 Yen-Jen Chen
Yen-Jen Chen Kai-Ming Jhang
Kai-Ming Jhang Wen-Fu Wang
Wen-Fu Wang Guan-Cheng Lin4†
Guan-Cheng Lin4† Shao-Wei Yen
Shao-Wei Yen Hsin-Hung Wu
Hsin-Hung Wu- 1Department of Psychiatry, Changhua Christian Hospital, Changhua, Taiwan
- 2Department of Neurology, Changhua Christian Hospital, Changhua, Taiwan
- 3Department of Recreation and Holistic Wellness, Ming Dao University, Changhua, Taiwan
- 4Department of Business Administration, National Changhua University of Education, Changhua, Taiwan
- 5Department of Information Management, National Changhua University of Education, Changhua, Taiwan
- 6Department of M-Commerce and Multimedia Applications, Asia University, Taichung, Taiwan
- 7Faculty of Education, State University of Malang, Malang, East Java, Indonesia
Purpose: The aim of this study was to identify the combination of patients with dementia and their caregivers' characteristics associated with long-term care (LTC) services usage.
Patients and methods: A cross-sectional study was conducted with 475 patients with mild, moderate, and severe dementia at Changhua Christian Hospital, Taiwan. Eleven types of variables from patients with dementia, nine types of variables from patients' caregivers, and 15 types of LTC services were used for this study. The Apriori algorithm was employed to identify the attributes from the patients and their caregivers who used a particular LTC service from a comprehensive viewpoint.
Results: A total of 75 rules were generated by the Apriori algorithm with support of 2%, confidence of 80%, and lift >1. Among these rules, 25 rules belonged to home personal care services which were summarized further into four general rules for home personal care services. On the other hand, 50 rules belonged to assistive devices that were summarized further into 21 general rules based on their similarities. Patient's walking ability, patient's emotional liability, unemployed or retired caregivers, caregivers' feelings with either helplessness or hopelessness, and caregivers who cared for patients with dementia solely were found to be the critical variables to use home personal care services. In contrast, patient's walking ability, age, and severity as well as caregivers' age, mood, marital status, caregiving burden, and the patient being cared for mainly by a foreign care helper were found to be the critical variables to use assistive devices.
Conclusion: This study showed preliminary results on the LTC service usage from patients with dementia and their caregivers residing in the community. Understanding the patient–caregiver dyad's profile leads the service providers, policymakers, and the referral team to tailor service provisions better to meet the needs and identify the potential target groups. The findings in this study serve as references to reduce caregivers' burden as well as to improve the quality of care for patients with dementia.
Introduction
Population aging is one of the major public health issues influencing all developed countries including Taiwan. Taiwan is an aged society in 2022 and is predicted to become a superaged society by 2025. The number of patients with dementia has increased dramatically with rapid growth of the elderly population. In a nation-wide population-based study in Taiwan, the prevalence of dementia increased significantly from 4.7 per 100 people to 7.6 per 100 people from 2004 to 2010, although the incidence of dementia was similar during the same period (Liu et al., 2019). A high incidence of this disease in the older-adult population has a great impact on patients, their family, and the entire society.
The long-term care (LTC) system was set up in Taiwan in 2007 as a response to an aging society. To help families of patients with dementia further, the government in Taiwan established the Long-Term Care (LTC) Act 2.0 in 2017, which covered people with dementia over the age of 50 (Hsu and Chen, 2019). According to the payment categorization in LTC Plan 2.0, long-term care resources were divided into four parts: personal and professional care (including in-home and community-based services such as home personal care or daycare services, home nursing or home rehabilitation services, etc.), transportation services (shuttling from home to hospital), assistive devices (walkers, wheelchairs, commode chairs, relief air mattress, etc.) and in-house barrier-free environment modification (suitable devices that are suggested by therapists and granted partly by the government), and respite care for family caregivers (provided by personal care attendants to allow family caregivers rest for hours to days) (Hsu and Chen, 2019; Yang et al., 2020; Ministry of Health and Welfare, 2022). The goal of LTC Plan 2.0 is to keep aging in place so as to establish an accessible, affordable, and universal long-term care service system. Care management center in the health bureau of each county draws up care plans and links services. Most of the costs are borne by the government (covering by taxes).
Dementia and dependency are predictive factors for LTC service usage and the utilization is related to the level of disability (Wu et al., 2014; Fabius et al., 2022). Older adults' service use patterns partially explain the transitions between community and institutionalization (Chen and Berkowitz, 2012). However, the decision to move to a nursing home or stay resident in the community is complex and multifactorial. Neuropsychiatric symptoms, walking capability, and living status also contribute to the decision of either nursing home stay or home care assistance (Chen et al., 2022). Use of home care assistance service was postulated to potentially lower the probability of nursing home placement (Greiner et al., 2014).
In Taiwan, the overall LTC service utilization rate for patients with dementia was about one-third and home personal care service and assistive devices were the items commonly applied for (Wang W. F. et al., 2021). Drivers of long-term care considerations may be even more complicated. Factors such as dementia stage, capability of activity daily living (ADL), resource of informal and paid care, relationship between the care provider and the recipient, sociocultural context, and the LTC system design all needed to be considered (Morrisby et al., 2018; Shepherd-Banigan et al., 2021). A national dementia registry enrolled 1,268 Taiwanese and revealed that aberrant motor behaviors, dysfunction in ADLs, higher caregiver burden, not residing with family members, and not employing a migrant caregiver were the factors associated with LTC service usage (Tsai et al., 2022).
Investigating dozens of factors at the same time is sometimes effortful and the interpretations become difficult. However, the Apriori algorithm reveals important statistical correlations from viewpoints involving several dimensions or aspects (Chen et al., 2019, 2021; Yan et al., 2019; Lin et al., 2020). Each attribute is viewed as a dimension by appointing threshold values of support and confidence (Han and Kamber, 2006). Therefore, the aim of the present study was to apply the Apriori algorithm to identify the combination of patients with dementia and their caregivers' characteristics associated with LTC services use, especially home personal care service and assistive device in particular.
Patients and method
This study included 1,201 patients who were diagnosed with mild cognitive impairment or dementia at the memory clinic of Changhua Christian Hospital from October 2015 to June 2021. The diagnosis of dementia was based on the clinical dementia rating (CDR) scale by clinical psychologists (Morris, 1997). Based on the collected data, the use of long-term care services was low among patients with very mild dementia (CDR = 0.5). In order to draw up rules on the usage of LTC services by caregivers with stronger demands, this study excluded the data from patients with very mild dementia. In contrast, this study focused on patients with mild, moderate, and severe dementia, and a total of 475 valid data sets were finally used. The clinical trial number was CCH IRB 220225, which was approved by the Institutional Review Board of Changhua Christian Hospital. In addition, this study used the retrospective study design, while the need for informed consent was waived off by the Institutional Review Board of Changhua Christian Hospital. All data were recorded in the electronic medical chart with the highest confidentiality and compliance with the Declaration of Helsinki.
The variables from patients with dementia consisting of age, gender, marital status, living status, type of dementia, CDR, walking ability, psychological symptoms, mood symptoms, and behavioral symptoms are summarized in Table 1. The care recipient's mood and behavioral and psychological symptoms of dementia (BPSD) for the patients were assessed by using a two-point scale to record the data (1 if the mood/symptom was applied; 0 if not). The presence of BPSD was evaluated by psychologists or trained nursing case managers. Most of the BPSDs listed in the neuropsychiatric inventory (NPI) were recorded by clinical psychologists (Cummings et al., 1994). Other abnormal behaviors, such as pathological crying or laughing, akathisia, wandering, cursing others, and akinesia which were frequently observed in patients with dementia, were also noted by trained nursing case managers. Emotional liability refers to emotional and uncontrollable emotions, and/or emotions that are out of proportion to circumstances, defined by the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) (American Psychiatric Association, 2013).
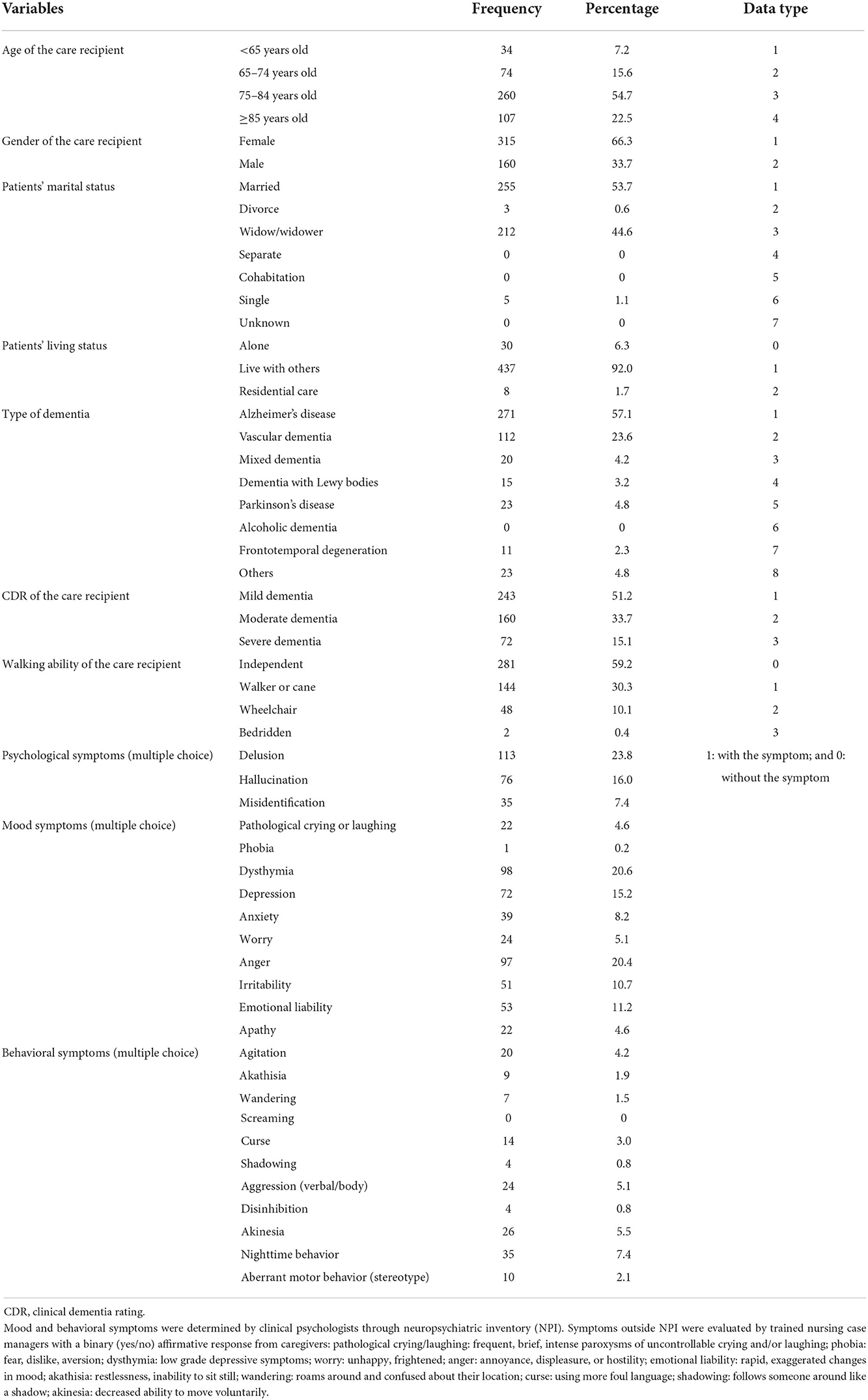
Table 1. Demographic information of the patients and data types.
The variables from caregivers including the age, relation to the patient with dementia, employment, marital status, education, type of primary care, frequency of care, caregiver's mood, and Zarit burden interview (ZBI) caregiving burden are summarized in Table 2. The caregiver's mood was assessed by the 12-item Chinese Health Questionnaire (CHQ-12), which is a short, self-administered screening tool for general mental health (Chong and Wilkinson, 1989). Emotional liability included in this study was selected, if rapid, exaggerated changes in the caregiver's mood were noted. The caregiver's mood was assessed by using a two-point scale to record the data, i.e., 1 if the mood was applied; 0 if not. Besides, the ZBI caregiving burden assessed by the Zarit burden interview (ZBI) (Bédard et al., 2001) had four categories, including little or no burden (0–20 points), mild to moderate burden (21–40 points), moderate to severe burden (41–60 points), and severe burden (61–88 points).
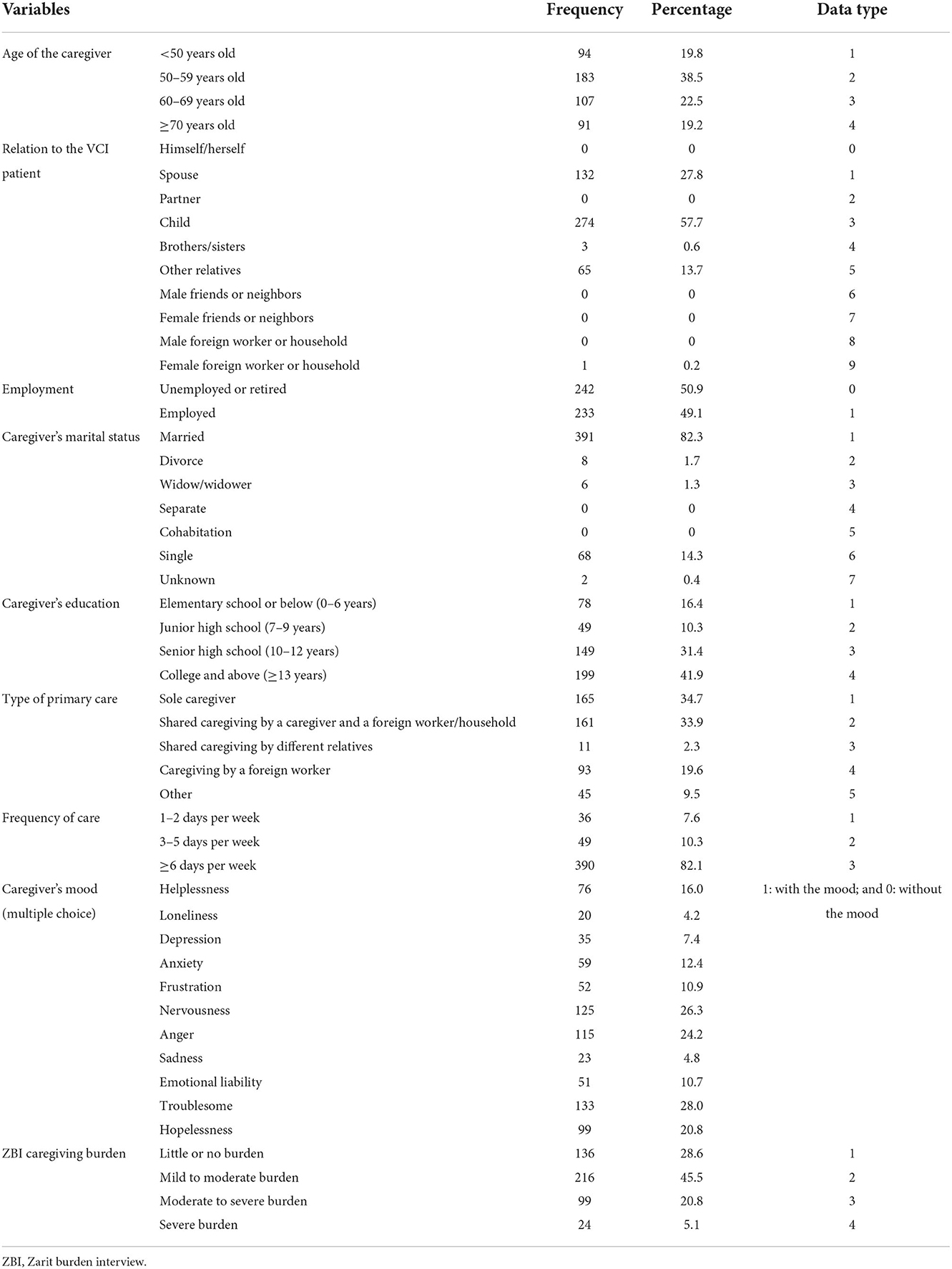
Table 2. Demographic information of the caregivers and data types.
Fifteen long-term care services for older patients with dementia are depicted in Table 3. If patients and their caregivers used a particular LTC service, a value of 1 is assigned. If not, a value of 0 is given. Based on Table 3, assistive devices (27.8%), home personal care services (19.2%), and community care centers (13.1%) were the top three LTC services utilized by patients with dementia and their caregivers.

Table 3. Long-term care (LTC) services for older patients with dementia.
The purpose of this study was to identify which attributes from patients and/or caregivers could result in different usages of the LTC services. The Apriori algorithm has been proven to be very effective in identifying statistical correlations from a multidimensional viewpoint in dementia-related areas by setting up support, confidence, and lift (Jhang et al., 2019, 2020; Chang et al., 2021). Thus, the Apriori algorithm was used in this study. The definitions and formulas of support, confidence, and lift are given below (Chang et al., 2021; Jhang et al., 2021). The support of an association rule A ⇒ B is defined by calculating the percentage of transactions containing both A and B in the database depicted in Equation (1):
The confidence of the association rule A ⇒ B is used to compute the percentage of transactions containing A and also containing B simultaneously in the database in Equation (2):
Lift measures the correlation between A and B, as shown in Equation (3). If a lift has a value of 1, A and B are independent and no rule will be generated. If a lift has a value >1, A and B are dependent and correlated positively.
The Apriori algorithm in IBM SPSS Modeler 18 was employed. Data type for each variable was defined by the numerical values as shown in Tables 1, 2 for patients with dementia and their caregivers, respectively. The input variables for antecedents from Table 1 were care recipient's age, gender, marital status, living status, type of dementia, CDR, walking ability, three types of psychological symptoms, 10 types of mood symptoms, and 11 types of behavioral symptoms. In addition, the caregiver's age, relation to the patient, employment, marital status, education, type of primary care, frequency of care, 11 types of caregiver's moods, and ZBI caregiving burden from Table 2 were input variables for antecedents. On the other hand, 15 types of LTC services were the input variables for the consequent. Due to the heterogeneous data, the minimum support was set to 2%, whereas the minimum confidence was set to 80% with a lift >1.
Results
The major characteristics of patients with dementia depicted in Table 1 were female (66.3%), aged 75–84 years (54.7%), and who had Alzheimer's disease (57.1%) with mild dementia (51.2%). In addition, nearly 60% of the patients with dementia could walk independently. On the other hand, 38.5% of the caregivers were aged 50–59 years, and nearly 60% of the caregivers were the children of the patients based on Table 2. More than 80% of the caregivers were married, and 50.9% of the caregivers were unemployed or retired. The type of primary care for care recipient was either sole caregiver (34.7%) or shared caregiving by a caregiver and a foreign worker/household (33.9%). Frequency of care ≥6 days per week was the majority (82.1%). Additionally, the caregiving burden mainly fell into either mild to moderate burden (45.5%) or little or no burden (28.6%).
There were 75 rules generated by the Apriori algorithm with support of 2%, confidence of 80%, and lift >1. Among these rules, 25 belonged to home personal care services and 50 belonged to assistive devices. Based on these 25 rules, four general rules were summarized, based on their similarities to home personal care services. On the other hand, based on these 50 rules, 21 general rules were summarized, based on their similarities to assistive devices.
The first general rule depicted in Table 4 indicated that home personal care services would be required when a sole caregiver whose age was ≥70 years with a mood of helplessness took care of a patient with dementia, regardless of a mix of patient's living status, patient's marital status, caregiver's marital status, frequency of care, or relation to the patient. The second general rule showed that when a sole caregiver who had a mood of helplessness took care of a patient with dementia who had the walking ability by a walker or cane, home personal care services would be needed. The variables of frequency of care and patient's living status were not the critical determinants for home personal care services. For the third general rule, home personal care services would be needed when a sole caregiver who had moods of hopelessness, nervousness, and troublesome took care of a patient with dementia, regardless of the frequency of care and patient's living status. Finally, the fourth general rule indicated that when a caregiver was unemployed or retired and had a mood of hopelessness but who needed to take care of a patient with dementia with a mood symptom of emotional liability, home personal care services should be provided. In addition, frequency of care was not a critical variable to determine the use of home personal care services.
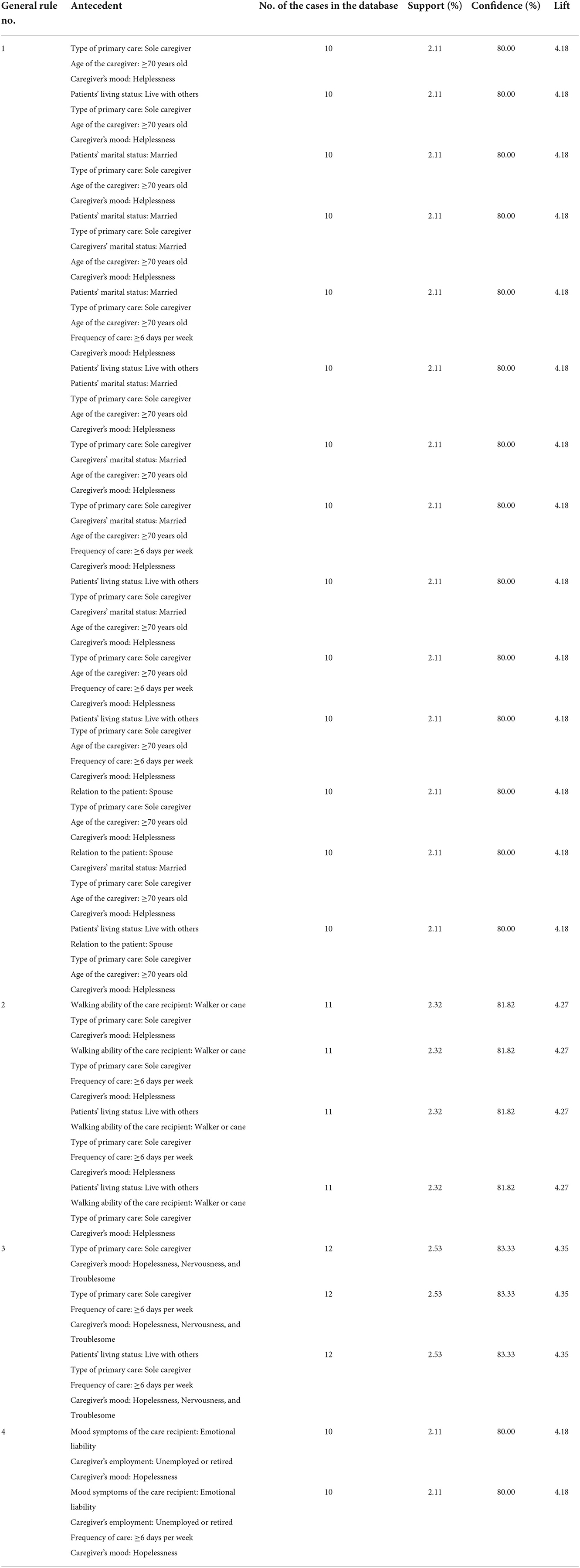
Table 4. Four general rules for home personal care services.
As shown in Table 5, assistive devices were needed when a patient with dementia needed a wheelchair and was cared for by a foreign worker with a frequency of ≥6 days per week (first general rule); when a patient with dementia whose age was 75–84 years had a psychological symptom of hallucination along with a caregiver's mood of troublesome (second general rule); when a female patient with moderate dementia was cared for by a foreign worker (third general rule); when an employed person who had mild to moderate burden needed to provide care for a patient with dementia cared for by a foreign worker (fourth general rule); when a patient with moderate dementia whose age was ≥85 years was cared for by an unemployed or retired caregiver whose age was 60–69 years with mild to moderate caregiving burden (fifth general rule); when a female patient with severe dementia living with others was cared for by a caregiver who had mild to moderate caregiving burden (sixth general rule); when an employed person whose age was 50–59 years with the education of college and above needed to provide care for a patient with dementia cared for by a foreign worker (seventh general rule); when an employed person whose age was 50–59 years provided care for a patient with dementia but whose marital status was widow or widower cared for by a foreign worker (eighth general rule); and when a child provided care for a married patient with Alzheimer's disease cared for by a foreign worker (ninth general rule).

Table 5. Twenty-one general rules for assistive devices.
Moreover, assistive devices were needed when a female patient with dementia whose age was 75–84 years with the walking ability by a walker or cane was cared for by a caregiver whose mood was hopelessness (tenth general rule); when a patient with moderate dementia whose marital status was widow or widower with the walking ability by a walker or cane was cared for by a caregiver whose mood was troublesome (eleventh general rule); when a female and married patient with dementia who had the walking ability by a walker or cane was cared for by a caregiver whose education was senior high school (twelfth general rule); when a patient with moderate dementia whose marital status was widow or widower was cared for by his or her child whose age was 50–59 years with the mood of troublesome (thirteenth general rule); when a patient with moderate dementia with the age of 75–84 years whose marital status was widow or widower was cared for by a caregiver whose mood was troublesome by a frequency of ≥6 days per week (fourteenth general rule); when a patient with dementia whose age was 75–84 years was cared for by his or her child who had mild to moderate caregiving burden and the mood of hopelessness with the frequency of ≥6 days per week (fifteenth general rule); and when a patient with dementia with the age of 75–84 years who had the walking ability by a walker or cane was cared for by a caregiver who had mild to moderate burden with the mood of troublesome (sixteenth general rule).
From seventeenth to twenty-first general rules as shown in Table 5, each general rule only consisted of one rule due to its rule dissimilarities. When a patient with dementia living with others who needed a wheelchair was cared for by a caregiver whose age was 50–59 years with the education of college and above, assistive devices were required (seventeenth general rule). A female and married patient with dementia who had the walking ability by a walker or cane was cared for by a married caregiver and a foreign worker/household needed assistive devices (eighteenth general rule). When a child who had mild to moderate burden provided care for a patient with Alzheimer's disease was cared for by a foreign worker with the frequency of ≥6 days per week, assistive devices were needed (nineteenth general rule). Assistive devices were required when a male patient with Alzheimer's disease was cared for by an unemployed or retired caregiver who had the moods of troublesome and hopelessness (twentieth). Finally, twenty-first general rule indicated that assistive devices were needed when a patient with dementia with the mood symptom of anger who had the walking ability by a walker or cane was cared for by a married and unemployed or retired caregiver with the frequency of ≥6 days per week.
Discussion
This study identified certain combinations of the patient–caregiver dyads which resort to either home personal care services or assistive devices for patients with dementia in Taiwan.
In general, patient's living status, patient's walking ability, and mood condition with caregivers' age, caregiving frequency, and employment status were associated with the use of home personal care services. Patients who were taken care of by informal caregivers with the frequency of ≥6 days per week and the caregivers who experienced helplessness or hopeless mood were associated with the use of home personal care services. Patients with emotional liability or being taken care of by their spouses who were aged ≥70 years or unemployed caregivers were also associated with the use of home personal care services. On the other hand, patient's age, marital status, dementia severity, and ambulatory status as well as caregivers' age, type of primary care, frequency of care, caregivers' mood, and caregivers' burden were associated with the use of assistive devices. People living with dementia applying assistive devices were older (≥75 years old), had moderate to severe dementia, needed assistance in walking or were wheelchair bound, and were being cared for mainly by a foreign care helper.
As in Western countries, LTC service is a complex package in Taiwan that is allocated to use different services in the same manner regarding the severity of disability and dementia (Feldman et al., 2021; Van Cleve and Degenholtz, 2022). Our findings provided a glimpse of the LTC service usage among patient–caregiver dyads of patients with dementia in Taiwan. Generosity and accessibility of the LTC service also contribute to the results (Wysocki et al., 2015; Wang S. et al., 2021).
Factors that are related to institutionalization and assisted living service in community sometimes overlapped. Physical function, cognition, and mood condition are worthy of keeping an eye on. Not surprisingly, the health profiles including age, dementia severity, and walking ability are associated with the LTC service usage (Liu et al., 2018). Care recipient's dependency is positively correlated with the utilization of LTC services (Feldman et al., 2021; Van Cleve and Degenholtz, 2022). This profile may drive the LTC service to fit their users better.
Caregivers' employment status also appears to be in relation to the association rules. Feldman et al. (2021) also found caregivers not working had a greater likelihood of service usage. Behavioral and psychological symptoms presented in 80% of the dementia population from the onset of cognitive dysfunction lead to heavy burden on both the patients and their caregivers (Lyketsos et al., 2002; Baharudin et al., 2019). Home health aides and home personal care services are reported to reduce caregivers' burden in mean caregiver strain scores (Reckrey et al., 2021). Patients with emotional liability, anxiety mood, and hallucination are found to be associated with the LTC usage in the present study. Our study also reveals that the picture of higher strain of caregiving presenting as a feeling of being over relied on may force the patients and their caregivers to resort to both services. It is worth considering the need of social services, physical function, cognition, and mood condition. Mood conditions of both patients and their caregivers are worth recording and intervention. Non-pharmacological and pharmacological treatments for BPSD, as well as the caregiver support group and education to relieve caregiver's helplessness, are important assistance measures for caregivers who take care of people with dementia (Livingston et al., 2005; McLoughlin, 2022).
The strength of the present study includes comprehensive characteristics of people living with dementia and their caregivers, as well as care mode and care load. Another strength of the present study is the fact that through using the Apriori algorithm, the caring scenario associated with the LTC service usage could be elucidated. However, there are some study limitations. First, when applying the Apriori algorithm, there is no universal approach to set up support and confidence values in order to generate association rules. In general, a higher confidence value, say 90% or above, is recommended when a conditional probability is applied to study the associations of attributes. In contrast to confidence, setting a support value is usually correlated with the diversity of factors included in the analysis. Higher support values reduce the number of rules and easily summarize meaningful results, whereas lower support values help in generating some essential rules with low frequencies. Because of the heterogeneity between patients' and caregivers' characteristics and the usage of LTC services, the confidence and support values were set as 80% and 2% in order to generate association rules. No rules could achieve above 90% confidence value, which weakened the conditional probability of associations. Second, some important factors associated with LTC service usage, including average family income and accessibility of the LTC service, were not included in the present study. Third, the cross-sectional design made it difficult to determine the causal relationship between the correlates and the usage of LTC services.
This study provides preliminary results on the LTC service usage from people living with dementia and their caregivers residing in the community. Understanding the patient–caregiver dyad's profile leads the service providers, policymakers, and the referral team to tailor service provisions better to meet the needs and identify the potential target groups.
Conclusion
This study identified 75 rules on the usage of LTC services by a comprehensive analysis of the characteristics of patients with dementia and their caregivers. There were 25 rules belonging to home personal care services, which could be summarized further into four general rules. Patient's walking ability (by a walker or cane), patient's emotional liability, unemployed or retired caregivers, caregivers' feelings with either helplessness or hopelessness, and caregivers who cared for the patients with dementia solely were found to be the critical variables to use home personal care services. On the contrary, patient's walking ability (mainly by a walker or cane), age, and severity as well as caregivers' age, mood, marital status, caregiving burden, and the patient being cared for mainly by a foreign care helper were found to be the critical variables to use assistive devices services. Aside from each patient's and caregiver's basic characteristics and caregiving load, the present study highlighted that mood conditions of both patients and caregivers were associated with LTC services usage. It is worthy to check and give an appropriate intervention for the abnormal mood status of people with dementia and their caregivers. These general rules serve as references to provide either home personal care services or assistive devices to reduce caregivers' burden as well as to improve the quality of care for patients with dementia.
Data availability statement
The datasets presented in this article are not readily available because following our hospital's regulation, individual de-identified data should pass both the Research and Development Committee and Institutional Review Board (IRB). Researchers should write a research proposal and apply a clinical trial for the IRB of our hospital. All data listed in the present manuscript can be obtained through email if both committees agree the application. Further inquiries can be directed to the corresponding author.
Ethics statement
The Clinical Trial Number was CCH IRB 220225, which was approved by the Institutional Review Board of Changhua Christian Hospital. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Funding
This study was supported by grants from the National Health Research Institutes, Taiwan (PH-111-GP-08).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th. Edition. Washington, DC: American Psychiatric Publishing. doi: 10.1176/appi.books.9780890425596
Baharudin, A. D., Din, N. C., Subramaniam, P., and Razali, R. (2019). The associations between behavioral-psychological symptoms of dementia (BPSD) and coping strategy, burden of care and personality style among low-income caregivers of patients with dementia. BMC Public Health. 19, 447. doi: 10.1186/s12889-019-6868-0
Bédard, M., Molloy, D. W., Squire, L., Dubois, S., Lever, J. A., O'Donnell, M., et al. (2001). The Zarit burden interview: a new short version and screening version. Gerontologist. 41, 652–657. doi: 10.1093/geront/41.5.652
Chang, C. C., Wang, W. F., Li, Y. Y., Chen, Y. A., Chen, Y. J., Liao, Y. C., et al. (2021). Using the Apriori algorithm to explore caregivers' depression by the combination of the patients with dementia and their caregivers. Risk Manag. Healthc. Policy. 14, 2953–2963. doi: 10.2147/RMHP.S316361
Chen, W. J., Wang, W. F., and Liu, Y. H. (2019). Using Apriori algorithm to explore the influence of pressure from patients with dementia on caregivers from a medical center in Taiwan. J. Qual. 26, 395–418. doi: 10.6220/joq.201912_26(6).0004
Chen, Y. A., Chang, C. C., Wang, W. F., Lin, Y. S., Jhang, K. M., Lo, T. Y., et al. (2021). Association between caregivers' burden and neuropsychiatric symptoms in female patients with Alzheimer's disease with varying dementia severity. J. Multidiscip. Healthc. 14, 929–940. doi: 10.2147/JMDH.S298196
Chen, Y. J., Wang, W. F., Jhang, K. M., Chang, M. C., Chang, C. C., Liao, Y. C., et al. (2022). Prediction of institutionalization for patients with dementia in Taiwan according to condition at entry to dementia collaborative care. J. Appl. Gerontol. 41, 1357–1364. doi: 10.1177/07334648211073129
Chen, Y. M., and Berkowitz, B. (2012). Older adults' home- and community-based care service use and residential transitions: a longitudinal study. BMC Geriatr. 12, 44. doi: 10.1186/1471-2318-12-44
Chong, M. Y., and Wilkinson, G. (1989). Validation of 30- and 12-item versions of the Chinese Health Questionnaire (CHQ) in patients admitted for general health screening. Psychol Med. 19, 495–505. doi: 10.1017/S0033291700012526
Cummings, J. L., Mega, M., Gray, K., Rosenberg-Thompson, S., Carusi, D. A., Gornbein, J., et al. (1994). The neuropsychiatric inventory: comprehensive assessment of psychopathology in dementia. Neurology. 44, 2308–2314. doi: 10.1212/WNL.44.12.2308
Fabius, C. D., Okoye, S. M., Mulcahy, J., Burgdorf, J. G., and Wolff, J. L. (2022). Associations between use of paid help and care experiences among medicare-medicaid enrolled older adults with and without dementia. J. Gerontol. B Psychol. Sci. Soc. Sci. doi: 10.1093/geronb/gbac072
Feldman, S. J., Solway, E., Kirch, M., Malani, P., Singer, D., Roberts, J. S., et al. (2021). Correlates of formal support service use among dementia caregivers. J. Gerontol. Soc. Work. 64, 135–150. doi: 10.1080/01634372.2020.1816589
Greiner, M. A., Qualls, L. G., Iwata, I., White, H. K., Molony, S. L., Sullivan, M. T., et al. (2014). Predicting nursing home placement among home- and community-based services program participants. Am. J. Manag. Care. 20, e535–536.
Han, J., and Kamber, M. (2006). Data Mining: Concepts and Techniques, 2nd ed. New York: Morgan Kaufmann Publishers.
Hsu, H. C., and Chen, C. F. (2019). LTC 2.0: the 2017 reform of home- and community-based long-term care in Taiwan. Health Policy. 123, 912–916. doi: 10.1016/j.healthpol.2019.08.004
Jhang, K. M., Chang, M. C., Lo, T. Y., Lin, C. W., Wang, W. F., Wu, H. H., et al. (2019). Using the Apriori algorithm to classify the care needs of patients with different types of dementia. Patient Prefer Adherence 13, 1899–1912. doi: 10.2147/PPA.S223816
Jhang, K. M., Wang, W. F., Chang, H. F., Chang, M. C., and Wu, H. H. (2021). Characteristics predicting a high caregiver burden in patients with vascular cognitive impairment: using the Apriori algorithm to delineate the caring scenario. Risk Manag. Healthc. Policy 14, 1335–1351. doi: 10.2147/RMHP.S297204
Jhang, K. M., Wang, W. F., Chang, H. F., Liu, Y. H., Chang, M. C., Wu, H. H., et al. (2020). Care needs of community-residing male patients with vascular cognitive impairment. Neuropsychiatr. Dis. Treat. 16, 2613–2621. doi: 10.2147/NDT.S277303
Lin, Y. S., Wang, W. F., and Liu, Y. H. (2020). The study of care targets combination in women with Alzheimer's disease: a case study in a medical center in Taiwan. J. Qual. 27, 1–25. doi: 10.6220/joq.202002_27(1).0001
Liu, C. C., Li, C. Y., Sun, Y., and Hu, S. C. (2019). Gender and age differences and the trend in the incidence and prevalence of dementia and Alzheimer's disease in Taiwan: a 7-year national population-based study. Biomed. Res. Int. 2019, 5378540. doi: 10.1155/2019/5378540
Liu, L. F., Wang, W. M., and Chen, Y. J. (2018). The effectiveness of home services in Taiwan: a people-centered approach. Int. J. Environ. Res. Public Health. 15, 2605. doi: 10.3390/ijerph15112605
Livingston, G., Johnston, K., Katona, C., Paton, J., and Lyketsos, C. G. (2005). Systematic review of psychological approaches to the management of neuropsychiatric symptoms of dementia. Am. J. Psychiatry. 162, 1996–2021. doi: 10.1176/appi.ajp.162.11.1996
Lyketsos, C. G., Lopez, O., Jones, B., Fitzpatrick, A. L., Breitner, J., DeKosky, S., et al. (2002). Prevalence of neuropsychiatric symptoms in dementia and mild cognitive impairment: results from the cardiovascular health study. JAMA. 288, 1475–1483. doi: 10.1001/jama.288.12.1475
McLoughlin, B. (2022). Group-based interventions for carers of people with dementia: a systematic review. Innov. Aging. 6:igac011. doi: 10.1093/geroni/igac011
Ministry of Health Welfare (2022). Long-Term Care Service Application and Payment (in Chinese). Taiwan: Ministry of Health and Welfare. Available online at: https://1966.gov.tw/LTC/cp-4010-42524-201.html (accessed June 10, 2022).
Morris, J. C. (1997). Clinical dementia rating: a reliable and valid diagnostic and staging measure for dementia of the Alzheimer type. Int. Psychogeriatr. 9, 173–176. discussion 177–178. doi: 10.1017/S1041610297004870
Morrisby, C., Joosten, A., and Ciccarelli, M. (2018). Do services meet the needs of people with dementia and carers living in the community? A scoping review of the international literature. Int. Psychogeriatr. 30, 5–14. doi: 10.1017/S1041610217001491
Reckrey, J. M., Boerner, K., Franzosa, E., Bollens-Lund, E., and Ornstein, K. A. (2021). Paid caregivers in the community-based dementia care team: do family caregivers benefit? Clin Ther. 43, 930–941. doi: 10.1016/j.clinthera.2021.03.022
Shepherd-Banigan, M., James, H. J., Smith, V. A., Plassman, B. L., Jutkowitz, E., Belanger, E., et al. (2021). Drivers of long-term care considerations by persons with cognitive impairment. J. Appl. Gerontol. 40, 648-660. doi: 10.1177/0733464820903908
Tsai, C. F., Huang, M. H., Cheng, C. M., Lee, J. J., Wang, W. F., Huang, L. C., et al. (2022). Determinants of long-term care service use by persons with dementia: A national dementia registry study conducted in Taiwan. Int. J. Geriatr. Psychiatry. 37, 5719. doi: 10.1002/gps.5719
Van Cleve, R., and Degenholtz, H. B. (2022). Patterns of home and community based service use by beneficiaries enrolled in the Pennsylvania medicaid aging waiver. J. Appl. Gerontol. 2022, 7334648221094578. doi: 10.1177/07334648221094578
Wang, S., Yan, D., Temkin-Greener, H., and Cai, S. (2021). Nursing home admissions for persons with dementia: role of home- and community-based services, Health Serv Res. 56, 1168-1178. doi: 10.1111/1475-6773.13715
Wang, W. F., Su, Y. Y., and Jhang, K. M. (2021). Patterns of home- and community-based services in older adults with dementia: an analysis of the long-term care system in Taiwan. BMC Geriatr. 21, 290. doi: 10.1186/s12877-021-02231-9
Wu, C. Y., Hu, H. Y., Huang, N., Fang, Y. T., Chou, Y. J., and Li, C. P. (2014). Determinants of long-term care services among the elderly: a population-based study in Taiwan. Plos ONE. 9, e89213. doi: 10.1371/journal.pone.0089213
Wysocki, A., Butler, M., Kane, R. L., Kane, R. A., Shippee, T., Sainfort, F., et al. (2015). Long-term services and supports for older adults: a review of home and community-based services versus institutional care. J. Aging Soc. Policy. 27, 255–279. doi: 10.1080/08959420.2015.1024545
Yan, G. J., Wang, W. F., Jhang, K. M., Lin, C. W., and Wu, H. H. (2019). Association between patients with dementia and high caregiving burden for caregivers from a medical center in Taiwan. Psychol. Res. Behav Manag. 12, 55–65. doi: 10.2147/PRBM.S187676
Keywords: long-term care services, patients with dementia, caregivers, patient–caregiver dyad, Apriori algorithm, home personal care services, assistive devices
Citation: Chen Y-J, Jhang K-M, Wang W-F, Lin G-C, Yen S-W and Wu H-H (2022) Applying Apriori algorithm to explore long-term care services usage status—Variables based on the combination of patients with dementia and their caregivers. Front. Psychol. 13:1022860. doi: 10.3389/fpsyg.2022.1022860
Received: 19 August 2022; Accepted: 18 November 2022;
Published: 13 December 2022.
Edited by:
Hui Zeng, Xiangya School of Nursing, Central South University, ChinaReviewed by:
Felipe Soto-Pérez, University of Salamanca, SpainXianghua Xu, Hunan Cancer Hospital/The Affiliated Cancer Hospital of Xiangya School of Medicine, China
Copyright © 2022 Chen, Jhang, Wang, Lin, Yen and Wu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hsin-Hung Wu, aGh3dUBjYy5uY3VlLmVkdS50dw==
†These authors have contributed equally to this work and share first authorship