 Áron Horváth
Áron Horváth Luca Vig
Luca Vig Eszter Ferentzi
Eszter Ferentzi Ferenc Köteles
Ferenc Köteles- 1Doctoral School of Psychology, ELTE Eötvös Loránd University, Budapest, Hungary
- 2Institute of Health Promotion and Sport Sciences, ELTE Eötvös Loránd University, Budapest, Hungary
Interoception in the broader sense refers to the perception of internal states, including the perception of the actual state of the internal organs (visceroception) and the motor system (proprioception). Dimensions of interoception include (1) interoceptive accuracy, i.e., the ability to sense internal changes assessed with behavioral tests, (2) confidence rating with respect to perceived performance in an actual behavioral test, and (3) interoceptive sensibility, i.e., the self-reported generalized ability to perceive body changes. The relationship between dimension of cardioceptive and proprioceptive modalities and their association with affect are scarcely studied. In the present study, undergraduate students (N = 105, 53 males, age: 21.0 ± 1.87 years) filled out questionnaires assessing positive and negative affect (Positive and Negative Affect Schedule), interoceptive sensibility (Body Awareness Questionnaire), and body competence (Body Competence Scale of the Body Consciousness Questionnaire). Following this, they completed a behavioral task assessing cardioceptive accuracy (the mental heartbeat tracking task by Schandry) and two tasks assessing proprioceptive accuracy with respect to the tension of arm flexor muscles (weight discrimination task) and the angular position of the elbow joint (joint position reproduction task). Confidence ratings were measured with visual analog scales after the tasks. With the exception of a weak association between cardioceptive accuracy and the respective confidence rating, no associations between and within modalities were found with respect to various dimensions of interoception. Further, the interoceptive dimensions were not associated with state and trait positive and negative affect and perceived body competence. In summary, interoceptive accuracy scores do not substantially contribute to conscious representations of cardioceptive and proprioceptive ability. Within our data, non-pathological affective states (PANAS) are not associated with the major dimensions of interoception for the cardiac and proprioceptive modalities.
Introduction
Interoception refers to the processing of information originating from within the body (Cameron, 2002). Originally, it was a synonym for visceroception; later, the inclusion of somatosensory and proprioceptive information was also proposed (Vaitl, 1996; Ceunen et al., 2016; Berntson et al., 2018). The current paper applies this broad approach to interoception. Thus, conscious aspects of interoception include body sensations associated with emotions, awareness of non-emotive body processes and the perception of the actual state of the locomotor system.
The recently accepted conceptualization of conscious aspects of interoception describes at least two major dimensions (Ceunen et al., 2013; Garfinkel and Critchley, 2013; Garfinkel et al., 2015a). Interoceptive accuracy (IAc or sensitivity) refers to the acuity of perception of internal changes and states as assessed by behavioral methods. Its self-report counterpart, i.e., the perceived performance in an a behavioral test of acuity, is called confidence. Finally, the perceived general ability to sense body changes is called interoceptive sensibility (IS) or awareness in the literature. Empirical evidence shows that the association between these three dimensions of cardiac interoception is weak or non-existing (see below).
It is worth noting that there is an inconsistency in the literature with respect to the concept of interoceptive sensibility. Unfortunately, it is not clear which questionnaires should be used to assess the dispositional aspect of interoceptive sensibility. Garfinkel et al. (2015a) recommend the Body Awareness Scale of the Body Perception Questionnaire (Porges, 1993). The Body Awareness Questionnaire (BAQ) (Shields et al., 1989) and the Multidimensional Assessment of Interoceptive Awareness (Mehling et al., 2012) have been also used in the literature (Meessen et al., 2016; Ferentzi et al., 2019). Although the former does not make a distinction between visceroception and proprioception, whereas the latter includes only visceroceptive modalities, a recent study indicated a substantial overlap between the two constructs (Ferentzi et al., 2020).
Concerning the emotional experience, the primary importance of visceroception has been suggested by many authors (James, 1884, James, 1890; Lange, 1885; Damasio, 1994), whereas others emphasize the role of the somatosensory system (Darwin, 1872; Tomkins, 1962, 1981; Izard, 1971). These models assume the causal role of interoceptive information in the development of affective experience thus they are called peripheral theories of emotion. Central theories do not suppose such a causal link (Cannon, 1927, 1931; Panksepp, 1982, 1991; Oatley and Johnson-laird, 1987; Davis, 1989; LeDoux, 1990); still, they accept that emotions are typically characterized by peripheral changes that prepare the organism for the behavioral response. As a proportion of these changes, both visceral and somatosensory, may reach conscious awareness, an association between the emotional experience and the perception of body changes can be explained by central theories too.
Cardiac response plays a central role in the physiological component of emotional reactions, as they are usually characterized by an increased energetic demand (Lacey and Lacey, 1978). It is widely assumed that, in line with the tenets of peripheral theories of emotion, the accuracy of perception of cardiac activity, dubbed cardioceptive accuracy, contributes to the emotional experience (Wiens et al., 2000; Pollatos et al., 2005). On the other hand, a more intense emotional reaction (e.g., if it is accompanied by sympathetic activation) can improve the perception of heartbeats (Schandry et al., 1993; O’Brien et al., 1998; Fairclough and Goodwin, 2007). Empirical studies revealed a positive association between the intensity (arousal) component of emotions and cardioceptive accuracy (Wiens et al., 2000; Barrett et al., 2004; Pollatos et al., 2005, 2007b; Herbert et al., 2007, 2010). Also, improved cardiac accuracy was found to be related to the actual level of anxiety in a number of studies (Schandry, 1981; Ludwick-Rosenthal and Neufeld, 1985), whereas no such associations were reported in others (Pollatos et al., 2007a; Werner et al., 2013). From a theoretical point of view cardioceptive confidence may also contribute to the affective experience. For example, manipulated feedback on heart rate was enough to intensify the emotional reaction (Valins, 1966, 1967). Even more intriguingly, if actual and perceived heart rate did not correspond, the latter influenced the perceived level of arousal (Thornton and Hagan, 1976; Kerber and Coles, 1978; Woll and McFall, 1979; Parkinson, 1985).
Proprioceptive information is also assumed to play a substantial role in the formation of emotional experience. According to different theories (for a review, see Moors, 2009), somatic and/or motor changes, modulated by cognitive processing, are cornerstones of the arising of affective feelings. Changes in the musculoskeletal system can modulate the emotional experience. Shafir et al. (2015) showed that different affective feelings can be evoked by specific, complex movement patterns. Power posing may also change the affective experience; however results with respect to behavioral (more risk-taking) and hormonal responses (i.e., increased testosterone and decreased cortisol level) are controversial (Carney et al., 2010; Ranehill et al., 2015; Simmons and Simonsohn, 2017). In the same vein, EMG activity increases in many muscles and muscle groups in stressful situations (Lundberg et al., 1994; Wahlström et al., 2002; Krantz et al., 2004; Luijcks et al., 2014), and it is possible to reduce stress and anxiety through relaxation techniques (e.g., progressive relaxation, autogenic training), which operate (at least partially) through the systematic relaxation of muscles (Kanji et al., 2006; Rausch et al., 2006). Finally, Cacioppo et al. (1993) showed that the activation of arm flexor muscles activates the approach system, which biases the judgment of neutral stimuli to the positive direction. By contrast, activation of arm extensors stimulates the avoidance system, resulting in the opposite effect. Neumann and Strack (2000) drew a similar conclusion in a categorization task. Overall, these findings support the idea that the actual state of muscles can impact the emotional experience.
Based on the aforementioned role of proprioceptive information in the formation of the affective experience, it is logical to assume that, similar to cardioceptive information, individual differences in the accuracy of processing of proprioceptive information (aka proprioceptive accuracy) are related to differences in emotional processing. In accordance with this assumption, alterations in processing and integration of proprioceptive input can be associated with pathological conditions. For example, a greater reliance on proprioception during the completion of a motor task is associated with impairments in imitation and empathy in autism spectrum, and attention deficit hyperactivity disorder (Gao et al., 2019). In fibromyalgia, however, patients were found to be less reliant on proprioceptive information than healthy controls (Bardal et al., 2016). Also, decreased proprioceptive accuracy was found in chronic pain (Tsay et al., 2015) and schizophrenia (Rosenbaum et al., 1959, 1965; Leventhal et al., 1982; Chang and Lenzenweger, 2005). In contrast, somatoform disorders are accompanied by higher proprioceptive accuracy (Scholz et al., 2001). It is also important to note that an emotionally intense state, e.g., the high level of stress, decreases proprioceptive accuracy (Şenol et al., 2018). However, not all studies confirmed the aforementioned relationships, there are null findings too, for example with respect to schizophrenia (Ritzler and Rosenbaum, 1974; Ritzler, 1977), fibromyalgia (Akyol et al., 2013; Ulus et al., 2013), and chronic pain (Tsay et al., 2015). Moreover, Horváth et al. (2019) found that there is no association between trait affect and proprioceptive accuracy, as assessed with the Joint Position Reproduction test in the elbow joint. Additionally, proprioceptive accuracy was not correlated with body awareness–a construct that overlaps with interoceptive sensibility (Ferentzi et al., 2020)–and perceived body competence (Ferentzi et al., 2017; Horváth et al., 2019).
When investigating the role of interoceptive accuracy, it is a fundamental question whether individual characteristics in information processing established in one modality (e.g., cardioception) can be generalized to other modalities (e.g., proprioception). Ferentzi et al. (2018) reported no association between modalities of interoception. A significant association was found only between measures within the same modality for three visceroceptive modalities (i.e., pain threshold and tolerance, gastric fullness and unpleasantness, and the intensity and unpleasantness of bitter taste), but there was no association between the two included measures of proprioceptive accuracy (ipsilateral and contralateral version of the joint position reproduction test in the elbow joint). These and other results (Garfinkel et al., 2017) show that interoceptive accuracy cannot be generalized across interoceptive modalities.
With respect to joint-related proprioceptive accuracy, a number of measurement paradigms were developed (Han et al., 2016). Studies investigating the association between different tests in one joint (Barrack et al., 1984; Grob et al., 2002; Jong et al., 2005; Elangovan et al., 2014; Li et al., 2016; Niespodziński et al., 2018; Yang et al., 2020) consistently report that accuracy is test-specific. The same conclusion can be drawn with respect to cardioception: accuracy scores obtained by heartbeat discrimination methods that use forced-choice methods and methods that use heartbeat tracking (i.e., counting) typically show no or only weak associations (Pennebaker and Hoover, 1984; Weisz et al., 1988; Phillips et al., 1999; Schaefer et al., 2012; Hart et al., 2013; Schulz et al., 2013; Michal et al., 2014; Garfinkel et al., 2015a,b; Forkmann et al., 2016; Ring and Brener, 2018). Moreover, proprioceptive measurement methods can be conducted with respect to different joints; Han et al. (2013) and Waddington and Adams (1999) revealed that accuracy, assessed with the same paradigm (active movement extent discrimination apparatus) is joint-specific, and only the same joints of the left and right side of the body show an association. The actual exertion (or tension) of muscles represents another proprioceptive modality; a fundamental difference is that activation of the muscles is controlled by a feed-forward mechanism thus the efferent information plays a similarly important role in the processing of the actual state as the afferent input (Miall and Wolpert, 1996; Cullen, 2004). Further, joint-related acuity primarily relies on receptors located in the joints (Ruffini end organs), whereas muscle-related accuracy is impacted by afference from receptors in the muscles (muscle spindles) (Batson, 2009; Jha et al., 2017).
Confidence rating, the self-reported dimension of interoception, appears to be independent of interoceptive accuracy for healthy participants (e.g., Ehlers et al., 1995). In another study, accuracy and confidence were associated among high performers in both applied heartbeat perception tasks, i.e., the mental tracking and the discrimination task (Garfinkel et al., 2015a). The authors interpret their results as a dissociation of the assessed dimensions of interoception which was replicated by others regarding the mental tracking task (Forkmann et al., 2016; Meessen et al., 2016). A weak positive association between cardioceptive accuracy and confidence was found in another study (Köteles et al., 2020a). Besides heartbeat perception, interoceptive confidence with respect to respiration has been also investigated and the dissociation between accuracy and confidence was confirmed (Garfinkel et al., 2016). In the field of proprioception, however, confidence has not been assessed to date.
The major goal of the present study is to shed more light on the associations within and between the dimensions of cardioception and two modalities of proprioception, i.e., the sense of joint position and muscle tension. We also wanted to explore the associations between affect and the behavioral and self-report measures of these modalities.
The following hypotheses were tested. First, accuracy and confidence show a weak positive association within the same modality (H1). Second, accuracy and confidence between modalities are independent of each other (H2). Third, cardioceptive accuracy and confidence are associated with affect, whereas proprioceptive accuracy and confidence are not (H3). Finally, we assumed that proprioceptive accuracy and confidence would not be associated with perceived body competence and body awareness (H4).
Materials and Methods
Participants
A priori sample size calculation for r = 0.3, α = 0.05 (one-tailed), 1-β = 0.9 indicated a minimum required sample size of N = 92 (Faul et al., 2007). Participants were undergraduate students of Eötvös Loránd University (N = 105, 53 males, age: 21.0 ± 1.87 years, 95 right handed). Participants consuming alcohol and/or taking psychoactive drugs within 8 h before the experiment, and those with severe injury/disability of the arm were excluded. Participation was rewarded with partial course credit. Joint Position Reproduction test was missing for nine individuals due to technical problems. The study was approved by the Research Ethics Committee of the university. Before participation, everyone signed an informed consent form.
Behavioral Measures
Proprioceptive Accuracy–Joint Position Sense
Joint Positions Sense was assessed with a version of the Joint Position Reproduction Test (JPR) (Goble, 2010), where participants had to reproduce elbow joint positions. We tested the non-dominant arm of the participants. Participants were blindfolded, seated, and asked to keep a standard posture (upper arms parallel with the ground and in line with the body). During the measurement, they placed their upper arm on a rotatable lever, which was connected to a motor, and made possible the accurate (±0.1 degree) measurement and movement of the elbow joint. They had to hold a handle and keep their hand on a button. 180 degree indicated fully extend elbow. From starting position, the machine moved the arm of the participant to the target positions with a speed of 12 degree/s. After spending 4 s there, the device moved back the lever to the starting position. After 1 s, the lever started to move again, with a speed of 8 degree/s. The task of the participants was to press the button, when they felt that their arm reached the target position. Following this, the lever moved the arm back to the starting position again and a new trial begun. The starting position was always 160 degree, while the target position changed from trial to trial. Overall, nine trials were conducted, with nine different target positions (150, 135, 120, 105, 90, 75, 60, 45, and 30 degree). Every target position was presented once; the order of presentation was randomized. To calculate the accuracy of Joint Position Reproduction, an error score (i.e., the difference between the target and the reproduced position (i.e., the difference between the target and the reproduced position) was calculated for each trial. Outliers above and below two standard deviation were removed and missing values were imputed by using the fully conditional specification (MCMC) and linear regression model options of SPSS v20 software. To determine accuracy, we used two error scores: constant and variable error (Schutz and Roy, 1973; Boisgontier et al., 2012; Goble et al., 2012). Constant error is the mean of the error scores and shows the magnitude and direction of the systematic distortion in position judgments. Negative values of constant error score indicate bias toward the inside direction, whereas positive values indicate bias toward the outside direction. Internal consistency of constant error was acceptable (Cronbach’s alpha: 0.751). Variable error is the standard deviation of the error scores and shows the inconsistency of judgments (i.e., higher variable error shows higher level of inconsistency.
Proprioceptive Accuracy–Weight Discrimination
To assess weight discrimination ability, participants had to compare the weight of two objects (Chang and Lenzenweger, 2005). These objects were glass bottles filled with water, identical in shape and size. During the measurement, participants eyes’ were covered; they had to keep a standing posture, keep their left upper arm next to their body, and their lower arm in a flexion of approximately 90 degree.
Overall, 32 comparisons were made. The weight of one of the presented bottles was always 200 g. In one half of the trials (16), the other bottle was 200 g (identical pairs), while in the other half (16), it was 215 g (different pairs). The presentation order of the pairs and that of the bottles within pairs were randomized. Participants had to hold every bottle for 8 s, verbally judge if they were the same weight or one was heavier. For heavier judgments, it also had to be indicated which weight was heavier. Weight discrimination ability was calculated by dividing the number of correct trials by the number of all trials.
Cardioceptive Accuracy
Cardioceptive accuracy was assessed with a mental heartbeat-counting paradigm (Schandry, 1981). Participants had to count their heartbeats silently, while sitting on a chair, with their hands on their laps. They were explicitly encouraged to count if they had the lightest heartbeat sensation in any part of their body but were also asked not to count if they did not have any sensation. After a practice trial, which lasted for 15 s, three test trials of different lengths (25, 35, and 50 s) were conducted. The test trials were presented in a randomized order. The number of heartbeats were recorded with the NeXus recording system (NeXus Wireless Physiological Monitoring and Feedback: NeXus-10 Mark II, Version 1.02; BioTrace + Software for NeXus-10 Version: V201581; Mind Media BV, Herten, the Netherlands). For every interval, an accuracy score was calculated as: 1–| (HB recorded–HB counted)/HB recorded|. For every individual, the scores of the three intervals were averaged to calculate cardioceptive accuracy. Internal consistency of the Schandry task was high (Cronbach’s alpha = 0.906).
Questionnaires and Questions
Confidence Ratings
After every task (Joint Position Sense, Weight Discrimination, Cardioceptive accuracy), participants’ subjective judgment about their performance (“How do you think you performed in this test?”) was recorded. For this purpose, they had to indicate their perceived performance on a 10 cm-long, vertical visual analog scale. The anchor points were “The best possible” and “The worst possible.” We measured the distance of the crossed part of the line from the bottom of the visual analog scale in millimeters. Higher values indicate higher levels of confidence.
Interoceptive Sensibility–Body Awareness
Body Awareness Questionnaire measures the self-reported sensitivity to bodily processes, and the ability to anticipate bodily reactions (Shields et al., 1989; Köteles, 2014). Participants have to answer 18 questions on seven-point Likert-scales (e.g., “I notice distinct body reactions when I am fatigued”), where higher scores mean higher levels of body awareness (except one reversed item). Internal reliability in this sample was good (Cronbach’s α = 0.848).
Body Competence
Body Competence was assessed with the Body Competence Scale of Miller’s Private and Public Body Consciousness Questionnaire (Miller et al., 1981). The scale consists of four questions (e.g., “I’m better coordinated than most people”), rated on a five-point Likert scale. Higher values indicate higher levels of perceived physical competence. Internal consistency of the scale in this study was good (Cronbach’s α = 0.835).
Affect
We used the Positive and Negative Affect Schedule (PANAS) to asses affect (Watson, 1988; Gyollai et al., 2011). The questionnaire can be used with two different instructions, to measure state and trait aspects of affect. The questionnaire is divided into two subscales, positive affect (PA) (e.g., enthusiasm), and negative affect (NA) (e.g., nervousness); both measured with 10 items. Participants have to rate how intensely they feel the given emotional state on a five-point Likert scale, from 1 (“Very slightly or not at all”) to 5 (“Very much”). Higher scores refer to higher levels of positive and negative affect, respectively. Cronbach’s α values indicated acceptable to high levels of internal consistency in this study (Positive Trait: 0.872, Positive State: 0.922, Negative Trait: 0.854, Negative State: 0.794).
Procedure and Statistical Analysis
Data was collected in two phases. Participants had to fill out the questionnaires (with the exception of state PANAS) at home in an online form. The order of the questionnaires was: demographic data, trait PANAS, BAQ, Body Competence. Behavioral measures were conducted individually in the laboratory in a randomized order. Before the behavioral tasks, participants had to fill out the state PANAS questionnaire. Statistical analysis was conducted using the Jasp v0.11 software (JASP Team, 2019) using both the frequentist and Bayesian approach. Due to violations of the requirement of normality, associations were estimated using non-parametric correlations, i.e., Spearman’s rho in the frequentist analysis and Kendall’s Tau in the Bayesian analysis. For the Bayesian analysis, values below 0.33 indicated the superiority of the null-hypothesis, and values over 3 indicated the superiority of the alternative hypothesis (Wetzels and Wagenmakers, 2012).
Results
Descriptive statistics of the assessed variables are presented in Table 1.
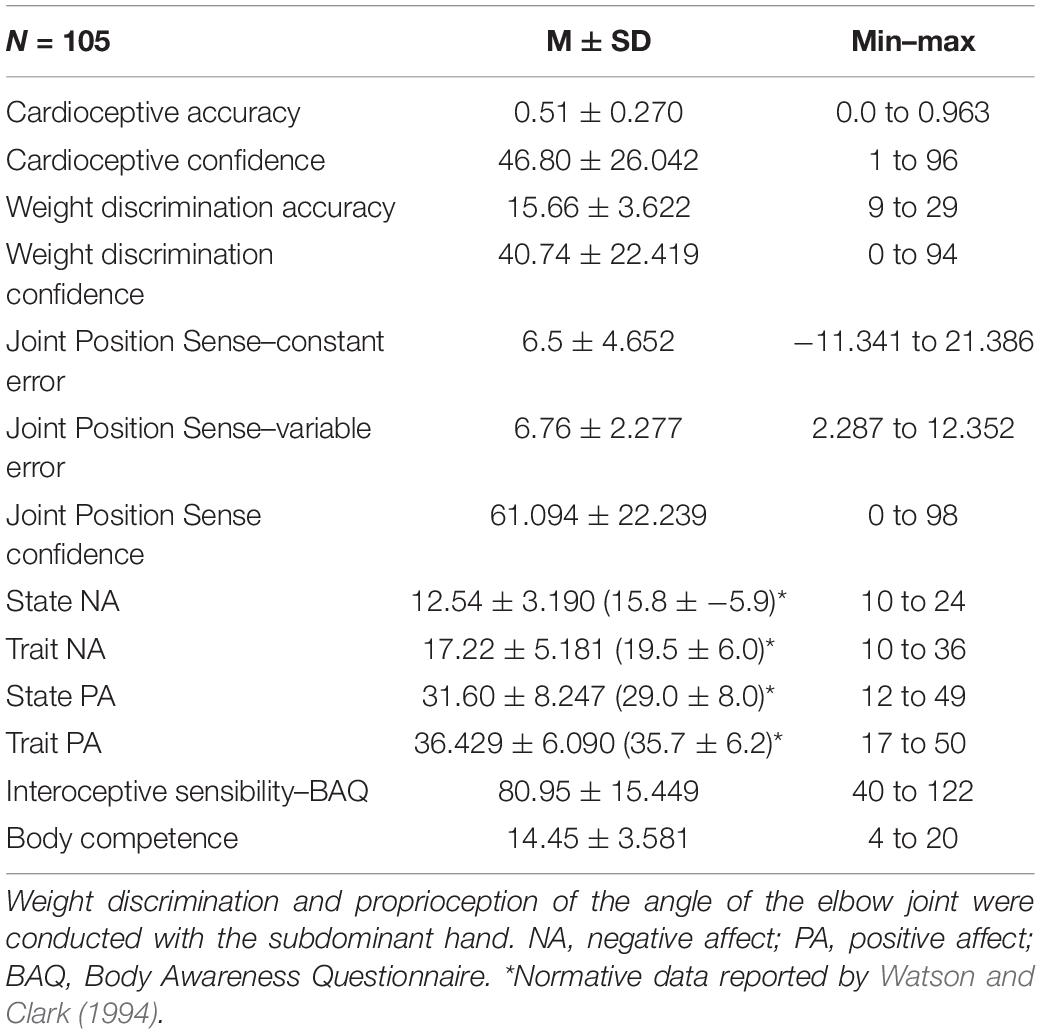
Table 1. Descriptive statistics of the assessed variables.
No significant associations but one between accuracy and confidence ratings (H1) within the included interoceptive modalities were revealed (Table 2). For cardioception, accuracy was weakly (rs = 0.25, p < 0.05) related to confidence (Figure 1); this was supported by the Bayesian analysis (BF10 = 5.063). The null model (i.e., the lack of association) was more probable for all other modalities.
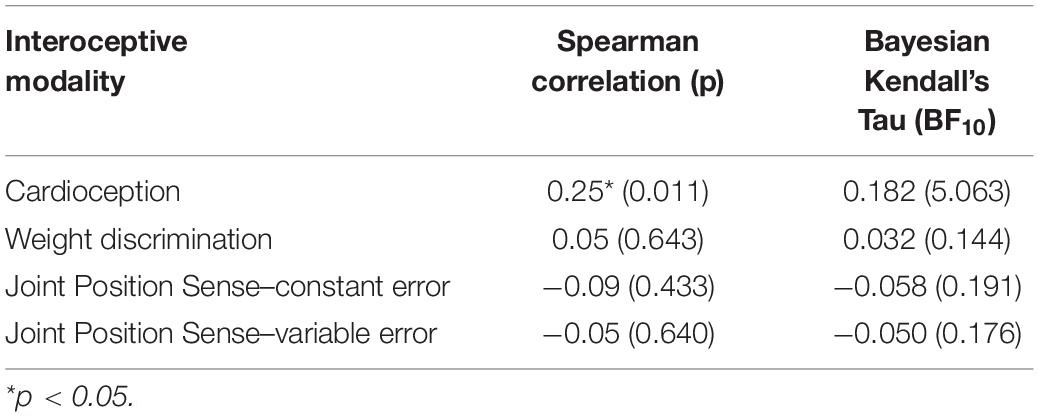
Table 2. Correlations between accuracy and confidence for the three interoceptive modalities.
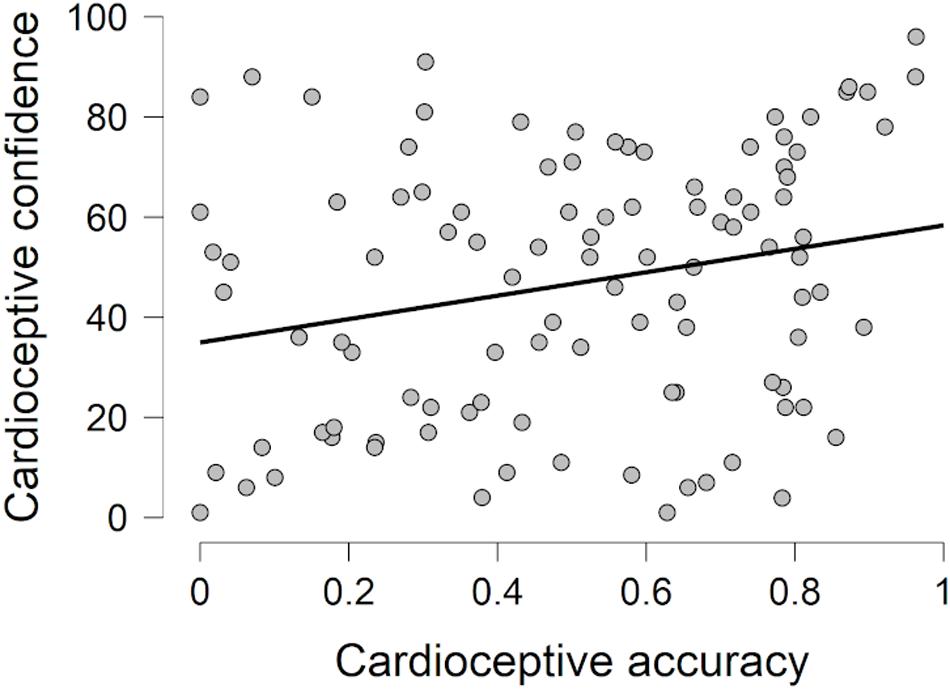
Figure 1. Association between cardioceptive accuracy and cardioceptive confidence ratings.
Concerning associations between indicators of accuracy (H2), no significant correlation was found. Only the two joint position sense related indices (i.e., constant and variable error) showed a moderate association (rs = 0.41, p < 0.001; rτ = 0.28, BF10 = 500.816); Bayesian analysis indicated the superiority of the null hypothesis for all other cases (Table 3).

Table 3. Correlations between accuracies for the three interoceptive modalities.
With respect to confidence ratings, no significant association was found between cardioceptive and weight discrimination related confidence (rs = 0.09, p = 0.374; rτ = 0.067, BF10 = 0.212), between cardioceptive and joint position sense related confidence (rs = 0.14, p = 0.198; rτ = 0.092, BF10 = 0.314), and joint position sense and weight discrimination related confidence (rs = −0.07, p = 0.518; rτ = −0.037, BF10 = 0.155). Again, Bayesian analysis indicated the superiority of the null hypothesis for all cases (Table 4).
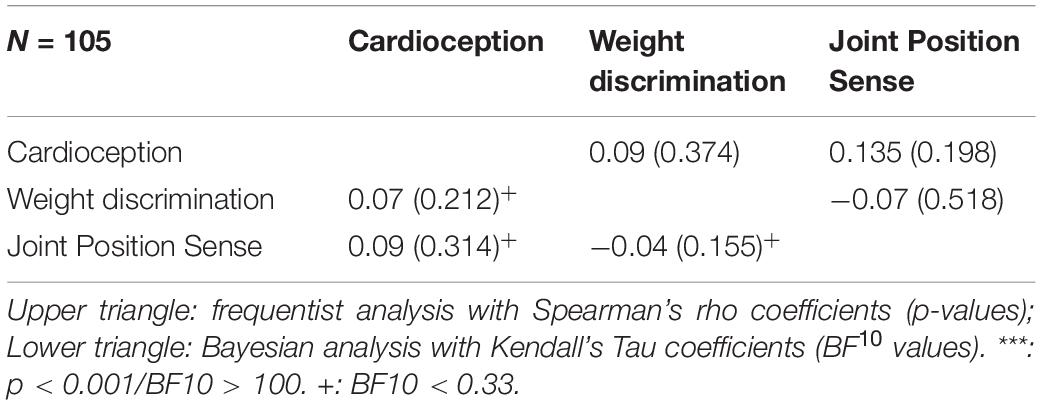
Table 4. Correlations between confidence ratings for the three interoceptive modalities.
Between measures of interoception and questionnaire scores (H3, H4), correlation analysis indicated no significant correlations (Table 5). Bayesian analysis indicated the superiority of the null hypothesis for most of the cases and was inconclusive (i.e., in the 0.33–3 domain) for the remaining associations (Table 6).
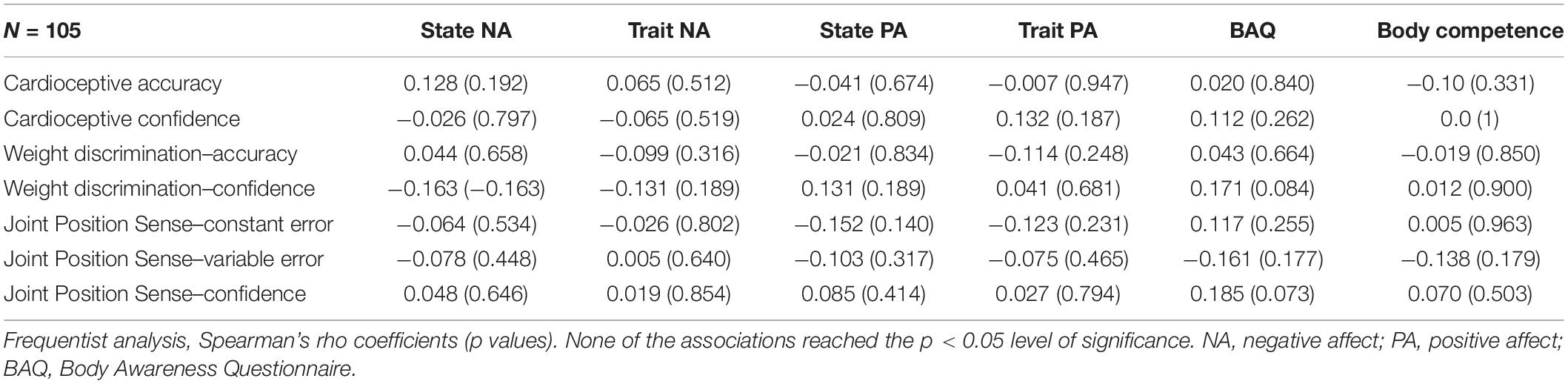
Table 5. Associations between indicators of interoceptive accuracy and confidence ratings and questionnaire scores.
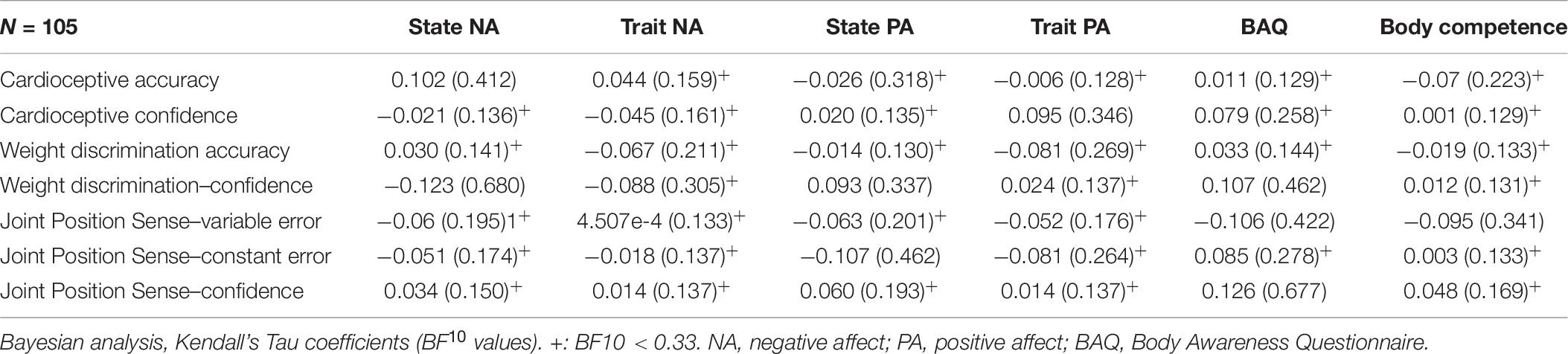
Table 6. Associations between indicators of interoceptive accuracy and confidence ratings and questionnaire scores.
Discussion
The goal of the present study was to investigate the associations between different modalities (cardioception and two proprioceptive modalities) of interoception and their dimensions (accuracy, confidence ratings and sensibility). Associations with positive and negative affect and perceived body competence were also investigated. Overall, accuracy and confidence were associated with respect to the cardiac modality only; further, no between-modality associations and associations with interoceptive sensibility, affect, and body competence were found.
Interoceptive Accuracy and Confidence
Contrary to our first hypothesis, accuracy and confidence were found to be independent of each other with respect to the two proprioceptive modalities. In other words, people are not able to sense their actual performance in these tasks. In the cardioceptive modality, however, similar to previous studies (Garfinkel et al., 2015a), we found a weak positive association between accuracy and confidence. This latter finding is in line with the insight that top-down information substantially impacts performance in the mental tracking task (Ring et al., 2015; Ring and Brener, 2018; Zamariola et al., 2018; Desmedt et al., 2020). Although a strict instruction was applied (i.e., participants were explicitly encouraged not to count if they did not have any sensation to report), which presumably decreases the impact of top-down factors (Ehlers et al., 1995; Desmedt et al., 2018), the involvement of conscious processes in the tracking task is substantial. If one combines knowledge on the usual frequency of his or her heartbeats with the number and timing of actually sensed and counted heartbeats, performance in the task can be estimated (Desmedt et al., 2020). In the case of the proprioceptive modalities, however, no such information is available, thus actual and perceived accuracy show complete dissociation.
In line with our second hypothesis, interoceptive accuracy and the respective confidence ratings proved to be modality-specific. We replicated the findings of Ferentzi et al. (2018), namely that cardioceptive accuracy, as assessed with the mental heartbeat tracking task, does not correlate with measures of proprioceptive accuracy (joint position reproduction and weight discrimination tests in this study). Moreover, in accordance with the findings of other studies (Barrack et al., 1984; Grob et al., 2002; Jong et al., 2005; Elangovan et al., 2014; Li et al., 2016; Niespodziński et al., 2018; Yang et al., 2020), no association between accuracies with respect to two proprioceptive modalities was found. This lack of association might reflect the actual independence of the two abilities; however, conceptual differences (i.e., the weight discrimination test does not involve a reproduction element and it was measured with a forced choice paradigm) can also explain this finding.
The confidence-related findings were similar to those for accuracy: there were no associations between cardioceptive and proprioceptive tasks, and between the two proprioceptive tasks. Empirical results concerning interoceptive confidence across modalities are scarce. Garfinkel et al. (2015a) found a strong positive association between confidence ratings of two heartbeat perception tasks (i.e., mental heartbeat tracking task and the discrimination task). In our data, this indicates that the perception of performance is not only more or less independent of actual performance, but also differs between modalities; cardioception-related confidence rating show closer connection than those of proprioceptive confidence. This also suggests that top-down factors that usually impact perception, such as previous experiences and expectations, may show considerable modality-specific differences.
Interoception and Affect
Contrary to our expectation (H3), we did not find any association between state and trait positive and negative affect and cardioception-related accuracy and confidence In fact, Bayesian analysis supported the lack of association for the majority of the analyses. The same was true for the two proprioceptive modalities. There are several possible explanations for these null-findings. Cardioceptive accuracy showed associations with arousal but not with valence in studies where emotions were experimentally evoked and the two dimensions were assessed independently (Wiens et al., 2000; Barrett et al., 2004; Pollatos et al., 2005, 2007b; Herbert et al., 2007, 2010; Köteles et al., 2020b). The approach used in the present study, however, primarily measures affective states that are accompanied with high arousal (Lox et al., 2010) thus cannot separate these components. Further, the actual affective state of participants was measured, which is necessary less intense than experimentally evoked affective states. Under such conditions, the already weak association between cardioception and emotional experience may disappear. Concerning chronic (trait-like) emotional states, previous studies assessed anxiety, an affective state accompanied with marked vegetative changes (i.e., sympathetic activation), particularly for patients with related disorders (e.g., Domschke et al., 2010). For positive and negative affect in healthy participants, however, the intensity of the emotions, including both the experience and the vegetative changes, are much lower. Also, we did not asses other interoceptive channels that might be associated with the emotional experience. This holds particularly true for proprioceptive accuracy, where the investigation of a single joint and task represent only one aspect of the proprioceptive accuracy of the whole body (Han et al., 2013). Secondly, emotions assessed with self-report might not be at the same level of consciousness as accuracy and confidence related decisions (Smith and Lane, 2015).
Proprioception and Body-Related Questionnaires
Finally (H4), we replicated the findings on the independence of proprioceptive accuracy and interoceptive sensibility and body competence (Horváth et al., 2019) and extended them to another proprioceptive modality (weight discrimination) and confidence rating. The lack of association between interoceptive sensibility, a construct that integrates interoceptive experience across multiple channels, and interoceptive confidence ratings is particularly intriguing.
Also, our results indicate that the self-reported acute dimension of interoception is also modality-specific, i.e., cannot be generalized. As both constructs represent perceived abilities and the former is embedded in the latter (at least theoretically), their independence is clearly worthy of further investigation.
Limitations
We investigated a sample of young people without known pathology; in this population, strong emotions were rarely presented. This leads to the decrease of variance in affective ratings which in turn makes the detection of associations difficult. The Schandry task has received considerable criticism recently (Ring et al., 2015; Desmedt et al., 2018, 2020; Ring and Brener, 2018; Zamariola et al., 2018); thus, although we applied a strict instruction which decreases the role of top-down factors, cardioception-related findings of the study might be flawed. Also, the joint reproduction task involves memory processes. Thus, cognitive abilities unrelated to interoception might also influence participants’ performance.
Conclusion
Our findings indicate that interoceptive accuracy and confidence ratings are independent from each other in two proprioceptive modalities (joint reproduction with respect to the elbow joint and weight discrimination using the arm flexor muscles) and they are only weakly associated in the cardioceptive modality. There are no associations between accuracy and confidence ratings within the three interoceptive modalities. Finally, proprioceptive and cardioceptive accuracy and confidence ratings are not related to the acute and chronic affective state, interoceptive sensibility/body awareness and perceived body competence.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Research Ethics Committee of the Faculty of Education and Psychology at ELTE Eötvös Loraìnd University. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
All authors contributed to the conception and design of the study, read and commented on the last version of the manuscript. ÁH and LV contributed to the assessment of data. FK processed the data and performed the statistical analyses. ÁH wrote the first draft of the manuscript. EF and FK wrote sections of the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This research was supported by the Hungarian National Scientific Research Fund (KH 130319).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
Akyol, Y., Ulus, Y., Tander, B., Bilgici, A., and Kuru, O. (2013). Muscle strength, fatigue, functional capacity, and proprioceptive acuity in patients with fibromyalgia/Fibromiyaljili hastalarda kas gucu, yorgunluk, fonksiyonel kapasite ve proprioseptif keskinlik. Turk. J. Phys. Med. Rehabil. 59, 292–299.
Bardal, E. M., Roeleveld, K., Ihlen, E., and Mork, P. J. (2016). Micro movements of the upper limb in fibromyalgia: The relation to proprioceptive accuracy and visual feedback. J. Electromyogr. Kinesiol. 26, 1–7. doi: 10.1016/j.jelekin.2015.12.006
Barrack, R. L., Skinner, H. B., and Cook, S. D. (1984). Proprioception of the knee joint. Paradoxical effect of training. Am. J. Physical Med. 63, 175–181.
Barrett, L. F., Quigley, K. S., Bliss-Moreau, E., and Aronson, K. R. (2004). Interoceptive sensitivity and self-reports of emotional experience. J. Personal. Soc. Psychol. 87, 684–697. doi: 10.1037/0022-3514.87.5.684
Batson, G. (2009). Update on proprioception: Considerations for dance education. J. Dance Med. Sci. Offic. Publicat. Int. Assoc. Dance Med. Sci. 13, 35–41.
Berntson, G. G., Gianaros, P. J., and Tsakiris, M. (2018). “Interoception and the autonomic nervous system: Bottom-up meets top-down,” in The interoceptive mind. From homeostasis to awareness, eds M. Tsakiris and H. De Preester (Oxford: Oxford University Press), 3–23.
Boisgontier, M. P., Olivier, I., Chenu, O., and Nougier, V. (2012). Presbypropria: The effects of physiological ageing on proprioceptive control. Age 34, 1179–1194. doi: 10.1007/s11357-011-9300-y
Cacioppo, J. T., Priester, J. R., and Berntson, G. G. (1993). Rudimentary determinants of attitudes: II. Arm flexion and extension have differential effects on attitudes. J. Personal. Soc. Psychol. 65, 5–17. doi: 10.1037/0022-3514.65.1.5
Cameron, O. G. (2002). Visceral Sensory Neuroscience. Interoception. Oxford: Oxford University Press.
Cannon, W. B. (1927). The James-Lange theory of emotions: A critical examination and an alternative theory. Am. J. Psychol. 39, 106–124. doi: 10.2307/1415404
Cannon, W. B. (1931). Again the James-Lange and the thalamic theories of emotion. Psychol. Rev. 38, 281–295. doi: 10.1037/h0072957
Carney, D. R., Cuddy, A. J. C., and Yap, A. J. (2010). Power posing: Brief nonverbal displays affect neuroendocrine levels and risk tolerance. Psychol. Sci. 21, 1363–1368. doi: 10.1177/0956797610383437
Ceunen, E., Van Diest, I., and Vlaeyen, J. W. S. (2013). Accuracy and awareness of perception: Related, yet distinct (commentary on Herbert et al., 2012). Biol. Psychol. 92, 426–427. doi: 10.1016/j.biopsycho.2012.09.012
Ceunen, E., Vlaeyen, J. W. S., and Van Diest, I. (2016). On the origin of interoception. Front. Psychol. 7:743. doi: 10.3389/fpsyg.2016.00743
Chang, B. P., and Lenzenweger, M. F. (2005). Somatosensory processing and schizophrenia liability: Proprioception, exteroceptive sensitivity, and graphesthesia performance in the biological relatives of schizophrenia patients. J. Abnor. Psychol. 114, 85–95. doi: 10.1037/0021-843X.114.1.85
Cullen, K. E. (2004). Sensory signals during active versus passive movement. Curr. Opin. Neurobiol. 14, 698–706. doi: 10.1016/j.conb.2004.10.002
Darwin, C. (1872). The Expression of the Emotions in Man and Animals. South Carolina: CreateSpace Independent Publishing Platform.
Davis, M. (1989). Neural systems involved in fear-potentiated startle. Ann. N Y. Acad. Sci. 563, 165–183. doi: 10.1111/j.1749-6632.1989.tb42197.x
Desmedt, O., Corneille, O., Luminet, O., Murphy, J., Bird, G., and Maurage, P. (2020). Contribution of Time Estimation and Knowledge to Heartbeat Counting Task Performance under Original and Adapted Instructions. Biol. Psychol. 154:107904. doi: 10.1016/j.biopsycho.2020.107904
Desmedt, O., Luminet, O., and Corneille, O. (2018). The heartbeat counting task largely involves non-interoceptive processes: Evidence from both the original and an adapted counting task. Biol. Psychol. 138, 185–188. doi: 10.1016/j.biopsycho.2018.09.004
Domschke, K., Stevens, S., Pfleiderer, B., and Gerlach, A. L. (2010). Interoceptive sensitivity in anxiety and anxiety disorders: An overview and integration of neurobiological findings. Clin. Psychol. Rev. 30, 1–11. doi: 10.1016/j.cpr.2009.08.008
Ehlers, A., Breuer, P., Dohn, D., and Fiegenbaum, W. (1995). Heartbeat perception and panic disorder: Possible explanations for discrepant findings. Behav. Res. Ther. 33, 69–76.
Elangovan, N., Herrmann, A., and Konczak, J. (2014). Assessing Proprioceptive Function: Evaluating Joint Position Matching Methods Against Psychophysical Thresholds. Physical. Ther. 94, 553–561. doi: 10.2522/ptj.20130103
Fairclough, S. H., and Goodwin, L. (2007). The effect of psychological stress and relaxation on interoceptive accuracy: implications for symptom perception. J. Psycho. Res. 62, 289–295. doi: 10.1016/j.jpsychores.2006.10.017
Faul, F., Erdfelder, E., Lang, A.-G., and Buchner, A. (2007). G∗Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 39, 175–191.
Ferentzi, E., Bogdány, T., Szabolcs, Z., Csala, B., Horváth, Á, and Köteles, F. (2018). Multichannel investigation of interoception: Sensitivity is not a generalizable feature. Front. Hum. Neurosci. 12:223. doi: 10.3389/fnhum.2018.00223
Ferentzi, E., Horváth, Á, and Köteles, F. (2019). Do body-related sensations make feel us better? Subjective well-being is associated only with the subjective aspect of interoception. Psychophysiology 56:e13319. doi: 10.1111/psyp.13319
Ferentzi, E., Köteles, F., Csala, B., Drew, R., Tihanyi, B. T., Pulay-Kottlár, G., et al. (2017). What makes sense in our body? Personality and sensory correlates of body awareness and somatosensory amplification. Personal. Individ. Differ. 104, 75–81. doi: 10.1016/j.paid.2016.07.034
Ferentzi, E., Olaru, G., Geiger, M., Vig, L., Köteles, F., and Wilhelm, O. (2020). Examining the Factor Structure and Validity of the Multidimensional Assessment of Interoceptive Awareness. J. Personal. Assess. 0, 1–10. doi: 10.1080/00223891.2020.1813147
Forkmann, T., Scherer, A., Meessen, J., Michal, M., Schächinger, H., Vögele, C., et al. (2016). Making sense of what you sense: Disentangling interoceptive awareness, sensibility and accuracy. Int. J. Psychophysiol. 109, 71–80. doi: 10.1016/j.ijpsycho.2016.09.019
Gao, Q., Ping, X., and Chen, W. (2019). Body Influences on Social Cognition Through Interoception. Front. Psychol. 10:2066. doi: 10.3389/fpsyg.2019.02066
Garfinkel, S. N., and Critchley, H. D. (2013). Interoception, emotion and brain: New insights link internal physiology to social behaviour. Commentary on: ‘Anterior insular cortex mediates bodily sensibility and social anxiety’ by Terasawa et al. (2012). Soc. Cognit. Affect. Neurosci. 8, 231–234. doi: 10.1093/scan/nss140
Garfinkel, S. N., Manassei, M. F., Engels, M., Gould, C., and Critchley, H. D. (2017). An investigation of interoceptive processes across the senses. Biol. Psychol. 129, 371–372. doi: 10.1016/j.biopsycho.2017.08.010
Garfinkel, S. N., Manassei, M. F., Hamilton-Fletcher, G., Bosch, Y. I., den, Critchley, H. D., et al. (2016). Interoceptive dimensions across cardiac and respiratory axes. Philosop. Transact. R. Soc. London 371:20160014. doi: 10.1098/rstb.2016.0014
Garfinkel, S. N., Seth, A. K., Barrett, A. B., Suzuki, K., and Critchley, H. D. (2015a). Knowing your own heart: Distinguishing interoceptive accuracy from interoceptive awareness. Biol. Psychol. 104, 65–74. doi: 10.1016/j.biopsycho.2014.11.004
Garfinkel, S. N., Tiley, C., O’Keeffe, S., Harrison, N. A., Seth, A. K., and Critchley, H. D. (2015b). Discrepancies between dimensions of interoception in autism: Implications for emotion and anxiety. Biol. Psychol. 114, 117–126. doi: 10.1016/j.biopsycho.2015.12.003
Goble, D. J. (2010). Proprioceptive acuity assessment via joint position matching: From basic science to general practice. Physical Ther. 90, 1176–1184. doi: 10.2522/ptj.20090399
Goble, D. J., Aaron, M. B., Warschausky, S., Kaufman, J. N., and Hurvitz, E. A. (2012). The influence of spatial working memory on ipsilateral remembered proprioceptive matching in adults with cerebral palsy. Exp. Brain Res. 223, 259–269. doi: 10.1007/s00221-012-3256-8
Grob, K. R., Kuster, M. S., Higgins, S. A., Lloyd, D. G., and Yata, H. (2002). Lack of correlation between different measurements of proprioception in the knee. J. Bone Joint Surg. 84-B, 614–618. doi: 10.1302/0301-620X.84B4.0840614
Gyollai, A., Simor, P., Koteles, F., and Demetrovics, Z. (2011). Psychometric properties of the Hungarian version of the original and the short form of the Positive and Negative Affect Schedule (PANAS). Neuropsychopharmacol. Hungarica 13, 73–79.
Han, J., Anson, J., Waddington, G., and Adams, R. (2013). Proprioceptive performance of bilateral upper and lower limb joints: Side-general and site-specific effects. Exp. Brain Res. 226, 313–323. doi: 10.1007/s00221-013-3437-0
Han, J., Waddington, G., Adams, R., Anson, J., and Liu, Y. (2016). Assessing proprioception: A critical review of methods. J. Sport Health Sci. 5, 80–90. doi: 10.1016/j.jshs.2014.10.004
Hart, N., McGowan, J., Minati, L., and Critchley, H. D. (2013). Emotional regulation and bodily sensation: Interoceptive awareness is intact in borderline personality disorder. J. Personal. Dis. 27, 506–518. doi: 10.1521/pedi_2012_26_049
Herbert, B. M., Pollatos, O., and Schandry, R. (2007). Interoceptive sensitivity and emotion processing: An EEG study. Int. J. Psychophysiol. 65, 214–227. doi: 10.1016/j.ijpsycho.2007.04.007
Herbert, B. M., Pollatos, O., Flor, H., Enck, P., and Schandry, R. (2010). Cardiac awareness and autonomic cardiac reactivity during emotional picture viewing and mental stress. Psychophysiology 47, 342–354. doi: 10.1111/j.1469-8986.2009.00931.x
Horváth, Á, Ferentzi, E., and Köteles, F. (2019). Proprioceptive accuracy is not associated with self-reported body awareness, body competence, and affect. Physiol. Int. 106, 347–354.
JASP Team (2019). JASP(Version 0.11) [Computer software] (0.11) [Computer software]. Amsterdam: University of Amsterdam. Available online at: https://jasp-stats.org/
Jha, P., Ahamad, I., Khurana, S., Ali, K., Verma, S., and Kumar, T. (2017). Proprioception: An Evidence Based Narrative Review. Res. Inves. Sports Med. 1:RISM.000506.
Jong, A., de, Kilbreath, S. L., Refshauge, K. M., and Adams, R. (2005). Performance in Different Proprioceptive Tests Does Not Correlate in Ankles With Recurrent Sprain. Arch. Phys. Med. Rehabil. 86, 2101–2105. doi: 10.1016/j.apmr.2005.05.015
Kanji, N., White, A., and Ernst, E. (2006). Autogenic training to reduce anxiety in nursing students: Randomized controlled trial. J. Adv. Nurs. 53, 729–735. doi: 10.1111/j.1365-2648.2006.03779.x
Kerber, K. W., and Coles, M. G. (1978). The role of perceived physiological activity in affective judgments. J. Exp. Soc. Psychol. 14, 419–433. doi: 10.1016/0022-1031(78)90039-2
Köteles, F. (2014). A Testi Tudatosság Kérdõív magyar verziójának (BAQ-H) vizsgálata jógázó és fiatal felnõtt kontroll mintán. Mentálhigiéné És Pszichoszomatika 15, 373–391. doi: 10.1556/Mental.15.2014.4.4
Köteles, F., Éliás, I., Szabolcs, Z., Körmendi, J., Ferentzi, E., and Szemerszky, R. (2020a). Accuracy of reproduction of physical training load is not associated with resting heartbeat perception in healthy individuals. Biol. Psychol. 150:107831. doi: 10.1016/j.biopsycho.2019.107831
Köteles, F., Teufel, B., Körmendi, J., Ferentzi, E., and Szemerszky, R. (2020b). Cardioceptive accuracy is associated with arousal but not with valence and perceived exertion under physical load. Psychophysiology 57:e13620. doi: 10.1111/psyp.13620
Krantz, G., Forsman, M., and Lundberg, U. (2004). Consistency in physiological stress responses and electromyographic activity during induced stress exposure in women and men. Integrat. Physiol. Behav. Sci. 39, 105–118. doi: 10.1007/BF02734276
Lacey, B. C., and Lacey, J. I. (1978). Two-way communication between the heart and the brain. Significance of time within the cardiac cycle. Am. Psychol. 33, 99–113.
Lange, C. G. (1885). Om Sindsbevaegelser et Psyko-Fysiologisk Studie. Copenhagen: University of Copenhagen.
LeDoux, J. E. (1990). “Information flow from sensation to emotion plasticity in the neural computation of stimulus value,” in Learning and computational neuroscience: Foundations of adaptive networks, eds M. Gabriel and J. Moore (Cambridge: MIT Press), 3–52.
Leventhal, D. B., Schuck, J. R., Clemons, J. T., and Cox, M. (1982). Proprioception in schizophrenia. J. Nervous Mental Dis. 170, 21–26.
Li, L., Ji, Z.-Q., Li, Y.-X., and Liu, W.-T. (2016). Correlation study of knee joint proprioception test results using common test methods. J. Phys. Ther. Sci. 28, 478–482. doi: 10.1589/jpts.28.478
Lox, C. L., Martin Ginis, K. A., and Petruzzello, S. J. (2010). The Psychology of Exercise. Integrating Theory and Practice, 3rd Edn. Arizona: Holcomb Hathaway.
Ludwick-Rosenthal, R., and Neufeld, R. W. (1985). Heart beat interoception: A study of individual differences. Int. J. Psychophysiol. 3, 57–65.
Luijcks, R., Hermens, H. J., Bodar, L., Vossen, C. J., Van Os, J., and Lousberg, R. (2014). Experimentally Induced Stress Validated by EMG Activity. PLoS One 9:95215. doi: 10.1371/journal.pone.0095215
Lundberg, U., Kadefors, R., Melin, B., Palmerud, G., Hassmén, P., Engström, M., et al. (1994). Psychophysiological stress and emg activity of the trapezius muscle. Int. J. Behav. Med. 1, 354–370. doi: 10.1207/s15327558ijbm0104_5
Meessen, J., Mainz, V., Gauggel, S., Volz-Sidiropoulou, E., Sütterlin, S., and Forkmann, T. (2016). The relationship between interoception and metacognition. J. Psychophysiol. 30, 76–86. doi: 10.1027/0269-8803/a000157
Mehling, W. E., Price, C., Daubenmier, J. J., Acree, M., Bartmess, E., and Stewart, A. (2012). The Multidimensional Assessment of Interoceptive Awareness (MAIA). PLoS One 7:e48230. doi: 10.1371/journal.pone.0048230
Miall, R. C., and Wolpert, D. M. (1996). Forward Models for Physiological Motor Control. Neural Netw. Offic. J. Int. Neural Netw. Soc. 9, 1265–1279.
Michal, M., Reuchlein, B., Adler, J., Reiner, I., Beutel, M. E., Vögele, C., et al. (2014). Striking discrepancy of anomalous body experiences with normal interoceptive accuracy in depersonalization-derealization disorder. PLoS One 9:e89823. doi: 10.1371/journal.pone.0089823
Miller, L. C., Murphy, R., and Buss, A. H. (1981). Consciousness of body: Private and public. J. Personal. Soc. Psychol. 41, 397–406. doi: 10.1037/0022-3514.41.2.397
Moors, A. (2009). Theories of emotion causation: A review. Cognit. Emot. 23, 625–662. doi: 10.1080/02699930802645739
Neumann, R., and Strack, F. (2000). Approach and avoidance: The influence of proprioceptive and exteroceptive cues on encoding of affective information. J. Personal. Soc. Psychol. 79, 39–48. doi: 10.1037/0022-3514.79.1.39
Niespodziński, B., Kochanowicz, A., Mieszkowski, J., Piskorska, E., and Żychowska, M. (2018). Relationship between Joint Position Sense, Force Sense, and Muscle Strength and the Impact of Gymnastic Training on Proprioception. BioMed. Res. Int. 2018, 1–10. doi: 10.1155/2018/5353242
Oatley, K., and Johnson-laird, P. N. (1987). Towards a Cognitive Theory of Emotions. Cognit. Emot. 1, 29–50. doi: 10.1080/02699938708408362
O’Brien, W. H., Reid, G. J., and Jones, K. R. (1998). Differences in heartbeat awareness among males with higher and lower levels of systolic blood pressure. Int. J. Psychophysiol. 29, 53–63. doi: 10.1016/S0167-8760(98)00004-X
Panksepp, J. (1982). Toward a general psychobiological theory of emotions. Behav. Brain Sci. 5, 407–467. doi: 10.1017/S0140525X00012759
Panksepp, J. (1991). “Affective neurocience: A conceptual framework for the neurobiological study of emotions,” in International reviews of emotion research, ed. K. Strongman (New Jersey: Wiley), 59–99.
Parkinson, B. (1985). Emotional effects of false autonomic feedback. Psychol. Bull. 98, 471–494. doi: 10.1037/h0031873
Pennebaker, J. W., and Hoover, C. W. (1984). Visceral perception versus visceral detection: Disentangling methods and assumptions. Biofeedback Self Regul. 9, 339–352. doi: 10.1007/BF00998977
Phillips, G. C., Jones, G. E., Rieger, E. J., and Snell, J. B. (1999). Effects of the presentation of false heart-rate feedback on the performance of two common heartbeat-detection tasks. Psychophysiology 36, 504–510.
Pollatos, O., Herbert, B. M., Kaufmann, C., Auer, D. P., and Schandry, R. (2007a). Interoceptive awareness, anxiety and cardiovascular reactivity to isometric exercise. Int. J. Psychophysiol. 65, 167–173. doi: 10.1016/j.ijpsycho.2007.03.005
Pollatos, O., Herbert, B. M., Matthias, E., and Schandry, R. (2007b). Heart rate response after emotional picture presentation is modulated by interoceptive awareness. Int. J. Psychophysiol. 63, 117–124. doi: 10.1016/j.ijpsycho.2006.09.003
Pollatos, O., Kirsch, W., and Schandry, R. (2005). On the relationship between interoceptive awareness, emotional experience, and brain processes. Brain Res. Cognit. Brain Res. 25, 948–962. doi: 10.1016/j.cogbrainres.2005.09.019
Porges, S. W. (1993). Body Perception Questionnaire (Laboratory of Developmental Assessment). Maryland: University of Maryland.
Ranehill, E., Dreber, A., Johannesson, M., Leiberg, S., Sul, S., and Weber, R. A. (2015). Assessing the Robustness of Power Posing: No Effect on Hormones and Risk Tolerance in a Large Sample of Men and Women. Psychol. Sci. 26, 653–656. doi: 10.1177/0956797614553946
Rausch, S. M., Gramling, S. E., and Auerbach, S. M. (2006). Effects of a single session of large-group meditation and progressive muscle relaxation training on stress reduction, reactivity, and recovery. Int. J. Stress Manage. 13, 273–290. doi: 10.1037/1072-5245.13.3.273
Ring, C., and Brener, J. (2018). Heartbeat counting is unrelated to heartbeat detection: A comparison of methods to quantify interoception. Psychophysiology 55:e13084. doi: 10.1111/psyp.13084
Ring, C., Brener, J., Knapp, K., and Mailloux, J. (2015). Effects of heartbeat feedback on beliefs about heart rate and heartbeat counting: A cautionary tale about interoceptive awareness. Biol. Psychol. 104, 193–198. doi: 10.1016/j.biopsycho.2014.12.010
Ritzler, B. (1977). Proprioception and schizophrenia: A replication study with nonschizophrenic patient controls. J. Abnor. Psychol. 86, 501–509. doi: 10.1037/0021-843X.86.5.501
Ritzler, B., and Rosenbaum, G. (1974). Proprioception in schizophrenics and normals: Effects of stimulus intensity and interstimulus interval. J. Abnor. Psychol. 83, 106–111.
Rosenbaum, G., Cohen, B. D., Luby, E. D., Gottlieb, J. S., and Yelen, D. (1959). Comparison of sernyl with other drugs: Simulation of schizophrenic performance with sernyl, LSD-25, and amobarbital (amytal) sodium. I. Attention, motor function, and proprioception. AMA Arch. General Psychiatry 1, 651–656. doi: 10.1001/archpsyc.1959.03590060113013
Rosenbaum, G., Flenning, F., and Rosen, H. (1965). Effects of weight intensity on discrimination thresholds of normals and schizophrenics. J. Abnor. Psychol. 70, 446–450.
Schaefer, M., Egloff, B., and Witthöft, M. (2012). Is interoceptive awareness really altered in somatoform disorders? Testing competing theories with two paradigms of heartbeat perception. J. Abnor. Psychol. 121, 719–724. doi: 10.1037/a0028509
Schandry, R. (1981). Heart beat perception and emotional experience. Psychophysiology 18, 483–488. doi: 10.1111/j.1469-8986.1981.tb02486.x
Schandry, R., Bestler, M., and Montoya, P. (1993). On the relation between cardiodynamics and heartbeat perception. Psychophysiol. 30, 467–474. doi: 10.1111/j.1469-8986.1993.tb02070.x
Scholz, O. B., Ott, R., and Sarnoch, H. (2001). Proprioception in somatoform disorders. Behav. Res. Ther. 39, 1429–1438. doi: 10.1016/S0005-7967(00)00108-X
Schulz, A., Lass-Hennemann, J., Sütterlin, S., Schächinger, H., and Vögele, C. (2013). Cold pressor stress induces opposite effects on cardioceptive accuracy dependent on assessment paradigm. Biol. Psychol. 93, 167–174. doi: 10.1016/j.biopsycho.2013.01.007
Schutz, R. W., and Roy, E. A. (1973). Absolute Error. J. Motor Behav. 5, 141–153. doi: 10.1080/00222895.1973.10734959
Şenol, D., Uçar, C., Çay, M., Özbað, D., Canbolat, M., and Y∣ld∣z, S. (2018). The effect of stress-induced cortisol increase on the sense of ankle proprioception. Turk. J. Phys. Med. Rehabil. 65, 124–131. doi: 10.5606/tftrd.2019.2457
Shafir, T., Tsachor, R. P., and Welch, K. B. (2015). Emotion Regulation through Movement: Unique Sets of Movement Characteristics are Associated with and Enhance Basic Emotions. Front. Psychol. 6:2030. doi: 10.3389/fpsyg.2015.02030
Shields, S. A., Mallory, M. E., and Simon, A. (1989). The Body Awareness Questionnaire: Reliability and validity. J. Personal. Assess. 53:802. doi: 10.1207/s15327752jpa5304_16
Simmons, J. P., and Simonsohn, U. (2017). Power Posing: P-Curving the Evidence. Psychol. Sci. 28, 687–693. doi: 10.1177/0956797616658563
Smith, R., and Lane, R. D. (2015). The neural basis of one’s own conscious and unconscious emotional states. Neurosci. Biobehav. Rev. 57(Suppl. C), 1–29. doi: 10.1016/j.neubiorev.2015.08.003
Thornton, E. W., and Hagan, P. J. (1976). A failure to explain the effects of false heart-rate feedback on affect by induced changes in physiological response. Br. J. Psychol. 67, 359–365. doi: 10.1111/j.2044-8295.1976.tb01522.x
Tomkins, S. S. (1962). Affect, imagery, consciousness. Volume I: The positive affects. Berlin: Springer.
Tomkins, S. S. (1981). The role of facial response in the experience of emotion: A reply to Tourangeau and Ellsworth. J. Personal. Soc. Psychol. 40, 355–357. doi: 10.1037/0022-3514.40.2.355
Tsay, A., Allen, T. J., Proske, U., and Giummarra, M. J. (2015). Sensing the body in chronic pain: A review of psychophysical studies implicating altered body representation. Neurosci. Biobehav. Rev. 52, 221–232. doi: 10.1016/j.neubiorev.2015.03.004
Ulus, Y., Akyol, Y., Tander, B., Bilgici, A., and Kuru, Ö (2013). Knee proprioception and balance in turkish women with and without fibromyalgia syndrome. Türkiye Fiziksel Tıp ve Rehabilitasyon Dergisi 59, 128–132. doi: 10.4274/tftr.75428
Valins, S. (1966). Cognitive effects of false heart-rate feedback. J. Personal. Soc. Psychol. 4, 400–408. doi: 10.1037/h0023791
Waddington, G., and Adams, R. (1999). Ability to discriminate movements at the ankle and knee is joint specific. Perceptzral Motor Skills 89, 1037–1041.
Wahlström, J., Hagberg, M., Johnson, P., Svensson, J., and Rempel, D. (2002). Influence of time pressure and verbal provocation on physiological and psychological reactions during work with a computer mouse. Eur. J. Appl. Physiol. 87, 257–263. doi: 10.1007/s00421-002-0611-7
Watson, D. (1988). Intraindividual and interindividual analyses of positive and negative affect: Their relation to health complaints, perceived stress, and daily activities. J. Personal. Soc. Psychol. 54, 1020–1030. doi: 10.1037//0022-3514.54.6.1020
Watson, D., and Clark, L. A. (1994). The PANAS-X: Manual for the Positive and Negative Affect Schedule-Expanded Form. Iowa: The University of Iowa.
Weisz, J., Balázs, L., and Ádám, G. (1988). The influence of self-focused attention on heartbeat perception. Psychophysiology 25, 193–199. doi: 10.1111/j.1469-8986.1988.tb00987.x
Werner, N. S., Kerschreiter, R., Kindermann, N. K., and Duschek, S. (2013). Interoceptive awareness as a moderator of affective responses to social exclusion. J. Psychophysiol. 27, 39–50. doi: 10.1027/0269-8803/a000086
Wetzels, R., and Wagenmakers, E.-J. (2012). A default Bayesian hypothesis test for correlations and partial correlations. Psychonomic Bull. Rev. 19, 1057–1064. doi: 10.3758/s13423-012-0295-x
Wiens, S., Mezzacappa, E. S., and Katkin, E. S. (2000). Heartbeat detection and the experience of emotions. Cognit. Emot. 14, 417–427. doi: 10.1080/026999300378905
Woll, S. B., and McFall, M. E. (1979). The effects of false feedback on attributed arousal and rated attractiveness in female subjects. J. Personal. 47, 214–229. doi: 10.1111/j.1467-6494.1979.tb00200.x
Yang, N., Waddington, G., Adams, R., and Han, J. (2020). Joint position reproduction and joint position discrimination at the ankle are not related. Somatosensory Motor Res. 37, 97–105. doi: 10.1080/08990220.2020.1746638
Keywords: proprioception, cardioception, interoceptive accuracy, interoceptive sensibility, affect, body awareness
Citation: Horváth Á, Vig L, Ferentzi E and Köteles F (2021) Cardiac and Proprioceptive Accuracy Are Not Related to Body Awareness, Perceived Body Competence, and Affect. Front. Psychol. 11:575574. doi: 10.3389/fpsyg.2020.575574
Received: 23 June 2020; Accepted: 22 December 2020;
Published: 14 January 2021.
Edited by:
Simona Raimo, University of Campania Luigi Vanvitelli, ItalyReviewed by:
Vivien Ainley, Royal Holloway, University of London, United KingdomAnnika Petra Christine Lutz, University of Luxembourg, Luxembourg
Copyright © 2021 Horváth, Vig, Ferentzi and Köteles. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ferenc Köteles, a290ZWxlcy5mZXJlbmNAcHBrLmVsdGUuaHU=