 Yinuo Wu1†
Yinuo Wu1† Feng Jiang
Feng Jiang Yi-Lang Tang
Yi-Lang Tang Yuanli Liu
Yuanli Liu- 1Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China
- 2Institute of Health Yangtze River Delta, Shanghai Jiao Tong University, Shanghai, China
- 3Department of Population Medicine, Harvard Medical School, Boston, MA, United States
- 4Department of Psychiatry and Behavioral Sciences, Emory University, Atlanta, GA, United States
- 5Atlanta VA Medical Center, Decatur, GA, United States
- 6Department of Cardiology, Emergency General Hospital, Beijing, China
- 7School of Health Policy and Management, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China
Background: Medical disputes, medical disturbances, verbal and physical violence against physicians, and burnout have reached epidemic levels. They may negatively impact both physicians and the healthcare system. The experience of medical disputes, medical disturbances, verbal, and physical violence, and burnout and the correlates in physicians working in public hospitals in China needed to be investigated.
Methods: A nationwide cross-sectional survey study was conducted between 18 and 31 March 2019. An anonymous online questionnaire was administered. The questionnaire included the 22-item Maslach Burnout Inventory-Human Services Survey (Chinese version). We also collected data on demographic and job-related factors, as well as physicians’ experiences of medical disputes, medical disturbances, verbal and physical violence from patients and the patients’ family members.
Findings: In total, 22,213 physicians from 144 tertiary public hospitals in all of China’s 31 provinces completed the survey. The overall burnout rate among the surveyed physicians was 31.28%. Moreover, 33.48% of physicians experienced disputes, 20.86% experienced disturbances, 48.52% experienced verbal violence, and 5.84% experienced physical violence in the past 12 months. Factors found to be significantly associated with burnout included younger age, being divorced or widowed, having a lower educational background, working in internal medicine departments, longer working hours per day, working in general hospitals, being in East China, as well as having experienced disputes, disturbances, and physical and verbal violence.
Interpretation: Close to a third of the Chinese doctors working in the tertiary hospitals reportedly experienced burnout, and the problem is related to the unsafe working environment caused by the worsening doctor-patient relationship.
Introduction
Burnout is a work-related condition with symptoms consisting of emotional exhaustion, depersonalization, and a sense of reduced personal accomplishment (West et al., 2018). Physician burnout has been linked to adverse medical care, medical errors, poor physicians’ health and safety, including a higher risk of depression, alcohol abuse/dependence, and suicidal ideation, and higher intention to leave (Shanafelt et al., 2016; Collier, 2017; Panagioti et al., 2018; West et al., 2018; Dyer, 2019; Hu et al., 2019). It may also negatively impact healthcare organizations and systems. Several studies, involving different settings and specialties, showed that the prevalence of burnout was around 50% in practicing physicians (Embriaco et al., 2007; Rotenstein et al., 2018; Gas et al., 2019; Lin et al., 2019; Ma et al., 2019; The Lancet, 2019). Existing Chinese studies showed that the prevalence of burnout among oncologists, neurologists, and intensivists in China ranged from 51% to 61% (Zhou et al., 2017; See et al., 2018; Ma et al., 2019).
Negative workplace experiences, including disputes, disturbances, and verbal and physical violence, can create an unsafe and hostile working environment and lead to physician burnout (Hu et al., 2019). Medical disputes refer to any disputes between doctors (hospitals) and patients (and/or their family members) related to diagnosis and treatments (State Council of the PRC, 2018). A purposeful disturbance (Yi Nao in Chinese) is a type of medical dispute in which patients, their family members, or even “hired individuals” attempt to seek compensation for actual or perceived malpractice or dissatisfaction with services (such as death, unsuccessful surgeries, adverse side effects of medication, etc.). In doing so, they often threaten violence or assault medical staff (Hesketh et al., 2012; Zhou and Hao, 2019). This financially motivated mistreatment and violence against physicians is particularly common and severe in China, although the reasons are complex (Guo et al., 2019; The Lancet, 2020). Those medical mistreatments have further worsened the working environment for physicians, which may harm health care services. According to two previous surveys, the prevalences of disputes, verbal and physical violence reported by Chinese physicians were 7.96, 75.2, and 5.4%, respectively (Lu et al., 2015; Guo et al., 2019).
Despite frequent media reports of doctor-patient disputes and patient-led verbal and physical violence against physicians in China, there has been a gap in the literature on a comprehensive understanding of China’s physician burnout and its association with the rising incidence of disputes and violence in the Chinese healthcare facilities. A few previous estimates of mistreatment and burnout in physicians were based on surveys with relatively small sample size or involved only one specialty or a limited number of local hospitals (Li et al., 2003; Bennett et al., 2005; Chen et al., 2008; Fan et al., 2012; Kumar et al., 2013; Liang et al., 2014; Lin and Li, 2015; Kealy et al., 2016; Banerjee et al., 2017; Busis et al., 2017; Rassolian et al., 2017; Balzora and Weinshel, 2018; Brashear and Vickrey, 2018; Burki, 2018; Chang et al., 2018; Patti et al., 2018; Hu et al., 2019; Ma et al., 2019). One study conducted among surgery residents in the United States found that burnout was associated with verbal or physical abuse (Hu et al., 2019). It is essential to study the frequency and extent of burnout and mistreatment involving multiple hospitals and all typical clinical specialties. This survey was set to collect such data and examine the associations between physician burnout and demographic and job-related factors, especially mistreatment experiences.
Data and Methods
Study Design and Samples
The study was a part of the China National Healthcare Improvement Initiative Survey in 2019 (Zhou et al., 2018). The National Health Commission of China approved and supported this project. The survey was conducted on March 18–31, 2019. Totally 144 tertiary public hospitals in capital cities of the 31 provinces in mainland China were selected to participate in the survey. Among them were 59 general hospitals, 37 Traditional Chinese Medicine (TCM) hospitals, 33 maternal and children’s hospitals, five stomatological hospitals, four cancer hospitals, and six other specialty hospitals.
Based on their employee’s ID codes in the hospital staff lists, physicians were sampled through a systematic sampling method in each participating hospital. We invited 170 physicians from each hospital to participate in the survey. The survey was conducted anonymously through WeChat, a popular online social media application in China.
Ethics Statement
The protocol of this study was approved by the Ethics Committee (IEC) of the Emergency General Hospital in Beijing, China. All participants signed the informed consent before they proceeded to respond to the questionnaires. The informed consent statement explained the purpose of the survey, ensured that the data would be de-identified before analysis and that the hospitals’ administrators would not have access to their responses.
Measures
The items on medical disputes, purposeful disturbances, and violence were adapted from previously published and validated instruments (Liang et al., 2014; Lu et al., 2015; Guo et al., 2019; Zhou and Hao, 2019). Detailed operational definitions for medical disputes, medical disturbances, and violence were included in the questionnaire for better reliability.
Respondents were asked to report whether they experienced medical disputes or medical disturbances and reported the frequency of verbal violence and physical violence from patients and/or patients’ family members in the previous year.
The dimensions of burnout were assessed using the Maslach Burnout Inventory–Human Services Survey (MBI–HSS) (Chinese version), which was developed by the Chinese Academy of Sciences with solid reliability and validity (Li et al., 2003). It includes three subscales: emotional exhaustion (EE), depersonalization (DP), and low personal accomplishment (PA). As there are different thresholds for burnout (Rotenstein et al., 2018), we defined EE as EE score ≥27, DP as DP score ≥10, and PA as PA score ≤33. The overall burnout was defined as EE score ≥27 and/or DP score ≥10 (Maslach et al., 2010).
Additionally, we collected participants’ sociodemographic data, including age, sex, marital status, number of children, educational level; and job-related factors, including their departments, working hours per day, hospital type and the regions where the participants worked (East China, Middle China, and West China).
Before the survey was made available to all participants, a pilot survey was conducted among 150 physicians to assess the questionnaire’s overall coherence, balance, and clarity.
Statistical Analysis
Descriptive analyses were conducted for the variables. Continuous variables were shown with mean and standard deviation, while categorical variables were shown with percentages. Age and working hours were treated as a continuous variable. Chi-square tests were used to examine all categorical variables. Multivariable logistic regression models were used to examine all variables associated with burnout. Models of excluding and including mistreatment exposure were used to test the effects of mistreatment on burnout. The primary model examined the association between the composite mistreatment variable and burnout. All models were estimated with robust standard errors as physicians clustering within hospitals. Missing data were rare (<1%) and were excluded from the analyses.
Stata 15 (StataCorpLP, College Station, TX, United States) was used for these statistical analyses. All of the tests were two-sided, and the statistical significance was defined as P < 0.05.
Results
Description of Sample Characteristics and Related Factors
In total, 24,480 physicians were invited to participate, and 22,416 responded (response rate = 91.57%). After removing 203 participants with incomplete data, data from 22,213 physicians (99.09%) were included in the analysis. Their sociodemographic characteristics are shown in Table 1.
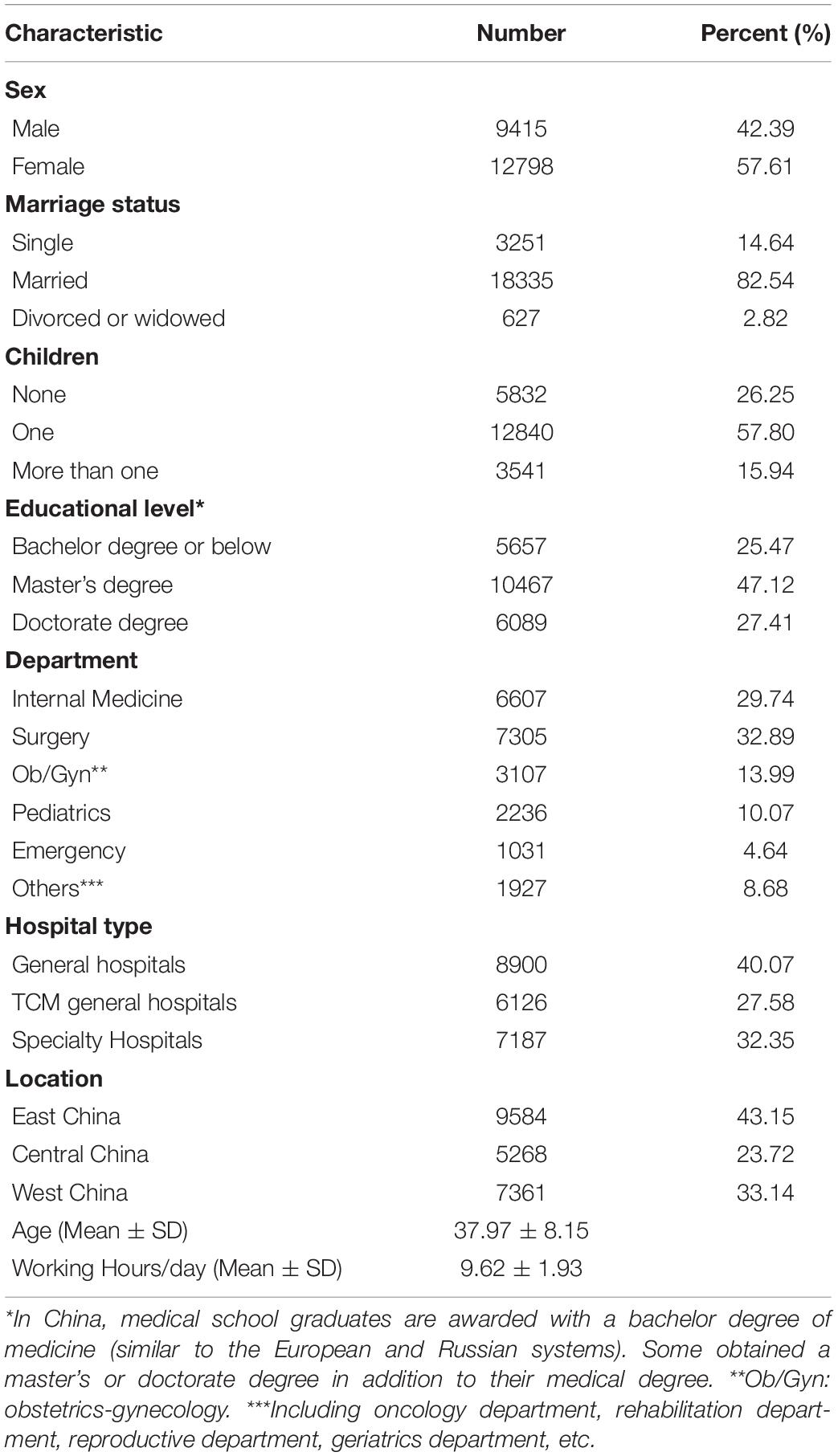
Table 1. Characteristics of physicians in tertiary public hospitals (N = 22,213).
Among all participants, 57.61% were women, 82.54% were married, and nearly three quarters (73.75%) had at least one child, and a similar percentage (74.53%) had a master’s or a doctorate degree in addition to an undergraduate medical degree. More than one third were in the surgery department (surgeons), 40.07% worked in general hospitals, and 43.15% worked in East China. The mean age was 37.97 ± 8.15 years old. On average, they worked 9.62 ± 1.93 h per day, and 66.54% worked longer than 8 h per day, exceeding the limit set by the Labor Law of China (China Legal System Publishing House, 2018).
Burnout Among Physicians
Table 2 shows the distribution of burnout across different subgroups of physicians. Overall burnout was reported by 31.28% physicians, with 17.89% reporting symptoms of EE, 27.60% reporting DP and 48.27% reporting PA. As shown in Table 3, physicians who were male, single, without children, working in pediatric departments, in general hospitals, in West China, experienced a higher rate of overall burnout.
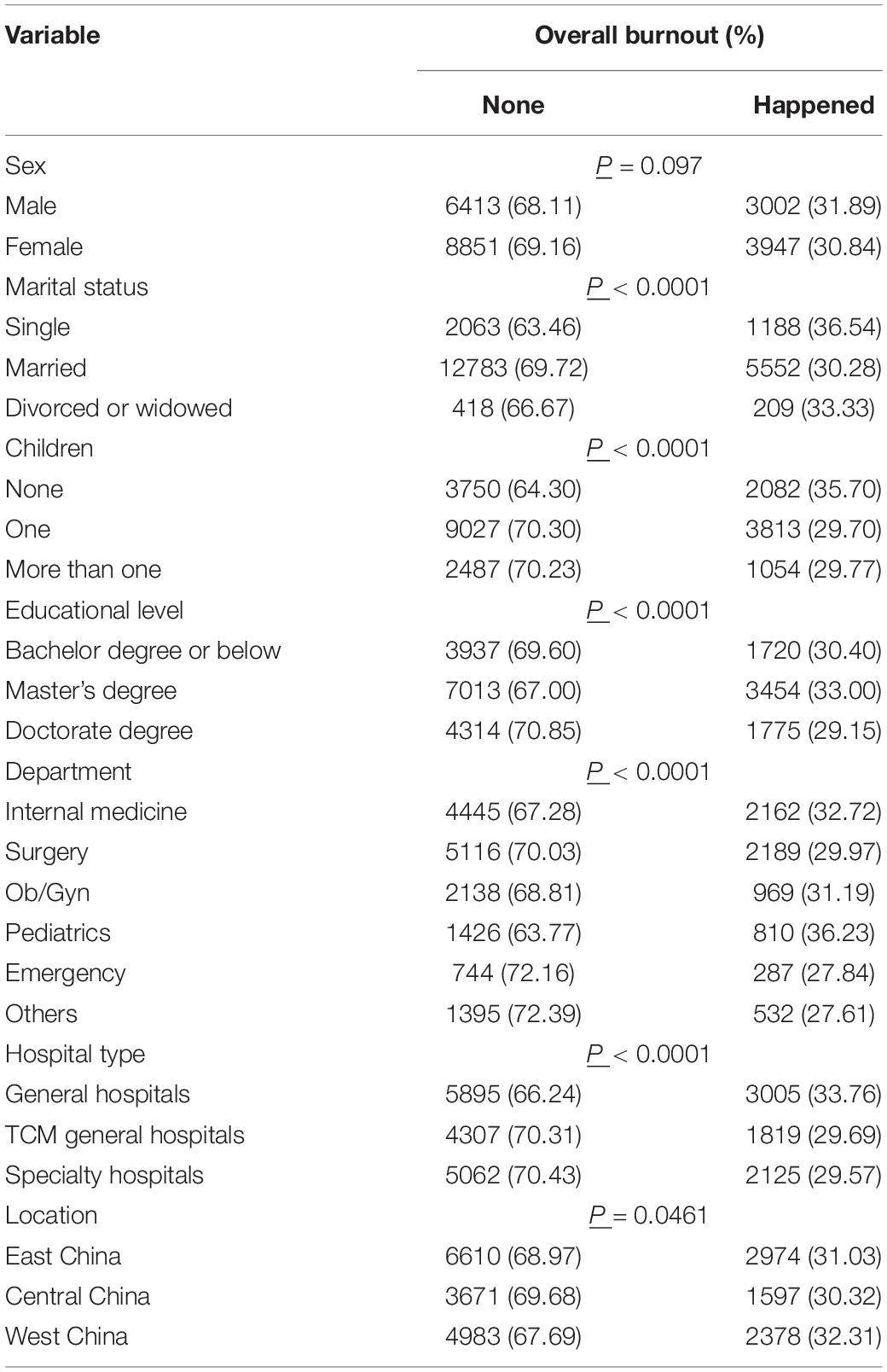
Table 2. Distribution of burnout.
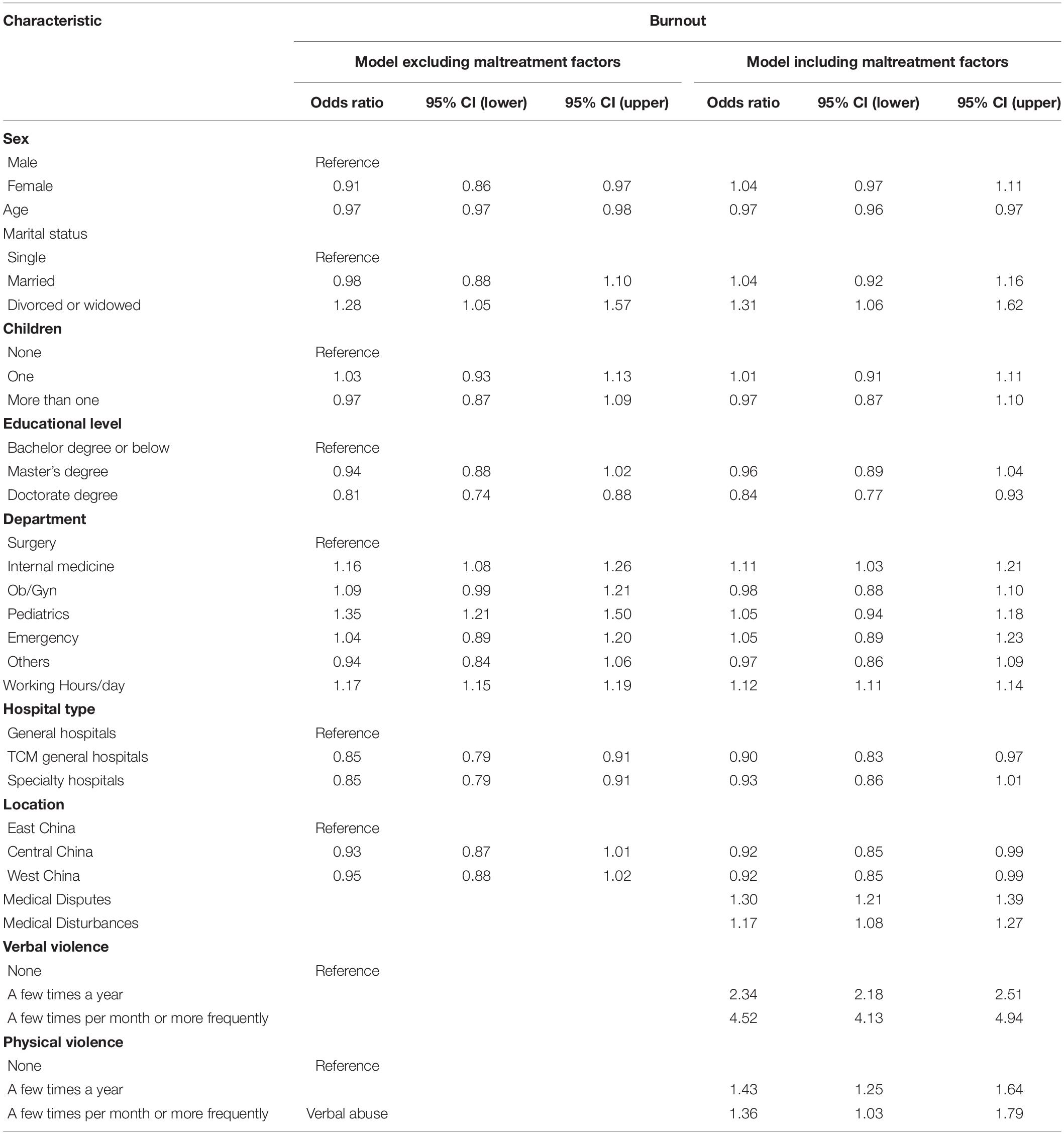
Table 3. Factors associated with burnout among Chinese physicians.
Medical Disputes, Medical Disturbances, Verbal, and Physical Violence
The frequency and distribution of different types of mistreatment are shown in Tables 4, 5.
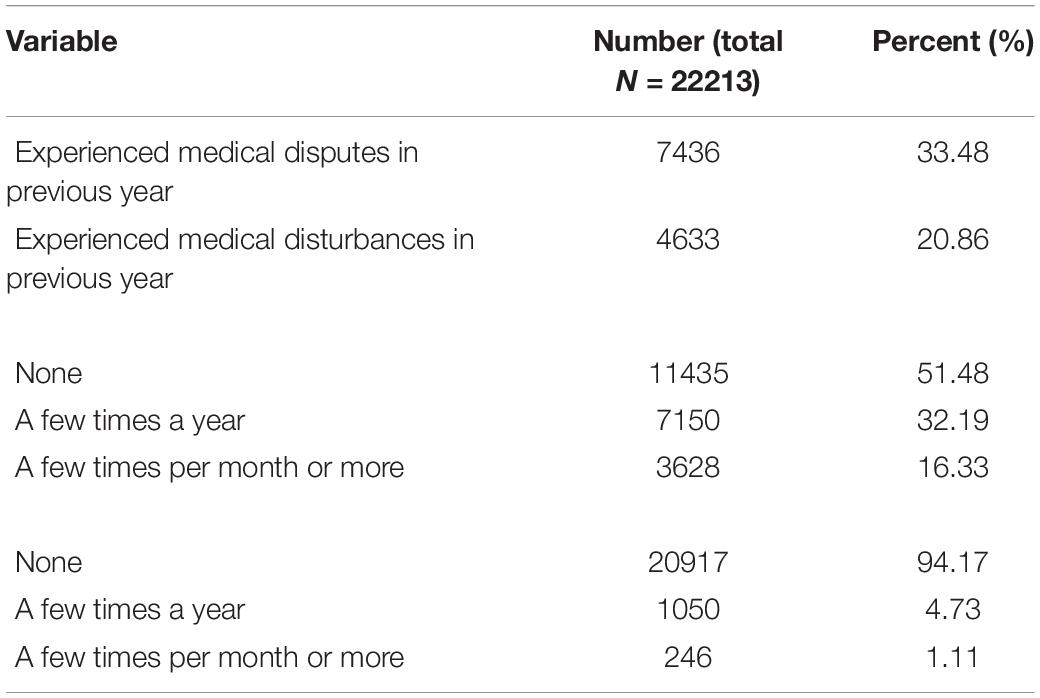
Table 4. Frequency of medical disputes, medical disturbances, verbal and physical violence among Chinese physicians.
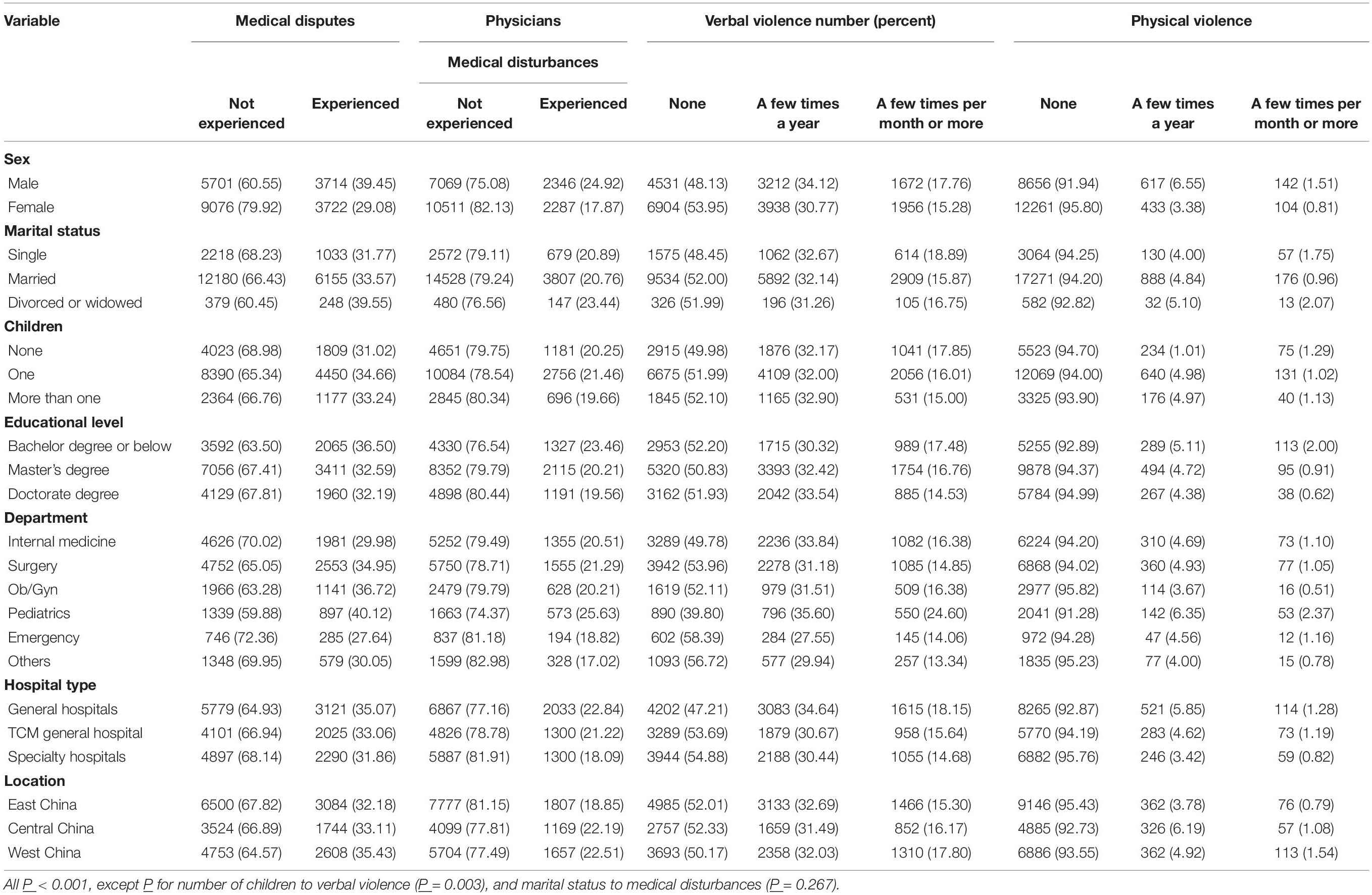
Table 5. Distribution of medical disputes, medical disturbance, verbal and physical violence among Chinese.
Among them, 33.48% reported medical disputes in the previous year. Higher rates of medical disputes were seen among physicians who were male, divorced or widowed, had one child, from a lower educational background, in pediatric departments, in general hospitals, and in West China. The logistic analysis showed that physicians who were older, working in obstetrics-gynecology (Ob/Gyn) and pediatrics departments, longer working hours/day, in West China were significantly more likely to experience (Supplementary Table 1).
One fifth (20.86%) of physicians reported experiencing medical disturbances, and male physicians reported a higher rate (24.92%) than female physicians (17.87%, P < 0.001). The overall trend of the subgroup analysis regarding medical disturbances was similar to that of medical disputes. Namely, the rate was higher in those who were divorced or widowed, had one child, had a lower educational background, and was in pediatric departments, general hospitals, and in West China. The logistic analysis showed that physicians who were older, working in Ob/Gyn and pediatrics departments, longer working hours/day, in Central China and West China were significantly more likely to experience medical disturbances (Supplementary Table 1).
Instances of verbal violence were also collected in the surveyed sample. In total, 48.52% reported experiencing verbal violence from patients and/or patients’ family members in the previous year (32.19% a few times a year, 16.33% a few times per month or more). The logistic analysis showed that physicians who were working in internal medicine, Ob/Gyn and pediatrics departments, working longer hours/day were more likely to experience verbal violence (Supplementary Table 1).
In total, 5.84% of physicians experienced physical violence in the previous year (4.73% a few times a year, 1.11% a few times per month or more). The logistic analysis showed that physicians who were older, working in pediatrics departments, working longer hours/day, in Central China and West China were more likely to experience physical violence (Supplementary Table 1).
Factors Associated With Burnout
We performed logistic analyses to identify factors associating with overall burnout (Table 3). In the unadjusted model, which excluded the mistreatment factors, physicians who were female (odds ratio[OR], 0.91; 95% confidence interval [CI], 0.86–0.97), the elder (OR, 0.97; 95% CI, 0.97–0.98), with a doctoral degree (reference group: physicians with a college degree or below, OR, 0.81; 95% CI, 0.74–0.88), working in TCM general hospitals and specialty hospitals (reference: working in general hospitals, OR, 0.85; 95% CI, 0.79–0.91), were less likely to experience overall burnout. While those who were divorced or widowed (reference: single, OR 1.28; 95% CI, 1.05–1.57), in internal medicine and pediatric departments (OR, with surgery departments as a reference, 1.16, 1.35; 95% CI, 1.08–1.26, 1.21–1.50, respectively), longer working hours per day (OR, 1.17; 95% CI, 1.15–1.19), were more likely to experience overall burnout.
When mistreatment factors were included, the association with sex and pediatric departments was no longer significant. The regional difference remained significant, as physicians in Central China and West China (OR, with East China as a reference, 0.92; 95% CI, 0.85–0.99, respectively) were less likely to have overall burnout.
Compared with the group that reported no verbal violence, physicians who reported more frequent verbal violence were more likely to have overall burnout. A similar trend was found with physical violence (Table 3).
Discussion
This study was the first nationwide survey on physician burnout in China and associated medical disputes, purposeful disturbances, violence among a large, nationally representative sample in China. By surveying physicians in tertiary public hospitals and obtaining a very high response rate, we comprehensively assessed the extent of burnout in China and its relationships to medical disputes, disturbances verbal and physical violence against physicians. We found that indeed the experience of mistreatment was significantly associated with physician burnout.
We found that the overall burnout rate in physicians in China is very close to the rate in Canadian pediatricians (34.1%) (Bennett et al., 2005), but lower than findings from other studies (West et al., 2016, 2018; The Lancet, 2019; Yates, 2020). For example, this percentage is lower than that of United States neurologists (60.1%) (Busis et al., 2017), United States oncologists (44.7%) (Shanafelt et al., 2014), United States surgeons (40%) (Shanafelt et al., 2009), French intensivists (46.5%) (Embriaco et al., 2007), Chinese neurologists (53.2%) (Zhou et al., 2017), and Chinese oncologists (51.0%) (Ma, 2017). Our findings are also lower than the findings of another online large sample survey (N > 15000, 29 specialties) in the United States, which found that 44% of physicians reported burnout (Lesile Kane, 2019). There are also some similarities: for example, the United States survey also found that female physicians, those working in internal medicine or Ob/Gyn departments, and those working longer hours were more likely to report burnout. The lower rate of burnout among Chinese physicians in this study, compared to their international counterparts, may be due to the overall high level of tolerance for workload in the continuously over-crowded hospitals, large and inclusive sample, very high response rate (>90%), and the timing of study (mid to late March) when physicians’ workload is traditionally lower in China (Zhang et al., 2018).
We found that one-third of physicians experienced medical disputes in the previous year in tertiary public hospitals. This high rate is very concerning. In recent years, the rate of medical disputes has increased rapidly in China, with the growth rate ranging from 11–24.5%, and the overall rate in this survey is even higher than all existing reports (Chen et al., 2008; Wu, 2015; Yu et al., 2018). The rate of medical disputes experienced by physicians varies from study to study. For example, Fan et al. (2012) found that there were 2.2 medical disputes per 100 physicians in Beijing and 1.32 per 100 physicians in Shanxi province, and both were lower than that in England and Germany, which were at 5.96 and 2.45%, respectively (Fan et al., 2012). Lu et al. (2015) showed that the rate of medical disputes was 5.89 per 100 physicians in 2010–2013. As many medical disputes are resolved by physicians and patients themselves without hospital management’s involvement, the data on the hospital-level is less than what was reported by physicians. Meanwhile, our findings showing that the physicians in the pediatrics, Ob/Gyn, and surgery departments reporting the highest rates of medical disputes is in line with several previous studies (Zhang and Zhao, 2014; Lin and Li, 2015; Wang et al., 2015).
In this study, 20.86% of physicians reported experiencing medical disturbances in the previous year. This alarmingly high rate of medical disturbances should serve as a warning, and it suggests up to a fifth of physicians in tertiary public hospitals were exposed to potential severe threats and safety risks at work. In recent years, the occurrence of medical disturbances has also sharply increased in China (The Lancet, 2020). According to a survey conducted by the Chinese Medical Doctors Association, within a sample of 48 hospitals, 47 hospitals (97.62%) had suffered from significant medical disturbances in 2006 (Chinese Medical Doctor Association, 2007). Our survey was the first to report national data of medical disturbances on an individual level among physicians.
According to our survey, the prevalence of frequent verbal violence and physical violence from patients or their family members was in line with other studies in China (Guo et al., 2019; Hu et al., 2019). In the past few years, some cases involving violence against physicians, especially those involving death or severe injury, have caused considerable public outrage. As an effort to curb such crimes, a law was recently hurriedly passed by the People’s Congress of China (Li and Gao, 2019).
Although medical disputes and workplace violence against doctors happen in almost all cultures, the overall situation has worsened in China’s past few decades (The Lancet, 2020). There, the patient-doctor relationship has become more contentious, and doctors are less respected. It has even affected the career trends among high school graduates, making them less likely to choose medicine as their career (Ma, 2017; Ou et al., 2019).
Many related factors, including cultural, institutional, and individual aspects, had been studied (Lin and Li, 2015; Lu et al., 2015; Amirthalingam, 2017; Reddy et al., 2019; Zhou and Hao, 2019). Concerning China’s situation, a few factors have been frequently discussed and considered to contribute to the rapid increase in these events. The proportion of the Chinese government’s health expenditure in the total national health expenditure is low, which was 58.0% in 2016, compared with the global average level of 74.3% (The World Bank, 2019). Meanwhile, the proportion of government input to the total income of public hospitals has been below 10% in recent years, which is one-third of the global average level (around 30%) (Hu and Zhu, 2019). On the social level, there is a conflict between the huge demand for health services and the limited rate of resource growth, especially in rural areas (Niu et al., 2016; Zeng et al., 2018). In the meantime, the cost of health care has increased rapidly, and many patients have unrealistic expectations (Zhao and Qiao, 2013; Wang et al., 2019). Professionally, many doctors in China lack the necessary training to be effective communicators and identify and deescalate conflicts (Wei et al., 2015). Hesketh et al. (2003) suggested that the “broken windows” theory might be a useful tool to conceptualize why workplace violence occurs and proposed proactiveness in dealing with minor forms of abuse or violence as early as possible.
In this study, mistreatment, more than any other individual or hospital characteristics, was significantly associated with overall burnout, consistent with the findings reported in a sample of surgery residents in the United States (Hu et al., 2019). This may be due to the negative psychological effects caused by mistreatment; meanwhile, the burnout physicians are also more likely to encounter mistreatment. The psychological status or the personality of a physician may be a core factor. Because the literature examining the association between mistreatment and physicians’ burnout is scarce, more studies are needed, especially studies examining pathways and mechanisms, effective interventions, or physicians’ recognition status.
Policymakers and hospital administrators need to be aware of these crucial issues, and urgent actions need to be taken, including increasing the healthcare budget, strengthening legal actions to protect physicians’ safety, hiring security guards in high-risk areas, recruiting more social workers, and improving staff training for effective communication and conflict resolution. A safer healthcare environment would improve physicians’ well-being and improve healthcare quality for patients.
Several limitations of this study should be pointed out. First, as in all cross-sectional studies, the causal relationship of different factors cannot be established. Second, our study did not include some other potentially influential factors. For example, personalities have been reported to be associated with burnout (Bughi et al., 2017; van der Wal et al., 2018), but we did not have data to measure it. Other potentially relevant factors, such as income level, staff and administrative support, and the use of electronic medical records (Fred and Scheid, 2018), have not been included in the survey. Third, we did not include any questions about sexual harassment, which is emerging as an essential aspect of the work environment. Fourth, the sample hospitals are tertiary public hospitals, not including primary medical units or other type hospitals, so the results may not be generalizable to all hospitals. Finally, we only focused on violence from patients and patients’ families, and we did not ask questions about violence from the staff. Studies show that violence from the staff was also common and as harmful as violence from patients (Abed et al., 2016; Moylan, 2017; Hu et al., 2019).
Conclusion
In conclusion, we found that burnout, experiences of medical disputes, purposeful disturbances, and physical and verbal violence were common among Chinese physicians. These experiences were significantly associated with overall burnout. Our results provided some insights into why and how a safer, more sustainable healthcare system might be established.
Data Availability Statement
All datasets presented in this study are available upon request.
Ethics Statement
The protocol of this study was approved by the Ethics Committee (IEC) of the Emergency General Hospital in Beijing, China. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
YW, FJ, JM, Y-LT, MW, and YL: conceptualization. YW: data curation and investigation. FJ: data analysis and writing an original draft. YL: funding acquisition. FJ and Y-LT: methodology. FJ, JM, Y-LT, and YL: writing revision and editing. All authors contributed to the article and approved the submitted version.
Funding
The National Health Commission of China funded this project.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors thank all the field survey interviewers for their dedicated fieldwork and physicians who participated in the survey for their time and effort in completing the survey. We would also like to thank Ms. Brianna Wong, BS, CCRC, at the Atlanta VA Medical Center; and Sida Tang, BA, for their comments on and editing of this manuscript.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2020.556517/full#supplementary-material
References
Abed, M., Morris, E., and Sobers-Grannum, N. (2016). Workplace violence against medical staff in healthcare facilities in Barbados. Occup. Med. 66, 580–583. doi: 10.1093/occmed/kqw073
Amirthalingam, K. (2017). Medical dispute resolution, patient safety and the doctor-patient relationship. Singapore Med. J. 58, 681–684. doi: 10.11622/smedj.2017073
Balzora, S., and Weinshel, E. (2018). Addressing physician burnout among practicing physicians. Clin. Gastroenterol. Hepatol. 16, 153–154. doi: 10.1016/j.cgh.2017.07.015
Banerjee, S., Califano, R., Corral, J., De Azambuja, E., De Mattos-Arruda, L., Guarneri, V., et al. (2017). Professional burnout in European young oncologists: results of the European society for medical oncology (ESMO) young oncologists committee burnout survey. Ann. Oncol. 28, 1590–1596. doi: 10.1093/annonc/mdx196
Bennett, S., Plint, A., and Clifford, T. J. (2005). Burnout, psychological morbidity, job satisfaction, and stress: a survey of Canadian hospital based child protection professionals. Arch. Dis. Child. 90, 1112–1116. doi: 10.1136/adc.2003.048462
Brashear, A., and Vickrey, B. G. (2018). Burnout in neurology: extinguishing the embers and rekindling the joy in practice. Neurology 91, 907–908. doi: 10.1212/wnl.0000000000006520
Bughi, S. A., Lie, D. A., Zia, S. K., and Rosenthal, J. (2017). Using a personality inventory to identify risk of distress and burnout among early stage medical students. Educ. Health 30, 26–30. doi: 10.4103/1357-6283.210499
Burki, T. K. (2018). Oncologists burnout in the spotlight. Lancet Oncol. 19:e238. doi: 10.1016/s1470-2045(18)30275-4
Busis, N. A., Shanafelt, T. D., Keran, C. M., Levin, K. H., Schwarz, H. B., Molano, J. R., et al. (2017). Burnout, career satisfaction, and well-being among US neurologists in 2016. Neurology 88, 797–808. doi: 10.1212/wnl.0000000000003640
Chang, E. Y., Bakinde, N., and Umar, A. (2018). Correlates and outcomes of physician burnout. JAMA Intern. Med. 178, 999–1000. doi: 10.1001/jamainternmed.2018.2384
Chen, S. X., Hu, P. F., Peng, X. M., Zai, Z. T., Tian, Y. L., and Liu, T. Q. (2008). The rapid growth of medical disputes: reasons and countermeasures in Guangdong public hospitals. Chin. Hosp. Manage. 28, 20–22.
China Legal System Publishing House (2018). Labor Law of the People’s Republic of China. Beijing: China Legal System Publishing House.
Chinese Medical Doctor Association (2007). The incidence of “medical disturbance” in 2006 was 97.92%. China Health 50, 34–36.
Collier, R. (2017). Physician burnout a major concern. CMAJ 189, E1236–E1237. doi: 10.1503/cmaj.1095496
Dyer, O. (2019). Physician burnout costs US $4.6bn a year, study finds. BMJ 365:l2361. doi: 10.1136/bmj.l2361
Embriaco, N., Azoulay, E., Barrau, K., Kentish, N., Pochard, F., Loundou, A., et al. (2007). High level of burnout in intensivists: prevalence and associated factors. Am. J. Respir. Crit. Care Med. 175, 686–692. doi: 10.1164/rccm.200608-1184OC
Fan, Z., Zhang, Y. L., Han, X. J., and Lu, G. M. (2012). Compare analysis on medical negligence claims incidence rate among Beijing, Shanxi, Germany and England. Chin. Hosp. 16, 2–3.
Fred, H. L., and Scheid, M. S. (2018). Physician burnout: causes, consequences, and (?) Cures. Tex. Heart Inst. J. 45, 198–202. doi: 10.14503/thij-18-6842
Gas, J., Bart, S., Michel, P., Peyronnet, B., Bergerat, S., Olivier, J., et al. (2019). Prevalence of and predictive factors for burnout among French urologists in training. Eur. Urol. 75, 702–703. doi: 10.1016/j.eururo.2018.12.037
Guo, J., Wu, S. C., Zhang, C. Y., Han, X. Y., Hu, L. L., Zhang, J., et al. (2019). The current situation of hospital violence aimed at medical staffs in 136 tertiary hospitals in China. Chin. J. Health Educ. 35, 312–317.
Hesketh, K. L., Duncan, S. M., Estabrooks, C. A., Reimer, M. A., Giovannetti, P., Hyndman, K., et al. (2003). Workplace violence in Alberta and British Columbia hospitals. Health Policy 63, 311–321. doi: 10.1016/s0168-8510(02)00142-2
Hesketh, T., Wu, D., Mao, L., and Ma, N. (2012). Violence against doctors in China. BMJ 345:e5730. doi: 10.1136/bmj.e5730
Hu, L. J., and Zhu, J. L. (2019). Research on the status quo and countermeasure of government input of public hospitals. Chinese Hospitals 23, 19–21.
Hu, Y. Y., Ellis, R. J., Hewitt, D. B., Yang, A. D., Cheung, E. O., Moskowitz, J. T., et al. (2019). Discrimination, abuse, harassment, and burnout in surgical residency training. N. Engl. J. Med. 381, 1741–1752. doi: 10.1056/NEJMsa1903759
Kealy, D., Halli, P., Ogrodniczuk, J. S., and Hadjipavlou, G. (2016). Burnout among Canadian psychiatry residents: a national survey. Can. J. Psychiatry 61, 732–736. doi: 10.1177/0706743716645286
Kumar, S., Sinha, P., and Dutu, G. (2013). Being satisfied at work does affect burnout among psychiatrists: a national follow-up study from New Zealand. Int. J. Soc. Psychiatry 59, 460–467. doi: 10.1177/0020764012440675
Lesile Kane (2019). Medscape National Physician Burnout, Depression & Suicide Report 2019. Berlin: Medscape.
Li, C. P., Shi, K., Luo, Z. X., Li, L., and Yang, R. (2003). An investigation on job burnout of doctor and nurse. Chin. J. Clin. Psychol. 11, 170–172.
Li, L., and Gao, L. (2019). Legal measures for prevetion of medical disputes-interpretation of “regulations on prevention and handling of medical disputes”. China Health Law 27, 7–11.
Liang, Z. J., Wu, C., Guo, H. Y., Yu, Y. L., and Yuchi, Z. H. (2014). Analysis of 430 cases of medical disputes data in a tertiary grade a comprehensive hospital. Chin. Hosp. Manage. 34, 57–59.
Lin, M., Battaglioli, N., Melamed, M., Mott, S. E., Chung, A. S., and Robinson, D. W. (2019). High prevalence of burnout among US emergency medicine residents: results from the 2017 national emergency medicine wellness survey. Ann. Emerg. Med. 74, 682–690. doi: 10.1016/j.annemergmed.2019.01.037
Lin, X. Y., and Li, W. (2015). Investigation on 1552 cases of medical dispute. Chin. Hosp. 19, 61–62.
Lu, G. M., Fan, Z., Han, X. J., Fan, J. L., Gong, X. M., Huang, Z. G., et al. (2015). Investigation on incidence and its compensation of medical disputes in 27 hospitals. Chin. Hosp. Manage. 35, 34–36.
Ma, S., Huang, Y., Yang, Y., Ma, Y., Zhou, T., Zhao, H., et al. (2019). Prevalence of burnout and career satisfaction among oncologists in China: a national survey. Oncologist 24, e480–e489. doi: 10.1634/theoncologist.2018-0249
Ma, Y. (2017). Study on effect of medical accidents on the students career-choosing psychology. China Health Ind. 14, 197–198.
Maslach, C., Susan, E., and Leiter, M. (2010). Maslach Burnout Inventory Manual, 3rd Edn. Menlo Park, CA: Mind garden.
Moylan, S. (2017). Occupational violence and staff safety in general practice. Aust. Fam. Physician 46, 952–956.
Niu, S. Z., Yan, J. F., and Niu, M. Y. (2016). Analysis of the current situation of medical disputes and countermeasures. Leg. Syst. Soc. 24, 185–186.
Ou, Y., Zhou, H., Tai, X. M., Yang, D. W., He, H. J., Wang, J., et al. (2019). Investigation and analysis of doctor -patient R elationship cognition and career tendency in medical graduates. China Health Ind. 16, 170–172.
Panagioti, M., Geraghty, K., Johnson, J., Zhou, A., Panagopoulou, E., Chew-Graham, C., et al. (2018). Association between physician burnout and patient safety, professionalism, and patient satisfaction: a systematic review and meta-analysis. JAMA Intern. Med. 178, 1317–1330. doi: 10.1001/jamainternmed.2018.3713
Patti, M. G., Schlottmann, F., and Sarr, M. G. (2018). The problem of burnout among surgeons. JAMA Surg. 153, 403–404. doi: 10.1001/jamasurg.2018.0047
Rassolian, M., Peterson, L. E., Fang, B., Knight, H. C. Jr., Peabody, M. R., Baxley, E. G., et al. (2017). Workplace factors associated with burnout of family physicians. JAMA Intern. Med. 177, 1036–1038. doi: 10.1001/jamainternmed.2017.1391
Reddy, I. R., Ukrani, J., Indla, V., and Ukrani, V. (2019). Violence against doctors: a viral epidemic? Indian J. Psychiatry 61, S782–S785. doi: 10.4103/psychiatry.IndianJPsychiatry_120_19
Rotenstein, L. S., Torre, M., Ramos, M. A., Rosales, R. C., Guille, C., Sen, S., et al. (2018). Prevalence of burnout among physicians: a systematic review. JAMA 320, 1131–1150. doi: 10.1001/jama.2018.12777
See, K. C., Zhao, M. Y., Nakataki, E., Chittawatanarat, K., Fang, W. F., Faruq, M. O., et al. (2018). Professional burnout among physicians and nurses in Asian intensive care units: a multinational survey. Intensive Care Med. 44, 2079–2090. doi: 10.1007/s00134-018-5432-1
Shanafelt, T. D., Balch, C. M., Bechamps, G. J., Russell, T., Dyrbye, L., Satele, D., et al. (2009). Burnout and career satisfaction among American surgeons. Ann. Surg. 250, 463–471. doi: 10.1097/SLA.0b013e3181ac4dfd
Shanafelt, T. D., Dyrbye, L. N., West, C. P., and Sinsky, C. A. (2016). Potential impact of burnout on the US physician workforce. Mayo Clin. Proc. 91, 1667–1668. doi: 10.1016/j.mayocp.2016.08.016
Shanafelt, T. D., Gradishar, W. J., Kosty, M., Satele, D., Chew, H., Horn, L., et al. (2014). Burnout and career satisfaction among US oncologists. J. Clin. Oncol. 32, 678–686. doi: 10.1200/jco.2013.51.8480
State Council of the PRC (2018). Regulations on Prevention and Handling of Medical Disputes [Online]. Beijing: The Central People’s Government of the People’s Republic of China.
The Lancet (2019). Physician burnout: a global crisis. Lancet 394:93. doi: 10.1016/s0140-6736(19)31573-9
The World Bank (2019). World Bank Open Data. Available online at: https://data.worldbank.org/ (accessed February 11, 2020).
van der Wal, R. A. B., Wallage, J., and Bucx, M. J. L. (2018). Occupational stress, burnout and personality in anesthesiologists. Curr. Opin. Anaesthesiol. 31, 351–356. doi: 10.1097/aco.0000000000000587
Wang, J. H., Li, X. M., Liu, G. D., Xie, F. Z., Liu, M. H., Wang, K. X., et al. (2019). Stigma towards Chinese doctors: concept, causes and logic. Chin. Hosp. Manage. 39, 56–58.
Wang, J. J., Zhong, L. T., Zeng, Q., Chen, G., Han, P., and Xu, S. Q. (2015). Analysis of the medical complaint data from 2009 to 2013 in a grade-a hospital in Beijing. Chin. Hosp. Manage. 35, 51–53.
Wei, Z. Z., Zhang, S. P., and Duan, H. M. (2015). Doctor-patient relationship research trend and doctor-patient dispute reason analysis. Chin. Med. Ethics 28, 937–939.
West, C. P., Dyrbye, L. N., Erwin, P. J., and Shanafelt, T. D. (2016). Interventions to prevent and reduce physician burnout: a systematic review and meta-analysis. Lancet 388, 2272–2281. doi: 10.1016/s0140-6736(16)31279-x
West, C. P., Dyrbye, L. N., and Shanafelt, T. D. (2018). Physician burnout: contributors, consequences and solutions. J. Intern. Med. 283, 516–529. doi: 10.1111/joim.12752
Wu, C. Q. (2015). On the solution to the current medical disputes in China. Med. Jurisprud. 7, 16–19.
Yates, S. W. (2020). Physician stress and burnout. Am. J. Med. 133, 160–164. doi: 10.1016/j.amjmed.2019.08.034
Yu, F., Xie, X., Ding, F., Xue, C., and Sun, Z. (2018). Changing procedures for resolving medical disputes in China. Intern. Med. J. 48, 1552–1553. doi: 10.1111/imj.14133
Zeng, Y., Zhang, L., Yao, G., and Fang, Y. (2018). Analysis of current situation and influencing factor of medical disputes among different levels of medical institutions based on the game theory in Xiamen of China: a cross-sectional survey. Medicine 97:e12501. doi: 10.1097/MD.0000000000012501
Zhang, N. L., and Zhao, J. (2014). Statistical analysis of medical dispute cases based on related literatures from 2009 to 2013. Med. Soc. 27, 55–58.
Zhang, Y. F., Shen, S., Gai, X. R., Zhao, Y. F., and Luo, H. (2018). Dynamic analysis and prediction of outpatient volume in a large general hospital in Beijing. Chin. J. Health Stat. 35, 590–592.
Zhao, D. H., and Qiao, X. B. (2013). A study of ethics problem in medical dispute reports of network media and the countermeasures. Acta Univ. Med. Nanjing 13, 474–478.
Zhou, H., Han, X., Zhang, J., Sun, J., Hu, L., Hu, G., et al. (2018). Job satisfaction and associated factors among medical staff in tertiary public hospitals: results from a national cross-sectional survey in China. Int. J. Environ. Res. Public Health 15:1528. doi: 10.3390/ijerph15071528
Zhou, H., and Hao, Z. M. (2019). Domestic and foreign research status of medical disturbance. China Health Ind. 16, 113–117.
Keywords: physician burnout, medical disputes, workplace violence, hospitals, China
Citation: Wu Y, Jiang F, Ma J, Tang Y-L, Wang M and Liu Y (2021) Experience of Medical Disputes, Medical Disturbances, Verbal and Physical Violence, and Burnout Among Physicians in China. Front. Psychol. 11:556517. doi: 10.3389/fpsyg.2020.556517
Received: 28 April 2020; Accepted: 21 October 2020;
Published: 29 January 2021.
Edited by:
Changiz Mohiyeddini, Oakland University William Beaumont School of Medicine, United StatesCopyright © 2021 Wu, Jiang, Ma, Tang, Wang and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jing Ma, amluZ21hODhAZ21haWwuY29t; Yuanli Liu, bGl1eWxfZnBvQDEyNi5jb20=
†These authors have contributed equally to this work