
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol. , 08 December 2021
Sec. Health Psychology
Volume 12 - 2021 | https://doi.org/10.3389/fpsyg.2021.779277
This article is part of the Research Topic Mental Health in Primary Health Care View all 14 articles
 María Elena Garrote-Cámara1,2
María Elena Garrote-Cámara1,2 Iván Santolalla-Arnedo2,3*Regina Ruiz de Viñaspre-Hernández2,3Vicente Gea-Caballero4Teresa Sufrate-Sorzano2,3Pablo del Pozo-Herce2,3,5Rebeca Garrido-García2,3,6Esther Rubinat-Arnaldo7,8,9
Iván Santolalla-Arnedo2,3*Regina Ruiz de Viñaspre-Hernández2,3Vicente Gea-Caballero4Teresa Sufrate-Sorzano2,3Pablo del Pozo-Herce2,3,5Rebeca Garrido-García2,3,6Esther Rubinat-Arnaldo7,8,9 Raúl Juárez Vela2,3
Raúl Juárez Vela2,3Background: Severe mental disorder (SMD) is understood in a first approximation as a disorder of thought, emotion, or behavior of long duration, which entails a variable degree of disability and social dysfunction. One of the most widely used assessment scales for agitated behavior, in its English version, is the Corrigan Agitated Behavior Scale (ABS); several studies have demonstrated solid psychometric properties of the English version, with adequate internal consistency.
Objective: The objective of this study was to evaluate the psychometric properties of the Spanish version of the ABS Corrigan scale, in a sample of patients with severe mental disorders. The psychometric analyses of the Spanish version of the ABS Corrigan included tests of the reliability and validity of its internal structure.
Results: The structure of the factorial loads of the analyzed elements is consistent with the hypothesized three-dimensional construction referred to in the original ABS. The results suggest that the reliability and validity of the three dimensions are acceptable (First 0.8, Second 0.8, and Third 0.7). The internal consistency of the Spanish version of the complete ABS and of each of the three domains that compose it is high, with values very close to those found in the original version, with approximate figures of 0.9.
Conclusion: In our study, the three domains aim to explain 64.1% of the total variance of the scale, which exceeds the 50% found in the original version.
Severe mental disorder (SMD) is understood in a first approximation as a disorder of thought, emotion, or behavior of long duration, which entails a variable degree of disability and social dysfunction (Vila et al., 2007). In the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), specifically, it is “a syndrome characterized by a clinically significant alteration of the cognitive state, emotional regulation or behavior of an individual, which reflects a dysfunction of psychological processes, biological or developmental that underlie their mental function” (American Psychiatric Association, 2013). According to the National Institute of Mental Health, SMD patients face a limitation in being able to carry out important activities in their daily lives (National Institute of Mental Health, 2019). There are very diverse pathologies that can be included in the concept of serious mental disorder, and they are usually classified according to the symptoms, evolution, chronicity and level of disability they cause in the lives of patients (World Health Organization, 2018). Patients with SMD experience a significant deterioration, which limits the development of their daily activities (Hazelden Foundation, 2016; Padilla et al., 2018). At present, the two most used taxonomies for the diagnosis of SMD are the Classification of Mental and Behavioral Disorders (ICD-11) of the World Health Organization (2018) and the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) of the American Psychiatric Association (2013). The main groups of diagnoses that give rise to the appearance of situations valued as a severe mental disorder are as follows: schizophrenia and a group of psychotic disorders; depressive disorder, manic disorder and bipolar disorder; anxiety disorders; and personality disorders (Pichot et al., 1995; Gobierno de Navarra, 2005). In Spain, the results of the 2017 National Health Survey (Ministry of Health, Consumer Affaris and Social Welfare, 2017) indicate that 10.8% of adults reported having been diagnosed with a mental health problem; women report a mental health problem more frequently than men, 14.1% versus 7.2%. Furthermore, 6.7% of adults report chronic anxiety, 9.1% of women and 4.3% of men. Depression is declared in the same proportion as anxiety (6.7%), and it is more than double in women (9.2%) than in men (4%).
All the diagnoses described above present a series of common characteristics, such as greater vulnerability to stress, difficulties in coping with the demands of the environment, problems in managing frustration, deficits in their abilities to manage autonomously, difficulties in social interaction and high dependence on other people and health and/or social services (Vila et al., 2007; Hazelden Foundation, 2016; Padilla et al., 2018). Symptoms of the disease and difficulties in interacting with the environment develop complications, such as psychomotor agitation, more prevalent in people suffering from a serious mental disorder. The prevalence of psychomotor agitation is high, up to 10% of patients seen in general emergency services (Pacciardi et al., 2013) and between 20 and 50% if we specifically consider psychiatric emergencies (Allen and Currier, 2004; Marco and Vaughan, 2005). Different studies relate psychomotor agitation with the suffering of a severe mental disorder (Bogner et al., 1999; Huber et al., 2016; Ostinelli et al., 2019), diverse psychiatric conditions, as well as some medical disorders (Galián Muñoz et al., 2011). Agitation of psychiatric origin is seen more frequently in patients with psychotic disorders, such as schizophrenia, schizoaffective disorder and the manic phase of bipolar disorder, as well as in some personality disorders (Feldman et al., 2001; Buckley et al., 2003; Battaglia, 2005; Serretti and Olgiati, 2005; Wittchen et al., 2011). In a manic episode, psychomotor agitation comes from the same phenomenology of the condition, where it is described as part of the symptom complex of mania with excessive motor and cognitive activity (Soutullo et al., 2011). In Spain, it is estimated that 25% of patients with schizophrenia and 15% of patients with bipolar disorder could suffer from at least one episode of agitation each year, with an average of two episodes per patient (Viñado et al., 2015).
Psychomotor agitation is characterized as a non-specific syndrome, of multifactorial etiology, which entails an alteration of motor behavior, consisting of a disproportionate and disorganized increase in motor functions and which may be accompanied by vegetative activation (profuse sweating, tachycardia, and mydriasis), severe anxiety, aggressiveness, panic, behavior lability, disinhibition or other intense emotional states (Allen and Currier, 2004; Pacciardi et al., 2013). The patient’s state of mind can manifest itself as nervous, euphoric and choleric, and laughter, crying and uncontrollable screaming are frequent, which can lead to verbal and/or physical aggressions, and therefore, pose a serious risk to both the patient themself (self-harm), as well as family members, healthcare personnel and the environment in general (hetero-harm) (Marco and Vaughan, 2005). On many occasions, the management of agitation presents difficulties, since they are usually people who are difficult to collaborate and who can present aggressive behaviors, disinhibition, which greatly hinders the assistance work, treatment and care of the patient.
Psychomotor agitation corresponds to one of the most important hospital emergencies in the care of severe mental disorder since it requires immediate professional assistance, and the safety of the patient is seriously compromised (Bogner et al., 2001; Buckley et al., 2003; Nott et al., 2006; Galián Muñoz et al., 2011; Ostinelli et al., 2019).
A large proportion of older people with mental disorders live at home and are cared for by their relatives, which requires the involvement of primary care physicians and rapid intervention (Adriaenssens et al., 2019). Whenever possible and when required by the patient, the patient should be assessed and cared for in their own environment, limiting trips to health centers for emergencies or seriousness, or for special tests (Snowdon, 2007). Home assessment should involve primary care professionals and should always take into account socio-demographic, somatic, functional and social aspects (Olivera et al., 2011). The assessment should result in the formulation of a care plan with clear objectives and defined responsibilities for members of the multidisciplinary team and the primary care team (Hoedemakers et al., 2019).
The evaluation of psychomotor agitation, as well as its management, constitutes a challenge for health professionals since this syndrome usually overwhelms their management skills. One of the most widely used assessment scales for agitated behavior, in its English version, is the Corrigan Agitated Behavior Scale (ABS; Corrigan, 1989). This scale provides both quantitative and qualitative data, determining the level of agitation and its characteristics at the level of lability, disinhibition and aggressiveness associated with the agitation episode (Corrigan, 1989; Corrigan and Bogner, 1994). It was designed by Corrigan (1989) to evaluate agitation in the context of patients in a period of post-encephalic trauma; however, since its design, it has been widely used in the evaluation of agitation in patients with severe mental disorders (Bogner et al., 1999; García et al., 2002; García - Ribera, 2014).
Given the importance of psychomotor agitation among the population suffering from a severe mental disorder and Spanish being the second most spoken language in the world (Instituto Cervantes, 2020), it is necessary to have a tool with which to assess agitation in these patients. The objective of this study was to evaluate the psychometric properties of the Spanish version of the ABS Corrigan scale in a sample of patients with severe mental disorder.
Before testing its psychometric properties, the Corrigan ABS scale was translated and culturally adapted from its original English version into Spanish. We follow the guidelines published by Beaton et al. (2000) who divided the process into the following six steps: (1) translation, (2) synthesis, (3) back-translation, (4) back-translation synthesis, (5) review by the expert committee of the translated version, and (6) preliminary tests.
The original ABS Corrigan scale was translated into Spanish by two independent translators, an expert in medical translation and a researcher familiar with the instrument and its characteristics (forward translation). The translators were instructed to use simple sentences and avoid metaphors, colloquial terminology, passive sentences, and hypothetical statements. In a meeting of the expert committee, made up of the authors and the translators, the differences between the two translations were discussed, and the initial translation was unified (reconciliation). This first Spanish translation was blindly re-translated into English (back-translation). Subsequently, the expert committee compared and contrasted the original and retro-translated versions, in order to achieve the most precise adaptation possible to the original language of the Spanish version and agreed, by consensus, on the final Spanish version of the ABS Corrigan to be used in the sample.
Finally, as it is a hetero-applied administration instrument, cognitive interviews were completed in a sample of 20 nursing professionals (cognitive debriefing) that confirmed the legibility of the elements as they were written.
This study was conducted in the north region of Spain (La Rioja) using a cross-sectional design. We enrolled a sample of n = 140 participants admitted to the Mental Health of Albelda de Iregua (La Rioja) who met the following inclusion criteria: (1) being diagnosed severe mental disorder, (2) be admitted to psychiatric hospitalization units at the Rioja Health Service, (3) present an episode of psychomotor agitation between 2015 and 2020, and (4) being 18 years or older. According to Norman and Streiner (1996) we enrolled 140 participants at least five patients for item of the scale. All data were collected by qualified nurses, who had been specifically trained for this purpose, during the patients’ admission.
The sample size was estimated according to the criteria to perform a factor analysis that contemplated a minimum of 10 subjects for each item (De Vet et al., 2005). The Corrigan Agitated Behavior Scale is a hetero-applied administration instrument, where the interviewer must evaluate 14 items, which are quantified with a Likert-type scale according to the observation of the professional (Bogner et al., 1999; García et al., 2002; García - Ribera, 2014). The scale was completed by trained nursing professionals; the psychomotor agitation data of patients with severe mental disorders, who developed an episode of psychomotor agitation during their admission to the psychiatric hospitalization units of the Rioja Health Service, were collected. The inclusion criteria were patients diagnosed with a severe mental disorder, of both sexes, older than 16 years, admitted to the psychiatric hospitalization units of the Rioja Health Service, and who developed an episode of psychomotor agitation between 2015 and 2020.
The scale includes 14 items that are grouped in the original English version into three factors: disinhibition, items 1, 2, 6, 7, 8, 9, and 10; aggressiveness, items 3, 4, 5, and 14; lability, items 11, 12, and 13 (Corrigan, 1989). There are 14 items that assess the ability to sustain attention: impulsiveness, pain tolerance and frustration management; cooperation and demand; violence and threats; explosiveness, anger and unpredictability; self-stimulating behaviors; pull objects or ties from the bed; roams the treatment areas; restlessness and excessive movement; repetitive behaviors; excessive, fast and loud language; sudden mood change; excessive facility for crying and/or laughing; self-injurious behaviors. The professional must score according to a Likert-type scale of 4 degrees of intensity, from 1 (absence) to 4 (extreme degree). The sum of the scores of the 14 items determines the severity of the agitation; the higher the score, the greater the severity. The score in each of the three factors determines if the episode is characterized more by its lability, disinhibition, or aggressiveness (Corrigan, 1989; Teri et al., 1992; Corrigan and Bogner, 1994; Spanish Society of Emergency and Emergency Nursing, 2009). In addition to the score for each item, socio-demographic data and the main diagnosis that led to admission were collected.
Sociodemographic and clinical variables were analyzed using descriptive statistics as the mean and standard deviation in the case of quantitative variables and frequencies in the case of categorical variables. In addition, other parametric techniques, including the mean, standard deviation, skewness, and kurtosis, were used to describe responses to items and summarize the total scale score. The psychometric analyses of the Spanish version of the ABS Corrigan included tests of reliability and validity of its internal structure. We evaluated the reliability of the scale by exploring internal consistency, and we calculated Cronbach’s alpha coefficient of the global scale and each of the theoretical dimensions, accepting significance values of 0.70 or higher as an indicator of good internal consistency (Argimon, 2012).
We evaluated the underlying factor structure of the ABS scale in Spanish using factor analysis. To assess the relevance of performing an exploratory factor analysis on the sample, the Kaiser–Meyer–Olkin (KMO) sample adequacy statistic and the Bartlett sphericity statistic were previously calculated. The suitability of the analysis was determined with a KMO greater than 0.6, and in the case of Bartlett’s test of sphericity, a rejection of the null hypothesis of sphericity of p < 0.05 to ensure that the use of the factorial model was adequate. An exploratory factor analysis (EFA) was performed using principal component analysis with a Varimax rotation to determine the number of latent constructs and the underlying factorial structure of domains on the ABS scale in its Spanish version. The number of factors on the scale was estimated, considering two complementary criteria: (1) the Kaiser–Guttman or latent root criterion and (2) the drop contrast criterion (Hair et al., 2005; Martínez et al., 2006; Tabachnick et al., 2007). The statistical software used was SPSS (IBM SPSS Statistics for Windows, Version 23.0, IBM Corp., Armonk, NY, United States).
The data collection was anonymous and did not collect personal data or devices that could identify the informant. The information was treated confidentially and anonymously since they had dissociated data, following the Data Protection Regulation (EU) 2016/679 of the European Parliament and the Spanish Organic Law 3/2018. The study was approved by the Ethics Committee of the Rioja Biomedical Research Center (CIBIR) (reference CEImLar P.I. 467) (Biomedical Research Center of La Rioja, 2021). The researchers do not declare any type of ethical, moral or legal conflict, nor do they claim to have received financial compensation of any other kind. The participants did not receive any type of compensation for answering the questionnaire, as it was voluntary.
Table 1 illustrates the main sociodemographic characteristics of the sample. The mean age of the sample was 45.61 years. In total, 52.9% of the sample were men, and 47.1% were women. Regarding the underlying pathology, 60.7% of the sample presented schizophrenia and other psychotic disorders, of which 60% were men and 40% were women; 9.3% presented a depressive episode, of which 30.8% were men and 69.2% were women; 2.1% presented a manic episode, all of which were women; 8.6% presented a bipolar episode, of which 33.3% were men and 66.7% were women; 10.7% presented a personality disorder, of which 40% were men and 60% were women; 8.6% presented other pathologies, of which 75% were men and 25% were women.
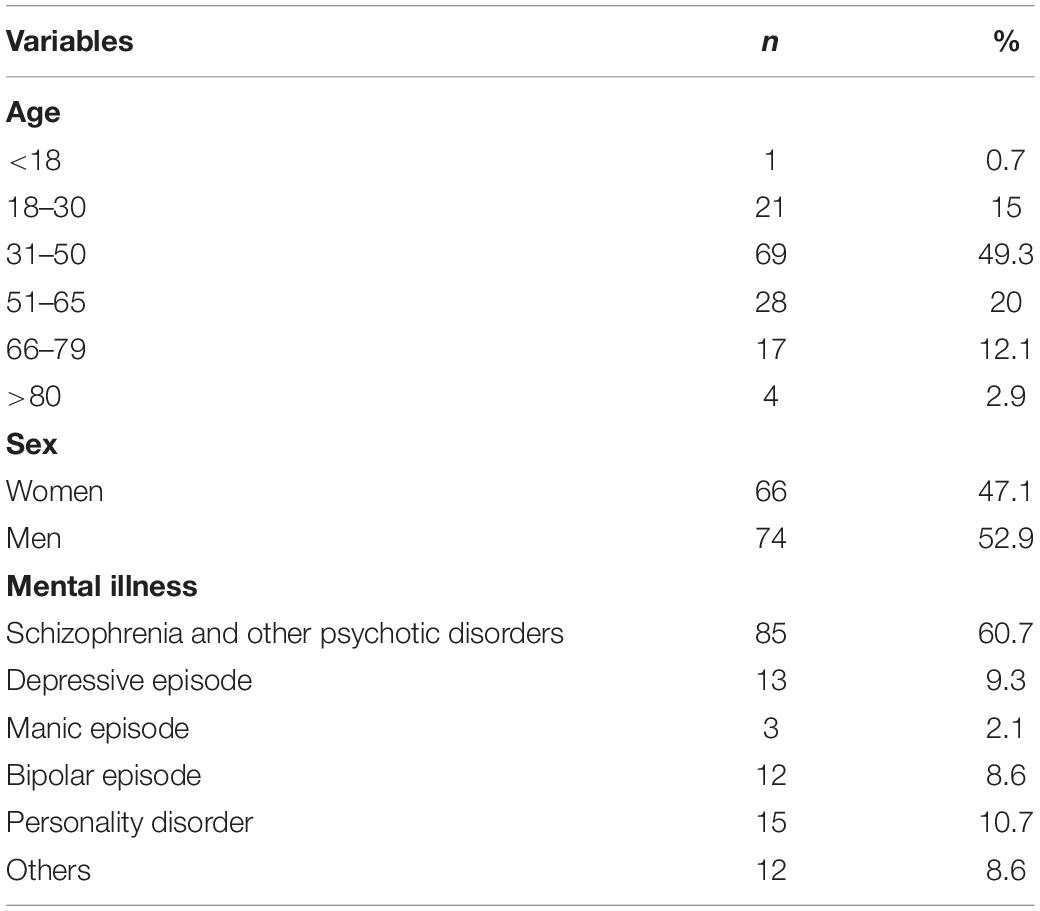
Table 1. Main sociodemographic characteristics of the sample (n = 140).
The mean, standard deviation (SD), asymmetry and kurtosis values for each of the items of the Spanish version of the scale of psychomotor agitation, ABS Corrigan, are indicated in Table 2. Most of the items are distributed normally, without excessive asymmetry and kurtosis. The items with the highest scores are item 2 “Impulsive, impatient, tolerates pain or frustration poorly” and item 3 “Uncooperative, does not let them take care of him, demanding.” The lowest scores were recorded by item 7 “Pulls the tubes or ties on the bed” and item 13 “Cries or laughs easily and excessively.”
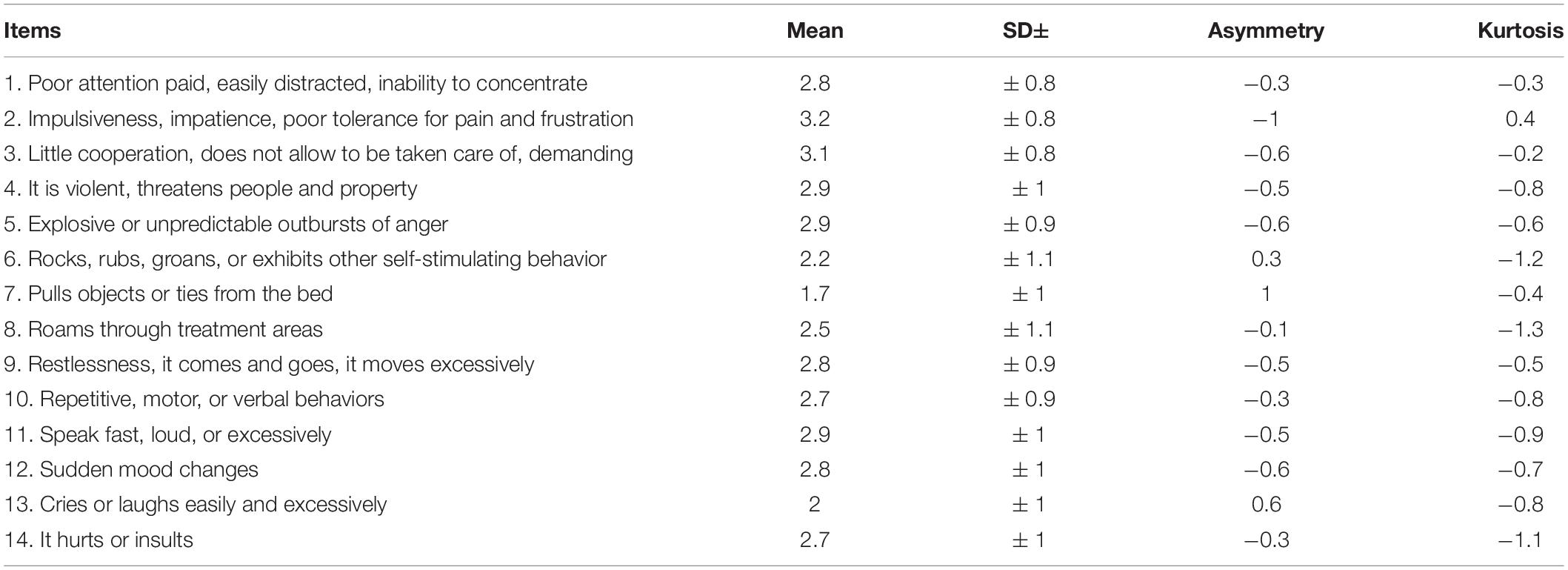
Table 2. Descriptive statistics of the items of the Spanish version of the ABS Corrigan scale.
In terms of reliability, the internal consistency of the Spanish version of the ABS Corrigan scale and its domains is excellent (Alexandre et al., 2013; Coluci et al., 2015; Cunha et al., 2016). Cronbach’s alpha for the total scale is 0.9, and for each of the scale dimensions, disinhibition is 0.8, aggressiveness is 0.8 and lability is 0.7 (see Table 3).
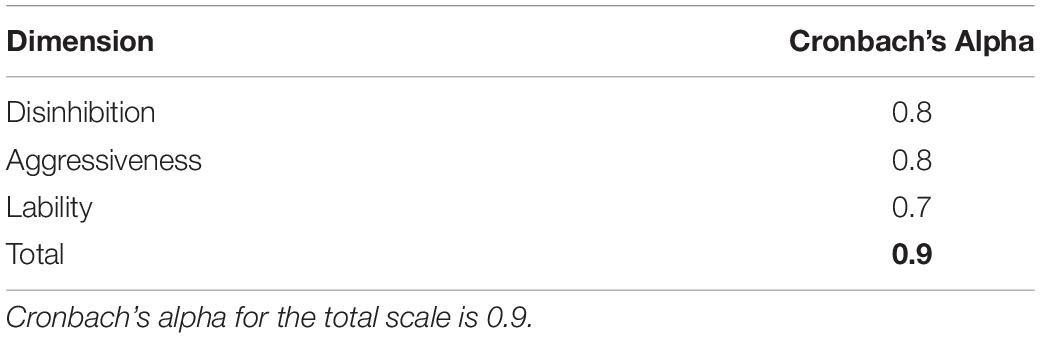
Table 3. Cronbach’s Alpha – ABS Corrigan. Scale dimensions.
The adequacy tests, before performing the exploratory factor analysis, resulted in a Kaiser–Meyer–Olkin (KMO) value of 0.9. Bartlett’s test of sphericity is significant (p < 0.01) both in the analysis of each of the domains and in the global analysis of the scale. Sampling suitability is high in the exploratory factor analysis.
The Kaiser–Guttman or latent root criterion identified three factors with eigenvalues greater than 1, as shown in Table 4, which would explain 64.1% of the total variance of the items. The second criterion, fall contrast or screen test, also showed through the sedimentation graph the presence of three factors, as reflected in Figure 1.
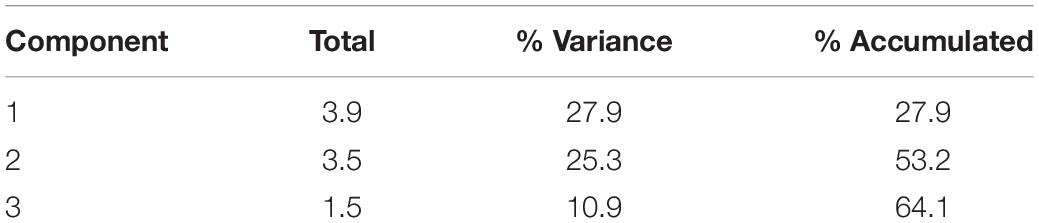
Table 4. Total explained variance – ABS Corrigan. Sum of rotation of charges square.
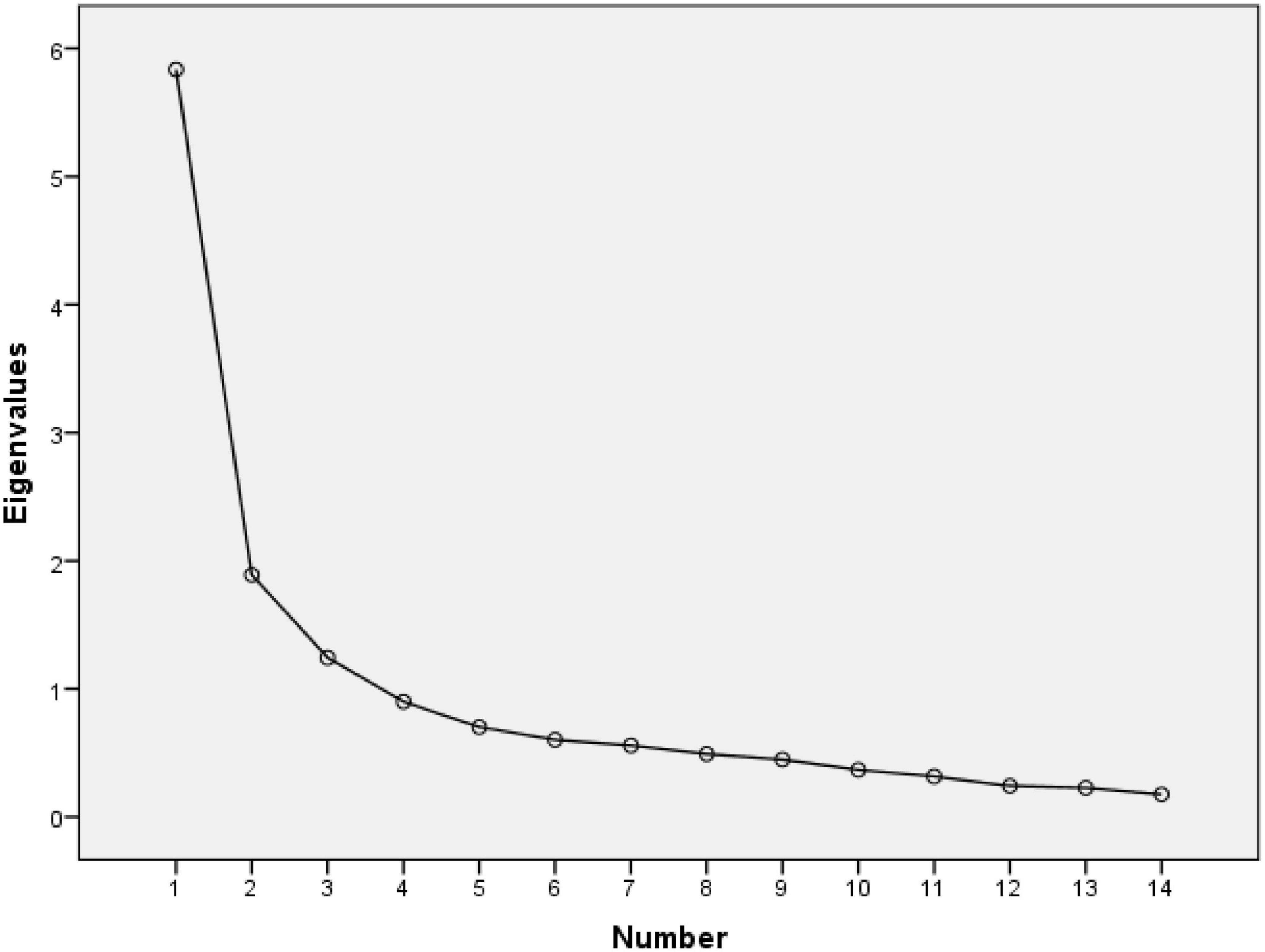
Figure 1. Sedimentation chart of the Spanish version of the ABS Corrigan.
The exploratory factor analysis (EFA) was developed using principal component analysis with a Varimax rotation, considering the following criteria: factor load >0.30, the number of items per factor according to the original version, the interpretability of the results and the theory that supports the ABS Corrigan scale. According to these criteria, the best solution was to identify three dimensions of grouping the items as in the original version; see Table 5. The dimension “disinhibition” included items 1, 2, 6, 7, 8, 9, and 10; the “aggressiveness” dimension included items 3, 4, 5, and 14; the dimension “lability” items 11, 12, and 13. In the matrix of the rotated component (Varimax) of Table 5, it is observed that the elements load significantly in the three previous factors.

Table 5. Rotated component matrix. Principal component analysis (Varimax).
The results of the exploratory factor analysis (EFA) suggest that the three dimensions determined in the ABS Corrigan evaluation scale originally validated in the US, “disinhibition,” “aggressiveness,” and “lability,” are applicable for this version in Spanish. The structure of the factorial loads of the analyzed elements is consistent with the hypothesized three-dimensional construction referred to in the original ABS. The results suggest that the reliability and validity of the three dimensions is acceptable. The results are largely consistent with the initial hypothesis.
The adaptation and cross-cultural validation into Spanish of the Agitated Behavior Scale (ABS Corrigan) was carried out, thus obtaining a culturally equivalent instrument that allows the evaluation of psychomotor agitation in patients with severe mental disorder, obtaining levels of severity of agitation, such as the exploration of three related domains, disinhibition, lability, and aggressiveness. The results of this study indicate that these three domains are applicable in patients with severe mental disorder, and the reliability and validity measures are satisfactory for their use in Spanish.
During the cross-cultural adaptation process, there were no language difficulties; only some expressions were slightly modified to ensure their cultural equivalence. The nursing professionals who participated in the study did not show any difficulties in filling in the scale after attending to and observing the patient’s psychomotor agitation. As it is a hetero-applied administration instrument, the patients do not need to understand the scale.
Several studies have demonstrated the solid psychometric properties of the English version, with an adequate internal consistency, Cronbach’s alpha between 0.801 and 0.921 (Corrigan, 1989; Corrigan and Bogner, 1994; Bogner et al., 1999; Vilibiæ et al., 2014; Hellweg and Schuster-Amft, 2016). The internal consistency of the Spanish version of the complete Corrigan Agitated Behavior Scale and of each of the three domains that compose it is high, with values very close to those found in the original version, with approximate figures of 0.9. Similar to the original English version, and the German version of the scale, Cronbach’s alpha of the aggression, disinhibition and lability subscales is lower than that of the total scale score, indicating that the total score remains the best overall measure of agitation (Corrigan, 1989; Corrigan and Bogner, 1994; Hellweg and Schuster-Amft, 2016). In our study, the three adopted domains explain 64.1% of the total variance of the scale, which exceeds the 50% found in the original version (Corrigan, 1989).
The exploratory factor analysis of this study supports the maintenance of the same three domains adopted in the original version and confirmed in the validated version in German (Corrigan, 1989; Corrigan and Bogner, 1994; Hellweg and Schuster-Amft, 2016). Although adequate correlations were observed in the German version, the correlations were lower than those in the original English version and in this study, in which we analyzed a Spanish version. This may be due to the fact that the German study was multidisciplinary compared to the Spanish version, which is monodisciplinary. The nursing professional knows the patient, is responsible for the patient’s health care, knows the signs and symptoms of the disease and is the first line of care for episodes of psychomotor agitation. The fact that these professionals assess the agitation episodes through the 14 items of the ABS Corrigan improve the adequacy of the results of the scale (Santolalla et al., 2015; Caqueo-Urízar et al., 2016; Hellweg and Schuster-Amft, 2016).
In the exploratory factor analysis, it is observed, for example, that there are items related to the aggressiveness dimension, such as item 4 “is violent, threatens person or property,” item 5 “explosive or with unpredictable anger attacks” and item 14 “harm or insult,” which highly identified with the dimension, as also observed in the study of the German version (Hellweg and Schuster-Amft, 2016). The aggressiveness dimension is perhaps one of the most related to psychomotor agitation in patients with severe mental disorder, especially regarding the diagnostic group of schizophrenia and other psychotic disorders, which helps healthcare professionals to evaluate the items related to this dimension (Lehman et al., 2004). In fact, psychomotor agitation is particularly prevalent among the population with schizophrenia and bipolar disorder (Witt et al., 2013; Zhou et al., 2015; Vieta and Garriga, 2016; Wu et al., 2018). In Spain, a recent report indicated that 25% of patients with schizophrenia and 15% of those with bipolar disorder could be expected to experience at least one episode of psychomotor agitation each year (Vieta et al., 2017). On the other hand, the lower load of item 3 “Uncooperative, does not let them take care of him, demanding” on the aggressiveness dimension can be related to cultural and translation factors, as the demand or little collaboration is not significantly related in our country with aggressiveness, so the nursing professional could score this item in a more random way (Real Academia Española, 2021).
In this line, item 8 “wanders through the treatment areas,” item 11 “speaks fast, loud, or excessively,” and item 12 “changes of mood suddenly,” with lower loads on its dimensions, can be more difficult to identify with its domain due to cultural factors or translation difficulties. Describing these items further could improve the response from professionals. These notes do not substantially change the use of the scale in its Spanish version, but they do inform us about the importance of not only the linguistic but also the cultural validation of the tools for measuring concepts as complex as agitation.
Psychomotor agitation is characterized by an interruption in the relationship or collaboration of the health professional and the patient, severely interfering with the evaluation, treatment, health care and prognosis of the underlying pathology. The management and care of the agitated patient constitute a first level health care demand. The safety of the patient, health care personnel and third parties; reducing the progression of the condition by acting on prodromal phases; and limiting complications during crises by their early discovery and management, must be guaranteed. The availability of a psychomotor agitation assessment scale, adapted to the language and culture of our country, with adequate psychometric properties, offers greater possibilities for prevention, adequate diagnosis, research, treatment and effective care, improving the prognosis and quality of life of affected patients (Santolalla et al., 2015; Caqueo-Urízar et al., 2016).
The sample used for data validation is sufficiently large to guarantee an adequate representation of patients with severe mental disorder. However, most of the sample for this study presents schizophrenia, in this sense it is recommended to focus the analysis only on these patients, since the rest of the sample is too stratified in other pathologies.
The results of this translation and validation study into the Spanish version of the Agitated Behavior Scale (ABS Corrigan) suggest that the reliability and validity of the three dimensions is acceptable, with data similar to the original English version and better fit than the German version (Corrigan, 1989; Hellweg and Schuster-Amft, 2016). The total scale score remains the best overall measure of agitation. The results are largely compatible with the initial hypothesis, which makes them useful for clinical and research use in our country.
The use of validated instruments means providing health professionals with reliable and valid tools. Different studies have demonstrated the solid properties of the Corrigan Agitated Behavior Scale in its English version. However, no studies have validated this scale in the Spanish language. With this study, we reveal psychometric characteristics and sociodemographic adaptation of the Corrigan Agitated Behavior Scale in patients with various mental disorders to one of the most widely spoken language in the world.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The study was approved by the Ethics Committee of the Rioja Biomedical Research Center (CIBIR) (reference CEImLar P.I. 467) (Centro de Investigación Biomédica, 2021). Written informed consent from the patients/participants was not required to participate in this study in accordance with the national legislation and the institutional requirements.
All authors listed have made a substantial, direct, and intellectual contribution to the work, and approved it for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Adriaenssens, J., Benahmed, N., and Ricour, C. (2019). Improving mental healthcare for the elderly in Belgium. Int. J. Health Plann. Manage. 34, e1948–e1960. doi: 10.1002/hpm.2858
Alexandre, N. M. C., Gallasch, C. H., Lima, M. H. M., and Rodrigues, R. C. M. (2013). Reliability in the development and evaluation of measurement instruments in the health field. Eletr. Nurs. J. 15, 802–809.
Allen, M. H., and Currier, G. W. (2004). Use of restraints and pharmacotherapy in academic psychiatric emergency services. Gen. Hosp. Psychiatry 26, 42–49. doi: 10.1016/j.genhosppsych.2003.08.002
American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders: (DSM-5) Washington, DC: American Psychiatric Association 10.
Argimon, J. M. (2012). Métodos de Investigación Clínica y Epidemiológica. 4rd Edn. Amsterdam: Elsevier.
Beaton, D., Bombardier, C., Guillemin, F., and Ferraz, M. B. (2000). Recommendations for the Cross-cultural Adaptation of Health Status Measures. New York, NY: American Academy of Orthopaedic Surgeons 1–9.
Bogner, J. A., Corrigan, J. D., Fugate, L., Mysiw, W. J., and Clinchot, D. (2001). Role of agitation in prediction of outcomes after traumatic brain injury. Am. J. Phys. Med. Rehabil. 80, 636–644. doi: 10.1097/00002060-200109000-00002
Bogner, J. A., Corrigan, J. D., Stange, M., and Rabold, D. (1999). Reliability of the agitated behavior scale. J. Head Trauma Rehabil. 14, 91–96.
Buckley, P. F., Noffsinger, S. G., Smith, D. A., Hrouda, D. R., and Knoll, J. L. (2003). Treatment of the psychotic patient who is violent. Psychiatr. Clin. North Am. 26, 231–272.
Caqueo-Urízar, A., Fond, G., Urzúa, A., Boyert, L., and Willians, D. (2016). Violent behavior and aggression in schizophrenia: prevalence and risk factors. a multicentric study from three latin-America countries. Schizophr. Res. 178, 23-28. doi: 10.1016/j.schres.2016.09.005
Centro de Investigación Biomédica (2021). Comité de Ética de la Investigación con Medicamentos. Madrid: Centro de Investigación Biomédica.
Coluci, M. Z. O., Alexandre, N. M. C., and Milani, D. (2015). Construction of measurement instruments in the area of health. Cien. Saude Colet. 20, 925-936. doi: 10.1590/1413-81232015203.04332013
Corrigan, J. D. (1989). Development of a scale for assessment of agitation following traumatic brain injury. J. Clin. Exp. Neuropsychol. 11, 261–277. doi: 10.1080/01688638908400888
Corrigan, J. D., and Bogner, J. A. (1994). Factor structure of the agitated behavior scale. J. Clin. Exp. Neuropsychol. 16, 386–392. doi: 10.1080/01688639408402649
Cunha, C. M., Almeida Neto, O. P., and Stackfleth, R. (2016). Main psychometric evaluation methods of measuring instruments reliability. Rev Atenção Saúde 14, 98–103.
De Vet, H. C., Adèr, H. J., Terwee, C. B., and Pouwer, F. (2005). Are factor analytical techniques used appropriately in the validation of health status questionnaires? A systematic review on the quality of factor analysis of the SF-36. Qual. Life Res.14, 1203–1218. doi: 10.1007/s11136-004-5742-3
Galián Muñoz, I., Bernal Torres, J., Díaz Sánchez, C., and Martínez Serrano, J. (2011). Protocolo de Atención a Pacientes con Agitación y/o Heteroagresividad. Murcia: Hospital Psiquiátrico Román Alberca.
García, J. B., Portilla, M. P. G., Fernández, M. T. B., Martínez, P. A. S., and García, M. B. (2002). Banco de Instrumentos Básicos Para la Práctica de la Psiquiatría Clínica. Madrid: Ars Médica.
Gobierno de Navarra (2005). Programa de Atención a Personas con Trastorno Mental Grave. Available online at: https://www.navarra.es/NR/rdonlyres/B66BCCE6-6744-4560-83E7-7729EE54C2D1/152344/PROGRAMATMG1.pdf (accessed September 2, 2021).
Feldman, H., Gauthier, S., Hecker, J., Vellas, B., Subbiah, P., and Whalen, E. (2001). A 24-week, randomized, double-blind study of donepezil in moderate to severe Alzheimer’s disease. Neurology 57, 613–620.
Hair, J., Black, W., Babin, B., Anderson, R., and Tatham, R. (2005). Multivariate Data Analysis, 6th Edn. New Jersey: Prentice Hall.
Hazelden Foundation (2016). Severe Mental Illness Defined by Duration and Disability. Available online at: http://www.bhevolution.org/public/severe_mental_illness.page (accessed July 17, 2021).
Hellweg, S., and Schuster-Amft, C. (2016). German version, inter- and intrarater reliability and internal consistency of the “Agitated Behavior Scale” (ABS-G) in patients with moderate to severe traumatic brain injury. Health Qual. Life Outcomes 14:106. doi: 10.1186/s12955-016-0511-x.
Hoedemakers, M., Marie Leijten, F. R., Looman, W., Czypionka, T., Kraus, M., Donkers, H., et al. (2019). Atención integrada para ancianos frágiles: un estudio cualitativo de un enfoque prometedor en los Países Bajos. Revista internacional de atención integrada 19:16. doi: 10.5334/ijic.4626
Huber, C. G., Hochstrasser, L., Meister, K., Schimmelmann, B. G., and Lambert, M. (2016). Evidence for an agitated-aggressive syndrome in early-onset psychosis correlated with antisocial personality disorder, forensic history, and substance use disorder. Schizophr. Res. 175, 198–203. doi: 10.1016/j.schres.2016.04.027
Instituto Cervantes (2020). CVC. Anuario 2020. Informe 2020. El español en cifras. Available online at: https://cvc.cervantes.es/lengua/anuario/anuario_20/informes_ic/p01.htm (accessed June 26, 2021).
Lehman, A. F., Lieberman, J. A., Dixon, L. B., McGlashan, T. H., Miller, A. L., Perkins, D. O., et al. (2004). Practice guideline for the treatment of partients with schizophrenia. Am. J. Psychiatry 161(2 Suppl.), 1–56.
Marco, C. A., and Vaughan, J. (2005). Emergency management of agitation in schizophrenia. Am. J. Emerg. Med. 23, 767–776. doi: 10.1016/j.ajem.2005.02.050
Martínez, M. R., Hernández, M. J., and Hernández, M. V. (2006). Psicometría. Madrid: Alianza Editorial.
Ministry of Health, Consumer Affaris and Social Welfare (2017). National Health Survey ENSE, Spain 2017. Madrid: Ministry Of Health, Consumer Affairs and Social Welfare.
National Institute of Mental Health (2019). Mental Illness. https://www.nimh.nih.gov/health/statistics/mental-illness (accessed June 15, 2021).
Nott, M. T., Chapparo, C., and Baguley, I. J. (2006). Agitation following traumatic brain injury: an Australian sample. Brain Inj. 20, 1175–1182. doi: 10.1080/02699050601049114
Olivera, J., Benabarre, S., Lorente, T., Rodriguez, M., Barros, A., Quintana, C., et al. (2011). Detecting psychogeriatric problems in primary care: factors related to psychiatric symptoms in older community patients. Ment. Health Fam. Med. 8, 11–19.
Ostinelli, E. G., D’Agostino, A., Shokraneh, F., Salanti, G., and Furukawa, T. A. (2019). Acute interventions for aggression and agitation in psychosis: study protocol for a systematic review and network meta-analysis. BMJ open 9:e032726. doi: 10.1136/bmjopen-2019-032726
Pacciardi, B., Mauri, M., Cargioli, C., Belli, S., Cutugno, B., Di Paolo, L., et al. (2013). Issues in the management of acute agitation: how much current guidelines consider safety? Front. Psychiatry 4:26. doi: 10.3389/fpsyt.2013.00026
Padilla, E. M., Posada, D. O., and Medina, P. S. (2018). La adherencia familiar en el trastorno mental grave. Atención Primaria 50, 519–526. doi: 10.1016/j.aprim.2017.06.010
Pichot, P., López-ibor Aliño, J. J., and Valdés Miyar, M. (1995). DSM-IV. Manual diagnóstico y estadístico de los Trastornos Mentales. Barcelona.
Real Academia Española (2021). Diccionario de la Lengua Española. 23.a Edn. Madrid: Real Academia Española.
Santolalla, I., Losa, M., and Silva, T. (2015). Impact of Drug Use on Psychomotor Agitation in Hospitalized Patients With Severe Mental Disorder, (Doctoral Thesis), España: King Juan Carlos University.
Serretti, A., and Olgiati, P. (2005). Profiles of “manic” symptoms in bipolar I, bipolar II and major depressive disorders. J. Affect Disord. 84, 159–166.
Snowdon, J. (2007). Psychogeriatric services in the community and in long-term care facilities: needs and developments. Curr. Opin. Psychiatry 20, 533–538. doi: 10.1097/YCO.0b013e3282c8c85e
Spanish Society of Emergency and Emergency Nursing (2009). El Paciente agitado. Madrid: Sociedad Española De Enfermería De Urgencias Y Emergencias.
Soutullo, C., Quintana, F., Vicario, M., and De Castro, P. (2011). Enfermedad bipolaro maníaco-depresiva. Mood dis. psych. 48, 5684-5692.
Tabachnick, B. G., Fidell, L. S., and Ullman, J. B. (2007). Using Multivariate Statistics. Boston, MA: Pearson, 481–498.
Teri, L., Rabins, P., Whitehouse, P., Berg, L., Reisberg, B., Sunderland, T., et al. (1992). Management of behavior disturbance in Alzheimer disease: current knowledge and future directions. Alzheimer Dis. Assoc. Disord. 6, 77-88.
Vieta, E., and Garriga, M. (2016). Adjunctive antidepressants in bipolar depression. Lancet Psychiatry 3, 1095–1096.
Vieta, E., Garriga, M., Cardete, L., Bernardo, M., Lombraña, M., Blanch, J., et al. (2017). Protocol for the management of psychiatricpatients with psychomotor agitation. BMC Psychiatry 17:328. doi: 10.1186/s12888-017-1490-0
Villa, L. P., Carracedo, R. A., Iglesias, V. F., Domínguez, L. G., Justo-Alonso, A., Sueiro, M. J. S., et al. (2007). Severe mental disorder. Rev. Electrón. Ter. Ocup. Galicia TOG 4.
Vilibiæ, M., Jukiæ, V., Pandžiæ-Sakoman, M., Bilic, P., and Milosevic, M. (2014). Association between total serum cholesterol and depression, aggression, and suicidal ideations in war veterans with posttraumatic stress disorder: a cross-sectional study. Croat Med J. 55, 520-529 doi: 10.3325/cmj.2014.55.520
Viñado, E. G., Lizano-Díez, I., Arissó, P. N. R., Moreno, J. M. V., and de Viu Bernad, C. M. (2015). El coste económico de los procedimientos de contención mecánica de origen psiquiátrico en España. Psiquiatria biológica 22, 12–16.
Witt, K., van Dorn, R., and Fazel, S. (2013). Risk factors for violence in psychosis: systematic review and meta-regression analysis of 110 studies. PLoS One 8:e55942. doi: 10.1371/journal.pone.0055942
Wittchen, H. U., Jacobi, F., Rehm, J., Gustavsson, A., Svensson, M., Jönsson, B., et al. (2011). The size and burden of mental disorders and other disorders of the brain in Europe 2010. Eur. Neuropsychopharmacol. 21, 655–679. doi: 10.1016/j.euroneuro.2011.07.018
World Health Organization (2018). International Classification of Diseases 11th Revision (ICD-11). Geneva: World Health Organization.
Wu, Y., Kang, R., Yan, Y., Gao, K., Li, Z., Jiang, J., et al. (2018). Epidemiology of schizophrenia and risk factors of schizophrenia-associated aggression from 2011 to 2015. J. Int. Med. Res. 46, 4039–4049. doi: 10.1177/0300060518786634
Keywords: nursing, psychometrics, mental health, psychiatry, psychomotor agitation
Citation: Garrote-Cámara ME, Santolalla-Arnedo I, Ruiz de Viñaspre-Hernández R, Gea-Caballero V, Sufrate-Sorzano T, del Pozo-Herce P, Garrido-García R, Rubinat-Arnaldo E and Juárez Vela R (2021) Psychometric Characteristics and Sociodemographic Adaptation of the Corrigan Agitated Behavior Scale in Patients With Severe Mental Disorders. Front. Psychol. 12:779277. doi: 10.3389/fpsyg.2021.779277
Received: 18 September 2021; Accepted: 04 November 2021;
Published: 08 December 2021.
Edited by:
Bárbara Oliván Blázquez, University of Zaragoza, SpainReviewed by:
María Cruz Pérez-Yus, University of Zaragoza, SpainCopyright © 2021 Garrote-Cámara, Santolalla-Arnedo, Ruiz de Viñaspre-Hernández, Gea-Caballero, Sufrate-Sorzano, del Pozo-Herce, Garrido-García, Rubinat-Arnaldo and Juárez Vela. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Iván Santolalla-Arnedo, aXZhbi5zYW50b2xhbGxhQHVuaXJpb2phLmVz
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.