 Peter Kay Chai Tay
Peter Kay Chai Tay Yi Yuan Ting1
Yi Yuan Ting1 Kok Yang Tan
Kok Yang Tan- 1Centre for Ageing Research and Education, Duke-NUS Medical School, Singapore, Singapore
- 2Humanities and Social Sciences, Murdoch University, Singapore, Singapore
Men and women exhibit clear differences in occupational choices. The present article elucidates sex differences in terms of formal care occupational choices and care styles based on evolutionary psychological perspectives. Broadly (1) the motivation to attain social status drives male preference for occupations that signals prestige and the desire to form interpersonal affiliation underlies female preference for occupations that involve psychosocial care for people in need; (2) ancestral sex roles leading to sexually differentiated cognitive and behavioral phenotypic profiles underlie present day sex differences in care styles where men are things-oriented, focusing on disease management while women are people-oriented, focusing on psychosocial management. The implications for healthcare and social care are discussed and recommendations for future studies are presented.
Introduction
Sex differences are evident in formal care occupations across cultures. Regardless of sex equity, males and females appear to undertake certain care occupations more over others. For instance, nurses are overwhelmingly females (O’Connor, 2015) while physicians and healthcare managers are predominantly males (Ku, 2011; Lowe, 2011). In the current review, we use evolutionary psychological (EP) frameworks (i.e., sexual strategies theory, sexual division of labor) to elucidate the innate tendencies driving sex differences in formal care occupations. Broadly, we argue that males provide care in positions that advertise social status while females are motivated to provide care for affiliation purposes. In addition, we postulate that males tend to focus on non-human (i.e., things) aspects of care while females tend toward more human (i.e., psychosocial) aspects. Based on this analysis, we examine the implications for healthcare and social care sectors.
Definitions of Care
In the current article, we focus on formal care in the healthcare and social care domains. Formal care refers to paid care and to some extent volunteered care coming from government and non-profit organizations. We exclude domestic helpers because they tend to differ from other formal carers in terms of cultural background and ethnicity; formal carers are usually employed in institutional settings as opposed to domestic helpers who are usually employed by agencies and private enterprises. We focus on formal care particularly in the healthcare and social care setting because sex differences in formal care has not been subjected to EP analysis to our knowledge.
There are clear sex preferences in the Science, Technology, Engineering, and Mathematics (STEM) domains (Lippa, 2010), and we expect the same sex preferences to underlie the formal care domains. Although sex ratio in STEM occupations has become less unbalanced in recent years, the sex differences remain in social disciplines such as Health and Welfare which has a greater proportion of female Ph.D. graduates (59%), contrasting with engineering, manufacturing, and construction (28%) (European Commission, 2016). Sex differences are also notable within formal care occupations. Globally, females outnumber males overwhelmingly and this sex difference is consistent across all ages, where the bulk of the female workers occupy people oriented professions such as nurses and social workers (Gupta et al., 2003; Rocheleau, 2017; Ministry of Manpower, 2018). The Luxemburg Income Study conducted with eighteen participating countries in Europe, America, Asia, and Oceania showed that across countries, at least 62–85% of health workers are females (Gupta et al., 2003). Specifically, a greater proportion of females worked in the nursing and midwifery specializations compared to physicians. In the following sections, we use EP theoretical frameworks to explicate the evolutionary roots that underlie these patterns.
Evolutionary Psychological Theories on Sex Differences Related to Care
In this article, EP analysis refers to conceptual analyses based on the postulation that evolutionary-driven innate factors underlie emergent behavioral tendencies, attitudes, and preferences. Specifically, we elucidate EP causes to understand how sex differences in formal care emerge and examine the implications for these differences.
Sexual Strategies and Occupational Choice
In humans, sexual selection involves a showcase of physical and psychological traits, evolved on the basis of attracting the opposite sex (Darwin, 1871; Puts, 2010). The sexual strategies theory explicates sex-specific qualities that confers evolutionary benefits which are thus attractive to the opposite sex: Among males, social status translates into reproductive advantage because females prefer males who possess traits which signal their ability to invest resources in their offspring (Buss, 1989; Buss and Schmitt, 2017), in part because of females’ physical vulnerability and demands associated with pregnancy and childbirth (Bjorklund and Shackelford, 1999). Thus, reproductive success among low status males is greatly reduced (Hopcroft, 2006; Fieder and Huber, 2007). This contrasts with male mate choice which largely focuses on indicators of fertility and child bearing capacities such as youth (Buss and Schmitt, 2017). Thus, female social status is less relevant to males, and females are comparatively less concerned about their own social status (Low et al., 2002).
For males, occupation provides one of the most salient opportunities to enhance their social status. Thus, males are more focused on their careers, devoting their resources to work that will generate high-impact products and gain recognition at work particularly during mid adulthood (Ferriman et al., 2009). Relating to social status, male sex role in most cultures emphasizes dominance (i.e., competitive behaviors) understood as “judgment of the status, power, and/or competence of others and their underlying motivation to seek it” (Adams et al., 2015). As such, hierarchical occupations which provide opportunities for attaining leadership positions will be particularly attractive to males.
While males are more concerned with social status and develop skills to advance their career, females tend toward affiliation and focus on building interpersonal relationships. In most societies, female sex role emphasizes on affiliation (i.e., communal behaviors) (Eagly, 1997; Eagly and Wood, 2013; Adams et al., 2015). Affiliation refers to the “judgment of solidarity, friendliness, and/or warmth and the underlying motivation to seek it” (Adams et al., 2015). In contrast to the fight-or-flight tendency among males, the tend-and-befriend hypothesis highlights that females are equipped with the natural skills to provide care, and creating and maintaining social networks (Taylor et al., 2000). For instance, an experimental study demonstrated that females are more likely to help others especially when it does not involve risks (Eckel and Grossman, 2008). Furthermore, both females and males prefer females as confidantes because females are more likely to engage in conversations related to relationships and provide social support (Barbee et al., 1993; Bank and Hansford, 2000; Kenrick, 2012), highlighting the relevance for females take on formal care roles that promote affiliation.
Sexual Division of Labor and Care Styles
Sexual division of labor highlights that males and females utilize their natural abilities to procure resources and achieve cooperative mutualism, where males function as “hunters” while females function as “gatherers” (Bird and Codding, 2015). Particularly, a great part of human ancestry is spent in the Savannah environment where males take on the role of hunting for large prey and toolmaking while females take on the role of providing childcare, and gathering and planting foods (Murdock and Provost, 1973; Marlowe, 2007; Bird and Codding, 2015). Even in cases when females are involved in hunting, they typically play supportive roles such as assisting the males in their hunting trips (Hurtado et al., 1985) or tracking game (Biesele and Barclay, 2001). Given this division of labor, traits favoring the sex-specific activities will developed accordingly among males and females. In particular, because hunters travel long distances over wide territories compared to gatherers, males develop better technical skills such as spatial and navigational ability, throwing skills and focused attention (Frost, 1998; Stoet, 2011). Conversely, given that gathering requires social interaction among individuals within a small area, females developed better social and linguistic skills (Stoet, 2011).
Consistent with this notion, males and females show abilities and preference for things and people, respectively (Lippa, 1998). Meta-analytic studies revealed sex differences in terms of occupational preferences where females show preferences for people oriented jobs, while males for object oriented jobs (Su et al., 2009), and these sex-specific preferences were observed in all 53 nations of a review study where the size of the sex differences were uncorrelated with global variation in gender equity (Lippa, 2010). This indicates that sex differences in occupational preferences are universal across cultures and do not diminish in more gender egalitarian cultures. As sex differences in sex-differentiated traits and occupational preference are robust and pervade across cultures, we expect similar sex patterns for care styles. Particularly, a greater proportion of males in formal care will take on tasks that require hard, technical skills and independence, while more females occupy the “softer” or more nurturing aspects of care. We now turn to the implications on healthcare and social care settings based on the current EP arguments.
Implications on Healthcare and Social Care Occupational Domains
Theoretical Implications
Existing theoretical frameworks in the literature tend to explain sex differences in formal care based on socialization and sex-role theories rather than evolutionary theories. As opposed to evolutionary theories, sex-role theories emphasize the impact of societal influence based on a person’s biological sex, leading to the development of sex stereotypic traits and perceptions (Vanwesenbeeck, 2009; Eagly and Wood, 2011). For instance, sex-role theory predicts that sex stereotyping about cognitive abilities and preferences is developed through socialization and nations that are more sex equal would have lower sex differentiated occupational pursuit (e.g., Riska, 2011). Yet, the sex differences appear universal, and unrelated to sex egalitarianism (Charles and Bradley, 2009; Lippa, 2010). In particular, the pursuit of STEM occupations observed the largest differences in sex egalitarian countries (e.g., Germany, Sweden, and Switzerland), and the smallest differences were observed in the least sex egalitarian countries (e.g., Colombia, Indonesia, and Tunisia) (Charles and Bradley, 2009). Thus, EP theories may provide better explanations for sex differences in occupation choices and provide more precise predictions. For instance, EP theorists argue that males take on STEM occupations because they tend to have innate preferences and possess relevant cognitive abilities such as spatial, mathematical and mechanical competencies (Geary, 2014), suggesting that sex preferences rather than sex inequality drives unbalanced sex ratios across occupations. This line of argument is further supported by studies on homosexuals displaying sex atypical preferences (e.g., Lippa, 2005). In particular, occupational choice appears to be influenced by sexual orientation where homosexual males report stronger preferences toward jobs such as school teacher, florist and social worker, and homosexual females report stronger preferences for jobs such as builder, carpenter, and electrical engineer compared to their heterosexual counterparts; bisexuals report job preferences between heterosexuals and homosexuals (Lippa, 2008).
Theories which exclude EP explanations risk mislabeling innate preferences as inequalities in formal care occupations. Some scholars argue that sexual discrimination underlies sex differences in formal care occupations and presumed that removing it would result in sex equity across occupations. For instance, it has been assumed that the underrepresentation of female physicians can be attributed to sex discrimination (Hannawi and Al Salmi, 2018). Notwithstanding that certain types of sex discrimination such as unequal remuneration exists and should be eliminated, extant evidence suggests that eradicating sex discrimination will not lead to equal sex ratio for formal care occupations (Lippa, 2010; Stoet and Geary, 2018). Furthermore, sex inequity fails to account for drastically low male workers in formal care occupations with little sex discriminatory practices like nursing and social work. Thus, scholars attempting to explain sex differences should integrate EP frameworks to develop more holistic and accurate theories to explain sex differences in formal care occupations.
Human Resource
Given that sex egalitarian countries tend to have the greatest sex differences in personality and occupational choices (Charles and Bradley, 2009; Lippa, 2010), sex specific policies such as increasing vacancies for the sex with lower hire proportion may not be effective. For instance, although demand for male-dominated blue-collar professions (e.g., manufacturing, mechanics) is shrinking while demand for female-dominated healthcare industry is growing, the resultant excess in male population in the work force did not lead to a corresponding increase in male employment in “pink-collar” formal care professions such as nursing or healthcare aides (Dill, 2017). Similarly, an overemphasis on sex-ratio reversal policies undermines the stronger effect of innate preferences. In particular, policies skewed toward promoting atypical sex employment may not ultimately lead to balanced sex employment and may be counterproductive. For instance, medical enrolment in favor of female applicants may place some eligible male applicants at a disadvantage (McKinstry, 2008). Furthermore, even though female students have a slight advantage in many STEM subjects compared to male students, female students nevertheless tend to pursue non-STEM education (Stoet and Geary, 2018).
Sex-role theorists argue that female physicians encounter greater occupational barriers because of the expectation that females are homemakers (Buddeberg-Fischer et al., 2010). Our present analysis suggests that instead, females have a natural inclination to provide care to their families. This understanding will change how we encourage females to remain as physicians. Particularly, females tend to trade-off their career development particularly when they have children so that they can devote more time for the family and more broadly, females also divert more resources toward the community, friends, and less on their careers (Ferriman et al., 2009). Thus, understanding innate preferences for sex differences underlying the effect of family demands and parenthood on career choices for medicine can provide potential solutions to facilitate the enrolment and maintenance of female physicians (Buddeberg-Fischer et al., 2010; Riska, 2011). On the other hand, males tend to undertake jobs that emphasize strong leadership and offer high extrinsic rewards such as higher income and prestige as indicative of one’s social status (Ku, 2011). Policies aimed to increase hiring of males in occupations such as nursing and social work will be more effective if is it coupled with changing societal perceptions of such professions. Awareness about the barriers toward females is nonetheless important, yet ignoring potential EP driven factors that would attract females and males into professions conventionally occupied by the opposite sex would be ineffective.
Preferences and Competencies in Care Tasks
The people-thing dimension highlights that males and females possess innate abilities and preferences (Lippa, 1998), and may manifest in specific care tasks that people adopt. For instance, males and females tend to focus on different aspects of a problem (e.g., an illness) and use different methods to solve the same problem (e.g., treatment method) in formal care settings. Concurring with the notion that ancestral males are largely responsible for the manufacturing of tools and weapons (Puts, 2010), modern males tend to be technology and skills oriented, and select formal care occupations such as surgical specialties, medical technicians, paramedic, radiology, and pathology (Hojat et al., 2002, 2005; Simpson, 2007). In contrast, females are people-oriented and tend to adopt roles in caring, understanding and supportive services in diagnosis and treatment contexts (Hojat et al., 2002, 2005), and occupy human and relational based professions such as childcare workers, social workers, nurses, health aides and community/social service specialists (Rocheleau, 2017). Even male nurses tend to focus on technical competence and rationality to preserve their masculine identity (Simpson, 2007).
To support males in nursing roles, it may be fruitful to develop their technical and rational skills as part of the job scope. Given the long standing perception that nurses receive poor wages (Evans, 2004), maintenance and recruitment of male nurses may also be more successful by dispelling this myth and emphasize that nursing career provides opportunities to advance technical skills and includes leadership track progression. In addition, while male nurses may be more adept at care tasks that require strength such as lifting and moving patients with mobility limitations, the job should provide opportunities for problem specific solutions. For instance, engaging male nurses in solving mobility problem in the hospital such as making use of devices to move patients may be more rewarding. Such task specific interests and abilities are revealed in a study in New Zealand which found that the top ten female dominated formal care occupations include dieticians/nutritionists, nurses, midwives and occupational therapists, which typically require more personal long-term care and emotional support to the care-recipients, while male dominated occupations such as orthoptists, surgeons, physicians, and optometrists, are driven more by technical knowledge and comprise of once-off visits (Grant et al., 2004). While the study also showed that formal care occupations that were male-dominated prior to the introduction of the equal opportunities legislation became more balanced over time, occupations that were previously female-dominated remained largely female-dominated (Grant et al., 2004).
Taken together, being cognizant about sex divergent ways of problem solving and decision making in the formal care setting is critical because care provision by males may have qualitative differences compared to females. For instance, while male clinicians tend to focus on disease specific factors, offering problem-focused solutions and technical medical interventions; they are less likely to spend time assuaging patients’ feelings of worries (Bensing et al., 1993; Boerma and van den Brink-Muinen, 2000). On the other hand, female clinicians may focus on the psychoemotional and interpersonal management of the disease such as using counseling approaches (Boerma and van den Brink-Muinen, 2000), and have a greater tendency to provide continued care in the form of more frequent and more follow up consultations (Bensing et al., 1993; Jefferson et al., 2015). Instead of pushing sex equal agendas, it is likely more effective to explore further how different male and female qualities can contribute to the same formal care function.
Discussion
In the current review, we highlight the relevance of using EP theories to understand sex differentiated preferences and competencies for formal care occupations. Sex differences as elucidated by sex-role theorists are based on the observation that many sex differences vary in magnitude across cultures and in few cases are consistent with sex-role theories (Schmitt, 2015). However, this notion has been disconfirmed by cross-cultural research observing persistent sex differences across psychological traits in personality, attitudes and cognitive abilities as predicted by EP theories (Schmitt, 2015). Furthermore, EP theories have the potential to explain why cultural universals and variations can be observed in sex differences (Pirlott and Schmitt, 2014).
While we use EP theories to elucidate the emergence of sex differences in formal care occupations, we do not think that these explanations negate the effects of socialization and culture. In addition, we acknowledge that sex differences in occupational preference may not apply to individuals who are already integrated in a sex atypical field. For instance, while males may gravitate toward things and females toward people, the EP explanations may not apply to individuals who have self-sorted into their preferred (sex atypical) occupations. Further, one should not cast judgments or dissuade individuals from pursuing a particular career path purely based on EP explanations. It may not be feasible to ensure sex parity in every occupation. However, barriers that impede females or males from advancing in the career of their choice (e.g., hiring or pay discrimination between males and females) should be systematically removed or reformed.
Conclusion
Today, psychologists understand that pure social constructivist views are insufficient in explaining sex differences and in some instances lead to incorrect conclusions. Furthermore, evidence is clear that innate tendencies exert considerable cognitive and behavioral outcomes. Thus, giving equal weighs to EP and sociocultural theories clarifies the issues related to sex differences in formal care by enabling the understanding of sex differences as emergent phenomena of the interaction between evolved tendencies and sociocultural pressures. Ultimately, this method of examination will generate more holistic views of sex differences in formal care occupations (see Table 1 for other examples and predictions using the EP analytic approach). We propose that key decision makers within the healthcare and social care sectors work with instead of against sex differences elucidated herein and researchers to be sensitive to innate sex preferences in developing research programs. Ultimately, understanding and accepting sex differences elucidated by EP theories not only enhances our knowledge, it sheds light on how problems and research can be fine-tuned based on more precise and nuanced insights additionally informed by sociocultural theories.
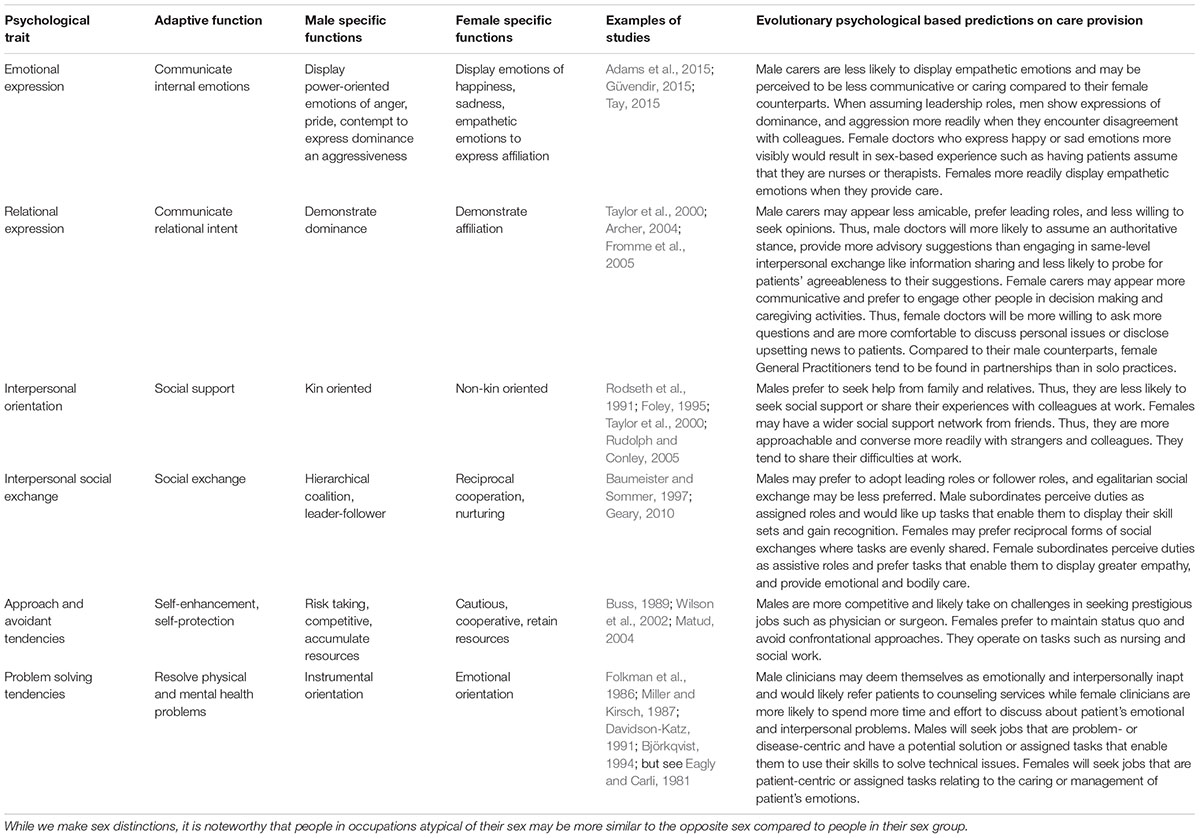
Table 1. Examples of sex differentiated adaptive traits and the predictions for the approach, understanding, and implications of care provision.
Author Contributions
PT contributed to the conceptualization, drafting, and revision of the manuscript. YT and KT conducted the literature, and reviewed and drafted the manuscript.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
Adams, R. B., Hess, U., and Kleck, R. E. (2015). The intersection of gender-related facial appearance and facial displays of emotion. Emot. Rev. 7, 5–13. doi: 10.1177/1754073914544407
Archer, J. (2004). Sex differences in aggression in real-world settings: a meta-analytic review. Rev. Gen. Psychol. 8, 291–322. doi: 10.1037/1089-2680.8.4.291
Bank, B. J., and Hansford, S. L. (2000). Gender and friendship: why are men’s best same-sex friendships less intimate and supportive? Pers. Relationsh. 7, 63–78. doi: 10.1111/j.1475-6811.2000.tb00004.x
Barbee, A. P., Cunningham, M. R., Winstead, B. A., Derlega, V. J., Gulley, M. R., Yankeelov, P. A., et al. (1993). Effects of gender role expectations on the social support process. J. Soc. Issues 49, 175–190. doi: 10.1111/j.1540-4560.1993.tb01175.x
Baumeister, R. F., and Sommer, K. L. (1997). What do men want? Gender differences and two spheres of belongingness: comment on cross and Madson (1997). Psychol. Bull. 12, 38–44. doi: 10.1037//0033-2909.122.1.38
Bensing, J. M., van den Brink-Muinen, A., and de Bakker, D. H. (1993). Gender differences in practice style: a dutch study of general practitioners. Med. Care 31, 219–229. doi: 10.1097/00005650-199303000-00004
Biesele, M., and Barclay, S. (2001). Ju/’hoan women’s tracking knowledge and its contribution to their husbands’ hunting success. Afr. Study Monogr. 26, 67–84.
Bird, R., and Codding, B. (2015). “The Sexual Division of Labor,” in Emerging Trends in the Social and Behavioral Sciences, eds R. Scott and S. Kosslyn (Hoboken, NJ: John Wiley & Sons).
Bjorklund, D. F., and Shackelford, T. K. (1999). Differences in parental investment contribute to important differences between men and women. Curr. Dir. Psychol. Sci. 8, 86–89. doi: 10.1111/1467-8721.00020
Björkqvist, K. (1994). Sex differences in physical, verbal, and indirect aggression: a review of recent research. Sex Roles 30, 177–188. doi: 10.1007/bf01420988
Boerma, W. G., and van den Brink-Muinen, A. (2000). Gender-related differences in the organization and provision of services among general practitioners in europe: a signal to health care planners. Med. Care 38, 993–1002. doi: 10.1097/00005650-200010000-00003
Buddeberg-Fischer, B., Stamm, M., Buddeberg, C., Bauer, G., Hämmig, O., Knecht, M., et al. (2010). The impact of gender and parenthood on physicians’ careers - professional and personal situation seven years after graduation. BMC Health Serv. Res. 10:40. doi: 10.1186/1472-6963-10-40
Buss, D. M. (1989). Sex differences in human mate preferences: evolutionary hypotheses tested in 37 cultures. Behav. Brain Sci. 12, 1–49.
Buss, D. M., and Schmitt, D. P. (2017). “Sexual Strategies Theory,” in Encyclopedia of Evolutionary Psychological Science, eds T. K. Shackelford and V. A. Weekes-Shackelford (Cham: Springer International Publishing), 1–5. doi: 10.1007/978-3-319-16999-6_1861-1
Charles, M., and Bradley, K. (2009). Indulging our gendered selves? sex segregation by field of study in 44 Countries. Am. J. Sociol. 114, 924–976. doi: 10.1086/595942
Darwin, C. (1871). The Descent of Man and Selection in Relation to Sex, Vol. 1. London: John Murray. doi: 10.1086/595942
Davidson-Katz, K. (1991). “Gender roles and health,” in Handbook of Social and Clinical Psychology: The Health Perspective, eds C. Snyder and D. R. Forsyth (Elmsford, NY: Pergamon Press), 179–196.
Dill, K. (2017). Male-Dominated Jobs are Declining, but These 10 are Still Growing. CNBC. Available at: https://www.cnbc.com/2017/04/18/the-10-fastest-growing-male-dominated-jobs.html (accessed November 10, 2018).
Eagly, A. H. (1997). Sex differences in social behavior: Comparing social role theory and evolutionary psychology. Am. Psychol. 52, 1380–1383. doi: 10.1037//0003-066x.52.12.1380.b
Eagly, A. H., and Carli, L. L. (1981). Sex of researchers and sex-typed communications as determinants of sex differences in influenceability: a meta-analysis of social influence studies. Psychol. Bull. 90, 1–20. doi: 10.1037//0033-2909.90.1.1
Eagly, A. H., and Wood, W. (2011). Feminism and the evolution of sex differences and similarities. Sex Roles 64, 758–767. doi: 10.1007/s11199-011-9949-9
Eagly, A. H., and Wood, W. (2013). The nature–nurture debates: 25 years of challenges in understanding the psychology of gender. Persp. Psychol. Sci. 8, 340–357. doi: 10.1177/1745691613484767
Eckel, C. C., and Grossman, P. J. (2008). “Differences in the economic decisions of men and women: Experimental evidence,” in Handbook of Experimental Economics Results, Vol. 1, eds C. R. Plott and V. L. Smith (Linacre House: Elsevier), 509–519. doi: 10.1016/s1574-0722(07)000571
Evans, J. (2004). Men nurses: a historical and feminist perspective. J. Adv. Nurs. 47, 321–328. doi: 10.1111/j.1365-2648.2004.03096.x
Ferriman, K., Lubinski, D., and Benbow, C. P. (2009). Work preferences, life values, and personal views of top math/science graduate students and the profoundly gifted: developmental changes and gender differences during emerging adulthood and parenthood. J. Pers. Soc. Psychol. 97, 517–532. doi: 10.1037/a0016030
Fieder, M., and Huber, S. (2007). The effects of sex and childlessness on the association between status and reproductive output in modern society. Evol. Hum. Behav. 28, 392–398. doi: 10.1016/j.evolhumbehav.2007.05.004
Foley, R. (1995). The adaptive legacy of human evolution: a search for the environment of evolutionary adaptedness. Evol. Anthropol. 4, 194–203. doi: 10.1002/evan.1360040603
Folkman, S., Lazarus, R. S., Dunkel-Schetter, C., DeLongis, A., and Gruen, R. J. (1986). Dynamics of a stressful encounter: cognitive appraisal, coping, and encounter outcomes. J. Pers. Soc. Psychol. 50, 992–1003. doi: 10.1037//0022-3514.50.5.992
Fromme, E. K., Drach, L. L., Tolle, S. W., Ebert, P., Miller, P., Perrin, N., et al. (2005). Men as caregivers at the end of life. J. Palliat. Med. 8, 1167–1175.
Frost, P. (1998). Sex differences may indeed exist for 3-D navigational abilities: but was sexual selection responsible? Behav. Brain Sci. 21, 443–444.
Geary, D. C. (2010). Male, Female: The Evolution of Human Sex Differences, 2nd Edn. Washington, DC: American Psychological Association.
Grant, V. J., Robinson, E., and Muir, P. (2004). Sex ratios in healthcare occupations: population based study. BMJ 328, 141–142. doi: 10.1136/bmj.328.7432.141
Gupta, N., Diallo, K., Zurn, P., and Dal Poz, M. R. (2003). Assessing human resources for health: what can be learned from labour force surveys? Hum. Res. Health 1:5. doi: 10.1186/1478-4491-1-5
Güvendir, E. (2015). Why are males inclined to use strong swear words more than females? An evolutionary explanation based on male intergroup aggressiveness. Lang. Sci. 50, 133–139. doi: 10.1016/j.langsci.2015.02.003
Hannawi, S., and Al Salmi, I. (2018). Time to address gender inequalities against female physicians. Int. J. Health Plan. Manag. 33, 532–541. doi: 10.1002/hpm.2476
Hojat, M., Gonnella, J. S., Nasca, T. J., Mangione, S., Veloksi, J. J., and Magee, M. (2002). The jefferson scale of physician empathy: further psychometric data and differences by gender and specialty at item level. Acad. Med. 77, S58–S60.
Hojat, M., Zuckerman, M., Magee, M., Mangione, S., Nasca, T., Vergare, M., et al. (2005). Empathy in medical students as related to specialty interest, personality, and perceptions of mother and father. Pers. Individ. Diff. 39, 1205–1215. doi: 10.1016/j.paid.2005.04.007
Hopcroft, R. L. (2006). Sex, status, and reproductive success in the contemporary United States. Evol. Hum. Behav. 27, 104–120. doi: 10.1016/j.evolhumbehav.2005.07.004
Hurtado, A. M., Hawkes, K., Hill, K., and Kaplan, H. (1985). Female subsistence strategies among Ache hunter-gatherers of Eastern Paraguay. Hum. Ecol. 13, 1–28. doi: 10.1007/bf01531086
Jefferson, L., Bloor, K., and Spilsbury, K. (2015). Exploring gender differences in the working lives of UK hospital consultants. J. R. Soc. Med. 108, 184–191. doi: 10.1177/0141076814558523
Kenrick, D. T. (2012). The 7 Worst Things About Being a Male: The Psychological Burdens of Carrying Around a Y Chromosome Psychology Today. New York, NY: Sussex Publishers, LLC. doi: 10.1177/0141076814558523
Ku, M. C. (2011). When does gender matter?:gender differences in specialty choice among physicians. Work Occup. 38, 221–262. doi: 10.1177/0730888410392319
Lippa, R. A. (1998). Gender-related individual differences and the structure of vocational interests: the importance of the people–things dimension. J. Pers. Soc. Psychol. 74, 996–1009. doi: 10.1037/0022-3514.74.4.996
Lippa, R. A. (2005). Sexual orientation and personality. Ann. Rev. Sex Res. 16, 119–153. doi: 10.1080/10532528.2005.10559831
Lippa, R. A. (2008). Sex differences and sexual orientation differences in personality: findings from the bbc internet survey. Arch. Sex. Behav. 37, 173–187. doi: 10.1007/s10508-007-9267-z
Lippa, R. A. (2010). Sex differences in personality traits and gender-related occupational preferences across 53 nations: testing evolutionary and social-environmental theories. Arch. Sex. Behav. 39, 619–636. doi: 10.1007/s10508-008-9380-7
Low, B. S., Simon, C. P., and Anderson, K. G. (2002). An evolutionary ecological perspective on demographic transitions: Modeling multiple currencies. Am. J. Hum. Biol. 14, 149–167. doi: 10.1002/ajhb.10043
Lowe, W. (2011). “Silences in healthcare education and practice: Gender and sexuality,” in Gay and Lesbian Issues and Psychology Review, Vol. 7, ed. D. W. Riggs (Melbourne: The Australian Psychological Society), 180–190.
Marlowe, F. W. (2007). Hunting and gathering the human sexual division of foraging labor. Cross Cult. Res. 41, 170–195. doi: 10.1177/1069397106297529
Matud, M. P. (2004). Gender differences in stress and coping styles. Pers. Individ. Diff. 37, 1401–1415. doi: 10.1016/j.paid.2004.01.010
McKinstry, B. (2008). Are there too many female medical graduates? Yes. BMJ 336, 748–748. doi: 10.1136/bmj.39505.491065.94 Available at: Singapore: http://stats.mom.gov.sg/Pages/Singapore-Yearbook-Of-Manpower-Statistics-2018-Labour-Force.aspx (accessed November 10, 2018).
Miller, S. M., and Kirsch, N. (1987). “Sex differences in cognitive coping with stress,” in Gender & Stress, eds R. Barnett, L. Biener, and G. Baruch (New York, NY: The Free Press), 278–307.
Ministry of Manpower (2018). Singapore Yearbook of Manpower Statistics 2018: Labour Force Table(s). Available at: Singapore: http://stats.mom.gov.sg/Pages/Singapore-Yearbook-Of-Manpower-Statistics-2018-Labour-Force.aspx
Murdock, G. P., and Provost, C. (1973). Factors in the division of labor by sex: a cross-cultural analysis. Ethnology 12, 203–225. doi: 10.2307/3773347
O’Connor, T. (2015). Men choosing nursing:negotiating a masculine identity in a feminine world. J. Men’s Stud. 23, 194–211. doi: 10.1177/1060826515582519
Pirlott, A. G., and Schmitt, D. P. (2014). “Gendered sexual cultures,” in Culture Reexamined: Broadening our Understanding of Social and Evolutionary Influences, ed. A. Cohen (Washington, DC: American Psychological Association), 191–215. doi: 10.1037/14274-007
Puts, D. A. (2010). Beauty and the beast: mechanisms of sexual selection in humans. Evol. Hum. Behav. 31, 157–175. doi: 10.1016/j.evolhumbehav.2010.02.005
Riska, E. (2011). Gender and medical careers. Maturitas 68, 264–267. doi: 10.1016/j.maturitas.2010.09.010
Rocheleau, M. (2017). Chart: The Percentage of Women and Men in Each Profession. Available at: https://www.bostonglobe.com/metro/2017/03/06/chart-the-percentage-women-and-men-each-profession/GBX22YsWl0XaeHghwXfE4H/story.html (accessed November 10, 2018).
Rodseth, L., Wrangham, R. W., Harrigan, A. M., Smuts, B. B., Dare, R., Fox, R., et al. (1991). The human community as a primate society. Curr. Anthropol. 32, 221–254.
Rudolph, K. D., and Conley, C. S. (2005). The socioemotional costs and benefits of social-evaluative concerns: do girls care too much? J. Pers. 73, 115–138. doi: 10.1111/j.1467-6494.2004.00306.x
Schmitt, D. P. (2015). “The Evolution of Culturally-Variable Sex Differences: Men and Women Are Not Always Different, but When They Are…It Appears Not to Result from Patriarchy or Sex Role Socialization,” in The Evolution of Sexuality, eds T. K. Shackelford and R. D. Hansen (Cham: Springer International Publishing), 221–256. doi: 10.1007/978-3-319-09384-0_11
Simpson, R. (2007). “Emotional labour and identity work of men in caring roles,” in Gendering Emotions in Organizations, eds P. Lewis and R. Simpson (New York: Palgrave), 57–73.
Stoet, G. (2011). Sex differences in search and gathering skills. Evol. Hum. Behav. 32, 416–422. doi: 10.1016/j.evolhumbehav.2011.03.001
Stoet, G., and Geary, D. C. (2018). The gender-equality paradox in science, technology, engineering, and mathematics education. Psychol. Sci. 29, 581–593. doi: 10.1177/0956797617741719
Su, R., Rounds, J., and Armstrong, P. I. (2009). Men and things, women and people: a meta-analysis of sex differences in interests. Psychol. Bull. 135, 855–884. doi: 10.1037/a0017364
Tay, P. K. C. (2015). The adaptive value associated with expressing and perceiving angry-male and happy-female faces. Front. Psychol. 6:851. doi: 10.3389/fpsyg.2015.00851
Taylor, S. E., Klein, L. C., Lewis, B. P., Gruenewald, T. L., Gurung, R. A., and Updegraff, J. A. (2000). Biobehavioral responses to stress in females: tend-and-befriend, not fight-or-flight. Psychol. Rev. 107, 411–429. doi: 10.1037//0033-295x.107.3.411
Vanwesenbeeck, I. (2009). Doing gender in sex and sex research. Arch. Sex. Behav. 38, 883–898. doi: 10.1007/s10508-009-9565-8
Wilson, M., Daly, M., and Pound, N. (2002). “An evolutionary psychological perspective on the modulation of competitive confrontation and risk-taking,” in Hormones, Brain and Behavior, eds D. Pfaff, A. Arnold, A. Etgen, S. Fahrbach, and R. Rubin (San Diego, CA: Academic Press), 381–408. doi: 10.1016/b978-012532104-4/500962
Keywords: sex differences, occupation, sexual strategies theory, sexual division of labor, care styles
Citation: Tay PKC, Ting YY and Tan KY (2019) Sex and Care: The Evolutionary Psychological Explanations for Sex Differences in Formal Care Occupations. Front. Psychol. 10:867. doi: 10.3389/fpsyg.2019.00867
Received: 12 December 2018; Accepted: 02 April 2019;
Published: 17 April 2019.
Edited by:
María del Carmen Pérez-Fuentes, University of Almería, SpainReviewed by:
Cristina García-Ael, National University of Distance Education (UNED), SpainM. Teresa Anguera, University of Barcelona, Spain
Scott William Semenyna, University of Lethbridge, Canada
Copyright © 2019 Tay, Ting and Tan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Peter Kay Chai Tay, cGV0ZXIudGF5LnJlc2VhcmNoQGdtYWlsLmNvbQ==