 Hui Yu
Hui Yu Shicun Xu
Shicun Xu Hui Li7
Hui Li7 Xiaofeng Wang
Xiaofeng Wang Yuanyuan Wang
Yuanyuan Wang
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol. , 17 November 2022
Sec. Health Psychology
Volume 13 - 2022 | https://doi.org/10.3389/fpsyg.2022.1012393
This article is part of the Research Topic Social Determinants of Psychological Illness and Well-Being Across the Life Course View all 9 articles
Introduction: The urban–rural household registration system in China has been documented with profound social consequences in almost all areas of people’s life. This study aims to investigate the underlying mechanism of the rural and urban discrepancies on mental health conditions among a large sample of college students in China.
Methods: A survey was distributed among college students in China. A total of 96,218 college students from 63 colleges completed the survey, answering questions on their urban–rural household registration, disposable household income, subjective social status, feelings of loneliness, and anxiety and depression symptoms. Confirmatory Factor Analysis (CFA) and Structural Equation Modelling (SEM) analyses were conducted, testing the effect of urban–rural registration on one’s mental health, mediated by subjective social status, and loneliness.
Results: Structural Equation Modelling (SEM) results revealed that the urban–rural household registration showed a direct effect on anxiety (B = −0.03, 95% CI [−0.038, −0.022], β = −0.03, p < 0.001) and depression (B = −0.03, 95% CI [−0.035, −0.023], β = −0.03, p < 0.001), indicating that rural household registration had a negative association with anxiety and depression symptoms, albeit the standardised estimate being very small. The indirect path from the urban–rural registration mediated through subjective social status and loneliness to anxiety and depression was both significant, with B = 0.01, 95% CI [0.010, 0.010], β = 0.01, p < 0.001, and B = 0.01, 95% CI [0.0090, 0.0090], β = 0.01, p < 0.001, respectively. The results of the indirect paths demonstrated that students of the rural household registration reported higher anxiety and depression symptoms through a lower subjective social status and higher level of loneliness.
Conclusion: This study indicated that decreasing the disparity of social status and tackling loneliness is the key to improve the overall mental health of college students. The urban–rural household registration system may have a very small direct effect on the college students’ mental health; but students of urban registration enjoyed higher subjective social status, which had a clear protective effect against anxiety and depression symptoms.
The discrepancies between life in urban and rural residents such as household income, access to healthcare infrastructure, physical and mental health, and other important areas in life are documented in many countries including the rich and industrialised ones. For example, according to the 2015 American Community Survey, it has been documented that the median household income for rural households was about 4% lower than the median for urban households in the United States (Bishaw and Posey, 2016). Another study based its analysis on the 2016 March Current Population Survey Public Use Microdata also confirmed that in 2015, 16.7% of the rural population was poor, in comparison to 13.0% of the urban population in the United States (Thiede et al., 2017). On the other hand, some other data suggested the rural as an idyllic place to live, with residents enjoying the beautiful landscapes and more neighbourhood communities, living a happier and healthier life than people living in the urban areas. For example, House et al. (2000) reported that city residents had a mortality hazard rate ratio of 1.62 relative to rural or small town residents, after adjusting for sociodemographic and health variables. It is clear that the urban–rural division is not straightforward, and the regional inequality must be accounted for by multifactorial reasons (McCann, 2020).
The psychological factor closely linked to reginal inequality, or the affluence level of the neighbourhood, is one’s perceived social status. The association between low subjective social status with an array of health problems have been documented, such as physical health (O'Leary et al., 2021), anxiety and depression (Singh-Manoux et al., 2003; Zvolensky et al., 2017). Adler (2009) explicitly claimed that health disparities between Socioeconomic Status (SES) categories could not be explained by poverty in addition to inadequate or lack of health care, but SES went under the skin and had a profound impact on one’s health – the question is how. Indeed, the exact mechanism linking one’s social status and health has not been clearly understood.
One possible pathway is through the feeling of loneliness, being left out and isolated from others (Hughes et al., 2004). Loneliness has been identified as one major risk factor for anxiety and depression (Cacioppo et al., 2006; Ebesutani et al., 2015), and many other health-risky behaviours including suicide attempts (Solmi et al., 2020). On the other hand, loneliness feeling is closely associated with social status: people from lower SES experienced disproportionally high level of loneliness (Domenech-Abella et al., 2017; Macdonald et al., 2018). In addition, subjective social status has shown to be associated with loneliness in the same direction and with similar effect as objectively measured SES (Rubin et al., 2016; Ayalon, 2019). Therefore, it demonstrates that one’s perceived social status is relatively accurate and can be used as a good indicator of one’s actual SES (Adler, 2009). Moreover, loneliness may be an important mediator linking social status and mental health outcomes.
In China, an arbitrary urban–rural household registration system, i.e., HuKou system, has been established since 1955, which gives the urban registrants entitlement in better education, housing, jobs, and health care than rural registrants (Wu and Treiman, 2004). The gaps between life of urban and rural registrants have been consistently documented, with urban registrants having higher education attainment and earning more money (China Statistical Yearbook, 2019), reporting better health (Chen et al., 2017), using more health care services (Li et al., 2018), and more. In particular, success in obtaining degrees in the Higher Education sector are crutial for an individuals’ life chances and social position (Hung, 2022). However, due to various cultural and socioenvironmental reasons, treatment and care for people with mental health need have been long under-served (Xu et al., 2018). Only in 2009, severe mental illnesses were incorporated into the national public health service programme (Xu et al., 2014). As a result, not many research has studied the discrepancies of the mental health status between people with urban and rural household registration and their underlying mechanism. The few available studies mainly documented that the prevalence of depression was higher among elderlies of rural than urban registrants (Zhang et al., 2012). However, not much information is available on the urban–rural mental health status of young adults studying at universities.
The present study is the first that aims to examine the effect of urban–rural registration and subjective social status on anxiety and depression symptoms, mediated through feeling of loneliness among university students in China. It is hypothesised that: (1) the urban–rural household registration would have both direct effect and indirect effects through subjective social status and loneliness, on anxiety and depression; and (2) subjective social status would have both direct effect and indirect effect through loneliness, on anxiety and depression.
Data of this study was part of a cross-sectional survey collected from university students in Jilin Province, China. All students from all the 63 colleges in Jilin Province were invited to the survey; and they were sent the information of the study and a Quick Response (QR) code. Students could quickly go to the survey link from the QR code if they decided to participate. In total, 96,218 students completed and returned the survey between October to November 2021, of which 40,065 were males (41.64%) and 56,153 females (58.36%). In addition, 48,932 (50.86%) of the students were of urban household registration, while 47,286 (49.14%) students were of rural household registration. The mean age of the sample was 19.59 (SD = 1.74). The other demographic characters of the sample were summarised in Table 1.
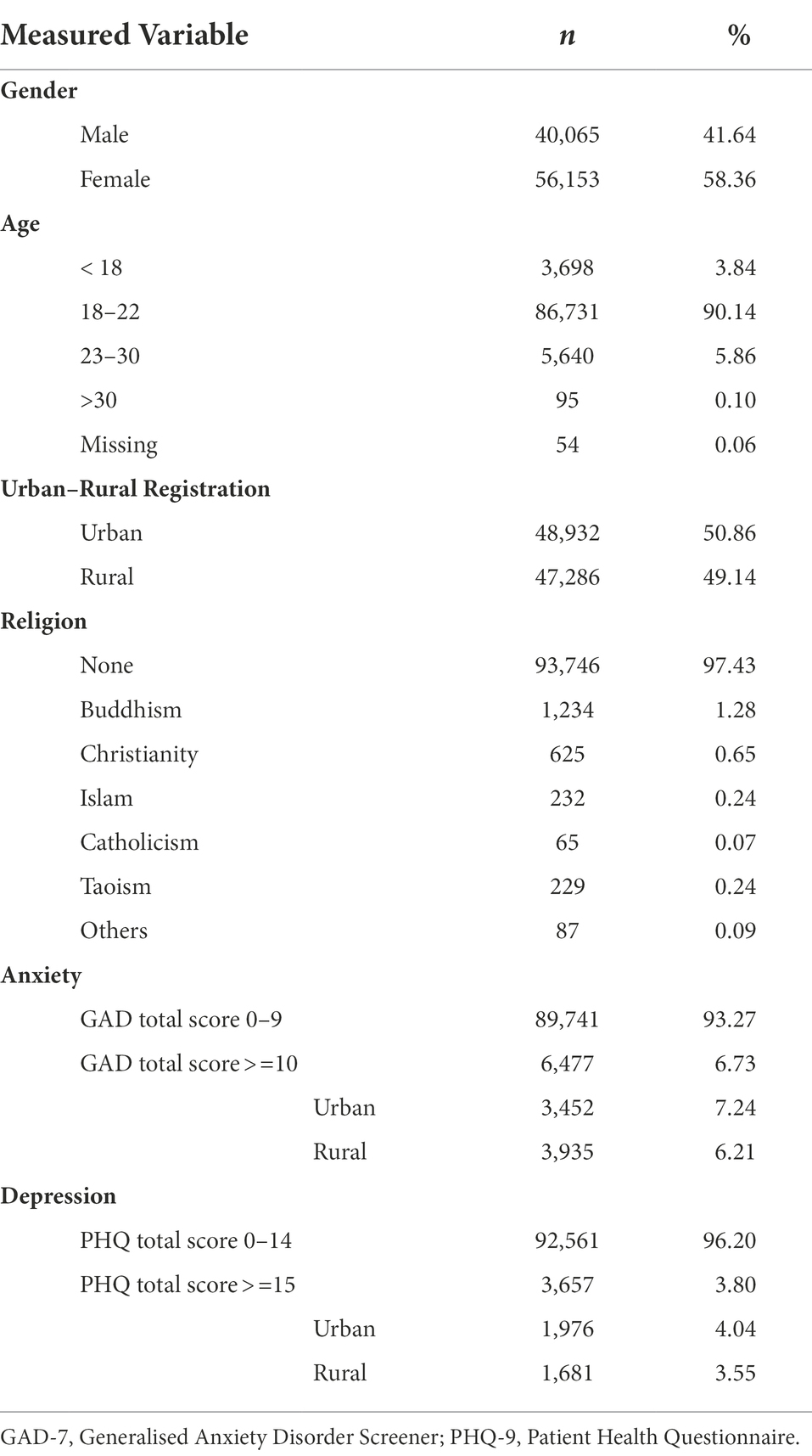
Table 1. Summary of demographic characteristics of the sample.
All subjects gave their informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of Jilin University (Project identification code: 2021-9-29).
Participants were asked to indicate their household registration being either urban or rural with one question.
Participants were presented with a picture of a 10-rung ladder, and asked to rate where they stand in the Chinese society, with higher rungs indicating higher subjective social status (Singh-Manoux et al., 2003).
The Short Scale for Measuring Loneliness (Hughes et al., 2004) was used to measure the participants reported level of loneliness. There were 3 items and they measure how one feels they lack companionship, are left out or isolated from others. The rating was on a 1–3 scale, with 1 = hardly ever, 2 = some of the time, and 3 = often. The total score of loneliness was calculated, ranging from 3 to 9, with a higher score indicating a higher level of perceived loneliness. The internal consistency of the scale was good, with Cronbach’s alpha being 0.82.
The Generalised Anxiety Disorder Screener (GAD-7) (Löwe et al., 2008) was used to measure the participants’ anxiety symptoms. There were 7 items; participants were asked to rate on each symptom on a 0–3 scale based on their experiences during the past 2 weeks, where 0 = not at all, 1 = several days, 2 = more than half of the days, and 3 = nearly every day. The total score of GAD-7 was calculated, ranging from 0 to 21, with a higher score indicating more severe anxiety symptoms. The Cronbach’s alpha was 0.92 in this sample. In Table 1, a cut-off score of > = 10 was used to indicate self-reported moderate or severe level of anxiety symptoms, based on the validation of GAD-7 in a general population (Löwe et al., 2008).
The Patient Health Questionnaire (PHQ-9) (Kroenke et al., 2001) was used to measure the participants’ depression symptoms. There were 9 items, and similar to the GAD-7, participants were asked to rate on a 0–3 scale based on their experiences during the past 2 weeks. The total score of PHQ-9 was calculated, ranging from 0 to 27, with a higher score indicating more severe depression symptoms. The Cronbach’s alpha was 0.89 in this sample. In Table 1, a cut-off score of > = 15 was used to indicate self-reported moderately severer to severe level of depression symptoms, based on the validation of PHQ-9 in a general population (Kroenke et al., 2001).
Participants were asked to indicate the disposable income per family member per year on a 1–6 scale, where 1 = less than 6,000 RMB, 2 = 6,000–14,000 RMB, 3 = 14,000–23,000 RMB, 4 = 23,000-36,000, 5 = 36,000–70,000 RMB, and 6 = more than 70,000 RMB. This scale was adopted from China Statistical Yearbook (2019).
All analyses were carried out using R version 4.0.3 for Mac. The Confirmatory Factor Analysis (CFA) and the Structural Equation Modelling (SEM) analysis were conducted using the Lavaan package for R (Rosseel, 2012). The dataset was randomly divided into a development and holdout sample (also known as a training and testing sample), with 20% of the original dataset (N = 19,244) used for the CFA measurement model fitting, while the other 80% of the original dataset (N = 76,974) used for the SEM model testing. This procedure is to reduce the risk of over-fitting the model using the same dataset. Model fit indexes including the Comparative Fit Index (CFI), the Tucker-Lewis Index (TLI), and the Root Mean Square Error of Approximation (RMSEA) were used to assess the goodness of the model fit. It is commonly considered that a CFI/TLI higher than 0.95, and a RMSEA smaller than 0.05, indicate a good model fit. As the sample size is so large, only p < 0.001 was considered statistically significant in this study.
The sample is consisting of 96,218 university students, among which 50.86% are from urban household and 49.14% from rural household. The means and SDs of the study variables by urban–rural registration were summarised in Table 2. In addition, Welch two sample t-tests were conducted to test whether there was a significant difference between the urban and rural groups on the study variables. Results showed that students of urban household registration reported a significantly higher disposable income than those of rural registration, t(93243) = 81.60, p < 0.001, and the effect size was moderate, with Cohen’s d = 0.50. Students of urban household registration also reported a moderate effect sized higher subjective social status than students of rural registration, t(96130) = 71.45, p < 0.001, Cohen’s d = 0.45. The t-test result also showed that students of urban registration reported lower loneliness than students of rural registration, t(9611) = −4.15, p < 0.001; however, the effect size was negligible, with Cohen’s d = 0.02. The students of urban and rural household registration reported similar level of anxiety and depression symptoms, measured by GAD-7 and PHQ-9 total scores, respectively. Although it must be pointed out that Chi-squre tests revealed a significantly higher percentage among urban students than rural students scoring on the high end of the anxiety (GAD > = 10) and depression (PHQ > = 15) scales (see Table 1), χ2 (df = 1) = 40.77, p < 0.001, and χ2 (df = 1) = 15.36, p < 0.001, for anxiety and depression symptoms, respectively.
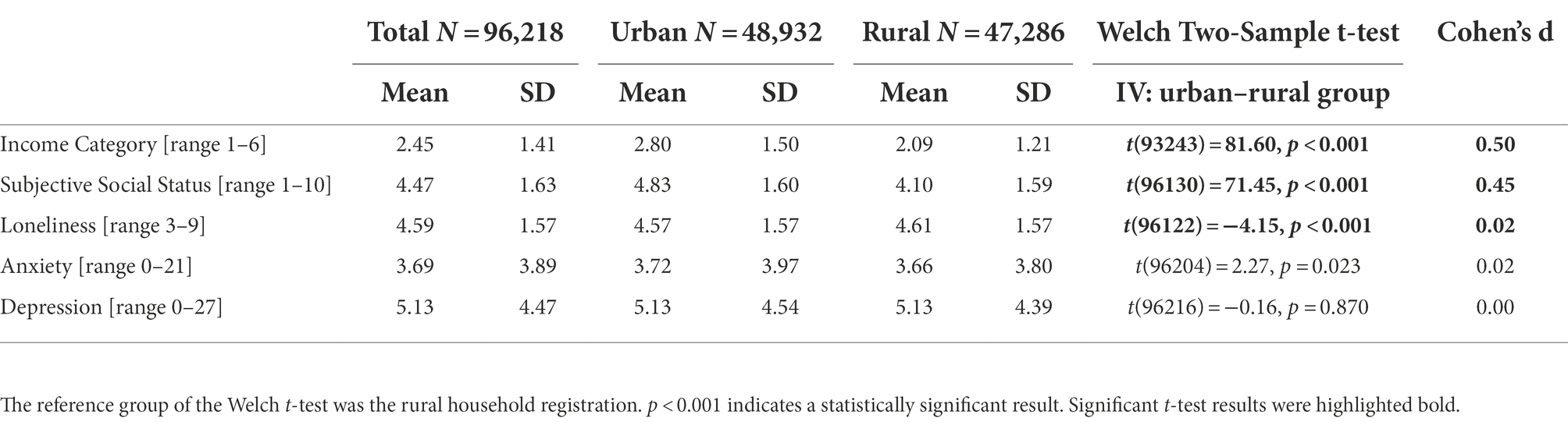
Table 2. Means and SDs of the study variables by urban–rural registration.
A CFA model of loneliness, anxiety, and depression measured by the Short Scale for Measuring Loneliness, GAD-7, and PHQ-9 was first established by the training sample, consisting of 20% of the original dataset. The model fit indices indicated an adequate fit, with CFI = 0.996, TLI = 0.995, and RMSEA = 0.021. The standardised factor loading estimates ranged from 0.56 to 0.83, and all the measured items significantly loaded to their latent construct, with p < 0.001. The details of the path estimates were summarised in Table 3 and Figure 1.
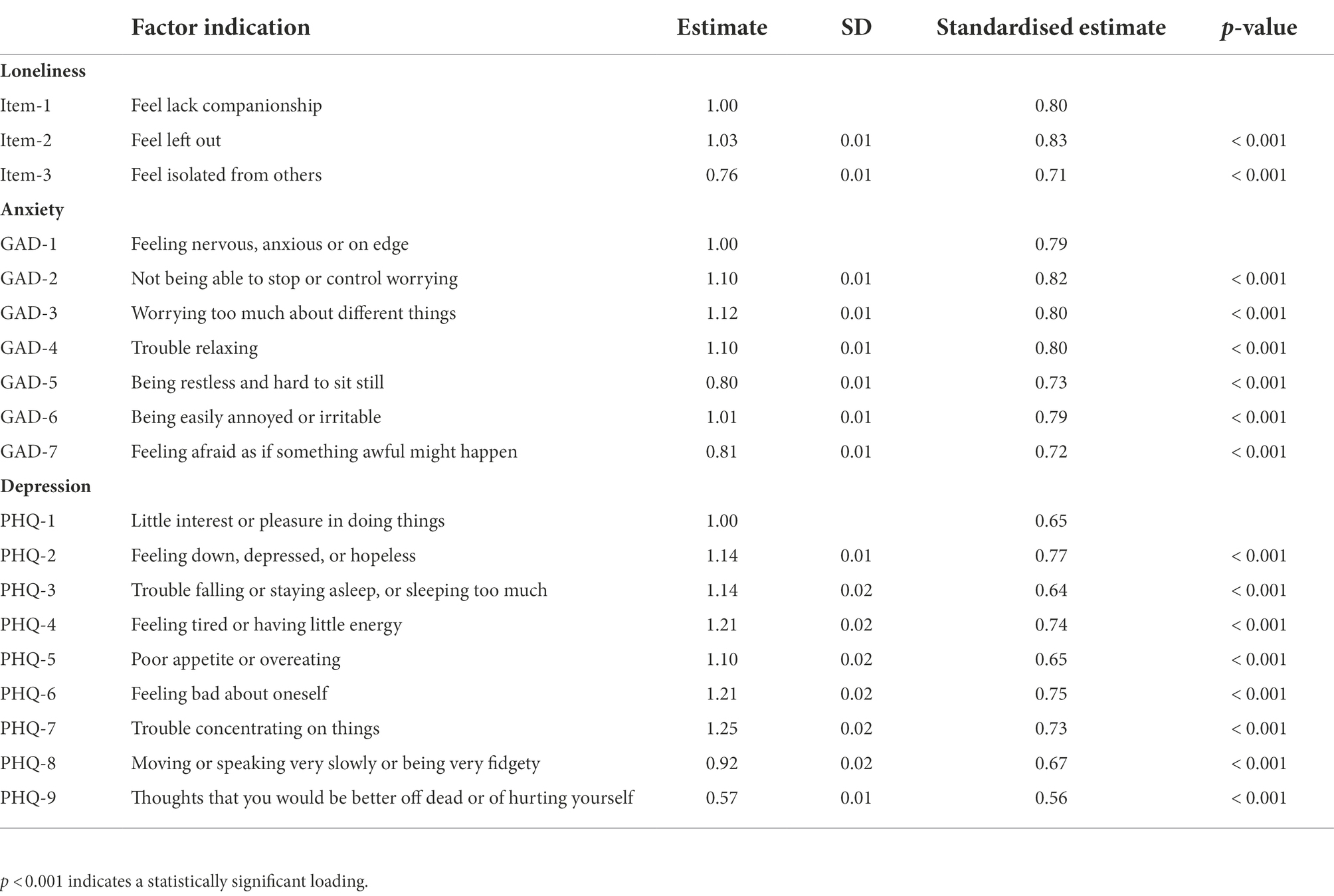
Table 3. CFA measurement model of loneliness, anxiety, and depression.
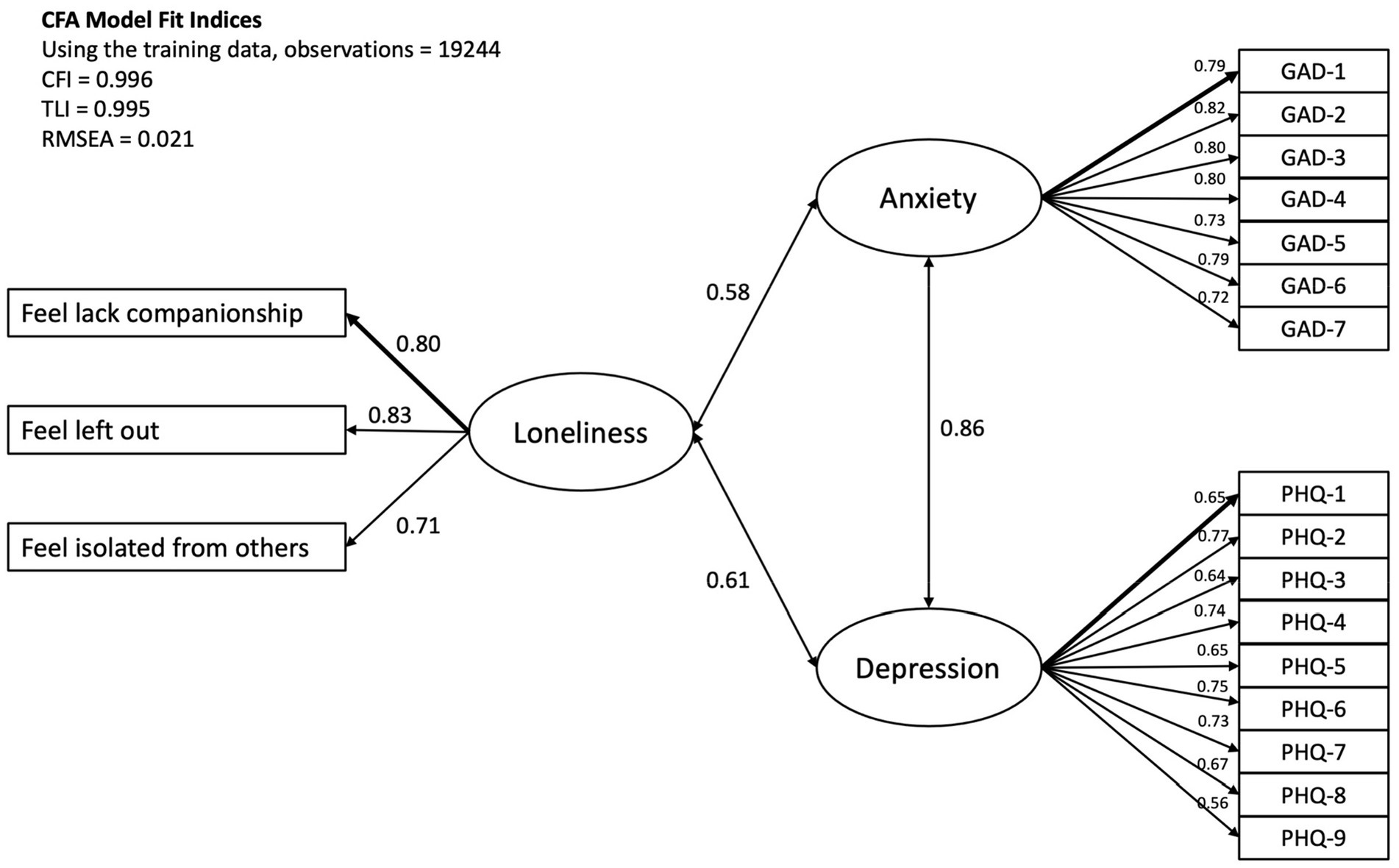
Figure 1. The CFA measurement model of loneliness, anxiety, and depression. The standardised loading estimates were shown in the figure, and all paths were significant with p < 0.001.
An SEM model testing the urban–rural registration predicting anxiety and depression, mediated by perceived social status and loneliness and with sex and income as covariates was conducted by the testing sample, consisting of 80% of the original dataset. The model fit indices indicated an adequate fit, with CFI = 0.995, TLI = 0.995, and RMSEA = 0.020. The analysis revealed that the urban–rural household registration showed a direct effect on anxiety (B = -0.03, 95% CI [−0.038, −0.022], β = −0.03, p < 0.001) and depression (B = −0.03, 95% CI [−0.035, −0.023], β = −0.03, p < 0.001), indicating that rural household registration was negatively associated with anxiety and depression symptoms, albeit the standardised estimate being very small. On the other hand, students of rural household registration reported a significantly lower subjective social status than those of urban registration (B = −0.41, 95% CI [−0.42, −0.38], β = −0.12, p < 0.001), while subjective social status had a protective effect against anxiety (B = −0.02, 95% CI [−0.023, −0.019], β = −0.06, p < 0.001) and depression (B = −0.03, 95% CI [−0.030, −0.026], β = −0.10, p < 0.001). Subjective social status had a negative effect on loneliness (B = −0.04, 95% CI [−0.043, −0.039], β = −0.13, p < 0.001), meaning the higher the subjective social status, the lower level of reported loneliness; while loneliness was positively associated with anxiety (B = 0.61, 95% CI [0.60, 0.62], β = 0.58, p < 0.001) and depression (B = 0.53, 95% CI [0.52, 0.54], β = 0.61, p < 0.001).
Sex and income were used as covariates in the model. Sex was significantly associated with all predicting, mediating and outcome variables, with females reporting a higher subjective social status (B = 0.27, 95% CI [0.24, 0.29], β = 0.08, p < 0.001), greater loneliness (B = 0.04, 95% CI [0.031, 0.047], β = 0.04, p < 0.001), greater anxiety (B = 0.05, 95% CI [0.045, 0.061], β = 0.05, p < 0.001) and depression symptoms (B = 0.03, 95% CI [0.019, 0.031], β = 0.03, p < 0.001) than males. Income was also significantly associated with higher subjective social status (B = 0.45, 95% CI [0.44, 0.45], β = 0.38, p < 0.001), greater anxiety (B = 0.01, 95% CI [0.010, 0.014], β = 0.03, p < 0.001), and depression (B = 0.01, 95% CI [0.0060, 0.010], β = 0.03, p < 0.001) symptoms.
The indirect paths from the urban–rural registration mediated through subjective social status and loneliness to anxiety and depression were both significant, with B = 0.01, 95% CI [0.010, 0.010], β = 0.01, p < 0.001, and B = 0.01, 95% CI [0.0090, 0.0090], β = 0.01, p < 0.001, respectively. The results of the indirect paths demonstrated that students of the rural household registration reported higher anxiety and depression symptoms through a lower subjective social status and higher level of loneliness. The total effect of urban–rural household registration on anxiety and depression (B = −0.02, 95% CI [−0.028, −0.012], β = −0.02, p < 0.001, and B = −0.02, 95% CI [−0.029, −0.013], β = −0.02, p < 0.001 respectively), however, indicated that rural registration was negatively associated with mental health conditions.
The indirect paths from the subjective social status to anxiety and depression through loneliness were also significant, with B = −0.02, 95% CI [−0.027, −0.023], β = −0.07, p < 0.001, and B = −0.02, 95% CI [−0.024, −0.020], β = −0.08, p < 0.001, respectively. The indirect paths demonstrated that students with higher subjective social status reported lower anxiety and depression through feeling lower level of loneliness. The total effect of subjective social status on anxiety and depression (B = −0.04, 95% CI [−0.046, −0.042], β = −0.13, p < 0.001, and B = −0.05, 95% CI [−0.050, −0.046], β = −0.18, p < 0.001 respectively) also indicated that subjective social status had an overall protective effect against mental health conditions. The details of the path estimates were summarised in Table 4 and Figure 2.
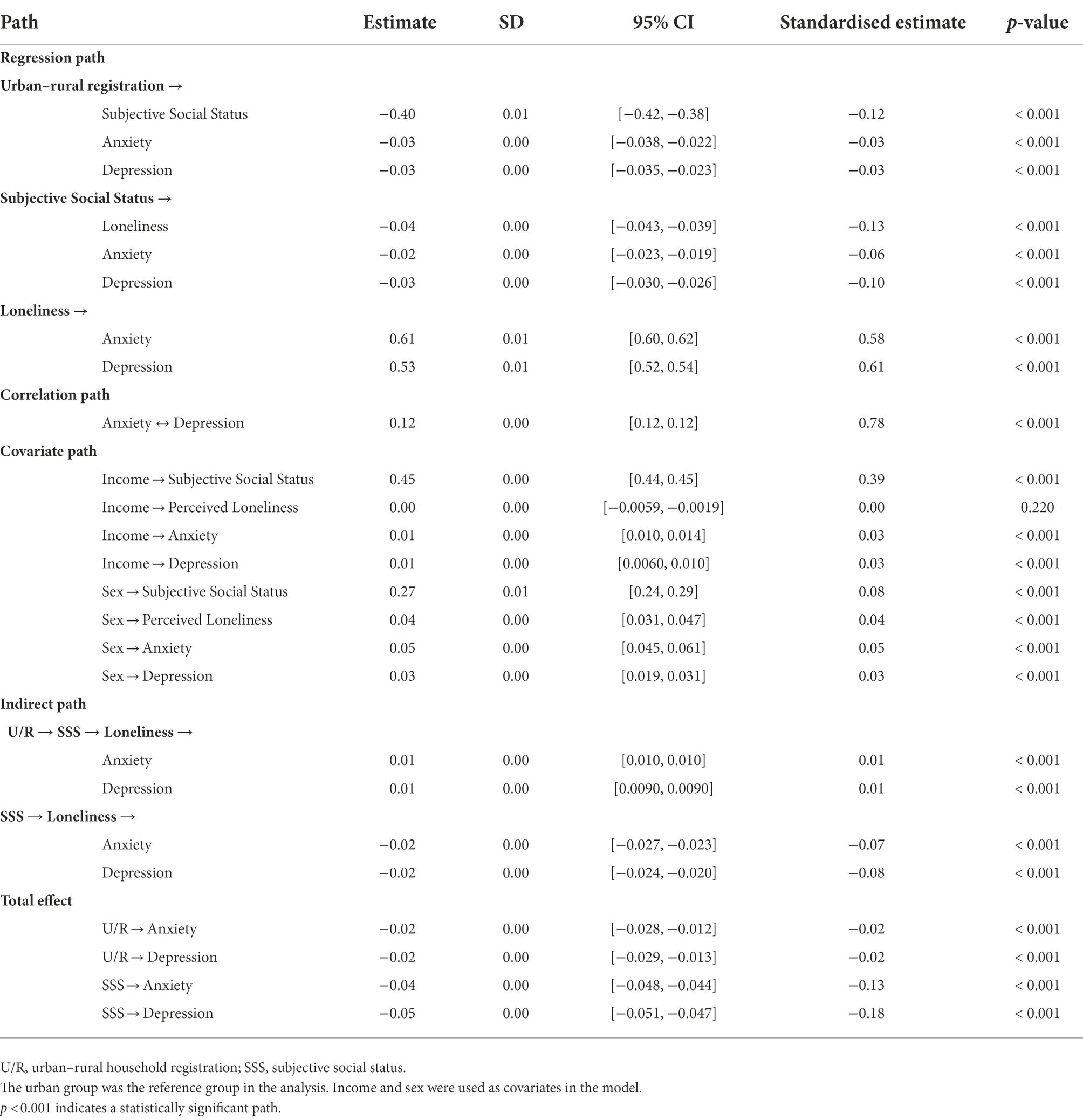
Table 4. SEM testing model: Urban–rural registration predicting anxiety and depression, mediated by subjective social status and loneliness.
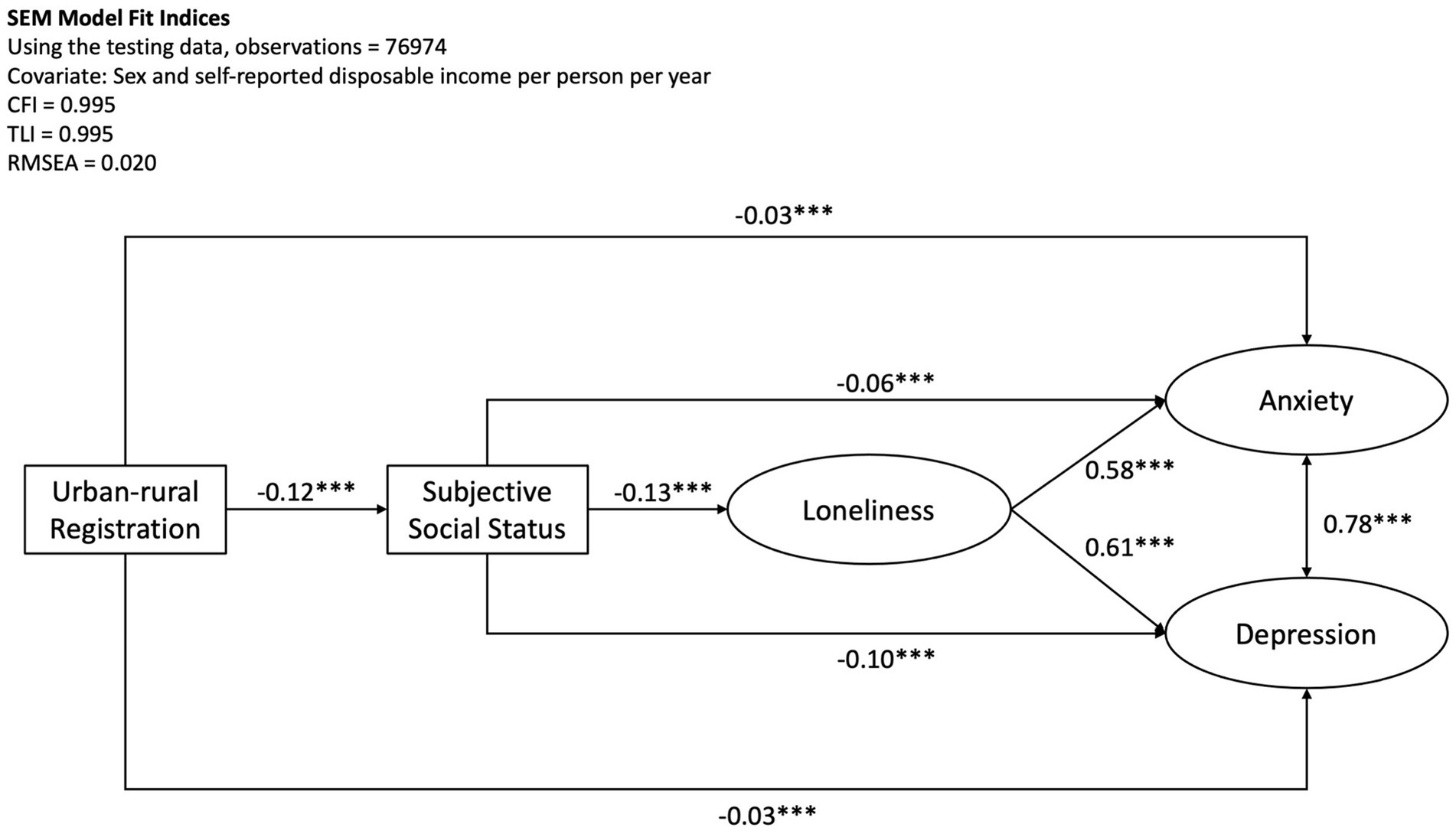
Figure 2. SEM model testing urban–rural registration predicting anxiety and depression mediated by subjective social status and loneliness. The standardised path estimates were shown in the figure, and all paths were significant with p < 0.001. Sex and self-reported disposable income were covariates in the model.
The results of SEM analysis supported both hypotheses: (1) the urban–rural household registration had a significant direct effect and indirect effect through subjective social status and loneliness on anxiety and depression symptoms; and (2) subjective social status had a significant direct effect and indirect effect through loneliness on anxiety and depression symptoms.
It was curious that the rural registration showed a positive association to anxiety and depression through lower subjective social status and higher self-reported loneliness path; and the rural registration also showed a negative association to anxiety and depression through the direct path, which resulted in an overall negative association between the rural registration and mental health conditions. This was surprising and in contrast to the commonly perceived image of the urban–rural discrepancies in China, which almost always indicated that people of urban registration would be better-off than those of rural registration in all documented areas (Wu and Treiman, 2004; Zhang et al., 2012; Xu et al., 2018). HuKou system posts strict restrictions of people’s access to education, health care, insurance, and even purchasing houses in an area that is other than the registered location (Xu et al., 2014). As the migration route within China is almost exclusively from rural to cities, this restriction mainly disfavours people with rural household registration. Therefore, unlike in the Western countries, where within-country movement is free, the Chinese urban–rural disparities were mostly viewed as unequivocally advantageous to urban registrants.
However, the result of this study seemed to be contradicting this common understanding by showing a positive effect of rural registration against mental health conditions. The result, however, must be put into perspective. Firstly, the simple two-sample t-test indicated that there was no significant difference between students of urban and registration on reported anxiety and depression symptoms. Secondly, when the relevant psychological factors were put into the model, the urban–rural registration showed significant effect on anxiety and depression symptoms. However, the standardised path coefficients for the direct effect and total effect of urban–rural registration on anxiety and depression were very small in scale. Lastly, the sample of this study mainly comprised of university students who were full of hopes and did not have much life experience yet. Therefore, those young adults of rural registration might not have had encountered real life challenges due to HuKou restriction yet, such as finding a job, buying a house etc. Treiman (2012) showed that the group of people of rural registration living in the cities occupied less nonmanual jobs, earned less money, possessed fewer amenities in their household than people of urban registration. It has also been documented that people with rural HuKou but lived in the cities reported higher depression symptoms than those who had urban HuKou (Song and Smith, 2019). It might be a matter of time for the gap in the “predicted direction” to appear when people of rural registration reported higher level of stress.
On the other hand, the positive effect of green spaces on one’s mental health has been firmly confirmed by research and incorporated into urban design (Brown et al., 2018). Our result might be useful to indicate that majority of students of rural registration still benefit from the closeness to nature at a young age. In particular, our data documented that urban students were more likely than rural students to score on the high end of the anxiety and depression scales. There was also evidence to show that elderly rural residents had high level of community support and reported relatively good health (Xu et al., 2021). In addition, there has been increasing evidence that the gap between life in rural and urban areas has been decreasing (Treiman, 2012; Zhang and Treiman, 2013). The current policy changes also helped to change people’s attitude to the value of rural HuKou by giving the rural residence some exclusive benefits (Chen and Fan, 2016). Although the institutional barrier of the HuKou system to restrict people of the rural registration from upward social mobility has been great, there is hope that tertiary education might help the hopeful young adults to pursue a desirable life wherever they choose with freedom.
Regarding the effect of subjective social status on anxiety and depression, the result of this study supported existing literature that higher social status predicted a lower level of loneliness and therefore, was association with lower anxiety and depression symptoms. It has been well documented that loneliness is unequal among the population with different SES background, with lower SES associated to higher perceived loneliness (Qualter et al., 2021). In our sample, in comparison to the better-off peers, the young students from poorer families might feel it more difficult to make firends when there are financial concerns: for example, they may be more reluctant to go out with their peers for social events. Although in the oriental context, the alarmingly high prevalence of loneliness and their underlying mechnism have not been fully understood, it was reported to be associated with and moderated by level of income (Badman et al., 2022). The result of our model clearly indicated a link between low subjective social status and greater feelings of loneliness.
Martín-María et al. (2021) showed that phone call programs tackling loneliness feeling could significantly reduce one’s reported anxiety and depression symptoms. Social prescribing by clinical professionals as a means to combact loneliness in the modern society by linking individuals to the local non-clinical providers in the community has become more common in many Western societies (Liebmann et al., 2022). The result from the current study also showed that loneliness was positively associated with anxiety and depression with significant path coefficients, adding to the ever growing literature that loneliness plays an important role in mental health conditions (Erzen and Çikrikci, 2018; Wilkialis et al., 2021). In addition, higher subjective social status also had a direct protective effect against anxiety and depression. In particular, as students of the rural HuKou reported a significantly lower subjective social status, the indirect effect from the urban–rural registration through subjective social status and loneliness proved disadvantageous to those with rural HuKou. Song and Smith (2019) showed that people with rural registration endured the highest level of hardships and adversities throughout life; those who had converted their rural registration to urban registration and lived in cities had better income and fewer hardships than those who continued living in the rural areas, but were disadvantaged in a variety of health measures than those who were born with urban registration. Importantly, the cited study showed that these differences could be mainly accounted for by differences in socioeconomic status. The result of our study added new evidence to linking the urban–rural division as well as subjective social status to mental health outcomes.
In the model, sex and income were uses as covariates. Results indicated that both covariates were important in the model with most path coefficients being significant and in the predicted directions. In particular, females reported significantly higher subjective social status, greater feeling of loneliness, greater anxiety and depression symptoms. These results were in line with a great amount of literature documenting the gender difference of loneliness (Rokach, 2018) and mental health (Hallers-Haalboom et al., 2020; Hyde and Mezulis, 2020), but the reported higher subjective social status may need some explanation. The income gap favouring males over females has been firmly established in all studies areas, and China is no exception. However, there has been a tradition of materially pampering daughters more than sons in some areas of China (Kim et al., 2018), which might have lead to the observed positive association that females reported higher subjective social status than males. Conversely, this may also be the simple result that females inflated their social status more than males in this context (Kennedy and Kray, 2022). The mechanism behind this observation is beyond this study’s scope, but this result would lead to interesting future research examining the gender similarities and differences in the association between real income, subjective social status and mental health conditions.
The major limitation of this study is that it is a cross-sectional study using a group of young adults who are still studying in universities. As discussed, it is of vital importance to understand whether over time, these bunch of hopeful young adults would experience higher level of mental health conditions, and to what extent, the arbitrary urban–rural household registration system would inhibit the rural registrants from getting the life they wish to realise. A longitudinal follow-up study in different stages of their lives would be most powerful to answer the above-mentioned questions. However, this study provides an important puzzle piece that contributes significantly to understand the whole picture of the health disparities in Chinese society.
In conclusion, this study clearly demonstrated the complexity of the effect of urban–rural household registration on mental health in China. However, it was straightforward that decreasing the disparity of social status is the key to improve the overall mental health of university students. In addition, loneliness is an important pathway linking social status and mental health. Intervention programs tackling loneliness would yield positive results in decreasing anxiety and depression.
The raw data supporting the conclusions of this article will be made available by the corresponding authors on reasonable request.
The studies involving human participants were reviewed and approved by Jilin University. The patients/participants provided their written informed consent to participate in this study.
HY, YW, and SX were responsible for the conception, organisation, and execution of the study and manuscript revision. SX, XW, QS, and HL were responsible for the data collection. HY was responsible for the statistical analysis and verification of the underlying data. HY and YW were responsible for the manuscript preparation. All authors had full access to all the data in the study and confirmed their responsibility for the decision to submit it for publication.
This study was founded by the National Natural Science Foundation of China (NSFC) Grant number 82201708.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Adler, N. E. (2009). Health disparities through a psychological lens. Am. Psychol. 64, 663–673. doi: 10.1037/0003-066X.64.8.663
Ayalon, L. (2019). Subjective social status as a predictor of loneliness: the moderating effect of the type of long-term care setting. Res. Aging 41, 915–935. doi: 10.1177/0164027519871674
Badman, R. P., Nordström, R., Ueda, M., and Akaishi, R. (2022). Perceptions of social rigidity predict loneliness across the Japanese population. Sci. Rep. 12, 16073–16014. doi: 10.1038/s41598-022-20561-5
Bishaw, A., and Posey, K. G. (2016). A Comparison of Rural and Urban America: Household Income and Poverty ; Washington: US Census Bureau.
Brown, S. C., Perrino, T., Lombard, J., Wang, K., Toro, M., Rundek, T., et al. (2018). Health disparities in the relationship of neighborhood greenness to mental health outcomes in 249,405 US Medicare beneficiaries. Int. J. Environ. Res. Public Health 15:430. doi: 10.3390/ijerph15030430
Cacioppo, J. T., Hughes, M. E., Waite, L. J., Hawkley, L. C., and Thisted, R. A. (2006). Loneliness as a specific risk factor for depressive symptoms: cross-sectional and longitudinal analyses. Psychol. Aging 21, 140–151. doi: 10.1037/0882-7974.21.1.140
Chen, C., and Fan, C. C. (2016). China's Hukou puzzle: why don't rural migrants want urban hukou? China Rev. 16, 9–39.
Chen, H., Liu, Y., Zhu, Z., and Li, Z. (2017). Does where you live matter to your health? Investigating factors that influence the self-rated health of urban and rural Chinese residents: evidence drawn from Chinese general social survey data. Health Qual. Life Outcomes 15, 1–11. doi: 10.1186/s12955-017-0658-0
China Statistical Yearbook (2019). Available at: http://www.stats.gov.cn/tjsj/ndsj/2019/indexch.htm (Accessed March 2022).
Domenech-Abella, J., Mundó, J., Lara, E., Moneta, M. V., Haro, J. M., and Olaya, B. (2017). The role of socio-economic status and neighborhood social capital on loneliness among older adults: evidence from the Sant Boi aging study. Soc. Psychiatry Psychiatr. Epidemiol. 52, 1237–1246. doi: 10.1007/s00127-017-1406-9
Ebesutani, C., Fierstein, M., Viana, A. G., Trent, L., Young, J., and Sprung, M. (2015). The role of loneliness in the relationship between anxiety and depression in clinical and school-based youth. Psychol. Sch. 52, 223–234. doi: 10.1002/pits.21818
Erzen, E., and Çikrikci, Ö. (2018). The effect of loneliness on depression: a meta-analysis. Int. J. Soc. Psychiatry 64, 427–435. doi: 10.1177/0020764018776349
Hallers-Haalboom, E. T., Maas, J., Kunst, L. E., and Bekker, M. H. (2020). The role of sex and gender in anxiety disorders: being scared “like a girl”? Handb. Clin. Neurol. 175, 359–368. doi: 10.1016/B978-0-444-64123-6.00024-2
House, J. S., Lepkowski, J. M., Williams, D. R., Mero, R. P., Lantz, P. M., Robert, S. A., et al. (2000). Excess mortality among urban residents: how much, for whom, and why? Am. J. Public Health 90, 1898–1904.
Hughes, M. E., Waite, L. J., Hawkley, L. C., and Cacioppo, J. T. (2004). A short scale for measuring loneliness in large surveys: results from two population-based studies. Res. Aging 26, 655–672. doi: 10.1177/0164027504268574
Hung, J. (2022). Hukou system influencing the structural, institutional inequalities in China: the multifaceted disadvantages rural Hukou holders face. Soc. Sci. 11:194. doi: 10.3390/socsci11050194
Hyde, J. S., and Mezulis, A. H. (2020). Gender differences in depression: biological, affective, cognitive, and sociocultural factors. Harv. Rev. Psychiatry 28, 4–13. doi: 10.1097/HRP.0000000000000230
Kennedy, J. A., and Kray, L. J. (2022). Gender similarities and differences in dishonesty. Current opinion. Psychology 48:101461. doi: 10.1016/j.copsyc.2022.101461
Kim, S. W., Brown, K.-E., and Fong, V. L. (2018). How flexible gender identities give young women advantages in China’s new economy. Gend. Educ. 30, 982–1000. doi: 10.1080/09540253.2016.1274380
Kroenke, K., Spitzer, R. L., and Williams, J. B. (2001). The PHQ-9: validity of a brief depression severity measure. J. Gen. Intern. Med. 16, 606–613. doi: 10.1046/j.1525-1497.2001.016009606.x
Li, J., Shi, L., Liang, H., Ding, G., and Xu, L. (2018). Urban-rural disparities in health care utilization among Chinese adults from 1993 to 2011. BMC Health Serv. Res. 18, 1–9. doi: 10.1186/s12913-018-2905-4
Liebmann, M., Pitman, A., Hsueh, Y.-C., Bertotti, M., and Pearce, E. (2022). Do People perceive Benefits in the use of social prescribing to address loneliness and/or social Isolation? A qualitative meta-synthesis of the literature. BMC health services research 22, 1–29.
Löwe, B., Decker, O., Müller, S., Brähler, E., Schellberg, D., Herzog, W., et al. (2008). Validation and standardization of the generalized anxiety disorder screener (GAD-7) in the general population. Med. Care 46, 266–274. doi: 10.1097/MLR.0b013e318160d093
Macdonald, S. J., Nixon, J., and Deacon, L. (2018). ‘Loneliness in the city’: examining socio-economics, loneliness and poor health in the north east of England. Public Health 165, 88–94. doi: 10.1016/j.puhe.2018.09.003
Martín-María, N., Caballero, F. F., Lara, E., Domènech-Abella, J., Haro, J. M., Olaya, B., et al. (2021). Effects of transient and chronic loneliness on major depression in older adults: a longitudinal study. Int. J. Geriatr. Psychiatry 36, 76–85. doi: 10.1002/gps.5397
McCann, P. (2020). Perceptions of regional inequality and the geography of discontent: insights from the UK. Reg. Stud. 54, 256–267. doi: 10.1080/00343404.2019.1619928
O'Leary, D., Uysal, A., Rehkopf, D. H., and Gross, J. J. (2021). Subjective social status and physical health: the role of negative affect and reappraisal. Soc. Sci. Med. 291:114272. doi: 10.1016/j.socscimed.2021.114272
Qualter, P., Hennessey, A., Yang, K., Chester, K. L., Klemera, E., and Brooks, F. (2021). Prevalence and social inequality in youth loneliness in the UK. Int. J. Environ. Res. Public Health 18:10420. doi: 10.3390/ijerph181910420
Rokach, A. (2018). The effect of gender and culture on loneliness: a mini review. Emerg. Sci. J. 2, 59–64. doi: 10.28991/esj-2018-01128
Rosseel, Y. (2012). Lavaan: an R package for structural equation modeling and more. Version 0.5–12 (BETA). J. Stat. Softw. 48, 1–36.
Rubin, M., Evans, O., and Wilkinson, R. B. (2016). A longitudinal study of the relations among university students' subjective social status, social contact with university friends, and mental health and well-being. J. Soc. Clin. Psychol. 35, 722–737. doi: 10.1521/jscp.2016.35.9.722
Singh-Manoux, A., Adler, N. E., and Marmot, M. G. (2003). Subjective social status: its determinants and its association with measures of ill-health in the Whitehall II study. Soc. Sci. Med. 56, 1321–1333. doi: 10.1016/S0277-9536(02)00131-4
Solmi, M., Veronese, N., Galvano, D., Favaro, A., Ostinelli, E. G., Noventa, V., et al. (2020). Factors associated with loneliness: an umbrella review of observational studies. J. Affect. Disord. 271, 131–138. doi: 10.1016/j.jad.2020.03.075
Song, Q., and Smith, J. P. (2019). Hukou system, mechanisms, and health stratification across the life course in rural and urban China. Health Place 58:102150. doi: 10.1016/j.healthplace.2019.102150
Thiede, B., Greiman, L., Weiler, S., Beda, S., and Conroy, T. (2017). Charts that illustrate the divide between rural and urban America. PBS NewsHour: The Rundown. Available at: https://www.pbs.org/newshour/nation/six-charts-illustrate-divide-rural-urban-america (Accessed March 2022).
Treiman, D. J. (2012). The “difference between heaven and earth”: urban–rural disparities in well-being in China. Res. Soc. Stratification Mobil. 30, 33–47. doi: 10.1016/j.rssm.2011.10.001
Wilkialis, L., Rodrigues, N. B., Cha, D. S., Siegel, A., Majeed, A., Lui, L. M., et al. (2021). Social isolation, loneliness and generalized anxiety: implications and associations during the COVID-19 quarantine. Brain Sci. 11:1620. doi: 10.3390/brainsci11121620
Wu, X., and Treiman, D. J. (2004). The household registration system and social stratification in China: 1955–1996. Demography 41, 363–384. doi: 10.1353/dem.2004.0010
Xu, J., Wang, J., King, M., Liu, R., Yu, F., Xing, J., et al. (2018). Rural–urban disparities in the utilization of mental health inpatient services in China: the role of health insurance. Int. J. Health Econ. Manag. 18, 377–393. doi: 10.1007/s10754-018-9238-z
Xu, J., Wang, J., Liu, R., Xing, J., Su, L., Yu, F., et al. (2014). Mental health inpatient treatment expenditure trends in China, 2005-2012: evidence from Shandong. J. Ment. Health Policy Econ. 17, 173–182.
Xu, S., Wang, Y., and Yu, H. (2021). The mechanism of human connectedness in relationship to physical health, mental health, and cognitive function among the elderly in rural China. Front. Psychiatry 12:702603. doi: 10.3389/fpsyt.2021.702603
Zhang, Z., and Treiman, D. J. (2013). Social origins, hukou conversion, and the wellbeing of urban residents in contemporary China. Soc. Sci. Res. 42, 71–89. doi: 10.1016/j.ssresearch.2012.08.004
Zhang, L., Xu, Y., Nie, H., Zhang, Y., and Wu, Y. (2012). The prevalence of depressive symptoms among the older in China: a meta-analysis. Int. J. Geriatr. Psychiatry 27, 900–906. doi: 10.1002/gps.2821
Zvolensky, M. J., Paulus, D. J., Bakhshaie, J., Viana, A. G., Garza, M., Manning, K., et al. (2017). Subjective social status and anxiety and depressive symptoms and disorders among low income latinos in primary care: the role of emotion dysregulation. Cogn. Ther. Res. 41, 686–698. doi: 10.1007/s10608-017-9844-y
Keywords: rural–urban linkages, HuKou system, subjective social status, loneliness, anxiety, depression, college and university students
Citation: Yu H, Xu S, Li H, Wang X, Sun Q and Wang Y (2022) A man-made divide: Investigating the effect of urban–rural household registration and subjective social status on mental health mediated by loneliness among a large sample of university students in China. Front. Psychol. 13:1012393. doi: 10.3389/fpsyg.2022.1012393
Edited by:
Jingyi Wang, Fudan University, ChinaCopyright © 2022 Yu, Xu, Li, Wang, Sun and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shicun Xu, eHVzaGljdW5Aamx1LmVkdS5jbg==; Yuanyuan Wang, YW5nZWxheXVhbnl1YW53YW5nQGdtYWlsLmNvbQ==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.