 Spyridon Kontaxis1,2*Estela Laporta1,2Esther Garcia2,3Ana Isabel Guerrero4Ana Zabalza4Martinis Matteo5Roselli Lucia5Sara Simblett6Janice Weyer7Matthew Hotopf6Vaibhav A. Narayan8Zulqarnain Rashid9Amos A. Folarin9,10Richard J. B. Dobson9,10Mathias Due Buron11Letizia Leocani5Nicholas Cummins9Srinivasan Vairavan8Gloria Dalla Costa5Melinda Magyari11Per Soelberg Sørensen11Carlos Nos4Raquel Bailón1,2Giancarlo Comi5,12 the RADAR-CNS Consortium13
Spyridon Kontaxis1,2*Estela Laporta1,2Esther Garcia2,3Ana Isabel Guerrero4Ana Zabalza4Martinis Matteo5Roselli Lucia5Sara Simblett6Janice Weyer7Matthew Hotopf6Vaibhav A. Narayan8Zulqarnain Rashid9Amos A. Folarin9,10Richard J. B. Dobson9,10Mathias Due Buron11Letizia Leocani5Nicholas Cummins9Srinivasan Vairavan8Gloria Dalla Costa5Melinda Magyari11Per Soelberg Sørensen11Carlos Nos4Raquel Bailón1,2Giancarlo Comi5,12 the RADAR-CNS Consortium13- 1Laboratory of Biomedical Signal Interpretation and Computational Simulation (BSICoS), University of Zaragoza, Zaragoza, Spain
- 2Biomedical Research Networking Center in Bioengineering, Biomaterials and Nanomedicine (CIBER-BBN), Barcelona, Spain
- 3Department of Microelectronics and Electronic Systems, Autonomous University of Barcelona, Barcelona, Spain
- 4Multiple Sclerosis Centre of Catalonia (CEMCAT), Department of Neurology/Neuroimmunology, Hospital Universitari Vall D’Hebron, Universitat Autónoma de Barcelona, Barcelona, Spain
- 5Faculty of Medicine and Surgery, Vita Salute San Raffaele University, Milan, Italy
- 6Institute of Psychiatry, Psychology and Neuroscience, King’s College London, London, United Kingdom
- 7RADAR-CNS Patient Advisory Board, London, United Kingdom
- 8Research and Development Information Technology, London, United Kingdom
- 9Department of Biostatistics and Health Informatics, Institute of Psychiatry, Psychology and Neuroscience, King’s College London, London, United Kingdom
- 10Institute of Health Informatics, University College London, London, United Kingdom
- 11Danish Multiple Sclerosis Centre, Department of Neurology, Copenhagen University Hospital Rigshospitalet, Copenhagen, Denmark
- 12Casa di Cura del Policlinico, Milan, Italy
- 13The RADAR-CNS Consortium, London, United Kingdom
Objective: The aim of this study was to evaluate the association between changes in the autonomic control of cardiorespiratory system induced by walk tests and outcome measures in people with Multiple Sclerosis (pwMS).
Methods: Electrocardiogram (ECG) recordings of 148 people with Relapsing-Remitting MS (RRMS) and 58 with Secondary Progressive MS (SPMS) were acquired using a wearable device before, during, and after walk test performance from a total of 386 periodical clinical visits. A subset of 90 participants repeated a walk test at home. Various MS-related symptoms, including fatigue, disability, and walking capacity were evaluated at each clinical visit, while heart rate variability (HRV) and ECG-derived respiration (EDR) were analyzed to assess autonomic nervous system (ANS) function. Statistical tests were conducted to assess differences in ANS control between pwMS grouped based on the phenotype or the severity of MS-related symptoms. Furthermore, correlation coefficients (r) were calculated to assess the association between the most significant ANS parameters and MS-outcome measures.
Results: People with SPMS, compared to RRMS, reached higher mean heart rate (HRM) values during walk test, and larger sympathovagal balance after test performance. Furthermore, pwMS who were able to adjust their HRM and ventilatory values, such as respiratory rate and standard deviation of the ECG-derived respiration, were associated with better clinical outcomes. Correlation analyses showed weak associations between ANS parameters and clinical outcomes when the Multiple Sclerosis phenotype is not taken into account. Blunted autonomic response, in particular HRM reactivity, was related with worse walking capacity, yielding r = 0.36 r = 0.29 (RRMS) and r > 0.5 (SPMS). A positive strong correlation r > 0.7 r > 0.65 between cardiorespiratory parameters derived at hospital and at home was also found.
Conclusion: Autonomic function, as measured by HRV, differs according to MS phenotype. Autonomic response to walk tests may be useful for assessing clinical outcomes, mainly in the progressive stage of MS. Participants with larger changes in HRM are able to walk longer distance, while reduced ventilatory function during and after walk test performance is associated with higher fatigue and disability severity scores. Monitoring of disorder severity could also be feasible using ECG-derived cardiac and respiratory parameters recorded with a wearable device at home.
1 Introduction
Multiple Sclerosis (MS) is a chronic inflammatory disorder characterized by demyelination of the nerve fibers in the human Central Nervous System (CNS) (Faissner et al., 2019). Progressive neurodegeneration owing to chronic demyelination causes varied neurological deficits, which may considerably reduce the quality of life in people with MS (pwMS) (McGinley et al., 2021). The high prevalence of MS (2.8 million people in 2020) together with the relatively young onset age (between 20 and 40 years) have a significant impact on personal and societal costs (Wallin et al., 2019; Walton et al., 2020).
Although the exact cause of MS remains uncertain, it is considered an inflammatory autoimmune disorder that is influenced by both genetic and environmental risk factors (Baecher-Allan et al., 2018). A general consensus is that the disorder begins with inflammatory lesions (known as focal plaques) due to the dysregulation of the Blood-Brain Barrier (BBB) (Mahad et al., 2015). The disruption of the BBB increases the trans-endothelial migration of activated leukocytes into the CNS, which can initiate inflammatory responses by releasing pro-inflammatory cytokines (Ortiz et al., 2014). Furthermore, the sympathetic and parasympathetic branches of the Autonomic Nervous System (ANS) play a key role in the bidirectional communication between the immune system and the CNS (Racosta and Kimpinski, 2016). Sympathetic influence on immune response can be direct, via adrenoceptors on immune cells, or indirect, through innervation of major immune organs (Pongratz and Straub, 2014). The parasympathetic division of the ANS, through the activation of the efferent vagus nerve, inhibits pro-inflammatory cytokine release and protects against systemic inflammation (Pavlov and Tracey, 2012). Impairment of the ANS can either trigger inflammatory states or may fail to activate anti-inflammatory mechanisms, causing a vicious neuroinflammatory cycle that amplifies tissue damage (Findling et al., 2020).
Dysfunction of the ANS is being increasingly recognized as an important aspect of MS, with an estimated prevalence of 45%–84% (Racosta and Kimpinski, 2016). The main clinical manifestations of autonomic disturbances are associated with abnormal cardiovascular control (Findling et al., 2020), aberrant thermoregulation (Christogianni et al., 2018), gastrointestinal symptoms (Aghaz et al., 2018), and pelvic organ dysfunction (Aharony et al., 2017). Retrospective studies have shown that autonomic symptoms may be a key player in both prodromal phase and development of clinically established MS (Disanto et al., 2018; Almeida et al., 2019; Skorić et al., 2019). Autonomic dysregulation is also implicated in other common MS-related symptoms, such as fatigue (Ayache and Chalah, 2017; Capone et al., 2020), sleep disturbances (Hensen et al., 2018; Sakkas et al., 2019), and clinical depression (Gold et al., 2005; Morris et al., 2018). Therefore, these findings highlight the importance of monitoring the ANS dysfunction in people with MS.
The functionality of the ANS is often assessed based on changes in cardiovascular parameters during diagnostic tests including, Valsalva maneuver, deep breathing, and tilt-table test (Ziemssen and Siepmann, 2019). The variation in ANS activity, which is known as autonomic reactivity, is particularly important since it reflects the ability of an individual to cope with a challenging situation (Carnevali et al., 2018; Kontaxis et al., 2020). In order homeostasis to be maintained, cardiovascular parameters, such as Heart Rate (HR), are constantly changing. Short-term and long-term variations of HR, the so-called Heart Rate Variability (HRV), have emerged as the most valuable non-invasive measure of ANS function (Billman, 2011). Reduced contribution of the ANS to cardiac regulation, reflected as lower HRV, signifies pathological changes associated with autonomic dysfunction (Ernst, 2017). Reduced HRV in pwMS, compared to healthy subjects, has been reported in numerous studies (Racosta and Kimpinski, 2016; Findling et al., 2020). Moreover, the severity of HRV deficit appears to be associated with the progression of the disorder (Studer et al., 2017; Adamec et al., 2018). It has been hypothesized that autonomic imbalance towards a sympathetic dominance may have a pathogenic role in the development of MS, while parasympathetic dysfunction correlates with the progression of the disorder (Pintér et al., 2015; Racosta and Kimpinski, 2016).
However, there is no consensus regarding the presence of relation between HRV and the most common disorder characteristics, such as disability and fatigue. The most widely used disability rating scale in MS is the Expanded Disability Status Scale (EDSS) (Inojosa et al., 2020b), while the Fatigue Severity Scale (FSS) is one of the most well-known questionnaires evaluating the fatigue severity in pwMS (Krupp et al., 1989). The EDSS is mainly based on the evaluation of functional systems including ambulation, i.e., the maximal walking distance without rest, and several functional systems such as visual, sensory, and cerebral, among others (Kurtzke, 1983). The FSS evaluates both physical and cognitive aspects of fatigue and their interference in daily living (Beckerman et al., 2020). Previous studies have shown a significant positive relation between EDSS scores and HRV parameters reflecting sympathetic dominance (Studer et al., 2017; Zawadka-Kunikowska et al., 2020), while in (Damla et al., 2018), no significant association between HRV and EDSS was found. Although HRV tended to be different in pwMS with and without fatigue, no significant correlation with FSS scores has been observed (Flachenecker et al., 2003; Sander et al., 2019). The absence of consensus regarding the relation of HRV with these MS-related symptoms could be partially explained by the subjective nature of the questionnaires (van Munster and Uitdehaag, 2017). For instance, the EDSS assessment is subjective to the examining neurologist (Inojosa et al., 2020a), while perception of fatigue in pwMS can be increased by comorbid conditions such as sleeping disturbances and depression (Sternberg, 2017).
Among the most common MS-related characteristics are also walking limitations that can be used to complement other less objective clinical measures (Bethoux and Bennett, 2011; Kieseier and Pozzilli, 2012). The 6-Minute Walk Test (6 MWT), which records the maximum distance a patient walks in 6 min, has been the most commonly applied measure of walking capacity in MS (Cederberg et al., 2019). In routine clinical assessment, the 2-Minute Walk Test (2 MWT) can be considered a practical replacement for the 6 MWT, which often tends to be more burdensome for individuals with MS (Andersen et al., 2016; Scalzitti et al., 2018). Current research on the walking assessments is focused only on changes in the HR profile rather than fluctuations in HRV parameters. Emerging evidence suggests that, in pwMS, a lower increase in the HR induced by walking is associated with higher levels of disability (Bosnak-Guclu et al., 2012; Dalgas et al., 2014). Although blunted autonomic reactivity to endurance exercise or tilt-up table test has been previously reported in pwMS (Studer et al., 2017; Zawadka-Kunikowska et al., 2020; Gerasimova-Meigal et al., 2021), no relationship between reactivity indices and disability or fatigue scores was found (Gervasoni et al., 2018; Rampichini et al., 2020).
A possible explanation for the lack of consensus regarding the potential use of HRV may also be the heterogeneity of the applied methods and the influence of respiration in the estimation of HRV indices. Changes in respiratory parameters, such as respiration rate and tidal volume, can confound the relationship between ANS function and HRV indices (Grossman and Taylor, 2007). To the best of the authors’ knowledge, none of the previous studies has taken into account the effect of respiration on HRV in pwMS. Recent studies suggest that besides monitoring respiration when analyzing HRV indices, there is an increasing awareness of the need to include respiration parameters in MS (Rzepiński et al., 2022). Previous studies in pwMS have shown that autonomic imbalance could influence breathing control and upper airway muscle activity (Hensen et al., 2018). In (Heine et al., 2016), a significant association between disorder severity and cardiopulmonary fitness was found. Respiratory dysfunction frequently occurs in people with advanced MS contributing significantly to morbidity and mortality (Tzelepis and McCool, 2015).
In order to monitor deterioration in pwMS, a continuous monitoring of clinical state is required. Remote measurement technologies (RMT), including a variety of sensors, can actively and passively collect numerous data that can assess symptom severity and progression, or response to treatment (White et al., 2022). With the advances in RMT over the last few decades, it could be now possible to provide real-time objective multidimensional indications of patients’ clinical symptoms (Malasinghe et al., 2019). A growing number of studies have explored the feasibility and potential effectiveness of RMTs in measuring a variety of physiological parameters among pwMS (Bradshaw et al., 2017; Alexander et al., 2020). The vast majority of RMTs are employed for non-invasive measurement of physical activity, while wearable sensors measuring cardiac activity still require further research before being included as tools for assessing autonomic dysfunction among pwMS (Fuller et al., 2020; Xiang and Bernard, 2021).
In this study, changes in HRV and respiratory parameters derived from the ECG induced by walk tests are analyzed for assessing clinical outcomes in pwMS. Correlation analyses with clinical markers of disorder severity and progression are performed. The main hypothesis tested here is that stress response to walk tests quantified by autonomic reactivity indices and respiratory parameters are useful for assessing clinical outcomes. This study also explores the feasibility and acceptability of home-based monitoring in pwMS.
2 Materials and methods
2.1 Dataset
The data used in this study were collected as part of the Remote Assessment of Disease and Relapse-Central Nervous System (RADAR-CNS) research programme1. RADAR-CNS is an IMI2 project that aims to develop new ways of measuring disorders related to CNS, such as MS, using remote monitoring technologies, i.e., wearable devices and mobile sensors. The MS work package of RADAR-CNS, which consists of multiple clinical sites spread across several European countries, started recruiting participants in June 2018. Since then, active (questionnaires and physical tests), and passive monitoring strategies (wearable and smartwatch devices) have been in place by three sites: Ospedale San Raffaele in Milan, Italy, Vall d’Hebron Institut de Recerca in Barcelona, Spain, and the University Hospital Copenhagen, Rigshospitalet in Copenhagen, Denmark (Ranjan et al., 2019). Outcome measures in pwMS were assessed every 3 months during clinical visits in the hospital, while the phenotype of the disorder, i.e., either relapsing-remitting MS (RRMS) or secondary progressive MS (SPMS), was assessed at the first clinical visit. In each clinical visit, participants underwent an experimental protocol that consists of three stages: (a) a Basal stage
As of 1 November 2021, 206 pwMS had been enrolled in the RADAR-MS study, and a total of 384 clinical visits had been conducted (99, 58, 34, 9, 5, and 1 patient(s) had one to six clinical visits, respectively). Although ECG data during the 2 MW T
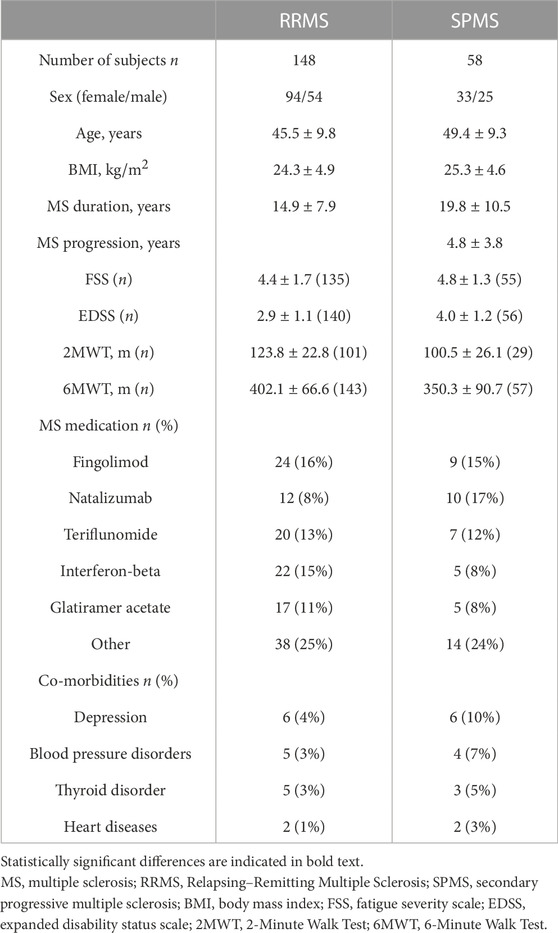
TABLE 1. Mean ± standard deviation of demographic data and baseline clinical data.
2.2 Heart rate variability and respiration indices
In this section the estimation of ECG-derived cardiorespiratory parameters that reflect ANS function is described. However, surface measurements of heart activity may include various types of noise, and thus ECG should be first preprocessed. To remove the baseline wander, the ECG signal was filtered using a forward-backward filter with cut-off frequency of 0.5 Hz. To reduce the effect of jitter into HRV parameters, the ECG was up-sampled from 125 to 1,000 Hz (Malik et al., 1996). Then, a wavelet-based detector was applied to identify the position of the QRS-complexes (Martínez et al., 2004). HRV was generated from the beat occurrence time series based on the integral pulse frequency modulation (IPFM) model, which accounts for misdetections and the presence of ectopic beats (Bailón et al., 2010). The IPFM model assumes that ANS modulation on the sinoatrial node can be represented by a band-limited signal. To derive spectral parameters, the modulating signal was sampled at 4 Hz, and the power spectral density was obtained by applying Welch’s periodogram in segments of length 5 min. A Hamming window of 100 s (50% overlap), which offers high temporal resolution and it allows the robust estimation of the lowest frequency of interest (4 periods for 0.04 Hz), was selected.
From short-term recordings, two main spectral components are distinguished in the low-frequency (LF) band ([0.04, 0.15] Hz) and in the high-frequency (HF) band ([0.15, 0.4] Hz). HF spectral power is considered a measure of parasympathetic nervous system activity, mainly due to the respiratory sinus arrhythmia, while LF fluctuations in HRV have been suggested to represent both sympathetic and parasympathetic modulations (Malik et al., 1996). Note that in order HF spectral power to reflect parasympathetic activity, respiratory rate must lay in the HF band. However, sometimes during exercise respiratory rate may be higher than the upper limit of the HF band. Hence, the extended HF band (eHF), which goes up to half the mean HR (fHR), i.e., the Nyquist frequency for HRV signals, is preferred (Bailón et al., 2007). Thus, the normalized LF power, i.e., the relative value of the LF power in proportion to the total (LF and eHF) power, is calculated for estimating sympathovagal balance (SB). Note that for the correct estimation of SB, respiratory rate must not lay in the LF band. In this study, since no respiration signal was recorded, respiratory parameters are estimated from the ECG. The ECG-derived respiration (EDR) signal, named slope range (Kontaxis et al., 2019), is used to obtain the mean respiratory rate (fr) from EDR spectra, and the standard deviation of the EDR signal (σr), is used as surrogate of tidal volume (Varon et al., 2020). It should be noted that a median absolute deviation-based rule was implemented to remove outliers from the EDR signal before parameter estimation (Bailón et al., 2006).
Besides HRM (HRMS), sympathovagal balance (SBS), and respiratory parameters (

FIGURE 1. HRV analysis during the 2MWT (A) HRV signal, (B) EDR signal, (C) HR profile, and (D) HRV spectrum.
2.3 Statistical analysis
Since a small percentage of subjects has measurements for more than two clinical visits, the statistical analysis is performed by averaging first measurements across multiple visits for each subject. Statistical analysis is conducted to assess differences in ANS regulation between groups of pwMS with different clinical outcomes. First of all, ANS function in pwMS with different phenotype (RRMS or SPMS) is considered. Participants with low (FSS <4) or high (FSS ≥4) fatigue scores (FSSL or FSSH, respectively), and with low (EDSS ≤2.5) or high (EDSS ≥4.5) disability scores (EDSSL or EDSSH, respectively), consist in groups of interest (Krupp et al., 1989; Manouchehrinia et al., 2017). Since there is no cut-off value for grouping pwMS based on 6MWT or 2MWT scores, the lower and upper quartiles are used. Participants are grouped into low or high 6MWT (6MWTL or 6MWTH). For separating pwMS based on statistical distribution, the 6MWT is selected as it has a higher completeness (97%) compared to 2MWT (63%), see Table 1. Statistically significant group differences (RRMS vs. SPMS, FSSL vs. FSSH, EDSSL vs. EDSSH, and 6MWTL vs. 6MWTH) are assessed with the two-sample t-test for independent samples, and the Mann-Whitney U non-parametric test when appropriate. Shapiro-Wilk and the two-sample F-test are conducted for ensuring normality and equality of variances, respectively. Differences in baseline demographic data are also evaluated.
Regression models based on a clinical measure (Phenotype, FSS, EDSS, 6MWT, 2MWT) with demographic variables (Sex, Age, BMI) as covariates are also used in order to determine significant predictors for autonomic variables. Partial correlation (Pearson r) analyses controlling for demographic variables (Sex, Age, BMI) are carried out for testing bivariate associations between the most significant ANS parameters and clinical outcomes. Since ANS function might differ according to the phenotype of the disorder, correlation analyses are also conducted separately for the populations of RRMS and SPMS. Finally, correlation coefficients between ANS parameters derived at hospital and at home are calculated to test the feasibility of RMT to monitor disorder severity in pwMS outside clinical settings. The significance threshold in this study is set to p < 0.05.
3 Results
Figure 2 illustrates the boxplots of HRV and respiratory parameters for different groups of pwMS. Groups based on phenotype consist of 148 and 58 subjects for RRMS and SPMS group, respectively, while the groups of (low, high) scores for FSS, EDSS, and 6MWT, consist of (64, 131), (70, 35), and (51, 51) subjects, respectively. Regarding phenotype, SPMS group, compared to RRMS, shows statistically significant higher HRM during walk test (Figure 2A) and increased sympathovagal balance after test execution (Figure 2B). Participants with low fatigue scores reached higher HRM level during
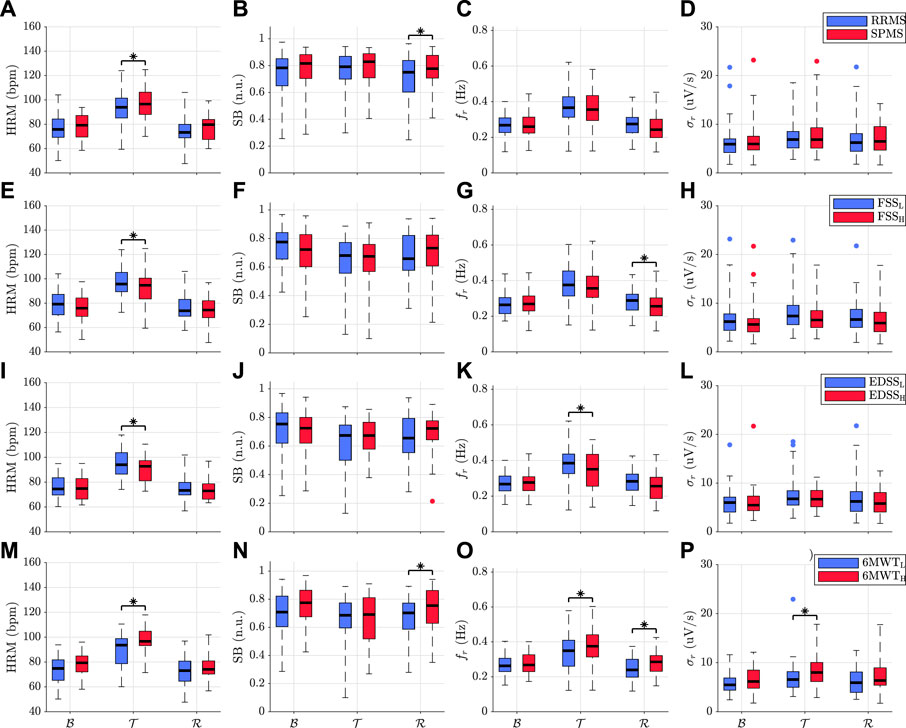
FIGURE 2. Boxplots of HRV and respiratory parameters for different groups of pwMS. Groups based on (A–D) phenotype, (E–H) fatigue severity, (I–L) disability level, and (M–P) walking capacity. Statistically significant group differences are denoted with an asterisk.
Significant predictors of ANS parameters in pwMS are presented in Table 2. Regression analysis results confirm that MS phenotype is an independent predictor for
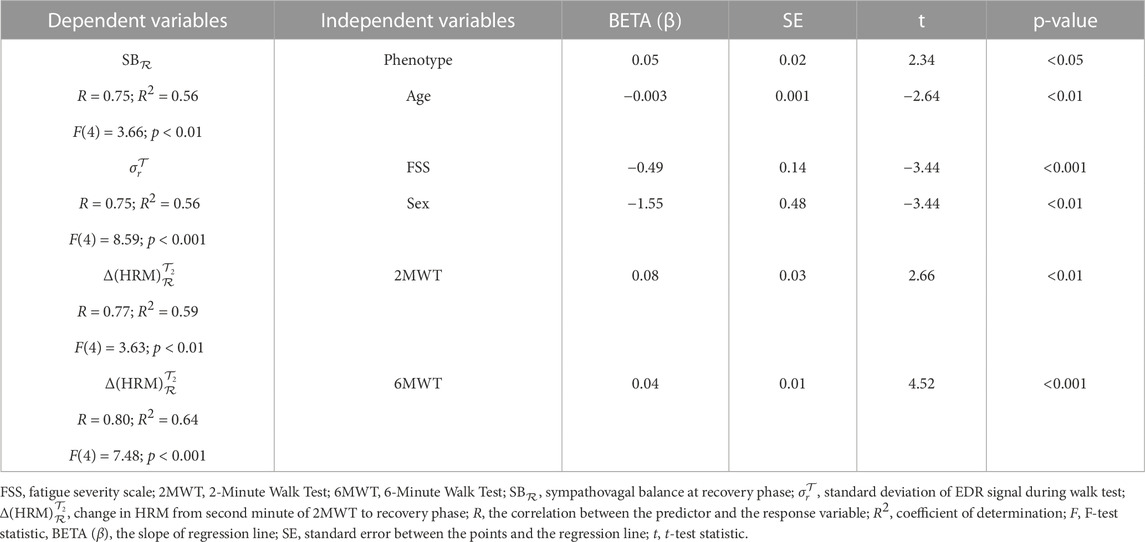
TABLE 2. Regression models to determine ANS parameters by clinical features.
Results of partial correlation analyses are summarized in Table 3. It can be seen that, analyzing all pwMS without taking into account the phenotype of the disorder, there is a weak association between ANS parameters and outcome measures. In particular, a moderate positive correlation between 6MWT and reactivity indices of HRM, implies that higher autonomic reactivity is associated with pwMS who were able to walk longer distance. The increase of HRM during the last minute of the 2MWT with respect to recovery stage
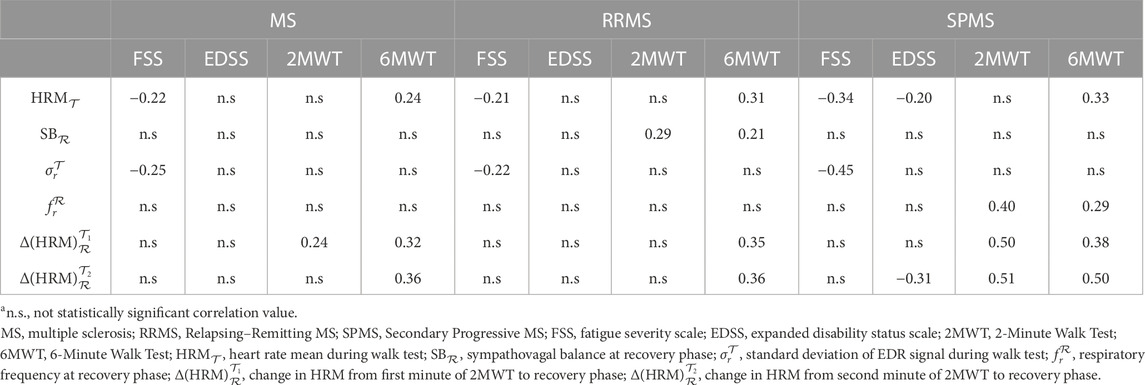
TABLE 3. Partial correlation coefficient r between ANS parameters and clinical outcomes.
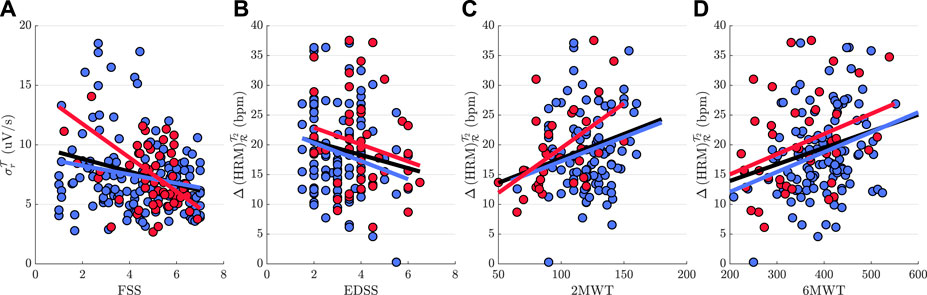
FIGURE 3. Scatter plots of the most significant ANS parameters for each clinical outcome measure (A) FSS, (B) EDSS, (C) 2MWT, and (D) 6MWT. A blue and red line are fitted to the data of RRMS and SPMS group, respectively, while a black line is fitted to the data without taking into account the phenotype of the disorder.
Finally, ANS parameters derived at home and at clinical visit while participants were performing the 2MWT, including
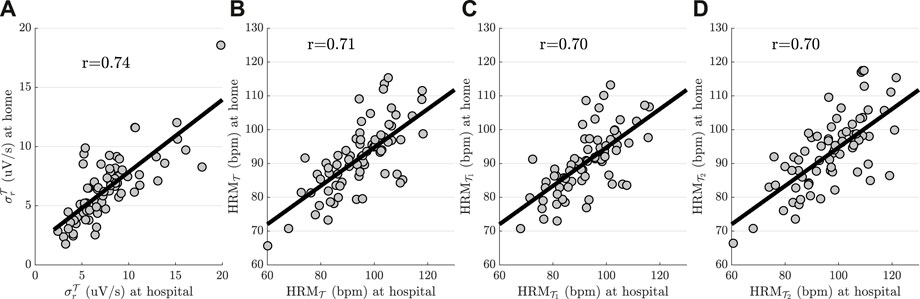
FIGURE 4. Scatter plots of the most significant ANS parameters derived during 2MWT performed at hospital and at home. (A)
4 Discussion
In this study the association between ANS response to walk tests and outcome measures in pwMS is investigated. Autonomic function is assessed with HRV and respiratory parameters derived from a wearable device, while MS-related symptoms, including fatigue severity, disability level, and walking capacity, are evaluated with rating scales and walk tests performed during periodical clinical visits. The feasibility of ANS parameters to provide a home-based monitoring of clinical markers is also explored.
HRV analysis can be used to assess the dynamic balance between the sympathetic and parasympathetic systems, allowing to infer the autonomic function. Results show that HRV parameters differ among participants depending on the MS phenotype. People with SPMS, compared to RRMS, show higher HRM while performing walk tests and larger SB after test performance (Figures 2A,B). Further statistical analyses revealed that the phenotype of MS was a significant predictor of sympathovagal balance (Table 2). Increased sympathetic dominance is associated with autonomic imbalance, which is often reported to be more pronounced in the progressive variant of the MS (Zawadka-Kunikowska et al., 2020; Gerasimova-Meigal et al., 2021). These results are in agreement with previous studies which found that pwMS exhibit higher HR levels during exercise compared to healthy subjects (Savci et al., 2005), and more prominent differences in autonomic tone during recovery phase (Gervasoni et al., 2018). Anticipatory stress dynamics prior to test execution could be implicated in the absence of significant differences between MS subgroups during basal conditions (Juster et al., 2012; Adamec et al., 2018; Reynders et al., 2020).
Autonomic dysregulation, besides the key role it plays in the progression of the disorder, it is also involved in the vast majority of MS-related symptoms (Findling et al., 2020). Results show that pwMS with low FSS and EDSS scores reach higher HRM values during walk tests (Figures 2E,I). Greater fatigue and disability severity in pwMS may be associated with loss in the capacity to increase cardiovascular output during exercise (Capone et al., 2020). Lower HR in moderate compared to mild disability group of pwMS at the end of walk tests was also observed in (Bosnak-Guclu et al., 2012). Similar to patients with chronic fatigue syndrome, HR was lower during exercise tests relative to control subjects (De Becker et al., 2000; Nelson et al., 2019). Furthermore, reduced cardiovascular output can lead to less ventilatory efficiency (Inbar et al., 2001; Javierre et al., 2010). This is in accordance with the lower respiratory rates (
Abnormalities in cardiac and/or ventilatory function can limit exercise performance capacity in pwMS (Wens et al., 2016). Participants who were able to walk longer distance (6MWTH) exhibit higher
Autonomic response to stress can provide valuable information regarding the monitoring of clinical outcomes in MS (Briones-Buixassa et al., 2015; Rzepiński et al., 2022). Besides changes from baseline to stress exposure, the length and persistence of stress reactions following the demanding challenge should be considered (Juster et al., 2012). The findings of this study reveal that walked distance and HRM reactivity indices have a positive relationship (Table 3). The increment of HRM during the last minute of the 2MWT with respect to recovery stage shows the best performance (r = 0.36) (r = 0.32) in pwMS (RRMS and SPMS). Furthermore, 2MWT and 6MWT scores were found as significant predictors of increased HRM reactivity measured with
The weak associations between outcome measures and ANS parameters might be attributed to differences in autonomic regulation between people with RRMS and SPMS (Adamec et al., 2018). Correlation analyses show better results taking into account the phenotype of the disorder (Figure 3). Reactivity indices of HRM and walk test scores, in particular, show a strong positive association in people with SPMS, yielding (r = 0.50 and r = 0.51) (r = 0.51 and r = 0.6) for 6MWT and 2MWT scores, respectively (Table 3). In (Hansen et al., 2013), walking capacity in pwMS was also found to be highly correlated with the impairment in adapting HR. Moreover, results show that pwMS who were able to walk longer distance reach higher respiratory rate during recovery, while less-fatigued pwMS show a larger cardiopulmonary effort during walk test (
Inconsistencies regarding the link between disorder severity and SB can be muddled by changes in respiration, since the beat-to-beat fluctuation in HR at the frequency of the respiratory cycle, which is known as the respiratory sinus arrhythmia component, is mediated by the parasympathetic branch of the ANS (Billman et al., 2015; Ziemssen and Siepmann, 2019). In this study, the influence of respiration on SB estimation is taken into account by tracking the respiratory rate and by modifying the classical HF band in HRV analysis. Beyond the heterogeneity of the applied methods, the assessment of ANS functionality using different autonomic tests could lead to discrepancies regarding the role of autonomic reactivity in MS. For instance, contradictory results have been reported about autonomic responses to mental and orthostatic stress (Studer et al., 2017; Vlcek et al., 2018; Imrich et al., 2021), while walk tests and deep breathing protocols may enhance differences in ANS regulation between pwMS and healthy subjects (Paltamaa et al., 2008; Wens et al., 2016; Gerasimova-Meigal et al., 2021).
Walk tests may be one of the most straightforward procedures for inducing autonomic changes, not only in clinical settings but also at home (Singh et al., 2014). With the development of RMTs, such as, smartphones, wearable sensors or home-based devices, ANS parameters can be monitored remotely Malasinghe et al. (2019). Strong correlation between ANS parameters derived at home and at clinical visits during the performance of walk tests (Figure 4) implies that RMTs can be used for home-based monitoring of disorder severity in pwMS. Aside from complementing clinical assessments, reducing clinic contact allows also pwMS who would not normally engage in studies to participate (Owens, 2020). Furthermore, the feasibility of RMT to detect small changes in impairment or functional improvement on a more regular basis could accurately represent long-term changes in the clinical state of pwMS (Alexander et al., 2020).
Although RMTs offer a lot of potential for research, they do have important limitations. Many technologies have a high initial engagement level that fades quickly if usage is not constantly monitored after the initial enthusiasm and commitment of users (Dorsey et al., 2017). In this study, only a small subset of subjects (about 60%) performed walk tests at home. Unintentional walk testing, which does not modify casual activity habits, may increase the number of pwMS who are less motivated to perform such tests for extended periods. According to a recent study, unintentional walk testing has been shown to be practical and useful for assessing walking capacity in free-living activities (Sokas et al., 2021). Another important limitation is the interpretation of SB during walk test. Despite vagal withdrawal, hyperpnea could entail a significant increase in HF power due to the mechanical effect of respiration on HRV (Cottin et al., 2008). Hence, a rise in sympathetic tone, and consequently in SB, might be blurred when respiratory rate and respiratory pattern are not taken into account. A better assessment of the SB could be achieved by removing respiratory influences from HRV (Varon et al., 2018).
Apart from monitoring respiration while assessing HRV indices, the need of evaluating respiratory function in pwMS is becoming increasingly apparent. Recent studies suggest that pwMS are at increased risk for sleep disturbances (Braley and Boudreau, 2016; Sakkas et al., 2019). Intermittent hypoxia produced by apneas during the night might enhance oxidative stress and aggravate MS neurodegeneration (Hensen et al., 2018). In addition to being a trigger for an acute MS exacerbation, sleep disorders contribute significantly to fatigue and other chronic MS symptoms (Braley and Boudreau, 2016; Sahraian et al., 2017). Thus, respiratory function should be assessed early in the illness course so that rehabilitation can be planned to prevent respiratory complications and improve quality of life in pwMS (Muhtaroglu et al., 2020). It should be also noted that autonomic tests assessing respiratory function (e.g., deep breathing test) (Rzepiński et al., 2022), could be more suitable instead of walk tests to quantify autonomic response in people with SPMS who often suffer from limited ambulation (Wens et al., 2016). Screening for both ventilatory and cardiac function could open a window of opportunities for the early diagnosis of the progressive stage of MS that is often established retrospectively and delayed (Inojosa et al., 2021). Finally, confirming findings of previous studies, both clinical outcomes and demographic characteristics (Table 2) may be also considered as significant predictors of autonomic function in pwMS Rzepiński et al. (2019). Thus, further research should be conducted for people with primary progressive MS, including a healthy control group as well, taking into account differences in more demographic predictors (e.g., fitness levels), and changes in medication or other disease modifying treatments (e.g., haematopoietic stem cell transplantation).
In conclusion, the findings of this study show that autonomic function as measured by HRV differs according to MS phenotype, with sympathetic dominance to be more pronounced in SPMS compared to RRMS. Autonomic response to walk tests quantified by autonomic reactivity indices and respiratory parameters are useful for assessing clinical outcomes mainly in the progressive stage of MS. Moreover, pwMS with larger autonomic reactivity, in particular, are able to walk longer distance, while reduced ventilatory function during and after walk test performance is associated with higher fatigue and disability severity scores. Finally, this study demonstrates that monitoring of disorder severity could be feasible using ECG-derived cardiac and respiratory parameters recorded with a wearable device at home.
Data availability statement
The datasets presented in this article are not readily available because of ethic requirements. Requests to access the datasets should be directed to the RADAR-CNS consortium and will be subject to local ethics clearances. Please email the corresponding author for details.
Ethics statement
The studies involving human participants were reviewed and approved by Casa di Cura del Policlinico, Hospital Universitari Vall d’Hebron, Copenhagen University Hospital Rigshospitalet. The patients/participants provided their written informed consent to participate in this study.
Author contributions
SK, EL, EG, NC, SV, and RB contributed to the study design. SK, EL, and RB contributed to the data analysis and manuscript writing. AG, AZ, MM, RL, MB, LL, and GC contributed to the data collection. VN, SS, ZR, AF, and RD contributed to the administrative and technical support of the study. JW, LL, GC, MM, PS, CN, and GC contributed to the clinical support of the study. MH (PI of RADAR-CNS) contributed to funding and oversight of data collection. All authors contributed to the critical revision of the manuscript.
Funding
The RADAR-CNS project has received funding from the Innovative Medicines Initiative 2 Joint Undertaking under grant agreement No 115902. This Joint Undertaking receives support from the European Union’s Horizon 2020 research and innovation programme and EFPIA (www.imi.europa.eu). This communication reflects the views of the RADAR-CNS Consortium and neither IMI nor the European Union and EFPIA are liable for any use that may be made of the information contained herein. Morover, the work was supported by the Grant TED2021-131106B-I00 funded by MCIN/AEI/ 10.13039/501100011033 and by the “European Union NextGenerationEU/PRTR”.
Acknowledgments
We thank all the members of the RADAR-CNS patient advisory board for their contribution to the device selection procedures, and their invaluable advice throughout the study protocol design.
Conflict of interest
MB has received speaker honoraria from Novartis.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
2https://www.bittium.com/medical/bittium-faros
References
Adamec, I., Crnošija, L., Junaković, A., Skorić, M. K., and Habek, M. (2018). Progressive multiple sclerosis patients have a higher burden of autonomic dysfunction compared to relapsing remitting phenotype. Clin. Neurophysiol. 129, 1588–1594. doi:10.1016/j.clinph.2018.05.009
Aghaz, A., Alidad, A., Hemmati, E., Jadidi, H., and Ghelichi, L. (2018). Prevalence of dysphagia in multiple sclerosis and its related factors: Systematic review and meta-analysis. Iran. J. Neurol. 17, 180–188.
Aharony, S. M., Lam, O., and Corcos, J. (2017). Evaluation of lower urinary tract symptoms in multiple sclerosis patients: Review of the literature and current guidelines. Can. Urol. Assoc. J. 11, 61–64. doi:10.5489/cuaj.4058
Alexander, S., Peryer, G., Gray, E., Barkhof, F., and Chataway, J. (2020). Wearable technologies to measure clinical outcomes in multiple sclerosis: A scoping review. Mult. Scler. Int. 1352458520946005, 1643–1656. doi:10.1177/1352458520946005
Almeida, M. N., Silvernale, C., Kuo, B., and Staller, K. (2019). Bowel symptoms predate the diagnosis among many patients with multiple sclerosis: A 14-year cohort study. Neurogastroenterol. Motil. 31, e13592. doi:10.1111/nmo.13592
Andersen, L. K., Knak, K. L., Witting, N., and Vissing, J. (2016). Two-and 6-minute walk tests assess walking capability equally in neuromuscular diseases. Neurology 86, 442–445. doi:10.1212/WNL.0000000000002332
Ayache, S. S., and Chalah, M. A. (2017). Fatigue in multiple sclerosis–insights into evaluation and management. Neurophysiol. Clin. 47, 139–171. doi:10.1016/j.neucli.2017.02.004
Baecher-Allan, C., Kaskow, B. J., and Weiner, H. L. (2018). Multiple sclerosis: Mechanisms and immunotherapy. Neuron 97, 742–768. doi:10.1016/j.neuron.2018.01.021
Bailón, R., Laguna, P., Mainardi, L., and Sornmo, L. (2007). “Analysis of heart rate variability using time-varying frequency bands based on respiratory frequency,” in 2007 29th Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. (IEEE), 6675–6678. doi:10.1109/IEMBS.2007.4353891
Bailón, R., Laouini, G., Grao, C., Orini, M., Laguna, P., and Meste, O. (2010). The integral pulse frequency modulation model with time-varying threshold: Application to heart rate variability analysis during exercise stress testing. Ieee. Trans. Biomed. Eng. 58, 642–652. doi:10.1109/TBME.2010.2095011
Bailón, R., Sornmo, L., and Laguna, P. (2006). A robust method for ecg-based estimation of the respiratory frequency during stress testing. Ieee. Trans. Biomed. Eng. 53, 1273–1285. doi:10.1109/TBME.2006.871888
Beckerman, H., Eijssen, I. C., van Meeteren, J., Verhulsdonck, M. C., and de Groot, V. (2020). Fatigue profiles in patients with multiple sclerosis are based on severity of fatigue and not on dimensions of fatigue. Sci. Rep. 10, 1–10. doi:10.1038/s41598-020-61076-1
Bethoux, F., and Bennett, S. (2011). Evaluating walking in patients with multiple sclerosis: Which assessment tools are useful in clinical practice? Int. J. MS Care 13, 4–14. doi:10.7224/1537-2073-13.1.4
Billman, G. E. (2011). Heart rate variability–a historical perspective. Front. Physiol. 2, 86. doi:10.3389/fphys.2011.00086
Billman, G. E., Huikuri, H. V., Sacha, J., and Trimmel, K. (2015). An introduction to heart rate variability: Methodological considerations and clinical applications. Front. Physiol. 6, 55. doi:10.3389/fphys.2015.00055
Bosnak-Guclu, M., Guclu-Gunduz, A., Nazliel, B., and Irkec, C. (2012). Comparison of functional exercise capacity, pulmonary function and respiratory muscle strength in patients with multiple sclerosis with different disability levels and healthy controls. J. Rehabil. Med. 44, 80–86. doi:10.2340/16501977-0900
Bradshaw, M. J., Farrow, S., Motl, R. W., and Chitnis, T. (2017). Wearable biosensors to monitor disability in multiple sclerosis. Neurol. Clin. Pract. 7, 354–362. doi:10.1212/CPJ.0000000000000382
Braley, T. J., and Boudreau, E. A. (2016). Sleep disorders in multiple sclerosis. Curr. Neurol. Neurosci. Rep. 16, 50–58. doi:10.1007/s11910-016-0649-2
Briones-Buixassa, L., Milà, R., M Aragonès, J., Bufill, E., Olaya, B., and Arrufat, F. X. (2015). Stress and multiple sclerosis: A systematic review considering potential moderating and mediating factors and methods of assessing stress. Health Psychol. Open 2, 2055102915612271. doi:10.1177/2055102915612271
Capone, F., Motolese, F., Falato, E., Rossi, M., and Di Lazzaro, V. (2020). The potential role of neurophysiology in the management of multiple sclerosis-related fatigue. Front. Neurol. 11, 251. doi:10.3389/fneur.2020.00251
Carnevali, L., Koenig, J., Sgoifo, A., and Ottaviani, C. (2018). Autonomic and brain morphological predictors of stress resilience. Front. Neurosci. 12, 228. doi:10.3389/fnins.2018.00228
Cederberg, K. L., Sikes, E. M., Bartolucci, A. A., and Motl, R. W. (2019). Walking endurance in multiple sclerosis: Meta-analysis of six-minute walk test performance. Gait posture 73, 147–153. doi:10.1016/j.gaitpost.2019.07.125
Christogianni, A., Bibb, R., Davis, S. L., Jay, O., Barnett, M., Evangelou, N., et al. (2018). Temperature sensitivity in multiple sclerosis: An overview of its impact on sensory and cognitive symptoms. Temperature 5, 208–223. doi:10.1080/23328940.2018.1475831
Cottin, F., Médigue, C., and Papelier, Y. (2008). Effect of heavy exercise on spectral baroreflex sensitivity, heart rate, and blood pressure variability in well-trained humans. Am. J. Physiol. - Heart Circ. Physiol. 295, H1150–H1155. doi:10.1152/ajpheart.00003.2008
Dalgas, U., Kjølhede, T., Gijbels, D., Romberg, A., Santoyo, C., de Noordhout, B. M., et al. (2014). Aerobic intensity and pacing pattern during the six-minute walk test in patients with multiple sclerosis. J. Rehabil. Med. 46, 59–66. doi:10.2340/16501977-1231
Dalla Costa, G., Leocani, L., Montalban, X., Guerrero, A. I., Sørensen, P. S., Magyari, M., et al. (2020). Real-time assessment of Covid-19 prevalence among multiple sclerosis patients: A multicenter European study. Neurol. Sci. 41, 1647–1650. doi:10.1007/s10072-020-04519-x
Damla, O., Altug, C., Pinar, K. K., Alper, K., Dilek, I. G., and Kadriye, A. (2018). Heart rate variability analysis in patients with multiple sclerosis. Mult. Scler. Relat. Disord. 24, 64–68. doi:10.1016/j.msard.2018.06.012
De Becker, P., Roeykens, J., Reynders, M., McGregor, N., and De Meirleir, K. (2000). Exercise capacity in chronic fatigue syndrome. Arch. Intern. Med. 160, 3270–3277. doi:10.1001/archinte.160.21.3270
Disanto, G., Zecca, C., MacLachlan, S., Sacco, R., Handunnetthi, L., Meier, U. C., et al. (2018). Prodromal symptoms of multiple sclerosis in primary care. Ann. Neurol. 83, 1162–1173. doi:10.1002/ana.25247
Dorsey, E. R., McConnell, M. V., Shaw, S. Y., Trister, A. D., and Friend, S. H. (2017). The use of smartphones for health research. Acad. Med. 92, 157–160. doi:10.1097/ACM.0000000000001205
Ernst, G. (2017). Heart-rate variability—More than heart beats? Front. Public Health 5, 240. doi:10.3389/fpubh.2017.00240
Faissner, S., Plemel, J. R., Gold, R., and Yong, V. W. (2019). Progressive multiple sclerosis: From pathophysiology to therapeutic strategies. Nat. Rev. Drug Discov. 18, 905–922. doi:10.1038/s41573-019-0035-2
Findling, O., Hauer, L., Pezawas, T., Rommer, P. S., Struhal, W., and Sellner, J. (2020). Cardiac autonomic dysfunction in multiple sclerosis: A systematic review of current knowledge and impact of immunotherapies. J. Clin. Med. 9, 335. doi:10.3390/jcm9020335
Flachenecker, P., Rufer, A., Bihler, I., Hippel, C., Reiners, K., Toyka, K., et al. (2003). Fatigue in ms is related to sympathetic vasomotor dysfunction. Neurology 61, 851–853. doi:10.1212/01.wnl.0000080365.95436.b8
Fuller, D., Colwell, E., Low, J., Orychock, K., Tobin, M. A., Simango, B., et al. (2020). Reliability and validity of commercially available wearable devices for measuring steps, energy expenditure, and heart rate: Systematic review. JMIR mHealth uHealth 8, e18694. doi:10.2196/18694
Gerasimova-Meigal, L., Sirenev, I., and Meigal, A. (2021). Evidence of autonomic dysfunction in patients with relapsing-remitting multiple sclerosis: Heart rate variability and cardiovascular parameters. Pathophysiology 28, 10–19. doi:10.3390/pathophysiology28010002
Gervasoni, E., Bove, M., Sinatra, M., Grosso, C., Rovaris, M., Cattaneo, D., et al. (2018). Cardiac autonomic function during postural changes and exercise in people with multiple sclerosis: A cross-sectional study. Mult. Scler. Relat. Disord. 24, 85–90. doi:10.1016/j.msard.2018.06.003
Gold, S. M., Mohr, D. C., Huitinga, I., Flachenecker, P., Sternberg, E. M., and Heesen, C. (2005). The role of stress-response systems for the pathogenesis and progression of ms. Trends Immunol. 26, 644–652. doi:10.1016/j.it.2005.09.010
Grossman, P., and Taylor, E. W. (2007). Toward understanding respiratory sinus arrhythmia: Relations to cardiac vagal tone, evolution and biobehavioral functions. Biol. Psychol. 74, 263–285. doi:10.1016/j.biopsycho.2005.11.014
Hansen, D., Wens, I., Dendale, P., and Eijnde, B. O. (2013). Exercise-onset heart rate increase is slowed in multiple sclerosis patients: Does a disturbed cardiac autonomic control affect exercise tolerance? NeuroRehabilitation 33, 139–146. doi:10.3233/NRE-130938
Hansen, D., Wens, I., Keytsman, C., Verboven, K., Dendale, P., and Eijnde, B. (2015). Ventilatory function during exercise in multiple sclerosis and impact of training intervention: Cross-sectional and randomized controlled trial. Eur. J. Phys. Rehabil. Med. 51, 557–568.
Heine, M., Wens, I., Langeskov-Christensen, M., Verschuren, O., Eijnde, B. O., Kwakkel, G., et al. (2016). Cardiopulmonary fitness is related to disease severity in multiple sclerosis. Mult. Scler. Int. 22, 231–238. doi:10.1177/1352458515581437
Hensen, H. A., Krishnan, A. V., and Eckert, D. J. (2018). Sleep-disordered breathing in people with multiple sclerosis: Prevalence, pathophysiological mechanisms, and disease consequences. Front. Neurol. 8, 740. doi:10.3389/fneur.2017.00740
Imrich, R., Vlcek, M., Penesova, A., Radikova, Z., Havranova, A., Sivakova, M., et al. (2021). Cardiac autonomic function in patients with early multiple sclerosis. Clin. Auton. Res. 31, 553–562. doi:10.1007/s10286-021-00790-w
Inbar, O., Dlin, R., Rotstein, A., and Whipp, B. J. (2001). Physiological responses to incremental exercise in patients with chronic fatigue syndrome. Med. Sci. Sports Exerc. 33, 1463–1470. doi:10.1097/00005768-200109000-00007
Inojosa, H., Proschmann, U., Akgün, K., and Ziemssen, T. (2021). A focus on secondary progressive multiple sclerosis (spms): Challenges in diagnosis and definition. J. Neurol. 268, 1210–1221. doi:10.1007/s00415-019-09489-5
Inojosa, H., Schriefer, D., and Ziemssen, T. (2020b). Clinical outcome measures in multiple sclerosis: A review. Autoimmun. Rev. 19, 102512. doi:10.1016/j.autrev.2020.102512
Inojosa, H., Schriefer, D., Klöditz, A., Trentzsch, K., and Ziemssen, T. (2020a). Balance testing in multiple sclerosis—Improving neurological assessment with static posturography? Front. Neurol. 11, 135. doi:10.3389/fneur.2020.00135
Javierre, C., Guillamò, E., Blázquez, A., Comella, A., Martínez-Rodríguez, R., Garrido, E., et al. (2010). Respiratory response to low-intensity physical exercise in women with chronic fatigue syndrome. Apunt. l’Esport 45, 169–173. doi:10.1016/j.apunts.2010.01.004
Juster, R.-P., Perna, A., Marin, M.-F., Sindi, S., and Lupien, S. J. (2012). Timing is everything: Anticipatory stress dynamics among cortisol and blood pressure reactivity and recovery in healthy adults. Stress 15, 569–577. doi:10.3109/10253890.2012.661494
Kieseier, B. C., and Pozzilli, C. (2012). Assessing walking disability in multiple sclerosis. Mult. Scler. Int. 18, 914–924. doi:10.1177/1352458512444498
Kontaxis, S., Gil, E., Marozas, V., Lázaro, J., Garcia, E., Posadas-de Miguel, M., et al. (2020). Photoplethysmographic waveform analysis for autonomic reactivity assessment in depression. Ieee. Trans. Biomed. Eng. 68, 1273–1281. doi:10.1109/TBME.2020.3025908
Kontaxis, S., Lázaro, J., Corino, V. D., Sandberg, F., Bailón, R., Laguna, P., et al. (2019). Ecg-derived respiratory rate in atrial fibrillation. Ieee. Trans. Biomed. Eng. 67, 905–914. doi:10.1109/TBME.2019.2923587
Krupp, L. B., LaRocca, N. G., Muir-Nash, J., and Steinberg, A. D. (1989). The fatigue severity scale: Application to patients with multiple sclerosis and systemic lupus erythematosus. Arch. Neurol. 46, 1121–1123. doi:10.1001/archneur.1989.00520460115022
Kurtzke, J. F. (1983). Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (edss). Neurology 33, 1444–1452. doi:10.1212/wnl.33.11.1444
Madsen, L. T., Dalgas, U., Hvid, L. G., and Bansi, J. (2019). A cross-sectional study on the relationship between cardiorespiratory fitness, disease severity and walking speed in persons with multiple sclerosis. Mult. Scler. Relat. Disord. 29, 35–40. doi:10.1016/j.msard.2019.01.024
Mahad, D. H., Trapp, B. D., and Lassmann, H. (2015). Pathological mechanisms in progressive multiple sclerosis. Lancet Neurol. 14, 183–193. doi:10.1016/S1474-4422(14)70256-X
Malasinghe, L. P., Ramzan, N., and Dahal, K. (2019). Remote patient monitoring: A comprehensive study. J. Ambient. Intell. Humaniz. Comput. 10, 57–76. doi:10.1007/s12652-017-0598-x
Malik, M., Bigger, J. T., Camm, A. J., Kleiger, R. E., Malliani, A., Moss, A. J., et al. (1996). Heart rate variability: Standards of measurement, physiological interpretation, and clinical use. Eur. Heart J. 17, 354–381. doi:10.1093/oxfordjournals.eurheartj.a014868
Manouchehrinia, A., Westerlind, H., Kingwell, E., Zhu, F., Carruthers, R., Ramanujam, R., et al. (2017). Age related multiple sclerosis severity score: Disability ranked by age. Mult. Scler. Int. 23, 1938–1946. doi:10.1177/1352458517690618
Martínez, J. P., Almeida, R., Olmos, S., Rocha, A. P., and Laguna, P. (2004). A wavelet-based ecg delineator: Evaluation on standard databases. Ieee. Trans. Biomed. Eng. 51, 570–581. doi:10.1109/TBME.2003.821031
McGinley, M. P., Goldschmidt, C. H., and Rae-Grant, A. D. (2021). Diagnosis and treatment of multiple sclerosis: A review. JAMA 325, 765–779. doi:10.1001/jama.2020.26858
Morris, G., Reiche, E. M. V., Murru, A., Carvalho, A. F., Maes, M., Berk, M., et al. (2018). Multiple immune-inflammatory and oxidative and nitrosative stress pathways explain the frequent presence of depression in multiple sclerosis. Mol. Neurobiol. 55, 6282–6306. doi:10.1007/s12035-017-0843-5
Muhtaroglu, M., Ertugrul Mut, S., Selcuk, F., and Malkoc, M. (2020). Evaluation of respiratory functions and quality of life in multiple sclerosis patients. Acta Neurol. belg. 120, 1107–1113. doi:10.1007/s13760-018-0967-z
Nelson, M. J., Bahl, J. S., Buckley, J. D., Thomson, R. L., and Davison, K. (2019). Evidence of altered cardiac autonomic regulation in myalgic encephalomyelitis/chronic fatigue syndrome: A systematic review and meta-analysis. Medicine 98, e17600. doi:10.1097/MD.0000000000017600
Ortiz, G. G., Pacheco-Moisés, F. P., Macías-Islas, M. Á., Flores-Alvarado, L. J., Mireles-Ramírez, M. A., González-Renovato, E. D., et al. (2014). Role of the blood–brain barrier in multiple sclerosis. Arch. Med. Res. 45, 687–697. doi:10.1016/j.arcmed.2014.11.013
Owens, A. P. (2020). The role of heart rate variability in the future of remote digital biomarkers. Front. Neurosci. 14, 582145. doi:10.3389/fnins.2020.582145
Paltamaa, J., Sarasoja, T., Leskinen, E., Wikström, J., and Mälkiä, E. (2008). Measuring deterioration in international classification of functioning domains of people with multiple sclerosis who are ambulatory. Phys. Ther. 88, 176–190. doi:10.2522/ptj.20070064
Pavlov, V. A., and Tracey, K. J. (2012). The vagus nerve and the inflammatory reflex—Linking immunity and metabolism. Nat. Rev. Endocrinol. 8, 743–754. doi:10.1038/nrendo.2012.189
Pintér, A., Cseh, D., Sárközi, A., Illigens, B. M., and Siepmann, T. (2015). Autonomic dysregulation in multiple sclerosis. Int. J. Mol. Sci. 16, 16920–16952. doi:10.3390/ijms160816920
Pongratz, G., and Straub, R. H. (2014). The sympathetic nervous response in inflammation. Arthritis Res. Ther. 16, 504–512. doi:10.1186/s13075-014-0504-2
Racosta, J. M., and Kimpinski, K. (2016). Autonomic dysfunction, immune regulation, and multiple sclerosis. Clin. Auton. Res. 26, 23–31. doi:10.1007/s10286-015-0325-7
Rampichini, S., Gervasoni, E., Cattaneo, D., Rovaris, M., Grosso, C., Maggioni, M. A., et al. (2020). Impaired heart rate recovery after sub-maximal physical exercise in people with multiple sclerosis. Mult. Scler. Relat. Disord. 40, 101960. doi:10.1016/j.msard.2020.101960
Ranjan, Y., Rashid, Z., Stewart, C., Conde, P., Begale, M., Verbeeck, D., et al. (2019). Radar-base: Open source mobile health platform for collecting, monitoring, and analyzing data using sensors, wearables, and mobile devices. JMIR mHealth uHealth 7, e11734. doi:10.2196/11734
Reynders, T., Gidron, Y., De Ville, J., Bjerke, M., Weets, I., Van Remoortel, A., et al. (2020). Relation between heart rate variability and disease course in multiple sclerosis. J. Clin. Med. 9, 3. doi:10.3390/jcm9010003
Rzepiński, Ł., Zawadka-Kunikowska, M., Maciejek, Z., Newton, J. L., and Zalewski, P. (2019). Early clinical features, time to secondary progression, and disability milestones in polish multiple sclerosis patients. Medicina 55, 232. doi:10.3390/medicina55060232
Rzepiński, Ł., Zawadka-Kunikowska, M., Newton, J. L., Zalewski, P., and Słomko, J. (2022). Cardiovascular autonomic dysfunction in multiple sclerosis—Findings and relationships with clinical outcomes and fatigue severity. Neurol. Sci. 43, 4829–4839. doi:10.1007/s10072-022-06099-4
Sahraian, M. A., Rezaali, S., Hosseiny, M., Doosti, R., Tajik, A., and Moghadasi, A. N. (2017). Sleep disorder as a triggering factor for relapse in multiple sclerosis. Eur. Neurol. 77, 258–261. doi:10.1159/000470904
Sakkas, G. K., Giannaki, C. D., Karatzaferi, C., and Manconi, M. (2019). Sleep abnormalities in multiple sclerosis. Curr. Treat. Options Neurol. 21, 4. doi:10.1007/s11940-019-0544-7
Sander, C., Modes, F., Schlake, H.-P., Eling, P., and Hildebrandt, H. (2019). Capturing fatigue parameters: The impact of vagal processing in multiple sclerosis related cognitive fatigue. Mult. Scler. Relat. Disord. 32, 13–18. doi:10.1016/j.msard.2019.04.013
Savci, S., Inal-Ince, D., Arikan, H., Guclu-Gunduz, A., Cetisli-Korkmaz, N., Armutlu, K., et al. (2005). Six-minute walk distance as a measure of functional exercise capacity in multiple sclerosis. Disabil. Rehabil. 27, 1365–1371. doi:10.1080/09638280500164479
Scalzitti, D. A., Harwood, K. J., Maring, J. R., Leach, S. J., Ruckert, E. A., and Costello, E. (2018). Validation of the 2-minute walk test with the 6-minute walk test and other functional measures in persons with multiple sclerosis. Int. J. MS Care 20, 158–163. doi:10.7224/1537-2073.2017-046
Shirbani, F., Barin, E., Lee, Y.-C., Ng, K., Parratt, J. D. E., Butlin, M., et al. (2018). Characterisation of cardiac autonomic function in multiple sclerosis based on spontaneous changes of heart rate and blood pressure. Mult. Scler. Relat. Disord. 22, 120–127. doi:10.1016/j.msard.2018.03.018
Singh, S. J., Puhan, M. A., Andrianopoulos, V., Hernandes, N. A., Mitchell, K. E., Hill, C. J., et al. (2014). An official systematic review of the European respiratory society/american thoracic society: Measurement properties of field walking tests in chronic respiratory disease. Eur. Respir. J. 44, 1447–1478. doi:10.1183/09031936.00150414
Skorić, M. K., Crnošija, L., Gabelić, T., Barun, B., Adamec, I., Junaković, A., et al. (2019). Autonomic symptom burden can predict disease activity in early multiple sclerosis. Mult. Scler. Relat. Disord. 28, 250–255. doi:10.1016/j.msard.2019.01.005
Sokas, D., Paliakaitė, B., Rapalis, A., Marozas, V., Bailón, R., and Petrėnas, A. (2021). Detection of walk tests in free-living activities using a wrist-worn device. Front. Physiol. 12, 706545. doi:10.3389/fphys.2021.706545
Sternberg, Z. (2017). Impaired neurovisceral integration of cardiovascular modulation contributes to multiple sclerosis morbidities. Mol. Neurobiol. 54, 362–374. doi:10.1007/s12035-015-9599-y
Studer, V., Rocchi, C., Motta, C., Lauretti, B., Perugini, J., Brambilla, L., et al. (2017). Heart rate variability is differentially altered in multiple sclerosis: Implications for acute, worsening and progressive disability. Mult. Scler. J. Exp. Transl. Clin. 3, 2055217317701317. doi:10.1177/2055217317701317
Tzelepis, G. E., and McCool, F. D. (2015). Respiratory dysfunction in multiple sclerosis. Respir. Med. 109, 671–679. doi:10.1016/j.rmed.2015.01.018
van Munster, C. E., and Uitdehaag, B. M. (2017). Outcome measures in clinical trials for multiple sclerosis. CNS Drugs 31, 217–236. doi:10.1007/s40263-017-0412-5
Varon, C., Lázaro, J., Bolea, J., Hernando, A., Aguiló, J., Gil, E., et al. (2018). Unconstrained estimation of hrv indices after removing respiratory influences from heart rate. IEEE J. Biomed. Health Inf. 23, 2386–2397. doi:10.1109/JBHI.2018.2884644
Varon, C., Morales, J., Lázaro, J., Orini, M., Deviaene, M., Kontaxis, S., et al. (2020). A comparative study of ecg-derived respiration in ambulatory monitoring using the single-lead ecg. Sci. Rep. 10, 5704–5714. doi:10.1038/s41598-020-62624-5
Vlcek, M., Penesova, A., Imrich, R., Meskova, M., Mravcova, M., Grunnerova, L., et al. (2018). Autonomic nervous system response to stressors in newly diagnosed patients with multiple sclerosis. Cell. Mol. Neurobiol. 38, 363–370. doi:10.1007/s10571-017-0511-3
Wallin, M. T., Culpepper, W. J., Nichols, E., Bhutta, Z. A., Gebrehiwot, T. T., Hay, S. I., et al. (2019). Global, regional, and national burden of multiple sclerosis 1990–2016: A systematic analysis for the global burden of disease study 2016. Lancet Neurol. 18, 269–285. doi:10.1016/S1474-4422(18)30443-5
Walton, C., King, R., Rechtman, L., Kaye, W., Leray, E., Marrie, R. A., et al. (2020). Rising prevalence of multiple sclerosis worldwide: Insights from the Atlas of MS, third edition. Mult. Scler. Int. 26, 1816–1821. doi:10.1177/1352458520970841
Wens, I., Eijnde, B. O., and Hansen, D. (2016). Muscular, cardiac, ventilatory and metabolic dysfunction in patients with multiple sclerosis: Implications for screening, clinical care and endurance and resistance exercise therapy, a scoping review. J. Neurol. Sci. 367, 107–121. doi:10.1016/j.jns.2016.05.050
White, K. M., Williamson, C., Bergou, N., Oetzmann, C., de Angel, V., Matcham, F., et al. (2022). A systematic review of engagement reporting in remote measurement studies for health symptom tracking. NPJ Digit. Med. 5, 82–10. doi:10.1038/s41746-022-00624-7
Xiang, X. M., and Bernard, J. (2021). Telehealth in multiple sclerosis clinical care and research. Curr. Neurol. Neurosci. Rep. 21, 14–17. doi:10.1007/s11910-021-01103-4
Zawadka-Kunikowska, M., Rzepiński, Ł., Newton, J. L., Zalewski, P., and Słomko, J. (2020). Cardiac autonomic modulation is different in terms of clinical variant of multiple sclerosis. J. Clin. Med. 9, 3176. doi:10.3390/jcm9103176
Keywords: autonomic nervous system, heart rate variability, ECG-derived respiration, relapsing-remitting multiple sclerosis, secondary progressive multiple sclerosis, fatigue, disability, walking capacity
Citation: Kontaxis S, Laporta E, Garcia E, Guerrero AI, Zabalza A, Matteo M, Lucia R, Simblett S, Weyer J, Hotopf M, Narayan VA, Rashid Z, Folarin AA, Dobson RJB, Buron MD, Leocani L, Cummins N, Vairavan S, Costa GD, Magyari M, Sørensen PS, Nos C, Bailón R, Comi G and the RADAR-CNS Consortium (2023) Autonomic response to walk tests is useful for assessing outcome measures in people with multiple sclerosis. Front. Physiol. 14:1145818. doi: 10.3389/fphys.2023.1145818
Received: 16 January 2023; Accepted: 15 March 2023;
Published: 06 April 2023.
Edited by:
Mario Habek, University of Zagreb, CroatiaReviewed by:
Magdalena Krbot Skoric, University Hospital Centre Zagreb, CroatiaŁukasz Rzepiński, 10th Military Research Hospital and Polyclinic, Poland
Ivan Adamec, University Hospital Centre Zagreb, Croatia
Copyright © 2023 Kontaxis, Laporta, Garcia, Guerrero, Zabalza, Matteo, Lucia, Simblett, Weyer, Hotopf, Narayan, Rashid, Folarin, Dobson, Buron, Leocani, Cummins, Vairavan, Costa, Magyari, Sørensen, Nos, Bailón, Comi and the RADAR-CNS Consortium. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Spyridon Kontaxis, sikontax@gmail.com