 Danni Chi
Danni Chi Xiangju Du
Xiangju Du Hong Ma
Hong Ma Yuanyuan Zhang
Yuanyuan Zhang- Department of Psychosomatic Medicine, Ningbo Kangning Hospital, Ningbo, China
Introduction: The Young Positive Schema Questionnaire (YPSQ) examines early adaptive or positive schemas as a counterpart to early maladaptive ones. This study investigated the validity and reliability of the Chinese version of the YPSQ (CYPSQ).
Methods: A convenient community sample of 634 individuals, most of whom were college students, were recruited through a mobile survey. R Careless was used to screen for careless responses. A final sample of 336 was obtained. Confirmatory factor analyses (CFA) of the CYPSQ were conducted using SPSS AMOS 25. Other statistical analyses were conducted using SPSS 25.
Results: An 11-factor CYPSQ was identified with an acceptable factor structure (χ2/df = 2.13, SRMR = 0.04, RMSEA = 0.06, GFI = 0.80, TLI = 0.90, and CFI = 0.91). Convergent and discriminant validity were confirmed in most aspects. Concurrent validity was evident with resilience, life satisfaction, depression, and anxiety. Internal reliability was satisfied as the Cronbach’s alphas of the 11 factors of the CYPSQ ranged between 0.70 and 0.88.
Conclusion: The findings supported the reliability and validity of the CYPSQ in Mainland China.
Introduction
Schema therapy is an integrative method that combines attachment theories and cognitive behavior therapy. It was proposed and developed by Young et al. (2003). A negative or early maladaptive schema (EMS) or negative schema refers to a broad and pervasive pattern of cognitions, memories, emotions, and physical sensations vis-à-vis oneself and one’s relationships with others, which is dysfunctional to a significant degree (Young et al., 2003). Negative schemas are the outcomes of unmet core emotional needs in childhood and/or adolescence (i.e., acceptance, autonomy, reasonable limits, realistic expectations, and connection) and are elaborated upon throughout one’s lifetime (Young et al., 2003). Empirical studies have found that negative schemas are the transdiagnostic mechanisms of personality and affective disorders (Wang et al., 2010; Bamelis et al., 2014; Peeters et al., 2021). However, individuals with maladaptive schemas in some areas can also have adaptive or positive schemas in other areas.
Traditional clinical psychology is criticized as overly focused on the psychopathology of mental issues, and increasing interest has been invested in positive clinical psychology in recent decades (Seligman et al., 2006; Wood and Tarrier, 2010; Rashid, 2015). Positive or early adaptive schemas are expected when a person’s core emotional needs are sufficiently met, which are counterparts of negative schemas (Lockwood and Perris, 2012). Like EMS, positive schemas comprise cognitions, memories, bodily sensations, and neurobiological reactions of individuals with both themselves, and others but are positive and functional (Lockwood and Perris, 2012). Positive schemas explained extra variance in psychopathological outcomes, life satisfaction, resilience, and self-efficacy after controlling for EMSs (Louis et al., 2018; Paetsch et al., 2020). They are unique constructs with the potential to improve one’s wellbeing and mental health. Therefore, it is important to evaluate positive schemas in clinical and general populations.
The Young Positive Schema Questionnaire (YPSQ, Louis et al., 2018) was developed within the schema therapy framework to assess 14 positive schemas in adults. As the concept and measurement of positive schemas were proposed a few years ago (Lockwood and Perris, 2012; Louis et al., 2018), the validity and reliability of the YPSQ are yet to be verified in Mainland China. Thus, the present study investigated the psychometric properties of the Chinese version of YPSQ (CYPSQ) in Mainland China.
Materials and methods
Research design
This study used a cross-sectional design to evaluate the validity and reliability of CYPSQ. The original 56-item CYPSQ included 14 factors (Figure 1), according to Louis et al. (2018). In this study, the minimum desired sample size was 300 as it satisfied a ratio of five samples per item and was suggested as good for factor analysis (Comrey and Lee, 1992).
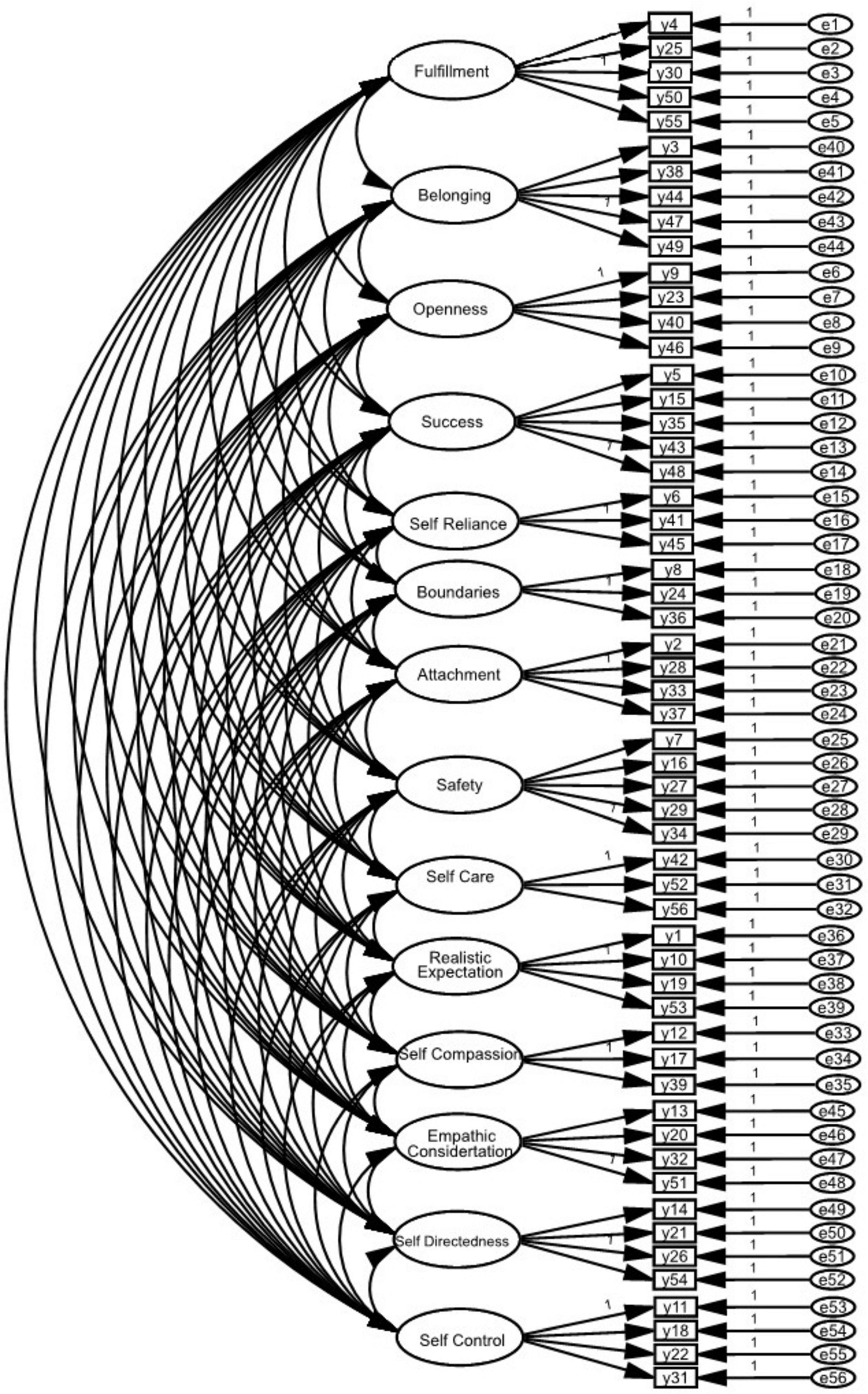
Figure 1. Factor construct of the 14-factor Young Positive Schema Questionnaire (YPSQ) (Louis et al., 2018).
Permission to use and adjust the CYPSQ was obtained from the original author (Louis et al., 2018), who offered both English and Chinese versions of the YPSQ. A group of researchers, including a psychologist with a Ph.D in psychology in an English-speaking country and two psychiatrists with advanced levels of English proficiency, evaluated the appropriateness of CYPSQ. Minor adjustments were made to ensure that the scale was understandable in Mainland China. The original author was informed of the changes. After that, 10 nurses went through the CYPSQ and reported that there was no confusion.
Ethical considerations
This study was completely anonymous and voluntary and was approved by the Institutional Ethics Committee of Ningbo Kangning Hospital (NBKNYY-2021-LC-50). Written consent was obtained from participants in accordance with the ethical standards of national laws. The study was conducted in accordance with the Declaration of Helsinki (Bošnjak, 2001; Tyebkhan, 2003; World Medical Association, 2013) and the Standards of Ethics in Sport and Exercise Science Research (Harriss et al., 2019).
Participants
Recruitment took place from 16 February to 19 April, 2022. Recruitment information was delivered through an online survey platform that was accessed through a mobile phone. Snowball sampling was applied in recruiting the community participants. The inclusion criteria were: aged between 18 and 75 years, fluent in Chinese, and capable of understanding and answering the survey. The convenience sample comprised 634 individuals, most of whom were college students. After evaluating eligibility and screening the data for careless responses and outliers, a final sample of 336 individuals was obtained for the validity and reliability tests, which is adequate for a confirmatory factor analysis (CFA).
Instruments
Demographics
Participants were asked to provide information on their age, gender, and educational background.
Young Positive Schema Questionnaire
The Young Positive Schema Questionnaire (YPSQ) is a self-report inventory comprising 14 factors and 56 items (Louis et al., 2018). Participants were asked to rate the degree to which the statements applied to them over the preceding month. Each item is rated on a 6-point Likert-type scale, ranging from 1 (completely untrue of me) to 6 (describes me perfectly). Higher scores indicate more positive schemas. The Cronbach’s α of each factor in the 14-factor original and 10-factor German YPSQ were above 0.70 (Louis et al., 2018; Paetsch et al., 2020). This was also the case in the 11-factor CYPSQ as seen in this study. The Cronbach’s α of the overall score of the 11-factor CYPSQ was 0.98 in this study.
Life satisfaction scale
The life satisfaction subscale from the Comprehensive Inventory of Thriving (CIT; Su et al., 2014) was used to measure life satisfaction over the preceding month. The original CIT was valid and reliable (Duan et al., 2020), and subscales could be used selectively (Su et al., 2014). This self-report life satisfaction subscale comprises three items, each of which is rated on a 5-point Likert-type scale, ranging from 1 (strongly disagree) to 5 (strongly agree). Higher scores indicate greater life satisfaction. The Cronbach’s α was 0.88 in this study.
Resilience scale
The Chinese version of the 10-item Connor–Davidson Resilience Scale (CD-RISK-10; Connor and Davidson, 2003) was used to measure the resilience level of participants over the preceding month. The CD-RISK-10 is a 5-point Likert-type scale, ranging from 0 (not true at all) to 4 (true nearly all the time). Higher scores indicate greater resilience. The CD-RISK-10 is a self-report scale and has been used among Chinese college students and shown good validity and reliability (Yu and Zhang, 2007; Cheng et al., 2020). The Cronbach’s α was 0.93 in this study.
Anxiety scale
The 7-item Generalized Anxiety Disorder (GAD-7; Spitzer et al., 2006) scale was used to examine the anxiety level of participants in this study. Participants were asked to rate their degree of anxiety over the preceding month. Each item is rated on a 4-point Likert-type scale, ranging from 0 (not at all) to 3 (nearly every day). Higher scores indicate higher levels of anxiety. The GAD-7 has good validity and reliability for screening anxiety in clinical practice and research. The Cronbach’s α of the GAD-7 was 0.92 in this study.
Depression scale
The 9-item Patient Health Questionnaire (PHQ-9; Kroenke et al., 2001) is a 9-item self-administered questionnaire and was used to measure depressive mood. Participants were asked to rate the degree of their depression over the preceding month. Each item was rated on a 4-point Likert-type scale, ranging from 0 (not at all) to 3 (nearly every day). Higher scores indicate higher levels of depression. The Cronbach’s α of the PHQ-9 was 0.91 in this study.
Statistical analyses
The web-based recruitment method usually results in a relatively higher number of careless responses (Johnson, 2005). Several strategies were adopted to screen the outliers and careless responses as suggested (Johnson, 2005; Yentes and Wilhelm, 2018). Careless R package was used to test the maximum longstring and the Mahalanobis D outlier indices with a default significant level of p < 0.01 (Yentes and Wilhelm, 2018). There is no golden standard for the cut-off number of longstring index or response time. Some studies recommend a maximum of 14 longstrings (Costa and McCrae, 2008) and no less than 2 s per English item as appropriate (Huang et al., 2012), but there are no relevant references for Chinese scales. In this study, similar criteria were applied. Cases were removed if any of the following were present: longstrings larger than 16, mean response time for each item less than 2 s, flagged Mahalanobis D, and absolute Z scores larger than 3.29 of the 56-item YPSQ.
The demographics were analyzed using descriptive statistics. The scale scores were computed as the means of items. T-tests were used to examine the mean differences in the YPSQ based on gender. The missing completely at random test suggested that the missing values were completely at random (chi-square = 3,435.01, p = 1.00) and missing values were excluded using pairwise deletion. Bivariate correlations were examined with Pearson correlation. The significance level of this study was set at p < 0.05. The CFA was examined using SPSS AMOS 25. Goodness-of-fit indices (GFIs) used in this study included the standardized root-mean residual (SRMR), the root-mean square error of approximation (RMSEA), the GFI, the Comparative Fit Index (CFI), and the Tucker–Lewis Index (TLI). The RMSEA, CFI, and TLI were calculated with the original 336 data set. The GFI and SRMR were calculated with the imputed data sets, as the AMOS 25 did not provide GFI and SRMR in data sets with missing data. The GFI and SRMR in these imputed data sets were the same. Recommended indices, such as χ2/df between 2 and 3, SRMR ≤ 0.08, RMSEA ≤ 0.08, GFI ≥ 0.90, CFI ≥ 0.90, and TLI ≥ 0.90, were used (Hu and Bentler, 1999). Convergent validity was confirmed by examining the standardized factor loadings, construct or composite reliability, and average variance extracted (AVE) value. Composite reliability and AVE values greater than 0.70 and 0.50, respectively, were considered valid (Fornell and Larcker, 1981; Hair et al., 2014). Discriminant validity was verified using the correlation coefficients between factors and the root square of the AVE value of each factor, and concurrent validity was examined using Pearson’s correlation between the CYPSQ factors and measures of resilience, life satisfaction, depression, and anxiety. Reliability was confirmed using the criterion of Cronbach’s α > 0.70 (Nunnally and Bernstein, 1994).
Results
This study examined the construct and concurrent validity, and internal reliability of CYPSQ in a Chinese community sample.
Demographics
Table 1 presents the demographics of the participants. The mean age of the participants was 27.11 years (SD = 11.75), as the sample was mainly from a college community. Most participants (91.0%) received college-level education or above and were female (n = 247, 73.5%).
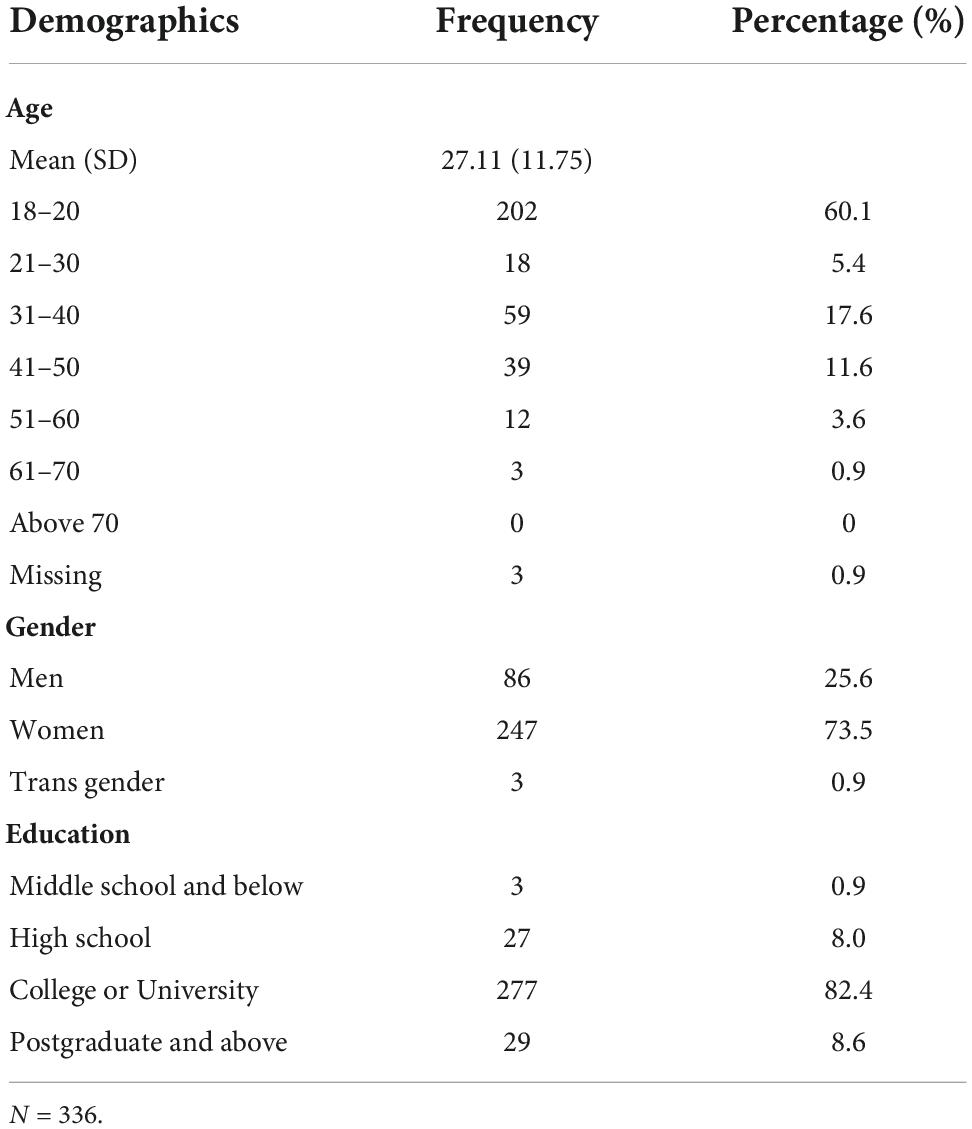
Table 1. Demographics of participants.
In the present study, women reported lower levels of success (t = 2.60, p = 0.01), competence (t = 3.10, p < 0.01), safety (t = 2.94, p < 0.01), self-compassion (t = 2.41, p = 0.02), and self-control (t = 2.95, p < 0.01) than men, and no significant differences between genders were found for other factors (Table 2). Age was positively correlated with all the 11 CYPSQ factors (Table 3).
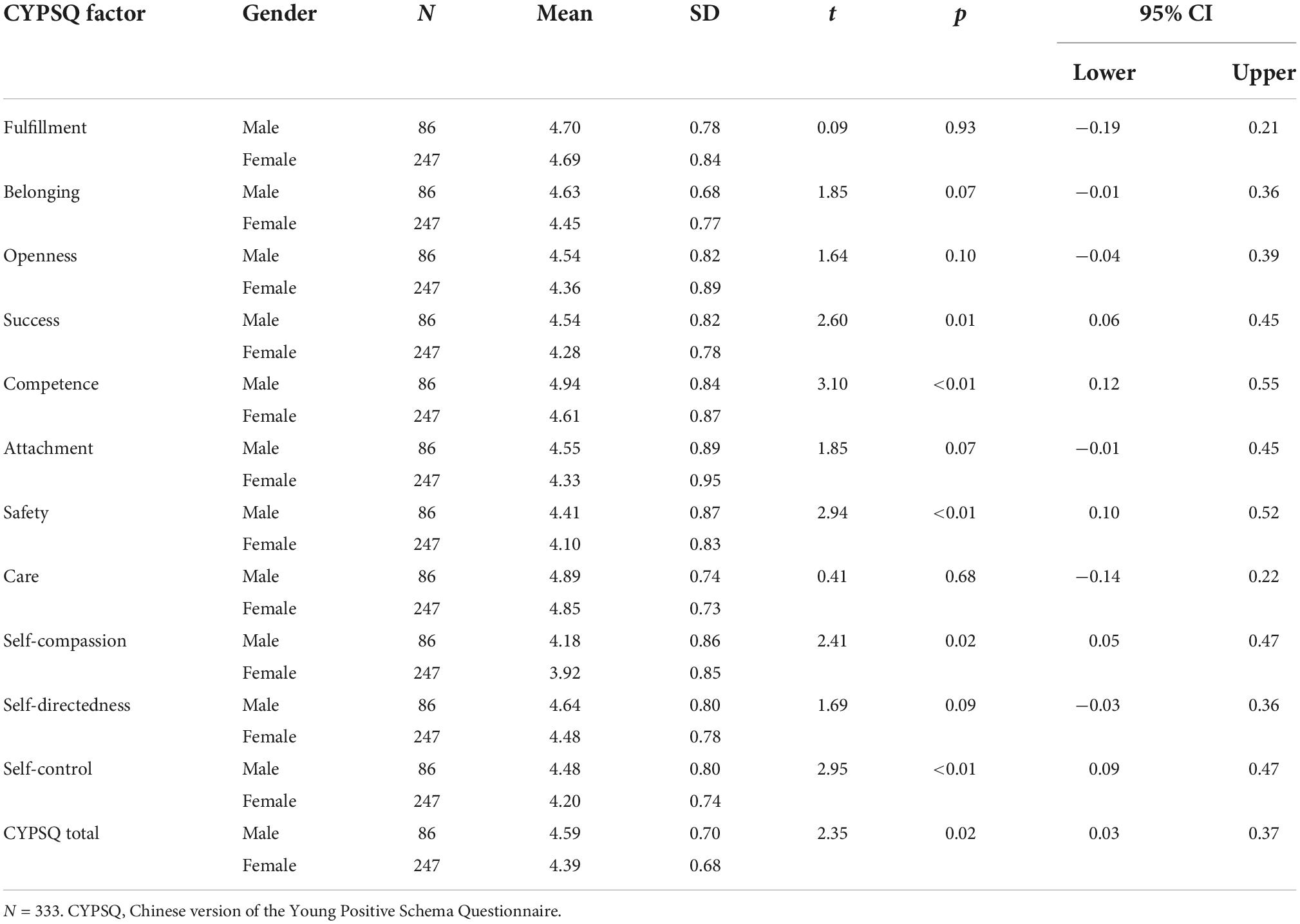
Table 2. Gender differences on the 11-factor Chinese version of the Young Positive Schema Questionnaire (CYPSQ).
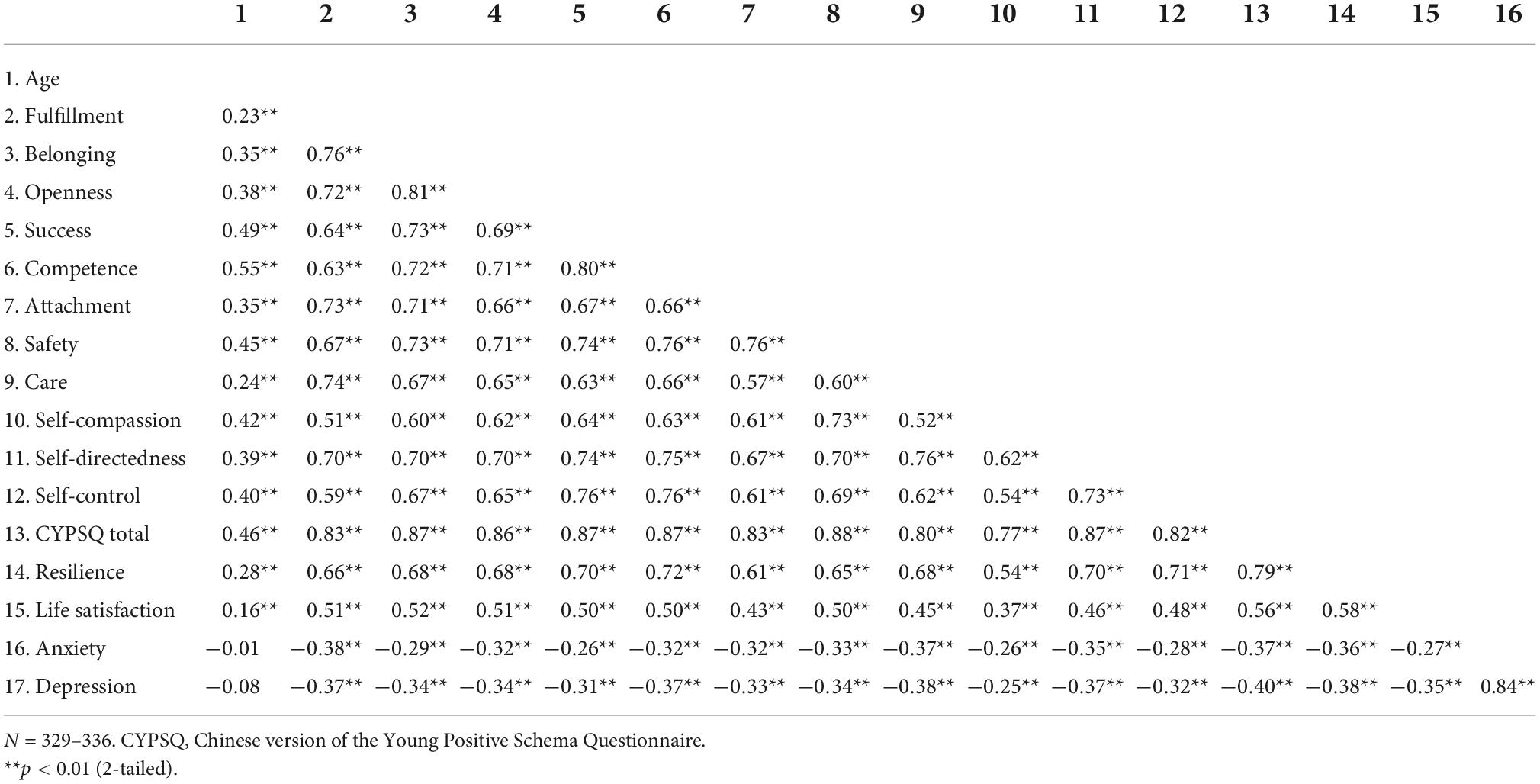
Table 3. Concurrent validity of the 11-factor Chinese version of the Young Positive Schema Questionnaire (CYPSQ).
Construct validity
Assessing the fit of the model
The Kaiser–Meyer–Olkin measure of sampling adequacy was 0.97, and Bartlett’s test for sphericity was significant (chi-square = 13,502.89, p < 0.001), indicating appropriateness for factor analysis. The construct validities of the 14- and 1-factor CYPSQ were examined using CFA.
The fit indices of the 14-factor CYPSQ were χ2/df = 2.20, SRMR = 0.05, RMSEA = 0.06, GFI = 0.74, CFI = 0.87, and TLI = 0.86. Modifications were made to improve the construct. First, items with factor loadings lower than 0.60 (Items 4, 36, 2, 1, 19, 13, and 32) were removed. Then, the CFA was run again, the factor of realistic expectation (Items 10 and 53) was highly correlated with the factors of emotional fulfillment, self-care, and self-direction (correlation coefficient: 1.03, 1.05, and 1.06, respectively), and was thus removed. According to theories and data, self-reliance and boundaries (each factor with only two items and highly correlated with a correlation coefficient of 0.92) were combined and renamed as self-reliance and boundaries. The CFA was re-run and the factor of empathic consideration was combined with self-care (r = 0.95) and renamed as care. Items 8 and 42 were removed owing to covariance with many other items according to modification indices. Item 25 was removed owing to loadings lower than 0.6 (0.59). Finally, an 11-factor model with 44 items was obtained (Table 2). The fit indices were χ2/df = 2.13, SRMR = 0.04, RMSEA = 0.06, GFI = 0.80, TLI = 0.90, and CFI = 0.91, which were acceptable (Hu and Bentler, 1999).
The fit indices of the 1-factor CYPSQ with all 56 items were χ2/df = 2.81, SRMR = 0.05, RMSEA = 0.07, GFI = 0.64, CFI = 0.79, and TLI = 0.78. To improve the construct of the 1-factor CYPSQ, 11 items with factor loadings lower than 0.60 (Items 4, 36, 2, 1, 19, 12, 17, 13, 20, 22, and 32) were removed. The fit indices of this 1-factor construct with 45 items were χ2/df = 3.05, SRMR = 0.05, RMSEA = 0.08, GFI = 0.68, CFI = 0.82, and TLI = 0.81, which were less acceptable than the 11-factor construct (Hu and Bentler, 1999).
Convergent validity
Table 4 summarizes the convergent validity indices. Standardized factor loadings ranged from 0.61 to 0.87. AVE values ranged from 0.48 to 0.65, and most of them were above 0.50, which were considered adequate (Fornell and Larcker, 1981). Composite reliability values ranged from 0.73 to 0.90, which were all above the criterion of 0.70.
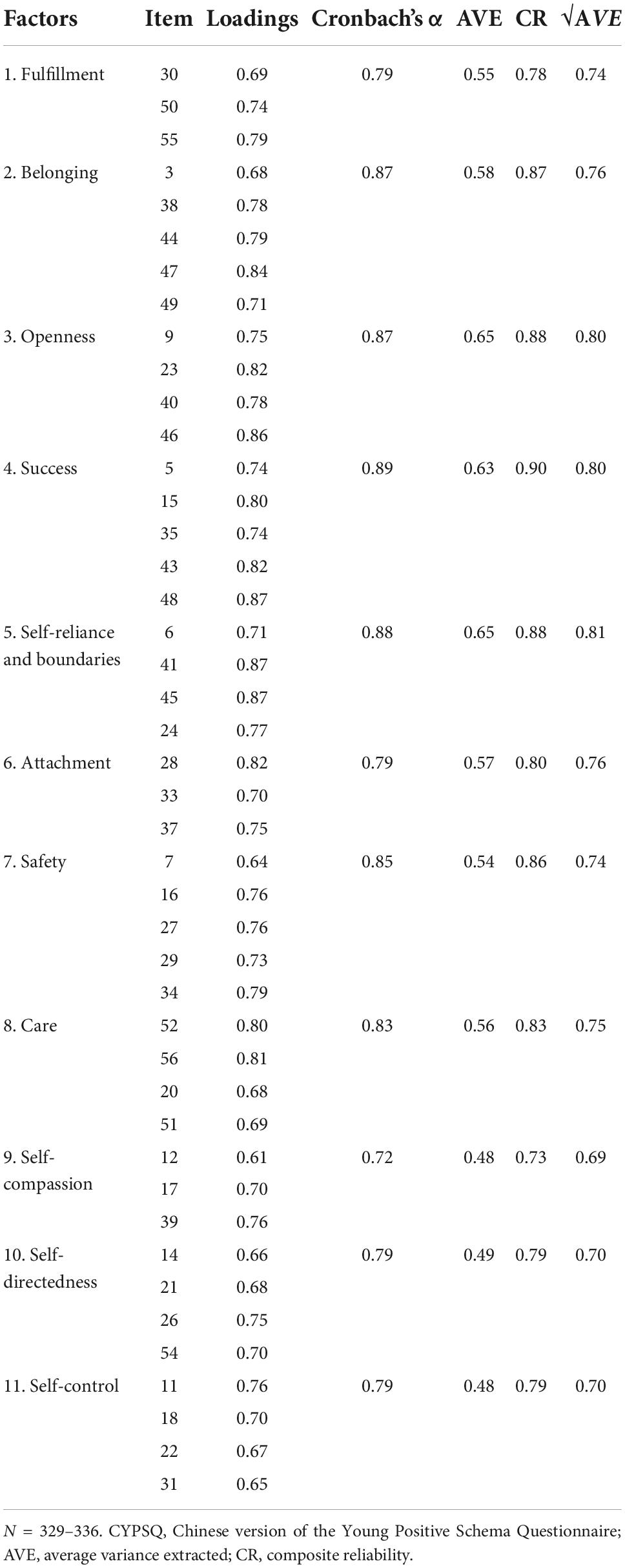
Table 4. Convergent validity and internal reliability of the 11-factor Chinese version of the Young Positive Schema Questionnaire (CYPSQ).
Discriminant validity
As shown in Table 5, discriminant validity was satisfied in most cases as the correlation coefficient for each factor was smaller than the root square of the AVE.
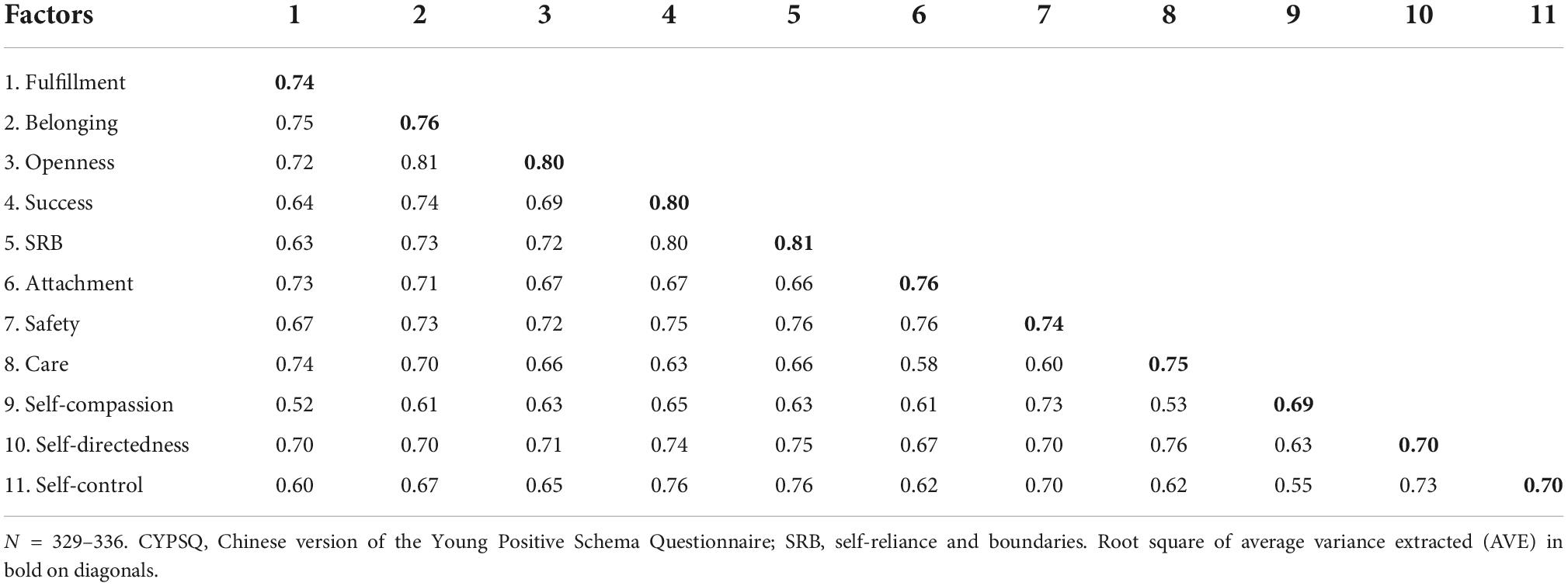
Table 5. Discriminant validity of the 11-factor Chinese version of the Young Positive Schema Questionnaire (CYPSQ).
Concurrent validity
Concurrent validity was tested by examining the correlations between factors of life satisfaction, resilience, anxiety, depression, and factors of the CYPSQ. All 11 CYPSQ factors were positively correlated with life satisfaction and resilience, and negatively correlated with anxiety and depression (Table 3).
Internal reliability
Internal reliability was verified as the Cronbach’s α and composite reliability values of the 11 factors of CYPSQ ranged from 0.72 to 0.89 and 0.73 to 0.90, respectively (Table 4), and these were all above the criterion of 0.70 (Fornell and Larcker, 1981; Nunnally and Bernstein, 1994).
Discussion
The concept and theories of early adaptive or positive schemas are important complements to the EMS theory. However, as the concept and measurement of positive schema were proposed and published only recently (Lockwood and Perris, 2012; Louis et al., 2018), the psychometric information of the CYPSQ in Mainland China is still lacking. Therefore, this study examined the psychometric properties of the CYPSQ in a community sample from Mainland China.
Main findings
Demographics
The findings of this study show that older people reported higher levels of all the 11 positive schemas. Few published studies have reported on the relationship between age and positive schemas. Thus, no comparison could be made. However, negative schemas were reported as dynamic constructs and may fade or intensify owing to specific contexts throughout the duration of one’s life (Legra et al., 2017). It was possible that positive schemas of the general population were developed through the course of individuals’ lives. Replications are required to confirm this finding.
Women reported lower levels of success, competence, safety, self-compassion, and self-control than men. No significant gender differences were found on other CYPSQ factors. According to the authors’ knowledge, no published studies have reported gender differences in positive schemas. Thus, no further comparisons could be made. However, a study among people with eating disorders and alcohol and substance use disorders found that women reported higher levels of maladaptive schemas such as abandonment, defectiveness, social undesirability, failure, dependence, subjugation, and self-sacrifice than men (Pauwels et al., 2013). Another study among people with alcohol dependence reported higher levels of self-sacrifice in women (Janson et al., 2019). It seems that women are more likely to be other-directed rather than self-directed, and are less likely to pursue success and competence. Studies across various cultures will help understand the sociocultural influence on positive schemas.
Construct validity
The findings of this study verified good psychometric properties with regard to most aspects of validity and reliability of the CYPSQ among a sample of 336 Chinese community residents. The original 14-factor YPSQ was verified in community samples from Singapore, the US, and Malaysia. However, this study identified an 11-factor YPSQ with 44 items instead of the original 14-factor YPSQ with 56 items. Nine positive schemas were conceptually fully retained: fulfillment (Items 4 and 25 were removed), belonging, openness, success, attachment (Item 2 was removed), safety, self-compassion, self-directedness, and self-control. The three items of self-reliance and one from boundaries (Item 24) were combined and renamed as self-reliance and boundaries. Two items each from self-care (Items 52 and 56) and empathic consideration (Items 20 and 51) were combined and renamed as care. The realistic expectation was removed. Similarly, a 10-factor YPSQ with 41 items was identified in a German community sample (Paetsch et al., 2020). It seems that the construct of YPSQ might vary a bit across cultures.
In the present study, the model fit indices of the 11-factor YPSQ were acceptable, the convergent validity was confirmed in all 11 factors, and the divergent validity was evident in 7 factors. Some factors showed a slightly lower divergent validity as they described a group of similar schemas. For example, fulfillment, belonging, and openness were positive schemas referring to social connection and acceptance; and self-directedness and self-control were about reasonable limits (Louis et al., 2018). The findings regarding convergent and divergent validities were consistent with those from other studies (Louis et al., 2018; Paetsch et al., 2020).
Concurrent validity
The findings of this study show that people with higher levels of positive schemas are more resilient and satisfied with life, and report lower levels of anxiety and depression. Positive schemas explained extra variance in depression, anxiety, stress, global severity of psychopathology, life satisfaction, resilience, and self-efficacy after controlling for EMSs (Louis et al., 2018; Paetsch et al., 2020). The positive schemas showed potential for reducing psychopathological outcomes and increasing one’s wellbeing. Future studies (especially longitudinal ones) can investigate such a possibility in clinical samples.
Internal reliability
The internal reliability was verified as all the Cronbach’s α and composite reliability values were above 0.70, indicating sufficient internal reliability (Fornell and Larcker, 1981; Nunnally and Bernstein, 1994). Similarly, the Cronbach’s α in the original 14- and 10-factor German YPSQ were all above 0.70, indicating good internal reliability across several population groups (Louis et al., 2018; Paetsch et al., 2020).
Implications and limitations
This study verified the validity and reliability of an 11-factor CYPSQ in a Chinese Mainland community sample. It is important to note that the evaluation of positive schema can balance the overt attention to psychopathology in clinical psychology. The findings of this study may contribute toward investigating the role of positive schemas in improving mental health and psychological wellbeing in Mainland China. Future studies are needed to examine the psychometric properties of the CYPSQ in clinical populations. Some limitations of this study require attention. As this study was cross-sectional, the test-retest reliability and predictive validity could not be verified. This study was conducted in a convenient community sample, and the results may not represent the general population in Mainland China.
Conclusion
This study verified the validity and reliability of the 11-factor CYPSQ in a Chinese community sample. Older people reported higher levels of all positive schemas than younger people, and men showed higher levels of some positive schemas (i.e., success, competence, safety, self-compassion, and self-control) than women. The findings show that positive schema levels may vary across population groups with different demographics (e.g., age and gender). This study may promote quantitative research on the role of positive schemas in improving mental health in Mainland China. The potentials of positive schemas in improving mental health and wellbeing need further longitudinal investigations.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by the Institutional Review Board of Ningbo Kangning Hospital (NBKNYY-2021-LC-50). The patients/participants provided their written informed consent to participate in this study.
Author contributions
DC and YZ contributed to study design, advised on methodology, reviewed and edited the thesis and manuscript, and finalized the manuscript. HM, YW, and DC reviewed and revised the Chinese version of YPSQ. XD, YW, and HZ analyzed the data. HM, XD, and HZ prepared the original draft of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by the Ningbo Medical and Health Brand Discipline (PPXK2018-08).
Acknowledgments
We thank all participants of this study. This study could not have been possible without their participation.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Bamelis, L. L., Evers, S. M., Spinhoven, P., and Arntz, A. (2014). Results of a multicenter randomized controlled trial of the clinical effectiveness of schema therapy for personality disorders. Am. J. Psychiatry 171, 305–322. doi: 10.1176/appi.ajp.2013.12040518
Bošnjak, S. (2001). The Declaration of Helsinki – the cornerstone of research ethics. Arch. Oncol. 9, 179–184.
Cheng, C., Dong, D., He, J., Zhong, X., and Yao, S. (2020). Psychometric properties of the 10-item Connor–Davidson Resilience Scale (CD-RISC-10) in Chinese undergraduates and depressive patients. J. Affect. Disord. 261, 211–220. doi: 10.1016/j.jad.2019.10.018
Comrey, A. L., and Lee, H. B. (1992). A first course in factor analysis, 2nd Edn. New York, NY: Psychology Press. doi: 10.4324/9781315827506
Connor, K. M., and Davidson, J. R. (2003). Development of a new resilience scale: The Connor-Davidson resilience scale (CD-RISC). Depress. Anxiety 18, 76–82. doi: 10.1002/da.10113
Costa, P. T. Jr., and McCrae, R. R. (2008). “The revised NEO personality inventory (NEO-PI-R),” in The SAGE handbook of personality theory and assessment: Personality measurement and testing, Vol. 2, eds G. J. Boyle, G. Matthews, and D. H. Saklofske (Thousand Oaks, CA: SAGE), 179–198. doi: 10.4135/9781849200479.n9
Duan, W., Fei, Y., Zhao, J., and Guo, X. (2020). Incremental validity of the comprehensive inventory of thriving in predicting self-reporting mental and physical health among community populations. J. Health Psychol. 25, 1366–1373. doi: 10.1177/1359105318755265
Fornell, C., and Larcker, D. F. (1981). Structural equation models with unobservable variables and measurement error: Algebra and statistics. J. Mark. Res. 18, 382–388. doi: 10.2307/3150980
Hair, J., Hult, T., Ringle, C., and Sarstedt, M. (2014). A primer on partial least squares structural equation modeling (PLS-SEM). Thousand Oaks, CA: Sage.
Harriss, D. J., MacSween, A., and Atkinson, G. (2019). Ethical standards in sport and exercise science research: 2020 update. Int. J. Sports Med. 40, 813–817. doi: 10.1055/a-1015-3123
Hu, L. T., and Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 6, 1–55. doi: 10.1080/10705519909540118
Huang, J. L., Curran, P. G., Keeney, J., Poposki, E. M., and DeShon, R. P. (2012). Detecting and deterring insufficient effort responding to surveys. J. Bus. Psychol. 27, 99–114. doi: 10.1007/s10869-011-9231-8
Janson, D. L., Harms, C. A., Hollett, R. C., and Segal, R. D. (2019). Differences between men and women regarding early maladaptive schemas in an Australian adult alcohol dependent clinical sample. Subst. Use Misuse 54, 177–184. doi: 10.1080/10826084.2018.1480038
Johnson, J. A. (2005). Ascertaining the validity of individual protocols from web-based personality inventories. J. Res. Pers. 39, 103–129. doi: 10.1016/j.jrp.2004.09.009
Kroenke, K., Spitzer, R. L., and Williams, J. B. (2001). The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 16, 606–613. doi: 10.1046/j.1525-1497.2001.016009606.x
Legra, M. J. H., Verhey, F. R. J., and van Alphen, S. P. J. (2017). A first step toward integrating schema theory in geriatric psychiatry: A Delphi study. Int. Psychogeriatr. 29, 1069–1076. doi: 10.1017/s1041610217000412
Lockwood, G., and Perris, P. (2012). “A new look at core emotional needs,” in The Wiley-Blackwell handbook of schema therapy: Theory, research, and practice, eds M. van Vreeswijk, J. Broersen, and M. Nadort (Oxford: Wiley Blackwell), 41–66. doi: 10.1002/9781119962830.ch3
Louis, J. P., Wood, A. M., Lockwood, G., Ho, M.-H. R., and Ferguson, E. (2018). Positive clinical psychology and schema therapy (ST): The development of the Young Positive Schema Questionnaire (YPSQ) to complement the Young Schema Questionnaire 3 Short Form (YSQ-S3). Psychol. Assess. 30, 1199–1213. doi: 10.1037/pas0000567
Nunnally, J. C., and Bernstein, I. H. (1994). Psychometric theory, 3 Edn. New York, NY: McGraw-Hill.
Paetsch, A., Moultrie, J., Kappelmann, N., Fietz, J., Bernstein, D. P., and Kopf-Beck, J. (2020). The Young Positive Schema Questionnaire (YPSQ): German validation, domain structure, and network analysis in patients and matched controls. J. Pers. Assess. 104, 522–531. doi: 10.1080/00223891.2021.1966020
Pauwels, E., Claes, L., Smits, D., Dierckx, E., Muehlenkamp, J. J., Peuskens, H., et al. (2013). Validation and reliability of the Young Schema Questionnaire in a flemish inpatient eating disorder and alcohol and substance use disorder sample. Cogn. Ther. Res. 37, 647–656. doi: 10.1007/s10608-012-9501-4
Peeters, N., van Passel, B., and Krans, J. (2021). The effectiveness of schema therapy for patients with anxiety disorders, OCD, or PTSD: A systematic review and research agenda. Br. J. Clin. Psychol. 61, 579–597. doi: 10.1111/bjc.12324
Rashid, T. (2015). Positive psychotherapy: A strength-based approach. J. Posit. Psychol. 10, 25–40. doi: 10.1080/17439760.2014.920411
Seligman, M. E., Rashid, T., and Parks, A. C. (2006). Positive psychotherapy. Am. Psychol. 61, 774–788. doi: 10.1037/0003-066x.61.8.774
Spitzer, R. L., Kroenke, K., Williams, J. B., and Löwe, B. (2006). A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 166, 1092–1097. doi: 10.1001/archinte.166.10.1092
Su, R., Tay, L., and Diener, E. (2014). The development and validation of the Comprehensive Inventory of Thriving (CIT) and the Brief Inventory of Thriving (BIT). Appl. Psychol. Health Well Being 6, 251–279. doi: 10.1111/aphw.12027
Tyebkhan, G. (2003). Declaration of Helsinki: The ethical cornerstone of human clinical research. Indian J. Dermatol. Venereol. Leprol. 69, 245–247.
Wang, C. E., Halvorsen, M., Eisemann, M., and Waterloo, K. (2010). Stability of dysfunctional attitudes and early maladaptive schemas: A 9-year follow-up study of clinically depressed subjects. J. Behav. Ther. Exp. Psychiatry 41, 389–396. doi: 10.1016/j.jbtep.2010.04.002
Wood, A. M., and Tarrier, N. (2010). Positive clinical psychology: A new vision and strategy for integrated research and practice. Clin. Psychol. Rev. 30, 819–829. doi: 10.1016/j.cpr.2010.06.003
World Medical Association (2013). Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 310, 2191–2194. doi: 10.1001/jama.2013.281053
Yentes, R. D., and Wilhelm, F. (2018). Careless: Procedures for computing indices of careless responding. R packages version 1.2.0.
Young, J. E., Klosko, J. S., and Weishaar, M. E. (2003). Schema therapy: A practitioner’s guide. New York, NY: Guilford Press.
Keywords: early adaptive schema, positive schema, resilience, life satisfaction, depression, anxiety
Citation: Chi D, Du X, Ma H, Wang Y, Zhang Y and Zhong H (2022) Validity and reliability of the Chinese version of the Young Positive Schema Questionnaire. Front. Psychol. 13:1048954. doi: 10.3389/fpsyg.2022.1048954
Received: 20 September 2022; Accepted: 21 November 2022;
Published: 02 December 2022.
Edited by:
Hamid Sharif Nia, Mazandaran University of Medical Sciences, IranReviewed by:
Antonio Hernández-Mendo, University of Malaga, SpainValentina Marinescu, University of Bucharest, Romania
Copyright © 2022 Chi, Du, Ma, Wang, Zhang and Zhong. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yuanyuan Zhang, eXVhbnl1YW56aGFuZ0Bwcm90b25tYWlsLmNvbQ==