 Rosa Ayesa-Arriola1,2*Esther Setién-Suero1Karl D. Neergaard3Adele Ferro4,5Mar Fatjó-Vilas2,6Marcos Ríos-Lago7,8Soraya Otero1,9Jose M. Rodríguez-Sánchez2,10Benedicto Crespo-Facorro1,2
Rosa Ayesa-Arriola1,2*Esther Setién-Suero1Karl D. Neergaard3Adele Ferro4,5Mar Fatjó-Vilas2,6Marcos Ríos-Lago7,8Soraya Otero1,9Jose M. Rodríguez-Sánchez2,10Benedicto Crespo-Facorro1,2- 1Department of Psychiatry, Marqués de Valdecilla University Hospital, IDIVAL, School of Medicine, University of Cantabria, Santander, Spain
- 2Centro Investigación Biomédica en Red de Salud Mental (CIBERSAM), Madrid, Spain
- 3Department of Chinese and Bilingual Studies, The Hong Kong Polytechnic University, Hong Kong, China
- 4Department of Experimental Clinical Medicine, University of Udine, Udine, Italy
- 5Department of Mental Health and Neuroscience, Fondazione IRCCCS, Granda Ospedale Maggiore Policlinico, Milan, Italy
- 6Departament of Animal Biology, Faculty of Biology, Institute of Biomedicine of the University of Barcelona, Universitat de Barcelona, Barcelona, Spain
- 7Department de Psicologia Basica II, Faculty of Psychology, Universidad de Educación a Distancia, Madrid, Spain
- 8Unidad de Daño Cerebral, Red Menni de Atención al Daño Cerebral, Hospital Beata María Ana, Madrid, Spain
- 9Child and Adolescent Psychiatry Unit, Marqués de Valdecilla University Hospital, Santander, Spain
- 10Centro Investigación en Red de Salud Mental de Bizkaia-Osakidetza, Biscay, Spain
This study aimed to confirm whether first-episode psychosis patients present a stable trait impairment in theory of mind (ToM) and to examine the potential relationship between ToM and clinical symptomatology and neurocognition. Patients with a first episode of psychosis (N = 160) and healthy controls (N = 159) were assessed with an extensive neuropsychological test battery, which included a mental state decoding task known as “The Reading the Mind in the Eyes” (Eyes test), at baseline and reassessed after 1 and 3 years. The clinical group performed below healthy controls on the Eyes test while not showing test-retest differences between baseline and follow-up administrations. Analyses revealed age, education and premorbid IQ as potential moderators. Poorer performance on the Eyes test was not linked to clinical symptomatology but was associated with greater neurocognitive deficit, particularly related to processing speed. The persistence of ToM deficits in patients suggests that there are trait related metalizing impairments in first episode psychosis. This study shows the influence of processing speed and moderator variables on efficient ToM.
Introduction
There has been a growing interest over the last three decades in theory of mind (ToM), defined as the ability to attribute mental states to oneself and others (Baron-Cohen, 1991). ToM impairment has been confirmed in schizophrenia (Sprong et al., 2007; Bora et al., 2009), with important implications for social functioning (Bora et al., 2006). However, whether ToM deficits are state dependent or trait characteristics, and the nature of the relationship with neurocognitive deficits and clinical symptoms remains controversial.
A review of the literature supports the hypothesis that deficits in ToM are specific rather than secondary to symptoms or general cognitive decline. Bora et al. remark in their meta-analysis (Bora et al., 2009), that the persistence of ToM deficits, even in “remitted” patients, suggests trait related metalizing impairments in schizophrenia. However, a more severe ToM impairment related to positive and negative symptoms (Bora et al., 2008), and well as disorganization and other behavioral symptoms (Brüne, 2005b), point toward specific ToM deficits in schizophrenia as state dependent (Pousa et al., 2008). In terms of neurocognitive functioning, studies are contradictory when establishing ToM deficits as an independent trait (Bozikas et al., 2011) or secondary to general neurocognitive dysfunction (Pentaraki et al., 2012), and particularly related to working memory, attention and executive functions (Bozikas et al., 2011).
Regretfully, as So et al. (2010) pointed out, most of the available studies are limited in their generalizability in that they have small samples sizes without appropriate healthy control groups, and few are longitudinal or differ in the measurement of ToM performance. Meanwhile, few studies have examined ToM in first episode psychosis (FEP) patients (Inoue et al., 2006; Thompson et al., 2012; Bora and Pantelis, 2013; Fernandez-Gonzalo et al., 2014). To the best of our knowledge, two studies with FEP presented longitudinal, 1-year follow-up, designs: Addington et al. (2006) with 50 FEP and 55 non-psychiatric controls; and Horan et al. (2012) with 55 FEP patients, but without long-term information for a control group. While studies that investigate ToM impairment in early phases are important to understanding the nature of ToM dysfunction in schizophrenia, longitudinal studies are necessary to investigate the trajectory of ToM deficits and to shed light on the controversy of whether such deficits are state-like or trait-like.
Aims of the Study
The aims of our study were to explore whether there is a difference in ToM performance in FEP patients relative to healthy individuals and to determine the stability on performance at 1 and 3-year follow-ups. We hypothesized that FEP patients would have persistently lower performance compared to that of healthy volunteers. We also aimed to explore the ties between ToM and other neuropsychological and clinical variables. We hypothesized that ToM deficits would be related to neurocognitive decline and residual symptomatology.
Methods
Participants
The study sample comes from a large epidemiological program on first-episode psychosis (PAFIP) at University Hospital Marques de Valdecilla (Santander, Spain). Ethical approval was obtained from the local Ethics Committee. A more detailed description of PAFIP has been previously given (Pelayo-Terán et al., 2008).
The patient group consisted of 160-medication naïve subjects (Age: 16–60, M: 32.11) included in the first-episode psychosis program of Cantabria, Spain, (PAFIP) recruited from January 2005 to December 2010. Written informed consent was obtained from all participants after complete description of the study. The patients met the following criteria: (1) 15–60 years of age; (2) living in the catchment area; (3) were experiencing their first episode of psychosis; (4) had no prior treatment with antipsychotic medication or, if previously treated, a total life-time of adequate antipsychotic treatment of less than 6 weeks; and (5) met the DSM-IV criteria for brief psychotic disorder, schizophreniform disorder, schizophrenia or not otherwise specified (NOS) psychosis. The diagnoses were confirmed through the use of the Structured Clinical Interview for DSM-IV (SCID–I) (First et al., 1996) conducted by an experienced psychiatrist 6 months on from the baseline visit. Diagnoses of FEP patients were classified as: schizophrenia (N = 87), schizophreniform disorder (N = 40), brief psychotic disorder (N = 22) and psychosis NOS (N = 11). These patients were randomly assigned to: aripiprazol (N = 64), quetiapine (N = 46) or ziprasidone (N = 50).
A group of 159 healthy volunteers (Age: 15–51, M: 29.01) were initially recruited from the community through advertisements. They had no current or past history of psychiatric, neurological or general medical illnesses, including substance abuse and significant loss of consciousness as determined by using an abbreviated version of the Comprehensive Assessment of Symptoms and History (CASH) (Andreasen et al., 1992).
Sociodemographic and Clinical Variables
The patients were screened for demographic and clinical characteristics: age, education and symptoms of psychosis, assessed by mean scores on the Scale for the Assessment of Negative Symptoms (SANS) (Andreasen, 1983) and the Scale for the Assessment of Positive Symptoms (SAPS) (Andreasen, 1984). The SANS and SAPS scores were used in generating dimensions of positive (scores for hallucinations and delusions), disorganized (scores for formal thought disorder, bizarre behavior, and inappropriate affect) and negative (scores for alogia, affective fattening, apathy, and anhedonia) symptoms (Grube et al., 1998). Depressive symptoms were evaluated using the Calgary Depression Scale for Schizophrenia (CDSS) (Addington et al., 1992).
Neuropsychological Assessment
The neuropsychological evaluation was performed at any time between week-6 and week-13, as this time is considered optimal for patients' stabilization (González-Blanch et al., 2007). Trained neuropsychologists administered the tests.
The tests were grouped in the following cognitive domains consistently shown to be impaired in schizophrenia (Nuechterlein et al., 2004): 1- Verbal memory: the Rey Auditory Verbal Learning Test (RAVLT) (Rey, 1964) (list recall score); 2- Visual memory: Rey Complex Figure (RCF) (Osterrieth, 1944) (delayed recall); 3- Working memory: WAIS-III digits forward and backward subtests (Wechler, 1997) (standard total score); 4- Executive function: Trail Making Test (TMT) (Reitan and Wolfson, 1985; Periáñez et al., 2007) (trail B-A score); 5-Processing speed: WAIS-III digit symbol subtest (Wechler, 1997) (standard total score); 6- Motor dexterity: Grooved Pegboard Test (Lezak, 1995) (time to complete with dominant hand); 7- Attention: Continuous Performance Test (CPT) (Cegalis and Bowlin, 1991) (correct responses); 8- Premorbid IQ: WAIS-III vocabulary subtest (Wechler, 1997).
Theory of Mind Task
The Reading the Mind in the Eyes (Eyes test) (Baron-Cohen et al., 2001) was applied to assess ToM abilities. The test requires participants to identify the mental state just from the eye region. Studies that have used the Eyes test have provided evidence of a different aspect of ToM ability: mental state decoding skill (Bora et al., 2006).
Statistical Analysis
The Statistical Package for Social Science, version 19.0 (SPSS Inc., Chicago, IL), was used for statistical analyses.
Parametric χ2 and t-tests were first used to compare patients and healthy volunteers on demographic characteristics and ToM measure. Due to the longitudinal nature of the present study, repeated measure analysis of variance (ANOVA-r), adjusted for the covariates sex, age, education, and premorbid IQ, were then used to compare main effects of group, as well as group-by-time interactions on ToM. The relationship between ToM, and clinical and neuropsychological variables were then tested with Pearson correlations. Post-hoc comparisons were Bonferroni corrected. Finally, t-test and logistic regression analyses were conducted to overcome correlational limitations. The performance of the regression model was examined via Nagelkerke's R2, a measure of the proportion of explained variation in the logistic regression models, and in addition, logistic regression yields odds ratios (ORs), which measures the strengths of associations.
All statistical tests were two-tailed, and significance was determined at the 0.05 level.
Results
Sociodemographic and ToM Group Comparisons
A comparison of the 160 FEP patients and the 159 healthy controls regarding sociodemographic and ToM characteristics is presented in Table 1. Patients showed significantly reduced skills in ToM as can be seen in Figure 1.
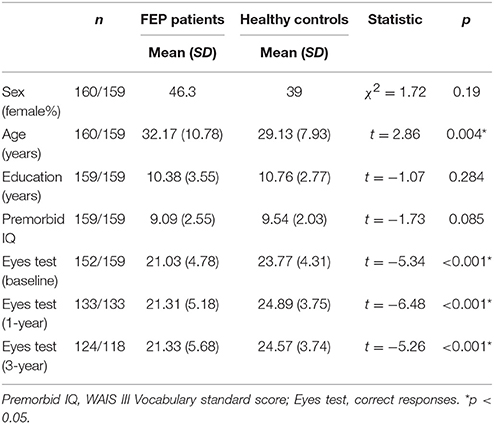
Table 1. Comparison of sociodemographic characteristics and ToM measure for FEP patients and healthy controls.
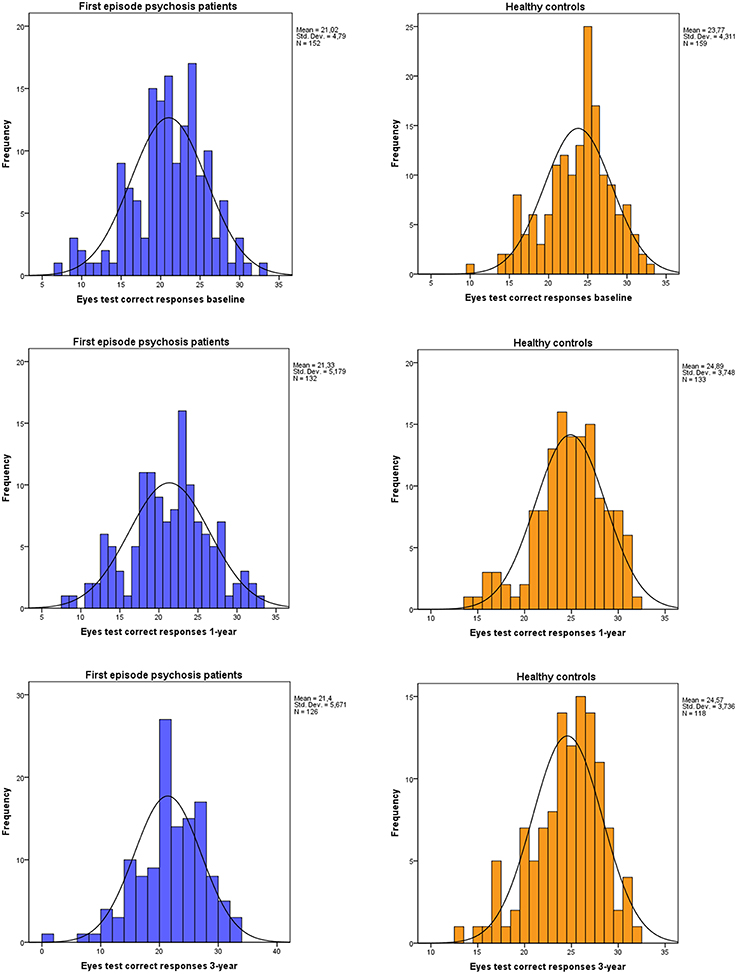
Figure 1. Distributions of correct responses to the Eyes test at baseline, 1- and 3-year follow-up for both first episode psychosis patients, and healthy controls.
Between-group effect on Eyes test for 107 patients and 111 healthy controls at baseline, 1-year and 3-years follow-up assessments revealed a significant main effect of group (F = 31; df = 1; p < 0.001), showing the patients significant impairment. There were no significant effects in within-group and time-by-group interaction in the Eyes test performance. Age (F = 4.04; df = 1; p < 0.046), education (F = 4.16; df = 1; p < 0.042) and particularly premorbid IQ (F = 28.2; df = 1; p < 0.001) were significant covariates (see Figure 2).
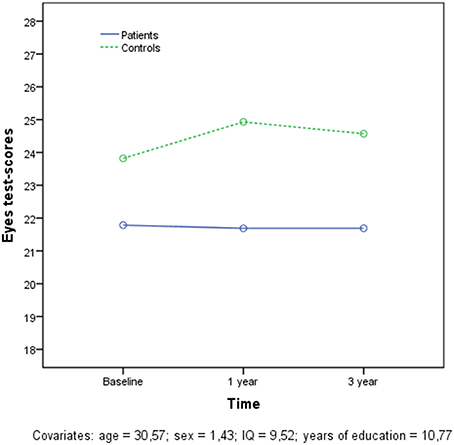
Figure 2. Longitudinal results in the Eyes test for both patients and controls.
Relationships of ToM with Clinical and Neurocognitive Variables
We conducted correlations analyses among clinical and neurocognitive variables presented in Table 2. Due to the large number of variables analyzed, Bonferroni correction was applied to the level 0.003 (0.05/15). After Bonferroni correction, the Eyes test did not correlate with any baseline or follow-up clinical variables: however, it moderately correlated with all baseline and 1 and 3-year follow-up neuropsychological measures (all p < 0.003, except verbal memory).
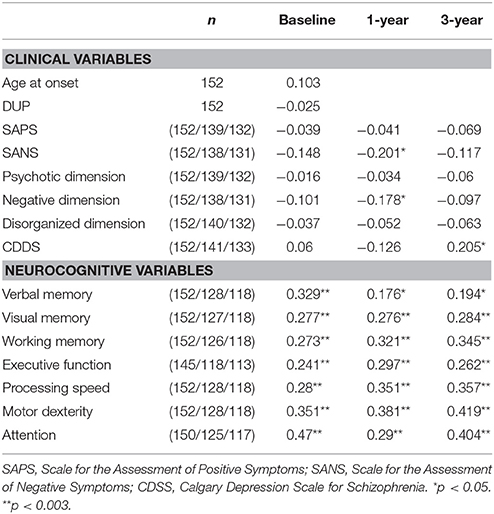
Table 2. Correlations of Eyes test with baseline, 1-year and 3-year clinical and neurocognitive variables.
In order to further explore the relationship between ToM and neurocognive function we subgrouped patients according the Eyes test's mean score in healthy subjects (Eyes test ≤ 24 = deficit ToM; Eyes test > 24 = normal ToM). Based on those criteria, 119 (78%) patients presented low performance vs. 33 (22%) which were classified as normal at Eyes test baseline assessment. Using the same methodology, at 1 and 3-year follow-up, 34 (26%) and 40 (33%) exhibited efficient ToM vs. 98 (74%) and 83 (67%) showing Eyes test underperformance, respectively. The deficit and non-deficit ToM subgroups showed significant differences in all seven cognitive domain scores at baseline (all p < 0.017), all but visual memory and executive functions at 1-year follow-up, and all but working memory and executive functions at 3-year follow-up. Z-scores comparisons of neuropsychological performance in the three assessment moments are presented in Table 3 and the neuropsyhological profiles in each ToM subgroup and assessment time can be consulted in Figure 3.
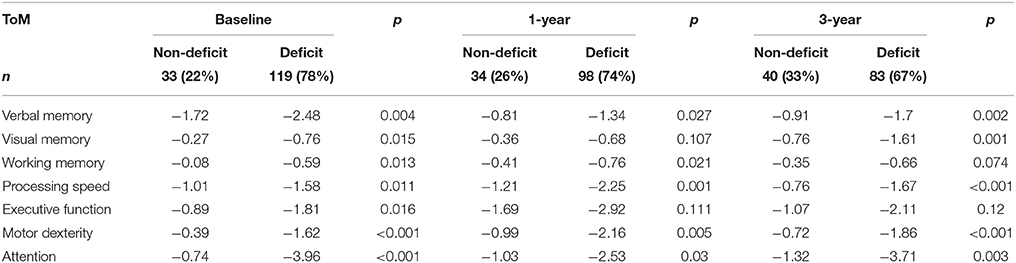
Table 3. Paired t-test comparisons of Z-scores neuropsychological performance in ToM subgroups at baseline, 1 and 3-year follow up.
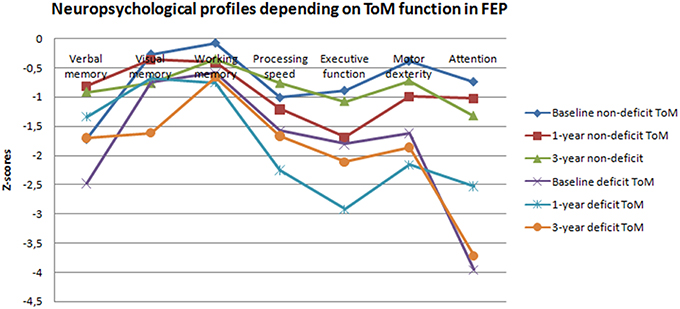
Figure 3. Neuropsychological profiles according on ToM function in first episode psychosis patients.
Regression Model of the Relationship between Neurocognitive Performance and ToM
Logistic regression analyses were conducted to determine the independent effect of the seven cognitive domains on ToM. Table 4 lists the results obtained. Processing speed (OR = 1.635; 95%CI 1.049–2.55; p = 0.03) was the unique significant contributor to efficient ToM, showing a trend toward significance in visual memory (OR = 1.431; 95%CI 0.949–2.158; p = 0.087). These regressions showed a well fitted model [χ2(7) = 24.047, p = 0.001, R2 Nagelkerke = 0.255] that predicted ToM performance with 73.9% accuracy and classified correctly 87.8% of patients with efficient ToM and 45.9% of patients with ToM impairment.
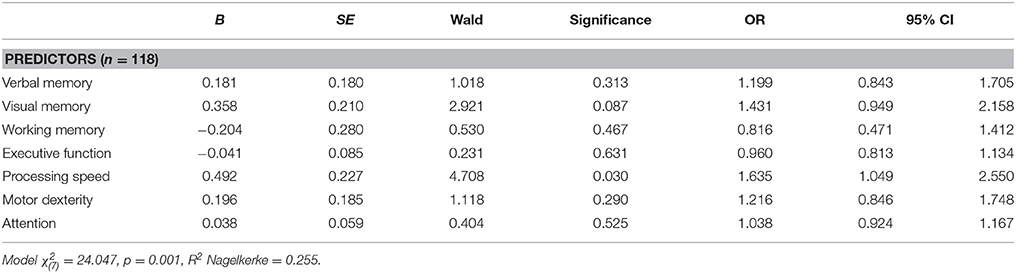
Table 4. Neurocognitive predictors of ToM in FEP at 3-year follow-up.
Discussion
This study investigated ToM deficits in FEP patients while overcoming previous studies' limitations. We confirmed that impairment in ToM is a stable trait feature in the largest sample of FEP patients analyzed to date with a longitudinal 3-year follow-up design.
Research in this field suggests that many FEP patients experience a range of difficulties in recognizing the emotions and intentions of others, as well as reflecting upon and questioning their own thinking. However, it was unclear the extent to which these deficits are stable over time, and their associations with core aspects of the disorder, such as symptoms and neurocognition. Our results showed that ToM deficit in FEP are present at illness onset, remains long-term stable, and are not related with clinical symptoms but neuropsychological deficits. Results support the notion that ToM dysfunction may be characteristic of psychosis, which does not change with treatment, consistent with the assertion that deficits in ToM are a trait of schizophrenia (Lysaker et al., 2011). The persistence of ToM deficits, even in remitted patients, suggests that they are trait related metalizing impairments (Bora et al., 2008). Previous studies found metacognitive deficits even in patients who were totally free of residual symptoms (Hamm et al., 2012), whereas some studies suggest ToM abilities seem to be related to both, positive and negative symptoms (Kohler et al., 2010). We did not find association between ToM and with clinical symptoms, neither in the acute nor in the stable phase.
Concerning neurocognitive results, we interpreted the ToM deficits as being related to a more general cognitive dysfunction confirmed in schizophrenia and FEP patients (Bora et al., 2006, 2008). Multiple cognitive deficits could mediate the observed impairments of ToM ability (Bora et al., 2009). In the present study, inefficient processing speed emerges as the neurocognitive domain specifically related to ToM dysfunction. Processing speed and episodic memory are the domains most frequently reported as significantly impaired in a large body of schizophrenia studies (Schaefer et al., 2013).
Two theoretical approaches have explained ToM deficits in autism spectrum disorders (Wilkinson and Ball, 2012). The “Theory-Theory” hypothesizes that the inference of others' mental states is an innate and learner orientated specific domain, suggesting a developmental trajectory for the understanding of mental state concepts. This approach, notably supported by Baron-Cohen, argues that there are selective deficits in ToM develop over time, resulting in individuals inability to integrate social information (e.g., attentional cues) and make effective mental state inferences about other individuals. On the contrary, “Simulation-Theory” proposes that inferences about others' mental states arise by imagining oneself in the position of the other person and simulating what they might believe, desire or intend. The argument is that the difficulty experienced by individuals in understanding mental states reflects a deficit in some aspect of the simulation process, feeding incorrect information into the simulation procedure (i.e., information relating mainly to their own perspective). A new position, called “hybrid consensus,” considers the interactions of both theories and their interdependencies, and may represent the future for empirical evidence. The indications are that pervasive domain general deficits in, for example, executive functioning and working memory, may provide some of the key components for an explanation of the wide range of developmental difficulties seen in autism and schizophrenia spectrum disorders.
It is reasonable that poor emotion recognition, found in patients with schizophrenia spectrum disorders, may be more than just impaired in the capacity to correctly infer emotions from the eyes of other people. Patients may struggle to understand other's emotions when they also are less able to process and integrate information coming from many channels into complex ideas about the self and others (Lysaker et al., 2014). Our results are in accordance with McGlade et al. (2008), confirming that mental estate decoding is mediated by global cognitive function, and particularly by the influence of processing speed. Rehabilitation of sensory processing, in both its speed and its accuracy, could improve ToM ability.
Although previous studies have not found significant effect of age on performance in ToM tasks (Green et al., 2012), our results confirm age as a moderator on the Eyes test. The older we are, the more accurate our recognition of facial emotion. The potential moderating influences of IQ deficits on ToM performance in remitted patients, as well as the potential interactions involving education have been previously suggested (Kettle et al., 2008; Bora et al., 2009). Regretfully, the problem of how IQ interferes with ToM performance remains unresolved, in part because the IQ and ToM test used in the available studies vary considerably (Brüne, 2005a). With respect to years of education, we found this variable a moderator in Eyes test performance. Using a similarly recruited Spanish sample population, with a total of 358 participants from both sexes and an age range from 18 to 65, the Fernández-Abascal et al. (2013) study, conducted a test re-test reliability of the Eyes test. All participants attended tertiary education, following our criteria of a mean of 14 years of education and thus were matched on years of education (10.38 and 10.76 years respectively). Eyes test mean scores in Fernandez-Abascal (27.18, SD 3.59) differed nearly by 4 points from our healthy control group (23.77, SD 4.31). We suggest differences in education could explain differences in Eyes test scores in these two Spanish healthy sample populations. This could be consistent with our results that found education as a moderator of Eyes test performance. Such a finding, while deserving further investigation, is encouraging when considering the use of training programs to improve social cognition (Rocha and Queirós, 2013; Sacks et al., 2013). This is of particular note because it supports the notion that education could improve social cognition.
The main strengths of this study lie in its sampling and design. We used two large and homogeneous samples, representatives of FEP patients and healthy control subjects, from the same catchment area; the 3-year longitudinal design and the employment of an instrument for ToM assessment with proven good psychometric properties (see systematic review Vellante et al., 2013). However, the study has several limitations. First, a data analytic consideration was the presence of missing data. Of the 160 FEP patients and 159 healthy controls initially included, 111 in each group entered the 3-year ANCOVA model. Second, the effect of medication was not examined. Patients were taking antipsychotic medications that might have influenced performance. It should be said though that previous studies have not found evidence for a medication effect on ToM performance because deficits in emotion perception were found at illness onset and show minimal response to effective antipsychotic treatment (Herbener et al., 2005; Chen et al., 2012). Third, in accordance with Kettle et al. (2008), deficits could also reflect problems in semantic knowledge of mental state terms in the Eyes test in the FEP group. Although all participants were provided a glossary of mental state terms used in the test, our data found relationship between Eyes test performance and WAIS-III vocabulary subtest. Finally, we did not analyze the relationship between ToM and real world functioning due to it being beyond the scope of the present paper.
In sum, the findings of this study confirmed stable, thus trait ToM deficit in FEP patients. The relationship between ToM deficits and neurocognitive function, as well as the possible link with daily functioning, support the implementation of training programs for social cognitive impairments in FEP patients.
Author Contributions
All the authors have participated and have made substantial contributions to this paper. RA: design, statistical analysis, interpretations of data and drafting the article. ES, MF, and MR: statistical analysis, interpretations of data and revising the article. KN and AF: interpretations of data and revising the article. SO, JR, and BC: conception, design and revising.
Funding
This work was supported by the Instituto de Salud Carlos III (FIS CP07/00008 and PI14/00918) and Fundación Instituto de Investigación Marqués de Valdecilla. No pharmaceutical industry has participated in the study.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Abbreviations
FEP, First Episode Psychosis; ToM, theory of mind.
References
Addington, D., Addington, J., Maticka-Tyndale, E., and Joyce, J. (1992). Reliability and validity of a depression rating scale for schizophrenics. Schizophr. Res. 6, 201–208. doi: 10.1016/0920-9964(92)90003-N
Addington, J., Saeedi, H., and Addington, D. (2006). Influence of social perception and social knowledge on cognitive and social functioning in early psychosis. Br. J. Psychiatry 189, 373–378. doi: 10.1192/bjp.bp.105.021022
Andreasen, N. C. (1983). Scale for the Assessment of Negative Symptoms (SANS). Iowa City: University of Iowa.
Andreasen, N. C. (1984). Scale for the Assessment of Positive Symptoms (SAPS). Iowa City: University of Iowa.
Andreasen, N. C., Flaum, M., and Arndt, S. (1992). The Comprehensive Assessment of Symptoms and History (CASH). An instrument for assessing diagnosis and psychopathology. Arch. Gen. Psychiatry 49, 615–623. doi: 10.1001/archpsyc.1992.01820080023004
Baron-Cohen, S. (1991). The development of a theory of mind in autism: deviance and delay? Psychiatr. Clin. North Am. 14, 33–51.
Baron-Cohen, S., Wheelwright, S., Hill, J., Raste, Y., and Plumb, I. (2001). The “Reading the Mind in the Eyes” Test revised version: a study with normal adults, and adults with Asperger syndrome or high-functioning autism. J. Child Psychol. Psychiatry 42, 241–251. doi: 10.1111/1469-7610.00715
Bora, E., Eryavuz, A., Kayahan, B., Sungu, G., and Veznedaroglu, B. (2006). Social functioning, theory of mind and neurocognition in outpatients with schizophrenia; mental state decoding may be a better predictor of social functioning than mental state reasoning. Psychiatry Res. 145, 95–103. doi: 10.1016/j.psychres.2005.11.003
Bora, E., Gökcen, S., Kayahan, B., and Veznedaroglu, B. (2008). Deficits of social-cognitive and social-perceptual aspects of theory of mind in remitted patients with schizophrenia: effect of residual symptoms. J. Nerv. Ment. Dis. 196, 95–99. doi: 10.1097/NMD.0b013e318162a9e1
Bora, E., and Pantelis, C. (2013). Theory of mind impairments in first-episode psychosis, individuals at ultra-high risk for psychosis and in first-degree relatives of schizophrenia: systematic review and meta-analysis. Schizophr. Res. 144, 31–36. doi: 10.1016/j.schres.2012.12.013
Bora, E., Yucel, M., and Pantelis, C. (2009). Theory of mind impairment in schizophrenia: meta-analysis. Schizophr. Res. 109, 1–9. doi: 10.1016/j.schres.2008.12.020
Bozikas, V. P., Giannakou, M., Kosmidis, M. H., Kargopoulos, P., Kioseoglou, G., Liolios, D., et al. (2011). Insights into theory of mind in schizophrenia: the impact of cognitive impairment. Schizophr. Res. 130, 130–136. doi: 10.1016/j.schres.2011.04.025
Brüne, M. (2005a). Emotion recognition, ‘theory of mind,’ and social behavior in schizophrenia. Psychiatry Res. 133, 135–147. doi: 10.1016/j.psychres.2004.10.007
Brüne, M. (2005b). “Theory of mind” in schizophrenia: a review of the literature. Schizophr. Bull. 31, 21–42. doi: 10.1093/schbul/sbi002
Cegalis, J., and Bowlin, J. (1991). Vigil: Software for the Assessment of Attention. Nashua, NH: Forthought.
Chen, Y., Cataldo, A., Norton, D. J., and Ongur, D. (2012). Distinct facial processing in schizophrenia and schizoaffective disorders. Schizophr. Res. 134, 95–100. doi: 10.1016/j.schres.2011.08.001
Fernández-Abascal, E. G., Cabello, R., Fernández-Berrocal, P., and Baron-Cohen, S. (2013). Test-retest reliability of the ‘Reading the Mind in the Eyes’ test: a one-year follow-up study. Mol. Autism 4:33. doi: 10.1186/2040-2392-4-33
Fernandez-Gonzalo, S., Jodar, M., Pousa, E., Turon, M., Garcia, R., Rambla, C. H., et al. (2014). Selective effect of neurocognition on different theory of mind domains in first-episode psychosis. J. Nerv. Ment. Dis. 202, 576–582. doi: 10.1097/NMD.0000000000000164
First, M. B., Spitzer, R. L., Gibbon, M., and Williams, J. B. W. (1996). Structured Clinical Interview for DSM-IV Axis I Disorders, Clinician Version (SCID-CV). Washington, DC: American Psychiatric Press, Inc.
González-Blanch, C., Crespo-Facorro, B., Alvarez-Jiménez, M., Rodríguez-Sánchez, J. M., Pelayo-Terán, J. M., Peréz-Iglesias, R., et al. (2007). Cognitive dimensions in first-episode schizophrenia spectrum disorders. J. Psychiatr. Res. 41, 968–977. doi: 10.1016/j.jpsychires.2006.08.009
Green, M. F., Bearden, C. E., Cannon, T. D., Fiske, A. P., Hellemann, G. S., Horan, W. P., et al. (2012). Social cognition in schizophrenia, Part 1: performance across phase of illness. Schizophr. Bull. 38, 854–864. doi: 10.1093/schbul/sbq171
Grube, B. S., Bilder, R. M., and Goldman, R. S. (1998). Meta-analysis of symptom factors in schizophrenia. Schizophr. Res. 31, 113–120. doi: 10.1016/S0920-9964(98)00011-5
Hamm, J. A., Renard, S. B., Fogley, R. L., Leonhardt, B. L., Dimaggio, G., Buck, K. D., et al. (2012). Metacognition and social cognition in schizophrenia: stability and relationship to concurrent and prospective symptom assessments. J. Clin. Psychol. 68, 1303–1312. doi: 10.1002/jclp.21906
Herbener, E. S., Hill, S. K., Marvin, R. W., and Sweeney, J. A. (2005). Effects of antipsychotic treatment on emotion perception deficits in first-episode schizophrenia. Am. J. Psychiatry 162, 1746–1748. doi: 10.1176/appi.ajp.162.9.1746
Horan, W. P., Green, M. F., DeGroot, M., Fiske, A., Hellemann, G., Kee, K., et al. (2012). Social cognition in schizophrenia, Part 2: 12-month stability and prediction of functional outcome in first-episode patients. Schizophr. Bull. 38, 865–872. doi: 10.1093/schbul/sbr001
Inoue, Y., Yamada, K., Hirano, M., Shinohara, M., Tamaoki, T., Iguchi, H., et al. (2006). Impairment of theory of mind in patients in remission following first episode of schizophrenia. Eur. Arch. Psychiatry Clin. Neurosci. 256, 326–328. doi: 10.1007/s00406-006-0608-z
Kettle, J. W., O'Brien-Simpson, L., and Allen, N. B. (2008). Impaired theory of mind in first-episode schizophrenia: comparison with community, university and depressed controls. Schizophr. Res. 99, 96–102. doi: 10.1016/j.schres.2007.11.011
Kohler, C. G., Walker, J. B., Martin, E. A., Healey, K. M., and Moberg, P. J. (2010). Facial emotion perception in schizophrenia: a meta-analytic review. Schizophr. Bull. 36, 1009–1019. doi: 10.1093/schbul/sbn192
Lysaker, P. H., Leonhardt, B. L., Brüne, M., Buck, K. D., James, A., Vohs, J., et al. (2014). Capacities for theory of mind, metacognition, and neurocognitive function are independently related to emotional recognition in schizophrenia. Psychiatry Res. 219, 79–85. doi: 10.1016/j.psychres.2014.05.004
Lysaker, P. H., Olesek, K. L., Warman, D. M., Martin, J. M., Salzman, A. K., Nicolò, G., et al. (2011). Metacognition in schizophrenia: correlates and stability of deficits in theory of mind and self-reflectivity. Psychiatry Res. 190, 18–22. doi: 10.1016/j.psychres.2010.07.016
McGlade, N., Behan, C., Hayden, J., O'Donoghue, T., Peel, R., Haq, F., et al. (2008). Mental state decoding v. mental state reasoning as a mediator between cognitive and social function in psychosis. Br. J. Psychiatry 193, 77–78. doi: 10.1192/bjp.bp.107.044198
Nuechterlein, K. H., Barch, D. M., Gold, J. M., Goldberg, T. E., Green, M. F., and Heaton, R. K. (2004). Identification of separable cognitive factors in schizophrenia. Schizophr. Res. 72, 29–39. doi: 10.1016/j.schres.2004.09.007
Osterrieth, P. A. (1944). Contribution a l'étude de la perception et de la memoire (The test of copying a complex figure: a contribution to the study of perception and memory). Arch. Psychol. 30, 286–350.
Pelayo-Terán, J. M., Pérez-Iglesias, R., Ramírez-Bonilla, M. L., González-Blanch, C., Martínez-García, O., Pardo-García, G., et al. (2008). Epidemiological factors associated with treated incidence of of first-episode non-affective psychosis in Cantabria: insights from the Clinical Programme on Early Phases of Phychosis. Early Interv. Psychiatry 2, 178–187. doi: 10.1111/j.1751-7893.2008.00074.x
Pentaraki, A. D., Stefanis, N. C., Stahl, D., Theleritis, C., Toulopoulou, T., Roukas, D., et al. (2012). Theory of Mind as a potential trait marker of schizophrenia: a family study. Cogn. Neuropsychiatry 17, 64–89. doi: 10.1080/13546805.2011.568289
Periáñez, J. A., R-Lago, M., Rodríguez-Sánchez, J. M., Adrover-Roig, D., S1nchez-Cubillo, I., Crespo-Facorro, B., et al. (2007). Trail Making Test in traumatic brain injury, schizophrenia, and normal ageing: sample comparisons and normative data. Arch. Clin. Neuropsychol. 22, 433–447. doi: 10.1016/j.acn.2007.01.022
Pousa, E., Duñó, R., Brebion, G., David, A. S., Ruiz, A. I., and Obiols, J. E. (2008). Theory of mind deficits in chronic schizophrenia: evidence for state dependence. Psychiatry Res. 158, 1–10. doi: 10.1016/j.psychres.2006.05.018
Reitan, R. M., and Wolfson, D. (1985). The Halstead–Reitan Neuropsycholgical Test Battery: Therapy and Clinical Interpretation. Tucson, AZ: Neuropsychological Press.
Rocha, N. B., and Queirós, C. (2013). Metacognitive and social cognition training (MSCT) in schizophrenia: a preliminary efficacy study. Schizophr. Res. 150, 64–68. doi: 10.1016/j.schres.2013.07.057
Sacks, S., Fisher, M., Garrett, C., Alexander, P., Holland, C., Rose, D., et al. (2013). Combining computerized social cognitive training with neuroplasticity-based auditory training in schizophrenia. Clin. Schizophr. Relat. Psychoses 7, 78A–86A. doi: 10.3371/CSRP.SAFI.012513
Schaefer, J., Giangrande, E., Weinberger, D. R., and Dickinson, D. (2013). The global cognitive impairment in schizophrenia: consistent over decades and around the world. Schizophr. Res. 150, 42–50. doi: 10.1016/j.schres.2013.07.009
So, S. H., Garety, P. A., Peters, E. R., and Kapur, S. (2010). Do antipsychotics improve reasoning biases? A review. Psychosom. Med. 72, 681–693. doi: 10.1097/PSY.0b013e3181e7cca6
Sprong, M., Schothorst, P., Vos, E., Hox, J., and van Engeland, H. (2007). Theory of mind in schizophrenia: meta-analysis. Br. J. Psychiatry 191, 5–13. doi: 10.1192/bjp.bp.107.035899
Thompson, A., Papas, A., Bartholomeusz, C., Allott, K., Amminger, G. P., Nelson, B., et al. (2012). Social cognition in clinical “at risk” for psychosis and first episode psychosis populations. Schizophr. Res. 141, 204–209. doi: 10.1016/j.schres.2012.08.007
Vellante, M., Baron-Cohen, S., Melis, M., Marrone, M., Petretto, D. R., Masala, C., et al. (2013). The “Reading the Mind in the Eyes” test: systematic review of psychometric properties and a validation study in Italy. Cogn. Neuropsychiatry 18, 326–354. doi: 10.1080/13546805.2012.721728
Wechler (1997). Wechsler Adult Intelligence Scale-III. San Antonio, TX: The Psychological Corporation.
Keywords: first episode psychosis, theory of mind, processing speed, clinical symptoms, schizophrenia
Citation: Ayesa-Arriola R, Setién-Suero E, Neergaard KD, Ferro A, Fatjó-Vilas M, Ríos-Lago M, Otero S, Rodríguez-Sánchez JM and Crespo-Facorro B (2016) Evidence for Trait Related Theory of Mind Impairment in First Episode Psychosis Patients and Its Relationship with Processing Speed: A 3 Year Follow-up Study. Front. Psychol. 7:592. doi: 10.3389/fpsyg.2016.00592
Received: 25 January 2016; Accepted: 11 April 2016;
Published: 02 May 2016.
Edited by:
Antonella Marchetti, Università Cattolica del Sacro Cuore, ItalyReviewed by:
Xi-Nian Zuo, Chinese Academy of Sciences, ChinaMeredith Ria Wilkinson, De Montfort University, UK
Copyright © 2016 Ayesa-Arriola, Setién-Suero, Neergaard, Ferro, Fatjó-Vilas, Ríos-Lago, Otero, Rodríguez-Sánchez and Crespo-Facorro. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rosa Ayesa-Arriola, rayesa@humv.es