 Liesbeth Bosgraaf
Liesbeth Bosgraaf Marinus Spreen
Marinus Spreen Kim Pattiselanno
Kim Pattiselanno Susan van Hooren
Susan van Hooren- 1Faculty of Healthcare and Social Work, NHL Stenden University of Applied Sciences, Leeuwarden, Netherlands
- 2Alliade, Care Group, Heerenveen, Netherlands
- 3KenVaK, Research Center for Arts Therapies, Heerlen, Netherlands
- 4Faculty of Psychology, Open University, Heerlen, Netherlands
- 5Faculty of Healthcare, Zuyd University of Applied Sciences, Heerlen, Netherlands
Background: Art therapy (AT) is frequently offered to children and adolescents with psychosocial problems. AT is an experiential form of treatment in which the use of art materials, the process of creation in the presence and guidance of an art therapist, and the resulting artwork are assumed to contribute to the reduction of psychosocial problems. Although previous research reports positive effects, there is a lack of knowledge on which (combination of) art therapeutic components contribute to the reduction of psychosocial problems in children and adolescents.
Method: A systematic narrative review was conducted to give an overview of AT interventions for children and adolescents with psychosocial problems. Fourteen databases and four electronic journals up to January 2020 were systematically searched. The applied means and forms of expression, therapist behavior, supposed mechanisms of change, and effects were extracted and coded.
Results: Thirty-seven studies out of 1,299 studies met the inclusion criteria. This concerned 16 randomized controlled trials, eight controlled trials, and 13 single-group pre–post design studies. AT interventions for children and adolescents are characterized by a variety of materials/techniques, forms of structure such as giving topics or assignments, and the use of language. Three forms of therapist behavior were seen: non-directive, directive, and eclectic. All three forms of therapist behavior, in combination with a variety of means and forms of expression, showed significant effects on psychosocial problems.
Conclusions: The results showed that the use of means and forms of expression and therapist behavior is applied flexibly. This suggests the responsiveness of AT, in which means and forms of expression and therapist behavior are applied to respond to the client's needs and circumstances, thereby giving positive results for psychosocial outcomes. For future studies, presenting detailed information on the potential beneficial effects of used therapeutic perspectives, means, art techniques, and therapist behavior is recommended to get a better insight into (un)successful art therapeutic elements.
Introduction
Psychosocial problems are highly prevalent among children and adolescents with an estimated prevalence of 10%−20% worldwide (Kieling et al., 2011; World Health Organization, 2018). These problems can severely interfere with everyday functioning (Bhosale et al., 2015; Veldman et al., 2015) and increase the risk of poorer performance at school (Veldman et al., 2015). The term psychosocial problems is used to emphasize the close connection between psychological aspects of the human experience and the wider social experience (Soliman et al., 2020) and cover a wide range of problems, namely, emotional, behavioral, and social. Emotional problems are often referred to as internalizing problems, such as anxiety, depressive feelings, withdrawn behavior, and psychosomatic complaints. Behavioral problems are often considered as externalizing problems, such as hyperactivity, aggressive behavior, and conduct problems. Social problems are problems related to the ability of the child to initiate and maintain social contacts and interactions with others. Often, emotional, behavioral, and social problems occur jointly (Vogels, 2008; Jaspers et al., 2012; Ogundele, 2018). The etiology of psychosocial problems is complex and varies with regard to the problem(s) and/or the specific individual. A number of theories seek to explain the etiology of psychosocial problems. The most common theory in Western psychology and psychiatry is the biopsychosocial theory, which assumes that a combination of genetic predisposition and environmental stressors triggers the onset of psychosocial problems (Lehman et al., 2017). But also, attachment theories get renewed attention (Duschinsky et al., 2015). These theories focus on the role of the early caregiver–child relationships and assume that (a lack of) security of attachment affects the child's self-(emotion)regulatory capacity and therefore his or her emotional, behavioral, and social competence (Veríssimo et al., 2014; Brumariu, 2015; Groh et al., 2016). Research has identified a number of biological, psychological, and environmental factors that contribute to the development or progression of psychosocial problems (Arango et al., 2018), namely, trauma, adverse childhood experiences, genetic predisposition, and temperament (Boursnell, 2011; Sellers et al., 2013; Wright and Simms, 2015; Patrick et al., 2019).
Psychosocial problems in children and adolescents are a considerable expense to society and an important reason for using health care. But, most of all, psychosocial problems can have a major impact on the future of the child's life (Smith and Smith, 2010). Effective interventions for children and adolescents, aiming at psychosocial problems, could prevent or reduce the likelihood of long-term impairment and, therefore, the burden of mental health disorders on individuals and their families and the costs to health systems and communities (Cho and Shin, 2013).
The most common treatments of psychosocial problems in children and adolescents include combinations of child- and family-focused psychological strategies, including cognitive behavioral therapy (CBT) and social communication enhancement techniques and parenting skills training (Ogundele, 2018). These interventions are designed with the idea that cognitions affect the way that children and adolescents feel and behave (Fenn and Byrne, 2013). However, this starting point is considered not suitable for all youngsters, in particular, for children and adolescents who may find it difficult to formulate or express their experiences and feelings (Scheeringa et al., 2007; Teel, 2007). For such situations in clinical practice, additional therapies are often offered. Art therapy (AT) is such a form of therapy.
AT is an experiential form of treatment and has a special position in the treatment of children and adolescents because it is an easily accessible and non-threatening form of treatment. Traditionally, AT is (among others) used to improve self-esteem and self-awareness, cultivate emotional resilience, enhance social skills, and reduce distress (American Art Therapy Association, 2017), and research has increasingly identified factors, such as emotion regulation (Gratz et al., 2012) and self-esteem (Baumeister et al., 2003) as mechanisms underlying multiple forms of psychosocial problems.
Art therapists work from different orientations and theories, such as psychodynamic; humanistic (phenomenological, gestalt, person-centered); psychoeducational (behavioral, cognitive–behavioral, developmental); systemic (family and group therapy); as well as integrative and eclectic approaches. But also, there are various variations in individual preference and orientation by art therapists (Van Lith, 2016). In AT, the art therapist may facilitate positive change in psychosocial problems through both engagement with the therapist and art materials in a playful and safe environment. Fundamental principles in AT for children and adolescents are that visual image-making is an important aspect of the natural learning process and that the children and adolescents, in the presence of the art therapist, can get in touch with feelings that otherwise cannot easily be expressed in words (Waller, 2006). The ability to express themselves and practice skills can give a sense of control and self-efficacy and promotes self-discovery. It, therefore, may provide a way for children and clinicians to address psychosocial problems in another way than other types of therapy (Dye, 2018).
Substantial clinical research concerning the mechanisms of change in AT is lacking (Gerge et al., 2019), although it is an emerging field (Carolan and Backos, 2017). AT supposed mechanisms of change can be divided into working mechanisms specific for AT and overall psychotherapeutic mechanisms of change, such as the therapeutic relationship between client and therapist or the expectations or hope (Cuijpers et al., 2019). Specific mechanisms of change for AT include, for instance, the assumption that art can be an effective system for the communication of implicit information (Gerge, and Pedersen, 2017) or that art-making consists of creation, observation, reflecting, and meaning-making, which leads to change and insight (Malchiodi, 2007).
Recently, it has been shown that AT results in beneficial outcomes for children and adolescents. Cohen-Yatziv and Regev (2019) published a review on AT for children and adolescents and found positive effects in children with trauma or medical conditions, in juvenile offenders, and in children in special education and with disabilities. While increasing insight into the effects of AT for different problem areas among children is collected, it remains unclear whether specific elements of AT interventions and mechanisms of change may be responsible for these effects. In clinical practice, art therapists base their therapy on rich experiential and intuitive knowledge. This knowledge is often implicit and difficult to verbalize, also known as tacit knowledge (Petri et al., 2020). Often, it is based on beliefs or common sense approaches, without a sound basis in empirical results (Haeyen et al., 2017). This intuitive knowledge and beliefs consist of (theoretical) principles, art therapeutic means and forms of expression, and therapist behavior [including interactions with the client(s) and handling of materials] that art therapists judge necessary to produce desired outcomes (Schweizer et al., 2014). Identifying the elements that support positive outcomes improves the interpretation and understanding of outcomes, provides clues which elements to use in clinical practice, and will give a sound base for initiating more empirical research on AT (Fixsen et al., 2005). The aim of this review is to provide an overview of the specific elements of art therapeutic interventions that were shown to be effective in reducing psychosocial problems in children and adolescents. In this review, we will focus on applied means and forms, therapist behavior, supposed mechanisms of change of art therapeutic interventions. As the research question was stated, i.e., which art therapeutic elements support positive outcomes in psychosocial problems of children and adolescents (4–20)?
Methods
Study Design
A systematic narrative review is performed according to the guidelines of the Cochrane Collaboration for study identification, selection, data extraction, and quality appraisal. Data analysis was performed, conforming narrative syntheses.
Eligibility Criteria
In this review, we included peer-reviewed published randomized controlled trials (RCTs), non-randomized clinical controlled trials (CCTs), and studies with group pre–posttest designs for AT of psychosocial problems in children and adolescents (4–20 years). Studies were included regardless of whether AT was present within the experimental or control condition. Qualitative data were included when data analysis methods specific for this kind of data were used. Only publications in English, Dutch, or German were included. Furthermore, only studies in which AT was provided by a certified art therapist to individuals or groups, without limitations on duration and number of sessions, were inserted. Excluded were studies in which AT was structurally combined with another non-verbal therapy, for instance, music therapy. Studies on (sand)play therapy were also excluded. Concerning the outcome, studies needed to evaluate AT interventions on psychosocial problems. Psychosocial problems were broadly defined as emotional, behavioral, and social problems. Considered emotional (internalizing) problems were, for instance, anxiety, withdrawal, depressive feelings, psychosomatic complaints, and posttraumatic stress problems/disorder. Externalizing problems were, for instance, aggressiveness, restlessness, delinquency, and attention/hyperactivity problems. Social problems were problems that the child has in making and maintaining contact with others. Also included were studies that evaluated AT interventions targeted at children/adolescents with psychosocial problems and showed results on supposed underlying mechanisms such as, for instance, self-esteem and emotion regulation.
Searches
Fourteen databases and four electronic journals were searched: PUBMED, Embase (Ovid), PsycINFO (EBSCO), The Cochrane Library (Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials), Web of Science, Cinahl, Embase, Eric, Academic Search Premier, Google Scholar, Merkurstab, ArtheData, Relief, and Tijdschrift Voor Vaktherapie (Journal of Arts Therapies in the Netherlands). A search strategy was developed using keywords (art therapy in combination with a variety of terms regarding psychosocial problems) for the electronic databases according to their specific subject headings or structure. For each database, search terms were adapted according to the search capabilities of that database (Appendix 1). The search period had no limitation until the actual first search date: October 5, 2018. The search was repeated on January 30, 2020. If online versions of articles could not be traced, the authors were contacted with a request to send the article to the first author. The reference lists of systematic reviews, found in the search, were hand searched for supplementing titles to ensure that all possible eligible studies would be detected.
Study Selection
A single RefWorks file of all identified references was produced. Duplicates were removed. The following selection procedure was independent of each other carried out by four researchers (LB, SvH, MS, and KP). Titles and abstracts were screened for eligibility by three researchers (LB, SvH, and KP). The full texts were subsequently assessed by three researchers (LB, MS, and KP) according to the eligibility criteria. Any disagreement in study selection between a pair of reviewers was resolved through discussion or by consultation of the fourth reviewer (SvH).
Quality of the Studies
The quality of the studies was assessed by two researchers (LB and KP) applying the EPHPP “Quality Assessment Tool for Quantitative Studies” (Thomas et al., 2004). Independent of each other, they came to an opinion, after which consultation took place to reach an agreement. To assess the quality, the Quality Assessment Tool was used, which has eight categories: selection bias, study design, confounders, blinding, data collection methods, withdrawal and dropouts, intervention integrity, and analysis. Once the assessment was completed, each examined study received a mark ranging between “strong,” “moderate,” and “weak.” The EPHPP tool has a solid methodological rating (Thomas et al., 2004).
Data Collection and Analysis
The following data were collected from the included studies: continent/country, type of publication of study, year of publication, language, impact factor of the journal published, study design, the primary outcome, measures, setting, type of clients, comorbidity, physical problems, total N, experimental N, control N, proportion male, mean age, age range, the content of the intervention, content control, co-intervention, theoretical framework AT, other theoretical frameworks, number of sessions, frequency sessions, length sessions, outcome domains and outcome measures, time points, outcomes, and statistics. An inductive content analysis (Erlingsson and Brysiewicz, 2017) was conducted on the characteristics of the employed ATs concerning the means and forms of expression, the associated therapist behavior, the described mechanisms of change, and whether there were significant effects of the AT interventions. A narrative analysis was performed.
Results
Study Selection
The first search (October 2018) yielded 1,285 unique studies. In January 2020, the search was repeated, resulting in 14 additional unique studies, making a total of 1,299. Four additional studies identified from manually searching the reference lists from 30 reviews were added, making a total of 1,303 studies screened on title and abstract. In the first search, 1,085 studies, and in the second search, nine studies were excluded, making a total of 1,094 studies being excluded on title and abstract. This resulted in 209 full-text articles to assess eligibility. In the full-text selection phase, from the first search, another 167 studies were excluded; in the second search, five studies were excluded. This makes a total of 172 studies being excluded in the full-text phase. Twenty-three studies were excluded because a full text was unavailable; five studies because the language was not English, Dutch, or German; 99 studies did not meet the AT definition; 16 studies had a wrong design; 10 studies did not treat psychosocial problems; and 19 studies concerned a wrong population. In total, 37 studies were included (see Figure 1 for an overview of the complete selection process).
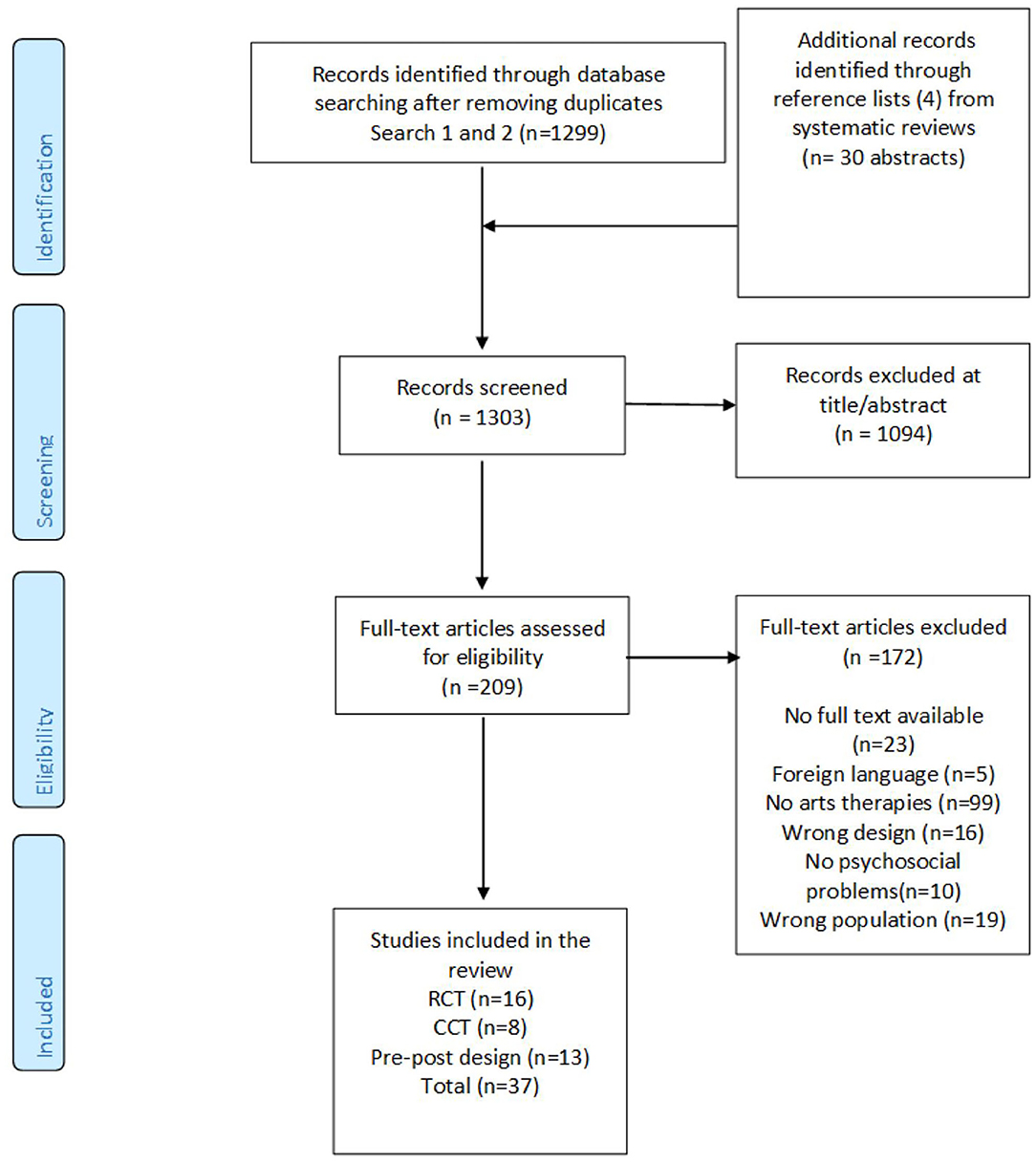
Figure 1. PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow chart.
Study Design
The final review included 16 RCTs, eight CCTs, and 13 single-group pre–post designs (total n = 37). Of the RCTs, a mixed-method design, involving both quantitative and qualitative data, was used in two studies. In one RCT, the control group received AT meeting our criteria, while the experimental group did not receive such a therapy (11). In another RCT, the experimental and the control group both received AT meeting our criteria (13). Also, two CCT studies used a mixed-method design, but these qualitative results were not included due to inappropriate analysis. Of the single-group pre–posttest designs, two studies had a mixed-method (quantitative and qualitative) design (Table 1).
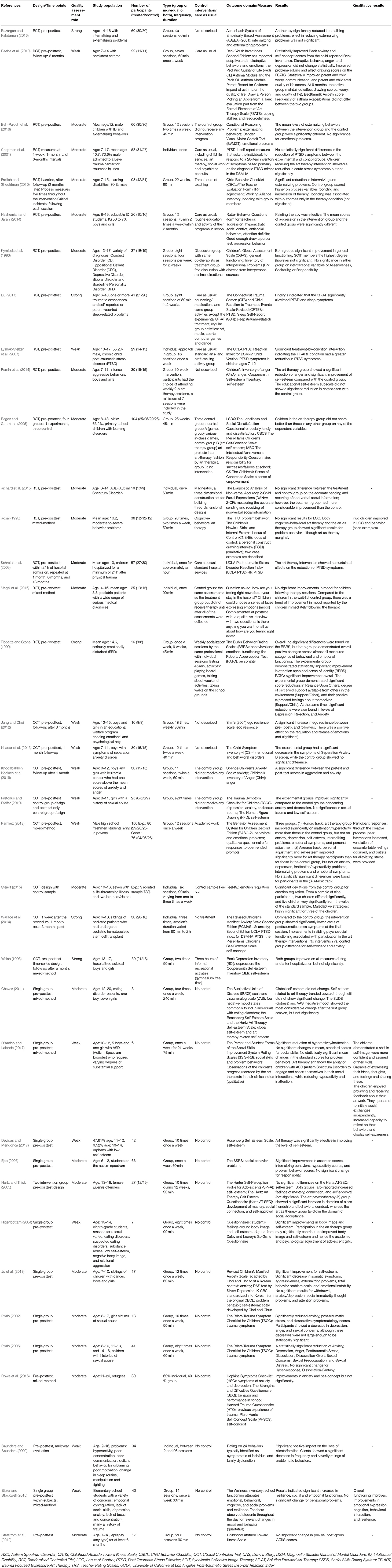
Table 1. Study characteristics/outcome.
Quality of the Studies
Of the 16 RCTs, two studies were evaluated as weak, 11 studies received a moderate score, and three studies were labeled as strong. Concerning the CCTs, five studies were evaluated as weak, one study as moderate, and two studies as strong. Of the 13 pre–posttest designs, five studies were assessed as weak and eight studies as moderate (Table 1).
Study Population
The studies in this review included children and adolescents (ages 2–20) with a wide range of psychosocial problems and diagnoses. Most of the studies included children from the age of 6 years onward, with children's groups ranging from 6 to 15, adolescent groups ranging from 11 to 20, and mixed groups with an age range of 6–20 years. In 13 studies, both boys and girls were included, three studies only included boys, three studies only included girls, and 18 studies did not report the gender of the participants. Psychiatric diagnoses were reported, such as depression, autism spectrum disorder (ASD), conduct disorder (CD), post-traumatic stress disorder (PTSD), and mild intellectual disability (MID). However, also more specific problems were reported, such as children with suicidal thoughts and behavior, children having a brother/sister with a life-threatening disease, boys and girls in an educational welfare program needing emotional and psychological help, and orphans with a low self-esteem. Another group of children that were reported had medical concerns, such as persistent asthma, traumatic injuries, or serious medical diagnoses such as cancer, often combined with anxiety problems and/or trauma-related problems (Table 1).
Number of Participants
The sample sizes of the RCTs ranged from 16 to 109. The total number of children of all RCTs was 707, of which 317 were allocated to an experimental condition and 390 to a control condition (Table 1). The sample sizes of the CCTs ranged from 15 to 780, and the total number of participants was 1,115. The total number of participants who received an AT treatment was 186; the total number of the control groups was 929. Notice that the sample size for the CCTs was influenced by one study in which a control sample database of 780 was used. The sample size of the included pre–posttest designs ranged from 8 to 94 participants, with a total number of 411 participants (Table 1).
Type of Intervention, Frequency, and Treatment Duration
In the 37 studies, a total of 39 AT interventions were studied. In two studies, two AT interventions were studied. Of the 39 interventions, 30 studies evaluated group interventions, seven studies evaluated an individually offered intervention, one study evaluated an individual approach within a group setting, and in one study, the intervention was alternately offered as a group intervention or as an individual intervention. The number of sessions of the AT interventions varied from once to 25 times. The frequency of the AT interventions varied from once a week (n = 14) or twice a week (n = 5) and variations such as four times a week in 2 weeks (n = 1); six sessions were varying from one to three times a week (n = 1), 10 sessions during 12 weeks (n = 1), and eight sessions in 2 weeks (n = 1). The frequency of sessions has not been reported in nine studies. In five studies, the intervention was offered once (Table 1).
Control Interventions
In six RCTs, care, as usual, was given to the control groups. In study four, this also concerned AT, but it was offered in a program that consisted of different forms of treatment as child life services, social work, and psychiatric consults and therefore did not meet our criteria for inclusion. The control groups receiving “care as usual” received routine education and activities of their programs in school (6); counseling/medications and group activities as art, music, sports, computer games, and dance (8); standard arts- and craft-making activities in a group (9); and standard hospital services (14). One study did not specify what happened as care as usual (2). In five RCTs, a specific intervention of activity was offered in the control condition. These control interventions involved 3 h of teaching (5), a discussion group (7), offering play material (magneatos) (12), and a range of games (11), and one study offered weekly socialization sessions, these sessions were offered by the same professionals as the experimental group, and activities were playing board games, talking about weekend activities, and taking walks on the school grounds (16). Two RCT studies did not mention the condition in the control group (1, 10). Two studies mentioned that the control group did not receive any intervention program (3, 11). One study mentioned that the control group had the same assessments as the treatment group but did not receive therapy until all of the assessments were collected (15).
Regarding the eight CCTs, two studies described the control condition in more detail, consisting of academic work (21) or 3 h of informal recreational activities (24). No intervention was offered to the control group in four studies (19, 20, 22, 23). The control intervention was not described within two studies (17, 18) (Table 1).
Applied Means and Forms of Expression
The applied means and forms of expression in the AT interventions could be classified into three categories: art materials/techniques, topics/assignments given, and language as a form of verbal expression accompanying the use of art materials. Results will be shown for 39 AT interventions in total, coming from 37 studies (Table 2). Two studies applied two different types of AT interventions. These two types of AT will be referred to as 13 a/b and 29 a/b.

Table 2. Characteristics AT interventions.
Materials/Techniques
Regarding the category art materials/techniques, three subcategories were found. In the first subcategory, only two-dimensional art media/techniques were used, such as drawing, painting, or printing (the art product possessed length and width, but not depth). Used as materials were for instance, (acrylic) paint, markers, color pencil, crayons, gouache and water, white pieces of paper, cardboard, construction paper with pencils and colored markers, a “sketch” coloring, pencils, markers, and oil pastels (1, 3, 6, 7, 10, 14, 18, 21, 23). No specific art techniques concerning the way the materials were applied were mentioned in this subcategory. In the second subcategory, both two-dimensional and three-dimensional art media and techniques (art that can be defined in three dimensions: height, width, and depth) were offered: clay, papier-mâché masks, paint, paper decoration forms and markers, pictures and journals, paper, cardboard, construction materials, hospital socks, buttons and threads, sewing materials, magic beans, sand, fiberfill, photos, wood, stone, plaster, felt and other textiles, and yarn. In this subcategory, specific art techniques were mentioned, such as paper cutting and paper folding, collage technique, bookmaking, building a face, basket-making, clay techniques, guided fantasy, group painting, story-making through a doll, placing feelings in boxes, drawing/sculpting feelings, making clay shapes, creating self-portraits, and molding clay (2, 5, 8, 11, 13a, 19, 20, 22, 26, 27, 28, 29a, 29b, 30, 31, 32, 33, 36, 37). In the third category, both two-dimensional and three-dimensional art materials/techniques were applied, which matched the specific assignment or topic given (4, 9, 12, 13b, 14, 15, 17, 24, 25). For instance, drawings were made, and the collage technique was used to make a book (9). Four sets of facial features (eyes, noses, mouths, and brows), as well as a mannequin head, were offered for representing facial emotions (12), and in one study, patients used buttons, threads, and sewing materials with which they constructed their Healing Sock Creature, which the children filled with magic beans, sand, or fiberfill (15).
Topics/Assignments
Three subcategories were found concerning the category topics/assignments. The first subcategory, free working with the materials without topics/assignments given, was applied in five AT interventions (3, 5, 11, 13a, 16). In the second subcategory, 26 AT interventions used assignment(s) or gave topics (1, 2, 4, 7, 8, 9, 10, 12, 13b, 14, 15, 17, 19, 20, 21, 22, 23, 24, 25, 27, 29 a/b, 32, 33, 36, 37). The third subcategory concerned combinations of these two. Two studies mixed free working and giving topics/assignments (28, 30), and seven studies did not describe the intervention explicit enough to classify them (6, 18, 26, 31, 34, 35, 36). A wide range of activities based on topics and/or assignments were reported. Eleven categories could be detected; (1) getting familiar with the art material (1, 17) like “learning about art media” (1) and “warm-up clay activities and introduction to theme-related clay techniques” (17); (2) focusing on family perspective, like for instance, “draw first childhood memory/family relations”(1, 23), drawing family as animal (19); (3) working with visualization, fantasy, and meditation (1, 10, 20, 21), such as guided fantasy with clay, and story-making through a doll (20); (4) expressing emotions (1, 14, 19, 20, 23, 32) like “the participant was asked to create four different faces, representing happiness, sadness, anger, and fear” (14) or “make an anger collage” (19); (5) focusing on specific problems such as chronic disease or stress-related events (2, 4, 8, 9, 14, 15, 19, 37) such as “the experience associated with stress is drawn on small white paper and the future solution contents will be drawn on colorful, larger paper” (8) and “drawing feelings, drawing perpetrators, placing of these in boxes” (19); (6) applying group activities (10, 19, 20, 32), for instance, “make a group painting”(20) and “all the children were asked to work on a group project to bring closure by drawing a ceremony on a large paper together with comments” (10); (7) working on an exhibition of artwork (10, 32), for instance, “at the end, a small exhibition of artwork was made” (10); (8) focusing on the material/technique (17, 21, 27, 37) such as “making shapes using clay” (17) and “mold clay into a pleasing form, which could be an animal, a person, an object, or an abstract form” (21); (9) focusing on specific art techniques (19, 21, 29) such as “arrange a variety of objects in a pleasing orientation and draft the still life with a pencil” (21) or “make a photo collage”(19); (10) working with a product/object as a result (24, 25, 27, 32) such as, for instance, “making a bracelet” (32), “making paper bags” (27), or creating therapeutic art books (25); (11) applying general activities (1, 7, 19, 22, 27, 32) like drawing of a picture (7) and “the given theme was heroes”(22). Two studies (13b, 33) gave assignments/topics but did not specify these.
The Role of Language
Three subcategories were found concerning the role of language as a form of verbal expression accompanying the use of art materials and techniques: the produced artwork was mainly discussed afterward in a group meeting or on an individual basis (1, 2, 3, 4, 9, 10, 11, 13b, 14, 17, 29, 36) or feelings and concerns were mainly discussed and reflected on while working (5, 12, 13a, 15, 18, 22, 25, 26, 28) and other varieties such as: the work was (verbally) presented (4) and/or patients also retold the narrative created (5). In one study (7), the originator gave a title, offered associations to it, and said how he/she felt before and after drawing other members gave their associations. In one study (8), all artworks were gathered as a collection and reviewed at the end of the intervention (last session) together with the parents.
Therapist Behavior
Regarding therapist behavior, the information is structured in two categories: the therapist behavior, including social interactions with the client(s), and the handling of materials by the therapist, including material interactions with the client(s).
Therapist Behavior, Including Social Interactions With Their Client(s)
The information revealed three broad behaviors: non-directive behavior, directive behavior, and behavior that can be considered eclectic. Non-directive behavior refers to AT interventions in which the therapists showed mainly a following and facilitating attitude toward the children/adolescents. Thirteen AT interventions applied this kind of therapist behavior (13a, 15, 16, 17, 18, 20, 21, 22, 23, 25, 29a, 30, 36). Interactions with clients were for example, “the therapist was non-interpretive, with the participants creating their direct statements and finding their meanings in the individual artwork they created” (21) and “the therapist facilitates the creation of the artistic product and is supportive” (13a). Directive behavior refers to AT interventions in which the therapist showed an active and leading role toward the children/adolescents. Ten AT interventions (4, 8, 10, 11, 12, 13b, 24, 26, 28, 29b) used this kind of therapist behavior. Interactions with the clients were, for example, “the therapist asks exception/difference questions” (8) or “the participant was directed to choose a mouth, nose, eyes, and brows that represented the correct emotion” (12). A mix of these two types of therapist behaviors (eclectic) was applied in nine AT interventions (2, 5, 7, 9, 14, 32, 33, 34, 35), for instance: “each adolescent was asked at the beginning of the session to do a ‘feelings check-in’ describing how he or she was feeling in the moment and a ‘feelings check-out’ at the end of the session. In the art-making period, a minimal discussion took place” (9) or “art therapists worked with their clients to form therapeutic goals during initial sessions, followed by both structured and unstructured weekly AT sessions” (34). In seven AT interventions (1, 3, 6, 19, 27, 31, 37), insufficient information was given to classify the therapist's behavior.
The Handling of Materials by the Therapist, Including Material Interactions With the Client(s)
Information was provided by seven studies: “the therapist assists and supports the youngster in carrying out the activity” (5), “the therapist embeds solution-focused questions and skills in the art-making process” (8), “during working with materials, there was minimal discussion” (9), “the child was directed to choose features/materials that represented the correct emotion” (12), “the therapist gave delineated verbal instructions and directions for art media” (13a), “the therapist-assisted the child having difficulty with a specific medium” (13b), “the therapist became the co-creator” (15), and “the therapist avoided giving art instructions” (25).
Supposed Mechanisms of Change
In the introduction and discussion sections of the articles, a range of supposed mechanisms of change as substantiation of the intervention and outcomes were described (Table 2). The supposed mechanisms of change could be categorized into two categories: art therapy specific and general psychotherapeutic mechanisms of change.
Specific Mechanisms of Change
Eight subcategories of a specific mechanism of change were detected. The first category was Art therapy as a form of expression to reveal what is inside. This large subcategory, could be divided into three forms: art as a form of visualizing and communication in general (1, 13, 15, 19, 20, 26, 28, 33, 35, 36), such as, “it enables the child to visualize” (15); art as a manageable expression and/or regulation of emotions (1, 2, 3, 7, 8, 10, 19, 20, 23, 27, 28, 31, 33, 35, 37), e.g., “through art emotions can be processed” (2); and art as a way of expression through specific processes (1, 4, 5, 9, 10, 11, 14, 15, 17, 19, 22, 25, 28, 29, 31, 32), for instance, “reduces threat inherent in sharing experiences of trauma by permitting a constructive use of displacement via the production of imagistic representations” (9). The second category was Art therapy as a way of becoming aware of oneself, mentioned by 10 studies (1, 2, 11, 13, 16, 23, 24, 25, 35, 36), for instance, “to regain a sense of personal agency” (1). The third category was defined as art therapy as a way to form a narrative of life, like “facilitation of the integration of the experience into one's larger, autobiographical life narrative” (4), while the fourth category dealt with art therapy as integrative activation of the brain through experience, which was mentioned in six studies (4, 12, 14, 16, 34, 26), for instance, “utilizing the integrative capacity of the brain by accessing the traumatic sensations and memories in a manner that is consistent with the current understanding of the transmission of experience to language”(4). The fifth category art therapy as a form of exploration and/or reflection was mentioned in seven studies (1, 9, 15, 18, 30, 5, 8), for instance, “to explore existential concerns” (1), and the sixth category the specifics of the art materials/techniques offered in art therapy was mentioned in three studies (13, 17, 30), for instance, “because they could change the shape as they wished, which contributed to a positive evaluation of their own performance”(17). The seventh category art therapy as a form to practice and/or learn skills was mentioned in four studies (10, 19, 28, 33), for example, “in art therapy interventions, children can learn coping responses, new skills, or problem-solving techniques” (10). Finally, the eighth category art therapy, as an easily accessible, positive and safe intervention by the use of art materials was mentioned by 15 studies (1, 2, 6, 8, 10, 16, 19, 23, 24, 25, 28, 29, 30, 32, 37), for instance, “non-verbal expression that is possible in art therapy is a safe way”(10).
General Mechanisms of Change
Two subcategories of general mechanisms of change could be defined. The first subcategory was defined as art therapy as a form of group process, mentioned by eight studies (7, 9, 13, 18, 20, 29, 30, 36), for instance, “present thoughts and feelings in a non-verbal way within the structure of the group”(7). The second, the therapeutic alliance in art therapy, was mentioned by six studies (5, 8, 16, 18, 26, 29), for instance, “the primary role of the therapist as listening, accepting, and validating” (16).
Synthesized Findings
Means and Forms of Expression and Therapist Behavior
Concerning the search for similarities and differences, the three found forms of therapist behavior were used to distribute the means and forms, which gave the following results.
The Therapist Behavior Was Non-directive
The therapist showed mainly a following and facilitating attitude toward the children/adolescents; in this category (n = 13), the use of means and forms of expression was variable, but most often, children and adolescents worked on base of topics and assignments with both two- and three-dimensional materials and techniques, while during working, process and product were discussed. Specifically, four AT interventions used only two-dimensional materials/techniques (15, 18, 21, 23), six AT interventions offered both two- and three-dimensional materials/techniques (13a, 20, 22, 29a, 30, 36), and three AT interventions offered materials/techniques fitting the topic/assignment (15, 17, 25), which included a combination of two- and three-dimensional materials/techniques. Three AT interventions let the clients work freely without topics and assignments given (13a, 18, 30), eight AT interventions were based on topics/assignments (15, 20, 21, 22, 23, 25, 29a, 36), and two AT interventions combined both ways (17, 30). Concerning the use of language, in three AT interventions, there was a discussion on process/product afterward (17, 29a, 36), in five AT interventions, there was a verbal exchange while working (13a, 15, 18, 22, 25), and five studies (16, 20, 21, 23, 30) in this category did not make their use of language explicit as an additional form of expression. The most mentioned subcategories of supposed mechanisms of change for this category were “art therapy as a form of expression to reveal what is inside,” “art therapy as a form of exploration,” and “art therapy as a way of experiencing the self.”
The Therapist Behavior Was Directive
The therapist showed mainly an active and leading role toward the children/adolescents; the use of means and forms of expression was again variable in this category (n = 10), but most often, children and adolescents worked on base of topics and assignments with both two- and three-dimensional materials/techniques, whereby the process and work were reflected upon afterward in different forms. Specifically, one intervention used only two-dimensional materials/techniques (10), five AT interventions offered both two- and three-dimensional materials/techniques (8, 11, 26, 28, 29b), and four AT interventions offered materials/techniques fitting the topic/assignment (4, 12, 13b, 24), which included two- and three-dimensional materials/techniques. Two AT interventions let the clients work without topics and assignments given (11, 28), and seven AT interventions were based on topics/assignments (4, 8, 10, 12, 13b, 24, 29b), one AT intervention combined both ways (28), and one study did not provide information on this topic (26). Concerning the use of language, in five AT interventions, there was a discussion on process/product afterward (4, 10, 11, 13b, 29b), in three AT interventions, there was a verbal exchange while working (12, 26, 28), and one study used language in a specific form (reviewing the collection with children and parents) (8). One AT intervention discussed the work afterward in a different form (a narrative retold) (4). One intervention did not make the use of language explicit as an additional form of expression (24). The most-reported subcategories of supposed mechanisms of change were the same as for the non-directive therapist behavior.
The Therapist Both Performed Directive and Non-directive Behavior (Eclectic) Toward Clients
Also, the use of means and forms of expression was variable in this category (n = 9). All kinds of materials/techniques were used but most often were worked on base of topics/assignments. The use of language was not often mentioned, but if it was used, it was used as a discussion afterward. Specifically: two AT interventions used only two-dimensional materials/techniques (7, 14), four AT interventions offered both two- and three-dimensional materials/techniques (2, 5, 32, 33), and two AT interventions offered materials/techniques fitting the topic/assignment (9, 14), which included both two- and three-dimensional materials/techniques. One study did not provide information on this topic (34). In one AT intervention, the clients worked freely without topics and assignments given (14), and six AT interventions were based on topics/assignments (2, 5, 7, 9, 32, 33). Concerning the use of language, in three AT interventions, there was a discussion on process/product afterward (2, 9, 14), no AT interventions mentioned a verbal exchange while working, and four studies (32, 33, 34, 35) in this category did not make their use of language explicit as an additional form of expression. The most-reported subcategories of supposed mechanisms of change for this category were “art therapy as a form of expression to reveal what is inside”; “art therapy as a form of exploration,” and “art therapy as an easily/safe accessible intervention.”
In seven studies (1, 3, 6, 19, 27, 31, 37), the AT interventions were not enough explicated to make combinations.
Outcomes
Therapist Behaviors in Relation to Psychosocial Outcomes
The division into three categories of non-directive, directive, and eclectic therapist behavior gave the opportunity to show outcomes in accordance with these. To structure the outcome, these are reported by categorizing psychosocial problems into internalizing problems, externalizing problems, and social problems and in outcomes that can be considered underlying mechanisms of psychosocial problems. These underlying mechanism outcomes were divided into the domains self-concept/self-esteem and emotion regulation.
Non-directive Therapist Behavior
Eight studies (15, 16, 18, 20, 21, 23, 25, 36), which applied the non-directive therapist behavior, focused on Internalizing Problems as an outcome. These results showed significant improvement in post-traumatic stress symptoms (23); emotional functioning (36, 16), depression, rejection, and anxiety (16), reduction of symptoms of Separation Anxiety Disorder (18), and symptoms of anxiety and depression (20). The quality of two studies (16, 23) was strong, and the other three studies were assessed as being of weak quality. Also, four times no significant improvement was reported for negative mood states (15), negative mood and distress (25), feelings of anxiety (23), and anxiety, depression, internalizing problems, and emotional symptoms (21). The quality of these studies was strong (23) or weak (15, 21, 25).
Five studies (13a, 16, 21, 29, 36) showed results for Externalizing Problems. The results showed significant improvement in inattention/hyperactivity problems for the Honors track group (21) (weak), behavioral conduct (29) (moderate), attention span (16) (strong), and problem behavior (13a) (moderate). However, also, no significant improvement was reported on behavioral problems (36, 16) and inattention/hyperactivity for the Average track group (21).
Four studies (16, 21, 29a, 36) reported results for Social Problems. A significant effect was found on social functioning and resilience (36) (weak), social acceptance (29a) (moderate), personal adjustment (21), and degree of perceived support available from others and reliance upon others (16) (strong). No significant improvement was found for personal adjustment (21). The qualitative data revealed improvement in behavioral and peer interaction (36, 21).
Some studies evaluating interventions with non-directive therapist behavior showed results on outcomes that can be considered underlying mechanisms of psychosocial problems. For the domain Self-concept/Self-esteem, nine studies (13a, 16, 20, 21, 23, 25, 29a, 30, 36) showed results on this domain. They reported significant improvement in self-esteem (21, 30); feelings around body image (30) (weak); self-approval (29a); sense of identity, overall personality, positive feelings about themselves (16); and resilience (36). Also, no significant improvement was shown on this domain, e.g., self-esteem (10, 21, 25, 29a), self-concept (23) (strong), and Locus of Control (13a) (refers to how strongly people believe they have control over the situations and experiences), which was a study of moderate quality. Qualitative results showed improvement in this domain on resilience (13, 36). Two studies reported results on Emotion Regulation. In one study, a significant improvement was seen in emotion regulation and maladaptive strategies (22) (moderate), while in another study, no improvement was found. This study was assessed as being a weak study (17). Qualitative results showed that participants reported that “ventilation of uncomfortable feelings occurred, and an outlet for alleviating stress was provided” (21), and there were improvements in emotional expression and cognition (36).
Directive Therapist Behavior
Four studies that applied the directive therapist behavior (4, 8, 24, 28) showed results for Internalizing Problems. In these studies, there was a significant improvement in internalizing behaviors (28), PTSD, and sleep-related problems (8). The quality of these studies was moderate (28) and strong (8). No significant improvement was reported for mood, depression (24), PTSD, and acute stress (4). The quality of these two studies was strong and moderate.
Four studies (10, 13b, 26, 28) reported results for Externalizing Problems, and significant improvement was found on anger (10), problem behavior (13b), hyperactivity/inattention (26), hyperactivity scores, and problem behavior (28). Also, no significant improvement was reported, specifically on problem behaviors (26). The qualitative results of these AT interventions described improved classroom behavior (13). The quality of these studies was moderate (10, 13, 28) and weak (26).
Four studies (11, 26, 28, 29) reported results for Social Problems. These studies reported significant improvement for close friendship (29) and assertion (28). But in other studies, no significant improvement was reported for social skills (26), socially lonely (11), and responsibility (28). The quality of the studies was assessed as being moderate (11, 29) and weak (26, 28). Qualitative results revealed that “the clients appeared to initiate social exchanges more independently and were improved on sharing feelings, thoughts, and ideas” (26).
Some studies applying directive therapist behavior showed results on (supposed) underlying mechanisms. Five studies (10, 11, 13, 24, 29) showed results on Self-esteem/Self-concept. Significant improvement was found on self-esteem (10) and self-approval (29). Also, no significant improvement was found on self-esteem (29, 24, 11), a sense of empowerment (11), responsibility for success/failure at school (11), Locus of Control (13), and educational self-esteem (10). The quality of the studies was strong (24) and moderate (10, 11, 13, 29). Also, positive qualitative results were reported in this domain, i.e., “a shift in self-image, were more confident and assured of their skills, and were more capable of expressing their ideas, thoughts, and feelings and in sharing these. They also showed an increased capacity to reflect on their behaviors and display self-awareness” (26) and improved Locus of Control (13). One study reported no significant improvement in Emotion Regulation (12). This study was of moderate quality.
Eclectic Therapist Behavior
Seven studies (2, 5, 9, 14, 32, 33, 34) in which interventions with eclectic therapist behavior was applied showed results on Internalizing Problems. Significant improvement was reported on internalizing problems (5), anxiety (2, 32, 33), and parent & child worry (2), depression, dissociation, sexual concerns, sexual preoccupation, and sexual distress (33), dissociative symptomatology (32), and post-traumatic stress (9, 32, 33). However, no significant results were reported on anxiety (34), depression (2, 32), dissociation (fantasy) (33), sexual concerns (32), and PTSD symptoms (14). The quality was assessed as being weak (2, 9) and moderate (14, 32, 33, 34).
Five studies (2, 5, 32, 33, 35) reported on Externalizing Problems, and they reported significant improvement on externalizing problems (5), problematic behaviors (35), and anger (33). No significant improvement was reported for disruptive behavior (2), hyper-response (33), and anger (2, 32). The study quality was weak (2, 35) and moderate (5, 32, 33).
Two studies (2, 7) reported on Social Problems, and significant improvement was found for parent and child communication (2) (weak). No significant improvement was reported on sociability, responsibility, and assertiveness (7).
Within the category eclectic therapist behavior, one study showed results on underlying mechanisms, specifically no significant improvement on Self-concept (34). This study was being assessed with moderate quality.
Overall Results
As is shown in Table 3, more than 50% of the studies on the effects of AT interventions using non-directive therapist behavior showed significant effects on the outcome domains, with high impact on externalizing (80%), social problems (75%), and internalizing problems (62,5%). Self-esteem/self-concept and emotion regulation showed lower figures, with 55.6 and 50%, respectively. AT interventions in which directive therapist behavior was used showed a different picture. The number for treating externalizing problems stood out, with 100% of the studied AT interventions being significantly effective in this domain. However, percentages of significant interventions for internalizing problems, social problems, self-esteem/self-concept were equal to or <50%. AT interventions using eclectic therapist behavior showed best results on internalizing and externalizing problems with, respectively 71.4 and 60% of the AT interventions that were evaluated on these outcome domains.

Table 3. Number and percentage of interventions per type of therapist behavior showing significant effects on outcomes.
Discussion
The purpose of this systematic narrative review was to provide an overview of AT interventions that were effective in reducing psychosocial problems in children and adolescents. The emphasis was on the applied means and forms of expression during AT, the therapeutic behavior applied, and the supposed mechanisms of change to substantiate the use of the intervention. The main results showed that a broad spectrum of art materials and techniques are used in AT treatments for psychosocial problems in children and adolescents. No specific art materials or techniques stood out. Also, forms of structure such as working on the basis of topics or assignments and the way language is applied during or after the sessions vary widely and do not seem to relate to a specific category of therapist behavior. From this point of view, it seems less important which (combination of) materials/techniques and forms of structure art therapists use in treatments of psychosocial problems. The wide variety of materials, techniques, and assignments that are used in AT shows that AT is very responsive to individual cases in their treatments. This is in line with the concept that art therapists can attune to the client's possibilities and needs with art materials/techniques (Franklin, 2010).
Therapist behavior appeared to be the only distinctive component in the interventions. Three broad forms were found: non-directive, directive, and eclectic. In practice, art therapists often define their practice with orientations such as psychodynamic, gestalt, person-centered, etc. or choose an approach according to their individual preferences (Van Lith, 2016). For instance, a stance in which the therapist sees its role as being a witness to the experience of the inherent process of knowing the self (Allen, 2008) is often related to a non-directive therapist behavior or a stance in which they elicit meaning-making by engendering a new perspective (Karkou and Sanderson, 2006) is often related to a form of directive therapist behavior. Also, many art therapists work from the point of view that the art therapist should adapt to the client needs, which can be considered an eclectic approach (Van Lith, 2016) and which incorporates both forms of therapist behavior. Next to individual preferences, many psychotherapeutic approaches are being used in art therapeutic treatments of children and adolescents (Graves-Alcorn and Green, 2014; Frey, 2015; Gardner, 2015; Van Lith, 2016). However, in the end, they all range on a continuum from non-directive to directive therapist behavior (Yasenik and Gardner, 2012).
The results of this review show that AT for children and adolescents with psychosocial problems can lead to improvement in all domains for all three forms of therapist behavior in combination with a variety of means and forms. And, although the focus of this review was less on therapy outcomes, the results confirm the conclusion of Cohen-Yatziv and Regev (2019) that AT for children and adolescents with psychosocial problems can be effective. Non-directive therapist behavior, whereby the therapist is following and facilitating, shows the most significant effects in this study for psychosocial problems, next to eclectic therapist behavior for internalizing and externalizing problems. Also, it was striking that directive therapist behavior was effective for externalizing problems in all studies evaluating interventions with this type of therapist behavior, while this was not the case for the other outcome domains. Children and adolescents with externalizing problems may thus profit from directive, non-directive, and eclectic art therapist behavior. In addition, the findings suggest that we need to carefully consider using directive behavior in children with internalizing or social problems.
To substantiate the use of the AT interventions and the results, a variety of supposed mechanisms of change were described. Both specific and more general mechanisms of change were reported to substantiate AT interventions. The majority concerned specific AT mechanisms of change. Often, AT is considered a form of expression to reveal what is inside or its effects are explained by an exploration of feelings, emotions, and thoughts. These mechanisms of change were seen in AT interventions with non-directive, directive, and eclectic therapist behavior. The simultaneous occurrence of supposed mechanisms of change in all these categories of therapist behavior that differ substantially from one another can be explained by the central use of art materials, which distinguishes AT from the other ATs and from other psychotherapeutic approaches (Malchiodi, 2012). It can be considered as an additional and specific value of AT and, therefore, frequently used as substantiation for the used AT interventions and their effects.
Corresponding between the studies that showed positive results was the adaptation of the materials/techniques, forms of structure, and therapist behavior to the problems and needs of the children and adolescents involved. This process is called responsiveness. Responsiveness consists of interacting in a way such that the other is understood, valued, and supported in fulfilling important personal needs and goals. It can be seen as a moment-by-moment process of the therapeutic alliance between therapist and client (Sousa et al., 2011). Responsiveness supports and strengthens both the relationship and its members (Reis and Clark, 2013). In AT, therapist behavior and the use of materials and techniques can both be adapted to these needs and may be considered an important element in explaining the positive effects of AT. Processes such as responsiveness and therapeutic alliance relate partially to attachment theories. In AT, a therapeutic alliance includes, next to the client and art therapist, a third “object,” the art medium, comprised of art materials, art-making, and artworks (Bat Or, and Zilcha-Mano, 2018). From the perspective of attachment theory, the encounter between client and art material in AT may reflect attachment-related dynamics (Snir et al., 2017). Therefore, art therapists recapitulate positive relational aspects through purposeful creative experiences that offer sensory opportunities to reinforce a secure attachment (Malchiodi and Crenshaw, 2015). In this way, materials and techniques can offer the child and adolescent a “safe bridge” to bond with the therapist and explore and grow in developmental areas that are treated.
Given the results, relational, experiential (combined with art) knowledge to connect to the children's and adolescent's problems and needs seems indispensable for art therapists. This study included AT interventions performed by certified art therapists. Art therapists get a thorough education in relational and experiential (art) skills and obtain tacit knowledge through practice. By having more insight into the importance of the role of therapist behavior and the use of materials/techniques in AT interventions for children and adolescents, art therapists can improve results. Choices for therapist behavior and the use of materials/techniques should not depend that much on context or individual preference but on the client's problems and needs and which therapist behavior fits the client best. The results of this study provide clues on which and how to use AT elements in clinical practice, but above all, it gives a sound base for initiating more empirical research on AT. For practice and research purposes, a thorough elaboration and description of the therapist behavior in manuals are then of importance.
Strengths and Limitations of This Review
In this study, a narrative synthesis was performed because of the focus on substantive aspects and the heterogeneity of the studies. A common criticism of narrative synthesis is that it is difficult to maintain transparency in the interpretation of the data and the development of conclusions. It threatens the value of the synthesis and the extent to which the conclusions are reliable. For instance, in this study, we searched for similarities and differences in two core elements of AT (Schweizer et al., 2014). Sometimes, forced choices had to be made in the division of the defined components into group categories and, eventually, to divide them into categories of therapist behavior. Separating and distinguishing components of an intervention are not straightforward.
From the literature, it is known that studies with positive results are overrepresented in the literature (Mlinarić et al., 2017). Probably also in this study, therefore, publication bias must be taken into account when interpreting the results.
Also, regarding showing significant results, some studies showed significant and no significant results in the same domain. This can cause bias, for example, considering a study to be significantly effective in internalizing problems, but in reality, the study shows significant results in anxiety, but for instance, not in depression. It should be taken into account that, in this study, only a broad overarching view is given.
In this study, we included RCTs, CCTs, and group pre–posttest designs because these three designs (in this order) can be considered to provide the most reliable evidence (Bondemark and Ruf, 2015). Questionable is whether these types of designs are the most appropriate designs for (a part of) the research question posed in this study. For detailed, more qualitative information on interventions, case studies seem very suitable. Potential advantages of a single case study are seen in the detailed description and analysis to gain a better understanding of “how” and “why” things happen (Ridder, 2017).
Recommendations
Remarkably, seven studies did not describe their AT interventions sufficiently explicitly concerning the use of means and forms of expression and therapist behavior. This, while art materials/techniques and therapist behavior constitute the basis for AT interventions (Moon, 2012). Insight into the core elements of interventions helps us better understand why and how certain interventions work. By understanding these components of an intervention, we can compare interventions and improve the effectiveness of interventions (Blase and Fixsen, 2013). Therefore, for future AT studies, it is recommended to present more information on used therapeutic perspectives, means, art materials and techniques, and therapist behavior.
The results of this study show that AT interventions for children and adolescents are characterized by a variety of materials/techniques, forms of structure such as giving topics or assignments, the use of language, and therapist behavior. These results point out to more specific aspects of the dual relationship of material–therapist, which contributes to the effects, such as, for instance, responsiveness. More (qualitative) research into these specific aspects of the therapeutic relationship and the role of the relational aspects of the material could provide more insight and be of great value regarding AT for children and adolescents.
The results of the AT interventions show that AT leads to positive results for psychosocial problems, although, in some studies, both significant and not significant results were seen within a domain. A more personalized research approach, which is linked to individual treatment goals, can possibly give more clarity on the effects. Goal Attainment Scales (GAS) can be considered useful for this purpose.
Conclusions
This study shows that the use of means and forms of expression and therapist behavior is applied flexibly. This suggests a responsiveness of AT, in which means and forms of expression and therapist behavior are applied to respond to the client's needs and circumstances, thereby giving positive (significant) results for psychosocial problems. Searching for specific elements in the use of materials and the three defined forms of therapist behavior that influence the result is therefore recommended.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author Contributions
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
Funding
This research was funded by NHL/Stenden, University of Applied Science in Leeuwarden and Care-group Alliade in Heerenveen, Netherlands.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We would like to thank Mrs. T. van Ittersum of the Research Institute SHARE/Research office UMCG in Groningen for her help with search strategy and data collection.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2020.584685/full#supplementary-material
References
Allen, P. B. (2008). Commentary on community-based art studios: underlying principles. Art Therapy 25, 11–12. doi: 10.1080/07421656.2008.10129350
American Art Therapy Association (2017). Facts, figures and helpful resources from AATA. Avaliable online at: https://multibriefs.com/briefs/aata/review122117.pdf (accessed July 11, 2020).
Arango, C., Díaz-Caneja, C. M., McGorry, P. D., Rapoport, J., Sommer, I. E., Vorstman, J. A., et al. (2018). Preventive strategies for mental health. Lancet Psychiatry 5, 591–604. doi: 10.1016/S2215-0366(18)30057-9
Bat Or, M., and Zilcha-Mano, S. (2018). The Art Therapy Working Alliance Inventory: the development of a measure. International Journal of Art Therapy. 24(2), 76–87. doi: 10.1080/17454832.2018.1518989
Baumeister, R. F., Campbell, J. D., Krueger, J. I., and Vohs, K. D. (2003). Does high self-esteem cause better performance, interpersonal success, happiness, or healthier lifestyles? Psychol. Sci. Public Interest 4, 1–44. doi: 10.1111/1529-1006.01431
Bazargan, Y., and Pakdaman, S. (2016). The effectiveness of art therapy on reducing internalizing and externalizing problems of female adolescents. Arch. Iran. Med. 19, 51–56
Beebe, A., Gelfand, E. W., and Bender, B. (2010). A randomized trial to test the effectiveness of art therapy for children with asthma. J. Allergy Clin. Immunol. 126, 263–266.e1. doi: 10.1016/j.jaci.2010.03.019
Beh-Pajooh, A., Abdollahi, A., and Hosseinian, S. (2018). The effectiveness of painting therapy program for the treatment of externalizing behaviors in children with intellectual disability. Vulnerable Child. Youth Stud. 13, 221–227 doi: 10.1080/17450128.2018.1428779
Bhosale, S. A., Singru, S., and Khismatrao, D. (2015). Study of Psychosocial Problems among adolescent students in Pune, India. Ameen J. Med. Sci. 8, 150–155.
Blase, K., and Fixsen, D. (2013). Core intervention components: Identifying and operationalizing what makes programs work. Washington, DC: Office of the Assistant Secretary for Planning and Evaluation, Office of Human Services Policy, U.S. Department of Health and Human Services.
Bondemark, L., and Ruf, S. (2015). Randomized controlled trial: the gold standard or an unobtainable fallacy? Eur. J. Orthodont. 37, 457–461. doi: 10.1093/ejo/cjv046
Boursnell, M. (2011). Parents with mental illness: the cycle of intergenerational mental illness. Child. Australia 36, 26–35. doi: 10.1375/jcas.36.1.26
Brumariu, L. E. (2015). Parent-child attachment and emotion regulation. New Dir. Child Adolesc. Dev. 2015, 31–45. doi: 10.1002/cad.20098
Carolan, R., and Backos, A. (2017). Emerging Perspectives in Art Therapy: Trends, Movements, and Developments, 1st Edn. New York, NY: Routledge.
Chapman, L., Morabito, D., Ladakakos, C., Schreier, H., and Knudson, M. M. (2001). The effectiveness of art therapy interventions in reducing Post Traumatic Stress Disorder (PTSD) symptoms in pediatric trauma patients. Art Therapy 18, 100–104. doi: 10.1080/07421656.2001.10129750
Chaves, E. (2011). The creation of art books with adolescents diagnosed with an eating disorder: effectiveness, self-esteem, and related factors (Dissertation). Retrieved from: https://digitalcommons.du.edu/etd/122/
Cho, S. M., and Shin, Y. M. (2013). The promotion of mental health and the prevention of mental health problems in child and adolescent. Korean J. Pediatr. 56:459. doi: 10.3345/kjp.2013.56.11.459
Cohen-Yatziv, L., and Regev, D. (2019). The effectiveness and contribution of art therapy work with children in 2018 -what progress has been made so far? A systematic review. Int. J. Art Therapy 24, 100–112. doi: 10.1080/17454832.2019.1574845
Cuijpers, P., Reijnders, M., and Huibers, M. J. H. (2019). The role of common factors in psychotherapy outcomes. Annu. Rev. Clin. Psychol. 15, 207–231. doi: 10.1146/annurev-clinpsy-050718-095424
Daley, J., and Lecroy, C. W. (2001). Empowering Adolescent Girls: Examining the Present and Building Skills for the Future with the “Go Girls” Program (Norton Professional Books (Paperback)). New York, NY: W. W. Norton & Company.
D'Amico, M., and Lalonde, C. (2017). The effectiveness of art therapy for teaching social skills to children with autism spectrum disorder. Art Therapy 34, 176–182. doi: 10.1080/07421656.2017.1384678
Devidas, N. S. A. P., and Mendonca, T. L. (2017). A study to evaluate the effectiveness of art therapy on self esteem among the orphans in selected orphanages at Mangalore. Asian J. Nurs. Educ. Res. 7:376. doi: 10.5958/2349-2996.2017.00075.1
Duschinsky, R., Greco, M., and Solomon, J. (2015). The politics of attachment: lines of flight with bowlby, deleuze and guattari. Theory. Cult. Soc. 32, 173–195. doi: 10.1177/0263276415605577
Dye, M. (2018). Evaluating the benefits of art therapy interventions with grieving children (Ph. D. Thesis). James Madison University, JMU Scholarly Commons. Avaliable online at: https://commons.lib.jmu.edu/edspec201019/129
Epp, K. M. (2008). Outcome-based evaluation of a social skills program using art therapy and group therapy for children on the autism spectrum. Child. Sch. 30, 27–36. doi: 10.1093/cs/30.1.27
Erlingsson, C., and Brysiewicz, P. (2017). A hands-on guide to doing content analysis. Afr. J. Emerg. Med. 7, 93–99. doi: 10.1016/j.afjem.2017.08.001
Fenn, K., and Byrne, M. (2013). The key principles of cognitive-behavioral therapy. Innovation: Educ. Insp. Genrl. Pract. 6, 579–585. doi: 10.1177/1755738012471029
Fixsen, D. L., Naoom, S. F., Blase, K. A., Friedman, R. M., and Wallace, F. (2005). Implementation research: a synthesis of the literature. Tampa, FL: University of South Florida, Louis de la Parte Florida Mental Health Institute, National Implementation Research Network. FMHI Publication No. 231.
Franklin, M. (2010). Affect regulation, mirror neurons, and the third hand: formulating mindful empathic art interventions. Art Therapy 27, 160–167. doi: 10.1080/07421656.2010.10129385
Freilich, R., and Shechtman, Z. (2010). The contribution of art therapy to the social, emotional, and academic adjustment of children with learning disabilities. Arts Psychother. 37, 97–105. doi: 10.1016/j.aip.2010.02.003
Frey, D. (2015). “Play therapy interventions with adults,” in Play Therapy; A Comprehensive Guide to Theory and Practice, eds D. Crenshaw, and A. Stewart (New York, NY: Guilford), 452–464.
Gardner, B. (2015). “Play therapy with adolescents,” in Play Therapy: A Comprehensive Guide to Theory and Practice, eds D. Crenshaw, and A. Stewart (New York, NY: Guilford), 439–451.
Gerge, A., Hawes, J., Eklöf, L., and Pedersen, I. N. (2019). Proposed mechanisms of change in arts-based psychotherapies. Voices 19:31. doi: 10.15845/voices.v19i2.2564
Gerge, A., and Pedersen, I. N. (2017). Analyzing pictorial artifacts from psychotherapy and art therapy when overcoming stress and trauma. The Arts in Psychotherapy. 54, 56–68. doi: 10.1016/j.aip.2017.02.001
Gratz, K. L., Levy, R., and Tull, M. T. (2012). Emotion regulation as a mechanism of change in an acceptance-based emotion regulation group therapy for deliberate self-harm among women with borderline personality pathology. J. Cogn. Psychother. 26, 365–380. doi: 10.1891/0889-8391.26.4.365
Graves-Alcorn, S., and Green, E. (2014). “The expressive arts therapy continuum: history and theory,” in Integrating Expressive Arts and Play Therapy with Children and Adolescents, eds E. Green, and A. Drewes (New York, NY: Wiley), 1016.
Groh, A. M., Fearon, R. M. P., van IJzendoorn, M. H., Bakermans-Kranenburg, M. J., and Roisman, G. I. (2016). Attachment in the early life course: meta-analytic evidence for its role in socioemotional development. Child Dev. Perspect. 11, 70–76. doi: 10.1111/cdep.12213
Haeyen, S., van Hooren, S., Dehue, F., and Hutschemaekers, G. (2017). Development of an art-therapy intervention for patients with personality disorders: an intervention mapping study. Int. J. Art Therapy 23, 125–135. doi: 10.1080/17454832.2017.1403458
Hartz, L., and Thick, L. (2005). Art therapy strategies to raise self-esteem in female juvenile offenders: a comparison of art psychotherapy and art as therapy approaches. Art Therapy 22, 70–80. doi: 10.1080/07421656.2005.10129440
Hashemian, P., and Jarahi, L. (2014). Effect of painting therapy on aggression in educable intellectually disabled students. Psychology 05, 2058–2063. doi: 10.4236/psych.2014.518208
Higenbottam, W. (2004). In her image. Canad. Art Therapy Assoc. J. 17, 10–16. doi: 10.1080/08322473.2004.11432256
Jang, H., and Choi, S. (2012). Increasing ego-resilience using clay with low SES (Social Economic Status) adolescents in group art therapy. Arts Psychother. 39, 245–250. doi: 10.1016/j.aip.2012.04.001
Jaspers, M., de Winter, A. F., Veenstra, R., Ormel, J., Verhulst, F. C., and Reijneveld, S. A. (2012). Preventive child health care findings on early childhood predict peer-group social status in early adolescence. J. Adolesc. Health 51, 637–642. doi: 10.1016/j.jadohealth.2012.03.017
Jo, M. J., Hong, S., and Park, H. R. (2018). Effects of art intervention program for siblings of children with cancer: a pilot study. J. Pediatr. Oncol. Nurs. 35, 178–187. doi: 10.1177/1043454218762702
Karkou, V., and Sanderson, P. (2006). Arts Therapies: a Research-Based Map of the Field. Edinburgh: Elsevier Churchill Livingstone.
Khadar, M. G., Babapour, J., and Sabourimoghaddam, H. (2013). The effect of art therapy based on painting therapy in reducing symptoms of Oppositional Defiant Disorder (ODD) in elementary school boys. Procedia Soc. Behav. Sci. 84, 1872–1878. doi: 10.1016/j.sbspro.2013.07.051
Khodabakhshi Koolaee, A., Vazifehdar, R., Bahari, F., and Akbari, M. E. (2016). Impact of painting therapy on aggression and anxiety of children with cancer. Caspian J. Pediatr. 2, 135–141.
Kieling, C., Baker-Henningham, H., Belfer, M., Conti, G., Ertem, I., Omigbodun, O., et al. (2011). Child and adolescent mental health worldwide: evidence for action. Lancet 378, 1515–1525. doi: 10.1016/S0140-6736(11)60827-1
Kymissis, P., Christenson, E., Swanson, A. J., and Orlowski, B. (1996). Group treatment of adolescent inpatients: a pilot study using a structured therapy approach. J. Child Adolesc. Group Therapy 6, 45–52. doi: 10.1007/BF02548513
Lehman, B. J., David, D. M., and Gruber, J. A. (2017). Rethinking the biopsychosocial model of health: understanding health as a dynamic system. Soc. Personal. Psychol. Compass 11:e12328. doi: 10.1111/spc3.12328
Liu, C. (2017). Examining the effectiveness of Solution-Focused Art Therapy (SF-AT) for sleep problems of children with traumatic experience. Avaliable online at: https://www.semanticscholar.org/paper/Examining-the-Effectiveness-of-Solution-Focused-Art-Liu/07047beab98ae0d76fad50d96ebc13f0da2d6ffb
Lyshak-Stelzer, F., Singer, P., Patricia, St. John, P., and Chemtob, C. M. (2007). Art therapy for adolescents with posttraumatic stress disorder symptoms: a pilot study. Art Therapy 24, 163–169. doi: 10.1080/07421656.2007.10129474
Malchiodi, C. A., and Crenshaw, D. A. (2015). Creative Arts and Play Therapy for Attachment Problems. New York, NY: The Guilford Press.
Mlinarić, A., Horvat, M., and Šupak Smolčić, V. (2017). Dealing with the positive publication bias: why you should really publish your negative results. Biochem. Medica 27, 13–15. doi: 10.11613/BM.2017.030201
Moon, B. L. (2012). Art therapy teaching as performance art. Art Therapy 29, 192–195. doi: 10.1080/07421656.2012.730954
Ogundele, M. O. (2018). Behavioral and emotional disorders in childhood: a brief overview for pediatricians. World J. Clin. Pediatr. 7, 9–26. doi: 10.5409/wjcp.v7.i1.9
Patrick, P. M., Reupert, A. E., and McLean, L. A. (2019). A cross-sectional study on intergenerational parenting and attachment patterns in adult children of parents with mental illness. Child Fam. Soc. Work 24, 601–609. doi: 10.1111/cfs.12641
Petri, G., Beadle-Brown, J., and Bradshaw, J. (2020). Redefining self-advocacy: a practice theory-based approach. J. Policy Pract. Intel. Disabilities 17, 207–218. doi: 10.1111/jppi.12343
Pifalo, T. (2002). Pulling out the thorns: art therapy with sexually abused children and adolescents. Art Therapy 19, 12–22. doi: 10.1080/07421656.2002.10129724
Pifalo, T. (2006). Art therapy with sexually abused children and adolescents: extended research study. Art Therapy 23, 181–185. doi: 10.1080/07421656.2006.10129337
Pretorius, G., and Pfeifer, N. (2010). Group art therapy with sexually abused girls. S. Afr. J. Psychol. 40, 63–73. doi: 10.1177/008124631004000107
Ramin, A., Mousavi, M., and Sohrabi, N. (2014). Effects of art therapy on anger and self-esteem in aggressive children. Procedia Soc. Behav. Sci. 113, 111–117. doi: 10.1016/j.sbspro.2014.01.016
Ramirez, K. A. (2013). Art therapy for enhancing academic experience of male high school freshmen (Ph. D. Dissertation). Avaliable online at: https://digitalcommons.lesley.edu/expressive_dissertations/28/?utm_source=digitalcommons.lesley.edu%2Fexpressive_dissertations%2F28&utm_medium=PDF&utm_campaign=PDFCoverPage/
Regev, D., and Guttmann, J. (2005). The psychological benefits of artwork: the case of children with learning disorders. Arts Psychother. 32, 302–312. doi: 10.1016/j.aip.2005.02.001
Reis, H. T., and Clark, M. S. (2013). “Responsiveness,” in Oxford Library of Psychology. The Oxford Handbook of Close Relationships, eds J. A. Simpson and L. Campbell (Oxford University Press), 400–423.
Richard, D. A., More, W., and Joy, S. P. (2015). Recognizing emotions: testing an intervention for children with autism spectrum disorders. Art Therapy 32, 13–19. doi: 10.1080/07421656.2014.994163
Ridder, H. G. (2017). The theory contribution of case study research designs. Bus. Res. 10, 281–305. doi: 10.1007/s40685-017-0045-z
Riley, S. (1999). Brief therapy: an adolescent invention. Art Therapy 16, 83–86. doi: 10.1080/07421656.1999.10129669
Rosal, M. L. (1993). Comparative group art therapy research to evaluate changes in locus of control in behavior disordered children. Arts Psychother. 20, 231–241. doi: 10.1016/0197-4556(93)90018-W
Ross, C. (1996). Something to Draw On: Activities and Interventions Using an Art Therapy Approach. 1st Edn. London, UK: Jessica Kingsley.
Rowe, C., Watson-Ormond, R., English, L., Rubesin, H., Marshall, A., Linton, K., et al. (2016). Evaluating art therapy to heal the effects of trauma among refugee youth. Health Promot. Pract. 18, 26–33. doi: 10.1177/1524839915626413
Saunders, E. J., and Saunders, J. A. (2000). Evaluating the effectiveness of art therapy through a quantitative, outcomes-focused study. Arts Psychother. 27, 99–106. doi: 10.1016/S0197-4556(99)00041-6
Scheeringa, M. S., Salloum, A., Arnberger, R. A., Weems, C. F., Amaya-Jackson, L., and Cohen, J. A. (2007). Feasibility and effectiveness of cognitive-behavioral therapy for posttraumatic stress disorder in preschool children: two case reports. J. Trauma. Stress 20, 631–636. doi: 10.1002/jts.20232
Schreier, H., Ladakakos, C., Morabito, D., Chapman, L., and Knudson, M. M. (2005). Posttraumatic stress symptoms in children after mild to moderate pediatric trauma: a longitudinal examination of symptom prevalence, correlates, and parent-child symptom reporting. J. Trauma. 58, 353–363. doi: 10.1097/01.TA.0000152537.15672.B7
Schweizer, C., Knorth, E. J., and Spreen, M. (2014). Art therapy with children with Autism spectrum disorders: a review of clinical case descriptions on ‘what works.’ Arts Psychother. 41, 577–593. doi: 10.1016/j.aip.2014.10.009
Sellers, R., Collishaw, S., Rice, F., Thapar, A. K., Potter, R., Mars, B., et al. (2013). Risk of psychopathology in adolescent offspring of mothers with psychopathology and recurrent depression. Br. J. Psychiatry 202, 108–114. doi: 10.1192/bjp.bp.111.104984
Siegel, J., Iida, H., Rachlin, K., and Yount, G. (2016). Expressive arts therapy with hospitalized children: a pilot study of co-creating healing sock creatures©. J. Pediatr. Nurs. 31, 92–98. doi: 10.1016/j.pedn.2015.08.006
Sitzer, D. L., and Stockwell, A. B. (2015). The art of wellness: a 14-week art therapy program for at-risk youth. Arts Psychother. 45, 69–81. doi: 10.1016/j.aip.2015.05.007
Smith, J. P., and Smith, G. C. (2010). Long-term economic costs of psychological problems during childhood. Soc. Sci. Med. 71, 110–115. doi: 10.1016/j.socscimed.2010.02.046
Snir, S., Regev, D., and Shaashua, Y. H. (2017). Relationships between attachment avoidance and anxiety and responses to art materials. Art Therapy 34, 20–28. doi: 10.1080/07421656.2016.1270139
Soliman, E. S., Mahdy, R. S., Fouad, H. A., Abbas, R. A., and Fayed, A. (2020). Multiple risk factors affecting childhood psychosocial dysfunction in primary school Egyptian children. Middle East Current Psychiatry 27:16. doi: 10.1186/s43045-020-00023-2
Sousa, Z., Ribeiro, E., and Horvath, A. (2011). Therapeutic responsiveness as a moment-to-moment process of alliance: development of a conceptual-empirical model and an observational system (Ph. D. Thesis). Avaliable online at: https://www.researchgate.net/publication/289374352_Therapeutic_Responsiveness_as_a_moment-to-moment_process_of_Alliance_Development_of_a_conceptual-empirical_model_and_an_observational_system (accessed July 16, 2020).
Stafstrom, C. E., Havlena, J., and Krezinski, A. J. (2012). Art therapy focus groups for children and adolescents with epilepsy. Epilepsy Behav. 24, 227–233. doi: 10.1016/j.yebeh.2012.03.030
Steiert, A. (2015). Helden(–bilder) als emotionale unterstützung in der kunsttherapie mit kindern und jugendlichen im kontext lebensbedrohlicher erkrankungen. Musik Tanz-Und Kunsttherapie 26, 24–28. doi: 10.1026/0933-6885/a000159
Thomas, B. H., Ciliska, D., Dobbins, M., and Micucci, S. (2004). A process for systematically reviewing the literature: providing the research evidence for public health nursing interventions. Worldviews Evid. Based Nurs. 1, 176–184. doi: 10.1111/j.1524-475X.2004.04006.x
Tibbetts, T. J., and Stone, B. (1990). Short-term art therapy with seriously emotionally disturbed adolescents. Arts Psychother. 17, 139–146. doi: 10.1016/0197-4556(90)90024-K
Van Lith, T. (2016). Art therapy in mental health: a systematic review of approaches and practices. Arts Psychother. 47, 9–22. doi: 10.1016/j.aip.2015.09.003
Veldman, K., Reijneveld, S. A., Almansa Ortiz, J., Verhulst, F. C., and Bültmann, U. (2015). Mental health trajectories from childhood to young adulthood affect the educational and employment status of young adults: results from the TRAILS study. J. Epidemiol. Commun. Health 69, 588–593. doi: 10.1136/jech-2014-204421
Veríssimo, M., Santos, A. J., Fernandes, C., Shin, N., and Vaughn, B. E. (2014). Associations between attachment security and social competence in preschool children. Merrill-Palmer Q. 60:80. doi: 10.13110/merrpalmquar1982.60.1.0080
Vogels, A. G. C. (2008). The Identification by Dutch Preventive Child Health Care of Children With Psychosocial Problems: Do Short Questionnaires Help? (Thesis). Faculty of Medical Sciences, University Medical Center Groningen, The Netherlands.
Wallace, J., Packman, W., Huffman, L. C., Horn, B., Cowan, M., Amylon, M. D., et al. (2014). Psychosocial changes associated with participation in art therapy interventions for siblings of pediatric hematopoietic stem cell transplant patients. Art Therapy 31, 4–11. doi: 10.1080/07421656.2014.873685
Waller, D. (2006). Art therapy for children: how it leads to change. Clin. Child Psychol. Psychiatry 11, 271−282. doi: 10.1177/1359104506061419
Walsh, S. M. (1993). Future images: An art intervention with suicidal adolescents. Appl Nurs Res. 6, 111–118. doi: 10.1016/s0897-1897(05)80171-5
World Health Organization (2018). Child and adolescent mental health. Avaliable online at: https://www.who.int/mental_health/maternal-child/child_adolescent/en/ (accessed August 11, 2020).
Wright, A. G. C., and Simms, L. J. (2015). A metastructural model of mental disorders and pathological personality traits. Psychol. Med. 45, 2309–2319. doi: 10.1017/S0033291715000252
Keywords: art therapy, psychosocial problems, children, adolescents, systematic narrative review
Citation: Bosgraaf L, Spreen M, Pattiselanno K and Hooren Sv (2020) Art Therapy for Psychosocial Problems in Children and Adolescents: A Systematic Narrative Review on Art Therapeutic Means and Forms of Expression, Therapist Behavior, and Supposed Mechanisms of Change. Front. Psychol. 11:584685. doi: 10.3389/fpsyg.2020.584685
Received: 20 July 2020; Accepted: 24 August 2020;
Published: 08 October 2020.
Edited by:
Jennifer Drake, Brooklyn College (CUNY), United StatesCopyright © 2020 Bosgraaf, Spreen, Pattiselanno and Hooren. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Liesbeth Bosgraaf, bGllc2JldGguYm9zZ3JhYWZAbmhsc3RlbmRlbi5jb20=