 Graziella Orrù
Graziella Orrù Davide Bertelloni
Davide Bertelloni Francesca Diolaiuti
Francesca Diolaiuti Ciro Conversano
Ciro Conversano Rebecca Ciacchini
Rebecca Ciacchini Angelo Gemignani
Angelo Gemignani
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol. , 18 June 2021
Sec. Quantitative Psychology and Measurement
Volume 12 - 2021 | https://doi.org/10.3389/fpsyg.2021.669384
The coronavirus disease 2019 (COVID-19) outbreak has caused not only significant physical health problems but also mental health disorders. Anxiety and fear appear to be the main psychological symptoms associated with COVID-19. The aim of this study was to investigate whether anxiety and fear related to COVID-19 are influenced by sociodemographics and whether specific conditions, such as positivity for COVID-19 or death among relatives and friends, can further enhance these symptoms. In this cross-sectional study, 697 Italians responded to an online survey assessing sociodemographic information, the presence/absence of positive cases, or deaths due to COVID-19 among relatives or acquaintances. The Coronavirus Anxiety Scale (CAS) and Fear of COVID-19 Scale (FCS-19S) were administered in order to assess the levels of anxiety and fear associated with COVID-19. The data were collected in November 2020. Anxiety and fear scores were positively correlated. Both male and female subjects with higher CAS scores also displayed higher FCS-19S scores. The CAS and FCS-19S scores tended to increase with age, with older subjects exhibiting higher scores than younger subjects. Additionally, respondents with lower educational levels demonstrated higher scores on both the CAS and FCS-19S. Similarly, respondents living with older people and/or experiencing the death of one or more relatives due to COVID-19 exhibited corresponding outcomes. This study demonstrates how the levels of anxiety and fear, measured by CAS and FCS-19S associated with COVID-19, are influenced by gender, age, cohabitation status, educational levels, and the presence of positive cases or deaths due to COVID-19.
The coronavirus disease 2019 (COVID-19) was declared a worldwide pandemic by the World Health Organization (WHO) in March 2020, but its outbreak was first documented in Wuhan, China, in December 2019. The number of confirmed cases stands at more than 110 million worldwide, while the COVID-19 death toll has passed 2 million (www.worldometers.info; accessed on February 17, 2020 at 03.24 p.m.).
At the time of writing, the COVID-19 pandemic outbreak is undoubtedly causing, and will continue to cause, disastrous economic, financial, political, social, and psychological consequences. While the initial focus was directed toward the physical manifestations of infection (i.e., pneumonia, fever, cough, fatigue, slight dyspnea, headache, and sore throat) (Pascarella et al., 2020), the scientific community soon identified the negative impact of COVID-19 on the brain (Orrù et al., 2020), and mental health (Brooks et al., 2020; Di Giuseppe et al., 2020; Iachini et al., 2020; Orrù et al., 2021). A significant additional factor should be noted in terms of the impact of COVID-19 on emerging adults, afraid not only of the possible negative effects of COVID-19 personally but also in terms of their role as possible carriers in the face of weaker and more fragile subjects. A study carried out by Germani et al. (2020) demonstrated that young people are more worried and afraid of COVID-19 than those “older” than themselves, precisely because of the greater possibility of becoming potential symptomatic or asymptomatic carriers (Germani et al., 2020). The Inter-Agency Standing Committee Guidelines on Mental Health and Psychosocial Support recommends the integration of multiple levels of intervention in response to epidemics and/or emergency situations. In this context, researchers and clinical psychologists attempt to address such consequences by accurately screening the psychological and psychosocial impact of COVID-19, by planning specific tailored interventions accordingly. Researchers also attempt to identify techniques aimed at the prevention of the development of psychological distress due to COVID-19, such as the investigation of Lopez et al. on the role of mindfulness before and during the COVID-19 lockdown, revealing that COVID-19-related anxiety and fear interfere with the mindfulness profile (Lopez et al., 2021).
In fact, a significant increase in psychological distress and associated disorders (i.e., generalized anxiety, panic disorder, and acute stress disorder) has been observed in the general population worldwide over the last 8 months (Iachini et al., 2020; Qian and Li, 2020). Specifically, Iachini et al. (2020) investigated the psychological factors regulating the influence of interpersonal space (such as the 1.80 m of interpersonal distance required by law) and its impact on psychological well-being, finding that higher levels of anxiety, fear, and stress have led to an increase in interpersonal distances, causing a significant decrease in psychological well-being. More specifically, the abovementioned conditions caused by the spread of COVID-19 create not only uncertainty, fear, denial, anxiety, insomnia, dissociative symptoms, depressive disorders, emotional distress, suicidal thoughts or attempts to commit suicide, alcohol, and substance misuse in the general population but also the risk of relapse in those living with preexisting mental disorders (Di Giuseppe et al., 2020; Torales et al., 2020). Such factors are also particularly relevant to healthcare professionals as they represent worsening factors both in terms of their own mental health and their professional performance in areas such as the care plan treatment of patients (Xiang et al., 2020) and communication with family members during the final stage of life of an individual (Iasevoli et al., 2012).
Negative emotions such as anxiety and fear may be related to a number of aspects of the COVID-19 pandemic, specifically physical deterioration, prolonged distress, the death of a loved one, social isolation or prolonged confinement, financial hardship, and uncertainty (Huang and Zhao, 2020). Indeed, the study carried out by Huang and Zhao (2020) during the COVID-19 outbreak demonstrated that the overall rate of anxiety in the general population was approximately 35.1%. This outcome is particularly significant and indicative of the importance of prioritizing psychological testing aimed at an in-depth understanding of signs and symptoms (Orru et al., 2009), as well as offering adequate procedures and prompt responses.
The purpose of this study was to investigate the levels of fear and anxiety measured by using the Coronavirus Anxiety Scale (CAS) (Mozzoni and Franzot, 2020; Sherman and Lee, 2020) and the Fear of COVID-19 Scale (FCS-19S) (Ahorsu et al., 2020; Soraci et al., 2020), associated with the COVID-19 outbreak in the Italian population. Specifically, the investigation was carried out as to whether those domains were influenced by variables such as gender, age, cohabitation status, and educational levels. Additionally, this study explored whether specific factors such as positivity for COVID-19 or death among friends, relatives, and acquaintances may further enhance the levels of fear and anxiety.
In accordance with the abovementioned aims, two validated measures, namely, CAS and FCS-19S, were administered.
A total of 704 responses were gathered through an online survey conducted between November 1 and November 10, 2020 from individuals living in Italy. Of these, seven were excluded from subsequent analyses (i.e., one did not fall within the target age range and six did not provide the informed consent). A total of 697 participants were thus assigned to final analyses (i.e., n = 107 males; n = 590 females).
The subjects were asked specific COVID-19-related information such as the presence/absence of positive cases or deaths among relatives, close friends, or acquaintances. The CAS (Mozzoni and Franzot, 2020; Sherman and Lee, 2020) and FCS-19S (Ahorsu et al., 2020; Soraci et al., 2020) were employed in order to assess the levels of fear and anxiety due to COVID-19.
The CAS (Mozzoni and Franzot, 2020; Sherman and Lee, 2020): The CAS is a self-report tool designed to measure the levels of dysfunctional anxiety associated with COVID-19. It is made up of five items employing a 5-point Likert scale (i.e., responses ranging from never to almost every day in the last 2 weeks). Should the total score equal 9 or higher, dysfunctional anxiety is likely.
Fear of COVID-19 Scale (Ahorsu et al., 2020; Soraci et al., 2020): The FCS-19S is a self-report tool designed to measure the levels of dysfunctional fear associated with COVID-19. It is made up of five items employing a 5-point Likert scale (responses ranging from strongly disagree to strongly agree). The minimum score possible for each question is 1 and the maximum is 5. The total score can be calculated by adding the score of each item (ranging from 7 to 35).
The survey was launched online on November 1, 2020 at 9:00 a.m. (GMT + 1). Respondents were recruited through social media campaigns on sites including Facebook and LinkedIn or through a direct link sent to participants by e-mail. The participants were informed of the purposes of the study and were asked to provide consent on the treatment of personal data. All procedures followed the ethical standards and were approved by the Ethics Committee of the University of Pisa (No. 0036344/2020).
Descriptive statistics were used in order to examine the available data. For each variable, the number of subjects and the relative percentage of the total scores, as well as the mean (M) and SD of the scores obtained through CAS and FCS-19, were reported. Comparisons between the female and male groups were performed using a t-test. The Spearman's correlation was calculated in order to assess the relationships between psychological variables, sociodemographic characteristics, and COVID-19 situational experiences. The p-values <0.05 and 95% confidence intervals were considered statistically significant. The significant correlations were then further investigated. The analysis was conducted using R-3.4.3 for Windows.
A total of 697 participants (n = 107 males; n = 590 females) completed the online survey. The sociodemographic characteristics of the sample, measurement scores, and COVID-19 experiences are summarized in Table 1.
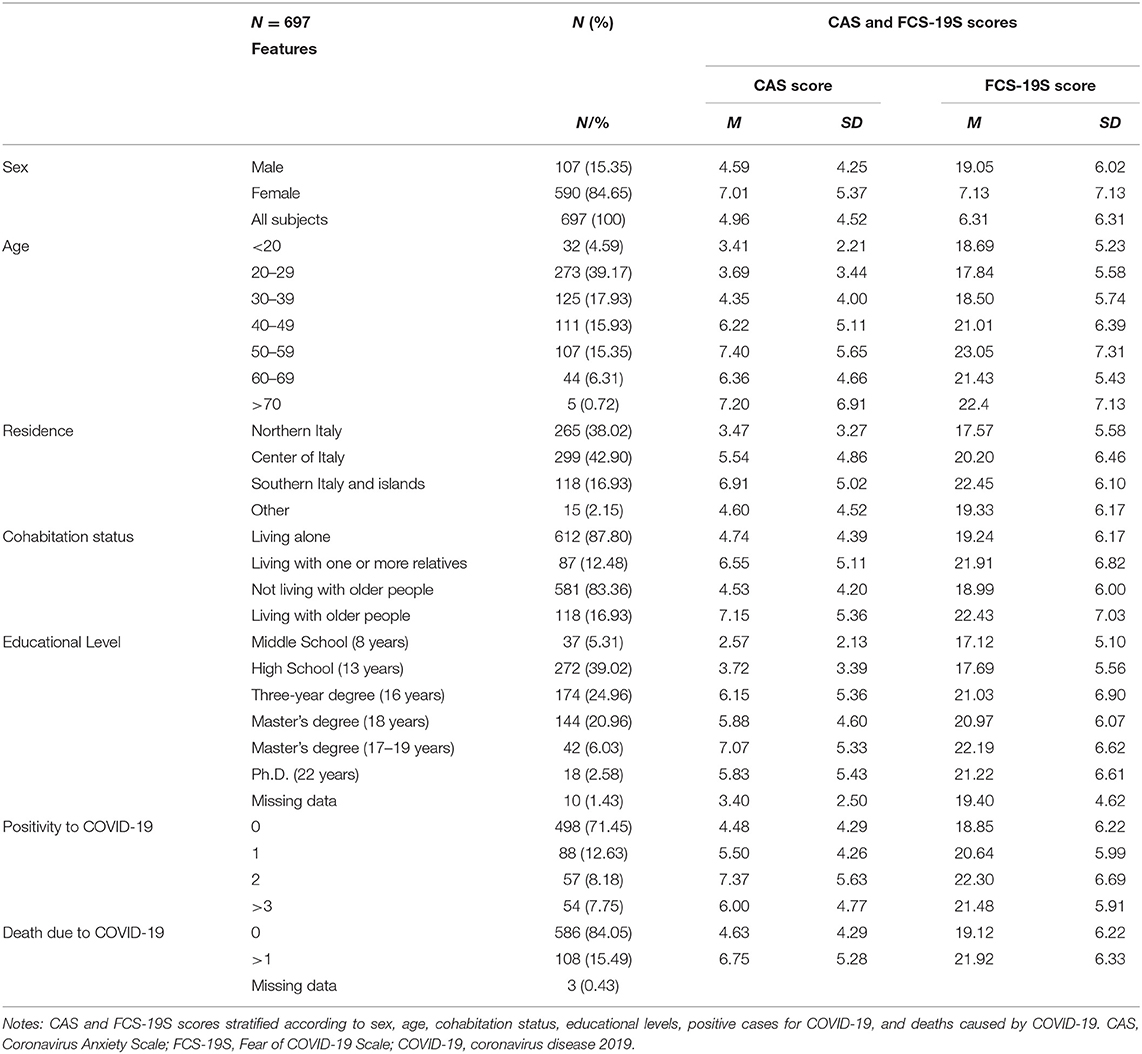
Table 1. Sample characteristics describe the number of subjects (N), percentage (%), mean (M), and standard deviation (SD).
The correlation analysis between demographics, CAS, FCS-19S, and COVID-19 situational experiences is reported in Table 2. A positive correlation was identified in the case of age and CAS score (r = 0.30) and of CAS and FCS-19S scores (r = 0.76).
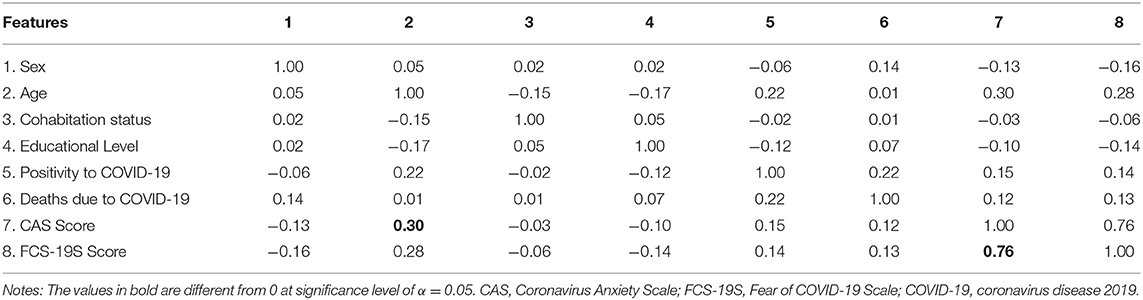
Table 2. Spearman's correlation coefficient (r) among CAS, FCS-19S, demographics, and COVID-19 situational experiences.
With regard to the CAS, a score of ≥9 indicated a level of anxiety beyond the normal levels. In this study, 141 subjects displayed scores of ≥9, approximately 20.23% of the total sample. No cut-offs are available in the case of the FCS-19S. However, the questionnaire indicates that the scores range from 5 to 35 with higher scores suggesting higher levels of fear. A total of 108 subjects (i.e., 15.49% of total participants) showed scores between 25 and 30, while 51 subjects (i.e., 7.32% of total participants) scored >30. Overall, 159 subjects (i.e., 22.81% of total participants) reported the FCS-19S scores of >25.
The correlation analysis demonstrated a significant gender difference in CAS and FCS-19S scores (Figure 1). Specifically, the data analysis displayed higher CAS and FCS-19S scores in females than in males (p < 0.001). The data also revealed a positive and significant correlation between CAS and FCS-19S scores. In fact, subjects with higher scores on the CAS also displayed higher scores on the FCS-19S (r = 0.76; p < 0.05) (Figure 1A). Such correlations were also observed in the subgroups composed of males (r = 0.74; p < 0.05) and females (r = 0.81; p < 0.05) (Figures 1B,C, respectively).
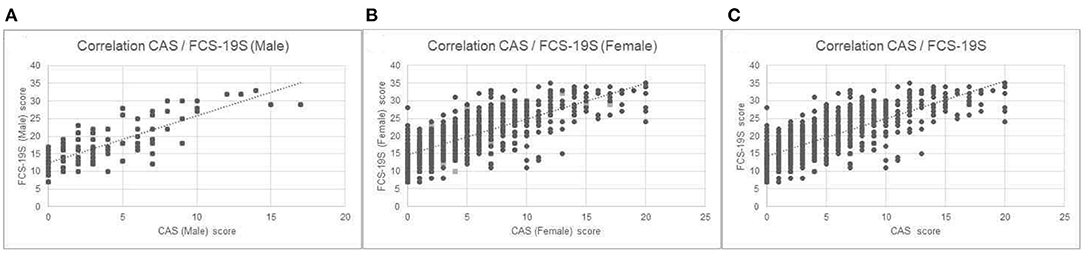
Figure 1. (A) Correlation between CAS and FCS-19S scores; (B) correlation between CAS scores and FCS-19S scores in the female subgroup; and (C) correlation between CAS scores and FCS-19S scores in the male subgroup. CAS, Coronavirus Anxiety Scale; FCS-19S, Fear of COVID-19 Scale; COVID-19, coronavirus disease 2019.
A positive correlation was identified for age, CAS, and FCS-19S (see Table 1), and age and CAS score (r = 0.30) (see Table 2). As it is evident from Figures 2A,B, the CAS and FCS-19S scores increased with age. Specifically, age groups with the highest scores were those ranging from 50 to 59 and >70, both for CAS and FCS-19S.
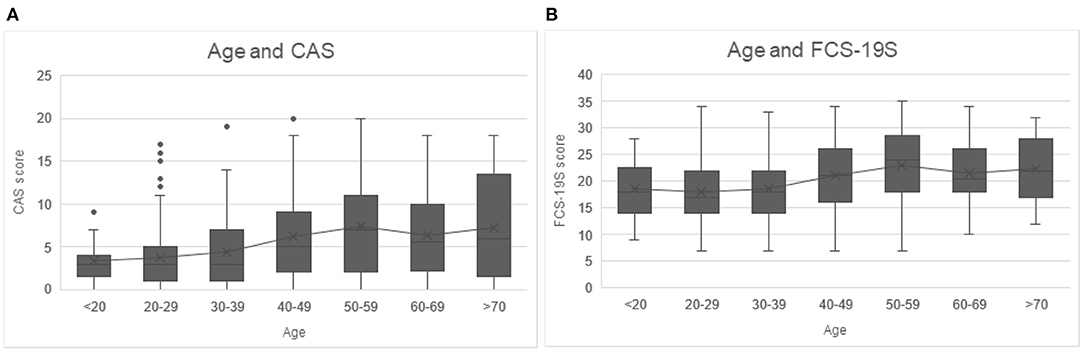
Figure 2. (A) CSA scores increased as people age, with higher CAS scores in the age group ranging from 50 to 59 and >70. (B) Higher FCS-19S scores as people age, with increasing age of the subjects, with higher FCS-19S scores in the age group ranging from 50 to 59 years and >70. CAS, Coronavirus Anxiety Scale; FCS-19S, Fear of COVID-19 Scale; COVID-19, coronavirus disease 2019.
No significant differences were detected between CAS and FDS-19S scores in people living alone compared with those living with one or more relatives (i.e., children and spouse). However, subjects living with elderly people showed significantly higher levels of anxiety (i.e., higher CAS scores) than those who do not (p < 0.01). Similarly, higher levels of fear (i.e., higher FDS-19S scores) were observed in subjects living with elderly people compared with those who do not, yet no significant differences were identified (p = 0.058).
This study also investigated whether educational levels can be associated with CAS and FCS-19S scores or, rather, whether higher levels of education can be associated with lower CAS and FDS-19S scores. The sample was originally gathered according to the following levels of education: (i) Middle School (MS) (8 years); (ii) High School (HS) (13 years); (iii) Bachelor's Degree (BD) (16 years); (iv) Master's Degree (MD1) (18 years); (v) 1st or 2nd level Master's Degree (MD2) (1st level MD2: 17 years if obtained subsequent to BD; 2nd level MD2: 19 years if obtained subsequent to MD1); and (vi) Ph.D. (Ph.D.) (22 years). Figure 3 illustrates the relationship between the educational levels and scale scores measured through CAS and FCS-19S. Higher levels of education were associated with lower CAS and FCS-19S scores.
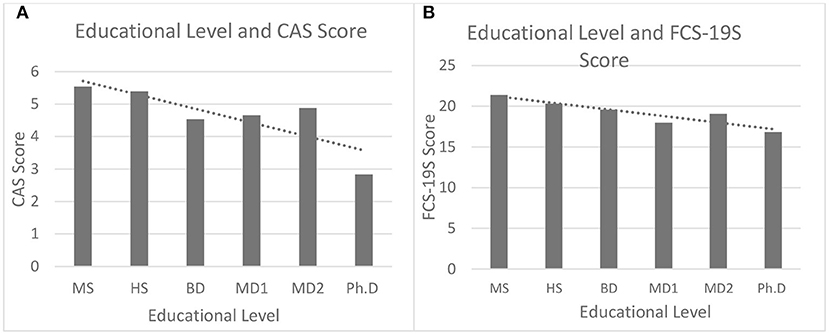
Figure 3. The relationship between the level of education and CAS scores (A) and FCS-19S scores (B). MS, Middle School; HS, High School; BD, Bachelor's Degree; MD1, Master's Degree; MD2, 1st or 2nd level Master's Degree; PhD, PhD.; CAS, Coronavirus Anxiety Scale; FCS-19S, Fear of COVID-19 Scale; COVID-19, coronavirus disease 2019.
For a better understanding of the effects relating to higher and lower educational levels on CAS and FCS-19S scores, the participants were divided into two subgroups based on the educational levels: the first subgroup (Group 1) included individuals with MS and HS qualifications, while the second subgroup (Group 2) included individuals with BD, MD (1 and 2), and Ph.D. qualifications. Significantly higher CAS (p < 0.01) and FCS-19S scores (p < 0.01) were detected in Group 1 as compared with Group 2 (Figure 4). These data suggest that individuals with a lower educational level may be more susceptible to experiencing higher levels of anxiety and fear.
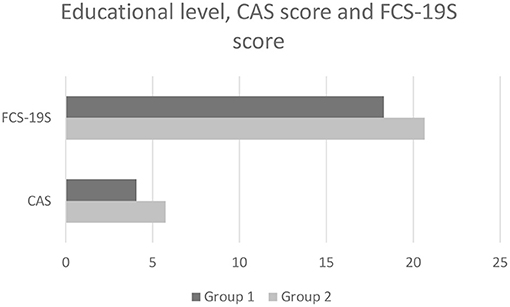
Figure 4. The average CAS and FCS-19S scores in Group 1 vs. Group 2. CAS, Coronavirus Anxiety Scale; FCS-19S, Fear of COVID-19 Scale; COVID-19, coronavirus disease 2019.
In order to investigate whether specific conditions such as the presence/absence of COVID-19 positivity or COVID-19-related deaths among friends and/or relatives may further enhance the levels of fear or anxiety measured by CAS and FCS-19S, every individual was asked to reply to the following questions:
1) How many cases of COVID-19 positivity (including yourself) can you report among your family members?
2) How many deaths have you suffered due to COVID-19 among family members or acquaintances?
In terms of the first question, the results showed those subjects indicating at least one case of positivity to COVID-19 among family members displayed significantly higher CAS (p < 0.01) and FCS-19S scores (p < 0.01) compared with those who did not indicate any positive cases of COVID-19. The results for the second question illustrated that individuals who have experienced the death of at least one family member due to COVID-19 also displayed higher CAS and FCS-19S scores than those who had not (Figure 5).
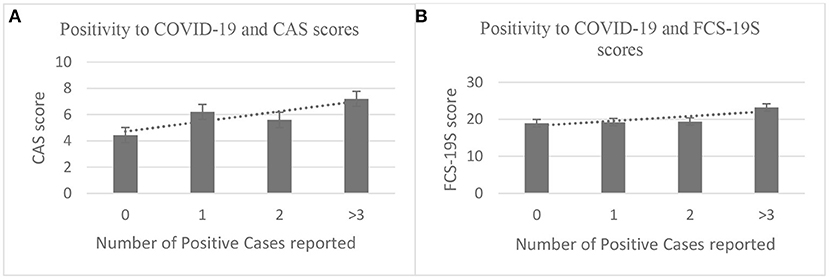
Figure 5. Higher CAS and FCS-19S scores were associated with a higher number of positive cases reported [(A, B), respectively]. CAS, Coronavirus Anxiety Scale; FCS-19S, Fear of COVID-19 Scale; COVID-19, coronavirus disease 2019.
With regard to the second question, the analyzed responses revealed that subjects reporting one or more deaths due to COVID-19 showed higher CAS and FCS-19S scores (p < 0.001 and p < 0.01, respectively) compared with those who did not report any deaths among family members or acquaintances (Figure 6).
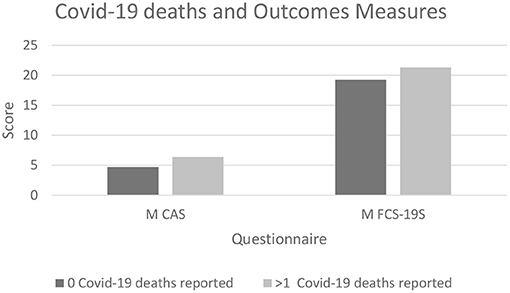
Figure 6. The graph shows significantly higher CAS and FCS-19S scores in subjects who have suffered at least one loss due to COVID-19 (p < 0.001 and p < 0.01, respectively) compared with those who did experience it. CAS, Coronavirus Anxiety Scale; FCS-19S, Fear of COVID-19 Scale; COVID-19, coronavirus disease 2019.
The aim of this study was to investigate the levels of fear and anxiety, as measured by CAS and FCS-19S, associated with the COVID-19 outbreak among the Italian population. Specifically, the study investigated whether those domains were influenced by variables such as (1) gender, (2) age, (3) cohabitation status, (4) educational levels, and (5) situational experiences related to COVID-19. Additionally, this study aimed to explore whether specific factors such as positivity for COVID-19 or death among friends, relatives, and acquaintances may further enhance the levels of fear and anxiety.
This study demonstrates a possible positive correlation among different variables considered, i.e., anxiety, fear, and COVID-19 outbreak experiences. The anxiety and fear scores measured by CAS and FCS-19S were positively correlated, with subjects demonstrating higher CAS scores also showing higher FCS-19S scores. Similar outcomes were detected in the analysis of the subgroups investigating gender differences. Females showed significantly higher levels of anxiety and fear than males. These data are consistent with other findings, suggesting that, typically, females show a higher predisposition to anxiety compared with males (Foot and Koszycki, 2004; Seo et al., 2017). In fact, women have been reported to display higher rates of affective disorders than men (Bebbington et al., 1998; Cyranowski et al., 2000; Bijl et al., 2002; Kessler, 2003; Leach et al., 2008). According to a number of studies, the lifetime prevalence of affective disorders is approximately double in female subjects as compared with their male counterparts (Bebbington et al., 1998; Cyranowski et al., 2000; Bijl et al., 2002; Kessler, 2003; Leach et al., 2008). However, these findings are in contrast with other studies reporting lower scores (Faravelli et al., 2013; Salk et al., 2017). Taken collectively, the implications of the studies described above suggest that the findings reported preclude robust conclusions and require further investigation.
Additionally, an investigation was carried out in order to determine whether the levels of anxiety and fear associated with COVID-19 are negatively influenced by age. The findings demonstrate that CAS and FCS-19S scores tend to increase with age; in fact, older subjects presented higher scores as compared with younger subjects. Such outcomes are in contrast with other studies reporting lower scores as age increases (Faravelli et al., 2013; Salk et al., 2017).
In terms of the third aim, cohabitation status was analyzed. The results demonstrated that respondents living with elderly people exhibited higher levels of anxiety and fear associated with COVID-19. In addition, the educational level (the fourth aim of this study) was an extremely significant variable as subjects with a lower educational level demonstrated higher levels of anxiety and fear associated with COVID-19 compared with subjects with a higher educational level. Such results seem to successfully confirm other findings, which clearly demonstrate that educational levels may influence the degree of anxiety and depression experienced and reduce manifestations of psychopathological symptoms (Bjelland et al., 2008; Chazelle et al., 2011). In contrast, other studies have concluded that participants with higher educational levels reported higher psychological distress than those with lower levels (Qiu et al., 2020; Wang et al., 2020). Further studies clarifying and expanding on this issue are therefore of particular interest.
Finally, this study investigated whether specific conditions such as positivity for COVID-19 or death among friends and/or relatives may further enhance such symptoms. In this context, the results demonstrated that subjects reporting at least one case of positivity to COVID-19 among family members displayed significantly higher CAS and FCS-19S scores compared with those who did not indicate a positive case of COVID-19. Furthermore, the results demonstrated that individuals who have experienced the death of at least one family member due to COVID-19 displayed higher CAS and FCS-19S scores than those who had not.
This study has the following limitations: (1) the sample under this study is not sufficiently broad or representative of the general population (i.e., this study was hindered by a significant gender imbalance). Future studies must therefore aim to expand the number of participants and ensure that it is representative of the general population; (2) recruitment channels (mainly the Internet) may lead to bias, and it is therefore necessary that future studies expand and equalize recruitment channels; (3) the data were collected from November 1, 2020 to November 10, 2020, a period in which Italian legislation divided regions by color, with each color imposing varying limitations to social life and mobility. For these reasons, at the time of completing the questionnaire, the subjects were living in different regions with varying degrees of limitations, which may also have affected anxiety and fear levels. It is therefore considered appropriate that future studies investigate subjects living under the same legislative conditions (i.e., limitations to social life and mobility); (4) the CAS was validated in the English language by Sherman and Lee (2020), but has not yet been entirely validated in its Italian form. An online Italian translation by Mozzoni and Franzot (2020) is available, yet published data does not exist on Italian norms and validation of the scale. Future studies should therefore make use of validated tools or a validated Italian version of the CAS, if available.
In conclusion, this study suggests that anxiety and fear associated with COVID-19 are influenced by gender differences, age, cohabitation status, and education levels. Additionally, positivity to COVID-19 and death caused by COVID-19 seem to have profound adverse effects on mental health, death distress, perceived risk, and happiness among the general population.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by University of Pisa. The patients/participants provided their written informed consent to participate in this study.
GO, DB, and FD devised the main research topic, planned the online survey, carried out the analysis, conceived the conceptual ideas and proof outline, and drafted the manuscript. GO, DB, FD, CC, RC, and AG revised the manuscript critically. GO and CC provided an extensive revision of the final version of the manuscript. All the authors gave the final approval for the version to be published.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors thank all participants who voluntarily contributed to this study.
Ahorsu, D. K., Lin, C. Y., Imani, V., Saffari, M., Griffiths, M. D., and Pakpour, A. H. (2020). The fear of COVID-19 scale: development and initial validation. Int. J. Ment. Health Addict. 2020, 1–9. doi: 10.1007/s11469-020-00270-8
Bebbington, P. E., Dunn, G., Jenkins, R., Lewis, G., Brugha, T., Farrell, M., et al. (1998). The influence of age and sex on the prevalence of depressive conditions: report from the National Survey of Psychiatric Morbidity. Psychol. Med. 28, 9–19. doi: 10.1017/S0033291797006077
Bijl, R. V., de Graaf, R., Ravelli, A., Smit, F., and Vollebergh, W. A. (2002). Gender and age-specific first incidence of DSM-III-R psychiatric disorders in the general population. Soc. Psychiatry Psychiatr. Epidemiol. 37, 372–379. doi: 10.1007/s00127-002-0566-3
Bjelland, I., Krokstad, S., Mykletun, A., Dahl, A. A., Tell, G. S., and Tambs, K. (2008). Does a higher educational level protect against anxiety and depression? The HUNT study. Soc. Sci. Med. 66, 1334–1345. doi: 10.1016/j.socscimed.2007.12.019
Brooks, S. K., Webster, R. K., Smith, L. E., Woodland, L., Wessely, S., Greenberg, N., et al. (2020). The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet 395, 912–920. doi: 10.1016/S0140-6736(20)30460-8
Chazelle, E., Lemogne, C., Morgan, K., Kelleher, C. C., Chastang, J. F., and Niedhammer, I. (2011). Explanations of educational differences in major depression and generalised anxiety disorder in the Irish population. J. Affect. Disord. 134, 304–314. doi: 10.1016/j.jad.2011.05.049
Cyranowski, J. M., Frank, E., Young, E., and Shear, M. K. (2000). Adolescent onset of the gender difference in lifetime rates of major depression: a theoretical model. Arch. Gen. Psychiatry 57, 21–27. doi: 10.1001/archpsyc.57.1.21
Di Giuseppe, M., Zilcha-Mano, S., Prout, T. A., Perry, J. C., Orrù, G., and Conversano, C. (2020). Psychological impact of coronavirus disease 2019 among Italians during the first week of lockdown. Front. Psychiatry 11:576597. doi: 10.3389/fpsyt.2020.576597
Faravelli, C., Scarpato, M. A., Castellini, G., and Sauro, C. L. (2013). Gender differences in depression and anxiety: the role of age. Psychiatry Res. 210, 1301–1303. doi: 10.1016/j.psychres.2013.09.027
Foot, M., and Koszycki, D. (2004). Gender differences in anxiety-related traits in patients with panic disorder. Depress. Anxiety 20, 123–130. doi: 10.1002/da.20031
Germani, A., Buratta, L., Delvecchio, E., and Mazzeschi, C. (2020). Emerging adults and COVID-19: the role of individualism-collectivism on perceived risks and psychological maladjustment. Int. J. Environ. Res. Public Health. 17:3497. doi: 10.3390/ijerph17103497
Huang, Y., and Zhao, N. (2020). Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: a web-based cross-sectional survey. Psychiatry Res. 288:112954. doi: 10.1016/j.psychres.2020.112954
Iachini, T., Frassinetti, F., Ruotolo, F., Sbordone, F. L., Ferrara, A., Arioli, M., et al. (2020). Psychological and situational effects on social distancing and well-being during the COVID-19 pandemic: not a question of real risk. Front. Psychol. 11:577684. doi: 10.31234/osf.io/r7usv
Iasevoli, M., Giantin, V., Voci, A., Valentini, E., Zurlo, A., Maggi, S., et al. (2012). Discussing end-of-life care issues with terminally ill patients and their relatives: comparisons among physicians, nurses and psychologists. Aging Clin. Exp. Res. 24, 35–42.
Kessler, R. C. (2003). Epidemiology of women and depression. J. Affect. Disord. 74, 5–13. doi: 10.1016/S0165-0327(02)00426-3
Leach, L. S., Christensen, H., Mackinnon, A. J., Windsor, T. D., and Butterworth, P. (2008). Gender differences in depression and anxiety across the adult lifespan: the role of psychosocial mediators. Soc. Psychiatry Psychiatr. Epidemiol. 43, 983–998. doi: 10.1007/s00127-008-0388-z
Lopez, A., Caffò, A. O., Tinella, L., Di Masi, M. N., and Bosco, A. (2021). Variations in mindfulness associated with the COVID-19 outbreak: differential effects on cognitive failures, intrusive thoughts, and rumination. Appl. Psychol. Health Well Being. 00:1–20. doi: 10.1111/aphw.12268
Mozzoni, M., and Franzot, E. (2020). Coronavirus Anxiety Scale (CAS). Department of Psychology, Christopher Newport University, Virginia, USA.
Orrù, G., Conversano, C., Malloggi, E., Francesconi, F., Ciacchini, R., and Gemignani, A. (2020). Neurological complications of COVID-19 and possible neuroinvasion pathways: a systematic review. Int. J. Environ. Res. Public Health 17:6688. doi: 10.3390/ijerph17186688
Orrù, G., Marzetti, F., Conversano, C., Vagheggini, G., Miccoli, M., Ciacchini, R., et al. (2021). Secondary traumatic stress and burnout in healthcare workers during COVID-19 outbreak. Int. J. Environ. Res. Public Health 18:337. doi: 10.3390/ijerph18010337
Orru, G., Sampietro, S., Catanzaro, S., Girardi, A., Najjar, M., Giantin, V., et al. (2009). Serial position effect in a free recall task: differences between probable dementia of Alzheimer type (PDAT), vascular (VaD) and mixed etiology dementia (MED). Arch. Gerontol. Geriatr. 49, 207–210. doi: 10.1016/j.archger.2009.09.030
Pascarella, G., Strumia, A., Piliego, C., Bruno, F., Del Buono, R., Costa, F., et al. (2020). COVID-19 diagnosis and management: a comprehensive review. J. Intern. Med. 288, 192–206. doi: 10.1111/joim.13091
Qian, D., and Li, O. (2020). The relationship between risk event involvement and risk perception during the COVID-19 outbreak in China. Appl. Psychol. Health Well Being 2020:10.1111/aphw.12219. doi: 10.1111/aphw.12219
Qiu, J., Shen, B., Zhao, M., Wang, Z., Xie, B., and Xu, Y. (2020). A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: implications and policy recommendations. Gen. Psychiatry;33:e100213. doi: 10.1136/gpsych-2020-100213
Salk, R. H., Hyde, J. S., and Abramson, L. Y. (2017). Gender differences in depression in representative national samples: meta-analyses of diagnoses and symptoms. Psychol. Bull. 143, 783–822. doi: 10.1037/bul0000102
Seo, D., Ahluwalia, A., Potenza, M. N., and Sinha, R. (2017). Gender differences in neural correlates of stress-induced anxiety. J. Neurosci. Res. 95, 115–125. doi: 10.1002/jnr.23926
Sherman, A., and Lee. (2020). Coronavirus Anxiety Scale: a brief mental health screener for COVID-19 related anxiety. Death Stud. 44, 393–401. doi: 10.1080/07481187.2020.1748481
Soraci, P., Ferrari, A., Abbiati, F. A., Del Fante, E., De Pace, R., Urso, A., et al. (2020). Validation and psychometric evaluation of the Italian version of the Fear of COVID-19 Scale. Int. J. Ment. Health Addict. 2020, 1–10. doi: 10.1007/s11469-020-00277-1
Torales, J., O'Higgins, M., Castaldelli-Maia, J. M., and Ventriglio, A. (2020). The outbreak of COVID-19 coronavirus and its impact on global mental health. Int. J. Soc. Psychiatry 66, 317–320. doi: 10.1177/0020764020915212
Wang, H., Xia, Q., Xiong, Z., Li, Z., Xiang, W., Yuan, Y., et al. (2020). The psychological distress and coping styles in the early stages of the 2019 coronavirus disease (COVID-19) epidemic in the general mainland Chinese population: A web-based survey. PLoS One, 15(5), e0233410.
Keywords: COVID-19 pandemic, anxiety, fear, CAS, FCS-19S, mental health, psychopathology
Citation: Orrù G, Bertelloni D, Diolaiuti F, Conversano C, Ciacchini R and Gemignani A (2021) A Psychometric Examination of the Coronavirus Anxiety Scale and the Fear of Coronavirus Disease 2019 Scale in the Italian Population. Front. Psychol. 12:669384. doi: 10.3389/fpsyg.2021.669384
Received: 18 February 2021; Accepted: 25 May 2021;
Published: 18 June 2021.
Edited by:
Andrea Bonanomi, Catholic University of the Sacred Heart, ItalyReviewed by:
Andrea Bosco, University of Bari Aldo Moro, ItalyCopyright © 2021 Orrù, Bertelloni, Diolaiuti, Conversano, Ciacchini and Gemignani. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Graziella Orrù, Z3JhemllbGxhLm9ycnVAdW5pcGkuaXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.