 Ekaterina Kuzmina
Ekaterina Kuzmina Mira Goral
Mira Goral Monica Norvik
Monica Norvik Brendan S. Weekes
Brendan S. Weekes
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychol., 04 April 2019
Sec. Psychology of Language
Volume 10 - 2019 | https://doi.org/10.3389/fpsyg.2019.00445
This article is part of the Research TopicWords in the WorldView all 18 articles
Patterns of language impairment in multilingual speakers with post-stroke aphasia are diverse: in some cases the language deficits are parallel, that is, all languages are impaired relatively equally, whereas in other cases deficits are differential, that is, one language is more impaired than the other(s). This diversity stems from the intricate structure of the multilingual language system, which is shaped by a complex interplay of influencing factors, such as age of language acquisition, frequency of language use, premorbid proficiency, and linguistic similarity between one's languages. Previous theoretical reviews and empirical studies shed some light on these factors, however no clear answers have been provided. The goals of this review were to provide a timely update on the increasing number of reported cases in the last decade and to offer a systematic analysis of the potentially influencing variables. One hundred and thirty cases from 65 studies were included in the present systematic review and effect sizes from 119 cases were used in the meta-analysis. Our analysis revealed better performance in L1 compared to L2 in the whole sample of bilingual speakers with post-stroke aphasia. However, the magnitude of this difference was influenced by whether L2 was learned early in childhood or later: those who learned L2 before 7 years of age showed comparable performance in both of their languages contrary to the bilinguals who learned L2 after 7 years of age and showed better performance in L1 compared to L2. These robust findings were moderated mildly by premorbid proficiency and frequency of use. Finally, linguistic similarity did not appear to influence the magnitude of the difference in performance between L1 and L2. Our findings from the early bilingual subgroup were in line with the previous reviews which included mostly balanced early bilinguals performing comparably in both languages. Our findings from the late bilingual subgroup stressed the primacy of L1 and the importance of age of L2 learning. In addition, the evidence from the present review provides support for theories emphasizing the role of premorbid proficiency and language use in language impairment patterns in bilingual aphasia.
Aphasia describes a multitude of acquired language impairment resulting from brain injury, most often but not exclusively following a stroke. Bilinguals are individuals who use more than one language on a regular basis (Grosjean, 2013). Reports of individuals with bilingual aphasia have emerged as an important constraint on theories of the neurobiology of language (Gollan and Kroll, 2001; Ullman, 2001; Abutalebi et al., 2009; Miozzo et al., 2010; Weekes, 2010). Studies of bilingual aphasia began with anecdotal case studies reported by Ribot (1882) and Pitres (1895/1983). However, the wider theoretical implications of these cases are only more obvious today with the advent of sophisticated models of bilingual language processing. Two enduring questions in the field are whether a first-acquired language (L1) is less vulnerable to brain damage compared with later-learned languages (L2), and whether a language that is used more often premorbidly can be privileged after injury. Ribot's law holds that earlier acquired memories (including linguistic) are more resistant to brain damage whereas Pitres' law assumes that the premorbidly dominant language will be less vulnerable, independent of the age of acquisition (AoA) of that language. A related question is whether the cognitive and neural representations for L1 and L2 are shared or depend on different cognitive and neural mechanisms (e.g., Chee et al., 1999, 2000; Abutalebi et al., 2001; Ullman, 2001; Green, 2003; Perani and Abutalebi, 2005; Giussani et al., 2007). In our view, answers to these questions can be revealing for theories of the neurobiology of language (e.g., Libben, 2017) as well as for the design of intervention for language impairments in multilingual speakers in a variety of contexts, including immigrants and refugees across the globe (Pot et al., 2018).
The evidence emerging from studies of bilingual individuals who are recovering language function after a stroke shows that both early acquisition and premorbid language dominance contribute to language recovery and should constrain therapy (Lorenzen and Murray, 2008; Faroqi-Shah et al., 2010; Knoph, 2013; Conner et al., 2018). In many instances, equivalent patterns of aphasia in all languages spoken premorbidly are assumed, an assumption that implies shared cognitive and neural representations for these languages. The shared bilingual neural substrate (SBNS) hypothesis specifically assumes that bilingual speakers who acquire L2 early in life have a common neural network with shared lexical-semantic and syntactic representations from each language in the brain (Miozzo et al., 2010; Costa et al., 2012; Nadeau, 2019). This assumption is compatible with cognitive neuropsychological models of typical bilingual language processing (Gollan and Kroll, 2001; Faroqi-Shah and Waked, 2010) and with the view that linguistic differences between languages spoken premorbidly do not matter. One prediction from these accounts is that brain damage from stroke will result in equivalent impairment for bilingual speakers in any two languages spoken premorbidly (Paradis, 2004; Weekes, 2010).
Methodological limitations in the sampling of multilingual people with aphasia reported in previous reviews, as detailed below, and the generally accepted view that L2 processing is moderated by AoA (for a review see Abutalebi, 2008), lead us to conjecture that language status (L1 vs. L2) would be a significant predictor of language impairment after stroke for bilingual speakers. According to the convergence hypothesis proposed by Green (2003), which is consistent with the SBNS, dissociations observed in bilingual speakers between L1 and L2 could reflect greater recruitment of cognitive resources assumed to be necessary to process an explicitly learned language (L2), rather than differential neuronal representations (see Chee et al., 1999, 2000; Ullman, 2001). Furthermore, the dominance of language use in the linguistic environment of a person with aphasia will have an impact upon the patterns of aphasia after stroke, according to Pitres' law (Goral et al., 2012; see also Gollan et al., 2015). Therefore, there is merit to explore the roles that AoA, premorbid language proficiency and use, as well as language similarity have on performance in bilingual speakers after a stroke.
The goal of the present meta-analysis is thus to examine what constrains language impairment following stroke in multilingual speakers, and specifically, to investigate whether AoA, premorbid language proficiency, use and exposure, as well as linguistic similarity between spoken languages determine reported patterns of aphasia in L1 and L2.
Decades of research show that language difficulties associated with aphasia are highly selective and can affect only one language modality (e.g., comprehension vs. production) or linguistic aspect (e.g., syntactic processing). Many persons living with aphasia are multilingual (Roberts and Kiran, 2007; Ansaldo and Saidi, 2014). When a multilingual speaker has aphasia following a stroke, the languages spoken premorbidly may show comparable or differential patterns of impairment (Paradis, 2004; Weekes, 2010). Differential patterns may manifest as greater impairment in one language compared to another, or as differences in the characteristics of aphasia. The reasons for differential impairments are less certain. Theories of differential language processing and of impaired mechanisms of language control have been put forward to account for the patterns observed (e.g., Ullman, 2001; Abutalebi and Green, 2008). Furthermore, research shows that AoA, premorbid language proficiency, use and exposure, as well as linguistic similarity between spoken languages influence patterns of differential impairment observed in multilingual aphasia (e.g., Fabbro, 2001; Paradis, 2001, 2004; Lorenzen and Murray, 2008; Goral et al., 2012, 2013).
Previous reviews asked whether multilingual speakers with aphasia evidence comparable levels of language impairment in all languages spoken premorbidly. For example, Albert and Obler (1978) reviewed 108 cases of multilingual aphasia and found comparable distributions of parallel and non-parallel impairment among those who were early “compound” bilinguals and those who learned their L2 later in life. Their review demonstrated no dominant pattern of results supporting only Ribot's law or only Pitres' law, and that variables, such as age, age of language acquisition, and education influenced the outcome.
Paradis (2001) reviewed 132 cases published in the period from 1990 to 1999 and found that 81 cases (61%) showed parallel impairment in both languages [“when both (or all) languages are similarly impaired and restored at the same rate,” p. 70], 24 (18%) had differential impairment (“impairment is of different degree in each language relative to premorbid mastery,” p. 70), and the remainder was shared by 12 cases (9%) with blended impairment (“when patients systematically mix or blend features of their languages at any all levels of linguistic structure,” p. 70), 9 cases (7%) with selective impairment (“when patients do not regain the use of one or more of their languages,” p. 70), and 6 cases (5%) with successive impairment (“when one language does not begin to reappear until another has been maximally recovered,” p. 70). It is important to notice that the distribution of the impairment pattern percentages in this review was highly influenced by the two relatively large group studies from which 99 cases (75%) were taken. In the first study by Junqué et al. (1995), impairment patterns of 50 early equally proficient Catalan-Spanish aphasic bilinguals with unequal premorbid frequency of language use were reported. In the second one by Vilariño et al. (1997), comparable impairment corresponding to premorbid proficiency was reported as the most frequent pattern based on the assessment of 49 early Galician-Spanish bilinguals with aphasia. Thus, the majority (75%) of the 132 cases included in the Paradis (2001) review were early, relatively balanced bilingual speakers of two closely related languages. Additionally, it is important to note that, firstly, the reviewed cases were of varying etiology (e.g., stroke, tumor), secondly, it was not systematically specified what language performance measures were used for assessment, and, finally, the criteria for making a decision about the comparability of impairments in both languages were not explicitly defined.
Fabbro (2001) used the Bilingual Aphasia Test (BAT, Paradis and Libben, 1987) to assess 20 Friulian-Italian early (L2 learned between 5 and 7 year) bilingual speakers with aphasia, who premorbidly used both languages on a regular basis and had a stroke from 1 to 96 months before the assessment. Premorbid proficiency of the participants was not directly assessed, the author allegedly assumed that all participants were equally proficient in both languages. According to the author's interpretation of the results, 13 participants (65%) had comparable impairments in both languages, 4 participants (20%) performed significantly worse in L2, and 3 participants (15%) performed significantly worse in L1 (We note that for one of these three last participants, p-value was 0.07 indicating the absence of significant differences.) The researcher concluded that these percentages were in line with the previous review by Paradis (2001). However, Fabbro's study included early balanced (having comparable premorbid proficiency in both languages) bilinguals only. Moreover, decisions about the difference between performance in L1 and L2 were made based on running significance tests separately for each of 20 participants, subjecting the results to a Type I error (overestimation of significant difference).
Other reviews have identified additional relevant variables. In their review, Lorenzen and Murray (2008) suggested that language similarity (proportion of cognates shared) was a significant constraint on language recovery in bilingual speakers after stroke. Ansaldo et al. (2008) argued, as others have earlier (see Paradis, 2004), that motivation impacts on recovery. Overall, extant reviews suggest that equivalent patterns of language impairment in bilingual aphasia are more common, but a large minority of cases do show differential or selective patterns of impairment. These reviews also highlight the variables that predict recovery in post-stroke bilingual aphasia: AoA, language proficiency, language use, and linguistic similarity.
AoA refers to the age at which people learn language. It has long been argued that words acquired at an early age are the ones that are most preserved in aphasia (Rochford and Williams, 1965; Brysbaert and Ellis, 2016; Bakhtiar et al., 2017) although experimental evidence has been mixed, with some later-learned words found to be more easily retrieved in some cases of aphasia (e.g., Goral et al., 2013). Much research has studied the question of whether languages that are learned later in childhood or in adulthood, as compared to early acquired first language(s), are organized or processed by different neural mechanisms (this discussion is beyond the scope of this paper but see Ullman, 2001; Birdsong, 2006; Abutalebi and Green, 2007 among others). In the literature on bilingual aphasia, most reports highlight the age in which the languages spoken were first acquired (e.g., for all 130 cases included in this review).
Whereas this question preoccupied early reviews (Albert and Obler, 1978; Junqué et al., 1995), relatively few recent studies of bilingual aphasia explicitly addressed the role of age of language learning on language impairment. Among those who did, Tschirren et al. (2011) found no evidence of differential performance in their late bilinguals, suggesting that late learning of L2 is not always an impediment after a stroke. They did, however, find that AoA had an impact on syntactic processing in the two languages. Other studies have found lower performance in a later-learned language than earlier-acquired ones despite pre-aphasia high levels of proficiency (e.g., Goral et al., 2006; Kiran and Iakupova, 2011; Kurland and Falcon, 2011). However, as noted by these authors, levels of premorbid proficiency in all languages spoken is difficult to assess. We address this issue next.
To determine language impairments in multilingual speakers with aphasia one needs to estimate their premorbid proficiency in these languages. However, premorbid language proficiency can only be estimated indirectly primarily via subjective ratings. Several questionnaires have been developed to elicit such ratings (Paradis and Libben, 1987; Muñoz and Marquardt, 2003; Kiran et al., 2010), but it has been demonstrated that self-ratings are not completely consistent with objective measures (Tomoschuk et al., 2018). Therefore, having no access to objective measures of proficiency prior to brain damage is a limitation. Recent studies have examined the notion that levels of language proficiency are highly related to levels of language exposure and use, suggesting that understanding patterns of language use could augment decisions about degree of language proficiency when only subjective measures are available (Kiran and Tuchtenhagen, 2005).
Multilinguals are likely to attain and maintain high proficiency in languages they use regularly and frequently, especially if these languages are spoken in their living environment. When one language or more is not used, it could undergo processes of reduced activation and attrition (Köpke et al., 2007). Furthermore, living in the environment where one language is predominantly used can lead to inhibition of less used languages in immersed L2 learners (Linck et al., 2009). Thus, it can be assumed that the linguistic context at the time of the stroke can contribute to better perseverance and/or recovery of the relevant language in people with aphasia. In several studies, findings pointed to the role of the linguistic environment on the response to therapy (Goral et al., 2012, 2013), which are consistent with the importance of language context in addition to age of acquisition and language proficiency.
Differential performance between languages that are linguistically similar (e.g., Friulian and Italian) may be surprising but is in fact reported. Less expected is equivalent patterns of aphasia in languages that are linguistically different (e.g., Chinese and English). One reason for these reports is that manifestations of aphasia syndromes (e.g., agrammatism) are not possible in some languages and therefore similar patterns in linguistically different languages will not be observed (Weekes, 2010). Similarly, it is possible that different constraints that characterize linguistic systems (e.g., the depth of an orthography or complexity of morphology) will produce differential patterns of recovery (see Menn and Obler, 1990; Paradis, 2001; Weekes, 2005, 2012). When languages are similar in terms of their cognates (words that have a similar meaning and form in different languages), for example, Spanish and Catalan, linguistic distance is relatively small compared to languages without cognates, for example, Spanish and Mandarin. Despite this, selective impairments can be seen between linguistically similar languages.
Linguistic similarity has been associated with recovery in bilingual aphasia (Kohnert, 2004; Kendall et al., 2015). However, competition between cognates has also been observed (e.g., Kurland and Falcon, 2011). Linguistic similarity has been considered when testing differential impairment across languages. For example, Roberts and Deslauriers (1999) found that a group of 15 early balanced French-English bilinguals with aphasia were more accurate at naming pictures representing cognates compared to noncognates. As well, Goral et al. (2010) found cross-language effects from linguistic structures that were similar across languages but not for aspects that were different between languages of a trilingual speaker with aphasia. Similarly, Fabbro (2001) reported the most common error among Friulian-Italian bilinguals with aphasia when producing Friulian was pronoun omission, which is acceptable in many instances in Italian but ungrammatical in Friulian.
We note that the concept of linguistic similarity has been ill-defined in the literature. In the study of second or third language learning, one approach [Typological Primacy Model (TPM); Rothman, 2015] seeks to define language typology based on structural similarities and differences, rather than on the basis of language families and historical linguistics. In studies of bilingual language processing language similarities at the lexical level has been discussed with respect to the concept of cognates (e.g., Schepens et al., 2013). In most papers on bilingual aphasia no formal definition is offered (e.g., Ansaldo and Saidi, 2014).
Whether the first language of bilingual speakers who acquire aphasia is more likely to be better preserved, and the identification of the influencing variables that may moderate this outcome is not only interesting theoretically but is also critical to clinical practices. Language and communication assessment in aphasia may not reveal an accurate picture unless the individuals are assessed in all their languages and unless detailed information about their language history and use is obtained. Moreover, decisions about the language in which intervention is best conducted could be informed by evidence about relative degrees of impairments in the languages of the person with aphasia. There is a growing body of treatment studies that examine the effectiveness of intervention in aphasia depending on the language in which the treatment is delivered. Current findings are equivocal regarding the variables (premorbid proficiency, AoA, language use) that affect therapy outcome and cross-language generalization (e.g., Goral, 2012; Kiran et al., 2013a,b; Nadeau, 2019).
Aphasia is multidimensional and rarely presents as a pure syndrome in neurology (Caramazza, 1984; Caramazza and McCloskey, 1988; Nickels et al., 2011). Studies of bilingual speakers with aphasia—who are necessarily idiosyncratic in their language background—are ipso facto unique. It is therefore hardly surprising to find a majority of research in bilingual aphasia are case studies. Criticisms of case reports are longstanding, plentiful and still topical (Shallice, 1979; Caplan, 1988; McCloskey and Caramazza, 1988; Coltheart, 2017) and are not limited to the field of aphasia and have been usurped by the so called case-series approach (Schwartz and Dell, 2010; Lambon Ralph et al., 2011; Rapp, 2011). The defining quality of the case-series is the capacity to use patterns of covariance to understand underlying cognitive mechanisms, including key elements: a reasonable sample size suitable for identifying complex trends in idiosyncratic data; administration of a common set of cognitive tests; and open criteria for defining a sample motivated by theoretical questions or clinical and neuroanatomical criteria (Rapp, 2011). The single case is commonly associated with the universality assumption that characterizes “orthodox” cognitive neuropsychology (Caramazza, 1986), while the case-series approach is prima facie more compatible with the assumptions of “population thinking” (Bub, 2011). As Rapp (2011) notes despite the increase in “population thinking,” little work has been done in aphasia to understand the extent and nature of individual variability with regard to the types of cognitive mechanisms commonly investigated in cognitive psychology and neuroscience.
In this meta-analysis we attempt to honor the variability presented in the case studies and the case-series, and at the same time extract patterns that transcend the variability and allow us to generalize from the existing literature. Given the theoretical questions raised about the neurobiology of language and the above-mentioned reports about potential predictors of impairments in aphasia in bilingual speakers, we aimed to answer the five following research questions:
1) Do bilingual speakers with post-stroke aphasia show a difference in performance between the language acquired first (L1) and the later learned language (L2)?
2) Are the possible differences between L1 and L2 of different magnitude between early bilinguals and late bilinguals? Does AoA as a continuous variable moderate the outcomes in the early and late bilingual subgroups separately?
3) Does premorbid language proficiency moderate the possible differences between L1 and L2?
4) Does frequency of language use moderate the possible differences between L1 and L2?
5) Does linguistic similarity between the languages spoken by the bilingual moderate the possible differences between L1 and L2?
The following electronic databases were searched: PubMed, Science Direct, PsycINFO, CINAHL, TAYLOR, and FRANCIS Online. Five construct-related search terms (multilingual, bilingual, trilingual, quadrilingual, polyglot) and seven population-related search terms (aphasia, language disorder, language impairment, anomia, stroke, vascular, hemorrhage) were used. The search was limited to peer-reviewed papers published in the period from 2000 until 2018 and written in English. The search strings adapted for each database are reported in the Supplementary Material. First, titles of search hits were screened to define the relevance of a study to the review. Second, abstracts and method sections of results were screened for matching inclusion criteria.
Papers reporting behavioral accuracy data on language performance of multilingual persons with post-stroke aphasia were included for complete screening.
Two inclusion criteria related to participants were used. The first criterion was presence of aphasia resulting from a single cerebrovascular accident. Participants with aphasia of other etiologies (e.g., tumor, head injury, dementia) were excluded. The second criterion was the bilingual or multilingual status of participants. The categorization of participants as bilinguals or multilinguals by an author was used to decide whether to include participants into the review. Although variation in the definitions of bilingualism/multilingualism used by different authors can be assumed, all of the included participants could be described as persons who used more than one language to communicate on a regular basis in everyday life before the stroke. This was done to ensure that a participant had at least sufficient proficiency for everyday conversation prior to their stroke (B1 level according to the Common European Framework of Reference for Languages). Thus, the operational definition of bilingualism/multilingualism was primarily based on a criterion of premorbid language use (Grosjean, 1982). For participants whose performance was reported in several papers, information was taken from all of the papers, if the assessment time was equivalent. When the same person was described in multiple papers at different data points, the earliest performance was coded. Five studies reported data on more than two languages of the participants. For all of these cases, performance in L1 and the most frequently used language were extracted and analyzed. If several L2s were equally used, the earlier acquired language was chosen for the analysis.
Three inclusion criteria related to tests were also used. The first criterion was that a test should directly measure language performance (e.g., auditory syntactic comprehension, picture naming, reading aloud). Studies reporting performance only on tests indirectly measuring language performance (e.g., Color-Word Stroop) were not included. The second criterion was that reported performance was shown as correct responses out of the total number of tested items in various language tasks. Cases where accuracy was reported in percentages in a way that the total number of tested items in the task could not be estimated were excluded. Those studies where the total number of items used in the test was not reported, but a published test had this information (e.g., the Bilingual Aphasia Test) were included. The third criterion was the reported performance (accuracy and total number of items in the task) included data from more than one language. Cases were performance in only one language was reported were not included. After screening, 65 studies were included in the final dataset. Figure 1 shows the details of the literature search and screening process with resulting number of studies.
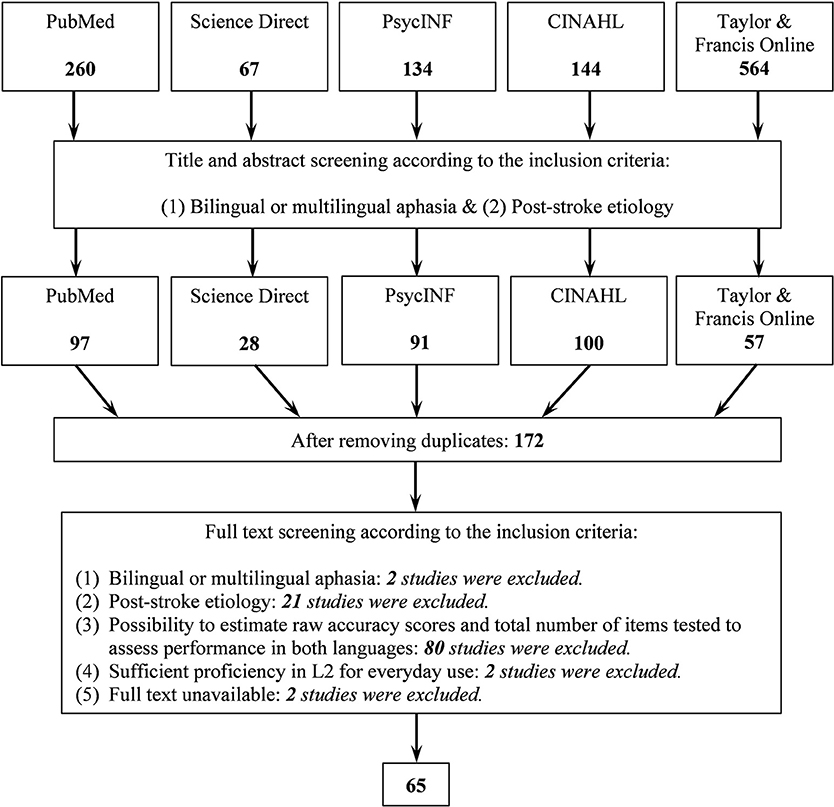
Figure 1. Flowchart of the search process. Numbers show how many studies were included at each stage.
Cases from the finally selected studies were coded according to the three study-related variables (first author or the first two authors, year of publication, first five words of the title), seven clinico-demographic case-related variables (gender, age in years at the time of assessment, years of education, month post onset at the assessment, type and severity of aphasia, lesion side), four language background variables (age of L2 acquisition, premorbid language proficiency, language use, linguistic similarity between languages), three test-related variables (test name, testing paradigm, language modality assessed by the test), and four language performance variables (numbers of items correctly performed in L1 in a specific test, total number of items in the test used to assess L1, number of items correctly performed in L2 in a specific test, total number of items in the test used to assess L2).
Coding of several above mentioned variables requires elaboration. Age of L2 acquisition was coded either as a number if it was directly reported as such, or as a time period (i.e., early childhood, primary school, later than early childhood, high school, early adulthood, adulthood) if it was directly reported or could be inferred from case descriptions. Based on the age of L2 acquisition variable, we created an adjusted variable, where we transformed categorical labels into numbers according to the following criteria: early childhood = 3 year, primary school = 7 year, later than early childhood = 10 year, high school = 14 year, early adulthood = 20 year, adulthood = 25 year. This adjustment allowed us to perform the moderator analysis treating AoA as a continuous variable.
Language proficiency was coded using three levels, namely “higher in L1,” “equal,” “higher in L2” proficiency, based on the information from case descriptions. Language use was coded based on the information from the cases using also three levels, namely “more in L1,” “equal,” “more in L2” use. To assist the coding of the language use variable, we additionally coded the following variables: language used (1) to communicate with parents, (2) with other relatives, (3) with a partner, (4) with children, (5) with friends, (6) in school as an instruction language, (7) in further education as an instruction language, (8) as a subject of formal language classes, (9) at work, (10) for reading, (11) for writing, (12) to watch TV and listen to the radio, (13) based on a self-report, (14) for therapy, (15) in the environment as an official language. These variables were used to facilitate the decision on the language use variable.
The linguistic similarity variable was coded based on how far languages are located from each other in the language family classification in two ways (rather than using for instance the TPM Rothman, 2015, which is less feasible for a meta-analysis of this scope). Firstly, language pairs from different families (e.g., English is from Indo-European family and Chinese is from Sino-Tibetan family) were coded with the level “different,” whereas all other pairs represented the “similar” level. Secondly, to make the coding of the linguistic similarity variable more precise, the three-level coding was applied: (1) language pairs from different families were coded “different” (e.g., English and Chinese), (2) language pairs which shared only the same family were coded “close” (e.g., German and Spanish), and finally, (3) language pairs which shared more than the same family were coded “very close” (i.e., English-Norwegian, Cantonese-Mandarin, Spanish-Catalan, Afrikaans-English, Malayalam-Kannada, English-Dutch, Yiddish-English, Balochi- Persian, Spanish-Italian, Italian-French, Kurdish-Persian, Spanish-French, Galician-Spanish).
Performance scores were recorded separately for each test (e.g., object naming, reading aloud words, syntactic auditory comprehension). Table 1 represents the variety of the tests included in the analysis. For tests without a defined maximum score from the spontaneous and semi-spontaneous production testing paradigm, numbers of correct information units, and corresponding total numbers of units were used as measures.
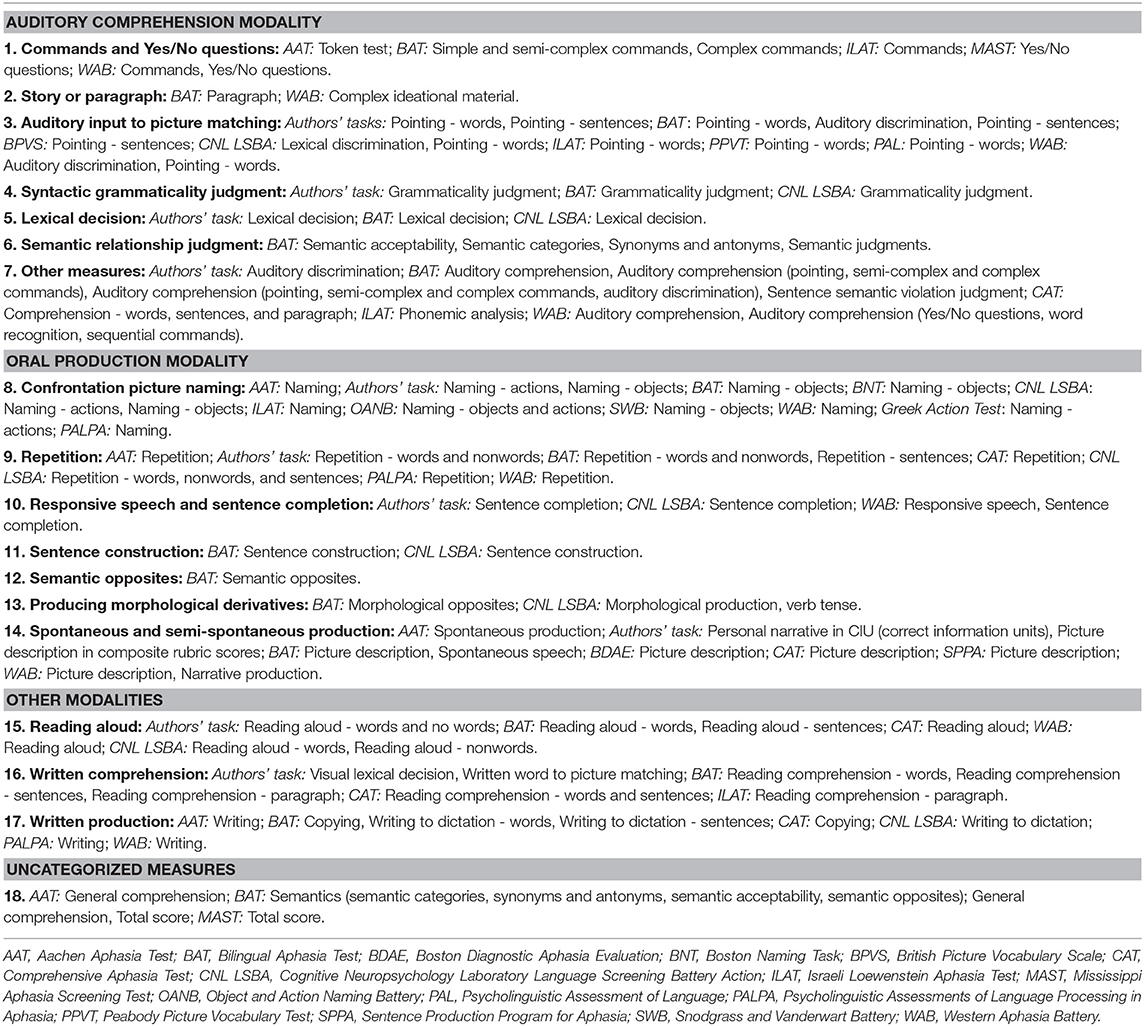
Table 1. Summary of the included modalities, testing paradigms, and tests.
In the majority of the studies, participants were assessed with multiple tests. Firstly, scores from the individual tests were pooled together based on 18 testing paradigms summarized in Table 1. Then, scores from testing paradigms were pooled together based on the two main language modalities, namely auditory comprehension and oral production. Thus, seven testing paradigms (i.e., auditory comprehension of commands and yes/no questions, auditory comprehension of a story or paragraph, auditory based pointing, auditory syntactic grammaticality judgment, auditory lexical decision, auditory semantic relationship judgment, and other scores including sums of auditory comprehension related tests) were pooled together into auditory comprehension scores. Seven other testing paradigms (i.e., confrontation picture naming, repetition, responsive speech and sentence completion, sentence construction, oral production of semantic opposites, oral production of morphological derivatives, spontaneous and semi-spontaneous production) were pooled together into oral production scores. The other modalities category included three testing paradigms: reading aloud, written comprehension, and written production. Other tests which could not be categorized under these three modalities were kept separately. Finally, scores from auditory comprehension, oral production, other modalities, and uncategorized measures were pooled together to get the overall performance scores.
We performed correlational analysis to explore relationships between scores accumulated into the testing paradigms, scores pooled into the two main language modalities (auditory comprehension and oral production), and scores pooled into overall performance category (see Table 2). Spearman's correlation coefficients between the overall performance, total auditory comprehension, and total oral production scores varied from rs = 0.57 to rs = 0.94 suggesting moderate to very strong relationships. For the rest of the correlations, 79 (73%) varied from rs = 0.61 to rs = 0.95 indicating strong and very strong relationships, 21 (19%) varied from rs = 0.40 to rs = 0.59 indicating moderate relationships, and 8 (7%) correlation coefficients varied from rs = 0.30 to rs = 0.39 indicating weak relationships. Based on the results of this analysis, we concluded that the procedure of pooling scores from various test paradigms into the auditory comprehension and oral production modalities, as well as later pooling all available language performance scores into the overall performance category was justified.
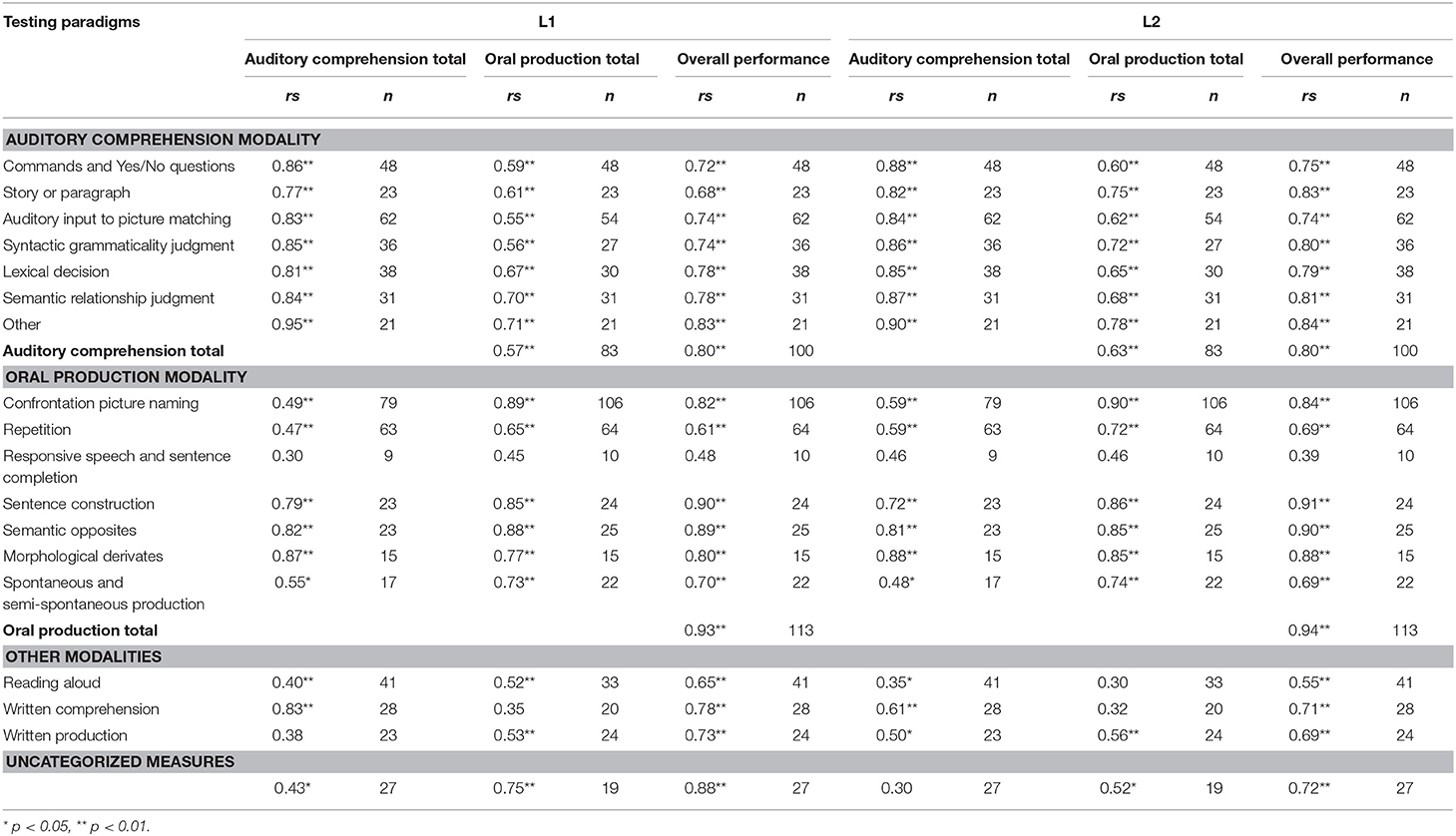
Table 2. Correlations between the testing paradigms and the three types of scores used in the analysis.
In the beginning of the coding stage, the authors coded three studies together and agreed on the coding criteria. Disagreements were resolved via discussion. Then the first author coded 40 studies, 62%, and the second and the third authors coded the remaining studies. Later we randomly selected 16 studies, 25%, which were coded by two authors. For the language use and premorbid proficiency variables, which often required decision making, all studies were coded by two authors and any discrepancies were resolved by discussion including three authors. The Cohen's kappa values suggested strong interrater agreement for both language use, k = 0.807, p < 0.001, and proficiency, k = 0.818, p < 0.001 variables (Fleiss et al., 2003).
The metafor R package (Viechtbauer, 2010) was used for statistical analysis. To estimate effect sizes for the difference in performance between L1 and L2, we calculated risk ratios with the help of escalc function. According to the documentation of escalc, the argument RR provides logarithms of risk ratios, making them symmetric around zero as well as helping to decrease the positive skew in their distribution. The effect sizes in our sample are independent, because each effect size represents the difference in performance between L1 and L2 for a specific case.
First, we fitted random-effect models with the help of rma function to investigate whether there were differences in performance between L1 and L2 for the three types of scores: overall performance, auditory comprehension, and oral production. Then we performed the moderator analysis fitting mixed-effect models with the help of the same function to explore whether the possible difference in performance between L1 and L2 may be affected by the four variables of interest (i.e., early-late bilingual status, premorbid language proficiency, language use, and linguistic similarity). In addition to the moderator analysis on the early-late bilingual status variable, we analyzed whether AoA as a continuous variable moderates the outcomes in the early and late subgroups separately. The overall and moderator analyses were performed for the whole sample as well as for the early and late AoA subgroups, as well as separately for overall performance, auditory comprehension, and oral production scores.
Additionally, it was explored how participants' age at the time of assessment, years of education, and months post onset moderated the magnitude of the difference in performance between L1 and L2. The R scripts used for the analysis as well as the detailed report of the analysis are provided in Supplementary Material.
Three funnel plots, each showing distribution of effect sizes for overall performance, auditory comprehension, and oral production, were created to detect cases with immensely high standard errors (SEs) (see Figure 2). The standard error in the present analysis depended on the number of items used to assess a certain language modality: as the number of the tested items increases, SE gets smaller, and the precision gets higher. Based on visual examination of the funnel plots for overall performance, auditory comprehension, and oral production, the cut-off point was set at SE = 0.3. Thus, five, five, and 16 cases were removed for overall performance, auditory comprehension, and oral production scores, respectively. Given that large differences in performance between languages in the clinical population of persons with aphasia are meaningful and highly probable, we did not remove the data points with relatively large effect sizes. After deleting cases based on SEs, log (RR) = −1.30 had the largest absolute value among the datapoints from all three funnel plots. This value meant that in this case performance in L1 was 73% worse than in L2.
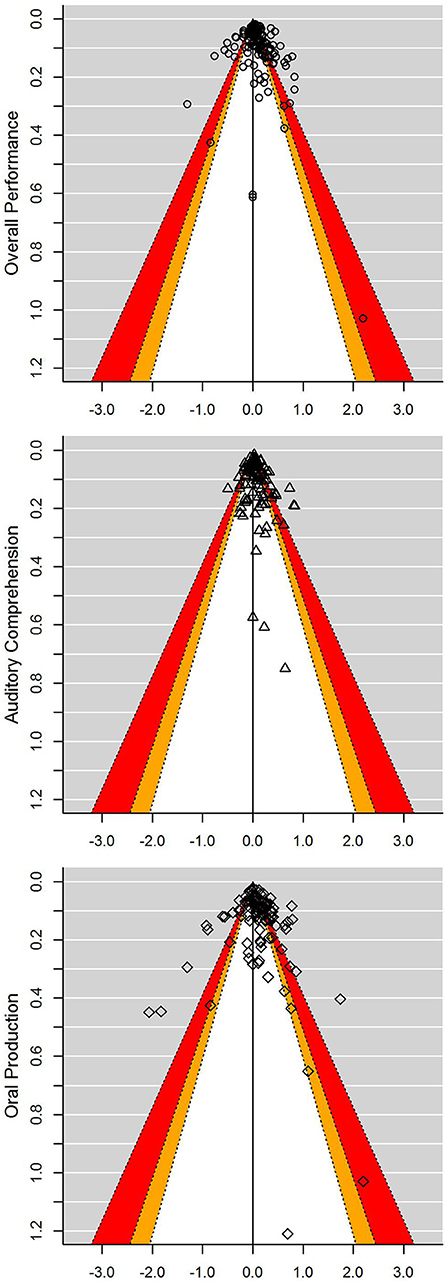
Figure 2. Contour enhanced funnel plots for each of the three types of scores analyzed. Contours change shades at p-levels 0.1 (white), 0.05 (orange), and 0.01 (red). Logarithms of risk ratios are plotted against the SEs, and the reference line indicating the random-effects model estimates for each the three types of scores analyzed. Positive and negative abscissas represent better performance in L1 and L2, respectively.
A total of 65 peer-reviewed published studies, from which 130 cases were extracted, were included in the review. Given that the analysis we performed required having information on which language was acquired first, six cases representing simultaneous bilinguals who acquired both languages from the age of zero, were excluded from the sample.
Twenty seven (22%), 65 (52%), and 32 (26%) cases were taken from group (n = 4), multi-case (n = 19), and single-case studies (n = 32), respectively. Sixty two (50%) cases were extracted from studies with research questions unrelated to testing differences between the languages of multilingual people with aphasia (n = 31); the remaining 62 (50%) cases were extracted from studies with research questions related to testing differences between one's languages (n = 24). Detailed information about the cases is summarized in Data Sheet 1 in Supplementary Material. Further analysis performed on the trimmed data showed that the study type (i.e., research question related vs. unrelated to testing L1/L2 differences) did not significantly moderate the outcomes for overall performance, QM[1] = 2.89, p = 0.24, auditory comprehension, QM[1] = 0.21, p = 0.90,or oral production, QM[1] = 0.76, p = 0.68.
Descriptive information on the demographic and clinical details of the sample used for the analysis as well as the early and late AoA subgroups is summarized in Table 3.
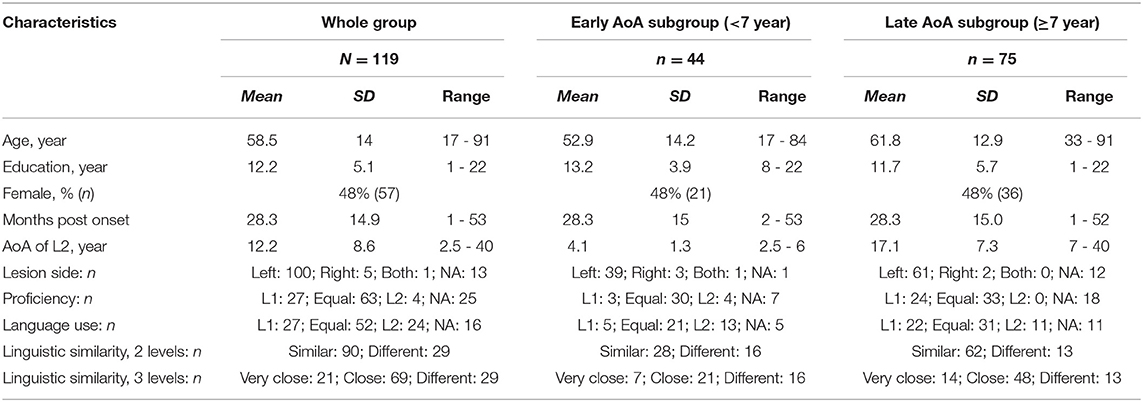
Table 3. Demographic and clinical details of the whole sample and AoA subgroups.
After data trimming, the difference in performance between L1 and L2 was investigated using overall performance scores. We found a statistically significant effect size, RR = 1.10 [1.05, 1.15], p < 0.0001, QE [118] = 1025.14, suggesting that overall performance in L1 was on average 10% better than in L2 (see Figure 3). For auditory comprehension scores, we also found a statistically significant effect size, RR = 1.06 [1.02, 1.10], p < 0.0001, QE [90] = 363.41, suggesting that auditory comprehension in L1 was on average 6% better than in L2. Similarly, a statistically significant effect size, RR = 1.10 [1.03, 1.17], p < 0.0001, QE [90] = 686.25, was found for oral production scores suggesting that performance in L1was on average 10% better than in L2.
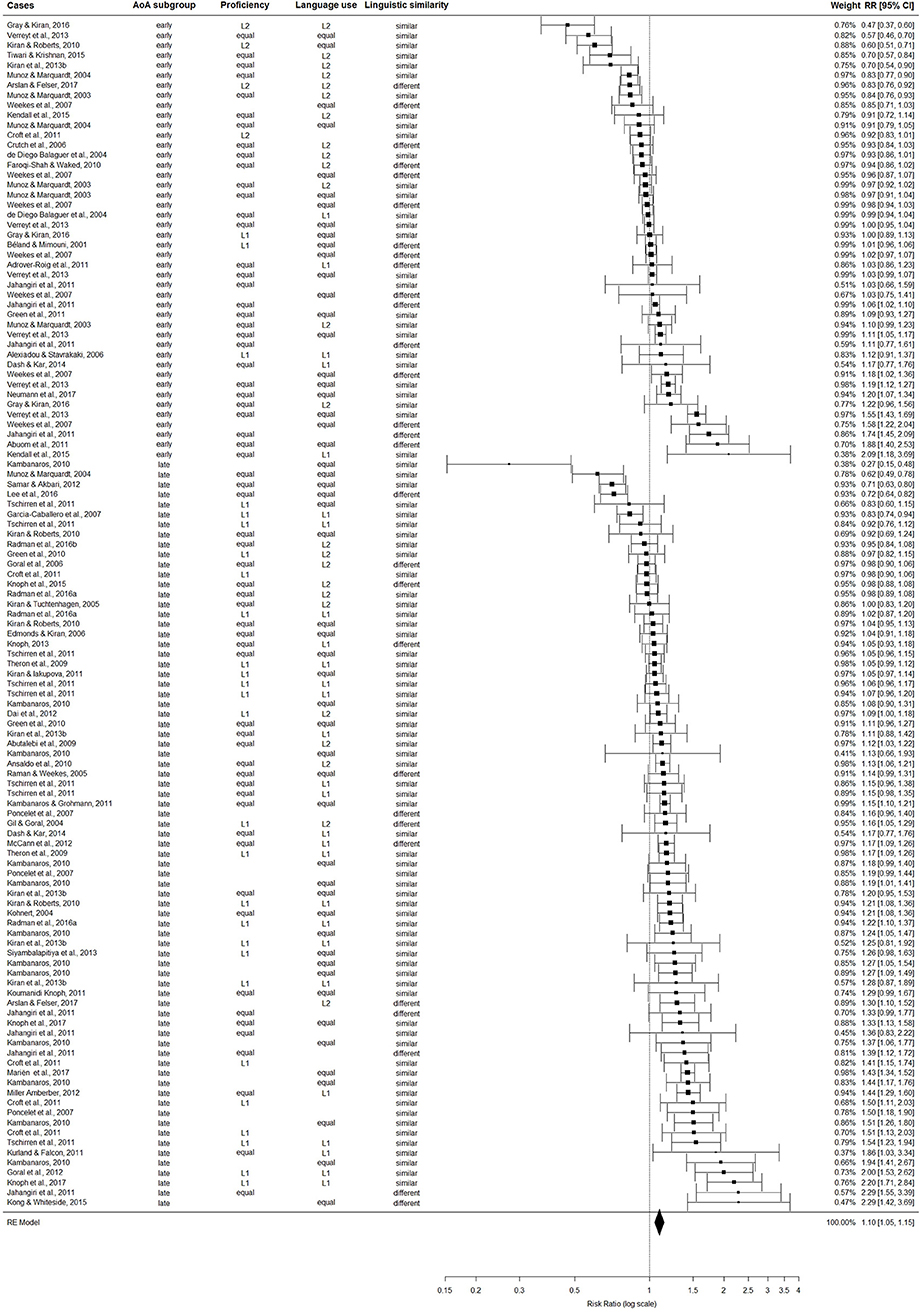
Figure 3. For the whole trimmed sample (k = 119), the figure displays effect sizes (Risk Ratios) and corresponding 95% confidence intervals (CI) for the comparison between overall language performance in the earlier-acquired (L1) and later-learned (L2) languages. Values larger than one indicate better performance in L1 compared to L2 and values smaller than one indicate worse performance in L1 compared to L2.
Details of the moderator analysis (effects sizes, 95% CIs, and statistics of the moderator tests) are summarized in Table 4.
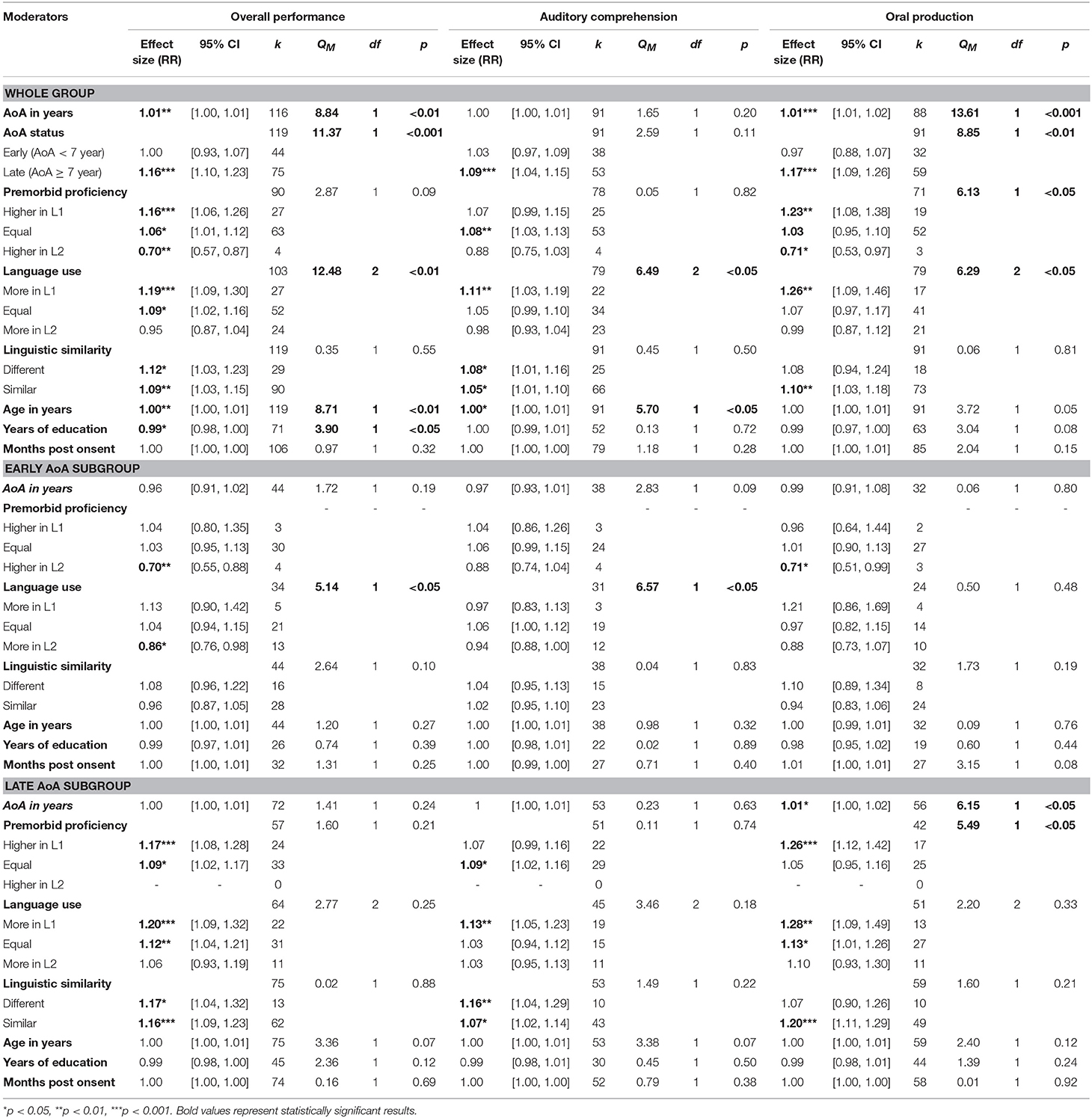
Table 4. Details of the moderator analysis.
In the whole sample, AoA as a continuous variable moderated overall performance, QM[1] = 8.84, p < 0.01, and oral production, QM[1] = 13.61, p < 0.001, in the direction that as AoA increased, the magnitude of the L1 advantage (better performance in L1 compared to L2) increased. AoA as a continuous variable did not moderate auditory comprehension in the whole sample, QM[1] = 1.65, p = 0.20.
To decide on the cut-off point for making the early and late AoA subgroups, we visually explored the distribution of overall performance outcomes plotted against AoA as a continuous variable (see the plot in Data Sheet 3, p.53 in Supplementary Material). Based on this visual examination, 7 year appeared to be a reasonable cut-off point.
AoA status as a binary variable (early/late) significantly moderated overall performance, QM[1] = 11.37, p < 0.001, and oral production, QM[1] = 8.85, p < 0.01. Individuals who acquired L2 before 7 year showed a significantly smaller difference between L1 and L2 in overall performance, RR = 1.00 [0.93, 1.07], p = 0.99, compared to those who acquired L2 after 7 year, where performance in L1 was significantly better than in L2, RR = 1.16 [1.10, 1.23], p < 0.0001. Similarly for oral production, the early AoA subgroup showed a significantly smaller difference between L1 and L2, RR = 0.97 [0.88, 1.07], p = 0.60, compared to the late AoA subgroup, where performance in L1 was significantly better than in L2, RR = 1.17 [1.09, 1.26], p < 0.0001. The early-late bilingual status did not moderate auditory comprehension, QM[1] = 2.59, p = 0.11.
Additionally, we explored how AoA as a continuous variable moderated the outcomes in the early and late AoA subgroups separately. In the early AoA subgroup, AoA did not moderate overall performance, QM[1] = 1.72, p = 0.19, auditory comprehension, QM[1] = 2.83, p = 0.09, or oral production, QM[1] = 0.06, p = 0.80. In the late AoA subgroup, AoA moderated oral production, QM[1] = 6.15, p < 0.05, but not overall performance, QM[1] = 1.41, p = 0.24, or auditory comprehension, QM[1] = 0.23, p = 0.63.
Given that there were only four effect sizes in the higher L2 proficiency group, they were excluded from the analysis and described separately. In the whole group, premorbid language proficiency did not moderate either overall performance QM[1] = 2.87, p = 0.09, or auditory comprehension, QM[1] = 0.05, p = 0.82. Proficiency significantly moderated oral production, QM[1] = 6.13, p < 0.05. Individuals with equal proficiency in both languages had a significantly smaller difference between L1 and L2 in oral production, RR = 1.03 [0.95, 1.10], p = 0.49, compared to those who were more proficient in L1, RR = 1.23 [1.08, 1.38], p < 0.01. Individuals with higher L2 proficiency performed significantly better in L2 overall, RR = 0.70 [0.57, 0.87], p < 0.01, and in oral production, RR = 0.71 [0.53, 0.97], p < 0.05, but not in auditory comprehension, RR = 0.88 [0.75, 1.03], p = 0.12.
Given that 81% (n = 30) of the cases in the early AoA subgroup had equal proficiency and other two proficiency groups included three (L1) and four (L2) cases each, the moderator analysis was not performed and only descriptive statistics are reported here. Individuals with higher L1 proficiency performed comparably in the two languages overall, RR = 1.04 [0.80, 1.35], p = 0.77, as well as in auditory comprehension, RR = 1.04 [0.86, 1.26], p = 0.67, and oral production, RR = 0.96 [0.64, 1.44], p = 0.84. Similarly, participants with equal proficiency performed comparably overall, RR = 1.03 [0.95, 1.13], p = 0.47, as well as in auditory comprehension, RR = 1.06 [0.99, 1.15], p = 0.10, and oral production, RR = 1.01 [0.90, 1.13], p = 0.84. In contrast, the four participants with higher L2 proficiency described above were all early bilinguals; again, they showed significantly better performance in L2 overall, RR = 0.70 [0.55, 0.88], p < 0.01, as well as in oral production, RR = 0.71 [0.51, 0.99], p < 0.05, but not in auditory comprehension, RR = 0.88 [0.74, 1.04], p = 0.13.
In the late AoA subgroup, where 58% (n = 33) had equal proficiency and the rest (n = 24) had higher L1 proficiency, language proficiency did not moderate overall performance, QM[1] = 1.60, p = 0.21, and auditory comprehension, QM[1] = 0.11, p = 0.74, but was a significant moderator for oral production, QM[1] = 5.49, p < 0.05. Individuals with higher L1 proficiency performed significantly better in L1, RR = 1.26 [1.12, 1.42], p < 0.001, whereas the equal proficiency group showed comparable performance in oral production, RR = 1.05 [0.95, 1.16], p = 0.36.
For the whole group, language use moderated overall performance, QM[2] = 12.48, p < 0.01, auditory comprehension, QM[2] = 6.49, p < 0.05, and oral production, QM[2] = 6.29, p < 0.05. Individuals who premorbidly used L1 more frequently had significantly greater magnitude of L1 advantage in overall performance, RR = 1.19 [1.09, 1.30], p < 0.001, as well as individuals who equally used both languages, RR = 1.09 [1.02, 1.16], p < 0.05, compared to the group with more L2 use who showed comparable performance in both languages, RR = 0.95 [0.87, 1.04], p = 0.25. Individuals who premorbidly used L1 more frequently performed significantly better in L1 in both auditory comprehension, RR = 1.11 [1.03, 1.19], p < 0.01, and oral production, RR = 1.26 [1.09, 1.46], p < 0.01, compared to the L2 more frequent usage group who again showed comparable performance in both languages, (auditory comprehension: RR = 0.98 [0.93, 1.04], p = 0.60; oral production: RR = 0.99 [0.87, 1.12], p = 0.84). There were no significant differences between the more L1 and equal use groups for overall performance, auditory comprehension, and oral production.
Given that there were only five individuals in the early AoA group with greater L1 use, they were excluded from the moderator analysis and described separately. In the early AoA subgroup, language use moderated the outcomes for overall performance, QM[1] = 5.14, p < 0.05, and auditory comprehension, QM[1] = 6.57, p < 0.05, but not for oral production, QM[1] = 0.50, p = 0.48. In overall performance, individuals with more frequent L2 use showed significantly better performance in L2, RR = 0.86 [0.76, 0.98], p < 0.05, compared to those with equal use, who showed comparable overall performance, RR = 1.04 [0.94, 1.15], p = 0.43. Similarly for auditory comprehension, individuals with more L2 use showed comparable performance with a trend toward better performance in L2, RR = 0.94 [0.88, 1.00], p = 0.07, whereas the equal use group showed comparable performance with a trend toward better performance in L1, RR = 1.06 [1.00, 1.12], p = 0.07. The more L1 use group showed comparable performance overall, RR = 1.13 [0.90, 1.42], p = 0.27, in auditory comprehension, RR = 0.97 [0.83, 1.13], p = 0.70, and oral production, RR = 1.21 [0.86, 1.69], p = 0.27.
For the late AoA subgroup, language use did not moderate overall performance, QM[2] = 2.77, p = 0.25, auditory comprehension, QM[2] = 3.46, p = 0.18, or oral production, QM[2] = 2.20, p = 0.33.
For the whole group, binary linguistic similarity (different/similar languages) did not moderate overall performance, QM[1] = 0.35, p = 0.55, auditory comprehension, QM[1] = 0.45, p = 0.50, or oral production, QM[1] = 0.06, p = 0.81.
For the early AoA subgroup, binary linguistic similarity did not moderate overall performance, QM[1] = 2.64, p = 0.10, auditory comprehension, QM[1] = 0.04, p = 0.83, or oral production, QM[1] = 1.73, p = 0.19.
For the late AoA subgroup, binary linguistic similarity did not moderate overall performance, QM[1] = 0.02, p = 0.88, auditory comprehension, QM[1] = 1.49, p = 0.22, or oral production, QM[1] = 1.60, p = 0.21.
Similarly, linguistic similarity coded with three levels (very close/close/different languages) did not appear to be a significant moderator for overall performance (whole group: k = 119, QM[2] = 0.78, p = 0.68; early: k = 44, QM[2] = 2.87, p = 0.24; late: k = 75, QM[2] = 1.96, p = 0.38), auditory comprehension (whole group: k = 91, QM[2] = 0.52, p = 0.77; early: k = 38, QM[2] = 0.05, p = 0.98; late: k = 53, QM[2] = 1.49, p = 0.48), or oral production (whole group: k = 91, QM[2] = 0.17, p = 0.92; early: k = 32, QM[2] = 1.99, p = 0.37; late: k = 59, QM[2] = 2.08, p = 0.35).
In the whole sample, age moderated the outcomes for overall performance, QM[1] = 8.71, p < 0.01, and auditory comprehension, QM[1] = 5.70, p < 0.05: as age increased, the magnitude of L1 advantage increased. There was no significant moderation for oral production, QM[1] = 3.72, p = 0.054. Years of education moderated overall performance, QM[1] = 3.90, p < 0.05: as years of education increased, the magnitude of L1 advantage decreased. There were no significant effects of education either for auditory comprehension, QM[1] = 0.13, p = 0.72, or for oral production, QM[1] = 3.04, p = 0.08. Months post onset did not moderate overall performance, QM[1] = 0.97, p = 0.32, auditory comprehension, QM[1] = 1.18, p = 0.28, or oral production, QM[1] = 2.04, p = 0.15.
When the AoA subgroups were analyzed separately, age did not moderate outcomes for overall performance (early: QM[1] = 1.20, p = 0.27; late: QM[1] = 3.36, p = 0.07), auditory comprehension (early: QM[1] = 0.98, p = 0.32; late: QM[1] = 3.38, p = 0.07), or oral production (early: QM[1] = 0.09, p = 0.76; late: QM[1] = 2.40, p = 0.12). Similarly, years of education did not moderate overall performance (early: QM[1] = 0.74, p = 0.39; late: QM[1] = 2.36, p = 0.12), auditory comprehension (early: QM[1] = 0.02, p = 0.89; late: QM[1] = 0.45, p = 0.50), or oral production (early: QM[1] = 0.60, p = 0.44; late: QM[1] = 1.39, p = 0.24). Finally, months post onset did not moderate overall performance (early: QM[1] = 1.31, p = 0.25; late: QM[1] = 0.16, p = 0.69), auditory comprehension (early: QM[1] = 0.71, p = 0.40; late: QM[1] = 0.79, p = 0.38),or oral production (early: QM[1] = 3.15, p = 0.08; late: QM[1] = 0.01, p = 0.92).
The questions motivated this systematic review were whether people with aphasia are likely to exhibit better performance in their first-acquired (L1) than in a later-learned (L2) language, and whether age of acquisition (AoA), premorbid language proficiency, use and exposure, and linguistic similarity between the person's languages affect the consequences of aphasia in L1 and L2. We followed the PRISMA guidelines for a systematic review (Gates and March, 2016) and included 65 studies and 130 bilingual individuals with aphasia. Meta-analyses of effects sizes revealed the following answers to our questions.
We found that in the 119 bilingual speakers included in the analysis as a group, L1 was significantly better preserved than L2. This finding could be considered at odds with the view that different languages are processed in shared neural substrata for bilingual speakers (e.g., Abutalebi, 2008) and with the view held by many researchers and clinicians that bilingual people with aphasia tend to show equivalent language impairments after a stroke. The comparable impairment view has been supported by several reports in the literature. For example, Fabbro (2001) identified equivalent impairments in L1 and L2 in ≈60% of the cases he reviewed, who were early bilinguals with high proficiency in both languages. Unlike the findings reported by Fabbro (2001) and those reported in Albert and Obler (1978), our results appear to support Ribot (1882), which predicts that the earlier acquired language is more resistant to brain damage. This is also consistent with findings of better preservation in aphasia of words that are learned early in life compared to those learned later in life (for review see Brysbaert and Ellis, 2016).
We contend that our more rigorous analysis, which included a larger number of participants from a diversity of multilingual speakers of typologically different languages, is more reliable than the conclusions drawn from prior reviews. We note that the effect of language status (L1 vs. L2) confirmed here is often seen in case reports of bilingual speakers with aphasia but has rarely been analyzed according to the criteria developed in the present review.
Moreover, there has been a tendency in the literature on bilingual aphasia toward reporting performance of single cases according to the question of whether language impairments are parallel or differential (Paradis, 1983; Fabbro, 2001). We believe that posing this question can be misleading. It is critical to first determine whether parallel impairments should be expected, depending on the characteristics of the bilingual individuals. Indeed, it is possible that the reports of ≈60% of bilingual participants with aphasia demonstrating comparable impairments in both their L1 and L2 found in previous reviews are driven by early bilinguals and misrepresent the state of affairs for late bilinguals. We therefore divided our sample into early and late bilinguals to examine the observed difference between L1 and L2 separately for the two types of bilinguals. Furthermore, we examined whether additional bilingual characteristics, namely, specific AoA, frequency of language use, premorbid language proficiency, and linguistic similarity moderate the difference between L1 and L2.
When we examined AoA as a binary categorical variable, our results demonstrated significant differences between early and late bilinguals. Specifically, late bilinguals, who acquired their other language after the age of seven, showed significantly better overall performance in L1 than in the later-learned language. In contrast, the early bilinguals who acquired their languages before the age of seven showed comparable performance in both languages. This result is consistent with previous findings from reports of balanced bilingual speakers who showed comparable levels of impairment (e.g., Fabbro, 2001; Kiran and Roberts, 2010). This difference between the two subgroups was significant despite the fact that the majority of individuals in both subgroups had equal pre-stroke proficiency in both their languages (81% and 58% in the early and late bilingual subgroups, respectively). Our finding of an effect of language status (i.e., significant difference between L1 and L2 performance) post stroke for late bilinguals challenges the assumptions of the shared bilingual neural substrate (SBNS) and the convergence hypothesis (Green, 2003). It is also at odds with the conclusions of Tschirren et al. (2011). It is possible that the differences in syntactic processing reported by Tschirren et al. (2011), together with generally comparable impairment, are the sort of outcomes that have contributed to the differential findings our meta-analysis revealed.
We found that, in the whole sample, AoA as a continuous variable moderated overall performance, oral production, but not auditory comprehension. This is consistent with findings that in bilinguals who are not highly proficient, language production is typically more difficult than language comprehension (e.g., Swain, 1985). It is possible that the substantial variance of performance among the late bilinguals (but not in the early bilinguals) included here allowed for the effect of AoA to emerge. Future studies could further examine the AoA at which the patterns of results change. Of interest, we found an effect of age, with older individuals showing the greater magnitude of L1 advantage compared to younger ones; the interaction of age and AoA could be further examined in future studies.
Thus, AoA moderated performance differences between L1 and L2 when early and late bilinguals were compared, which may suggest that a language that is acquired early enjoys a unique status and could potentially be differentially processed in the brain (e.g., Giussani et al., 2007). In contrast, the finding that AoA as a continuous variable significantly moderated only oral production in the late AoA subgroup only suggests that the exact AoA matters less. This is consistent with some views of the role of AoA in bilingualism (Birdsong and Molis, 2001). We note that we divided the participants into the early and late subgroups based on a theoretically motivated rationale. We found that in our sample, age 7 year was a natural breakpoint, considering that individuals started schooling in L2 at this age. A similar cut-off point (6 year) for early and later AoA was also used in the meta-analytic review on the bilingual advantage by Lehtonen et al. (2018).
Our findings of better overall performance in L1 than in L2 have implications for the cognitive neuropsychology of bilingual aphasia as well as for clinical aphasiology. Nevertheless, as expected, this finding was qualified by several variables identified in the literature as potential moderators: premorbid language proficiency, language use, and linguistic similarity (e.g., Goral et al., 2006; Ansaldo et al., 2008; Lorenzen and Murray, 2008). It can be argued that language proficiency and language use are typically correlated. As a rule, speakers who use a language with frequency and regularity are more likely to be highly proficient in that language (e.g., Gollan et al., 2015; Peñaloza et al., 2017). However, there are also instances in which people report greater use than proficiency, especially in L2. For the individuals included in the analysis in the current review, there was a significant association between these two variables (n = 85 p < 0.01, Cramer's V = 0.34); in our analyses, we examined the effects of language proficiency and language use separately.
We tested whether premorbid language proficiency moderated the magnitude of the difference in performance between L1 and L2. One could assume that a premorbidly more proficient language would be better preserved after a stroke. Our results partially supported this hypothesis. Individuals with higher L1 proficiency and those with equal proficiency in their two languages showed the pattern observed for the sample as a whole, namely, better overall performance in L1 when compared to L2. There were only four individuals in the sample who reported higher premorbid L2 proficiency than L1 proficiency and they appeared to perform better in L2 compared to L1. No statistically significant differences were found between the higher premorbid L1 proficiency group compared with the equal proficiency group in overall performance and auditory comprehension scores, however the magnitude of L1 advantage in oral production scores was significantly greater for the group with higher L1 proficiency. These results overall suggest that L2 proficiency plays a role in the degree of impairment only when it surpasses the proficiency in L1. Given that the higher L2 proficiency group was very small in the present review, this assumption requires further investigation.
We also examined how proficiency moderated the effect of language status in the early bilingual and late bilingual subgroups separately. We observed that in the early bilingual group, individuals with higher L1 and with equal proficiency showed the pattern observed for the subgroup as a whole, namely, comparable performance in both languages. The four individuals who reported higher premorbid L2 proficiency were all early bilinguals and, as mentioned above, performed better in L2. There were no effects of proficiency in the late bilingual subgroup except for oral production, for which the magnitude of L1 advantage was significantly bigger for those individuals who reported higher L1 proficiency than those who reported to be equally proficient in both languages.
Thus, language proficiency appears to have a relatively small role in the results of overall differences between L1 and L2, except for those cases where L2 achieved higher proficiency than L1. This finding does not support the view that language proficiency has a greater role in determining language representation and processing in bilinguals than AoA (e.g., Perani et al., 1998; Abutalebi et al., 2001). We also found that the more years of education individuals had, the smaller was the magnitude of L1 advantage. This suggests that education in L2 could be used as an additional source of information for determining premorbid L2 proficiency.
It is of interest to note how language proficiency was measured in the reviewed studies. There was great variability in the measures and tools used (e.g., section A of the BAT; the Language Use Questionnaire, Muñoz et al., 1999), but generally, most studies included subjective self-ratings of the participants of their language abilities prior to the stroke. These self-ratings ranged in terms of the size of the scale and whether each ability was rated separately. In a few cases, family members' ratings were included as well. In none of the studies, formal measures of premorbid language abilities (e.g., language proficiency test, language placement test) were available.
Language use has been discussed in recent publications on bilingual language performance (Linck et al., 2009), as a determining variable in degree of impairment as well as degree of recovery from aphasia (Goral et al., 2012, 2013; Knoph et al., 2017). This is particularly true for individuals who live in a monolingual L2 environment following immigration for example.
We examined whether the magnitude of the difference between L1 and L2 was influenced by language use. One could hypothesize that the more used language would be better preserved (Pitres, 1895/1983). Our results partially supported this hypothesis. In the whole group, those with more frequent use of L1 showed significantly better performance in L1 compared to L2 in all of the three outcomes, whereas those who rated their L2 use as more frequent than their L1 performed comparably in both languages in all three outcomes. For the early AoA subgroup, those who used L2 more often showed better performance in L2 based on overall performance scores, whereas those who used L1 more frequently and those who used both languages equally showed comparable performance in both languages in all three outcomes. Better performance in L2 compared to L1 was not found in the late bilinguals, whereas better performance in L1 and comparable performance were the typical patterns.
Similar to the findings for language proficiency in oral production performance, we found evidence of significantly greater magnitude of L1 advantage in the group with more frequent L1 use compared with the group where L2 was more frequently used, but not with the group where both languages were equally used. These findings suggest that language use affected the magnitude of L1 advantage when L2 became the most frequently used language. Thus, like premorbid language proficiency, language use has a moderating role on the findings, which does not seem to be independent of AoA.
There has been discussion in the literature regarding the degree to which language similarity influences the comparability of impairment in bilingual aphasia (Lorenzen and Murray, 2008). Whereas, on the one hand, one might predict that more similar languages would look similarly impaired following a stroke, there is little evidence to support this prediction and there is controversy in the literature regarding the role of language similarity on the neuronal organization of the languages of a bilingual (Kumar, 2014; Wong et al., 2016). On the other hand, one could assume that because linguistically similar languages share a significant portion of lexico-semantic representation (e.g., cognates), more cognitive control may be required to overcome cross-language interference. Our analyses revealed no effect of linguistic similarity. This finding is consistent with recent studies that attributed greater importance of language proficiency and use than of linguistic similarity (e.g., Muñoz and Marquardt, 2003; Ansaldo and Saidi, 2014; Kastenbaum et al., 2019). The finding is also consistent with neuroimaging studies that have demonstrated overlap in processing and representation among languages of bilinguals even for those who use languages that are very different from each other (e.g., Abutalebi et al., 2001; Wong et al., 2016).
We note, however, that quite a few studies have reported an effect of cognates, which is one aspect of language similarity that has been studied in aphasia (Kohnert, 2004; Kurland and Falcon, 2011; Kendall et al., 2015). Our finding of no role of linguistic similarity could be considered in opposition to such studies. It is possible that linguistic similarity affects the manifestation of specific linguistic aspects, consistent with findings that reported interference between languages that are similar (Fabbro, 2001; Goral et al., 2006), but that the degree of language similarity does not affect overall relative levels of impairment. Thus, it may be that effects of linguistic similarity on performance will be evident in tasks that require syntactic processing for languages that share or differ in specific morpho-syntactic aspects (e.g., Nilipour and Paradis, 1995; Yiu and Worrall, 1996; Goral et al., 2010) and in those that demand lexical-semantic processing for languages that share more or fewer cognates (Kohnert, 2004; Kurland and Falcon, 2011). We also note that dissociations in performance for bilingual patients with reading and writing disorders suggest that language type can constrain patterns of bilingual aphasia (see Weekes, 2012; Goral, 2019).
The number of significant effect sizes we found points to the robustness of our findings, although the greater L2 proficiency results were based on a small number of cases and should be interpreted with caution. Furthermore, there was great variability among the studies included in the review, both in terms of the participants' characteristics and the language performance measures (see Table 1). Indeed, the variability of measures used is a limitation of the present data as well as of the field in general. Our data highlight the importance of greater uniformity of assessment in bilingual aphasia, which was one rationale for the development of the BAT (Paradis and Libben, 1987), although, other tools are clearly needed to assess specific languages and linguistic aspects.
We are mindful of drawing conclusions from the data beyond the domain of bilingual aphasia. Our results confirm the view that individual differences in the unique language background characteristics of a bilingual speaker are very likely to impact on the presentation of aphasia in more than one language. Additionally, an open question to date is to what degree differences in performance between L1 and L2 in late bilinguals are due to differential impairment levels or to differential pre-stroke mastery levels. Another conclusion which should be viewed with caution is the one regarding AoA. Although the transformation of the AoA into the binary classification (early/late) based on 7 year of age was motivated theoretically, other cut-off points can be considered in the future research. Furthermore, a lack of effects of specific AoA within the AoA subgroups could partially be a result of relatively low inter-individual variability in this variable.
Finally, the analyses we conducted did not allow us to consider in-depth language impairment patterns of multilingual individuals with aphasia, such as for instance, uncontrollable language blending and antagonistic recovery (Paradis, 1977, 2001), which are of great importance for understanding cognitive mechanisms of language. Moreover, given the cross-sectional nature of the present study, it does not inform us about the dynamics of language performance, which was an important aspect in the classification of recovery patterns in multilingual aphasia (Paradis, 1977, 2001).
To conclude, the current systematic review and meta-analysis revealed a better performance in L1 compared to L2 in bilingual speakers with aphasia. It also demonstrated that the magnitude of this difference was moderated by whether the bilinguals learned their two languages early in childhood or later. The better performance in L1 was a robust finding, which was moderated by premorbid language proficiency and frequency of use. Finally, linguistic similarity did not appear to interact with the magnitude of the difference in performance between L1 and L2.
The results we report here from a meta-analysis reflect the patterns observed in case studies, case-series, and group studies of multilingual individuals with aphasia. Cognitive neuropsychology has been a dominant theoretical movement in the study of aphasia for nearly 50 years. One defining feature of cognitive neuropsychology is the study of the single case and its bedrock assumption is that group studies are not meaningful because they average data across participants and consequently mask individual differences (Caramazza, 1986; though see Caplan, 1988; Grodzinsky et al., 1999). In the past decade, cognitive neuropsychologists have evolved toward advocating a case-series approach which retains the individual differences in single cases while accommodating the general patterns of performance in clinical groups (Schwartz and Dell, 2010; Rapp, 2011). For this reason, the problems of averaging that are debated extensively in the cognitive neuropsychological literature (e.g., McCloskey and Caramazza, 1988) do not apply to case-series designs. We contend that the type of meta-analysis conducted here also retains the individual patterns of performance.
Our findings reinforce the calls for (1) assessing all languages and collecting language background information (e.g., language use, premorbid language proficiency) of multilingual speakers with aphasia to obtain the most accurate assessment of their language abilities and (2) reporting performance in a way allowing researchers to compare the records among different studies, i.e., disclosing names of the assessment tools and scales used.
Growing understanding of the roles of such variables as premorbid language proficiency, language use and exposure, AoA, and structural similarities between one's languages will improve assessment practices and management options for multilingual speakers with aphasia. At the very least, multilingual speakers with aphasia should be assessed and treated with the understanding that it could be their earlier-acquired language that may be the key to greater success in restoring communication abilities.
The dataset and R script used for the analysis are provided in Supplementary Material.
EK contributed to this study by designing the study concept, searching the databases, screening the data, coding the studies, planning and conducting the data analysis, interpreting the results, and writing the manuscript. MG contributed by designing the study concept, coding the studies, interpreting the results, writing the manuscript, and providing the external assistance for preparing the manuscript. MN contributed to the study concept and coded the studies. BW contributed by inspiring the very idea of the study, designing the study concept, interpreting the results, and writing the manuscript.
The study was funded by the University of Oslo.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Our sincere gratitude goes to Bård Uri Jensen and Katarina Antolovic for their help in preparing the present study.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2019.00445/full#supplementary-material
*Abuom, T. O., Obler, L. K., and Bastiaanse, R. (2011). Using Swahili and English to test explanations of agrammatism. Aphasiology 25, 559–575. doi: 10.1080/02687038.2010.538417
Abutalebi, J. (2008). Language control and lexical competition in bilinguals: an event-related fMRI study. Cereb. Cortex 18, 1496–1505 doi: 10.1093/cercor/bhm182
Abutalebi, J., Cappa, S. F., and Perani, D. (2001). The bilingual brain as revealed by functional neuroimaging. Bilingualism Lang. Cogn. 4, 179–190. doi: 10.1017/S136672890100027X
Abutalebi, J., and Green, D. (2007). Bilingual language production: the neurocognition of language representation and control. J. Neurolinguistics 20, 242–275. doi: 10.1016/j.jneuroling.2006.10.003
Abutalebi, J., and Green, D. (2008). Control mechanisms in bilingual language production: neural evidence from language switching studies. Lang. Cogn. Process. 23, 557–582. doi: 10.1080/01690960801920602
*Abutalebi, J., Rosa, P. A., Tettamanti, M., Green, D. W., and Cappa, S. F. (2009). Bilingual aphasia and language control: a follow-up fMRI and intrinsic connectivity study. Brain Lang. 109, 141–156. doi: 10.1016/j.bandl.2009.03.003
*Adrover-Roig, D., Galparsoro-Izagirre, N., Marcotte, K., Ferré, P., Wilson, M. A., and Inés Ansaldo, A. (2011). Impaired L1 and executive control after left basal ganglia damage in a bilingual Basque–Spanish person with aphasia. Clin. Linguist. Phon. 25, 480–498. doi: 10.3109/02699206.2011.563338
Albert, M. L., and Obler, L. K. (1978). The Bilingual Brain: Neuropsychological and Neurolinguistic Aspects of Bilingualism. New York, NY: Academic Press.
*Alexiadou, A., and Stavrakaki, S. (2006). Clause structure and verb movement in a Greek-English speaking bilingual patient with Broca's aphasia: evidence from adverb placement. Brain Lang. 96, 207–220. doi: 10.1016/j.bandl.2005.04.006
*Altman, C., Goral, M., and Levy, E. S. (2012). Integrated narrative analysis in multilingual aphasia: the relationship among narrative structure, grammaticality, and fluency. Aphasiology 26, 1029–1052. doi: 10.1080/02687038.2012.686103
Ansaldo, A. I., Marcotte, K., Scherer, L., and Raboyeau, G. (2008). Language therapy and bilingual aphasia: clinical implications of psycholinguistic and neuroimaging research. J. Neurolingu. 21, 539–557. doi: 10.1016/j.jneuroling.2008.02.001
Ansaldo, A. I., and Saidi, L. G. (2014). Aphasia therapy in the age of globalization: cross-linguistic therapy effects in bilingual aphasia. Behav. Neurol. 2014:603085. doi: 10.1155/2014/603085
*Ansaldo, A. I., Saidi, L. G., and Ruiz, A. (2010). Model-driven intervention in bilingual aphasia: evidence from a case of pathological language mixing. Aphasiology 24, 309–324. doi: 10.1080/02687030902958423
*Arslan, S., and Felser, C. (2017). Comprehension of wh -questions in Turkish– German bilinguals with aphasia: a dual-case study. Clin. Linguist. Phon. 2017, 1–21. doi: 10.1080/02699206.2017.1416493
Bakhtiar, M., Jafary, R., and Weekes, B. S. (2017). Aphasia in Persian: implications for cognitive models of lexical processing. J. Neuropsychol. 11, 414–435. doi: 10.1111/jnp.12095
*Béland, R., and Mimouni, Z. (2001). Deep dyslexia in the two languages of an Arabic/French bilingual patient. Cognition 82, 77–126. doi: 10.1016/S0010-0277(01)00148-2
Birdsong, D. (2006). Age and second language acquisition and processing: a selective overview. Lang. Learn. 56, 9–49. doi: 10.1111/j.1467-9922.2006.00353.x
Birdsong, D., and Molis, M. (2001). On the evidence for maturational constraints in second-language acquisition. J. Mem. Lang. 44, 235–249. doi: 10.1006/jmla.2000.2750
Brysbaert, M., and Ellis, A. W. (2016). Aphasia and age of acquisition: are early-learned words more resilient? Aphasiology 30, 1240–1263. doi: 10.1080/02687038.2015.1106439
Bub, D. (2011). Facing the challenge of variation in neuropsychological populations: lessons from biology. Cogn. Neuropsychol. 28, 445–450. doi: 10.1080/02643294.2012.671766
Caplan, D. (1988). On the role of group studies in neuropsychological and pathopsychological research. Cogn. Neuropsychol. 5, 535–547. doi: 10.1080/02643298808253273
Caramazza, A. (1984). The logic of neuropsychological research and the problem of patient classification in aphasia. Brain Lang. 21, 9–20. doi: 10.1016/0093-934X(84)90032–4
Caramazza, A. (1986). On drawing inferences about the structure of normal cognitive systems from the analysis of patterns of impaired performance. Brain Lang. 5, 41–66. doi: 10.1016/0278-2626(86)90061–8
Caramazza, A., and McCloskey, M. (1988). The case for single-patient studies. Cogn. Neuropsychol. 5, 517–527. doi: 10.1080/02643298808253271
Chee, M. W., Caplan, D., Soon, C. S., Sriram, N., Tan, E. W., Thiel, T., et al. (1999). Processing of visually presented sentences inMandarin and English with fMRI. Neuron 23, 127–137. doi: 10.1016/S0896-6273(00)80759-X
Chee, M. W., Weekes, B., Lee, K. M., Soon, C. S., Schreiber, A., Hoon, J. J., et al. (2000). Overlap and dissociation of semantic processing of characters English words and pictures: evidence from fMRI. Neuroimage 12, 392–403 doi: 10.1006/nimg.2000.0631
Coltheart, M. (2017). The assumptions of cognitive neuropsychology: reflections on Caramazza (1984); Caramazza (1986). Cogn. Neuropsychol. 34, 397–402.doi: 10.1080/02643294.2017.1324950
Conner, P., Goral, M., Anema, I., Borodkin, K., Haendler, Y., Knoph, M., et al. (2018). The role of language proficiency and linguistic similarity in crosslinguistic treatment effects in aphasia. J. Clin. Linguist. Phon. 32, 739–757. doi: 10.1080/02699206.2018.1435723
Costa, A., Calabria, M., Marne, P., Hernández, M., Juncadella, M., Gascón-Bayarri, J., et al. (2012). On the parallel deterioration of lexico-semantic processes in the bilinguals' two languages: evidence from Alzheimer's disease. Neuropsychologia 50, 740–753. doi: 10.1016/j.neuropsychologia.2012.01.008
*Croft, S., Marshall, J., Pring, T., and Hardwick, M. (2011). Therapy for naming difficulties in bilingual aphasia: which language benefits? Int. J. Lang. Commun. Disord. 46, 48–62. doi: 10.3109/13682822.2010.484845
*Crutch, S. J., Ridha, B. H., and Warrington, E. K. (2006). The different frameworks underlying abstract and concrete knowledge: evidence from a bilingual patient with a semantic refractory access dysphasia. Neurocase 12, 151–163. doi: 10.1080/13554790600598832
*Dai, E. Y. L., Kong, A. P. H., and Weekes, B. S. (2012). Recovery of naming and discourse production: a bilingual anomic case study. Aphasiology 26, 737–756. doi: 10.1080/02687038.2011.645013
*Dash, T., and Kar, B. R. (2014). Bilingual language control and general purpose cognitive control among individuals with bilingual aphasia: evidence based on negative priming and flanker tasks. Behav. Neurol. 2014:679706. doi: 10.1155/2014/679706
*de Diego Balaguer, R., Costa, A., Sebasti'an-Gall'es, N., Juncadella, M., and Caramazza, A. (2004). Regular and irregular morphology and its relationship with agrammatism: evidence from two Spanish-Catalan bilinguals. Brain Lang. 91, 212–222. doi: 10.1016/j.bandl.2004.02.007
*Edmonds, L. A., and Kiran, S. (2006). Effect of semantic naming treatment on crosslinguistic generalization in bilingual aphasia. J. Speech Lang. Hear. Res. 49:729. doi: 10.1044/1092-4388(2006/053)
Fabbro, F. (2001). The bilingual brain: bilingual aphasia. Brain Lang. 79, 201–210. doi: 10.1006/brln.2001.2480
Faroqi-Shah, Y., Frymark, T., Mullen, R., and Wang, B. (2010). Effect of treatment for bilingual individuals with aphasia: a systematic review of the evidence. J. Neurolinguist. 23, 319–341. doi: 10.1016/j.jneuroling.2010.01.002
*Faroqi-Shah, Y., and Waked, A. N. (2010). Grammatical category dissociation in multilingual aphasia. Cogn. Neuropsychol. 27, 181–203. doi: 10.1080/02643294.2010.509340
Fleiss, J., Levin, B., and Paik, M. (2003). Statistical Methods for Rates and Proportions, 3rd Edn. New York, NY: Wiley and Sons.
*García-Caballero, A., García-Lado, I., González-Hermida, J., Area, R., Recimil, M. J., Juncos Rabadán, O., et al. (2007). Paradoxical recovery in a bilingual patient with aphasia after right capsuloputaminal infarction. J. Neurol. Neurosurg. Psychiatry 78, 89–91. doi: 10.1136/jnnp.2006.095406
Gates, N. J., and March, E. G. (2016). A Neuropsychologist' s guide to undertaking a systematic review for publication: making the most of PRISMA guidelines. Neuropsychol. Rev. 26, 109–120. doi: 10.1007/s11065-016-9318-0
*Gil, M., and Goral, M. (2004). Nonparallel recovery in bilingual aphasia: effects of language choice, language proficiency, and treatment. Int. J. Bilingualism 8, 191–219. doi: 10.1177/13670069040080020501
Giussani, C., Roux, F. E., Lubrano, V., Gaini, S. M., and Bello, L. (2007). Review of language organisation in bilingual patients: what can we learn fromdirect brain mapping? Acta Neurochir. 149, 1109–1116. doi: 10.1007/s00701-007-1266-2
Gollan, T. H., and Kroll, J. F. (2001). “Lexical access in bilinguals,” in A Handbook of Cognitive Neuropsychology:What Deficits Reveal About the HumanMind, ed. B. Rapp (New York, NY: Psychology Press), 321–345.
Gollan, T. H., Starr, J., and Ferreira, V. S. (2015). More than use it or lose it: the number-of-speakers effect on heritage language proficiency. Psychonomic Bull. Rev. 22, 147–155. doi: 10.3758/s13423-014-0649-7
Goral, M. (2012). “Cross-language treatment effects in multilingual aphasia,” in Aspects of Multilingual Aphasia, eds M. R. Gitterman, M. Goral, and L. K. Obler (Bristol, UK: Multilingual Matters), 106–121.
Goral, M. (2019). “Acquired reading disorders in bilingualism,” in Handbook of the Neuroscience of Multilingualism, ed J. W. Schwieter (Hoboken, NJ: J-Blackwell), 592–607.
*Goral, M., Levy, E. S., and Kastl, R. (2010). Cross-language treatment generalization: A case of trilingual aphasia. Aphasiology 24, 170–187. doi: 10.1080/02687030902958308
*Goral, M., Levy, E. S., Obler, L. K., and Cohen, E. (2006). Cross-language lexical connections in the mental lexicon: evidence from a case of trilingual aphasia. Brain Lang. 98, 235–247. doi: 10.1016/j.bandl.2006.05.004
*Goral, M., Naghibolhosseini, M., and Conner, P. S. (2013). Asymmetric inhibitory treatment effects in multilingual aphasia. Cogn. Neuropsychol. 30, 564–577. doi: 10.1080/02643294.2013.878692
*Goral, M., Rosas, J., Conner, P. S., Maul, K. K., and Obler, L. K. (2012). Effects of language proficiency and language of the environment on aphasia therapy in a multilingual. J. Neurolinguist. 25, 538–551.doi: 10.1016/J.JNEUROLING.2011.06.001
*Gray, T., and Kiran, S. (2013). A theoretical account of lexical and semantic naming deficits in bilingual aphasia. J. Speech Lang. Hear. Res. 56, 1314–1327. doi: 10.1044/1092-4388(2012/12-0091)
*Gray, T., and Kiran, S. (2016). The relationship between language control and cognitive control in bilingual aphasia. Bilingualism Lang. Cogn. 19, 433–452. doi: 10.1017/S1366728915000061
Green, D. (2003). “Neural basis of lexicon and grammar in L2 acquisition: the convergence hypothesis,” in The Interface Between Syntax and the Lexicon in Second Language Acquisition, eds R. van Hout, A. Hulk, F. Kuiken, and R. Towell (Amsterdam: John Benjamins), 197–208.
*Green, D. W., Grogan, A., Crinion, J., Ali, N., Sutton, C., and Price, C. J. (2010). Language control and parallel recovery of language in individuals with aphasia. Aphasiology 24, 188–209. doi: 10.1080/02687030902958316
*Green, D. W., Ruffle, L., Grogan, A., Ali, N., Ramsden, S., Schofield, T., et al. (2011). Parallel recovery in a trilingual speaker: the use of the bilingual aphasia test as a diagnostic complement to the comprehensive aphasia test. Clin. Linguist. Phon. 25, 499–512. doi: 10.3109/02699206.2011.560990
Grodzinsky, Y., Piñango, M. M., Zurif, E., and Drai, D. (1999). The critical role of group studies in neuropsychology: comprehension regularities in Broca's aphasia. Brain Lang. 67, 134–147. doi: 10.1006/brln.1999.2050
Grosjean, F. (1982). Life with Two Languages: An Introduction to Bilingualism. Cambridge, MA: Harvard University Press.
Grosjean, F. (2013). “Bilingualism: a short introduction,” in The Psycholinguistics of Bilingualism, eds F. Grosjean and P. Li. Sussex (Oxford: Wiley-Blackwell), 7–25.
*Jahangiri, N., Azarpazhooh, M. R., Ghaleh, M., and Seifhashemi, F. (2011). Thalamic and striatocapsular bilingual aphasia. Asia Pac. J. Speech Lang. Hear. 14, 187–196. doi: 10.1179/jslh.2011.14.4.187
Junqué, C., Vendrell, J., and Vendrell, P. (1995). “Differential impairments and specific phenomena in 50 Catalan-Spanish bilingual aphasic patients,” in Aspects of Bilingual Aphasia, ed M. Paradis (New York, NY: Elsevier Science Ltd), 177–209.
*Kambanaros, M. (2010). Action and object naming versus verb and noun retrieval in connected speech: comparisons in late bilingual Greek–English anomic speakers. Aphasiology 24, 210–230. doi: 10.1080/02687030902958332
*Kambanaros, M. (2016). Verb and noun word retrieval in bilingual aphasia: a case study of language- and modality-specific levels of breakdown. Int. J.Bilingual Educ. Bilingualism 19, 169–184. doi: 10.1080/13670050.2015.1037717
*Kambanaros, M., and Grohmann, K. K. (2011). Profiling performance in L1 and L2 observed in Greek-English bilingual aphasia using the bilingual aphasia test: a case study from Cyprus. Clin. Linguist. Phon. 25, 513–529. doi: 10.3109/02699206.2011.563899
*Kambanaros, M., Messinis, L., and Anyfantis, E. (2012). Action and object word writing in a case of bilingual aphasia. Behav. Neurol. 25, 215–222. doi: 10.3233/BEN-2012-119006
Kastenbaum, J., Bedore, L., Peña, E., Sheng, L., Mavis, I., Sebastian-Vaytadden, R., et al. (2019). The influence of proficiency and language combination on bilingual lexical access. Bilingualism 22, 300–330. doi: 10.1017/S1366728918000366
*Kendall, D., Edmonds, L., Van Zyl, A., Odendaal, I., Stein, M., and Van derMerwe, A. (2015). What can speech production errors tell us about cross-linguistic processing in bilingual aphasia? Evidence from four English/Afrikaans bilingual individuals with aphasia. S. Afr. J. Commun. Disord. 62, 1–10. doi: 10.4102/sajcd.v62i1.111
*Kiran, S., Grasemann, U., Sandberg, C., and Miikkulainen, R. (2013a). A computational account of bilingual aphasia rehabilitation. Bilingualism 16, 325–342. doi: 10.1017/S1366728912000533
*Kiran, S., and Iakupova, R. (2011). Understanding the relationship between language proficiency, language impairment and rehabilitation: evidence from a case study. Clin. Linguist. Phon. 25, 565–583. doi: 10.3109/02699206.2011.566664
*Kiran, S., and Lebel, K. (2007). Crosslinguistic semantic and translation priming in normal bilingual individuals and bilingual aphasia. Clin. Linguist. Phon. 21, 277–303. doi: 10.1080/02699200701243873
Kiran, S., Pena, E., Bedore, L., and Sheng, L. (2010). “Evaluating the Relationship between category generation and language use and proficiency,” in Paper presented at the Donostia Workshop on Neurobilingualism (San Sebastian).
*Kiran, S., and Roberts, P. M. (2010). Semantic feature analysis treatment in Spanish–English and French–English bilingual aphasia. Aphasiology 24, 231–261. doi: 10.1080/02687030902958365
*Kiran, S., Sandberg, C., Gray, T., Ascenso, E., and Kester, E. (2013b). Rehabilitation in bilingual aphasia: evidence for within- and between-language generalization. Am. J. Speech Lang. Pathol. 22:85. doi: 10.1044/1058-0360(2013/12-0085)
*Kiran, S., and Tuchtenhagen, J. (2005). Imageability effects in normal Spanish–English bilingual adults and in aphasia: evidence from naming to definition and semantic priming tasks. Aphasiology 19, 315–327. doi: 10.1080/02687030444000778
*Knoph, M. I. K. (2013). Language intervention in Arabic-English bilingual aphasia: a case study. Aphasiology 27, 1440–1458. doi: 10.1080/02687038.2013.832139
*Knoph, M. I. N., Lind, M., and Simonsen, H. G. (2015). Semantic feature analysis targeting verbs in a quadrilingual speaker with aphasia. Aphasiology 29, 1473–1496. doi: 10.1080/02687038.2015.1049583
*Knoph, M. I. N., Simonsen, H. G., and Lind, M. (2017). Cross-linguistic transfer effects of verb-production therapy in two cases of multilingual aphasia. Aphasiology 31:2017. doi: 10.1080/02687038.2017.1358447
*Kohnert, K. (2004). Cognitive and cognate-based treatments for bilingual aphasia: a case study. Brain Lang. 91, 294–302. doi: 10.1016/j.bandl.2004.04.001
*Kong, A. P., and Whiteside, J. (2015). Early recovery of a multi-lingual speaker with aphasia using Cantonese and English. Speech Lang. Hear. 18, 133–139. doi: 10.1179/2050572814Y.0000000059
Köpke, B., Schmid, M. S., Keijzer, M., and Dostert, S. (eds.). (2007). Language Attrition: Theoretical Perspectives. Amsterdam; Philadelphia, PA: John Benjamins.
*Koumanidi Knoph, M. I. (2011). Language assessment of a Farsi-Norwegian bilingual speaker with aphasia. Clin. Linguist. Phon. 25, 530–539. doi: 10.3109/02699206.2011.563900
Kumar, U. (2014). Effect of orthography over neural regions in bilinguals: Aa view from neuroimaging. Neurosci. Lett. 580, 94–99. doi: 10.1016/j.neulet.2014.07.053
*Kurland, J., and Falcon, M. (2011). Effects of cognate status and language of therapy during intensive semantic naming treatment in a case of severe nonfluent bilingual aphasia. Clin. Linguist. Phon. 25, 584–600. doi: 10.3109/02699206.2011.565398
Lambon Ralph, M. A., Patterson, K., and Plaut, D. C. (2011). Finite case-series or infinite single-case studies? Comments on “Case-series investigations in cognitive neuropsychology” by Schwartz and Dell (2010). Cogn. Neuropsychol. 28, 466–474. doi: 10.1080/02643294.2012.671765
*Lee, B., Moon, H. I., Lim, S. H., Cho, H., Choi, H., and Pyun, S. B. (2016). Recovery of language function in Korean-Japanese crossed bilingual aphasia following right basal ganglia hemorrhage. Neurocase 22, 300–305. doi: 10.1080/13554794.2016.1141966
Lehtonen, M., Soveri, A., Laine, A., Järvenpää, J., de Bruin, A., and Antfolk, J. (2018). Is bilingualism associated with enhanced executive functioning in adults? A meta-analytic review. Psychol. Bull. 144, 394–425. doi: 10.1037/bul0000142
*Levy, E. S., Goral, M., Castelluccio De Diesbach, C., and Law, F. (2011). Stronger accent following a stroke: the case of a trilingual with aphasia. Clin. Linguist. Phon. 25, 815–830. doi: 10.3109/02699206.2011.570408
Libben, M. (2017). “Non-selective language activation and bilingualism as the default mental lexicon,” in Bilingualism: A Framework for Understanding the Mental Lexicon, eds M. Libben, M. Goral, and G. Libben (John Benjamins), 103–122.
Linck, J. A., Kroll, J. F., and Sunderman, G. (2009). Losing access to the native language while immersed in a second language: evidence for the role of inhibition in second- language learning. Psychol. Sci. 20, 1507–1515. doi: 10.1111/j.1467-9280.2009.02480.x
Lorenzen, B., and Murray, L. L. (2008). Bilingual aphasia: a theoretical and clinical review. Am. J. Speech Lang. Pathol. 17, 299–317. doi: 10.1044/1058-0360(2008/026)
*Mariën, P., van Dun, K., Van Dormael, J., Vandenborre, D., Keulen, S., Manto, M., et al. (2017). Cerebellar induced differential polyglot aphasia: a neurolinguistics and fMRI study. Brain Lang. 175, 18–28. doi: 10.1016/j.bandl.2017.09.001
*McCann, C., Lee, T., Purdy, S. C., and Paulin, A. K. (2012). The use of the bilingual aphasia test with a bilingual Mandarin-New Zealand English speaker with aphasia. J. Neurolinguist. 25, 579–587. doi: 10.1016/j.jneuroling.2011.04.001
McCloskey, M., and Caramazza, A. (1988). Theory and methodology in cognitive neuropsychology: a response to our critics. Cogn. Neuropsychol. 5, 583–623, doi: 10.1080/02643298808253276
*Meinzer, M., Obleser, J., Flaisch, T., Eulitz, C., and Rockstroh, B. (2007). Recovery from aphasia as a function of language therapy in an early bilingual patient demonstrated by fMRI. Neuropsychologia, 45, 1247–1256. doi: 10.1016/j.neuropsychologia.2006.10.003
Menn, L., and Obler, L. K. (eds.). (1990). Agrammatic Aphasia: A Cross-Language Narrative Sourcebook. Amsterdam; Philadelphia, PA: John Benjamins Publishing, CO. 1369–1389.
*Miller Amberber, A. (2012). Language intervention in French-English bilingual aphasia: evidence of limited therapy transfer. J. Neurolingu. 25, 588–614. doi: 10.1016/j.jneuroling.2011.10.002
Miozzo, M., Costa, A., Hernández, M., and Rapp, B. (2010). Lexical processing in the bilingual brain: evidence from grammatical/morphological deficits. Aphasiology 24, 262–287. doi: 10.1080/02687030902958381
*Munarriz, A., Ezeizabarrena, M. J., and Gutierrez-Mangado, M. J. (2016). Differential and selective morpho-syntactic impairment in Spanish-Basque bilingual aphasia. Bilingualism 19, 810–833. doi: 10.1017/S136672891400042X
*Muñoz, M. L., and Marquardt, T. P. (2003). Picture naming and identification in bilingual speakers of Spanish and English with and without aphasia. Aphasiology 17, 1115–1132. doi: 10.1080/02687030344000427
Muñoz, M. L., and Marquardt, T. P. (2004). The influence of language context on lexical retrieval in the discourse of bilingual speakers with aphasia. J. Multilingual Commun. Disord. 2, 1–17. doi: 10.1080/14769670310001625345
Muñoz, M. L., Marquardt, T. P., and Copeland, G. (1999). A comparison of the code switching patterns of aphasic and neurologically normal bilingual speakers of English and Spanish. Brain Lang. 66, 249–274. doi: 10.1006/brln.1998.2021
Nadeau, S. E. (2019). Bilingual aphasia: explanations in population encoding. J. Neurolingu. 49, 117–143. doi: 10.1016/j.jneuroling.2018.10.002
*Neumann, Y., Walters, J., and Altman, C. (2017). Codeswitching and discourse markers in the narratives of a bilingual speaker with aphasia. Aphasiology 31, 221–240. doi: 10.1080/02687038.2016.1184222
Nickels, L., Howard, D., and Best, W. (2011). On the use of different methodologies in cognitive neuropsychology: drink deep and from several sources. Cogn. Neuropsychol. 28, 475–485. doi: 10.1080/02643294.2012.672406
Nilipour, R., and Paradis, M. (1995). “Breakdown of functional categories in three Farsi–English bilingual aphasic patients,” in Aspects of Bilingual Aphasia, ed M. Paradis (Oxford, UK: Pergamon Press), 123–138.
Paradis, M. (1977). “Bilingualism and aphasia,” in Studies in Neurolinguistics, H. Whitaker and H. A.Whitaker (New York, NY: Academic Press), 65–121.
Paradis, M. (ed.). (1983). Readings on Aphasia in Bilinguals and Polyglots. Montreal, QC: Marcel Didier.
Paradis, M. (2001). “Bilingual and polyglot aphasia,” in Language and Aphasia, ed R. S. Berndt (Amsterdam: Elsevier Science), 69–91.
Paradis, M. (2004). A Neurolinguistic Theory of Bilingualism. Amsterdam; Philadelphia, PA: John Benjamins.
Paradis, M., and Libben, G. (1987). The Assessment of Bilingual Aphasia. Hillsdale, NJ: Lawrence Erlbaum.
Peñaloza, C., Rao, L., and Kiran, S. (2017). “The association between language use and proficiency and L2 performance in bilingual adults with aphasia. Front. Hum. Neurosci,” in Conference Abstract: Academy of Aphasia 55th Annual Meeting. (Baltimore, Maryland).
Perani, D., and Abutalebi, J. (2005). The neural basis of first and second language processing. Curr. Opin. Neurobiol. 15, 202–206. doi: 10.1016/j.conb.2005.03.007
Perani, D., Paulesu, E., Galles, N. S., Duoux, E., De-haene, S., Bettibardi, V., Cappa, S., et al. (1998). Bilingual brain: proficiency and age of acquisition in a second language. Brain 121, 1841–1852
Pitres, A. (1895/1983). “Aphasia in polyglots,” in Readings on Aphasia in Bilinguals and Polyglots, ed M. Paradis (Montreal, QC: Marcel Didier), 26–49.
*Poncelet, M., Majerus, S., Raman, I., Warginaire, S., and Weekes, B. S. (2007). Naming actions and objects in bilingual aphasia: a multiple case study. Brain Lang. 103, 158–159. doi: 10.1016/j.bandl.2007.07.078
Pot, A., Keijzer, M., and De Bot, K. (2018). The language barrier in migrant aging. Int. J. Bilingual Educ. Bilingual. 2018, 1–19. doi: 10.1080/13670050.2018.1435627
*Radman, N., Mouthon, M., Di Pietro, M., Gaytanidis, C., Leemann, B., Abutalebi, J., et al. (2016a). The role of the cognitive control system in recovery from bilingual aphasia: a multiple single-case fMRI study. Neural Plasticity 2016:7086. doi: 10.1155/2016/8797086
*Radman, N., Spierer, L., Laganaro, M., Annoni, J. M., and Colombo, F. (2016b). Language specificity of lexical-phonological therapy in bilingual aphasia: a clinical and electrophysiological study. Neuropsychol. Rehabil. 26, 532–557. doi: 10.1080/09602011.2015.1047383
*Raman, I., and Weekes, B. S. (2005). Acquired dyslexia in a Turkish-English speaker. Ann. Dyslexia 55, 79–104. doi: 10.1007/s11881-005-0005-8
Rapp, B. (2011). Case-series in cognitive neuropsychology: promise, perils, and proper perspective. Cogn. Neuropsychol. 28, 435–444. doi: 10.1080/02643294.2012.697453
Ribot, T. A. (1882). Diseases of Memory: An Essay in the Positive Psychology. New York, NY: Appleton.
Roberts, P. M., and Deslauriers, L. (1999). Picture naming of cognate and non-cognate nouns in bilingual aphasia. J. Commun. Disord. 32, 1–23. doi: 10.1016/S0021-9924(98)00026-4
Roberts, P. M., and Kiran, S. (2007). “Assessment and treatment of bilingual aphasia and bilingual anomia,” in Ramos Speech and Language Disorders in Bilinguals, eds A. Ardila and E. Ramos (New York, NY: Nova Science), 109–130.
Rochford, G., and Williams, M. (1965). Studies in the development and breakdown of the use of names. J. Neurol. Neurosurg. Psychiatry 28, 407–413.
Rothman, J. (2015). Linguistic and cognitive motivations for the Typological Primacy Model (TPM) of third language (L3) transfer: timing of acquisition and proficiency considered. Bilingual. Lang. Cogn. 18, 179–190. doi: 10.1017/S136672891300059X
*Samar, R. G., and Akbari, M. (2012). A language teacher in the haze of bilingual aphasia: a Kurdish-Persian case. Proc. Soc. Behav. Sci. 32, 252–257. doi: 10.1016/j.sbspro.2012.01.037
Schepens, J., Dijkstra, T., Grootjen, F., and van Heuven, W. J. (2013). Crosslanguage distributions of high frequency and phonetically similar cognates. PLoS ONE 8:e63006. doi: 10.1371/journal.pone.0063006
Schwartz, M. F., and Dell, G. S. (2010). Case-series investigations in cognitive neuropsychology. Cogn. Neuropsychol. 27, 477–494. doi: 10.1080/02643294.2011.574111
Shallice, T. (1979). Case study approach in neuropsychological research. J. Clin. Neuropsychol. 1, 183–211. doi: 10.1080/01688637908414450
*Siyambalapitiya, S., Chenery, H. J., and Copland, D. A. (2013). Lexicalsemantic representation in bilingual aphasia: findings from semantic priming and cognate repetition priming. Aphasiology 27, 1302–1321. doi: 10.1080/02687038.2013.817521
Swain, M. (1985). “Communicative competence: some roles of comprehensible input and comprehensible output in its development,” in Input in Second Language Acquisition, eds S. Gass and C. Madden (Rowley, MA: Newbury House), 235–253.
*Theron, K., van der Merwe, A., Robin, D. A., and Groenewald, E. (2009). Temporal parameters of speech production in bilingual speakers with apraxic or phonemic paraphasic errors. Aphasiology 23, 557–583. doi: 10.1080/02687030701801717
*Tiwari, S., and Krishnan, G. (2015). Selective L2 cognate retrieval deficit in a bilingual person with aphasia: a case report. Speech Lang. Hear. 18, 243–248. doi: 10.1179/2050572815Y.0000000008
Tomoschuk, B., Ferreira, V. S., and Gollan, T. H. (2018). When a seven is not a seven: self-ratings of bilingual language proficiency differ between and within language populations. Bilingualism 2018, 1–21. doi: 10.1017/S1366728918000421
*Tschirren, M., Laganaro, M., Michel, P., Martory, M. D., Di Pietro, M., Abutalebi, J., et al. (2011). Language and syntactic impairment following stroke in late bilingual aphasics. Brain Lang. 119, 238–242. doi: 10.1016/j.bandl.2011.05.008
Ullman, M. T. (2001). A neurocognitive perspective on language: the declarative/procedural model. Nat. Rev. Neurosci. 2, 717–726. doi: 10.1038/35094573
*Verreyt, N., De Letter, M., Hemelsoet, D., Santens, P., and Duyck, W. (2013). Cognate effects and executive control in a patient with differential bilingual aphasia. Appl. Neuropsychol. 20, 221–230. doi: 10.1080/09084282.2012.753074
Viechtbauer, W. (2010). Conducting meta-analyses in R with the metafor package. J. Stat. Softw. 36, 1–48. doi: 10.18637/jss.v036.i03
Vilariño, I., Prieto, J. M., Robles, A., Lema, M., and Noya, M. (1997). A study of bilingual Galician-Castilian aphasic patients. Rev. Neurol. 25, 1165–1167.
Weekes, B. S. (2005). Acquired disorders of reading and writing: crossscript comparisons. Behav. Neurol. 16, 51–57. doi: 10.1155/2005/492935
Weekes, B. S. (2010). Issues in bilingual aphasia: an introduction. Aphasiology 24, 123–125. doi: 10.1080/02687030902958274
Weekes, B. S. (2012). Acquired dyslexia and dysgraphia across scripts. Behav. Neurol. 25, 159–163. doi: 10.3233/BEN-2012-119000
*Weekes, B. S., Su, I.-F., Yin, W., and Zhang, X. (2007). Oral reading in bilingual aphasia: evidence from Mongolian and Chinese. Bilingual. Lang. Cogn. 10, 201–210. doi: 10.1017/s1366728907002945
Wong, B., Yin, B., and O'Brien, B. (2016). Neurolinguistics: structure, function, and connectivity in the bilingual brain. BioMed. Res. Int. 2016, 1–22. doi: 10.1155/2016/7069274
*^References marked with an asterisk indicate studies included in the present meta-analysis.
Keywords: bilingual aphasia, stroke, linguistic similarity, AoA, premorbid proficiency, language use, meta-analysis
Citation: Kuzmina E, Goral M, Norvik M and Weekes BS (2019) What Influences Language Impairment in Bilingual Aphasia? A Meta-Analytic Review. Front. Psychol. 10:445. doi: 10.3389/fpsyg.2019.00445
Received: 05 November 2018; Accepted: 13 February 2019;
Published: 04 April 2019.
Edited by:
Gonia Jarema, Université de Montréal, CanadaReviewed by:
Arturo Hernandez, University of Houston, United StatesCopyright © 2019 Kuzmina, Goral, Norvik and Weekes. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ekaterina Kuzmina, cmluYS5rdXptaW5hQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.