 David Fernández-García
David Fernández-García María Del Carmen Giménez-Espert
María Del Carmen Giménez-Espert Elena Castellano-Rioja
Elena Castellano-Rioja Vicente Prado-Gascó
Vicente Prado-Gascó
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol. , 18 December 2020
Sec. Educational Psychology
Volume 11 - 2020 | https://doi.org/10.3389/fpsyg.2020.585826
This article is part of the Research Topic The Marketization of Higher Education: The State of the Union between the Student as Consumer and the Free Market View all 8 articles
Clinical practices are considered one of the cornerstones in nurses' education. This study provides a framework to determine how factors in the academic environment, influence nursing student's satisfaction with their practices. A cross-sectional analytical study was conducted in a convenience sample of 574 nursing students at a private university in Valencia, during the 2016/2017 academic year, 79% (456) were women. Two statistical methodologies were used for data analysis: hierarchical regression models (HRM) and fuzzy sets qualitative comparative analysis (fsQCA). The HRM indicate that the students' mean score influences all dimensions of satisfaction. Furthermore, in the fsQCA, the type of service and center, as well as the type of management, the preference in the choice of the practice center and the number of students per period per clinical educator influence satisfaction with clinical practices. These results could be used to understand how academic factors influence nursing students' satisfaction with their clinical practices and to create intervention programmes that improve it. This will help prepare students to be the future nursing workforce.
Marketing literature has shown an interest in the relationship between quality management and consumer satisfaction (Rauyruen and Miller, 2007), because perceptions of quality and judgments of satisfaction have been recognized as fundamental aspects in explaining desirable consumer behaviors (Zeithaml et al., 1993). One of the major challenges that higher education institutions face today is improving the quality of the education system (Pucciarelli and Kaplan, 2016). The approaches created since the 1980s, based around the importance of studying the concept of quality of service and its evaluation (Parasuraman et al., 1985; Cronin and Taylor, 1992), have led to a paradigm in which it has been consolidated as a key aspect in the success of any business model (Parasuraman et al., 1988; Cronin and Taylor, 1992). In the field of higher education, interest in this concept has increased as a result of the growth in the number of university students, the interest in improving public services, the increase in competition in the education market and the tension between efficiency and quality (Green, 1994). Advances in the study of the quality of the service have shown a relationship between its dimensions and the satisfaction of the user/consumer (Falk et al., 2010), and with the intention to purchase and later recommendation (Olorunniwo et al., 2006).
Quality of service has been defined in many ways, but one of the most widely accepted definitions is a type of activity that reflects the excellence or superiority of a particular service, placing the emphasis of this quality on the relationship between the employee and the user (Parasuraman et al., 1985). In the educational sphere, it refers to quality in terms of the purpose of the product, i.e., quality must be judged according to whether the product or service offered accomplishes the stated purpose (Green, 1994). Finally, when evaluating quality from the perspective of expectations, it is essential to address the needs of users, by considering subjective factors related to the judgments of the people who receive the product or service (Moreno et al., 2015). The quality of an educational system, a university degree or nursing practices can be measured using many different variables, since many factors affect it, but the satisfaction that this system, this degree or these practices generate among users has long been one of the variables to be taken into account, thus becoming a key element in teaching quality (Löfmark et al., 2012). In addition, in order to provide a quality service, it is necessary to resolve all the aspects related to the functioning of the organization, taking into account that the differences between service expectations and perceptions can be added to others, such as discrepancies in the organization's functioning (García-Pascual et al., 2020).
The perceptions of quality and satisfaction judgments a student may have about their degree course, the institution and their organization have been recognized as key constructs in explaining the behaviors of “consumers” of a product, which in this case is an educational product (Rauyruen and Miller, 2007). In fact, several studies state that the satisfaction created by the educational process is an inherent element of quality (Löfmark et al., 2012), and as such analyzing the students' view of their clinical training can provide very valuable information for reconstructing and improving the teaching activity and the level of nursing education (Papathanasiou et al., 2014). Including student participation and perceptions in the evaluation of the quality of educational programs is therefore essential (Haraldseid et al., 2015), since improving the students' experience in their clinical learning environment can improve students' learning outcomes (Payne, 2016) and satisfaction.
Clinical practices are considered one of the cornerstones in nurses' education. Indeed, in order to be able to practice professionally as a nurse, a wide range of skills must be acquired in real environments so that the student can provide the patient with quality care (Bengtsson and Ohlsson, 2010; DeBourgh, 2012; Lewallen and DeBrew, 2012). Half of the education of nursing students in the European Union (EU) is conducted in clinical environments (Directive 2013/55/EU of the European Parliament of the Council, 2013). The quality of clinical environments and the competence of the clinical supervisor in the mentoring of nursing students (Jack et al., 2018; Pitkänen et al., 2018) substantially affects the learning of nurses (Pramila-Savukoski et al., 2020). The teaching in clinical practices involves student-centered learning, and not only in the knowledge that must be acquired (Bengtsson and Ohlsson, 2010). This new competency-based learning approach aims to enable nursing students to participate in self-directed learning (Lekan et al., 2011), maintaining fundamental and close communication with their clinical educators (Papathanasiou et al., 2014, Vizcaya-Moreno et al., 2018). Feedback (Almalkawi et al., 2018) and evaluation of students' learning by clinical supervisors is critical (Tuomikoski et al., 2019), so that they can apply their knowledge, skills and critical thinking (Haraldseid et al., 2015; Aktaş and Karabulut, 2016; Glynn et al., 2017).
This means new rules should be adopted so that the student and the teacher become agents who participate in the educational process. The supervision of practical training is increasingly important in the new nursing curricula for this reason. The interaction between the educator and the learner is a central element of the educational service, and one of the main indicators of satisfaction (Oldfield and Baron, 2000; Vizcaya-Moreno et al., 2018). Some studies report that the clinical education period is characterized by poor physical and mental health, a loss of interest in the profession and unacceptable care (Jeffries et al., 2013; Zamanzadeh et al., 2015; Drayton-Brooks et al., 2017). However, other studies mention positive experiences in the acquisition of knowledge, skills and attitudes of students in their clinical practices (Mulready-Shick and Flanagan, 2014; Nishioka et al., 2014; Glynn et al., 2017). The quality of clinical practices is a very significant influence on student's adherence, academic performance and closely related to their professional development of nursing competence (Perry et al., 2018). Based on previous literature, our hypothesis is as follows: (H1) Higher mean student scores will predict higher levels of satisfaction with clinical practice in nursing students.
This satisfaction of a nursing student during their clinical practice and their consequent involvement in the process can be influenced by many different factors, ranging from social and psychological factors to environmental and academic factors (El Ansari and Oskrochi, 2004). The literature includes studies that highlight the following factors in nursing students' satisfaction with their practices: the clinical educator, the learning environment, the activities carried out by the student and the organization of the practices (Milton-Wildey et al., 2014; Salamonson et al., 2015; Payne, 2016). These findings suggest the following hypothesis: H2 Preference in the choice of the practice center, the distance to the practice center, the number of students assigned to the clinical educator, the type of service, the type of center and the type of management have an influence on nursing students' satisfaction with clinical practice. Nursing students' satisfaction with their clinical practice helps students feel prepared for their future work, and is associated with their future work intentions (Milton-Wildey et al., 2014). Employment policies for recruiting and retaining nursing staff in hospitals should also be concerned with strategies to improve student education in their training (Barnett et al., 2010). Nurses are essential professionals in healthcare systems (Allen, 2018), and in order to prepare students adequately for the workplace and retain them in the workforce, the curricula of educational programs must succeed in providing students with the knowledge necessary to competently manage their role providing patient care in a difficult work environment (Hayes et al., 2006). These aspects are basic in any profession, but they are paramount for nurses because of the need for student nurses in order to offset the retirement of nurses (Aiken et al., 2009) and a serious shortage of nurses around the world (World Health Organization, 2020). In addition, the lack of job satisfaction among nurses has been associated with professional dissatisfaction as a powerful predictive factor for considering moving abroad (Ma et al., 2010), in search of better salaries, and a better quality of life (Granero-Lazaro et al., 2017).
This study focused on assessing how factors in the academic environment (preference in the choice of the practice center, the mean score of students, distance to the practice center, number of students assigned to the clinical educator, type of service, type of center and type of management) influence nursing students' satisfaction with their practice, using two different approaches: hierarchical regression models (HRM) and qualitative comparative analysis (QCA).
A cross-sectional analytical study was conducted in a convenience sample of 574 students on the nursing degree course at a private university in Valencia. Seventy-nine percentage (454) were women and the average age was (M = 24.4; SD = 6). See Table 1 for detailed information.
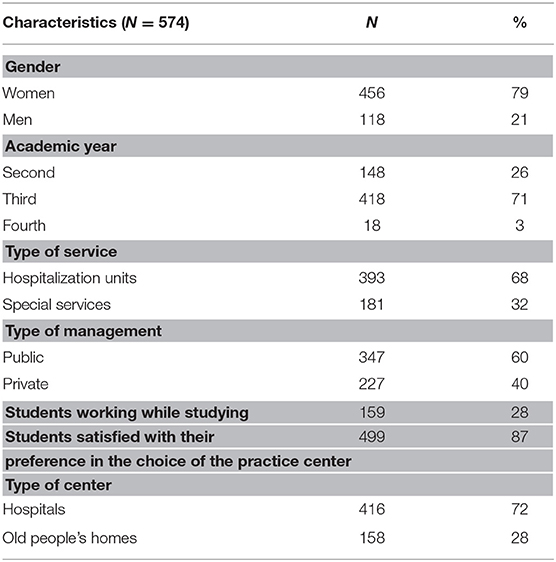
Table 1. Characteristics of the sample.
This study complied with the basic principles of the Helsinki Declaration (World Medical Association, 2013), with an emphasis on the anonymity of the data collected, confidentiality and non-discrimination of participants. This study was approved by the Research Ethics Committee of the University where the study was developed. All participants received detailed information about the objective and the procedure and were informed about confidentiality. The inclusion criteria were being a student on the clinical practice of the nursing degree course who gave their informed consent prior to their inclusion in the study. The anonymity and confidentiality of the information provided were respected. The data collection was carried out during the 2016/2017 academic year and consisted of completing an online questionnaire lasted about 20 min.
The variables related to the service (a type of service, type of management and type of center), preference in the choice of the practice center, the mean score of students, distance to the practice center and the number of students assigned to the clinical educator.
The following validated instruments were used to measure the perceived satisfaction with the practices:
Clinical Learning Environment (CLE-1995; Dunn and Burnett, 1995), is a 23-item instrument composed of five subscales: staff-student relationships, preceptor's commitment, patient relationships, student satisfaction and hierarchy and ritual, rated on a 5-point Likert scale ranging between 1 (strongly disagree) and 5 (strongly agree). Examples of the items are: “I am happy with the experience I have had on this ward” “This was a good ward for my learning.” The reliability coefficients using Cronbach's alpha range from high (0.85) to marginal (0.63).
Clinical Learning Environment and Supervision (CLES-2002; Saarikoski and Leino-Kilpi, 2002), is a 27-item instrument divided into five sub-dimensions with the following number of items: ward atmosphere (five items); leadership style of the ward manager (four items); premises of nursing care on the ward (four items); premises of learning on the ward (six items) and supervisory relationship (eight items). The respondent answers the statements on a five-step Likert-type scale. The alternatives in the Likert scale were: (1) fully disagree; (2) disagree to some extent; (3) neither agree nor disagree; (4) agree to some extent and (5) fully agree. Examples of the items are: “The staff were easy to approach,” “There was a positive atmosphere on the ward.” The reliability coefficients of the sub-dimensions in this sample ranged from high (0.94) to marginal (0.73) using Cronbach's alpha.
Clinical Learning Environment Inventory (CLEI-2003; Chan, 2003). This instrument has 35 items, with 7 each items assessing five scales: personalization, student involvement, task orientation, innovation, and individualization, using a 4-point Likert-type scale with the alternatives of (1) strongly agree, (2) agree, (3) disagree, and (4) strongly disagree. Sample items include: “Students are generally allowed to work at their own pace,” “There are opportunities for students to express opinions in this ward.” Chan developed an instrument with two roles: for measuring the student's real perceived satisfaction with their practices, and for measuring the student's desired satisfaction with their practices. This aims to determine whether what the student wants is similar to their real experience. All the dimensions were Cronbach's Alpha >0.66, in both the real and in the desire instrument.
Clinical Learning environment, supervision and nurse teacher (CLES+T – 2008; Saarikoski et al., 2008). This consists of 34 items on five scales; supervisory relationship, pedagogical atmosphere on the ward, role of the nurse teacher, leadership style of the ward manager, and premises of nursing on the ward. The alternatives in the 5-step continuum scale (used in all phases of the study) were: (1) fully disagree, (2) disagree to some extent, (3) neither agree nor disagree, (4) agree to some extent, and (5) fully agree. Sample items included “In our common meetings I felt that we are colleagues,” and “The focus on the meetings was on my learning needs.” The reliability coefficients of the other sub-dimensions of CLES+T instrument using Cronbach's alpha ranged from high (0.96) to marginal (0.77). In this study the validated Spanish version was used (Vizcaya-Moreno et al., 2015). Cronbach's alpha was between 0.80 and 0.97.
Clinical Assessment Instrument (IEC-2009; Navarro, 2009), containing 67 items and five subscales in the Spanish language, 12 on program organization, 19 on teaching practice, 14 on student role, eight on student environment learning and eight on clinical experience. Each item was answered on a five-category Likert scale: 1 “strongly disagree,” 2 “partially disagree,” 3 “neither disagree nor agree,” 4 “partially agree” and 5 “strongly agree.” Sample items included “The objectives proposed were relevant to the achievement of learning,” and “Teachers facilitate students' clinical learning.” Cronbach's alpha was between 0.92 and 0.71.
To measure student participation in nursing activities during clinical practice (Slaughter-Smith et al., 2012; Zhang et al., 2012; Kristofferzon et al., 2013), the NIC taxonomy (NIC = Nursing Interventions Classification) (Ahn and Choi, 2015) was used. The instrument showed adequate psychometric properties: χ2/df = 1.36; NNFI = 0.97; CFI = 0.97; IFI = 0.97; RMSEA = 0.02 (IC = 0.018–0.025); αtotal = 0.96; αclinicaleducator = 0.97; α learningenvironment = 0.94; αactivitiesperformed = 0.93; α universityorganization = 0.92. It consisted of a 43-item separated into four dimensions of satisfaction (with the clinical educator, the activities performed, the learning environment and the university organization) and the average overall satisfaction for each of these dimensions. A 5-point Likert scale was chosen, where 1 was the equivalent to “totally disagree” and 5 to “totally agree.” Sample items included “Nursing professionals are interested in the supervision of students,” and “Working conditions were appropriate for learning.”
Descriptive analysis (mean, standard deviation) and hierarchical regression models (HRM) were used by means of the IBM SPSS Statistics 24 software package (IBM Corporation), while the qualitative comparative analysis (QCA) was carried out by means of fsQCA 2.5 (Claude and Christopher, 2014).
Linear regression methods compare the individual contribution of each variable to determine which one best explains the result. fsQCA is a variant of qualitative comparative analysis (QCA) and is based on defining the conditions that lead to the configurations causing the result of interest, expressing the combination rather than the individual contribution (Vis, 2012). The fundamental characteristics of this methodology are as follows (Ragin, 2008, 2014): (1) fsQCA studies are based on Boolean algebra, and its associated tools (e.g., truth table, consistency and coverage scores, set coincidence). (2) fsQCA is based on qualitative evidence using small or medium-sized samples, although although working with larger samples is possible (Vis, 2012); (3) fsQCA is based on the combination of variables, including equifinality, i.e., the different paths that lead a specific outcome; (4) fsQCA is used in regional analysis among other disciplines because of its advantages over correlation methods (García-Álvarez-Coque et al., 2017). This method has been developed to effectively approach research questions about which combination of conditions is associated with a particular result (Greckhamer et al., 2018).
The raw data was prepared according to the literature before performing the QCA (Ragin, 2008). First, all the missing values were eliminated and the variables recalibrated (Eng and Woodside, 2012). In our case (0 = woman;1 = man), (0 = second year; 0.49 = third year; 1 = fourth year), (0 = not working while studying; 1 = working while studying), (0 = specialized services; 1 = hospitalization), (0 = public institution; 1 = private institution), (0 = home care provider; 1 = hospitals), (0 = dissatisfied preference in the choice of the practice center; 1 = satisfied preference in the choice of the practice center) and all the dimensions of satisfaction were recoded (totality, clinical educator, learning environment, activities performed and organization of clinical practice) (0 = 3; 0.49 = 3.1 to 4; 1 = 4.1 to 5). The continuous variables, i.e., those related to the average student score, distance from the practice center and the number of students assigned to the clinical educator were recalibrated with fsQCA 2.5, by multiplying their components and then considering the three proposed thresholds (Woodside, 2013): 10% (low level or all outside the set), 50% (medium level, neither inside nor outside the set) and 90% (high level or all inside the set). The participants' responses to the analysis variables were coded as 0 and 1, where 0 means absence and 1 means presence. However, for continuous variables and interview factors composed of different elements, three values had to be taken into account to automatic recalibration. In the first (0), an observation with this value is completely outside the defined range (low level of agreement/value, in our case low satisfaction); the second (0.5) considers a mid-point, neither inside nor outside the framework (average level of agreement/value, average level of satisfaction); and the last (1) considers the observation completely within the framework (high level of agreement/value, high level of satisfaction) (Ragin, 2008).
The necessary and sufficient conditions were then used to assess the influence on the satisfaction of the variables associated with the service (type of service, type of management and type of center), preference in the choice of the practice center, average score of students, distance to the practice center and the number of students assigned to the clinical educator. The fsQCA analysis revealed three possible solutions for sufficient analysis: complex, parsimonious and intermediate (the latter was recommended by Ragin, 2008).
The most important descriptors and calibration values of the variables examined are shown in Table 2.
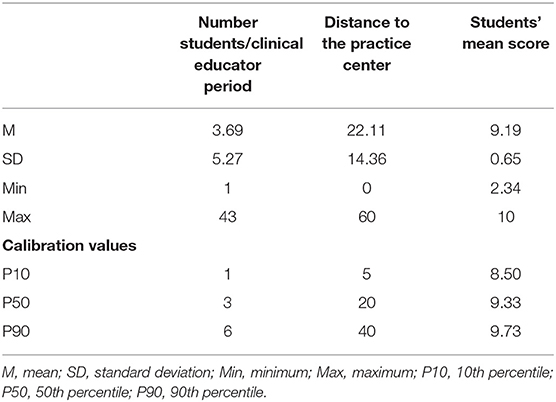
Table 2. Main descriptions and calibration values.
The variables studied were analyzed using hierarchical regression models. The criteria variables were satisfaction (total, clinical educator, activities performed, learning environment and university organization of the clinical practice). The independent variables were related to the service (type of service, type of management and type of center), preference in the choice of the practice center, students' mean score, distance to the practice center and number of students assigned to the clinical educator. First, the variables of preference in the choice of the practice center, students' mean score, distance to the practice center were performed, and the number of students per clinical educator period were then entered in a second step. Finally, the variables related to the service (type of service, type of management and type of center) were included in the third step.
The variables related to the preference in the choice of the practice center, students' mean score, distance to the practice center were included, and the number of students per clinical educator period (Table 3) was estimated for 5% of overall satisfaction (R2 adjusted = 0.05, p ≤ 0.001), 4% of clinical educator satisfaction (R2 adjusted = 0.04, p ≤ 0.001), 5% of environment satisfaction (R2 adjusted = 0.05, p ≤ 0.001) and finally 2% of activity satisfaction (R2 adjusted = 0.02, p ≤ 0.01).
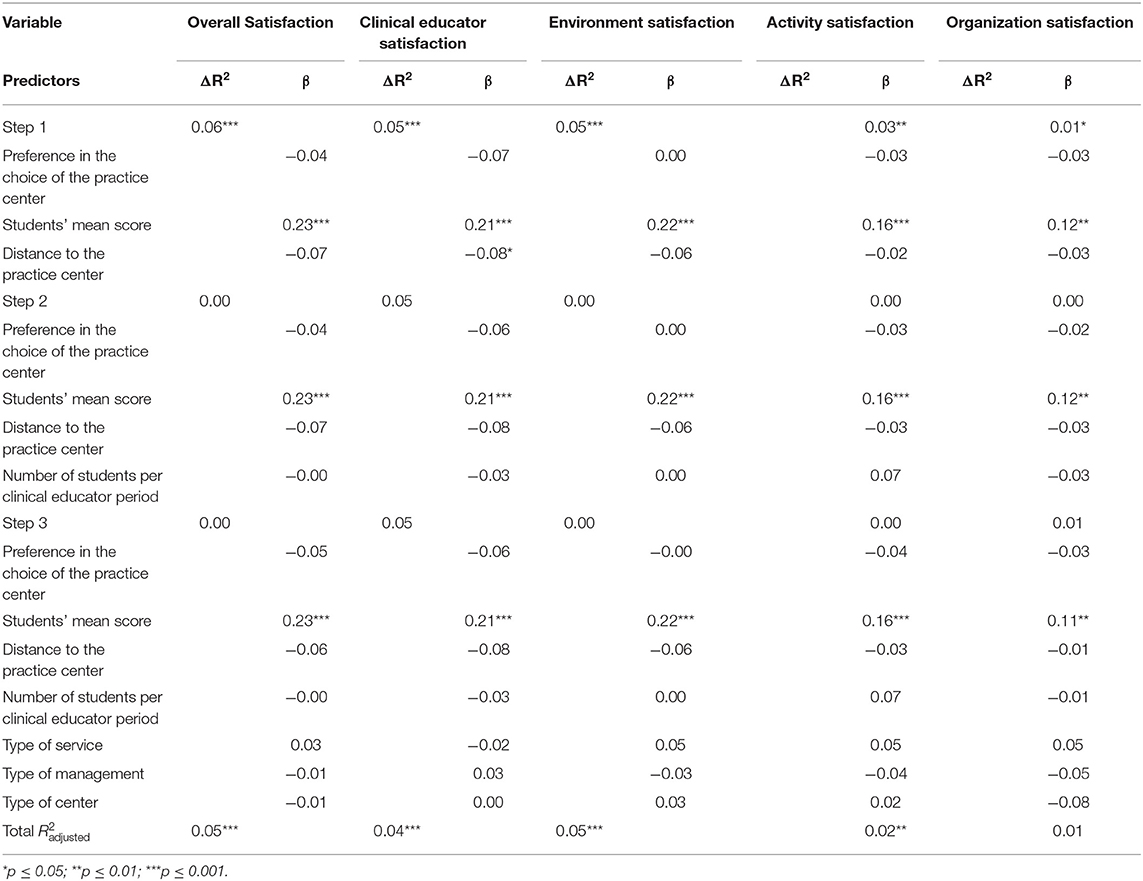
Table 3. Hierarchical regression analysis with the satisfaction variable.
The linear regression model showed that the mean score of students determined a positive and significant beta coefficient in their satisfaction in overall terms (β = 0.23; p ≤ 0.001), and with their clinical educator (β = 0.21; p ≤ 0.001), environment (β = 0.22; p ≤ 0.001), activity (β = 0.16; p ≤ 0.001) and organization (β = 0.11; p ≤ 0.01).
Necessary conditions are those that must always be present for a given outcome to occur, while sufficient conditions refer to those conditions (or a combination of them), that can lead to an outcome, even if they are not always present (Ragin, 2008).
The results obtained (Table 4), showed that it appears that there are no necessary conditions for satisfaction since the consistency is <0.90 in all cases (Ragin, 2008).
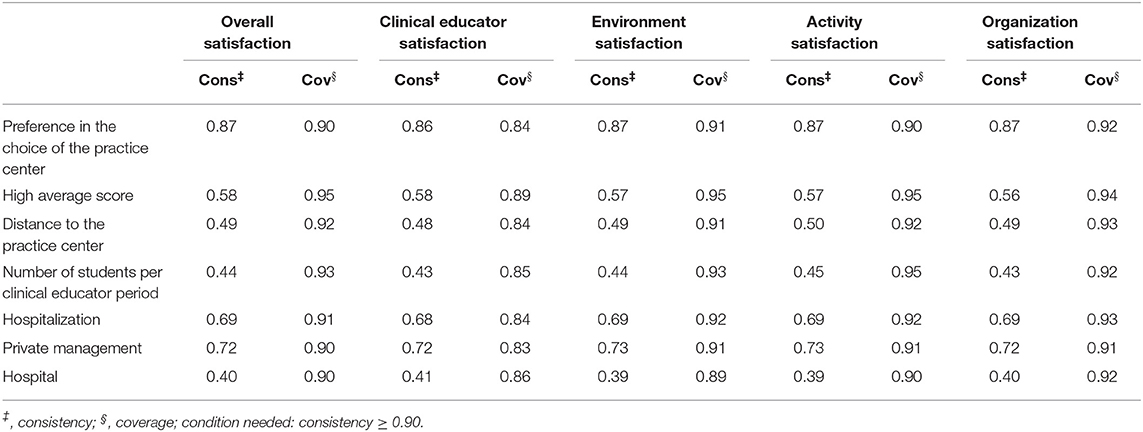
Table 4. Necessary condition analysis for satisfaction.
A sufficiency analysis considers the solution coverage (variance explained, the number of observations that can be explained by a given combination of conditions) and the solution consistency (the reliability or relevance of the model). It also includes raw coverage (variance explained, how many cases or observations can be explained by a particular path or combination of conditions) and the unique coverage indicates the number of observations that can be clarified by one given path, but not by others (Ragin, 2008; Eng and Woodside, 2012).
Table 5 summarizes the three main sufficient conditions for the intermediate satisfaction solution according to the format Fiss (2011). In sufficiency analyses, a model is informative, when the consistency is above or around 0.75 (Eng and Woodside, 2012). When measuring overall satisfaction, 13 paths explained 74% of the high levels of overall satisfaction (overall consistency = 0.94; overall coverage = 0.74). The most important path for explaining it was the interaction of preference in the choice of the practice center, hospital and the proximity to the practice center (raw coverage = 0.33; consistency = 0.94), which accounted for 33% of cases with high overall satisfaction.
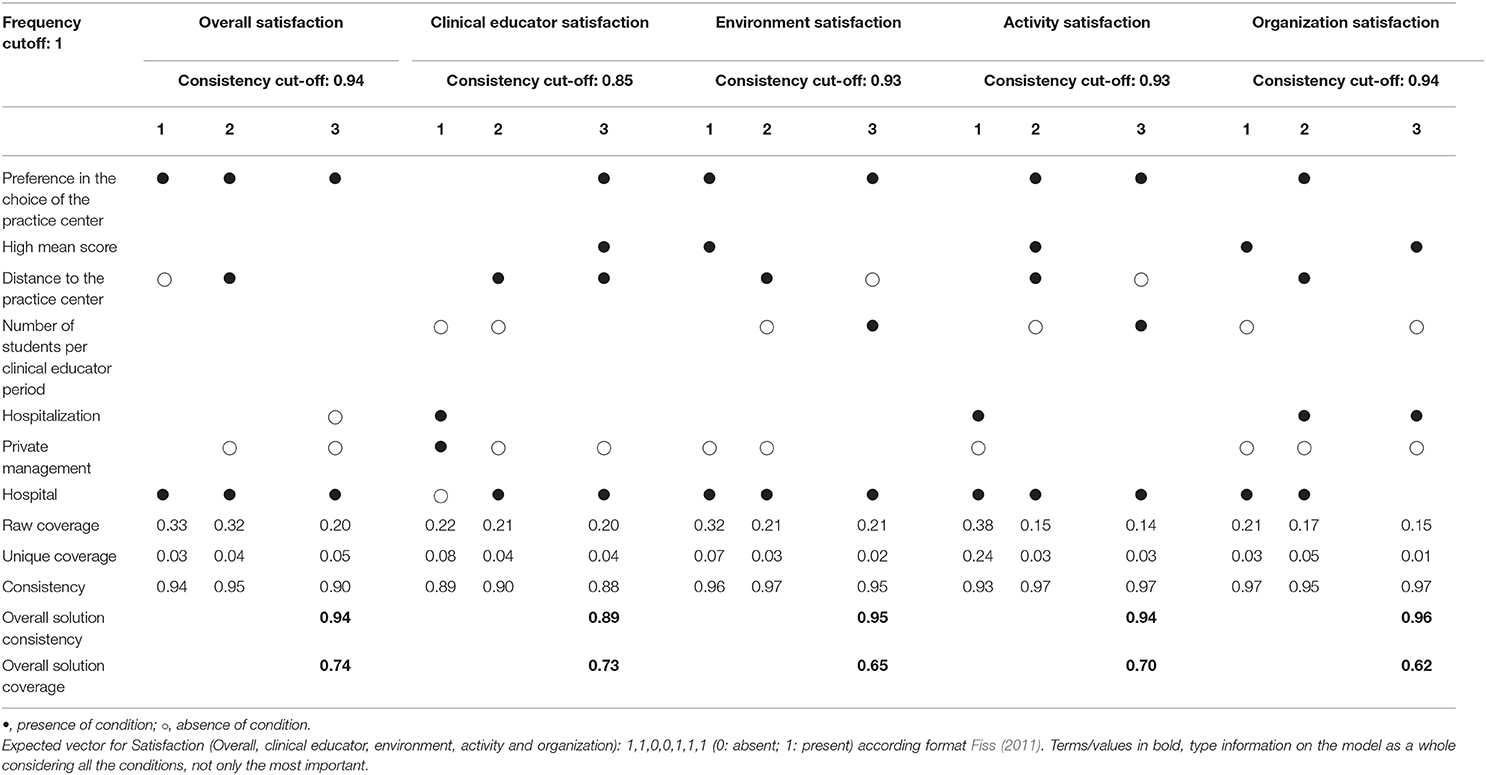
Table 5. Summary of the three main sufficient conditions for the intermediate solution of satisfaction.
Sixteen paths were found that explained 73% in the high levels of satisfaction with the clinical educator (overall consistency = 0.89; overall coverage = 0.73). The most important path that explains high levels of satisfaction with the clinical educator was the result of the interaction of hospitalization, private management, home care and low student numbers per clinical educator period, which accounted for 22% of the cases with high satisfaction with the clinical educator (raw coverage = 0.22; consistency = 0.89).
Twelve paths explained 65% of high levels of satisfaction with the learning environment (overall consistency = 0.95; overall coverage = 0.65). The most important path for explaining high levels of satisfaction with the learning environment was the interaction of preference in the choice of the practice center, students' high mean score, hospital and public management, which accounted for 32% of the cases (raw coverage = 0.32; consistency = 0.96).
When high levels of satisfaction with the activities performed were considered, 10 paths explained 70% (overall consistency = 0.94; overall coverage = 0.70). The most important path for explaining high levels of satisfaction with the activities performed arose from the combination of hospital, hospitalization and public management, which accounted for 38% of the cases (raw coverage = 0.38; consistency = 0.93).
Finally, 16 paths accounted for 62% in the high levels of satisfaction with the organization of the clinical practice (overall consistency = 0.96; overall coverage = 0.62). The most important path accounts for 21% of the cases (raw coverage = 0.21; consistency = 0.97), and this was the combination the hospital, the students' high mean score, a small number of students period/clinical educator, and public management.
This study extends the research on factors influencing nursing students' satisfaction in clinical practices where they learn important practical skills, their professional role, behavior, attitudes and values (Sandvik et al., 2014). The factors influencing the satisfaction with their clinical practice related to the academic environment (preference in the choice of the practice center, mean students' grade, distance to the practice center, number of students assigned to the clinical educator) and the service (type of service, type of center and type of management) were examined using complementary methodologies regression models and fsQCA models.
In general, the first hypothesis, i.e., higher mean student scores predict higher levels of satisfaction with clinical practices in nursing students, can be accepted in the regression model and partially accepted in fsQCA model. The regression models showed that the unique predictive variable is the students' mean score for all dimensions of satisfaction (overall satisfaction, with the clinical educator, the activities performed, the learning environment and the university organization). According to the literature, one of the most predictive indicators for measuring academic performance is the academic grade (Takashima et al., 2019). In the fsQCA model, the students' mean score is a condition for satisfaction with the learning environment and with the organization of the clinical practice. A quality learning environment and adequate organization of practices are considered key elements in the satisfaction of nursing students (Bisholt et al., 2014). For this reason, including student participation and perceptions in the evaluation of the quality of educational programs is today considered essential (Haraldseid et al., 2015), given that improving student experiences in their clinical learning environment can improve student learning outcomes and their satisfaction with the clinical practice (Pimparyon et al., 2000; Payne, 2016).
In the second hypothesis, the preference in the choice of the practice center, the distance to the practice center, the number of students assigned to the clinical educator, type of service, the type of center and the type of management have an influence on nursing students' satisfaction with clinical practices. This hypothesis can be accepted in the fsQCA model and partially accepted in the regression model. In general, fsQCA present higher levels of prediction than regression models. In the regression models, the variables related to the academic environment slightly estimated all the dimensions of satisfaction apart from university organization. The necessary conditions for satisfaction did not apply in the fsQCA models. In the sufficiency analysis, the most important conditions for predicting overall satisfaction were preference in the choice of the practice center, hospital and proximity to the practice center. For the clinical educator, the conditions were hospitalization, private management, home care and few students per clinical educator period. For satisfaction with the learning environment, the interactions were preference in the choice of the practice center, students' high mean score, hospital and public management. In the activities performed, the interactions were hospital, hospitalization and public management. Finally, in satisfaction with the clinical practice organization, the interactions were the hospital, students' high mean score, a low number of students period/clinical educator and public management. These results confirm that the number of students, type of center, management and service were conditions considered fundamental for the satisfaction of nursing students with the clinical educator and with the organization of the clinical practice by the university (Dunn and Burnett, 1995; Bergjan and Hertel, 2013; Ahn and Choi, 2015; Wafaa-Gameel et al., 2015). The service in which the clinical practice was carried out and the supervision of the clinical educator have a direct impact on the students' learning and satisfaction with the clinical educator and the organization of the clinical practice, the guidance and information (Milton-Wildey et al., 2014). Constructive feedback and reflective discussion from the clinical educator (Burden et al., 2018) improves the students' clinical knowledge and reasoning (McSharry and Lathlean, 2017). In that the student receives from the university, as part of the strategy to provide better support for students, influences the student's perception of the learning environment in the hospital (Chuan and Barnett, 2012; Lamont et al., 2015).
In addition, fsQCA models showed that the type of center (hospital) and public management were important conditions in satisfaction with the learning environment and with the activities. The type of service is a significant condition in satisfaction with the clinical educator and the activities. The literature indicates that human resources, materials, and even the way students are supervised are different in publicly managed facilities (O'Brien et al., 2019). Appropriate planning of the type of center, service, the students' clinical placement and students' clinical learning activities are important to ensure that the environment offers the student an appropriate learning situation (Sundler et al., 2014) and gives the student an overall perspective of nursing work and the various interventions that professionals may have to perform, from hospital to primary care (McInnes et al., 2015) so that the student has a comprehensive vision and education of nursing.
Despite the interest of the research, this study has some limitations. The study was conducted using a convenience sample at a single university, and as such the results cannot be generalized. It would be necessary to use a larger and more representative sample of other universities in future research. Another limitation of the study is the use of self-report measures, which can introduce social desirability biases. Using other heterocompleted measures and/or having objective external measurements would be necessary in future research.
As for implications for practice, this study provides information about how the interactions of conditions influence nursing students' satisfaction with clinical practice using fsQCA. There are no studies that examine the different academic variables that influence nursing students' satisfaction with clinical practice using this methodology. Likewise, the QCA models and linear models have different objectives and should be used in a complementary way (Ragin, 2008). In conclusion, the regression model shows the unique predictive variable is the students' mean score for all dimensions of satisfaction. In the fsQCA model, the students' mean score, the type of center (hospital), the type of management (public), the type of service, the preference in the choice of the practice center and the number of students were conditions considered fundamental for the satisfaction of nursing students with their clinical practice (with their educator, environment, activities and organization). These results can be considered on the interventions and practices programs related to the improvement of clinical practice. These measures will have a positive impact on student satisfaction and offers the student an appropriate learning situation (Sundler et al., 2014). They can be incorporated into university programs to improve the education of future professionals through clinical teaching models based collaboration between the university and the hospital to enhance evidence-based learning, thereby achieving significant changes in the quality of student education (Harvey et al., 2013). In addition, improved clinical practice planning enhances clinical educator attitudes (O'Brien et al., 2014).
A proper understanding of how the education of future nursing professionals is involved in the working relationship and the professional aspirations of students within the different roles in nursing could lead to appropriate strategies for creating more effective and robust collaboration between universities and hospitals (Limoges and Jagos, 2015). Appropriate education programmes and improved management in the recommended clinical settings are required to facilitate the transition of nurses from university to practice (Jeffries et al., 2013; Zamanzadeh et al., 2015; Drayton-Brooks et al., 2017), increase nurse retention (Ward and McComb, 2018), and positive attitudes. This study can be considered a first step toward the study of academic environmental factors that influence the satisfaction of nursing students with their practices.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Research Ethics Committee of the Catholic University of Valencia San Vicente Mártir UCV 2017-2018-032. The patients/participants provided their written informed consent to participate in this study.
DF-G, MCG-E, EC-R, and VP-G: made a substantial contribution to the concept or design of the work, or acquisition, analysis or interpretation of data, drafted the article or revised it critically for important intellectual content, approved the version to be published, and have participated sufficiently in the work to take public responsibility for appropriate portions of the content. All authors contributed to the article and approved the submitted version.
The publication of this article has been financed 50% by the Universidad Católica de Valencia San Vicente Mártir.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We thank to all nursing students who participated in this study.
Ahn, Y. H., and Choi, J. (2015). Factors affecting Korean nursing student empowerment in clinical practice. Nurse Educ. Today 35, 1301–1306. doi: 10.1016/j.nedt.2015.08.007
Aiken, L. H., Cheung, R. B., and Olds, D. M. (2009). Education policy initiatives to address the nurse shortage in the United States: in these economic times, it is shortsighted to allow attractive nursing jobs to go vacant when scores of prospective students are being turned away from nursing schools. Health Affairs 28, 646–656. doi: 10.1377/hlthaff.28.4.w646
Aktaş, Y. Y., and Karabulut, N. (2016). A Survey on Turkish nursing students' perception of clinical learning environment and its association with academic motivation and clinical decision making. Nurse Educ. Today 36, 24–128. doi: 10.1016/j.nedt.2015.08.015
Allen, D. (2018). Translational mobilisation theory: A new paradigm for understanding the organizational elements of nursing work. Int. J. Nurs. Stud. 79, 36–42. doi: 10.1016/j.ijnurstu.2017.10.010
Almalkawi, I., Jester, R., and Terry, L. (2018). Exploring mentors' interpretation of terminology and levels of competence when assessing nursing students: an integrative review. Nurse Educ. Today 69, 95–103. doi: 10.1016/j.nedt.2018.07.003
Barnett, T., Namasivayam, P., and Narudin, D. A. A. (2010). A critical review of the nursing shortage in Malaysia. Int. Nurs. Rev. 57, 32–39. doi: 10.1111/j.1466-7657.2009.00784.x
Bengtsson, M., and Ohlsson, B. (2010). The nursing and medical students motivation to attain knowledge. Nurse Educ. Today 30, 150–156. doi: 10.1016/j.nedt.2009.07.005
Bergjan, M., and Hertel, F. (2013). Evaluating students' perception of their clinical placements — Testing the clinical learning environment and supervision and nurse teacher scale (CLES+T scale) in Germany. Nurse Educ. Today 33, 1393–1398. doi: 10.1016/j.nedt.2012.11.002
Bisholt, B., Ohlsson, U., Engström, A. K., Johansson, A. S., and Gustafsson, M. (2014). Nursing students' assessment of the learning environment in different clinical settings. Nurse Educ. Pract.14, 304–310. doi: 10.1016/j.nepr.2013.11.005
Burden, S., Topping, A. E., and O'Halloran, C. (2018). Mentor judgements and decision-making in the assessment of student nurse competence in practice: a mixed-methods study. J. Adv. Nurs. 74, 1078–1089. doi: 10.1111/jan.13508
Chan, D. S. (2003). Validation of the clinical learning environment inventory. West. J. Nurs. Res. 25, 519–532. doi: 10.1177/0193945903253161
Chuan, O. L., and Barnett, T. (2012). Student, tutor and staff nurse perceptions of the clinical learning environment. Nurse Educ. Pract. 12, 192–197. doi: 10.1016/j.nepr.2012.01.003
Claude, R., and Christopher, R. (2014). Acq [Computer Programme], Version 2.1.12. Houston, TX: University of Houston-Downtown.
Cronin, J., and Taylor, S. (1992). Measuring service quality: a reexamination and extension. J. Mark. 56, 55–68. doi: 10.1177/002224299205600304
DeBourgh, G. A. (2012). Synergy for patient safety and quality: academic and service partnerships to promote effective nurse education and clinical practice. J. Prof. Nurs. 28, 48–61. doi: 10.1016/j.profnurs.2011.06.003
Directive 2013/55/EU of the European Parliament of the Council (2013). Official Journal of the European Union no L 354/132. Available online at: http://data.europa.eu/eli/dir/2013/55/oj (accessed November 04, 2020).
Drayton-Brooks, S. M., Gray, P. A., Turner, N. P., and Newland, J. A. (2017). Building clinical education training capacity in nurse practitioner programs. J. Prof. Nurs. 33, 422–428. doi: 10.1016/j.profnurs.2017.02.002
Dunn, S. V., and Burnett, P. (1995). The development of a clinical learning environment scale. J. Adv. Nurs. 22, 1166–1173. doi: 10.1111/j.1365-2648.1995.tb03119.x
El Ansari, W., and Oskrochi, R. (2004). What ≪really≫ affects health professions students' satisfaction with their educational experience? Implications for practice and research. Nurse Educ. Today 24, 644–655. doi: 10.1016/j.nedt.2004.09.002
Eng, S., and Woodside, A. G. (2012). Configural analysis of the drinking man: fuzzy-set qualitative comparative analyses. Addict. Behav. 37, 541–543. doi: 10.1016/j.addbeh.2011.11.034
Falk, T., Hammerschmidt, M., and Schepers, J. J. (2010). The service quality-satisfaction link revisited: exploring asymmetries and dynamics. J. Acad. Mark. Sci. 38, 288–302. doi: 10.1007/s11747-009-0152-2
Fiss, P. C. (2011). Building better causal theories: a fuzzy set approach to typologies in organization research. Acad. Manage. J. 54, 393–420. doi: 10.5465/amj.2011.60263120
García-Álvarez-Coque, J. M., Mas-Verdú, F., and Roig-Tierno, N. (2017). Technological innovation versus non-technological innovation: different conditions in different regional contexts? Qual. Quant. 51, 1955–1967. doi: 10.1007/s11135-016-0394-2
García-Pascual, F., Prado-Gascó, V., Alguacil, M., Valantine, I., and Calabuig-Moreno, F. (2020). Future intentions of fitness center customers: effect of emotions, perceived well-being and management variables. Front. Psychol. 11:2425. doi: 10.3389/fpsyg.2020.547846
Glynn, D. M., McVey, C., Wendt, J., and Russell, B. (2017). Dedicated educational nursing unit: clinical instructors role perceptions and learning needs. J. Prof. Nurs. 33, 108–112. doi: 10.1016/j.profnurs.2016.08.005
Granero-Lazaro, A., Blanch-Ribas, J. M., Roldán-Merino, J. F., Torralbas-mOrtega, J., and Escayola-Maranges, A. M. (2017). Crisis in the health sector: Impact on nurses? Working conditions. Enferm. Clin. 27, 163–171. doi: 10.1016/j.enfcle.2017.03.004
Greckhamer, T., Furnari, S., Fiss, P. C., and Aguilera, R. V. (2018). Studying configurations with qualitative comparative analysis: best practices in strategy and organization research. Strateg. Organ 16, 482–495. doi: 10.1177/1476127018786487
Green, D. (1994). What Is Quality in Higher Education? London: Society for Research into Higher Education, Ltd.
Haraldseid, C., Friberg, F., and Aase, K. (2015). Nursing students' perceptions of factors influencing their learning environment in a clinical skills laboratory: a qualitative study. Nurse Educ. Today 35, e1–e6. doi: 10.1016/j.nedt.2015.03.015
Harvey, T., Calleja, P., and Thi, D. P. (2013). Improving access to quality clinical nurse teaching—A partnership between Australia and Vietnam. Nurse Educ. Today 33, 671–676. doi: 10.1016/j.nedt.2012.02.001
Hayes, L. J., O'Brien-Pallas, L., Duffield, C., Shamian, J., Buchan, J., Hughes, F., et al. (2006). Nurse turnover: a literature review. Int. J. Nurs. Stud. 43, 237–263. doi: 10.1016/j.ijnurstu.2005.02.007
Jack, K., Hamshire, C., Harris, W. E., Langan, M., Barrett, N., and Wibberley, C. (2018). “My mentor didn't speak to me for the first four weeks”: perceived unfairness experienced by nursing students in clinical practice settings. J. Clin. Nurs. 27, 929–938. doi: 10.1111/jocn.14015
Jeffries, P. R., Rose, L., Belcher, A. E., Dang, D., Hochuli, J. F., Fleischmann, D., et al. (2013). A clinical academic practice partnership: a clinical education redesign. J. Prof. Nurs. 29, 128–136. doi: 10.1016/j.profnurs.2012.04.013
Kristofferzon, M., Mårtensson, G., Mamhidir, A., and Löfmark, A. (2013). Nursing students' perceptions of clinical supervision: The contributions of preceptors, head preceptors and clinical lecturers. Nurse Educ. Today 33, 1252–1257. doi: 10.1016/j.nedt.2012.08.017
Lamont, S., Brunero, S., and Woods, K. P. (2015). Satisfaction with clinical placement – The perspective of nursing students from multiple universities. Collegian 22, 125–133. doi: 10.1016/j.colegn.2013.12.005
Lekan, D. A., Corazzini, K. N., Gilliss, C. L., and Bailey, D. E. (2011). Clinical leadership development in accelerated baccalaureate nursing students: an education innovation. J. Prof. Nurs. 27, 202–214. doi: 10.1016/j.profnurs.2011.03.002
Lewallen, L. P., and DeBrew, J. K. (2012). Successful and unsuccessful clinical nursing students. J. Nurs. Educ. 51, 389–395. doi: 10.3928/01484834-20120427-01
Limoges, J., and Jagos, K. (2015). The influences of nursing education on the socialization and professional working relationships of Canadian practical and degree nursing students: a critical analysis. Nurse Educ. Today 35, 1023–1027. doi: 10.1016/j.nedt.2015.07.018
Löfmark, A., Thorkildsen, K., Råholm, M. B., and Natvig, G. K. (2012). Nursing students' satisfaction with supervision from preceptors and teachers during clinical practice. Nurse Educ. Pract. 12, 164–169. doi: 10.1016/j.nepr.2011.12.005
Ma, A. X., Quinn Griffin, M. T., Capitulo, K. L., and Fitzpatrick, J. J. (2010). Demands of immigration among Chinese immigrant nurses. Int. J. Nurs. Pract. 16, 443–453. doi: 10.1111/j.1440-172X.2010.01868.x
McInnes, S., Peters, K., Hardy, J., and Halcomb, E. (2015). Clinical placements in Australian general practice: (Part 1) the experiences of pre-registration nursing students. Nurse Educ. Pract. 15, 437–442. doi: 10.1016/j.nepr.2015.04.003
McSharry, E., and Lathlean, J. (2017). Clinical teaching and learning within a preceptorship model in an acute care hospital in Ireland; a qualitative study. Nurse Educ. Today 51, 73–80. doi: 10.1016/j.nedt.2017.01.007
Milton-Wildey, K., Kenny, P., Parmenter, G., and Hall, J. (2014). Educational preparation for clinical nursing: the satisfaction of students and new graduates from two Australian universities. Nurse Educ. Today 34, 648–654. doi: 10.1016/j.nedt.2013.07.004
Moreno, F. C., Prado-Gasco, V., Hervas, J. C., Nunez-Pomar, J., and Sanz, V. A. (2015). Spectator emotions: effects on quality, satisfaction, value, and future intentions. J. Bus. Res. 68, 1445–1449. doi: 10.1016/j.jbusres.2015.01.031
Mulready-Shick, J., and Flanagan, K. (2014). Building the evidence for dedicated education unit sustainability and partnership success. Nurs. Educ. Perspect. 35, 287–293. doi: 10.5480/14-1379
Navarro, N. (2009). Diseño y validación de un instrumento de evaluación clínica (Design and validation of a clinical evaluation instrument). Rev. Educ. Ciencias Salud 6, 79–86.
Nishioka, V., Coe, M., Hanita, M., and Moscato, S. (2014). Dedicated education unit: nurse perspectives on their clinical teaching role. Nurs. Educ. Perspect. 35, 294–300. doi: 10.5480/14-1381
O'Brien, A., Giles, M., Dempsey, S., Lynne, S., McGregor, M. E., Kable, A., et al. (2014). Evaluating the preceptor role for pre-registration nursing and midwifery student clinical education. Nurse Educ. Today 34, 19–24. doi: 10.1016/j.nedt.2013.03.015
O'Brien, A. T., Mcneil, K., and Dawson, A. (2019). The student experience of clinical supervision across health disciplines–Perspectives and remedies to enhance clinical placement. Nurse Educ. Pract. 34, 48–55. doi: 10.1016/j.nepr.2018.11.006
Oldfield, B. M., and Baron, S. (2000). Student perceptions of service quality in a UK university business and management faculty. Qual. Assur. Educ. 8, 85–95. doi: 10.1108/09684880010325600
Olorunniwo, F., Hsu, M. K., and Udo, G. J. (2006). Service Quality, customer satisfaction, and behavioral intentions in the service factory. J. Serv. Mark. 20, 59–72. doi: 10.1108/08876040610646581
Papathanasiou, I. V., Tsaras, K., and Sarafis, P. (2014). Views and perceptions of nursing students on their clinical learning environment: teaching and learning. Nurse Educ. Today 34, 57–60. doi: 10.1016/j.nedt.2013.02.007
Parasuraman, A., Zeithalm, V., and Berry, L. (1985). A Conceptual model of service quality and its implications for future research. J. Mark. 49, 41–50. doi: 10.1177/002224298504900403
Parasuraman, A., Zeithalm, V., and Berry, L. (1988). SERVQUAL: a multiple-item scale for measuring consumer perceptions of service quality. J. Retail. 64, 12–40.
Payne, C. (2016). Transitions into practice: first patient care experiences of baccalaureate nursing students. Nurse Educ. Today 16, 251–257. doi: 10.1016/j.nepr.2015.09.011
Perry, C., Henderson, A., and Grealish, L. (2018). The behaviours of nurses that increase student accountability for learning in clinical practice: an integrative review. Nurse Educ. Today 65, 177–186. doi: 10.1016/j.nedt.2018.02.029
Pimparyon, S. M., Caleer, S., Pemba, S., and Roff, P. (2000). Educational environment, student approaches to learning and academic achievement in a Thai nursing school. Med. Teach. 22, 359–364. doi: 10.1080/014215900409456
Pitkänen, S., Kääriäinen, M., Oikarainen, A., Tuomikoski, A., Elo, S., Ruotsalainen, H., et al. (2018). Healthcare students' evaluation of the clinical learning environment and supervision – a cross-sectional study. Nurse Educ. Today 62, 143–149. doi: 10.1016/j.nedt.2018.01.005
Pramila-Savukoski, S., Juntunen, J., Tuomikoski, A. M., Käriäinen, M., Tomietto, M., Kaučič, B. M., et al. (2020). Mentors' self-assessed competence in mentoring nursing students in clinical practice: a systematic review of quantitative studies. J. Clin. Nurs. 29, 684–705. doi: 10.1111/jocn.15127
Pucciarelli, F., and Kaplan, A. (2016). Competition and strategy in higher education: managing complexity and uncertainty. Bus. Horiz. 59, 311–320. doi: 10.1016/j.bushor.2016.01.003
Ragin, C. C. (2008). Redesigning Social Inquiry: Fuzzy Sets and Beyond. Chicago: The University of Chicago Press.
Ragin, C. C. (2014). The Comparative Method: Moving Beyond Qualitative and Quantitative Strategies. Berkeley, CA: University of California Press.
Rauyruen, P., and Miller, K. E. (2007). Relationship quality as a predictor of B2B customer loyalty. J. Bus. Res. 60, 21–31. doi: 10.1016/j.jbusres.2005.11.006
Saarikoski, M., Isoaho, H., Warne, T., and Leino-Kilpi, H. (2008). The nurse teacher in clinical practice: developing the new sub-dimension to the clinical learning environment and supervision (CLES) scale. Int. J. Nurs. Stud. 45, 1233–1237. doi: 10.1016/j.ijnurstu.2007.07.009
Saarikoski, M., and Leino-Kilpi, H. (2002). The clinical learning environment and supervision by staff nurses: developing the instrument. Int. J. Nurs. Stud. 39, 259-267. doi: 10.1016/S0020-7489(01)00031-1
Salamonson, Y., Everett, B., Halcomb, E., Hutchinson, M., Jackson, D., Mannix, J., et al. (2015). Unravelling the complexities of nursing students' feedback on the clinical learning environment: a mixed methods approach. Nurse Educ. Today 35, 206–211. doi: 10.1016/j.nedt.2014.08.005
Sandvik, A., Eriksson, K., and Hilli, Y. (2014). Becoming a caring nurse –A Nordic study on students' learning and development in clinical education. Nurse Educ Pract. 14, 286–292. doi: 10.1016/j.nepr.2013.11.001
Slaughter-Smith, C., Helms, J. E., and Burris, R. (2012). Nursing staff perceptions of student contributions in clinical settings. J. Nurs. Educ. 51, 54–57. doi: 10.3928/01484834-20111130-02
Sundler, A. J., Björk, M., Bisholt, B., Ohlsson, U., Engström, A. K., and Gustafsson, M. (2014). Student nurses' experiences of the clinical learning environment in relation to the organization of supervision: a questionnaire survey. Nurse Educ. Today 34, 661–666. doi: 10.1016/j.nedt.2013.06.023
Takashima, M., Burmeister, E., Ossenberg, C., and Henderson, A. (2019). Assessment of the clinical performance of nursing students in the workplace: exploring the role of benchmarking using the Australian Nursing Standards Assessment Tool (ANSAT). Collegian 26, 502–506. doi: 10.1016/j.colegn.2019.01.005
Tuomikoski, A., Ruotsalainen, H., Mikkonen, K., and Kääriäinen, M. (2019). Nurses' experiences of their competence at mentoring nursing students: a systematic review of qualitative studies. Nurse Educ. Today 85:104258. doi: 10.1016/j.nedt.2019.104258
Vis, B. (2012). The Comparative advantages of fsQCA and regression analysis for moderately Large-N analyses. Sociol. Methodol. 41, 168–198. doi: 10.1177/0049124112442142
Vizcaya-Moreno, M. F., Pérez-Cañaveras, R. M., De Juan, J., and Saarikoski, M. (2015). Development and psychometric testing of the clinical learning environment, supervision and nurse teacher evaluation scale (CLES+ T): the Spanish version. Int. J. Nurs. Stud. 52, 361–367. doi: 10.1016/j.ijnurstu.2014.08.008
Vizcaya-Moreno, M. F., Pérez-Cañaveras, R. M., Jiménez-Ruiz, I., and de Juan, J. (2018). Student nurse perceptions of supervision and clinical learning environment: a phenomenological research study. Enfermeria Glob. 17, 319–331. doi: 10.6018/eglobal.17.3.276101
Wafaa-Gameel, A., EL-Banan, S. H. A., and Al-Seraty, W. H. (2015). Effective clinical learning environment as perceived by nursing students at AL dawadmi, applied medical sciences college: actual versus preferred characteristics. Int. J. Nurs. Educ. 5, 1–6. doi: 10.15520/ijnd.2015.vol5.iss05.94.01-06
Ward, A. E., and McComb, S. A. (2018). Formalising the precepting process: a concept analysis of preceptorship. J. Clin. Nurs. 27, 873–881. doi: 10.1111/jocn.14203
Woodside, A. G. (2013). Moving beyond multiple regression analysis to algorithms: calling for adoption of a paradigm shift from symmetric to asymmetric thinking in data analysis and crafting theory. J. Bus. Res. 66, 463–472. doi: 10.1016/j.jbusres.2012.12.021
World Health Organization (2020). State of the World's Nursing 2020: Investing in Education, Jobs and Leadership. Licence: CC BY-NC-SA 3.0 IG. Retrieved from: http://apps.who.int/iris (accessed November 02, 2020).
World Medical Association (2013). “Ethical principles for medical research involving human subjects,” in 64th WMA General Assembly October 2013, Fortaleza, Brazil.
Zamanzadeh, V., Jasemi, M., Valizadeh, L., Keogh, B., and Taleghani, F. (2015). Lack of preparation: Iranian nurses' experiences during transition from college to clinical practice. J. Prof. Nurs. 31, 365–373. doi: 10.1016/j.profnurs.2015.01.005
Zeithaml, V. A., Berry, L. L., and Parasuraman, A. (1993). The nature and determinants of customer expectations of service. J. Acad. Mark. Sci. 21, 1–12. doi: 10.1177/0092070393211001
Keywords: clinical practice, evaluation, graduate education, nursing, student experience, satisfaction
Citation: Fernández-García D, Giménez-Espert MDC, Castellano-Rioja E and Prado-Gascó V (2020) What Academic Factors Influence Satisfaction With Clinical Practice in Nursing Students? Regressions vs. fsQCA. Front. Psychol. 11:585826. doi: 10.3389/fpsyg.2020.585826
Received: 21 July 2020; Accepted: 24 November 2020;
Published: 18 December 2020.
Edited by:
Edward J. N. Stupple, University of Derby, United KingdomReviewed by:
Norat Roig-Tierno, ESIC Business & Marketing School, SpainCopyright © 2020 Fernández-García, Giménez-Espert, Castellano-Rioja and Prado-Gascó. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: María Del Carmen Giménez-Espert, bWFyaWEuYy5naW1lbmV6QHV2LmVz
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.