 Cláudia de Faria Cardoso1,2,3†
Cláudia de Faria Cardoso1,2,3† Natalia Tiemi Ohe1†
Natalia Tiemi Ohe1† Vera Lúcia Taba1,2Tamyres Tomaz Paiva4
Vera Lúcia Taba1,2Tamyres Tomaz Paiva4 Ovidiu Constantin Baltatu1,2,5*‡
Ovidiu Constantin Baltatu1,2,5*‡ Luciana Aparecida Campos1,2,6*‡
Luciana Aparecida Campos1,2,6*‡- 1Institute of Biomedical Engineering at Anhembi Morumbi University, Sao Jose dos Campos, Brazil
- 2Center of Innovation, Technology and Education (CITE) at Sao Jose dos Campos Technology Park, Sao Jose dos Campos, Brazil
- 3Hospital São Francisco de Assis, Jacareí, Brazil
- 4Federal University of Paraiba, Joao Pessoa, Brazil
- 5College of Medicine and Health Sciences, Khalifa University, Abu Dhabi, United Arab Emirates
- 6College of Health Sciences, Abu Dhabi University, Abu Dhabi, United Arab Emirates
Background: A short version of the Posttraumatic Diagnostic Scale (PDS) comprising only re-experiencing symptom items has been recently validated on Japanese adults. This short-version-PDS had good psychometric properties among Japanese adults with and without posttraumatic stress disorder (PTSD). The aim of this study was to translate and culturally validate the short-version-PDS for the Brazilian sociolinguistic context.
Methods: A translation of the short-version-PDS was performed based on established guidelines. We enrolled 53 patients with PTSD as a potential comorbidity. The translation and cross-cultural adaptation of the short-version-PDS included forward and back-translation by a Japanese Brazilian researcher and a certified translator; synthesis was achieved by consensus, backward translation, pilot test, and finalization. Content validity coefficient (CVC) was used to assess quality of adaptation. Internal consistency was calculated using Cronbach's alpha coefficient. Spearman correlations were between the new short-version-PDS and the Brazilian version of the posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5), and a receiver operating characteristic (ROC) curve was used to determine the best cut-off values for the short-version-PDS.
Results: The short-version-PDS was well accepted by all subjects, none of the questions were experienced as inappropriate, and all questions of the 3 items were judged important. Item 1 presented CVCt = 0.92; item 2 had a CVCt = 0.87 and item 3 had a CVCt = 0.95. The internal consistency of the final version as measured by Cronbach's alpha was 0.78. The short-version-PDS scale correlated positively with the DSM-5 scale with a Spearman rho of 0.64 (95%CI [0.4-0.8], p < 0.001). The receiver operating characteristic (ROC) curve value was 0.97 (95%CI [0.9-1.0], p < 0.001). The cut-off score for a maximum Youden Index of 0.8 to distinguish moderate from severe from slight PTSD was > 31.0 with sensitivity and specificity are 86.4 and 93.5%, respectively.
Conclusions: This Brazilian Portuguese version of the short-version-PDS had good psychometric properties among Brazilian adults with and without PTSD. Transferability and generalizability of the cut-off scores should be further analyzed.
Background
Mental health has been the focus of increasing attention due to the risks of those exposed to emergency settings, as they may be affected by physical and mental disorders, such as burnout and posttraumatic stress disorder (PTSD) (Carmassi et al., 2020). Mental health has been identified as a research area with potential benefits for research prioritization and policy setting in both the COVID-19 pandemic and future large-scale public health crises (Liu et al., 2020). The COVID-19 pandemics caused striking prevalence rates of symptoms of depression and anxiety (Lai et al., 2020; Perlis, 2020; Tan et al., 2020).
Post-traumatic stress disorder (PTSD) has consequences that can lead to poor quality of life and increased use of health and social services (Atwoli et al., 2015; Bothe et al., 2020). It is a problem that can affect people who directly experience or witness potentially stressful situations (Association Psychiatric Association, 2013), and it is twice as common in women than in men (Yehuda et al., 2015). The overall lifetime prevalence of PTSD reported in the World Mental Health Surveys studies was 3.9% for a randomly selected trauma (Kessler et al., 2017). The prevalence of PTSD in the Brazilian population, as well as has been reported over the years and in other countries, varies according to the social, economic, and demographic context (Ribeiro et al., 2013). Despite being a highly prevalent disorder, it is commonly underdiagnosed (da Silva et al., 2019). Early diagnosis can favor treatment, reducing the impairment in the daily activities of the affected person. Screening tools can be facilitators in the search for diagnosis (Price et al., 2016). Screening scales are especially useful when time is short and demand is high, as is the case in situations of natural disasters, accidents, war conflicts and pandemics. In cases like these, time and resources are scarce and short scales are even more advantageous (Itoh et al., 2017b). While self-report instruments cannot be used for diagnosis, the availability of brief assessment tools often determines whether or not a condition is assessed. For example, a two-item depression screening instrument (Löwe et al., 2005) has significantly improved the frequency with which the disorder is evaluated. Selecting the most appropriate validated collection tool for measurable outcomes to use is essential for successful patient-centered healthcare (Botero et al., 2016). For this, limiting the number of data collection points through developing and validating short versions of surveys/questionnaires to prevent survey fatigue are of interest. Short PTSD scales are being developed screening tools that are best suited to the primary care setting and for those re-experiencing PTSD symptoms (Spoont et al., 2013).
A short version of the Posttraumatic Diagnostic Scale (PDS) comprising only re-experiencing symptom items has been recently validated on Japanese adults (Itoh et al., 2017a). This Japanese short version of the Post-Traumatic Diagnosis scale (short-version-PDS) was developed based on the symptoms of trauma re-experience, because it considers them as differential for the diagnosis, because it is more related to the general severity of the symptoms and because other symptoms are ambiguous for the diagnosis (Itoh et al., 2017b). The scale consists of three items with a Likert scale for the intensity of the symptom mentioned in each item. The Japanese short-version-PDS 3-item scale has good psychometric properties among Japanese adults with and without PTSD (Itoh et al., 2017a) and has been utilized to build prediction models for depressive symptoms in large population studies (Takahashi et al., 2020). This short-version-PDS 3-item scale comprising “intrusive images (B1),” “nightmares (B2),” and “physiological reactions when reminded of the trauma (B5),” and the 2-item scale of “nightmares (B2)” and “physiological reactions when reminded of the trauma (B5)” had the highest AUCs and were generally higher than were those for previous short scales to diagnose the PTSD severity score (Itoh et al., 2017a).
Since the Japanese short-version-PDS is highly correlated with a PTSD severity score and has good psychometric properties among adults with and without PTSD (Itoh et al., 2017b), the aim of this study was to translate and culturally validate the Japanese short-version-PDS for the Brazilian sociolinguistic context.
Methods
Ethical Approval
Permission to translate the scale was obtained from the original author, Itoh et al. (2017a). All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study was approved by the Medical Ethics Committee of Anhembi Morumbi University in accordance with resolution 466/2012 and 340/2004 of the National Health Council (Ministry of Health) for research on human beings (CAAE 13494719.7.0000.5492).
Study Participants
All subjects participating to the study were recruited from voluntary patients at the Hospital São Francisco de Assis, Jacareí—SP, Brazil. The final version of the Portuguese translation of the short-form PDS was extended to 53 volunteers who were referred to the clinical psychology unit from other clinical units on the basis of potentially traumatic experience. Only volunteers with at least one potentially traumatic experience were included. Patients with PTSD as a potential comorbidity, such as pregnancy loss, cancer diagnosis, and end-stage renal disease patients on hemodialysis, were recruited from the Hospital São Francisco de Assis' maternity, oncology, and hemodialysis clinics. The research was performed from September 2019 to June 2020. Participants were aged 19-66 years (Mean = 32.37; SD = 10.06), most were female (88.4%), married or cohabiting (69.8%), with completed high school (69.8%). Retrospective baseline demographic information and clinical data were collected. Patient-level data were anonymized by removing all patient-identifying details and allocating a unique study code to each recording. Written informed consent was obtained from all subjects.
Instruments: Short-Version-PDS and DSM-5 Scales
The short-version-PDS is a self-assessment tool that seeks to investigate the intrusive symptoms that define the diagnosis of PTSD in adults (Itoh et al., 2017b). It consists of a list of potentially traumatic events and contains three of the five statements listed in DSM-5 “Diagnostic Criterion B.” The instruction is to consider the symptoms perceived in the last thirty days. To assess the severity of the symptom, short-version-PDS involves a Likert-type scale, with four response options, ranging from 0 to 3, corresponding to “No time / Only once,” “Less than once a week/Sometimes,” “Two to four times a week/Many times,” “Five or more times a week/Almost always.” The scale has a minimum score of 0 points and a maximum of 9 points.
To test the short-version-PDS translation in Brazilian, the Brazilian version of the posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5) was used as a comparison (Osório et al., 2017). The PCL-5 consists of 20 items that are used to test for PTSD symptoms as described by the DSM-5. Respondents use a 5-point scale (0–4) to show how much the symptom bothered them in the previous month for each of the 20 things, ranging from “not at all” to “extremely.” A cutoff point of 36 presented the higher overall efficiency for predicting a PTSD diagnosis (Pereira-Lima et al., 2019).
Translation and Cultural Adaptation
The method adopted for the cross-cultural adaptation of the screening scale was based on the model proposed by Beaton et al. (2000). Three translations from Japanese into Portuguese Brazilian were carried out by bilingual translators. The first translator was instructed on the research. The other translators were unaware of the research and carried out the translation in order to find cultural, semantic, and idiomatic adaptations. The consensus of the translations was reached, and the result was analyzed by two of the translators, one with knowledge of the research, the other not. Then, back-translation and pilot test were performed with six volunteers. The final analysis was carried out by a committee of health experts with experience in assisting people with a traumatic history. The panel of experts were professionals with training in the medical, nursing, occupational therapy, psychology and social programs.
For theoretical analysis of the 3 items of the instrument, the experts evaluated the 3 translations and the synthesis under the criteria of the content validity technique. The evaluation criteria were semantic, linguistic, cultural, conceptual, clarity, and precision (Beaton et al., 2000). The content validity coefficient (CVC) was calculated for each item of the instrument and for the instrument as a whole (CVCt) (Filgueiras and Hall, 2017). The CVC values accepted to consider the quality of an aspect or item judged must be >0.80 (Filgueiras and Hall, 2017).
The panel of experts measured the translations on a Likert scale ranging from 1 “very poor” to 4 “very good” in each of the items of short-version-PDS in order to assess the level of adequacy of the translation in relation to the proposed listed points. The questionnaires were applied in a private hospital, with mixed clientele (SUS, private, plans).
Data Analysis
Internal consistency refers to how accurately survey or test items intended to evaluate the same construct actually do so. Internal consistency was assess using Cronbach's alpha coefficient which is a measure of scale reliability (MEDCALC, MedCalc Software Ltd., Ostend, Belgium, www.medcalc.org). An acceptable internal consistency, defined by Cronbach's alpha coefficient, ranged from 0.7 to 0.95 (Bland and Altman, 1997).
The validity of a test depends on the hypothesis presented for the proposed application of the test, the degree to which it claims to assess a construct (Cordeiro et al., 2020). Convergent validity refers to how closely the new scale is related to other measurements and variables of the same construct (Krabbe, 2017). Divergent validity investigates whether structures that are supposed to be unrelated are actually unrelated. For validity testing, we used Spearman's correlation coefficient r to measure a relationship between the Portuguese Brazilian versions of the short-version-PDS and DMS-5 scales. The correlation intensity was rated as negligible (0.30), low (0.30 to 0.50), moderate (0.51 to 0.70), high (0.71 to 0.90), and very high (>0.90) (Mukaka, 2012).
Diagnostic utility was evaluated using the area under the receiver-operating characteristic (ROC). To measure the diagnostic accuracy, the following indices were used: area under the curve (AUC) with standard error (SE) and its binomial exact 95% confidence interval; Youden's J index; sensitivity (Sn); specificity (Sp). Spearman's correlation coefficient and ROC were done using GraphPad Prism version 6.0e for Mac OS X, GraphPad Software, La Jolla California USA, www.graphpad.com.
Results
Translation and Cross-Cultural Adaptation Process of the Short-Version-PDS
The final version of the Brazilian Short-Version-PDS is attached as Supplementary Material 1.
In the pre-test, the experts indicated the synthesis for the three items evaluated as the best representation with CVC coefficients > 0.70 (Table 1). Although translation 2 of item 1 reached a coefficient above the cutoff point, the synthesis in this item and in the others reached the highest score. If the coefficients are below the cutoff point, this item must be reformulated and sent to the judges again. As our goal was to find the best translation, we found the one with the highest agreement rate. Therefore, the translation that best suits the characteristics of PTSD, consisted of the translation synthesis. The calculation of the total content validity (CVCt) also demonstrated that the synthesis for all items is more suitable for test applications. This is because the experts mostly agreed that this item is the one that best represents PTSD. Item 1 presented CVCt = 0.92; item 2 had a CVCt = 0.87 and item 3 had a CVCt = 0.95.
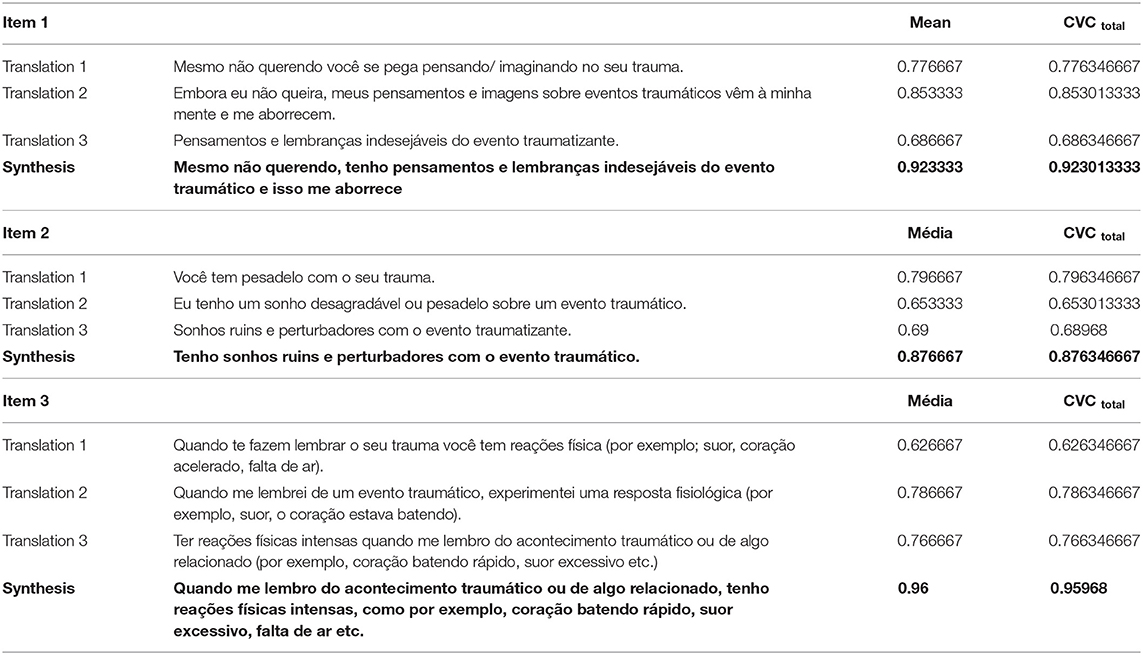
Table 1. Brazilian translation and synthesis of the three Short-Version-PDS items.
For the analysis of the final version, reliability was performed using Cronbach's alpha (0.78), which proved to be statistically significant.
Correlation Between the Translated Short-Version-PDS and the DMS-5 Scale
There was a strong positive correlation between the two Portuguese Brazilian versions of the short-version-PDS and DMS-5 scales as indicated by a Spearman's rho of 0.64 (95%CI: 0.44 to 0.78).
Prediction Value of the Translated Short-Version-PDS for the Severity of PTSD
The calculated area under a ROC curve was 0.97 ± 0.02 with significance value of P < 0.0001 (Figure 1). The short-version-PDS is good at distinguishing between patients with aggravated (mild, moderate, and severe) and those with slight disease diagnosed with DSM-5 score, with a cutoff value > 31 and a sensitivity prediction of 86.4% and specificity 93.5%.
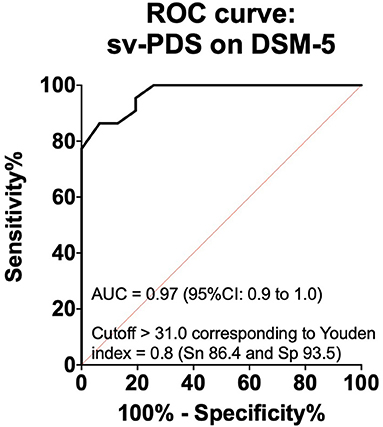
Figure 1. Receiver operating characteristic (ROC) curve for sv-PDS (short version of the Posttraumatic Diagnostic Scale) for the diagnosis of PTSD.
Discussion
The results of this study showed the psychometric adequacy of Brazilian Portuguese translation of a Japanese short-version-PDS, suggesting that the instrument is adequate for use in Brazilian contexts. This Brazilian translation and cross-cultural adaptation of the Japanese short-version-PDS was found to have good reliability, validity, and diagnostic utility.
The goal of the content analysis was to analyze the cross-cultural adaptation and content validity of the Japanese short-version-PDS 3-item scale as a tool for assessing PTSD in Brazilian population. The Japanese short-version-PDS was compared to the Japanese PTSD checklist for DSM-IV (PCL) (which are the same as those in the DSM-5) (Asukai et al., 2003; Itoh et al., 2017a). Similarly, in this study, we compared PTSD diagnosis using the Brazilian version of the latest short-version-PDS to PTSD diagnosis using the Brazilian version of the PCL-5, which has demonstrated high reliability and diagnostic utility for PTSD (Pereira-Lima et al., 2019).
The translated version reached an adequate degree of agreement by the expert panel when assessed its equivalence in terms of several criteria (i.e., semantic, linguistic, cultural, conceptual, clarity, and precision) through a quantitative measurement (CVC calculation). The final structure of the content analysis consistency with the original scale allowed subjects with PTSD to be evaluated in the Portuguese-speaking context.
The volunteers in this study had a direct exposure to a traumatic incident as described by DSM-5 Criterion A for PTSD, which included medical conditions such as cardiovascular (Remch et al., 2018), oncology (Cordova et al., 2017), and obstetrics and gynecology (Canfield and Silver, 2020), as well as work-related events (Giorgi et al., 2020). When tested on volunteers with at least one potentially traumatic experience, the Brazilian short-version-PDS had a strong positive correlation with the validated Brazilian DMS-5 scale in diagnostic abilities for PTSD between, as indicated by Spearman's rho and ROC curve, and defined as strong correlation > 0.60 in behavioral sciences (Cohen, 1988). This indicates that the new Brazilian short-version-PDS has convergent validity, that is, that the two instruments measure the same theoretical construct, that is, they measure Post Traumatic Stress Disorder.
Public health crises such as COVID-19 pandemic have provided significant challenges for mental health care systems. In such crises, reconsidering ways of working in a rapid time scale are of major interest (Smith et al., 2020). During such public health crises, developing and applying valid short screening tools are necessary to identify high-risk groups for posttraumatic stress disorder (PTSD) (Itoh et al., 2017a).
Limitations of the Study
There are several limitations that should be taken into consideration. Although the Brazilian short-version-PDS demonstrated content validity, it is not without limitations, one of which is that it needs to be applied to a larger sample for a factorial validity. Due to the sample size, the results of this study could be deemed as “preliminary results.” Since the participants were drawn from a single hospital, they could not represent all Brazilians. Furthermore, due to practical constraints, we did not assess the test–retest reliability. Finally, in order to demonstrate more proof of validity, we must conduct additional research to determine if the short-version-PDS and DSM-5 PTSD scales are linked to a specific factor (e.g., emotional exhaustion, tension, anxiety) and if there is reciprocity in the existing relationships.
Conclusion
This study indicates that the Brazilian short-version-PDS had good psychometric properties among Brazilian adults with and without PTSD. This scale showed internal consistency, validity and diagnostic utility. Follow up studies will allow to screen patients while minimize contact (self-rating), as is common with internet surveys. Transferability and generalizability of the cut-off scores should be further analyzed.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Medical Ethics Committee of Anhembi Morumbi University. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
CdF, LC, and OB: study conception and design. CdF, and NO: performed the study. CdF, VT, TP, LC, and OB: assays and data analysis. CdF, NO, VT, TP, LC, and OB: interpretation of the data. OB and LC: writing of the manuscript. CdF, NO, VT, and TP: critical revision of the manuscript regarding the important intellectual content. All authors contributed to the article and approved the submitted version.
Funding
This research was funded by the Center of Innovation, Technology and Education (CITE, 2018-005) and by Khalifa University of Science and Technology (Award No. FSU-2020-33) to OB. OB was supported by the National Council for Scientific and Technological Development (CNPq, 307760/2018-9). CF received an Anhembi Morumbi University—Laureate International Universities Master's scholarship.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2021.614554/full#supplementary-material
References
Association and Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders. Philadelphia, PA: Association and Psychiatric Association.
Asukai, N., Hirohata, S., Kato, H., and Konishi, T. (2003). Psychometric properties of the Japanese-language version of the clinician-administered PTSD scale for DSM-IV. Jap. J. Traum.Stress 1:47–53.
Atwoli, L., Stein, D. J., Koenen, K. C., and McLaughlin, K. A. (2015). Epidemiology of posttraumatic stress disorder: prevalence, correlates and consequences. Curr. Opin. Psychiatry 28, 307–311. doi: 10.1097/YCO.0000000000000167
Beaton, D. E., Bombardier, C., Guillemin, F., and Ferraz, M. B. (2000). Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 25, 3186–3191. doi: 10.1097/00007632-200012150-00014
Bland, J. M., and Altman, D. G. (1997). Cronbach's alpha. BMJ 314, 572. doi: 10.1136/bmj.314.7080.572
Botero, J. P., Thanarajasingam, G., and Warsame, R. (2016). Capturing and incorporating patient-reported outcomes into clinical trials: practical considerations for clinicians. Curr. Oncol. Rep. 18:61. doi: 10.1007/s11912-016-0549-2
Bothe, T., Jacob, J., Kröger, C., and Walker, J. (2020). How expensive are post-traumatic stress disorders? Estimating incremental health care and economic costs on anonymised claims data. Eur. J. Health Econ. 21, 917–930. doi: 10.1007/s10198-020-01184-x
Canfield, D., and Silver, R. M. (2020). Detection and prevention of postpartum posttraumatic stress disorder: a call to action. Obstet. Gynecol. 136, 1030–1035. doi: 10.1097/AOG.0000000000004093
Carmassi, C., Foghi, C., Dell'Oste, V., Cordone, A., Bertelloni, C. A., Bui, E., et al. (2020). PTSD symptoms in healthcare workers facing the three coronavirus outbreaks: What can we expect after the COVID-19 pandemic. Psychiatry Res. 292:113312. doi: 10.1016/j.psychres.2020.113312
Cohen (1988). Statistical Power Analysis for the Behavioral Sciences. 2nd ed. New Jersey, NJ: Lawrence Erlbaum Associates. doi: 10.4324/9780203771587
Cordeiro, L., Villagomez, A., Swain, D., Deklotz, S., and Tartaglia, N. (2020). Adaptive skills in FXS: a review of the literature and evaluation of the PEDI-computer adaptive test (PEDI-CAT) to measure adaptive skills. Brain Sci. 10:351. doi: 10.3390/brainsci10060351
Cordova, M. J., Riba, M. B., and Spiegel, D. (2017). Post-traumatic stress disorder and cancer. Lancet Psychiatry 4, 330–338. doi: 10.1016/S2215-0366(17)30014-7
da Silva, H. C., Furtado da Rosa, M. M., Berger, W., Luz, M. P., Mendlowicz, M., Coutinho, E. S. F., et al. (2019). PTSD in mental health outpatient settings: highly prevalent and under-recognized. Rev. Bras. Psiquiatr. 41, 213–217. doi: 10.1590/1516-4446-2017-0025
Filgueiras, A., and Hall, C. R. (2017). Psychometric properties of the Brazilian-adapted version of Sport Imagery Questionnaire. Psicol. Reflex. Crit. 30:22. doi: 10.1186/s41155-017-0075-7
Giorgi, G., Lecca, L. I., Alessio, F., Finstad, G. L., Bondanini, G., Lulli, L. G., et al. (2020). COVID-19-related mental health effects in the workplace: a narrative review. Int. J. Environ. Res. Public Health 17:57. doi: 10.3390/ijerph17217857
Itoh, M., Ujiie, Y., Nagae, N., Niwa, M., Kamo, T., Lin, M., et al. (2017a). A new short version of the Posttraumatic Diagnostic Scale: validity among Japanese adults with and without PTSD. Eur. J. Psychotraumatol. 8:1364119. doi: 10.1080/20008198.2017.1364119
Itoh, M., Ujiie, Y., Nagae, N., Niwa, M., Kamo, T., Lin, M., et al. (2017b). The Japanese version of the Posttraumatic Diagnostic Scale: Validity in participants with and without traumatic experiences. Asian J. Psychiatr. 25, 1–5. doi: 10.1016/j.ajp.2016.09.006
Kessler, R. C., Aguilar-Gaxiola, S., Alonso, J., Benjet, C., Bromet, E. J., Cardoso, G., et al. (2017). Trauma and PTSD in the WHO world mental health surveys. Eur. J. Psychotraumatol. 8:1353383. doi: 10.1080/20008198.2017.1353383
Krabbe, P. F. M. (2017). “Chapter 7-Validity,” in The Measurement of Health and Health. Cambridge, MA: Academic Press.
Lai, J., Ma, S., Wang, Y., Cai, Z., Hu, J., Wei, N., et al. (2020). Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw. Open 3:e203976. doi: 10.1001/jamanetworkopen.2020.3976
Liu, N., Chee, M. L., Niu, C., Pek, P. P., Siddiqui, F. J., Ansah, J. P., et al. (2020). Coronavirus disease 2019 (COVID-19): an evidence map of medical literature. BMC Med. Res. Methodol. 20:177. doi: 10.1186/s12874-020-01059-y
Löwe, B., Kroenke, K., and Gräfe, K. (2005). Detecting and monitoring depression with a two-item questionnaire (PHQ-2). J. Psychosom. Res. 58, 163–171. doi: 10.1016/j.jpsychores.2004.09.006
Mukaka, M. M. (2012). Statistics corner: a guide to appropriate use of correlation coefficient in medical research. Malawi Med. J. 24, 69–71.
Osório, F. L., Silva, T. D. A. D., Santos, R. G. D., Chagas, M. H. N., Chagas, N. M. S., Sanches, R. F., et al. (2017). Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): transcultural adaptation of the Brazilian version. Arch. Clin. Psychiatry (São Saulo) 44, 10–19. doi: 10.1590/0101-60830000000107
Pereira-Lima, K., Loureiro, S. R., Bolsoni, L. M., Apolinario da Silva, T. D., and Osório, F. L. (2019). Psychometric properties and diagnostic utility of a Brazilian version of the PCL-5 (complete and abbreviated versions). Eur. J. Psychotraumatol. 10:1581020. doi: 10.1080/20008198.2019.1581020
Perlis, R. H. (2020). Exercising heart and head in managing coronavirus disease 2019 in wuhan. JAMA Netw. Open 3:e204006. doi: 10.1001/jamanetworkopen.2020.4006
Price, M., Szafranski, D. D., van Stolk-Cooke, K., and Gros, D. F. (2016). Investigation of abbreviated 4 and 8 item versions of the PTSD Checklist 5. Psychiatry Res. 239, 124–130. doi: 10.1016/j.psychres.2016.03.014
Remch, M., Laskaris, Z., Flory, J., Mora-McLaughlin, C., and Morabia, A. (2018). Post-traumatic stress disorder and cardiovascular diseases: a cohort study of men and women involved in cleaning the debris of the world trade center complex. Circ. Cardiovasc. Qual. Outcomes 11:e004572. doi: 10.1161/CIRCOUTCOMES.117.004572
Ribeiro, W. S., Mari, J., de, J., Quintana, M. I., Dewey, M. E., Evans-Lacko, S., et al. (2013). The impact of epidemic violence on the prevalence of psychiatric disorders in São Paulo and Rio de Janeiro, Brazil. PLoS ONE 8:e63545. doi: 10.1371/journal.pone.0063545
Smith, K., Ostinelli, E., Macdonald, O., and Cipriani, A. (2020). COVID-19 and telepsychiatry: an evidence-based guidance for clinicians. JMIR Ment Health. 7:e21108. doi: 10.2196/21108
Spoont, M., Arbisi, P., Fu, S., Greer, N., Kehle-Forbes, S., Meis, L., et al. (2013). Screening for Post-Traumatic Stress Disorder (PTSD) in Primary Care: A Systematic Review. Washington, DC: Department of Veterans Affairs.
Takahashi, Y., Ueki, M., Yamada, M., Tamiya, G., Motoike, I. N., Saigusa, D., et al. (2020). Improved metabolomic data-based prediction of depressive symptoms using nonlinear machine learning with feature selection. Transl. Psychiatry 10:157. doi: 10.1038/s41398-020-0831-9
Tan, B. Y. Q., Chew, N. W. S., Lee, G. K. H., Jing, M., Goh, Y., Yeo, L. L. L., et al. (2020). Psychological impact of the COVID-19 pandemic on health care workers in Singapore. Ann. Intern. Med. 173, 317–320. doi: 10.7326/M20-1083
Keywords: posttraumatic diagnostic scale, cross-cultural adaptation, Brazil, content validity coefficient, receiver operating characteristic (ROC) curve analysis
Citation: de Faria Cardoso C, Ohe NT, Taba VL, Paiva TT, Baltatu OC and Campos LA (2021) Cross-Cultural Adaptation, Reliability, and Validity of a Brazilian of Short Version of the Posttraumatic Diagnostic Scale. Front. Psychol. 12:614554. doi: 10.3389/fpsyg.2021.614554
Received: 12 October 2020; Accepted: 23 March 2021;
Published: 23 April 2021.
Edited by:
Christian Franceschini, University of Parma, ItalyReviewed by:
Serena Scarpelli, Sapienza University of Rome, ItalyVittorio Lenzo, Università per Stranieri Dante Alighieri, Italy
Copyright © 2021 de Faria Cardoso, Ohe, Taba, Paiva, Baltatu and Campos. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Luciana Aparecida Campos, Y2FtcG9zYmFsdGF0dSYjeDAwMDQwO2dtYWlsLmNvbQ==; Ovidiu Constantin Baltatu, b2NiYWx0YXR1JiN4MDAwNDA7Z21haWwuY29t
†These authors have contributed equally to this work
‡These authors share senior authorship