 Nikos Apostolopoulos
Nikos Apostolopoulos George S. Metsios1
George S. Metsios1 Matthew A. Wyon
Matthew A. Wyon
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Psychol., 18 August 2015
Sec. Performance Science
Volume 6 - 2015 | https://doi.org/10.3389/fpsyg.2015.01128
Stretching exercises to increase the range of motion (ROM) of joints have been used by sports coaches and medical professionals for improving performance and rehabilitation. The ability of connective and muscular tissues to change their architecture in response to stretching is important for their proper function, repair, and performance. Given the dearth of relevant data in the literature, this review examined two key elements of stretching: stretch intensity and stretch position; and their significance to ROM, delayed onset muscle soreness (DOMS), and inflammation in different populations. A search of three databases, Pub-Med, Google Scholar, and Cochrane Reviews, identified 152 articles, which were subsequently categorized into four groups: athletes (24), clinical (29), elderly (12), and general population (87). The use of different populations facilitated a wider examination of the stretching components and their effects. All 152 articles incorporated information regarding duration, frequency and stretch position, whereas only 79 referred to the intensity of stretching and 22 of these 79 studies were deemed high quality. It appears that the intensity of stretching is relatively under-researched, and the importance of body position and its influence on stretch intensity, is largely unknown. In conclusion, this review has highlighted areas for future research, including stretch intensity and position and their effect on musculo-tendinous tissue, in relation to the sensation of pain, delayed onset muscle soreness, inflammation, as well as muscle health and performance.
Stretching refers to a movement applied by an external and/or internal force in order to increase one's joint range of motion i.e., flexibility (Light et al., 1984; Weerapong et al., 2004). Forms of stretching include active, passive, dynamic, static, ballistic, and proprioceptive neuromuscular facilitation (PNF) (Sady et al., 1982; Shellock and Prentice, 1985; Alter, 2004; Bonnar et al., 2004; Shrier, 2004). Traditionally, stretching exercises have been advocated by sports coaches and medical professionals as a means for performance enhancement and injury prevention by regaining joint range of motion (ROM) i.e., increasing flexibility (Hortobágyi et al., 1985; Taylor et al., 1990; Wilson et al., 1991).
Stretching depends on the active and passive tension of the muscle, the musculo-tendinous unit (MTU), as well as the proprioceptors of the musculoskeletal system, the muscle spindles, and the Golgi tendon organs (Nikolaou et al., 1987; Guissard and Duchateau, 2006; Knudson, 2006; Abdel-aziem et al., 2013). The tension created by muscle can be classified as either active or passive, with active referring to the interaction of the actin and myosin filaments of muscle, and passive to the elongation of the connective tissue beyond their resting length (Knudson, 2006). Both active and passive define the length-dependent properties of muscle which is strongly related to stretching, for the interaction of each implies that exercise interventions, like stretching, may have a complex effect on skeletal muscle, dependent on the interaction of the tissues and the nature of the training stimulus (Knudson, 2006). In other words, when muscle is stretched using stretching techniques [i.e., static, active, dynamic, or PNF] these may account for changes in the active and passive tension of muscle improving the ROM about a joint (Knudson, 1999).
The MTU features prominently in stretching, with Kubo et al. (2001) suggesting the potential mechanism for reduced risk of injury with increased flexibility is the change in its viscoelastic properties. During stretching, with the MTU being held at a constant length, the passive force at that length gradually declines, resulting in a stress relaxation (Magnusson et al., 1995). In-vivo (Magnusson et al., 1995) and in-vitro (Taylor et al., 1990) studies have observed that repeated stretching of the MTU to a constant length reduces peak passive tension, suggesting that this reduction in the viscosity and/or stiffness of the MTU during stretching is responsible for the increase in the joint ROM (Kubo et al., 2001).
Within the muscle fibers and tendons are located the proprioceptors, sensors providing information about joint angle, muscle length, and muscle tension. Two proprioceptors related to stretching are the muscle spindles (respond to changes in length) and the Golgi tendon organs (respond to changes in tension) (Guissard and Duchateau, 2006; Abdel-aziem et al., 2013), relaying information about muscular tension to the central nervous system (Abdel-aziem et al., 2013). Therefore, the interplay of muscle tension (active and passive), the MTU and viscoelasticity and the proprioceptive tissue (muscle spindles and Golgi tendon organ), are important when considering how stretching may influence the increase or decrease of flexibility and the ROM about a joint.
In the literature, four stretch parameters have been identified as being important for potentially influencing the increase or decrease of flexibility of a joint: intensity, duration, frequency (Marschall, 1999), and stretch position (Wyon et al., 2009). The focus of this review was on the intensity of the stretch and stretch position. Intensity is important for the magnitude of force generated during stretching may influence the response of the tissue. For instance, too little force may result in an elastic response with little or no gain in ROM (Jacobs and Sciascia, 2011), while the application of too much force may injure the tissue, leading to an inflammatory response (Brand, 1984; McClure et al., 1994). The rationale for including stretch position is that this may directly or indirectly influence the intensity of the stretch, for muscle and tendon tissue and their components (i.e., collagen) are known to respond to altered levels of activity (Kjaer, 2004). The position assumed during stretching may influence the magnitude of the force generated prior to and during the stretch potentially altering the response of the muscle and tendon tissue. In a study by Abdel-aziem et al. (2013), comparing a standing hamstring stretch to a supine lying stretch, the supine lying stretch isolated the hamstring muscle better, was more comfortable, but more importantly facilitated a better relaxation response during the stretch. In this review, four positions were identified: loaded, supported, therapist, and machine, with each being defined in the Materials and Methods Section (stretching intensity and position). Though joint angle, force direction, magnitude, and duration of stretch may remain identical, this does not preclude the notion that a force might be generated in relation to the stretch position heightening the stress or strain on the muscle, tendon, and the MTU. Even though the force generated during the stretch on the muscle and tendon tissue is not known with regard to different stretch positions, suggesting further research, what is known and has been observed is that the load imparted by force affects the structural and functional adaptation of the tissue (Kjaer, 2004).
This adaptation of muscle to force refers to muscle plasticity, a mechanical property suggesting the ability of muscle cells to alter their structure and function in response to various stimuli (Martins et al., 2013). It has been observed that the stretch of muscle cells interact closely with skeletal muscle tissue suggesting an adaptive process when subjected to a mechanical load (Kjaer, 2004). Load has been defined as a either a cyclic or static stretch, strain or shear stress, with a combination of these loads being responsible for altering the shape of a body resulting in an adaptation (Salameh and Dhein, 2013). These forces can deform the extracellular matrix (ECM), which links tissues of the body together playing an important role in the tissue structure maintenance of tendons, ligaments and muscle (Kjaer, 2004). Studies on stretching have indicated that stretching can promote sarcomeregenesis, a synthesis of contractile protein produced by specific muscle, by machanotransduction (Martins et al., 2013). During stretching, this mechanical stimulus affects the ECM, with the integrins, the transmembrane receptors bridging cell-ECM interactions, detecting and transmitting this stimulus into the cell interior (De Deyne, 2001). This stimulus activates a series of nuclear proteins modifying gene transcription regulating sarcomeregenesis (De Deyne, 2001). With intensity defined as the magnitude of force or torque being applied to the joint during a stretching exercise (Jacobs and Sciascia, 2011), and stress relaxation refers to a decrease in the force necessary to hold a tissue at a particular length over time, the combination of intensity and stretch position may play a significant role in increasing the ROM about a joint, possibly through the process of sarcomeregenesis. Subsequently, the combination of stretch intensity and position with duration and frequency may play a significant role in increasing ROM (Wyon et al., 2009, 2013), possibly influencing the body's response with regard to delayed onset muscle soreness (DOMS) or inflammation (Smith et al., 1993).
DOMS, is a sensation of dull, aching pain, combined with tenderness and stiffness occurring 24 h post unaccustomed exercise, peaking 1–3 days, disappearing by 7–10 days (MacIntyre et al., 1995). It is generally accepted that DOMS is associated with muscle and/or connective tissue damage, and/or subsequent inflammatory responses induced by eccentric exercise (Nosaka et al., 2002). According to Smith (1991) the observed events associated with acute inflammation are also seen with DOMS: swelling, loss of function, and pain. The symptoms and signs arising from normal tissue exposed to high intensity stimuli generally reflect the intensity, localization, and timing of the initiating stimuli (Kidd and Urban, 2001). Stretch intensity has been inherently mediated by pain, with stretching beyond the pain threshold for prolonged periods associated with an inflammatory response (Jacobs and Sciascia, 2011). Given the relationship of pain to tissue damage, and its relationship to inflammation (Merskey and Bogduk, 1994), it is very interesting that, although duration and frequency have attracted scientific attention, the magnitude of the stretch intensity and the body's position during stretching have not attracted as much.
It has been observed in the literature that the independent variables of duration and frequency, being “quantitative” in nature, are used extensively (Tables 1–4). They are probably easier to manipulate with participants instructed to hold a particular stretch for a certain length of time (duration) repeated for several sets (frequency). However, the independent variables of stretch intensity and position are more difficult to manipulate. They are “ordinal” in nature referring to a feeling, a perception unique to each participant. Experimenters often resort to descriptive terms to convey the sensation, what the intensity should feel like during the stretching exercise (i.e., discomfort, pain etc.), and the position adopted during the exercise (i.e., standing vs. a supine position). Therefore, given the difficulty manipulating stretching intensity and position, most articles mention them in conjunction with duration and frequency relative to applications both clinically and athletically. To date there are no systematic reviews focused on stretch intensity and body position and how this may affect the soft and connective tissue. This is interesting since stretch intensity and body position have been included in the design of stretching experiments presuming their relevance, however they have not been fully investigated. In fact, most systematic reviews refer to stretching in response to muscle performance (Weerapong et al., 2004; Rubini et al., 2007; Kay and Blazevich, 2012), muscle soreness and injury risk (Herbert and Gabriel, 2002; Connolly et al., 2003; Thacker et al., 2004), and increases in ROM (Decoster et al., 2005; Harvey et al., 2006).
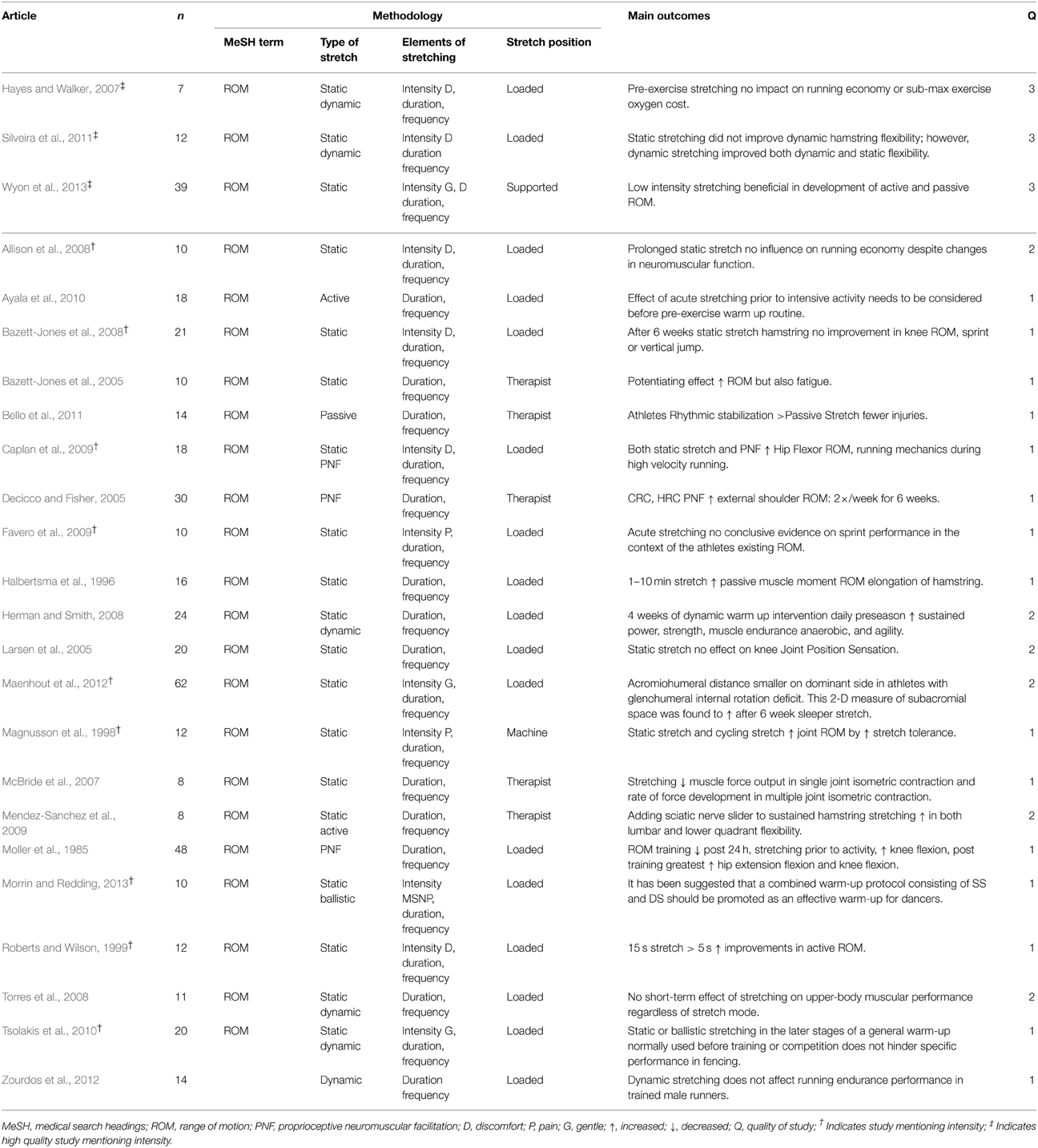
Table 1. Athlete population.
With this literature review four populations were chosen (athlete, clinical, elderly, and general) each highlighting a variance with the use of and importance of stretching. It should be noted that the general population referenced studies that do not specifically refer to athletes, clinical, and the elderly. Within the athletic group, athletes, coaches, and trainers recommend stretching in an effort to both prevent injury and enhance performance (Thacker et al., 2004). In the clinical population, stretching is used to deal with numerous pathophysiological conditions such as; stroke, contractures, and various musculoskeletal disorders in order to provide relief from pain. With the elderly population, the greatest concern with stretching is increasing the movement of the lower limb in order to improve gait and mobility (Christiansen, 2008; Cristopoliski et al., 2009). However, though these variances amongst these populations are important, the emphasis of this review is to investigate how stretch intensity and body position may impact and influence the soft and connective tissue of these populations, given the dearth of studies with regard to these parameters of stretching.
Using the following limits: humans (adults), English language, clinical trials, randomized controlled trials, and reviews, three databases were consulted (PubMed/Medline, Google Scholar, and Cochrane reviews), in order to determine stretch intensity and its association to stretching. The Medical Subject Heading (MeSH) terms, “stretch” and “stretching exercises,” were utilized in combination with “ROM,” “DOMS,” and “inflammation” in four different populations: athletes, clinical, elderly, and general population. The athlete group consisted of all studies mentioning an athletic activity which included only athletes, the clinical group concerned patients with any disease/injury, and the elderly group included individuals of 65+ years of age. The general group comprised all remaining studies not adhering to the criteria set for the three aforementioned groups. In addition, a “quality of study” assessment as set out by Jadad et al. (1996) was employed to evaluate the quality of the selected studies. Eligibility for each study was based on the following criteria. If studies were described as randomized they were given a point, with a further point awarded if the method of randomization was described. Randomization was deemed appropriate if it allowed each participant to have the same access of receiving the intervention, if this criteria was not met a point was deducted. Studies were also given a point if they were described as double blind, with another point assigned if both the person administering and the participant receiving the intervention could not identify it. If this criteria was not met a point was deducted. In turn, a point was given if the study described the number and the reasons for participant withdrawal. The maximum score for each study was five with the minimum for an included report being one. Scores of three or greater were deemed of high quality. Studies that did not meet any of the criteria were excluded from the literature review. The initial search produced 400 relevant articles, of which 205 overlapped between databases, leaving 195 studies. Of these studies, 43 were excluded for not satisfying any of the criteria of the “quality of study” assessment as described above. This resulted in the inclusion of 152 articles (Athlete n = 24; Clinical n = 29; Elderly n = 12; General n = 87) for this review (Figure 1, PRISMA flow diagram).
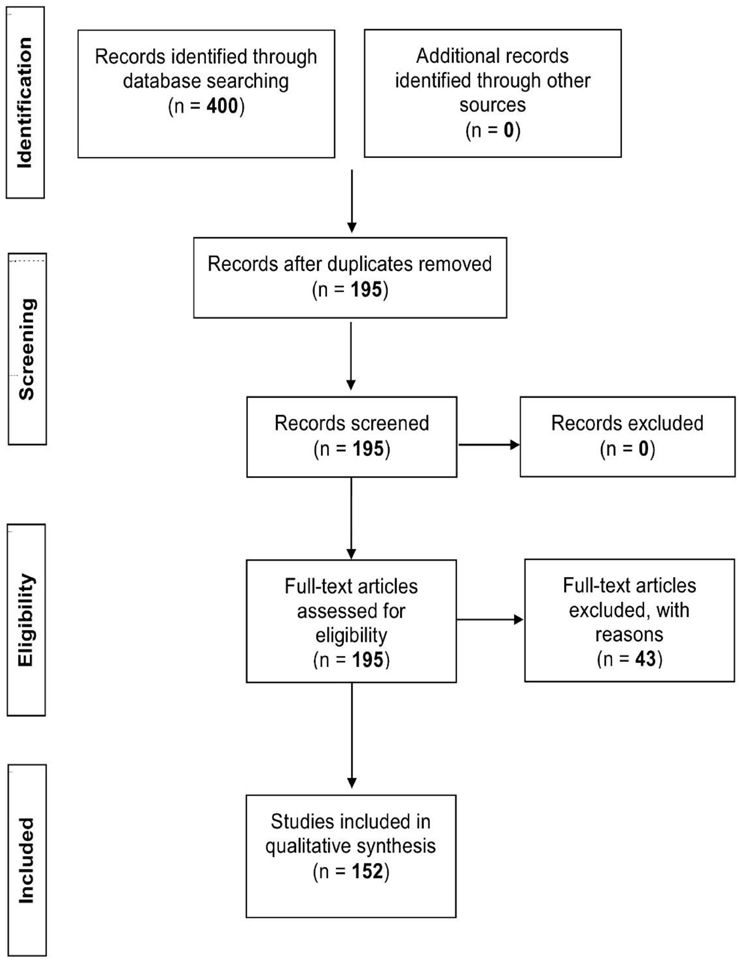
Figure 1. PRISMA flow diagram.
For the purpose of this literature review, the stretch intensity for each article was assessed if it referenced to a subjective sensation of the stretch: discomfort, gentle (feeling of gentle pull on the muscle), maximum stretch no pain (MSNP), and pain, or mentioned the use of a scale (i.e., numerical, visual, and soreness rating scale). In turn, position was assessed by assessing the execution of the stretching exercise as either being: supported, loaded, therapist, and machine assisted. Supported referred to the placement of the body in a position where it is stable with a broad base of support (i.e., lying down vs. standing up). A loaded stretch, pertained to placing the body in a stretch position where the muscle that is being stretched is also called upon to help support the body during the stretch (i.e., a lying down hamstring stretch vs. a stand up hamstring stretch). The last two stretch positions referred to the use of a machine (e.g., isokinetic dynamometer) or a therapist as the means of applying the force on the muscle-tendon unit. The sensations and positions described above are conscious in nature (Proske and Gandevia, 2012), with the individual being aware of tension generated by the muscle during the stretching. This sensory input involved generates an awareness that may influence stretch intensity.
Twenty-four studies were identified in which all mentioned duration and frequency, but only 12 referenced intensity (Magnusson et al., 1998; Roberts and Wilson, 1999; Hayes and Walker, 2007; Allison et al., 2008; Bazett-Jones et al., 2008; Caplan et al., 2009; Favero et al., 2009; Tsolakis et al., 2010; Silveira et al., 2011; Maenhout et al., 2012; Morrin and Redding, 2013; Wyon et al., 2013) (Table 1). Of these 12 studies, 11 had participants perform a loaded stretch of which six had them stretch to discomfort (Roberts and Wilson, 1999; Hayes and Walker, 2007; Allison et al., 2008; Bazett-Jones et al., 2008; Caplan et al., 2009; Silveira et al., 2011). It is interesting to note that two studies observed stretching had no impact on running economy (Hayes and Walker, 2007; Allison et al., 2008), one study noticed no improvement in knee ROM (Bazett-Jones et al., 2008), with another observing no improvement in dynamic hamstring flexibility (Silveira et al., 2011). However, this study did observe that dynamic stretching did improve both dynamic and static flexibility. Interestingly the two remaining studies indicated that stretching to discomfort resulted in a benefit with an increase in hip flexor ROM (Caplan et al., 2009) and active ROM (Roberts and Wilson, 1999). Such a contradiction suggests the need to perform more studies specifically looking at how stretching to discomfort during a loaded stretch may affect the musculoskeletal system. Two studies had participants stretch using a gentle intensity stretch (Tsolakis et al., 2010; Maenhout et al., 2012). Tsolakis et al. observed that gentle stretching used before training or competition did not hinder performance in fencing (Tsolakis et al., 2010), with Maenhout et al. noticing an increase in subacromial space after 6 weeks of stretching (Maenhout et al., 2012). Two studies which had participants stretch to pain used different stretch positions, loaded (Favero et al., 2009) and machine (Magnusson et al., 1998) with results indicating that acute stretching did not improve sprint performance (Favero et al., 2009) and an increase in ROM was due to stretch tolerance (Magnusson et al., 1998). This is in direct contrast to the studies which observed an improvement with the use of gentle intense stretching (Tsolakis et al., 2010; Maenhout et al., 2012). In turn, the study by Wyon et al. which referred to both a gentle and discomfort intense stretch with support, observed an increase in both active and passive ROM with use of a gentle stretch (Wyon et al., 2013).
It is worth highlighting, that within this population, only three studies were of high quality (Hayes and Walker, 2007; Silveira et al., 2011; Wyon et al., 2013) (Refer to Table 1), indicating the need to perform more studies in order to observe how intensity and body position may impact the athletic population.
Twenty-nine studies have been conducted on clinical populations suffering from neck pain, cancer, continuous obstructive pulmonary disease, contractures, as well as joint and trigger point issues (Table 2). All 29 studies mentioned duration and frequency, with seven referencing stretch intensity(Light et al., 1984; Hanten et al., 2000; Horsley et al., 2007; Cunha et al., 2008; Maluf et al., 2010; Trampas et al., 2010; Renan-Ordine et al., 2011), of which only two were of high quality (Horsley et al., 2007; Maluf et al., 2010). These high quality studies had participants perform loaded stretches with Maluf et al. having patients stretch to discomfort, while Horsley et al. used a MSNP. Interestingly, the study by Horsley et al. observed no benefit with use of stretching with regard to wrist contracture of stroke patients, a central nervous system (CNS) issue, while Maluf et al. indicated a benefit of stretching for transmandibular pain, a peripheral nervous system (PNS) issue.
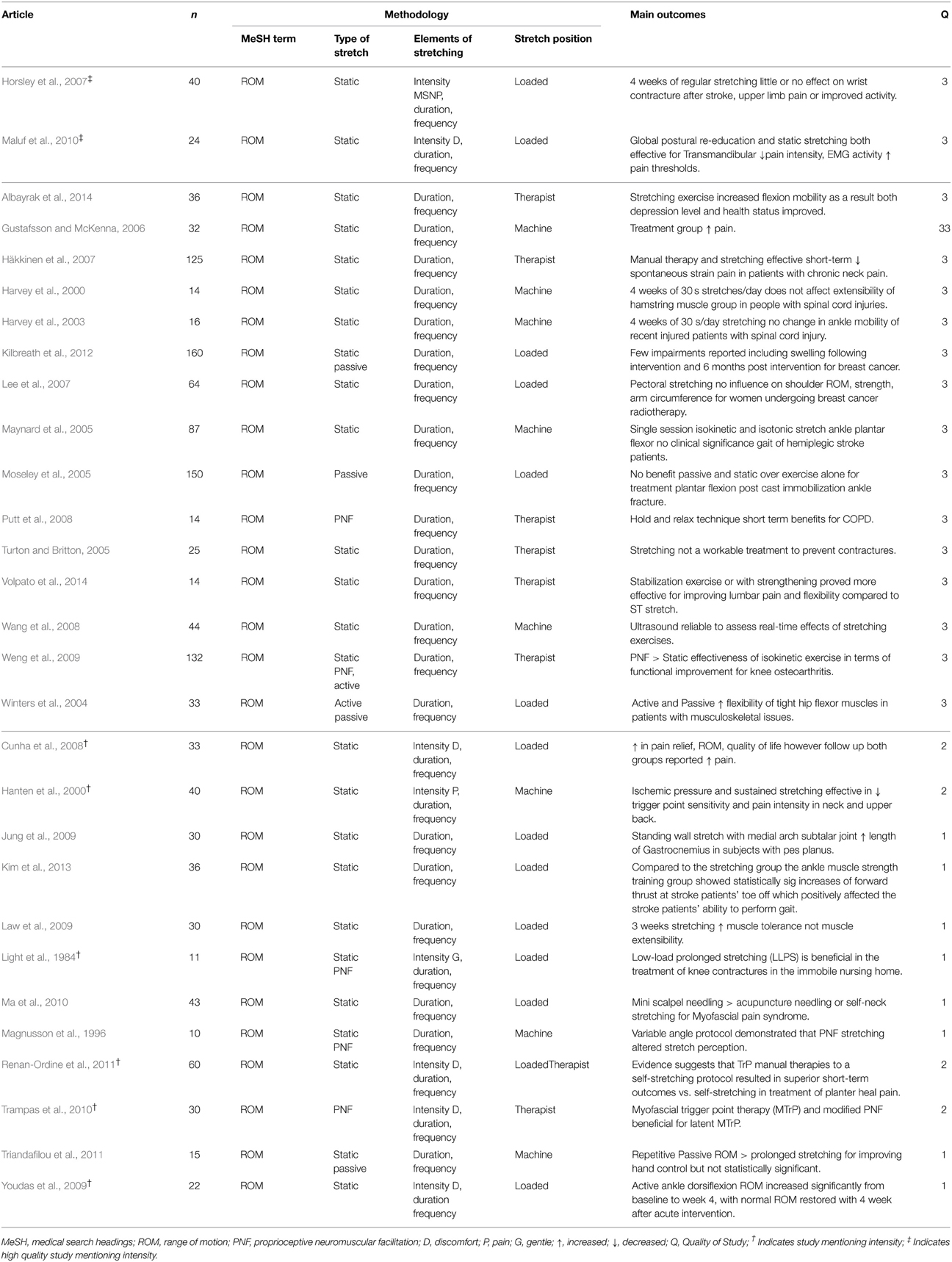
Table 2. Clinical population.
Of the five remaining lower quality studies referencing intensity (Light et al., 1984; Hanten et al., 2000; Cunha et al., 2008; Trampas et al., 2010; Renan-Ordine et al., 2011), three had participants stretch to discomfort while performing a loaded stretch (Cunha et al., 2008; Renan-Ordine et al., 2011) or with use of a therapist (Trampas et al., 2010). Of the remaining two studies Hanten et al. had patients stretch to pain with use of a machine (Hanten et al., 2000) and Light et al. used a loaded stretch with a gentle stretch intensity (Light et al., 1984). Interestingly, amongst the seven studies referencing intensity, two studies observed the response of participants to global postural re-education, a technique that simultaneously stretches all the muscles in either a posterior or anterior muscle chain. These studies contradicted each other, with the high quality study indicating an increase in pain relief (Maluf et al., 2010), with the other study reporting an increase in pain post-intervention (Cunha et al., 2008). This contradiction exemplifies the current state of knowledge regarding stretch intensity and position and further suggests the need for higher quality research studies. It may be the need to standardize methodologies and data collection in order to ensure better outcomes. A contradiction was also observed between two low quality studies concerned with trigger points (TrP) (Trampas et al., 2010; Renan-Ordine et al., 2011). Renan-Ordine et al. suggested that trigger point (TrP) manual therapies were superior over use of self-stretching (Renan-Ordine et al., 2011), with Trampas et al. indicating that stretching was more beneficial for latent myofascial TrPs (Trampas et al., 2010). In addition, another study that looked at a combination of a gentle intensity with a loaded stretch, reported a benefit in the treatment of knee contractures (Light et al., 1984). It is interesting to note that a study combining stretch to discomfort through a therapist, and a study combining a loaded stretch with gentle intensity both showed a benefit. The use of a therapist may well have increased stability and the ability of the participants to relax, which yielded the same effect to that seen with use of a gentle loaded stretch. This observation also applies to the last study, which reported a decrease in TrP sensitivity and pain intensity in the neck following stretching to an intensity of pain via use of a machine (Hanten et al., 2000); here, the machine provided a stable controlled environment, possibly allowing participants to relax during the intervention.
Out of the 29 studies 15 studies which did not mention intensity, rated a three out of five using the quality criteria scores (Harvey et al., 2000, 2003; Winters et al., 2004; Maynard et al., 2005; Moseley et al., 2005; Turton and Britton, 2005; Gustafsson and McKenna, 2006; Häkkinen et al., 2007; Lee et al., 2007; Putt et al., 2008; Wang et al., 2008; Weng et al., 2009; Kilbreath et al., 2012; Albayrak et al., 2014; Volpato et al., 2014). Of these high quality studies, six studies revealed no benefit regarding spinal cord and contracture issues with use of static stretching (Harvey et al., 2000, 2003; Maynard et al., 2005; Turton and Britton, 2005; Gustafsson and McKenna, 2006; Horsley et al., 2007). Four studies on spinal cord injuries used a machine to stabilize stretch position (Harvey et al., 2000, 2003; Maynard et al., 2005; Gustafsson and McKenna, 2006) and the one study on contractures used a therapist to provide the stretch (Turton and Britton, 2005). It has been observed that stretching does not affect CNS injuries and disorders, but alters PNS function. This view is supported by five studies which indicate that static stretching was beneficial for treating neck pain (Häkkinen et al., 2007), a positive morphologic change of the iliotibial band (Wang et al., 2008), knee osteoarthritis (Weng et al., 2009) and an increase of hip flexor ROM (Winters et al., 2004) as well tight hip flexors (Winters et al., 2004). Participants were stretched via a machine (Wang et al., 2008), a therapist (Häkkinen et al., 2007; Putt et al., 2008; Weng et al., 2009), or performed a loaded stretch (Winters et al., 2004). The study by Albayrak also supported the view of the influence of stretching on the PNS observing that an increase in mobility improved both the depression level and health status of the patients (Albayrak et al., 2014).
Twelve studies with designated control groups, reported the benefits of stretching in the elderly. Improvements were seen in various outcomes, including gait length and speed as well as flexibility and mobility (Feland et al., 2001; Kerrigan et al., 2003; Gadjosik et al., 2005; Zakas et al., 2006; Christiansen, 2008; Batista et al., 2009; Cristopoliski et al., 2009; Stanziano et al., 2009; González-Ravé et al., 2012; Locks et al., 2012; Watt et al., 2011a,b) (Table 3). All the articles reported duration and frequency, with five referring to stretch intensity of which two were of high quality (Zakas et al., 2006; Cristopoliski et al., 2009), with three being of low quality (Feland et al., 2001; Batista et al., 2009; González-Ravé et al., 2012).
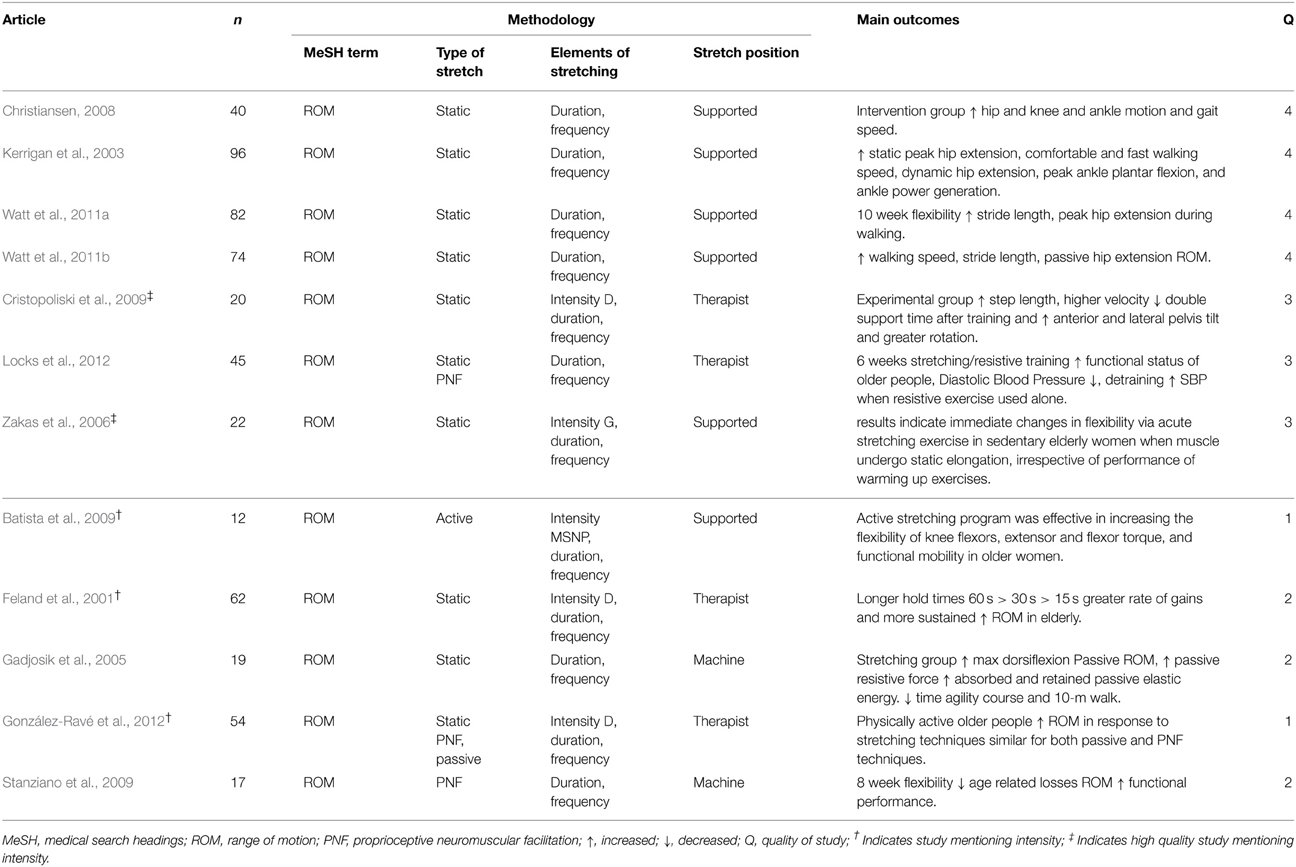
Table 3. Elderly population.
The two high quality studies had the elderly participants perform a supported stretch (Zakas et al., 2006) or were stretched by a therapist using a static stretch (Cristopoliski et al., 2009). One study observed an improvement in flexibility (Zakas et al., 2006), with the other seeing an increase in step length resulting in an increase in higher velocity during walking (Cristopoliski et al., 2009). Five studies which rated a high quality but did not mention stretch intensity used static stretching (Kerrigan et al., 2003; Christiansen, 2008; Watt et al., 2011a,b), or in combination with a PNF stretch (Locks et al., 2012). All participants performed a supported and stable stretch, which resulted in an increase in gait, walking speed, stride length, ROM for hip extension, and plantar flexion.
Of the remaining five studies which were low quality, three mentioned intensity, with one study having participants perform a static stretch with use of a therapist (Feland et al., 2001), another with use of a therapist exposed the elderly to a static stretch in combination with PNF and passive (González-Ravé et al., 2012), with the last study having the elderly perform an active supported stretch (Batista et al., 2009). All three observed that stretching was beneficial with regard to increasing flexibility of knee flexors, extensors (Batista et al., 2009), as well as increasing ROM of the hamstring, hip, and shoulder (Feland et al., 2001; González-Ravé et al., 2012). The other studies used machines to induce stretching, and found an increase in dorsiflexion and passive resistance force, and a decrease in age-related losses of ROM (Gadjosik et al., 2005; Stanziano et al., 2009). It is interesting to note that with the elderly population all the studies had the participants perform a supported stretch, or made use of a therapist or a machine. None of the participants performed loaded stretches.
A total of 87 articles were included in the general population, with all articles referencing duration and frequency, and 55 mentioning intensity (Table 4). Of these 55 articles 15 were of high quality and 40 of low quality. Within the high quality studies, one study had participants stretch to pain during a loaded stretch, and reported that static stretching was more likely compared to ballistic to cause DOMS (Smith et al., 1993). Six studies had participants stretch to discomfort, with five of these having participants perform a loaded stretch (McNair and Stanley, 1996; Curry et al., 2009; Rancour et al., 2009; Cipriani et al., 2012; Wicke et al., 2014). The last study made use of a machine to generate stress on the muscle tendon unit during the stretch (Medeiros et al., 1977). The study by Medeiros et al. indicated both isometric and passive stretching produce similar results on hip joint ROM (Medeiros et al., 1977). McNair et al. observed that a combination of a loaded stretch with discomfort was more effective for increasing dorsiflexion compared to jogging (McNair and Stanley, 1996). The study by Wicke et al. (2014) suggested that self-PNF can be used in place of static stretching to increase ROM about a joint. The study by Cipriani et al. (2012) indicated no sex differences in terms of stretch response, with Curry et al. (2009) observing that dynamic flexibility enhanced performance on power outcomes greater than static stretching. The study by Rancour et al. (2009) suggested that intermittent stretch training (i.e., 2 or 3 times per week) was sufficient to maintain ROM gains acquired from a static stretching programme.
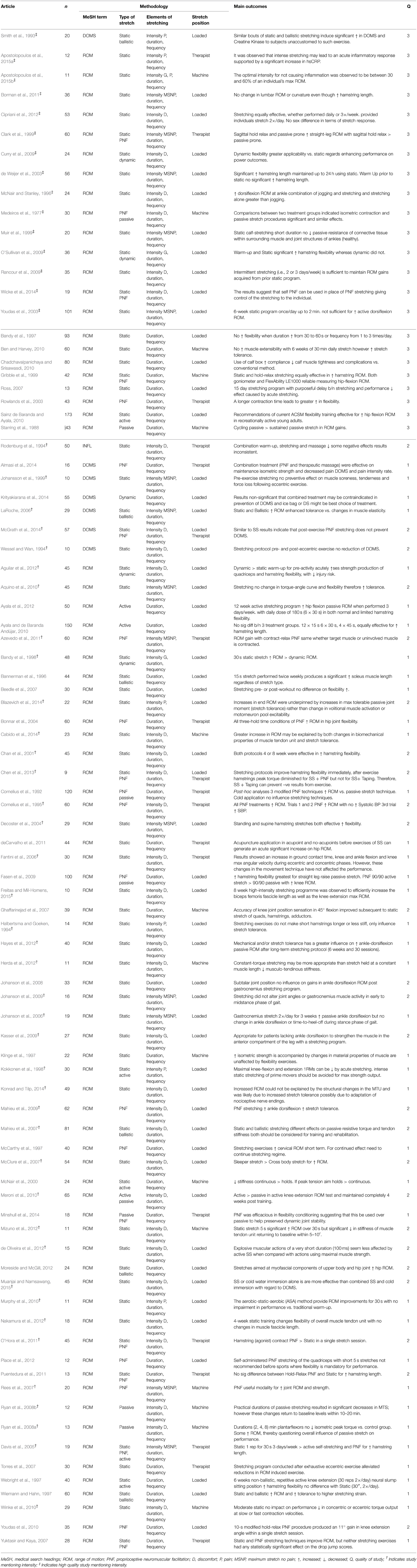
Table 4. General population.
Of the remaining eight high quality studies, four referred to MSNP during a loaded stretch position (Muir et al., 1999; de Weijer et al., 2003; Youdas et al., 2009; Borman et al., 2011), one observed the use of a therapist during a MSNP stretch (Clark et al., 1999), with the last observing the results of a gentle loaded stretch (O'sullivan et al., 2009). Overall, it is interesting to note that articles referring to stretches performed with MSNP and gentle indicated a benefit within the participants compared to the stretches utilizing pain and discomfort during a loaded stretch. Finally, two studies referred to stretch intensity, with use of a therapist and a machine (Apostolopoulos et al., 2015a,b). In the first study participants were stretched to pain with use of a therapist concluding that an intense stretch can cause inflammation (Apostolopoulos et al., 2015a). Similarly, the second study, which used a machine to stretch participants at various stretch intensities concluded that a very intense stretch caused inflammation (Apostolopoulos et al., 2015b).
Regarding the 40 low quality studies, 25 had participants stretch to discomfort of which 15 in combination with a loaded stretch (Wessel and Wan, 1994; Chan et al., 2001; Mahieu et al., 2007; McClure et al., 2007; Mahieu et al., 2009; Meroni et al., 2010; Aguilar et al., 2012; de Oliveira et al., 2012; Hayes et al., 2012; Morais de Oliveira et al., 2012; Nakamura et al., 2012; Chen et al., 2013; Konrad and Tilp, 2014; McGrath et al., 2014; Freitas and Mil-Homens, 2015; Muanjai and Namsawang, 2015), four used therapists (Rodenburg et al., 1994; Cornelius et al., 1995; Fantini et al., 2006; O'Hora et al., 2011), while the remaining six made use of machines (Ryan et al., 2008a,b; Winke et al., 2010; Herda et al., 2012; Mizuno et al., 2012; Cabido et al., 2014). In turn, of the 25 articles four suggested that the changes observed with stretching were due to stretch tolerance rather than mechanical (Mahieu et al., 2009; Hayes et al., 2012; Cabido et al., 2014; Konrad and Tilp, 2014). In contrast four articles observed changes in the musculoskeletal system in response to stretching (Herda et al., 2012; Mizuno et al., 2012; Nakamura et al., 2012; Freitas and Mil-Homens, 2015).
Of the 15 remaining articles, nine referred to MSNP, with six referencing a loaded stretch (Johansson et al., 1999; Decoster et al., 2004; Johanson et al., 2006, 2009; LaRoche, 2006; Aquino et al., 2010), two with a therapist (Davis et al., 2005; Azevedo et al., 2011), and the last one had participants perform the stretch with use of a machine (Rees et al., 2007). Similar to the articles that referred to discomfort, two indicated that stretch tolerance was the reason for the observed increase in ROM (LaRoche, 2006; Aquino et al., 2010).
Four articles had participants stretch to pain, three performing a loaded stretch (Kokkonen et al., 1998; Murphy et al., 2010; Blazevich et al., 2012) and one with a therapist (Halbertsma and Goeken, 1994). Two studies suggested that the increase in ROM was due to stretch tolerance (Halbertsma and Goeken, 1994; Blazevich et al., 2014). The last two low quality studies referred to gentle loaded stretches (Bandy et al., 1998; Kasser et al., 2009).
Fifty-eight studies referenced static stretching by itself or in combination with other stretching techniques concerned with ROM (Table 4). Four studies referred to static stretching or in combination of with regard to DOMS (Wessel and Wan, 1994; Johansson et al., 1999; LaRoche, 2006; McGrath et al., 2014). It is interesting to note that all four had participants perform a loaded stretch.
When comparing articles that referenced loaded stretches to either therapists, machines when referring to discomfort, pain, MSNP, and gentle, it was observed that articles using therapists, and machines indicated an improvement in ROM overall (Rodenburg et al., 1994; Cornelius et al., 1995; Davis et al., 2005; Fantini et al., 2006; Rees et al., 2007; Ryan et al., 2008a,b; Herda et al., 2012; Mizuno et al., 2012). In contrast, when a stretch using a therapist was performed to pain this did not improve the ROM of the hamstring muscles (Halbertsma and Goeken, 1994). Further investigation is needed to determine the reason for the observed influence of the therapist and machine with use of comparing MSNP vs. pain.
Overall the 40 low quality studies were inconclusive as to whether stretching was beneficial. This discrepancy may be due to the influence of discomfort or pain with use of a loaded stretch, vs. use of a machine or therapist were there is possibly more control and support during the execution of the stretch. More research is needed to be performed to determine if this is the case or not.
It is worthwhile to note that 10 studies lacked a designated control group (Cornelius et al., 1995; Kokkonen et al., 1998; McNair et al., 2000; Beedle et al., 2007; Ghaffarinejad et al., 2007; Torres et al., 2007; Meroni et al., 2010; Murphy et al., 2010; Winke et al., 2010; Cabido et al., 2014), with only four studies referencing all three stretching parameters (intensity, duration, and frequency). Of these four studies, three used a loaded stretch position (Kokkonen et al., 1998; Meroni et al., 2010; Murphy et al., 2010) with two referencing pain, and another last referring to discomfort. Unfortunately, the lack of a control group makes these studies inconclusive, reinforcing the need to design and conduct higher quality studies in order to properly observe and determine the importance of stretch intensity and position.
The aim of this review was to examine the relevance of stretch intensity and position in different populations, and to investigate the potential relationship of the two in terms of inflammation, DOMS and ROM. A total of 152 articles were identified for this literature review. The majority of the studies in each of the four populations were of low quality based on the “quality of study” criteria selected for this review. Based on the criteria used there is a need for higher quality material regarding these important exercise and training elements and their influence on athletic performance as well as rehabilitation.
A common theme in the four populations is that the associated studies refer mainly to duration and frequency, with only a few referencing intensity. The likely reason for this is that duration and frequency are easier to manipulate and quantify (Feland et al., 2001). Concerning stretch intensity and position, discrepancies were prevalent within the four groups. In the athletic group, all the studies dealt with ROM, with only 12 mentioning intensity (Magnusson et al., 1998; Roberts and Wilson, 1999; Hayes and Walker, 2007; Allison et al., 2008; Bazett-Jones et al., 2008; Caplan et al., 2009; Favero et al., 2009; Tsolakis et al., 2010; Silveira et al., 2011; Maenhout et al., 2012; Morrin and Redding, 2013; Wyon et al., 2013). It is noticeable that five (Hayes and Walker, 2007; Allison et al., 2008; Bazett-Jones et al., 2008; Favero et al., 2009; Silveira et al., 2011) out of the seven studies (Roberts and Wilson, 1999; Hayes and Walker, 2007; Allison et al., 2008; Bazett-Jones et al., 2008; Caplan et al., 2009; Favero et al., 2009; Silveira et al., 2011) which combined a loaded stretch with an intensity of discomfort and pain observed no improvement. The one study that referred to a supported stretch while participants were performing a stretch of either a gentle or discomfort intensity, observed that the participants performing a gentle supported stretch had the greatest gains in both active and passive ROM (Wyon et al., 2013). This begs the question as to whether a loaded stretch may influence stretch intensity. However, these studies that referred to discomfort and pain during a loaded stretch (Allison et al., 2008; Bazett-Jones et al., 2008; Caplan et al., 2009; Favero et al., 2009) were of low quality, thus preventing definite conclusions to be drawn based on the criteria of the literature review that looked at higher quality studies which mentioned stretch intensity.
In line with the athlete group, studies comprising the clinical equivalent were primarily focused on ROM. However, greater dependency was placed on the use of therapists and machines to achieve optimal stretch position. Regarding intensity, two studies examining global posture re-education referred to intensity during a loaded stretch position (Cunha et al., 2008; Maluf et al., 2010). Unfortunately, contradictory results were reported with one (Cunha et al., 2008) (low quality study) indicating an increase in pain at follow up, and the other (Maluf et al., 2010) whereas the latter (high quality study) did not report this finding. In contrast, two low quality studies making use of a supported stretch position revealed beneficial effects (Hanten et al., 2000; Trampas et al., 2010). It seems likely that this supported position may allow for better stability assuring a better control and application of stretch intensity (Wyon et al., 2009). It should be noted, that though a large number of the studies where of high quality, the focus was whether these studies mentioned intensity and at what level was the intensity of the stretch (i.e., discomfort, pain, gentle).
The elderly population was also concerned with the influence of stretching exercises on ROM. Unlike the other populations, the elderly group did not have participants perform a loaded stretch, possibly anxious about loading an aged muscle. Most of the studies were of high quality. In general, the observed benefits in this population were related to the participants performing a supported stretch or being stretched by a therapist in a supported position (i.e., lying on a plinth). With the muscles and connective tissue in a stable environment, greater control can be imparted on the magnitude of the intensity. This is important since several age-related musculoskeletal and physiological changes such as muscle atrophy, reduced capacity for healing, and loss of strength and elasticity has been associated with the elderly (Feland et al., 2001).
In line with the other groups reported herein, most of the studies in the general population focused on ROM. Referring to a loaded stretch in conjunction with intensity (i.e., discomfort, pain, and MSNP), no definitive trend emerged as to the benefit of this combination. However, studies mentioning stretch intensity during a supported stretch position (machine and/or therapist) did reveal a benefit (Rees et al., 2007; Winke et al., 2010). With use of therapists to stretch participants, greater support of the musculo-tendinous structure could account for the decrease in intensity of the stretch during stretching.
It is noteworthy that although all 152 articles considered duration and frequency, only 79 (51.33%) referred to intensity. Of these 79 articles, only 22 (27.84%) (Medeiros et al., 1977; Smith et al., 1993; McNair and Stanley, 1996; Clark et al., 1999; Muir et al., 1999; de Weijer et al., 2003; Youdas et al., 2003; Zakas et al., 2006; Hayes and Walker, 2007; Horsley et al., 2007; Cristopoliski et al., 2009; Curry et al., 2009; O'sullivan et al., 2009; Rancour et al., 2009; Maluf et al., 2010; Borman et al., 2011; Silveira et al., 2011; Cipriani et al., 2012; Wyon et al., 2013; Wicke et al., 2014; Apostolopoulos et al., 2015a,b) were of high quality [Refer to tables, studies are indicated with an (‡)]. Fifteen of the studies referenced loaded stretch positions with eight having the participants stretch to discomfort (McNair and Stanley, 1996; Hayes and Walker, 2007; Curry et al., 2009; Rancour et al., 2009; Maluf et al., 2010; Silveira et al., 2011; Cipriani et al., 2012; Wicke et al., 2014), one to pain (Smith et al., 1993), five to MSNP (Muir et al., 1999; de Weijer et al., 2003; Youdas et al., 2003; Horsley et al., 2007; Borman et al., 2011), with the last study having participants stretch to a gentle stretch intensity (O'sullivan et al., 2009). One study had participants stretched to pain with use of a therapist (Apostolopoulos et al., 2015a). The majority of the studies referencing discomfort, pain and MSNP presented conflicting results as to whether stretching was beneficial. However, it is interesting to note that the gentle loaded stretch (O'sullivan et al., 2009) compared to the remaining six high quality studies, which referenced supported gentle stretches (Zakas et al., 2006; Wyon et al., 2013), discomfort with use of a therapist (Cristopoliski et al., 2009) or machine (Medeiros et al., 1977; Apostolopoulos et al., 2015b), and a MSNP with a therapist (Clark et al., 1999), all indicated that stretching under these conditions was beneficial. The study by Apostolopoulos et al. (2015b) comparing various stretch intensities based on an individual's maximum ROM (mROM) concluded that stretches between 30 and 60% mROM (gentle stretch intensity) did not cause inflammation, whereas a stretch of 90% mROM (pain) caused inflammation.
A study which had dancers perform either a gentle stretch or a discomfort intense stretch in a supported position; observed for the gentle intense supported stretch produced the greatest gains in terms of increasing active and passive ROM (Wyon et al., 2013). It is likely that the gentle supported stretch position influenced the series and parallel elastic components, and thereby prevented the activation of a stretch reflex. When a relaxed muscle is stretched, the change in length is shared between the series and parallel elastic components (Buller, 1975). In contrast, when a muscle contracts isometrically, the parallel elastic element is unloaded, while the series elastic element is stretched by an amount dependent on the force developed to the muscle. The activation of the series elastic element stimulates the Golgi Tendon Organ, since this is in series with this component (Kandel et al., 2000). The increase in muscle tension during activation may be a by-product of a loaded stretch in conjunction with an intensity level perceived as a discomfort or pain. This indicates the potential importance of the effect of the force generated during stretching exercises, as well as the position assumed by the participant during the actual stretching exercise.
The elongation of passive muscle from short to medium lengths requires little application of force. However, stretching muscle to greater lengths requires a large force (Jespersen, 1950). The force generated during a single intense stretch has been associated with several outcomes: overt skeletal muscle injury (inflammation, myofiber degeneration, and dysfunction), skeletal muscle adaptation (regeneration and growth with functional gains), and/or mal-adaptation (a sub-degenerative or sub-necrotic state that is usually associated with low levels of persistent inflammation and loss of function) (Cutlip et al., 2009). The intensity of the stretch during a stretching exercise has been described as the magnitude of the force, and it has been suggested that if the force applied is too much this may injure the tissue resulting in an inflammatory response (Brand, 1984; McClure et al., 1994). In the study conducted by Light et al. it was observed that use of a low-load prolonged stretch was found to be superior to a high-load brief stretch in treating knee contractures in 11 elderly patients. Therefore, this study may suggest that a low intense passive stretch held at a constant length may lead to a stress relaxation. According to Kubo et al. (2001), a stretch being held at a constant length influences the MTU resulting in a reduction in the stiffness which may be responsible in the increase in the joint ROM. Therefore, the magnitude of the force applied during the stretch may influence acute and chronic ROM.
As previously highlighted, the body's response to this force is to activate components of the immune system which, depending on the severity of the response, may result in significant impairment (Cuthbertson, 1942). Chronic exposure to high force development has been shown to create inflammatory manifestations (Archambault et al., 2001; Stauber and Willems, 2002; Barbe and Barr, 2006). Such mechanical loading, associated with the overstretching of sarcomeres beyond the myofilament overlap, creates a physical disruption of the musculoskeletal fibers, resulting in pain and inflammation (Gregory et al., 2002). In turn, the activated local pathways of the damaged tissue further mediates inflammation and tissue damage (Armstrong et al., 1983; Fridén et al., 1986; Geronilla et al., 2003).
This systematic review reveals that only a few of the published papers in this area of research examined articles addressing the intensity of stretching, even across a variety of population groups. This component of stretching may be linked to increased inflammation in chronic conditions when stretching is used to deal with clinical conditions or improving the ROM of soft and connective tissue in both therapeutic and athletic environments. In addition, due to the lack of good quality studies, it is difficult to draw conclusions about the effects of stretching intensity and/or position on the observed effects of stretching. More research is required concerning the appropriate application of stretching intensity, and the critical role it might play in optimizing musculoskeletal health. What is needed is a high quality study perhaps using a new research paradigm. This study would examine the efficiency of a low intense supported stretch as a means to increasing ROM, without setting off the stretch reflex, while minimizing inflammation.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Abdel-aziem, A. A., Draz, A. H., Mosaad, D. M., and Abdelraou, O. R. (2013). Effect of body position and type of stretching on hamstring flexibility. Int. J. Med. Res. Health Sci. 2, 399–406. doi: 10.5958/j.2319-5886.2.3.070
Aguilar, A. J., DiStefano, L. J., Brown, C. N., Herman, D. C., Guskiewicz, K. M., and Padua, D. A. (2012). A dynamic warm-up model increases quadriceps strength and hamstring flexibility. J. Strength Cond. Res. 26, 1130–1141. doi: 10.1519/JSC.0b013e31822e58b6
Albayrak, I., Ugurlu, H., and Salli, A. (2014). The effectiveness of various physical therapy and rehabilitation modalites in patients developing contracture due to immobilization. J. Phys. Med. Rehabil. Sci. 17, 117–127.
Allison, S., Bailey, D., and Folland, J. (2008). Prolonged static stretching does not influence running economy despite changes in neuromuscular function. J. Sports Sci. 26, 1489–1495. doi: 10.1080/02640410802392715
Almasi, J., Jalalvand, A., and Farokhroo, N. (2014). The effect of PNF stretching and therapeutic massage combination treatment on markers of exercise induced muscle damage. Int. J. Biosci. 4, 217–228. doi: 10.12692/ijb/4.4.217-228
Apostolopoulos, N., Metsios, G. S., Nevill, A., Koutedakis, Y., and Wyon, M. (2015b). Stretch intensity vs inflammation: a dose-dependent association? Int. J. Kinesiol. Sports Sci. 3, 27–31. doi: 10.7575/aiac.ijkss.v.3n.1p.27
Apostolopoulos, N., Metsios, G. S., Taunton, J., Koutedakis, Y., and Wyon, M. (2015a). Acute inflammation response to stretching: a randomised trial. Ital. J. Sports Rehabil. Posturol. 2, 368–381. doi: 10.17385/ItaJSRP.015.3008
Aquino, C. F., Fonseca, S. T., Gonçalves, G. G., Silva, P. L., Ocarino, J. M., and Mancini, M. C. (2010). Stretching versus strength training in lengthened position in subjects with tight hamstring muscles: a randomized controlled trial. Man. Ther. 15, 26–31. doi: 10.1016/j.math.2009.05.006
Archambault, J. M., Hart, D. A., and Herzog, W. (2001). Response of rabbit achilles tendon to chronic repetitive loading. Connect. Tissue Res. 42, 13–23. doi: 10.3109/03008200109014245
Armstrong, R. B., Ogilvie, R. W., and Schwane, J. A. (1983). Eccentric exercise-induced injury to rat skeletal muscle. J. Appl. Physiol. 54, 80–93.
Ayala, F., and de Baranda Andújar, P.S. (2010). Effect of 3 different active stretch durations on hip flexion range of motion. J. Strength Cond. Res. 24, 430–436. doi: 10.1519/JSC.0b013e3181c0674f
Ayala, F., Sainz De Baranda, P., and De Ste Croix, M. (2010). Effect of active stretch on hip flexion range of motion in female futsal players. J. Sports Med. Phys. Fitness. 50, 428–435.
Ayala, F., Sainz de Baranda, P., De Ste Croix, M., and Santonja, F. (2012). Reproducibility and criterion-related validity of the sit and reach test and toe touch test for estimating hamstring flexibility in recreationally active young adults. Phys. Ther. Sport 13, 219–226. doi: 10.1016/j.ptsp.2011.11.001
Azevedo, D. C., Melo, R. M., Alves Corrêa, R. V., and Chalmers, G. (2011). Uninvolved versus target muscle contraction during contract-relax proprioceptive neuromuscular facilitaiton stretching. Phys. Ther. Sport. 12, 117–121. doi: 10.1016/j.ptsp.2011.04.003
Bandy, W. D, Irion J. M., and Briggler, M. (1997). The effect of time and frequency of static stretching on flexibility of the hamstring muscles. Phys. Ther. 77, 1090–1096.
Bandy, W., Irion, J., and Briggler, M. (1998). The effect of static stretch and dynamic range of motion training on the flexibility of the hamstring muscles J. Orthop. Sports Phys. Ther. 27, 295–300. doi: 10.2519/jospt.1998.27.4.295
Bannerman, N., Pentecost, E., Rutter, S., Willoughby, S., and Vujnovich, A. (1996). Increase of soleus muscle length: a comparison between two stretching techniques. N. Z. J. Physiother. 24, 15–18.
Barbe, M. F, Barr, A. E. (2006). Inflammation and the pathophysiology of work-related musculoskeletal disorders. Brain Behav. Immun. 20, 423–429. doi: 10.1016/j.bbi.2006.03.001
Batista, L. H., Vilar, A. C., de Almeida Ferreira, J. J., Rebelatto, J. R., and Salvini, T. F. (2009). Active stretching improves flexibility, joint torque, and functional mobility in older women. Am. J. Phys. Med. Rehabil. 88, 815–822. doi: 10.1097/PHM.0b013e3181b72149
Bazett-Jones, D., Gibson, M., and McBride, J. (2008). Sprint and vertical jump performances are not affected by six weeks of static hamstring stretching. J. Strength Cond. Res. 22, 25–31. doi: 10.1519/JSC.0b013e31815f99a4
Bazett-Jones, D. M., Winchester, J. B., and McBride, J. M. (2005). Effect of potentiation and stretching on maximal force, rate of force development, and range of motion. J. Strength Cond. Res. 19, 421–426. doi: 10.1519/14193.1
Beedle, B. B., Leydig, S. N., and Carnucci, J. M. (2007). No difference in pre-and postexercise stretching on flexibility. J. Strength Cond. Res. 21, 780–783. doi: 10.1519/R-20736.1
Bello, M., Mesiano Maifrino, L. B., Gama, E. F., and Rodrigues de Souza, R. (2011). Rhythmic stabilization versus conventional passive stretching to prevent injuries in indoor soccer athletes: a controlled clinical trial. J. Bodyw. Mov. Ther. 15, 380–383. doi: 10.1016/j.jbmt.2010.11.002
Ben, M., and Harvey, L. (2010). Regular stretch does not increase muscle extensibility: a randomized controlled trial. Scand. J. Med. Sci. Sports. 20, 136–144. doi: 10.1111/j.1600-0838.2009.00926.x
Blazevich, A. J., Cannavan, D., Waugh, C. M., Miller, S. C., Thorlund, J. B., Aagaard, P., et al. (2014). Range of motion, neurochemical, and architectural adaptations to plantar flexor stretch training in humans. J. Appl. Physiol. 117, 452–462. doi: 10.1152/japplphysiol.00204.2014
Blazevich, A., Cannavan, D., Waugh, C., Faith, F., Miller, S., and Kay, A. (2012). Neuromuscular factors influencing the maximum stretch limit of the human plantar flexors. J. Appl. Physiol. 113, 1446–1455. doi: 10.1152/japplphysiol.00882.2012
Bonnar, B. P., Deivert, R. G., and Gould, T. E. (2004). The relationship between isometric contraction durations during hold-relax stretching and improvement of hamstring flexibility. J. Sports Med. Phys. Fitness. 44, 258.
Borman, N. P., Trudelle-Jackson, E., and Smith, S. S. (2011). Effect of stretch positions on hamstring muscle length, lumbar flexion range of motion, and lumbar curvature in healthy adults. Physiother. Theory Pract. 27, 146–154. doi: 10.3109/09593981003703030
Buller, A. (1975). “The physiology of skeletal muscle,” in Neurophysiology, ed C. Hunt (Baltimore, MD: University Park Press), 275–302.
Cabido, C. E. T., Bergamini, J. C., Andrade, A. G. P., Lima, F. V., Menzel, H.-J., and Chagas, M. H. (2014). Acute effect of constant torque and angle stretching on range of motion, muscle passive properties, and stretch discomfort perception. J. Strength Cond. Res. 28, 1050–1057. doi: 10.1519/JSC.0000000000000241
Caplan, N., Rogers, R., Parr, M. K., and Hayes, P. R. (2009). The effect of proprioceptive neuromuscular facilitation and static stretch training on running mechanics. J. Strength Cond. Res. 23, 1175–1180. doi: 10.1519/JSC.0b013e318199d6f6
Chadchavalpanichaya, N., and Srisawasdi, G. (2010). The effect of calf stretching box on stretching calf muscle compliance: a prospective, randomized single-blinded controlled trial. J. Med. Assoc. Thai. 93, 1470–1479.
Chan, S. P., Hong, Y., and Robinson, P. D. (2001). Flexibility and passive resistance of the hamstrings of young adults using two different static stretching protocols. Scand. J. Med. Sci. Sports 11, 81–86. doi: 10.1034/j.1600-0838.2001.011002081.x
Chen, C.-H., Huang, T.-S., Chai, H.-M., Jan, M.-H., and Lin, J.-J. (2013). Two stretching treatments for the hamstrings: proprioceptive neuromuscular facilitation versus kinesio taping. J. Sport Rehabil. 22, 59–66.
Christiansen, C. (2008). The effects of hip and ankle stretching on gait function of older people. Arch. Phys. Med. Rehabil. 89, 1421–1428. doi: 10.1016/j.apmr.2007.12.043
Cipriani, D. J., Terry, M. E., Haines, M. A., Tabibnia, A. P., and Lyssanova, O. (2012). Effect of stretch frequency and sex on the rate of gain and rate of loss in muscle flexibility during a hamstring-stretching program: a randomized single-blind longitudinal study. J. Strength Cond. Res. 26, 2119–2129. doi: 10.1519/JSC.0b013e31823b862a
Clark, S., Christiansen, A., Hellman, D. F., Hugunin, J. W., and Hurst, K. M. (1999). Effects of ipsilateral anterior thigh soft tissue stretching on passive unilateral straight-leg raise. J. Orthop. Sports Phys. Ther. 29, 4–12. doi: 10.2519/jospt.1999.29.1.4
Connolly, D. A. J., Sayers, S. P., and McHugh, M. P. (2003). Treatment and prevention of delayed onset muscle soreness. J. Strength Cond. Res. 17, 197–208. doi: 10.1519/00124278-200302000-00030
Cornelius, W. L., Ebrahim, K., Watson, J., and Hill, D. W. (1992). The effects of cold application and modified PNF stretching techniques on hip joint flexibility in college males. Res. Q. Exerc. Sport 63, 311–314. doi: 10.1080/02701367.1992.10608747
Cornelius, W. L., Jensen, R. L., and Odell, M. E. (1995). Effects of PNF stretching phases on acute arterial blood pressure. Can. J. Appl. Physiol. 20, 222–229. doi: 10.1139/h95-016
Cristopoliski, F., Barela, J. A., Leite, N., Fowler, N. E., and Rodacki, A. L. (2009). Stretching exercise program improves gait in the elderly. Gerontology 55, 614–620. doi: 10.1159/000235863
Cunha, A. C., Burke, T. N., França, F. J., and Marques, A. P. (2008). Effect of global posture re-education and of static stretching on pain, range of motion, and quality of life in women with chronic neck pain: a randomized clinical trial. Clinics 63, 763–770. doi: 10.1590/S1807-59322008000600010
Curry, B., Chengkalath, D., Crouch, G., Romance, M., and Manns, P. (2009). Acute effects of dynamic stretching, static stretching and light aerobic activity on muscular performance in women. J. Strength Cond. Res. 23, 1811–1819. doi: 10.1519/JSC.0b013e3181b73c2b
Cuthbertson, D. (1942). Post-shock metabolic response. Lancet i, 433–437. doi: 10.1016/S0140-6736(00)79605-X
Cutlip, R. G., Baker, B. A., Hollander, M., and Ensey, J. (2009). Injury and adaptive mechanisms in skeletal muscle. J. Electromyogr. Kinesiol. 19, 358–372. doi: 10.1016/j.jelekin.2008.06.007
Davis, D. S., Ashby, P. E., McCale, K. L., McQuain, J. A., and Wine, J. M. (2005). The effectiveness of 3 stretching techniques on hamstring flexibility using consistent stretching parameters. J. Strength Cond. Res. 19, 27–32. doi: 10.1519/14273.1
De Deyne, P. G. (2001). Application of passive stretch and its implications for muscle fibers. Phys. Ther. 81, 819–827.
de Oliveira, A. L., Greco, C. C., and Molina, R. (2012). The rate of force development obtained at early contraction phase is not influenced by active static stretching. J. Strength Cond. Res. 26, 2174–2179. doi: 10.1519/JSC.0b013e31823b0546
de Weijer, V. C., Gorniak, G. C., and Shamus, E. (2003). The effect of static stretch and warm-up exercise on hamstring length over the course of 24 hours. J. Orthop. Sports Phys. Ther. 33, 727–733. doi: 10.2519/jospt.2003.33.12.727
deCarvalho, A. O., Cabral, L., and Rubini, E. (2011). Acupuncture improves flexibility: acute effect of acupuncture before a static stretch of hip adductors. Med. Acupunct. 23, 27–33. doi: 10.1089/acu.2010.0773
Decicco, P., and Fisher, M. (2005). The effect of proprioceptive neuromuscular facilitation stretching on shoulder range of motion in overhand athletes. J. Sports Med. Phys. Fitness. 45, 183.
Decoster, L. C., Cleland, J., Altieri, C., and Russell, P. (2005). The effects of hamstring stretching on range of motion: a systematic review. J. Orthop. Sports Phys. Ther. 35, 377–387. doi: 10.2519/jospt.2005.35.6.377
Decoster, L. C., Scanlon, R. L., Horn, K. D., and Cleland, J. (2004). Standing and supine hamstring stretching are equally effective. J. Athl. Train. 39, 330–334.
Fantini, C. H., Menzel, H.-J., and Chagas, M. H. (2006). “Influence of stretching exercise on performance and movement technique during drop jumps,” in XXIV International Symposium on Biomechanics in Sports (ISBS) Symposium, 2006 (Salzburg, Austria), 671–674.
Fasen, J. M., O'Connor, A. M., Schwartz, S. L., Watson, J. O., Plastaras, C. T., Garvan, C. W., et al. (2009). A randomized controlled trial of hamstring stretching: comparison of four techniques. J. Strength Cond. Res. 23, 660–667. doi: 10.1519/JSC.0b013e318198fbd1
Favero, J. P., Midgley, A. W., and Bentley, D. J. (2009). Effects of an acute bout of static stretching on 40 m sprint performance: influence of baseline flexibility. Res. Sports Med. 17, 50–60. doi: 10.1080/15438620802678529
Feland, J., Myrer, J., Schulthies, S., Fellingham, G., and Measom, G. (2001). The effect of duration of stretching of the hamstring muscle group for increasing range of motion in people aged 65 years or older. Phys. Ther. 81, 1110–1117.
Freitas, S. R., and Mil-Homens, P. (2015). Effect of 8 week high intensity stretching training on biceps femoris architecture. J. Strength Cond. Res. 29, 1737–1740. doi: 10.1519/JSC.0000000000000800
Fridén, J., Sfakianos, P. N., and Hargens, A. R. (1986). Muscle soreness and intramuscular fluid pressure: comparison between eccentric and concentric load. J Appl Physiol. 61, 2175–2179.
Gajdosik, R. L., Vander Linden, D. W., McNair, P. J., Williams, A. K., and Riggin, T. J. (2005). Effects of an eight-week stretching program on the passive-elastic properties and function of the calf muscles of older women. Clin. Biomech. 20, 973–983. doi: 10.1016/j.clinbiomech.2005.05.011
Geronilla, K. B., Miller, G. R., Mowrey, K. F., Wu, J. Z., Kashon, M. L., Brumbaugh, K., et al. (2003). Dynamic force responses of skeletal muscle during stretch-shortenning cycles. Eur. J. Appl. Physiol. 90, 144–153. doi: 10.1007/s00421-003-0849-8
Ghaffarinejad, F., Taghizadeh, S., and Mohammadi, F. (2007). Effect of static stretching of muscles surrounding the knee on knee joint position sense. Br. J. Sports Med. 41, 684–687. doi: 10.1136/bjsm.2006.032425
González-Ravé, J. M., Sánchez-Gómez, A., and Santos-García, D. J. (2012). Efficacy of two different stretch training programs (passive vs. proprioceptive neuromuscular facilitation) on shoulder and hip range of motion in older people. J. Strength Cond. Res. 26, 1045–1051. doi: 10.1519/JSC.0b013e31822dd4dd
Gregory, J. E., Brockett, C. L., Morgan, D. L., Whitehead, N. P., and Proske, U. (2002). Effect of eccentric muscle contractions on Golgi tendon organ responses to passive and active tension in the cat. J. Physiol. 538, 209–218. doi: 10.1113/jphysiol.2001.012785
Gribble, P., Gusklewicz, K., Prentice, W., and Shields, E. (1999). Effects of static and hold-relax stretching on hamstring range of motion using the FlexAbility LE 1000. J. Sports Rehabili. 8, 195–208.
Guissard, N., and Duchateau, J. (2006). Neural aspects of muscle stretching. Exerc. Sport Sci. Rev. 34, 154–158. doi: 10.1249/01.jes.0000240023.30373.eb
Gustafsson, L., and McKenna, K. (2006). A programme of static positional stretches does not reduce hemiplegic shoulder pain or maintain shoulder range of motion-a randomized controlled trial. Clin. Rehabil. 20, 277–286. doi: 10.1191/0269215506cr944oa
Häkkinen, A., Salo, P., Tarvainen, U., Wirén, K., and Ylinen, J. (2007). Effect of manual therapy and stretching on neck muscle strength and mobility in chronic neck pain. J. Rehabil. Med. 39, 575–579. doi: 10.2340/16501977-0094
Halbertsma, J. P., van Bolhuis, A. I., and Goeken, L. N. H. (1996). Sports stretching: effect on passive muscle stiffness of short hamstrings. Arch. Phys. Med. Rehabil. 77, 688–692. doi: 10.1016/S0003-9993(96)90009-X
Halbertsma, J. P., and Göeken, L. N. (1994). Stretching exercises: effect on passive extensibility and stiffness in short hamstrings of healthy subjects. Arch. Phys. Med. Rehabil. 75, 976–981.
Hanten, W. P., Olson, S. L., Butts, N. L., and Nowicki, A. L. (2000). Effectiveness of a home program of ischemic pressure followed by a sustained stretch for treatment of myofascial trigger points. Phys. Ther. 80, 997–1003.
Harvey, L. A., Batty, J., Crosbie, J., Poulter, S., and Herbert, R. D. (2000). A randomized trial assessing the effects of 4 weeks of daily stretching on ankle mobility in patients with spinal cord injuries. Arch. Phys. Med. Rehabil. 81, 1340–1347. doi: 10.1053/apmr.2000.9168
Harvey, L., Byak, A., Ostrovskaya, M., Glinsky, J., Katte, L., and Herbert, R. (2003). Randomized trial of the effects of four weeks of daily stretch on extensibility of hamstring muscles in people with spinal cord injuries. Aust. J. Physiother. 49, 176–181. doi: 10.1016/S0004-9514(14)60237-3
Harvey, L., Herbert, R., and Crosbie, J. (2006). Does stretching induce lasting increases in joint ROM? A systematic review. Phys. Res. Int. 7, 1–13.
Hayes, B. T., Harter, R. A., Widrick, J. J., Williams, D. P., Hoffman, M. A., and Hicks-Little, C. A. (2012). Lack of neuromuscular origins of adaptation after a long-term stretching program. J. Sports Rehabil. 21, 99–106.
Hayes, P., and Walker, A. (2007). Pre-exercise stretching does not impact upon running economy. J. Strength Cond. Res. 21, 1227–1232. doi: 10.1519/R-19545.1
Herbert, R. D., and Gabriel, M. (2002). Effects of stretching before and after exercise on muscle soreness and risk of injury: systematic review. BMJ 325, 1–5. doi: 10.1136/bmj.325.7362.468
Herda, T. J., Costa, P. B., Walter, A. A., Ryan, E. D., and Cramer, J. T. (2012). The time course of the effects of constant-angle and constant-torque stretching on the muscle-tendon unit. Scand. J. Med. Sci. Sports 24, 62–67. doi: 10.1111/j.1600-0838.2012.01492.x
Herman, S. L., and Smith, D. T. (2008). Four-week dynamic stretching warm-up intervention elicits longer-term performance benefits. J. Strength Cond. Res. 22, 1286–1297. doi: 10.1519/JSC.0b013e318173da50
Horsley, S. A., Herbert, R. D., and Ada, L. (2007). Four weeks of daily stretch has little or no effect on wrist contracture after stroke: a randomised controlled trial. Aust. J. Physiother. 53, 239–245. doi: 10.1016/S0004-9514(07)70004-1
Hortobágyi, T., Faludi, J., Tihanyi, J., and Merkely, B. (1985). Effects of intense stretching flexibility training on the mechanical profile of the knee extensors and on the range of motion of the hip joint. Int. J. Sports Med. 6, 317–321. doi: 10.1055/s-2008-1025862
Jacobs, C. A., and Sciascia, A. D. (2011). Factors that influence the efficacy of stretchng programs for patients with hypomobility. Sports Health 3, 520–523. doi: 10.1177/1941738111415233
Jadad, A. R., Moore, R. A., Carroll, D., Jenkinson, C., Reynolds, D. J., Gavaghan, D. J., et al. (1996). Assessing the quality of reports of randomized clinical trials: is blinding necessary. Control. Clin. Trials 17, 1–12. doi: 10.1016/0197-2456(95)00134-4
Johanson, M., Baer, J., Hovermale, H., and Phouthavong, P. (2008). Subtalar joint position during gastrocnemius stretching and ankle dorsiflexion range of motion. J. Athl. Train. 43, 172–178. doi: 10.4085/1062-6050-43.2.172
Johanson, M. A., Cuda, B. J., Koontz, J. E., Stell, J. C., and Abelew, T. A. (2009). Effect of stretching on ankle and knee angles and gastrocnemius activity during the stance phase of gait. J Sports Rehabili. 18, 521–534.
Johanson, M., Wooden, M., Catlin, P., Hemard, L., Lott, K., Romalino, R., et al. (2006). Effects of gastrocnemius stretching on ankle dorsiflexion and time-to heel-off during the stance phase of gait. Phys. Ther. Sport. 7, 93–100. doi: 10.1016/j.ptsp.2006.02.002
Johansson, P. H., Lindström, L., Sundelin, G., and Lindström, B. (1999). The effects of preexercise stretching on muscular soreness, tenderness and force loss following heavy eccentric exercise. Scand. J. Med. Sci. Sports. 9, 219–225. doi: 10.1111/j.1600-0838.1999.tb00237.x
Jung, D.-Y., Koh, E.-K., Kwon, O.-Y., Yi, C.-H., Oh, J.-S., and Weon, J.-H. (2009). Effect of medial arch support on displacement of the myotendinous junction of the gastrocnemius during standing wall stretching. J. Orthop. Sports Phys. Ther. 39, 867–874. doi: 10.2519/jospt.2009.3158
Kandel, E., Schwartz, J., and Jessell, T. (eds.). (2000). Principles of Neural Science, 4th Edn. New York, NY: McGraw-Hill.
Kasser, R. J., Pridmore, K., Hoctor, K., Loyd, L., and Wortman, A. (2009). Comparison of stretching versus strengthening for increasing active ankle dorsiflexion range of motion. Top. Geriatr. Rehabil. 25, 211–221. doi: 10.1097/TGR.0b013e3181b02d4a
Kay, A. D., and Blazevich, A. J. (2012). Effect of acute static stretch on maximal muscle performance: a systematic review. Med. Sci. Sports Exerc. 44, 154–164. doi: 10.1249/MSS.0b013e318225cb27
Kerrigan, D. C., Xenopoulos-Oddsson, A., Sullivan, M. J., Lelas, J. J., and Riley, P. O. (2003). Effect of a hip flexor-stretching program on gait in the elderly. Arch. Phys. Med. Rehabil. 84, 1–6. doi: 10.1053/apmr.2003.50056
Kidd, B. L., and Urban, L. A. (2001). Mechanisms of inflammatory pain. Br. J. Anaesth. 87, 3–11. doi: 10.1093/bja/87.1.3
Kilbreath, S., Refshauge, K., Beith, J., Ward, L., Simpson, J., and Hansen, R. (2012). Upper limb progressive resistance training and stretching exercises following surgery for early breast cancer: a randomized controlled trial. Breast Cancer Res. Treat. 113, 667–676. doi: 10.1007/s10549-012-1964-1
Kim, T. H., Yoon, J. S., and Lee, J. H. (2013). The effect of ankle joint muscle strengthening training and static muscle stretching training on stroke patients' C.O.P sway amplitude. J. Phys. Ther. Sci. 25, 1613–1616. doi: 10.1589/jpts.25.1613
Kjaer, M. (2004). Role of extracellular matrix in adaptation of tendon and skeletal muscle to mechanical loading. Physiol. Rev. 84, 649–698. doi: 10.1152/physrev.00031.2003
Klinge, K., Magnusson, S. P., Simonsen, E. B., Aagaard, P., Klausen, K., and Kjaer, M. (1997). The effect of strength and flexibility training on skeletal muscle electromyographic activity, stiffness, and viscoelastic stress relaxation response. Am. J. Sports Med. 25, 710–716. doi: 10.1177/036354659702500522
Knudson, D. (1999). Stretching during warm-up: do we have enough evidence? J. Phys. Educ. Recreation Dance 70, 24–27. doi: 10.1080/07303084.1999.10605682
Kokkonen, J., Nelson, A. G., and Cornwell, A. (1998). Acute muscle stretching inhibits maximal strength performance. Res. Q. Exerc. Sport. 69, 411–415. doi: 10.1080/02701367.1998.10607716
Konrad, A., and Tilp, M. (2014). Increased range of motion after static stretching is not due to changes in muscle and tendon structures. Clin. Biomech. 29, 636–642. doi: 10.1016/j.clinbiomech.2014.04.013
Krityakiarana, W., Budworn, J., Khajohnanan, C., Suramas, N., and Puritasang, W. (2014). Effect lof ice bad, dynamic stretchng and combined treatments on the prevention and treatmetn of delayed onset muscle soreness. Int. J. Physiother. Res. 2, 799–805. doi: 10.16965/ijpr.2014.696
Kubo, K., Kanehisa, H., Kawakami, Y., and Fukunaga, T. (2001). Influence of static stretching on viscoelastic properties of human tendon structures in vivo. J. Appl. Physiol. 90, 520–527.
LaRoche, D. (2006). Effects of stretching on passive muscle tension and response to eccentric exercise. Am. J. Sports Med. 34, 1000–1007. doi: 10.1177/0363546505284238
Larsen, R., Lund, H., Christensen, R., Røgind, H., Danneskiold-Samsøe, B., and Bliddal, H. (2005). Effect of static stretching of quadriceps and hamstring muscles on knee joint position sense. Br. J. Sports Med. 39, 43–46. doi: 10.1136/bjsm.2003.011056
Law, R. Y., Harvey, L. A., Nicholas, M. K., Tonkin, L., De Sousa, M., and Finniss, D. G. (2009). Stretch exercises increase tolerance to stretch in patients with chronic musculoskeletal pain: a randomized controlled trial. Phys. Ther. 89, 1016–1026. doi: 10.2522/ptj.20090056
Lee, T. S., Kilbreath, S. L., Refshauge, K. M., Pendlebury, S. C., Beith, J. M., and Lee, M. J. (2007). Pectoral stretching program for women undergoing radiotherapy for breast cancer. Breast Cancer Res. Treat. 102, 313–321. doi: 10.1007/s10549-006-9339-0
Light, K. E., Nuzik, S., Personius, W., and Barstrom, A. (1984). Low-load prolonged stretch vs high-load brief stretch in treating knee contractures. Phys. Ther. 64, 330–333.
Locks, R. R., Costa, T. C., Koppe, S., Yamaguti, A. M., Garcia, M. C., and Gomes, A. R. S. (2012). Effects of strength and flexibility training on functional performance of healthy older people. Rev. Bras. Fisioter. 16, 184–190. doi: 10.1590/S1413-35552012000300003
Ma, C., Wu, S., Li, G., Xiao, X., Mai, M., and Yan, T. (2010). Comparison of miniscalpel-needle release, acupuncture needling and stretching exercise to trigger point in myofascial pain syndrome. Clin. J. Pain. 26, 251–257. doi: 10.1097/AJP.0b013e3181b8cdc8
MacIntyre, D., Reid, W., and McKenzie, D. (1995). Delayed onset muscle soreness: the inflammatory response to muscle injury and its clinical implications. Sports Med. 20, 24–40. doi: 10.2165/00007256-199520010-00003
Maenhout, A., Van Eessel, V., Van Dyck, L., Vanraes, A., and Cools, A. (2012). Quantifying acromioclavicular distance in overhead athletes with glenohumeral internal rotation loss and the influence of a stretching program. Am. J. Sports Med. 40, 2105–2112. doi: 10.1177/0363546512454530
Magnusson, S. P., Simonsen, E. B., Aagaard, P., Gleim, G. W., McHugh, M. P., and Kjaer, M. (1995). Viscoelastic responses to repeated static stretching in human skeletal muscle. Scand. J. Med. Sci. Sports. 5, 342–347. doi: 10.1111/j.1600-0838.1995.tb00056.x
Magnusson, S., Aagaard, P., Simonsens, E., and Bojsen-Møller, F. (1998). A biomechanical evaluation of cyclic and static stretch in human skeletal muscle. Int. J. Sports Med. 19, 310–316. doi: 10.1055/s-2007-971923
Magnusson, S., Simonsen, E., Aagaard, P., Dyhre-Poulosen, P., McHugh, M., and Kjaer, M. (1996). Mechanical and physiological responses to stretching with and without preisometric contraction in human skeletal muscle. Arch. Phys. Med. Rehabil. 77, 373–378. doi: 10.1016/S0003-9993(96)90087-8
Mahieu, N. N., Cools, A., De Wilde, B., Boon, M., and Witvrouw, E. (2009). Effect of proprioceptive neuromuscular facilitation stretching on the plantar flexor muscle-tendon tissue properties. Scand. J. Med. Sci. Sports 19, 553–560. doi: 10.1111/j.1600-0838.2008.00815.x
Mahieu, N. N., McNair, P., DeMuynck, M., Stevens, V., Blanckaert, I., Smits, N., et al. (2007). Effect of static and ballistic stretching on the muscle-tendon tissue properties. Med. Sci. Sport Exerc. 39, 494–501. doi: 10.1249/01.mss.0000247004.40212.f7
Maluf, S., Moreno, B., Crivello, O., Cabral, C., Bortolotti, G., and Marques, A. (2010). Global postural re-education and static stretching exercises in the treatment of myogenic temporomandibular disorders: a randomized study. J. Manipulative Physiol. Ther. 33, 500. doi: 10.1016/j.jmpt.2010.08.005
Marschall, F. (1999). Wie beinflussen unterschiedliche Dehnintensitaten kurzfristig die Veranderung der Bewegungsreichweite? (Effects of different stretch-intensity on the acute change of range of motion). Dtsch. Z. Sportmed. 50, 5–9.
Martins, W. R., Carvalho, M. M., Mota, M. R., Cipriano, G. F. B., Mendes, F. A. S., Diniz, L. R., et al. (2013). Diacutaneous fibrolysis versus passive stretching after articular immobilisation: muscle recovery and extracellular matrix remodelling. OA Med. Hypothesis 1, 17–22. doi: 10.13172/2053-0781-1-2-1023
Maynard, V., Bakheit, A. M., and Shaw, S. (2005). Comparison of the impact of a single session of isokinetic or isotonic muscle stretch on gait in patients with spastic hemiparesis. Clin. Rehabil. 19, 146–154. doi: 10.1191/0269215505cr853oa
McBride, J. M., Deane, R., and Nimphius, S. (2007). Effect of stretching on agonist-antagonist muscle activity and muscle force output during single and multiple joint isometric contractions. Scand. J. Med. Sci. Sports. 17, 54–60. doi: 10.1111/j.1600-0838.2005.00495.x
McCarthy, P., Olsen, J., and Smeby, I. (1997). Effects of contract-relax stretching procedures on active range of motion of the cervical spine in the transverse plane - a brief report. Clin. Biomech. 12, 136–138. doi: 10.1016/S0268-0033(96)00060-5
McClure, P., Balaicuis, J., Heiland, D., Broersma, M. E., Thorndike, C. K., and Wood, A. (2007). A randomized controlled comparison of stretching procedures for posterior shoulder tightness. J. Orthop. Sports Phys. Ther. 37, 108–114. doi: 10.2519/jospt.2007.2337
McClure, P. W., Blackburn, L. G., and Dusold, C. (1994). The use of splints in the treatment of joint stiffness: biologic rationale and an algorithm for making clinical decisions. Phys. Ther. 74, 1101–1107.
McGrath, R. P., Whitehead, J. R., and Caine, D. J. (2014). The effects of proprioceptive neuromuscular facilitation stretching on post-exercise delayed onset muscle soreness in young adults. Int. J. Exerc. Sci. 7, 14–21.
McNair, P. J., and Stanley, S. N. (1996). Effect of passive stretching and jogging on the series elastic muscle stiffness and range of motion of the ankle joint. Br. J. Sports Med. 30, 313–318. doi: 10.1136/bjsm.30.4.313
McNair, P. J, Dombroski, E. W., Hewson, D. J., and Stanley, S. N. (2000). Stretching at the ankle joint: viscoelastic responses to holds and continuous passive motion. Med. Sci. Sport Exerc. 33, 354–358. doi: 10.1097/00005768-200103000-00003
Medeiros, J. M., Smidt, G. L., Burmeister, L. F., and Soderberg, G. L. (1977). The influence of isometric exercise and passive stretch on hip joint motion. Phys. Ther. 57, 518–523.
Méndez-Sánchez, R., Alburquerque-Sendín, F., Fernández-de-las-Peñas, C., Barbero-Iglesias, F. J., Sánchez-Sánchez, C., Calvo-Arenillas, J. I., and Huijbregts, P. (2009). Immediate effects of adding a sciatic nerve slider technique on lumber and lower quadrant mobility in soccer players: a pilot study. J. Altern. Compliment. Med. 16, 669–675. doi: 10.1089/acm.2009.0403
Meroni, R., Cerri, C., Lanzarini, C. G., Barindelli, G., Morte, G. D., Gessaga, V., et al. (2010). Comparison of active stretching technique and static stretching on hamstring flexibility. Clin. J. Sport Med. 20, 8–14. doi: 10.1097/JSM.0b013e3181c96722
Minshull, C., Eston, R., Bailey, A., Rees, D., and Gleeson, N. (2014). The differential effects of PNF versus passive stretch conditioning on neuromuscular performance. Eur. J. Sport Sci. 14, 233–241. doi: 10.1080/17461391.2013.799716
Mizuno, T., Matsumoto, M., and Umemura, Y. (2012). Decrements in stiffness are restored within 10 min. Int. J. Sports Med. 36, 484–490. doi: 10.1055/s-0032-1327655
Möller, M. H., Oberg, B. E., and Gilquist, J. (1985). Stretching exercise and soccer: effect of stretching on range of motion in the lower extremity in connection with soccer training. Int. J. Sports Med. 6, 50–52. doi: 10.1055/s-2008-1025813
Morais de Oliveira, A. L., Greco, C. C., Molina, R., and Denadai, B. S. (2012). The rate of force development obtained at early contraction phase is not influenced by active static stretching. J. Strength Cond. Res. 26, 2174–2179. doi: 10.1519/JSC.0b013e31823b0546
Moreside, J. M., and McGill, S. M. (2012). Hip joint range of motion improvements using three different interventions. J. Strength Cond. Res. 26, 1265–1273. doi: 10.1519/JSC.0b013e31824f2351
Morrin, N., and Redding, E. (2013). Acute effects of warm-up stretch protocols on balance, vertical jump height, and range of motion in dancers. J. Dance Med. Sci. 17, 34–40. doi: 10.12678/1089-313X.17.1.34
Moseley, A. M., Herbert, R. D., Nightingale, E. J., Taylor, D. A., Evans, T. M., Robertson, G. J., et al. (2005). Passive stretching does not enhance outcomes in patients with plantarflexion contracture after cast immobilization for ankle fracture: a randomized controlled trial. Arch. Phys. Med. Rehabil. 86, 1118–1126. doi: 10.1016/j.apmr.2004.11.017
Muanjai, P., and Namsawang, J. (2015). Effects of stretching and cold-water immersion on fucntional signs of muscle soreness follwoing plyometric training. J. Phys. Educ. Sport 15, 128–135. doi: 10.7752/jpes.2015.01021
Muir, I. W., Chesworth, B. M., and Vandervoort, A. A. (1999). Effect of a static calf-stretching exercise on the resistive torque during passive ankle dorsiflexion in healthy subjects. J. Orthop. Sports Phys. Ther. 29, 106–115. doi: 10.2519/jospt.1999.29.2.106
Murphy, J. R., Di Santo, M. C., Alkanani, T., and Behm, D. G. (2010). Aerobic activity before and following short-duration static stretching improves range of motion and performance vs. a traditional warm-up. Appl. Physiol. Nutr. Metab. 35, 679–690. doi: 10.1139/H10-062
Nakamura, M., Ikezoe, T., Takeno, Y., and Ichihashi, N. (2012). Effects of a 4-week static stretch training program on passive stiffness of human gastrocnemius muscle-tendon unit in vivo. Eur. J. Appl. Physiol. 112, 2749–2755. doi: 10.1007/s00421-011-2250-3
Nikolaou, P. K., Macdonald, B. L., Glisson, R. R., Seaber, A. V., and Garrett, W. E. Jr. (1987). Biomechanical and histological evaluation of muscle after controlled strain injury. Am. J. Sports Med. 15, 9–14. doi: 10.1177/036354658701500102
Nosaka, K., Newton, M., and Sacco, P. (2002). Delayed-onset msucle soreness does not reflect the magnitude of eccentric exercise-induced muscle damage. Scand. J. Med. Sci. Sports 12, 337–346. doi: 10.1034/j.1600-0838.2002.10178.x
O'Hora, J., Cartwright, A., Wade, C. D., Hough, A. D., and Shum, G. L. (2011). Efficacy on static stretching and proprioceptive neuromuscular facilitation stretch on hamstrings length after a single session. J. Strength Cond. Res. 25, 1586–1591. doi: 10.1519/JSC.0b013e3181df7f98
O'Sullivan, K., Murray, E., and Sainsbury, D. (2009). The effect of warm-up static stretching and dynamic stretching on hamstring flexibility in previously injured subjects. BMC Musculoskelet. Disord. 10:37. doi: 10.1186/1471-2474-10-37
Place, N., Blum, Y., Armand, S., Maffiuletti, N. A., and Behm, D. G. (2012). Effects of a short proprioceptive neuromuscular facilitation stretching bout on quadriceps neuromuscular function, flexibility and vertical jump performance. J. Strength Cond. Res. 27, 463–470. doi: 10.1519/JSC.0b013e3182576ffe
Proske, U., and Gandevia, S. (2012). The proprioceptive sense: thier roles in signaling body shape, body position and movement, and muscle force. Physiol. Rev. 92, 1651–1697. doi: 10.1152/physrev.00048.2011
Puentedura, E. J., Huijbregts, P. A., Celeste, S., Edwards, D., In, A., Landers, M. R., et al. (2011). Immediate effects of quantified hamstring stretching: hold-relax proprioceptive neuromuscular facilitation versus static stretching. Phys. Ther. Sport. 12, 122–126. doi: 10.1016/j.ptsp.2011.02.006
Putt, M. T., Watson, M., Seale, H., and Paratz, J. D. (2008). Muscle stretching technique increases vital capacity and range of motion in patients with chronic obstructve pulmonary disease. Arch. Phys. Med. Rehabil. 89, 1103–1107. doi: 10.1016/j.apmr.2007.11.033
Rancour, J., Holmes, C. F., and Cipriani, D. J. (2009). The effects of intermittent stretching following a 4-week static stretching protocol: a randomized trial. J. Strength Cond. Res. 23, 2217–2222. doi: 10.1519/JSC.0b013e3181b869c7
Rees, S., Murphy, A., Watsford, M., McLachlan, K., and Coutts, A. (2007). Effects of proprioceptive neuromuscular facilitation stretching on stiffness and force-producing characterisitics of the ankle of inactive women. J. Strength Cond. Res. 21, 572–577. doi: 10.1519/R-20175.1
Renan-Ordine, R., Alburquerque-Sendín, F., de Souza, D. P., Cleland, J. A., and Fernández-de-Las-Peǹas, C. (2011). Effectiveness of myofascial trigger point manual therapy combined with a self-stretching protocol for the management of plantar heel pain: a randomized controlled trial. J. Orthop. Sports Phys. Ther. 41, 43–50. doi: 10.2519/jospt.2011.3504
Roberts, J. M., and Wilson, K. (1999). Effect of stretching duration on active and passive range of motion in the lower extremity. Br. J. Sports Med. 33, 259–263. doi: 10.1136/bjsm.33.4.259
Rodenburg, J. B., Steenbeek, D., Schiereck, P., and Bär, P. R. (1994). Warm-up, stretching and massage diminish harmful effects of eccentric exercise. Int. J. Sports Med. 15, 414–419. doi: 10.1055/s-2007-1021080
Ross, M. (2007). Effect of a 15-day pragmatic hamstring stretching program on hamstring flexibility and single hop for distance test performance. Res. Sports Med. 15, 271–281. doi: 10.1080/15438620701693298
Rowlands, A. V., Marginson, V. F., and Lee, J. (2003). Chronic flexibility gains: effect of isometric contraction duration during proprioceptive neuromuscular facilitation stretching techniques. Res. Q. Exerc. Sport 74, 47–51. doi: 10.1080/02701367.2003.10609063
Rubini, E. C., Costa, A. L. L., and Gomes, P. S. C. (2007). The effects of stretching on strength performance. Sports Med. 37, 213–224. doi: 10.2165/00007256-200737030-00003
Ryan, E. D., Beck, T. W., Herda, T. J., Hull, H. R., Hartman, M. J., Costa, P. B., et al. (2008b). The time course of musculotendinous stiffness responses following different durations of passive stretching. J. Orthop. Sports Phys. Ther. 38, 632–639. doi: 10.2519/jospt.2008.2843
Ryan, E. D., Beck, T. W., Herda, T. J., Hull, H. R., Hartman, M. J., Stout, J. R., et al. (2008a). Do practical durations of stretching alter muscle strength? a dose-response study. Med. Sci. Sport Exerc. 40, 1529–1537. doi: 10.1249/MSS.0b013e31817242eb
Sady, S., Wortman, M., and Blanke, D. (1982). Flexibility training: ballistic, static or proprioceptive neuromusculaar facilitation? Arch. Phys. Med. Rehabil. 63, 261–263.
Sainz de Baranda, P., and Ayala, F. (2010). Chronic flexibility improvements after 12 week of stretching program utilizing the ACSM recommendations: hamstring flexibility. Int. J. Sports Med. 31, 389–396. doi: 10.1055/s-0030-1249082
Salameh, A., and Dhein, S. (2013). Effects of mechanical forces and stretch on intercellular gap junction coupling. Biochim. Biophys. Acta. 1828, 147–156. doi: 10.1016/j.bbamem.2011.12.030
Shellock, F. G., and Prentice, W. E. (1985). Waring-up and stretching for improved physical performance and prevention of sports-related injuries. Sports Med. 2, 267–278. doi: 10.2165/00007256-198502040-00004
Shrier, I. (2004). Does stretching improve performance? A systematic and critical review of the literature. Clin. J. Sport Med. 14, 267–273. doi: 10.1097/00042752-200409000-00004
Silveira, G., Sayers, M., and Waddington, G. (2011). Effect of dynamic versus static stretching in the warm-up on hamstring flexibility. Sport J. 14, 1–8.
Smith, L. L. (1991). Acute inflammation: the underlying mechanism in delayed onset muscle soreness? Med. Sci. Sports Exerc. 23, 542–551. doi: 10.1249/00005768-199105000-00006
Smith, L. L., Brunetz, M. H., Chenier, T. C., McCammon, M. R., Houmard, J. A., Franklin, M. E., et al. (1993). The effects of static and ballistic stretching on delayed onset muscle soreness and creatine kinase. Res. Q. Exerc. Sport. 64, 103–107. doi: 10.1080/02701367.1993.10608784
Stanziano, D. C., Roos, B. A., Perry, A. C., Lai, S., and Signorile, J. F. (2009). The effects of an active-assisted stretching program on functional performance in elderly persons: a pilot study. Clin. Interv. Aging. 4, 115–120.
Starring, D. T., Gossman, M. R., Nicholson, G. G. Jr., and Lemons, J. (1988). Comparison of cyclic and sustained passive stretching using a mechanical device to increase resting length of hamstring muscles. Phys. Ther. 68, 314–320.
Stauber, W. T., and Willems, M. E. (2002). Prevention of histopahtologic changes from 30 repeated stretches of active rat skeletal muscles by long inter-stretch rest times. Eur. J. Appl. Physiol. 88, 94–99. doi: 10.1007/s00421-002-0672-7
Taylor, D. C., Dalton, J. D., Seaber, A. V., and Garrett, W. E. (1990). Viscoelastic properties of muscle-tendon units. Ther biomechanical effects of stretching. Am. J. Sports Med. 18, 300–309. doi: 10.1177/036354659001800314
Thacker, S. B., Gilchrist, J., Stroup, D. F., and Kimsey, C. D. Jr. (2004). The impact of stretching on sports injury risk: a systematic review of the literature. Med. Sci. Sports Exerc. 36, 371–378. doi: 10.1249/01.MSS.0000117134.83018.F7
Torres, E. M., Kraemer, W. J., Vingren, J. L., Volek, J. S., Hatfield, D. L., Spiering, B. A., et al. (2008). Effects of stretching on upper-body muscular performance. J. Strength Cond. Res. 22, 1279–1285. doi: 10.1519/JSC.0b013e31816eb501
Torres, R., Appell, H. J., and Duarte, J. A. (2007). Acute effects of stretching on muscle stiffness after a bout of exhaustive eccentric exercise. Int. J. Sports Med. 28, 590–594. doi: 10.1055/s-2007-964865
Trampas, A., Kitsios, A., Sykaras, E., Symeonidis, S., and Lazarou, L. (2010). Clincial massage and modified proprioceptive neuromuscular facilitation stretching in males with latent myofascial trigger points. Phys. Ther. Sport. 11, 91–98. doi: 10.1016/j.ptsp.2010.02.003
Triandafilou, K. M., Ochoa, J., Kang, X., Fischer, H. C., Stoykov, M. E., and Kamper, D. G. (2011). Transient impact of prolonged versus repetitive stretch on hand motor control in chronic stroke. Top. Stroke Rehabil. 18, 316–324. doi: 10.1310/tsr1804-316
Tsolakis, C., Douvis, A., Tsigganos, G., Zacharogiannis, E., and Smirniotou, A. (2010). Acute effects of stretching on flexibility, power and sport specific performance in fencers. J. Hum. Kinet. 26, 105–114. doi: 10.2478/v10078-010-0054-x
Turton, A., and Britton, E. (2005). A pilot randomized controlled trial of a daily muscle stretching regime to prevent contractures in the arm after stroke. Clin. Rehabil. 19, 600–612. doi: 10.1191/0269215505cr891oa
Volpato, C. P., Added, M. A. N., de Paula, X., Richter, G. C., Tanaka, V., de Carvalho, N. A. A., et al. (2014). Influence of stretching and strengthening of the iliopsoas associated with lumbar segmental stabilization exercises in patients with low back pain: the pilot study. J. Exerc. Sports Orthop. 1, 1–5.
Wang, H.-K., Ting-Fang Shih, T., Lin, K.-H., and Wang, T.-G. (2008). Real-time morphologic changes of the iliotibial band during therapeutic stretching;an ultrasonographic study. Man. Ther. 13, 334–340. doi: 10.1016/j.math.2007.03.002
Watt, J. R., Jackson, K., Franz, J. R., Dicharry, J., Evans, J., and Kerrigan, D. C. (2011a). Effect of a supervised hip flexor stretching program on gait in elderly individuals. PM R 3, 324–329. doi: 10.1016/j.pmrj.2010.11.012
Watt, J. R., Jackson, K., Franz, J. R., Dicharry, J., Evans, J., and Kerrigan, D. C. (2011b). Effect of a supervised hip flexor stretching program on gait in frail elderly patients. PM R 3, 330–335. doi: 10.1016/j.pmrj.2011.01.006
Webright, W. G., Randolph, B. J., and Perrin, D. (1997). Comparison of nonballistic active knee extension in neural slump position and static stretch techniques on hamstring flexibility. J. Orthop. Sports Phys. Ther. 26, 7–13. doi: 10.2519/jospt.1997.26.1.7
Weerapong, P., Hume, P., and Kolt, G. (2004). Stretching: mechanisms and benefits for sport performance and injury performance. Phys. Ther. Rev. 9, 189–206. doi: 10.1179/108331904225007078
Weng, M.-C., Lee, C.-L., Chen, C.-H., Hsu, J.-J., Lee, W.-D., Huang, M.-H., et al. (2009). Effects of different stretching techniques on the outcomes of isokinetic exercise in patients with knee osteoarthritis. Kaohsiung J. Med. Sci. 25, 306–315. doi: 10.1016/S1607-551X(09)70521-2
Wessel, J., and Wan, A. (1994). Effect of stretching on the intensity of delayed-onset muscle soreness. Clin. J. Sport Med. 4, 83–87. doi: 10.1097/00042752-199404000-00003
Wicke, J., Gainey, K., and Figueroa, M. (2014). A Comparison of self-administered proprioceptive neuromuscular facilitation to static stretching on range of motion and flexibility. J. Strength Cond. Res. 28, 168–172. doi: 10.1519/JSC.0b013e3182956432
Wiemann, K., and Hahn, K. (1997). Influences of strength, stretching and circulatory exercises on flexibility parameters of the human hamstrings. Int. J. Sports Med. 18, 340–346. doi: 10.1055/s-2007-972643
Wilson, G. J., Wood, G. A., and Elliot, B. C. (1991). The relationship between stiffness of the musculature and static flexibility: an alternative explanation for the occurrence of muscular injury. Int. J. Sports Med. 12, 403–407. doi: 10.1055/s-2007-1024702
Winke, M., Jones, N., Berger, C., and Yates, J. (2010). Moderate static stretching and torque production of the knee flexors. J. Strength Cond. Res. 24, 706–710. doi: 10.1519/JSC.0b013e3181c7c557
Winters, M., Blake, C., Trost, J., Marcello-Brinker, T., Lowe, L., Garber, M., et al. (2004). Passive versus active stretching of hip flexor muscles in subjects with limited hip extension: a randomized clinical trial. Phys. Ther. 84, 800–807.
Wyon, M., Felton, L., and Galloway, S. (2009). A comparison of 2 stretching modalities on lower-limb range of motion measurements in recreational dancers. J. Strength Cond. Res. 23, 2144–2148. doi: 10.1519/JSC.0b013e3181b3e198
Wyon, M. A., Smith, A., and Koutedakis, Y. (2013). A comparison of strength and stretch interventions on active and passive ranges of movement in dancers: a randomized controlled trial. J. Strength Cond. Res. 27, 3053–3059. doi: 10.1519/JSC.0b013e31828a4842
Youdas, J. W., McLean, T. J., Krause, D. A., and Hollman, J. H. (2009). Changes in active ankle dorsiflexion range of motion after acute inversion ankle sprain. J. Sport Rehabil. 18, 358–374.
Youdas, J., Haeflinger, K., Kreun, M., Holloway, A., Kramer, C., and Hollman, J. (2010). The efficacy of two modified proprioceptive neuromuscular facilitation stretching techniques in subjects with reduce hamstring length. Phys. Theory Pract. 26, 240–250. doi: 10.3109/09593980903015292
Youdas, J. W., Krause, D. A., Egan, K. S., Therneau, T. M., and Laskowski, E. R. (2003). The effect of static stretching of the calf muscle-tendon unit on active ankle dorsiflexion range of motion. J. Orthop. Sports Phys. Ther. 33, 408–417. doi: 10.2519/jospt.2003.33.7.408
Yuktasir, B., and Kaya, F. (2007). Investigation into the long-term effects of static and PNF stretching exercises on range of motion and jump performance. J. Bodyw. Mov. Ther. 13, 11–21. doi: 10.1016/j.jbmt.2007.10.001
Zakas, A., Doganis, G., Zakas, N., and Vergou, A. (2006). Acute effects of active warm-up and stretching on the flexibility of elderly women. J. Sports Med. Phys. Fitness 46, 617–622.
Keywords: stretching, intensity, inflammation, performance, injury, rehabilitation
Citation: Apostolopoulos N, Metsios GS, Flouris AD, Koutedakis Y and Wyon MA (2015) The relevance of stretch intensity and position—a systematic review Front. Psychol. 6:1128. doi: 10.3389/fpsyg.2015.01128
Received: 15 March 2015; Accepted: 20 July 2015;
Published: 18 August 2015.
Edited by:
Emma Redding, Trinity Laban Conservatoire of Music and Dance, UKReviewed by:
Marco Barbero, University of Applied Sciences and Arts of Southern Switzerland - SUPSI, SwitzerlandCopyright © 2015 Apostolopoulos, Metsios, Flouris, Koutedakis and Wyon. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Matthew A. Wyon, Research Centre for Sport, Exercise and Performance, Institute of Sport, University of Wolverhampton, Gorway Rd., Walsall, WS1 3BD, UK,bS53eW9uQHdsdi5hYy51aw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.