974.tb00706.x
Freudenberger, H. J., and Richelson, G. (1980). Burnout: The high cost of high achievement. New York, NY: Bantam books.
Gallese, V., and Goldman, A. (1998). Mirror neurons and the simulation theory of mind-reading. Trends Cogn. Sci. 2, 493–501.
*Galleta-Williams, H., Esmail, A., Grigoroglou, C., Zghebi Salwa, S., Zhou Anli, Y., Hodkinson, A., et al. (2020). The importance of teamwork climate for preventing burnout in UK general practices. Eur. J. Public Health 30, iv36–iv38. doi: 10.1093/eurpub/ckaa128
Gillam, S. (2022). Quality improvement in primary care: The essential guide. Boca Raton, FL: CRC Press. doi: 10.1201/9780429084041
Graffy, J., Grant, J., Boase, S., Ward, E., Wallace, P., Miller, J., et al. (2009). UK research staff perspectives on improving recruitment and retention to primary care research; nominal group exercise. Fam. Pract. 26, 48–55. doi: 10.1093/fampra/cmn085
Grol, S., Molleman, G., van Heumen, N., van den Muijsenbergh, M., Haan, N. S. D., and Schers, H. (2022). Effecten van de hervorming van de ouderenzorg (Effects of Elder Care Reform). Huisarts Wet. 65, 13–17. doi: 10.1007/s12445-021-1369-7
*Gyõrffy, Z., Dweik, D., and Girasek, E. (2014). Reproductive health and burn-out among female physicians: Nationwide, representative study from Hungary. BMC Women’s Health 14:121. doi: 10.1186/1472-6874-14-121
Hakanen, J. J., Bakker, A. B. A., and Demerouti, E. E. E. (2005). How dentists cope with their job demands and stay engaged : The moderating role of job resources. Eur. J. Oral Sci. 113, 479–487. doi: 10.1111/j.1600-0722.2005.00250.x
Halbesleben, J. R. (2003). “Assessing the construct validity of alternative measures of burnout: Investigating the Oldenburg burnout inventory and the Utrecht engagement scale,” in Proceedings of the southern management association 2003 meeting, (Princeton, NJ: Citeseer), 661.
*Hall, L. H., Johnson, J., Heyhoe, J., Watt, I., Anderson, K., and O’Connor, D. B. (2018). Strategies to improve general practitioner well-being: Findings from a focus group study. Fam. Pract. 35, 511–516. doi: 10.1093/fampra/cmx130
*Hall, L. H., Johnson, J., Watt, I., and O’Connor, D. B. (2019). Association of GP wellbeing and burnout with patient safety in UK primary care: A cross-sectional survey. Br. J. Gen. Pract. 69, e507–e514. doi: 10.3399/bjgp19X702713
Hatfield, E., Cacioppo, J., and Rapson, R. (1994). Emotional contagion. Cambridge: Cambridge University Press.
Haynes, B. R. (2006). Forming research questions. J. Clin. Epidemiol. 59, 881–886. doi: 10.1016/j.jclinepi.2006.06.006
Headey, B., and Wearing, A. (1989). Personality, life events, and subjective well-being: Toward a dynamic equilibrium model. J. Pers. Soc. Psychol. 57:731.
Heckhausen, J., Wrosch, C., and Schulz, R. (2010). A motivational theory of life-span development. Psychol. Rev. 117, 32–60. doi: 10.1037/a0017668
*Hirsch, O., and Adarkwah, C. C. (2018). The issue of burnout and work satisfaction in younger GPs—A cluster analysis utilizing the HaMEdSi study. Int. J. Environ. Res. Public Health 15:2190. doi: 10.3390/ijerph15102190
Hobfoll, S. E. (2002). Social and psychological resources and adaptation. Rev. Gen. Psychol. 6, 307–324. doi: 10.1037/1089-2680.6.4.307
Hong, Q. N., Fàbregues, S., Bartlett, G., Boardman, F., Cargo, M., Dagenais, P., et al. (2018). The mixed methods appraisal tool (MMAT) version 2018 for information professionals and researchers. Educ. Inform. 34, 285–291. doi: 10.3233/EFI-180221
*Houkes, I., Winants, Y. H. W. M., and Twellaar, M. (2008). Specific determinants of burnout among male and female general practitioners. A cross-lagged panel analysis. J. Occup. Organ. Psychol. 81, 249–276. doi: 10.1348/096317907X218197
*Houkes, I., Winants, Y., Twellaar, M., and Verdonk, P. (2011). Development of burnout over time and the causal order of the three dimensions of burnout among male and female GPs. A three-wave panel study. BMC Public Health 11:240. doi: 10.1186/1471-2458-11-240
Hussain, N., Bookwala, A., Sancheti, P., and Bhandari, M. (2011). The 3-min appraisal of a meta-analysis. Indian J. Orthop. 45, 4–5. doi: 10.4103/0019-5413.73652
Juniper, B., White, N., and Bellamy, P. (2010). A new approach to evaluating the well-being of police. Occup. Med. 60, 560–565. doi: 10.1093/occmed/kqq130
*Karakose, T. (2014). An evaluation of the relationship between general practitioners’ job satisfaction and burnout levels. Stud. Ethno Med. 8, 239–244. doi: 10.1080/09735070.2014.11917639
Karasek, R. A. Jr. (1979). Job demands, job decision latitude, and mental strain: Implications for job redesign. Adm. Sci. Q. 24, 285–308.
*Kjeldmand, D., and Holmström, I. (2008). Balint groups as a means to increase job satisfaction and prevent burnout among general practitioners. Ann. Fam. Med. 6, 138–145. doi: 10.1370/afm.813
Kloos, P. (2020). COVID-19 in de huisartsenpraktijk(COVID-19 in general practice). Huisarts Wet. 63, 76–78. doi: 10.1007/s12445-020-0844-x
Kop, N., Euwema, M., and Schaufeli, W. (1999). Burnout, job stress and violent behaviour among dutch police officers. Work Stress 13, 326–340. doi: 10.1080/02678379950019789
Kringos, D. S., Boerma, W. G. W., Hutchinson, A., van der Zee, J., and Groenewegen, P. P. (2010). The breadth of primary care: A systematic literature review of its core dimensions. BMC Health Serv. Res. 10:65. doi: 10.1186/1472-6963-10-65
Kristensen, T. S., Borritz, M., Villadsen, E., and Christensen, K. B. (2005). The copenhagen burnout inventory: A new tool for the assessment of burnout. Work Stress 19, 192–207. doi: 10.1080/02678370500297720
*Lamothe, M., Boujut, E., Zenasni, F., and Sultan, S. (2014). To be or not to be empathic: The combined role of empathic concern and perspective taking in understanding burnout in general practice. BMC Fam. Pract. 15:15. doi: 10.1186/1471-2296-15-15
*Lee, R. T., and Ashforth, B. E. (1996). A meta-analytic examination of the correlates of the three dimensions of job burnout. J. Appl. Psychol. 81:123. doi: 10.1037/0021-9010.81.2.123
Leiter, M. P. (2018). “Burnout as a developmental process: Consideration of models,” in Professional burnout: Recent developments in theory and research, eds W. Schaufeli, C. Maslach, and T. Marek (Boca Raton, FL: CRC Press), 237–250. doi: 10.4324/9781315227979-18
Long, H. A., French, D. P., and Brooks, J. M. (2020). Optimising the value of the critical appraisal skills programme (CASP) tool for quality appraisal in qualitative evidence synthesis. Res. Methods Med. Health Sci. 1, 31–42. doi: 10.1177/2632084320947559
*Lovell, B. L., Lee, R. T., and Frank, E. (2009). May I long experience the joy of healing: Professional and personal wellbeing among physicians from a Canadian province. BMC Fam. Pract. 10:18. doi: 10.1186/1471-2296-10-18
*Marcelino, G., Cerveira, J. M., Carvalho, I., Costa, J. A., Lopes, M., Calado, N. E., et al. (2012). Burnout levels among portuguese family doctors: A nationwide survey. BMJ Open 2:e001050. doi: 10.1136/bmjopen-2012-001050
Maslach, C., and Jackson, S. E. (1981). The measurement of experienced burnout. J. Organ. Behav. 2, 99–113. doi: 10.1002/job.4030020205
Maslach, C., and Leiter, M. P. (1997). The truth about burnout how organizations cause personal stress and what to do about it. San Francisco, CA: Jossey-Bass.
Maslach, C., and Schaufeli, W. B. (1993). “Historical and conceptual development of burnout,” in Professional burnout: Recent developments in theory and research, eds W. B. Schaufeli, C. Maslach, and T. Marek (Milton Park: Taylor & Francis), 1–16. doi: 10.4324/9781315227979-1
Maslach, C., Jackson, S. E., and Leiter, M. P. (1996). Maslach burnout inventory manual. Mountain View, CA: CPP.
Maslach, C., Schaufeli, W. B., and Leiter, M. P. (2001). Job burnout. Annu. Rev. Psychol. 52, 397–422. doi: 10.1146/annurev.psych.52.1.397
Mccrae, R. R., and Costa, P. T. Jr. (2008). “The five-factor theory of personality,” in Handbook of personality: Theory and research, eds O. P. John, R. W. Robins, and L. A. Pervin (New York, NY: The Guilford Press), 159–181.
McEwen, B. S. (2017). Neurobiological and systemic effects of chronic stress. Chronic Stress 1:2470547017692328. doi: 10.1177/2470547017692328
Mitchell, S., Oliver, P., Gardiner, C., Chapman, H., Khan, D., Boyd, K., et al. (2021). Community end-of-life care during the COVID-19 pandemic: Findings of a UK primary care survey. BJGP Open 5, 1–14. doi: 10.3399/BJGPO.2021.0095
*Montero-Marin, J., Tops, M., Manzanera, R., Piva Demarzo, MM., Álvarez de Mon, M., and García-Campayo, J. (2015). Mindfulness, Resilience, and Burnout Subtypes in Primary Care Physicians: The Possible Mediating Role of Positive and Negative Affect. Front. Psychol. 6:1895. doi: 10.3389/fpsyg.2015.01895
*Murray, M., Murray, L., and Donnelly, M. (2016). Systematic review of interventions to improve the psychological well-being of general practitioners. BMC Fam. Pract. 17:36. doi: 10.1186/s12875-016-0431-1
Nadelson, S., and Nadelson, L. S. (2014). Evidence-based practice article reviews using CASP tools: A method for teaching EBP. Worldviews Evid. Based Nurs. 11, 344–346. doi: 10.1111/wvn.12059
*Nørøxe, K. B., Pedersen, A. F., Bro, F., and Vedsted, P. (2018). Mental well-being and job satisfaction among general practitioners: A nationwide cross-sectional survey in Denmark. BMC Fam. Pract. 19:130. doi: 10.1186/s12875-018-0809-3
*O’Dea, B., O’Connor, P., Lydon, S., and Murphy, A. W. (2017). Prevalence of burnout among Irish general practitioners: A cross-sectional study. Irish J. Med. Sci. 86, 447–453. doi: 10.1007/s11845-016-1407-9
O’Driscoll, M. P., Brough, P., and Kalliath, T. (2009). Stress and coping. Oxford: Oxford University Press. doi: 10.1093/oxfordhb/9780199211913.003.0011
Onwuegbuzie, A. J. (2003). Effect sizes in qualitative research: A prolegomenon. Qual. Quant. 37, 393–409. doi: 10.1023/A:1027379223537
Ormel, J., and Schaufeli, W. B. (1991). Stability and change in psychological distress and their relationship with self-esteem and locus of control: A dynamic equilibrium model. J. Pers. Soc. Psychol. 60:288.
*Ožvačić Adžić, Z., Katić, M., Kern, J., Soler, J., Cerovečki, V., and Polašek, O. (2013). Is burnout in family physicians in croatia related to interpersonal quality of care? Arch. Industr. Hygiene Toxicol. 64, 69–78. doi: 10.2478/10004-1254-64-2013-2307
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., et al. (2021). The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 372, n71. doi: 10.1136/bmj.n71
*Pedersen, A. F., and Vedsted, P. (2014). Understanding the inverse care law: A register and survey-based study of patient deprivation and burnout in general practice. Int. J. Equ. Health 13, 121–121. doi: 10.1186/s12939-014-0121-3
*Pedersen, A. F., Andersen, C. M., Olesen, F., and Vedsted, P. (2013). Risk of burnout in danish GPs and exploration of factors associated with development of burnout: A two-wave panel study. Int. J. Fam. Med. 2013, 603713. doi: 10.1155/2013/603713
*Pedersen, A. F., Ingeman Mads, L., and Vedsted, P. (2018). Empathy, burn-out and the use of gut feeling: A cross-sectional survey of Danish general practitioners. BMJ Open 8:e020007. doi: 10.1136/bmjopen-2017-020007
*Pedersen, A. F., Vedsted, P., and Nørøxe, K. B. (2020). Influence of patient multimorbidity on GP burnout: A survey and register-based study in Danish general practice. Br. J. Gen. Pract. 70, e95–e101. doi: 10.3399/bjgp20X707837
*Pedersen, L. B., Hvidt, E. A., Waldorff, F. B., and Andersen, M. K. (2021). Burnout of intrinsically motivated GPs when exposed to external regulation: A combined panel data survey and cluster randomized field experiment. Health Policy 125, 459–466. doi: 10.1016/j.healthpol.2021.01.004
Pickering, C., and Byrne, J. (2014). The benefits of publishing systematic quantitative literature reviews for PhD candidates and other early-career researchers. High. Educ. Res. Dev. 33, 534–548. doi: 10.1080/07294360.2013.841651
*Putnik, K., and Houkes, I. (2011). Work related characteristics, work-home and home-work interference and burnout among primary healthcare physicians: A gender perspective in a Serbian context. BMC Public Health 11:716. doi: 10.1186/1471-2458-11-716
*Riley, R., Spiers, J., Buszewicz, M., Taylor, A. K., Thornton, G., and Chew-Graham, C. A. (2018). What are the sources of stress and distress for general practitioners working in England? A qualitative study. BMJ Open 8, e017361. doi: 10.1136/bmjopen-2017-017361
Sandelowski, M., Barroso, J., and Voils Corrine, I. (2007). Using qualitative metasummary to synthesize qualitative and quantitative descriptive findings. Res. Nurs. Health 30, 99–111. doi: 10.1002/nur.20176
Schäfer, W. L., Boerma, W. G., Spreeuwenberg, P., Schellevis, F. G., and Groenewegen, P. P. (2016). Two decades of change in European general practice service profiles: Conditions associated with the developments in 28 countries between 1993 and 2012. Scandin. J. Prim. Health Care 34, 97–110. doi: 10.3109/02813432.2015.1132887
Schaufeli, W. B., and Leiter, M. P. (1996). The maslach burnout inventory-test manual. Palo Alto, CA: Consulting Psychologists Press.
Schaufeli, W. B., and Taris, T. W. (2005). The conceptualization and measurement of burnout: Common ground and worlds apart The views expressed inWork & StressCommentaries are those of the author(s), and do not necessarily represent those of any other person or organization, or of the journal. Work Stress 19, 256–262. doi: 10.1080/02678370500385913
Schaufeli, W. B., and Taris, T. W. (2014). “A critical review of the job demands-resources model: Implications for improving work and health,” in Bridging occupational, organizational and public health, eds G. F. Bauer and O. Hämmig (Berlin: Springer), 43–68. doi: 10.1007/978-94-007-5640-3_4
Schaufeli, W. B., Desart, S., and De Witte, H. (2020). Burnout assessment tool (BAT)—development, validity, and reliability. Int. J. Environ. Res. Public Health 17:9495. doi: 10.3390/ijerph17249495
*Schaufeli, W. B., Maassen, G. H., Bakker, A. B., and Sixma, H. J. (2011). Stability and change in burnout: A 10-year follow-up study among primary care physicians. J. Occup. Organ. Psychol. 84, 248–267. doi: 10.1111/j.2044-8325.2010.02013.x
Schaufeli, W., De Witte, H., and Desart, S. (2019). Handleiding burnout assessment tool (BAT). KU Leuven: Intern rapport.
Selye, H. (1950). Stress and the general adaptation syndrome. Br. Med. J. 1:1383. doi: 10.1136/bmj.1.4667.1383
*Soler, J. K., Yaman, H., Esteva, M., Dobbs, F., Asenova, R. S., and Katic, M. (2008). Burnout in European family doctors: The EGPRN study. Fam. Pract. 25, 245–265. doi: 10.1093/fampra/cmn038
*Stanetić, K., and Tesanović, G. (2013). Influence of age and length of service on the level of stress and burnout syndrome. Med. Pregl. 66, 153–162. doi: 10.2298/MPNS1304153S
Sundin, L., Hochwälder, J., and Lisspers, J. (2011). A longitudinal examination of generic and occupational specific job demands, and work-related social support associated with burnout among nurses in Sweden. Work 38, 389–400. doi: 10.3233/WOR-2011-1142
*Taris, T. W., Bakker Arnold, B., Schaufeli Wilmar, B., Stoffelsen, J., and Van Dierendonck, D. (2005). Job control and burnout across occupations. Psychol. Rep. 97, 955–961. doi: 10.2466/pr0.97.3.955-961
Tipa, R. O., Tudose, C., and Pucarea, V. L. (2019). Measuring burnout among psychiatric residents using the Oldenburg burnout inventory (OLBI) instrument. J. Med. Life 12:354. doi: 10.25122/jml-2019-0089
*Torppa, M. A., Kuikka, L., Nevalainen, M., and Pitkala, K. H. (2015). Emotionally exhausting factors in general practitioners’ work. Scand. J. Prim. Health Care 33, 178–183. doi: 10.3109/02813432.2015.1067514
Tuckey, M. R., and Hayward, R. (2011). Global and occupation-specific emotional resources as buffers against the emotional demands of fire-fighting. Appl. Psychol. 60, 1–23. doi: 10.1111/j.1464-0597.2010.00424.x
van Ballegooijen, J., van Wijngaarden-Timmermans, C., Jonker, K., and Rozenboom, I. (2021). Het belang van familierelaties (The importance of family relationships). Huisarts Wet. 64, 48–50. doi: 10.1007/s12445-021-1235-7
Van der Doef, M., and Maes, S. (2002). Teacher-specific quality of work versus general quality of work assessment: A comparison of their validity regarding burnout,(psycho) somatic well-being and job satisfaction. Anxiety Stress Coping 15, 327–344. doi: 10.1080/1061580021000056500
Van der Zee, J., Kroneman, M., and Boerma, W. (2004). De Nederlandse huisarts in Europees perspectief (The Dutch GP in a European perspective). Huisarts Wet. 47, 569–578. doi: 10.1007/BF03083894
*van Ham, I. (2006). De arbeidssatisfactie van de Nederlandse huisarts. Groningen: Proefschrift Rijksuniversiteit.
*Vedsted, P., Sokolowski, I., and Olesen, F. (2013). Open access to general practice was associated with burnout among general practitioners. Int. J. Fam. Med. 2013:383602. doi: 10.1155/2013/383602
*Verhoef, N. C., De Ruiter, M., Blomme, R. J., and Curfs, E. C. (2021). Relationship between generic and occupation-specific job demands and resources, negative work-home interference and burnout among GPs. J. Manag. Organ. 27, 1–29. doi: 10.1017/jmo.2021.16
Verlee, E., Van der Sande, R., Abel, R., Brandon, S., De Groot, J., Quist-Anholts, G., et al. (2017). Landelijke eerstelijns samenwerkings afspraak zorg voor kwetsbare ouderen (National First-line Collaborative Agreement Care for frail elderly). Huisarts Wet. 60, 1–12. doi: 10.1007/s12445-017-0171-z
Verstappen, W., and Hobma, S. (2002). De nederlandse huisartsen: Een kennisintensieve organisatie? (The Dutch GPs: A knowledge-intensive organization?). Huisarts Wet. Nederlands 45, 614–615. doi: 10.1007/BF03082827
Wallace, J. E., Lemaire, J. B., and Ghali, W. A. (2009). Physician wellness: A missing quality indicator. Lancet 374, 1714–1721.
Walster, E., Berscheid, E., and Walster, G. W. (1973). New directions in equity research. J. Pers. Soc. Psychol. 25:151.
*Werdecker, L., and Esch, T. (2021). Burnout, satisfaction and happiness among German general practitioners (GPs): A cross-sectional survey on health resources and stressors. PLoS One 16:e0253447. doi: 10.1371/journal.pone.0253447
Whiting, P., Wolff, R., Mallett, S., Simera, I., and Savović, J. (2017). A proposed framework for developing quality assessment tools. Syst. Rev. 6:204. doi: 10.1186/s13643-017-0604-6
Williams, E. S., Savage, G. T., and Linzer, M. (2006). A proposed physician-patient cycle model. Stress and Health 22, 131–137.
*Yuguero, O., Marsal, J. R., Esq.uerda, M., and Soler-González, J. (2017b). Occupational burnout and empathy influence blood pressure control in primary care physicians. BMC Fam. Pract. 18:63. doi: 10.1186/s12875-017-0634-0
*Yuguero, O., Marsal, J. R., Esquerda, M., Galvan, L., and Soler-González, J. (2019). Cross-sectional study of the association between empathy and burnout and drug prescribing quality in primary care. Prim. Health Care Res. Dev. 20:e145. doi: 10.1017/S1463423619000793
*Yuguero, O., Marsal, J., Esquerda, M., Vivanco, L., and Soler-González, J. (2017a). Association between low empathy and high burnout among primary care physicians and nurses in Lleida, Spain. Eur. J. Gen. Pract. 23, 4–10. doi: 10.1080/13814788.2016.1233173
*indicates references which are included in the review.
Keywords: general practitioners, systematic quantitative literature review, occupation-specific determinants, generic determinants, ecological validity
Citation: Verhoef NC and Blomme RJ (2022) Burnout among general practitioners, a systematic quantitative review of the literature on determinants of burnout and their ecological value. Front. Psychol. 13:1064889. doi: 10.3389/fpsyg.2022.1064889
Received: 08 October 2022; Accepted: 23 November 2022;
Published: 15 December 2022.
Edited by:
Pedro Mota Veiga, University of Beira Interior, PortugalReviewed by:
Elsa Vitale, Bari Local Health Authority, ItalyCopyright © 2022 Verhoef and Blomme. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nicolaas Cornelis Verhoef, bmljby5waG9lbml4QHBsYW5ldC5ubA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.