 Lubna Anis
Lubna Anis Grace Perez2
Grace Perez2 Karen M. Benzies
Karen M. Benzies Nicole Letourneau
Nicole Letourneau
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol. , 16 December 2020
Sec. Quantitative Psychology and Measurement
Volume 11 - 2020 | https://doi.org/10.3389/fpsyg.2020.574719
Reflective function (RF) is defined as an individual’s ability to understand human behavior in terms of underlying mental states including thoughts, feelings, desires, beliefs, and intentions. More specifically, the capacity of parents to keep their child’s mental states in mind is referred to as parental RF. RF has been linked to adult mental health and parental RF to children’s mental health and development. The gold standard measure of RF is the interview-based Reflective Functioning Scale (RFS) applied to the Parent Development Interview (PDI) or Adult Attachment Interview (AAI), which while well validated, is time-and labor-intensive to administer. Given the increasing need for reliable, valid, and rapid RF assessment in wide-ranging settings, two alternative measures were considered including the Reflective Function Questionnaire (RFQ) and Parental Reflective Function Questionnaire (PRFQ). We determined the convergent validity of these measures in comparison with the PDI-rated RFS. A sample of mothers and fathers (n = 150) was drawn from a sub-study of the ongoing Alberta Pregnancy Outcomes and Nutrition (APrON) longitudinal cohort when their children were 42–60 months of age. Pearson correlations and multiple linear regression was conducted, followed by splitting the sample to compute Cohen’s kappas measures of agreement. Two subscales of the PRFQ correlated significantly (p < 0.05) with the gold standard PDI-rated RFS, providing evidence for convergent validity. As a brief multidimensional measure of parental RF, the PRFQ offers an alternative for measurement of RF in large-scale studies of parental development and child health.
In recent years, the concept of Reflective Function (RF) has gained attention in research and clinical practice in both health and social sciences (Fonagy et al., 2002; Ordway et al., 2014; Antonsen et al., 2016). RF is defined as an individual’s capacity to perceive human behavior considering underlying mental states including thoughts, feelings, desires, and intentions (Fonagy and Target, 1997; Midgely and Vrouva, 2013). Early work describing RF referred to adults’ ability to envision mental states in themselves and in others (Fonagy et al., 1991a, b). Subsequently, researchers elaborated on this work to particularly address the capacity of parents to understand their children’s mental states to regulate their behavior, referred to as parental RF (Fonagy and Target, 1998; Slade, 2005). The capacity for being reflective is thought to be fundamental to humans’ ability to navigate the social world (Bateman and Fonagy, 2012). Impairments in RF have been associated with poor mental health such as depression (Lemma et al., 2011; Luyten et al., 2012a; Ekeblad et al., 2016) and borderline personality disorder (Fonagy and Bateman, 2007, 2008; Fischer-Kern et al., 2015). Reduced parental RF has also been associated with poor child development (Ensink et al., 2017; Borelli et al., 2019; Morosan et al., 2020).
Many measures are currently available to assess RF (Luyten et al., 2012b; Schiborr et al., 2013); however, the only well-validated gold standard measure that directly assesses RF is the interview-based Reflective Functioning Scale (RFS; Fonagy et al., 1998), typically applied to the Adult Attachment Interview (AAI; George et al., 1996) or the Parent Development Interview (PDI; Slade et al., 2004; Sleed et al., 2020). This interview-based measure of RF yields clinically rich data from which a RF score may be determined (Bouchard et al., 2008), but interviews often take 1–3 h to administer, followed by 2–4 of coding by highly trained professionals (De Roo et al., 2019). Therefore, there is a need for more time-saving and cost-efficient tools suitable for use in large-scale studies or in community settings. Two such measures include the Reflective Function Questionnaire (RFQ; Fonagy et al., 2016) and Parental Reflective Function Questionnaire (PRFQ; Luyten et al., 2017a, b), which exhibit good construct validity, internal consistency, and reliability (Rutherford et al., 2015; Fonagy et al., 2016; Luyten et al., 2017a). The RFQ has been compared with the gold standard RFS applied to the PDI in only one study with mixed results (Handeland et al., 2019). However, the PRFQ has never been compared with the gold standard RFS to our knowledge. Thus, the purpose of the current investigation was to determine the convergent validity, that is, the degree to which the RFQ and PRFQ correlate with the gold standard RFS, applied to the PDI (Karp et al., 2018).
Fonagy et al. (1991a, b) from the University College London were the first to introduce the construct of RF, proposing that RF is the operationalization of mentalization theory. Mentalization refers to the capacity to evoke, understand, and reflect on one’s own and others’ state(s) of mind while having insight into what one is (and others are) feeling and why. Fonagy et al. (1991a) proposed that the ability to mentalize develops as a function of the parent’s accustomed reading and regulating of their child’s internal state from the child’s perspective. This capacity enables the parent to understand their child as separate from the parent with mental states that are distinct from those of the parent and others (Winnicott, 1962; Fonagy and Target, 1998). Building on Fonagy’s work, Slade (2005) formally introduced the concept of parental RF to include parental ability to mentalize about themselves and their child. Parental RF is distinct from general RF as the concept of parental RF is more parent–child relationship-specific (Fonagy and Target, 1998; Slade, 2005). Although general RF and parental RF may be expected to be correlated, these two capacities may not be similar (Fonagy et al., 2016) and a correlation of r = 0.50 has been reported between general RF when scored from the AAI (George et al., 1996) and parental RF as scored on the PDI (Slade et al., 2004; Steele et al., 2008; Sleed et al., 2020).
There is growing consensus that RF is a developmental attainment that is sensitive to the effect of early interactions with primary caregivers (Fonagy and Target, 1997; Fonagy et al., 2003; Steele et al., 2008). Mothers’ disposition to reflect on and elaborate on about mental states is linked with their children’s social-emotional development (Laible, 2004; Garner et al., 2008; Meins et al., 2013). The importance of maternal RF for children’s developmental outcomes can be attributed to its main role in the transmission of attachment security from the mother to the child (Slade et al., 2005; Steele et al., 2008). Fonagy et al. (2002) proposed a developmental model of RF, suggesting that awareness of mental states develops in the context of early attachment relationships, in which children learn to identify and reflect their own affects through observing the parent’s responsiveness in their subjective experience. Also, parental ability to imagine the subjective experience of their developing children is thought to expedite the development of children’s self-regulation, along with representation of and communication about affects (Fonagy et al., 2002). Empirically, parental RF is associated with infant attachment (Stacks et al., 2014; Ensink et al., 2016) along with child and adolescent RF (Ensink et al., 2016; Duval et al., 2018). Furthermore, parental RF focused intervention demonstrated improvement in maternal RF in a sample of incarcerated women with custody retention issues (Baradon et al., 2008; Sleed et al., 2013).
The RFS is the primary psychometric tool used to measure capacity for RF (Fonagy et al., 1998). An elaborate coding procedure is required based on the narratives from AAI (George et al., 1996), and PDI (Slade et al., 2004; Sleed et al., 2020). Trained coders provide a global score on an 11-point scale that ranges from antireflective to exceptionally reflective. The RFS exhibits good inter-rater reliability after training (Fonagy et al., 1998), with Pearson correlations ranging between 0.86 and 0.91 (Bouchard et al., 2008), as well as an intra-class correlation coefficient of 0.86 (Levy et al., 2006). The RFS has been operationalized into two overlapping, yet different, measurement constructs, i.e., adult/self and parental RF. Whereas adult/self RF is principally rated from the AAI and spotlights adults’ ability to reflect on their childhood experiences with parental figures in mentalizing terms, parental RF has a more specific focus on parental capacity of the self/adult to mentalize about and reflect on their relationship with their children (principally rated from interviews on parenthood) (Slade et al., 2003; Slade, 2005).
The requirement for time-consuming interviews, specialist training, and costly human resources hamper research efforts and limit the RFS’s utilization outside of research settings, which is unfortunate, considering the affluent clinical potential implicit in the assessment of RF. The RFS has also been criticized for generating only global scores for overall, adult/parent and child RF, which may fail to address the complexity of the mentalizing process (Taubner et al., 2013). In seeking other options, Schiborr et al. (2013) identified different measurement approaches to assessing RF-related concepts. These approaches include assessments of insightfulness (Bretherton et al., 1989; Oppenheim and Koren-Karie, 2009), meta-emotional representation (Gottman et al., 1996), maternal mind-mindedness (the propensity to attribute meaning to the child) (Meins, 1998), the use of mental-state terms (Ruffman et al., 2002), mental-state language (Schechter et al., 2006), and mental-state references (Slaughter et al., 2008). Again, their time- and cost-intensive nature and less direct focus on RF hampers their use in large-scale studies and routine clinical applications (Fonagy et al., 2016; Handeland et al., 2019).
There is a need for a short, self-report questionnaire to measure reflective function as an aspect of parenting for use with mothers and fathers. This tool would be a valuable screening measure in the context of time- and resource-limited child health services, and for population-based research. Attempts to develop such measures include the RFQ (Luyten et al., 2012a) and the PRFQ (Fonagy et al., 2016). The RFQ exhibits good internal consistency reliability (α = 0.70 or greater). Convergent validity has been established between the two subscales of RFQ (RFQ Certainty and RFQ Uncertainty subscales) and allied concepts of alexithymia [with RFQ uncertainty, Spearman’s ρ(199) = 0.66, with RFQ Certainty, Spearman’s ρ(199) = −0.46, both ps < 0.001], empathy [with RFQ Uncertainty, Spearman’s ρ(209) = −0.37, and with RFQ Certainty, Spearman’s ρ(209) = 0.28], and mindfulness [RFQ Uncertainty, Spearman’s ρ(204) = −0.56, and with RFQ Certainty (Spearman’s ρ(204) = 0.39, both ps < 0.001)] (Fonagy et al., 2016). The test–retest reliability and internal consistency of the subscales were found to be satisfactory to excellent; the subscales were unrelated to demographic characteristics (Fonagy et al., 2016). Also, the PRFQ demonstrates good internal consistency for all subscales; Pre-mentalizing (α = 0.70), Interest and Curiosity (α = 0.74), and Certainty in Mental States (α = 0.82) (Luyten et al., 2017b).
To date, the validity and reliability of the RFQ and the PRFQ have been determined mostly in clinical, but not normative or non-clinical samples (Luyten et al., 2012a; Badoud et al., 2015; Fonagy et al., 2016; Morandotti et al., 2018). Moreover, the distinction between mothers’ and fathers’ capacity for RF have been examined predominately in clinical samples (Fonagy et al., 1991b; Cooke et al., 2017), with fathers’ RF given less attention. To develop a better understanding of parental RF of mothers and fathers, further research with a community sample is needed. The purpose of the current study is to assess the psychometric properties of the RFQ (Luyten et al., 2012b) and PRFQ (Fonagy et al., 2016) by determining the extent to which they correlate with the gold standard RFS applied to the PDI to establish convergent validity. Given the emphasis of both the PDI and PRFQ on parenting, we hypothesized that the PDI-rated RFS scores would correlate more strongly with the PRFQ than the RFQ.
Mothers and fathers took part in a follow-up sub-study of their 3.5–5 years old children, enrolled in the Alberta Pregnancy Outcomes and Nutrition (APrON) longitudinal cohort study (Kaplan et al., 2014). The follow-up focused on parental RF, parent–child interaction quality, attachment, and child development in preschoolers and data were collected at clinic visits at the regional child development center by trained research assistants. Parents took part in a process of informed consent at enrollment in both the APrON study and follow-up sub-study. Honoraria were provided to compensate families for the burden of participating in the sub-study.
Between 2011 and 2012, mothers were enrolled via maternity, ultrasound, and obstetrics clinics and media advertisements (Manca et al., 2013; Kaplan et al., 2014). Pregnant women were enrolled after 27 weeks gestation; they were over 16 years of age and English speakers. Mothers who were known or reported illicit drug users were ineligible. At enrollment, fathers were defined as males who self-reported to be the child’s father. At the 3.5–5 years follow-up clinic visit, mothers and fathers were recruited and enrolled in the present sub-study based on the following criteria: (a) child was in the target age-range of 60 months of age or less, i.e., preschooler; (b) family resided in the city where research was being conducted; (c) mother and father were in co-parenting relationship. To elaborate, participating fathers were expected to report being in a co-parenting relationship with the child’s mother, which meant engaged in day-to-day decision making about the child, but not necessarily co-habiting. Parental marital status was recorded. Both parents signed consents to participate in the follow-up. Families with a child who had a genetic disorder characterized by an intellectual or motor disability were excluded from this follow-up. Families were recruited until complete data were obtained on 75 mother–father pairs.
At the 3.5–5 years visit, to characterize the sample, we collected data on parents’ demographic and descriptive characteristics (e.g., mothers’ and fathers’ ethnicity, education, income, and marital status) and stressors (i.e., depression, addictions, adverse childhood experiences) which might affect RF, from surveys completed at clinic visits or sent in by mail. Trained interviewers, the authors LA and MH, conducted the PDI semi-structured interview (Slade et al., 2004) to assess parents’ RF and participants completed the PRFQ (Fonagy et al., 2016) and RFQ (Luyten et al., 2012a).
To determine descriptive statistics of the sample, we assessed depression with the Edinburgh Postnatal Depression Scale (EPDS; Cox et al., 1987; Cox et al., 2014), addictions with the Alcohol, Smoking, and Substance Involvement Screening Test questionnaire (ASSIST; World Health Organization Assist Working Group, 2002) and childhood adversities with the Adverse Childhood Experiences (ACE; Felitti et al., 1998) questionnaire. The EPDS is a 10-item self-report questionnaire that measures depression with specificity of 67.7%, and sensitivity of 66.7–69% (Cox et al., 1987). A cut-off point of ≥ 13 typically indicates greater likelihood of major depressive disorder (Khalifa et al., 2015). The ASSIST questionnaire measures drug addiction and dependence on alcohol, cannabis, cocaine, amphetamine, sedatives or sleeping pills, and other drugs (inhalants, hallucinogens, opioids, etc.) over the lifetime. The ASSIST questionnaire exhibits high internal consistency and validity (construct, concurrent, and discriminant) (Humeniuk and Ali, 2006). ASSIST scores three or less (10 for alcohol) indicate a lower risk of problems associated with the use of the substance involved (World Health Organization Assist Working Group, 2002). The ACE questionnaire is a 10-item self-report measure used to measure the association between multiple types of abuse experienced before age 18 years and various types of health outcomes (Felitti et al., 1998). Murphy et al. (2014) determined excellent internal consistency (α = 0.88) and validity of the ACE Questionnaire.
The PDI is a 20-item semi-structured interview used to examine parents’ representations of their child in the context of the parent–child relationship. Conducted in separate interviews with each parent, the PDI takes approximately 1 h to complete. This narrative was audio-recorded and transcribed for coding by RFS-trained coders (Fonagy et al., 1998). Applying the RFS coding scheme to the PDI is designed to measure a person’s capacity to reflect on his/her own as well as others’ mental states from the narrative depictions of behavior and reflections of self and others in relational or mutual contexts. Passages in the interview are scored on an 11-point scale ranging from negative or antireflective RF (−1 = low RF) to full or exceptional RF (9 = high RF) based on exhibition of criteria such as awareness and identification of one’s own and other’s mental states, the recognition of limitations to reflect on and ability to demonstrate awareness of diverse perspectives (Slade et al., 2004). RF scores are generated in 3 subscales: PDI-rated RFS Self score, PDI-rated RFS Child score and PDI-rated RFS Total score (Slade et al., 2004). Scores of 5 or above indicate higher parental RF (Slade et al., 2005), while scores of 4 or less indicate lower parental RF (Kelly et al., 2005; Levy et al., 2006; Taubner et al., 2013).
Fonagy’s 11-point RFS has acceptable reliability and validity (Bouchard et al., 2008). In our study, author MH coded 90 interviews and a master coder/trainer from The New School University, NYC, United States coded 60 interviews. To assess inter-rater reliability, the PDI-rated RFS scores were grouped into two categories with higher RF > 3 and lower RF ≤ 3, based on the original scale rating of −1 to +9 and based on the average RF score of 3 in our sample. Coder agreement was assessed on 10% (n = 15) of PDI’s double coded for RF by author MH and the master RF coder. They achieved > 80% agreement overall, with 86% for PDI-rated RFS Total scores and PDI-rated RFS Self scores and 80% for the PDI-rated RFS Child scores.
The most recent version of the RFQ is an 8-item self-reported questionnaire developed to capture RF in general. It takes 3 min to administer. The questionnaire consists of two subscales including: RFQ Certainty and RFQ Uncertainty about mental states. Responses are rated on a 7-point Likert scale which contains answers ranging from 1 to 7 (Strongly Agree). The RFQ Certainty subscale measures the extent to which a person is certain about mental states and is assessed by how much they disagree with statements such as “People’s thoughts are a mystery to me.” The 7-point item is rescored (3, 2, 1, 0, 0, 0, 0 with 3 = disagree strongly) in such a way that agreement to any degree (or a neutral response) demonstrates more optimal mentalizing (awareness of the opaqueness of mental states), and strong disagreement reflects hyper-mentalizing. With the RFQ Uncertainty subscale, uncertainty about mental states is assessed by the degree to which a person agrees with statements such as “Sometimes I do things without really knowing why” and is rescored (0, 0, 0, 0, 1, 2, 3; with 3 = agree strongly). High scores represent hypomentalizing, and lower scores represent more optimal mentalizing (Cucchi et al., 2018; Handeland et al., 2019). Scores range from 0 to 3. The RFQ exhibits good reliability and validity. Currently, the RFQ has no well-established clinical cut-offs for its subscales (Peter Fonagy, personal communication, March 27, 2020). Cronbach alpha coefficients for our sample are reported in Table 4.
The most recent version of the PRFQ is an 18-item self-reported questionnaire that assesses parental RF and takes 5 min to administer. It includes items related to parental interest and curiosity in their child’s mental states and how these mental states may have an impact on behavior. Luyten et al. (2017b) developed three subscales to capture key features of parental RF including: (a) Pre-mentalizing subscale to assess non-mentalizing modes specific to parents with maladaptation in RF (e.g., inability to dive into the subjective experiences of the child), (b) Certainty in Mental States subscale to examine the capacity to identify and understand the opaqueness of mental states, and (c) Interest and Curiosity subscale that relates to parental interest and curiosity in mental states (Slade, 2005; Slade et al., 2007; Steele et al., 2008). The subscales were identified by exploratory factor and verified by confirmatory factor analysis (Rutherford et al., 2015). Each subscale consists of 6 items and each item is rated on a 7-point Likert scale. Items #11 and #16 are reverse coded and then the mean is calculated for the six items (University College London, 2020). According to the questionnaire developers (Luyten et al., 2017b), items were created based on descriptions and exemplars in the RF manuals for the AAI (Fonagy et al., 1998) and PDI (Slade et al., 2007). As shown, the PRFQ has good internal consistency. Scores from each sub-scale range from 1 to 7. Cronbach’s alpha coefficients for our sample are presented in Table 4.
The PRFQ has no well-established clinical cut-offs for its subscales (Luyten, personal communication, March 27, 2020). For the PRFQ Pre-mentalizing subscale, higher scores indicate lower levels of parental RF (Luyten et al., 2017a; Pazzagli et al., 2018). For the PRFQ Certainty in Mental States and Interest and Curiosity subscales, scoring to predict high or low scores was less clear, with the literature referring to either: (a) high scores indicating high RF, or (b) both low and very high scores indicating lower RF. In other words, average levels of both PRFQ Certainty in Mental States and Interest and Curiosity subscales may be more optimal, whereas either low or very high levels may be more dysfunctional (Luyten et al., 2017b).
To aid in interpreting results, we made the decision to ensure that higher scores on all subscales for RFQ and PRFQ measures were consistent with higher RF by reverse scoring as appropriate. For the two variables PRFQ Certainty in Mental States and Interest and Curiosity in which either high scores or middling scores may be most consistent with higher RF (Luyten et al., 2017a), we transformed these variables by squaring the deviations from the sample mean for the two PRFQ subscales [score = (y − mean)2] (Mood et al., 1974). This approach created continuous variables for PRFQ Certainty in Mental States and PRFQ Interest and Curiosity scores with the recoded lower scores (closer to original mean) considered more optimal RF and higher scores would be lower RF. Again, to ensure that all interpreted variables were consistent with the interpretation of higher scores indicating higher RF, we reverse scored the transformed variables (see Table 1 for details). However, to be exhaustive, we report on both the (a) untransformed and (b) transformed and reverse scored versions of each variable.
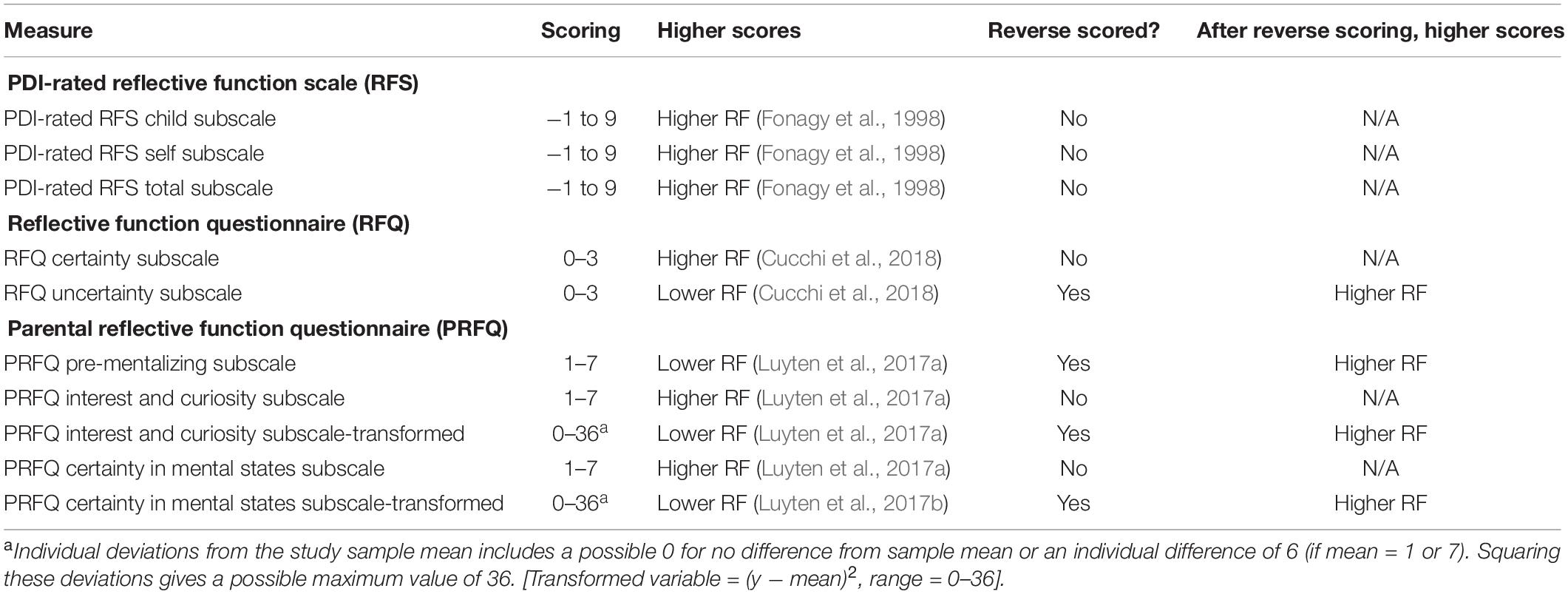
Table 1. Description of reflective function (RF) measures.
We analyzed data using IBM SPSS Statistics 26.0. We analyzed demographic and descriptive features of the sample with assessment of central tendency and frequencies. To ensure mothers’ and fathers’ scores were different from each other or did not differ based on membership in a given couple/family (that is, a given parent’s score was not influenced by their couple/family or not “independent”), prior to grouping for analyses, we conducted intraclass correlations, correlations, and examined scatterplots. Mothers’ and fathers’ scores were not correlated and were thus deemed independent. Nonetheless, we included a variable called “gender” to enable examination of mothers’ and fathers’ scores. We also investigated the descriptive properties of RF measures as shown in Table 3.
Then, we conducted reliability analysis to determine the internal consistency of the items of the questionnaires (PRFQ and RFQ) measured by using Cronbach’s alpha coefficients (Tavakol and Dennick, 2011). In order to study the relationship between RF scores from PDI-rated RFS and the questionnaires (PRFQ and RFQ), we computed Pearson’s correlation (Cohen, 1988; Benesty et al., 2009). We then regressed the significant RF questionnaire subscales scores on to PDI-rated RFS scores in separate multiple regression analyses (Iwasaki, 2020) with parents’ gender as a covariate.
We examined Cohen (1960) kappa, a measure of agreement (Harris and Brown, 2010) among the subscale scores and PDI-rated RFS scores using typical, exploratory, clinically meaningful quartiles at 25th (low) and 75th (high) percentile cut-offs. This also enabled the observation of associations by comparing extremes in this community sample. Reverse scoring was employed, as mentioned above, to enable interpretation of higher scores consistent with higher RF. However, to ensure transparency, we also report results from untransformed variables as well as results from variables with extreme outliers removed. We performed tests only with the significant subscales (from RFQ or PRFQ with PDI-rated RFS scores) identified in earlier analyses.
Specifically, we then determined the accuracy, that is, we examined the low and high categories for the gold standard PDI-rated RFS, to assess agreement with low and high categories on the PRFQ measure. We determined the sensitivity, that is, whether the PRFQ correctly identified low scores on the gold standard. We examined specificity, that is, whether the PRFQ correctly identified high scores on the gold standard. We also calculated the positive predictive value (i.e., among those detected by the PRFQ as low RF, how many are actually low as measured by the gold standard) and negative (i.e., among those detected by the PRFQ as high, how many are actually high as measured by the gold standard) (Yusoff, 2010). For all analyses, alpha was set at 0.05, two-tailed.
The characteristics of our sample are depicted in Table 2. Mothers (n = 75) and fathers (n = 75) completed the PDI interviews and the questionnaire measures of PRFQ and RFQ with no missing data. Table 3 presents the descriptive statistics of the RF measures (PDI-rated RFS, RFQ, and PRFQ), with the mean PDI-rated RFS scores ranging from 3.13 to 3.18 on the scale of −1 to 9. Table 4 shows that the Cronbach’s alpha ranged from 0.69 to 0.78 for the PRFQ and RFQ which demonstrates satisfactory internal consistency (Tavakol and Dennick, 2011). To determine convergent validity, Tables 5, 6 present the results of Pearson correlation analysis and subsequent multiple linear regression models, respectively, for the correlated variables. Of the three subscales of the PRFQ, we found significant correlations among the PRFQ Interest and Curiosity subscale (untransformed variable) and the PRFQ Certainty in Mental States (transformed and reverse—scored variable) with the PDI-rated Self, Child, and Total scores. We also found a significant correlation between PRFQ Pre-mentalizing and PDI-rated RFS Child scores, with trends approaching significance for PDI-rated RFS Self scores.
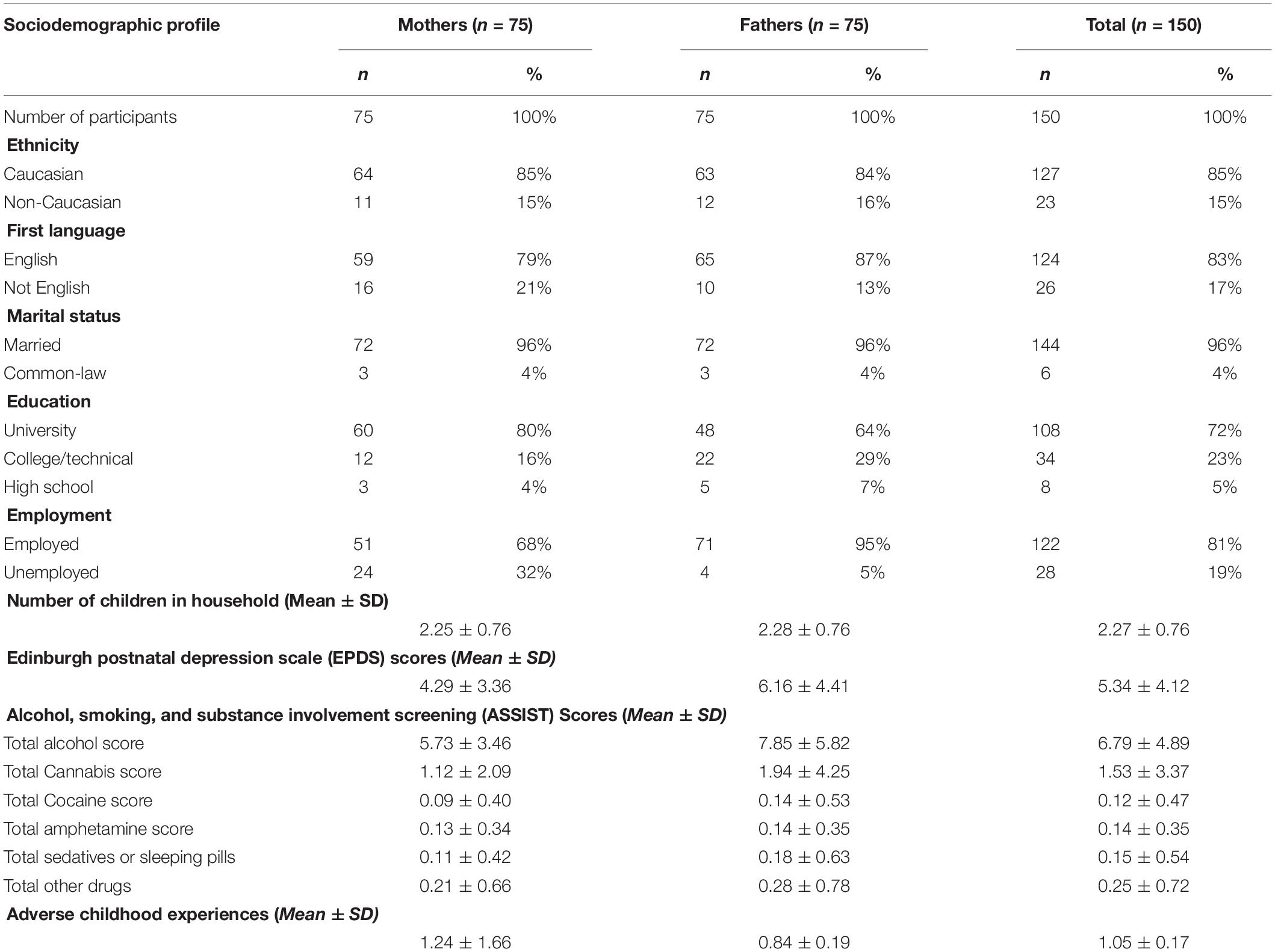
Table 2. Sociodemographic profile of the sample (n = 150).
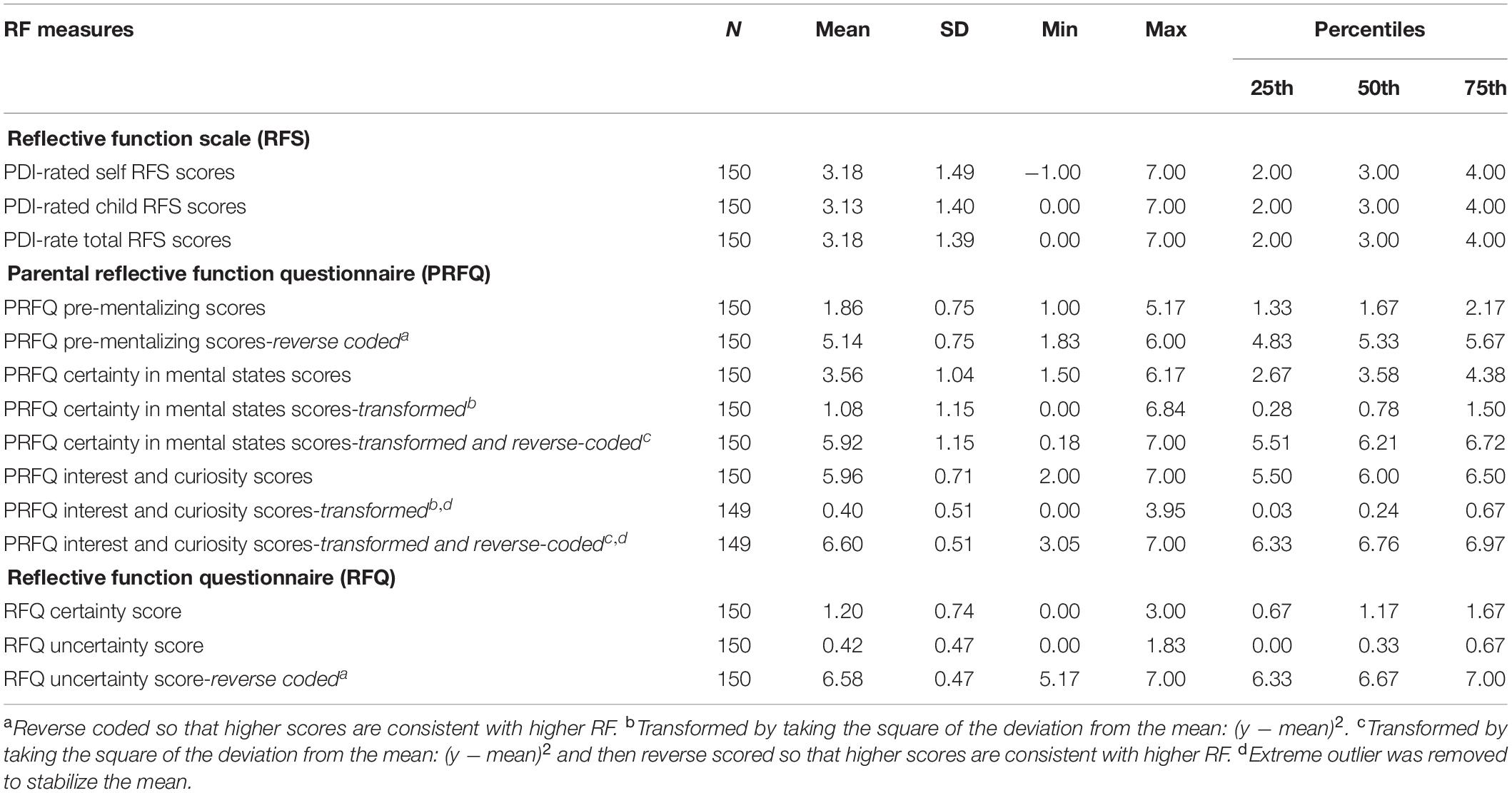
Table 3. Descriptive statistics of RF measures.
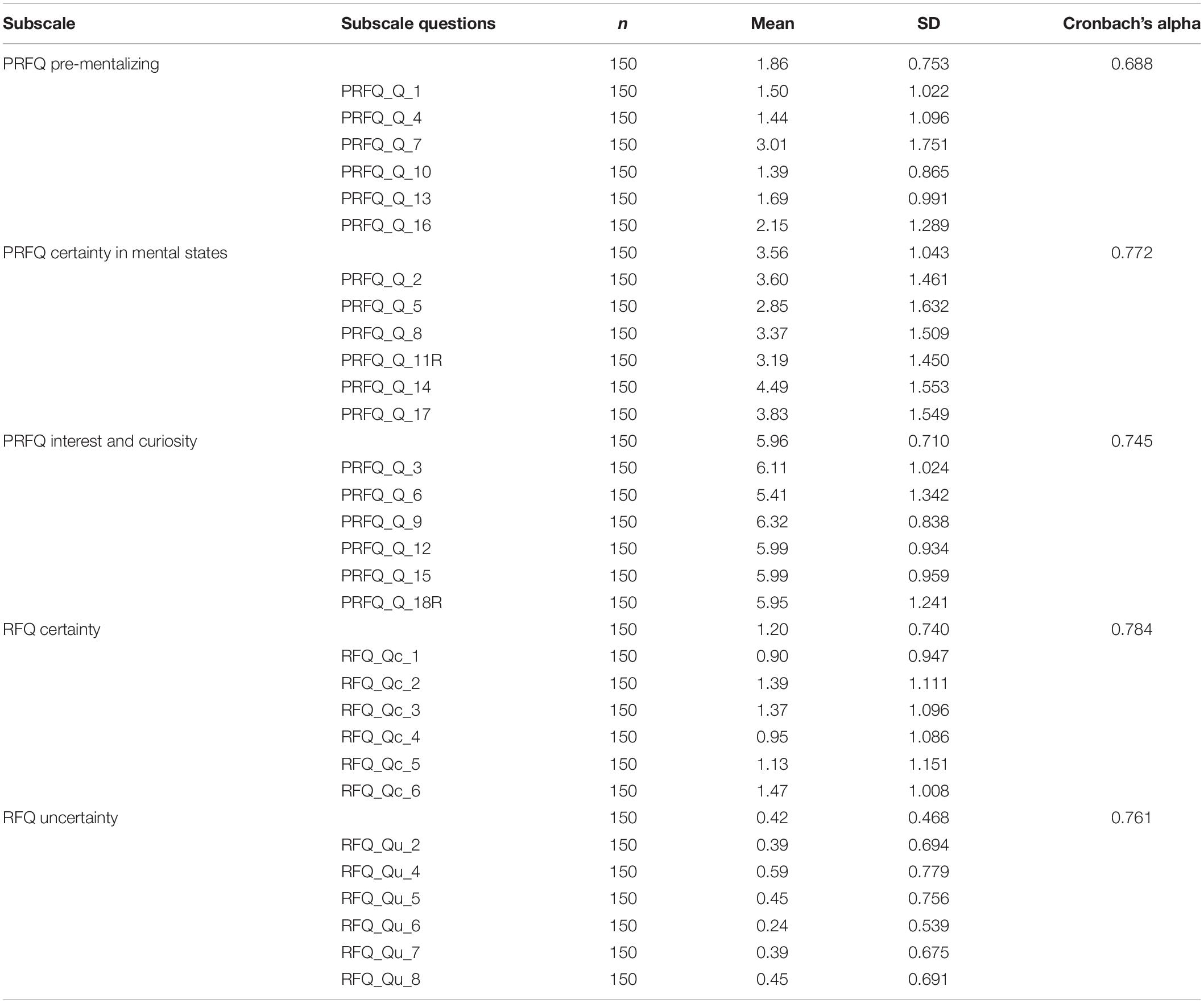
Table 4. Descriptive statistics of the outcome variables (questionnaire domains) and Cronbach’s alpha (as per original untransformed coding).
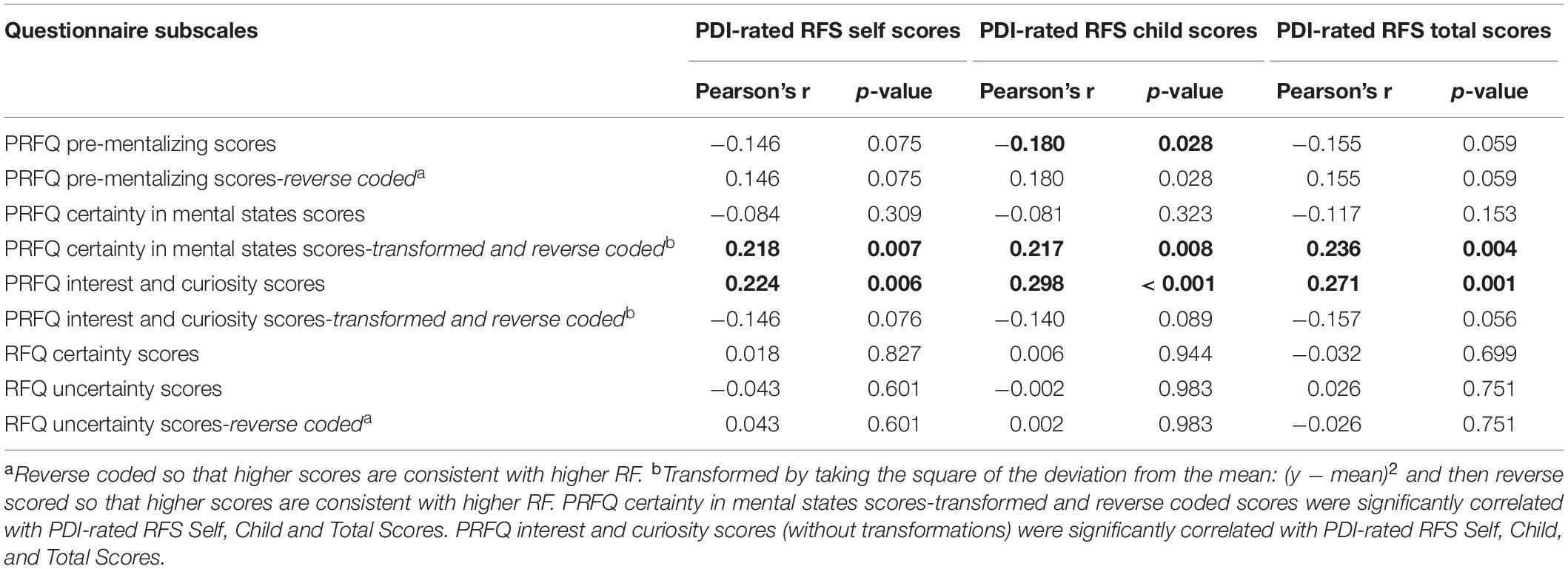
Table 5. Pearson’s product moment correlation coefficients.
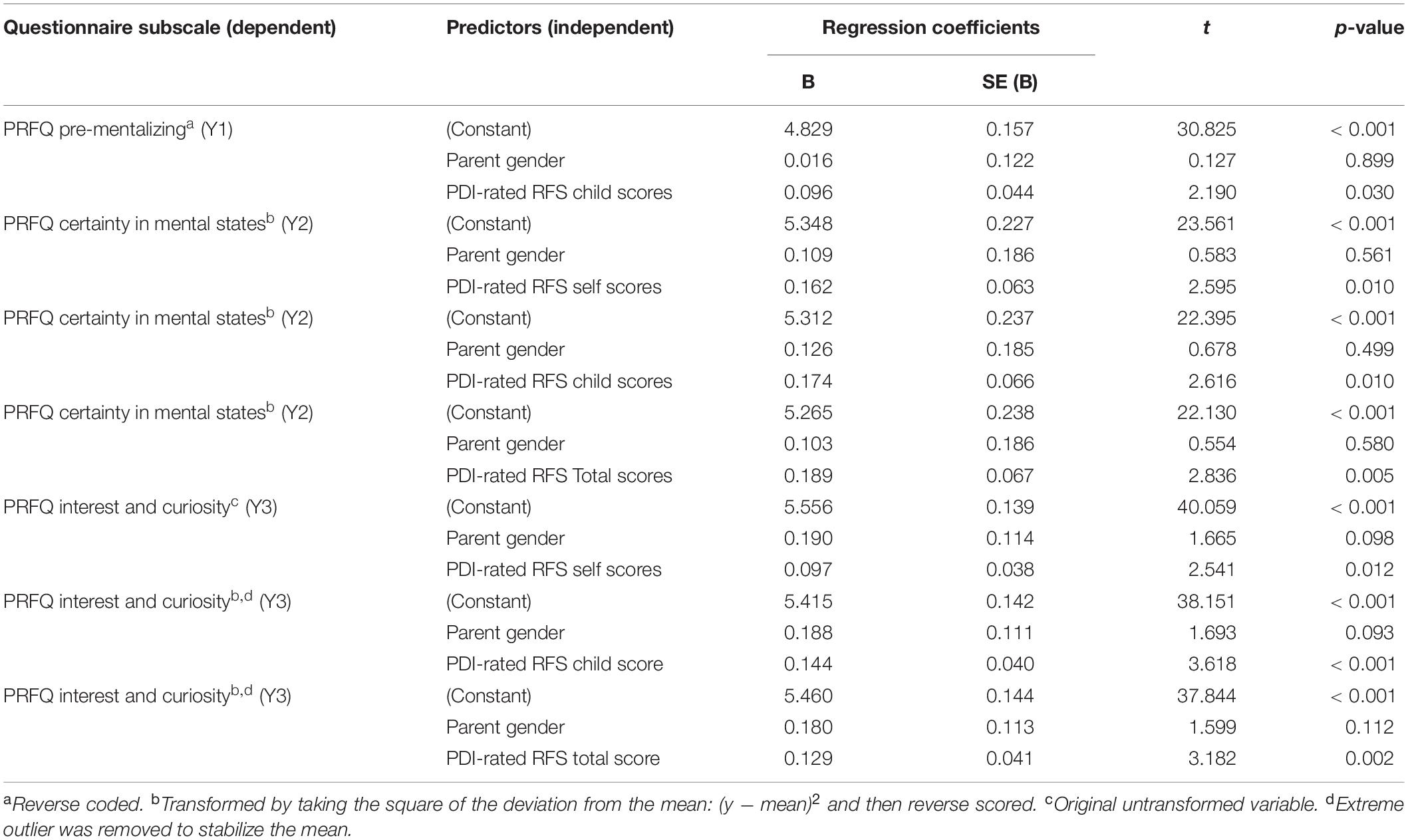
Table 6. Linear regression coefficients for outcome variables correlated with PDI-rated RFS scores.
To elaborate, scores on the PRFQ Certainty in Mental States (transformed and reverse scored) and PRFQ Interest and Curiosity (original scoring) subscales correlated significantly with the gold standard PDI-rated RFS, Fonagy et al. (1998) 11-point scale. In other words, higher scores correlated with higher RF for those sub-scales. Also, scores on the PRFQ Pre-mentalizing (original scoring) correlated negatively with the PDI-rated RFS Child scores in that higher pre-mentalizing was indicative of lower RF toward the Child. Thus, our hypothesis was supported. Linear regression models confirmed these relationships, accounting for parent gender. None of the subscales of RFQ were significantly correlated with PDI-rated RFS Total scores.
Cohen’s kappa coefficients of agreement among the PRFQ and RFQ subscale scores and PDI-rated RFS scores are presented in Table 7. Of the significant kappa statistics (all but PRFQ Pre-mentalizing), weak agreements were noted ranging from 0.16 for PRFQ Certainty in Mental States to 0.25 for Interest and Curiosity with higher scores indicated higher RF. Finally, the results of sensitivity and specificity of the PRFQ subscales with positive and negative predictive values to detect “Low” (< 2, i.e., 25th percentile) PDI-rated RFS scores are presented in Table 8. Positive predictive values ranged from 37 to 45%, showing that PRFQ subscale scores had low predictive ability to detect low RF on the PDI-rated RFS subscales. In contrast, negative predictive values ranged from 76 to 80% showing that the PRFQ subscale scores had high predictive ability to detect high RF on the PDI-rated RFS subscales.
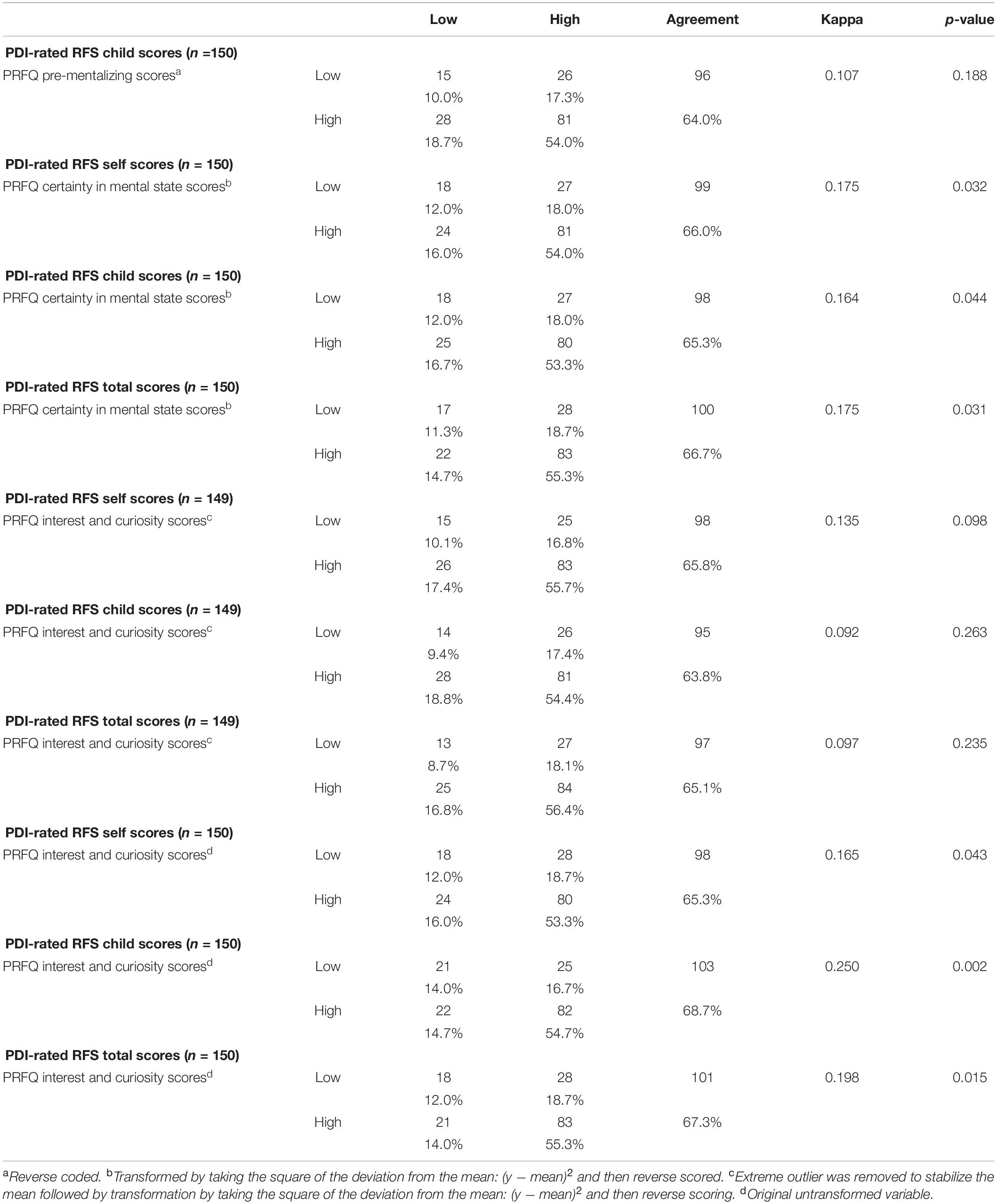
Table 7. Measure of agreement among the questionnaire subscale scores correlated with PDI rated scores using the 25th percentile values as cut-off points for low and high scores.
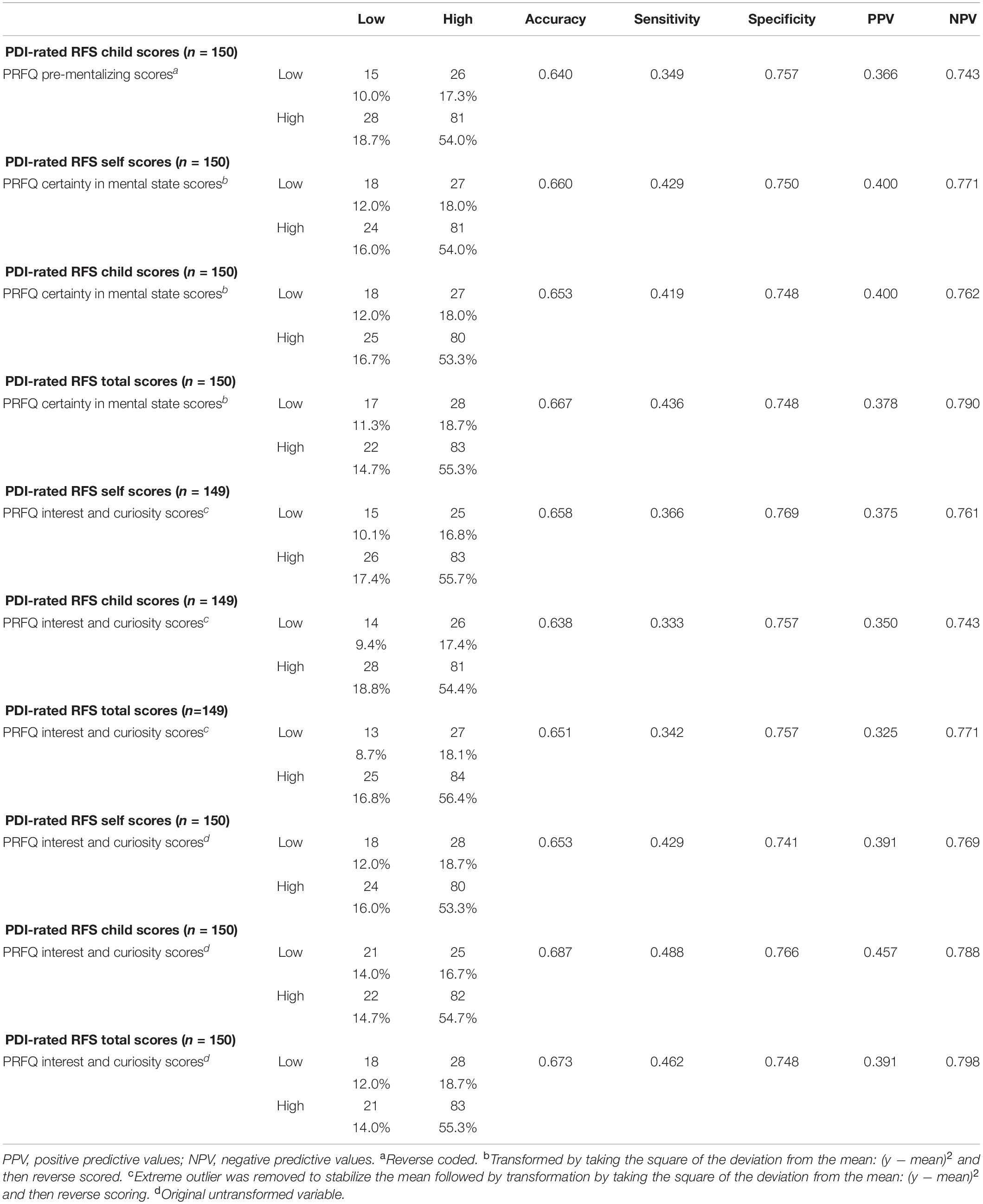
Table 8. Sensitivity and specificity of the questionnaire subscales to detect “Low” and “High” PDI-rated RFS scores using the 25th percentile values as cut-off points for low and high scores.
Our data provided preliminary evidence for the convergent validity of the PRFQ to the PDI-rated RFS scores, along with acceptable internal consistency reliability of its subscales. None of the subscales of the RFQ correlated with the PDI-rated RFS scores. Analyses employed the newly validated versions of the PRFQ (Luyten et al., 2017a) and RFQ (Fonagy et al., 2016), hence complementing to existing research (Cucchi et al., 2018) with more robust measures. Given the sample means demonstrating low risk for depression on the EPDS, low risk for substance abuse on the ASSIST, and low early adversity on the ACE questionnaire, these findings may be applicable to other community (non-clinical) samples.
The findings from our study are supported by existing literature (Slade et al., 2005, 2007). High levels of parental RF are thought to be explicated in keen interest and curiosity in mental states that leads to an exploration for understanding (Slade et al., 2004, 2007). High ratings on the PDI-rated RFS indicate an increasingly explicit and refined understanding of how mental states work and impact behavior (Slade et al., 2004). Accordingly, parents’ higher levels of interest and curiosity in reflecting about their child’s subjective experience and taking their own mental states and their child’s perspective were correlated. Overall, a parent’s interest and curiosity in mental states reflects certainty in her/his knowledge about her/his child, resulting in greater communication and involvement with the child.
In contrast, lower PRFQ Pre-mentalizing scores, demonstrating lower capacity for demonstrating a genuine curiosity in the subjective experience of the child, were correlated with lower PDI-rated RFS Child scores. Our findings demonstrated the degree to which the participants reported struggling in comprehending their children’s mental states accurately which is supported by previous research (Slade et al., 2007; Luyten et al., 2017b). The relationship between the PRFQ Pre-mentalizing and the PDI-rated RFS scores agrees with existing research conducted on the PRFQ (Rostad and Whitaker, 2016; Luyten et al., 2017a). Accordingly, if a parent finds it challenging to understand the child’s internal world, he or she may find it challenging to think or talk about the child’s mental states. This aligns with suggestions put forward by the RF researchers that these pre-mentalizing modes of understanding mental states from parents’ perspective are often associated with making malicious attributions and an inability to understand and interpret child’s internal subjective world (Rostad and Whitaker, 2016), the features that research suggests are characteristic of parents with severe mentalizing problems (Slade et al., 2005; Suchman et al., 2010).
Interestingly, the parents’ scores on PRFQ Certainty in Mental States (transformed and reverse coded) correlated positively with PDI-rated RFS scores, while the untransformed variable did not. This finding is supported by existing research (Luyten et al., 2017b) demonstrating that average levels of PRFQ Certainty in Mental States and Interest and may be most optimal, whereas either low or very high levels of RF may be more malevolent. Theoretically, the development of pathological levels of RF demonstrates that being highly certain of others’ mental states (e.g., thoughts, feelings) tend to be a type of RF deficit (Fonagy et al., 2003). One persuasive explanation may be that the parents, who have high levels of certainty about mental states, may attain a PRFQ Certainty in Mental States score that, in fact, does not reflect their real RF capacity, because their pseudo-mentalizing statements may come from statements that are given high RF scores (Handeland et al., 2019). Stated simply, too low or too high levels of certainty about mental states can lead to rigidity and a collapse of RF (Fonagy et al., 2016).
Also, we did not find significant associations between the PDI-rated RFS scores and the RFQ, which implies that the RFQ may not be useful to capture the essence of the parental RF. While we expected this, as the PDI assesses parenting in the current context and not family of origin context, as assessed with the AAI, our findings contrast with others. Handeland et al. (2019) found that the RFQ Uncertainty was significantly negatively associated with PDI-rated RFS Self scores. However, Handeland et al. (2019) used the Norwegian version of the RFQ-8 which is relatively new and has no well-established or validated cut-off for clinically high scores on its scales. The cut-offs in the study were based on an assumption that a mean score of at least 1 on either of these scales represents a marked RF deficit. Also, the findings from their study were not supported by the fact that the RFQ Certainly was not correlated with PDI-rated RFS Self scores. Given the strong negative correlation between the RFQ Certainty and Uncertainty scales (Fonagy et al., 2016; Cucchi et al., 2018; Handeland et al., 2019), to a certain extent, findings demonstrating low scores on one scale need to be coupled with high scores on the other, and vice versa.
To our knowledge, our study stands to be the first to compare the PRFQ with the RFS from the PDI. As suggested, the time- and cost-intensiveness of the RFS applied to an interview, is addressed by the quick and efficient PRFQ. Reducing the patient/participant burden of assessing RF will improve feasibility of administration in clinical and research settings. Further, while the RFS applied to the PDI generally yields global scores of participants’ RF, the PRFQ yields information about specific dimensions of mentalizing—pre-mentalizing and certainty, interest, and curiosity about mental states, which may have important implications for clinicians and researchers (Fonagy et al., 2016). As a result, the PRFQ, as a reliable and valid clinically meaningful self-report measure of RF, may be best suited for administration in wide-ranging settings.
The current research has several strengths including an adequate sample size of both mothers and fathers and “master” level coding of PDI interviews for RF. Moreover, while the PRFQ has been validated mostly in the small, clinical or at-risk samples to date (Luyten et al., 2017b), we report the validity of the PRFQ in a large normative community sample. We conclude that all three subscales of the PRFQ have satisfactory convergent validity with the PDI-rated RFS. Given that the PRFQ scores show high specificity (negative predictive values ranging from 76 to 80%) in predicting high RF scores, the PRFQ may replace the PDI-rated RFS when scores are high on the PRFQ, as may be expected in low-risk samples. However, PRFQ scores exhibit low sensitivity scores (positive predictive values ranging from 37 to 45%) in predicting low RF scores, thus for high-risk samples, it may be recommended to follow up with the PDI interview when the RF scores are low on the PRFQ. A potential limitation is that participants may attempt to appear more reflective than they are in an attempt to please the researcher, as in the case of acquiescent response or social desirability. As this will be an ongoing limitation of any test of RF (De Roo et al., 2019), caution should be taken before forensic use, in for example, court cases related to child custody. This is a problem with any self-report measure. Given that this is the first study of its kind, a replication of the current project that includes Adult Attachment Interview (AAI; George et al., 1996) in the mix with the RFS is recommended for future research.
Our evaluation of convergent validity demonstrated that the PRFQ is significantly correlated with the gold standard RFS applied to the PDI in measuring theoretically similar concepts of RF in parents. The results from our study provide evidence for the reliability and validity of the PRFQ as brief multifaceted measure of parental RF, offering potentially valuable methodological approaches for studies of parental development, especially in low-risk populations.
The data analyzed in this study is subject to the following licenses/restrictions: N/A. Requests to access these datasets should be directed to LA, bGFuaXNAdWNhbGdhcnkuY2E=.
The studies involving human participants were reviewed and approved by Conjoint Health Research Ethics Board, University of Calgary. The patients/participants provided their written informed consent to participate in this study.
LA formulated the research question and oversaw all aspects of manuscript preparation from literature review, the data collection, the data analysis, interpreted the results, and undertook writing and submission. GP helped with the data analysis, overseeing the literature review, interpretation of the results, and writing. NL helped formulate the research question, oversaw the literature review and data analysis, and interpreted the results and writing. KB and CE helped oversee the literature review and data analysis, and interpreted the results and writing. MH helped review the literature review, interpretation of the results, and writing. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Antonsen, B. T., Johansen, M. S., Rø, F. G., Kvarstein, E. H., and Wilberg, T. (2016). Is reflective functioning associated with clinical symptoms and long-term course in patients with personality disorders? Compr. Psychiatry 64, 46–58. doi: 10.1016/j.comppsych.2015.05.016
Badoud, D., Luyten, P., Fonseca-Pedrero, E., Eliez, S., Fonagy, P., and Debbané, M. (2015). The French version of the Reflective Functioning Questionnaire: validity data for adolescents and adults and its association with non-suicidal self-injury. PLoS One 10:e0145892. doi: 10.1371/journal.pone.0145892
Baradon, T., Fonagy, P., Bland, K., Lénárd, K., and Sleed, M. (2008). New Beginnings–an experience-based programme addressing the attachment relationship between mothers and their babies in prisons. J. Child Psychother. 34, 240–258. doi: 10.1080/00754170802208065
Bateman, A. W., and Fonagy, P. E. (2012). Handbook of Mentalizing in Mental Health Practice. Arlington, VA: American Psychiatric Publishing.
Benesty, J., Chen, J., Huang, Y., and Cohen, I. (2009). Pearson Correlation Coefficient. In Noise Reduction in Speech Processing. Berlin: Springer, 1–4.
Borelli, J. L., Cohen, C., Pettit, C., Normandin, L., Target, M., Fonagy, P., et al. (2019). Maternal and child sexual abuse history: an intergenerational exploration of children’s Adjustment and maternal trauma-reflective functioning. Front. Psychol. 10:1062. doi: 10.3389/fpsyg.2019.01062
Bouchard, M. A., Target, M., Lecours, S., Fonagy, P., Tremblay, L. M., Schachter, A., et al. (2008). Mentalization in adult attachment narratives: reflective functioning, mental states, and affect elaboration compared. Psychoanal. Psychol. 25:47. doi: 10.1037/0736-9735.25.1.47
Bretherton, I., Biringen, Z., Ridgeway, D., Maslin, C., and Sherman, M. (1989). Attachment: the parental perspective. Infant Ment. Health J. 10, 203–221.
Cohen, J. (1960). A coefficient of agreement for nominal scales. Educ. Psychol. Meas. 20, 37–46. doi: 10.1177/001316446002000104
Cohen, J. (1988). The t Test for Means. Statistical Power Analysis for the Behavioural Sciences, 2nd Edn. Hillsdale, NJ: Lawrence Erlbaum Associates.
Cooke, D., Priddis, L., Luyten, P., Kendall, G., and Cavanagh, R. (2017). Paternal and maternal reflective functioning in the Western Australian Peel child health study. Infant Ment. Health J. 38, 561–574. doi: 10.1002/imhj.21664
Cox, J. L., Holden, J. M., and Henshaw, C. (2014). Perinatal Mental Health: The Edinburgh Postnatal Depression Scale (EPDS) Manual, 2nd Edn. London: RCPsych Publications.
Cox, J. L., Holden, J. M., and Sagovsky, R. (1987). Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 150, 782–786. doi: 10.1192/bjp.150.6.782
Cucchi, A., Hampton, J. A., and Moulton-Perkins, A. (2018). Using the validated Reflective Functioning Questionnaire to investigate mentalizing in individuals presenting with eating disorders with and without self-harm. PeerJ 6:e5756. doi: 10.7717/peerj.5756
De Roo, M., Wong, G., Rempel, G. R., and Fraser, S. N. (2019). Advancing optimal development in children: examining the construct validity of a Parent Reflective Functioning Questionnaire. JMIR Pediatr. Parent. 2:e11561. doi: 10.2196/11561
Duval, J., Ensink, K., Normandin, L., Sharp, C., and Fonagy, P. (2018). Measuring reflective functioning in adolescents: relations to personality disorders and psychological difficulties. Adolesc. Psychiatry 8, 5–20. doi: 10.2174/2210676608666180208161619
Ekeblad, A., Falkenström, F., and Holmqvist, R. (2016). Reflective functioning as predictor of working alliance and outcome in the treatment of depression. J. Consult. Clin. Psychol. 84, 67–78. doi: 10.1037/ccp0000055
Ensink, K., Bégin, M., Normandin, L., and Fonagy, P. (2016). Maternal and child reflective functioning in the context of child sexual abuse: pathways to depression and externalising difficulties. Eur. J. Psychotraumatol. 7:30611. doi: 10.3402/ejpt.v7.30611
Ensink, K., Bégin, M., Normandin, L., and Fonagy, P. (2017). Parental reflective functioning as a moderator of child internalizing difficulties in the context of child sexual abuse. Psychiatry Res. 257, 361–366. doi: 10.1016/j.psychres.2017.07.051
Felitti, V. J., Anda, R. F., Nordenberg, D., Williamson, D. F., Spitz, A. M., Edwards, V., et al. (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: the Adverse Childhood Experiences (ACE) Study. Am. J. Prev. Med. 14, 245–258. doi: 10.1016/s0749-3797(98)00017-8
Fischer-Kern, M., Doering, S., Taubner, S., Hörz, S., Zimmermann, J., Rentrop, M., et al. (2015). Transference-focused psychotherapy for borderline personality disorder: change in reflective function. Br. J. Psychiatry 207, 173–174.
Fonagy, P., and Bateman, A. (2008). The development of borderline personality disorderA mentalizing model. J. Pers. Disord. 22, 4–21. doi: 10.1521/pedi.2008.22.1.4
Fonagy, P., and Bateman, A. W. (2007). Mentalizing and borderline personality disorder. J. Ment. Health 16, 83–101. doi: 10.1080/09638230601182045
Fonagy, P., Luyten, P., Moulton-Perkins, A., Lee, Y. W., Warren, F., Howard, S., et al. (2016). Development and validation of a self-report measure of mentalizing: the reflective functioning questionnaire. PLoS One 11:e0158678. doi: 10.1371/journal.pone.0158678
Fonagy, P., Steele, M., Moran, G., Steele, H., and Higgitt, A. (1991a). Measuring the ghost in the Nursery: a Summary of the main findings of the Anna Freud Centre-University College London Parent-C. Bull. Anna. Freud. Centre 14, 115–131.
Fonagy, P., Steele, M., Steele, H., Moran, G. S., and Higgitt, A. C. (1991b). The capacity for understanding mental states: the reflective self in parent and child and its significance for security of attachment. Infant Ment. Health J. 12, 201–218. doi: 10.1002/1097-0355(199123)12:3<201::aid-imhj2280120307>3.0.co;2-7
Fonagy, P., and Target, M. (1997). Attachment and reflective function: their role in self-organization. Dev. Psychopathol. 9, 679–700. doi: 10.1017/s0954579497001399
Fonagy, P., and Target, M. (1998). Mentalization and the changing aims of child psychoanalysis. Psychoanal. Dialogues 8, 87–114. doi: 10.1080/10481889809539235
Fonagy, P., Target, M., Gergely, G., Allen, J. G., and Bateman, A. (2003). The developmental roots of borderline personality disorder in early attachment relationships: a theory and some evidence. Psychoanal. Inq. 23, 412–459. doi: 10.1080/07351692309349042
Fonagy, P., Target, M., Steele, H., and Steele, M. (1998). Reflective-Functioning Manual, Version 5.0, for Application to Adult Attachment Interviews. London: University College London.
Fonagy, P. G., Jurist, G., and Target, E. M. (2002). Affect Regulation, Mentalization, and the Development of the Self. New York, NY: Other Press.
Garner, P. W., Dunsmore, J. C., and Southam-Gerow, M. (2008). Mother-child conversations about emotions: linkages to child aggression and prosocial behavior. Soc. Dev. 17, 259–277. doi: 10.1111/j.1467-9507.2007.00424.x
George, C., Kaplan, N., and Main, M. (1996). Adult Attachment Interview. London: University College London.
Gottman, J. M., Katz, L. F., and Hooven, C. (1996). Parental meta-emotion philosophy and the emotional life of families: theoretical models and preliminary data. J. Fam. Psychol. 10, 243–268. doi: 10.1037/0893-3200.10.3.243
Handeland, T. B., Kristiansen, V. R., Lau, B., Håkansson, U., and Øie, M. G. (2019). High degree of uncertain reflective functioning in mothers with substance use disorder. Addict. Behav. Rep. 10:100193. doi: 10.1016/j.abrep.2019.100193
Harris, L. R., and Brown, G. T. (2010). Mixing interview and questionnaire methods: practical problems in aligning data. Pract. Assess. Res. Eval. 15:1.
Humeniuk, R., and Ali, R. (2006). Validation of the Alcohol, Smoking and Substance Involvement Screening Test (ASSIST) and Pilot Brief Intervention: A Technical Report of Phase II Findings of the WHO ASSIST Project. Geneva: WHO Press.
Iwasaki, M. (2020). “Multiple regression analysis from data science perspective,” in Advanced Studies in Behaviormetrics and Data Science Behaviormetrics: Quantitative Approaches to Human Behavior, ed. A. Okada (Basel: Springer Nature), 131–140. doi: 10.1007/978-981-15-2700-5_8
Kaplan, B. J., Giesbrecht, G. F., Leung, B. M., Field, C. J., Dewey, D., Bell, R. C., et al. (2014). The Alberta Pregnancy Outcomes and Nutrition (APrON) cohort study: rationale and methods. Matern. Child Nutr. 10, 44–60. doi: 10.1111/j.1740-8709.2012.00433.x
Karp, J. N., Makol, B. A., Keeley, L. M., Qasmieh, N., Deros, D. E., Weeks, J. W., et al. (2018). Convergent, incremental, and criterion-related validity of multi-informant assessments of adolescents’ fears of negative and positive evaluation. Clin. Psychol. Psychother. 25, 217–230. doi: 10.1002/cpp.2156
Kelly, K., Slade, A., and Grienenberger, J. F. (2005). Maternal reflective functioning, mother–infant affective communication, and infant attachment: exploring the link between mental states and observed caregiving behavior in the intergenerational transmission of attachment. Attach. Hum. Dev. 7, 299–311. doi: 10.1080/14616730500245963
Khalifa, D. S., Glavin, K., Bjertness, E., and Lien, L. (2015). Postnatal depression among Sudanese women: prevalence and validation of the Edinburgh Postnatal Depression Scale at 3 months postpartum. Int. J. Women’s Health 7:677. doi: 10.2147/ijwh.s81401
Laible, D. (2004). Mother-child discourse in two contexts: links with child temperament, attachment security, and socioemotional competence. Dev. Psychol. 40, 979–992. doi: 10.1037/0012-1649.40.6.979
Lemma, A., Target, M., and Fonagy, P. (2011). The development of a brief psychodynamic intervention (Dynamic Interpersonal Therapy) and its application to depression: a pilot study. Psychiatry 74, 41–48. doi: 10.1521/psyc.2011.74.1.41
Levy, K. N., Meehan, K. B., Kelly, K. M., Reynoso, J. S., Weber, M., Clarkin, J. F., et al. (2006). Change in attachment patterns and reflective function in a randomized control trial of transference-focused psychotherapy for borderline personality disorder. J. Consult. Clin. Psychol. 74:1027. doi: 10.1037/0022-006x.74.6.1027
Luyten, P., Fonagy, P., Lowyck, B., and Vermote, R. (2012a). “Assessment of mentalization,” in Handbook of Mentalizing in Mental Health Practice, eds A. W. Bateman and P. Fonagy (Arlington, VA: American Psychiatric Publishing), 43–65.
Luyten, P., Mayes, L. C., Nijssens, L., and Fonagy, P. (2017a). The parental reflective functioning questionnaire: development and preliminary validation. PLoS One 12:e0176218. doi: 10.1371/journal.pone.0176218
Luyten, P., Nijssens, L., Fonagy, P., and Mayes, L. C. (2017b). Parental reflective functioning: theory, research, and clinical applications. Psychoanal. Study Child 70, 174–199. doi: 10.1080/00797308.2016.1277901
Luyten, P., Van Houdenhove, B., Lemma, A., Target, M., and Fonagy, P. (2012b). A mentalization-based approach to the understanding and treatment of functional somatic disorders. Psychoanal. Psychother. 26, 121–140. doi: 10.1080/02668734.2012.678061
Manca, D. P., O’Beirne, M., Lightbody, T., Johnston, D. W., Dymianiw, D., Anis, L., et al. (2013). The most effective strategy for recruiting a pregnancy cohort: a tale of two cities. BMC Pregnancy Childbirth 13:75. doi: 10.1186/s13223-017-0199-4
Meins, E. (1998). The effects of security of attachment and material attribution of meaning on children’s linguistic acquisitional style. Infant Behav. Dev. 21, 237–252. doi: 10.1016/s0163-6383(98)90004-2
Meins, E., Muñoz-Centifanti, L., Fernyhough, C., and Fishburn, S. (2013). Maternal mind-mindedness and children’s behavioral difficulties: mitigating the impact of low socio-economic status. J. Abnorm. Child Psychol. 41, 543–553. doi: 10.1007/s10802-012-9699-3
Midgely, N., and Vrouva, I. (eds) (2013). Minding the Child: Mentalization-Based Interventions with Children, Young People and their Families. New York, NY: Routledge.
Mood, A. M., Graybill, F. A., and Boes, D. C. (1974). Introduction to the Theory of Statistics 1974. New York, NY: McGraw-Hill Kogakusha.
Morandotti, N., Brondino, N., Merelli, A., Boldrini, A., De Vidovich, G. Z., Ricciardo, S., et al. (2018). The Italian version of the Reflective Functioning Questionnaire: validity data for adults and its association with severity of borderline personality disorder. PLoS One 13:e0206433. doi: 10.1371/journal.pone.0206433
Morosan, L., Ghisletta, P., Badoud, D., Toffel, E., Eliez, S., and Debbané, M. (2020). Longitudinal relationships between reflective functioning, empathy, and externalizing behaviors during adolescence and young adulthood. Child Psychiatry Hum. Dev. 51, 59–70. doi: 10.1007/s10578-019-00910-8
Murphy, A., Steele, M., Dube, S. R., Bate, J., Bonuck, K., Meissner, P., et al. (2014). Adverse childhood experiences (ACEs) questionnaire and adult attachment interview (AAI): implications for parent child relationships. Child Abuse Negl. 38, 224–233. doi: 10.1016/j.chiabu.2013.09.004
Oppenheim, D., and Koren-Karie, N. (2009). Infant–parent relationship assessment: parents’ insightfulness regarding their young children’s internal worlds. Handb. Infant Ment. Health 3, 266–280.
Ordway, M. R., Sadler, L. S., Dixon, J., and Slade, A. (2014). Parental reflective functioning: analysis and promotion of the concept for paediatric nursing. J. Clin. Nurs. 23, 3490–3500. doi: 10.1111/jocn.12600
Pazzagli, C., Delvecchio, E., Raspa, V., Mazzeschi, C., and Luyten, P. (2018). The parental reflective functioning questionnaire in mothers and fathers of school-aged children. J. Child Fam. Stud. 27, 80–90. doi: 10.1007/s10826-017-0856-8
Rostad, W. L., and Whitaker, D. J. (2016). The association between reflective functioning and parent–child relationship quality. J. Child Fam. Stud. 25, 2164–2177. doi: 10.1007/s10826-016-0388-7
Ruffman, T., Slade, L., and Crowe, E. (2002). The relation between children’s and mothers’ mental state language and theory-of-mind understanding. Child Dev. 73, 734–751. doi: 10.1111/1467-8624.00435
Rutherford, H. J., Booth, C. R., Luyten, P., Bridgett, D. J., and Mayes, L. C. (2015). Investigating the association between parental reflective functioning and distress tolerance in motherhood. Infant Behav. Dev. 40, 54–63. doi: 10.1016/j.infbeh.2015.04.005
Schechter, D. S., Myers, M. M., Brunelli, S. A., Coates, S. W., Zeanah, C. H. Jr., Davies, M., et al. (2006). Traumatized mothers can change their minds about their toddlers: understanding how a novel use of videofeedback supports positive change of maternal attributions. Infant Ment. Health J. 27, 429–447. doi: 10.1002/imhj.20101
Schiborr, J., Lotzin, A., Romer, G., Schulte-Markwort, M., and Ramsauer, B. (2013). Child-focused maternal mentalization: a systematic review of measurement tools from birth to three. Measurement 46, 2492–2509. doi: 10.1016/j.measurement.2013.05.007
Slade, A. (2005). Parental Reflective Functioning: An introduction. Attach. Hum. Dev. 7, 269–281. doi: 10.1080/14616730500245906
Slade, A., Aber, J. L., Berger, B., Bresgi, I., and Kaplan, M. (2003). The Parent Development Interview. Unpublished manuscript, New York, USA: City University of New York.
Slade, A., Bernbach, E., Grienenberger, J., Levy, D. W., and Locker, A. (2004). The Parent Development Interview and the Pregnancy Interview: Manuals for Scoring. New Haven, CT: City College of New York and Yale Child Study Center.
Slade, A., Grienenberger, J., Bernbach, E., Levy, D., and Locker, A. (2005). Maternal reflective functioning, attachment, and the transmission gap: a preliminary study. Attach. Hum. Dev. 7, 283–298. doi: 10.1080/14616730500245880
Slade, A., Patterson, M., and Miller, M. (2007). Addendum to Reflective Functioning Scoring Manual for use with the Pregnancy Interview. New York, NY: The Psychological Center at the City College of New York.
Slaughter, V., Peterson, C. C., and Carpenter, M. (2008). Maternal talk about mental states and the emergence of joint visual attention. Infancy 13, 640–659. doi: 10.1080/15250000802458807
Sleed, M., Baradon, T., and Fonagy, P. (2013). New Beginnings for mothers and babies in prison: a cluster randomized controlled trial. Attach. Hum. Dev. 15, 349–367. doi: 10.1080/14616734.2013.782651
Sleed, M., Slade, A., and Fonagy, P. (2020). Reflective Functioning on the Parent Development Interview: validity and reliability in relation to socio-demographic factors. Attach. Hum. Dev. 22, 310–331. doi: 10.1080/14616734.2018.1555603
Stacks, A. M., Muzik, M., Wong, K., Beeghly, M., Huth-Bocks, A., Irwin, J. L., et al. (2014). Maternal reflective functioning among mothers with childhood maltreatment histories: Links to sensitive parenting and infant attachment security. Attach. Hum. Dev. 16, 515–533. doi: 10.1080/14616734.2014.935452
Steele, M., Kaniuk, J., Hodges, J., Asquith, K., Hillman, S., and Steele, H. (2008). “Measuring mentalization across contexts: links between representations of childhood and representations of parenting in an adoption sample,” in Mind to Mind: Infant Research, Neuroscience, and Psychoanalysis, eds E. Jurist, A. Slade, and S. Bergner (New York, NY: Other Press), 115–138.
Suchman, N. E., DeCoste, C., Castiglioni, N., McMahon, T. J., Rounsaville, B., and Mayes, L. (2010). The Mothers and Toddlers Program, an attachment-based parenting intervention for substance using women: Post-treatment results from a randomized clinical pilot. Attach. Hum. Dev. 12, 483–504. doi: 10.1080/14616734.2010.501983
Taubner, S., Hörz, S., Fischer-Kern, M., Doering, S., Buchheim, A., and Zimmermann, J. (2013). Internal structure of the reflective functioning scale. Psychol. Assess. 25:127. doi: 10.1037/a0029138
University College London (2020). The Parental Reflective Functioning Questionnaire (PRFQ). Available online at: https://www.ucl.ac.uk/psychoanalysis/research/parental-reflective-functioning-questionnaire-prfq (Accessed May 26, 2020)
Winnicott, D. W. (1962). The theory of the parent-infant relationship—Contributions to discussion. Int. J. Psycho Anal. 43, 256–257.
World Health Organization Assist Working Group (2002). The alcohol, smoking and substance involvement screening test (ASSIST): development, reliability and feasibility. Addiction 97, 1183–1194. doi: 10.1046/j.1360-0443.2002.00185.x
Keywords: reflective function, measurement, reflective function scale, reflective function questionnaire, parental reflective function questionnaire, convergent validity, APrON study
Citation: Anis L, Perez G, Benzies KM, Ewashen C, Hart M and Letourneau N (2020) Convergent Validity of Three Measures of Reflective Function: Parent Development Interview, Parental Reflective Function Questionnaire, and Reflective Function Questionnaire. Front. Psychol. 11:574719. doi: 10.3389/fpsyg.2020.574719
Received: 22 June 2020; Accepted: 10 November 2020;
Published: 16 December 2020.
Edited by:
Giuseppe Sartori, University of Padua, ItalyReviewed by:
Cristina Mazza, University of Studies G. d’Annunzio Chieti and Pescara, ItalyCopyright © 2020 Anis, Perez, Benzies, Ewashen, Hart and Letourneau. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lubna Anis, bGFuaXNAdWNhbGdhcnkuY2E=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.