
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol., 18 February 2021
Sec. Health Psychology
Volume 12 - 2021 | https://doi.org/10.3389/fpsyg.2021.616526
This article is part of the Research TopicNew Perspectives in Bereavement and Loss: Complicated and Disenfranchised Grief Along the Life CycleView all 9 articles
 Hod Orkibi1*
Hod Orkibi1* Gianmarco Biancalani2
Gianmarco Biancalani2 Mihaela Dana Bucuţã3
Mihaela Dana Bucuţã3 Raluca Sassu3
Raluca Sassu3 Michael Alexander Wieser4
Michael Alexander Wieser4 Luca Franchini5
Luca Franchini5 Melania Raccichini5
Melania Raccichini5 Bracha Azoulay1
Bracha Azoulay1 Krzysztof Mariusz Ciepliñski6
Krzysztof Mariusz Ciepliñski6 Alexandra Leitner4
Alexandra Leitner4 Silvia Varani5
Silvia Varani5 Ines Testoni1,2
Ines Testoni1,2As part of a European Erasmus Plus project entitled Death Education for Palliative Psychology, this study assessed the ways in which Master’s Degree students in psychology and the creative arts therapies self-rated their confidence and interest in death education and palliative and bereavement care. In five countries (Austria, Israel, Italy, Poland, Romania), 344 students completed an online questionnaire, and 37 students were interviewed to better understand their views, interest, and confidence. The results revealed some significant differences between countries, and showed that older respondents with previous experience as formal caregivers for end-of-life clients showed greater interest in obtaining practical clinical competence in these fields. A mediation analysis indicated that students’ previous care experiences and past loss experiences were related to students’ current interest in death education and palliative and bereavement care through the mediation of their sense of confidence in this field. The qualitative findings identified five shared themes: life and death, learning about death, the psychological burden, personal experience and robust training, and four key training needs. Overall, students’ interest in studying and working with terminal illness and death are rooted in internal resources, a preliminary sense of confidence, but also external requirements.
Coping with death, including end of life management and the process of mourning, constitute ongoing challenges in contemporary society (Fonseca and Testoni, 2012; Testoni et al., 2016). One way to address this challenge in higher education is through death education (DeEd; also termed “thanatology”). Teaching DeEd to healthcare students may help overcome the taboos associated with death and dying. It can serve to increase students’ awareness of the distress associated with loss and bereavement and hone their skills in death management (Testoni et al., 2019c). This international study is part of a larger project supported by the Erasmus plus program of the European Union. The overarching aim of the project is to explore how DeEd can inform palliative and bereavement care in the training of psychologists and arts therapists. This report focuses on findings from the exploratory phase of the project, which aimed at characterizing students’ interests and sense of competence with respect to death and bereavement care.
The origins of DeEd can be traced back to the death-awareness movement in the United States in the 1960s–1970s that was designed to help overcome death anxiety through cognitive resources (Feifel, 1959). Death anxiety can be experienced as mortality salience; namely, the existential awareness that death is inevitable, not only when the person experiences death, but also when one is simply confronted with the notions of death and dying (Testoni, 2015). To reduce this unpleasant feeling and to live life at one’s best, DeEd aims to increase awareness and effective communication of death- related issues, as well as ways to cope with loss and grief (Testoni et al., 2018, 2019a,d, 2020b; DeSpelder and Strickland, 2019).
Healthcare professionals use DeEd to deal with the distress of death and loss, since an inability to handle the anguish of death on the part of caregivers can lead to dehumanization of the patient, which is considered to be a factor predicting burnout for those working in these fields (Testoni et al., 2019b). A particularly difficult task for healthcare professionals is communicating bad news to dying individuals or their family members. In this case the recipients must be informed of an adverse event such as a difficult diagnosis, an unfortunate prognosis, or traumatic events involving loved ones whose implications they cannot evaluate. This constitutes the point of no return (Testoni, 2015). However, the communication of this information requires competence and a specific set of skills and expertise, starting with the medical context in which the family and the dying person find themselves. Although this can be a routine part of the work of some healthcare professionals, they may not have the specific skills in part because DeEd is currently not integrated into the training of healthcare professionals (Testoni, 2015). In fact, psychologists, arts therapists, doctors and nurses often lack the skills needed to communicate bad news and deal with the anticipated mourning which follows (Testoni et al., 2019b). Another factor that hinders the communication of bad news is the fear of death itself: when people face death they often come to grips with their own finitude, and may therefore not be able to face the terror associated with death (Solomon et al., 2000; Burke et al., 2010).
Terror Management Theory posits that the conflict between individuals’ awareness of the inevitability of their own death (i.e., mortality salience) and the natural instinct of self-preservation gives rise to a paralyzing fear of death (Solomon et al., 2000). To cope with such terror, people adopt sophisticated defense strategies similar to those used to reduce the discomfort caused by cognitive dissonance (Festinger, 1957). In particular, when realizing that death is inevitable, individuals try to rebalance the dissonance between wanting to survive and the awareness of having to die through symbolic constructs aimed at denying death; for example by taking comfort in the fact that one’s memory or good deeds will live forever (Solomon et al., 2017; Yaakobi, 2019). Studies generally report a non-linear relationship between death anxiety and levels of religiosity: death anxiety increases from low to medium religiosity, but decreases with increasing religiosity, from medium to high (Testoni et al., 2020b). It was claimed that the curvilinear relationship observed in the non-religious may indicate that death anxiety reduces “irreligiosity,” whereas among the religious greater religiosity reduces death anxiety (Jong, 2021, p. 40). These findings could imply that profound (as opposed to superficial) contemplation of religious themes could help reduce death anxiety and would therefore be relevant to DeEd courses (Neimeyer, 1994).
In the professional context, there is some evidence that care workers’ own death anxiety may have a negative impact on their own ability to care for dying patients, and that DeEd can reduce death anxiety (Peters et al., 2013). Studies on students have shown not only a reduction in their own death anxiety (McClatchey and King, 2015; Wallace et al., 2019) but also an increase in their perceived ability to cope with death and dying (Claxton-Oldfield et al., 2006). The development of awareness of the existence of death, along with the skills needed to psychologically manage the terror that can result from mortality salience episodes can help people manage death anxiety (Solomon et al., 2000). To achieve this goal, death education is fundamental (Testoni, 2015). This study thus constitutes a preliminary investigation of the perceptions of students considering careers involving contact with terminally ill patients. Although these issues are addressed in this study at the university level alone, training in DeEd can also be useful for personal development and professional work (Corr and Corr, 2003). Dealing with these issues can help students acquire ways to handle work episodes involving death and dying. These include announcing a terminal diagnosis to a sick patient, the management of anticipatory mourning, the death of the patient, the management of bereavement with family members, etc. However, death, dying and bereavement do not only involve individuals but also communities with respect to funeral arrangements, commemorations, death-related legal issues, good citizenship and civil responsibility (e.g., organ donation, volunteer work), death-related issues throughout the lifespan from children to older adults. Different cultural groups also have diverse religious or spiritual views and practices toward death and bereavement (Corr and Corr, 2003). DeEd therefore covers a broad and diverse range of topics.
Palliative care (PC) “is an approach that improves the quality of life of patients and their families facing the problems associated with life-threatening illness, through the prevention and relief of suffering” (World Health Organization [WHO], 2020). The Atlas of Palliative Care in Europe 2019 published by the European Association for Palliative Care (Arias-Casais et al., 2019) indicates that the number of specialized PC services and the integration of PC into the national health systems vary across EU countries. The majority (76%) have adapted their General Health Laws and included PC as a mandatory service, as a patient’s right, or as a human right. PC is included in the list of primary care health services in 36 countries (71%). The lack of education and training opportunities in the Palliative Medicine field have repeatedly been identified as obstacles to the development of the discipline in the EU (Paal et al., 2019). Here, a search in official national documents and websites only identified a few academic programs and courses that focus on DeEd and palliative and bereavement care in the five countries associated with the Erasmus plus project: Austria, Israel, Italy, Poland, and Romania. This paucity of training programs underscores the need to include PC in the DeEd curriculum.
DeEd as well as palliative and bereavement care are of growing educational and practical interest but are still relatively under-investigated in the context of higher education. The specific aim of the exploratory mixed methods study reported here was to assess how students enrolled in master’s degree (MA) programs in psychology (i.e., mostly in clinical specializations) or the creative arts therapies (in Israel alone) self-rate their confidence and interest in DeEd and palliative and bereavement care. Both quantitative and qualitative data were collected and analyzed to better understand the students’ responses. The qualitative data aimed to complement the quantitative data, as in a mixed methods sequential explanatory design where quantitative data is followed by qualitative data (Ivankova et al., 2006).
In the five countries that participated in the Erasmus plus project, students were invited to fill in an anonymous online questionnaire in their local language using research survey software (December 2010–February 2020). Overall, 344 MA students (85% female) were recruited: Italy (n = 102), Poland (n = 91), Romania (n = 64), Austria (n = 47), and Israel (n = 40). At the end of the survey, the students were also invited to indicate whether they would agree to take part in a short interview on the topic. The use of data for research purposes was approved by the ethics committees of the participating universities.
The online questionnaire included the following demographic questions: age, gender, marital status, religion, level of observance, field of BA degree and whether the curriculum included any of the following course topics: death education, bereavement, loss, grief, palliative care, creative arts therapies, psychodrama, or none of these. Background information included: experience as a formal caregiver to end-of-life clients (e.g., at a hospice, hospital, non-governmental organization, etc.), loss of someone close in the last 2 years, having anyone close who currently has a terminal illness. Students were also asked about the master’s degree they were currently enrolled in, their year of study, and whether the curriculum included any of the abovementioned course topics. In terms of interests, all the students were asked about the general topics of the project: obtaining practical clinical skills for working with clients coping with end-of life conditions and/or bereavement, acquiring theoretical knowledge about end-of-life conditions and/or bereavement, actually working with these clients, and learning about arts therapies and/or psychodrama interventions for these clients. Responses were rated on a scale from 1 (Very disinterested) to 5 (Very interested). Although we considered it important and useful to probe the content of each specific item of interest, we also calculated an overall mean score for the five items with higher scores reflecting greater interest. The Cronbach’s alphas were: 0.87 for the total sample, 0.86 in Italy, 0.75 in Austria, 0.91 in Romania, 0.81 in Israel, and 0.86 in Poland.
In terms of student perceptions, the students were asked whether they believed in God, a higher power, a spiritual force, or other. They were also asked the extent to which they agreed with the following two items: death is terminal, and there is nothing after death, or death is a passage to another dimension where existence somehow continues. Responses to these two items were rated on a scale from 1 (Strongly disagree) to 5 (Strongly agree).
Two additional items assessed students’ intolerance of ambiguity in life: “the ambiguities in life stress me” and “uncertainty makes me uneasy, anxious, or stressed.” A mean score was calculated for the two intolerance items, with higher scores reflecting greater intolerance. The Cronbach’s alphas were: 0.74 for the total sample, 0.74 in Italy, 0.53 in Austria, 0.78 in Romania, 0.89 in Israel, and 0.72 in Poland. Responses for these two items were rated on the same type of five-point scale.
To assess confidence, students were asked the extent to which they agreed with six statements (based on Whittaker et al., 2013) that were rated on a five-point scale. An example item is “I am confident about helping people with their bereavement.” A mean score was calculated for the six items, with higher scores reflecting greater confidence. The Cronbach’s alphas were: 0.85 for the total sample, 0.74 in Italy, 0.87 in Austria, 0.86 in Romania, 0.89 in Israel, and 0.84 in Poland.
Qualitative interview data were collected by the research team in each country from students enrolled in their universities. The interviews were conducted by either a research assistant (with sufficient expertise and experience to conduct the interview) or the principal investigator in each country. It was clarified that participation was voluntary, and confidentiality and anonymity were guaranteed. All students responded to three qualitative opened-ended questions: What do life and death mean to you? How do you feel about studying palliative care and bereavement (theory and practice)? How do you feel about working with clients who are coping with terminal illness, loss, and bereavement? Interviews were held either face-to-face or via a videoconference platform, and lasted 30 min on average.
All the quantitative data from the survey were analyzed with SPSS for descriptive statistics, correlations, t-tests, and analysis of covariance for cross-country differences. Exploratory analyses of mediation models were examined through path analysis (i.e., structural equation modeling for observed variables), using the Lavaan software R package (Rosseel, 2012). Given the binary and ordinal nature of the data, the diagonally weighted least squares estimator was used. The fit of the mediation models to the data were evaluated using the criteria of a non-significant chi square, χ2/df ≤ 3, a comparative fit index (CFI) ≥ 0.95, a Tucker-Lewis coefficient (TLI) ≥ 0.95, a root mean square error of approximation (RMSEA) ≤ 0.08 (Schreiber et al., 2006).
Overall, for the qualitative data, 37 students were interviewed, on a first- come- first- served basis from among those who agreed to do so after completing the questionnaire. The purpose of the semi-structured interview was to explore the training needs of students in psychology in the field of DeEd and palliative and bereavement care in depth. Special attention was paid to the emotional impact of these themes on the students, how they perceived the training process, and what meanings they attached to life and death as deeply human and universal themes. In Austria, five MA students in psychology were interviewed (three females), aged 24–50. In Israel, five MA degree students in creative arts therapies were interviewed (three females), aged 28–46. In Italy, 27 MA students in psychology (17 females) were interviewed, aged 24–30. In Poland, five MA psychology students were interviewed (two females), aged 21–24. In Romania, five MA psychology students were interviewed (all female), aged 22–23. All the interviews were conducted in the country language. Data were analyzed separately in each country’s language for dominant themes by applying a thematic analysis procedure (Braun and Clarke, 2006). After the findings were thematically analyzed, all the emergent themes were reported in English by each country’s researcher. Next, all the themes were compared, contrasted, and integrated by one researcher from the project team who is an expert in qualitative analysis. The themes reported were common across all countries. Note that the fact that Italy had more interviewees did not impact the findings because the data were redundant and repetitive.
Demographics and Background. Out of the total sample of N = 344, most students (79%) were enrolled in psychology programs, but 11% from Israel were studying creative arts therapies, and 9% indicated “another” major. Most students (68%) were in their second year of MA studies. Most students were single (37%), Christian (66%), and 51% stated they believed in God. In addition, 13% reported having been the formal caregiver to end-of-life clients and 41% had lost someone close to them in the last 2 years. Most students (47%) reported that the BA degree curriculum did not include any courses on death, bereavement or palliative care, and most (38%) had never read anything on end-of-life, bereavement and/or palliative care. Most (43%) reported that their MA curriculum did not include courses on the topics investigated here. Only 13% of all the students reported currently having someone close to them suffering from a terminal illness. See Tables 1, 2 for global and country-specific data.
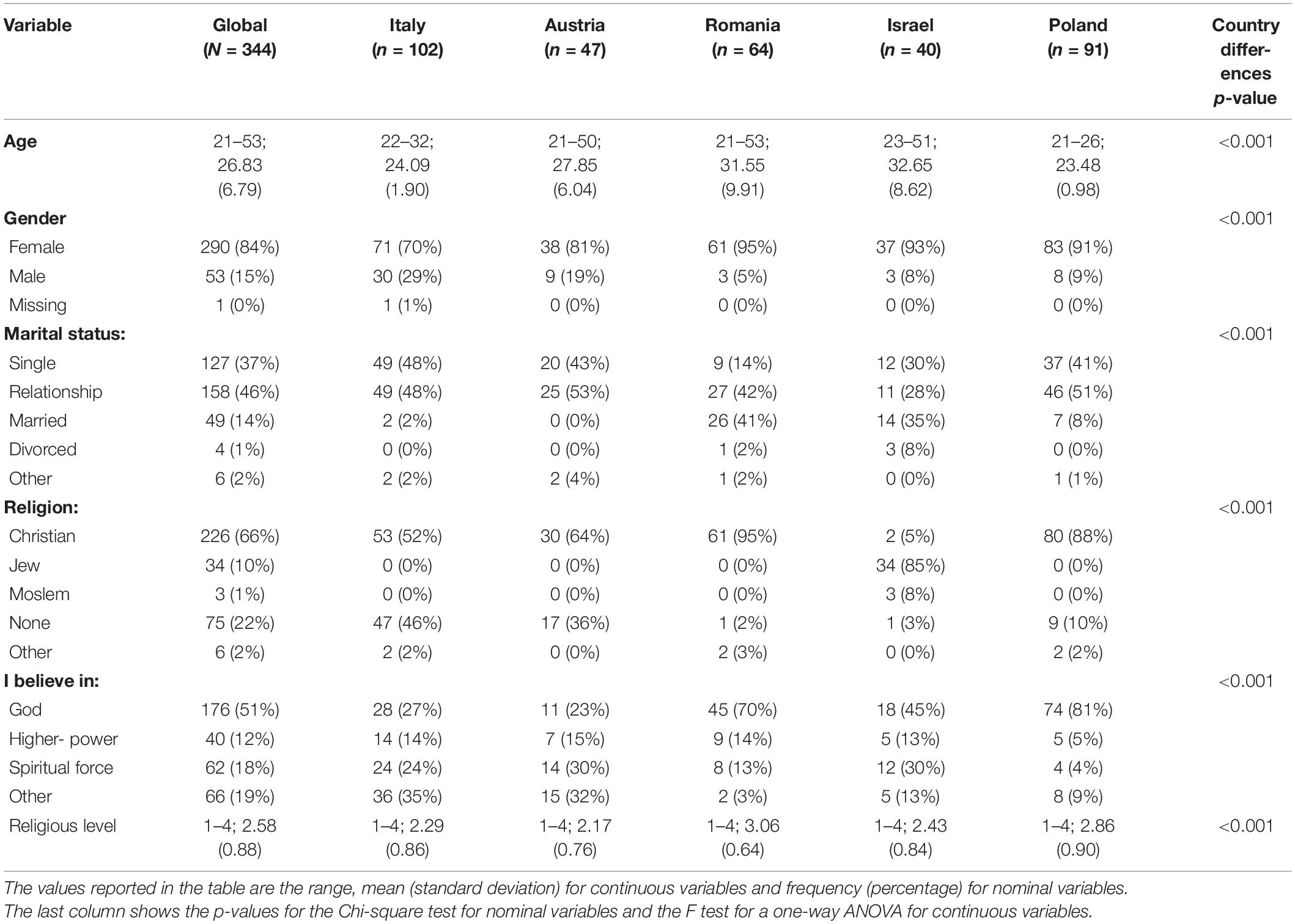
Table 1. Descriptive statistics for demographic variables and differences between countries for each variable.
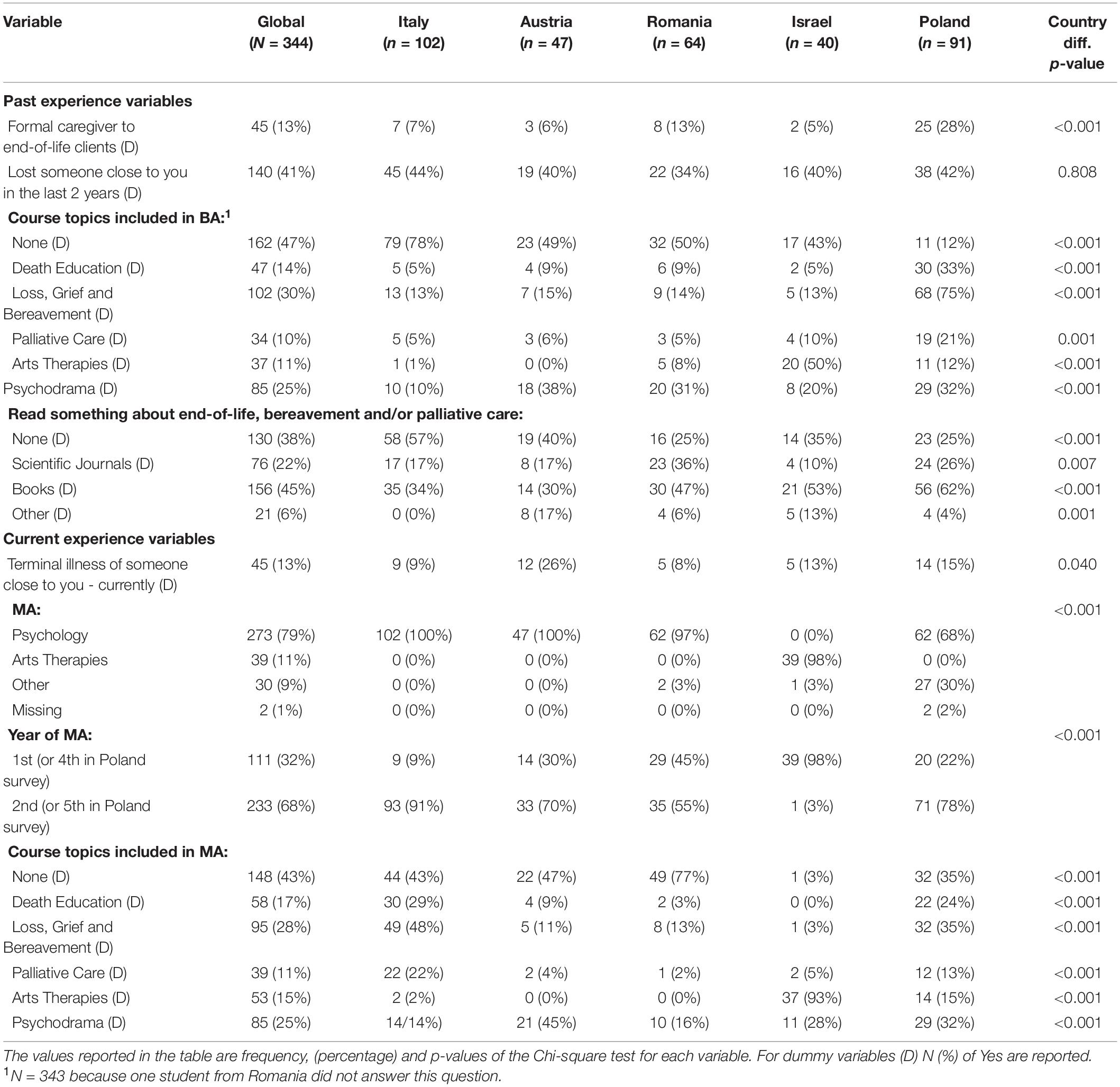
Table 2. Descriptive statistics for the student experience variables and differences between countries for each variable.
Student Interest. The analyses indicated that students’ reported interest in the project topics (5-item composite score) was positively correlated with age (r = 0.21, p < 0.001), level of religious observance (r = 0.12, p < 0.05) and was higher for females than males (t = 4.25, df = 341, p < 0.001, Cohen’s d = 0.56). Conversely, interest was negatively correlated with not having read anything about these topics (r = −0.26, p < 0.001).
Student Confidence. Student reported confidence about working in these fields (6-item composite score) was positively correlated with age (r = 0.26, p < 0.001), level of observance (r = 0.19, p < 0.001), past experience as formal caregiver to end-of-life clients (r = 0.11, p < 0.05), and past experience of losing someone close (r = 0.11, p < 0.05), although the latter correlations were small in magnitude. Students’ confidence negatively correlated with not having read anything about these topics before (r = −0.23, p < 0.001).
Student Perceptions. Perception of death as terminal was positively correlated to not having read anything about these topics previously (r = 0.23, p < 0.001) and not have any course about these topics in the BA curriculum (r = 0.21, p < 0.001); conversely, it correlated negatively with level of observance (r = −0.56, p < 0.05), past experience as a formal caregiver to end-of-life clients (r = −0.14, p < 0.05) and was lower for females than males (t = −2.89, df = 341, p < 0.01, Cohen’s d = −0.40). Perception of death as a passage positively correlated with level of observance (r = 0.55, p < 0.001), past experience as a formal caregiver to end-of-life clients (r = 0.18, p < 0.01) and was higher for females than males (t = 3.53, df = 341, p < 0.001, Cohen’s d = 0.49); conversely, it was negatively correlated to not having any course about these topics on the BA curriculum (r = −0.15, p < 0.01). Intolerance of ambiguity negatively correlated with age (r = −0.20, p < 0.001) and was higher for females than males (t = 3.45, df = 341, p < 0.01, Cohen’s d = 0.48).
Country Differences. As seen in Table 1, in terms of the dominant religion in each country, an expected statistically significant difference between Israel and other countries was found with a prevalence of Jews in Israel and a prevalence of Christians in all other countries. In addition, students from Italy, Austria, and Israel reported similar levels of religiosity with significantly lower scores than students from Romania. Students from Poland reported similar levels of religiosity as students from Romania, but they also reported significantly higher scores than students from Italy and Austria. As shown in Table 3, ANCOVAs for each target variable indicated statistically significant differences by country, with small to medium effect sizes. Compared to other countries, students from Poland reported less interest in studying these topics and reported less confidence about working in palliative and bereavement care. In contrast, students from Romania indicated more confidence and interest than students from Italy and also indicated more confidence than students from Austria. In Poland, fewer students perceived death as a terminal event, compared to Italy and Romania. Finally, intolerance of ambiguity was higher in Israel than in the other countries except Italy, whereas students from Italy reported more intolerance of ambiguity than students from Austria and Poland.
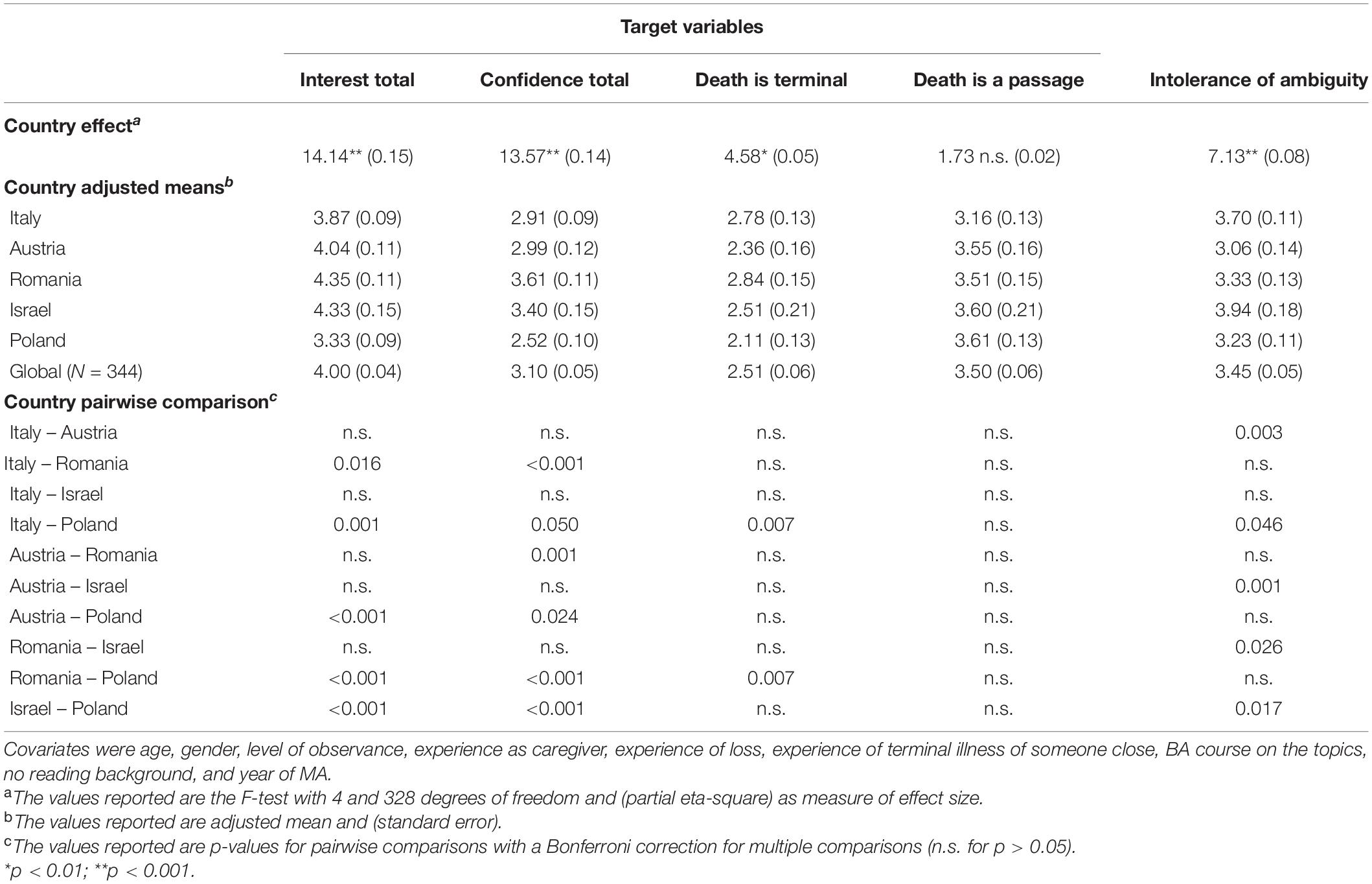
Table 3. ANCOVAs for country effect on target variables.
A mediation model was tested for the association between past care experiences and past loss experiences (as 2 distinct predictors) and the total interest score (as 1 outcome), with the total student score on confidence in palliative and bereavement care as the mediator. The effects of age, gender, and country on the mediator and outcome variables were controlled for. We started with a saturated model estimating all direct and indirect effects, which yielded no significant effects of age and no significant direct effect of past loss experiences on the outcome. The final model, without these non-significant effects, had good fit to the data: χ2/df = 0.248, CFI = 1.00, TLI = 1.00, RMSEA = 0.00. Significant indirect effects were found for both past care experiences (β = 0.05, z = 2.83, p = 0.005) and past loss experiences (β = 0.05, z = 2.39, p = 0.017), as depicted in Figure 1. As shown, there was also a significant direct effect of past care experiences on students’ interest (β = 0.11, z = 2.00, p = 0.045).
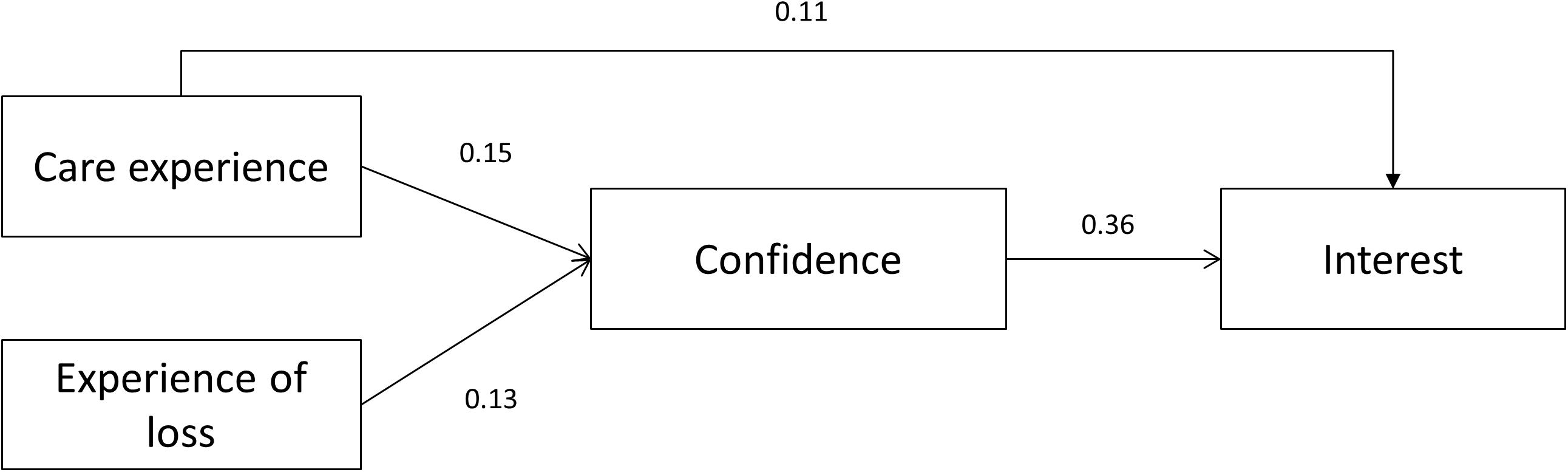
Figure 1. Mediation model with student competence as a mediator between past experiences and interests. Students’ past care experiences and past loss experiences related to students’ current interest in death education and palliative and bereavement care, through the mediation of their sense of confidence in this field. Coefficients presented are standardized linear regression coefficients. Control variables and non-significant paths are omitted for clarity. All p values are <0.05.
The integrated findings from the interviews of students from each county are presented in Table 4. Five shared themes emerged: life and death, learning about death, the psychological burden, personal experience and robust training, and four key training needs (Austria = AU, Israel = IL, Italy = IT, Poland = PL, Romania = RO). Overall, the qualitative findings suggested that the students’ interest in studying and working with terminal illness and death was impacted by internal resources and external requirements. Students’ beliefs about life and death, personal values, their own experience with illness and death, and openness to personal and professional growth appeared to be a foundation for training in the field of death, palliative and bereavement care. These factors are likely to shape students’ confidence in themselves and their ability to accept this challenge.
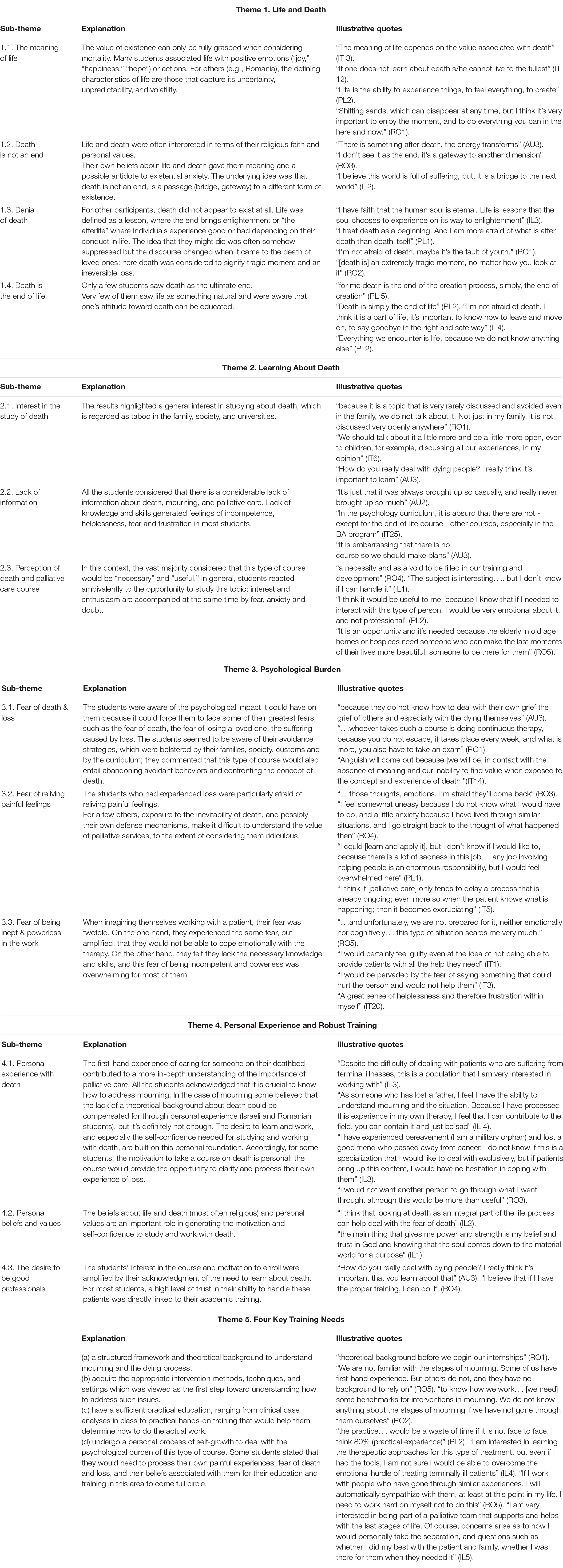
Table 4. Themes from qualitative analysis.
The purpose of this exploratory study was to assess how MA students in psychology and the arts therapies self-rate their confidence and interest in DeEd, palliative and bereavement care. Quantitatively, the students reported moderate levels of confidence in their ability to work with terminally ill patients (3 on a 1–5 scale), but older students exhibited greater confidence in their ability to work with these patients than younger students. This is consistent with findings showing that nurses’ age was correlated with positive attitudes toward death and caring for dying patients (Lange et al., 2008), as well as with the care staff’s self-efficacy toward end-of-life communication, in six European countries (ten Koppel et al., 2019).
Older students also seem to have more tolerance of ambiguity, similar to findings reported for Australian medical students (Leung et al., 2019). Notably, students with a greater tolerance of ambiguity may have greater ability to operate effectively in an uncertain or unpredictable situation (Merrill et al., 1994). The results suggested that younger students were more likely to have negative attitudes toward uncertain or unpredictable situations. The Israeli students had greater tolerance of ambiguity than students in other countries. This finding may be attributed to the constant uncertainty associated with the turbulent political situation and military conflict, which is reasonable because we assessed general intolerance of ambiguity in life, rather than ambiguity specific to PC or bereavement practices.
Previous experience as a formal caregiver for end-of-life clients and previous experience of losing someone close were associated with greater confidence in the ability to engage in palliative and bereavement care. This is generally consistent with findings that greater previous experience in working with dying patients is associated with a more positive attitude toward death and caring for dying patients in nurses (Lange et al., 2008; Peters et al., 2013). It is also consistent with the finding that greater self-confidence in a given vocational domain is positively correlated with greater interest in that domain (Bullock-Yowell et al., 2011). Congruently, high self-confidence in one’s abilities to learn and perform in a given domain and one’s strong interest in that domain are both potential determinants of a career choice (Betz and Rottinghaus, 2006).
Students from Romania reported the highest confidence and interest in working with terminally ill patients. These students’ interest may be attributed to the demand in Romania’s labor market for specialists in the field of palliative and bereavement care. Romanian students’ confidence may be attributed to several factors possibly associated with greater self-efficacy beliefs in their ability to work with dying and mourning patients. The quantitative and qualitative data suggest that these factors may include maturity and thus greater life experience, as well as field training in medical institutions, psychotherapy training in parallel to the MA which nurtures better self-understanding and management of negative emotions associated with death and dying, in addition to their higher levels of religiosity that may alleviate death anxiety (Solomon et al., 2017). In contrast, students from Poland reported the least confidence and interest, possibly because the members of this group were relatively younger (and consequently less mature) than the respondents from other countries. At the same time, they reported having taken more courses at the BA level related to death, loss, grief, bereavement, and palliative care. Most also reported a richer experience in reading books and scientific articles about end-of-life, bereavement and/or palliative care. Thus, although the Polish students were familiar with the theoretical literature, they were not confident about engaging in clinical work with end-of-life clients. This is consistent with the opinion expressed by one of the respondents in his qualitative interview about the importance of practical experience in education. On the other hand, a quarter of the Polish participants (more than in the other countries) had previous experience as the formal caregiver for end-of-life clients, probably mostly as volunteers. It can be assumed that this experience was both personally important but also difficult for young persons and could be correlated with the feeling of not being confident enough to work in this area.
In terms of practical considerations, healthcare students should be provided with the opportunity to learn more about the history and current situation of PC as well as the ethical and legal issues involved (Payne and Junger, 2011; Arias-Casais et al., 2019). A PC training curriculum should also consider students’ self-awareness and reflective processes in terms of their own experiences, values, and belief systems such as recognizing dying as an inevitable process in life. Death anxiety should also be addressed, because it has a negative impact on individuals’ care-taking abilities (Peters et al., 2013). Thus, given the association between death anxiety and religiosity, a quality PC training curriculum should also consider students’ levels of religiosity. Specifically, in countries where students have low or moderate religiosity (e.g., Austria, Italy, Israel) fostering profound contemplation of religious themes (death, the afterlife, spirituality, etc.) may facilitate the reduction of potentially deleterious death anxiety (Testoni et al., 2020a). Relatedly, to support diversity and a multicultural perspective, students should be given a comparative overview of death and dying in different religions (McClatchey and King, 2015). Other domains of competence include care planning and collaborative practice, cross-cultural perspectives on death, spiritual influences on the experience of dying and terminal illness, and learning about the mourning patterns of anticipatory and complicated grief. Healthcare students should be able to communicate skillfully and sensitively with patients, their families, and inter-professional teams within and outside the healthcare system (Connolly et al., 2016).
Many of these competencies can be fostered through experiential role plays and simulations which can contribute to better practical skills and improved emotional experiences in students’ clinical placement (Venkatasalu et al., 2015; Valen et al., 2020). Experiential training can also include practices offered by creative arts therapists who are credentialed healthcare professionals who have completed a MA and have clinical training in using the creative and expressive processes of art-making and its outcomes to ameliorate disabilities and illnesses and optimize health and well-being within a therapeutic relationship (Azoulay and Orkibi, 2015; Orkibi et al., 2017a, b; Orkibi, 2019; Orkibi and Feniger-Schaal, 2019; Feniger-Schaal and Orkibi, 2020; Shafir et al., 2020). The professional disciplines are visual/plastic art therapy, psychodrama, drama therapy, dance movement therapy, music therapy, and poetry/biblio therapy. These arts-based disciplines are especially valuable for clients who have difficulties expressing themselves in words alone. Creative arts therapists work with clients of all ages across a variety of settings, including in palliative and bereavement care (Hartley and Payne, 2008; Beilharz et al., 2018; Wood et al., 2019) as well as grief work (Blatner, 2000; Bolton, 2008; Thompson and Neimeyer, 2014; Brooke and Miraglia, 2015; Testoni et al., 2018). The use of the arts does not only help patients, but also families support their loved ones through the dying process and into bereavement. Studies have shown that terminal cancer patients in a hospice palliative care unit benefited from visual arts appreciation and hands-on creative artwork (Lefèvre et al., 2016). Painting permits patients to shift from a state of anxiety and existential dread to a more accepting, fluid awareness of the dying process. Additional benefits to the patient include improved quality of life, self-expression, and meaning-making (Safrai, 2013). Music has been found to help patients’ pain management and provide opportunities for self-expression (Gallagher, 2013). At the same time, music has also been used with both dying patients and their families to create lasting legacies prior to death, thus enabling the surviving family members find comfort after their loved one has passed away (O’Callaghan, 2013). Dance-movement based treatment has also been shown to allow patients to express interconnected physical and emotional pain, release tension, and reintegrate with their estranged bodies (Woolf and Fisher, 2015; Endrizzi et al., 2016). Drama and story-making have also been suggested as means of coping with death and despair and may instill hope during the period of bereavement (Gersie, 1992). Finally, the arts have also been used successfully with healthcare providers on a range of issues including visual art for burnout reduction in oncology and palliative care doctors (Tjasink and Soosaipillai, 2019), and drama for enhancing empathy and compassion in medical students (Deloney and Graham, 2003; Goodwin and Deady, 2013). Overall, this suggests that healthcare professions students enrolled in DeEd can benefit from both theoretical and experiential knowledge in the implementation of the arts in palliative and bereavement care. This type of training may also raise students’ awareness of arts-based services for patients, their family members, the healthcare team, and the community.
Three potential limitations of this study should be mentioned. One is the observational nature of the survey data, which precludes drawing causal inferences about the students’ actual acquisition of skills and knowledge. Future evaluations should therefore include data collected before and after training to examine actual competence and skill development. Also, while self-report data reflect students’ perceptions of their competence and skills, this may introduce social desirability and self-enhancing biases, as well as self-selection bias (Bethlehem, 2010). Therefore, data from trainers and/or supervisors should be triangulated with the students’ perceptions and to further clarify or confirm our data here. Finally, some of the small to moderate statistically significant correlations could be attributed to the large sample size.
Despite these limitations, the quantitative results and qualitative findings provide meaningful insights into the needs, perceptions, and experiences of both psychology and arts therapies MA students. An in-depth analysis of future data will further inform the design of a layered curriculum to adequately prepare students, on both the personal and professional levels, to competently care for clients who face death and loss.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by ethics committees of the participating universities. The patients/participants provided their written informed consent to participate in this study.
All authors contributed to the conception and design of the study, data collection and qualitative data analysis, and manuscript revision, read, and approved the submitted version. HO also contributed to quantitative data analysis.
This research was funded by the Erasmus+Program of the European Union. Specifically, the funding for this study comes from the Erasmus plus project: “Death Education for Palliative Psychology” (DE4PP), project code: 2019-1-IT02-KA203-063243.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Arias-Casais, N., Garralda, E., Rhee, J. Y., De Lima, L., Pons, J. J., Clark, D., et al. (2019). Atlas of Palliative Care in Europe 2019. Vilvoorde: EAPC Press.
Azoulay, B., and Orkibi, H. (2015). The four-phase CBN Psychodrama model: a manualized approach for practice and research. Arts Psychother. 42, 10–18. doi: 10.1016/j.aip.2014.12.012
Beilharz, K., Poulos, C., Poulos, R., Fodera, J., Cole, A., and MacLeod, R. (2018). “Creative art making in palliative care,” in Textbook of Palliative Care, eds R. D. MacLeod and L. Van den Block (Cham: Springer International Publishing), 1–21. doi: 10.1007/978-3-319-31738-0_38-1
Bethlehem, J. (2010). Selection bias in web surveys. Int. Stat. Rev. 78, 161–188. doi: 10.1111/j.1751-5823.2010.00112.x
Betz, N. E., and Rottinghaus, P. J. (2006). Current research on parallel measures of interests and confidence for basic dimensions of vocational activity. J. Career Assess. 14, 56–76. doi: 10.1177/1069072705281348
Blatner, A. (2000). “Psychodramatic methods for facilitating bereavement,” in Psychodrama with Trauma Survivors: Acting Out your Pain, eds P. F. Kellerman and M. K. Hudgins (London: Jessica kingsley publishers), 41–50.
Braun, V., and Clarke, V. (2006). Using thematic analysis in psychology. Qual. Res. Psychol. 3, 77–101. doi: 10.1191/1478088706qp063oa
Brooke, S. L., and Miraglia, D. A. (2015). Using the Creative Therapies to Cope with Grief and Loss. Springfield, IL: Charles C. Thomas Publisher.
Bullock-Yowell, E., Peterson, G. W., Wright, L. K., Reardon, R. C., and Mohn, R. S. (2011). The contribution of self-efficacy in assessing interests using the self-directed search. J. Couns. Dev. 89, 470–478. doi: 10.1002/j.1556-6676.2011.tb02844.x
Burke, B. L., Martens, A., and Faucher, E. H. (2010). Two decades of terror management theory: a meta-analysis of mortality salience research. Pers. Soc. Psychol. Rev. 14, 155–195. doi: 10.1177/1088868309352321
Claxton-Oldfield, S., Crain, M., and Claxton-Oldfield, J. (2006). Death anxiety and death competency: the impact of a palliative care volunteer training program. Am. J. Hosp. Palliat. Care 23, 464–468. doi: 10.1177/1049909106294882
Connolly, M., Ryan, K., and Charnley, K. (2016). Developing a palliative care competence framework for health and social care professionals: the experience in the Republic of Ireland. BMJ Support. Palliat. Care 6, 237–242. doi: 10.1136/bmjspcare-2015-000872
Corr, C., and Corr, D. (2003). “Death education,” in Handbook of Death & Dying, Vol. 1, ed. C. D. Bryant (Thousand Oaks, CA: Sage), 292–301.
Deloney, L. A., and Graham, C. J. (2003). Developments: wit: using drama to teach first-year medical students about empathy and compassion. Teach. Learn. Med. 15, 247–251. doi: 10.1207/S15328015TLM1504_06
DeSpelder, L. A., and Strickland, A. L. (2019). The Last Dance: Encountering Death and Dying, 11th Edn. New York, NY: McGraw-Hill Education.
Endrizzi, C., Ghelleri, V., Palella, M., and D’Amico, G. (2016). Movement psychotherapy in a hospice: two case studies. Body Mov. Dance Psychother. 11, 46–59. doi: 10.1080/17432979.2015.1110534
Feniger-Schaal, R., and Orkibi, H. (2020). Integrative systematic review of drama therapy intervention research. Psychol. Aesthet. Creat. Arts 14, 68–80. doi: 10.1037/aca0000257
Fonseca, L. M., and Testoni, I. (2012). The emergence of thanatology and current practice in death education. Omega 64, 157–169. doi: 10.2190/OM.64.2.d
Gallagher, L. (2013). Creative arts therapies for palliative medicine. Prog. Palliat. Care 21, 63–64. doi: 10.1179/0969926013Z.00000000073
Gersie, A. (1992). Storymaking in Bereavement: Dragons Fight in the Meadow. London: Jessica Kingsley.
Goodwin, J., and Deady, R. (2013). The art of mental health practice: the role of drama in developing empathy. Perspect. Psychiatr. Care 49, 126–134. doi: 10.1111/ppc.12004
Ivankova, N. V., Creswell, J. W., and Stick, S. L. (2006). Using mixed-methods sequential explanatory design: from theory to practice. Field Methods 18, 3–20. doi: 10.1177/1525822x05282260
Jong, J. (2021). Death anxiety and religion. Curr. Opin. Psychol. 40, 40–44. doi: 10.1016/j.copsyc.2020.08.004
Lange, M., Thom, B., and Kline, N. E. (2008). Assessing nurses’ attitudes toward death and caring for dying patients in a comprehensive cancer center. Oncol. Nurs. Forum 35, 955–959. doi: 10.1188/08.Onf.955-959
Lefèvre, C., Ledoux, M., and Filbet, M. (2016). Art therapy among palliative cancer patients: aesthetic dimensions and impacts on symptoms. Palliat. Support. Care 14, 376–380. doi: 10.1017/S1478951515001017
Leung, J., Cloninger, C. R., Hong, B. A., Cloninger, K. M., and Eley, D. S. (2019). Temperament and character profiles of medical students associated with tolerance of ambiguity and perfectionism. PeerJ 7:e7109. doi: 10.7717/peerj.7109
McClatchey, I. S., and King, S. (2015). The impact of death education on fear of death and death anxiety among human services students. Omega 71, 343–361. doi: 10.1177/0030222815572606
Merrill, J. M., Camacho, Z., Laux, I. F., Lorimor, R., Thornby, J. I., and Vallbona, C. (1994). Uncertainties and ambiguities: measuring how medical students cope. Med. Educ. 28, 316–322. doi: 10.1111/j.1365-2923.1994.tb02719.x
Neimeyer, R. A. (1994). Death Anxiety Handbook: Research, Instrumentation, and Application. New York, NY: Taylor & Francis.
O’Callaghan, C. (2013). Music therapy preloss care though legacy creation. Prog. Palliat. Care 21, 78–82. doi: 10.1179/1743291X12Y.0000000044
Orkibi, H. (2019). Positive psychodrama: a framework for practice and research. Arts Psychother. 66:101603. doi: 10.1016/j.aip.2019.101603
Orkibi, H., Azoulay, B., Regev, D., and Snir, S. (2017a). Adolescents’ dramatic engagement predicts their in-session productive behaviors: a psychodrama change process study. Arts Psychother. 55, 46–53. doi: 10.1016/j.aip.2017.04.001
Orkibi, H., Azoulay, B., Snir, S., and Regev, D. (2017b). In-session behaviours and adolescents’ self-concept and loneliness: a psychodrama process–outcome study. Clin. Psychol. Psychother. 24, O1455–O1463. doi: 10.1002/cpp.2103
Orkibi, H., and Feniger-Schaal, R. (2019). Integrative systematic review of psychodrama psychotherapy research: trends and methodological implications. PLoS One 14:e0212575. doi: 10.1371/journal.pone.0212575
Paal, P., Brandstötter, C., Lorenzl, S., Larkin, P., and Elsner, F. (2019). Postgraduate palliative care education for all healthcare providers in Europe: results from an EAPC survey. Palliat. Support. Care 17, 495–506.
Payne, S., and Junger, S. (2011). Guidance on postgraduate education for psychologists involved in palliative care. Eur. J. Palliat. Care 18, 238–252.
Peters, L., Cant, R., Payne, S., O’Connor, M., McDermott, F., Hood, K., et al. (2013). How death anxiety impacts nurses’ caring for patients at the end of life: a review of literature. Open Nurs. J. 7, 14–21. doi: 10.2174/1874434601307010014
Rosseel, Y. (2012). Lavaan: an R package for structural equation modeling and more. Version 0.5–12 (BETA). J. stat. softw. 48, 1–36.
Safrai, M. B. (2013). Art therapy in hospice: a catalyst for insight and healing. Art Ther. 30, 122–129. doi: 10.1080/07421656.2013.819283
Schreiber, J. B., Nora, A., Stage, F. K., Barlow, E. A., and King, J. (2006). Reporting structural equation modeling and confirmatory factor analysis results: a review. J. Edu. Res. 99, 323–338. doi: 10.3200/JOER.99.6.323-338
Shafir, T., Orkibi, H., Baker, F. A., Gussak, D., and Kaimal, G. (2020). Editorial: the state of the art in creative arts therapies. Front. Psychol. 11:68. doi: 10.3389/fpsyg.2020.00068
Solomon, S., Greenberg, J., and Pyszczynski, T. (2000). Pride and prejudice: fear of death and social behavior. Curr. Directions Psychol. Sci. 9, 200–204. doi: 10.1111/1467-8721.00094
Solomon, S., Testoni, I., and Bianco, S. (2017). Clash of civilizations? Terror Management Theory and the role of the ontological representations of death in contemporary global crisis. TPM Test. Psychom. Methodol. Appl. Psychol. 24, 379–398.
ten Koppel, M., Onwuteaka-Philipsen, B. D., van der Steen, J. T., Kylänen, M., Van den Block, L., Smets, T., et al. (2019). Care staff’s self-efficacy regarding end-of-life communication in the long-term care setting: results of the PACE cross-sectional study in six European countries. Int. J. Nurs. Stud. 92, 135–143. doi: 10.1016/j.ijnurstu.2018.09.019
Testoni, I. (2015). L’ultima nascita: Psicologia del morire e Death Education. Torino: Bollati Boringhieri.
Testoni, I., Biancalani, G., Ronconi, L., and Varani, S. (2019a). Let’s start with the end: bibliodrama in an italian death education course on managing fear of death, fantasy-proneness, and alexithymia with a mixed-method analysis. Omega J. Death Dying. doi: 10.1177/0030222819863613
Testoni, I., Bottacin, M., Fortuna, B. C., Zamperini, A., Marinoni, G. L., and Biasco, G. (2019b). Palliative care and psychology education needs in nursing courses: a focus group study among Italian undergraduates. Psicologia della Salute 2, 80–99. doi: 10.3280/PDS2019-002004
Testoni, I., Cordioli, C., Nodari, E., Zsak, E., Marinoni, G. L., Venturini, D., et al. (2019c). Language re-discovered: a death education intervention in the net between kindergarten, family and territory. Ital. J. Sociol. Educ. 11, 331–346.
Testoni, I., Palazzo, L., De Vincenzo, C., and Wieser, M. A. (2020a). Enhancing existential thinking through death education: a qualitative study among high school students. Behav. Sci. 10:113. doi: 10.3390/bs10070113
Testoni, I., Parise, G., Zamperini, A., Visintin, E. P., Toniolo, E., Vicentini, S., et al. (2016). The “sick-lit” question and the death education answer. Papageno versus Werther effects in adolescent suicide prevention. Hum. Affairs 26, 153–166. doi: 10.1515/humaff-2016-0016
Testoni, I., Piscitello, M., Ronconi, L., Zsák, É, Iacona, E., and Zamperini, A. (2019d). Death education and the management of fear of death via photo-voice: an experience among undergraduate students. J. Loss Trauma 24, 387–399. doi: 10.1080/15325024.2018.1507469
Testoni, I., Ronconi, L., Cupit, I. N., Nodari, E., Bormolini, G., Ghinassi, A., et al. (2020b). The effect of death education on fear of death amongst Italian adolescents: a nonrandomized controlled study. Death Stud. 44, 179–188. doi: 10.1080/07481187.2018.1528056
Testoni, I., Ronconi, L., Palazzo, L., Galgani, M., Stizzi, A., and Kirk, K. (2018). Psychodrama and moviemaking in a death education course to work through a case of suicide among high school students in italy [Original Research]. Front. Psychol. 9:441. doi: 10.3389/fpsyg.2018.00441
Thompson, B. E., and Neimeyer, R. A. (2014). Grief and the Expressive Arts: Practices for Creating Meaning. New York, NY: Routledge.
Tjasink, M., and Soosaipillai, G. (2019). Art therapy to reduce burnout in oncology and palliative care doctors: a pilot study. Int. J. Art Ther. 24, 12–20. doi: 10.1080/17454832.2018.1490327
Valen, K., Haug, B., Holm, A. L., Jensen, K. T., and Grov, E. K. (2020). From palliative care developed during simulation, to performance in clinical practice—descriptions from nursing students. J. Hosp. Palliat. Nurs. 22, 204–212. doi: 10.1097/njh.0000000000000644
Venkatasalu, M. R., Kelleher, M., and Shao, C. H. (2015). Reported clinical outcomes of high-fidelity simulation versus classroom-based end-of-life care education. Int. J. Palliat. Nurs. 21, 179–186. doi: 10.12968/ijpn.2015.21.4.179
Wallace, C. L., Cohen, H. L., and Jenkins, D. A. (2019). Transforming students’ attitudes and anxieties toward death and loss:The role of prior death experiences. Omega 79, 52–71. doi: 10.1177/0030222817710140
Whittaker, B., Watson, S., Todd, S., Broadhurst, D., and Faull, C. (2013). Evaluation Toolkit: Assessing Outcomes of End of Life Care Learning Events. Nottingham: University of Nottingham.
Wood, M. I. J. M., Jacobson, B., and Cridford, H. (2019). The International Handbook of Art Therapy in Palliative and Bereavement Care. New York, NY: Routledge.
Woolf, S., and Fisher, P. (2015). The role of dance movement psychotherapy for expression and integration of the self in palliative care. Int. J. Palliat. Nurs. 21, 340–348. doi: 10.12968/ijpn.2015.21.7.340
World Health Organization [WHO] (2020). WHO Definition of Palliative Care. https://www.who.int/cancer/palliative/definition/en/ (accessed June 20, 2020).
Keywords: palliative care, loss, bereavement, death education, arts therapies, psychodrama, students
Citation: Orkibi H, Biancalani G, Bucuţã MD, Sassu R, Wieser MA, Franchini L, Raccichini M, Azoulay B, Ciepliñski KM, Leitner A, Varani S and Testoni I (2021) Students’ Confidence and Interest in Palliative and Bereavement Care: A European Study. Front. Psychol. 12:616526. doi: 10.3389/fpsyg.2021.616526
Received: 13 October 2020; Accepted: 01 February 2021;
Published: 18 February 2021.
Edited by:
Manuel Fernández-Alcántara, University of Alicante, SpainReviewed by:
Cristina Monforte-Royo, International University of Catalonia, SpainCopyright © 2021 Orkibi, Biancalani, Bucuţã, Sassu, Wieser, Franchini, Raccichini, Azoulay, Ciepliñski, Leitner, Varani and Testoni. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hod Orkibi, aG9ya2liaUB1bml2LmhhaWZhLmFjLmls
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.