
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol. , 16 August 2021
Sec. Health Psychology
Volume 12 - 2021 | https://doi.org/10.3389/fpsyg.2021.680614
This article is part of the Research Topic Occupational Health Psychology: From Burnout to Well-being at Work View all 22 articles
 Xin Zhang1,2†
Xin Zhang1,2† Jiahui Wang1,2†
Jiahui Wang1,2† Yanhua Hao1,2†Ke Wu3
Yanhua Hao1,2†Ke Wu3 Mingli Jiao1,2Libo Liang1,2Lijun Gao1,2
Mingli Jiao1,2Libo Liang1,2Lijun Gao1,2 Ning Ning1,2Zheng Kang1,2Linghan Shan1,2Wenfeng He4Yongchen Wang5
Ning Ning1,2Zheng Kang1,2Linghan Shan1,2Wenfeng He4Yongchen Wang5 Qunhong Wu1,2*Wenqiang Yin6*
Qunhong Wu1,2*Wenqiang Yin6*Objectives: The sudden outbreak of the novel coronavirus disease (COVID-19) plunged healthcare workers (HCWs) into warfare. This study aimed to determine the prevalence of burnout and the factors associated with it among frontline HCWs fighting COVID-19.
Methods: A cross-sectional survey was conducted among frontline HCWs fighting against the COVID-19 in Wuhan, Harbin, and Shenzhen during the period from February 18 to March 4. Finally, HCWs were recruited using cluster sampling, 1,163 HCWs were included in the final analysis. Burnout was measured using a 22-item Maslach Burnout Inventory scale (MBI scale).
Results: Of the participants, 48.6% suffered from burnout, and 21.8% showed a high degree of burnout. Doctors (b = 3.954, P = 0.011) and nurses (b = 3.067, P = 0.042) showed higher emotional exhaustion (EE) than administrators. Participants who worked continuously for more than 8 h a day (b = 3.392, P = 0.000), those who were unable to eat three regular daily meals (b = 2.225, P = 0.008), whose daily water intake was no more than 800 ml (b = 3.007, P = 0.000), who slept for no more than 6 h (b = 1.609, P = 0.036), and who were infected or had colleagues who were infected with COVID-19 (b = 4.182, P = 0.000) experienced much higher levels of EE, while those who could adhere to infection control procedures (b = −5.992, P = 0.000), who were satisfied with their hospital’s infection control measures(b = −3.709, P = 0.001), and who could receive sufficient psychological crisis intervention (b = −1.588, P = 0.039) reported lower levels of EE.
Conclusion: The study reveals that burnout is prevalent among frontline HCWs and that the known factors associated with burnout, such as workload, and the factors directly associated with COVID-19, such as having insufficient protection, can affect burnout symptoms in frontline HCWs. Synergized and comprehensive interventions should be targeted at reducing its occurrence among frontline HCWs fighting COVID-19.
The novel coronavirus disease (COVID-19) pandemic is a global public health emergency which has greatly impacted health systems and people’s lives worldwide. The COVID-19 pandemic has posed unprecedented challenges to the global health system (Lai et al., 2020), public health laboratories (Corman et al., 2020), hospitals, and critical care departments (Arabi et al., 2020). Healthcare systems and personnel were, for a time, overstretched and overwhelmed. Many frontline healthcare workers (HCWs) have experienced the darkest period of their professional lives. To fulfill their commitment to the responsibilities and obligations of the medical profession, frontline HCWs have done their utmost to rescue the dying and heal the wounded, diagnosing, treating, and nursing COVID-19 patients around the clock. Thus, frontline HCWs fighting against the COVID-19 pandemic have faced severe challenges and have experienced more health problems than non-frontline HCWs, including burnout symptoms, depressive symptoms, and insomnia (Şahin et al., 2020; Serrão et al., 2021), mental health of frontline HCWs fighting against the COVID-19 pandemic is a problem which require attention.
Burnout has been a major concern in the fields of both occupational health and mental health (Wu et al., 2013; Arabi et al., 2020). The outbreak of COVID-19 triggered widespread alarm among HCWs about the potential for burnout. In Asia, according to Li D et al., 34.2% of HCWs from Wuhan Jinyintan Hospital experienced COVID-19 related burnout (Li et al., 2021). Another study developed in China showed that during the COVID-19 pandemic 36.5% of Chinese HCWs experienced burnout (Huo et al., 2021). Matsuo et al. found that the prevalence of burnout among HCWs in Japan during the COVID-19 outbreak was 31.4% (Matsuo et al., 2020). According to Khasne RW et al., more than half (52.8%) of HCWs in India experienced COVID-19-related burnout (Khasne et al., 2020). According to Alsulimani LK et al., the prevalence of burnout among HCWs in Saudi Arabia, which has one of the best healthcare systems in the Middle East (AlHumaid et al., 2020),was 75% during the COVID-19 pandemic (Alsulimani et al., 2021). In Europe, Italy was severely impacted by COVID-19, and Italian HCWs reported relevant work-related burnout symptoms (Barello et al., 2020; Lasalvia et al., 2021). According to MD Trani, 56% of HCWs in Italy showed EE (Di Trani et al., 2021). In Portugal, Duarte I et al. concluded that more than half of HCWs had symptoms of personal burnout (Duarte et al., 2020). In Africa, owing to both the COVID-19 pandemic and civil war, 67.1% of Libyan HCWs reported having EE (Elhadi et al., 2020). Although the relationship between burnout symptoms and the COVID-19 pandemic has been proved, further research about the risk factors and how to alleviate burnout symptoms among frontline HCWs fighting against COVID-19 is still needed.
HCWs often work under great pressure and experience negative emotions owing to the nature of their work (Huo et al., 2021). Against the background of the COVID-19 outbreak, HCWs have faced more pressure than usual, every frontline HCW has faced enormous pressure. A recent study has reconfirmed the negative impact of the long-lasting pandemic in Saudi Arabia among healthcare students (Shaikh et al., 2021). HCWs were exposed to increased pressure, excessive workloads, extended work hours (Huo et al., 2021), and sleep deprivation—all of which are well-documented factors leading to burnout (Wang et al., 2005; Németh, 2016). Under the extraordinary conditions of the pandemic, HCWs have had insufficient protection against the disease and an increased risk of nosocomial infection (Centers for Disease Control and Prevention, 2008). Scholars have demonstrated the relationship between insufficient protection and anxiety and depression among HCWs during the COVID-19 pandemic (Pouralizadeh et al., 2020; Cag et al., 2021). The heavy workload, disruption of quotidian routines, and risk of COVID-19 infection experienced by HCWs owing to the pandemic all negatively affect the health of frontline HCWs. Chinese HCWs rose to the challenge, they grappled with the epidemic at the front line across the country, during the pandemic. However, to the best of our knowledge, scant research has specifically focused on both the known factors of burnout, such as excessive workload, and the factors directly associated with COVID-19 among Chinese HCWs. Therefore, the relationship between factors related to COVID-19 and burnout still needs to be explored in China.
Burnout is related to a wide range of harmful health outcomes, such as insomnia (Salvagioni et al., 2017), depression (Lu et al., 2020), loss of enthusiasm for work (Christian, 2015), decreased job satisfaction (Khamisa et al., 2015), resignation and early retirement (Khan et al., 2018), an increased risk of suicide (Johnson et al., 2018), and death by overwork (Yang et al., 2019). Most countries are currently under the double pressure of economic recovery and COVID-19 control, and thus must confront numerous challenges. For example, many governments have been reimposing and subsequently lifting restrictions according to new developments of the coronavirus disease. At the time of writing, new variants of COVID-19 have caused surges of the disease in the United Kingdom (Kirby, 2021). The Chinese government has implemented strategies for the ongoing prevention and control of COVID-19, as sporadic cases of the disease on the mainland have continued to be reported (The State Council Information Office of the People’s Republic of China, 2020). As HCWs worldwide need to not only perform their routine tasks, but also be alert to the danger of COVID-19, they are continually encountering the risk factors for burnout, and thus it is critical to alleviate HCWs’ burnout symptoms to maintain their mental and physical health, which Ali, S. et al. posited is a prerequisite for conquering the pandemic (Ali et al., 2020a). HCWs are on the frontline of this battle and are the last line of defence against COVID-19.
In this study, we aim to contribute to the knowledge of health systems worldwide by determining the prevalence and risk factors for burnout syndrome among frontline HCWs battling COVID-19 in China. Our study was conducted during an extraordinary period of the pandemic, in the time periods categorized by the Chinese government as Stage II (Initial Progress in Containing the Virus) and Stage III (Newly Confirmed Domestic Cases on the Chinese Mainland Drop to Single Digits) (The State Council Information Office of the People’s Republic of China, 2020). We propose that effective methods for alleviating burnout symptoms could be obtained by exploring the risk factors associated with burnout among frontline HWCs. Our research findings provide healthcare professionals and policy makers implications for the future surges of COVID-19 in a country or region. This study is valuable as we examine not only the known factors of burnout, such as workload, excessive working hours, diet, and sleep deprivation, but also the specific factors associated with COVID-19, such as HCWs’ infection protection and infection status.
A cross-sectional survey was conducted among COVID-19 frontline HCWs in China from 1 February 8 to March 4, 2020, as China was going through Stage II and Stage III of the pandemic (The State Council Information Office of the People’s Republic of China, 2020). Our study’s participants were selected through cluster sampling. We identified three cities—Wuhan, Harbin, and Shenzhen—representing areas which were severely impacted by COVID-19. We used the formula:. The necessary sample size was 246 for each city, and after considering issues related to questionnaire recovery and efficiency, we added 10% to this total sample size. Ultimately, the minimum necessary sample size was 273 for each city. Our survey targeted three hospitals in each city, and we communicated with the hospital deans directly via personal contacts or email. We clarified significance and importance of our study to deans, if they indicated the willingness to join our study, deans of hospitals clarified significance and importance of our study to HCWs, frontline HCWs who were working in the departments related to COVID-19 were invited to participate in the survey. Finally, we recruited participants through eight hospitals—three in Wuhan, three in Harbin, and two in Shenzhen.
HCWs answered the questionnaires during their breaks from work. Only completed questionnaires can be submitted. A total of 1,389 subjects completed the questionnaire. As the inclusion criterion was HCWs on the COVID-19 frontlines, the respondents were asked to answer the question, “Are you a frontline healthcare worker who is working for patients with COVID-19, such as diagnosing, treating, or nursing patients with COVID-19?”; 217 respondents were excluded from the survey. The research team reviewed the questionnaires, and excluded questionnaires in which most answers were the same; nine questionnaire respondents were excluded. Finally, 1,163 valid questionnaires were included (effective rate = 83.73%), among them 570 HCWs from Wuhan, 312 HCWs from Harbin, and 281 HCWs from Shenzhen. The participants were all recruited from capital cities and worked in tertiary public hospitals (Figure 1).
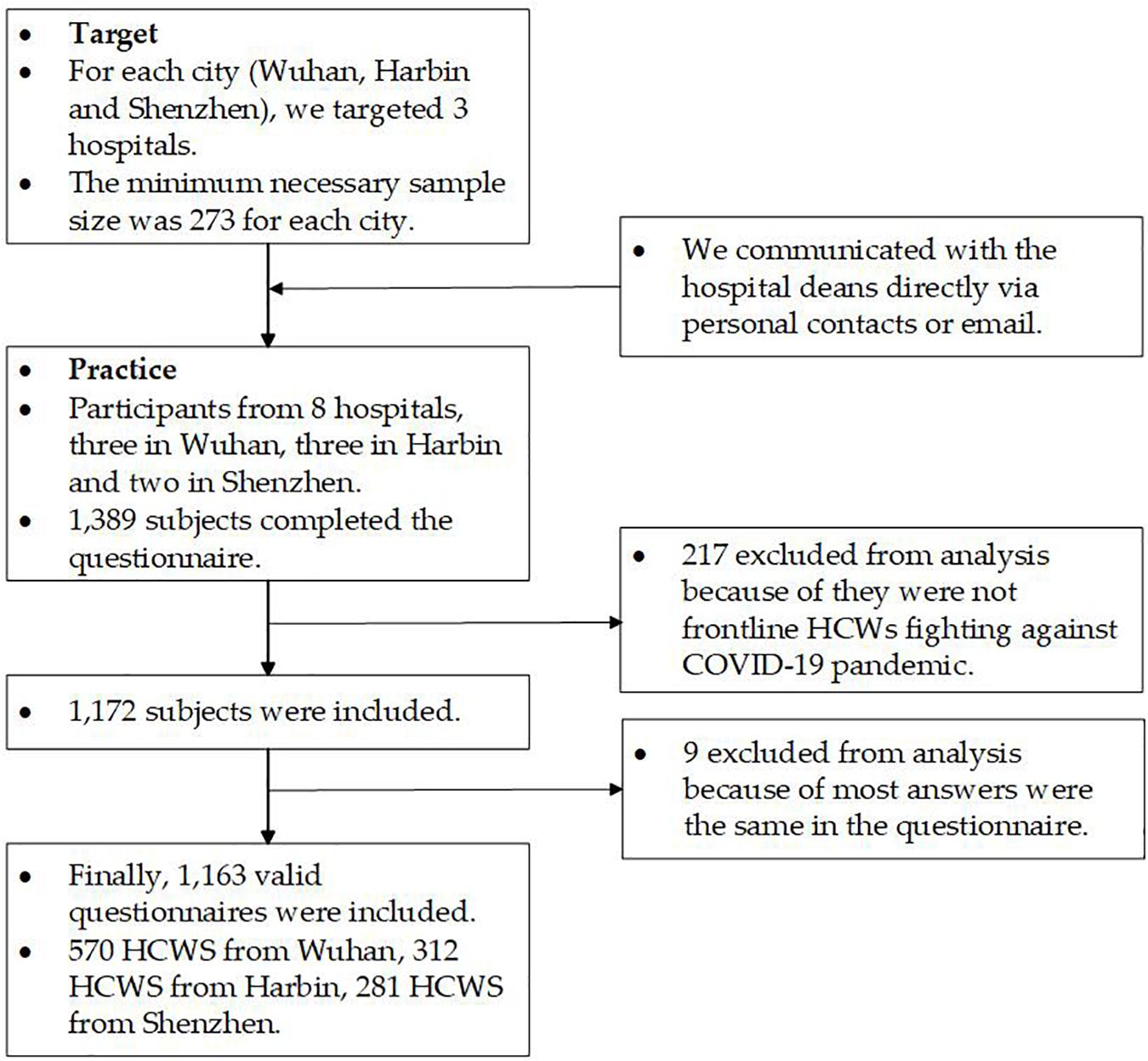
Figure 1. Study flow diagram.
We received approval from the ethics committee of Harbin Medical University to conduct this study (Harbin, Heilongjiang, China), ID: HMUIRB20200003.
Our instrument comprised items on participants’ demographic information, the Maslach Burnout Inventory (MBI) scale, work situation, diet and sleep patterns, status of infection protection, status of COVID-19 infection of themselves and their colleagues, and status of psychological crisis intervention.
The basic socio-demographic information included age, gender, and job category. The job category was grouped into four types: nurses, doctors, technicians, and administrators.
Burnout among participants was assessed using the MBI scale. The MBI scale contains 22 items (Maslach et al., 1996). In this study, we used the Chinese version revised by Li and Liu (2000). The subscales included emotional exhaustion (EE, 9 items), depersonalisation (DP, 5 items), and personal accomplishment (PA, 8 items). All items were scored on a seven-point Likert scale, ranging from 0 (never) to 6 (every day). As in previous studies and according to convention, burnout was defined as high EE (scores of 27 or greater) and/or high DP (scores of 10 or greater) as opposed to a total score (Maslach and Jackson, 1981; Rotenstein et al., 2018; West et al., 2018). Higher scores on the EE and DP subscales indicate a higher burnout symptom, while PA was inversely associated with burnout (Gan et al., 2019; Brady et al., 2020). The low PA defined as scores of 33 or lower (Bourne et al., 2019). HCWs were categorised as having a high level of burnout if they scored high on EE and DP and low on PA (Gan et al., 2019).
In the reliability and validity analysis of MBI scale, the first point to consider about variables is internal consistency reliability. Cronbach’s α for the whole scale was 0.930; 0.936 for the EE subscale; 0.859 for the DP subscale; and 0.877 for the PA subscale; all of which demonstrated a high level of reliability. The second point to consider about variables is validity. The validity check is done in two stages as convergent validity and discriminant validity. The composite reliability (CR) and the explained average variance extracted (AVE) values were considered for convergent validity. The discriminant validity of all constructs met the Fornell and Larcker criteria (Fornell and Larcker, 1981). Table 1 presents a summary of the factor loadings, CR, AVE, and convergence validity. The standardized factor loadings of items are between 0.552 and 0.863, with good item reliability. The CR values of the 3 constructs range from 0.855 to 0.924, exceeding 0.7 (Hair et al., 2011). The AVE value of EE and DP constructs were higher than the threshold of 0.5, and the AVE value of PA constructs was closed to 0.5, which confirms the constructs’ convergent validity (Ye et al., 2019). Also, X2/df = 7.673, the comparative fit index = 0.927, the Tucker-Lewis fit index = 0.910, and the root mean square error of approximation = 0.076. The MBI scale showed acceptable reliability and validity (Table 1).
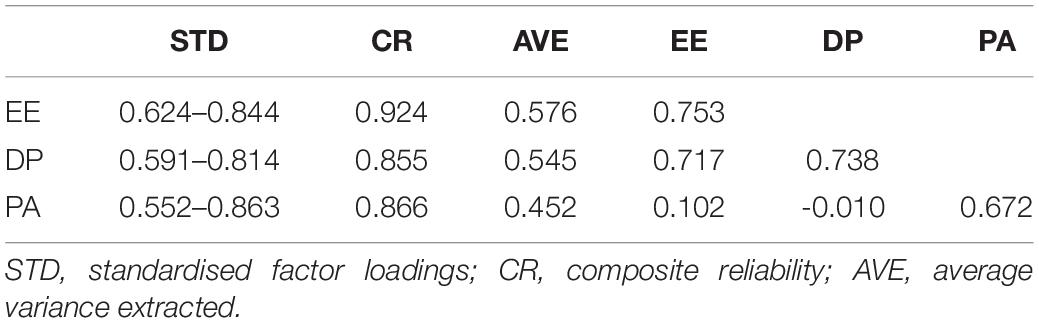
Table 1. Convergent validity and discriminant validity.
Participants’ work situations were assessed with one open-ended question: “How many hours do you work every day?”.
Participants’ diet and sleep patterns were assessed with one item: “Are you able to eat three regular daily meals?” to which they answered yes or no, and two open-ended questions: “How many millilitres (ml) of water do you drink every day?” and “How many hours did you sleep per day in the past week?”
Participants’ status of infection protection were assessed with two items: “Could you adhere to infection control procedures?” and “Are you satisfied with the hospitals’ infection control measures?” to which they answered yes or no.
The status of COVID-19 infection of participants and their colleagues were assessed with two items: “Have you ever been infected with COVID-19?” and “Have your colleagues ever been infected with COVID-19?” to which they answered yes or no.
The status of psychological crisis intervention were assessed with one item: “Could you receive sufficient psychological crisis intervention?” to which they answered yes or no.
IBM® SPSS® Statistics 25.0, Mplus Version 7.0 and STATA 16.0 were used for the data analysis in this study. Heterogeneity analysis were computed using STATA 16.0. Heterogeneity were assessed using the I2 statistic. We explored the heterogeneity of age, gender, EE, DP, and PA among Wuhan, Harbin and Shenzhen, the results showed that there was no statistical significance between age (I2 = 0.0%, P = 0.965), gender (I2 = 0.0%, P = 0.990), EE(I2 = 0.0%, P = 0.983), DP(I2 = 0.0%, P = 0.982), and PA (I2 = 0.0%, P = 0.827) and location. Validity of MBI scale was tested using MplusVersion 7.0 (Muthén and Muthén, 1998–2012). The t-test, ANOVA test, and multiple linear regression were tested using IBM SPSS Statistics 25.0. The t-test and ANOVA test were performed to assess whether the independent variables were statistically significant. Stepwise multiple linear regression analysis was used to estimate the predictors of HCWs’ burnout and its three subscales. The significance level was set at 0.05.
The analysis revealed that burnout is widespread. High EE was found in 434 participants (37.3%), 466 participants (40.1%) showed high DP, and 750 participants (64.5%) showed low PA. Of the participants, 565 (48.6%) exhibited burnout. Of these 565 participants, 254 (21.8% of all participants) showed a high degree of burnout.
The number of missing responses and items that were answered with “not applicable” are shown in Table 1 and ranged from 0.8 to 2.1%. Characteristics of subjects and distributions of each dimension of burnout in categorical items are also shown in Table 1. Among the participants, 72.3% were female and 27.7% were male, and 45.7% were older than or aged 35. Mean PA differed between age groups (t = −2.030, P = 0.043). Of these, 55.2% were nurses, 27.0% were doctors, 10.7% were technicians, and 7.1% were administrators. Mean EE (F = 6.741, P = 0.000), mean DP (F = 7.103, P = 0.000), and mean PA (F = 4.178, P = 0.006) differed between job category groups. Doctors had higher EE scores and higher DP scores than administrators (Table 2).
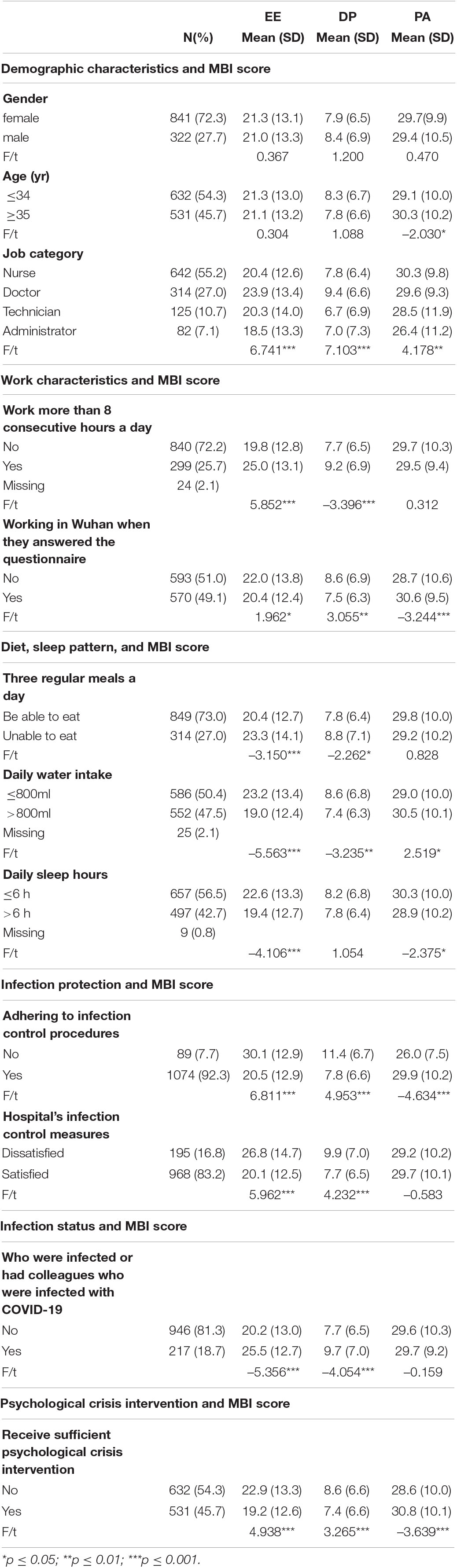
Table 2. Descriptive statistics and univariate analysis results.
Of the participants, 25.7% worked more than 8 consecutive hours a day and showed higher EE scores (t = −5.852, P = 0.000) and higher DP scores (t = −3.396, P = 0.001). Nearly half of the participants (49.1%) were working in Wuhan when they answered the questionnaire and showed lower EE scores (t = 1.962, P = 0.050), lower DP scores (t = 3.055, P = 0.002), and higher PA scores (t = −3.244, P = 0.001) (Table 2).
A total of 27.0% of the participants expressed that they were unable to eat three regular daily meals and showed higher EE scores (t = −3.150, P = 0.001) and higher DP scores (t = −2.262, P = 0.018). A total of 50.4% of the participants drank no more than 800 ml of water every day and showed higher EE scores (t = −5.563, P = 0.000), higher DP scores (t = −3.235, P = 0.010), and lower PA scores (t = 2.519, P = 0.012). The average amount of sleep obtained by participants was 6–1/2 h per day in the past week while 56.5% slept for no more than 6 h per day and showed higher EE scores (t = −4.106, P = 0.000) and higher PA scores (t = −2.375, P = 0.018) (Table 2).
A total of 7.7% of the participants reported that they could not adhere to infection control procedures and showed higher EE scores (t = 6.811, P = 0.000), higher DP scores (t = 4.953, P = 0.000), and lower PA scores (t = −4.634, P = 0.000) than those who could adhere to infection control procedures. Among the participants, 16.8% were “dissatisfied” and 83.2% were “satisfied” with their hospital’s infection control measures. Participants who reported “dissatisfied” showed higher EE scores (t = 5.962, P = 0.000) and higher DP scores (t = 4.232, P = 0.000).
A total of 946 participants (81.3%) reported that neither themselves nor their colleagues were infected while 217 participants (18.7%) reported that they or their colleagues were infected. Among the 217 participants, 65 (5.6%) reported that they were infected, 213 (18.3%) reported that their colleagues were infected, and 61 (5.2%) reported that both themselves and their colleagues were infected. Participants who reported that they or their colleagues were infected showed higher EE scores (t = −5.356, P = 0.000) and higher DP scores (t = −4.054, P = 0.000) (Table 2).
Of the participants, 54.3% reported that they did not receive sufficient psychological crisis intervention and showed higher EE scores (t = 4.938, P = 0.000), higher DP scores (3.265, P = 0.001), and lower PA scores (t = −3.639, P = 0.000) than those who expressed that they did receive sufficient psychological crisis intervention (Table 2).
Participants worked an average of 8.1 ± 4.2 h per day. The average working hours for nurses, doctors, technicians, and administrators were 6.7, 9.9, 9.6, and 9.6 h per day, respectively (F = 57.249, P = 0.000) (Table 3).
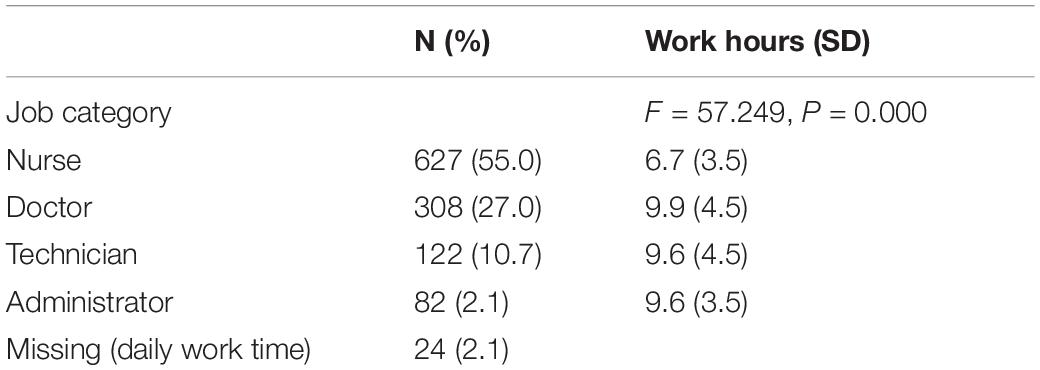
Table 3. Average working hours for participants with different characteristics.
Participants who were nurses (b = 3.067, P = 0.042), who were doctors (b = 3.954, P = 0.011), who were working continuously for more than 8 h a day (b = 3.392, P = 0.000), who were unable to eat three regular daily meals (b = 2.225, P = 0.008), whose daily water intake was no more than 800 ml (b = 3.007, P = 0.000), who obtained no more than 6 h of sleep a day (b = 1.609, P = 0.036), and who were infected or had colleagues who were infected with COVID-19 (b = 4.182, P = 0.000) were more likely to experience high EE. Participants who could adhere to infection control procedures (b = −5.992, P = 0.000), who were satisfied with their hospital’s infection control measures (b = −3.709, P = 0.001), and who could receive sufficient psychological crisis intervention (b = −1.588, P = 0.039) were more likely to experience lower EE (Table 4).
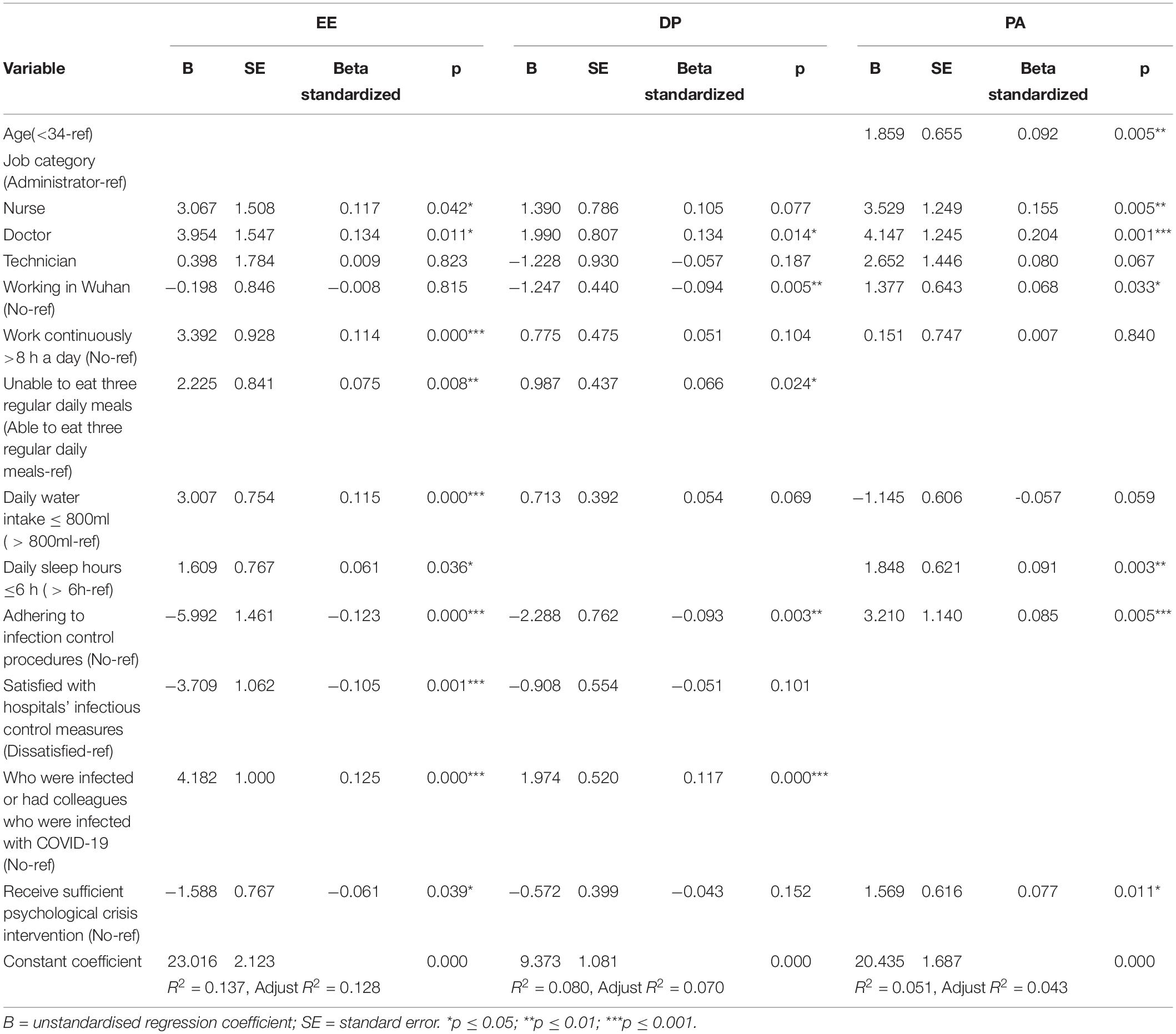
Table 4. Multiple linear regression analysis results for EE, DP, and PA.
Participants who were doctors (b = 1.990, P = 0.014), who were unable to eat three regular daily meals (b = 0.987, P = 0.024), and who were infected or had colleagues who were infected with COVID-19 (b = 1.974, P = 0.000) were more likely to experience higher DP. Participants who were working in Wuhan (b = −1.247, P = 0.005) and who could adhere to infection control procedures (b = −2.288, P = 0.003) were more likely to experience lower DP (Table 4).
Participants who were aged ≥35 (b = 1.859, P = 0.005), who were nurses (b = 3.529, P = 0.005), who were doctors (b = 4.147, P = 0.001), who were working in Wuhan (b = 1.377, P = 0.033), who got no more than 6 h of sleep a day (b = 1.848, P = 0.003), who could adhere to infection control procedures (b = 3.210, P = 0.005), and who could receive sufficient psychological crisis intervention (b = 1.569, P = 0.011) were more likely to experience higher PA (Table 4).
Frontline HCWs battling COVID-19 exhibited a high level of burnout in China. According various studies, the prevalence of burnout in HCWs in Asia during the COVID-19 pandemic varies from 31.4 to 75% (Khasne et al., 2020; Matsuo et al., 2020; Alsulimani et al., 2021; Huo et al., 2021). The large differences across these studies may result from regional disparities and variations in burnout definitions and assessment methods (Rotenstein et al., 2018). In our study, 48.6% of frontline HCWs were suffering from burnout, higher than the figure (36.5%) reported in a previous study conducted among Chinese HCWs during the pandemic (Huo et al., 2021). The prevalence of EE symptom (37.3%) is higher than that (34.2%) reported in another study conducted in Wuhan Jinyintan Hospital (Li et al., 2021).
The most important findings of the present study are the following: infection of HCWs, long continuous working hours, inability to eat three regular daily meals, insufficient water intake, and insufficient sleep increase burnout. Conversely, adherence to infection control procedures, satisfaction with their hospital’s infection control measures, and sufficient psychological crisis intervention could decrease burnout.
In this study, nurses and doctors who were working in Wuhan when they answered the questionnaire showed a lower level of DP and a higher level of PA in the multiple linear regression analysis. In other words, they showed less negative attitudes toward their job and workplace and higher personal accomplishment (Mealer et al., 2016; Bridgeman et al., 2018). During the Stage I (Swift Response to the Public Health Emergency), HCWs in Wuhan worked under great pressure, which attracted much attention of Chinese government and members of society. Later, from 23 January to 08 March 2020, more than 42,600 HCWs across China were dispatched to Hubei Province, especially Wuhan. The workload of HCWs in Hubei Province was alleviated by 346 medical teams from around the country (The State Council Information Office of the People’s Republic of China, 2020), as these additional human resources facilitated better work schedules and shorter work shifts. Local HCWs of Wuhan formed support groups with other HCWs from around the country, which provided HCWs further relief in terms of moral support. In addition to this psychological support, hospitals in Wuhan received material support from across China, such as rice, vegetables, meals, and personal protective equipment (PPE). Recent studies revealed that having resources such as social support, sufficient material, and adequate human resources (staff) correlate negatively with burnout (Algunmeeyn et al., 2020; Manzano García and Ayala Calvo, 2021). These measures could explain why HCWs in Wuhan had lower levels of DP and higher levels of PA.
People most at risk of infection are those who are in close contact with a COVID-19 patient or who care for COVID-19 patients (World Health Organization, 2020). Participants who indicated that they could adhere to infection control procedures showed lower levels of EE, lower levels of DP and higher levels of PA. Participants who indicated that they were satisfied with their hospital’s infection control measures showed lower levels of EE. Participants who reported that they or their colleagues were infected showed higher levels of EE and DP. Due to the suddenness of the outbreak, many HCWs did not have what they need to treat patients and they could not adhere to infection control procedures, which would lead to a risk of infection for HCWs (Ali et al., 2020b; Wang et al., 2020). Together with the fear of passing the virus on to their families and friends (Adams and Walls, 2020; Chen et al., 2020; Dong et al., 2020), HCWs’ concerns about having insufficient protection against COVID-19 causes negative emotional reactions. Recent studies found that having insufficient protection inflicts considerable mental damage on HCWs, such as anxiety and depression (Pouralizadeh et al., 2020; Cag et al., 2021). The results of our study showed that insufficient protection is one of the predictor variables of burnout symptoms among HCWs.
To protect HCWs, Chinese healthcare professionals and policymakers took various measures. First, the Chinese government stipulated comprehensive incentive plans to encourage production enterprises to accelerate production. Second, more stringent and comprehensive hospital infection control measures were implemented. On February 19, 2020, the National Health Commission issued a directive on strengthening the protection of HCWs (National Health Commission of the People’s Republic of China, 2020), and national, provincial, municipal, and local levels of expert committees on hospital infection control and treatment were established, resulting in the formulation and implementation of various protocols and procedures.
Due to the COVID-19 outbreak, the normal routine of HCWs was severely disrupted. First, they had to face increased workloads and insufficient rest. During the early stages of the outbreak, there were Chinese news reported that HCWs worked continuously for long time, sometimes exceeding 14 h (SINA Corporation, 2020). In our study, 25.7% of the participants worked for more than 8 consecutive hours a day. The average working hours for doctors were 9.9 h a day and for technicians, such as medical imaging doctors, were 9.6 h a day. Nurses had the shortest daily working hours (6.7 h) which was due to the fact that they provided direct care for COVID-19 patients and their occupational protective clothing could only maintain effective protection for 4–6 h. HCWs experienced higher levels of EE when they worked continuously for more than 8 h a day, which is consistent with previous research that found that HCWs’ long working hours were associated with higher levels of anxiety, despair, and burnout (Elmore et al., 2016; Çelmeçe and Menekay, 2020). Previous studies have reported that as workload increases, HCWs have less time to recover from stressful situations, which will lead to increased rates of EE (Bridgeman et al., 2018). Our study found that during the COVID-19 outbreak, frontline HCWs’ heavy workload and lack of rest breaks may lead to burnout symptoms (Bridgeman et al., 2018). To reduce the continuous work periods of frontline HCWs, Chinese hospital administrators attempted to establish a more rational work shift system that would allow frontline HCWs to have rest breaks and to regularly alternate high-pressure roles with other HCWs, and strictly implemented the new work shift system to reduce job intensity and workload (Kang et al., 2020).
Second, irregular meals are a risk factor for burnout symptoms. Of the participants, 27.0% indicated that they were unable to eat three regular daily meals and they showed higher EE and DP, which was consistent with a previous study in which nurses believed they experienced burnout because of skipped or shortened lunches (Russell, 2016). Many Chinese HCWs were unable to eat three regular daily meals, owing to excess work, limited access to food, and other reasons during the pandemic. In the earlier stages of the pandemic in Wuhan, food resources were limited, and three regular daily meals could not be guaranteed to HCWs. In Wuhan, to meet the dietary needs of HCWs and patients, governments worked together with enterprises, social groups, and volunteers. They purchased ingredients, recruited transport vehicles, and transported free meals and edible to hospital canteens. Providing nutritious and regular meals to HCWs to ensure that they have sufficient energy to prevent burnout is an important intervention to alleviate burnout—and should be considered the responsibility of governments, hospitals, and society.
Third, many HCWs’ daily water intake was insufficient. Of the participants, 50.4% drank no more than 800 ml a day and showed higher EE. According to Atay S et al., in Turkey, nurses cared for patients with COVID-19 reported the most severe problem was perspiration when wearing overalls/gowns (84.1%) (Atay and Cura, 2020). Another study developed North India showed that extreme sweating (59.6%) was a serious problem among frontline nurses (Jose et al., 2021). Heavy work with insufficient water intake, water loss, and mild levels of dehydration can produce disruptions in mood and cognitive functioning, which can easily cause physical fatigue (Popkin et al., 2010). Hospital administrators should install more water dispensers in the right places, keep water safe, and encourage HCWs to drink more water during their breaks.
Forth, sleep deprivation and circadian disorders are inherent occupational risks for burnout of HCWs (Stewart and Arora, 2019). The results of our study showed that the risks of sleep deprivation were noticeable among Chinese HCWs during the pandemic. Of the participants, 56.5% slept for no more than 6 h a day and experienced higher levels of EE. In Wuhan, to ensure that HCWs had more time to rest, hospitals arranged for HCWs to stay in hotels or hospital dormitories as close to their workplaces as possible. This practice gave HCWs some time to have rest and reduced HCWs’ concerns that they would pass the virus to their families and friends.
Psychological status plays a major role in physicians’ mental well-being (Elhadi et al., 2021). Given the sweeping mental health impact of COVID-19, protecting HCWs from the adverse psychological effects of the pandemic is critical (Albott et al., 2020). In our study, 45.7% of the participants reported that they received sufficient psychological crisis intervention and they showed lower EE and higher PA. Previous study has warned that psychological interventions targeting HCWs are urgently needed (Luo et al., 2020). Comprehensive psychological intervention should be carried out in the pandemic. First, at the national level, psychological crisis intervention should occupy a pivotal place in the overall deployment of COVID-19 controls (Li et al., 2020). For example, following The National Health Commission of China call for psychological crisis intervention programs, expert teams were established to compile guidelines, and mental health professionals were stationed in designated isolation hospitals to provide on-site services. Second, at the organizational level, effective psychological crisis interventions that could contribute to the reduction of burnout, such as short-term counselling (Rø et al., 2008), Balint groups which is a group training method (Huang et al., 2020), and psychological screening should be employed during the workday in the disease outbreak period (Liu Z. et al., 2020). Third, at the personal level, HCWs should attend to their physiological health and practice self-care for nutrition, rest, and sleep.
The relationship between gender and burnout is also somewhat controversial (Sanfilippo et al., 2017; Low et al., 2019), in our study, the gender variable was not an influencing factor of burnout in multiple linear regression analysis, which is similar to the results of studies developed in China during the COVID-19 outbreak (Liu X. et al., 2020; Li et al., 2021). In our study, HCWs who were older showed higher PA, which was similarity to a study conducted among HCWs in China (Huo et al., 2021). That may be because during the pandemic, compared to power factors such as infection control, the influence of the gender variable and age variable was masked.
Our research showed that the overwhelming demand for the care of COVID-19 patients placed unprecedented burdens on HCWs, resulting in burnout. Our study identified the following risks for burnout. First, a heavy workload will increase the prevalence of burnout among HCWs. Second, insufficient protection against COVID-19 and the infection status of HCWs are risk factors for burnout. Third, the disruption of normal daily routines is harmful to HCWs, including working for more than 8 continuous hours; obtaining no more than 6 h of sleep; irregular meals; and limited water intake. Fourth, the lack of timely psychological crisis intervention is a risk factor for burnout. Therefore, a synergized and comprehensive interventions should be developed by the government and hospital administrators to address the burnout of frontline HCWs and to fight the COVID-19 pandemic. First, government should re-route critical resources such as workforces and PPE to hospitals that were hit the hardest, as the Chinese government did when it sent additional medical teams to Wuhan. Second, forceful interventions should be developed by government and hospital administrators to protect HCWs from infection. Third, structural or organizational interventions, such as workload or work shift rotation should be performed to allow frontline HCWs to alternate high-pressure roles with other HCWs, and also guarantee them to receive three regular daily meals, sufficient water, and sufficient sleep. Last, psychological interventions targeting HCWs are urgently needed.
This study has several limitations. First, the data are cross-sectional, a causal relationship could not be confirmed. Second, we were limited to an online anonymous questionnaire, which may provide an over- or under-estimation of the responses. However, the online questionnaire was the safest method of data collection as face-to-face communication was risky during this period. Third, the study covered the period, February 18 to March 04, 2020, which was over a year ago. However, since the study was conducted during a pivotal period of the fight against COVID-19 in China and the period is unrepeatable, our research results are valuable to understanding the alleviation of burnout symptoms of HCWs against the background of the surge of unknown infectious diseases. Forth, data were collected from participants’ self-reports; thus, inherent bias was unavoidable. Fifth, in order to not consume too much of HCWs’ time, our study did not involve other psychological evaluations. Sixth, the survey did not cover all the related factors for burnout in health professionals. We designed the questionnaire according to practical situation of China, and due to the period we designed the questionnaire, literatures related to burnout of HCWs among COVID-19 pandemic were lacking, maybe there were some factors that affect the results didn’t included in our study. Last, there were some innate recall bias in our study.
In this study, we determined the prevalence of and risk factors for burnout syndrome among frontline HCWs fighting COVID-19. The results indicate that burnout—which is extremely harmful—is prevalent among frontline HCWs in the battle against COVID-19 in China. We found that infection of HCWs, long continuous working hours, inability to eat three regular daily meals, insufficient water intake, and insufficient sleep increase burnout. Conversely, adherence to infection control procedures, satisfaction with their hospital’s infection control measures, and sufficient psychological crisis intervention could decrease burnout. To alleviate the burnout symptoms of frontline HCWs, synergized and comprehensive interventions should be developed by governments and hospital administrators to address burnout. First, critical resource allocation should be prioritised in hospitals and workforces that are hit the hardest. Second, working in an unprotected environment, a lack of desperately needed PPE resources and infection status of HCWs may lead to burnout. Thus, governments and hospitals must protect HCWs from infection. Third, regarding hospital managers, a more rational workshift schedule should be strictly implemented to reduce the workload of those on the frontline. Fourth, hospital management measures, including the provision of nutritious and regular meals, sufficient drinking water, opportunity to sleep for more than 6 h, and more psychological interventions to counter burnout should be integrated into the coping strategy. In addition, psychological interventions targeting HCWs should be adopted at the national, organizational, and personal levels.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
XZ, KW, and QW: conceptualization. XZ, MJ, NN, and ZK: formal analysis. KW, LS, WH, WY, and YW: investigation. XZ, LL, and LG: data curation. XZ, JW, and YH: writing—original draft preparation. WY and QW: writing—review and editing. All authors have read and agreed to the published version of the manuscript.
This research was funded by QW of The National Key Social Science Fund of China (Grant No. 19AZD013), YH of National Natural Science Foundation of China (Grant No. 72042001), and LS of National Natural Science Foundation of China (Grant No. 71804036).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We would like to express our appreciation to all of the individuals for their involvement in the study, including each of HCWs for their support during the data collection.
COVID-19, Novel coronavirus disease; HCW, Healthcare worker; MBI scale, Maslach Burnout Inventory scale; EE, emotional exhaustion; DP, depersonalization; PA, personal accomplishment; PPE, personal protective equipment; CR, composite reliability; AVE, average variance extracted.
Adams, J. G., and Walls, R. M. (2020). Supporting the health care workforce during the COVID-19 global epidemic. JAMA 323, 1439–1440. doi: 10.1001/jama.2020.3972
Albott, C. S., Wozniak, J. R., McGlinch, B. P., Wall, M. H., Gold, B. S., and Vinogradov, S. (2020). Battle buddies: rapid deployment of a psychological resilience intervention for health care workers during the COVID-19 pandemic. Anesth. Analg. 131, 43–54. doi: 10.1213/ANE.0000000000004912
Algunmeeyn, A., El-Dahiyat, F., Altakhineh, M. M., Azab, M., and Babar, Z. U. (2020). Understanding the factors influencing healthcare providers’ burnout during the outbreak of COVID-19 in Jordanian hospitals. J. Pharm. Policy Pract. 13:53. doi: 10.1186/s40545-020-00262-y
AlHumaid, J., Ali, S., and Farooq, I. (2020). The psychological effects of the COVID-19 pandemic and coping with them in Saudi Arabia. Psychol. Trauma 12, 505–507. doi: 10.1037/tra0000623
Ali, S., Noreen, S., and Farooq, I. (2020a). COVID-19 and healthcare workers in Pakistan: are we losing this fight? J. Med. Sci. 28, 186–188.
Ali, S., Noreen, S., Farooq, I., Bugshan, A., and Vohra, F. (2020b). Risk assessment of healthcare workers at the frontline against COVID-19. Pak. J. Med. Sci. 36, S99–S103. doi: 10.12669/pjms.36.COVID19-S4.2790
Alsulimani, L. K., Farhat, A. M., Borah, R. A., AlKhalifah, J. A., Alyaseen, S. M., Alghamdi, S. M., et al. (2021). Health care worker burnout during the COVID-19 pandemic: a cross-sectional survey study in Saudi Arabia. Saudi Med. J. 42, 306–314. doi: 10.15537/smj.2021.42.3.20200812
Arabi, Y. M., Murthy, S., and Webb, S. (2020). COVID-19: a novel coronavirus and a novel challenge for critical care. Intensive Care Med. 46, 833–836.
Atay, S., and Cura, Ş. Ü. (2020). Problems encountered by nurses due to the use of personal protective equipment during the coronavirus pandemic: results of a survey. Wound Manag. Prev. 66, 12–16.
Barello, S., Plamenchi, L., and Graffigna, G. (2020). Burnout and somatic symptoms among frontline healthcare professionals at the peak of the Italian COVID-19 pandemic. Psychiatry Res. 290:113129. doi: 10.1016/j.psychres.2020.113129
Bourne, T., Shah, H., Falconieri, N., Timmerman, D., Lees, C., Wright, A., et al. (2019). Burnout, well-being and defensive medical practice among obstetricians and gynaecologists in the UK: cross-sectional survey study. BMJ Open 9:e030968. doi: 10.1136/bmjopen-2019-030968
Brady, K. J. S., Ni, P., Sheldrick, R. C., Trockel, M. T., Shanafelt, T. D., Rowe, S. G., et al. (2020). Describing the emotional exhaustion, depersonalization, and low personal accomplishment symptoms associated with Maslach Burnout Inventory subscale scores in US physicians: an item response theory analysis. J. Patient Rep. Outcomes 4:42.
Bridgeman, P. J., Bridgeman, M. B., and Barone, J. (2018). Burnout syndrome among healthcare professionals. Am. J. Health Syst. Pharm. 75, 147–152. doi: 10.2146/ajhp170460
Cag, Y., Erdem, H., Gormez, A., Ankarali, H., Hargreaves, S., Ferreira-Coimbra, J., et al. (2021). Anxiety among front-line health-care workers supporting patients with COVID-19: a global survey. Gen. Hosp. Psychiatry 68, 90–96. doi: 10.1016/j.genhosppsych.2020.12.010
Çelmeçe, N., and Menekay, M. (2020). The effect of stress, anxiety and burnout levels of healthcare professionals caring for COVID-19 patients on their quality of life. Front. Psychol. 11:597624. doi: 10.3389/fpsyg.2020.597624
Centers for Disease Control and Prevention (2008). Exposure to Stress: Occupational Hazards in Hospitals. Washington, DC: National Institute for Occupational Safety and Health.
Chen, Q., Liang, M., Li, Y., Guo, J., Fei, D., Wang, L., et al. (2020). Mental health care for medical staff in China during the COVID-19 outbreak. Lancet Psychiatry 7, e15–e16. doi: 10.1016/S2215-0366(20)30078-X
Christian, L. A. (2015). A passion deficit: occupational burnout and the new librarian: a recommendation report. Southeast. Libr. 62:2.
Corman, V. M., Landt, O., Kaiser, M., Molenkamp, R., Meijer, A., Chu, D. K. W., et al. (2020). Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Euro Surveil. 25:2000045.
Di Trani, M., Mariani, R., Ferri, R., De Berardinis, D., and Frigo, M. G. (2021). From resilience to burnout in healthcare workers during the COVID-19 emergency: the role of the ability to tolerate uncertainty. Front. Psychol. 12:646435. doi: 10.3389/fpsyg.2021.646435
Dong, Z. Q., Ma, J., Hao, Y. N., Shen, X. L., Liu, F., Gao, Y., et al. (2020). The social psychological impact of the COVID-19 pandemic on medical staff in China: a cross-sectional study. Eur. Psychiatry 63:e65. doi: 10.1192/j.eurpsy.2020.59
Duarte, I., Teixeira, A., Castro, L., Marina, S., Ribeiro, C., Jácome, C., et al. (2020). Burnout among Portuguese healthcare workers during the COVID-19 pandemic. BMC Public Health 20:1885. doi: 10.1186/s12889-020-09980-z
Elhadi, M., Msherghi, A., Elgzairi, M., Alhashimi, A., Bouhuwaish, A., Biala, M., et al. (2020). Burnout syndrome among hospital healthcare workers during the COVID-19 pandemic and civil war: a cross-sectional study. Front. Psychiatry 11:579563. doi: 10.3389/fpsyt.2020.579563
Elhadi, M., Msherghi, A., Elgzairi, M., Alhashimi, A., Bouhuwaish, A., Biala, M., et al. (2021). The mental well-being of frontline physicians working in civil wars under coronavirus disease 2019 pandemic conditions. Front. Psychiatry 11:598720. doi: 10.3389/fpsyt.2020.598720
Elmore, L. C., Jeffe, D. B., Jin, L., Awad, M. M., and Turnbull, I. R. (2016). National survey of burnout among US general surgery residents. J. Am. Coll. Surg. 223, 440–451. doi: 10.1016/j.jamcollsurg.2016.05.014
Fornell, C., and Larcker, D. F. (1981). Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 18, 39–50. doi: 10.2307/315131
Gan, Y., Jiang, H., Li, L., Yang, Y., Wang, C., Liu, J., et al. (2019). Prevalence of burnout and associated factors among general practitioners in Hubei, China: a cross-sectional study. BMC Public Health 19:1607. doi: 10.1186/s12889-019-7755-4
Hair, J. F., Ringle, C. M., and Sarstedt, M. (2011). PLS-SEM: indeed a silver bullet. J. Mark. Theory Pract. 19, 139–152. doi: 10.2753/MTP1069-6679190202
Huang, L., Harsh, J., Cui, H., Wu, J., Thai, J., Zhang, X., et al. (2020). A randomized controlled trial of Balint groups to prevent burnout among residents in China. Front. Psychiatry 10:957. doi: 10.3389/fpsyt.2019.00957
Huo, L., Zhou, Y., Li, S., Ning, Y., Zeng, L., Liu, Z., et al. (2021). Burnout and its relationship with depressive symptoms in medical staff during the COVID-19 epidemic in China. Front. Psychol. 12:616369. doi: 10.3389/fpsyg.2021.616369
Johnson, J., Hall, L. H., Berzins, K., Baker, J., Melling, K., and Thompson, C. (2018). Mental healthcare staff well-being and burnout: a narrative review of trends, causes, implications, and recommendations for future interventions. Int. J. Ment. Health Nurs. 27, 20–32. doi: 10.1111/inm.12416
Jose, S., Cyriac, M. C., and Dhandapani, M. (2021). Health problems and skin damages caused by personal protective equipment: experience of frontline nurses caring for critical COVID-19 patients in intensive care units. Indian J. Crit. Care Med. 25, 134–139. doi: 10.5005/jp-journals-10071-23713
Kang, L., Li, Y., Hu, S., Chen, M., Yang, C., Yang, B. X., et al. (2020). The mental health of medical workers in Wuhan, China dealing with the 2019 novel coronavirus. Lancet Psychiatry 7:e14.
Khamisa, N., Oldenburg, B. F., Peltzer, K., and Ilic, D. (2015). Work related stress, burnout, job satisfaction and general health of nurses. Int. J. Environ. Res. Public Health 12, 652–666.
Khan, A., Teoh, K. R., Islam, S., and Hassard, J. (2018). Psychosocial work characteristics, burnout, psychological morbidity symptoms and early retirement intentions: a cross-sectional study of NHS consultants in the UK. BMJ Open 8:e018720.
Khasne, R. W., Dhakulkar, B. S., Mahajan, H. C., and Kulkarni, A. P. (2020). Burnout among healthcare workers during COVID-19 pandemic in India: results of a questionnaire-based survey. Indian J. Crit. Care Med. 24, 664–671. doi: 10.5005/jp-journals-10071-23518
Kirby, T. (2021). New variant of SARS-CoV-2 in UK causes surge of COVID-19. Lancet Respir. Med. 9, e20–e21. doi: 10.1016/S2213-2600(21)00005-9
Lai, C.-C., Shih, T.-P., Ko, W.-C., Tang, H.-J., and Hsueh, P.-R. (2020). Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and corona virus disease-2019 (COVID-19): the epidemic and the challenges. Int. J. Antimicrob. Agents 55:105924.
Lasalvia, A., Amaddeo, F., Porru, S., Carta, A., Tardivo, S., Bovo, C., et al. (2021). Levels of burn-out among healthcare workers during the COVID-19 pandemic and their associated factors: a cross-sectional study in a tertiary hospital of a highly burdened area of north-east Italy. BMJ Open 11:e045127. doi: 10.1136/bmjopen-2020-045127
Li, D., Wang, Y., Yu, H., Duan, Z., Peng, K., Wang, N., et al. (2021). Occupational burnout among frontline health professionals in a high-risk area during the COVID-19 outbreak: a structural equation model. Front. Psychiatry 12:575005. doi: 10.3389/fpsyt.2021.575005
Li, W., Yang, Y., Liu, Z. H., Zhao, Y. J., Zhang, Q., Zhang, L., et al. (2020). Progression of mental health services during the COVID-19 outbreak in China. Int. J. Biol. Sci. 16, 1732–1738. doi: 10.7150/ijbs.45120
Li, X. M., and Liu, Y. J. (2000). Job stressors and burnout among staff nurses. Chin. J. Nurs. 35, 645–649. (in Chinese)
Liu, X., Chen, J., Wang, D., Li, X., Wang, E., Jin, Y., et al. (2020). COVID-19 outbreak can change the job burnout in health care professionals. Front. Psychiatry 11:563781. doi: 10.3389/fpsyt.2020.563781
Liu, Z., Wu, J., Shi, X., Ma, Y., Ma, X., Teng, Z., et al. (2020). Mental health status of healthcare workers in China for COVID-19 epidemic. Ann. Glob. Health 86:128. doi: 10.5334/aogh.3005
Low, Z. X., Yeo, K. A., Sharma, V. K., Leung, G. K., McIntyre, R. S., Guerrero, A., et al. (2019). Prevalence of burnout in medical and surgical residents: a meta-analysis. Int. J. Environ. Res. Public Health 16:1479. doi: 10.3390/ijerph16091479
Lu, W., Wang, H., Lin, Y., and Li, L. (2020). Psychological status of medical workforce during the COVID-19 pandemic: a cross-sectional study. Psychiatry Res. 288:112936. doi: 10.1016/j.psychres.2020.112936
Luo, M., Guo, L., Yu, M., Jiang, W., and Wang, H. (2020). The psychological and mental impact of coronavirus disease 2019 (COVID-19) on medical staff and general public – a systematic review and meta-analysis. Psychiatry Res. 291:113190. doi: 10.1016/j.psychres.2020.113190
Manzano García, G., and Ayala Calvo, J. C. (2021). The threat of COVID-19 and its influence on nursing staff burnout. J. Adv. Nurs. 77, 832–844. doi: 10.1111/jan.14642
Maslach, C., and Jackson, S. E. (1981). The measurement of experienced burnout. J. Organ. Behav. 2, 99–113.
Maslach, C., Jackson, S. E., and Leiter, M. P. (1996). Maslach Burnout Inventory Manual. Palo Alto, CA: Consulting Psychologists Press.
Matsuo, T., Kobayashi, D., Taki, F., Sakamoto, F., Uehara, Y., Mori, N., et al. (2020). Prevalence of health care worker burnout during the coronavirus disease 2019 (COVID-19) pandemic in Japan. JAMA Netw. Open 3:e2017271. doi: 10.1001/jamanetworkopen.2020.17271
Mealer, M., Moss, M., Good, V., Gozal, D., Kleinpell, R., and Sessler, C. (2016). What is burnout syndrome (BOS)? Am. J. Respir. Crit. Care Med. 194, 1–2. doi: 10.1164/rccm.1941P1
Muthén, L. K., and Muthén, B. O. (1998–2012). Mplus User’s Guide. 7th Edn. Los Angeles, CA: Muthén and Muthén.
National Health Commission of the People’s Republic of China (2020). Notice of General Office of National Health Commission for Strengthening the Protection of Medical Staff. Available online at: http://www.nhc.gov.cn/yzygj/s3594/202002/22457f0078a64babbe5c08b262b067ec.shtml (accessed April 3, 2020).
Németh, A. (2016). Orvosok kiégettségének összefüggése az egészséggel, életérzéssel, alváskörülményekkel [Burnout among doctors and its correlations with health, life satisfaction and sleep]. Orv. Hetil. 157, 623–630. doi: 10.1556/650.2016.30410 Hungarian
Popkin, B. M., D’Anci, K. E., and Rosenberg, I. H. (2010). Water, hydration, and health. Nutr. Rev. 68, 439–458.
Pouralizadeh, M., Bostani, Z., Maroufizadeh, S., Ghanbari, A., Khoshbakht, M., Alavi, S. A., et al. (2020). Anxiety and depression and the related factors in nurses of Guilan University of Medical Sciences hospitals during COVID-19: a web-based cross-sectional study. Int. J. Afr. Nurs. Sci. 13:100233. doi: 10.1016/j.ijans.2020.100233
Rø, K. E. I., Gude, T., Tyssen, R., and Aasland, O. G. (2008). Counselling for burnout in Norwegian doctors: one year cohort study. BMJ 337, 1146–1149.
Rotenstein, L. S., Torre, M., Ramos, M. A., Rosales, R. C., Guille, C., Sen, S., et al. (2018). Prevalence of burnout among physicians: a systematic review. JAMA 320, 1131–1150. doi: 10.1001/jama.2018.12777
Russell, K. (2016). Perceptions of burnout, its prevention, and its effect on patient care as described by oncology nurses in the hospital setting. Oncol. Nurs. Forum 43, 103–109. doi: 10.1188/16.ONF.103-109
Şahin, M. K., Aker, S., Şahin, G., and Karabekiroğlu, A. (2020). Prevalence of depression, anxiety, distress and insomnia and related factors in healthcare workers during COVID-19 pandemic in Turkey. J. Community Health 45, 1168–1177. doi: 10.1007/s10900-020-00921-w
Salvagioni, D. A. J., Melanda, F. N., Mesas, A. E., González, A. D., Gabani, F. L., and Andrade, S. M. (2017). Physical, psychological and occupational consequences of job burnout: a systematic review of prospective studies. PLoS One 12:e0185781. doi: 10.1371/journal.pone.0185781
Sanfilippo, F., Noto, A., Foresta, G., Santonocito, C., Palumbo, G. J., Arcadipane, A., et al. (2017). Incidence and factors associated with burnout in anesthesiology: a systematic review. Biomed Res. Int. 2017:8648925. doi: 10.1155/2017/8648925
Serrão, C., Duarte, I., Castro, L., and Teixeira, A. (2021). Burnout and depression in Portuguese healthcare workers during the COVID-19 pandemic-the mediating role of psychological resilience. Int. J. Environ. Res. Public Health 18:636. doi: 10.3390/ijerph18020636
Shaikh, S., Mohsin, S. F., Agwan, M. A. S., Ali, S., Alsuwaydani, Z. A., and AlSuwaydani, S. A. (2021). COVID-19: fear and anxiety among healthcare students in Saudi Arabia: a cross-sectional study. Eur. J. Mol. Clin. Med. 8, 1638–1647.
SINA Corporation (2020). The Doctor in Zhengzhou Worked Continuously for 14 hours, No Eating, No Drinking, No Toilet. The Reason Behind was Touching. Available online at: http://henan.sina.com.cn/news/2020-01-27/detail-iihnzahk6560216.shtml (accessed April 9, 2020).
Stewart, N. H., and Arora, V. M. (2019). The impact of sleep and circadian disorders on physician burnout. Chest 156, 1022–1030. doi: 10.1016/j.chest.2019.07.008
The State Council Information Office of the People’s Republic of China (2020). Fighting Covid-19 China in Action. Available online at: http://www.scio.gov.cn/ztk/dtzt/42313/43142/index.htm (accessed June 7, 2020).
Wang, S., Xie, L., Xu, Y., Yu, S., Yao, B., and Xiang, D. (2020). Sleep disturbances among medical workers during the outbreak of COVID-2019. Occup. Med. 70, 364–369. doi: 10.1093/occmed/kqaa074
Wang, Z., Xie, Z., Dai, J., Zhang, L., Huang, Y., and Chen, B. (2005). Physician burnout and its associated factors: a cross-sectional study in Shanghai. J. Occup. Health 56, 73–83.
West, C. P., Dyrbye, L. N., and Shanafelt, T. D. (2018). Physician burnout: contributors, consequences and solutions. J. Intern. Med. 283, 516–529.
World Health Organization (2020). Rational use of Personal Protective Equipment for Coronavirus Disease 2019 (COVID-19). Available online at:https://apps.who.int/iris/bitstream/handle/10665/331215/WHO-2019-nCov-IPCPPE_use-2020.1-eng.pdf (accessed March 23, 2020).
Wu, H., Liu, L., Wang, Y., Gao, F., Zhao, X., and Wang, L. (2013). Factors associated with burnout among Chinese hospital doctors: a cross-sectional study. BMC Public Health 13:786. doi: 10.1186/1471-2458-13-786
Yang, C., Chen, Z. L., Chen, L. Y., and Jiang, J. X. (2019). Burnout in healthcare: a sign of death by overwork for doctors in China. BMJ 366:l5582.
Keywords: burnout, COVID-19, healthcare workers, MBI scale, frontline healthcare workers
Citation: Zhang X, Wang J, Hao Y, Wu K, Jiao M, Liang L, Gao L, Ning N, Kang Z, Shan L, He W, Wang Y, Wu Q and Yin W (2021) Prevalence and Factors Associated With Burnout of Frontline Healthcare Workers in Fighting Against the COVID-19 Pandemic: Evidence From China. Front. Psychol. 12:680614. doi: 10.3389/fpsyg.2021.680614
Received: 15 March 2021; Accepted: 27 July 2021;
Published: 16 August 2021.
Edited by:
Sónia P. Gonçalves, University of Lisbon, PortugalReviewed by:
Michela Di Trani, Sapienza University of Rome, ItalyCopyright © 2021 Zhang, Wang, Hao, Wu, Jiao, Liang, Gao, Ning, Kang, Shan, He, Wang, Wu and Yin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Qunhong Wu, d3VxdW5ob25nQDE2My5jb20=; Wenqiang Yin, eWlud3ExOTY5QDEyNi5jb20=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.