
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
GENERAL COMMENTARY article
Front. Psychol. , 03 April 2017
Sec. Psychology for Clinical Settings
Volume 8 - 2017 | https://doi.org/10.3389/fpsyg.2017.00506
 Brian A. Sharpless1*
Brian A. Sharpless1* Karl Doghramji2
Karl Doghramji2by Jalal, B. (2016). Front. Psychol. 7:28. doi: 10.3389/fpsyg.2016.00028
We read with interest Dr. Jalal's recent publication on another potential treatment option for recurrent isolated sleep paralysis: Meditation Combined with Muscle Relaxation (MR Therapy). The author is to be commended for adding to the limited literature on ameliorating problematic cases of isolated sleep paralysis (ISP). As recently reviewed (Sharpless, 2016), there are few options available, pharmacological or otherwise, for the chronic and severe cases of ISP, and none of these yet possess compelling evidence in favor of their efficacy.
We appreciate the citation of our work in his article. However, we disagree with the author's claim that MR Therapy is the “first direct treatment” for ISP (Jalal, 2016, p. 1). This comment is puzzling given that our 2015 book (i.e., Sharpless and Doghramji, 2015) was cited in this same manuscript. Contained within is a manual titled Cognitive Behavioral-Therapy for Isolated Sleep Paralysis (CBT-ISP) and a corresponding adherence measure (pp. 237–272).
CBT-ISP is a brief, systematic approach that focuses upon helping patients both prevent and disrupt recurrent ISP episodes. In order to better clarify the nature of our own approach and to compare and contrast it to MR Therapy, we detail CBT-ISP in Table 1 below.
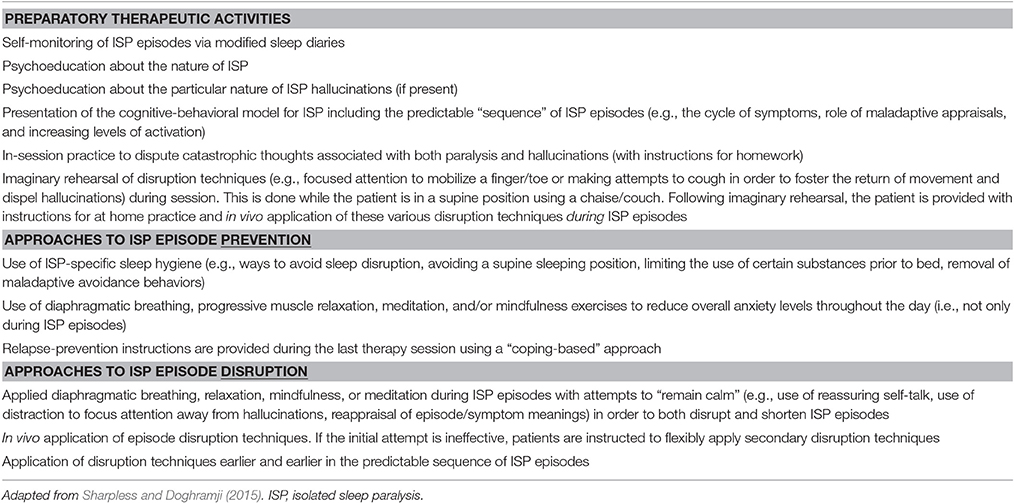
Table 1. Cognitive behavior therapy for isolated sleep paralysis (CBT-ISP).
As can be seen, there are areas of substantial overlap between CBI-ISP and MR Therapy. Both have strong emphases on various forms of relaxation, symptom reappraisals, shifts in attention away from episode content, and the practice of disruption techniques while patients are in a supine position. We should also note that both approaches are based upon panic disorder models.
However, there are some notable points of divergence. First, MR Therapy discourages attempts to move, whereas CBT-ISP actively encourages these attempts in order to directly disrupt episodes and shift attention away from potentially frightening symptoms (e.g., hallucinations). Our approach is based upon empirical work with sufferers who reported that these attempts were effective (Sharpless and Grom, 2016). Second, the author discourages attempts to control breathing whereas we view this as a potential source of relaxation to be used “in the moment.” Third, he encourages the use of prayer as a form of relaxation/meditation whereas we are more cautious about this, especially with patients who experience religious-themed hallucinations (e.g., demons, djinn). In general, CBT-ISP more strongly emphasizes psychoeducation, episode prevention, and consistent self-monitoring of ISP episodes (using modified sleep diaries) than MR Therapy, but both agree that directly disrupting ISP is important.
It is obviously preferable to have multiple treatment approaches available in a clinician's armamentarium as opposed to one. Efficacy rates for ISP approaches are not yet known, and it is very likely that both of these approaches will need to be modified in response to emerging data.
In closing, we believe that CBT-ISP (Sharpless and Doghramji, 2015) is the first direct treatment for ISP. However, it may be important to note that academic debates about temporal priority and differences in treatment foci are really moot points unless the phenomenon of recurrent ISP is more frequently assessed in research and clinical practice. This does not yet appear to be the case. At least two studies to date have shown that a minority of patients experience ISP to such a degree that it is associated with significant clinical consequences (Sharpless et al., 2010; Sharpless and Grom, 2016). Unfortunately, at the time of this writing there are not yet any empirically-supported treatment options available for sufferers.
All authors listed have made substantial, direct, and intellectual contribution to the work, and approved it for publication.
Both authors have received royalties from Oxford University Press for the publication of their book Sleep Paralysis: Historical, Psychological, and Medical Perspectives.
Jalal, B. (2016). How to Make the Ghosts in My Bedroom Disappear? Focused-Attention Meditation Combined with Muscle Relaxation (MR Therapy)—A Direct Treatment Intervention for Sleep Paralysis. Front. Psychol. 7:28. doi: 10.3389/fpsyg.2016.00028
Sharpless, B. A. (2016). A clinician's guide to recurrent isolated sleep paralysis. Neuropsychiatr. Dis. Treat. 12, 1761–1767. doi: 10.2147/NDT.S100307
Sharpless, B. A., and Doghramji, K. (2015). Sleep Paralysis: Historical, Psychological, and Medical Perspectives. New York, NY: Oxford University Press. doi: 10.1093/med/9780199313808.001.0001
Sharpless, B. A., and Grom, J. L. (2016). Isolated sleep paralysis: fear, prevention, and disruption. Behav. Sleep Med. 14, 134–139. doi: 10.1080/15402002.2014.963583
Keywords: sleep paralysis, isolated sleep paralysis, cognitive behavior therapy, parasomnia, sleep-wake disorders
Citation: Sharpless BA and Doghramji K (2017) Commentary: How to Make the Ghosts in my Bedroom Disappear? Focused-Attention Meditation Combined with Muscle Relaxation (MR Therapy)—A Direct Treatment Intervention for Sleep Paralysis. Front. Psychol. 8:506. doi: 10.3389/fpsyg.2017.00506
Received: 09 October 2016; Accepted: 17 March 2017;
Published: 03 April 2017.
Edited by:
Gianluca Castelnuovo, Università Cattolica del Sacro Cuore, ItalyReviewed by:
Christopher Charles French, Goldsmiths, University of London, UKCopyright © 2017 Sharpless and Doghramji. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Brian A. Sharpless, YmFzaGFycGxlc3NAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.