 Jinhui Li
Jinhui Li Yin-Leng Theng
Yin-Leng Theng Schubert Foo
Schubert Foo
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol. , 26 October 2020
Sec. Health Psychology
Volume 11 - 2020 | https://doi.org/10.3389/fpsyg.2020.552416
This article is part of the Research Topic Digital Games and Mental Health View all 16 articles
Background: Subthreshold depression is a common mental disorder in late life. Increasing studies have supported the positive effects of exergames to subthreshold depression. The current study aims to investigate how play mode potentially affects exergames’ effects on subthreshold depression among older adults.
Method: A between-group experiment was carried out to compare the effect of exergames with different play modes. Fifty-two Singaporean older adults with subthreshold depression were randomly assigned into two conditions, and performed either single-player or multiple-player Nintendo Wii Tennis exergames for 6 weeks, while the key variables of depression, social support and loneliness were measured at both pre- and post-study period.
Results: Findings from path analysis suggested that older adults in multiple-player exergames experienced lower levels of loneliness, and further more reduction on subthreshold depression, when compared to those in single-player exergames. Although social support was not affected by play mode, the significant relationship among social support, loneliness, and depression was found in the context of exergaming.
Conclusion: This study not only provides additional insight into a possible causal association lining play mode and health outcomes of exergames, but also opens the discussion of how to optimize antidepressive effect of exergames for older adults.
Subthreshold depression, or minor depression, is generally defined as a cluster of depressive symptoms, in which the number, duration, or quality is insufficient to meet the DSM-IV criteria of major depression (Bali and Jiloha, 2008). Although being below the clinical criteria of major depression, subthreshold depression often has a much higher prevalent rate across all age groups, particularly in aging population (Meeks et al., 2011). Subthreshold depression leads to significant negative outcomes in late life, including poorer physical health and even increased mortality (Montross et al., 2008).
With the advent of interactive digital technology, exergames, which combine the digital gaming and physical exercising (Oh and Yang, 2010), has become a popular alternative to traditional exercise programs and now are increasingly used in healthcare domains (Gil-Gomez et al., 2011). Recent research has examined the positive impacts of exergames on psychosocial well-beings among older adults, including improvements in loneliness and mood (Wollersheim et al., 2010; Kahlbaugh et al., 2011), self-esteem, and positive affect (Jung et al., 2009). In a systematic review, Li et al. (2015) have confirmed that exergames have medium effect on reducing the symptoms of depression among older generations. Increasing studies (Rosenberg et al., 2010; Zhou et al., 2012) have extended the positive effects of exergames to subthreshold depression. Another study from Li et al. (2017) further implied that exergames led to greater reduction on subthreshold depression among older adults, when compared to traditional exercise. However, the lack of depth of study in this area calls for further research that explores the influential factors that may affect their anti-depressive effects.
Several game studies examined the effects of exergames factors on attitudes, performance and physical conditions (O’Donovan et al., 2012; Park et al., 2014). However, to our knowledge, there is no particular study investigating the factors that influence the exergames’ impacts on depression. The current study is a pilot study with the aim to contribute to this new research domain, by investigating how one key factor in exergames – play mode – potentially affects its effect on subthreshold depression among older adults.
Play mode is an important theme in game studies. Play mode is usually categorized in video games history into two types: single-player mode (SP) and multiple-player mode (MP). SP refers to a particular game mode designed to be played by a single player, whereas MP refers to that designed to be played by two or more players simultaneously. Many previous studies investigated the effects of play mode on players’ motivation, performance and in-game experience (Smyth, 2007; Peng and Hsieh, 2012; Chen et al., 2015). Player modes were also supported to affect a player’s psychosocial attributes in real life, such as social support (de Kort and Ijsselsteijn, 2008; Uz and Cagiltay, 2015) and loneliness (Kahlbaugh et al., 2011). Social support and loneliness are common depression predictors supported by previous literature (Nezlek et al., 1994; Ingram et al., 1999; Singh and Misra, 2009). Hence, play mode in exergames may affect depression through the mediation effects of social support and loneliness. The below section provides the theoretical perspective for the assumptions of play mode effect on depression and related psychosocial attributes.
In social gerontology literature, the link between social support and depression is well established. Buffering Hypothesis (Cohen and Wills, 1985) is the most influential theoretical perspective on social support, which hypothesizes that social support reduces the effects of stressful life event on health through either the supportive actions of others or the belief that support is available (Lakey and Cohen, 2000). In other words, the existence of one’s social network, as well as substantive interactions generated among social ties, can buffer people from negative and stressful events. Therefore, social support acts to reduce the chances of stressors and negative events that provoke depression.
A sizable number of aging studies have established the relationship between social support and geriatric depression (Verstraten et al., 2005; Lee et al., 2012; Su et al., 2012). Given that a person’s social network decreases over time in late life (Antonucci, 1991), older adults receive less emotional support from social networking. This could increase the risk of depression. Barg et al. (2006) found that high adequacy of social support that older adults receive corresponds to low depressive scores. In a study with forty elderly aged 60 years and above, Patil et al. (2014) found a significant negative correlation between perceived social support and depression.
Besides the direct effect on geriatric depression, social support would also influence geriatric depression through loneliness. Loneliness refers to the subjective feeling state of being alone, separated, or apart from others (Tomaka et al., 2006). It is one of the strongest predictors of depression according to Singh and Misra (2009). Strong association between loneliness and geriatric depression was further confirmed in a large scale study (Aylaz et al., 2012). The longitudinal study of Cacioppo et al. (2006) supported that loneliness is a significant risk factor for depression among the aging population. Cohen-Mansfield and Parpura-Gill (2007) proposed a framework, Model of Depression and Loneliness, to examine factors influencing loneliness and depressed affect in older population. According to this framework, the reduced social contacts that occurs with age will influence loneliness, which, in turn, will affect depression. The feeling of loneliness is common for elderly people in their late life because of the lack of close family ties (e.g., living alone), impaired social support, and loss of mobility in social activities. The negative effect of social support on loneliness among older adults has found in many studies, especially on the Asian contexts (Kang et al., 2018; Chen et al., 2019). Lonely people suffer from more depressive symptoms, as they have been reported to be less happy, less satisfied, and more pessimistic (Singh and Kiran, 2013). As a result, loneliness may play a mediation role on the relationship between social support and depression among older adults.
In video games, social support is likely to be affected by different play mode. Many researchers have examined the social support derived from video games with multiple players (Trepte et al., 2012; Zhang and Kaufman, 2016a). In contrast with those in single-player games, players in multiple-player games need to learn and apply their social skills to achieve game goals. While interacting with others, players enhance their in-game social networking and interaction in these virtual social communities. This phenomenon is more obvious in games designed specifically for engaging cooperation and mutual assistance (Ewoldsen et al., 2012). In these collaborative games, players in a team assist each other and share successes and failures together. These social interactions strengthen group cohesion and interdependent bonds among teammates (Isbister, 2010; Banks, 2012), and foster strong feelings of virtual support and new friendships (Smyth, 2007). These virtual support and relationships in multiple-players gaming may affect and extend players’ pre-existing relationships in real life (Williams, 2006). Gentile and Gentile (2008) argued that social skills learned and practiced in the gaming environment could be generalized into the real context, which may promote prosocial behavior and enhance social support in daily life. Trepte et al. (2012) has presented a large-scale study to examine the theoretical framework of how social interactions in online multiple-player gaming affected offline social support. In their study, players’ social proximity and mutual familiarity during online interactions were supported to foster both online bridging social capital (people feel informed and inspired by each other) and bonding social capital (emotional support and understanding), while both social capital dimensions are positively related to offline social support.
The theoretical framework of gaming and social support provided above can be applied into the context of exergaming and older adults. It is reasonable to posit that exergames in multiple-player mode lead to higher level of social support than those in single-player mode, and the higher level of social support further results in greater reduction of depression among older adults.
Similar to social support, play mode in video games may affect loneliness through social interaction and communication among players. Li and Counts (2007) argued that MP games could actually increase communication between teammates via digital and traditional channels. Further, such game mode could create feelings of co-presence and make players feel more connected to each other (Lazzaro, 2004). The co-presence and connection to others could therefore reduce loneliness. A systematic review from Li et al. (2018) identified that playing MP exergames could improve older adults’ social well-being, through increasing social bonding with their peers and grandchildren. In the study from Kahlbaugh et al. (2011), older residents received personal visits from students who played a bowling game on Nintendo Wii console with them for 10 weeks. Results showed that older residents felt less lonely than they had at the start of the study. The decrease in loneliness was perhaps not due to playing the Wii itself, but by the interactions between older participants and students. In a large sample survey study, Lee and Ishii-Kuntz (1987) indicated that doing something together with other people reduced loneliness among older adults.
As a result, compared to SP exergames, the social interactions and communication in MP exergames lead to lower level of loneliness, and thus results in greater reduction of depression among older adults.
This study sought to build a conceptual model to address the influencing mechanism between exergame play mode and depression in old age. The model is rooted in cognitive-behavioral theories and conceptualizes depression as resulting from an interaction of social events and cognitive processes. It utilizes two key concepts, social support and loneliness, to clarify how play mode can facilitate the depression treatment in the exergaming context. Figure 1 shows the proposed conceptual model in this study. Based on the model, five hypotheses were proposed in the specific context of exergames and subthreshold depression in late life:
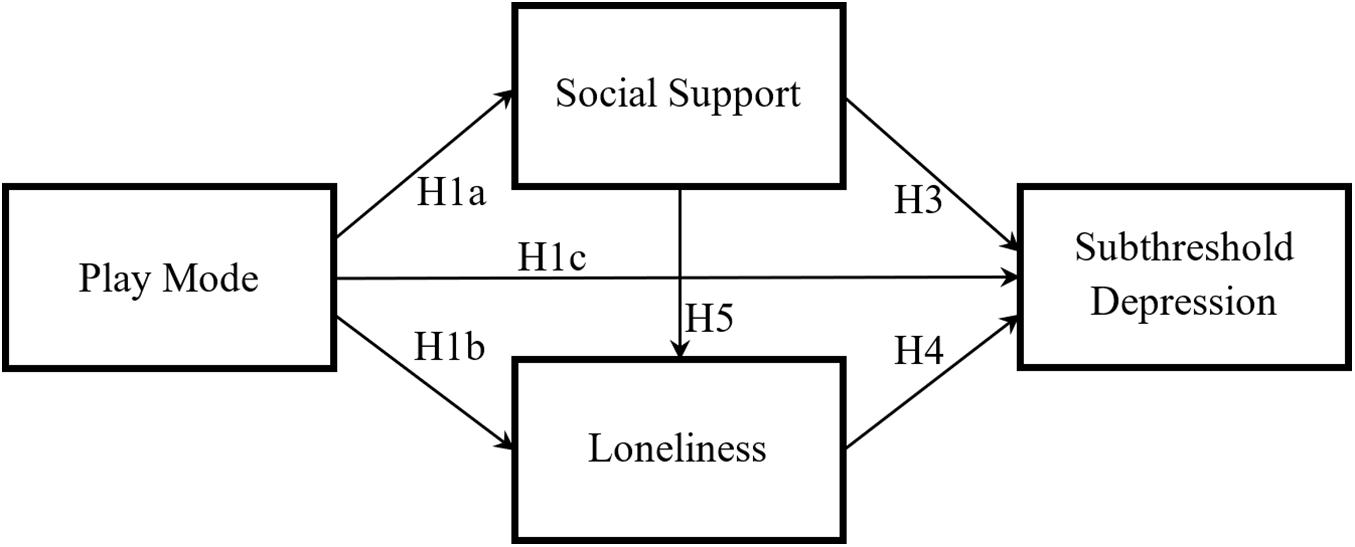
Figure 1. Proposed conceptual model.
H1: Compared to SP exergames, MP exergames lead to (a) a higher level of social support; (b) a lower level of loneliness; and (c) a lower level of subthreshold depression among older adults.
H3: Social support is negatively associated with subthreshold depression among older adults.
H4: Loneliness is positively associated with subthreshold depression among older adults.
H5: Social support is negatively associated with loneliness among older adults.
H6: Both (a) Social support and (b) loneliness mediate the effect of play mode on subthreshold depression among older adults.
Participants were recruited from two senior activity centers located in the western and northern parts of Singapore, respectively. The center managers assisted in delivering recruitment message and approached potential participants. Generally, older adults were included in the study if they were aged 55 and above, and diagnosed with subthreshold depression in the screening section. Patient Health Questionnaire – 9 (PHQ-9; Spitzer et al., 1994) was used as a screening tool for admission into the study. Followed the scale instructions from Kroenke and Spitzer (2002), the total PHQ-9 score below “4” indicated none depression, whereas “5” to “14” indicates mild to moderate depression, and “15” to “27” indicates moderately severe to severe depression. Therefore, only participants who scored 5–14 in PHQ-9 were included in the final pool. Given that the particular interventions, participants were asked to self-report their previous experience on exergaming system. Only those with no experience or little experience (less than a few hours performance) were included in the study. Further, through self-reporting and information obtained from center managers, participants were excluded if they had the following conditions which prevent them from performing the exergame correctly and safely: (a) have serious cognitive disorders (e.g., Parkinson disease or Alzheimer’s disease), (b) intellectual disability and physical limitations (severe mobile, visual, or hearing problems), (c) other depressive disorders (e.g., bipolar, dysthymic, schizophrenia), or (d) have received antidepressant medications (or other forms of depression therapies) within the last 3 months.
Based on a systematic review of Li et al. (2015) which examined the overall effect size of exergames on depression, a general effect size of 0.25 was used in the current study to determine the sample size. Through the G∗Power software with a priori analysis method, a sample of 54 participants is required in order to achieve the according general effect size with a power of 0.9 (α = 0.05). What’s more, the results of this systematic review shown that majority of previous studies used a small sample size of less than 50 participants. As a result, the current study targeted on 60 participants (30 per condition) which is slightly higher than recommended number.
In randomization process, each involved participant was labeled with a unique ID after screening, and an online tool1 was used to generate two experimental conditions with random participant IDs. In order to avoid the interaction, these two experimental conditions in the same center were conducted in different time slots.
The ethical approval of this study was obtained from the Institutional Review Board at the university where the research team was originally from (IRB-2014-07-039). Participation in this pilot study was voluntary, and informed consent was obtained for all participants before the study. Each participant was awarded SGD$15 equivalent of shopping voucher after having completed all sessions.
To manipulate play mode, two different exergame conditions – SP and MP – were involved in the study. Nintendo Wii Tennis was chosen as the exergame for both conditions because of two reasons. First, according to previous literatures (Gao and Mandryk, 2011; Theng et al., 2012), older adults were recommended to perform physical activities with simple and single movements because of their impaired physical and cognitive conditions. The Wii Tennis game fulfils these safety criteria and has already been used as exercise intervention for older adults in previous studies (Rosenberg et al., 2010; Maillot et al., 2012). Second, the tennis game contains both SP and MP modes, which could ensure equal comparison between two conditions.
In SP condition, participants were asked to perform the exergames individually and played against a virtual player. Due to practical considerations on schedule and arrangement, participants came with a group of 15 people in one session and took turns to play the exergames. Despite the group setting, each participant was instructed to play on their own and without any physical assistance from others during the gaming. The total time for a group was around 3 h in one session. In the MP condition, two participants formed a team and cooperated in the same game to play against two virtual players. Similar to SP condition, all participants in came with a group of 14 people (seven pairs of participants) and performed the exergames in one session. To balance the performance time with the SP condition, the total time for MP condition was around 1.5 h for each session. The MP mode in the study applied collaborative games but not competitive ones. Compared to collaborative mode with the shared objective, competitive mode with the personal objective may elicit anxiety and fear of failure (Wu et al., 2015). These emotions elicited in competitive games may have negative effects on depression.
Participants from both conditions performed the corresponding exergame interventions once a week for 6 consecutive weeks. During the intervention period, one or two student assistants coordinated each exergame session. They assisted in setting up the exergame and solved the technical problems occurred during the game playing.
Participants were asked to fill in two self-reported surveys at both pre-study (before the first exergame section) and post-study period (after the last exergame section). The basic demographic information of participants was collected in pre-study survey, including their age, gender, education level, living conditions, and physical health conditions. The three key variables, including subthreshold depression, social support, loneliness, were collected at both pre-study and post-study period. Trained student assistants from the research team assisted participants who had literacy and visual problems in filling the questionnaires. Both English and Chinese versions of questionnaire were used in the study. Most of the measurements were adopted from existing sources to ensure the validity. Participants selected the language version that matched their preference.
The PHQ-9 (Spitzer et al., 1994) is a self-administrated depression scale under the Primary Care Evaluation of Mental Disorders (PRIME-MD), which is a widely used diagnostic screening instrument in primary care. In addition to recognizing major depression, PHQ-9 is also a useful tool for detecting subthreshold depression in the general population (Martin et al., 2006). The validity and reliability as diagnostic and assessing measurements are well-established in previous studies (Kroenke et al., 2001; Löwe et al., 2004). The tool uses a four-point Likert scale (from 0 “Not at all” to 3 “Nearly every day”) to measure items such as “Little interest or pleasure in doing things” or “Feeling down, depressed or hopeless.” The total score ranges from 0 to 27, with a higher score indicating higher severity of depression. The Chinese version of PHQ-9 was adopted directly from the PHQ website2 organized by Pfizer Inc. The Cronbach’s α of PHQ in pre- and post-study are 0.57 and 0.70, respectively.
Social support was measured by the perceived social support subscale from Berlin Social-Support Scales (BSSS; Schulz and Schwarzer, 2003). Good reliability of BSSS was also found among elderly population (Patil et al., 2014). The BSSS subscale comprises eight items assessing emotional and instrumental aspects of social support. Participants indicate their agreement with the statements like “I know some people upon whom I can always rely” on a four-point Likert scale, from 1 “Very strongly disagree” to 7 “Very strongly agree.” The total score ranges from 8 to 56, and a higher add-up score indicates higher level of perceived social support. The Chinese version of BSSS was developed through back translations conducted by three Chinese doctoral students majored in communication studies. The Cronbach’s α of BSSS in pre- and post-study are 0.87 and 0.82, respectively.
The University of California Los Angeles (UCLA) Loneliness Scale (Russell, 1996) is commonly used for measuring loneliness of respondents including older adults. The present study applied a short form (8 items) of UCLA Loneliness Scale (ULS-8; Hays and DiMatteo, 1987). ULS-8 consists of eight items selected according to the results of an exploratory factor analysis. The scale has high internal consistency and high correlation with the original scale and other related measures (Hays and DiMatteo, 1987). The ULS-8 was revised to suit the elderly participants in current study. The scale employs a four-point Likert scale with values ranging from 1 “Never” to 4 “Always.” The total score of ULS-8 ranges from 8 to 32. No cut-off score was identified to define loneliness, but a higher score on this scale indicates a more intense feeling of loneliness. The Chinese version of the ULS-8 used in the study was developed from previous works (Chou et al., 2005; Zhou et al., 2012). The Cronbach’s α of ULS-8 in pre- and post-study are 0.64 and 0.73, respectively.
Descriptive statistics of key variables were first conducted for both pre- and post-study data, following by a series of mixed analysis of variance (mixed ANOVA) to examine the interaction effects between time (pre-study vs. post-study) and play mode (SP game vs. MP game). Time was input as a within-group variable while play mode as a between-group variable. Both the descriptive statistics and mixed ANOVA tests were performed in IBM SPSS version 23.
Path analysis was then applied to test the conceptual model proposed between play mode and subthreshold depression. Path analysis is one of the most common techniques used in structural equation modeling (SEM). SEM is a family of statistical methods with a special aim to develop and test theoretical models. SEM evaluates the relationships between observed and latent variables (Hoyle, 1995). In path analysis, goodness-of-fit is first evaluated, followed by the estimation of path coefficients. Path coefficients, also known as standardized regression coefficients, determine the effects of exogenous (predictor) variables on endogenous (predicted) variables.
Different from common SEM in cross-sectional designs, the conceptual model in the current study involved a categorical exogenous variable (play mode). Bollen (1989) clarified that the inclusion of categorical exogenous variables did not violate the assumption of multivariate normality underlying the commonly used maximum likelihood method of estimation. MacCallum and Austin (2000) further indicated that one can use SEM to model the relationships of experimentally manipulated independent variables (such as dummy variables), to other variables, including covariates, mediators, and outcomes. All path analyses were conducted in Mplus version 6.0 (Muthén and Muthén, 1998).
Fifty-eight participants met the inclusive criteria and were involved in actual study. During the 6-week intervention period, six participants were reported to be absent in more than two sessions, due to the reasons including loss of interest (two participants), conflict schedule (three participants), or poor health condition (one participant). They were considered as drop-out and did not included in the final analysis. Figure 2 illustrates the flow chart of the participants in the study.
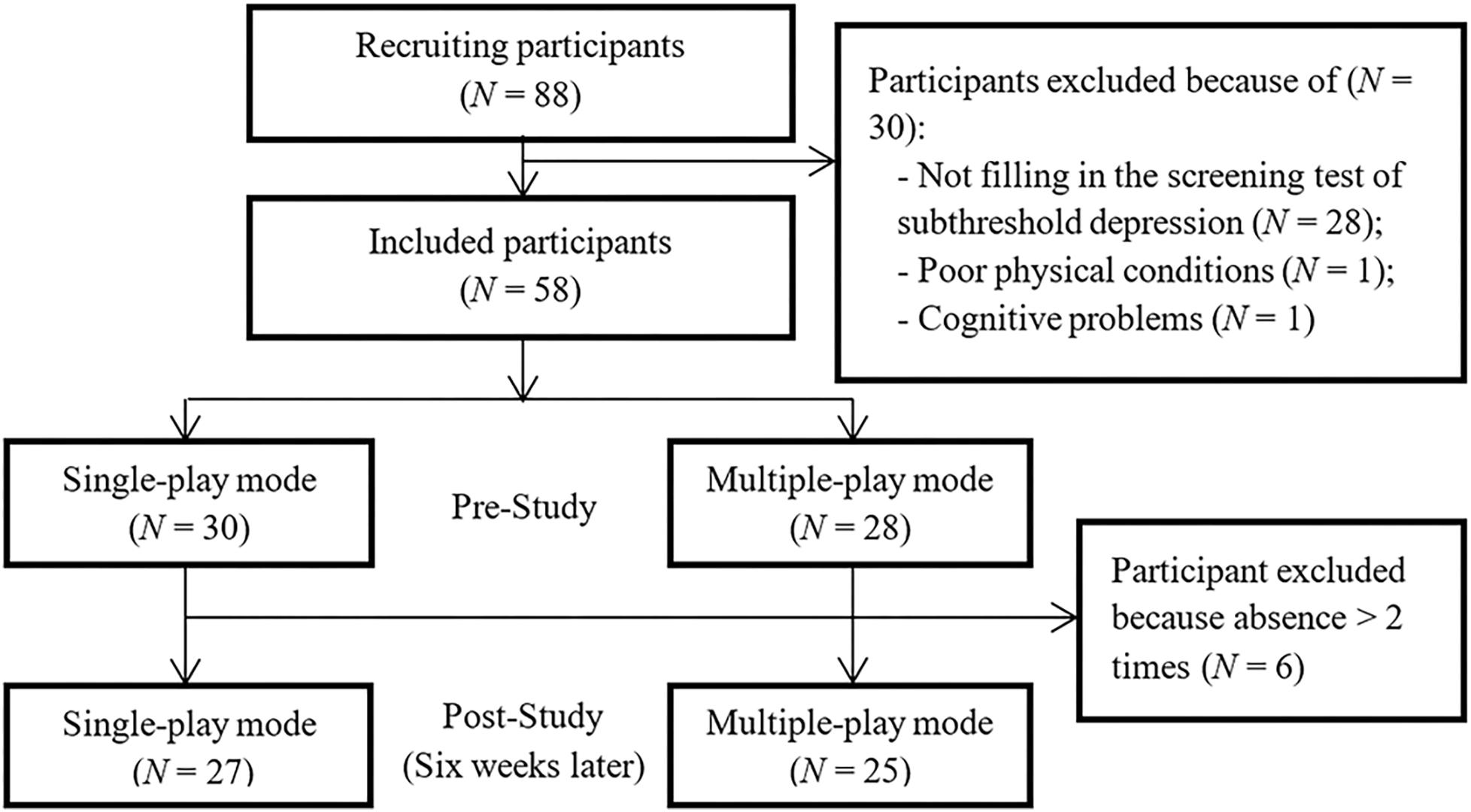
Figure 2. Flow chart of the participants.
A total of 52 participants completed both pre- and post-study surveys. The mean age of included participants was 72.12 (SD = 8.65), and 39 (75%) of them were female participants. Descriptive analysis was conducted across the two conditions on demographic characteristics and key psychosocial variables at pre-study period. Table 1 illustrates the detailed results. Findings from t-test and Chi-square tests indicated that participants from the two conditions did not have significant differences in demographic characteristics, as well as physical and cognitive status. Furthermore, no significant group difference emerged during the pre-study period in depression [t(50) = 0.56, p = 0.582], social support [t(50) = 1.24, p = 0.221], and loneliness [t(50) = 1.62, p = 0.111]. As a result, participants in SP and MP can be considered as equal in demographic, physical, and psychosocial conditions. Table 2 indicates key psychological outcomes across two conditions at both pre-study and post-study period. Findings indicates significant bivariate correlations among subthreshold depression, social support and loneliness after the intervention period.
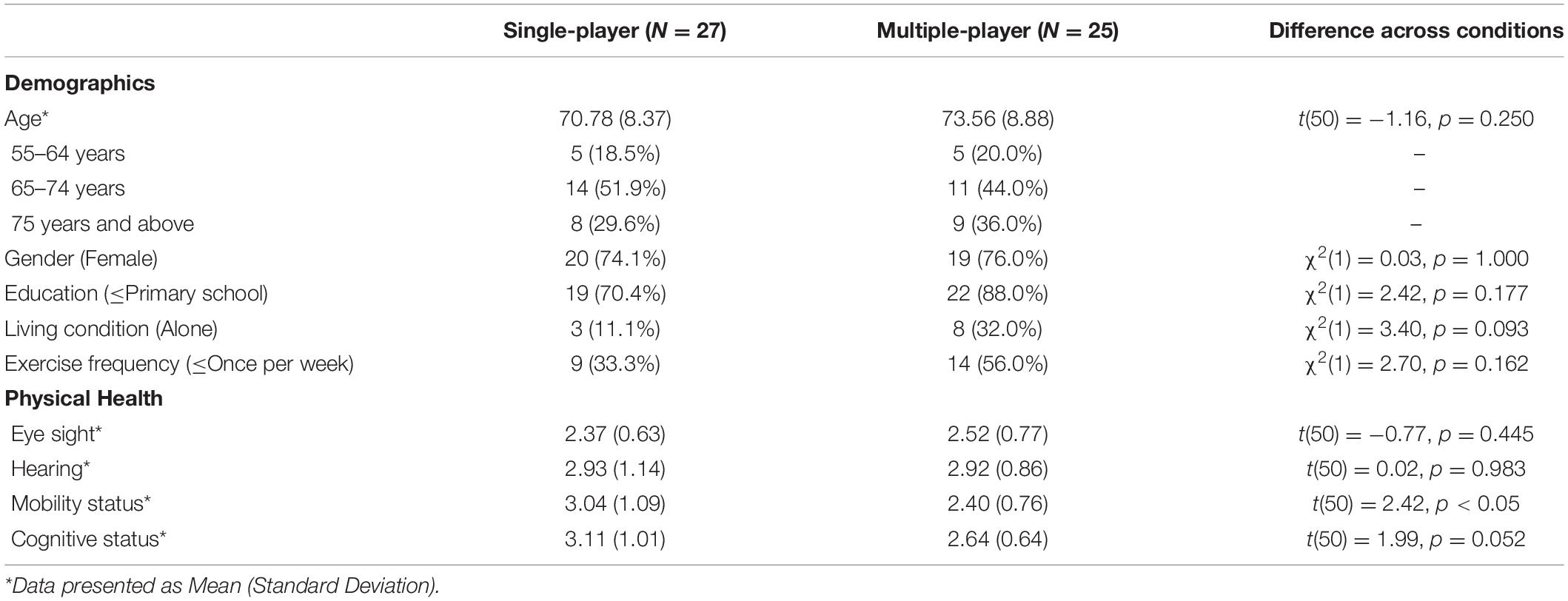
Table 1. Descriptive analysis across two conditions in study two (N = 52).
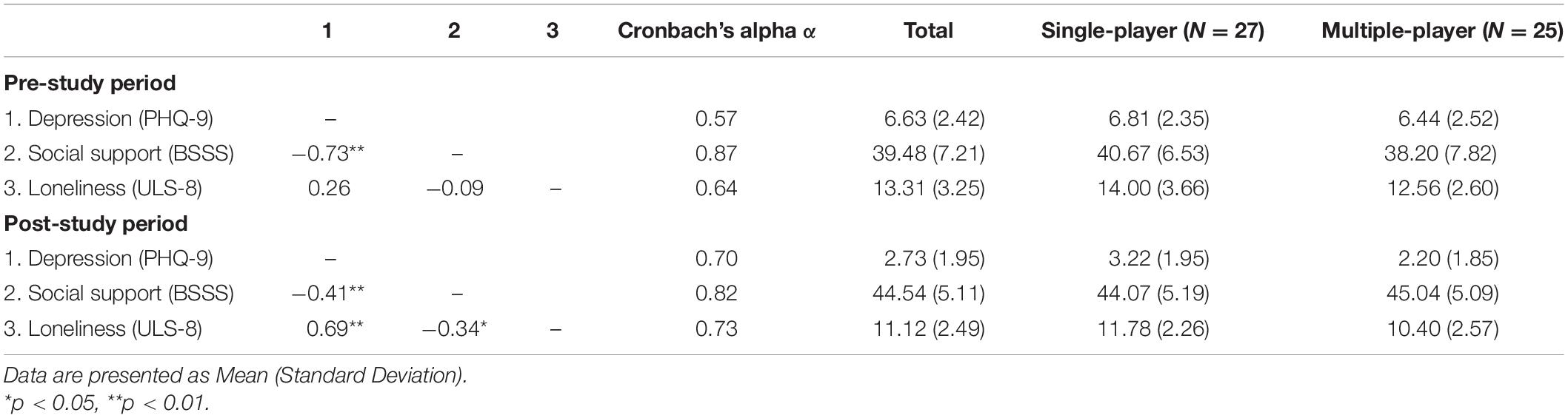
Table 2. Description of depression, social support, and loneliness (N = 52).
The results of the mixed ANOVA did not show any significant interaction effects between time and play mode on social support [F(1,50) = 2.710, p = 0.106, η2 = 0.051], loneliness [F(1,50) = 0.005, p = 0.944, η2 = 0.00], or subthreshold depression [F(1,50) = 0.802, p = 0.375, η2 = 0.016]. Figure 3 demonstrated the plots of the interaction effect among the three psychological variables. Despite the MP condition seemed to release more increase in social support and more reduction in subthreshold depression over the 6 weeks when compared to SP condition (Inspected from the descriptive statistics in Table 2), these changes were not statistically significant.
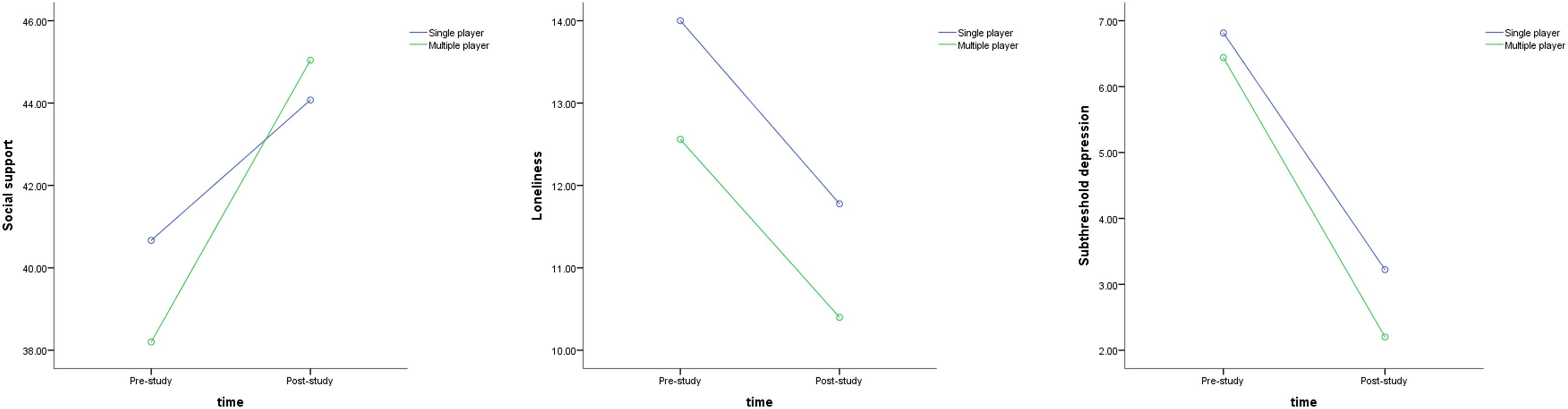
Figure 3. Interaction effects from ANOVA results.
Nevertheless, there were strong significant main effects of time on all the three key psychosocial attributes, including social support [F(1,50) = 24.152, p < 0.001, η2 = 0.326], loneliness [F(1,50) = 25.027, p < 0.001, η2 = 0.334], and subthreshold depression [F(1,50) = 117.431, p < 0.001, η2 = 0.701]. The findings indicated that the older adults had improvements on social support, loneliness, and subthreshold depression after the 6-week exergames playing. As a result, the strong effects of exergames were supported as a psychosocial intervention for older adults with subthreshold depression.
In path analysis, goodness-of-fit was first assessed through multiple fit statistics, including Chi-square test, Comparative Fit Index (CFI), Root Mean Square Error of Approximation (RMSEA), and Standardized Root Mean Square Residual (SRMR). Chi-square test (χ2) is the most basic fit statistic that compares predicted covariance matrix with observed matrix (Bentler, 2004). To reduce the effects of sample size, normed Chi-square (χ2/df) was calculated. A value of normed Chi-square smaller than 3 indicated an acceptable fit. CFI assesses the relative improvement in fit of the researcher’s model compared with a baseline model (Hu and Bentler, 1990). Values greater than roughly 0.90 may indicate reasonably good fit of the proposed model. RMSEA measures error of approximation (Steiger and Lind, 1980) with a value less or equal to 0.05 considered as good fit and 0.05–0.08 considered as fair fit. SRMR is a measure of the mean absolute value of the covariance residuals. A recommended cut-off point for SRMR is smaller than 0.08 (Hu and Bentler, 1990).
Based on the above criteria, the proposal model resulted in a good fit to data. Table 3 shows the goodness-of-fit indices and model fit results. Estimations of path coefficient and hypotheses testing were conducted after determining the final model. Figure 4 shows the results of the path analysis in the final model. During the hypotheses testing, significant negative effects of exergame play mode were observed on loneliness among older adults (β = −0.25, SE = 0.12, p = 0.042), thereby supporting H1b. However, H1a was not supported with no significant play mode effects on social support (β = 0.10, SE = 0.14, p = 0.488). Consequently, compared to SP exergames, MP exergames led to more reduction in loneliness among older adults, but not in social support. A strong and significant predictive effect from loneliness was also observed on subthreshold depression among older adults (β = 0.59, SE = 0.09, p < 0.001). Meanwhile, subthreshold depression was also significantly affected by social support, with β = −0.20, SE = 0.10, p = 0.047. Thus, both H3 and H4 were supported. However, the direct effect of exergame play mode was not significant on subthreshold depression among older adults (β = −0.08, SE = 0.10, p = 0.434), thereby not supporting H1c. Lastly, H5 was supported by a significant path from social support to loneliness (β = −0.32, SE = 0.12, p = 0.008), which highlights the potential effect of social support on loneliness during exergame playing.
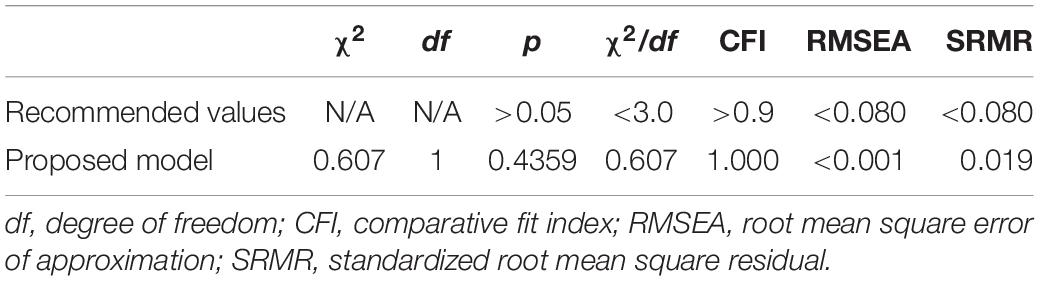
Table 3. Goodness-of-fit indices and model fits.
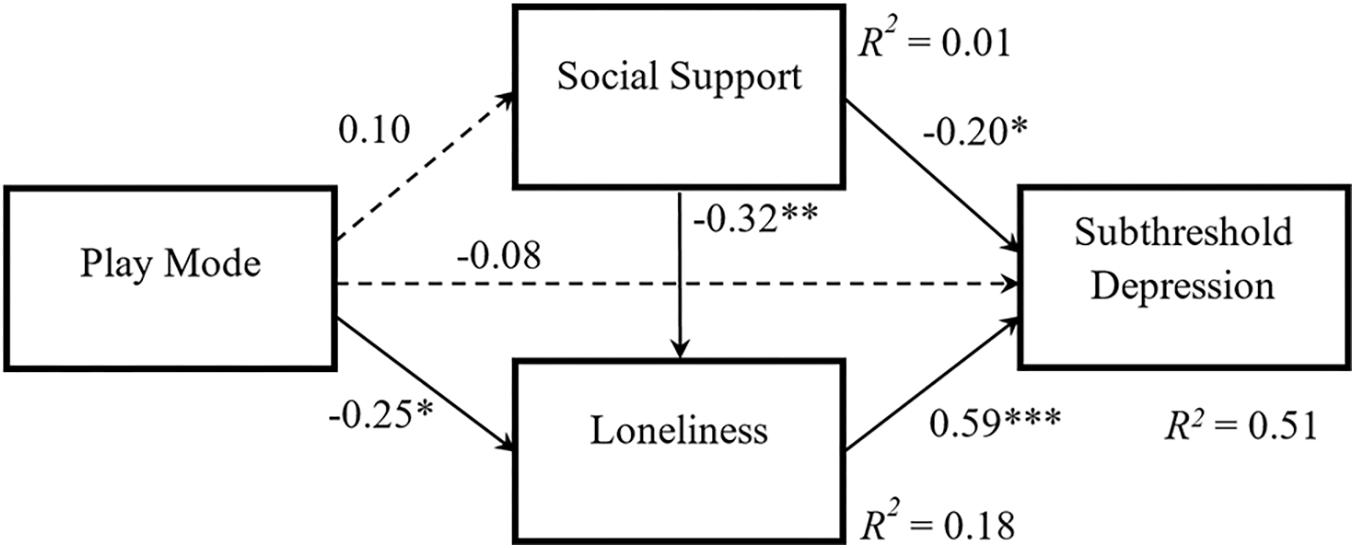
Figure 4. Results of path analysis in the final model. Path coefficients are standardized. The solid line indicates a significant path with ∗p < 0.05, ∗∗p < 0.01, ∗∗∗p < 0.001. The dashed line indicates non-significant path with p > 0.05.
Following the guideline by Stride et al. (2015), the mediation tests were further conducted on Mplus with Andrew Hayes’ PROCESS analysis. The mediation results indicated that play mode in exergames has a (approaching) significant indirect effect on subthreshold depression via medication of loneliness, with β = −0.15, SE = 0.08, p = 0.055. But the mediation role of social support was not supported in the relationship between play mode and subthreshold depression, with a non-significant indirect effect of β = −0.02, SE = 0.03, p = 0.511. Consequently, the results from the model examination supported H6b but not H6a.
A significant large R2 of 0.51 (p < 0.001) in subthreshold depression was reported during the post-study period. This result demonstrated that 51% of the unique variance of subthreshold depression was explained by independent and mediating variables mentioned above. Generally, the findings from path analysis support the final model in which four out of the six path coefficients are statistically significant. To sum up, compared to SP exergames, MP exergames reduced subthreshold depression via the effect on loneliness. Although social support was not supported to be a significant mediator of play mode, it independently affected loneliness and subthreshold depression among older adults.
The pilot study extended the discussion of play mode from in-game experience to mental health improvements. The study also introduced this important theme into the new domain of exergames for health. First of all, the significant improvements on depression and its related attributes between pre- and post-study period have supported the overall effectiveness of exergames as an emerging depression intervention for older adults. These findings were consistent with previous exergame studies (Rosenberg et al., 2010; Chao et al., 2015). It was well established that the physical activity triggers the release of certain body chemicals (such as β-endorphins or dopamine), which consequently result in the improvement of mood and feeling of well-being (Delgado and Moreno, 2000; Brosse et al., 2002).
More importantly, the study investigated the possible effect of play mode (SP vs. MP) on subthreshold depression among older adults through a between-group controlled study. The research serves as a pioneer study to examine the factors that mediate anti-depressive effects of play mode in exergames. Overall, the proposed mediation model in the study was generally supported by the path analysis. Good model fit and high R2 of dependent variable further confirmed the robustness of the final model. In this model, play mode was revealed to have indirect effects on subthreshold depression among older adults, which was mediated by loneliness. Accordingly, older adults who performed MP exergames experienced lower levels of loneliness, and further have more improvement on subthreshold depression, when compared to participants who performed SP exergames. The results support the hypotheses on play mode and psychosocial well-beings (H2 and H4), which are developed from previous studies (Lazzaro, 2004; Singh and Misra, 2009; Zhang and Kaufman, 2016b). The significant mediation link found in the study has further deepened the research domain of exergames and literature concerning psychosocial benefits. Several previous studies have indicated that exergames led to less loneliness and depression (Rosenberg et al., 2010; Kahlbaugh et al., 2011). The current study extended the findings by emphasizing the possible influencing role of play mode, that is, MP exergames have better effects over SP ones on alleviating loneliness and subthreshold depression.
By allowing different players to interact in a team, MP exergames could foster both virtual and real social interactions among players, thereby reducing the risk of social isolation and loneliness (Mueller et al., 2003; Staiano and Calvert, 2011). In a narrative review, Brox et al. (2011) further highlighted the importance of using MP exergames among older adults. They believed that MP exergames increased social interaction between older adults, reduced their social isolation and prevented loneliness and subthreshold depression. The current study provided important evidence to support the assumption from previous research, and confirmed the strong effects of play mode on loneliness and subthreshold depression among older adults.
However, the mediating role of social support was not supported in the study, which differed from the given expectation. Although MP exergames were assumed to increase social interaction among players (Mueller et al., 2003; Staiano and Calvert, 2011), in this study they did not lead to higher social support than SP exergames. Social support generally consists of two major categories, namely emotional and instrumental support (Wills, 1985; Langford et al., 1997). In the context of exergaming, MP simply cannot provide better instrumental support (e.g., tangible support or real assistance in daily life) over the SP. The increased social bonding and communication in MP exergaming context may not guarantee the rise in emotional support in real life within only 6 weeks. The group setting in SP may be another possible explanation of the non-significant finding.
Although the initial model did not reflect the dependency of social support and loneliness, the final model supports the effects of social support on loneliness and subthreshold depression in exergames. It shows that social support not only has a direct anti-depressive effect, but also has an indirect effect via loneliness. While the significant relationship among social support, loneliness, and depression has been examined for long time in the general context (Chi and Chou, 2001; Singh and Misra, 2009), many recent studies are exploring this relationship in the adoption of new technologies (He et al., 2014; Chopik, 2016). For example, a cross-sectional study from He et al. (2014) indicated that social support was negatively associated with depression of Internet addicts whereas loneliness plays a mediating role. In consistent with these studies, the current study extends the significant relationship to the context of exergaming. Meanwhile, despite social support not being affected by play mode, its variances, which were probably affected by other external factors, assumed a significant role in the effects of play mode on subthreshold depression. These findings imply that social support may act as a moderator in the relationship between play mode and subthreshold depression. Future studies are needed to examine this assumption.
The current study does incur some limitations. Firstly, the small sample size and short intervention time may affect the generalizability of the key results, which was mainly caused by the difficulties in recruiting and managing older participants. Although no strict and clear criteria are required in the sample size of SEM studies, many researchers in the field recommend using more than 200 subjects (Kline, 2011; Tabachnick and Fidell, 2013). The findings of path analysis in this pilot study should be interpreted with caution. Secondly, the proposed model only involved two possible mediators. Future research may include more variables and draw a more complete picture on the influencing mechanism of play mode effect on subthreshold depression among older adults in exergaming. Thirdly, only Wii Tennis was used in two conditions, due to the lack of available exergames in the current market. The key conclusions should be further examined with the use of other suitable exergames in the future. Fourthly, the PHQ-9 scale has a low internal consistency at the baseline. This problem might be caused by the screening process where we only recruited participants with a limited range of PHQ-9. Therefore, the conclusions of ANOVA should be further confirmed in future studies. Lastly, it would be more worthwhile to test the interaction effect between play mode and other exergame factors in future studies, such as comparing SP and MP in both non-exercise games and exergames.
To conclude, the study compared the effects of SP and MP exergames, and supported that play mode was important in affecting the anti-depressive effects of exergames. The model examination presents a novel understanding of the mechanism inside this influencing process. Specifically, multiple-player exergames promoted better improvements on subthreshold depression and loneliness among older adults, when compared to single-player exergames. The study highlights several practical and theoretical implications applicable for both game design and mental health research. For serious game design, evidence from current research emphasizes the importance of designing multiple-player exergames for older adults with a healthcare purpose. Schutter and Abeele (2008) conducted a participatory design study and their findings suggested that older adults preferred multiple-player games when they were involved in the design process of digital games. Therefore, to maximize the psychosocial effects, exergames should be designed with a preference of multiple-player mode for older players, and involve more elements to increase social interactions and support. For mental health research, the findings also contribute to exiting literature by providing additional insight into a possible causal association lining play mode and subthreshold depression in exergames. Most of the previous studies examined the effects of play mode in the behaviors and perceptions, such as motivation, gaming performance, and experience (Smyth, 2007; Peng and Hsieh, 2012; Chen et al., 2015). The current study extended and tested its possible link to mental health improvements. It further inspires the theoretical discussion of play mode effect under a broader domain of exergames for mental health, such as anxiety and dementia. Following the discussion of multiple-player mode in exergames, it may also be interesting for the future study to explore who to play with, especially on the psychosocial effects of inter-generational exergames.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Institutional Review Board (IRB) of Nanyang Technological University, Singapore (IRB-2014-07-039). The patients/participants provided their written informed consent to participate in this study.
JL: conceptualization, methodology, investigation, formal analysis, and writing. YT: conceptualization, supervision, project administration, resources, and reviewing and editing. SF: supervision, reviewing and editing, and funding acquisition. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Antonucci, T. C. (1991). “Attachment, social support, and coping with negative life events in mature adulthood,” in Life Span Developmental Psychology: Perspectives on Stress and Coping, eds E. M. Cummings, A. L. Greene, and K. Karraker (Hillside, NJ: Erlbaum), 261–276.
Aylaz, R., Aktürk, Ü, Erci, B., Öztürk, H., and Aslan, H. (2012). Relationship between depression and loneliness in elderly and examination of influential factors. Arch. Gerontol. Geriatr. 55, 548–554. doi: 10.1016/j.archger.2012.03.006
Bali, S., and Jiloha, R. C. (2008). Subsyndromal depression - A review. Delhi Psychiatry J. 11, 43–47.
Banks, M. (2012). Collocated Multiplayer Games and Social Interaction. London: University College London.
Barg, F. K., Huss- Ashmore, R., Wittink, M. N., Murray, G. F., Bogner, H. R., and Gallo, J. J. (2006). A mixed methods approach to understand depression in older adult. J. Gerontol. Ser. B 61, S329–S339.
Brosse, A. L., Sheets, E. S., Lett, H. S., and Blumenthal, J. A. (2002). Exercise and the treatment of clinical depression in adults: recent findings and future directions. Sports Med. 32, 741–760. doi: 10.2165/00007256-200232120-00001
Brox, E., Luque, L. F., Evertsen, G. J., and Hernández, J. E. G. (2011). “Exergames for elderly: Social exergames to persuade seniors to increase physical activity,” in Proceedings of the 5th International Conference on Pervasive Computing Technologies for Healthcare (PervasiveHealth), Dublin.
Cacioppo, T. J., Hughes, M. E., Waite, L. J., Hawkey, L. C., and Thisted, R. A. (2006). Loneliness as a specific factor of depressive symptoms: cross sectional and longitudinal study. Psychol. Aging 21, 141–151.
Chao, Y.-Y., Scherer, Y. K., Montgomery, C. A., Wu, Y.-W., and Lucke, K. T. (2015). Physical and psychosocial effects of Wii Fit exergames use in assisted living residents: a pilot study. Clin. Nurs. Res. 24, 589–603. doi: 10.1177/1054773814562880
Chen, C.-H., Wang, K.-C., and Lin, Y.-H. (2015). The comparison of solitary and collaborative modes of game-based learning on students’ science learning and motivation. Educ. Technol. Soc. 18, 237–248.
Chen, L., Alston, M., and Guo, W. (2019). The influence of social support on loneliness and depression among older elderly people in China: coping styles as mediators. J. Commun. Psychol. 47, 1235–1245. doi: 10.1002/jcop.22185
Chi, I., and Chou, K. (2001). Social support and depression among elderly Chinese people in Hong Kong. Int. J. Aging Hum. Dev. 52, 231–252. doi: 10.2190/v5k8-cnmg-g2up-37qv
Chopik, W. J. (2016). The benefits of social technology use among older adults are mediated by reduced loneliness. Cyberpsychol. Behav. Soc. Netw. 19, 551–556. doi: 10.1089/cyber.2016.0151
Chou, K.-L., Jun, L. W., and Chi, I. (2005). Assessing Chinese older adults’ suicidal ideation: chinese version of the Geriatric Suicide Ideation Scale. Aging Ment. Health 9, 167–171. doi: 10.1080/13607860412331336805
Cohen, S., and Wills, T. A. (1985). Stress, social support, and the buffering hypothesis. Psychol. Bull. 98, 310–357. doi: 10.1037/0033-2909.98.2.310
Cohen-Mansfield, J., and Parpura-Gill, A. (2007). Loneliness in older persons: a theoretical model and empirical findings. Int. Psychogeriatr. 19, 279–294. doi: 10.1017/s1041610206004200
de Kort, Y. A. W., and Ijsselsteijn, W. A. (2008). People, places, and play: player experience in a socio-spatial context. ACM Comp. Entertain. 6, 1–11. doi: 10.1145/1371216.1371221
Delgado, P. L., and Moreno, F. A. (2000). Role of norepinephrine in depression. J. Clin. Psychiatry 61, 5–12.
Ewoldsen, D. R., Eno, C. A., Okdie, B. M., Velez, J. A., Guadagno, R. E., and DeCoster, J. (2012). Effect of playing violent video games cooperatively or competitively on subsequent cooperative behavior. Cyberpsychol. Behav. Soc. Netw. 15, 277–280. doi: 10.1089/cyber.2011.0308
Gao, Y., and Mandryk, R. L. (2011). “GrabApple: The design of a casual exergame,” in Proceedings of the 10th International Conference on Entertainment Computing, Vancouver.
Gentile, D. A., and Gentile, J. R. (2008). Violent video games as exemplary teachers: a conceptual analysis. J. Youth Adoles. 9, 127–141. doi: 10.1007/s10964-007-9206-2
Gil-Gomez, J. A., Llorens, R., Alcaniz, M., and Colomer, C. (2011). Effectiveness of a Wii balance board-based system (eBaViR) for balance rehabilitation: a pilot randomized clinical trial in patients with acquired brain injury. J. Neuroeng. Rehabil. 8:30. doi: 10.1186/1743-0003-8-30
Hays, R. D., and DiMatteo, M. R. (1987). A short-form measure of loneliness. J. Pers. Assess. 51, 69–81. doi: 10.1207/s15327752jpa5101_6
He, F., Zhou, Q., Li, J., Cao, R., and Guan, H. (2014). Effect of social support on depression of internet addicts and the mediating role of loneliness. Int. J. Ment. Health Syst. 8:34.
Hoyle, R. H. (1995). “The structural equation modeling approach: Basic concepts and fundamental issues,” in Structural Equation Modeling: Concepts, Issues, and Applications, ed. R. H. Hoyle (Thousand Oaks, CA: Sage Publications Inc), 1–15.
Hu, L., and Bentler, P. M. (1990). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equat. Model. 6, 1–55. doi: 10.1080/10705519909540118
Ingram, K. M., Jones, D. A., Fass, R. J., Neidig, J. L., and Song, Y. S. (1999). Social support and unsupportive social interactions: their association with depression among people living with HIV. AIDS Care 11, 313–329. doi: 10.1080/09540129947947
Isbister, K. (2010). “Enabling Social Play: A Framework for Design and Evaluation,” in Evaluating User Experience in Games, ed. R. Bernhaupt (London: Springer), 11–22. doi: 10.1007/978-1-84882-963-3_2
Jung, Y., Li, K. J., Janissa, N. S., Gladys, W. L. C., and Lee, K. M. (2009). “Games for a better life: effects of playing Wii games on the well-being of seniors in a long-term care facility,” in Proceedings of the Sixth Australasian Conference on Interactive Entertainment, Sydney.
Kahlbaugh, P., Sperandio, A., Carlson, A., and Hauselt, J. (2011). Effects of playing Wii on well-being in the elderly: physical activity, loneliness, and mood. Activ., Adapt. Aging 35, 331–344. doi: 10.1080/01924788.2011.625218
Kang, H.-W., Park, M., and Wallace, J. P. (2018). The impact of perceived social support, loneliness, and physical activity on quality of life in South Korean older adults. J. Sport Health Sci. 7, 237–244. doi: 10.1016/j.jshs.2016.05.003
Kline, R. B. (2011). Principles and Practice of Structural Equation Modeling, 3rd Edn. New York, NY: Guilford Press.
Kroenke, K., and Spitzer, R. L. (2002). The PHQ-9: a new depression diagnostic and severity measure. Psychiatr. Ann. 32, 509–521. doi: 10.3928/0048-5713-20020901-06
Kroenke, K., Spitzer, R. L., and Williams, J. B. (2001). The PHQ-9: validity of a brief depression severity measure. J. Gen. Intern. Med. 16, 606–613. doi: 10.1046/j.1525-1497.2001.016009606.x
Lakey, B., and Cohen, S. (2000). “Social Support Theory and Measurement,” in Social Support Measurement and Intervention: A Guide for Health and Social Scientists, eds S. Cohen, L. G. Underwood, and B. H. Gottlieb (Oxford University Press), 29–52. doi: 10.1093/med:psych/9780195126709.003.0002
Langford, C. P. H., Bowsher, J., Maloney, J. P., and Lillis, P. P. (1997). Social support: a conceptual analysis. J. Adv. Nurs. 25, 95–100.
Lazzaro, N. (2004). Why We Play Games: Four Keys To More Emotion Without Story. Available online at: http://www.xeodesign.com/whyweplaygames/xeodesign_whyweplaygames.pdf (accessed September 11, 2015).
Lee, C.-T., Yeh, C.-J., Lee, M.-C., Lin, H.-S., Chen, V. C.-H., Hsieh, M.-H., et al. (2012). Social support and mobility limitation as modifiable predictors of improvement in depressive symptoms in the elderly: results of a national longitudinal study. Arch. Gerontol. Geriatr. 55, 530–538. doi: 10.1016/j.archger.2012.03.002
Lee, G. R., and Ishii-Kuntz, K. (1987). Social interaction, loneliness, and emotional well-being among the elderly. Res. Aging 9, 459–482. doi: 10.1177/0164027587094001
Li, J., Erdt, M., Chen, L., Cao, Y., Lee, S.-Q., and Theng, Y.-L. (2018). The social effects of exergames on older adults: systematic review and metric analysis. J. Med. Internet Res. 20:e10486. doi: 10.2196/10486
Li, J., Theng, Y. L., and Foo, S. (2015). Effect of exergame on depression: a systematic review and meta-analysis. Cyberpsychol. Behav. Soc. Netw. 19, 34–42.
Li, J., Theng, Y.-L., Foo, S., and Xu, X. (2017). Exergames vs. traditional exercise: investigating the influencing mechanism of platform effect on subthreshold depression among older adults. Aging Ment. Health 22, 1634–1641.
Li, K. A., and Counts, S. (2007). “Exploring social interactions and attributes of casual multiplayer mobile gaming,” in Proceedings of the 4th International Conference on Mobile Technology, Applications, and Systems and The 1st International Symposium On Computer Human Interaction In Mobile Technology, Singapore.
Löwe, B., Unützer, J., Callahan, C. M., Perkins, A. J., and Kroenke, K. (2004). Monitoring depression treatment outcomes with the patient health questionnaire-9. Med. Care 42, 1194–1201. doi: 10.1097/00005650-200412000-00006
MacCallum, R. C., and Austin, J. T. (2000). Applications of structural equation modeling in psychological research. Annu. Rev. Psychol. 51, 201–226.
Maillot, P., Perrot, A., and Hartley, A. (2012). Effects of interactive physical-activity video-game training on physical and cognitive function in older adults. Psychol. Aging 27, 589–600. doi: 10.1037/a0026268
Martin, A., Rief, W., Klaiberg, A., and Braehler, E. (2006). Validity of the Brief Patient Health Questionnaire Mood Scale (PHQ-9) in the general population. Gen. Hosp. Psychiatry 28, 71–77. doi: 10.1016/j.genhosppsych.2005.07.003
Meeks, T. W., Vahia, I. V., Lavretsky, H., Kulkarni, G., and Jeste, D. V. (2011). A tune in “a minor” can “b major”: a review of epidemiology, illness course, and public health implications of subthreshold depression in older adults. J. Affect. Disord. 129, 126–142. doi: 10.1016/j.jad.2010.09.015
Montross, L. P., Kasckow, J., Golshan, S., Solorzano, E., Lehman, D., and Zisook, S. (2008). Suicidal ideation and suicide attempts among middle-aged and older patients with schizophrenia spectrum disorders and concurrent subsyndromal depression. J. Nerv. Ment. Dis. 196, 884–890. doi: 10.1097/nmd.0b013e31818ec823
Mueller, F., Agamanolis, S., and Picard, R. (2003). “Exertion interfaces: sports over a distance for social bonding and fun,” in Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Ft. Lauderdale, FL. –2011
]BR84 Muthén, L. K., and Muthé, B. O. (1998–2011). Mplus User’s Guide (Version 6th). Los Angeles, CA: Muthén & Muthén.
Nezlek, J. B., Imbrie, M., and Shean, G. D. (1994). Depression and everyday social interaction. J. Pers. Soc. Psychol. 67, 1101–1111. doi: 10.1037/0022-3514.67.6.1101
O’Donovan, C., Hirsch, E., Holohan, E., McBride, I., McManus, R., and Hussey, J. (2012). Energy expended playing Xbox KinectTM and WiiTM games: a preliminary study comparing single and multiplayer modes. Physiotherapy 98, 224–229. doi: 10.1016/j.physio.2012.05.010
Oh, Y., and Yang, S. (2010). “Defining exergames & exergaming,” in Proceedings of the Meaningful Play, MSU Serious Games Program, East Lansing, MI.
Park, T., Lee, U., MacKenzie, S., Moon, M., Hwang, I., and Song, J. (2014). “Human factors of speed-based exergame controllers,” in Proceedings of the 32nd Annual ACM Conference on Human Factors in Computing Systems, Toronto, ON.
Patil, B., Shetty, N., Subramanyam, A., Shah, H., Kamath, R., and Pinto, C. (2014). Study of perceived and received social support in elderly depressed patients. J. Geriatr. Ment. Health 1, 28–31. doi: 10.4103/2348-9995.141921
Peng, W., and Hsieh, G. (2012). The influence of competition, cooperation, and player relationship in a motor performance centered computer game. Comp. Hum. Behav. 28, 2100–2106. doi: 10.1016/j.chb.2012.06.014
Rosenberg, D., Depp, C. A., Vahia, I. V., Reichstadt, J., Palmer, B. W., Kerr, J., et al. (2010). Exergames for subsyndromal depression in older adults: a pilot study of a novel intervention. Am. J. Geriatr. Psychiatry 18, 221–226. doi: 10.1097/jgp.0b013e3181c534b5
Russell, D. W. (1996). UCLA Loneliness Scale (Version 3): reliability, validity, and factor structure. J. Pers. Assess. 66, 20–40. doi: 10.1207/s15327752jpa6601_2
Schulz, U., and Schwarzer, R. (2003). Soziale Unterstützung bei der Krankheitsbewältigung. Die Berliner Social Support Skalen (BSSS). [Social support in coping with illness: the Berlin Social Support Scales (BSSS)]. Diagnostica 49, 73–82. doi: 10.1026//0012-1924.49.2.73
Schutter, B. D., and Abeele, V. V. (2008). “Meaningful play in elderly life,” in Proceedings of the International Communication Association, Montreal, QC.
Singh, A., and Misra, N. (2009). Loneliness, depression and sociability in old age. Indust. Psychiatry J. 18, 51–55. doi: 10.4103/0972-6748.57861
Singh, B., and Kiran, U. V. (2013). Loneliness among elderly women. Int. J. Human. Soc. Sci. Invent. 2, 10–14.
Smyth, J. M. (2007). Beyond self-selection in video game play: an experimental examination of the consequences of massively multiplayer online role-playing game play. Cyberpsychol. Behav. 10, 717–721. doi: 10.1089/cpb.2007.9963
Spitzer, R. L., Williams, J. B., Kroenke, K., Linzer, M., deGruy, F. V. r, Hahn, S. R., et al. (1994). Utility of a new procedure for diagnosing mental disorders in primary care. The PRIME-MD 1000 study. J. Am. Med. Assoc. 272, 1749–1756. doi: 10.1001/jama.272.22.1749
Staiano, A. E., and Calvert, S. L. (2011). Exergames for physical education courses: physical, social, and cognitive benefits. Child Dev. Perspect. 5, 93–98. doi: 10.1111/j.1750-8606.2011.00162.x
Steiger, J. H., and Lind, J. (1980). “Statistically-based tests for the number of common factors,” in Proceedings of the Annual Spring Meeting of the Psychometric Society, Iowa City.
Stride, C. B., Gardner, S., Catley, N., and Thomas, F. (2015). Mplus Code For The Mediation, Moderation, And Moderated Mediation Model Templates From Andrew Hayes’ PROCESS analysis examples. Available online at: http://www.offbeat.group.shef.ac.uk/FIO/mplusmedmod.htm (accessed September 09, 2020).
Su, D., Wu, X.-N., Zhang, Y.-X., Li, H.-P., Wang, W.-L., and Zhang, J.-P. (2012). Depression and social support between China’ rural and urban empty-nest elderly. Arch. Gerontol. Geriatr. 55, 564–569. doi: 10.1016/j.archger.2012.06.006
Theng, Y.-L., Chua, P. H., and Pham, T. P. (2012). “Wii as entertainment and socialisation aids for mental and social health of the elderly,” in Proceedings of the CHI ’12 Extended Abstracts on Human Factors in Computing Systems, (Austin, TX).
Tomaka, J., Thompson, S., and Palacios, R. (2006). The relation of social isolation, loneliness, and social support to disease outcomes among the elderly. J. Aging Health 18, 359–384. doi: 10.1177/0898264305280993
Trepte, S., Reinecke, L., and Juechems, K. (2012). The social side of gaming: how playing online computer games creates online and offline social support. Comp. Hum. Behav. 28, 832–839. doi: 10.1016/j.chb.2011.12.003
Verstraten, P. F. J., Brinkmann, W. L. J. H., Stevens, N. L., and Schouten, J. S. A. G. (2005). Loneliness, adaptation to vision impairment, social support and depression among visually impaired elderly. Int. Cong. Ser. 1282, 317–321. doi: 10.1016/j.ics.2005.04.017
Williams, D. (2006). On and Off the ’net: scales for social capital in an online era. J. Comp. Mediat. Commun. 11, 593–628. doi: 10.1111/j.1083-6101.2006.00029.x
Wills, T. A. (1985). “Supportive functions of interpersonal relationships,” in Social Support and Health, eds I. S. Cohen and L. Syme (Orlando, FL: Academic Press), 61–82.
Wollersheim, D., Merkes, M., Shields, N., Liamputtong, P., Wallis, L., Reynolds, F., et al. (2010). Physical and psychosocial effects of Wii video game use among older women. Int. J. Emerg. Technol. Soc. 8, 85–98.
Wu, Z., Li, J., and Theng, Y. L. (2015). Examining the influencing factors of exercise intention among older adults: a controlled study between exergame and traditional exercise. Cyberpsychol. Behav. Soc. Netw. 18, 521–527. doi: 10.1089/cyber.2015.0065
Zhang, F., and Kaufman, D. (2016a). “Can playing massive multiplayer online role playing games (MMORPGs) improve older adults’ socio-psychological wellbeing?,” in Computer Supported Education: 7th International Conference, CSEDU 2015, eds S. Zvacek, M. T. Restivo, J. Uhomoibhi, and M. Helfert (Cham: Springer International Publishing), 504–522. doi: 10.1007/978-3-319-29585-5_29
Zhang, F., and Kaufman, D. (2016b). “Can Playing Massive Multiplayer Online Role Playing Games (MMORPGs) Improve Older Adults’ Socio-Psychological Wellbeing?,” in Proceedings of the International Conference on Computer Supported Education, Rome. doi: 10.1007/978-3-319-29585-5_29
Keywords: social interaction, elderly, exercise games, Wii, mental health
Citation: Li J, Theng Y-L and Foo S (2020) Play Mode Effect of Exergames on Subthreshold Depression Older Adults: A Randomized Pilot Trial. Front. Psychol. 11:552416. doi: 10.3389/fpsyg.2020.552416
Received: 16 April 2020; Accepted: 05 October 2020;
Published: 26 October 2020.
Edited by:
Rachel Kowert, Independent researcher, Seattle, United StatesReviewed by:
Desirée Colombo, Jaume I University, SpainCopyright © 2020 Li, Theng and Foo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jinhui Li, bGlqaW5odWlAam51LmVkdS5jbg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.