 Adam Klocek
Adam Klocek Tomáš Řiháček
Tomáš Řiháček Hynek Cígler
Hynek Cígler
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol., 03 December 2020
Sec. Quantitative Psychology and Measurement
Volume 11 - 2020 | https://doi.org/10.3389/fpsyg.2020.595651
This article is part of the Research TopicNew Challenges in Globalized Societies: Cross-cultural Studies and Test AdaptationView all 13 articles
The Group Cohesiveness Scale (GCS, 7 items) measures patient-rated group cohesiveness. The English version of the scale has demonstrated good psychometric properties. This study describes the validation of the Czech version of the GCS. A total of 369 patients participated in the study. Unlike the original study, the ordinal confirmatory factor analysis (CFA) supported a two-dimensional solution (RMSEA = 0.075; TLI = 0.986). The analysis demonstrated the existence of two moderately to highly associated (r = 0.79) domains of group cohesiveness—affective and behavioral. The two-dimensional model was invariant across genders, age, education, and time (retest after 6 weeks) up to factor means level. Internal consistency reached satisfactory values for both domains (affective, ω = 0.86; behavioral, ω = 0.81). In terms of convergent validity, only weak association was found between the GCS domains and the group working alliance measured by the Group Outcome Rating Scale (GSRS). This is the first revision of the factor structure of the GCS in the European context. The scale showed that the Czech version of the GCS is a valid and reliable brief tool for measuring both aspects of group cohesiveness.
Group cohesion is one of the elemental group phenomena that allows other therapeutic processes to occur within the group therapy framework. It is defined as the ability of the members of a group to tolerate negative emotions and self-disclosure (Wongpakaran et al., 2013). Group cohesion partially overlaps with other group phenomena, such as the working alliance and empathy (Johnson et al., 2005). Group cohesion is conceptually akin to the working alliance in individual therapy. Although it is primarily based on the relationships among the group members, it can also be extended to the relationship with the therapists (Budman et al., 1989). Group cohesion is also related to empathy because a cohesive group demands that its members have an understanding of others’ feelings and experiences and can effectively express this understanding (Roark and Sharah, 1989).
Until recently, group phenomena and processes were measured by measures such as the Group Climate Questionnaire (MacKenzie, 1983), the Therapeutic Factors Inventory (Lese and MacNair-Semands, 2000), and the Working Alliance Inventory (Horvath and Greenberg, 1989). However, these scales were too lengthy to be used in routine care or rapid hospital environments (compared to research) and were not directly focused on group cohesion. Therefore, the Group Cohesiveness Scale (GCS1) was developed (Wongpakaran et al., 2013).
The GCS (Wongpakaran et al., 2013; see Table 1) was created from an original pool of 40 items and reduced to seven items representing two domains: cohesion and engagement. The former domain was represented by two items from the Therapeutic Factors Inventory, while the latter was represented by five items from the Group Climate Questionnaire. However, since both domains were similar in content, Wongpakaran et al. (2013) considered them to be representations of the unidimensional group cohesiveness construct.
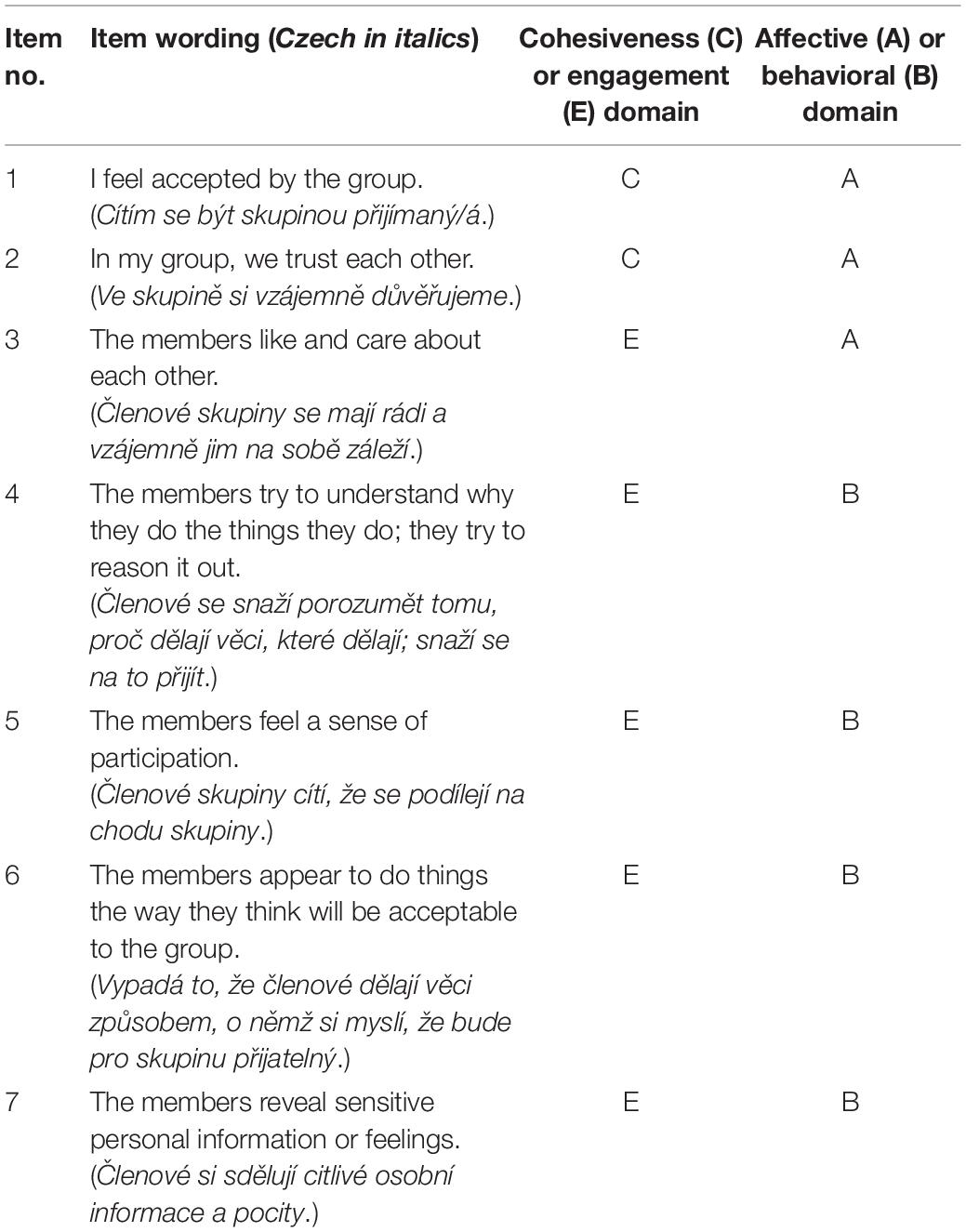
Table 1. Group Cohesiveness Scale (Wongpakaran et al., 2013).
Alternatively, Wongpakaran et al. (2013) suggested that the GCS items can be differentiated into the affective (items 1, 2, and 3) and behavioral (items 4, 5, 6, and 7) components of group cohesiveness. They argued that these components might be related to each other in a fashion similar to the unidimensional construct of depression, in which the feeling of sadness is functionally different from a behavioral lack of interest, yet both components measure the same latent construct of depression (Wongpakaran et al., 2013).
The distinction between the affective and behavioral components is consistent with the theoretical literature. According to Carron (1982), group cohesion is a “dynamic process that is reflected in the tendency for a group to stick together [emphasis added] and remain united in the pursuit of its goals and objectives. [emphasis added]” (p. 124). Similarly, Mudrack (1989) divided group cohesion into attraction-to-group (affective component) and commitment to the group task (behavioral component).
Originally, the GCS was standardized in the Thai language (Wongpakaran et al., 2013) in a clinical sample of 96 patients (56% women) with a mean age of 28.22 (SD = 6.84). Patients were hospitalized for up to 2 weeks. A principal component analysis revealed a unidimensional factor structure (57.2% of explained variance). Based on a confirmatory factor analysis (CFA) conducted on the same dataset, the authors claimed that the unidimensional model had moderately acceptable fit despite unsatisfactory RMSEA values (χ2(14) = 32.29; CFI = 0.94; TLI = 0.90; SRMR = 0.04; RMSEA = 0.12).
Although Wongpakaran et al. (2013) tried to fit a two-dimensional model (i.e., cohesion and engagement), they did not report the results, arguing that the two dimensions were too strongly correlated to be set apart (r = 0.83). Instead, they fine-tuned the unidimensional model based on modification indices by allowing residual correlations between pairs of items (items 1 and 2; items 2 and 3), reaching an excellent fit [χ2(12) = 12.41; CFI = 0.99; TLI = 0.99; SRMR = 0.04; RMSEA = 0.02]. Arguably, by allowing the residual correlations, the authors developed a model that was very similar to (but less parsimonious than) the suggested two-factor model with the affective and behavioral factors. Therefore, we found it desirable to formally test this alternative two-factor model as well. In terms of convergent validity, the GCS was correlated to the Group Benefit Questionnaire (r = 0.71, p < 0.001) and to the Cohesion to Therapist Scale (r = 0.77, p < 0.001) in the original study.
The GCS is a relatively new measure that has been employed in a limited number of studies thus far. Psychometric information about the GCS is rather scarce and often unsatisfactory given small sample sizes. Poyner-Del Vento et al. (2018) used the GCS as a measure of group cohesion in a pilot study in a sample of seven female military veterans. They found that removing item 6 (“The members appear to do things the way they think will be acceptable to the group”) increased the internal consistency of the scale from α = 0.72–0.90. Tulin et al. (2018) used the GCS to measure group cohesion in a sample of 109 students with internal consistency of α = 0.90. In another sample of 22 students, Ashby et al. (2018) found a mean interitem correlation of r = 0.43. This limited evidence does not allow us to thoroughly evaluate the GCS, and the applicability of the measure in Western culture is still missing.
This study aimed to validate the Czech version of the GCS using the ordinal CFA paradigm. Four models were tested, including the unidimensional model (model 1), the unidimensional model with residual covariances between items 1 and 2 and items 2 and 3 allowed (model 2), a two-factor model with the factors of cohesion (items 1 and 2 originally extracted from the Therapeutic Factors Inventory) and engagement (items 3–7 originally extracted from the Group Climate Questionnaire) (model 3), and a two-factor model with affective (items 1–3) and behavioral factors (items 4–7) (model 4). Furthermore, to assess the convergent validity, we used the Group Session Rating Scale (GSRS, Quirk et al., 2013), a measure of the group working alliance, as a comparison. Although group cohesion and group working alliance are distinct constructs, we expected the GCS scores to be related to the GSRS scores because both instruments measure non-specific group-based relational factors of the therapeutic process.
The sample included patients from seven clinical sites in the Czech Republic who provided informed consent to participate in research tracking the mechanisms of change during psychotherapy from January 2018 to December 2019. All patients underwent group therapy lasting from 4 to 12 weeks (depending on the site, median of 6 weeks). Data were collected on a paper-and-pencil form on a weekly basis during the whole treatment. Participants completed a battery of questionnaires regarding demographic variables, several outcome variables and several mechanisms of change, including group cohesion and working alliance. The study was approved by the Research Ethics Committee of Masaryk University (Ref. No. EKV-2017-029-R1).
In this study, the dataset used to validate the GCS included data from the second week of therapy (i.e., the first measurement of the group cohesion). Out of 448 patients who provided their baseline data, 380 patients (85%) participated in the second week of treatment. Out of 380 participants, 11 were characterized by missing data regarding the GCS, resulting in a total sample size of N = 369 patients. Differences between participants with missing data (n = 80) and the final sample (n = 369) in the demographics and clinical diagnosis data were investigated using t-tests and χ2-tests.
The treatment was integrative with major psychodynamic and minor humanistic and experiential aspects, supplemented with art, physical activity, music, ergo-, drama-, physio-, and biblio-therapy, relaxation and cognitive training, and community meetings2. Five sites were characterized by a frequency of five sessions of psychotherapy per week. The remaining two sites had three and four sessions per week, respectively. A session of group therapy lasted 90 min3.
The sample comprised small closed groups of inpatients within four clinical sites and small open groups of outpatients in a program with a daycare basis within three clinical sites. Twenty-five (16 female) therapists participated in this research (Mage = 44.13 years, SDage = 10.29). They were trained in the psychodynamic or psychoanalytic approach (n = 15), gestalt (n = 4), person-centered approach (n = 3), integrative approach (n = 2) or Daseinanalysis (n = 1). Their experience fluctuated between 1 and 25 years (M = 12.21, SD = 7.30).
The seven items of the GCS are scored on a Likert scale from 1 (strongly disagree) to 5 (strongly agree). None of the items is negatively worded. A higher score indicates higher perceived group cohesion. In the original study, the GCS yielded an average score of 4.73 out of 5 (SD = 0.62), the internal consistency of the whole scale was α = 0.87, and the item-total correlations ranged from 0.497 to 0.752.
The scale was translated into Czech from the English version. Five native Czech speakers (a psychology student, two psychologists, and two laypeople) created five independent Czech translations. A group of three people (the two psychologists and the psychology student) then discussed all the translations and consolidated them into a single version. Third, this version was back-translated into English by a bilingual, native English speaker and compared to the original English version. Fourth, the final Czech version was field-tested with five respondents to check the comprehensibility of the items.
The GSRS (Quirk et al., 2013) is a measure of the working alliance in group psychotherapy. It includes four 10-cm-long visual analog scales, each framed by a verbal anchor on both ends. The continuous dimension of each item is framed by bipolar points, and participants rate the group working alliance by making a mark on each scale. The response is measured as the length of the line from the left-hand side to the mark in millimeters. The range of the total score, computed as the sum of all items, can thus reach values between 0 and 400. A higher score indicates a better perceived working alliance. The scale was reported to be unidimensional, and the internal consistency ranged from α = 0.86 to 0.90 in the original study.
The statistical procedures were performed using statistical software R, version 4.0.2 (R Core Team, 2020). The significance level was set at p < 0.05.
The factor structure was estimated through ordinal CFA using the lavaan package (Rosseel, 2012). The ordinal factor analysis is equivalent to the two-parameter logistic graded response model in item response theory. Hence, this approach is not as vulnerable to the violation of assumptions as the standard factor analysis (Raykov and Marcoulides, 2011). Each item has five parameters (one slope and four thresholds between all neighboring response options). All five models were estimated using the stochastic weighted least squares means and variance adjusted estimator method (WLSMV), which seems to perform well with ordered categorical data (Raykov and Marcoulides, 2011). The fit indices employed in this study included χ2, χ2/df, root mean square error of approximation (RMSEA), Tucker-Lewis index (TLI), comparative fit index (CFI), and standardized root mean residual (SRMR). According to Hu and Bentler’s (1999) and Hooper et al. (2008) evaluation criteria, the χ2/df should not exceed 3, the RMSEA should optimally be below 0.05, but values up to 0.10 are still considered to indicate a satisfactory fit. The SRMR should not exceed 0.08. Optimally, the TLI and CFI should be above 0.95; nevertheless, values above 0.90 are still considered to indicate a satisfactory fit.
Within models with more than one dimension (models 3 and 4), factors were allowed to be correlated. Since model 3 contained a factor represented only by two items, these items were constrained to load equally on their factor. Otherwise, models were identified by standardizing the latent variable. The internal consistency was estimated using bootstrapped Cronbach’s alpha and McDonald’s omega coefficients (McDonald, 1999). In terms of convergent validity, the association between the GCS and the GSRS was tested on the level of latent scores.
The invariance was tested with regard to age, gender, education, and time. Measurement invariance was assessed by testing differences between nested models with continually increasing constraints: configural, metric (factor loadings), scalar (intercepts), strict (residuals), and factor means. Age groups were created by dividing the sample according to a median split. Gender invariance was assessed between male and female participants. Education invariance was assessed between higher (university, high technical school) and lower education (primary and secondary school with or without graduation) levels. Time invariance was assessed between the second and sixth weeks of group therapy (the sixth week was chosen pragmatically because in most sites, the therapy lasted only 6 weeks). We used four different fit indices to test the invariance, namely, Δχ2, ΔCFI, ΔSRMR, and ΔRMSEA. We employed “theta” parametrization and invariance guidelines with regard to ordinal data according to Wu and Estabrook (2016). Two groups are considered to be invariant if the item parameters (i.e., factor loadings, thresholds, intercepts, residuals, and factor means) are similar across groups.
Items 3 and 7 demonstrated missing response frequency at response option 1 (i.e., 1 or “strongly disagree”). The remaining items demonstrated near-to-missing response frequency (0.01) at response option 1. Response option 2 (unnamed) was also very seldom selected by the participants in all items. Therefore, all items were recoded into three categories (i.e., responses from 1 to 3 were recoded as a single category, representing a low level of group cohesion) for the purpose of testing the measurement invariance.
No significant differences between the final sample (N = 369) and the respondents with missing responses or respondents not participating in the study at the second week (n = 80, who were the remaining part of the initial sample of 449 participants) were found for the mean age, gender, education, and psychiatric diagnosis. The pattern of missingness could be considered missing at random. Therefore, only complete cases were included in the analyses.
The total sample included 369 patients (73.7% females). Their nationality included Czech (95%), Slovak (2%), and others (3%). The patients’ ages ranged from 18 to 71 years (Mage = 39.6, SD = 11.1). Psychiatric diagnoses were represented as follows: F4x (n = 261), F3x (n = 69), F6x (n = 53), F5x (n = 8), and F1x (n = 7). Several participants possessed multiple diagnoses (n = 33), mainly a combination of F4x and F6x (n = 13), F3x and F4x (n = 9), and F3x and F6x (n = 7). The remaining demographic variables are reported in Table 2.
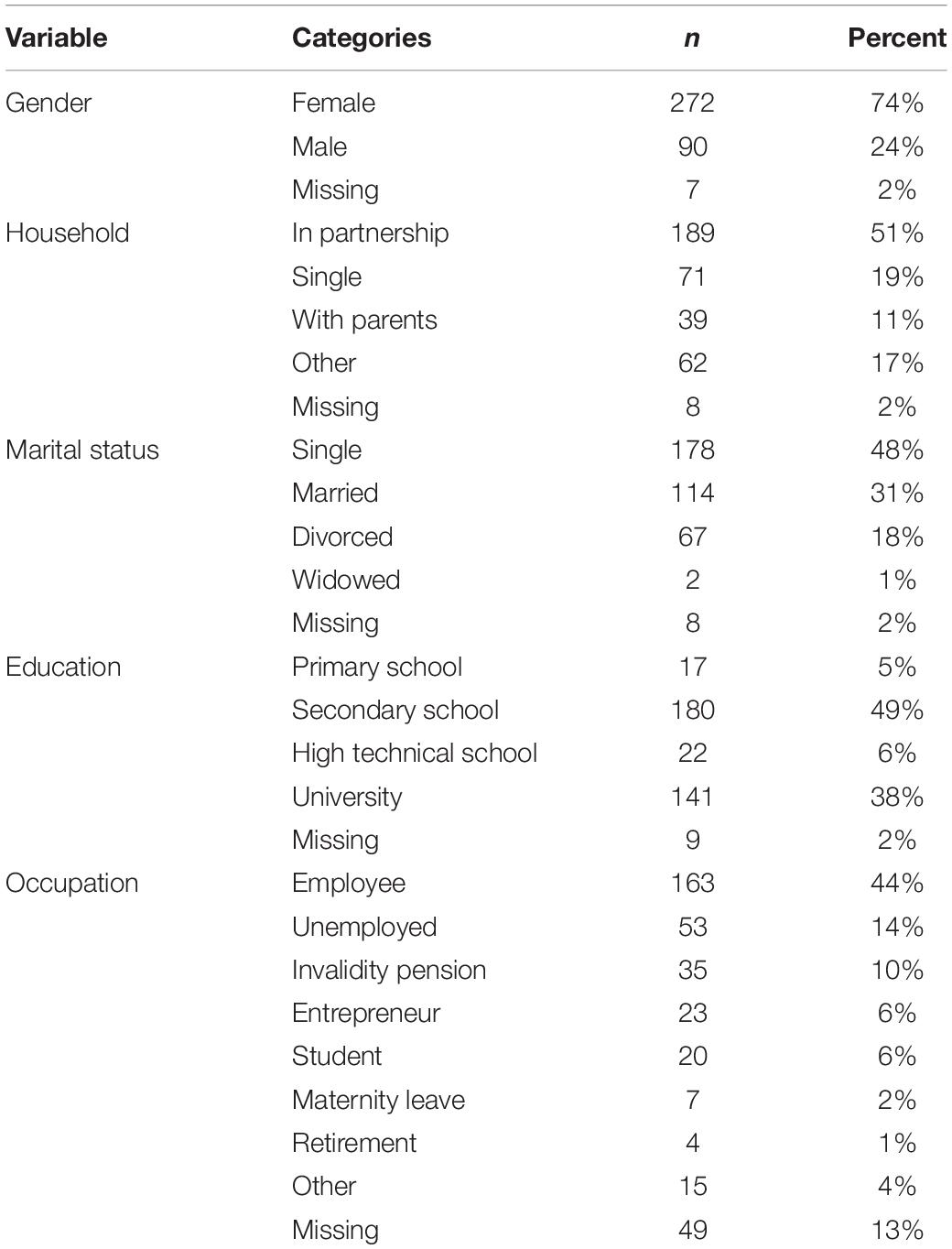
Table 2. Descriptive characteristics of the sample (N = 369).
The mean scores for each GCS item, the GCS total score, and the GSRS total score, as well as the internal consistency of the unidimensional model, are reported in Table 3. The average total score was 3.7 (SD = 0.69). Corrected item-total correlations ranged from 0.49 to 0.75.
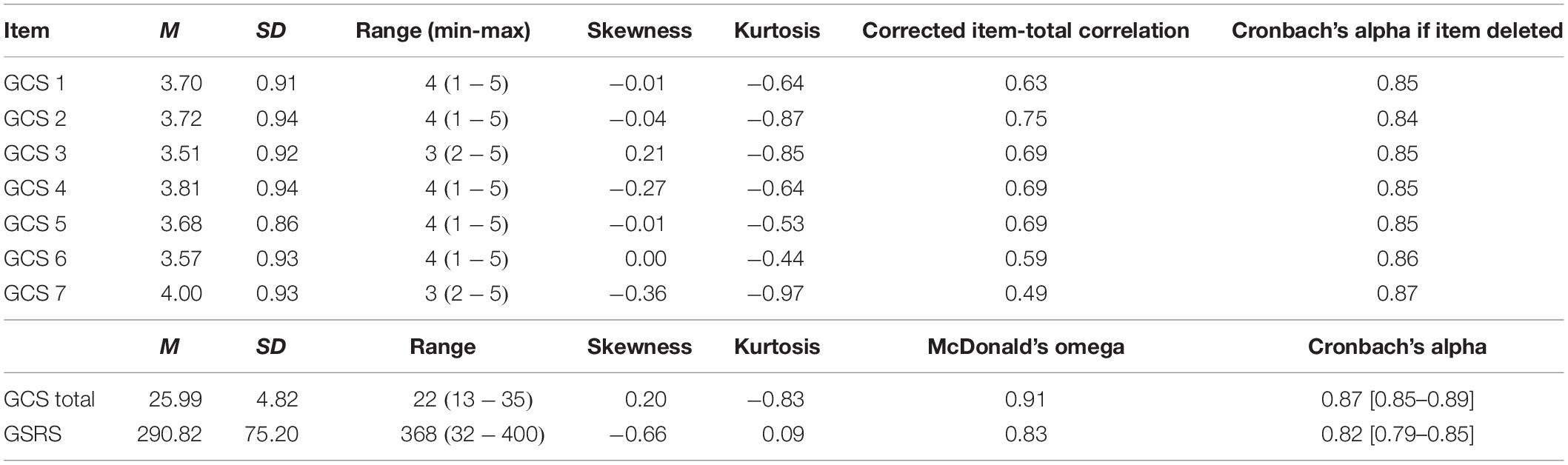
Table 3. Descriptive characteristics of scales (N = 369).
First, the assumptions of factor analysis were tested. The data did not show multivariate normality, and the standardized residuals were positively skewed. Homoscedasticity was not observed. After the preliminary data analyses, an ordinal factor analysis was employed to estimate the fit of the factor models using these skewed non-linear data. The RMSEA of the null model was 0.398. This value is above 0.148; thus, the TLI fit index could be interpreted (Kenny et al., 2015).
Second, four different factor solutions were tested for fit and compared (see Table 4). We concluded that the best fit was obtained by model 4, a two-factor solution with the affective and behavioral factors (see Table 5 and Figure 1). Model 4 fit the data significantly better than did model 1 [unidimensional; Δχ2(1) = 87.66, p < 0.0001] and model 3 [two-factor with the cohesion and engagement factors; Δχ2(2) = 104.31, p < 0.0001]. Furthermore, the fit of model 4 did not significantly differ from that of model 2 [unidimensional with residual correlations; Δχ2(1) = 2.35, p > 0.10]. However, model 4 can be considered superior in terms of parsimony as well as theoretical justification. While the affective factor represents the same underlying structure as the empirically derived residual correlations in model 2, it explains the item interrelationships more efficiently and is consistent with theoretical expectations (Carron, 1982; Mudrack, 1989).
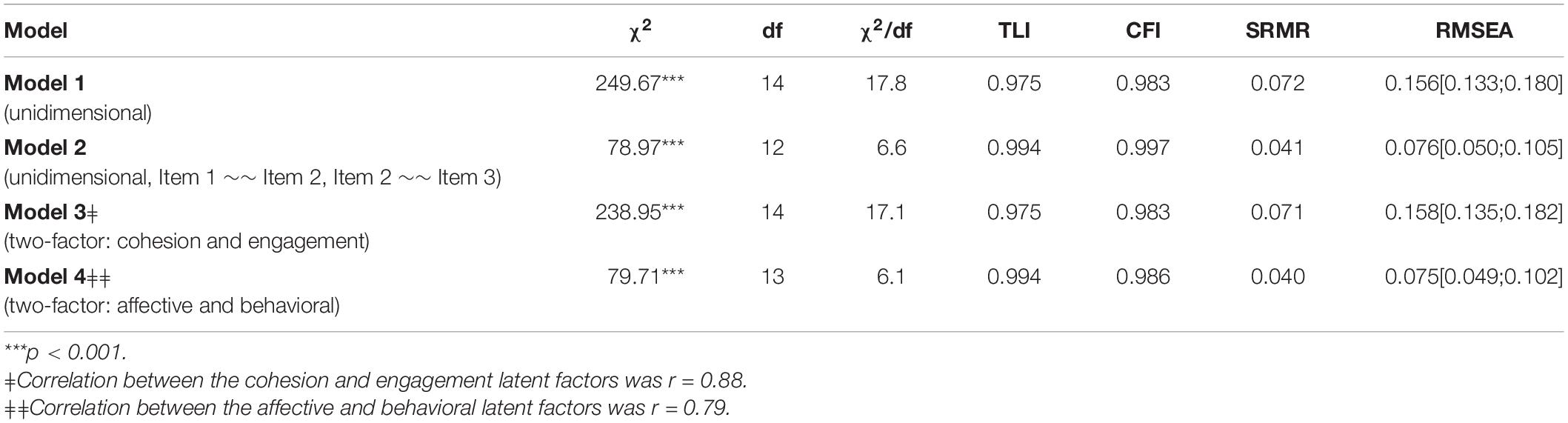
Table 4. Fit indices of the tested models (N = 369).
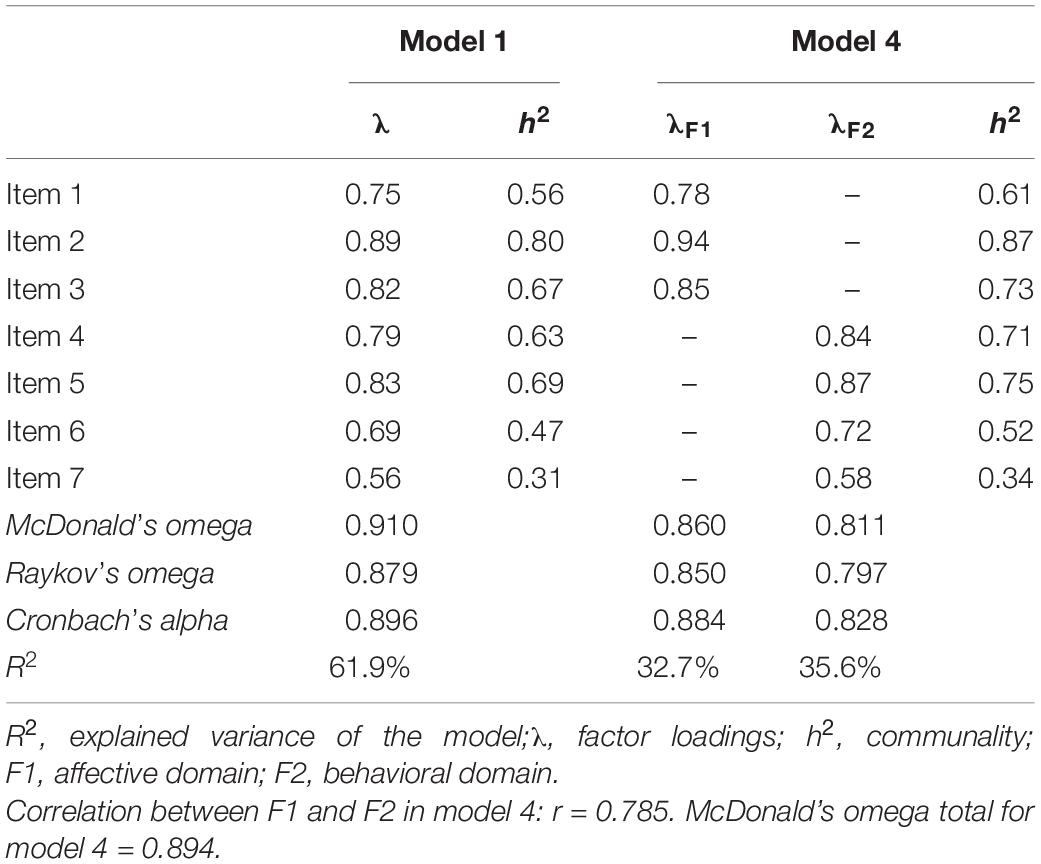
Table 5. Standardized regression weights (factor loadings) and errors (N = 369).
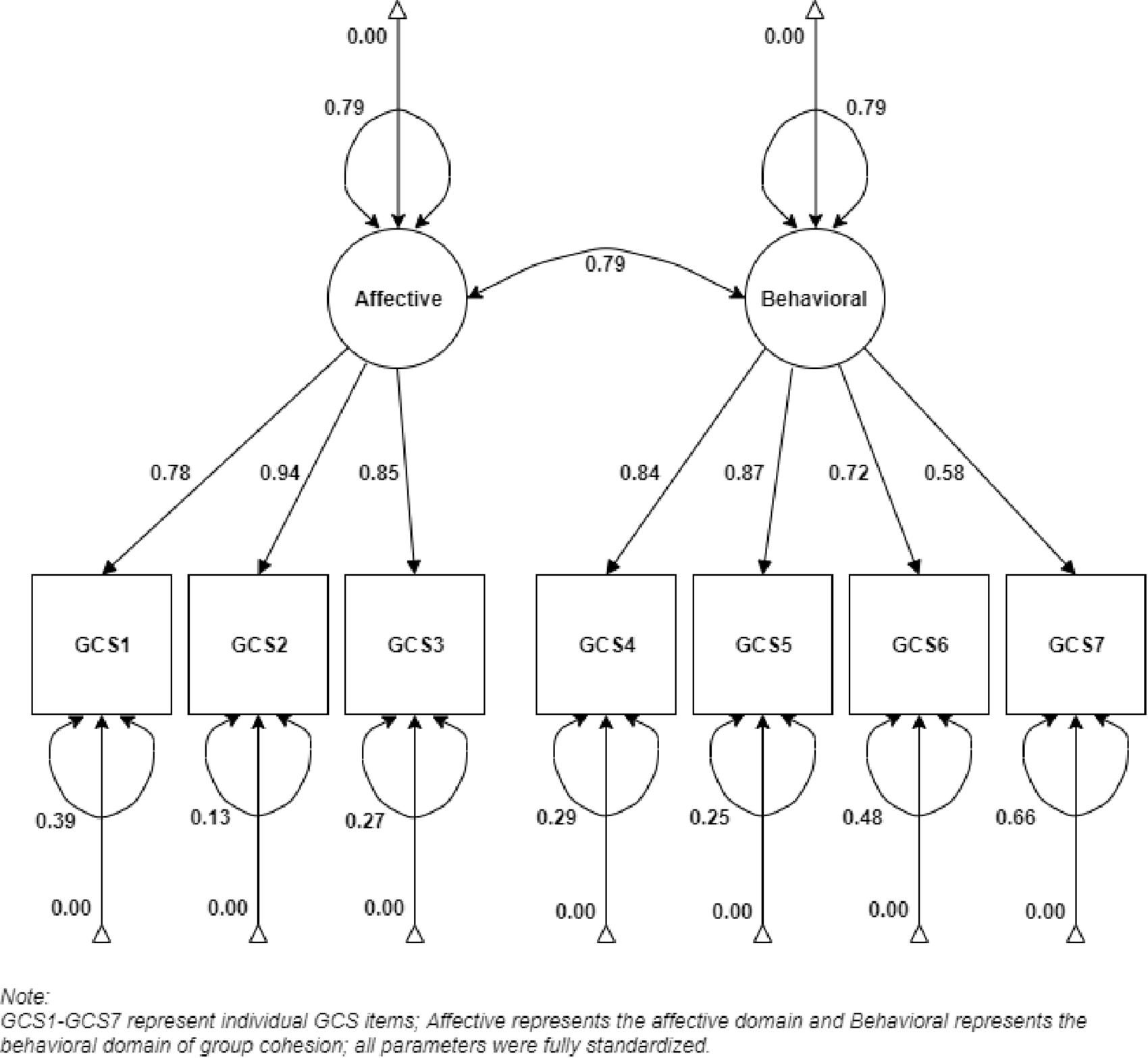
Figure 1. Factor structure of Group Cohesiveness Scale.
Measurement invariance was assessed for model 4 with respect to age, gender, and education (see Table 6). Several patients were lost due to missing responses on the demographic variables, namely, age (n = 9), gender (n = 7), and education (n = 9). Measurement invariance between the younger (n = 185) and older (n = 175) cohorts was reached on the configural, metric, scalar, factor mean, and residual levels. Even though the χ2-test was significant on the scalar and residual invariance level, other Δfit indices showed desirable values. Measurement invariance between women (n = 90) and men (n = 272) was reached on the configural, metric, scalar, and factor mean levels. Genders were not invariant only on the level of residual variances. Measurement invariance between lower (n = 197) and higher education levels (n = 163) was reached on the configural level. Even though the χ2-test was significant on both metric and scalar invariance levels, other Δfit indices showed desirable values, and the fit even increased with more restricted models. We could, therefore, consider the model invariant between education levels on the configural, metric, scalar, factor mean, and residual variance levels. Measurement invariance between the second (n = 369) and sixth weeks (n = 273) was reached on the configural level. Even though the χ2-test was significant on both the metric and scalar invariance levels, other Δfit indices showed desirable values, and the fit even increased with more restricted models. We could, therefore, consider the model invariant in time on the configural, metric, scalar, and factor mean levels. The final model was non-invariant only on the level of residual variances between the second and sixth weeks of measurement.
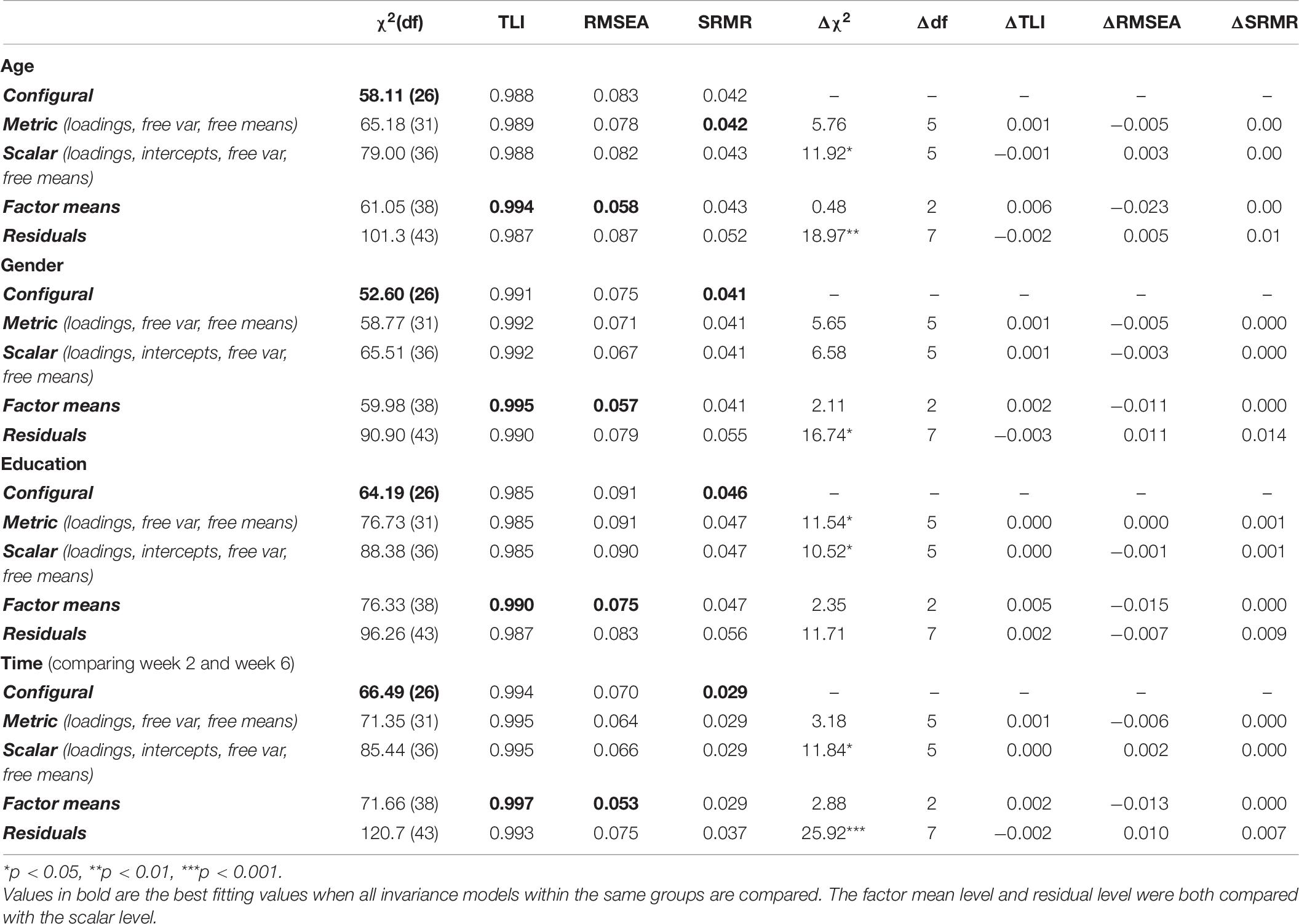
Table 6. Measurement invariance for Model 4 across age, gender, and education level.
The internal consistency of the final model was ω = 0.86 for the affective and ω = 0.81 for the behavioral domains (see Table 5). Additionally, the internal consistency of the general factor in model 1 was ω = 0.91. None of the GCS items would increase the internal consistency when dropped.
Thirteen participants had missing data on the GSRS scale, resulting in 367 patients. With respect to the final two-factor model with affective and behavioral dimensions (model 4), the affective domain was correlated more strongly with the GSRS (r = 0.449, p < 0.05) than the behavioral domain was (r = 0.290, p < 0.05). Additionally, a small to moderate positive correlation between the latent constructs of the unidimensional GCS (Model 1) and GSRS scales was found (r = 0.394, p < 0.05).
The present study described the validation of the Czech version of the Group Cohesiveness Scale (GCS). The average item scores and reliability were compatible with those of the original Thai version (Wongpakaran et al., 2013). However, we concluded that, based on a CFA, the most preferable model was a two-factor solution with the correlated affective and behavioral domains (model 4). This solution is more parsimonious than the fine-tuned unidimensional solution (model 2) suggested by Wongpakaran et al. (2013).
The final model demonstrated excellent fit and was invariant across age groups, genders, education levels, and time. The Czech version did not even show any problematic functioning of item 6 as presented in the English translation by Poyner-Del Vento et al. (2018). Theoretically, group cohesion is related to the working alliance (Johnson et al., 2005). However, in our study, we found only small to medium correlations between the GCS subscales and the GSRS. This finding was unexpected, since the GSRS measures patients’ relationships not only with the therapists/group leaders but also with other members of the group; therefore, there is an apparent overlap in what the instrument is expected to measure. Although the affective domain was more promising than the behavioral domain in terms of convergent validity, overall, the convergent validity of the GCS was not particularly supported in this study.
The GCS was conceived as a unidimensional construct by Wongpakaran et al. (2013). However, the unidimensional model (model 1) demonstrated an acceptable fit neither in their study nor in ours. Although the large correlation between the affective and behavioral factors may be interpreted in favor of the unidimensionality of the scale, the two dimensions are still independent to some degree and represent different phenomena conceptually. Theoretical support for the two-factor model with the affective and behavioral domains can already be found in the standardization study by Wongpakaran et al. (2013), even though these authors did not report fit indices for this model. Group cohesiveness has been recognized as a multidimensional construct several times in the past (Hogg, 1993). Mudrack’s (1989) definition of group cohesion as a combination of attraction-to-group and commitment to the group task provides a solid rationale for the differentiation of group cohesion into the affective and behavioral domain. The former is associated with the attraction to the group or its members and by collectively sharing positive, as well as negative, emotional experiences (Barsade and Knight, 2015). The latter, on the other hand, is associated with a commitment to the group (Mudrack, 1989) that may be manifested, for instance, by following group rules or giving gifts to other members (Lawler et al., 2000). Another literature supporting the two-dimensional model was Carron et al. (1985) who defined the individual group factor (commitment to other members of group) and task-social factor (interest in the goals of the group). Cota et al. (1995) in their review of group cohesion structure discussed both unidimensionality and multidimensionality resulting in favoring the multidimensional perspective (normative and behavioral components are divided and considered primary components of group cohesion). Kipnes et al. (2002) tested group cohesion dimensionality using two different instruments and claimed that cohesion is a multidimensional construct and offer a hierarchical structure [first order factors will be (1) bond to individual members and (2) level of trust and encouragement of the group as a whole].
In summary, given the high internal consistency of the unidimensional solution and the large correlation between the affective and behavioral dimensions, the GCS may be used as an essentially unidimensional measure of group cohesiveness. However, it should be done with caution and with the awareness of the fact that group cohesiveness may be, in fact, composed of different and partially independent phenomena.
The Czech version of the GCS demonstrated some features similar to those of the Thai version. Both versions were characterized by similar values of item-total correlations and internal consistency. Item loadings in terms of the unidimensional model were very similar for both versions as well. The GCS scores were relatively skewed in both studies. Patients tended to perceive their groups as rather cohesive in both cultures. Based on these similarities, we can argue that both versions are comparable.
However, certain differences between the Czech and Thai versions can be found. The two-dimensional solution as the best fitting solution is different from the original unidimensional solution. This may be attributed to cultural differences. Furthermore, the mean total score of the unidimensional model was higher in the Thai version (4.7) than in the Czech version (3.7). Therefore, Thai participants might perceive therapeutic groups as generally more cohesive than Czech participants do or might be less willing to report a lack of cohesion.
First, the sample was relatively heterogeneous and did not represent both genders equally (70% were female). Although this corresponds to the fact that most psychotherapy clients are women, future studies may investigate male groups to explore possible differences in the factor structure of group cohesion. Second, 67 patients dropped out of the study by the second week (i.e., the time when the first measurement of group cohesion took place). Although there were no significant differences between those who dropped out and those who continued with the treatment, this number of participants could have changed some subtle structures within the data. Third, two models yielded a satisfactory fit. The selection of the final model, even though theoretically anchored, is always relatively arbitrary in such cases. Moreover, none of the models fulfilled the criteria for a good fit regarding the χ2/df fit index. However, the chi-square test of model fit (and its derivatives) are sample size sensitive and could lead to the rejection of factor model even when residual variances are negligible. Fourth, the final two-factor model was invariant across age cohorts, genders, education levels, and time. Nevertheless, response options 1, 2, and 3 were clustered into a single response option because of missing response patterns in the data. This reduction of thresholds might have distorted our conclusions about the invariance. This response pattern might be explained by the tendency of group members to perceive their group likewise; hence, their responses to the measurement tool or to particular items could be limited to a very homogenous response style (Evans and Jarvis, 1980).
The Czech version of the GCS is a reliable and psychometrically valid tool for the measurement of the affective and behavioral domains of group cohesiveness. Thanks to its brevity, the scale is useful in the rapid hospital or therapeutic environment. As far as we know, this is the first psychometric validation of the GCS in Western culture and the Caucasian population. In this study, we revised the originally proposed unidimensional factor structure (Wongpakaran et al., 2013) and found support for the existence of the affective and behavioral domain of group cohesion.
The data analyzed in this study is subject to the following licenses/restrictions: The datasets analyzed during the current study are available from the corresponding author on reasonable request. Requests to access these datasets should be directed to AK, a2xvY2VrLmFkYW1AbWFpbC5tdW5pLmN6; https://www.researchgate.net/publication/344571321_GCS_full_dataset.
The studies involving human participants were reviewed and approved by the Research Ethics Committee of Masaryk University (Ref. No. EKV-2017-029-R1). The patients/participants provided their written informed consent to participate in this study.
AK: conceptualization, theoretical literature search, analysis, writing, and reviewing. TŘ: conceptualization and reviewing. HC: analysis and reviewing. All authors contributed to the article and approved the submitted version.
This research was funded by the Czech Ministry of Education, Youth, and Sports, internal grant MUNI/A/0993/2019.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Ashby, K. M., Collins, D. L., Helms, J. E., and Manlove, J. (2018). Let’s talk about race: evaluating a college interracial discussion group on race. J. Multicult. Counsel. Dev. 46, 97–114. doi: 10.1002/jmcd.12095
Barsade, S. G., and Knight, A. P. (2015). Group affect. Annu. Rev. Organ. Psychol. Organ. Behav. 2, 21–46. doi: 10.1146/annurev-orgpsych-032414-111316
Budman, S. H., Soldz, S., Demby, A., Davis, M., and Merry, J. (1993). What is cohesiveness? An empirical examination. Small Group Res. 24, 199–216. doi: 10.1177/1046496493242003
Budman, S. H., Soldz, S., Demby, A., Feldstein, M., Springer, T., and Davis, M. S. (1989). Cohesion, alliance and outcome in group psychotherapy. Psychiatry 52, 339–350. doi: 10.1080/00332747.1989.11024456
Carron, A. V. (1982). Cohesiveness in sport groups: interpretations and considerations. J. Sport Psychol. 4, 123–138.
Carron, A. V., Widmeyer, W. N., and Brawley, L. R. (1985). The development of an instrument to assess cohesion in sport teams: the group environment questionnaire. J. Sport Exerc. Psychol. 7, 244–266. doi: 10.1123/jsp.7.3.244
Cota, A. A., Evans, C. R., Dion, K. L., Kilik, L., and Longman, R. S. (1995). The structure of group cohesion. Pers. Soc. Psychol. Bull. 21, 572–580. doi: 10.1177/0146167295216003
Evans, N. J., and Jarvis, P. A. (1980). Group cohesion: a review and reevaluation. Small Group Behav. 11, 359–370. doi: 10.1177/104649648001100401
Hogg, M. A. (1993). Group cohesiveness: a critical review and some new directions. Eur. Rev. Soc. Psychol. 4, 85–111. doi: 10.1080/14792779343000031
Hooper, D., Coughlan, J., and Mullen, M. R. (2008). Structural equation modelling: guidelines for determining model fit. Electron. J. Bus. Res. Methods 6, 53–60.
Horvath, A. O., and Greenberg, L. S. (1989). Development and validation of the working alliance inventory. J. Counsel. Psychol. 36:223. doi: 10.1037/0022-0167.36.2.223
Hu, L. T., and Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 6, 1–55. doi: 10.1080/10705519909540118
Johnson, J. E., Burlingame, G. M., Olsen, J. A., Davies, D. R., and Gleave, R. L. (2005). Group climate, cohesion, alliance, and empathy in group psychotherapy: multilevel structural equation models. J. Couns. Psychol. 52, 310–321. doi: 10.1037/0022-0167.52.3.310
Kenny, D. A., Kaniskan, B., and McCoach, D. B. (2015). The performance of RMSEA in models with small degrees of freedom. Sociol. Methods Res. 44, 486–507. doi: 10.1177/0049124114543236
Kipnes, D. R., Piper, W. E., and Joyce, A. S. (2002). Cohesion and outcome in short-term psychodynamic groups for complicated grief. Int. J. Group Psychother. 52, 483–509. doi: 10.1521/ijgp.52.4.483.45525
Lawler, E. J., Thye, S. R., and Yoon, J. (2000). Emotion and group cohesion in productive exchange. Am. J. Sociol. 106, 616–657. doi: 10.1086/318965
Lese, K. P., and MacNair-Semands, R. R. (2000). The therapeutic factors inventory: development of a scale. Group 24, 303–317. doi: 10.1023/A:1026616626780
MacKenzie, K. R. (1983). “The clinical application of group measure,” in Advances in Group Psychotherapy: Integrating Research and Practice, eds R. R. Dies and K. R. MacKenzie (New York: International Universities Press), 159–170.
Mudrack, P. E. (1989). Defining group cohesiveness: a legacy of confusion? Small Group Behav. 20, 37–49. doi: 10.1177/104649648902000103
Poyner-Del Vento, P., Goy, E., Baddeley, J., and Libet, J. (2018). The caregivers’ attachment and relationship education class: a new and promising group therapy for caregivers of individuals with Parkinson’s disease. J. Couple Relationsh. Ther. 17, 97–113. doi: 10.1080/15332691.2017.1341356
Quirk, K., Miller, S., Duncan, B., and Owen, J. (2013). Group session rating scale: preliminary psychometrics in substance abuse group interventions. Counsel. Psychother. Res. 13, 194–200. doi: 10.1080/14733145.2012.744425
R Core Team (2020). R: A Language and Environment for Statistical Computing. Vienna: R Foundation for Statistical Computing.
Roark, A. E., and Sharah, H. S. (1989). Factors related to group cohesiveness. Small Group Behav. 20, 62–69. doi: 10.1177/104649648902000105
Rosseel, Y. (2012). Lavaan: an R package for structural equation modeling and more. Version 0.5–12 (BETA). J. Stat. Softw. 48, 1–36. doi: 10.1002/9781119579038.ch1
Tulin, M., Pollet, T. V., and Lehmann-Willenbrock, N. (2018). Perceived group cohesion versus actual social structure: a study using social network analysis of egocentric Facebook networks. Soc. Sci. Res. 74, 161–175. doi: 10.1016/j.ssresearch.2018.04.004
Wongpakaran, T., Wongpakaran, N., Intachote-Sakamoto, R., and Boripuntakul, T. (2013). The Group Cohesiveness Scale (GCS) for psychiatric inpatients. Perspect. Psychiatr. Care 49, 58–64. doi: 10.1111/j.1744-6163.2012.00342.x
Keywords: confirmatory factor analysis, group cohesion, Group Cohesiveness Scale, Czech validation study, affective and behavioral group cohesion
Citation: Klocek A, Řiháček T and Cígler H (2020) Psychometric Evaluation of the Czech Version of Group Cohesiveness Scale (GCS) in a Clinical Sample: A Two-Dimensional Model. Front. Psychol. 11:595651. doi: 10.3389/fpsyg.2020.595651
Received: 17 August 2020; Accepted: 11 November 2020;
Published: 03 December 2020.
Edited by:
Susana Sanduvete-Chaves, Seville University, SpainReviewed by:
Sai-fu Fung, City University of Hong Kong, Hong KongCopyright © 2020 Klocek, Řiháček and Cígler. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Adam Klocek, a2xvY2VrLmFkYW1AbWFpbC5tdW5pLmN6; YWtsb2Nlay5ha0BnbWFpbC5jb20=; Tomáš Řiháček, cmloYWNla0Bmc3MubXVuaS5jeg==
†ORCID: Adam Klocek, orcid.org/0000-0002-0797-4890; Tomáš Řiháček, orcid.org/0000-0001-5893-9289; Hynek Cígler, orcid.org/0000-0001-9959-6227
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.