 Steven K. Iorfa1*
Steven K. Iorfa1* Iboro F. A. Ottu2
Iboro F. A. Ottu2 Rotimi Oguntayo3
Rotimi Oguntayo3 Olusola Ayandele4*
Olusola Ayandele4* Samson O. Kolawole5
Samson O. Kolawole5 Joshua C. Gandi6
Joshua C. Gandi6 Abdullahi L. Dangiwa7
Abdullahi L. Dangiwa7 Peter O. Olapegba8
Peter O. Olapegba8- 1Department of Psychology, University of Nigeria, Nsukka, Nigeria
- 2Department of Psychology, University of Uyo, Uyo, Nigeria
- 3Department of Psychology, University of Ilorin, Ilorin, Nigeria
- 4Department of General Studie, The Polytechnic, Ibadan, Nigeria
- 5Department of Psychology, Nigeria Police Academy, Kano, Nigeria
- 6Department of Psychology, University of Jos, Jos, Nigeria
- 7Department of Sociology, Federal University, Dutse, Nigeria
- 8Department of Psychology, University of Ibadan, Ibadan, Nigeria
The novel coronavirus has not only brought along disruptions to daily socio-economic activities, but sickness and deaths due to its high contagion. With no widely acceptable pharmaceutical cure, the best form of prevention may be precautionary measures which will guide against infections and curb the spread of the disease. This study explored the relationship between COVID-19 knowledge, risk perception, and precautionary behavior among Nigerians. The study also sought to determine whether this relationship differed for men and women. A web-based cross-sectional design approach was used to recruit 1,554 participants (mean age = 27.43, SD = 9.75; 42.7% females) from all geopolitical zones in Nigeria, through social media platforms using a snowball sampling technique. Participants responded to web-based survey forms comprising demographic questions and adapted versions of the Ebola knowledge scale, SARS risk perception scale, and precautionary behavior scale. Moderated mediation analysis of the data showed that risk perception mediated the association between COVID-19 knowledge and precautionary behavior and this indirect effect was in turn moderated by gender. Results indicate that having adequate knowledge of COVID-19 was linked to higher involvement in precautionary behavior through risk perception for females but not for males. It was also noted that awareness campaigns and psychological intervention strategies on COVID-19 related activities may be particularly important for males more than females. Drawing from the health belief model, we recommend that COVID-19 awareness campaigns should target raising more awareness of the risks associated with the infection to make individuals engage more in precautionary behaviors.
Introduction
The outbreak of the novel Coronavirus disease (COVID-19) pandemic has led to disruptions to health, economics, politics and social order all across the world. The COVID-19 is a ravaging and infectious viral disease caused by a novel strain of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Due to the rapidly increasing and contagious nature of the disease and its overwhelming influence on critical care and frontline healthcare staff as well as the possibility of transmission by asymptomatic carriers, governments around the world closed their borders, announced total or partial lockdowns, movement restrictions, social distancing, and wearing of facemasks (Biscayart et al., 2020; Zaka et al., 2020; Zhao et al., 2020) as precautionary measures to curb the spread of the virus. However, as of August 10, 2020, the total number of infected persons worldwide had risen to 19,718,030 cases with 728,013 deaths while Nigeria had 46,867 confirmed cases and 950 deaths (John Hopkins University, 2020). While the most developed regions of the world have battled with the virus, recording thousands of infections and deaths, it is unknown how Nigeria with a fragile and less sophisticated healthcare system will be able to confront the disease and stop it from spreading among its densely populated and already vulnerable populations. With no proven and acceptable pharmaceutical cure, the best way to curb the virus and prevent it from spreading, may therefore be the adoption of precautionary behaviors (Güner et al., 2020; Wilder-Smith and Freedman, 2020; World Health Organization WHO, 2020b). Precautionary behavior such as quarantine of infected persons, social distancing (e.g., self-isolation, school, workplace and market closures, cancelation of large public gatherings, etc.) and hygienic practices (e.g., frequent handwashing with soap, using a face masks, use of hand sanitizers, etc.) have been identified as infection control measures which help curtail the spread of infections (Leppin and Aro, 2009). In extreme cases, community-wide containments are also adopted (Sjödin et al., 2020). Hatchett et al. (2007) stated that the quarantine measure adopted during the 1918 Influenza pandemic was largely responsible for halting the widespread of the influenza. According to Li et al. (2004), the number of secondary cases from an infected patient during the SARS outbreak of 2003 was clearly reduced if the infected patient was isolated within 4 days after onset of symptoms. Also, de Vlas et al. (2009) asserted that the enforcement of community-wide containments in China, was instrumental in the consistent and great decrease of infections during the SARS epidemic. In Nigeria, Liberia and other parts of West Africa, hygienic practices widely adopted during the 2014–2016 Ebola outbreaks (Althaus et al., 2015; Czerniewska and White, 2020) and the 2012 Hepatitis E outbreak in South Sudan (Phillips et al., 2015) proved very useful in curbing the spread of infections across the regions. All across the globe, the most effective way of delaying the spread of infections, especially in times when vaccines are not yet available, has been the adoption of precautionary behaviors (Tang et al., 2012; Ebrahim and Memish, 2020; Sjödin et al., 2020). However, the challenge often is the knowledge and awareness level of individuals about the infectiousness of diseases (Hassan et al., 2017; Alam et al., 2020) and whether such knowledge will translate into precautionary behavior (Ho et al., 2013; Cain et al., 2018; Li et al., 2020).
Already, a growing number of health-related studies suggest that there is very little association between knowledge of an infectious disease and actual engagement in a precautionary behavior (see for review Phillips et al., 2015; Seimetz et al., 2016; De Buck et al., 2017). Studies now suggest that the path from knowledge/awareness to actual precautionary behavior is often mediated by certain factors such as risk perceptions/worry (Brug et al., 2004; Taglioni et al., 2013), self efficacy (Rimal, 2000) attention, information surveillance and elaboration (Raza et al., 2020), etc. Vartti et al. (2009) reported that people who are more knowledgeable about the related etiology of the disease, tend to worry more about being infected and therefore suggesting a link between knowledge and risk perception. It is worthy of note also that the trajectory of an infectious disease is often determined by the behavior of individuals, and the behavior is in turn related to individuals’ risk perception (Abdelrahman, 2020; Vijayaraghavan and Singhal, 2020; Zhang et al., 2020) and beliefs about the disease (Janz and Becker, 1984). Also, though there is relatively high knowledge of COVID-19 around the globe and among Nigerians in particular (Olapegba et al., 2020a,b), there is the possibility that competing myths and sacred narratives (Chukwuorji and Iorfa, 2020) may be downplaying involvement in precautionary behavior and therefore, it is important to investigate the path from knowledge/awareness of COVID-19 to precautionary behavior and the mediators and moderators that may be on this path. This will help in understanding the correlates and pathways to curbing the spread of the virus in Nigeria and other parts of the globe.
A study of this nature in the COVID-19 era is important because not only is a widely acceptable pharmaceutical cure currently unavailable, but amidst the high levels of social awareness of the pandemic coupled with its sudden and virulent nature, a lot of conspiracy theories have sprung up (Ahmed et al., 2020; Georgiou et al., 2020) leading to a possible decrease in willingness to engage in precautionary behaviors (Allington et al., 2020; Van Bavel et al., 2020). Perceptions about the nature and causes of the pandemic are also largely unfounded around evidence (Chukwuorji and Iorfa, 2020) and may influence engagement in precautionary behaviors among the people as well. Therefore, since issues related to precautionary health behavior in populations have been linked to individuals’ belief systems as well as their perceived fear or risks of contracting a disease, this study, borrowing from the health belief model (HBM) may offer explanations to the failure of the Nigerian people in adopting disease prevention strategies and screening tests for early detection and curbing the spread of the disease. Findings from this study may be used to guide health promotion and disease prevention programs in times of the COVID-19 or other pandemics and epidemics that may arise in the future.
The HBM has been used to explain and predict individual changes in health behaviors (Becker, 1974; Jones et al., 2015) and may also be important in understanding precautionary behaviors in the COVID-19 era. Specifically, the HBM offers risk (threat) perceptions (perception of susceptibility to a disease and perception of the severity of the disease) as important elements (channels of influence) that help in predicting individual health-related behaviors (Becker, 1974; Champion and Skinner, 2008; Cameron et al., 2009). This study therefore investigated how COVID-19 knowledge and risk perceptions could influence precautionary behaviors, specifically if risk perception may be mediating the relationship between COVID-19 knowledge and precautionary behaviors. Also, in line with Gustafson’s (1998) argument that gender structures give rise to systematic gender differences in the perception of risks, the study also sought to investigate if gender could moderate the mediating path from COVID-19 through risk perception to precautionary behavior. Although some studies have shown greater risk perception among males than females, the gender effect on risk behavior is partially mediated by risk propensity (a predisposition to risk) and this new and important insight tends to show that risk perception could assume any direction, depending on the potency of other underlying variables (Harris et al., 2006; Jayathilake, 2013). Moreover, some variables such as the greater perceived likelihood of negative outcomes have been found to partially mediate female’s lower propensity toward risk choices in gambling, recreation, and health domains (Harris et al., 2006) as well as the tendency of women being more risk averse than men (Nelson, 2015). Based on these considerations therefore, the following hypotheses were formulated:
• COVID-19 knowledge will predict precautionary behaviors such that higher levels of COVID-19 knowledge will give rise to higher levels of precautionary behavior.
• Risk perception will predict precautionary behaviors such that higher levels of risk perception will give rise to higher levels of precautionary behavior.
• Risk perception will mediate the prediction of precautionary behavior by COVID-19 knowledge (mediation hypothesis) and this effect will be stronger for females than their male counterparts (moderated mediation hypotheses).
The conceptual model of the expected moderated mediation is shown in Figure 1.
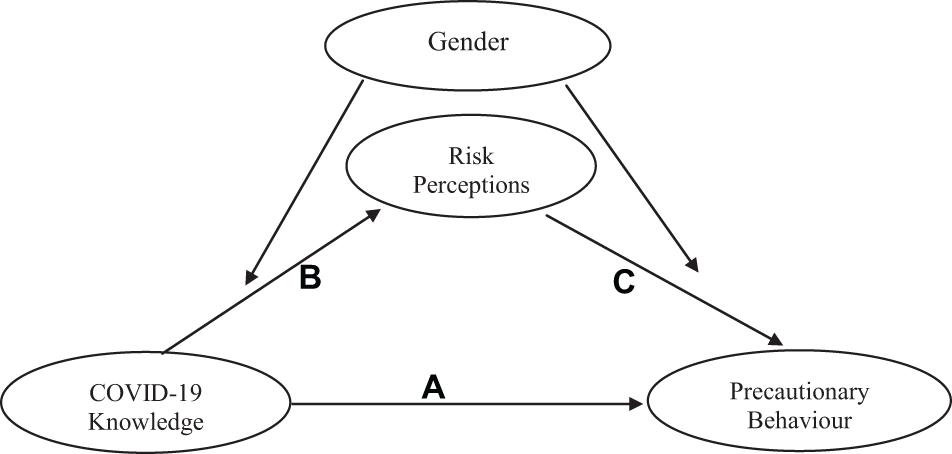
Figure 1. Conceptual model of moderated mediation for the effects of COVID-19 knowledge and risk perception on precautionary behavior.
Materials and Methods
Participants and Procedure
This web-based cross-sectional study was conducted in Nigeria using self-administered questionnaires between 20 April and 30 April 2020. The general population of study covered participants aged 15 years and above in the 36 states of Nigeria and the Federal Capital Territory. Participants were recruited online through a blend of Respondent-Driven Sampling (RDS) technique and Random Survey Sampling (RSS). RDS was considered appropriate due to social restrictions associated with the COVID-19 lockdown (occasioned by the rapid spread of the disease) which made it difficult to physically access prospective respondents at the time of data collection. Some persons across States, regions, and local governments in Nigeria were considered, and therefore helped in disseminating the survey links to others in the same category who also responded to the questionnaires. RSS was considered appropriate because it enables the dissemination of an online semi-structured questionnaire, with a consent form attached to it. The link to the questionnaire was sent through social media platforms (such as WhatsApp, Facebook, Instagram, Telegram, and Nairaland) to the key persons. Prospective respondents were then driven to share the link of the survey to residents in other parts of the country. Persons with access to the Internet, who understood the English Language, and were as well willing to give informed consent, were included. To arrive at 1,554 responses, reminder messages with links to the Google form were posted online daily. Ethical approval was sought from the Faculty of Social Sciences Ethical Board, University of Ibadan. Strict adherence to the ethical provisions on confidentiality and autonomy was also observed. Informed consent was obtained from participants using an embedded form. Participants were informed of the confidentiality of the study and also informed they could withdraw from the study at any point if they so desired.
Measures
The questionnaire assessed participants’ demographic characteristics (gender, age, marital status, ethnicity, educational qualification, religion, location, and perceived financial situation), and consisted of a battery of measures of COVID-19 knowledge, risk perceptions, and precautionary behavior.
COVID-19 Knowledge
COVID-19 knowledge was assessed using a 5-item Likert-type scale adapted from the Ebola knowledge scale (Rolison and Hanoch, 2015). Respondents’ knowledge of COVID-19 was arrived at by summing correct responses across item 1, source of COVID-19 [correct = (d)], item 2, transmission of COVID-19 [correct = (a), and (b),(c), or (d)], item 3, prevention of COVID-19, [correct = (b) and (d),(f), or (h)], item 4, symptoms of COVID-19 [correct = (a),(b), and (g)], and item 5, awareness of COVID-19 fatality, [correct = (a)], generating a maximum possible score of five.
COVID-19 Risk Perceptions
COVID-19 Risk Perceptions were measured using a 9-item Likert-type scale adapted from Brug et al. (2004)’s SARS risk perception Scale. Items were reworded to relate to coronavirus (e.g., “What level of threat do you think the COVID-19/Coronavirus pandemic poses to your job or studies?” and “How worried are you about contracting the Coronavirus?”). Participants rated these items on a 7-point Likert-type scale (1 = not at all likely, to 7 = extremely likely). A reliability coefficient (Cronbach’s alpha) of 0.71 was obtained in a pilot testing of the scale while the current data set yielded 0.75.
Precautionary Behavior
An adapted 10-item Likert-type scale was used to examine the precautionary behavior of participants during the COVID-19 pandemic (Barr et al., 2008; Duncan et al., 2009). The 10-item scale has statements dealing with actions taken in advance to protect against possible exposure to COVID-19. Sample items include: “I prefer to wash my hands pretty soon after shaking someone’s hand” and “I am comfortable going to very crowded places (reverse scored).” Participants rated items on a separate 7-point Likert type scale (one strongly disagree; seven strongly agree). Items four and six are reverse scored. A reliability coefficient (Cronbach’s alpha) of 0.80 was obtained in a pilot study of the scale while the current data set yielded an alpha of 0.75.
Data Analysis
The data were analyzed using SPSS version 22.0 software. Descriptive statistics, using frequencies, percentages, means, and standard deviations, were conducted for socio-demographic variables and precautionary behavior. To compute COVID-19 knowledge, the mean score and standard deviation for the sample population were calculated and scores above the norm were indicative of high knowledge of COVID-19, while scores below the norm indicated low knowledge of COVID-19. For risk perception and precautionary behavior, scores in each scale were summed to obtain a composite aggregate for each measure. Higher scores indicated higher risk perception or precautionary behavior (as the case was). Pearson’s correlation was used to establish the relationship between the demographics and major variables of interest. Moderated mediation analysis was carried out with model 58 of Hayes PROCESS macro for SPSS (Hayes, 2018). The model 58 of the Hayes PROCESS macro uses ordinary least squares (OSL) analysis for calculating the mediation and the moderated mediation effects and bootstrapping for calculating the confidence intervals (CI) (Miers et al., 2017). Our choice of these statistics was influenced by the consideration that a moderated mediation would test the influence of a fourth variable (gender) on the mediated relationship between COVID-19 knowledge and precautionary behavior. In this moderated mediation model, precautionary behavior was entered as the outcome variable, COVID-19 knowledge as the independent variable, risk perception as the mediator. Gender was included as the moderator on the dependent variables risk perception and precautionary behavior. Age was included as a covariate in the model. See Figure 1 for a representation of the conceptual model.
Results
Participants were 1,554 persons (42.7% females and 57.3% males; mean age = 27.43, SD = 9.75). The sample characteristics of participants, including educational qualification, perceived financial status, relationship status, religion, and geopolitical groupings, and their statistical values are shown in Table 1.
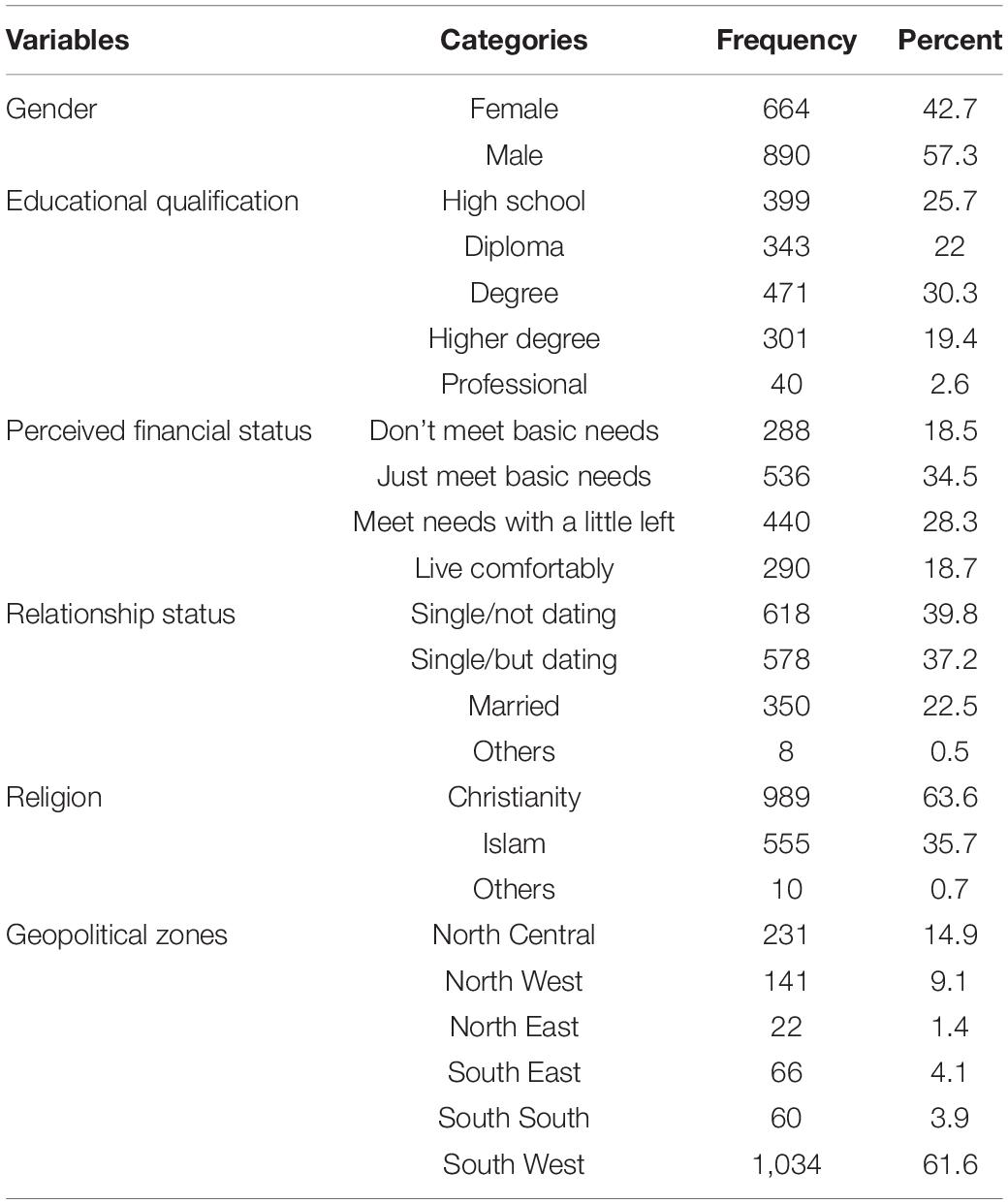
Table 1. Sample characteristics (n = 1,554).
Means, standard deviations, and correlations among the observed variables were computed separately for males and females and shown in Table 2. Among females, being older (older age) was related to higher COVID-19 knowledge (r = 0.09, p < 0.05), and higher precautionary behavior (r = 0.10, p < 0.01), but not risk perception (r = 0.04, p > 0.05). Higher COVID-19 knowledge was related to greater risk perception (r = 0.09, p < 0.05) and greater precautionary behavior (r = 0.18, p < 0.01). Higher risk perception was related to greater precautionary behavior (r = 0.23, p < 0.01) (Table 2).
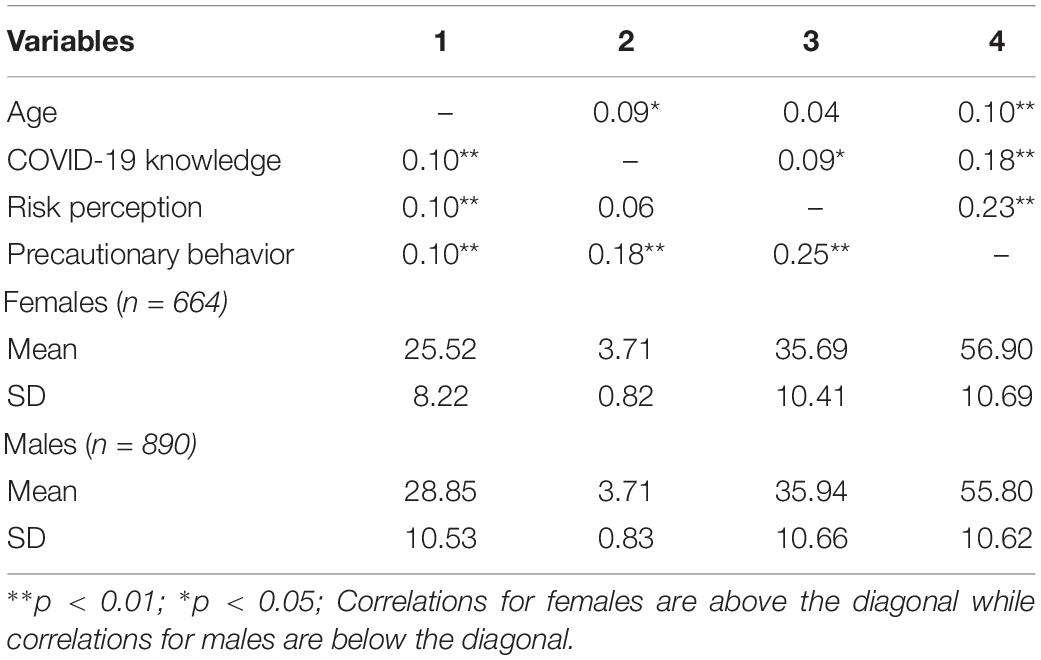
Table 2. Means, standard deviations, and intercorrelations of study variables separated by gender (n = 1,551).
For males, being older (older age) was related to higher COVID-19 knowledge (r = 0.10, p < 0.01), higher risk perception (r = 0.10, p < 0.01), and higher precautionary behavior (r = 0.10, p < 0.01). Higher COVID-19 knowledge was related to greater risk perception (r = 0.250, p < 0.01) and higher precautionary behavior (r = 0.18, p < 0.01). Risk perception was not related significantly to precautionary behavior (r = 0.06, p > 0.05).
In Table 3 it was found that older age predicted increased risk perception. Gender did not predict risk perception. Greater COVID-19 knowledge predicted elevated levels of risk perception. Gender did not moderate the association of COVID-19 knowledge and risk perception, given that the interaction term was not significant. The predictors accounted for 1% of the variance in risk perception [R2 = 0.01, F(4,1549) = 4.07, p = 0.003].
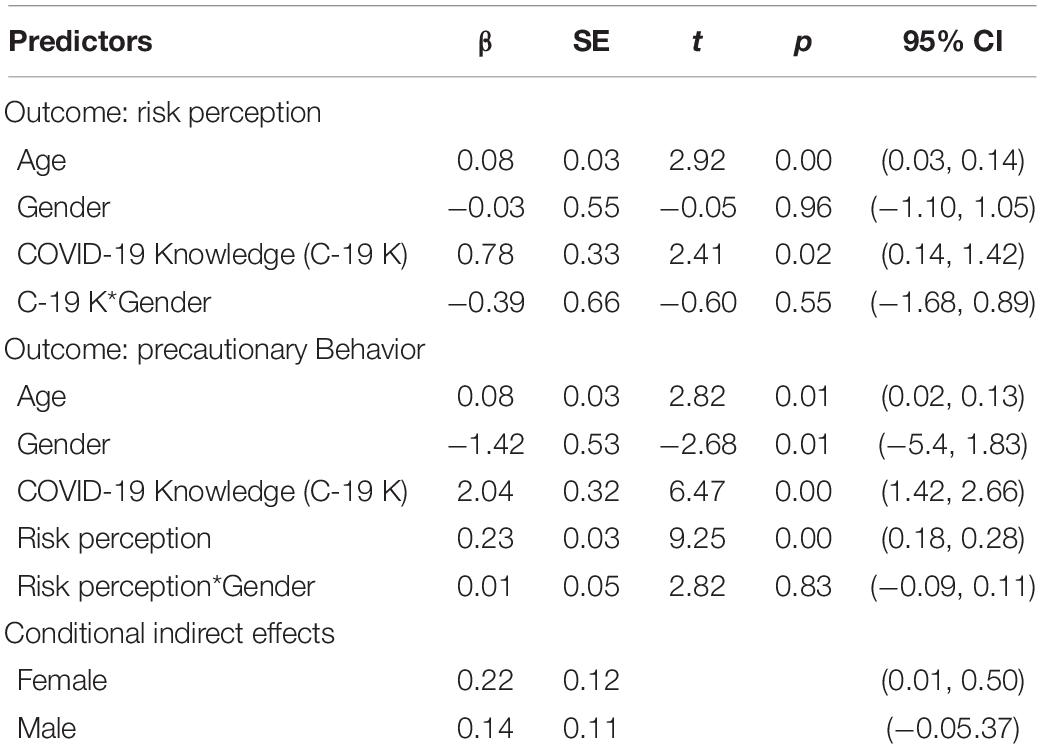
Table 3. Moderated mediation results for the link between COVID-19 knowledge and precautionary behavior.
In Table 3 also, it was found that older age predicted increased precautionary behavior. Gender did not predict precautionary behavior. Greater COVID-19 knowledge predicted elevated levels of precautionary behavior. Higher levels of risk perception predicted higher levels of involvement in precautionary behaviors. Gender did not moderate the association of risk perception and precautionary behavior, given that the interaction term was not significant. Our hypothesis of a moderated mediation effect was supported as evidenced by a significant indirect effect of COVID-19 knowledge on precautionary behavior through risk perception among females [B = 0.22, 95% CI = (0.01, 0.50)], but not males (B = 0.14, 95% CI = −0.05, 0.37). Note that the moderated mediation is significant when the 95% CI did not encompass zero as shown in the case for females. The predictors accounted for 9% of the variance in precautionary behavior [R2 = 0.09, F(5,1548) = 31.46, p = 0.00]. The moderated mediation model with standardized coefficients is presented in Figure 2.
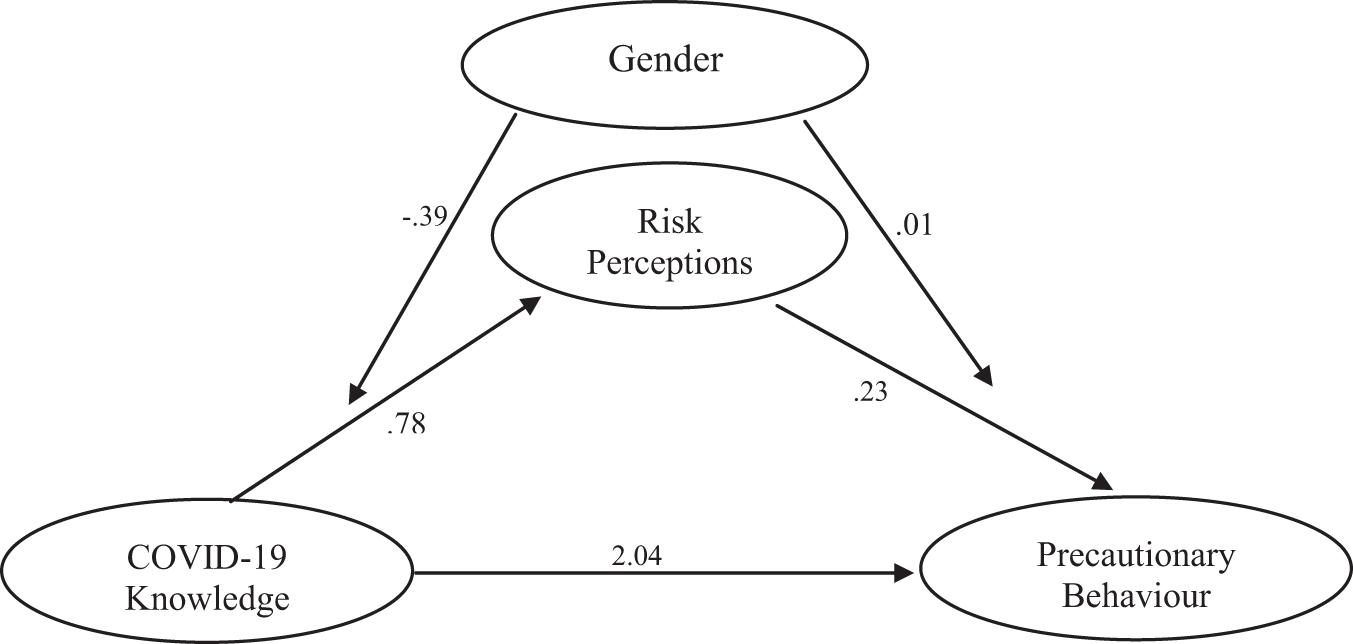
Figure 2. Moderated mediation model showing standardized coefficients.
Discussion
The study investigated COVID-19 knowledge, risk perception, and precautionary behavior among Nigerians and the moderated-mediation effect among the variables. Findings showed that COVID-19 knowledge had a significant influence on precautionary behavior. This supported our hypothesis and mirrored previous findings (Brug et al., 2004; Li et al., 2020). It is logical to expect that when individuals are aware of threats, they will adopt reasonable behaviors that may avert the threat from causing harm. However, other studies (e.g., Phillips et al., 2015; Seimetz et al., 2016; De Buck et al., 2017) did not report this relationship but rather suggested that knowledge in itself may not always lead to precautionary health behaviors until the relationship is mediated upon by other factors (Rimal, 2000; Taglioni et al., 2013; Raza et al., 2020). These may on the other hand explain the observation that even though the knowledge of the pandemic is relatively high, some individuals still do not adhere to precautionary measures according to the protocol laid down by authorities [see Table 4 (Appendix Table 1)]. They may be said to be exhibiting attitude-behavior discrepancies, a tendency to be oblivious of the negative consequences due to inherent self-interests (as can be seen in pockets of disobedience to precautionary health behaviors in the face of the pandemic).
Consistent with previous findings (e.g., Abdelrahman, 2020; Vijayaraghavan and Singhal, 2020; Zhang et al., 2020) therefore, we postulated also that perception of risk will serve as a pathway through which knowledge and awareness of COVID-19 will influence precautionary behavior and that this influence may be more for females than for males. We also tested the direct influences of risk perception, age, and gender on precautionary behavior. As hypothesized, risk perception significantly predicted precautionary behavior, agreeing with previous findings (Brug et al., 2004; Lau et al., 2010). This implies that perception of risk is an important variable that could inform valid and reliable precautionary behaviors and possible means of preventing a newly emerging contagious disease like COVID-19. Studies supporting the present result suggested that an individual’s ability to promote precautionary behavior largely relies on the perceived risk of contracting a disease and that risk perception is a strong predictor of precautionary behaviors (Lau et al., 2010; Zhang et al., 2020). Moreover, as outlined by the HBM, for individuals to willingly engage in precautionary behaviors, they may have to, first and foremost, significantly perceive the risk that such disease poses to them.
The study also showed that being older predicted more precautionary behavior and this is supported by Zhang et al. (2020)’s study. This finding indicates that older people and those with underlying comorbid diseases took more precautionary measures compared with younger people. International and national medical agencies have stated that older people and those with underlying diseases are more vulnerable to coronavirus and at risk of dying (World Health Organization WHO, 2020b). This may explain why elderly respondents reported engaging more in precautionary measures compared to the younger respondents who engaged in less precautionary behaviors as observed in the study.
The result that gender differences existed in precautionary behavior is in line with past studies where females have consistently been found to engage in more precautionary behaviors than their male counterparts (Brug et al., 2004; Bish and Michie, 2010). This implies that females have a greater tendency than males to engage in precautionary behaviors such as the washing of hands, use of hand sanitizers, wearing of face masks, cleaning of surfaces, and having plans to visit a hospital or call emergency numbers in case of suspected symptoms, etc. This may be related to the perceived global vulnerability of females to illness (Duncan et al., 2009; Dellar et al., 2015). This relationship between gender and precautionary behavior may probably indicate that females perceive themselves as more susceptible to adverse conditions than males.
Also, it was observed that risk perception mediated the relationship between COVID-19 knowledge and precautionary behavior. This outcome relates to previous studies, for instance, a study conducted among the Saudi and non-Saudi Arabian pilgrims in 2014 on the outbreak of Middle East respiratory syndrome showed that overall knowledge of causative agents, the symptoms of the virus and its similarity to the disease and risk perception of the virus were associated with precautionary behavior (Hosam et al., 2017). The results showed that knowledge influenced precautionary behavior through the perception of risk. In other words, individuals who reported high levels of knowledge of the disease but did not perceive it as a risk did not initiate and engage in precautionary behaviors. This finding also strongly supports the assertion of the HBM that risk perception serves as a channel of influence that helps in predicting health behavior (Becker, 1974; Champion and Skinner, 2008; Cameron et al., 2009).
We hypothesized that the effect of the mediator (risk perception) will be moderated by another variable (gender). This hypothesis was influenced by previous findings that risk perception differs across gender. Most times the moderation may occur on any or all path(s) in the mediation model. Although, few studies have investigated if gender moderates the pathway of knowledge/awareness of an infectious disease through risk perception to precautionary health behavior, our study contributed to existing body of knowledge on the moderating influence of gender on the pathway of knowledge/awareness of an infectious disease through risk perception to precautionary health behavior, thus advancing the science in this area for other researchers to explore. Though no direct study with similar focus and results were found, a meta-analytic study on gender differences in risk perception pointed out that gender influences perception of risk (Byrnes et al., 1999). Also, owing to the offspring risk hypothesis (Harris et al., 2006), females tend to perceive greater risks than males because they are primary caregivers by nature and if people perceive more risks in the world, they will possibly be more effective at preserving any offspring under their care. Moreover, this finding corroborates a recent study that showed gender differences in risk perception of drug use between males and females (Ottu and Umoren, in press). In sum, our findings showed that risk perception serves as a pathway through which COVID-19 knowledge may influence precautionary behavior and that this may be higher in females than in males.
Implication of Findings
Much more efforts are needed to understand the factors that promote precautionary behaviors in times of pandemics and these efforts may benefit from the findings in this study. One, the dynamic nature of infectious disease transmission suggests that behavior by several individuals may have a significant impact on the trajectory of an outbreak. However, individuals may not take precautions if they are not aware or have wrong or inadequate knowledge about the outbreak. Therefore, in line with the findings of our study that more accurate COVID-19 knowledge predicted greater precautionary behavior, and coupled with the fact that there are already myths and conspiracy theories surrounding the origin and nature of COVID-19 (Ahmed et al., 2020; Georgiou et al., 2020Shimizu, 2020), we recommend enlightenment campaigns aimed at promoting adequate knowledge of the COVID-19 pandemic as well as addressing the current misconceptions and misinformation about the disease. In places where such knowledge is already influenced by conspiracy theories, it is important to reorient the public on the real nature and origin of the disease. In unaffected areas, true risks may be low, but due to the worldwide media coverage of the pandemic, there is the possibility of elevated levels of risk perception. Therefore, the scientific community may leverage on this to explore ways to best communicate risks to individuals without unnecessarily causing panic. Individuals who perceive themselves as being at risk of contracting the virus should engage in precautionary behaviors as suggested in this study rather than form stereotypes and prejudices against persons perceived to be the sources of the disease outbreak as reported in earlier findings (Chukwuorji and Iorfa, 2020; Olapegba et al., 2020a,b). It is therefore, necessary that knowledge, realistic risks, and effective precautionary behaviors are communicated through various information sources so that people can engage in more preventive behaviors than depend on vaccines.
Consequently and in line with the HBM, individuals may need to be informed about the potential risks of infection to adopt the right precautionary measures (Brug et al., 2004). Campaigns at raising awareness of risks should therefore convey the consequences of the health issues associated with risk behaviors in a clear and unambiguous fashion. This will help individuals to understand perceived severity of the risks associated with the disease. Measures to control future outbreaks should not be limited to the development of vaccines, but also adequately informing the public about the true nature (and origin of the infections) as well as risks as these have shown to be predictors of precautionary behavior. The findings from this study along with previous findings justify the need to look more closely at the drivers of precautionary behaviors in individuals. This will serve as a proactive step toward curbing future endemics or pandemics.
Conclusion
Our study revealed, COVID-19 knowledge predicted precautionary behavior and risk perception significantly predicted precautionary behavior. Moreover, age and gender emerged as important variables associated with precautionary behavior. Older people readily showed a heightened tendency toward precautionary behavior than young persons. Females had higher likelihood of exhibiting precautionary behavior compared to males. In the area of mediation, risk perception aided the relationship between COVID-19 Knowledge and Precautionary behavior. In other words, knowledge influenced precautionary behavior through the perception of risk. The test for moderation indicated that gender (in this case, being female) was important as a precautionary index in risk perception than being male. Specifically, our results show that gender moderated the indirect path from COVID-19 Knowledge to precautionary behavior. It was also noted that awareness campaigns and psychological intervention strategies on COVID-19 related activities may be particularly important for males than females. Drawing from the health belief model, we recommend that COVID-19 awareness campaigns should target raising more awareness of the risks associated with the infection to make individuals engage more in precautionary behaviors.
Limitation of the Study
This study relatively utilized a limited number of participants considering the population of the country; studies utilizing larger sample sizes are suggested. The use of an online web survey data collection approach in our study may have resulted in underrepresentation of the unprivileged and the uneducated. The implication is that the views of that section of the society were left out of the study. This raises the issue of coverage in addition to other methodological concerns associated with non-probability sampling and these could pose problems of generalization. Thus, our findings should be treated with caution without considering these as representative of adequately sampled population with optimal distribution across commonly described socioeconomic strata. To our knowledge, this is the first study on the relationship between COVID-19 knowledge, risk perception, and precautionary behavior among Nigerians. This data could be used as a baseline to explore differences with samples made up of persons without access to the Internet.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
SI, OA, and PO designed the study. OA, RO, SK, JG, AD, SI, IO, and PO contributed to perform the investigation and data collection. SI and OA analyzed the data. SI, RO, and SK drafted the initial manuscript. SI, IO, OA, and PO critically revised the manuscript for important intellectual content. All authors discussed the results and contributed to the final manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
Abdelrahman, M. K. (2020). Personality traits, risk perception and social distancing during COVID-19. PsyArXiv [Preprint]. doi: 10.31234/osf.io/6g7kh
Ahmed, W., Vidal-Alaball, J., Downing, J., and Seguí, F. L. (2020). COVID-19 and the 5G conspiracy theory: social network analysis of Twitter data. J. Med. Internet Res. 22:e19458. doi: 10.2196/19458
Alam, A., Siddiqui, M. F., Imam, N., Ali, R., Mushtaque, M., and Ishrat, R. (2020). Covid-19: current knowledge, disease potential, prevention and clinical advances. Turk. J. Biol. 44, 121–131. doi: 10.3906/biy-2005-29
Allington, D., Duffy, B., Wessely, S., Dhavan, N., and Rubin, J. (2020). Health-protective behaviour, social media usage and conspiracy belief during the COVID-19 public health emergency. Psychol. Med. [Epub ahead of print]. doi: 10.1017/S003329172000224X
Althaus, C. L., Low, N., Musa, E. O., Shuaib, F., and Gsteiger, S. (2015). Ebola virus disease outbreak in Nigeria: transmission dynamics and rapid control. Epidemics 11, 80–84. doi: 10.1016/j.epidem.2015.03.001
Barr, M., Raphael, B., Taylor, M., Stevens, G., Jorm, L., Giffin, M., et al. (2008). Pandemic influenza in Australia: using telephone surveys to measure perceptions of threat and willingness to comply. Infect. Dis. 8, 117–130. doi: 10.1186/1471-2334-8-117
Becker, M. H. (1974). The Health Belief Model and personal health behavior. Health Educ. Monogr. 2, 324–508.
Biscayart, C., Angeleri, P., Lloveras, S., Chaves, T., Schlagenhauf, P., and Rodriguez-Morales, A. J. (2020). The next big threat to global health? 2019 novel coronavirus (2019-nCoV): what advice can we give to travelers? — Interim recommendations January 2020, from the Latin-American Society for Travel Medicine (SLAMVI). Travel Med. Infect. Dis. 33:101567. doi: 10.1016/j.tmaid.2020.101567
Bish, A., and Michie, S. (2010). Demographic and attitudinal determinants of protective behaviours during a pandemic: a review. Br. J. Health Psychol. 15, 797–824. doi: 10.1348/135910710x485826
Brug, J., Aro, A. R., Oenema, A., de Zwart, O., Richardus, J. H., and Bishop, G. D. (2004). SARS risk perception, knowledge, precautions, and information sources, the Netherlands. Emerg. Infect. Dis. 10, 1486–1489. doi: 10.3201/eid1008.040283
Byrnes, J. P., Miller, D. C., and Schafer, W. D. (1999). Gender differences in risk taking: a meta-analysis. Psychol. Bull. 125, 367–383. doi: 10.1037/0033-2909.125.3.367
Cain, A. A., Edwards, M. E., and Still, J. D. (2018). An exploratory study of cyber hygiene behaviors and knowledge. J. Inform. Security Applicat. 42, 36–45. doi: 10.1016/j.jisa.2018.08.002
Cameron, K. A., Rintamaki, L. S., Kamanda-Kosseh, M., Noskin, G. A., Baker, D. W., and Makoul, G. (2009). Using theoretical constructs to identify key issues for targeted message design: African American seniors’ perceptions about influenza and influenza vaccination. Health Commun. 24, 316–326. doi: 10.1080/10410230902889258
Champion, V., and Skinner, C. S. (2008). “The Health Belief Model,” in Health Behavior and Health Education. 4, eds K. Glanz, B. Rimer, and K. Viswanath (San Francisco, CA: Jossey-Bass), 45–65.
Chukwuorji, J. C., and Iorfa, S. K. (2020). Commentary on the coronavirus pandemic: Nigeria. Psychol. Trauma Theory Res. Pract. Policy 12, S188–S190. doi: 10.1037/tra0000786
Czerniewska, A., and White, S. (2020). Hygiene programming during outbreaks: a qualitative case study of the humanitarian response during the Ebola outbreak in Liberia. BMC Public Health 20:154. doi: 10.1186/s12889-020-8240-9
De Buck, E., Van Remoortel, H., Hannes, K., Govender, T., Naidoo, S., Avau, B., et al. (2017). Approaches to promote handwashing and sanitation behaviour change in low-and middle-income countries: a mixed method systematic review. Campbell Syst. Rev. 13, 1–447. doi: 10.1002/cl2.162
de Vlas, S. J., Feng, D., Cooper, B. S., Fang, L. Q., Cao, W. C., and Richardus, J. H. (2009). The impact of public health control measures during the SARS epidemic in mainland China. Trop. Med. Int. Health 14, 101–104. doi: 10.1111/j.1365-3156.2009.02348.x
Dellar, R. C., Dlamini, S., and Karim, Q. A. (2015). Adolescent girls and young women: key populations for HIV epidemic control. J. Int. AIDS Soc. 18(Suppl. 1), 19408. doi: 10.7448/IAS.18.2.19408
Duncan, L. A., Schaller, M., and Park, J. H. (2009). Perceived vulnerability to disease: development and validation of a 15-item self-report instrument. Pers. Individ. Diff. 37, 541–546. doi: 10.1016/j.paid.2009.05.001
Ebrahim, S. H., and Memish, Z. A. (2020). Saudi Arabia’s drastic measures to curb the COVID-19 outbreak: temporary suspension of the Umrah pilgrimage. J. Travel Med. 27:taaa029.
Georgiou, N., Delfabbro, P., and Balzan, R. (2020). COVID-19-related conspiracy beliefs and their relationship with perceived stress and pre-existing conspiracy beliefs. Pers. Individ. Diff. 166:110201. doi: 10.1016/j.paid.2020.110201
Güner, R., Hasanoǧlu, I., and Aktaş, F. (2020). COVID-19: prevention and control measures in community. Turk. J. Med. Sci. 50, 571–577. doi: 10.3906/sag-2004-146
Gustafson, P. E. (1998). Gender differences in risk perception: theoretical and methodological perspectives. Risk Anal. 18, 805–811. doi: 10.1023/b:rian.0000005926.03250.c0
Harris, C. R., Jenkins, M., and Glaser, D. (2006). Gender differences in risk assessment: why do women take fewer risks than men? Judg. Dec. Making 1, 48–63.
Hassan, O. A., Affognon, H., Rocklöv, J., Mburu, P., Sang, R., Ahlm, C., et al. (2017). The One Health approach to identify knowledge, attitudes and practices that affect community involvement in the control of Rift Valley fever outbreaks. PLoS Negl. Trop. Dis. 11:e0005383. doi: 10.1371/journal.pntd.0005383
Hatchett, R. J., Mecher, C. E., and Lipsitch, M. (2007). Public health interventions and epidemic intensity during the 1918 influenza pandemic. Proc. Natl. Acad. Sci. U.S.A. 104, 7582–7587. doi: 10.1073/pnas.0610941104
Hayes, A. F. (2018). Partial, conditional, and moderated moderated mediation: quantification, inference, and interpretation. Commun. Monogr. 85, 4–40. doi: 10.1080/03637751.2017.1352100
Ho, S. S., Peh, X., and Soh, V. W. (2013). The cognitive mediation model: factors influencing public knowledge of the H1N1 pandemic and intention to take precautionary behaviors. J. Health Commun. 18, 773–794. doi: 10.1080/10810730.2012.743624
Hosam, M. A., Raed, A. S., Alharthi, M. H., Ziyad, A. A., Nahar, S. A., Altowairqi, A. E., et al. (2017). Knowledge and awareness of Middle East respiratory syndrome coronavirus among Saudi and Non-Saudi Arabian pilgrims. Int. J. Health Sci. 11, 20–25.
Janz, N. K., and Becker, M. H. (1984). The health belief model: “a decade later”. Health Educ. Behav. 11, 1–47. doi: 10.1177/109019818401100101
Jayathilake, B. (2013). Gender Effects on Risk Perception and Risk Behaviour of Entrepreneurs at SMES in Sri Lanka. Asia J. Mark. Manag. Rev. 2, 1–11. doi: 10.4038/jccpsl.v15i1.4934
John Hopkins University (2020). Coronavirus COVID-19 Global Cases by the Center for Systems Science and Engineering (CSSE). Available online at: https://coronavirus.jhu.edu/map.html (accessed July 10, 2020).
Jones, C. L., Jensen, J. D., Scherr, C. L., Brown, N. R., Christy, K., and Weaver, J. (2015). The Health Belief Model as an explanatory framework in communication research: exploring parallel, serial, and moderated mediation. Health Commun. 30, 566–576. doi: 10.1080/10410236.2013.873363
Lau, J. T., Griffiths, S., Choi, K. C., and Lin, C. (2010). Prevalence of preventive behaviors and associated factors during early phase of the H1N1 influenza epidemic. Am. J. Infect. Control 38, 374–380. doi: 10.1016/j.ajic.2010.03.002
Leppin, A., and Aro, A. R. (2009). Risk perception related to SARS and avian influenza: theoretical foundations of current behavioral research. Int. J. Behav. Med. 16, 7–29. doi: 10.1007/s12529-008-9002-8
Li, J., Yang, A., Dou, K., Wang, L., Zhang, M., and Li, X. (2020). Chinese public’s knowledge, perceived severity, and perceived controllability of the COVID-19 and their associations with emotional and behavioural reactions, social participation, and precautionary behaviour: a national survey. PsyArXiv [Preprint]. doi: 10.31234/osf.io/5tmsh
Li, Y., Yu, I. T., Xu, P., Lee, J. H. W., Wong, T. W., Ooi, P. L., et al. (2004). Predicting super spreading events during the 2003 severe acute respiratory syndrome epidemics in Hong Kong and Singapore. Am. J. Epidemiol. 160, 719–728. doi: 10.1093/aje/kwh273
Miers, A. C., Ziermans, T., and van Rijn, S. (2017). Connecting the dots between schizotypal symptoms and social anxiety in youth with an extra X chromosome: a mediating role for catastrophizing. Brain Sci. 7:113. doi: 10.3390/brainsci7090113
Nelson, J. A. (2015). Are women really more risk averse than men? A reanalyis of the literature using expanded methods. J. Econ. Surv. 29, 566–585. doi: 10.1111/joes.12069
Olapegba, P. O., Ayandele, O., Kolawole, S. O., Oguntayo, R., Gandi, J. C., Dangiwa, A. L., et al. (2020a). COVID-19 Knowledge and Perceptions in Nigeria. PsyArXiv [Preprint]. doi: 10.31234/osf.io/j356x
Olapegba, P. O., Iorfa, S. K., Kolawole, S. O., Oguntayo, R., Gandi, J. C., Ottu, I. F. A., et al. (2020b). Survey data of COVID-19-related Knowledge, Risk Perceptions and Precautionary Behavior among Nigerians. Data Brief 30:105685. doi: 10.1016/j.dib.2020.105685
Ottu, I. F. A., and Umoren, A. M. (in press). Social influence processes and life orientation in risk perception of drug use among undergraduates. African. J. Drug Alcohol Stud.
Phillips, R. M., Vujcic, J., Boscoe, A., Handzel, T., Aninyasi, M., Cookson, S. T., et al. (2015). Soap is not enough: handwashing practices and knowledge in refugee camps, Maban County, South Sudan. Conflict Health 9:39.
Raza, S. H., Iftikhar, M., Mohamad, B., Pembecioǧlu, N., and Altaf, M. (2020). Precautionary behavior toward dengue virus through public service advertisement: mediation of the individual’s attention, information surveillance, and elaboration. SAGE Open 10:2158244020929301.
Rimal, R. N. (2000). Closing the knowledge-behavior gap in health promotion: the mediating role of self-efficacy. Health Commun. 12, 219–237. doi: 10.1207/s15327027hc1203_01
Rolison, J. J., and Hanoch, Y. (2015). Knowledge and risk perceptions of the Ebola virus in the United States. Preventive Med. Rep. 2, 262–264. doi: 10.1016/j.pmedr.2015.04.005
Seimetz, E., Kumar, S., and Mosler, H. J. (2016). Effects of an awareness raising campaign on intention and behavioural determinants for handwashing. Health Educ. Res. 31, 109–120. doi: 10.1093/her/cyw002
Shimizu, K. (2020). 2019-nCoV, fake news, and racism. Lancelet Correspondence 395, 685–686. doi: 10.1016/S0140-6736(20)30359-7
Sjödin, H., Wilder-Smith, A., Osman, S., Farooq, Z., and Rocklöv, J. (2020). Only strict quarantine measures can curb the coronavirus disease (COVID-19) outbreak in Italy, 2020. Euro. Surveill. 25:2000280. doi: 10.2807/1560-7917.ES.2020.25.13.2000280
Taglioni, F., Cartoux, M., Dellagi, K., Dalban, C., Fianu, A., Carrat, F., et al. (2013). The influenza A (H1N1) pandemic in Reunion Island: knowledge, perceived risk and precautionary behaviour. BMC Infect. Dis. 13:34. doi: 10.1186/1471-2334-13-34
Tang, S., Xiao, Y., Yuan, L., Cheke, R. A., and Wu, J. (2012). Campus quarantine (Fengxiao) for curbing emergent infectious diseases: lessons from mitigating A/H1N1 in Xi’an, China. J. Theor. Biol. 295, 47–58. doi: 10.1016/j.jtbi.2011.10.035
Van Bavel, J. J., Baicker, K., Boggio, P. S., Capraro, V., Cichocka, A., Cikara, M., et al. (2020). Using social and behavioural science to support COVID-19 pandemic response. Nat. Hum. Behav. 4, 460–471.
Vartti, A. M., Oenema, A., Schreck, M., Uutela, A., de Zwart, O., Brug, J., et al. (2009). SARS knowledge, perceptions, and behaviors: a comparison between Finns and the Dutch during the SARS outbreak in 2003. Int. J. Behav. Med. 16, 41–48. doi: 10.1007/s12529-008-9004-6
Vijayaraghavan, P., and Singhal, D. (2020). A descriptive study of Indian General Public’s Psychological responses during COVID-19 pandemic lockdown period in India. PsyArXiv [Preprint]. doi: 10.31234/osf.io/jeksn
Wilder-Smith, A., and Freedman, D. O. (2020). Isolation, quarantine, social distancing and community containment: pivotal role for old-style public health measures in the novel coronavirus (2019-nCoV) outbreak. J. Travel Med. 27:taaa020. doi: 10.1093/jtm/taaa020
World Health Organization [WHO] (2020a). Coronavirus Disease 2019 (COVID-19) Situation Report – 118. Geneva: World Health Organization.
World Health Organization [WHO] (2020b). Responding to Community Spread of COVID-19. Geneva: World Health Organization.
Zaka, A., Shamloo, S. E., Fiorente, P., and Tafuri, A. (2020). COVID-19 pandemic as a water shed moment: a call for systematic psychological health care for frontline medical staff. J. Health Psychol. [Epub ahead of print]. doi: 10.1177/135910532092514
Zhang, X., Wang, F., Zhu, C., and Wang, Z. (2020). Willingness to self-Isolate when facing a pandemic risk: model, empirical test, and policy recommendations. Int. J. Environ. Res. Public Health 17:197. doi: 10.3390/ijerph17010197
Zhao, S., Lin, Q., Ran, J., Musa, S. S., Yang, G., Wang, W., et al. (2020). Preliminary estimation of the basic reproduction number of novel coronavirus (2019-nCoV) in China, from 2019 to 2020: a data-driven analysis in the early phase of the outbreak. Int. J. Infect. Dis. 92, 214–217. doi: 10.1016/j.ijid.2020.01.050
Appendix
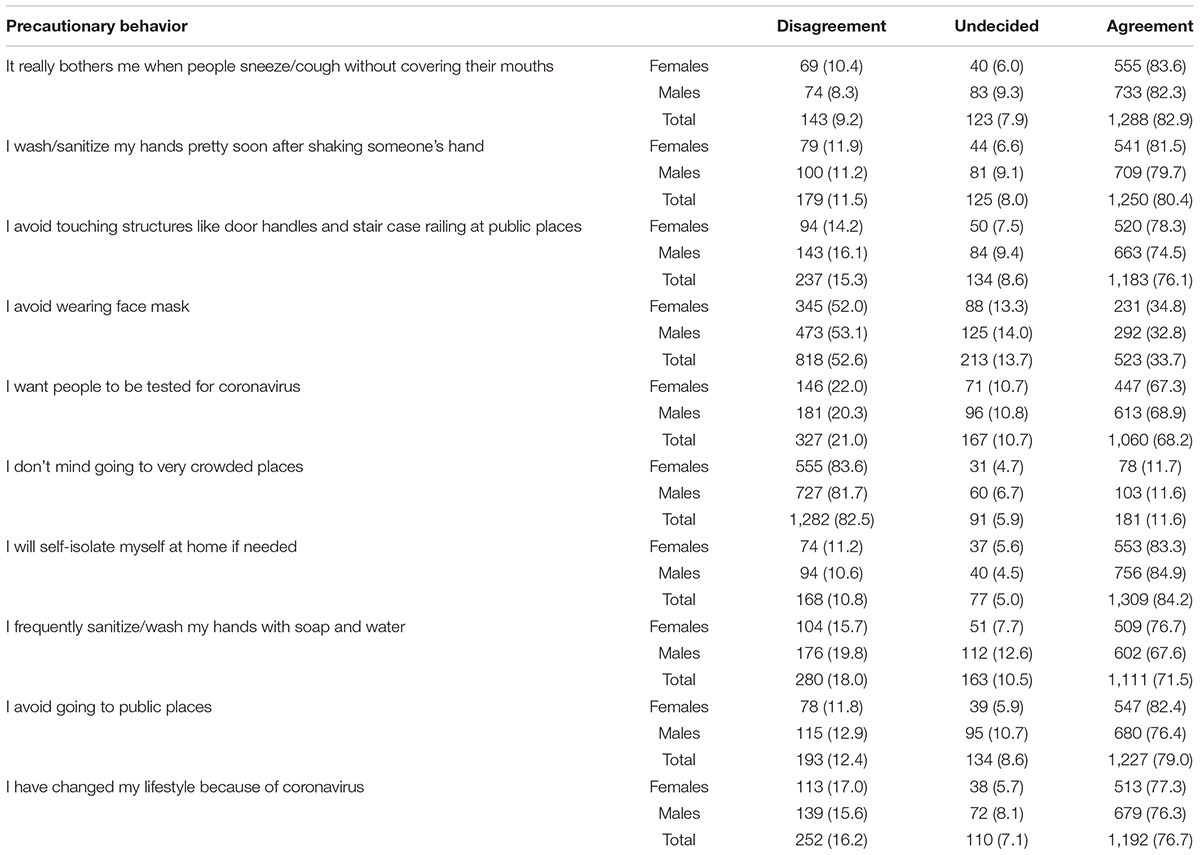
Table 4 | Precautionary behavior engaged in by Nigerians.
Keywords: COVID-19, knowledge, risk perception, precautionary behavior, Nigeria, gender
Citation: Iorfa SK, Ottu IFA, Oguntayo R, Ayandele O, Kolawole SO, Gandi JC, Dangiwa AL and Olapegba PO (2020) COVID-19 Knowledge, Risk Perception, and Precautionary Behavior Among Nigerians: A Moderated Mediation Approach. Front. Psychol. 11:566773. doi: 10.3389/fpsyg.2020.566773
Received: 28 May 2020; Accepted: 02 November 2020;
Published: 20 November 2020.
Edited by:
Tigran Melkonyan, University of Alabama, United StatesReviewed by:
Olufemi Ajumobi, University of Nevada, Reno, United StatesDušanka Mitrović, University of Novi Sad, Serbia
Copyright © 2020 Iorfa, Ottu, Oguntayo, Ayandele, Kolawole, Gandi, Dangiwa and Olapegba. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Steven K. Iorfa, c3RldmVuLmlvcmZhLjE3NjI4MEB1bm4uZWR1Lm5n; Olusola Ayandele, c29sYWF5YW5AZ21haWwuY29t