
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychol., 08 January 2019
Sec. Psychology for Clinical Settings
Volume 9 - 2018 | https://doi.org/10.3389/fpsyg.2018.02655
This article is part of the Research TopicThe State of the Art in Creative Arts TherapiesView all 37 articles
 Kim Dunphy1*
Kim Dunphy1* Felicity A. Baker1
Felicity A. Baker1 Ella Dumaresq1
Ella Dumaresq1 Katrina Carroll-Haskins2
Katrina Carroll-Haskins2 Jasmin Eickholt1,3
Jasmin Eickholt1,3 Maya Ercole1
Maya Ercole1 Girija Kaimal2
Girija Kaimal2 Kirsten Meyer1
Kirsten Meyer1 Nisha Sajnani4
Nisha Sajnani4 Opher Y. Shamir4Thomas Wosch3
Opher Y. Shamir4Thomas Wosch3Depression experienced by older adults is proving an increasing global health burden, with rates generally 7% and as high as 27% in the USA. This is likely to significantly increase in coming years as the number and proportion of older adults in the population rises all around the world. Therefore, it is imperative that the effectiveness of approaches to the prevention and treatment of depression are understood. Creative arts interventions, including art, dance movement, drama, and music modalities, are utilized internationally to target depression and depressive symptoms in older adults. This includes interventions led by trained arts therapists as well as other health and arts professionals. However, to date there has not been a systematic review that reports effects and examines the processes (why) and mechanisms (how) of creative arts interventions are used to address depression in this older age group. This systematic review of studies on creative arts interventions for older adults experiencing depression examined: outcomes of four creative arts modalities (art, dance movement, drama, and music); with particular attention paid to processes documented as contributing to change in each modality; and mechanisms considered to result from these processes. Our analysis of 75 articles (17 art, 13 dance, 4 drama, and 41 music) indicates mostly significant quantitative or positive qualitative findings, particularly for interventions led by creative arts therapists. Mechanisms of change gleaned from the studies that were common across modalities include physical (e.g., increased muscle strength; neurochemical effects, such as endorphin release), intra-personal (e.g., enhanced self-concept, strengthened agency and mastery; processing and communication of emotions), cultural (e.g., creative expression, aesthetic pleasure), cognitive (e.g., stimulation of memory), and social (e.g., increased social skills and connection), that were all considered to contribute to reduced depression and symptoms. Recommendations for future research includes stronger focus on testing of processes and mechanisms.
The number and proportion of older adults in the population has increased in virtually every country in the world over past decades, because of increased life expectancy and decreased fertility (United Nations Department of Economic Social Affairs Population Division, 2015). Current trends indicate an even greater global population of older people in coming years, with an estimated increase from about 12–22% (900 million to 2 billion) between 2015 and 2050 (Naghavi et al., 2015; World Health Organization, 2017b). Therefore, health issues impacting older adults are likely to make a significant contribution to the global health burden in coming decades (United Nations Department of Economic Social Affairs Population Division, 2017).
Depression affects approximately 7% of the world's older adults (World Health Organization, 2017a), with the highest rates in countries including Australia (10–15%) (National Ageing Research Institute, 2009) and USA (up to 27% with major depression and 31% with depressive symptoms) (Mental Health America, 2018). The most significant challenges are faced by older adults living in residential aged care, with rates as high as 35% (National Ageing Research Institute, 2009). Depression is three to four times more common in older people who have dementia (Bennett and Thomas, 2014). While prevalence is the same for both genders, functional disability causes by depression is greater for men (Forlani et al., 2014).
Depression is identified as the fourth leading cause of disability worldwide, and likely to be the second leading cause by 2020 (Murray and Lopez, 1996a,b). Depression leads to impaired functioning in daily life and can cause great suffering (Fiske et al., 2010). Depression also increases the perception of poor health, and the utilization of health care services and costs. Older adults with depressive symptoms have poorer functioning compared to those with other chronic medical conditions and higher rates of suicide. Mental health issues such as depression also impact physical health and vice versa (Bruce et al., 1994; Mental Health Foundation, 2018). Causes of depression are considered to include reduced involvement in daily life activities. This may be accompanied by self-critical thinking, which can exacerbate a depressed state. Protective factors relevant for depression in later life include age-related increases in psychological resilience, higher education and socio-economic status, engagement in valued activities, and religious or spiritual involvement (Fiske et al., 2010).
Documented depression treatments include pharmacological and non-pharmacological approaches. Pharmacological treatments indicate effectiveness in addressing symptoms of depression but are also associated with unwanted side effects (Beyond Blue, 2018; Department of Health, 2018). Psychology-informed approaches (behavioral therapy, cognitive behavioral therapy, cognitive bibliotherapy, problem-solving therapy, brief psychodynamic therapy and life review/reminiscence are indicated as effective (see for example, Thompson et al., 1987; Arean et al., 1993; Hsieh and Wang, 2003; Qualls and Knight, 2006). Preventive interventions including education, behavioral activation, cognitive restructuring, problem-solving skills training, group support, and life review have also received support (Fiske et al., 2010).
Creative arts (CA) modalities, including dance movement, drama, music, and visual arts, are also utilized internationally to target depression and associated symptoms. These include interventions by creative arts therapists (CAT) and by other therapists and health and arts professionals. While no systematic reviews have yet been published that examine research on depression and older adults across the CATs, previous reviews have been published for these modalities separately and for different age groups.
Two systematic reviews on art therapy (AT) and depression indicate that, for an all ages sample, art therapy has been utilized successfully (Blomdahl et al., 2013) and presents a cost-effective treatment model for mental health symptoms (Stevenson et al., 2015). In dance movement therapy (DMT), one systematic review of an all ages sample found that DMT may be beneficial for people experiencing depression, but without certainty because of small number of studies and low quality of evidence (Meekums et al., 2015). A meta-analysis of DMT studies including a sub-analysis for depression concluded that DMT may be effective in decreasing clinical symptoms (Koch et al., 2014). No systematic reviews on drama therapy (DT) for depression were found.
In music and music therapy (MT), a significant number of reviews indicate this modality's potential to support: reduced risk (Daykin et al., 2018); prevention (Sun et al., 2013); and decreased depression (Seinfeld et al., 2013; Chang et al., 2015; Innes et al., 2016; Travers et al., 2016; Zhao et al., 2016; Istvandity, 2017; Quach, 2017; van der Steen et al., 2017). Yet other music reviews reported no changes in depression (Ziv et al., 2008; Johnson et al., 2013; Vasionyte and Madison, 2013; Petrovsky et al., 2015; Xu et al., 2017).
A set of metaprocesses known as ‘common factors’ are understood to support growth and change through therapy (Ahessy, 2013). These common factors are largely informed by humanistic approaches to therapy which emphasize client-centered care (Rogers, 1951). They include therapeutic alliance, safety, empathy, inclusion, and unconditional positive regard (Wampold, 2001; Carr, 2008; Imel and Wampold, 2008).
While common factors are applicable to the creative arts therapies, there are additional processes employed in these approaches. Other therapies often target only cognitive processes, whereas the CATs seek to engage clients holistically across somatic, cognitive, emotional/intrapersonal, cultural (creative/aesthetic), and social/interpersonal aspects of the self. The integration of body and mind, or psyche, is a fundamental process of both DMT (Meekums, 2002; Sherwood, 2008) and AT, in which a “bodymind model” is proposed as a key contributor to change on a more meta level (Czamanski-Cohen and Weihs, 2016). In DT, core processes that reflect a holistic approach have been identified (Jones, 2007) along with metaprocesses (Cassidy et al., 2014) such as establishing safety, working in the here and now, being actively involved within or outside of the aesthetic frame, and working alongside the client while offering choice and control.
Adaptability is another technique employed in common by CA therapists, with methods, techniques, choices of medium and intervention styles adapted by therapists to best support the needs of each client or group, demonstrating responsivity to context and “attunement” (Kossak, 2009, 2015; Vermes, 2011; Holck and Geretsegger, 2016; Devereaux, 2017).
Finally, Koch (2017) has proposed key aesthetic processes that further distinguish the arts therapies from other approaches, such as intrinsic pleasure, authentic coherence, symbolism, transitional practices, and generativity. The application of processes that lead to and emerge from aesthetic expression are fundamental and most distinguishing of CAs from other types of therapy.
However, despite all this research, as yet there has not been a systematic review of the literature on the impact of CA interventions, both those that are led by CA therapists and other professionals, on depression and depressive symptoms in older adults and how these interventions are considered to work.
This article offers a systematic literature review on the use of creative arts interventions to target depression and depressive symptoms in older adults. The article reports: outcomes of interventions across four creative arts modalities (arts, dance movement, drama, and music), for older adults experiencing depression or depressive symptoms; interventions implemented; and processes and mechanisms understood to contribute to therapeutic change.
Our overarching research questions are: What are the effects of creative arts interventions on depression or depressive symptoms in older adults? How are these interventions understood to work?
This review examined studies about CA interventions, including CA therapy, intended to address depression or depressive symptoms, in older adults, across four modalities: art; dance; drama; and music; and combinations of these.
We examined studies utilizing all types of research methods and designs and did not specify particular comparators. We entered our review on the Prospero (International prospective register of systematic reviews) register (Centre for Reviews Dissemination, 2018) with registration number CRD42018091901.
This review included only articles that were:
• Published between 1.1.1997 and 1.2.18, in English language only;
• Of research, defined as investigation of a research question informed by quantitative or qualitative data, or both, including case studies and doctoral theses;
• Included only participants who were older adults (over 60 years, as per WHO definition) who had depression, as defined by DSM-V or ICD, and/or co-morbidity, or depressive symptoms with or without other disorders;
• Utilized a CA modality as an intervention to address such symptoms. This included CATs, which we define as interventions led by a CA therapist who were identified in the article as being trained or registered as a CAT in their specific modality, and other CA interventions led by other professionals;
• Locatable by the researchers.
We used the advanced search function on OVID, including databases: OVID Medliner (1946-present); CINAHL; EMBASE (Excerta Medica database); Medline; PsychINFO; Cochrane Central control trial register and Cochrane systematic reviews.
The following search terms were used:
• “depression” or “depress*” or “MDD” (major depressive disorder); “LLD” (late life depression)
• AND “older adults” or “old*” or “gerontology” “geriatric*” or “late-life” or “aged care” or “aged” or “aging” or” “elderly”
• Art therapy: “art therap*” or “arts therap*” or “art psychotherap**” or “visual art therap*”
• Dance movement: “dance therap*” or “dance movement therap*” or “dance movement psychotherap*” or “dance/movement therap*” or “movement therap*” or “movement psychotherap**” or “dance” or “dance effectiveness” or “therapeutic movement”
• Drama: “drama*therap*” or “psychodrama” or “psychodramatic drama*therap*” or “process* of change” or “applied drama” or “therapeutic theat*” or “improvi*ation” or “reminiscence theat*”
• Music: “song” or “guided imagery music” or improvi*ation” or song*writing” or “rap therap*” or “drum*” or “sing” or “choir” or “music” or “listen*”or “receptive music therap*.”
The first search process, and round of decision-making concerning inclusion-exclusion was undertaken by a junior researcher with expertise in each field [authors KC-H (AT), ED (DMT), ME (DT), and JE (MT)]. The second process of assessment against the data extraction points listed below was undertaken by the same researcher, then cross-checked by a senior researcher from each field, authors: GK (AT); KD (DMT); NS (DT); KM (DT), TW (MT), and FB (MT). Where decisions between the two researchers were not concordant, discussion between them was undertaken to reach final agreement.
Data analysis was undertaken in a staged process. First, all abstracts found through our search were considered against inclusion criteria listed above. This process is depicted in a PRISMA flow chart, provided in Figure 1.
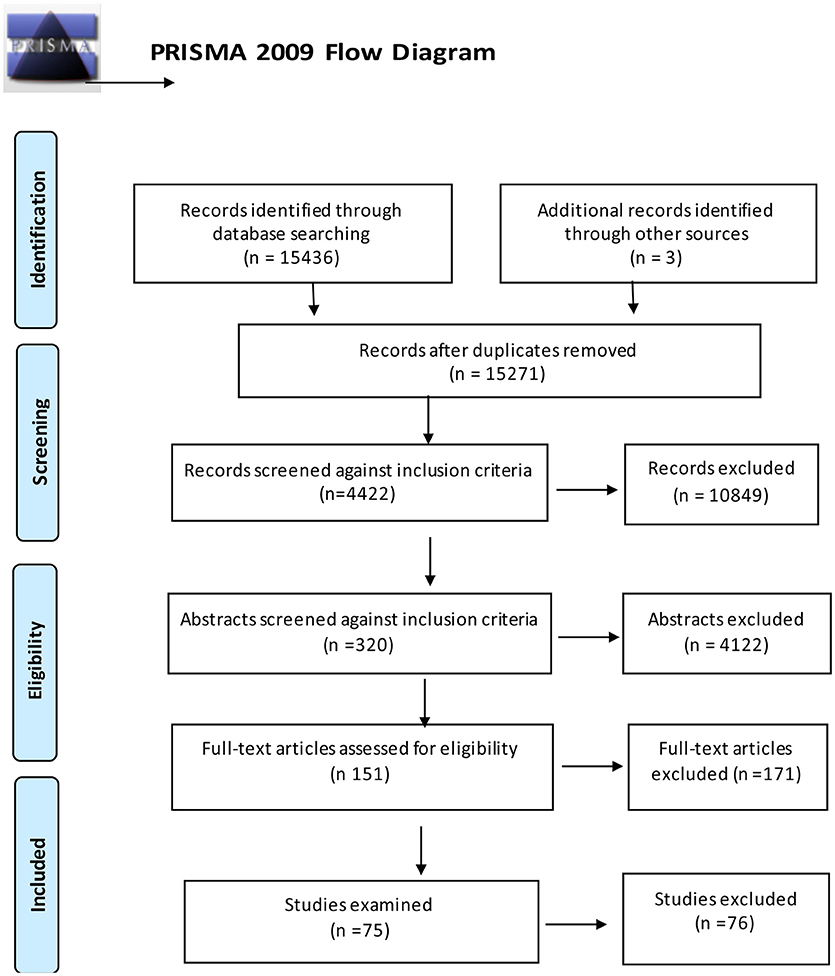
Figure 1. PRISMA flow diagram of studies retrieved.
Those fitting the criteria sufficiently were then analyzed and data extracted in the categories of: Participants—number and gender; Facilitator—training; Intervention—duration (number, length, and frequency of sessions), control/comparison, activities (what participants actually did); Outcomes—what and how assessed; Therapeutic techniques (defined as how the therapist operates in the intervention); Processes (defined as processes seen to elicit change in the client); and Mechanisms (what occurs within the client that results in change); and Study design. Articles were then assessed for quality using COREQ (qualitative studies) or PEDro tools (quantitative studies), or both tools (mixed-method studies). The COREQ is a formal checklist for evaluating the rigor and transparency of reporting in qualitative research, particularly for interviews and focus groups (Tong et al., 2007). The PEDro tool comprises elements agreed as suitable for quality assessment of RCT studies (Verhagen et al., 1998). One point was scored for each element of the study that met the criteria and these were tallied to arrive at a quality score for each study.
Seventeen art studies from an initial sample of 34 met all inclusion criteria as detailed in Table 1. Methodological approaches of these comprised: five qualitative studies, mostly individual case studies (de Guzman et al., 2011; Hoffmann, 2013) and interview methods; three mixed-methods; and nine quantitative studies, including comparisons of art therapy with other health interventions such as walking, music therapy, exercise, nature-based therapies, and community craft activities. Depression was addressed as a primary symptom (5/17); and as a co-morbid condition with Parkinson's disease (1/17), stroke (2/17), and dementia (2/17). Three studies focused on women because of the reported higher prevalence of depression with this population (3/17).
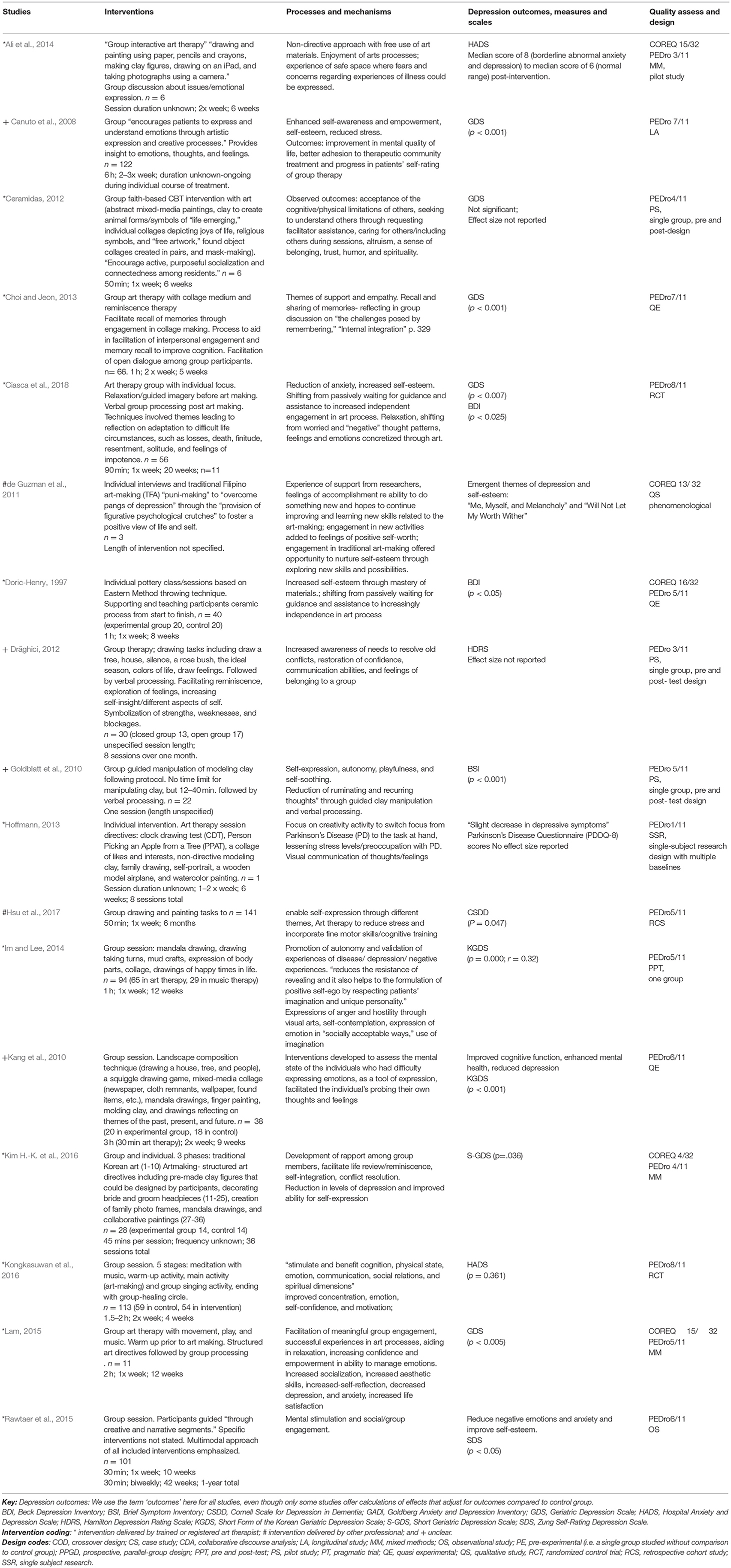
Table 1. Results of analysis of arts intervention studies.
Qualitative studies scored between 1 (2/5) and 8 (1/5) out of 11 on PEDro. The limitations of these studies included inadequate reporting details in data collection and lack of rigor in measures to ensure credibility in data analysis. Quantitative and mixed method studies scored between 4 (1/12) and 16 (2/12) out of 32 on COREQ. The main shortcomings of these studies were that samples were not randomized, blinded, or adequately powered. They tended to be small in scope and lacking rigorous efforts to ensure validity in the findings. The majority did not include adequate details on method to enable replication. No art studies reported any results from follow up.
Eleven/Seventeen studies were led by an art therapist, 2/17 by another professional; and 4/17 had a leader of unknown training. Twelve studies had significant findings: 8/12 led by an art therapist, 1/12 by another professional and 3/12 by a leader of unknown training.
Art programs were typically sessions of an hour, held once or twice a week over periods from 12 to 52 weeks. Interventions were typically offered as group format, with specific attention provided by therapists to individual group members. Two interventions were one on one programs (de Guzman et al., 2011; Hoffmann, 2013).
Art media options and activities included traditional crafts and arts (de Guzman et al., 2011; Ciasca et al., 2018) and clay and painting. For example, in one task, participants manipulated clay into a ball, divided it into parts and re-assembled it into another object, then shared their experiences in verbal discussion (Goldblatt et al., 2010). Choices of media were frequently discussed as important, particularly because of challenges identified with patients' physical mobility and fine motor control.
The therapeutic techniques reported in the art studies included the therapist being encouraging of participants' expression and learning through art making, sensitive to individual needs, encouraging of interaction and pro-social experiences between group members.
Based on the processes identified in the literature, we propose that the mechanisms of a change for depressive symptoms through art interventions are:
• Physical: engagement in a creative activity that had physical aspects was seen to catalyze relaxation and reduction of stress (Canuto et al., 2008; Goldblatt et al., 2010; Lam, 2015; Hsu et al., 2017)
• Cultural: the making of art was seen to facilitate creative expression and play (de Guzman et al., 2011; Kim H.-K. et al., 2016); the use of context-responsive creative expression was seen as significant; creative expression was enabled by use of accessible media of clay and painting (Goldblatt et al., 2010); evocation of familiarity and positive memories was catalyzed by use of culturally appropriate traditional crafts and arts (de Guzman et al., 2011; Ciasca et al., 2018)
• Emotional/intrapersonal: creation of art products was seen to provide valuable distance, and enable externalization and visual communication of inner subjective experiences (Goldblatt et al., 2010; Kang et al., 2010; Drăghici, 2012; Choi and Jeon, 2013; Ali et al., 2014; Im and Lee, 2014; Hsu et al., 2017; Ciasca et al., 2018); expression of positive and negative emotions (Kang et al., 2010; Ali et al., 2014; Im and Lee, 2014; Kim H.-K. et al., 2016; Kongkasuwan et al., 2016); promotion of autonomy (Doric-Henry, 1997; Canuto et al., 2008; Goldblatt et al., 2010; Ceramidas, 2012; Kongkasuwan et al., 2016); and positive views of self (Canuto et al., 2008; de Guzman et al., 2011; Drăghici, 2012; Rawtaer et al., 2015; Kongkasuwan et al., 2016; Ciasca et al., 2018); agency and mastery was seen to be strengthened by the act of completing an art piece (Doric-Henry, 1997; de Guzman et al., 2011; Hoffmann, 2013; Lam, 2015; Ciasca et al., 2018)
• Cognitive: art-making was seen to enable: reinforcement and recall of positive memories (Canuto et al., 2008; Choi and Jeon, 2013; Hoffmann, 2013; Kim H.-K. et al., 2016); addressing of concerns around death, loss and end of life (de Guzman et al., 2011; Ali et al., 2014); and distraction from ruminative thoughts (Goldblatt et al., 2010; Ciasca et al., 2018)
• Interpersonal: group work (with or without therapist's involvement) was seen to encourage socialization and sharing (Canuto et al., 2008; de Guzman et al., 2011; Ceramidas, 2012; Drăghici, 2012; Choi and Jeon, 2013; Ali et al., 2014; Im and Lee, 2014; Lam, 2015; Rawtaer et al., 2015; Kim H.-K. et al., 2016; Kongkasuwan et al., 2016).
Thirteen studies met all inclusion criteria from an initial sample of 29 as detailed in Table 2. Studies were predominantly RCTs (6/13); with quasi-experimental (3/13); and single condition over two or three time periods (4/13). Only one of the 13 studies was focused on depression as a primary diagnosis, with the other 12 addressing depressive symptoms.
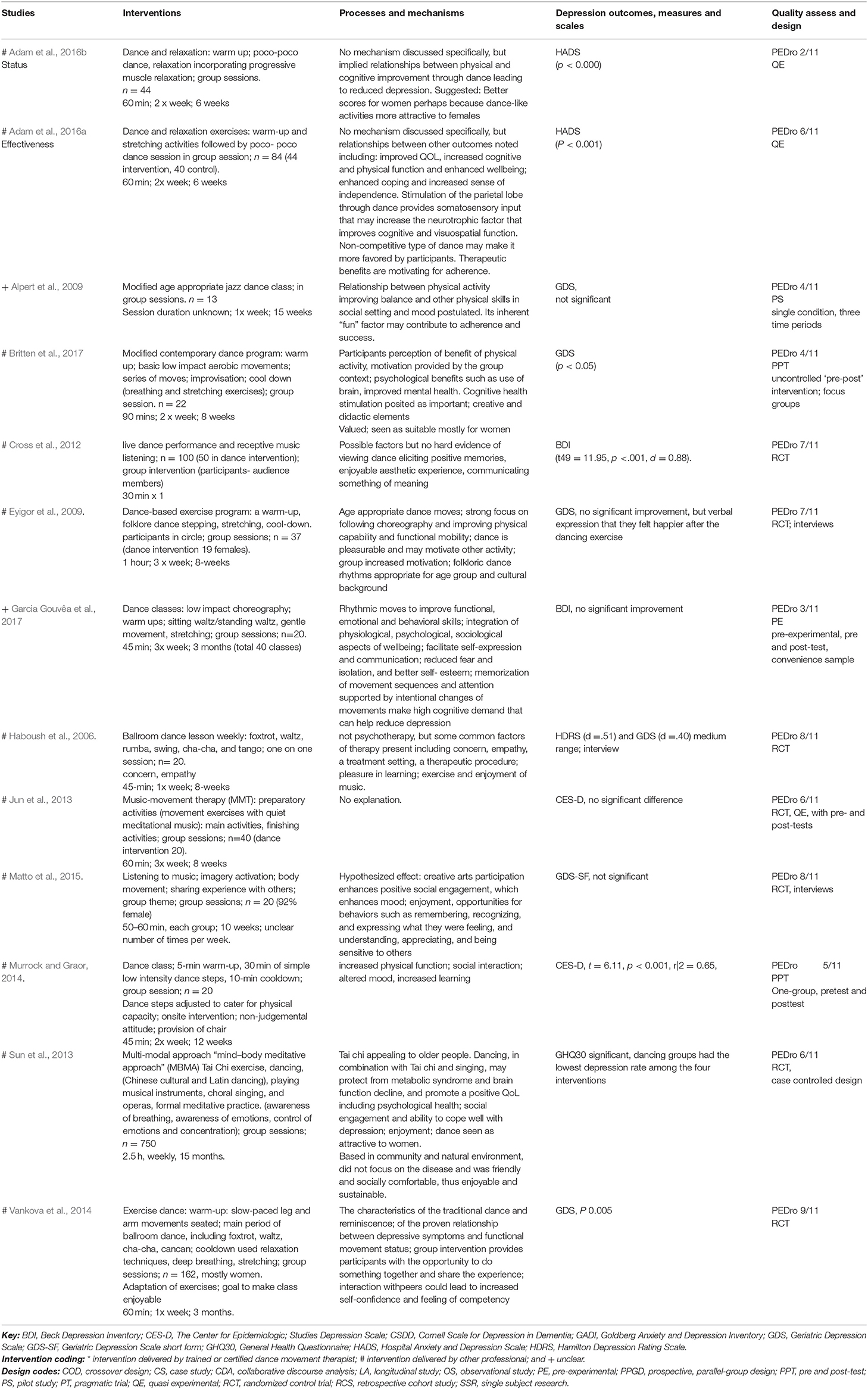
Table 2. Results of analysis of dance movement intervention studies.
Quality scores using PEDRO were evenly spread between 2 and 9 out of 11. Eleven of these studies were led by another professional; two by a leader of unknown training; and none by a dance movement therapist. This was despite several studies stating that the intervention was dance movement therapy, while providing no indication that a certified DM therapist was involved. One study (Cross et al., 2012) claimed to be DMT and included information about DMT in the literature review, but then described an intervention of clients watching professional dancers that seemed to have no relationship at all with DMT principles. In fact, no studies involving dance movement therapy were included in our final sample. Ten studies had significant findings: nine led by professional who was not a dance movement therapist, and one by a leader of unknown training.
Limitations of the dance studies included small sample sizes, with almost half having an n of 20 or less. Low PEDro scores was mostly caused by lack of concealment of allocation, lack of blinding of participants, therapists and assessors, and lack of random allocation. Another limitation was that few studies (4/13) included a mention of follow-up component. One study (Vankova et al., 2014) mentioned an improvement in GDS scores in one follow up (5.0–4.5), however, this data was not included in the results. Another study (Matto et al., 2015) reported follow up results indicating a decrease in GDS scores (2.44–2.19), supported by interviews with participants about their enjoyment in being part of the group where self-expression and understanding, appreciating and being sensitive to others was a commonly valued experience (p. 280). Two other studies mention a follow up but do not report results (Haboush et al., 2006; Jun et al., 2013).
Programs offered were typically sessions of between 30 and 90 min, with 60 min being most common; held between one and three times weekly, most often twice; for periods from one week to 15 months, most often 8 weeks. Interventions were typically offered as group sessions, with specific attention provided by trained therapists to individual group members. One study described a one on one program. Interventions were primarily focused on the acquisition and repetition of dance steps, including western dance styles such as jazz, contemporary and ballroom, as well as traditional and folk dances. Session structure most frequently was a brief warm up, then teaching of dance steps, followed by a final cool down which sometimes included relaxation.
The dance studies did not include much discussion about therapeutic processes, perhaps because none of the studies examined was led by a dance movement therapist. This was in contrast to other modalities where the majority of studies involved CA therapists. There was a strong emphasis on physical outcomes, particularly in the area of functional mobility. This was presumably because the studies were mostly facilitated by dance instructors and physical therapists who emphasized functional performance as a primary concern, which they addressed through programs that involved the acquisition of dance skills. In several studies, changes in clients' physical state through dance, such as improved balance and strengthened muscles, was seen to be related to reduced symptoms of depression, even though this had not been the central focus of the intervention. For example, Britten et al. (2017) reported reduced falls-risk as a result of dance participation, which was seen in turn to have positive impact on mood states such as depression. However, causal pathways were generally not articulated clearly or trialed in these studies.
Several studies included comment on the greater acceptance of dance-based interventions by women than men, thus explaining more successful engagement, stronger adherence, and better outcomes of female participants in many interventions.
Based on the processes identified in the literature, we propose that the mechanisms of a change for depressive symptoms through dance interventions are:
• Physical: improved physical performance and function including balance, muscle strength, joint sense and proprioception;
• Cultural: enjoyable aesthetic experiences;
• Cognitive: cognitive decline slowed through exercise and stimulation of brain circuits used to learn dance steps; activation of motor neurological brain regions through improvised or expressive movement that may contribute to changes in brain structure;
• Social: positive social engagement, stimulation and enhancement of communicative and relational capacities through shared experiences in dance.
Four studies met all inclusion criteria from an initial sample of 25 as detailed in Table 3. Methodological approaches included one quasi-experimental study (Keisari and Palgi, 2017), one mixed method (Wilkinson et al., 1998), two qualitative studies employing a combination of ethnographic observation, qualitative interviews, and practice reflections (Kontos et al., 2017) and one collaborative discourse analysis (Sajnani et al., 2018). One study addressed depression as the primary diagnosis (Keisari and Palgi, 2017), while the other three addressed depressive symptoms.
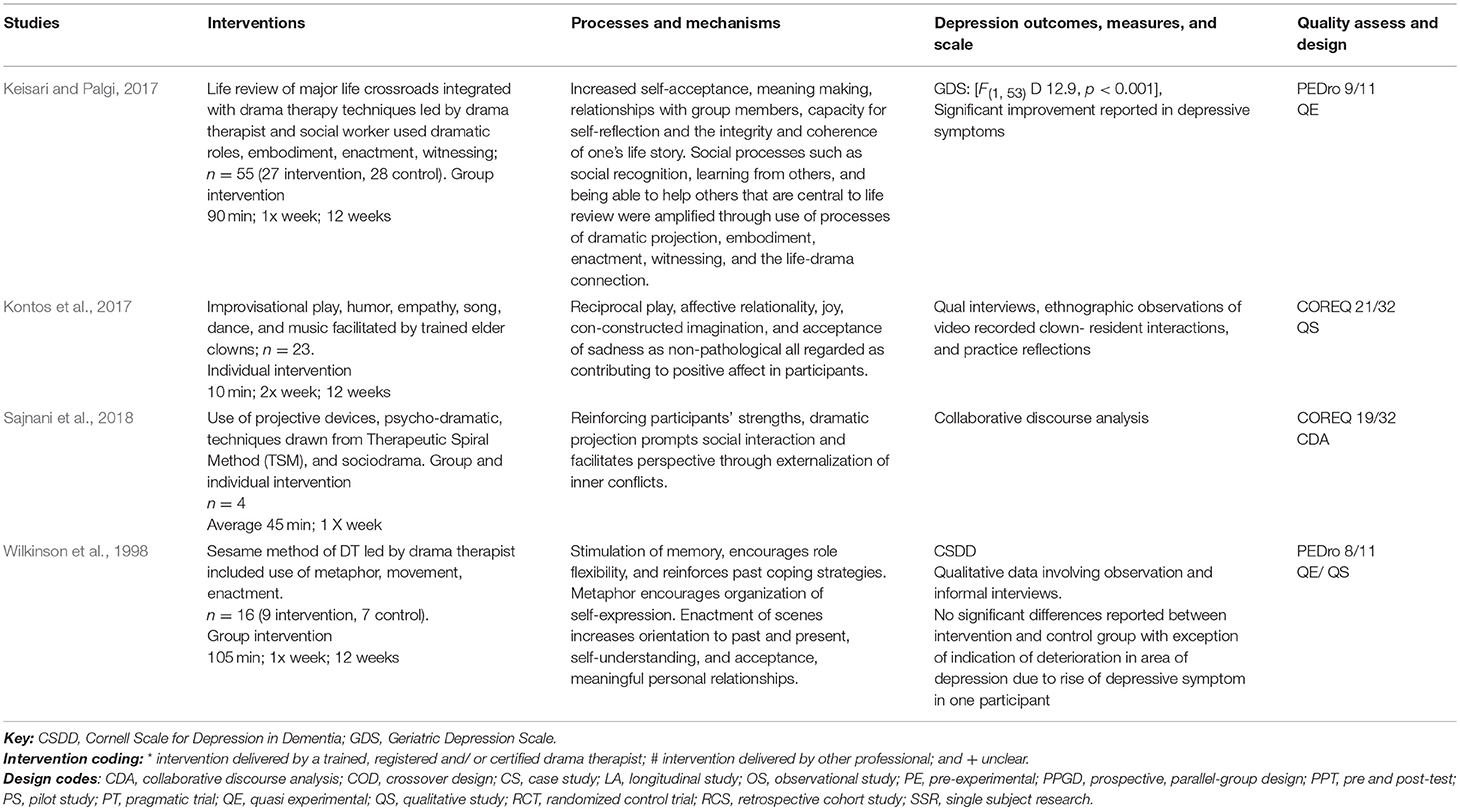
Table 3. Results of analysis of drama intervention studies.
The two studies employing quantitative methods scored between 8 and 9 out of 11 on PEDro. The limitations of these studies were that samples were small and not randomized or blinded. The two qualitative studies met between 19 and 21 elements of 32 in COREQ. The limitations of these studies included inadequate reporting of details in data collection, and a lack of reported efforts to increase the trustworthiness of findings. The main shortcoming overall was the lack of detail on the method and activities used that would enable replication.
Two interventions were led by a drama therapist, one by a drama therapist with another professional, and one by other professionals (elder clowns). Of the studies involving drama therapists, one reported significant quantitative findings and two reported no statistically significant findings but positive qualitative outcomes. The study led by elder-clowns reported positive qualitative outcomes. No follow up data was provided for any of these studies.
Programs offered by drama therapists were typically group sessions of between 45 and 105 min for an average of 80 min, held once weekly, for 12 weeks. One study facilitated by elder clowns involved two clowns per individual resident for 10 min twice weekly. Interventions involved therapists' technique of empathic attunement, and activities involving mirroring, doubling, and role-reversal, dramatic embodiment of inner conflicts, dramatic projective in the form of roleplay and enactment. Session structure in group interventions typically involved a warm up, a main action and a closure phase. One on one sessions conducted by elder clowns involved techniques of affective attunement and humor, and activities involving reciprocal play.
Each study that included drama therapy involved therapeutic techniques derived from meta-processes (Cassidy et al., 2014) including the therapist being involved while working in the here and now alongside clients, the establishment of safety through the choice of techniques and clients being offered control and choice to enable them to exercise initiative and creativity. Other core processes, as identified by Jones (2007), included play, dramatic embodiment, dramatic projection, personification, and impersonation (role-play), empathy and distancing, life-drama connection, witnessing, and transformation. These were used to facilitate clients' short and long term goals. For example, in the study involving drama therapy and life review, stories of group members were embodied by other group members who took on the roles identified in the single group member's story and created dramatic images. This was intended to enable the story owner to “gain new perspectives about their life decisions and deepen their understanding of the associations between these decisions, in a way that gives rise to a more positive identity” (Keisari and Palgi, 2017, p.1080).
The core processes used to activate internal resources and externalize internal conflicts were discussed by Sajnani et al. (2018). Wilkinson et al. (1998), reported activities being chosen to stimulate reminiscence, socialization, and “provide opportunities for more organized self-expression through the use of metaphor” (p. 195). In the study in which elder clowns interacted with older adults, the primary processes described were (a) affective relationality; (b) reciprocal playfulness; and (c) co-constructed imagination.
The studies reviewed suggest that shifts in depressive symptoms that result from drama interventions are catalyzed by mechanisms of change such as:
• Physical: engagement in playful, embodied activity contributing to sense of vitality and regulated, relaxed breathing;
• Cognitive: orientation to past and present, reinforcement of positive coping strategies, coherent organization of self-expression, increased memory recall, facilitation of meaning making;
• Emotional/intrapersonal: use of metaphors, roles, and playful, embodied enactments providing a suitable distance to activate internal resources and externalize and communicate inner conflicts and strengths, and facilitate emotional regulation;
• Social: individual and group activities prompting increased positive social interaction.
Forty-one studies met all inclusion criteria from an initial sample of 91 as detailed in Table 4. Depression was addressed as a primary diagnosis in 21 studies and as secondary diagnosis and depressive symptoms in 20 studies.
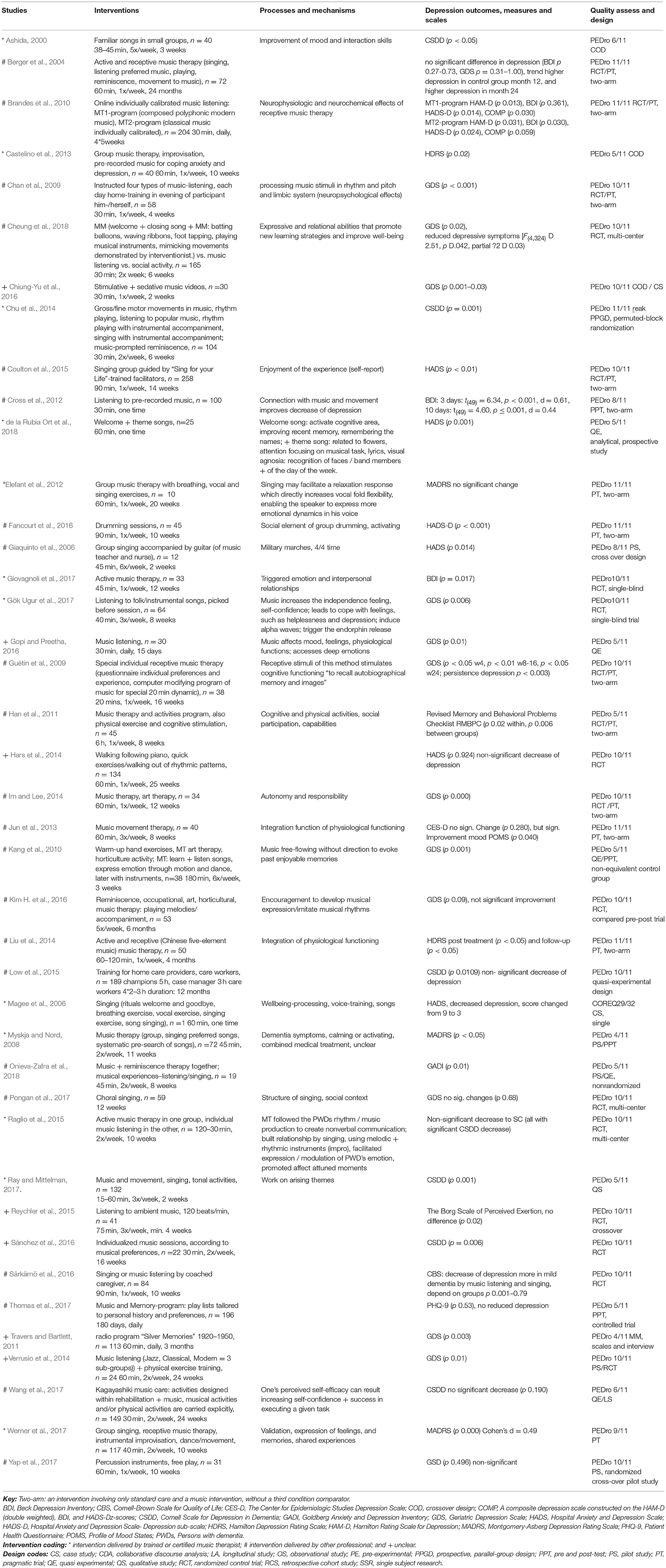
Table 4. Results of analysis of music intervention studies.
Sample sizes ranged between 1 and 12.576, with a mean sample of 379. Only six of the 41 studies included follow ups, undertaken after 3 or 6 months, all amongst most recent studies (Coulton et al., 2015; Kim H. et al., 2016; Sánchez et al., 2016; Särkämö et al., 2016; Pongan et al., 2017; Ray and Mittelman, 2017).
The quantitative studies scored between 4 and 11 on PEDro, and the one qualitative study met 29 of 32 elements in COREQ. Twelve interventions were led by a music therapist, 23 led by another professional; and six by a leader of unknown training. Twenty-six studies had significant findings: nine of these were led by a music therapist, twelve by another professional, and a further five had a leader of unknown training. Fifteen of the 26 music studies with significant findings were assessed as having high quality findings (8–11/11 on PEDro). The other six studies were assessed as being of low quality, with missing elements including blinding, similarity at baseline, concealed allocation, and clear randomization.
Programs offered were sessions of between 15 and 360 min, with 30–60 min being most common; held between once weekly and daily, most often weekly or twice per week; for periods from one day to 24 months, most often 10–12 weeks.
Very different methods and intervention types were included in treatment. Most frequently reported interventions in the 26 studies with successful outcomes were receptive music therapy and music listening (17). In nine studies, mixed intervention types (between two and five types) were included in treatment. Instrumental play and improvisation were also utilized in nine studies. In eight studies, individualized individual preferred music or reminiscence were also included with music listening or singing. In six studies, the intervention type was singing, and music movement was included in six studies as well. Activities were selected due to theoretical models or findings of therapeutic processes or mechanisms of change described in the following paragraphs.
Therapeutic processes described in the music studies were closely linked to mechanisms of change. These processes focussed on physical activation, processing of emotion and social relationships. Physical activation was seen to be activated through rhythmic patterns (including march rhythms in 4/4 time), physical reaction to emotions and improvement of movement. Processing of emotions supported changes from feelings of anger and fear to increased positive emotions and emotional responses including stimulation of happy memories, subjects' interests, preferred autobiographical music, and musical interests, and enjoyment through activation of the limbic and paralimbic systems. Processes relating to social relationships are described as interaction through playing of instruments, promotion of empathic relationships, increased communication, and reduced social isolation.
The studies reviewed suggest that shifts in depressive symptoms resulting from engagement in music and music therapy are a result of mechanisms of change across several domains:
• Physical: neurophysiological and neurochemical effects, such as endorphin release, stimulation of cognitive functioning i.e., reminiscence and activation of amygdala, hippocampus, and nucleus accumbens;
• Cultural (creative/aesthetic): processing of music stimuli in rhythm and pitch, musical experience including movement, physiological functioning, and imitating of musical rhythm;
• Intrapersonal: improvement of well-being, activation of remaining capabilities, self-efficacy, validation, increase of autonomy, and self-confidence developed through experiences of success;
• Social: improvement of interaction skills and relational abilities, to trigger interpersonal relationship, to stimulate social participation.
This review reveals significant differences between the creative arts modalities with respect to research quantity, type and quality. The number of studies about music interventions (n = 41) was significantly more than other modalities, i.e., art (n = 17), dance (n = 13), and drama (n = 4). Types of research were clearly distinct between modalities, with 40 of the 41 music studies, and all 13 dance studies being quantitative research, while art studies included predominantly quantitative, but also qualitative and mixed-methods studies, and the small number of drama studies involved qualitative, mixed-methods, and quantitative approaches. This indicates a need for more research in the creative arts therapy modalities that are as yet under-represented in the literature. While 13 dance studies were included in this review, none of those interventions was actually led by a dance movement therapist, so the need for more research in dance movement and drama therapy is particularly evident.
Quality issues differed between the modalities. Art therapy studies were found to be of medium quality with the main issues in quantitative studies being small sample size, a general lack of generalizability and a lack of rigorous efforts to ensure validity in the findings. Issues in qualitative studies in art therapy also relate to a lack of rigor to ensure creditable data analysis and inadequate reporting in data collection. This differs somewhat to the dance movement studies, which were largely RCTs and scored across the range from low to high on the PEDro scale roughly evenly. Quality issues for this modality relate to the lack of actual DMT interventions. Dance was the only modality for which this was an issue. Drama studies scored middle to high, with quality relatively high for quantitative studies (8 and 9/11 on PEDro), but lower for qualitative studies (19 and 21/32 on COREQ). Music studies scored high more consistently. Very few of the studies included follow up: art (0); dance 4/13; drama (0); and music 6/41.
The sections to follow discusses some of the most salient findings about each modality.
The choice of art media that is culturally relevant to the participant was repeatedly found to be a key factor of engagement. The fact that art interventions examined were at least 12 weeks long indicates that longer-term approaches might be most effective with this population. In consideration of the many mental and physical challenges faced by older adults, longer-term approaches might be more congruent with relationship building and sustaining the outcomes of art therapy. The effectiveness and impact of short-term programs remains to be studied. Future studies might also examine how personalized use of traditional art media might contribute to client outcomes. The quality of most art intervention studies was scored as medium to low (based on PEDRO and COREQ scores) with few studies effectively randomizing participants and/ or providing adequate details in the methodology.
The dance studies primarily focussed on the learning of dance steps and sequences, and repetition of these across sessions. Dance movement therapy, in contrast, often does not include the learning of structured steps, but rather prioritizes more improvised and expressive dance experiences. However, the effectiveness of learning of steps for amelioration of depression and its symptoms evidenced in these studies may point to it being a worthwhile consideration for DM therapists, especially for this older adult age group. One issue arising in the dance studies was the perception by participants and possibly program hosts that dance interventions are more suitable for women. As the rate of depression is the same for men and women, and its functional impacts are greater for men, this indicates a challenge, with an effective modality not potentially being considered by 50% of the people impacted by depression.
The quality of dance studies was varied, with ratings evenly distributed from the lowest to highest PEDro scores. Lower scoring studies were often missing elements of blinding of subjects, therapists, and assessors, and concealment of allocation.
While few in number, the three studies involving drama therapists indicated that positive outcomes could be achieved in programs of 12 weeks in length. The findings of these studies were consistent with recent literature in drama therapy emphasizing the benefits derived from opportunities for playful interaction and the externalization of significant experiences through drama; these processes were found to reinforce internal resources and contribute to a sense of generativity (see Jennings, 2018).
Twenty-six of the 41 music studies demonstrated significant findings in treatment of depression and depressive symptoms. The most effective interventions were provided by trained music therapists, with nine of the twelve studies involving these professionals having significant findings, whereas only twelve of the 23 studies involving other professionals had significant findings. Thus, interventions led by music therapists appeared more suitable than those led by other professionals for treatment for depression and for depressive symptoms of older adults. Effective interventions were diverse and included receptive music therapy and music listening, mixed intervention types, instrumental play and improvisation, and individualized, individual preferred music or reminiscence in music listening or singing.
We began this review with the intention of exploring the effects of creative arts interventions on older adults experiencing depression, as well as relationships documented between intervention activities, therapeutic processes, and mechanisms seen to lead to outcomes. However, this second task proved not to be straightforward, with studies often not providing adequate (or any) discussion about processes or mechanisms that were expected or elicited through interventions. In articles that did discuss processes or mechanisms, claims were largely not substantiated with data. Other studies appeared to have been predicated on theories of change about outcomes expected from activities and associated therapeutic processes but did not explicate these. This was particularly evident in the dance studies, where there was much focus on physical movement, without specific articulation of the well-evidenced relationship between physical exercise and reduced depression or depressive symptoms.
This finding gives rise to a consideration that we did not assess one important quality point, that of the quality of interventions. Given that the quality of an intervention is likely to significantly impact findings, this would seem an appropriate and relevant process. While we scored the methodological quality of studies using COREQ and PEDro tools, this process did not offer any insight about how well-considered interventions appeared, how well substantiated they were from theory or evidence, or whether justification for activities or processes to be employed was adequate. Thus, an additional quality process we recommend would be for the assessment of the quality of choices made and processes employed. The use of manualised interventions or descriptions of clear intervention protocols may contribute to better practice in this respect.
Another methodological challenge was the lack of discussion in the studies examined of the relationship between expected outcomes and specific symptoms of depression as identified in DSM-V or ICD manuals. We had initially tried to align outcomes of studies with these formally identified symptoms, but few studies specifically mentioned addressing these. We recommend that future studies pay specific attention to identified symptoms of depression.
One risk of bias in this study is the fact that all authors are creative arts therapists. We attempted to minimize bias caused by this factor by ensuring that at least two authors were involved in extracting data from each study and that they double checked each other's work. Other strategies we employed for reducing bias were the inclusion of all studies, those with significant and non-significant findings, and adherence to strict inclusion criteria.
An additional limitation for research that was considering creative arts broadly was that our study did not include studies on writing, or the broader categories of expressive and creative arts that were not modality specific. Future research may be best to include these topics.
Our first recommendation for future research is for studies that meet quality standards for both quantitative or qualitative approaches, given that so many of the studies we examined did not. Our findings indicated a significant need for well designed, detailed studies of the impact of all creative arts therapies in the targeted treatment of depression in older adults.
We recommend that future studies include more specific focus on how interventions work, as well as if they work, given the under-development of theories of change about how creative arts interventions are seen to be effective in addressing depression in studies reviewed, and the lack of clear explication and testing of processes and mechanisms considered to contribute to therapeutic outcomes. In addition, the differences between, and sequencing of, individual and group interventions remain understudied.
Creative arts therapies are increasingly being offered as part of a range of complementary therapies in integrative care settings. However, no studies examined their cost effectiveness, either comparing creative arts modalities with each other, or between CA modalities and other therapeutic approaches. This prompts a recommendation for future inquiry, which would increase understanding of how creative arts interventions, including CA therapies, might be utilized as psychosocial prescriptions to increase effectiveness and reduce costs of healthcare of older adults. Increased collaboration between creative art therapy researchers could also be useful for improving research outcomes. Future studies could also examine how new technology like virtual reality and telehealth might contribute to the potential of creative arts interventions for the health of older adults.
Given our findings that interventions led by certified creative arts therapists resulted in more significant or positive outcomes than interventions led by other professionals, we recommend that interventions for depression with older adults be provided by certified creative arts therapists. Because relatively few interventions included developed theories of change about interventions chosen, processes implemented and the expected relationship with these and changes in depressive symptoms, we consider that clinical practice may be similarly improved with better articulation of all of these considerations in the planning and delivery of interventions for depression.
This review examines evidence for the effects of creative art interventions on depression and depressive symptoms of older adults. The majority of 51 of the 75 studies examined demonstrated either significant quantitative or positive qualitative findings (12/17 of art, 10/13 of dance, 4/4 of drama and 26/41 of music, and music therapy). The quality assessment of these studies differed between disciplines, with medium quality in art studies, the full range from low to high in dance studies, middle to high in in drama therapy, and high in the majority of studies with significant findings in music. Certified art therapists were involved in the majority of studies with significant findings: in art, 8/12; in drama, 3/4; and in music, 9/12 studies involving music therapists and 12/23 studies involving other professionals. No studies involving DMT fitted this criterion.
Mechanisms of change gleaned from the studies include physical (improvements in balance, muscle strength; neurochemical effects, such as endorphin release), intra-personal (positive views of self; strengthened agency and mastery; communication and processing of emotions; coping strategies), cultural (creative expression, aesthetic pleasure), cognitive (stimulation of memory), and social (increased social skills and connection) elements that were all considered to be causal in reduced depression and symptoms. Recommendations for future research includes stronger focus on trialing of processes and mechanisms, considerations of the value of short vs. longer term therapy, and cost-effectiveness of creative arts therapy modalities in comparison with each other as well as with other type of therapeutic treatment.
FB, GK, NS, TW, and KD conceptualized the project and designed the study. KD co-ordinated the project, and led writing of introduction, method and discussion sections and integrative analysis. KC-H, ED, JE, ME, KM, and OS undertook the data gathering, first stage of analysis and data entry for sections on art therapy, dramatherapy, dance movement therapy, and music therapy respectively. GK, KM, NS, ED, KD, FB and TW undertook the second phase of analysis and write up of results for sections on art therapy, drama therapy, dance movement therapy and music therapy respectively. All authors contributed to manuscript revision and read and approved the submitted version. Authors are listed alphabetically except first three authors Dunphy, Baker, and Dumaresq.
Contributions were funded by University of Melbourne Mackenzie Post-Doctoral Research Fellowship (KD); University of Melbourne Academic Assistantship (ED); Drexel University College of Nursing and Health Professions Research Fellowship (KC-H); New York University Research Assistance grant (OS); DAAD through Federal Ministry of Education and Research, Germany (TW, JE).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors wish to acknowledge Patrick Condron and Georgina Binns from the University of Melbourne Library for invaluable consultation service.
AT, art therapy; DMT, dance movement therapy; DT, drama therapy; MT, music therapy; LLD, late life depression; MDD, major depressive disorder.
Adam, D., Ramli, A., and Shahar, S. (2016a). Effectiveness of a combined dance and relaxation intervention on reducing anxiety and depression and improving quality of life among the cognitively impaired elderly. Sultan Qab. Univ. Med. J. 16, 47–53. doi: 10.18295/squmj.2016.16.01.009
Adam, D., Shahar, S., and Ramli, A. (2016b). Status of functional balance and anxiety level among cognitive impaired elderly underwent dance and relaxation therapy. Inter. Med. J. 23, 686–690.
Ahessy, B. (2013). Creative Arts Therapies: what psychologists need to know. Irish Psychol. 1, 274–281.
Ali, K., Gammidge, T., and Waller, D. (2014). Fight like a ferret: a novel approach of using art therapy to reduce anxiety in stroke patients undergoing hospital rehabilitation. Med. Human. 40, 50–60. doi: 10.1136/medhum-2013-010448
Alpert, P. T., Miller, S. K., Wallmann, H., Havey, R., Cross, C., Chevalia, T., et al. (2009). The effect of modified jazz dance on balance, cognition, and mood in older adults. J. Am. Acad. Nurse Pract. 21, 108–115. doi: 10.1111/j.1745-7599.2008.00392.x
Arean, P. A., Perri, M. G., Nezu, A. M., Schein, R. L., Christopher, F., and Joseph, T. X. (1993). Comparative effectiveness of social problem-solving therapy and reminiscence therapy as treatments for depression in older adults. J. Consult. Clin. Psychol. 61, 1003–1010. doi: 10.1037/0022-006X.61.6.1003
Ashida, S. (2000). The effect of reminiscence music therapy sessions on changes in depressive symptoms in elderly persons with dementia. J. Music Ther. 37, 170–182. doi: 10.1093/jmt/37.3.170
Bennett, S., and Thomas, A. J. (2014). Depression and dementia: cause, consequence or coincidence. Maturitas 17, 184–190. doi: 10.1016/j.maturitas.2014.05.009
Berger, G., Bernhardt, T., Schramm, U., Müller, R., Landsiedel-Anders, S., Peters, J., et al. (2004). No effects of a combination of caregivers' support group and memory training/music therapy in dementia patients from a memory clinic population. Inter. J. Geriat. Psychiatry 19, 223–231. doi: 10.1002/gps.1055
Beyond Blue (2018). Medical Treatments for Depression. Available online at: https://www.beyondblue.org.au/the-facts/depression/treatments-for-depression/medical-treatments-for-depression
Blomdahl, C., Gunnarsson, B. A., Guregård, S., and Björklund, A. (2013). Exploring core processes facilitating therapeutic change in dramatherapy: A grounded theory analysis of published case studies. Arts Psychother. 40, 322–330. doi: 10.1016/j.aip.2013.05.009
Brandes, V., Terris, D., Fischer, C., Loerbroks, A., Jarczok, M., Ottowitz, G., et al. (2010). Receptive music therapy for the treatment of depression: a proof-of-concept study and prospective controlled clinical trial of efficacy. Psychother. Psychosom. 79, 321–322. doi: 10.1159/000319529
Britten, L., Addington, C., and Astill, S. (2017). Dancing in time: feasibility and acceptability of a contemporary dance programme to modify risk factors for falling in community dwelling older adults. BMC Geriatr. 17:83. doi: 10.1186/s12877-017-0476-6
Bruce, M. L., Seeman, T. E., Merrill, S. S., and Blazer, D. G. (1994). The impact of depressive symptomatology on physical disability: MacArthur studies of successful aging. Am. J. Public Health 84:1796. doi: 10.2105/AJPH.84.11.1796
Canuto, A., Meiler-Mitielu, C., Herrmann, F. R., Delaloye, C., Giannakopoulos, P., and Weber, K. (2008). Longitudinal assessment of psychotherapeutic day hospital treatment for elderly patients with depression. Intern. J. Geriatr. Psychiatry 23, 949–956. doi: 10.1002/gps.2016
Carr, A. (2008). What Works With Children, Adolescents, and Adults: A Review of Research on the Effectiveness of Psychotherapy. New York, NY: Routledge.
Cassidy, S., Turnbull, S., and Gumley, A. (2014). Exploring core processes facilitating therapeutic change in dramatherapy: a grounded theory analysis of published case studies. Arts Psychother. 41, 353–365. doi: 10.1016/j.aip.2014.07.003
Castelino, A., Fisher, M., Hoskyns, S., Zeng, I., and Waite, A. (2013). The effect of group music therapy on anxiety, depression and quality of life in older adults with psychiatric disorders. Aust. Psychiatry 21, 506–507. doi: 10.1177/1039856213492355
Centre for Reviews and Dissemination, University of York. (2018). Prospero: International Prospective Register of Systematic Reviews. Available online at: https://www.crd.york.ac.uk/prospero/ (Accessed 30 October, 2018).
Ceramidas, D. M. (2012). Faith-based cognitive behavioral therapy: easing depression in the elderly with cognitive decline. J. Christ. Nurs. 29, 42–48. doi: 10.1097/CNJ.0b013e318238f288
Chan, M., Chan, E., Mok, E., and Kwan Tse, F. (2009). Effect of music on depression levels and physiological responses in community-based older adults. Int. J. Mental Health Nurs. 18, 285–294. doi: 10.1111/j.1447-0349.2009.00614.x
Chang, Y. S., Chang, Y. S., Chu, H., Yang, C. Y., Tsai, J. C., Chung, M. H., et al. (2015). The efficacy of music therapy for people with dementia: a meta-analysis of randomised controlled trials. J. Clin. Nurs. 24, 3425–3440. doi: 10.1111/jocn.12976
Cheung, D. K., Lai, C. Y., Wong, F. Y., and Leung, M. P. (2018). The effects of the music-with-movement intervention on the cognitive functions of people with moderate dementia: a randomized controlled trial. Aging Mental Health 22, 306–315. doi: 10.1080/13607863.2016.1251571
Chiung-Yu, H., Yuan-Mei, H., and Hui-Ling, L. (2016). Effect of stimulative and sedative music videos on depressive symptoms and physiological relaxation in older adults. Res. Gerontol. Nurs. 9, 233–242. doi: 10.3928/19404921-20160906-02
Choi, Y. H., and Jeon, E. Y. (2013). The effects of group art therapy on cognition, depression and quality of life in elderly. J. Korean Acad. Comm. Health Nurs. 24, 323–331. doi: 10.12799/jkachn.2013.24.3.323
Chu, H., Yang, C., Lin, Y., Ou, K., Lee, T., O'Brien, A. P., et al. (2014). The impact of group music therapy on depression and cognition in elderly persons with dementia: a randomized controlled study. Biol. Res. Nurs. 16, 209–217. doi: 10.1177/1099800413485410
Ciasca, E. C., Ferreira, R. C., Santana, C. L. A., Forlenza, O. V., dos Santos, G. D., Brum, P. S., et al. (2018). Art therapy as an adjuvant treatment for depression in elderly women: A randomized controlled trial. Brazil. J. Psychiatry 40, 256–263. doi: 10.1590/1516-4446-2017-2250
Coulton, S., Clift, S., Skingley, A., and Rodriguez, J. (2015). Effectiveness and cost-effectiveness of community singing on mental health-related quality of life of older people: randomised controlled trial. Br. J. Psychiatry 207, 250–255. doi: 10.1192/bjp.bp.113.129908
Cross, K., Flores, R., Butterfield, J., Blackman, M., and Lee, S. (2012). The effect of passive listening versus active observation of music and dance performances on memory recognition and mild to moderate depression in cognitively impaired older adults. Psychol. Rep. 111, 413–423. doi: 10.2466/10.02.13.PR0.111.5.413-423
Czamanski-Cohen, J., and Weihs, K. L. (2016). The bodymind model: a platform for studying the mechanisms of change induced by art therapy. Arts Psychother. 51, 63–71. doi: 10.1016/j.aip.2016.08.006
Daykin, N., Mansfield, L., Meads, C., Julier, G., Tomlinson, A., Payne, A., et al. (2018). What works for wellbeing? A systematic review of wellbeing outcomes for music and singing in adults. Perspect. Public Health 138, 39–46. doi: 10.1177/1757913917740391
de Guzman, A. B., Satuito, J. C. B., Satumba, M. A. E., Segui, D. R. A., Serquina, F. E. C., Serrano, L. J. P., et al. (2011). Filipino arts among elders in institutionalized care settings. Educ. Gerontol. 37, 248–261. doi: 10.1080/03601270903534937
de la Rubia Ortí, J. E., García-Pardo, M. P., Iranzo, C. C., Madrigal, J. C., Castillo, S. S., Rochina, M. J., et al. (2018). Does music therapy improve anxiety and depression in Alzheimer's patients? J. Altern. Complem. Med. 24, 33–36. doi: 10.1089/acm.2016.0346
Department of Health (2018). Antidepressants. Melbourne, VIC: Victorian Government. Available online at: http://www.health.gov.au/internet/publications/publishing.nsf/Content/drugtreat-pubs-modpsy-toc~drugtreat-pubs-modpsy-3~drugtreat-pubs-modpsy-3-8~drugtreat-pubs-modpsy-3-8-ant
Devereaux, C. (2017). Neuroception and attunement in dance/movement therapy with autism. Am. J. Dance Ther. 39, 36–38. doi: 10.1007/s10465-017-9249-1
Doric-Henry, L. (1997). Pottery as art therapy with elderly nursing home residents. J. Am. Art Ther. Assoc. 14, 163–171. doi: 10.1080/07421656.1987.10759277
Drăghici, R. (2012). Experiential psychotherapy in geriatric groups. Procedia 33, 979–983. doi: 10.1016/j.sbspro.2012.01.268
Elefant, C., Baker, F. A., Lotan, M., Lagesen, S. K., and Skeie, G. O. (2012). The effect of group music therapy on mood, speech, and singing in individuals with Parkinson's disease–a feasibility study. J. Music Ther. 49, 278–302. doi: 10.1093/jmt/49.3.278
Eyigor, S., Karapolat, H., Durmaz, B., Ibisoglu, U., and Cakir, S. (2009). A randomized controlled trial of Turkish folklore dance on the physical performance, balance, depression and quality of life in older women. Arch. Gerontol. Geriatr. 48, 84–88 doi: 10.1016/j.archger.2007.10.008
Fancourt, D., Perkins, R., Ascenso, S., Carvalho, L. A., Steptoe, A., and Williamon, A. (2016). Effects of group drumming interventions on anxiety, depression, social resilience and inflammatory immune response among mental health service users. PLoS ONE 11:e151136. doi: 10.1371/journal.pone.0151136
Fiske, A., Wetherell, J., and Gatz, M. (2010). Depression in older adults. Annu Rev Clin Psycho 5, 363–389. doi: 10.1146/annurev.clinpsy.032408.153621
Forlani, C., Morri, M., Ferrari, B., Dalmonte, E., Menchetti, M., De Ronchi, D., et al. (2014). Prevalence and gender differences in late-life depression: a population-based study. Am. J. Geriatr. Psychiatry 22, 370–380. doi: 10.1016/j.jagp.2012.08.015
Garcia Gouvêa, J. A., Dias Antunes, M., Bortolozzi, F., Marques, A. G., and Marques Gomes Bertolini, S. M. (2017). Impact of senior dance on emotional and motor parameters and quality of life of the elderly. Revista Rede Enfermagem do Nordeste 18, 51–58. doi: 10.15253/2175-6783.2017000100008
Giaquinto, S., Cacciato, A., Minasi, S., Sostero, E., and Amanda, S. (2006). Effects of music-based therapy on distress following knee arthroplasty. Br. J. Nurs. 15, 576–579. doi: 10.12968/bjon.2006.15.10.21136
Giovagnoli, A., Manfredi, V., Parente, A., Schifano, L., Oliveri, S., Avanzini, G., et al. (2017). Cognitive training in Alzheimer's disease: a controlled randomized study. Neurol. Sci. 38, 1485–1493. doi: 10.1007/s10072-017-3003-9
Gök Ugur, H., Yaman Aktaş, Y., Orak, O. S., Saglambilen, O., and Aydin Avci, I. (2017). The effect of music therapy on depression and physiological parameters in elderly people living in a Turkish nursing home: a randomized-controlled trial. Aging Mental Health 21, 1280–1286. doi: 10.1080/13607863.2016.1222348
Goldblatt, R., Elkis-Abuhoff, D., Gaydos, M., and Napoli, A. (2010). Understanding clinical benefits of modeling clay exploration with patients diagnosed with Parkinson's disease. Arts Health 2, 140–148. doi: 10.1080/17533010903495405
Gopi, D., and Preetha, A. K. (2016). Effectiveness of music therapy on depressive symptoms among elderly in selected geriatric homes. Intern. J. Nursing Educ. 8, 163–166. doi: 10.5958/0974-9357.2016.00110.0
Guétin, S., Portet, F., Picot, M., Pommié, C., Messaoudi, M., Djabelkir, L., et al. (2009). Effect of music therapy on anxiety and depression in patients with Alzheimer's type dementia: randomised, controlled study. Demen. Geriatr. Cogn. Disord. 28, 36–46. doi: 10.1159/000229024
Haboush, A., Floyd, M., Caron, J., LaSota, M., and Alvarez, K. (2006). Ballroom dance lessons for geriatric depression: an exploratory study. Arts Psychother. 33, 89–97. doi: 10.1016/j.aip.2005.10.001
Han, P., Kwan, M., Chen, D., Yusoff, S., Chionh, H., Goh, J., et al. (2011). A controlled naturalistic study on a weekly music therapy and activity program on disruptive and depressive behaviors in dementia. Demen. Geriatr. Cogn. Disord. 30, 540–546. doi: 10.1159/000321668
Hars, M., Herrmann, F. R., Gold, G., Rizzoli, R., and Trombetti, A. (2014). Effect of music-based multitask training on cognition and mood in older adults. Age Ageing 43, 196–200. doi: 10.1093/ageing/aft163
Hoffmann, N. C. (2013). Using art therapy to address cognitive symptoms of Parkinson's disease. Int. J. User-Driven Healthcare 3, 74–95. doi: 10.4018/ijudh.2013070106
Holck, U., and Geretsegger, M. (2016). Musical and emotional attunement: unique and essential in music therapy with children on the autism spectrum. Nord. J. Music Ther. 25, 34–35. doi: 10.1080/08098131.2016.11783620
Hsieh, H. F., and Wang, J. J. (2003). Effect of reminiscence therapy on depression in older adults: a systematic review. Intern. J. Nurs. Stud. 4:335. doi: 10.1016/S0020-7489(02)00101-3
Hsu, T.-J., Tsai, H.-T., Hwang, A.-C., Chen, L.-Y., and Chen, L.-K. (2017). Predictors of non-pharmacological intervention effect on cognitive function and behavioral and psychological symptoms of older people with dementia. Geriatr. Gerontol. 17, 8–36. doi: 10.1111/ggi.13037
Im, M. L., and Lee, J. I. (2014). Effects of art and music therapy on depression and cognitive function of the elderly. Technol. Health Care 22, 453–458. doi: 10.3233/THC-140803
Imel, Z. E., and Wampold, B. E. (2008). “The importance of treatment and the science of common factors in psychotherapy,” in Handbook of Counseling Psychology 4th ed, eds, S. D. Brown and R. W. Lent. (Hoboken, NJ: John Wiley and Sons), 249–262.
Innes, K. E., Selfe, T. K., Khalsa, D. S., and Kandati, S. (2016). Effects of meditation versus music listening on perceived stress, mood, sleep, and quality of life in adults with early memory loss: a pilot randomized controlled trial. J. Alzheimer's Dis. 52, 1277–1298. doi: 10.3233/JAD-151106
Istvandity, L. (2017). Combining music and reminiscence therapy interventions for wellbeing in elderly populations: a systematic review. Complem. Ther. Clin. Pract. 28, 18–25. doi: 10.1016/j.ctcp.2017.03.003
Jennings, S. (2018). “Drama therapy in working with people with dementia: the need for playfulness in creative ageing as an antidote to depression and isolation,” in Arts Therapies in the Treatment of Depression, eds, A. Zubala and V. Karkou (London: Routledge), 204–216.
Johnson, J. K., Louhivuori, J., Stewart, A. L., Tolvanen, A., Ross, L., Era, P., et al. (2013). Quality of life (QOL) of older adult community choral singers in Finland. Int. Psychogeriatr. 25, 1055–1064. doi: 10.1017/S1041610213000422
Jun, E. M., Roh, Y. H., and Kim, M. J. (2013). The effect of music-movement therapy on physical and psychological states of stroke patients. J. Clin. Nurs. 22, 22–31. doi: 10.1111/j.1365-2702.2012.04243.x
Kang, H., Bae, Y., Kim, E., Lee, K., Chae, M., and Ju, R. (2010). An integrated dementia intervention for Korean older adults. J. Psychosoc. Nurs. Mental Health Serv. 48, 42–50. doi: 10.3928/02793695-20100930-01
Keisari, S., and Palgi, Y. (2017). Life-crossroads on stage: integrating life review and drama therapy for older adults. Aging Mental Health 21, 1079–1089. doi: 10.1080/13607863.2016.1199012
Kim, H., Yang, Y., Oh, J., Oh, S., Choi, H., Kim, K. H., et al. (2016). Effectiveness of a community-based multidomain cognitive intervention program in patients with Alzheimer's disease. Geriatr. Gerontol. Int. 16, 191–199. doi: 10.1111/ggi.12453
Kim, H.-K., Kim, K. M., and Nomura, S. (2016). The effect of group art therapy on older Korean adults with neurocognitive disorders. Arts Psychother. 47, 48–54. doi: 10.1016/j.aip.2015.11.002
Koch, S. (2017). Arts and health: active factors and a theory framework of embodied aesthetics. Arts Psychother. 54, 85–91. doi: 10.1016/j.aip.2017.02.002
Koch, S., Kunz, T., Lykou, S., and Cruz, R. (2014). Effects of dance movement therapy and dance on health-related psychological outcomes: a meta-analysis. Arts Psychother. 41, 46–64. doi: 10.1016/j.aip.2013.10.004
Kongkasuwan, R., Voraakhom, K., Pisolayabutra, P., Maneechai, P., Boonin, J., and Kuptniratsaikul, V. (2016). Creative art therapy to enhance rehabilitation for stroke patients: a randomized controlled trial. Clin. Rehab. 30, 1016–1023. doi: 10.1177/0269215515607072
Kontos, P., Miller, K., and Mitchell, G. J. (2017). Presence redefined: The reciprocal nature of engagement between elder-clowns and persons with dementia. Dementia 16, 46–66. doi: 10.1177/1471301215580895
Kossak, M. S. (2009). Therapeutic attunement: a transpersonal view of expressive arts therapy. Arts Psychother. 36, 13–18. doi: 10.1016/j.aip.2008.09.003
Kossak, M. S. (2015). Attunement in Expressive Arts Therapy: Toward an Understanding of Embodied Empathy. Springfield, IL: Charles C Thomas.
Lam, H. (2015). Effectiveness of Expressive Arts Therapy for Elderly With Depression and Anxiety. thesis, University of Hong Kong, Pokfulam.
Liu, X., Niu, X., Feng, Q., and Liu, Y. (2014). Clinical study: effects of five-element music therapy on elderly people with seasonal affective disorder in a Chinese nursing home. J. Trad. Chinese Med. 34, 159–161. doi: 10.1016/S0254-6272(14)60071-6
Low, L., Baker, J. R., Harrison, F., Jeon, Y., Haertsch, M., Camp, C., et al. (2015). The lifestyle engagement activity program (LEAP): implementing social and recreational activity into case-managed home care. J. Am. Med. Direct. Assoc. 16, 1069–1076. doi: 10.1016/j.jamda.2015.07.002
Magee, W., Brumfitt, S., Freeman, M., and Davidson, J. (2006). The role of music therapy in an interdisciplinary approach to address functional communication in complex neuro-communication disorders: a case report. Disab. Rehab. 28, 1221–1229. doi: 10.1080/09638280600630999
Matto, H. C., Tompkins, C. J., Ihara, E. S., Inoue, M., and Byrd, A. (2015). Results from a music, imagery, and movement treatment intervention in a long-term care facility. Fam. Soc. 96, 277–283. doi: 10.1606/1044-3894.2015.96.32
Meekums, B. (2002). Dance Movement Therapy: A Creative Psychotherapeutic Approach. Thousand Oaks, CA; London: Sage.
Meekums, B., Karkou, V., and Nelson, E. A. (2015). Dance movement therapy for depression. Cochr. Datab. Syst. Rev. 2:CD009895.
Mental Health America (2018). Depression in Older Adults. Available online at: http://www.mentalhealthamerica.net/depression-older-adults
Mental Health Foundation (2018). Physical Health and Mental Health. Available online at: https://www.mentalhealth.org.uk/a-to-z/p/physical-health-and-mental-health
Murray, C. J., and Lopez, A. D. (1996a). Evidence-based health policy–\lessons from the Global Burden of Disease Study. Science 274, 740–743. doi: 10.1126/science.274.5288.740
Murray, C. J. L., and Lopez, A. D. (Eds) (1996b). The Global Burden of Disease: A Comprehensive Assessment of Mortality and Disability from Diseases, Injuries, and Risk Factors in 1990 and Projected to 2020. Cambridge, MA: Harvard University Press.
Murrock, C. J., and Graor, C. H. (2014). Effects of dance on depression, physical function, and disability in underserved adults. J. Aging Phys. Activity 22, 380–385. doi: 10.1123/JAPA.2013-0003
Myskja, A., and Nord, P. (2008). 'The day the music died': a pilot study on music and depression in a nursing home. Nordic J. Music Ther. 17, 30–40. doi: 10.1080/08098130809478194
Naghavi, M., Wang, H., Lozano, R., Davis, A., Liang, X., Zhou, M., et al. (2015). Global, regional, and national age–sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 385, 117–171. doi: 10.1016/S0140-6736(14)61682-2
National Ageing Research Institute (2009). Depression in Older Age: A Scoping Study. Final Report. Melbourne, VIC: beyondblue.
Onieva-Zafra, M. D., Hernández-Garcia, L., Gonzalez-del-Valle, M. T., Parra-Fernández, M. L., and Fernandez-Martinez, E. (2018). Music intervention with reminiscence therapy and reality orientation for elderly people with Alzheimer's disease living in a nursing home: a pilot study. Holist Nurs Pract. 32, 43–50. doi: 10.1097/HNP.0000000000000247
Petrovsky, D., Cacchione, P. Z., and George, M. (2015). Review of the effect of music interventions on symptoms of anxiety and depression in older adults with mild dementia. Int. Psychogeriatr. 27, 1661–1670. doi: 10.1017/S1041610215000393
Pongan, E., Getenet, J. C., El Haouari, H., Navez, M., Laurent, B., Rouch, I., et al. (2017). Can musical or painting interventions improve chronic pain, mood, quality of Life, and cognition in patients with mild Alzheimer's disease? Evidence from a randomized controlled trial. J. Alzheimer's Dis. 60, 663–677. doi: 10.3233/JAD-170410
Quach, J. (2017). Do music therapies reduce depressive symptoms and improve QOL in older adults with chronic disease? Nursing 47, 58–63. doi: 10.1097/01.NURSE.0000513604.41152.0c
Qualls, S. H., and Knight, B. (2006). Psychotherapy for older adults with depression. Wiley Series in Clinical Geropsychology. Hoboken, NJ: John Wiley and Sons Inc.
Raglio, A., Bellandi, D., Baiardi, P., Gianotti, M., Ubezio, M. C., Zanacchi, E., et al. (2015). Effect of active music therapy and individualized listening to music on dementia: a multicenter randomized controlled trial. J. Am. Geriatr. Soc. 63, 1534–1539. doi: 10.1111/jgs.13558
Rawtaer, I., Mahendran, R., Yu, J., Fam, J., Feng, L., and Kua, E. H. (2015). Psychosocial interventions with art, music, tai chi and mindfulness for sub-syndromal depression and anxiety in older adults: a naturalistic study in Singapore. Asia-Pacific Psychiatry 7, 240–250. doi: 10.1111/appy.12201
Ray, K. D., and Mittelman, M. S. (2017). Music therapy: A nonpharmacological approach to the care of agitation and depressive symptoms for nursing home residents with dementia. Dementia 16, 689–710. doi: 10.1177/1471301215613779
Reychler, G., Mottart, F., Boland, M., Wasterlain, E., Pieters, T., Caty, G., et al. (2015). Influence of ambient music on perceived exertion during a pulmonary rehabilitation session: a randomized crossover study. Respiratory Care 60, 711–717. doi: 10.4187/respcare.03671
Rogers, C. (1951). Client-Centered Therapy: Its Current Practice, Implications, and Theory. Boston: Houghton Mifflin.
Sajnani, N., Cho, A., Landis, H., Raucher, G., and Trytan, N. (2018). “Collaborative discourse analysis on the use of drama therapy to treat depression in adults,” in Arts Therapies in the Treatment of Depression, eds, A. Zubala and V. Karkou (London: Routledge), 87–101.
Sánchez, A., Maseda, A., Marante-Moar, M. P., de Labra, C., Lorenzo-López, L., and Millán-Calenti, J. C. (2016). Comparing the effects of multisensory stimulation and individualized music sessions on elderly people with severe dementia: a randomized controlled trial. J. Alzheimer's Dis. 52, 303–315. doi: 10.3233/JAD-151150
Särkämö, T., Laitinen, S., Numminen, A., Kurki, M., Johnson, J. K., and Rantanen, P. (2016). Clinical and demographic factors associated with the cognitive and emotional efficacy of regular musical activities in dementia. J. Alzheimer's Dis. 49, 767–781. doi: 10.3233/JAD-150453
Seinfeld, S., Figueroa, H., Ortiz-Gil, J., and Sanchez-Vives, M. V. (2013). Effects of music learning and piano practice on cognitive function, mood and quality of life in older adults. Front. Psychol. 4:810. doi: 10.3389/fpsyg.2013.00810
Sherwood, P. (2008). Expressive artistic therapies as mind-body medicine. Body Mov. Dance Psychother. 3:81. doi: 10.1080/17432970802080040
Stevenson, M., Scope, A., Rawdin, A., and Sutton, A. (2015). The clinical and cost effectiveness of group art therapy for people with non-psychotic mental health disorders: a systematic review and cost-effectiveness analysis. BMC Psychiatry 15:151. doi: 10.1186/s12888-015-0528-4
Sun, J., Zhang, N., Buys, N., Zhou, Z.-Y., Shen, S.-Y., and Yuan, B.-J. (2013). The role of Tai Chi, cultural dancing, playing a musical instrument and singing in the prevention of chronic disease in Chinese older adults: a mind-body meditative approach. Int. J. Mental Health Prom. 15, 227–239. doi: 10.1080/14623730.2013.842337
Thomas, K. S., Baier, R., Kosar, C., Ogarek, J., Trepman, A., and Mor, V. (2017). Individualized music program is associated with improved outcomes for U.S. nursing home residents with dementia. Am. J. Geriatr. Psychiatry 25, 931–938. doi: 10.1016/j.jagp.2017.04.008
Thompson, L. W., Gallagher, D., and Breckenridge, J. S. (1987). Comparative effectiveness of psychotherapies for depressed elders. J. Consult. Clin. Psychol. 3:385. doi: 10.1037/0022-006X.55.3.385
Tong, A., Sainsbury, P., and Craig, J. (2007). Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int. J. Quality Health Care 19, 349–357. doi: 10.1093/intqhc/mzm042
Travers, C., and Bartlett, H. (2011). Silver memories: implementation and evaluation of a unique radio program for older people. Aging Mental Health 15, 169–177. doi: 10.1080/13607863.2010.508774
Travers, C., Brooks, D., Hines, S., O'Reilly, M., McMaster, M., Wei, H., et al. (2016). Effectiveness of meaningful occupation interventions for people living with dementia in residential aged care: a systematic review. Datab. Syst. Rev. Implem. Rep. 14, 163–225. doi: 10.11124/JBISRIR-2016-003230
United Nations Department of Economic and Social Affairs Population Division (2015). World Population Ageing. (ST/ESA/SER.A/390). Washington, DC: United Nations.
United Nations Department of Economic and Social Affairs Population Division (2017). World Population Prospects: The 2017 Revision, Key Findings and Advance Tables. Working Paper No. ESA/P/WP/248. Washington, DC: United Nations.
van der Steen, J. T., van Soest-Poortvliet, M. C., van der Wouden, J. C., Bruinsma, M. S., Scholten, R. M., and Vink, A. C. (2017). Music-based therapeutic interventions for people with dementia. Coch. Database Syst. Rev. 2:CD003477. doi: 10.1002/14651858.CD003477.pub3
Vankova, H., Holmerov, I., Machacova, K., Volicer, L., Veleta, P., and Celko, A. M. (2014). The effect of dance on depressive symptoms in nursing home residents. J. Am. Med. Direct. Assoc. 15, 582–587. doi: 10.1016/j.jamda.2014.04.013
Vasionyte, I., and Madison, G. (2013). Musical intervention for patients with dementia: a meta-analysis. J. Clin. Nurs. 22, 1203–1216. doi: 10.1111/jocn.12166
Verhagen, A. P., de Vet, H. C., de Bie, R. A., Kessles, A. G. H., Boers, L. M., Bouter, L. M., et al. (1998). The Delphi list: a criteria list for quality assessment of randomised clinical trials for conducting systematic reviews developed by Delphi consensus. J. Clin. Epidemiol. 51, 1235–1241. doi: 10.1016/S0895-4356(98)00131-0
Vermes, K. (2011). Intersensory and intersubjective attunement: philosophical approach to a central element of dance movement psychotherapy. Body Mov. Dance Psychother. 6, 31–42. doi: 10.1080/17432979.2010.533823
Verrusio, W., Andreozzi, P., Marigliano, B., Renzi, A., Gianturco, V., Pecci, M. T., et al. (2014). Exercise training and music therapy in elderly with depressive syndrome: a pilot study. Compl. Ther. Med. 22, 614–620. doi: 10.1016/j.ctim.2014.05.012
Wampold, B. E. (2001). Contextualizing psychotherapy as a healing practice: Culture, history, and methods. Appl. Prev. Psychol. 10, 69–86.
Wang, S., Yu, C., and Chang, S. (2017). Effect of music care on depression and behavioral problems in elderly people with dementia in Taiwan: a quasi-experimental, longitudinal study. Aging Mental Health 21, 156–162. doi: 10.1080/13607863.2015.1093602
Werner, J., Wosch, T., and Gold, C. (2017). Effectiveness of group music therapy versus recreational group singing for depressive symptoms of elderly nursing home residents: pragmatic trial. Aging Mental Health 21, 147–155. doi: 10.1080/13607863.2015.1093599
Wilkinson, N., Srikumar, S., Shaw, K., and Orrell, M. (1998). Drama and movement therapy in dementia: A pilot study. Arts Psychotherapy 25, 195–201. doi: 10.1016/S0197-4556(97)00102-0
World Health Organization (2017a). Depression: Fact Sheet. Geneva: World Health Organization. Available online at: http://www.who.int/mediacentre/factsheets/fs369/en/ (Accessed May 24, 2018).
World Health Organization (2017b). Mental Health of Older Adults: Fact Sheet. Available online at: http://www.who.int/mediacentre/factsheets/fs381/en/ (Accessed May 10, 2018).
Xu, B., Sui, Y., Zhu, C., Yang, X., Zhou, J., Li, L., et al. (2017). Music intervention on cognitive dysfunction in healthy older adults: a systematic review and meta-analysis. Neurol. Sci. 38, 983–992. doi: 10.1007/s10072-017-2878-9
Yap, A. F., Yu Heng, K., Chuen Seng, T., Ibrahim, S., and Seng Bin, A. (2017). Rhythm-centred music making in community living elderly: a randomized pilot study. BMC Compl. Altern. Med. 17:311. doi: 10.1186/s12906-017-1825-x
Zhao, K., Bai, Z., Bo, A., and Chi, I. (2016). A systematic review and meta-analysis of music therapy for the older adults with depression. Int. J. Geriatr. Psychiatry 31, 1188–1198. doi: 10.1002/gps.4494
Keywords: creative arts therapy, dance movement therapy, drama therapy, arts therapy, depression, older adults, processes, outcomes
Citation: Dunphy K, Baker FA, Dumaresq E, Carroll-Haskins K, Eickholt J, Ercole M, Kaimal G, Meyer K, Sajnani N, Shamir OY and Wosch T (2019) Creative Arts Interventions to Address Depression in Older Adults: A Systematic Review of Outcomes, Processes, and Mechanisms. Front. Psychol. 9:2655. doi: 10.3389/fpsyg.2018.02655
Received: 20 June 2018; Accepted: 10 December 2018;
Published: 08 January 2019.
Edited by:
Changiz Mohiyeddini, Northeastern University, United StatesReviewed by:
Rachel Lev-Wiesel, University of Haifa, IsraelCopyright © 2019 Dunphy, Baker, Dumaresq, Carroll-Haskins, Eickholt, Ercole, Kaimal, Meyer, Sajnani, Shamir and Wosch. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kim Dunphy, ay5kdW5waHlAdW5pbWVsYi5lZHUuYXU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.