 Jacqueline R. Anderson
Jacqueline R. Anderson Michael Killian
Michael Killian Jennifer L. Hughes
Jennifer L. Hughes A. John Rush
A. John Rush Madhukar H. Trivedi
Madhukar H. Trivedi- 1Department of Psychiatry, University of Texas Southwestern Medical Center, Dallas, TX, United States
- 2College of Social Work, Florida State University, Tallahassee, FL, United States
- 3Duke National University of Singapore, Singapore, Singapore
- 4Department of Psychiatry, Duke Medical School, Durham, NC, United States
- 5Department of Psychiatry, Texas Tech Health Science Center, Midland, TX, United States
Introduction: Resilience is a factor in how youth respond to adversity. The 88-item Adolescent Resilience Questionnaire is a comprehensive, multi-dimensional self-report measure of resilience developed with Australian youth.
Methods: Using a cross-sectional adolescent population (n = 3,222), confirmatory factor analysis was conducted to replicate the original factor structure. Over half of the adolescents were non-white and 9th graders with a mean age of 15.5.
Results: Our exploratory factor analysis shortened the measure for which we conducted the psychometric analyses. The original factor structure was not replicated. The exploratory factor analysis provided a 49-item measure. Internal consistency reliability for all 12 factors ranged from acceptable (α> 0.70–0.80). The revised factor total scores were highly and significantly correlated with item–total correlation coefficients (r > 0.63, p < 0.001).
Conclusion: This revised shorter 49-item version of the Adolescent Resilience Questionnaire could be deployed and has acceptable psychometric properties.
Introduction
Resilience, the ability to adapt to high levels of risk or adversity and achieve positive outcomes (Gartland et al., 2011), is associated with numerous positive psychological, functional, and behavioral outcomes, particularly in youth (Haskett et al., 2006; Farrell et al., 2011). Resilience is a protective factor, reducing the risk of developing mental health disorders such as depression or anxiety (Davydov et al., 2010; Collin-Vézina et al., 2011). Specifically, Sanders et al. (2015) found that greater resilience was associated with better well-being outcomes (e.g., pro-social behaviors, social participation, positive peer group, and educational involvement) in an at-risk youth sample. Further, youth resiliency is associated with fewer internalizing and externalizing symptoms (Hjemdal et al., 2011; Skrove et al., 2013).
Despite the strong relationship between resilience and positive psychological outcomes in adolescents, there is no consensus on how to best assess an adolescent’s resilience (Ahern et al., 2006; Windle et al., 2011; Smith-Osborne and Bolton, 2013). A recent review of self-report resilience measures identified just six out of 68 resilience measures that were appropriate for English-speaking, school-aged youth, with normative data from a United States sample (Vannest et al., 2019). Overall, it was determined there is no consensus as to a “gold standard” measure of resilience (Vannest et al., 2019), several authors have urged for further research into resilience in youth (Ahern et al., 2006; Windle et al., 2011; Smith-Osborne and Bolton, 2013; Vannest et al., 2019).
This report is based on data gathered in a large mental health promotion evaluation study conducted in the United States in which youth resilience was evaluated with the Adolescent Resilience Questionnaire (ARQ). The ARQ was selected for this study because it assesses resilience in multiple domains: individual, family, peers, school, and community.
The ARQ was originally developed as a comprehensive measure of resilience and validated on a sample of Australian adolescents, with the goal of ecological-translation to integrate individual and environment factors that contribute to overall resilience (Gartland et al., 2011). The ARQ was developed through literature reviews, focus groups, and multiple iterations of psychometric testing. The ARQ is comprised of 88 self-report items on a 5-point Likert scale, designed for adolescents between the ages of 11 and 19. The scale has since been translated into multiple languages (e.g., Romanian, Spanish, Persian, and Nepali). Across several studies investigating the psychometrics properties of the ARQ, researchers found mixed results in replicating the origin factor structure. However, when factor structure was replicated or modified (removing subscales), results indicated adequate internal consistency (range from 0.60 to 0.89) (Guilera et al., 2015; Marici, 2015; Cheraghi et al., 2017; Singh et al., 2019).
Based on these mixed results and the dearth of data on US youth, this report aimed to evaluate the psychometric properties of the 88-item ARQ using data obtained from a sample of opportunity. This evaluation suggested that a reduced number of items might form a more stable factor structure. The resulting 49-item ARQ was examined psychometrically through an exploratory factor analysis. This ARQ was also assessed for convergent and discriminant validity, as evidenced by correlations with quality of life and symptoms of psychopathology. Gender differences were explored.
Materials and Methods
Study Design and Participants
In the 2017–2018 and 2018–2019 academic years, a mental health promotion program was delivered to 1,000 of high school students in North Texas. This program was an expansion of a two-state study examining the feasibility and acceptability of the mental health promotion program (Lindow et al., 2020). As part of the mental health promotion program, a subset of students (n = 3,222) assented to participate in a research study to evaluate the program. A cross-sectional adolescent population completed the research questionnaires during a class period approximately 1 week before beginning the program. The study was approved by the UT Southwestern Institutional Review Board, and parents and students provided written informed consent/assent. From the mental health promotion program study data, the current study examined the students’ ratings of the Adolescent Resilience Questionnaire (ARQ).
Measures
Adolescent Resilience Questionnaire
The ARQ is an 88-item self-report measure for adolescents (11–19 years old) to assess both individual and environmental factors that contribute to resilience (Gartland et al., 2011). The measure assesses resilience from the individual domain and from several environmental domains (family, peers, school, and community). The individual domain measures resilience captured by 5 individual traits: Confidence (8 items), Emotional Insight (8 items), Negative Cognition (8 items), Social Skills (8 items), and Empathy and Tolerance (8 items). The environmental domains of family (11 items), peers (15 items), and school (16 items), are assessed based on the respondent’s engagement in each domain as reflected in the parameters of Connectedness and Availability. The final environmental domain (Community) is assessed by Connectedness (6 items). Each item is responded to on a five-point Likert scale, anchored by Almost never (1) and Almost always (5). The measure has good internal consistency (range between 0.70 and 0.90) (Gartland et al., 2011). By examining each domain, the ARQ assesses individual traits that contribute to resilience and the level of engagement in different environmental resources that may contribute to resilience in times of adversity. Higher scores indicate greater resilience whereas lower scores would indicate vulnerability to adverse events. Gender differences are similar to other literature, such that boys reported more self-confidence and were less likely to experience negative cognitions (Guilera et al., 2015).
Pediatric Quality of Life Enjoyment and Satisfaction (PQ-LES-Q) is a 15-item measure to assess quality of life and life satisfaction in children and adolescents (Endicott et al., 2006). Each item can be rated from 1 (very poor) to 5 (very good). The measure has been found to have good internal consistency of 0.87 (Endicott et al., 2006). Higher scores (scores range 1–65) show greater quality of life and life satisfaction. This measure was used to examine concurrent validity to show those with higher levels of resilience would have greater quality of life.
Quick Inventory of Depressive Symptomatology–Adolescents (QIDS-A) is comprised of 17 items, assessing symptoms associated with depression (Bernstein et al., 2010). Internal consistency is high for the self-report version (Cronbach’s alpha = 0.86) (Bernstein et al., 2010). Ranges for interpreting the QIDS-A are as follows: 6–10 for mild depression, 11–15 for moderate, 16–20 for severe, and greater than 21 for very severe depression. This measure was used to demonstrate discriminant validity, to demonstrate that higher resilience scores would correspond to lower levels of depression.
Generalized Anxiety Disorder 7-item (GAD-7) is a self-report measure to assess anxiety symptoms (Spitzer et al., 2006). Items responses are rated on a 4-point Likert scale from not at all (0) to nearly every day (3). Internal consistency is high (Cronbach’s alpha = 0.92). Scores of 5–9 indicate mild anxiety, 10–14 indicate moderate anxiety, and 15 or greater indicate severe anxiety. This measure was used to establish discriminant validity by evaluating whether persons with lower resilience scores would have higher levels of anxiety.
Statistical Analysis
Confirmatory factor analysis were conducted to examine the fit of the ARQ measurement model to the data and adolescents’ responses to items. Using Mplus 8.3 (Muthén and Muthén, 1998–2018), the factor model was tested using a number of indices of model fit. The model chi-square (χ2) tests the model variance-covariance matrix against that obtained from the data (the common fit function in SEM, Σ = ΣΘ) with smaller and non-significant χ2-values indicating better model fit (Kline, 2016). The Root Mean Square Error of Approximation (RMSEA; Kline, 2016), Comparative Fit Index (CFI; Hu and Bentler, 1999), and Tucker-Lewis Index (TLI; Tucker and Lewis, 1973) were used. CFI and TLI values each greater than 0.95, and RMSEA values lower than 0.08 indicate good model fit (Brown, 2014). The standardized root mean residual (SRMR; Brown, 2014) measures the standardized differences between the model and data variance-covariance matrices, values greater than 0.10 generally indicate poor model fit (Kline, 2016). Cronbach alpha coefficients were obtained to assess the internal consistency reliability of each factor. With model fit being poor with nearly all the original ARQ factors, exploratory factor analyses were undertaken to examine items for lack of fit to each factor. Items were examined and selected for possible removal from each model using theoretical and statistical methods. Authors reviewed each subscale and examined items for face validity with the overarching constructs. Items that did not seem to align with the face validity were flagged to examine statistically. Statistically if item significantly loaded onto multiple factors (i.e., substantially cross-loaded across extracted factors, loading > 0.40), if the item had comparatively high residual variance (i.e., residual variance = 1−r2, or variance in the item unexplained in the model), and if the removal of the item generated improved model fit based on numerous fit indices.
Various other statistical tests were used to assess the measurement validity of the ARQ including multivariate analysis of variance (MANOVA) to assess differences in ARQ factor scores across genders. Additionally, Pearson correlation coefficients were calculated to examine the association between ARQ factor scores and other self-report measure scores (e.g., symptoms of psychopathology and quality of life) reported by the adolescents.
Hypotheses
We hypothesized that the 88-item ARQ factor structure would be replicated and have adequate psychometric properties. We hypothesized we could reduce the 88-item ARQ to a shortened version with adequate psychometric properties.
Results
Demographic Characteristics
Table 1 summarizes the socio-demographic characteristics of the sample. Over half were non-white and 9th graders. Over two-thirds were in a two parent home. The average age of the sample was 15.5 years.
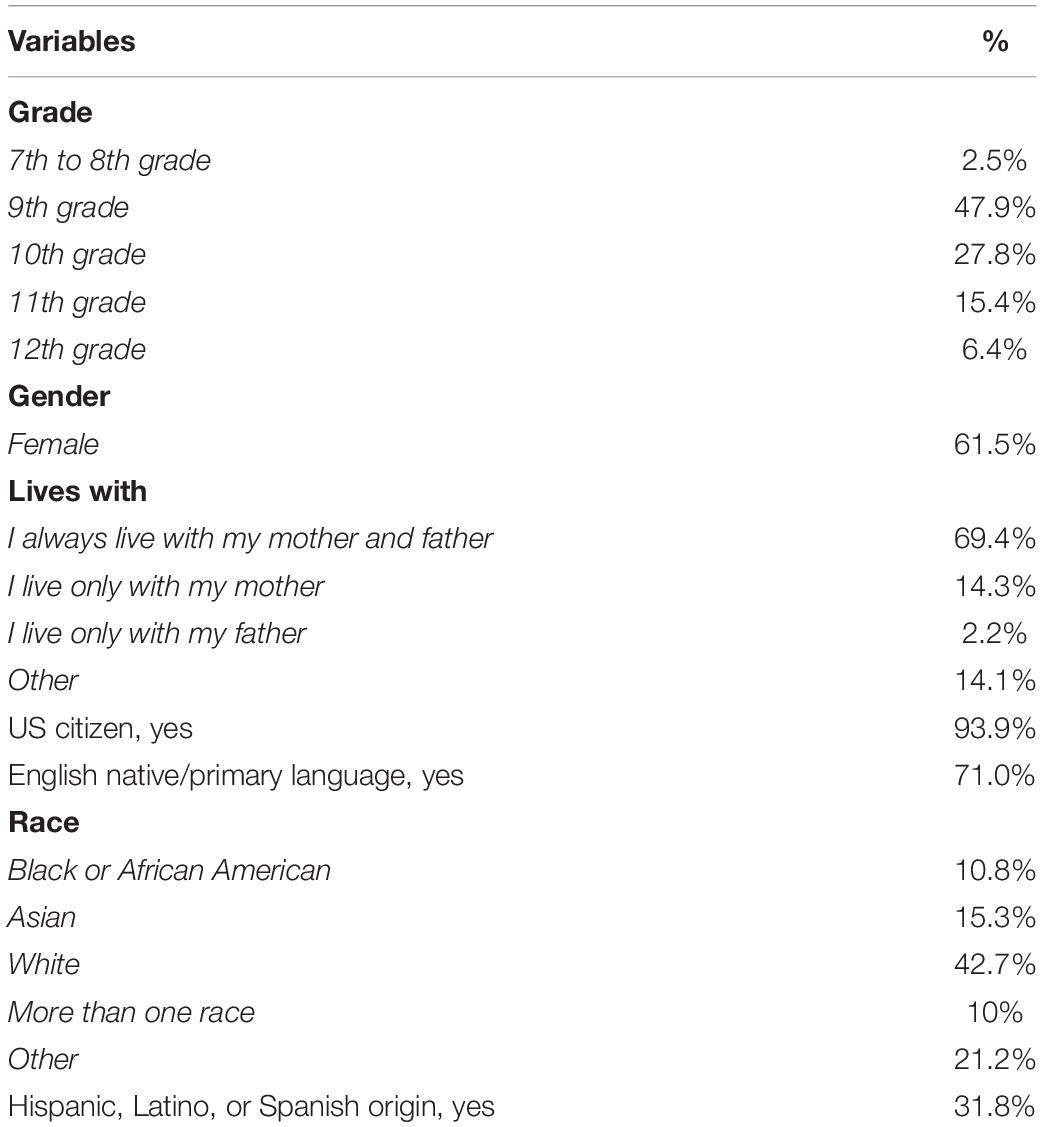
Table 1. Demographics.
ARQ Validity and Reliability
Confirmatory Factor Analysis (CFA)
Responses from 3,222 adolescents on the ARQ were used in CFA modeling examining the factor validity of each factor from the Individual, Family, Peer, School, and Community domains (see Table 2). Overall, the ARQ measurement model poorly fitted the data, except for the Negative Cognition factor within the Individual domain (χ2 = 289.66, df = 20, p < 0.001; RMSEA = 0.065, 95%; CI = 0.058, 0.071; CFI = 0.990, TLI = 0.986; SRMR = 0.018; standardized loadings range 0.582–0.824, α = 0.874). Alternative models were examined including all factors from each domain in correlated factor models (e.g., including all five factors from the Individual domain as correlated latent variables). Results again indicated poor fit of the correlated factor models for the factors within each the Individual, Family, Peer, and School domains (Table 2).
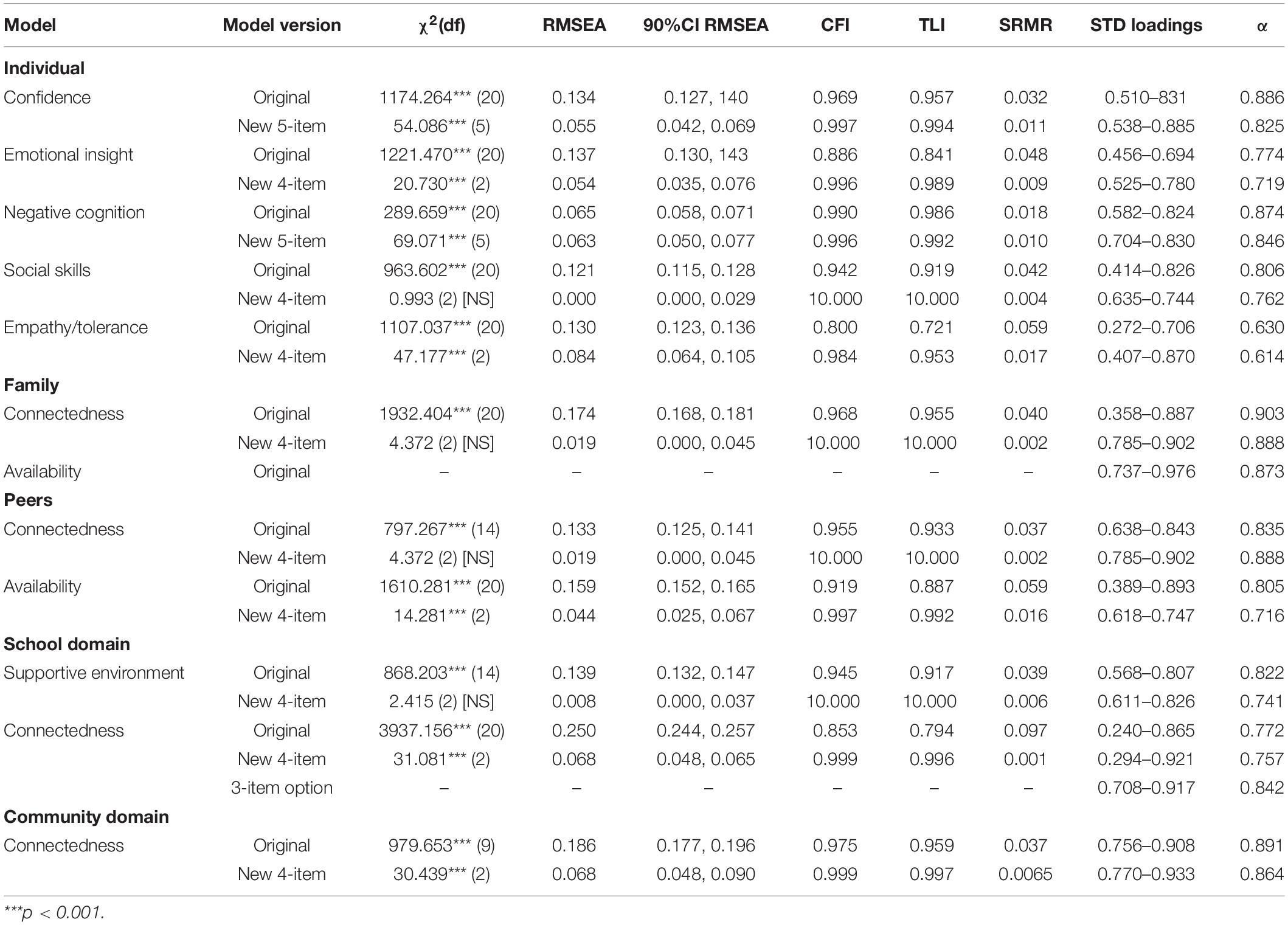
Table 2. Original and revised ARQ factor and measurement models through exploratory factor analysis (n = 3,222).
Exploratory Factor Analysis (EFA)
Given the poor fit of the data to the originally validated model containing 88 items, exploratory analyses were conducted to examine the measurement model of the ARQ. In order to improve model fit to the data, decrease respondent burden, and increase clinical utility, EFA was conducted on each factor to create a shortened version comprised of 49 items of the ARQ (ARQ49). Items were selected for removal from the model if they substantially cross-loaded across extracted factors (loading > 0.40), if the item had comparatively high residual variance (i.e., residual variance = 1−r2), and if the removal of the item generated improved model fit based on numerous fit indices.
Table 2 shows the EFA results and the revised factor models. In each case, dropping several items created a more concise measure of each factor within each domain. Through the removal of three or four items, model fit substantially improved and demonstrated excellent fit of the data to the revised measurement models within the ARQ. Internal consistency reliability for all factors ranged from acceptable (α > 0.70) to excellent (α > 0.80) except for Individual Empathy/Tolerance (α = 0.614). Compared to the original scores for each factor, the revised factor total scores were significantly and very highly correlated with item-total correlation coefficients ranging from r = 0.836 to 0.970 (each p < 0.001). Overall, the original ARQ total score from the 88-item version remained very highly correlated with the revised, shortened version (r = 0.977, p < 0.001), demonstrating comparability of scores from the two versions. The ARQ49 items are listed in Tables 3, 4.
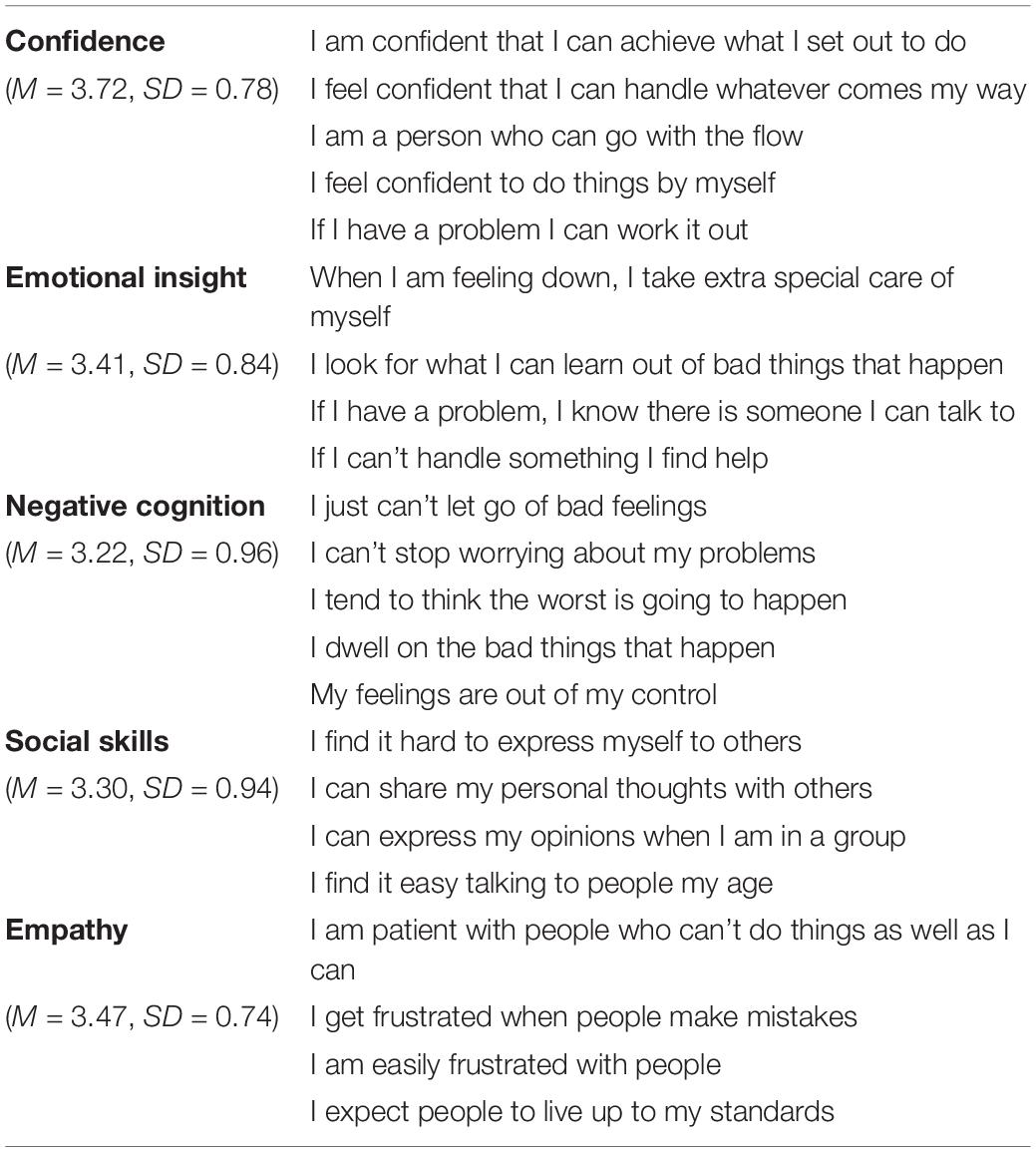
Table 3. Adolescent resilience questionnaire short form individual factor items.
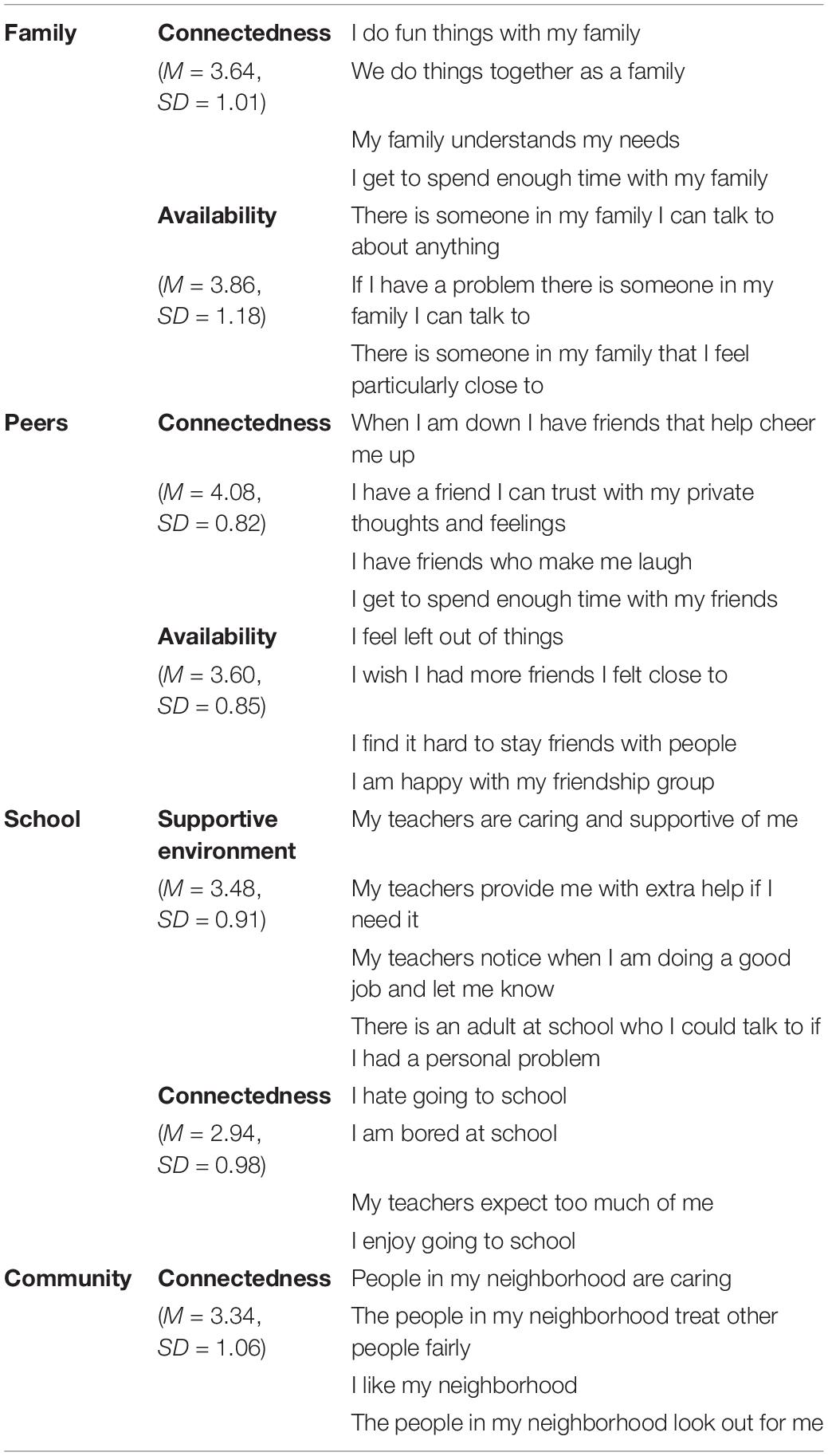
Table 4. Adolescent resilience questionnaire short form family, peer, school, and community factor items.
ARQ49 Scores and Correlates
Individual subscale correlations were conducted (Table 5). Individual subscales were correlated to quality of life and symptoms of psychopathology. Peer, Family, School, and Community subscales were investigated. These subscales were also correlated to quality of life and symptoms of psychopathology.
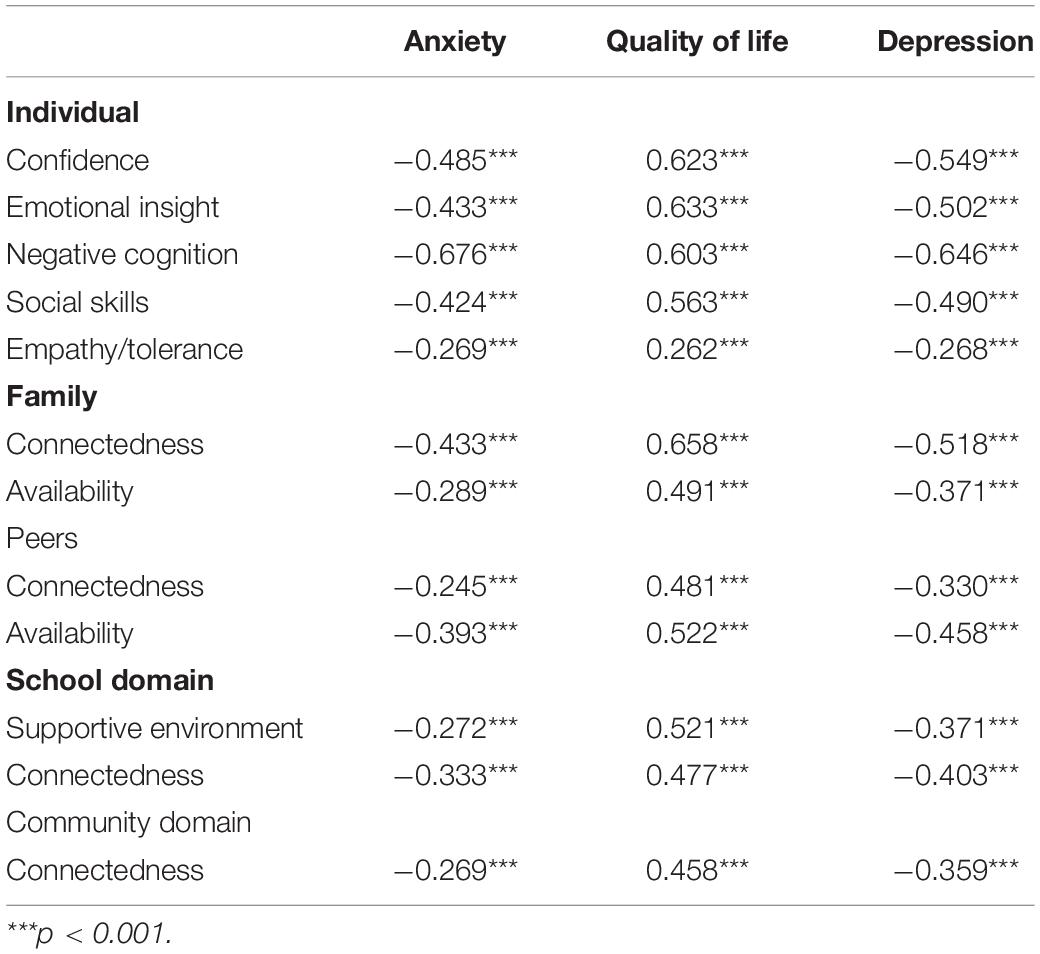
Table 5. Adolescent resilience questionnaire factor scores and correlates.
Gender
Minimal gender differences were found. ARQ49 scores were used in a MANOVA model with gender as a predictor. ARQ49 scores significantly differed among female and male adolescents [Wilk’s Lambda = 0.905, F(12, 3,012) = 26.34, p < 0.001, partial η2 = 0.095], though the effect size of gender across all ARQ scores was small. Specifically, male adolescents reported greater Individual Confidence [F(1, 3,023) = 91.242, p < 0.001, η2 = 0.029], Emotional Insight [F(1, 3,023) = 13.672, p < 0.001, η2 = 0.005], Negative Cognition [F(1, 3,023) = 138.039, p < 0.001, η2 = 0.044], Social Skills [F(1, 3,023) = 43.118, p < 0.001, η2 = 0.014], Peer Availability [F(1, 3,023) = 29.252, p <0.001, η2 = 0.01], and School Connectedness [F(1, 3,023) = 5.159, p = 0.023, η2 = 0.002]. Female adolescents reported greater Peer Connectedness [F(1, 3,023) = 16.9, p < 0.001, η2 = 0.006] and Family Connectedness [F(1, 3,023) = 11.758, p = 0.001, η2 = 0.004]. No significant differences were reported on Community Connectedness [F(1, 3,023) = 2.014, p = 0.156, η2 = 0.001], School Support Environment [F(1, 3,023) = 1.044, p = 0.307, η2 = 0], and Family Availability [F(1, 3,023) = 0.085, p = 0.771, η2 = 0], and Individual Empathy/Tolerance [F(1, 3,023) = 0.001, p < 0.975, η2 = 0]. All effect sizes were small (η2 = 0.001–0.044) for gender differences.
Pediatric Quality of Life Enjoyment and Satisfaction (PQ-LES-Q)
Quality of life and satisfaction scores from the PQ-LES-Q measure were significantly and strongly correlated with ARQ49 Individual subscale (Confidence, Emotional Insight, Negative Cognition, Social Skills) scores (r = 0.563–0.633, each p < 0.001) except for Individual Empathy/Tolerance which was weakly correlated (r = 0.262, p < 0.001). ARQ49 Family, Peer, School, and Community factor scores were similarly strongly correlated with PQ-LES-Q scores (r = 0.458–0.658, each p < 0.001). Higher ARQ49 scores were associated with adolescent reports of greater quality of life and satisfaction.
Depression and Anxiety
QIDS-A depressive symptom severity scores were significantly and negatively correlated with ARQ49 scores within the Individual subscales (r = −0.268 to −0.646, each p < 0.001), Family (r = −0.371 to −0.518, each p < 0.001), Peer (r = −0.330 to −0.458, each p <0.001), School (r = −0.371 to −0.403, each p <0.001), and Community factor scores (r = −0.359, p < 0.001). Similarly, GAD-7 scores were significantly and negatively correlated Individual (r = −0.269 to −0.676, each p < 0.001), Family (r = −0.289 to −0.433, each p < 0.001), Peer (r = −0.245 to −0.393, each p < 0.001), School (r = −0.272 to −0.333, each p < 0.001), and Community factor scores (r = −0.269, p < 0.001). Lower ARQ49 scores were associated with greater reports of depression and anxiety.
Discussion
This study evaluated the ARQ on a novel United States youth population (Gartland et al., 2011). Our initial confirmatory factor analysis did not support the factorial structure implied by the 12 scales structure provided by the developers (Gartland et al., 2011). Other studies have also had difficulty replicating the exact factor structure from the original study (Guilera et al., 2015; Marici, 2015; Cheraghi et al., 2017; Singh et al., 2019). Due to the difficulties of replicating the factor structure, we conducted exploratory analyses, which resulted in the ARQ49 with good fit and adequate internal consistency.
The ARQ49 had high correlations with the original 88-item version of the ARQ. After the measure revisions, gender differences were explored and small differences were found similar to the previous studies (Guilera et al., 2015; Marici, 2015; Cheraghi et al., 2017; Singh et al., 2019). For each subscale, internal consistencies were adequate to good. Subscales were examined for convergent (quality of life) and discriminant validity (symptoms of psychopathology), and they were determined to be adequate.
This is the first study to our knowledge to explore the psychometric properties of the ARQ in a United States population, and to develop and validate a briefer version of the measure, the ARQ49. The ARQ49 also reduces respondent burden. The ARQ49 psychometrics meet the strong standards recommended by several meta-analyses (Ahern et al., 2006; Windle et al., 2011; Smith-Osborne and Bolton, 2013; Vannest et al., 2019). Therefore, ARQ49 is a seventh measure of resilience validated on the United States youth population with adequate psychometric properties. One of the strengths of the scale is that it is a very comprehensive measure that examines not only individual traits, but also environmental factors that are likely to affect resilience. In addition to developing a shortened version of this measure, another strength of this study is the large sample size of diverse students from different types of schools across North Texas. Further, the current findings are similar not only to other ARQ studies, but similar to other resilience study’s to indicate resilience as a protective factor.
Clinicians should use this measure when wanting to measure resilience in youth across multiple domains (Family, Peers, School, and Community) to obtain a comprehensive understanding of the youth’s overall resilience. Further, clinicians could examine the different domains of resilience within the external or internal factors as targets of intervention or resilience development. For example, if a clinician noticed a student’s scores are normal in all areas except school connectedness, then the clinician could look for interventions to promote school connectedness with that student. Alternatively, a clinician could use a strength-based approach to highlight the higher scored domains with a student to create a change plan by using the student’s strengths. Beyond clinician usage, a school system could use this measure to assess their student body’s overall and domain specific resilience alongside a universal prevention or social emotional curriculum to understand how the curriculum promotes mental health. Additionally, resilience is important to understand short and long-term outcomes, the shortening of this measure may promote the use of this measure by decreasing the amount of time to complete it (Davydov et al., 2010; Collin-Vézina et al., 2011; Turner et al., 2017). Thus, ARQ49 could also be incorporated into assessments to understand mediators of trauma and development of psychopathology.
A limitation of this study is there was not another resilience measure in this assessment to use as a comparison with the ARQ49. Thus, it is unclear whether the ARQ49 is directly related to an established resilience measure validated in the United States. Due to the broad definition of resilience in the ARQ with external and internal factors, future studies should examine the relationship of the ARQ49 with another well-established measures of resilience in the United States such as six identified in the recent review (Vannest et al., 2019). The study included a cross-sectional population of adolescents in North Texas, so it may not be generalizable to the entire North American population. Replication of these findings with other youth residing in the United States is needed to further understand how the resilience measure is relevant in different regions. Finally, resilience is defined as the ability to overcome adversity (Gartland et al., 2011). However, the current study sample was from a general population, so it unclear whether the students sampled have had adverse experiences that would lead to the development of resilience. In future studies, researchers could use the ARQ49 to examine how adverse experiences lead to the development of higher or lower resilience scores.
Overall, the ARQ49 provides a comprehensive tool that assesses individual traits and environmental aspects of adolescent resilience with strong psychometric properties appropriate for adolescents in the United States.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by the University of Texas Southwestern Medical Center Institutional Review Board. Written informed consent to participate in this study was provided by the participants’ legal guardian, and written informed assent was provided by the participant.
Author Contributions
JA, JH, and MT conceived and designed the analyses. MK conducted the analyses. JH and MT oversaw the data collection and the related project. JA, AR, and MK wrote the manuscript with contribution from the other authors. All authors contributed to the article and approved the submitted version.
Funding
The Youth Aware of Mental Health program was funded in part by the Rees-Jones Foundation, REDCap (UL1 TR001105), the W.W. Caruth, Jr. Foundation, and the Hersh Foundation. The content is solely the responsibility of the authors and does not necessarily represent the official views of the various funding organizations.
Conflict of Interest
JH has served as Youth Aware of Mental Health (YAM) trainer, consulting for Mental Health in Mind International. JH also receives royalties from Guilford Press. AR has received consulting fees from Compass Inc., Curbstone Consultant LLC, Emmes Corp., Evecxia Therapeutics, Inc., Holmusk, Johnson and Johnson (Janssen), Liva-Nova, Neurocrine Biosciences Inc., Otsuka-US, Sunovion; speaking fees from Liva-Nova, Johnson and Johnson (Janssen); and royalties from Guilford Press and the University of Texas Southwestern Medical Center, Dallas, TX (for the Inventory of Depressive Symptoms and its derivatives). He is also named co-inventor on two patents: U.S. Patent No. 7,795,033: Methods to Predict the Outcome of Treatment with Antidepressant Medication, Inventors: McMahon FJ, Laje G, Manji H, Rush AJ, Paddock S, Wilson AS; and U.S. Patent No. 7,906,283: Methods to Identify Patients at Risk of Developing Adverse Events During Treatment with Antidepressant Medication, Inventors: McMahon FJ, Laje G, Manji H, Rush AJ, Paddock S. MT has served as an adviser or consultant for ACADIA Pharmaceuticals, Alkermes Inc, Allergan, Alto Neuroscience Inc., Applied Clinical Intelligence, LLC, Axsome Therapeutics, Boegringer Ingelheim, GreenLight VitalSign6 Inc., Janssen Pharmaceutical, Jazz Pharmaceutical, Lundbeck Research USA, Medscape, Merck Sharp & Dohme Corp., Myriad Neuroscience, Navitor, Otsuka America Pharmaceutical Inc., Perception Neuroscience Holdings, Pharmerit International, SAGE Therapeutics, Signant Health, Takeda Pharmaceuticals Inc.; he has received grants or research support from the NIMH, NIDA, the Cancer Prevention and Research Institute of Texas, Patient-Centered Outcomes Research Institute, and Janssen; and has received editorial compensation from Healthcare Global Village and Engage Health Media.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We wish to thank the participants, families, staff, and colleagues who made this project possible. We also thank Luis Gutierrez, MS, for his role in this project and the CDRC Risk and Resilience Network team. Finally, we thank Happy Carlock, B.A., for administrative support.
References
Ahern, N. R., Kiehl, E. M., Lou Sole, M., and Byers, J. (2006). A review of instruments measuring resilience. Issu. Comprehens. Pediatr. Nurs. 29, 103–125. doi: 10.1080/01460860600677643
Bernstein, I. H., Rush, A. J., Trivedi, M. H., Hughes, C. W., Macleod, L., Witte, B. P., et al. (2010). Psychometric properties of the Quick Inventory of Depressive Symptomatology in adolescents. Int. J. Methods. Psychiatr. Res. 19, 185–194. doi: 10.1002/mpr.321
Brown, T. A. (2014). Confirmatory factor analysis for applied research. New York: Guilford Publications.
Cheraghi, M. A., Ebadi, A., Gartland, D., Ghaedi, Y., and Fomani, F. K. (2017). Translation and validation of “Adolescent Resilience Questionnaire” for Iranian adolescents. Asian J. Psychiatr. 25, 240–245. doi: 10.1016/j.ajp.2016.12.001
Collin-Vézina, D., Coleman, K., Milne, L., Sell, J., and Daigneault, I. (2011). Trauma experiences, maltreatment-related impairments, and resilience among child welfare youth in residential care. Int. J. Ment. Health Addict. 9, 577–589. doi: 10.1007/s11469-011-9323-8
Davydov, D. M., Stewart, R., Ritchie, K., and Chaudieu, I. (2010). Resilience and mental health. Clin. Psychol. Rev. 30, 479–495.
Endicott, J., Nee, J., Yang, R., and Wohlberg, C. (2006). Pediatric quality of life enjoyment and satisfaction questionnaire (PQ-LES-Q): Reliability and validity. J. Am. Acad. Child Adolesc. Psychiatr. 45, 401–407. doi: 10.1097/01.chi.0000198590.38325.81
Farrell, A. D., Henry, D. B., Mays, S. A., and Schoeny, M. E. (2011). Parents as moderators of the impact of school norms and peer influences on aggression in middle school students. Child Devel. 82, 146–161. doi: 10.1111/j.1467-8624.2010.01546.x
Gartland, D., Bond, L., Olsson, C. A., Buzwell, S., and Sawyer, S. M. (2011). Development of a multi-dimensional measure of resilience in adolescents: the Adolescent Resilience Questionnaire. BMC Med. Res. Methodol. 11:134. doi: 10.1186/1471-2288-11-134
Guilera, G., Pereda, N., Paños, A., and Abad, J. (2015). Assessing resilience in adolescence: The Spanish adaptation of the Adolescent Resilience Questionnaire. Health Qual. Life Outcomes 13:100.
Haskett, M. E., Nears, K., Ward, C. S., and McPherson, A. V. (2006). Diversity in adjustment of maltreated children: Factors associated with resilient functioning. Clin. Psychol. Rev. 26, 796–812. doi: 10.1016/j.cpr.2006.03.005
Hjemdal, O., Vogel, P. A., Solem, S., Hagen, K., and Stiles, T. C. (2011). The relationship between resilience and levels of anxiety, depression, and obsessive–compulsive symptoms in adolescents. Clin. Psychol. Psychother. 18, 314–321. doi: 10.1002/cpp.719
Hu, Lt, and Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equat. Model. 6, 1–55. doi: 10.1080/10705519909540118
Kline, R. B. (2016). Principles and practice of structural equation modeling, 4th Edn. New York: The Guilford Press.
Lindow, J. C., Hughes, J. L., South, C., Gutierrez, L., Bannister, E., Trivedi, M. H., et al. (2020). Feasibility and acceptability of the youth aware of mental health (YAM) intervention in US adolescents. Arch. Suicide Res. 24, 269–284. doi: 10.1080/13811118.2019.1624667
Marici, M. (2015). Some psychometric properties of the family domain in the “Adolescent Resilience Questionnaire”. Proc. Soc. Behav. Sci. 187, 289–294. doi: 10.1016/j.sbspro.2015.03.054
Muthén, L. K., and Muthén, B. O. (1998–2018). Mplus User’s Guide, 8th Edn. Los Angeles, CA: Muthén & Muthén.
Sanders, J., Munford, R., Thimasarn-Anwar, T., Liebenberg, L., and Ungar, M. (2015). The role of positive youth development practices in building resilience and enhancing wellbeing for at-risk youth. Child Abuse Neglect 42, 40–53. doi: 10.1016/j.chiabu.2015.02.006
Singh, R., Mahato, S., Singh, B., Bhushal, S., and Fomani, F. K. (2019). Psychometric properties of adolescent resilience questionnaire among Nepalese adolescents in Lalitpur. Asian J. Psych. 45, 13–17. doi: 10.1016/j.ajp.2019.08.002
Skrove, M., Romundstad, P., and Indredavik, M. S. (2013). Resilience, lifestyle and symptoms of anxiety and depression in adolescence: the Young-HUNT study. Soc. Psych. Psychiatr. Epidemiol. 48, 407–416. doi: 10.1007/s00127-012-0561-2
Smith-Osborne, A., and Bolton, W. K. (2013). Assessing resilience: A review of measures across the life course. J. Evid. Based Soc. Work 10, 111–126. doi: 10.1080/15433714.2011.597305
Spitzer, R. L., Kroenke, K., Williams, J. B., and Löwe, B. (2006). A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch. Internal Med. 166, 1092–1097. doi: 10.1001/archinte.166.10.1092
Tucker, L. R., and Lewis, C. (1973). A reliability coefficient for maximum likelihood factor analysis. Psychometrika 38, 1–10. doi: 10.1007/bf02291170
Turner, H. A., Shattuck, A., Finkelhor, D., and Hamby, S. (2017). Effects of poly-victimization on adolescent social support, self-concept, and psychological distress. J. Interpers. Violence 32, 755–780. doi: 10.1177/0886260515586376
Vannest, K. J., Ura, S. K., Lavadia, C., and Zolkoski, S. (2019). Self-report Measures of Resilience in Children and Youth. Contempor. Sch. Psychol. 2019:475.
Keywords: adolescence, resilience (psychological), psychometrics, assessment, youth
Citation: Anderson JR, Killian M, Hughes JL, Rush AJ and Trivedi MH (2020) The Adolescent Resilience Questionnaire: Validation of a Shortened Version in U.S. Youths. Front. Psychol. 11:606373. doi: 10.3389/fpsyg.2020.606373
Received: 14 September 2020; Accepted: 03 November 2020;
Published: 27 November 2020.
Edited by:
Darko Roviš, University of Rijeka, CroatiaReviewed by:
Barbara Benoliel, Walden University, United StatesTina Jaeckle, Walden University, United States
Copyright © 2020 Anderson, Killian, Hughes, Rush and Trivedi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Madhukar H. Trivedi, bWFkaHVrYXIudHJpdmVkaUB1dHNvdXRod2VzdGVybi5lZHU=