
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol. , 28 April 2020
Sec. Psychology for Clinical Settings
Volume 11 - 2020 | https://doi.org/10.3389/fpsyg.2020.00771
 Luigi Lavorgna1†
Luigi Lavorgna1† Marialaura Di Tella2*†
Marialaura Di Tella2*† Giuseppina Miele3Stefania Federica De Mercanti4Lidia Mislin Streito4Virginia Perutelli2
Giuseppina Miele3Stefania Federica De Mercanti4Lidia Mislin Streito4Virginia Perutelli2 Simona Bonavita3
Simona Bonavita3 Lorys Castelli2‡
Lorys Castelli2‡ Marinella Clerico4‡
Marinella Clerico4‡Background: Family functioning relies on different factors that are related to the individual characteristics of each member, the social context in which the family nucleus is integrated, and the internal and interpersonal family factors. The Short Version of the Family Assessment Measure-III, Dyadic Adjustment Scale, Inventory of Parent and Peer Attachment, Twenty-item Toronto Alexithymia Scale, Hospital Anxiety and Depression Scale, and Multidimensional Scale of Perceived Social Support are among the most commonly employed self-report measures for the assessment of family functioning and related factors. Traditionally, these scales have been administered using paper-and-pencil versions. However, with increased access to the Internet, online administration of questionnaires has become more common. The present study aimed to validate an online version of each of the above-mentioned questionnaires in a heterogeneous sample of Italian healthy individuals.
Methods: One-hundred participants were recruited for each questionnaire. A crossover design was used in each validation. The minimum important difference (MID) was applied to evaluate the differences in the variances of the paper-and-pencil and online format scores. A MID >0.5 is a reasonable first approximation of a threshold of important change. Taking into account the cross over design, mean difference between pencil-and-paper and online versions, and Intraclass Correlation Coefficient were also estimated by mixed models.
Results: The MID was <0.5 for all the instruments used. Therefore, no significant difference was observed between the score variances of the paper-and-pencil and online formats of all the questionnaires. Moreover, for each questionnaire the difference between the means of online and paper-and-pencil administrations scores (mean O-P) was calculated. We reported 95% confidence intervals that did not include the 0; therefore, mean (O-P) was not statistically significant.
Conclusions: The current findings indicate that the online versions of all the questionnaires we administered can be considered reliable tools for the assessment of family functioning and related factors.
Family is a complex, dynamic system that continuously evolves in search of a balance between the complementary tendencies of stability and transformation (Malagoli Togliatti and Catugno, 1996; Skinner et al., 2000; Pellerone et al., 2017). The functioning of this complex and delicate system relies on different factors, which are related with both the individual characteristics of each member and the social context in which the family nucleus is integrated, as well as with internal and interpersonal family factors, such as communication, cohesion, adaptability, quality of marital/parental–child relationships, and problem-solving abilities (Patterson and Garwick, 1994; McFarlane et al., 1995; Martinez and Forgatch, 2002; Walsh, 2003; Wood et al., 2017). Specifically concerning the internal factors, the Process Model of Family Functioning provides a conceptual framework to understand and assess these aspects within the family unit (Steinhauer et al., 1984). This model integrates several interrelated constructs (i.e., communication, affective expression, role performance, involvement, control, values, and norms) which facilitate the achievement of the main goal of the family, that is, the successful accomplishment of different developmental and crisis tasks (i.e., task accomplishment; Skinner et al., 2000). Each task requires the family to reorganize itself and to go through the following different phases to solve the problem: task identification, exploration of alternative solutions, implementation of selected approaches, and evaluation of effects. This model underlines that, through the process of task accomplishment, each family may meet the objectives central to its own life (Skinner et al., 2000). Skinner et al. (1983) tried to operationalize the seven constructs of the Process Model by developing the Family Assessment Measure (FAM). The FAM is an extensive tool designed for use in both clinical and research settings. At present, the third-edition of the FAM, conceived by Skinner et al. (2000) about 20 years later, is one of the most commonly employed self-report measures to evaluate family functioning.
Within the family system, interpersonal and relational factors, such as marital relationship and parental bonding, play a crucial role in determining adequate family functioning (Katz and Woodin, 2002; Parke, 2004). Family members influence each other both directly and indirectly (Minuchin, 2002). While on one hand, fathers and mothers can affect mother–child and father–child relationships, respectively, through their reciprocal interaction, on the other hand, children can indirectly influence the husband–wife relationship by modifying each parent’s behavior (Parke, 2004). Previous evidence highlighted that marital quality is linked with parent–child interactions and family well-being. For instance, happily married couples were found to show greater sensitivity, support, and warmth during family interactions as compared to unhappily married couples (Cowan et al., 1994; Minuchin, 2002).
Given the complexity of marital and parental relationships, different levels of analyses are necessary to understand the underlying family dynamics. Indeed, marital relationships and parental–child interactions require separate assessments to enable a holistic understanding (Parke and O’Neil, 1999). Among the different self-report instruments that have been developed to evaluate marital and parental–child relationships, the Dyadic Adjustment Scale (DAS; Spanier, 1976) and Inventory of Parent and Peer Attachment (IPPA; Greenberg et al., 1984; Armsden and Greenberg, 1987) are used most commonly. Particularly, the DAS has been designed to assess adjustment in all types of dyadic relationships, while the IPPA evaluates parental and peer attachment relationships in adolescents.
Regarding the individual characteristics of family members, personality traits are known to influence how each individual interacts with another (e.g., Asendorpf and Wilpers, 1998). Among these factors, growing evidence seems to show that difficulties in adequately recognizing one’s own emotions (i.e., alexithymia) are associated with a variety of interpersonal problems, including social isolation (e.g., Kokkonen et al., 2001), insecure attachment (Troisi et al., 2001), and maladaptive behaviors (Fonagy et al., 2002; Kooiman et al., 2004; Montebarocci et al., 2004; Besharat, 2010). Alexithymic individuals typically show limited capacity in processing emotional information, with resulting difficulties in identifying, understanding, and expressing their own feelings. These difficulties lead them to experience problems in dealing and communicating with other people, which in turn may cause increased levels of distress for the individuals themselves (Conrad et al., 2009; Besharat, 2010). This can affect family and social interactions negatively, with the possibility of destruction of marital and parental–child relationships. Assessing the presence of alexithymia and the level of psychological distress it may cause can thus help practitioners understand, more deeply, the individual characteristics that may interfere with adequate family functioning. The 20-item Toronto Alexithymia Scale (TAS-20; Taylor et al., 1985) is most commonly employed to assess alexithymia. The TAS-20 is a self-report questionnaire which examines the main features of alexithymia (Taylor et al., 2003). Concerning the assessment of psychological distress, different instruments have been developed to evaluate the levels of anxiety/depressive symptoms in both healthy and clinical populations (e.g., the Beck Depression Inventory, Beck et al., 1996; State-Trait Anxiety Inventory, Spielberger et al., 1983; Hospital Anxiety and Depression Scale – HADS, Zigmond and Snaith, 1983). Among these measures, the HADS is used most commonly, especially in clinical settings.
The last aspect to be considered in the assessment of family functioning is the social context in which the family unit is located and integrated. Within the social context, people are often connected with each other by different types of relations, to form a so-called social network (Wellman, 1981). The social network usually provides individuals with support and help, such as verbal and non-verbal advice, tangible aid, and emotional comfort, either in everyday situations or emergency circumstances (Stokes, 1983). The social support, provided by the social network through this emotional, informational, and instrumental assistance, usually has beneficial emotional or behavioral effects on recipients (Gottlieb, 1983; House and Kahn, 1985). Over the past decades, growing evidence has shown that social ties and social support are positively and causally related to individuals’ mental and physical health, and longevity (Seeman, 1996; Cohen and Janicki-Deverts, 2009; Ertel et al., 2009; Umberson and Montez, 2010; Thoits, 2011). Within the family nucleus, the presence of adequate levels of social support can represent a valuable resource the family members can count on, especially in the case of extremely stressful situations, such as a serious chronic medical condition or disability of one of the members (Kazak et al., 1997; Pakenham and Bursnall, 2006; Jiang et al., 2015; Kissel and Nelson, 2016).
Among the different instruments designed to assess social support, the Multidimensional Scale of Perceived Social Support (MSPSS; Zimet et al., 1988) is employed most commonly. The MSPSS is a self-report questionnaire which has been designed to evaluate the adequacy of an individual’s social support from three specific sources: the family, friends, and a significant other (Zimet et al., 1988).
Taken together, all these factors can help clinicians and researchers understand the dynamics and functioning of families better. The above-mentioned questionnaires are valid instruments that can be administered easily to patients and healthy individuals. Traditionally, these questionnaires and, in general, self-report instruments, have been administered using paper-and-pencil versions.
However, with the increased access to the Internet, which has grown dramatically over the past two decades (Gwaltney et al., 2008), the online administration of scales and questionnaires (Nguyen et al., 2017) can prove advantageous because it enables clinicians and researchers to reach a large number of participants in a short time. Online versions of scales and questionnaires have also been shown to have higher compliance rates than paper-based versions (U.S. Department of Health and Human Services FDA Center for Drug Evaluation, and Research, 2006; Lavorgna et al., 2018). Moreover, online versions have been found to be equivalent to paper-and-pencil ones, and these two versions can thus be used interchangeably (Vallejo et al., 2007; Coons et al., 2009; Bishop et al., 2010). However, the migration of questionnaires and scales from a paper-and-pencil to an online version is considered as a modification of the instrument that requires evidence to confirm if the two modes of administration perform equally well to guarantee the same validity, reliability, and quality of data (Lavorgna et al., 2018). Therefore, the main aim of the present study was to validate an online version of each of the above-mentioned questionnaires and scales (i.e., the Brief FAM-III, DAS, IPPA, TAS-20, HADS, and MSPSS), as an accurate, reliable online tool to assess family functioning and related factors.
Considering the sample size used in previous studies on validation of web-based questionnaires and scales, 100 participants for each questionnaire and scale were recruited (Lavorgna et al., 2018). In particular, we enrolled 100 participants who completed exclusively the DAS, 100 adolescent participants who completed the IPPA questionnaire, and 110 participants in total who filled in the HADS, MSPSS, FAM-III, and TAS-20 (in the latter case, 92 participants initially answered to all four questionnaires, so 10 more participants were recruited to reach the total size of 100). Moreover, a sample size of 100 allowed us to identify an Intraclass Correlation Coefficient (ICC) of 0.9 with a 95% confidence interval and an error of 8%.
The data for the online versions of the questionnaires and scales were collected using the Google Form service. Inclusion criteria were the same as those indicated in articles reporting the Italian validation of measure assessed (Bressi et al., 1996; Gentili et al., 2002; Prezza and Principato, 2002; San Martini et al., 2009; Iani et al., 2014; Pellerone et al., 2017).
Participants were recruited to represent individuals with different social and cultural backgrounds. Particularly, individuals were enrolled from the following contexts:
1. the editorial board of a national Italian newspaper (Corriere della Sera), based in Campania Region;
2. the staff of the Marcianise City Hall, Caserta, Italy;
3. the staff of an Italian electronic company (Erregame);
4. the administration staff of an Italian telematic university (Pegaso);
5. an Italian scout group (A.G.E.S.C.I.);
6. a church community;
7. students of University of Naples Federico II, Naples, Italy.
We asked to all members of these different contexts their availability and willingness to take part in the study. The percentage of acceptance was about 50–60%. People who could not participate in the study, had prior work or family commitments or were not on their work shift during the recruitment process. Nobody refused to take part for other reasons or because not interested.
The study was approved by the AOU San Luigi Gonzaga Ethics Committee (CE 81/2019/U, 24 July, 2019; protocol number 10899, 2 August, 2019) and was conducted in accordance with the Declaration of Helsinki. All the participants provided written informed consent to participate in the study.
Participants were asked to provide the following sociodemographic information: gender, age, educational level, and years of living together/marriage (for participants who responded to the DAS).
The Brief FAM-III is one of the most frequently used self-report instruments to assess family functioning (Steinhauer et al., 1984; Skinner et al., 2000; Pellerone et al., 2017). It consists of three modules: the “General Scale,” which evaluates the family as a system; the “Dyadic Relationships Scale,” which examines how each family member perceives his/her relationship with another member; and the “Self-Rating Scale,” which allows each person to rate his or her own functioning within the family. Each scale consists of 14 items that are rated using a 4-point Likert scale.
In the present study, only the Self-Rating Scale was administered. This scale has shown good internal consistency, with Cronbach alpha values ranging from 0.80 to 0.88 (Skinner et al., 2000; Pellerone et al., 2017). In line with these results, in our sample the Cronbach’s alphas were good for the Self-Rating Scale of the Brief FAM-III (α paper-and-pencil = 0.86; α online = 0.86).
The DAS is a relationship adjustment self-reported measure (Spanier, 1976; Gentili et al., 2002) that is divided into four subscales: “Dyadic Consensus,” which evaluates the degree to which the respondent agrees with his/her partner; “Dyadic Satisfaction,” which assesses the degree to which the respondent feels satisfied with his/her partner; “Dyadic Cohesion,” which measures the degree to which the respondent and his/her partner participate in activities together; and “Affectional Expression,” which examines the degree to which the respondent agrees with his/her partner regarding emotional affection.
The DAS has shown good internal consistency (Cronbach alpha scores: 0.70–0.95) and test–retest reliability (Carey et al., 1993). In line with these results, in our sample the Cronbach’s alphas were excellent for the DAS (α paper-and-pencil = 0.92; α online = 0.92).
The IPPA is a self-report scale that measures adolescents’ perceptions of their attachment to their parents and peers. The first version of this instrument was developed by Greenberg et al. (1984) for adolescents aged 12–19 years. It comprises two subscales, one assessing attachment with parents and the other with peers. Subsequently, Armsden and Greenberg (1989) proposed a revised version in which the parental scale was split into two identical versions assessing attachment with mothers and fathers, respectively. This revised version consists of 75 items, equally divided between the three forms (i.e., maternal, paternal, and peer).
The items provide a global security attachment score and those on the following three dimensions of the attachment relationship: “Trust,” which refers to adolescents’ trust that parents and peers understand and respect their needs and desires; “Communication,” which refers to adolescents’ perception that parents and peers are sensitive and responsive to their emotional states; and “Alienation,” which refers to adolescents’ feelings of isolation, anger, and detachment experienced in attachment relationships with parents and peers.
The scale has shown good internal consistency (Cronbach alpha scores: 0.87 for the maternal form, 0.89 for the paternal form, and 0.92, for the peer form) and test–retest reliability (Armsden and Greenberg, 1987). In line with these results, in our sample the Cronbach’s alphas were excellent for the IPPA (α paper-and-pencil = 0.94; α online = 0.94).
The TAS-20 is a self-report instrument designed to assess alexithymia (Taylor et al., 1985; Bressi et al., 1996). The results provide a TAS-20 total score and three subscale scores that assess the following aspects of alexithymia: “Difficulty identifying feelings,” which measures the inability to identify specific emotions or to distinguish between emotions and the bodily sensations of emotional arousal; “Difficulty describing feelings,” which assesses the inability to verbalize one’s emotions to other people; and “Externally-oriented thinking,” which evaluates the tendency of individuals to focus their attention externally and not on the inner emotional experience (Taylor et al., 2003). The TAS-20 cut-off scores are as follows: ≤51 no alexithymia, 52–60 borderline alexithymia, ≥61 alexithymia.
The scale has shown good internal consistency (Cronbach’s alpha coefficients: ≥0.70) and test–retest reliability (Taylor et al., 2003). In line with these results, in our sample the Cronbach’s alphas were good for the TAS-20 (α paper-and-pencil = 0.88; α online = 0.87).
The HADS is self-report measure used to assess psychological distress in clinical populations (Zigmond and Snaith, 1983; Costantini et al., 1999; Castelli et al., 2009). The HADS has also been used widely as an effective tool to assess psychological distress in non-clinical populations (Brennan et al., 2010). It includes 14 items representing two subscales, anxiety (HADS-A) and depression (HADS-D). Each subscale consists of seven items that are rated on a 0–3 scale, with the total score ranging from 0 to 21. A score of eight or more suggests a clinically significant level of depression/anxiety symptoms.
The HADS has shown good concurrent validity, test–retest reliability, and internal consistency (Cronbach’s alpha scores = 0.82–0.90) (Bjelland et al., 2002). In line with these results, in our sample the Cronbach’s alphas were good for the HADS (α paper-and-pencil = 0.80; α online = 0.79).
The MSPSS is self-report measure of perceived social support (Zimet et al., 1988; Prezza and Principato, 2002). It consists of 12 items that are scored on a 7-point Likert-type scale. A total score and three subscale scores can be derived: “Significant Other,” “Family,” and “Friends.” Higher scores are associated with higher levels of perceived social support.
The MSPSS has shown good internal consistency (Cronbach alpha scores: 0.87–0.94) and test–retest reliability (Osman et al., 2014). In line with these results, in our sample the Cronbach’s alphas were excellent for the MSPSS (α paper-and-pencil = 0.93; α online = 0.93).
A crossover design was used in each validation, in which half of the participants (Group A1, A2, A3, A4, A5, and A6) were randomly selected to complete the paper-and-pencil format and the other half (Group B1, B2, B3, B4, B5, B6) completed the online format (Time 1). After a time-lapse of 3 weeks, to avoid learning effects, the groups were reversed, and the participants in Group A completed the scale in the online format and those in Group B completed the paper-and-pencil format (Time 2).
To evaluate the differences in score variances between the paper-and-pencil and online formats, we used the method proposed by Guyatt et al. (2002) for the instruments completed twice by the same participants. Specifically, we applied the minimum important difference (MID), defined as “the smallest difference in score in the absence of trouble and change in a patient’s management” (Jaeschke et al., 1989). For instance, if variances in pre and post test scores have a change score of under 0.5, there is no important alteration (Guyatt et al., 2002). Therefore, MID > 0.5 is a reasonable first approximation of a threshold of important change. Taking into account the cross over design of the present study, mean difference between pencil-and-paper and online versions, and ICC were also estimated by mixed models. Mean difference, ICC, and their 95% confidence intervals (95% CI) were reported. Effect size was also provided. Finally, a correlation matrix of the relationship between the questionnaires’ dimensions for the paper-and-pencil and online procedures, separately, was computed.
Sociodemographic characteristics for each group of participants have been presented in Table 1.
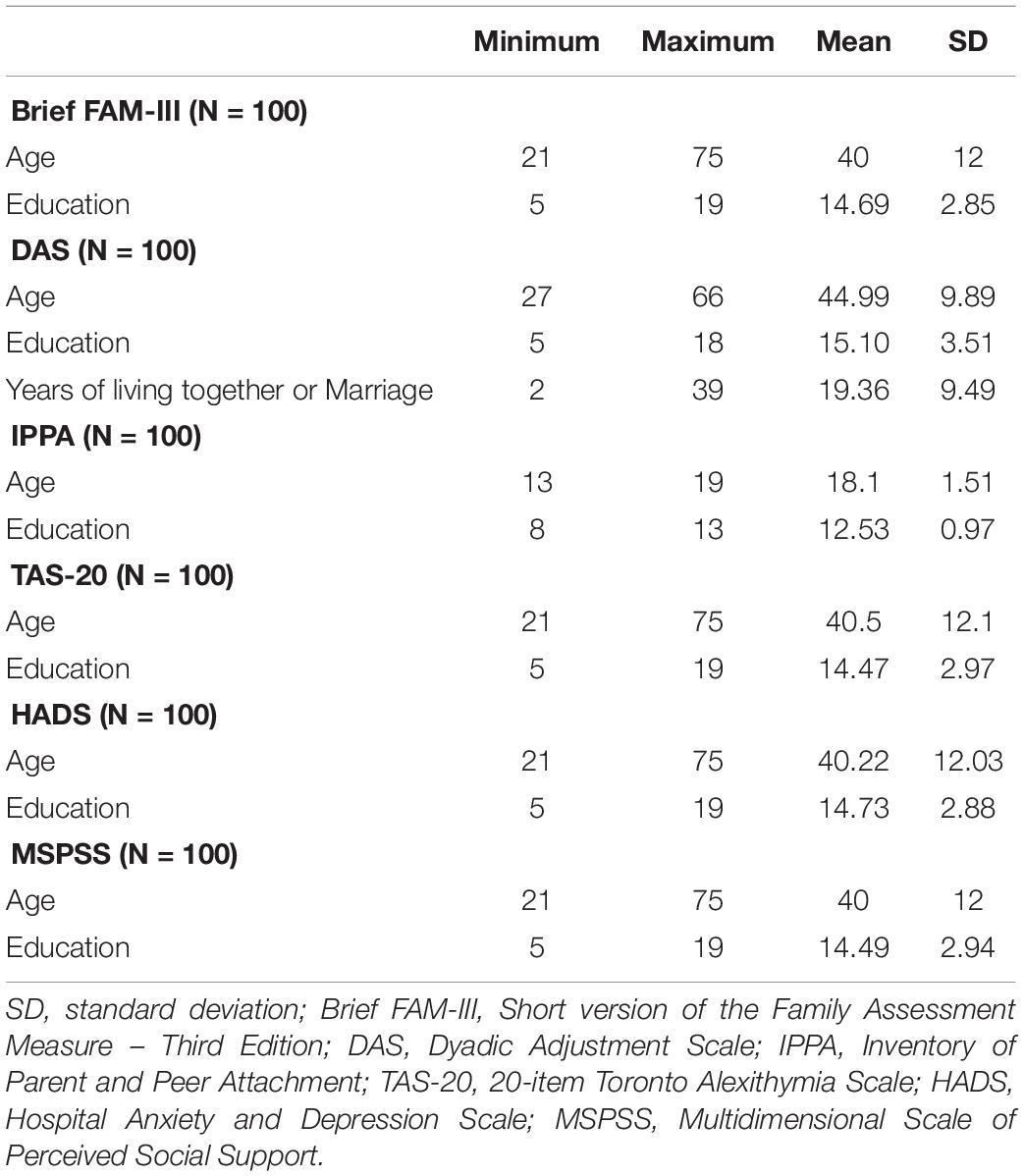
Table 1. Sociodemographic characteristics of the participants.
In our main analysis, the MID was <0.5 for all the instruments (Table 2). Therefore, no significant difference was observed between the score variances of the paper-and-pencil and online formats of the Brief FAM-III, DAS, IPPA, TAS-20, HADS, and MSPSS.
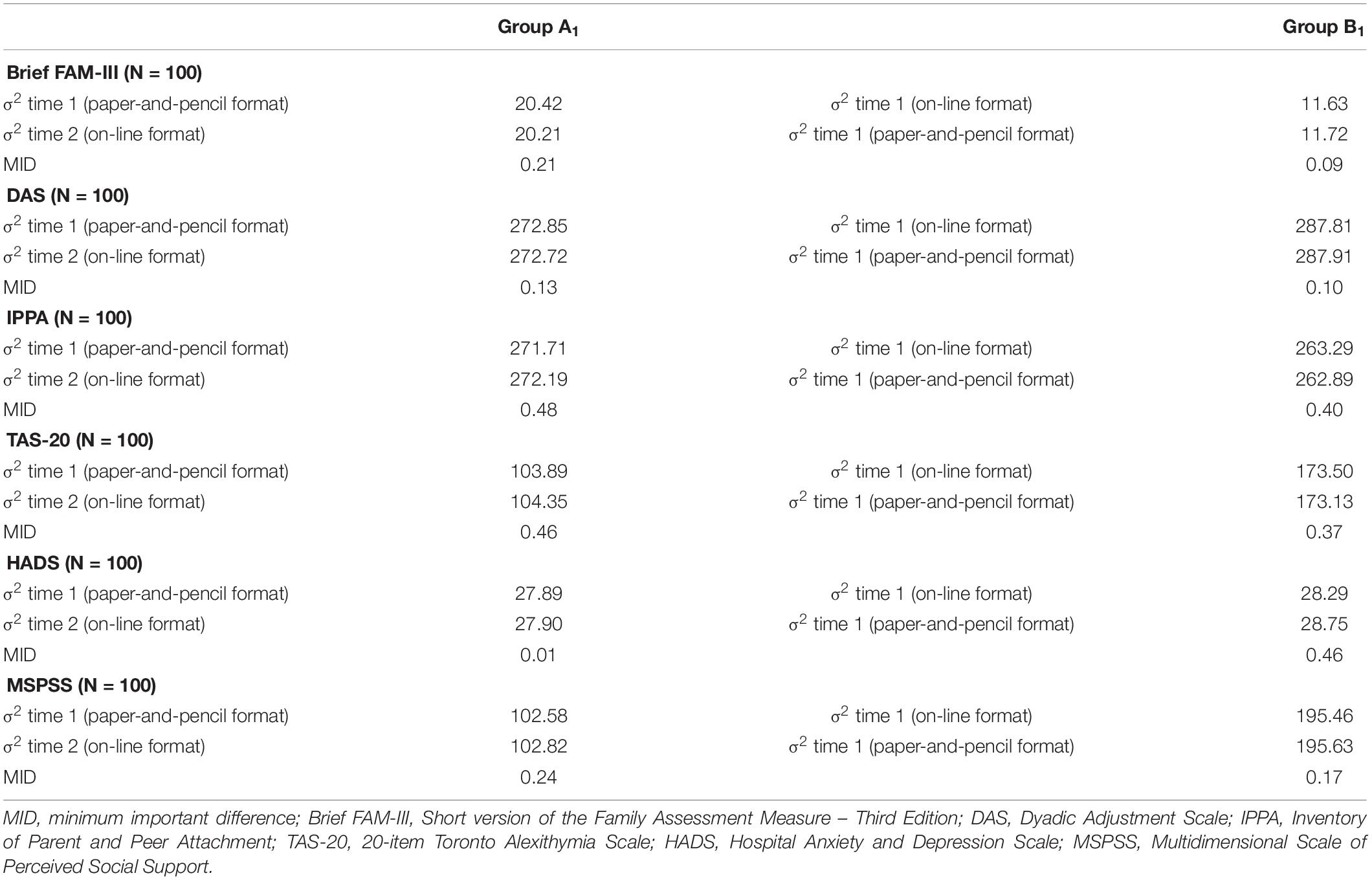
Table 2. Variance difference between the questionnaires scores for the paper-and-pencil and online formats.
In addition, for each of these questionnaires we calculated the difference between the means of online and paper-and-pencil administrations scores (mean O-P). We reported 95% CI that did not include the 0; therefore, mean (O-P) was not statistically significant. No statistically significant difference was thus observed between the paper-and-pencil and online formats. Effect size values also confirmed that there was no administration effect (Table 3).
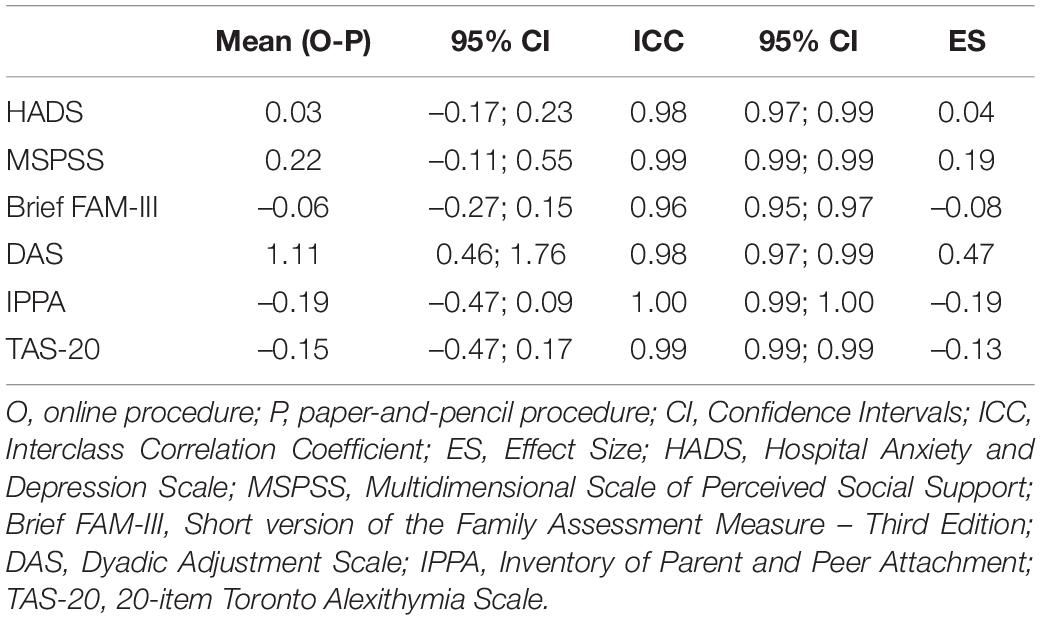
Table 3. Mean difference (mean O-P) between scores for the online and paper-and-pencil questionnaires, and Interclass Correlation Coefficient (ICC) are reported.
Finally, the correlation matrix showed no statistically significant results for each dimension of the questionnaires we administered in both paper-and-pencil and online formats (Supplementary Appendix A).
The present study aimed to validate the online version of the Brief FAM-III, DAS, IPPA, TAS-20, HADS, and MSPSS, to be used for assessing family functioning. The migration of questionnaires and scales from a paper-and-pencil to an online version is considered as a modification of an instrument that requires evidence to determine if the two administration formats perform equally well to guarantee the same validity, reliability, and quality of data (Lavorgna et al., 2018).
The results of our study showed no significant difference in the score variances of the paper-and-pencil and online formats of the Brief FAM-III, DAS, IPPA, TAS-20, HADS, and MSPSS. These findings were further supported using other analytic approaches, which showed no statistically significant difference for each of those questionnaires performed in online and paper-and-pencil formats. The online versions of these instruments can thus be considered reliable tools for the assessment of family functioning and related factors.
The questionnaires we validated represent an extensive battery that can allow clinicians and researchers to understand the relational dynamics of each family nucleus better. Indeed, family is a complex, dynamic system, the functioning of which relies on different factors such as individual characteristics of each member, the social context in which the family nucleus is integrated, and interpersonal family relationships (Patterson and Garwick, 1994; McFarlane et al., 1995; Martinez and Forgatch, 2002; Walsh, 2003; Wood et al., 2017). The Brief FAM-III, DAS, IPPA, TAS-20, HADS, and MSPSS represent valid instruments that can be employed to evaluate each of these factors to conduct an in-depth analysis of the features of family functioning.
The present study has some limitations. First, our sample was not representative of the general Italian population. Though we tried to enroll participants from different backgrounds, we could not include individuals from all the different Italian cultural contexts. Moreover, although we adopted the same procedure as the original validation articles of the measures we administered, we did not verify the validity of our results also on a clinical population. Therefore, further research should be conducted to replicate our findings with other clinical and non-clinical samples. Finally, future studies should also attempt to control for other sociodemographic variables that we could not control for in our study, such as occupation, socioeconomic status, and marital status.
Despite these limitations, our study was the first to validate the online versions of an extensive set of questionnaires to assess family functioning. We found evidence that the online versions of the Brief FAM-III, DAS, IPPA, TAS-20, HADS, and MSPSS represent accurate and reliable tools that could be easily administered to a large number of participants. A holistic assessment of the major factors that are related to family functioning can help clinicians and researchers understand family dynamics in clinical and non-clinical populations better.
The datasets generated for this study are available on request to the corresponding author.
The study involving human participants was reviewed and approved by the AOU San Luigi Gonzaga Ethics Committee (CE 81/2019/U, 24 July, 2019; protocol number 10899, 2 August, 2019) and was conducted in accordance with the Declaration of Helsinki. All the participants provided written informed consent to participate in the study. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
LL, SB, MC, and LC conceived and designed the study. LL, GM, SD, LS, and VP collected the data. LL, GM, and SB analyzed the data. LL, MD, LC, and MC interpreted the data. LL, MD, LC, and MC wrote the manuscript. All authors concluded the results, discussed and approved the final version of the manuscript.
The authors declare that this study received funding from Merck Group S.p.A. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors would like to thank the participants involved in the study.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2020.00771/full#supplementary-material
Armsden, G., and Greenberg, M. T. (1987). The inventory of parent peer attachment: individual differences and their relation to psychological well-being in adolescence. J. Youth. Adolesc. 16, 427–454. doi: 10.1007/BF02202939
Armsden, G., and Greenberg, M. T. (1989). The Inventory of Parent Peer Attachment (IPPA). Unpublished Report. Seattle, WA: University of Washington.
Asendorpf, J. B., and Wilpers, S. (1998). Personality effects on social relationships. J. Pers. Soc. Psychol. 74:1531. doi: 10.1037/0022-3514.74.6.1531
Beck, A. T., Steer, R. A., Ball, R., and Ranieri, W. F. (1996). Comparison of beck depression inventories-IA and-II in psychiatric outpatients. J. Pers. Assess. 67, 588–597. doi: 10.1207/s15327752jpa6703_13
Besharat, M. A. (2010). Relationship of alexithymia with coping styles and interpersonal problems. Procedia Soc. Behav. Sci. 5, 614–618. doi: 10.1016/j.sbspro.2010.07.152
Bishop, F. L., Lewis, G., Harris, S., McKay, N., Prentice, P., Thiel, H., et al. (2010). A within-subjects trial to test the equivalence of online and paper outcome measures: the Roland Morris disability questionnaire. BMC Musculoskelet. Disord. 8:113. doi: 10.1186/1471-2474-11-113
Bjelland, I., Dahl, A. A., Haug, T. T., and Neckelmann, D. (2002). The validity of the hospital anxiety and depression scale. An updated literature review. J. Psychosom. Res. 52, 69–77. doi: 10.1016/s0022-3999(01)00296-3
Brennan, C., Worrall-Davies, A., McMillan, D., Gilbody, S., and House, A. (2010). The hospital anxiety and depression scale: a diagnostic meta-analysis of case-finding ability. J. Psychosom. Res. 69, 371–378. doi: 10.1016/j.jpsychores.2010.04.006
Bressi, C., Taylor, G., Parker, J., Bressi, S., Brambilla, V., Aguglia, E., et al. (1996). Cross validation of the factor structure of the 20-item Toronto Alexithymia scale: an Italian multicenter study. J. Psychosom. Res. 41, 551–559. doi: 10.1016/S0022-3999(96)00228-0
Carey, M. P., Spector, I. P., Lantinga, L. J., and Krauss, D. J. (1993). Reliability of the dyadic adjustment scale. Psychol. Assess. 5, 238–240. doi: 10.1037/1040-3590.5.2.238
Castelli, L., Binaschi, L., Caldera, P., and Torta, R. (2009). Depression in lung cancer patients: is the HADS an effective screening tool? Support. Care Cancer 7, 1129–1132. doi: 10.1007/s00520-009-0604-8
Cohen, S., and Janicki-Deverts, D. (2009). Can we improve our physical health by altering our social networks? Perspect. Psychol. Sci. 4, 375–378. doi: 10.1111/j.1745-6924.2009.01141.x
Conrad, R., Wegener, I., Imbierowicz, K., Liedtke, R., and Geiser, F. (2009). Alexithymia, temperament and character as predictors of psychopathology in patients with major depression. Psychiatry Res. 165, 137–144. doi: 10.1016/j.psychres.2007.10.013
Coons, S. J., Gwaltney, C. J., Hays, R. D., Lundy, J. J., Sloan, J. A., Revicki, D. A., et al. (2009). Recommendations on evidence needed to support measurement equivalence between electronic and paper-based patient-reported outcome (PRO) measures: ISPOR ePRO good research practices task force report. Value Health 12, 419–429. doi: 10.1111/j.1524-4733.2008.00470.x
Costantini, M., Musso, M., Viterbori, P., Bonci, F., Del Mastro, L., Garrone, O., et al. (1999). Detecting psychological distress in cancer patients: validity of the Italian version of the Hospital Anxiety and Depression Scale. Support. Care Cancer 7, 121–127. doi: 10.1007/s005200050241
Cowan, P. A., Cowan, C. P., Schultz, M. S., and Heming, G. (1994). “Pre-birth to preschool family factors in children’s adaptation to kindergarten,” in Exploring Family Relationships with Other Social Contexts. Family Research Consortium: Advances in Family Research, eds R. D. Parke and S. G. Kellam (Hillsdale, NJ: Erlbaum), 75–114.
Ertel, K. A., Glymour, M. M., and Berkman, L. F. (2009). Social networks and health: a life course perspective integrating observational and experimental evidence. ı J. Soc. Pers. Relatsh. 26, 73–92. doi: 10.1177/0265407509105523
Fonagy, P., Gergely, G., Jurist, E., and Target, M. (2002). Affect Regulation, Metallization, and the Development of the Self. New York, NY: Other Press.
Gentili, P., Contreras, L., Cassaniti, M., and D’Arista, F. (2002). La Dyadic adjustment scale: una misura dell’adattamento di coppia [A measurement of dyadic adjustment: the dyadic adjustment scale]. Minerva Pschiatr. 43, 107–116.
Greenberg, M. T., Seigel, J. M., and Leich, C. J. (1984). “The nature and importance of attachment and partnership representations,” in Attachment from Infancy to Adulthood, eds K. E. Grossmann, K. Grossmann, and E. Waters (New York, NY: Guilford Press), 98–136.
Guyatt, G. H., Norman, G. R., Junipera, E. F., and Griffith, L. E. (2002). A critical look at transition ratings. J. Clin. Epidemiol. 55, 900–908. doi: 10.1016/s0895-4356(02)00435-3
Gwaltney, C. J., Shields, A. L., and Shiffman, S. (2008). Equivalence of electronic and paper and pencil administration of patient reported outcome measures: a meta analytic review. Value Health 11, 322–333. doi: 10.1111/j.1524-4733.2007.00231.x
House, J. S., and Kahn, R. L. (1985). “Measures and concepts of social support,” in Social Support and Health, eds S. Cohen and S. L. Syme (San Diego, CA: Academic Press), 83–108.
Iani, L., Lauriola, M., and Costantini, M. (2014). A confirmatory bifactor analysis of the hospital anxiety and depression scale in an Italian community sample. Health Qual. Life Outcomes 5, 12–84. doi: 10.1186/1477-7525-12-84
Jaeschke, R., Singer, J., and Guyatt, G. H. (1989). Measurement of health status. Ascertaining the minimal clinically important difference. Control. Clin. Trials 10, 407–415. doi: 10.1016/0197-2456(89)90005-6
Jiang, H., Wang, L., Zhang, Q., Liu, D. X., Ding, J., Lei, Z., et al. (2015). Family functioning, marital satisfaction and social support in hemodialysis patients and their spouses. Stress Health 31, 166–174. doi: 10.1002/smi.2541
Katz, L. F., and Woodin, E. M. (2002). Hostility, hostile detachment, and conflict engagement in marriages: effects on child and family functioning. Child Dev. 73, 636–652. doi: 10.1111/1467-8624.00428
Kazak, A. E., Barakat, L. P., Meeske, K., Christakis, D., Meadows, A. T., Casey, R., et al. (1997). Posttraumatic stress, family functioning, and social support in survivors of childhood leukemia and their mothers and fathers. J. Consult. Clin. Psychol. 65, 120–129. doi: 10.1037//0022-006x.65.1.120
Kissel, S. D., and Nelson, W. M. III (2016). Parents’ perceptions of the severity of their child’s autistic behaviors and differences in parental stress, family functioning, and social support. Focus Autism. Dev. Disabil. 31, 152–160. doi: 10.1177/1088357614537352
Kokkonen, P., Karvonen, J. T., Veijola, J., Laeksy, K., and Jokelainen, J. (2001). Perceived and sociodemographic correlates of alexithymia in a population sample of young adults. Compr. Psychiatry 42, 471–476. doi: 10.1053/comp.2001.27892
Kooiman, C. G., Vellinga, S., Spinhoven, P. H., Draijer, N., Trijsburg, R. W., and Rooijmans, H. G. M. (2004). Childhood adversities as risk factors for alexithymia and other aspects of affect dysregulation in adulthood. Psychother. Psychosom. 73, 107–116. doi: 10.1159/000075542
Lavorgna, L., Miele, G., Petruzzo, M., Lanzillo, R., and Bonavita, S. (2018). Online validation of the Italian version of the patient determined disease steps scale (PDDS) in people with multiple sclerosis. Mult. Scler. Relat. Disord. 21, 108–109. doi: 10.1016/j.msard.2018.02.014
Malagoli Togliatti, M., and Catugno, A. (1996). Psicodinamica delle Relazioni Familiari. [Psychodynamic of Family Relationships]. Bologna: Il Mulino.
Martinez, C. R. Jr., and Forgatch, M. S. (2002). Adjusting to change: linking family structure transitions with parenting and boys’ adjustment. J. Fam. Psychol. 16, 107–117. doi: 10.1037/0893-3200.16.2.107
McFarlane, A. H., Bellissimo, A., and Norman, G. R. (1995). Family structure, family functioning and adolescent well-being: the transcendent influence of parental style. J. Child. Psychol. Psychiatry 36, 847–864. doi: 10.1111/j.1469-7610.1995.tb01333.x
Minuchin, P. (2002). “Looking toward the horizon: present and future in the study of family systems,” in Retrospect and Prospect in the Psychological Study of Families, eds J. P. McHale and W. S. Grolnick (Mahwah, NJ: Lawrence Erlbaum Associates Publishers), 259–278.
Montebarocci, O., Codispoti, M., Baldaro, B., and Rossi, N. (2004). Adult attachment style and alexithymia. Pers. Individ. Dif. 36, 499–507. doi: 10.1016/S0191-8869(03)00110-7
Nguyen, A., Mosadeghi, S., and Almario, C. V. (2017). Persistent digital divide in access to and use of the Internet as a resource for health information: results from a California population-based study. Int. J. Med. Inform. 103, 49–54. doi: 10.1016/j.ijmedinf.2017.04.008
Osman, A., Lamis, D. A., Freedenthal, S., Gutierrez, P. M., and McNaughton-Cassill, M. (2014). The multidimensional scale of perceived social support: analyses of internal reliability, measurement invariance, and correlates across gender. J. Pers. Assess. 96, 103–112. doi: 10.1080/00223891.2013.838170
Pakenham, K. I., and Bursnall, S. (2006). Relations between social support, appraisal and coping and both positive and negative outcomes for children of a parent with multiple sclerosis and comparisons with children of healthy parents. Clin. Rehabil. 20, 709–723. doi: 10.1191/0269215506cre976oa
Parke, R. D. (2004). Development in the family. Annu. Rev. Psychol. 55, 365–399. doi: 10.1146/annurev.psych.55.090902.141528
Parke, R. D., and O’Neil, R. (1999). “Social relationships across contexts: family-peer linkages,” in Minnesota Symposium on Child Psychology, eds W. A. Collins and B. Laursen (Hillsdale, NJ: Erlbaum), 211–239.
Patterson, J. M., and Garwick, A. W. (1994). Levels of meaning in family stress theory. Fam. Process 33, 287–304. doi: 10.1111/j.1545-5300.1994.00287.x
Pellerone, M., Ramaci, T., Parrello, S., Guariglia, P., and Giaimo, F. (2017). Psychometric properties and validation of the Italian version of the family assessment measure third edition - short version - in a nonclinical sample. Psychol. Res. Behav. Manag. 10, 69–77. doi: 10.2147/PRBM.S128313
Prezza, M., and Principato, M. C. (2002). La rete sociale e il sostegno sociale. Conoscere la Comunitá. Bologna: Il Mulino.
San Martini, P., Zavattini, G. C., and Ronconi, S. (2009). L’Inventario per l’Attaccamento ai Genitori ed ai Pari (IPPA-Inventory of Parent and Peer Attachment). Un’indagine psicometrica su un campione italiano di adolescenti. G. Ital. Psicol. 36, 199–228. doi: 10.1421/29288
Seeman, T. E. (1996). Social ties and health: the benefits of social integration. Ann. Epidemiol. 6, 442–451. doi: 10.1016/S1047-2797(96)00095-6
Skinner, H., Steinhauer, P., and Sitarenios, G. (2000). Family assessment measure (FAM) and process model of family functioning. J. Fam. Ther. 22, 190–210. doi: 10.1111/1467-6427.00146
Skinner, H. A., Steinhauer, P. D., and Santa-Barbara, J. (1983). The family assessment measure. Can. J. Psychiatry 2, 91–105. doi: 10.1177/070674378402900202
Spanier, G. B. (1976). Measuring dyadic adjustment: new scales for assessing the quality of marriage and similar dyads. J. Marriage Fam. 15–28. doi: 10.2307/350547
Spielberger, C. D., Gorsuch, R. L., Lushene, R., Vagg, P. R., and Jacobs, G. A. (1983). State-trait Anxiety Inventory (form Y). Palo Alto, CA: Mind Garden.
Steinhauer, P. D., Santa-Barbara, J., and Skinner, H. A. (1984). The process model of family functioning. Can. J. Psychiatry 29, 98–111.
Stokes, J. P. (1983). Predicting satisfaction with social support from social network structure. Am. J. Commun. Psychol. 1, 141–152. doi: 10.1007/BF00894363
Taylor, G. J., Bagby, R. M., and Parker, J. D. (2003). The 20-Item Toronto Alexithymia Scale: IV. Reliability and factorial validity in different languages and cultures. J. Psychosom. Res. 55, 277–283. doi: 10.1016/S0022-3999(02)00601-3
Taylor, G. J., Ryan, D. P., and Bagby, R. M. (1985). Toward the development of a new self-report alexithymia scale. Psychother. Psychosom. 44, 191–199. doi: 10.1159/000287912
Thoits, P. A. (2011). Mechanisms linking social ties and support to physical and mental health. J. Health Soc. Behav. 52, 145–161. doi: 10.1177/0022146510395592
Troisi, A., D’Argenio, A., Peracchio, F., and Petti, P. (2001). Insecure attachment and alexithymia in young men with mood symptoms. J. Nerv. Ment. Dis. 189, 311–316. doi: 10.1097/00005053-200105000-00007
U.S. Department of Health and Human Services FDA Center for Drug Evaluation, and Research (2006). Guidance for industry: patient-reported outcome measures: use in medical product development to support labeling claims: draft guidance. Health Qual. Life Outcomes 114–79. doi: 10.1186/1477-7525-4-79
Umberson, D., and Montez, J. K. (2010). Social relationships and health: a flashpoint for health policy. J. Health. Soc. Behav. 51, S54–S66. doi: 10.1177/0022146510383501
Vallejo, M. A., Jordán, C. M., Díaz, M. I., Comeche, M. I., and Ortega, J. (2007). Psychological assessment via the internet: a reliability and validity study of online (vs paper-and-pencil) versions of the General Health Questionnaire-28 (GHQ-28) and the Symptoms Check-List-90-Revised (SCL-90- R). J. Med. Internet Res. 9:e2. doi: 10.2196/jmir.9.1.e2
Walsh, F. (2003). Family resilience: a framework for clinical practice. Fam. Process 42, 1–18. doi: 10.1111/j.1545-5300.2003.00001.x
Wellman, B. (1981). “Applying network analysis to the study of support,” in Social Network and Social Support, ed. B. H. Gottlieb (Beverly Hills, CA: Sage Publications).
Wood, L. E., Grau, J. M., Smith, E. N., Duran, P. A., and Castellanos, P. (2017). The influence of cultural orientation on associations between Puerto Rican adolescent mothers’ parenting and toddler compliance and defiance. Cultur. Divers. Ethnic Minor. Psychol. 23, 300–309. doi: 10.1037/cdp0000109
Zigmond, A. S., and Snaith, R. P. (1983). The hospital anxiety and depression scale. Acta Psychiatr. Scand. 67, 361–370. doi: 10.1111/j.1600-0447.1983.tb09716.x
Keywords: online validation, family functioning, marital relationships, parental and peer attachment, alexithymia, psychological distress, social support
Citation: Lavorgna L, Di Tella M, Miele G, De Mercanti SF, Streito LM, Perutelli V, Bonavita S, Castelli L and Clerico M (2020) Online Validation of a Battery of Questionnaires for the Assessment of Family Functioning and Related Factors. Front. Psychol. 11:771. doi: 10.3389/fpsyg.2020.00771
Received: 11 October 2019; Accepted: 30 March 2020;
Published: 28 April 2020.
Edited by:
Giada Pietrabissa, Catholic University of the Sacred Heart, ItalyReviewed by:
David Mellor, Deakin University, AustraliaCopyright © 2020 Lavorgna, Di Tella, Miele, De Mercanti, Streito, Perutelli, Bonavita, Castelli and Clerico. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marialaura Di Tella, bWFyaWFsYXVyYS5kaXRlbGxhQHVuaXRvLml0
†These authors share first authorship
‡These authors share senior authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.