 Pedro Marques-Quinteiro
Pedro Marques-Quinteiro Ana Margarida Graça
Ana Margarida Graça Francisco Antonio Coelho Jr.
Francisco Antonio Coelho Jr. Daniela Martins
Daniela Martins
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Psychol. , 29 July 2021
Sec. Organizational Psychology
Volume 12 - 2021 | https://doi.org/10.3389/fpsyg.2021.692433
This article is part of the Research Topic From Structure to Agency: Understanding Nurse's Agency in Quality and Safe Care View all 6 articles
This study integrates the job demands-resources model and authentic leadership theory to test the general hypothesis that authentic leadership is a job resource that enables flourishing and performance in healthcare teams. Furthermore, this article tests the hypothesis that the daily bed occupancy is a job demand that weakens this relationship. Participants were 106 nurses that were distributed across 33 teams from two hospitals. The results suggest that the authentic leadership of team leaders is positively related with subjective and objective team performance, but only when daily bed occupancy is low. Authentic leadership had no relationship with team flourishing, regardless of the daily bed occupancy. Our findings suggest that the extent to which authentic leadership is adequate to promote the performance of teams working in a hospital setting is sensitive to contextual boundary conditions. Leading authentically might only be effective under specific circumstances.
Recently, the COVID-19 pandemic has exposed healthcare personnel to tremendous levels of job-related stress. The novelty of the virus, the uncertainty of the most adequate medical procedures, and the unprecedent daily bed occupancy were amongst the main contextual factors that challenged the performance and well-being of healthcare nurses (Zhang et al., 2020). To thrive in such adverse conditions, nurse teams were heavily dependent on the leadership capacity of those in charge (e.g., Hofmeyer et al., 2020). Leadership is at the heart of effective teamwork and the extent to which team leaders enable team effectiveness outcomes such as performance, viability and satisfaction has been extensively supported across meta-analyses and literature reviews (Avolio et al., 2009; Kozlowski et al., 2009). Team leadership has been found to be particularly important in complex work environments such as healthcare, where the performance and the well-being of health professionals such as nurses are often pushed to the limit (e.g., Landeweerd and Boumans, 1994; Wong et al., 2013).
One promising leadership construct that has the potential to enable a high-quality work environment in healthcare is authentic leadership – “i.e., a pattern of transparent and ethical leader behavior that encourages openness in sharing information needed to make decisions while accepting followers’ inputs” (Avolio et al., 2009, p. 423). Authentic leadership is grounded in positive psychology, it is regarded as a way of leading ethically and truthfully, and it holds the promise of leveraging healthier, happier, and productive workplaces (Avolio et al., 2009). Research about authentic leadership is abundant, with studies showing a positive relationship between authentic leadership behaviors, productivity (Lyubovnikova et al., 2017), in-role performance (e.g., extra role behaviors), job satisfaction, and well-being in the workplace (Walumbwa et al., 2008; Mehmood et al., 2016; Hoch et al., 2018). For nurses, authentic leadership enables trustful relations between leaders and followers (Wong and Cummings, 2009), promotes interpersonal collaboration between peers (Regan et al., 2016), and reduces the frequency of adverse patient outcomes (Wong and Giallonardo, 2013).
However, while previous studies have reported a positive relationship between authentic leadership behaviors and leaders’ ratings of team performance (e.g., Lyubovnikova et al., 2017), empirical evidence that established an empirical link between authentic leadership behaviors and team objective performance indicators, and between authentic leadership behaviors and team subjective performance indicators (as rated by the team leader) are scant. Such scarcity of empirical findings limits our capacity to determine if authentic leadership can leave up to its promise, thus preventing theoretical refinement and the development of practical tools that foster authenticity in the workplace (Avolio et al., 2009). What is more, few studies exist that have addressed the relationship between authentic leadership and performance in nurses (e.g., Wong and Laschinger, 2013), or who regarded authentic leadership from a team level perspective (Kellett et al., 2006; Lyubovnikova et al., 2017).
Therefore, the current study aims to integrate the authentic leadership and teamwork literatures by examining the relationship between team leaders’ authentic leadership behaviors and teamwork outcomes in healthcare nurse teams. We do this considering the job demands-resources (JD-R) model, an isomorphic model that can adequately describe individual and team level phenomena in organizations (Bakker and Demerouti, 2017). The current study is then the first to integrate the JD-R model (Bakker and Demerouti, 2017) with the team leadership and the teamwork literatures (e.g., Marques-Quinteiro et al., 2020) to further expand current knowledge on how positive forms of leading can enable effective teamwork in complex work environments such as healthcare.
The JD-R model suggests the bolstering, positive influence of job resources – i.e., the physical, psychological, social, and organizational aspects that enable healthy and productive work (e.g., performing in a psychologically safe team environment) – at the individual and team level of analysis. These resources function as a tool that stimulates personal growth, learning, development and, mainly, they inhibit job demands and the physiological and psychological costs associated with them (Bakker and Demerouti, 2017). Hence, we propose that authentic leadership behaviors could be regarded as a job resource that has a positive relationship with teamwork outcomes, namely, performance and flourishing (Avolio et al., 2009; Laschinger and Fida, 2014), as they regard positive actions that are driven by moral and ethical standards that address team members’ individual and collective needs.
Research by Wong and Laschinger (2013) suggests that nurses who see their supervisors as more authentic (compared to those who do not), report being more satisfied with their job and perceive themselves as having a better performance. Later research by Laschinger and Fida (2014) also suggests that nurses’ supervisor’s authentic leadership behaviors act as resource that mitigates job dissatisfaction and reduces the risk of burnout. Through authentic leadership, team leaders build a positive work environment that is based on authenticity in emotional displays, transparency, and trustworthy relationships and foster self-regulation (Lyubovnikova et al., 2017), making it more likely for team members to engage with the goals and tasks set by their leaders and have a better performance. Furthermore, authentic leadership is associated with flourishing, defined as “the experience of life going well (…) a combination of feeling good and functioning effectively (…) with a high level of mental flourishing, and it epitomizes mental health” (Huppert and So, 2013, p. 838). As authentic leaders expose their team members to positive emotions that lead to optimism, satisfaction, and happiness, it should enable flourishing as an indicator of the well-being of team members (Avolio et al., 2009), Hence, we expect that:
Hypothesis 1: Team leaders’ authentic leadership behaviors are positively related with team flourishing (Hypothesis 1a) and team performance (Hypothesis 1b).
Hospital nurses face daily job demands, such as increased workload, role ambiguity, time pressure and sleep deprivation, which ultimately lead to lower levels of nurses’ well-being and patients’ quality care (e.g., Hemingway and Smith, 1999; Laschinger and Fida, 2014; Hofmeyer et al., 2020; Zhang et al., 2020). The JD-R model suggests that job demands are work environment elements forcing individuals to exert continued effort for prolonged periods (e.g., performing physically demanding tasks under high stress; Bakker and Demerouti, 2017). One contextual element of the healthcare environment is the daily bed occupancy, which provides a direct measure of the entire patient load passing through any given healthcare unit or department and is a direct measure of workload (Tarnow-Mordi et al., 2000; Grundmann et al., 2002; Carayon and Gürses, 2005; Chaudhury et al., 2006). In this study we test if daily bed occupancy – as a job demand – influences the extent to which positive leadership behaviors, such as authenticity, can enable effective teamwork. An increase in daily bed occupancy should add more strain to the teamwork of hospital nurses (Carayon and Gürses, 2005). While authentic leadership behaviors are a job resource that builds a positive work environment (which enables successful teamwork and psychological flourishing), the daily bed occupancy can buffer this relationship and act as a contextual stressor, dampening the positivity that results from authentic leadership behaviors. Consequently, the strength of the positive relationship between authentic leadership as a job resource and teamwork outcomes should be less for a higher number of daily bed occupancy as a job demand. We expect that:
Hypothesis 2: Team leaders’ authentic leadership behaviors are positively related with team flourishing (Hypothesis 2a) and team performance (Hypothesis 2b). This relationship is stronger when daily bed occupancy is low rather than high.
Data was collected in March 2017, at two hospitals in one European capital over one month. After obtaining approval from the ethical committees of both hospitals (who also intervene as participants’ representatives), two students visited the hospital facilities and invited nurse teams to complete an individual and anonymous paper and pencil questionnaire (e.g., surveys asked no information that would identify the participants). At each hospital, students met the in-shift head nurse of each healthcare unit to present the study and ask for their team’s participation. All in-shift head nurses consented with the study and gave permission to invite nurses to fill in the survey. Nurses were also asked to read the survey informed consent before they decide if they would enroll. Nurses’ participation was often contingent on the time they had available to complete the paper and pen survey, which means that the students sometimes had to return another time to collect the data.
Participants were from 33 nurse teams (N = 106 nurses) and their direct supervisors (N = 33 head nurses). The age of the participants ranged between 22 and 64 years old (M = 35.49, SD = 8.97), with 71.9% being female. Regarding participants educational background, 72.7% (n = 101), 15.1% had a degree specialization, and 8.6% had a master’s degree. Team tenure ranged between 1 and 30 years (M = 5.58, SD = 6.60). In Hospital 1, team size ranged between 1 and 6 nurses (M = 5.15, SD = 2.26). In Hospital 2, team size ranged between 3 and 13 (M = 7.21, SD = 2.32).
Authentic leadership was measured using a 15-item scale developed by Walumbwa et al. (2008). Team members were asked to share the frequency their team leader displayed authentic leadership behaviors, using a Likert-type scale ranging from 1 (Never) to 5 (Very frequently, if not always). An example of one item is “My team leader seeks feedback to improve interactions with others.” Cronbach alpha was0.96.
Team flourishing was measured using 8 items from Diener et al. (2010). Team members were asked to share the extent to which they agreed that they experienced flourishing, using a Likert-type scale ranging from 1 (Totally disagree) to 5 (Totally agree). An example of one item is “I am competent and capable in the activities that are important to me.” Cronbach alpha was 0.85.
Team leaders were asked to report the number of beds under their responsibility that were occupied (at survey completion), as a measure of daily bed occupancy.
Team performance was measured using 3 items developed by Aubé and Rousseau (2005). Team leaders were asked to share to what extent they agreed that their team was effective, using a Likert-type scale ranging from 1 (Totally disagree) to 5 (Totally agree). An example of one item is “The members of this team achieve the goals that were set to them.” Cronbach alpha was 0.88. Since leaders’ ratings provide a subjective measure of team performance, we also asked for an objective measure of team performance. Hence, team leaders were asked to report the number of medical discharges during their shift (at survey completion), as an objective measure of team performance as they signal an improvement in patient health status, which is the primary goal of healthcare teams (Guerlain et al., 2005).
Before the research hypotheses could be tested at the team level of analysis, the level of agreement between the ratings of team members (rwg) and the intraclass correlation indexes (ICC1 and ICC2) were estimated (James et al., 1993; Bliese, 2000). The rwg for authentic leadership and flourishing were 0.90 and 0.93, respectively; authentic leadership was ICC(1) 0.15 and ICC(2) 0.40; and flourishing was ICC(1) 0.04 and ICC(2) 0.15. Following recommendations by James et al. (1993) and Bliese (2000), the results of the aggregation indexes were regarded as acceptable to justify the aggregation of individual responses to the team level and continue with hypotheses testing. Even though the ICCs for team flourishing were low, Bliese (2000) suggests that this should not be a reason to discard aggregation as the lower ICC values only make hypothesis testing more conservative.
Table 1 reports the descriptive statistics and correlations. The results displayed in the correlation table show that team leaders authentic leadership behaviors were unrelated with team flourishing (r = 0.21, p = 0.24), team performance (r = 0.16, p = 0.38), and medical discharges (r = −0.003, p = 0.99). The lack of a statistically positive and significant correlation between authentic leadership behaviors and the outcome variables rejects Hypotheses 1a and 1b.
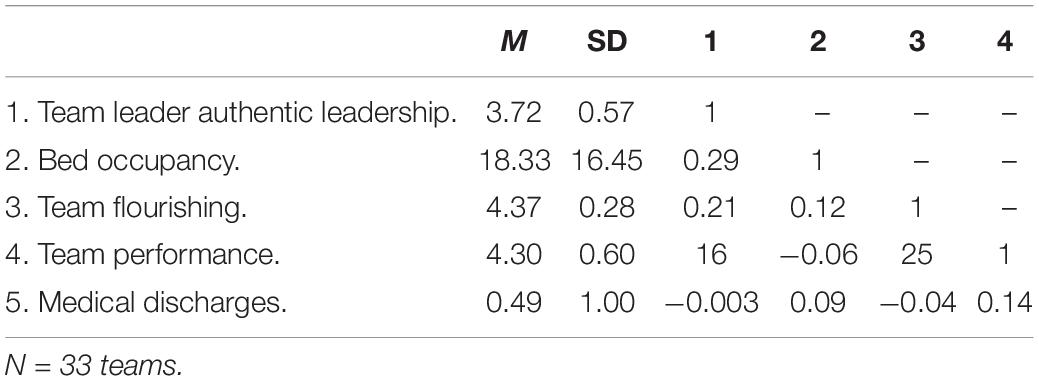
Table 1. Descriptive statistics and correlations.
Hypotheses 2a and 2b were tested using PROCESS for SPSS. The results suggest that daily bed occupancy does not moderate the relationship between team leaders’ authentic leadership and team flourishing, B = 0.001, SE = 0.01, t = 0.24, p = 0.81, 95% CI (−0.009, 0.012). This result rejects Hypothesis 2a.
The results displayed in Table 2 show that daily bed occupancy hinders the relationship between team leaders’ authentic leadership and team performance, B = –0.02, SE = 0.01, t = −2.23, p = 0.033, 95% CI (−0.045, −0.002). This result supports Hypothesis 2b. The interaction graph (left side) displayed in Figure 1 further suggests that the strength of the relationship between the authentic leadership behaviors of nurse team leaders and team performance is stronger at lower levels of daily bed occupancy. When the level of daily bed occupancy increases, authentic leadership behaviors become ineffective to enable good performance.
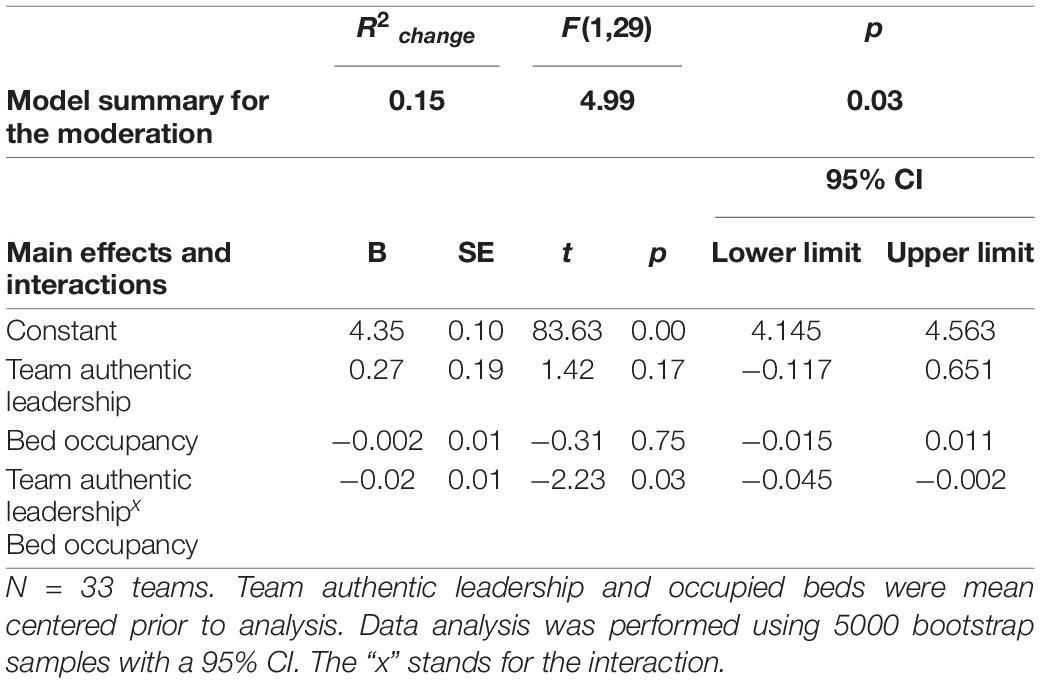
Table 2. Moderation results for team performance as the outcome variable.
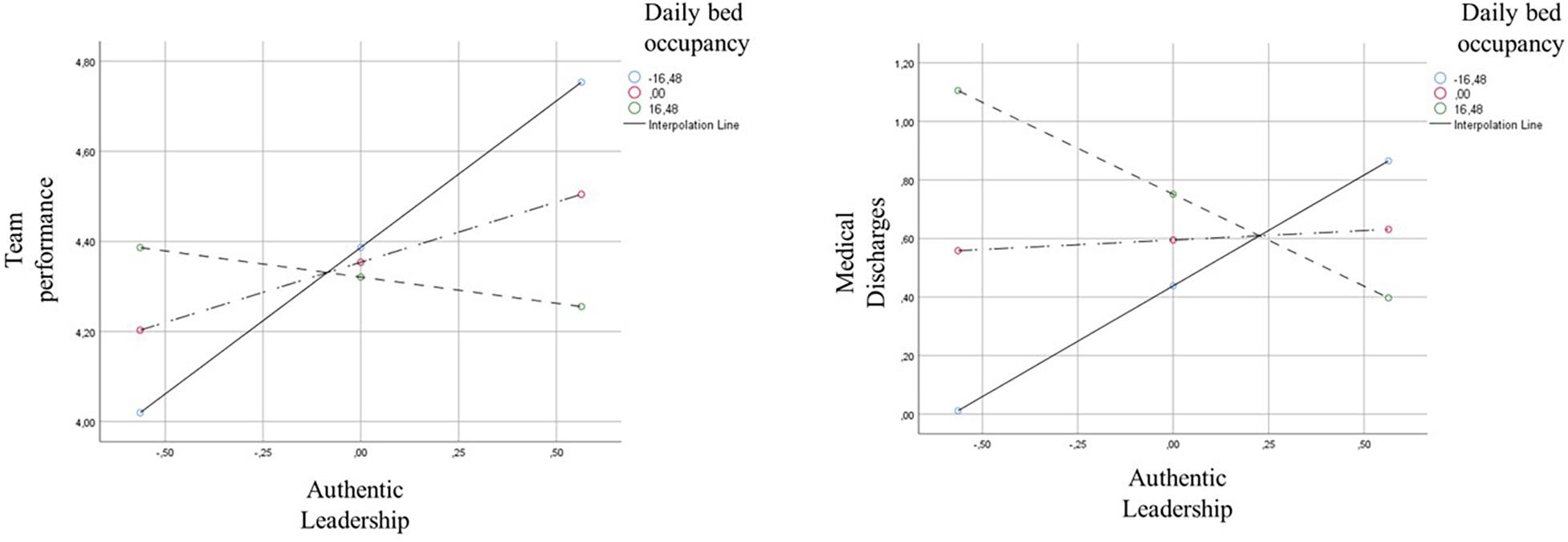
Figure 1. Moderation graphs for the interaction between team leaders’ authentic leadership and daily bed occupancy, regressed on team performance (left graph) and medical discharges (right graph).
Finally, in this study we also collected data on the number of medical discharges as a direct, objective measure of team performance. Like team leaders’ subjective ratings of team performance, the results presented in Table 3 highlight that daily bed occupancy negatively moderates the relationship between team leaders’ authentic leadership and medical discharges, B = –0.04, SE = 0.02, t = −2.38, p = 0.024, 95% CI (−0.078, −0.006). The interaction graph (right side) displayed in Figure 1 further suggests that the strength of the relationship between the authentic leadership behaviors of nurse team leaders and medical discharges is stronger at lower levels of daily bed occupancy. When the level of daily bed occupancy increases, authentic leadership behaviors become ineffective to enable medical discharges.
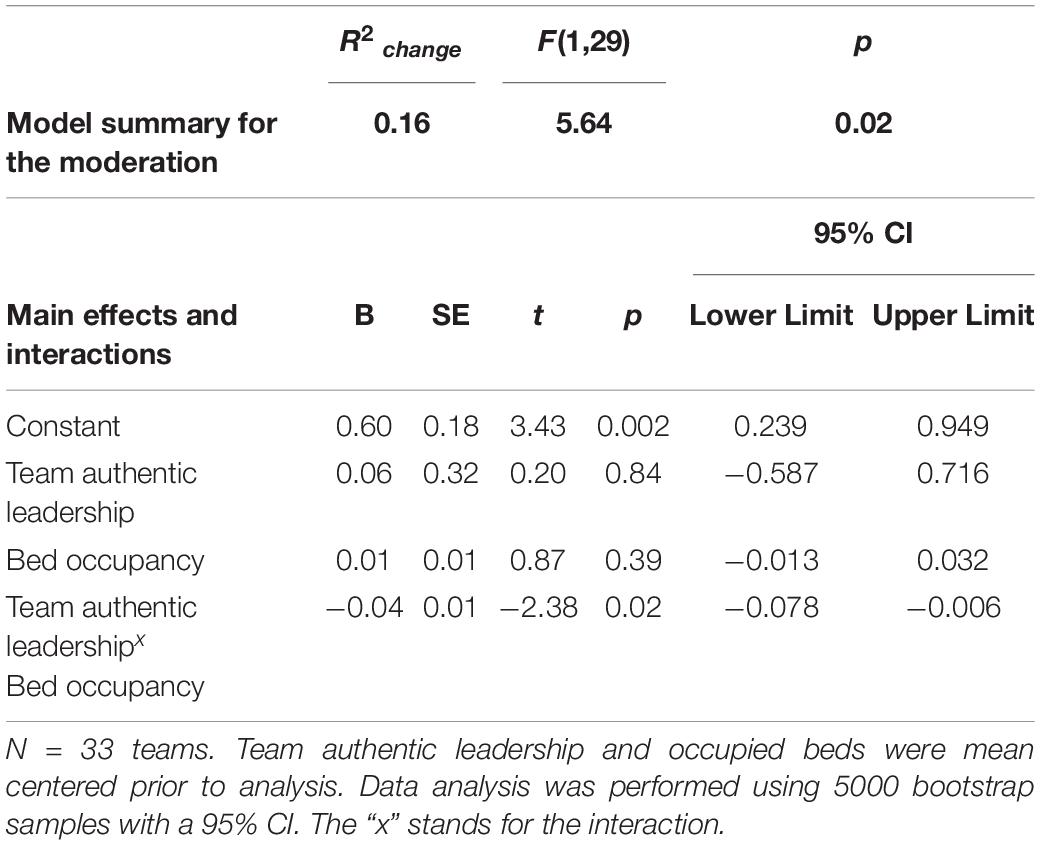
Table 3. Moderation results for medical discharges as the outcome variable.
This study integrated the JD-R model with the team leadership and the teamwork literatures to examine if the relationship between authentic leadership – as a job resource – and teamwork outcomes was sensitive to contextual boundary conditions – the number of occupied beds – as a job demand. The results partially support this hypothesis as they suggest that authentic leadership enables team performance only when the number of occupied beds is low. Additionally, contrary to what was expected, authentic leadership had no positive relationship with team flourishing.
Authentic leadership fosters positive work environments. Hence, studying the relationship between team leadership and teamwork outcomes in unique contexts (such as healthcare) is essential; it can help advance existing knowledge on the boundary conditions that define the relationship between authentic leadership behaviors and team results. Despite recent studies suggesting that authentic leadership enables positive results for individuals and collectives (e.g., Wong et al., 2013; Hoch et al., 2018), for nurses, only when contextual stressors are low does authentic leadership behaviors from the team leader build the expected quality care in the service provided and positive well-being between team members. Hence, as leadership is a process that unfolds in one setting, is sensitive to changes in it, and influences team outcomes (Kozlowski et al., 2009), our findings highlight the importance of context to better understand the relationship between authentic leadership and work-related outcomes.
These results raise some questions on how and in which contexts can an authentic leadership approach be effective and how other leadership approaches could complement authentic leadership to yield more positive organizational outcomes. This study contributes to extend theory on team leadership that has focused more on task-related leadership functions rather than social and psychological state-oriented leadership functions, despite general leadership theories always emphasizing both components (Burke et al., 2006; Avolio et al., 2009). Indeed, there is empirical evidence to demonstrate the importance of social-oriented leadership behaviors (Kozlowski et al., 2009; Morgeson et al., 2010), with leaders listening to team members and being able to manage their needs carefully to integrate those needs and clarify their roles (Graça and Passos, 2015).
Authentic leadership could be conceptualized as one part of social-oriented leadership that has an impact under certain contextual conditions, but other leadership components could be combined with authentic leadership (Hoch et al., 2018) to yield more impactful flourishing and performance results. For example, psychological and well-being states depend highly on feelings of self-efficacy and the team members having the resources and clear goals in place. Research shows that team members have less of an emotional reaction to stressors and, therefore, are in a better psychological state when leaders provide clear team goals, a clear specification of member roles, and unambiguous performance strategies (Zaccaro et al., 2001). This is particularly important in hospital teams, where collaboration and cooperation are enhanced through the definition of the mission and the team identity, the development of shared objectives, and the creation of independent roles for all team members (Landeweerd and Boumans, 1994), leadership actions that can complement authentic leadership behaviors. How leaders set these roles, as well as norms and expectations of interpersonal relationships, can provide direction, motivation, and social integration. This will make it easier to monitor the responses of team members, facilitating future team flourishing and performance. Moreover, specifically in high pressure situations where urgent decisions need to be made, setting goals, providing timely feedback and other task related functions can complement authentic leaders focusing solely on listening carefully to the ideas of others, and not emphasizing their own point of view at the expense of others, behaviors that can be counterproductive to make urgent decisions under high pressure (Sanchez-Manzanares et al., 2020).
Future studies can seek to combine authentic leadership approaches with task-related functions, to see an increase of both affective and objective team outcomes. Future studies could also build on the limitations of this research to test the robustness of our findings and expand them. First, the cross-sectional design in our study can raise concerns about common-method variance and assumptions of causality (Spector, 2019). This could be solved by adopting a temporal data collection approach, where each variable is collected on a different occasion (e.g., one per day; one per week). Alternatively, a longitudinal design could shed light on the temporal dynamics of team leadership and team outcomes, and how these are shaped by context. Second, future studies could also adopt a multilevel research design to test the extent to which contextual features of the nurses’ task environment (including bed occupancy rates), shape how team leadership behaviors collective and individual outcomes (e.g., performance and well-being). Third, the sample size of n = 33 is borderline for the determination of robust moderation effects, which leads us to ask researchers and practitioners to be careful in the generalization of these findings (Marôco, 2018). Future studies should try to replicate our findings using larger sample sizes that allow for more robust assumptions about the relationship between team authentic leadership, bed occupancy rates, team flourishing, and team performance. Finally, the performance of hospital teams is not easily assessed, especially because performance outcome indicators such as infection rate after surgery, patient mortality, and hospital readmissions cannot always be directly related with the quality of team processes (Neuman et al., 2014; Lyubovnikova et al., 2015; Schmutz et al., 2019). As an example, a team can deliver a specific treatment protocol with 100% accuracy, and the patient health condition still worsens. In the case of medical discharges, this might also be a lengthy process, that is dependent on clinical, bureaucratic, and social factors that can override teamwork. Therefore, future studies could consider the adoption of infection rates after treatment or surgery, as well as patient readmission as alternative measures of team performance.
To conclude, the outcomes of our research can be regarded by practitioners aiming to enhance their teams’ performance (especially in healthcare), should be mindful that positive, authentic leadership behaviors enable better team performance in healthcare, except when context adversity (e.g., bed occupancy rate) undermines the authentic leadership behaviors. What is more, leading authentically might not be enough to build positive states in nurse teams.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Comissão de Ética para a Saúde, Hospital Lusíadas Lisboa. The patients/participants provided their written informed consent to participate in this study.
PM-Q and AG wrote the manuscript. PM-Q and DM performed the analysis. FC reviewed the manuscript. DM collected the data. All authors contributed to the article and approved the submitted version.
William James Center for Research, ISPA – Instituto Universitário is financed by FCT (ref. UIDB/04810/2020).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank Catarina Carvalho for her role in data collection.
Aubé, C., and Rousseau, V. (2005). Team goal commitment and team effectiveness: the role of task interdependence and supportive behaviors. Group Dynamics: Theory Res. Pract. 9, 189–204. doi: 10.1037/1089-2699.9.3.189
Avolio, B. J., Walumbwa, F. O., and Weber, T. J. (2009). Leadership: current theories, research, and future directions. Annu. Rev. Psychol. 60, 421–449. doi: 10.1146/annurev.psych.60.110707.163621
Bakker, A. B., and Demerouti, E. (2017). Job demands–resources theory: taking stock and looking forward. J. Occup. Health Psychol. 22, 273–285. doi: 10.1037/ocp0000056
Bliese, P. D. (2000). “Within-group agreement, non-independence, and reliability: implications for data aggregation and analysis,” in Multilevel Theory, Research, and Methods in Organizations: Foundations, Extensions, and New Directions, eds K. J. Klein and S. W. J. Kozlowski (San Francisco, CA: Jossey-Bass), 349–381.
Burke, C. S., Stagl, K. C., Klein, C., Goodwin, G. F., Salas, E., and Halpin, S. M. (2006). What type of leadership behaviors are functional in teams? A meta-analysis. Leadersh. Q. 17, 288–307. doi: 10.1016/j.leaqua.2006.02.007
Carayon, P., and Gürses, A. P. (2005). A human factor engineering conceptual framework of nursing workload and patient safety in intensive care units. Intensive Crit. Care Nurs. 21, 284–301. doi: 10.1016/j.iccn.2004.12.003
Chaudhury, H., Mahmood, A., and Valente, M. (2006). Nurses’ perception of single-occupancy versus multioccupancy rooms in acute care environments: an exploratory comparative assessment. Appl. Nurs. Res. 19, 118–125. doi: 10.1016/j.apnr.2005.06.002
Diener, E., Wirtz, D., Tov, W., Kim-Prieto, C., Choi, D. W., Oishi, S., et al. (2010). New well-being measures: short scales to assess flourishing and positive and negative feelings. Soc. Indic. Res. 97, 143–156. doi: 10.1007/s11205-009-9493-y
Graça, A. M., and Passos, A. M. (2015). Team leadership across contexts: a qualitative study. Leadersh. Organ. Dev. J. 36, 489–511. doi: 10.1108/LODJ-08-2013-0114
Grundmann, H., Hori, S., Winter, B., Tami, A., and Austin, D. J. (2002). Risk factors for the transmission of methicillin-resistant Staphylococcus aureus in an adult intensive care unit: fitting a model to the data. J. Infect. Dis. 185, 481–488. doi: 10.1086/338568
Guerlain, S., Adams, R. B., Turrentine, F. B., Shin, T., Guo, H., Collins, S. R., et al. (2005). Assessing team performance in the operating room: development and use of a “black-box” recorder and other tools for the intraoperative environment. J. Am. Coll. Surg. 200, 29–37. doi: 10.1016/j.jamcollsurg.2004.08.029
Hemingway, M. A., and Smith, C. S. (1999). Organizational climate and occupational stressors as predictors of withdrawal behaviours and injuries in nurses. J. Occup. Organ. Psychol. 72, 285–299. doi: 10.1348/096317999166680
Hoch, J. E., Bommer, W. H., Dulebohn, J. H., and Wu, D. (2018). Do ethical, authentic, and servant leadership explain variance above and beyond transformational leadership? A meta-analysis. J. Manag. 44, 501–529. doi: 10.1177/0149206316665461
Hofmeyer, A., Taylor, R., and Kennedy, K. (2020). Fostering compassion and reducing burnout: how can health system leaders respond in the Covid-19 pandemic and beyond? Nurse Educ. Today 94:104502. doi: 10.1016/j.nedt.2020.104502
Huppert, F. A., and So, T. T. C. (2013). Flourishing across Europe: application of a new conceptual framework for defining well-being. Soc. Indic. Res. 110, 837–861. doi: 10.1007/s11205-011-9966-7
James, L. R., Demaree, R. G., and Wolf, G. (1993). rwg: an assessment of within-group interrater agreement. J. Appl. Psychol. 78, 306–309. doi: 10.1037/0021-9010.78.2.306
Kellett, J. B., Humphrey, R. H., and Sleeth, R. G. (2006). Empathy and the emergence of task and relations leaders. Leadersh. Q. 17, 146–162. doi: 10.1016/j.leaqua.2005.12.003
Kozlowski, S. W. J., Watola, D. J., Jensen, J. M., Kim, B. H., and Botero, I. C. (2009). “Developing adaptive teams: a theory of dynamic team leadership,” in The Organizational Frontiers Series. Team Effectiveness in Complex Organizations: Cross-Disciplinary Perspectives and Approaches, eds E. Salas, G. F. Goodwin, and C. S. Burke (New York, NY: Taylor & Francis Group), 113–155. doi: 10.4135/9781483349169.n6
Landeweerd, J. A., and Boumans, N. P. (1994). The effect of work dimensions and need for autonomy on nurses’ work satisfaction and health. J. Occup. Organ. Psychol. 67, 207–217. doi: 10.1111/j.2044-8325.1994.tb00563.x
Laschinger, H. K. S., and Fida, R. (2014). New nurses burnout and workplace wellbeing: the influence of authentic leadership and psychological capital. Burn. Res. 1, 19–28. doi: 10.1016/j.burn.2014.03.002
Lyubovnikova, J., Legood, A., Turner, N., and Mamakouka, A. (2017). How authentic leadership influences team performance: the mediating role of team reflexivity. J. Bus. Ethics 141, 59–70. doi: 10.1007/s10551-015-2692-3
Lyubovnikova, J., West, M. A., Dawson, J. F., and Carter, M. R. (2015). 24-Karat or fool’s gold? Consequences of real team and co-acting group membership in healthcare organizations. Eur. J. Work Organ. Psychol. 24, 929–950. doi: 10.1080/1359432X.2014.992421
Marôco, J. (2018). Análise Estatística com o SPSS Statistics, 7a edição Edn. Pero Pinheiro: ReportNumber, Lda.
Marques-Quinteiro, P., Santos, C. M. D., Costa, P., Graça, A. M., Marôco, J., and Rico, R. (2020). Team adaptability and task cohesion as resources to the non-linear dynamics of workload and sickness absenteeism in firefighter teams. Eur. J. Work Organ. Psychol. 29, 525–540. doi: 10.1080/1359432X.2019.1691646
Mehmood, Q., Hamstra, M. R., Nawab, S., and Vriend, T. (2016). Authentic leadership and followers’ in-role and extra-role performance: the mediating role of followers’ learning goal orientation. J. Occup. Organ. Psychol. 89, 877–883. doi: 10.1111/joop.12153
Morgeson, F. P., DeRue, D. S., and Karam, E. P. (2010). Leadership in teams: a functional approach to understanding leadership structures and processes. J. Manag. 36, 5–39. doi: 10.1177/0149206309347376
Neuman, M. D., Wirtalla, C., and Werner, R. M. (2014). Association between skilled nursing facility quality indicators and hospital readmissions. JAMA 312, 1542–1551. doi: 10.1001/jama.2014.13513
Regan, S., Laschinger, H. K., and Wong, C. A. (2016). The influence of empowerment, authentic leadership, and professional practice environments on nurses’ perceived interprofessional collaboration. J. Nurs. Manag. 24, E54–E61. doi: 10.1111/jonm.12288
Sanchez-Manzanares, M., Rico, R., Antino, M., and Uitdewilligen, S. (2020). The joint effects of leadership style and magnitude of the disruption on team adaptation: a longitudinal experiment. Group Organ. Manag. 45, 836–864. doi: 10.1177/1059601120958838
Schmutz, J. B., Meier, L. L., and Manser, T. (2019). How effective is teamwork really? The relationship between teamwork and performance in healthcare teams: a systematic review and meta-analysis. BMJ Open 9:e028280. doi: 10.1136/bmjopen-2018-028280
Spector, P. E. (2019). Do not cross me: optimizing the use of cross-sectional designs. J. Bus. Psychol. 34, 125–137. doi: 10.1007/s10869-018-09613-8
Tarnow-Mordi, W. O., Hau, C., Warden, A., and Shearer, A. J. (2000). Hospital mortality in relation to staff workload: a 4-year study in an adult intensive-care unit. Lancet 356, 185–189. doi: 10.1016/s0140-6736(00)02478-8
Walumbwa, F. O., Avolio, B. J., Gardner, W. L., Wernsing, T. S., and Peterson, S. J. (2008). Authentic leadership: development and validation of a theory-based measure. J. Manag. 34, 89–126. doi: 10.1177/0149206307308913
Wong, C. A., and Cummings, G. (2009). Authentic leadership: a new theory for nursing or back to basics? J. Health Organ. Manag. 23, 522–538. doi: 10.1108/14777260910984014
Wong, C. A., Cummings, G. G., and Ducharme, L. (2013). The relationship between nursing leadership and patient outcomes: a systematic review update. J. Nurs. Manag., 21, 709–724. doi: 10.1111/jonm.12116
Wong, C. A., and Giallonardo, L. M. (2013). Authentic leadership and nurse-assessed adverse patient outcomes. J. Nurs. Manag. 21, 740–752. doi: 10.1111/jonm.12075
Wong, C. A., and Laschinger, H. K. (2013). Authentic leadership, performance, and job satisfaction: the mediating role of empowerment. J. Adv. Nurs. 69, 947–959. doi: 10.1111/j.1365-2648.2012.06089.x
Zaccaro, S. J., Rittman, A. L., and Marks, M. A. (2001). Team leadership. Leadersh. Q. 12, 451–483. doi: 10.1016/S1048-9843(01)00093-5
Keywords: authentic leadership, job demands-resources model, performance, nurses, flourishing at work
Citation: Marques-Quinteiro P, Graça AM, Coelho FA Jr and Martins D (2021) On the Relationship Between Authentic Leadership, Flourishing, and Performance in Healthcare Teams: A Job Demands-Resources Perspective. Front. Psychol. 12:692433. doi: 10.3389/fpsyg.2021.692433
Received: 08 April 2021; Accepted: 09 July 2021;
Published: 29 July 2021.
Edited by:
Con Stough, Swinburne University of Technology, AustraliaReviewed by:
Lei Yao, Beijing Normal University, ChinaCopyright © 2021 Marques-Quinteiro, Graça, Coelho and Martins. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pedro Marques-Quinteiro, cHF1aW50ZWlyb0Bpc3BhLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.