 Marco Tommasi*
Marco Tommasi* Francesca Toro
Francesca Toro Simone Arnò
Simone Arnò Angelo Carrieri
Angelo Carrieri Marco Maria Conte
Marco Maria Conte Marianna Daria Devastato
Marianna Daria Devastato Laura PicconiMaria Rita SergiAristide Saggino
Laura PicconiMaria Rita SergiAristide Saggino- Department of Medicine and Aging Science, University of Chieti-Pescara, Chieti, Italy
The exceptional pandemic due to the 2019 coronavirus disease (COVID-19) has obliged all Italians to stay at home. In the literature, there are evidences that traumatic global events, such as natural catastrophes and pandemic, have negative effects on the physical and psychological health of the population. We carried out a survey to analyze the physical and psychological conditions of Italians during the pandemic. Due to the severe limitations in moving during the phase one lockdown, the survey was administered by internet. Results show that Italians followed the provisions established by the Italian government to avoid contamination, but 43% of them declared to have suffered from physical symptoms, in particular migraine, sleep disorders, persistent exhaustion, and difficulty of concentration. They have great fear to be contaminated or that relatives or friends can be contaminated, and they actively take actions to avoid contamination. Participants declared that they had suffered a lot of inconveniences due to restrictions in their movements, and that their life habits were strongly changed. They spent their time at home in different activities, but their psychological well-being was strongly impaired by the lockdown. The level of anxiety tripled, in relation to the prepandemic period, and 30% of males and 41% of females declared to have severe levels of depression. Participants with high levels of optimism and hopefulness show a stronger resilience against anxiety and depression. In addition, there is a negative correlation between anxiety and depression and the five factors of personality. These results show that psychological diseases must not be neglected, and that people in lockdown do need support for their psychological health, also with the help of internet and communication technologies.
Introduction
The 2019 coronavirus disease (COVID-19) pandemic is a global event that is causing enormous changes in lifestyles and daily activities of people of every part of the world. In Italy, particularly, the pandemic has caused a high level of deaths among Italian citizens (14.1% of the contaminated population), especially among persons who are over 65 years old. In all the world, there are more than 4.5 million cases of contaminated people with more than 312,000 deaths [data obtained from the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University on 5 May 20201). On the basis of this high risk for citizens health, the Italian government from 10 March declared the lockdown for all working and social activities (phase one lockdown); the closure of schools, universities, public offices, and private businesses; and the mandatory quarantine for all Italians who were contaminated by the virus. Italians have to stay at home, with the possibility to move outside only in cases of strong necessity, and they have to follow procedures for securing themselves against contamination. In addition, the Italian government reinforced the public medical system to deal with the pandemic. We decided to analyze, with a survey, the impact of the pandemic and of the first phase of the lockdown on the behavior and psychological well-being of people.
There are evidences from the literature that global negative events, such as natural catastrophes, cause physical damages and psychological distress (Janney et al., 1977; Kanno et al., 2013). Also, the pandemic has negative effects on psychological well-being, not only in physicians and medical workers who have to deal with the effects of the pandemic on human beings (Greenberg et al., 2020; Tan et al., 2020) but also in normal people who have to abruptly change their life habits (Wheaton et al., 2012; Sood, 2020). COVID-19 immediately emerged as a dangerous virus for human beings health because of its high level of contamination, and researchers recommended an immediate intervention to reduce its dangerousness (Wang et al., 2020). By reviewing studies of the psychological impact of previous pandemics [e.g., severe acute respiratory syndrome (SARS), H1N1, or Ebola], Brooks et al. (2020) evidenced that during the pandemic period, people suffer from stress, depression, and anxiety and can develop fears and worries about their economic status. The authors also claim that further research is necessary to analyze the impact of public health measures activated for preventing contamination and the real efficiency of these measures (Brooks et al., 2020). The pandemic can have negative impacts on physical health (Li et al., 2020), but other authors highlighted the strong necessity to study the effects of the pandemic and government restrictions of individual activities on people’s psychological health, especially on their level of anxiety and depression (Holmes et al., 2020). Psychological stress, anxiety, and depression have negative impacts not only on human beings but also on the entire society, from both an economic and a political standpoint (Gyani et al., 2013; Layard, 2013).
Italy was the first European country to face the risk of a pandemic on a large scale (Saglietto et al., 2020). The rapid increase of positive cases in the last days of February induced the Italian government to take severe measures that blocked nearly all working and social activities, and these measures could have had a strong impact on Italians’ mental health. In particular, the duration of the restrictive measures against free movement, the reduction of social contacts, the fear of possible infections, the shortage of economic resources or supplies, and the lack of clarity in information could have negatively affected citizens and their psychological well-being (Orrù et al., 2020); thus, methods of prevention for stress and mental health diseases (Marazziti et al., 2020) should be taken into consideration, also by the public authority, to reduce pandemic distress. Therefore, the pandemic can be considered a strong cause of stress for Italian people without any doubts, and it is necessary to estimate the level of psychological disease generated by the pandemic in order to develop the best methods of interventions to contrast its harmful impact on the life of each individual and on the functioning of the entire society. However, empirical data are necessary to evaluate the real physical and psychological conditions of the population.
Materials and Methods
Sample
The sample was composed of 418 participants (72.97% females). Mean age was 32.23 years (SD = 12.46). Table 1 shows the demographic characteristics of the sample. Even if there were participants of nearly all Italian regions (only Valle d’Aosta was not present), a higher percentage of participants were from the central and southern parts of Italy.
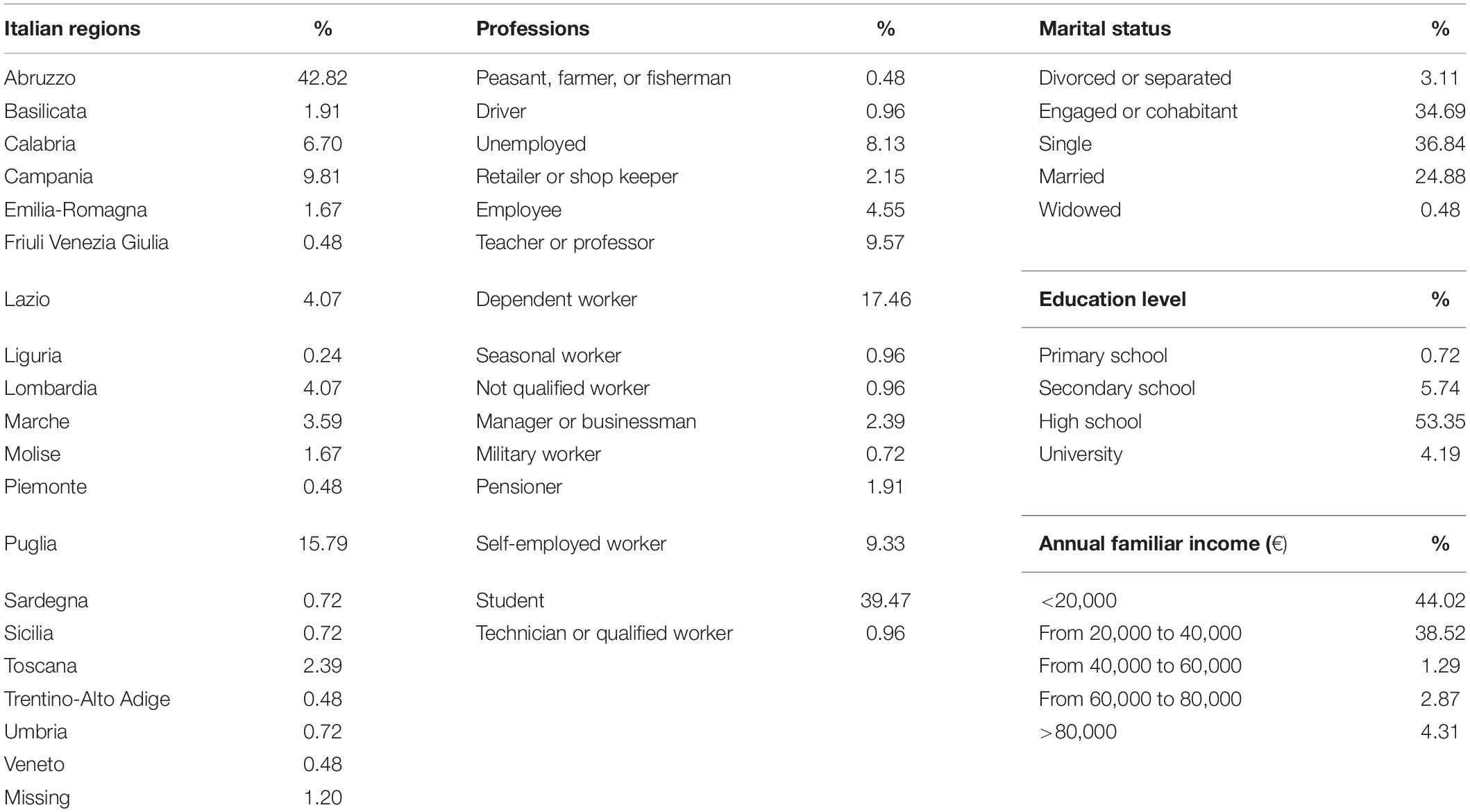
Table 1. Demographic characteristics and distribution of the Italian sample.
Materials
The online survey included different questions and psychological questionnaires to collect data about the physical and psychological conditions and the diseases produced by quarantine on participants. In addition, we provided questions about the level of knowledge of COVID-19 and its mechanisms of propagations. Personality traits, anxiety, depression, and resilience of participants were measured with standardized psychological tests.
Assessment of Participants’ Health Status
In the survey, questions were provided to collect information about the health status of participants. We asked if participants were contaminated or believed to have been contaminated by COVID-19, if they were eventually recovered in hospitals, if they suffered from other chronic pathologies (and in case of positive response, which was their pathology), what kind of physical symptoms they suffered in the last 2 weeks, how long was the duration of these symptoms, and if they had relatives or friends recovered from COVID-19.
Assessment of Participants’ Knowledge and Fear About COVID-19
To assess participants’ knowledge of COVID-19, a series of questions was used asking participants if they had correct or incorrect notions about COVID-19. For example, a correct notion is that COVID-19 causes respiratory diseases, and an incorrect notion is that it can infect only old people. Participants responded using a Likert scale from 1 (not true) to 4 (totally true). Another series of questions assessed participants’ knowledge of the various means of transmission of COVID-19 (e.g., via physical contact or fluid contamination). Participants had to evaluate the most probable means of contamination using a Likert scale from 1 (not true) to 4 (totally true). Other questions assessed different kinds of fear about COVID-19 (e.g., to be contaminated or that relatives or friends can be contaminated) using a Likert scale from 1 (no fear) to 4 (highest fear).
Assessment of Participants’ Problems and Behavior During the Lockdown
Participants were asked which were the most important problems they suffered after the movement restrictions due to lockdown or quarantine (e.g., obligation to stay at home or possible economic difficulties) using a Likert scale from 1 (not true) to 4 (totally true). We asked participants to rate the global disease caused by the lockdown (no disease, low disease, medium disease, high disease) and how strong was the impact of the lockdown on their life habits (no impact, low impact, medium impact, high impact, total impact). To assess the actions or behaviors participants took on to contrast contamination, we asked if they remained at home and what they did to avoid infection (e.g., if they washed their hands or wore masks when going out). In addition, we asked what kind of activity they were doing during their permanence at home when they were not working (e.g., watching TV or reading books). Other questions were provided to assess if they received social support from family, local institutions, or voluntary associations during the lockdown (“Are you receiving any help from someone or from services and institutions?”).
Assessment of Psychological Conditions
We assessed the personality traits of the five factor model of personality (extraversion, agreeableness, conscientiousness, emotional stability, and openness) using the Big Five Observer (BFO) questionnaire (Caprara et al., 1994). The BFO is composed of 40 items that are a couple of adjectives that define the characteristic of the five traits of personality. Scores were based on a Likert scale from 1 to 7. The higher the score, the higher the presence of the trait. Emotional stability of the BFO is the inverted measure of neuroticism (Caprara et al., 1994).
We assessed anxiety and depression of participants to have indications of their psychological well-being during the lockdown period. Anxiety was measured using the State Trait Anxiety Inventory (STAI) of Spielberger with 20 items (Spielberger, 1983). Scores were based on a Likert scale from 1 (not at all) to 4 (very much). We used the standardized scores of the Italian population collected for the CBA 2.0 to estimate if participants suffered from a severe level of anxiety (Sanavio, 1997). The global STAI scores corresponding to the 95th percentile were 55 and 61 for males and females, respectively. Depression was assessed using the short form of the Beck Depression Inventory (BDI) with 13 items (Beck and Beck, 1972). The Italian version of the BDI was validated by Sica and Ghisi (2007). Scores ranged from 0 to 3 for each item. Different levels of depression severity were established in relation to range scores (Beck and Beck, 1972; Reynolds and Gould, 1981; Knight, 1984; Stukenberg et al., 1990). Scores from 0 to 4 indicate the absence of depression, from 5 to 7 mild depression, from 8 to 15 moderate depression, and scores higher than 15 indicate severe depression. Participants’ resilience was estimated using the Revised Life Orientation Test (LOT-R) scale by Scheier et al. (1994), which measures optimism, and the Hope Herth Index (HHI) scale (Herth, 1992), which measures hopefulness. Resilience is composed of many characteristics or qualities (Richardson, 2002), and among the optimal characteristics indicated in a special issue of the American Psychologist and of the Journal of Social and Clinical Psychology, there are optimism (Peterson, 2000) and hope (Snyder, 2000). We selected optimism and hopefulness because other studies defined them as protective factors against traumas and negative life events (Madsen and Abell, 2010). The LOT-R scale has 10 items, with scores on a Likert scale from 1 (strongly disagree) to 5 (strongly agree), and it measures the level of optimism and faith on positive outcomes in the future. The higher the score, the higher the level of optimism. The Italian standardization of the LOT-R was made by Chiesi et al. (2013). The Italian standardization of the HHI was made by Ripamonti et al. (2012). The scale consists of 12 items with a Likert scale from 1 (strongly disagree) to 4 (strongly agree), and it assesses three dimensions of hopefulness: inner sense of temporality and future, that is the ability to preserve a positive vision of the future (HHI temp); interconnectedness with self and others or subjective beliefs to have a strong interior force and to be not isolated from others (HHI conn); and inner positive readiness and expectancy, that is the ability to react to negative situations and the confidence that our personal actions can improve negative situations (HHI exp). This scale was used particularly for estimating resilience in patients suffering from cancer disease (Ripamonti et al., 2012). In addition, we used the Italian standardized version of the Marlowe–Crowne (MC) scale for social desirability (Manganelli Rattazzi et al., 2000), to check the validity of subjective responses in psychological scales. We used the short form with nine items with a Likert scale from 1 (low social desirability) to 5 (high social desirability). Positive or negative correlations with MC indicate a tendency to over- or underestimate psychological characteristics or traits, respectively.
Procedure
Participants responded by compiling an online survey made with Google modules. The link of the survey was distributed via social networks (Facebook and WhatsApp). Participants were contacted through the social networks of the authors of this work and were asked to propagate the link to other relatives or friends. Participants before doing the survey were informed about the aims of the research, and they were given information about the privacy of their data. We followed the Helsinki Declaration of ethical principles for medical research involving human participants, and the study procedure received the approbation of the Department of Medicine and Aging Sciences for its execution. Before compiling the survey, participants had to declare their effective will to participate in the survey. Without this declaration, they could not start the compilation. Participation was voluntary. Because of the possibility to repeat the test, at the end of the survey, we asked participants if they wanted to compile the survey on a successive moment. Data were collected from 8 April to 5 May. Anonymity and privacy of the participants were guaranteed according the Italian and the European laws about privacy (Italian law n. 196/2003 and EU GDPR 679/2016, respectively).
Results
Missing Data
The online survey was projected to reduce the risk of missing data. For completing the survey, it was necessary to respond to all items. In addition, some items were activated only when participants declared to possess specific characteristics (e.g., items asking the kind of chronic pathology, if the participant declared it). In this way, we reduced the number of missing data to zero.
Assessment of Participants’ Health Status
Table 2 shows the participant’s health status. Nearly all participants declared not to be contaminated by COVID-19 (>95%). Of the participants, 4% declared that they believed to be contaminated, even if they did not make any medical test, and less than 1% declared to have been effectively contaminated.
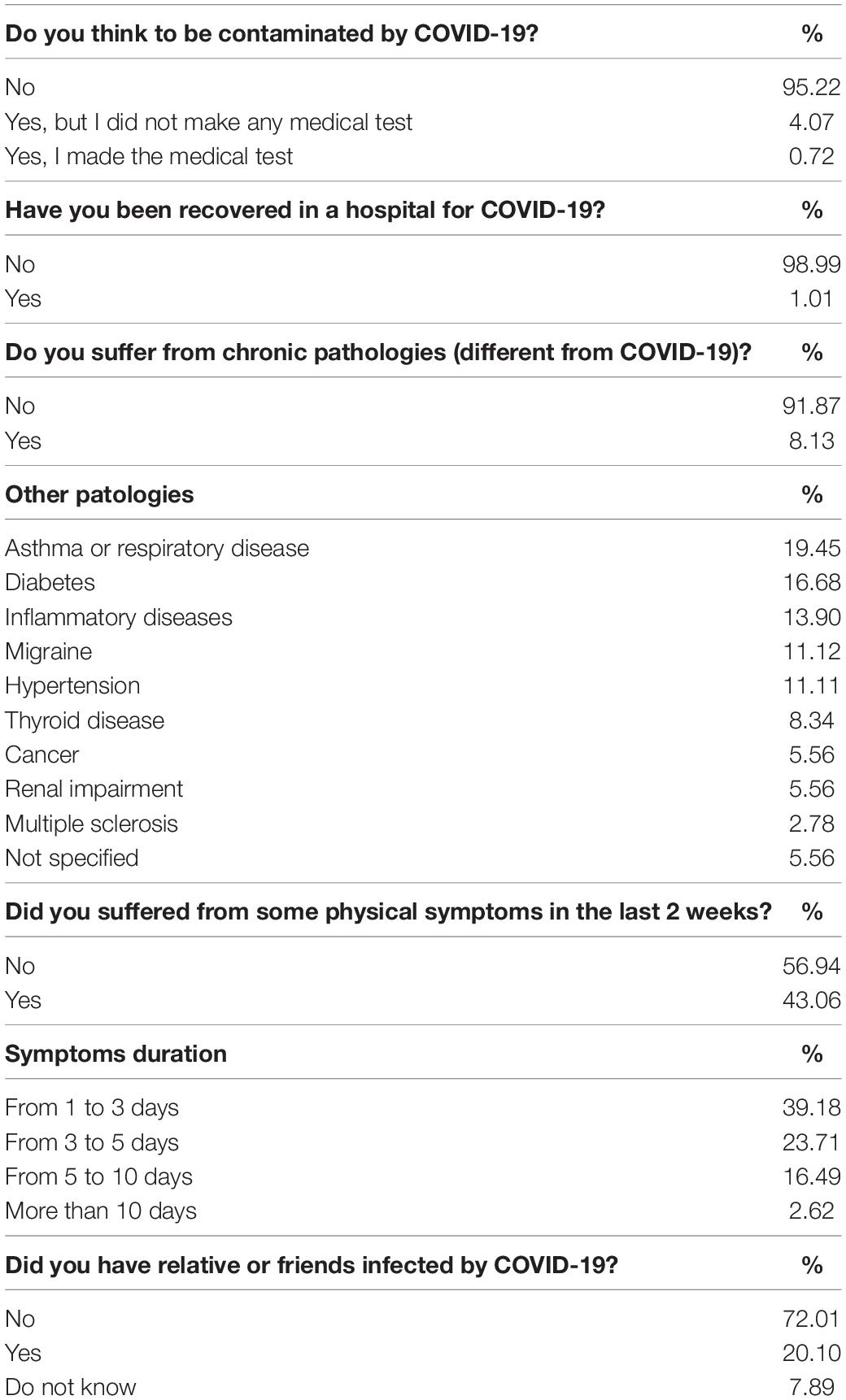
Table 2. Participants’ health status.
Only 1% of participants reported to have been hospitalized for COVID-19. Furthermore, 8.13% of participants suffered from chronic diseases, not related to COVID-19. The most frequent diseases were asthma, diabetes, inflammatory diseases, migraine, hypertension, and thyroid disease. In addition, 43% of participants declared to have suffered from physical symptoms in the last 2 weeks. The majority of symptoms lasted less than 10 days. Moreover, 20.1% of participants declared that they had some relatives or friends infected by COVID-19. Figure 1 shows the frequency of the different symptoms declared by participants. The most prevalent physical symptoms were insomnia or sleep disorder, followed by migraine, persistent exhaustion, and general malaise.
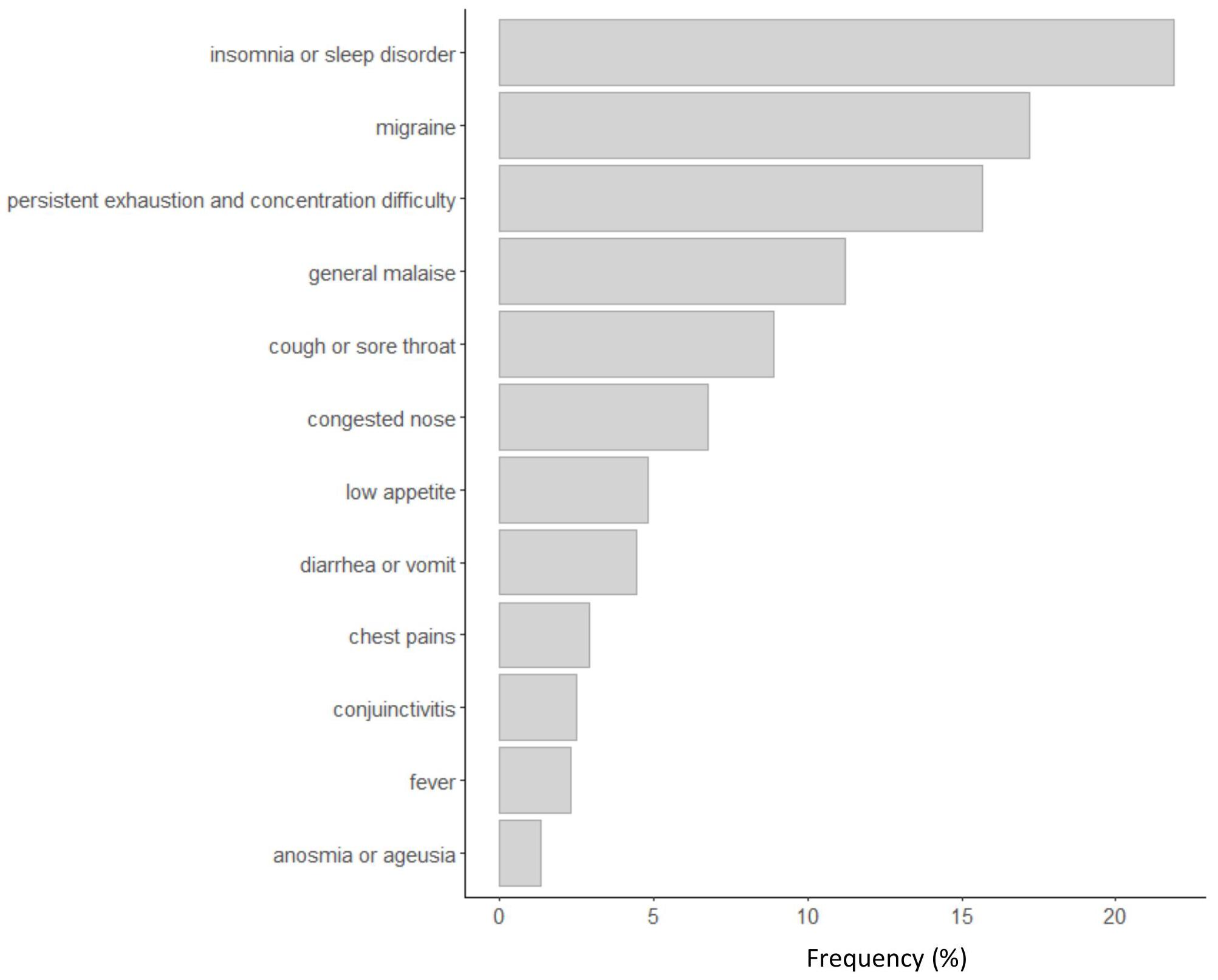
Figure 1. Frequency of physical symptoms declared by participants in the last 2 weeks.
Assessment of Participants’ Knowledge and Fear About COVID-19
Table 3 shows the mean ratings and standard deviation of participants’ scores when they were asked to respond to some items to assess their knowledge and fear about COVID-19 and the risk to be contaminated.
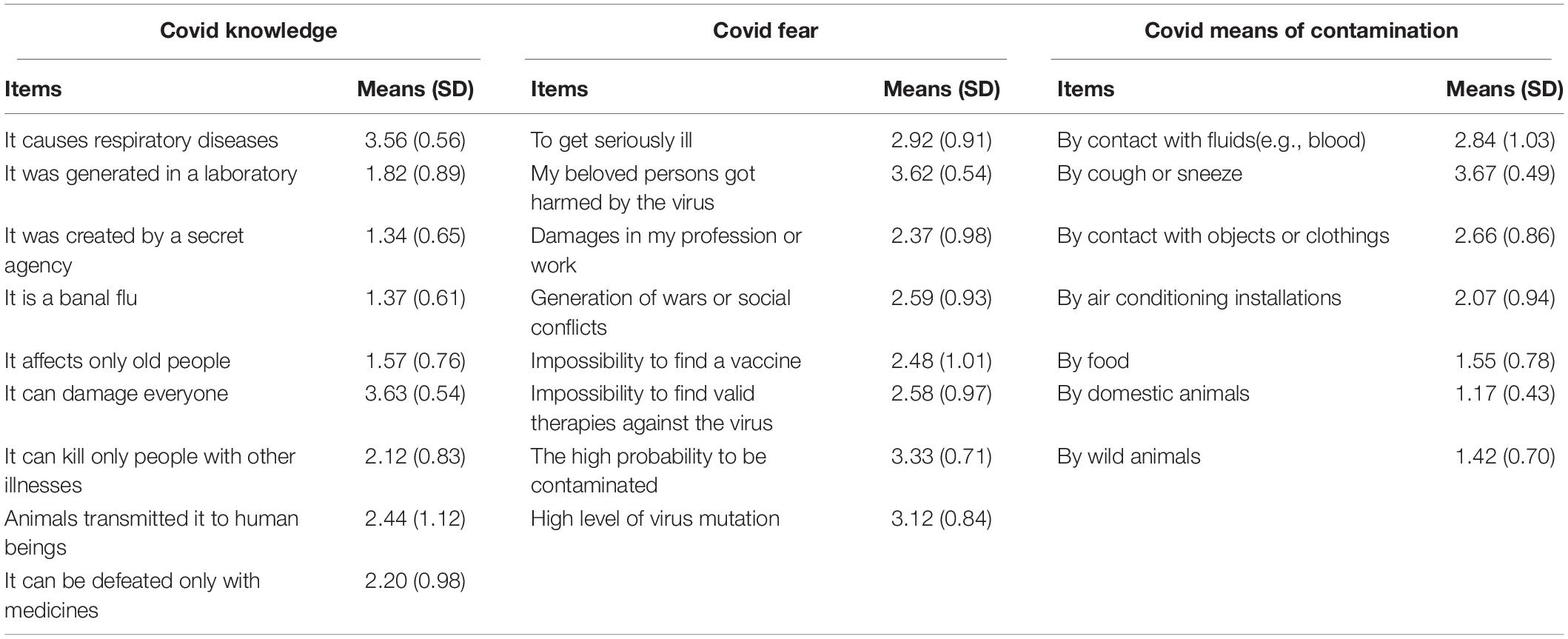
Table 3. Mean ratings and standard deviation (SD) of participants’ scores to assess knowledge and fear about COVID-19 and its means of contamination.
Participants know that COVID-19 creates respiratory disease, that it can contaminate everyone, and that, initially, it was transmitted by animals to humans. Participants do not generally believe that COVID-19 is an artificial virus created in the laboratory, that it is only a banal flu, and that it affects specifically old people. Participants show a high level of fear about COVID-19. The greatest fears are the possibility that beloved persons can be contaminated by the virus, the possibility to be contaminated, the genetic mutation of the virus, the difficulty to find valid therapies or vaccines, and the risk of social conflicts or wars. In relation to the means of contamination, participants say that the principal means are through air (cough or sneeze) and through contact with organic fluids (e.g., blood) or with contaminated objects.
Assessment of Participants’ Problems and Behavior During the Lockdown
Table 4 shows what are the principal problems that caused disease in participants. The principal causes are the impossibility to see relatives or friends, the duration of the lockdown, and the obligation to stay at home.
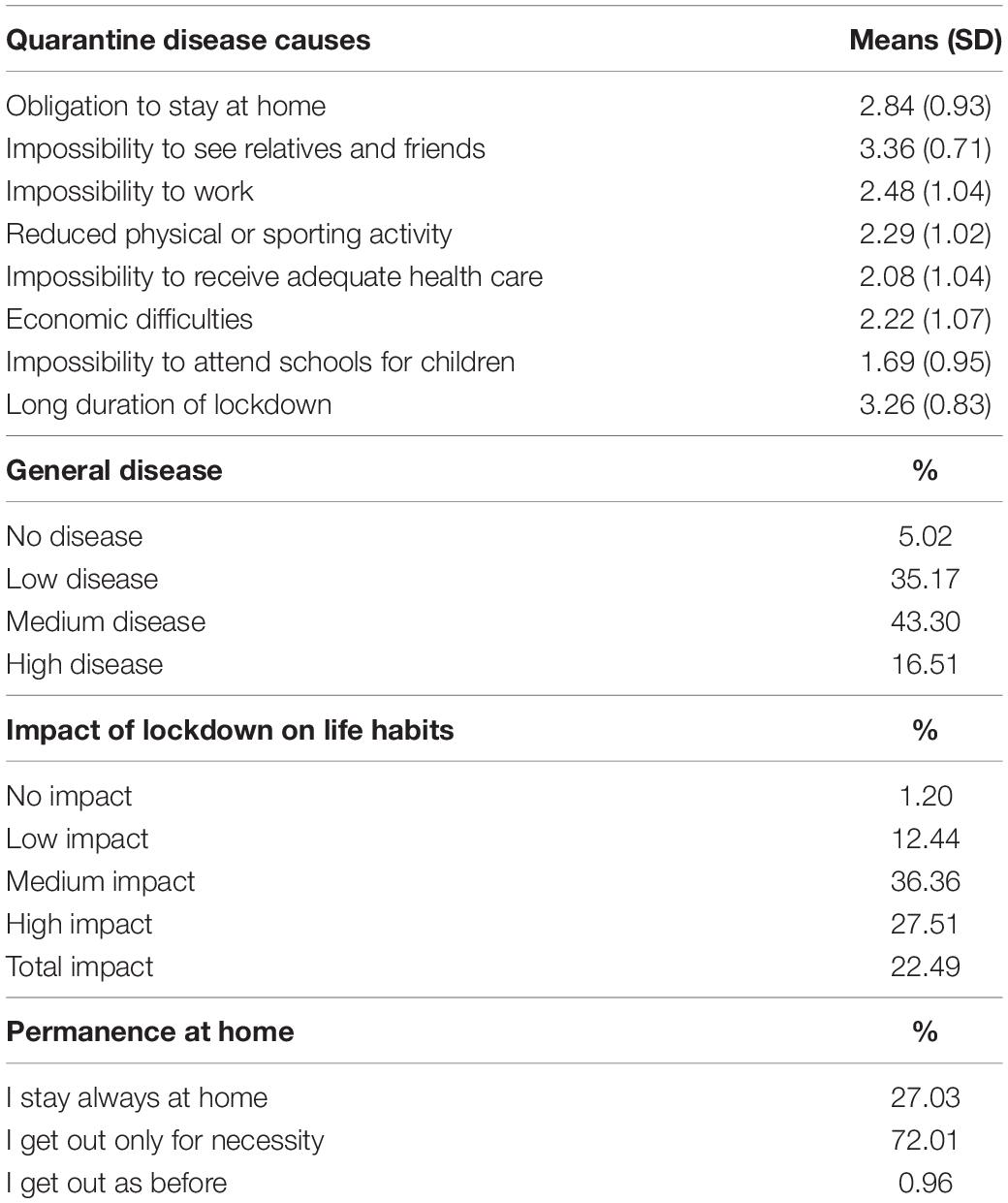
Table 4. Lockdown disease causes, global level of disease, impact of phase one lockdown on normal life, and permanence at home of the sample.
Of the participants, 59.81% reported a medium or high level of general disease, and 50% declared that the quarantine strongly changed their life and habits. Furthermore, 27% of participants stayed always at home, whereas 72% got out home only for necessity. Less than 1% declared to get out as they did before the lockdown. Figure 2 shows the activities practiced at home during the lockdown (when not working) by participants.
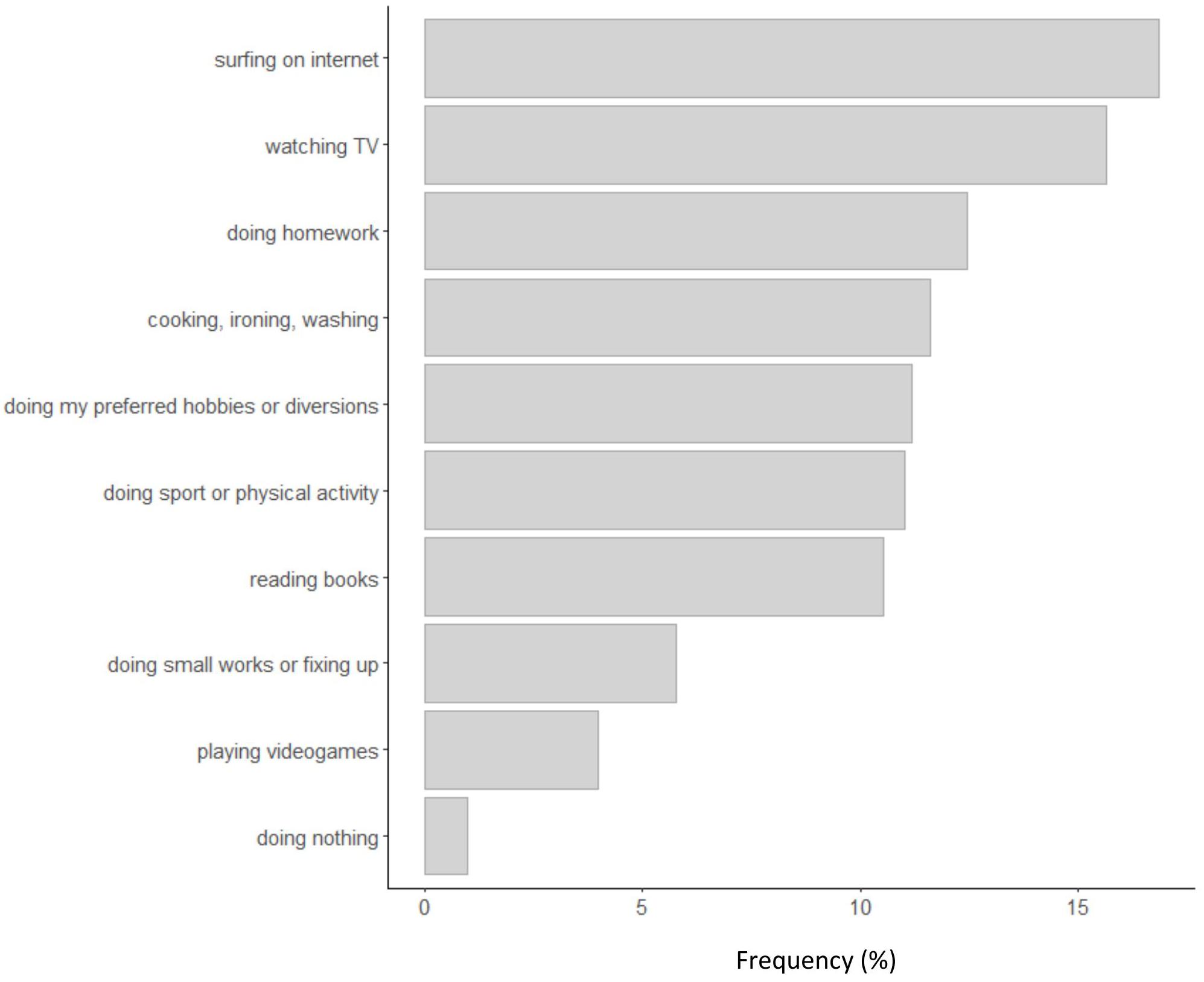
Figure 2. Frequency of activities practiced at home during the phase one lockdown.
Many of them watched TV or used the internet and did homework or hobbies. Very few people were completely inactive (less than 1%). Figure 3 shows what were the most frequent precautions taken by participants to avoid contamination.
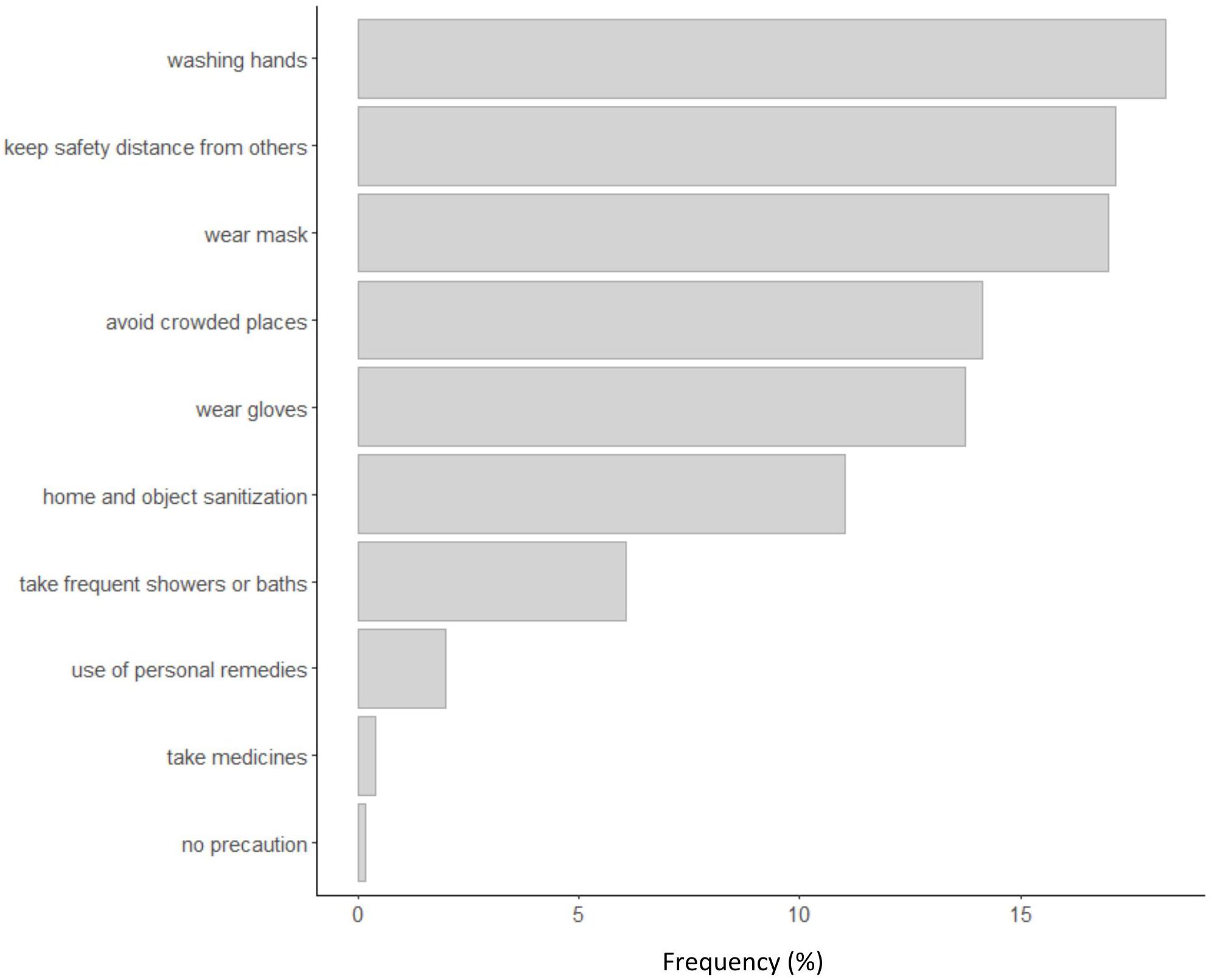
Figure 3. Frequency of precautions against contamination.
The most frequent precautions were the use of masks and gloves, washing hands frequently, sanitization of objects and rooms, observance of a safety distance from others, and avoidance of crowded places. Therefore, participants followed the principal instructions of the Italian Ministry of Public Health to reduce contamination risks. Less than 0.2% of participants declared that they did not take any precaution against contamination. Figure 4 shows the principal agents of social support received by participants during the lockdown. Participants received social support principally from family (parents, sons, relatives), family doctors, friends, civil protection, police, and volunteers.
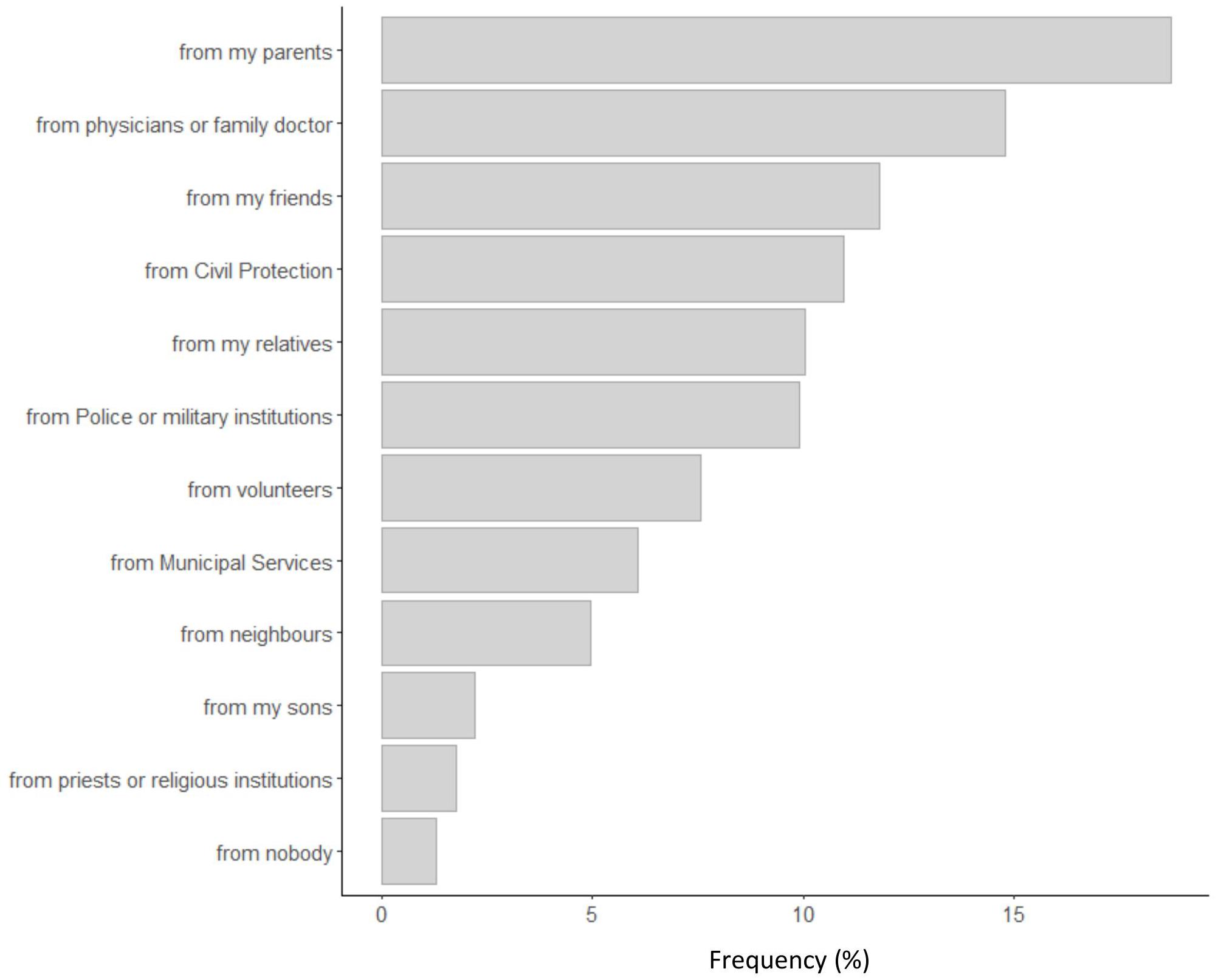
Figure 4. Frequency of social support agents for participants during the phase one lockdown.
Assessment of Psychological Conditions
Table 5 shows the descriptive, reliabilities and correlations of the psychological scales used to assess psychological well-being, psychological resilience, and personality. Values of skewness and kurtosis are included in the range of −2 and 2, confirming that score distributions are prevalently normal (Gravetter and Wallnau, 2014).
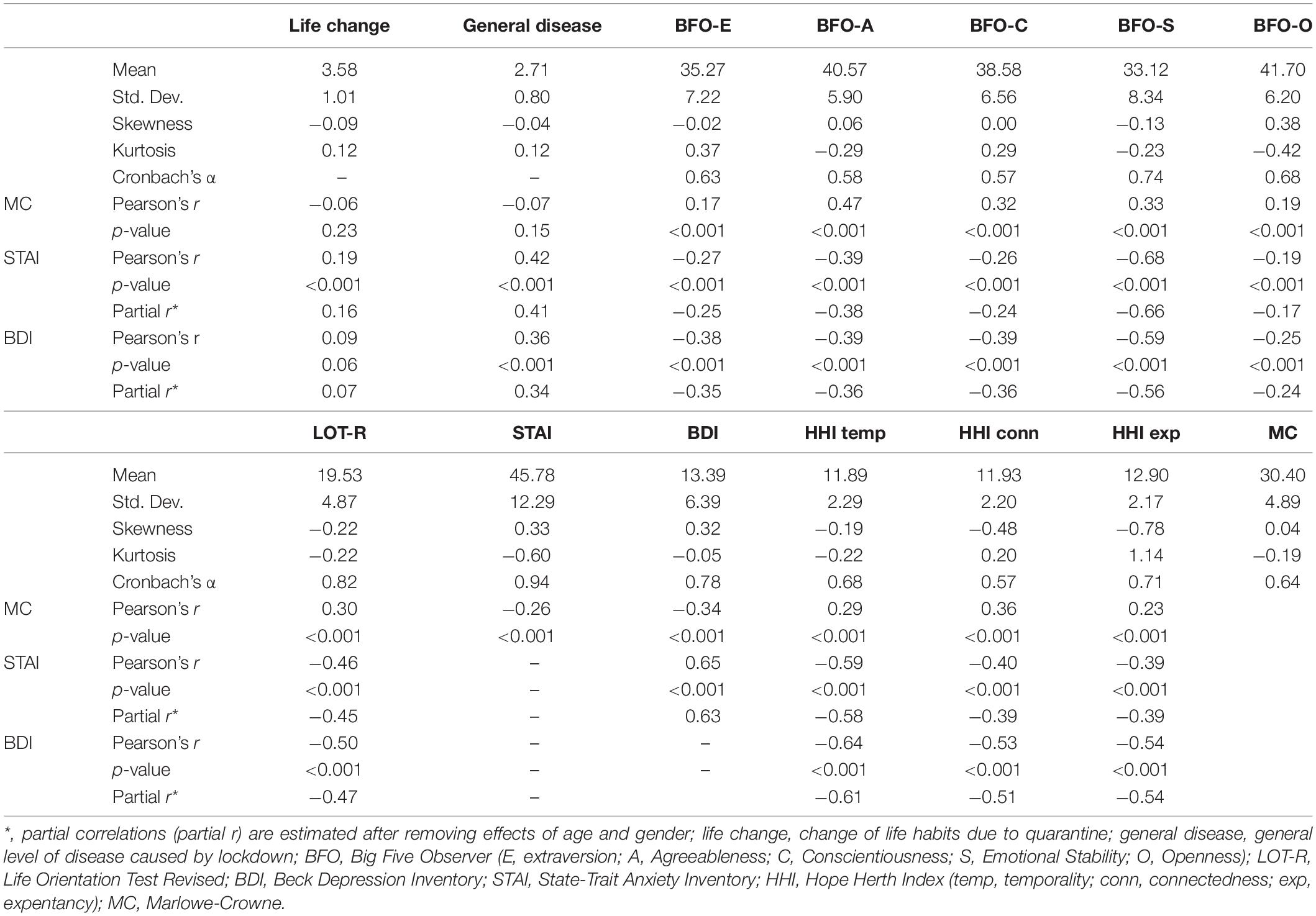
Table 5. Descriptive statistics (mean, standard deviation, skewness, and kurtosis), reliability (Cronbach’s α), and bivariate correlation between psychological variables and assessment of life change and disease generated by lockdown.
Cronbach’s α values indicate acceptable or good reliability for each psychological scale (Kline, 2000). There are significant correlations between the MC scale for social desirability and the psychological measures, but correlations have small effect sizes because they are lower than 0.5 (Cohen, 1992). Anxiety, assessed by STAI, and depression, assessed by BDI, are strongly correlated with each other (r = 0.65, p < 0.001) and are all significantly and negatively correlated with the five traits of personality (extraversion, agreeableness, conscientiousness, emotional stability, and openness). Correlations vary from −0.68 to −0.19 for STAI and from −0.59 to −0.25 for BDI. We also reported the partial correlations after removing the variance due to age and gender. The p-values of correlations were adjusted according to the false discovery rate procedure (Benjamini and Hochberg, 2000). Anxiety and depression have the highest correlations with emotional stability and the lowest correlations with openness. Therefore, personality traits have some relations on psychological well-being. Anxiety and depression are negatively correlated with optimism, assessed with LOT-R, and with the three dimensions of the HHI scale. Therefore, people with a high level of optimism and hopefulness are less affected by anxiety and depression. The variation of life habits (life change) has some relations on anxiety (r = 0.19, p < 0.001), but not on depression, whereas the disease caused by the lockdown is related to both o anxiety and depression (r = 0.42 and 0.36, respectively).
Figure 5 shows the scatterplots of the correlations reported in Table 5, in relation to anxiety, assessed with the STAI, and depression, assessed with the BDI. Raw scores were transformed into standardized scores (z points) for allowing comparisons between scales. Scatterplots do not evidence particular anomalies in data distributions.
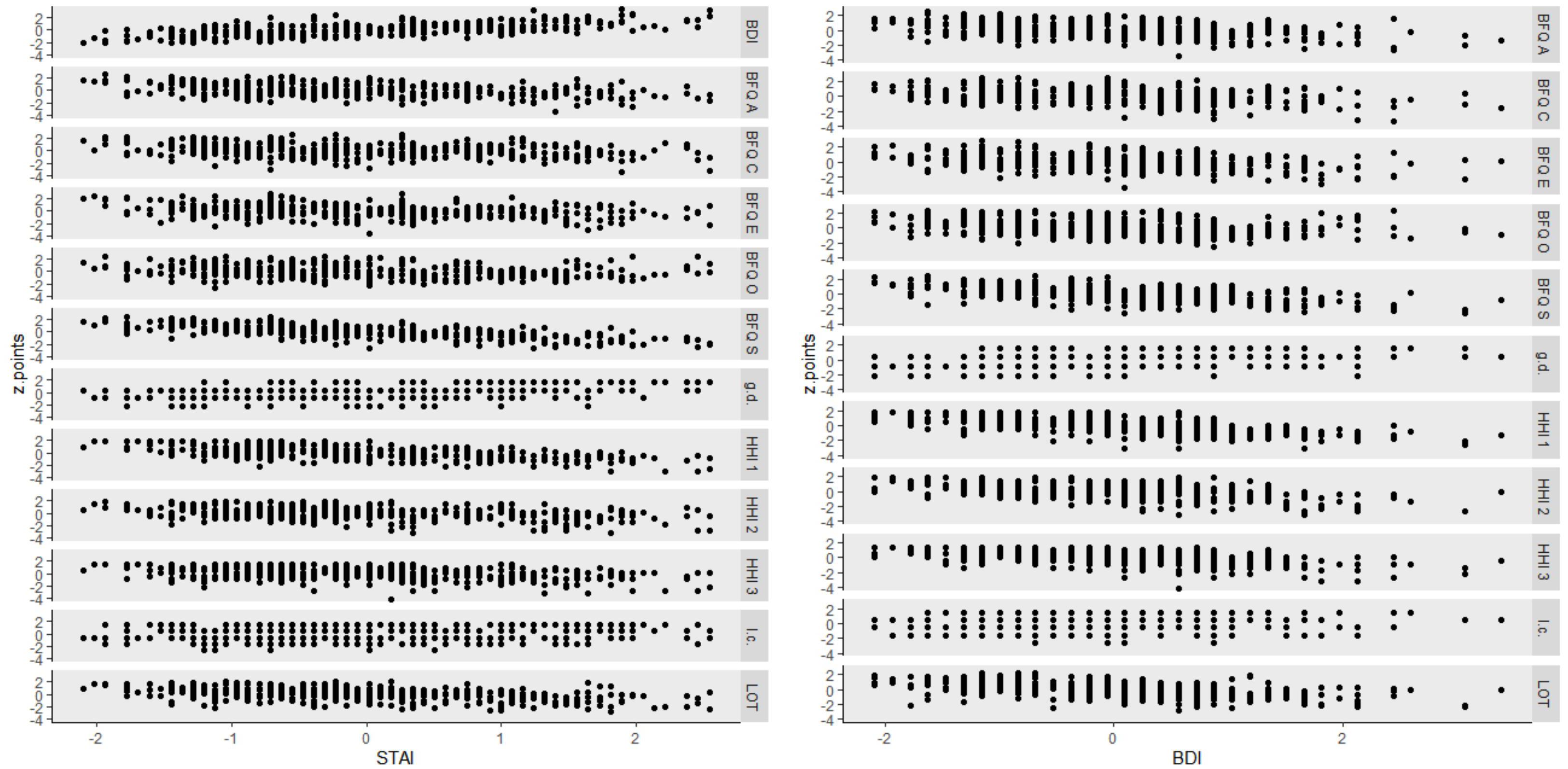
Figure 5. Scatterplots of the psychological measures (I.c., life change; g.d., general disease; BFQ E, extraversion; BFQ A, agreeableness; BFQ C, conscientiousness; BFQ S, emotional stability; BFQ O, openness; HHI1, temporality subscale of hopefulness; HHI 2, interconnectedness subscale of hopefulness; HHI 3, positive expectancy subscale of hopefulness) in relation to anxiety (STAI) and depression (BDI). Raw scores were transformed into standardized scores (z points) for allowing comparison between scales.
Of the participants, 15.04% of males obtained scores at the STAI equivalent to or higher than 55 (95th percentile for the male population), whereas 16.06% of females obtained scores at the STAI equivalent to or higher than 61 (95th percentile for the female population). Thus, the level of anxiety in the Italian sample during the phase one lockdown is practically tripled in relation to the cutoffs estimated in the normal population in the prepandemic period (Sanavio, 1997). The values of STAI corresponding to the mean of the Italian population are 37 for males and 40 for females (Sanavio, 1997). During the lockdown, the mean values of STAI increased to 41.45 and 47.38 for males and females, respectively. Therefore, the presence of a higher level of anxiety during the lockdown is confirmed by empirical data. Figure 6 shows the frequencies of the level of depression (none, mild, moderate, and severe) in participants. More than 50% of participants show moderate or severe symptoms of depression. In particular, 41.31% of females and 30.97% of males show severe symptoms of depression, respectively. Therefore, the presence of a high level of depression during the lockdown is also confirmed.
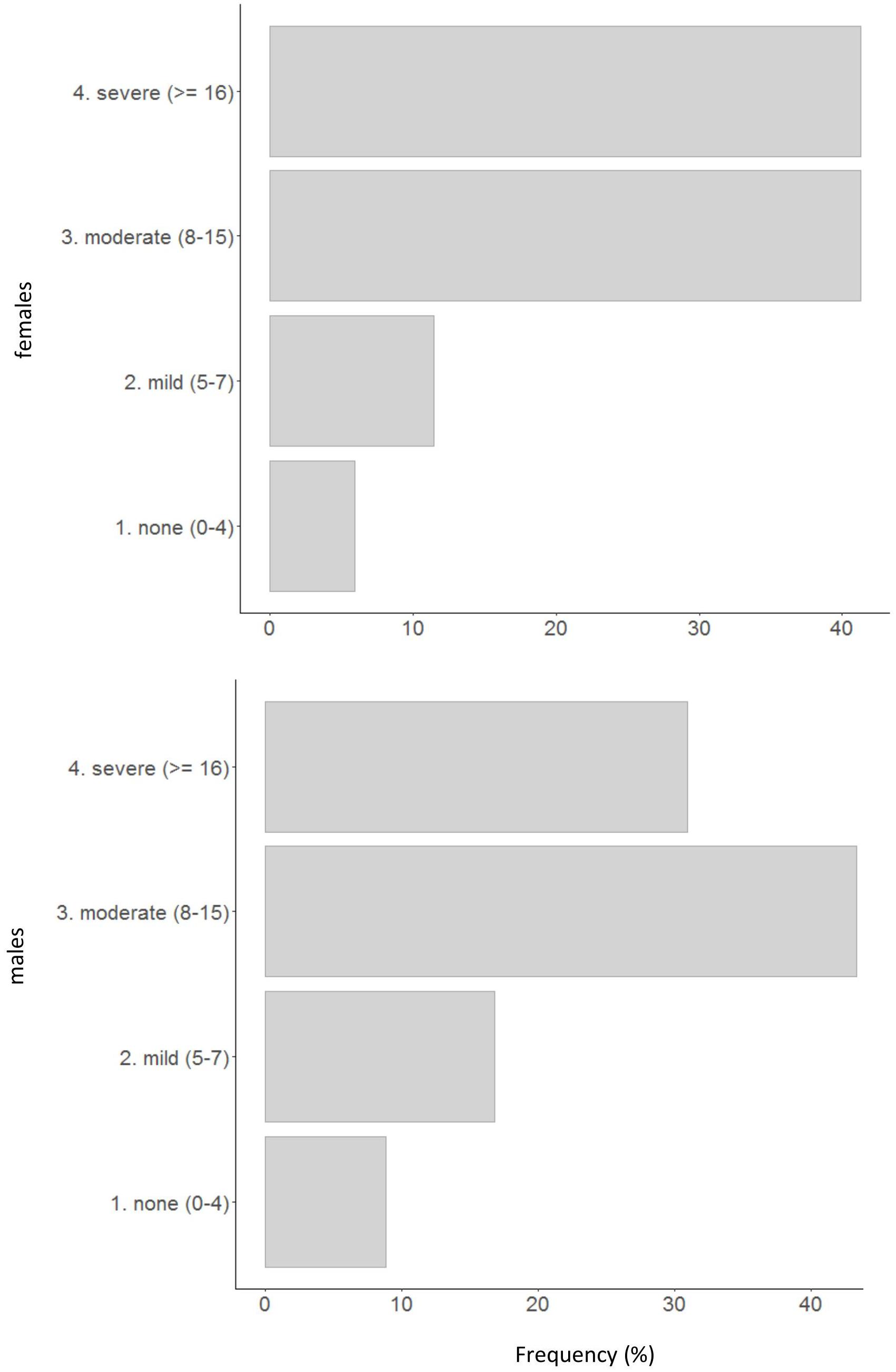
Figure 6. Frequency of depression levels in relation to BDI scores.
Discussion
During the lockdown period, people are obliged to stay at home, even if they have permission to go out (to buy food, medicines, or for strong necessities). The data collected from our sample show that people, during their mandatory permanence at home, are not totally inactive, and that they follow the provisions established by the Ministry of Public Health to avoid contamination (use of masks and glove, washing hands, safety distance observance from others, permanence at home). Only very few people declared to have been contaminated by COVID-19, and many of them still claimed to be in a good health conditions, even when they were people suffering from other chronic diseases. About 20% of individuals reported having at least one relative or friend infected by COVID-19, and this could have affected their psychological status. The physical symptoms reported by participants were, above all, symptoms connected with a stressful condition of life. Migraine, sleep disorders, difficulty of concentration, and persistent exhaustion are typical signs of stress (American Psychological Association, 2010). Participants were clearly aware that COVID-19 was not a banal flu, that it could contaminate everyone, and that contamination could happen through air dispersion of the virus or through contact with contaminated objects. They were worried about a possible contamination toward themselves or toward their relatives or friends, about a possible virus mutation, or about the difficulty to find a valid therapy against the virus.
The principal result of our study is that the level of anxiety and the level of depression are very high in Italians during the lockdown period. The percentage of extreme anxiety is tripled, in relation to the prepandemic measured levels (Sanavio, 1997), and about 50% of participants show a moderate or severe level of depression. About 30% of males and 41% of females suffer from severe depression. Therefore, there are evidences that the lockdown have had negative effects on psychological well-being. However, some participants showed low levels of anxiety and depression, in particular, those who had high level of optimism and hopefulness. These people have a positive vision of the future and a strong confidence that their actions and behaviors can improve the negative situation and these characteristics, reasonably, can attenuate their psychological sufferance. Also, personality traits have some relations with anxiety and depression. People with high level of extraversion, agreeableness, conscientiousness, emotional stability, and openness have lower tendency to suffer from anxiety and depression.
Generally, the negative effects of the lockdown on psychological conditions are evident, confirming the importance of mental health prevention (Marazziti et al., 2020) and the necessity of psychological interventions against the negative impact of the pandemic on individuals (Holmes et al., 2020). Participants need psychological support, even if they do not suffer from mental or physical diseases (Brooks et al., 2020; Marazziti et al., 2020). Because of the impossibility to freely move outside the home during the lockdown, it could be useful to develop digital technologies for providing psychological support via internet, social networks, or apps for smartphones (McCord et al., 2015; Silva et al., 2015; Orrù et al., 2020). Through internet, it could be possible not only to provide direct assistance to people at home with the help of clinical psychologists and psychiatrists but also to teach and explain techniques for reducing psychological diseases and improving well-being, as, for example, mindfulness (Bullis et al., 2014; Saggino et al., 2017; Sood, 2020).
Both governments and private institutions should invest on mental health care of citizens, when big catastrophes happen. When negative events with a radical impact on population activities happen, remedies for the population should be taken to overcome the consequential diseases (Holmes et al., 2020; Saglietto et al., 2020). Psychological diseases should not be neglected, because they have negative consequences on individuals, institutions, societies, and governments (Gyani et al., 2013; Layard, 2013; Brooks et al., 2020).
In 4 May, the Italian government declared the passage to the phase two of the pandemic for 18 May. Limits and restrictions of movement for the population were reduced, and some economic activities could restart. To test the evolution of anxiety and depression in this new phase, we asked participants if they wanted to repeat the survey. About 60% accepted positively to repeat the test.
One possible limit of this research is that the online survey cannot guarantee a perfect randomized selection of participants, but this was the only possibility because of the limits imposed by the lockdown. However, the different channels used to propagate the survey and the high number of participants allowed a collection of data from a sample composed of heterogeneous individuals of different parts of Italy. Another possible limit is the use of psychological tests, especially for the estimation of depression, that are not the typical test used by professional psychiatrists or clinical psychologists. However, we have to say that the BDI was used in more than 2000 studies (Richter et al., 1998), and that it is widely used by Italian clinical psychologists (Sica and Ghisi, 2007).
Data Availability Statement
The data analyzed in this study are subject to the following licenses/restrictions: Datasets are conserved by the authors in a safe place in respect of the Italian laws for the privacy. Requests to access these datasets should be directed to MT,bWFyY28udG9tbWFzaUB1bmljaC5pdA==.
Ethics Statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
MT contributed to providing materials, data analysis, programming online survey, and searching of literature sources. FT contributed to collecting participants, providing materials, helping in manuscript revision, and searching of literature sources. SA contributed to collecting participants, programming online survey, and helping in manuscript revision. AC, MC, MD, and MS contributed to collecting participants, helping in manuscript revision, and searching of literature sources. LP and AS contributed to data analysis, helping in manuscript revision, and searching of literature sources. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Footnotes
References
American Psychological Association (2010). Stress in America Findings. Washington, DC: American Psychological Association.
Beck, A. T., and Beck, R. W. (1972). Screening depressed patients in family practice: a rapid technic. Postgrad. Med. 52, 81–85. doi: 10.1080/00325481.1972.11713319
Benjamini, Y., and Hochberg, Y. (2000). On the adaptive control of the false discovery rate in multiple testing with independent statistics. J. Educ. Behav. Statist. 25, 60–83. doi: 10.2307/1165312
Brooks, S. K., Webster, R. K., Smith, L. E., Woodland, L., Wessely, S., Greenberg, N., et al. (2020). The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet 395, 912–920. doi: 10.1016/s0140-6736(20)30460-8
Bullis, J. R., Bøe, H. J., Asnaani, A., and Hofmann, S. G. (2014). The benefits of being mindful: trait mindfulness predicts less stress reactivity to suppression. J. Behav. Ther. Exper. Psychiatry 45, 57–66. doi: 10.1016/j.jbtep.2013.07.006
Caprara, G. V., Barbaranelli, C., and Borgogni, L. (1994). BFO: Big Five Observer: Manuale. Florence: Organizzazioni speciali.
Chiesi, F., Galli, S., Primi, C., Innocenti Borgi, P., and Bonacchi, A. (2013). The Accuracy of the Life Orientation Test-Revised (LOT-R) in measuring dispositional optimism: evidence from item response theory analyses. J. Pers. Assess. 95, 523–529. doi: 10.1080/00223891.2013.781029
Gravetter, F., and Wallnau, L. (2014). Essentials of Statistics for the Behavioral Sciences, 8th Edn, Belmont, CA: Wadsworth.
Greenberg, N., Docherty, M., Gnanapragasam, S., and Wessely, S. (2020). Managing mental health challenges faced by healthcare workers during covid-19 pandemic. Br. Med. J. 368:m1211. doi: 10.1136/bmj.m1211
Gyani, A., Shafran, R., Layard, R., and Clark, D. M. (2013). Enhancing recovery rates: lessons from year one of IAPT. Behav. Res. Therapy 51, 597–606. doi: 10.1016/j.brat.2013.06.004
Herth, K. (1992). Abbreviated instrument to measure hope: development and psychometric evaluation. J. Adv. Nurs. 17, 1251–1259. doi: 10.1111/j.1365-2648.1992.tb01843.x
Holmes, E. A., O’Connor, R. C., Perry, V. H., Tracey, I., Wessely, S., Arseneault, L., et al. (2020). Multidisciplinary research priorities for the COVID-19 pandemic: a call for action for mental health science. Lancet Psychiatry 7, 547–560.
Janney, J. G., Masuda, M., and Holmes, T. H. (1977). Impact of a natural catastrophe on life events. J. Hum. Stress 3, 22–47. doi: 10.1080/0097840x.1977.9936084
Kanno, T., Iijima, K., Abe, Y., Koike, T., Shimada, N., Hoshi, T., et al. (2013). Peptic ulcers after the Great East Japan earthquake and tsunami: possible existence of psychosocial stress ulcers in humans. J. Gastroenterol. 48, 483–490. doi: 10.1007/s00535-012-0681-1
Knight, R. G. (1984). Some general population norms for the short form Beck Depression Inventory. J. Clin. Psychol. 40, 751–753. doi: 10.1002/1097-4679(198405)40:3<751::aid-jclp2270400320>3.0.co;2-y
Layard, R. (2013). Mental health: the new frontier for labour economics. IZA J. Labor Policy 2, 2–16.
Li, B., Yang, J., Zhao, F., Zhi, L., Wang, X., Liu, L., et al. (2020). Prevalence and impact of cardiovascular metabolic diseases on COVID-19 in China. Clin. Res. Cardiol. 109, 531–538. doi: 10.1007/s00392-020-01626-9
Madsen, M. D., and Abell, N. (2010). Trauma resilience scale: validation of protective factors associated with adaptation following violence. Res. Soc. Work Pract. 20, 223–233. doi: 10.1177/1049731509347853
Manganelli Rattazzi, A. M., Canova, L., and Marcorin, R. (2000). La desiderabilità sociale. Un’analisi di forme brevi della scala di Marlowe e Crowne [Social desirability. An anlysis of short forms of Marlowe-Crowne’s Scale]. Test. Psicometr. Metodol. 7, 5–17.
Marazziti, D., Pozza, A., Di Giuseppe, M., and Conversano, C. (2020). The psychosocial impact of COVID-19 pandemic in Italy: a lesson for mental health prevention in the first severely hit European country. Psychol. Trauma Theory Res. Pract. Policy 12, 531–533. doi: 10.1037/tra0000687
McCord, C. E., Saenz, J. J., Armstrong, T. W., and Elliott, T. R. (2015). Training the next generation of counseling psychologists in the practice of telepsychology. Counsel. Psychol. Q. 28, 324–344. doi: 10.1080/09515070.2015.1053433
Orrù, G., Ciacchini, R., Gemignani, A., and Conversano, C. (2020). Psychological intervention measures during the COVID-19 pandemic. Clin. Neuropsychiatr. 17, 76–79.
Reynolds, W. M., and Gould, J. W. (1981). A psychometric investigation of the standard and short form beck depression inventory. Psychol. Rep. 51, 1167–1170. doi: 10.2466/pr0.1982.51.3f.1167
Richardson, G. E. (2002). The metatheory of resilience and resiliency. J. Clin. Psychol. 58, 307–321. doi: 10.1002/jclp.10020
Richter, P., Werner, J., Heerlein, A., Kraus, A., and Sauer, H. (1998). On the validity of the beck depression inventory. Psychopathology 31, 160–168.
Ripamonti, C. I., Buonaccorso, L., Maruelli, A., Bandieri, E., Boldini, S., Pessi, M. A., et al. (2012). Hope Herth Index (HHI): a validation study in Italian patients with solid and hematological malignancies on active cancer treatment. Tumori J. 98, 385–392. doi: 10.1177/030089161209800317
Saggino, A., Bartoccini, A., Sergi, M. R., Romanelli, R., Macchia, A., and Tommasi, M. (2017). Assessing mindfulness on samples of italian children and adolescents: the validation of the italian version of the child and adolescent mindfulness measure. Mindfulness 8, 1364–1372. doi: 10.1007/s12671-017-0712-3
Saglietto, A., D’Ascenzo, F., Zoccai, G. B., and De Ferrari, G. M. (2020). COVID-19 in Europe: the Italian lesson. Lancet 395, 1110–1111. doi: 10.1016/S0140-6736(20)30690-5
Sanavio, E. (1997). CBA-2.0: Cognitive Behavioural Assessment 2.0: Scale Primarie: Manual [CBA-2.0: Primary Scales Manual]. Firenze: Giunti OS.
Scheier, M. F., Carver, C. S., and Bridges, M. W. (1994). Distinguishing optimism from neuroticism (and trait anxiety, self-mastery, and self-esteem): a reevaluation of the Life Orientation Test. J. Pers. Soc. Psychol. 67, 1063–1078. doi: 10.1037/0022-3514.67.6.1063
Sica, C., and Ghisi, M. (2007). “The Italian versions of the beck anxiety inventory and the beck depression inventory-ii: psychometric properties and discriminant power,” in Leading-Edge Psychological Tests and Testing Research, ed. M. A. Lange (Hauppauge, NY: Nova Science Publishers), 27–50.
Silva, J. A. M. D., Siegmund, G., and Bredemeier, J. (2015). Crisis interventions in online psychological counseling. Trends Psychiatry Psychother. 37, 171–182. doi: 10.1590/2237-6089-2014-0026
Snyder, C. R. (2000). The past and possible futures of hope. J. Soc. Clin. Psychol. 19, 11–28. doi: 10.1521/jscp.2000.19.1.11
Sood, S. (2020). Psychological effects of the Coronavirus disease-2019 pandemic. Res. Hum. Med. Educ. 7, 23–26.
Spielberger, C. D. (1983). State-Trait Anxiety Inventory for Adults (STAI-AD). Washington, DC: APA PsycTests.
Stukenberg, K. W., Dura, J. R., and Kiecolt-Glaser, J. K. (1990). Depression screening scale validation in an elderly, community-dwelling population. Psychol. Assess. J. Consult. Clin. Psychol. 2, 134–138. doi: 10.1037/1040-3590.2.2.134
Tan, B. Y., Chew, N. W., Lee, G. K., Jing, M., Goh, Y., Yeo, L. L., et al. (2020). Psychological impact of the COVID-19 pandemic on health care workers in singapore. Ann. Intern. Med. 173, 317–320.
Wang, Y., Wang, Y., Chen, Y., and Qin, Q. (2020). Unique epidemiological and clinical features of the emerging 2019 novel coronavirus pneumonia (COVID-19) implicate special control measures. J. Med. Virol. 92, 568–576. doi: 10.1002/jmv.25748
Keywords: COVID-19, anxiety, depression, resilience, lockdown
Citation: Tommasi M, Toro F, Arnò S, Carrieri A, Conte MM, Devastato MD, Picconi L, Sergi MR and Saggino A (2020) Physical and Psychological Impact of the Phase One Lockdown for COVID-19 on Italians. Front. Psychol. 11:563722. doi: 10.3389/fpsyg.2020.563722
Received: 20 May 2020; Accepted: 12 November 2020;
Published: 17 December 2020.
Edited by:
Changiz Mohiyeddini, Oakland University William Beaumont School of Medicine, United StatesReviewed by:
Marco Guicciardi, University of Cagliari, ItalyMeichen Yu, University of Pennsylvania, United States
Copyright © 2020 Tommasi, Toro, Arnò, Carrieri, Conte, Devastato, Picconi, Sergi and Saggino. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marco Tommasi, bWFyY28udG9tbWFzaUB1bmljaC5pdA==