
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Physiol., 10 May 2023
Sec. Physio-logging
Volume 14 - 2023 | https://doi.org/10.3389/fphys.2023.1147260
This article is part of the Research TopicRobust, Reliable and Continuous Assessment in Health: The Challenge of Wearable and Remote TechnologiesView all 9 articles
 Thais Castro Ribeiro1,2*
Thais Castro Ribeiro1,2* Pau Sobregrau Sangrà3
Pau Sobregrau Sangrà3 Esther García Pagès2
Esther García Pagès2 Llorenç Badiella4Beatriz López-Barbeito5Sira Aguiló5
Llorenç Badiella4Beatriz López-Barbeito5Sira Aguiló5 Jordi Aguiló1,2
Jordi Aguiló1,2Introduction: The increasing burden on mental health has become a worldwide concern especially due to its substantial negative social and economic impact. The implementation of prevention actions and psychological interventions is crucial to mitigate these consequences, and evidence supporting its effectiveness would facilitate a more assertive response. Heart rate variability biofeedback (HRV-BF) has been proposed as a potential intervention to improve mental wellbeing through mechanisms in autonomic functioning. The aim of this study is to propose and evaluate the validity of an objective procedure to assess the effectiveness of a HRV-BF protocol in mitigating mental health symptoms in a sample of frontline HCWs (healthcare workers) who worked in the COVID-19 pandemic.
Methods: A prospective experimental study applying a HRV-BF protocol was conducted with 21 frontline healthcare workers in 5 weekly sessions. For PRE–POST intervention comparisons, two different approaches were used to evaluate mental health status: applying (a) gold-standard psychometric questionnaires and (b) electrophysiological multiparametric models for chronic and acute stress assessment.
Results: After HRV-BF intervention, psychometric questionnaires showed a reduction in mental health symptoms and stress perception. The electrophysiological multiparametric also showed a reduction in chronic stress levels, while the acute stress levels were similar in PRE and POST conditions. A significant reduction in respiratory rate and an increase in some heart rate variability parameters, such as SDNN, LFn, and LF/HF ratio, were also observed after intervention.
Conclusion: Our findings suggest that a 5-session HRV-BF protocol is an effective intervention for reducing stress and other mental health symptoms among frontline HCWs who worked during the COVID-19 pandemic. The electrophysiological multiparametric models provide relevant information about the current mental health state, being useful for objectively evaluating the effectiveness of stress-reducing interventions. Further research could replicate the proposed procedure to confirm its feasibility for different samples and specific interventions.
In recent years, mental health has become a global concern. The increasing prevalence of mental health disorders also impairs physical health, causing disability and negative economic and social impacts (Flores et al., 2018). The World Health Organization (WHO) recognizes that mental healthcare is an essential part of comprehensive care, thus supporting the need for actions to promote mental wellbeing and implement prevention interventions (World Health Organization, 2022). There is substantial literature regarding psychological interventions (Purtle et al., 2020), although there is scarce evidence supporting their validity, and limited quantitative outcomes have been considered (Ahmed et al., 2021; Cairns et al., 2021).
To advance in the field of mental health, it is crucial to establish reliable tools that allow to objectively assess the patient’s affectability and the effectiveness of applied interventions. The measurement of electrophysiological variables provides information about the functioning of the autonomic nervous system (ANS) and permits estimating the stress level non-invasively, being an extended quantitative approach for this purpose (Ahmed et al., 2022).
A sustained stress response generates an ANS imbalance as the body tends to hyperactivate the sympathetic nervous system (SNS) and the hypothalamus–pituitary–adrenal axis (HPA), leading to hormonal and physiological adaptations for a “fight-or-flight response.” The parasympathetic nervous system (PNS) typically facilitates the recovery of stress responses, giving flexibility to adapt to different daily situations, although under a chronic stress condition, this function is compromised (McCraty and Shaffer, 2015).
Cardiac function is strongly regulated by the brain through dynamic interactions between the SNS and PNS (Tonhajzerova et al., 2012). Heart rate variability (HRV), which reflects the fluctuation in time intervals between adjacent heartbeats, and its metrics have become widely used indices of these interactions, and hence, of psychological wellbeing. Low HRV has been associated with a diminished regulation capability of the ANS, cardiovascular outcomes, impairment of the immune system, aging, and other conditions. Moreover, high HRV has been linked with better performance, health, and adaptability (Kim et al., 2018). Nevertheless, evidence showed limitations when interpreting HRV parameters in a simplistic binary way (sympathetic and parasympathetic) and highlighted the complexity of this system and influencing factors, such as age and respiratory rate (Billman, 2013; Hernando et al., 2016; Hayano and Yuda, 2019).
In the literature, the outcomes more frequently selected to evaluate the effect of mental health interventions are as follows: a) psychometric questionnaires to subjectively estimate the anxiety state, stress level, and severity of depression, among others (Lehrer et al., 2020); b) HRV parameters to assess ANS functioning (Heiss et al., 2021); and c) electrodermal activity (EDA) indexes to evaluate sympathetic activation (Scavone et al., 2020). We hypothesize that use of subjective measures and single-objective indices limits the understanding of the stress response; hence, a multimodal approach is being proposed in the current study. Indices derived from electrocardiogram (ECG), EDA, peripheral skin temperature and respiration collectively may provide a more comprehensive information on physiological behavior and stress response (Garzón-Rey, 2017; Arza et al., 2018; García Pagès et al., 2023). Our research group has suggested combined models that include a set of electrophysiological variables, which were constructed from statistical models based on the usual clinical psychological assessment (self-reported questionnaires), thus providing a more robust estimation (Garzón-Rey et al., 2017; Aguiló Mir et al., 2021).
The heart rate variability biofeedback (HRV-BF) is a proactive intervention that allows easy multimodal signal recording and quantitative measurements, besides being broadly applied for mental health issues (Moss and Shaffer, 2017). One of the HRV-BF mechanisms is based on the physiological relation between cardiovascular and respiratory systems, which is mediated by the vagus nerve, also known as respiratory sinus arrhythmia (RSA), where the heart rate accelerates during inhalation and decelerates during exhalation. Breathing at a certain respiratory rate—in general between 4.5 and 6.5 cycles per minute (resonance frequency)—stimulates the cardiovascular system’s resonant properties, producing larger oscillations of heart rate, leading to higher HRV in individuals and other beneficial effects, such as better gas exchange (Yasuma and Ichiro Hayano, 2004).
The other mechanism of HRV-BF is the stimulation of the baroreflex, which is also vagally regulated and responsible for blood pressure (BP) homeostasis. Upon an increase in BP, the baroreflex induces a rapid adjustment in heart rate, reducing the blood flow and, subsequently, lowering BP (Lehrer, 2013). Again, when breathing at the resonance frequency, the RSA stimulates the baroreflex, thus strengthening its sensitivity. Therefore, HRV-BF training stimulates parasympathetic activity through both RSA and baroreflex, thus enhancing autonomic functioning (Lehrer, 2013).
The HRV-BF applications are diverse; importantly, it has been considered an effective intervention to reduce stress and anxiety (Yu et al., 2018; Kennedy and Parker, 2019), to mitigate posttraumatic stress symptoms (Schuman and Killian, 2019), and to reduce symptoms of depression (LinMei et al., 2019; Pizzoli et al., 2021). It was also proposed as a promising intervention to reduce physiological distress in healthcare workers (HCWs) in the COVID-19 pandemic (Aristizabal et al., 2020); however, there is no evidence in this context yet. Seeking to fill this gap and considering that frontline HCWs constitute a vulnerable group, especially with the emergence of the COVID-19 pandemic (Giorgi et al., 2020; Pappa et al., 2020; Sobregrau Sangrà et al., 2022), the current study applied an HRV-BF protocol in this population.
The main aim of this study is to propose and validate an objective procedure to easily assess the effectiveness of mental health interventions, specifically in this study of a personalized HRV-BF protocol in mitigating mental health symptoms in frontline HCWs who worked in the COVID-19 pandemic. For this purpose, we designed a PRE and POST experimental study based on two different approaches of psychological assessments. First, considering the gold-standard psychometric questionnaires and second, applying a recently developed electrophysiological multiparametric model that has been validated to assess chronic stress levels. As a secondary objective, we propose to investigate whether an acute stress model can distinguish the different stages of physiological response assessment (baseline, stress exposure, and recovery), and also the most relevant variables for this purpose in this population.
Twenty-one frontline HCWs were included in this study between March and July 2021, recruited from two Spanish tertiary hospitals: Hospital Clínic of Barcelona and Hospital del Mar of Barcelona. The study was conducted at the Hospital Clínic of Barcelona, and the protocol was approved by its Ethics Committee. All participants gave a written informed consent.
The inclusion criteria were to be a HCW directly involved with care of COVID-19 patients during the pandemic. The selection was made according to a high risk of developing post-traumatic stress disorder or a moderate perception of stress and/or anxiety according to cutoff points of current gold-standard questionnaires (i.e., a score of 30 or higher on PCL5; 14 or higher on PSS; and 10 or higher on STAI-S) and voluntarily agreeing to participate.
The HRV-BF protocol was designed based on (Lehrer et al., 2013) and comprises 5 weekly in-person sessions of 45–60 min, including specific instructions for daily practices. Each session was held individually in a quiet room conducted by a trained professional and scheduled according to participant availability. If a participant could not attend one of the sessions, it was rescheduled for as soon as possible in order to complete the protocol and to prevent a longer interval between sessions from compromising adherence to practice. Figure 1 shows the organization of the overall protocol by sessions.
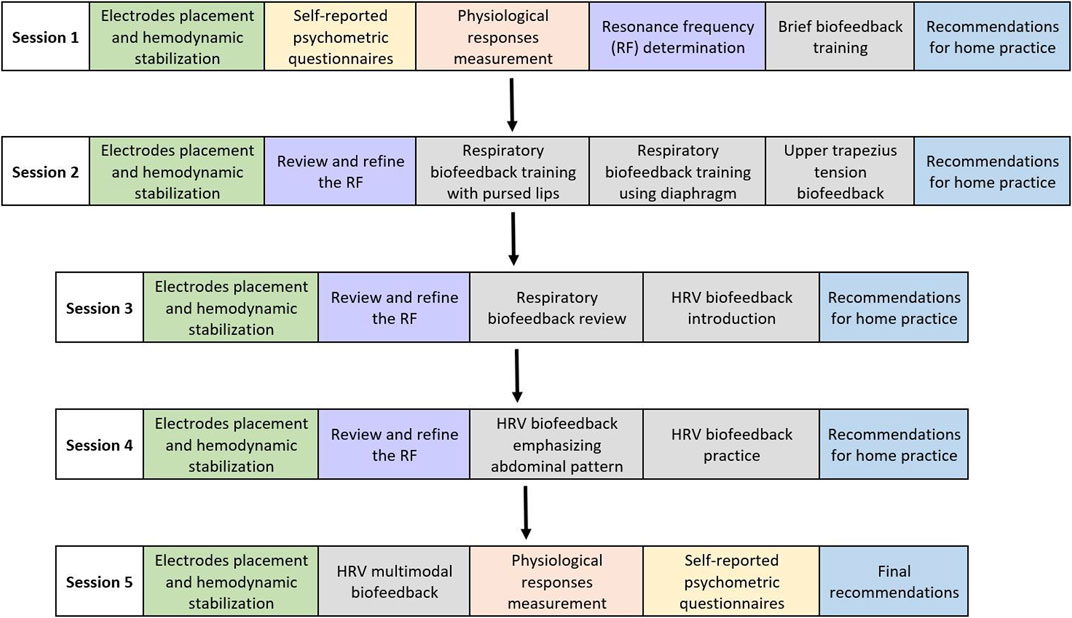
FIGURE 1. Scheme of the 5-session experimental protocol. The colors identify the different steps in each of the sessions. Those marked in gray represent the biofeedback training.
Participants provided information on demographics, working conditions, psychological background, use of medication, and social habits. Self-reported psychometric questionnaires (yellow blocks shown in Figure 1) were collected, and a physiological response measurement (salmon-colored blocks) was carried out prior to (PRE) and immediately after (POST) the HRV-BF training to perform comparisons.
In the first session, preceding the training, the individual’s resonance frequency (RF), i.e., the optimal breathing rate, was determined based on the following criteria: phase synchrony between respiration and HR and signal smoothness, maximal HRV (higher peak–trough amplitude), greater power in low-frequency (LF) band, and a peak around 0.1 Hz on the LF band (Lehrer et al., 2013; Shaffer and Meehan, 2020). RF was revised and fine-tuned in the following sessions (lilac-colored blocks).
In sessions 2, 3, 4, and 5, the biofeedback training (gray blocks) was focused on specific breathing techniques, such as pursed lips and diaphragmatic breathing, guided by respiration and heart rate variability real-time waves displayed by using BioTrace + software (Mind Media, 2018 version). Participants were instructed to practice specific breathing exercises daily for 10–20 min (blue blocks). For home practice, the given recommendations increased the difficulty level at each session: week 1: starting with brief periods of slow breathing practice with a pacer to correctly follow the rhythm of the individual’s resonance frequency. The pace of breathing would become more fluid and comfortable for the participant, and the practice time would be gradually increased; week 2: same as the previous one and adding diaphragmatic breathing awareness exercises, such as placing one hand over the abdomen and the other over the chest and breathing in such a way that the hand over the abdomen moves and the other is as still as possible. It could be performed lying down to facilitate the perception of the movement; week 3: performing the same exercise as before without using the hands and more frequently in a sitting position. One must start practicing using the pacer and then performing brief periods of free practice; week 4: performing breathing without using the pacer whenever they feel safe following the already incorporated rhythm; then one must start applying it on day-to-day activities. In case of insecurity to do it freely, they should start the practice with the pacer and try to perform in short free periods and gradually increase the duration; week 5: it is recommended to continue performing slow breathing on a daily basis and applying it in everyday situations, especially after or before a stressful event. The importance of daily practice to achieve physiological and long-term benefits is emphasized to engage the participants. The use of free applications on their mobiles was encouraged to practice RF at home with a pacer (Paced Breathing for Android and Awesome Breathing: Pacer Time for iOS).
Self-reported psychometric questionnaires consisted of gold-standard psychological questionnaires in validated Spanish versions to examine stress, anxiety, and depression under PRE–POST conditions. Stress was examined using the Perceived Stress Scale (PSS) (Remor, 2006) and the Visual Analog Stress Scale (VASS) (Lesage et al., 2012). The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL5) was applied as a screening for post-traumatic stress disorder (PTSD) symptoms (Blevins et al., 2015). Anxiety symptoms were evaluated using the State-Trait Anxiety Inventory (STAI) (Spielberger et al., 1983), while to assess depression, the Patient Health Questionnaire-9 (PHQ9) was used (Diez-Quevedo et al., 2001). All instrument descriptions are given in Table 1.
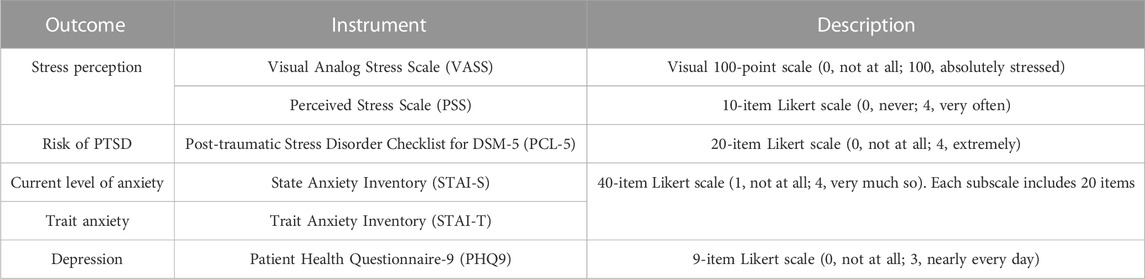
TABLE 1. Self-reported instruments used to assess the outcomes.
The reliability of these questionnaires was assessed for the study sample by Cronbach’s alpha, and estimates were all above 0.85, thus showing a high degree of internal consistency (O’Rourke and Hatcher, 2013).
Physiological monitoring provided an insight into differences in autonomic functioning in a stress-inducing situation before and after the intervention. The participants were asked to be seated in a comfortable chair with armrests and eyes open. The physiological response measurement was analyzed in three different stages: 1) baseline measurement (BM), taken as a reference when the participant is in a resting state; 2) stress exposure (SE), to evaluate the physiological reactivity facing stressors; and 3) recovery measurement (RM) to assess resilience after stressors.
The SE stage included three different stressors: a) 2-min Stroop task (originally Stroop, 1935), with an incongruent stimulus, in which the colors were written in an ink that does not match the color-word, and the participant should inform the color of the ink; b) 2-min mental arithmetic task (Kirschbaum et al., 1993), which consisted of performing mental calculations as quickly and accurately as possible; in case of an error, the participant should start over; c) 2-min telling about the experience of working on the frontlines of the COVID-19 pandemic and the feelings they could report (detailed in Figure 2). Differences between stressors were not analyzed in this study.
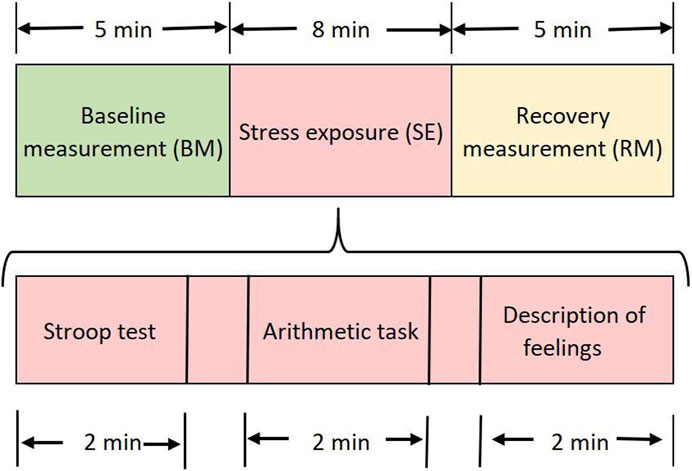
FIGURE 2. Schematic procedure for physiological response measurement PRE- and POST-intervention.
The electrophysiological data were recorded using the NeXus-10 MKII device (Mind Media BV, Herten, Netherlands) and the real-time waves displayed by Biotrace+ software (Mind Media, 2018 version) during each of the sessions. Electrocardiogram (ECG), photoplethysmogram (PPG), electrodermal activity (EDA), skin temperature (ST), and respiration (Resp) were signals simultaneously gathered. The electromyogram (EMG) of the upper trapezius muscle was monitored only for bringing awareness of muscular activation during breathing, although this signal was not included in the study analyses.
For the EDA, disposable electrodes were affixed to the palmar surface of the middle phalanges of the second and fourth digits; for PPG, the clip sensor was placed on the middle finger, and on the fingertip of the fifth finger was attached the ST sensor. The electrode was placed in the non-dominant hand to avoid excessive movements and possible large artifacts.
For lead 1 of the ECG signal, electrodes were placed below the right collarbone and below the left rib cage, whereas for lead 2, electrodes were placed on the fifth intercostal space along the mid-axillary line on the left and the other symmetrically on the right side. The reference electrode was placed on the left collarbone.
To monitor the Resp signal, an adjustable elastic band was placed over the abdomen and over clothing. This sensor detects abdominal expansion/contraction; for instance, when inhaling, the device stretches, and during exhalation, the sensor returns to its neutral position.
Simultaneously, the PPG, EDA, and ST signals were monitored through the Empatica E4 wearable wristband (Empatica Boston, United States). These data will be explored in further analysis looking for a more easy and unobtrusive way to assess the effectiveness of interventions, considering the number of HRV-BF sessions and the interval between them.
The different electrophysiological raw signals mentioned were analyzed in a 1-min window using BioSig browser in MATLAB software (Garzón-Rey et al., 2017), and several variables were extracted from each one of them as described in Table 2. For comparisons, the mean of all 1-min segments was computed as a single value per stage for each subject.
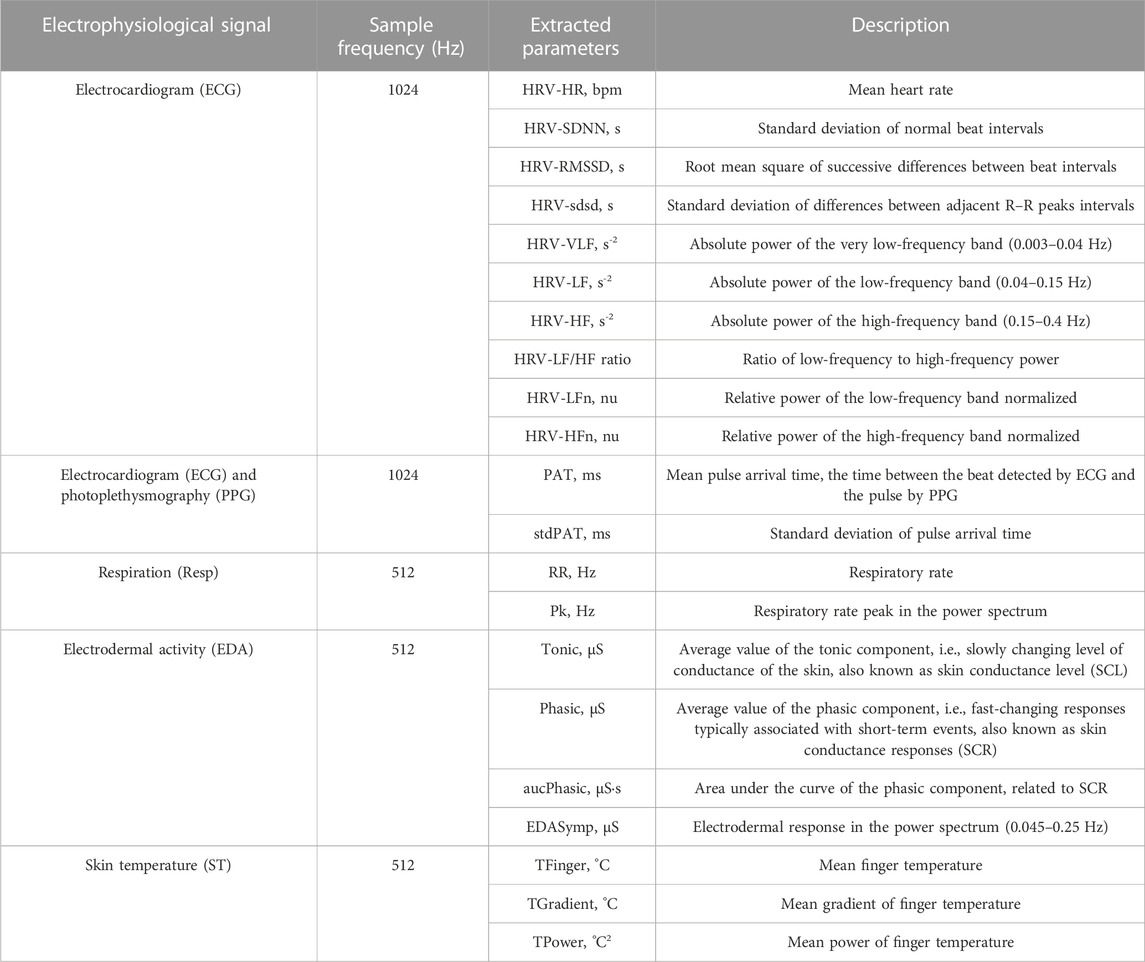
TABLE 2. Description of extracted parameters from electrophysiological variables.
In this study, the PPG signal will be used in conjunction with that of ECG to extract pulse arrival time (PAT) parameters. To extract HRV parameters, the ECG signal was chosen since it provides more accurate measurements.
From the ECG signal, the beat was detected through a discrete wavelet transform (Martínez et al., 2004). Given the robustness of the algorithm and the visual inspection of the quality of the ECG signals, no type of filtering was applied. Afterward, the existence of ectopic beats or false QRS detections was verified and fixed using the algorithm reported in Mateo and Laguna (2003) prior to the computation of the RR series. The algorithm searches for sudden changes in interbeat intervals, performs an interpolation where it has found non-normal beats, and based on this, proposes a correction to them. Segments of up to three interpolated/corrected beats have been accepted and are assumed to be normal. Following this, a time-domain analysis was performed to extract the mean heart rate (HRV-HR) in beats per minute; the standard deviation of differences between adjacent normal peak intervals (HRV-SDNN); and the root mean square of successive differences between beat intervals (HRV-RMSSD). For the frequency-domain analysis, the low- and high-frequency absolute powers (HRV-LF and HRV-HF, respectively) were computed from the spectral density of the HRV signal, calculated using Fourier transform. The HRV signal is obtained by subtracting from the instantaneous HR signal, a low-pass-filtered HR signal (cutoff frequency of 0.03 Hz), which mainly explains the changes in mean HR. The HRV–LF/HF ratio was computed by the ratio between absolute power in low- and high-frequency bands, i.e., HRV-LF/HRV-HF. The HRV-LFn and HRV-HFn represent the low- and high-frequency power normalized, respectively.
The PPG signal was filtered using a low-pass FIR filter with a cut-off frequency of 35 Hz (order 50) and, then, a high-pass FIR filter with a cut-off frequency of 0.3 Hz (order 5000). PPG artifacts were suppressed through a Hjorth-parameter-based PPG artifact detector described in Gil et al. (2009). Pulses were detected from the PPG signal on those time slots without artifacts by an algorithm based on Lazaro et al. (2014). Subsequently, the mean time difference between the R peak in the ECG signal and the point of 50% increase, corresponding to the pulse detected on the finger by the PPG signal, was considered the pulse arrival time (PAT), and its standard deviation (stdPAT) was also calculated.
The respiratory rate (RR) was estimated as the frequency to which the maximum peak (Pk) of the power density spectrum corresponds, estimated by means of fast Fourier transform (Lázaro et al., 2014). When the Pk was greater than 65%, then the RR was accepted as the respiratory rate. The respiration wave was filtered with an FIR passband filter with cutoff frequencies of 0.03 and 0.9 Hz. In 10 participants, the Resp parameters could not be calculated during the SE because they did not meet the condition aforementioned, probably due to the speech during the task, which affects the signal quality. The missing values were replaced by median imputation to perform the comparisons between stages.
The EDA signal was visually inspected to delete motion artifacts and linearly interpolated. The windows with interpolated segments larger than 25% were discarded, and the signal was then resampled at 4 Hz. Then, EDA was processed in two different ways. First, a time-domain analysis was conducted using a convex optimization model, called cvxEDA (Greco et al., 2016), which decomposes the signal as a linear combination of the tonic and phasic components (i.e., the skin conductance level and response, respectively) and some noise (incorporating the error of the model, artifacts, and other measurement errors). The average value of the tonic (Tonic) and phasic (Phasic) components and the area under the curve of the phasic component (aucPhasic) were calculated. The second way was a frequency-domain analysis of EDA, proposed to assess sympathetic tone through a parameter named EDASymp (Posada-Quintero et al., 2016). In this analysis, the EDA signal was filtered with an FIR bandpass filter with 0.01 and 0.9 Hz cutoff frequencies, and the power of the electrodermal response in the band 0.045–0.25 Hz (EDASymp) was computed. This bandwidth has been reported to correspond to sympathetic dynamics in non-exercise conditions.
Finally, for the skin temperature signal, visual inspection showed that the recorded signals did not contain significant artifacts; therefore, no pre-processing was needed. Apart from the skin temperature average value (TFinger), the gradient of the successive differences of TFinger every 10 s was calculated (TGradient), indicating the speed of temperature change. In relation to the amplitude, the power of the signal calculated as the mean of the square of the signal (TPower) is used.
For a more robust estimation of the stress level, we used two different models a) to assess the chronic stress level (Aguiló Mir et al., 2021), called electrophysiological signal-based stress model (ESBSm) and b) to assess the acute stress level, called ES3 (Garzón-Rey, 2017). These models were calculated from the variables extracted from the electrophysiological signals explained in the previous section.
The chronic stress level model (ESBSm) was designed to match up with a reference scale including psychometric questionnaires and biochemical variables, taken as a gold-standard indicator of stress response. ESBSm includes 11 standardized parameters extracted from ECG, Resp, and EDA and a few quadratic terms. Some parameters are previously logarithmically transformed to avoid data skewness effects. In the present study, this model is applied as an instrument to assess the effectiveness of the HRV-BF protocol since it allows detecting changes in the chronic stress level over time.
The acute stress level model (ES3) also fits the results of psychometric questionnaires and biochemical biomarkers in a sample subjected to an induced acute stress task. The ES3 includes four parameters extracted from ECG, EDA, and ST. In the present study, ES3 is used to assess whether changes occur between the different stages (BM, SE, and RM). As with the previous model, the analysis was also performed comparing values in PRE and POST conditions.
A descriptive statistical analysis was performed to summarize the sample characteristics. Continuous variables are presented as mean and standard deviation (SD), and categorical variables are presented as frequency and percentages.
For the psychometric questionnaires and chronic stress model (ESBSm) data, differences in PRE–POST intervention were evaluated with paired t-tests or Wilcoxon signed-rank tests, according to data distribution.
For the electrophysiological variables, in order to compare conditions (PRE and POST) and stages (BM, SE, and RM), a mixed model (repeated measures analysis of variance, ANOVA) was used. The compliance of the application criteria was assessed with the analysis of model residuals. Skewed variables were analyzed using log-transformation.
Post-hoc tests with Tukey’s correction were performed to assess the time and stage effects on physiological variables and on the acute stress model (ES3). A p < 0.05 was considered statistically significant. Statistical analysis was performed using SAS® v9.4 (SAS Institute, Cary, NC, United States).
The study sample consisted of 21 female participants who completed the protocol in an average of 36 ± 11.4 days. The daily practice accomplishment was 62.28% (±19.1) regarding overall target home practice of 28 days. The mean age was 37.7 ± 11.7 years (range: 19–59 years), with an average body mass index of 24.2 ± 3.8 kg/m2. Most of the participants were nurses (61.9%), followed by physicians (28.6%) and auxiliary nurses (9.5%). All sociodemographic and clinical information is detailed in Table 3.
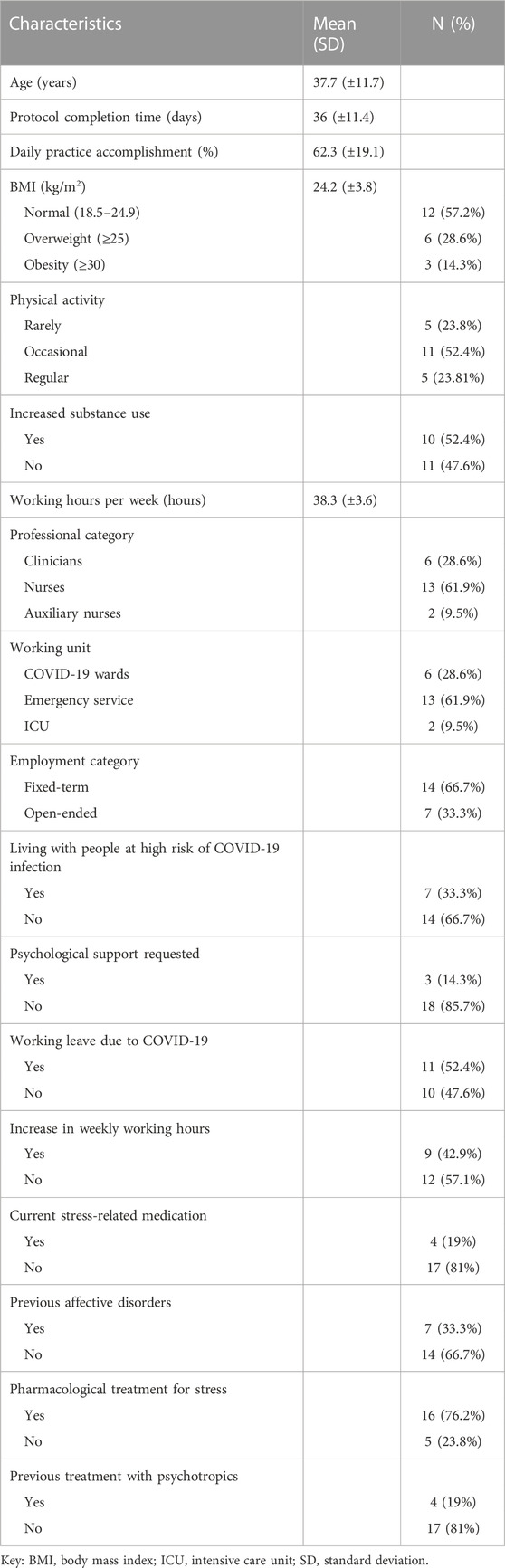
TABLE 3. Clinical and sociodemographic characteristics of participants.
Figure 3 shows the classification PRE- and POST-intervention of each psychometric questionnaire according to the cut-off points of previous studies (Aguiló Mir et al., 2021; Pedrozo-Pupo et al., 2020; Blevins et al., 2015; Kroenke et al., 2001). The classification is generally in three categories considering the degree of severity as low, moderate, or high, and in two categories for the PCL5 that classifies those with high or low risk of developing PTSD.
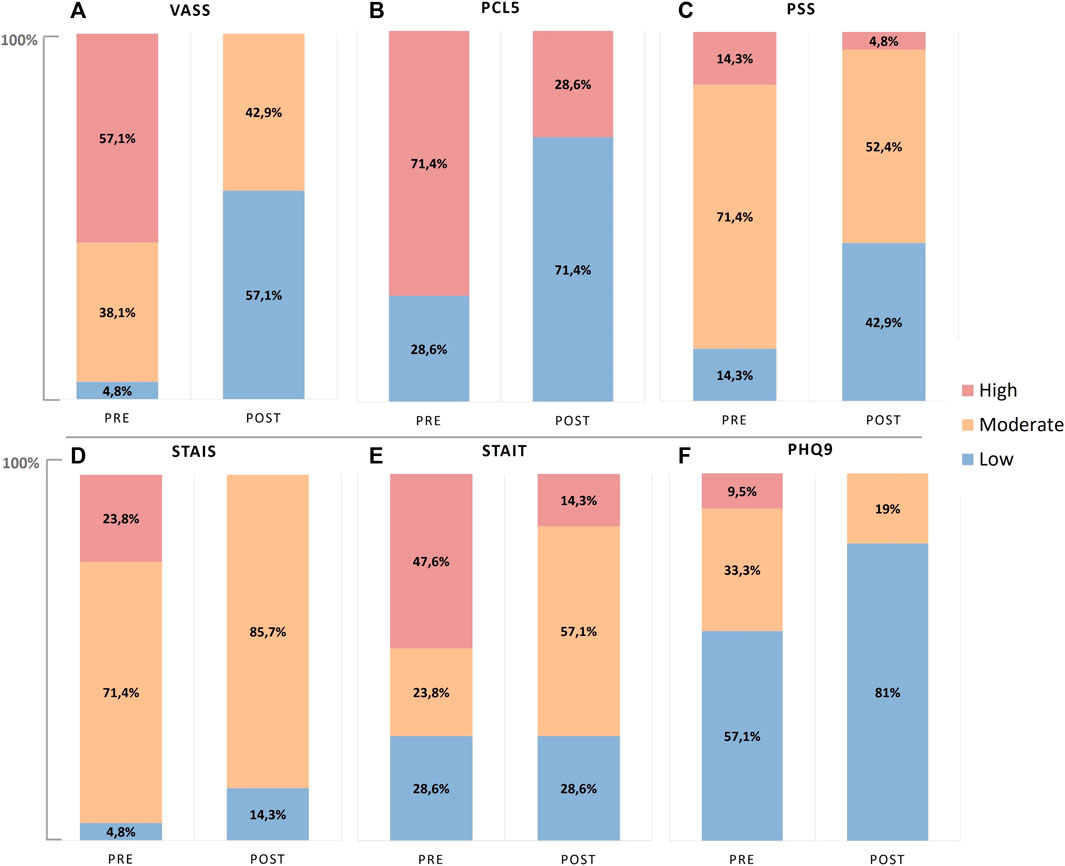
FIGURE 3. Severity classification of subjects based on the psychometrics cut-off points at PRE- and POST-intervention. (A) Stress perception with the Visual Analog Stress Scale (VASS), (B) risk to develop PTSD with Posttraumatic Stress Disorder Checklist for DSM-5 (PCL5), (C) perceived stress with the Perceived Stress Scale (PSS), (D) anxiety state with State Anxiety Inventory (STAI-S), (E) anxiety trait with Trait Anxiety Inventory (STAI-T), and (F) depression with Patient Health Questionnaire-9 (PHQ9).
In the PRE-intervention condition, the study sample presented predominantly high anxiety trait scores (47.6%), moderate anxiety state (71.4%), and moderate perceived stress (71.4%) and showed increased risk of developing PTSD (71.4%). Regarding the depression level, most were classified within the low range (57.1%), while two individuals (9.5%) showed scores for severe depression. After intervention, all these profiles improved; the risk of PTSD reduced to 28.6%, the majority presented low symptoms of depression (81%), while the moderate group showed reduction from 33.3% to 19%. In addition, substantial shifts from high to moderate anxiety and perceived stress can be observed.
From the bivariate analysis, the psychometric questionnaires showed a reduction in all scores after intervention, with exception of the STAI-T, which did reduce even though without statistical significance (p = 0.147). Comparisons between PRE- and POST-intervention are shown in Table 4.
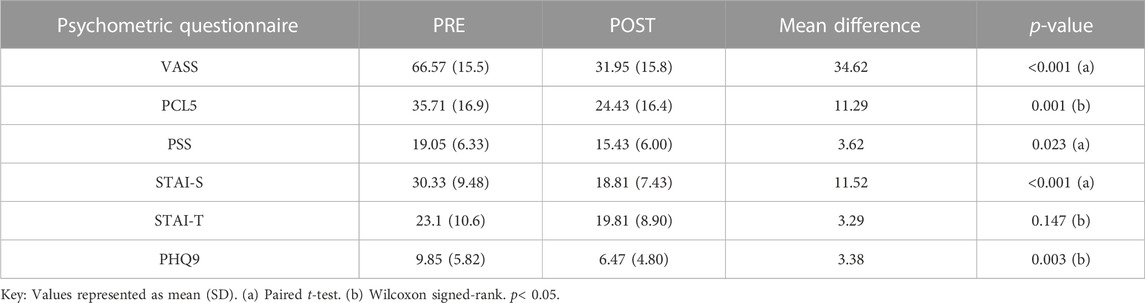
TABLE 4. PRE–POST psychometric questionnaire scores and corresponding statistical analysis.
As exploratory analyses, we examined whether PRE–POST changes are influenced by age, BMI, physical activity, and daily practice. There are no significant findings. However, there is an effect related to the initial condition, i.e., those with high initial scores are more likely to show improvement in self-reported questionnaires (VASS: p = 0.003; PSS: p = 0.016; PCL5: p = 0.036; PHQ9: p = 0.016; STAI-S: p < 0.001), apart from STAI-T (p = 0.081).
For PRE–POST comparisons, the baseline measurement (BM) was considered to mimic the conditions of the ESBSm chronic stress study. Figure 4 illustrates a reduction (77.6 vs. 62.8) found in the chronic stress level in POST-intervention when compared to PRE-intervention (paired t-test, p = 0.01), while the variance increased.
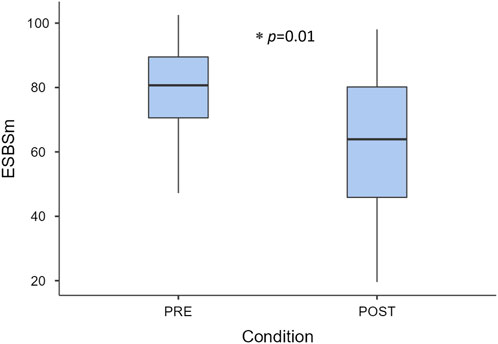
FIGURE 4. Chronic stress level at PRE- and POST-intervention measured by the multiparametric chronic stress model (ESBSm). Key: p < 0.05.
Similar to self-reported questionnaires, there is a significant effect related to the initial condition in the ESBSm results (p = 0.016), and no effect for age, BMI, or physical activity.
The bivariate analysis revealed some significant differences (Table 5), such as a decrease in mean respiratory rate from 0.259 to 0.222 Hz (i.e., 15.5 to 13.3 breaths per minute) and an increase in HRV-SDNN, HRV-LF/HF, and HRV-LFn, with no differences for HRV-RMSSD.

TABLE 5. Electrophysiological measure comparisons and corresponding statistical analysis.
No significant changes in PAT and peripheral temperature parameters were observed. For EDA, the phasic component showed an increase (p = 0.012), whereas the average of the tonic component decreased POST intervention, although not significantly (p = 0.199).
Differences in physiological response measurement, i.e., between the baseline measurement (BM), stress exposure (SE), and recovery measurement (RM), were analyzed to visualize possible changes in the behavior of the signals during a stress-induced task. All mean values and respective p-values could be seen in Supplementary Table S1. The most relevant variables are illustrated on the following plots. Some of them were log-transformed for a better visual representation and were indicated with (log) in the axis title.
The resting heart rate (HRV-HR) and pulse arrival time (PAT) showed significant differences in BM and RM stages when compared to SE (p < 0.001) under both conditions (Figures 5A, D, respectively). The HRV-SDNN changed its pattern, where BM differed from RM and SE stages in the PRE-intervention condition, which was not seen after intervention (Figure 5B). In the POST-intervention condition, SDNN values at baseline increased significantly (p = 0.027).
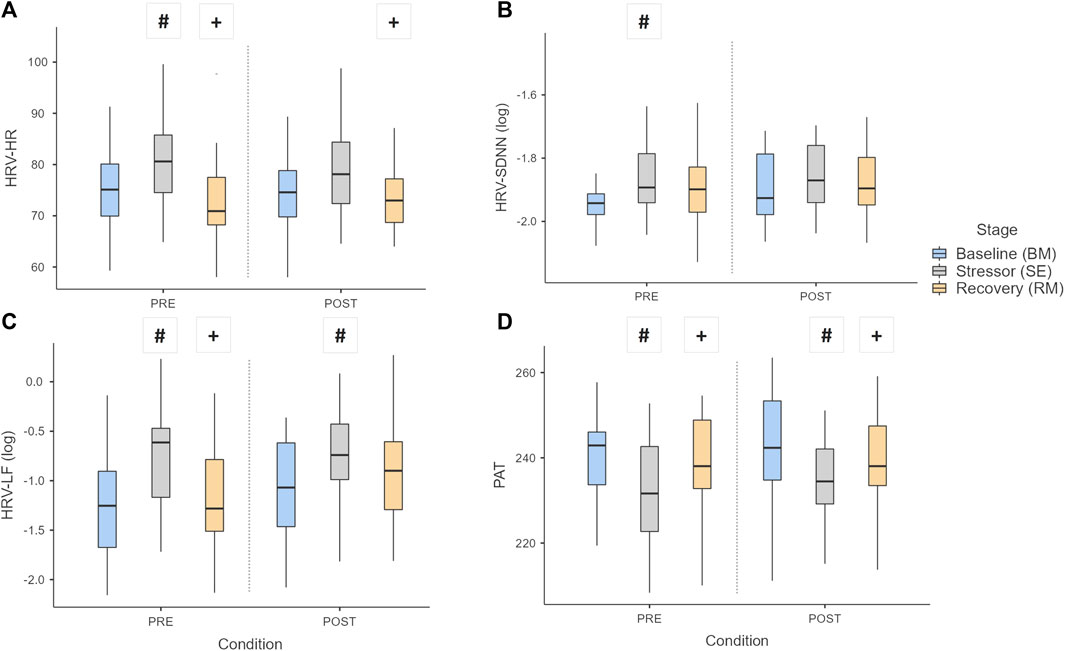
FIGURE 5. Boxplot of HRV parameters: (A) HR, (B) SDNN, (C) LF, and (D) PAT over the stages and conditions. Key: Light gray boxes show the significant differences between stages for each condition. (#) Differences between BM and the other stages (SE or RM). (+) Differences between RM and SE stages. p < 0.05.
Figure 5C shows the behavior of the power in low-frequency band (HRV-LF), revealing differences between RM and SE at PRE-intervention, which did not occur after intervention.
Figure 6 shows the pattern of EDA and ST parameters. The tonic component (Tonic) of EDA showed differences between the BM and the other stages (p < 0.001) in both conditions (Figure 6A); furthermore, values at SE and RM reduced significantly POST intervention (p = 0.047 and p = 0.021, respectively). The phasic component (Phasic) and EDASymp differed between stages (p ≤ 0.001), but only Phasic showed difference in BM after intervention (p = 0.012). Regarding skin temperature, the gradient (TGradient) showed differences between the BM and RM stages in relation to the SE, in exception to RM vs. SE under POST condition (Figure 6D).
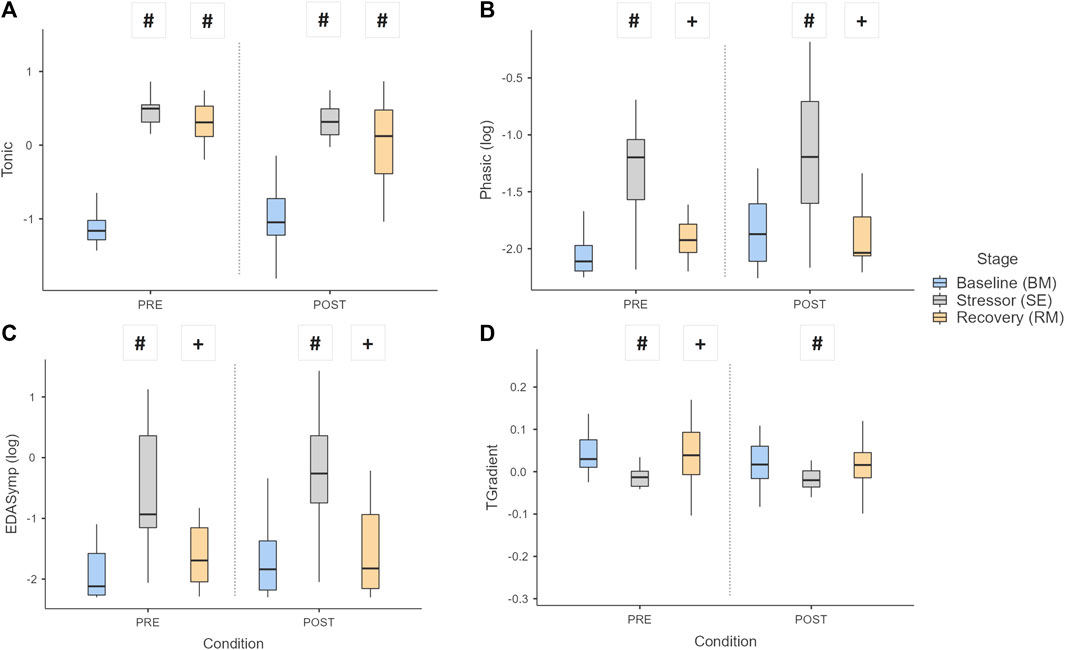
FIGURE 6. Boxplot of EDA and ST parameters: (A) Tonic, (B) Phasic, (C) EDASymp, and (D) TGradient, over the stages and conditions. Key: Light gray boxes show the significant differences between stages for each condition. (#) Differences between BM and the other stages (SE or RM). (+) Differences between RM and SE stages. p < 0.05.
No differences related to respiration were observed between stages (Figure 7A), although the respiratory rate was overall reduced after the intervention, significantly only in BM (p = 0.007). The ES3, the model to assess acute stress, did not reveal differences between stages, although the scores were all lower after intervention (Figure 7B).
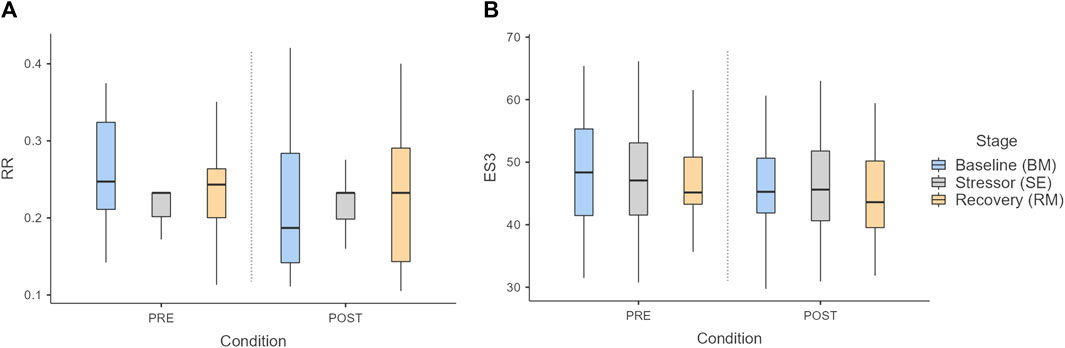
FIGURE 7. Boxplot of (A) respiratory rate (RR) and (B) ES3 acute stress model over the stages and conditions. Key: p < 0.05.
Our study applied a new objective tool, the chronic stress multiparametric model (ESBSm), to assess the effectiveness of a 5-session HRV-BF protocol for HCWs presenting mental health symptoms due to their work in the frontlines of the COVID-19 pandemic. The improvement in mental health is corroborated by lower scores on self-reported psychometric questionnaires after intervention, reducing stress, risk of post-traumatic stress disorder, and symptoms of anxiety and depression. These results are consistent with those of previous studies that use similar instruments to assess the impact on mental health as published in this review (Di Nota et al., 2021), with some studies in conjunction with an enhancement of certain physiological biomarkers, such as heart rate variability. Thus, the results obtained in the procedure using the ESBSm support the hypothesis that a combined electrophysiological model provides useful and robust information about mental health state and could be considered to assess non-invasively changes over time.
Furthermore, the acute stress model (ES3), applied to compare physiological reactivity at baseline, stressor, and recovery measurements, showed an overall decrease after intervention, although nonsignificant. Unlike the chronic stress model, which aims to find differences in cumulative stress, this model investigates differences in acute physiological responses caused by stress-inducing tasks. As expected, there was an increase in the ES3 score when facing a stressor and a reduction in resting periods, in both conditions. This behavior indicates that the intervention did not affect the acute stress response in the studied sample.
Regarding the electrophysiological variables, a reduction in the basal respiratory rate is observed, which indicates that the participants were able to self-regulate their breathing, and this is helpful to stress management and to recover the autonomic balance. Additionally, this improvement in respiratory rate leads to better gas exchange and less chance of hyperventilation, which often occurs in disorders such as anxiety (Leyro et al., 2021). Our analysis related to respiration during the stress-inducing tasks were compromised once the tasks involved speech, so the data did not present the expected increase in respiratory rate which was observed in other types of stressors, like cold or heat exposure (Tipton et al., 2017).
An improvement in some HRV parameters, such as standard deviation of normal beats (SDNN) and power in low frequency (LFn), was also observed. These parameters are often used to assess the effectiveness of biofeedback intervention as they are considered ANS biomarkers. SDNN varies especially due to RSA, which is mediated by the parasympathetic system and precisely trained in HRV-BF, so an increase in this parameter indicates a successful intervention (Limmer et al., 2021). Furthermore, the LF power is influenced by both sympathetic and parasympathetic branches of the ANS, but reflects baroreflex activity in resting conditions (McCraty and Shaffer, 2015). Differences on the HRV-LFn may be related to the changes in respiratory rate since the low-frequency band (0.04–0.15 Hz) is influenced by breathing at 9 bpm or lower (Shaffer and Ginsberg, 2017). In this sense, the increase in LF power is expected after HRV-BF and corroborates the results shown in previous studies (Gross et al., 2016; Hasuo et al., 2020).
The pulse arrival time, which is an index that varies inversely with blood pressure, showed a decrease during the stress-inducing task when compared to baseline and recovery measurements. This pattern is in accordance with previous studies that demonstrated this reactivity in healthy students during a similar protocol for stress elicitation (Armañac et al., 2019; García Pagès et al., 2023). Concerning the skin temperature, no differences were observed after the intervention. All the parameters extracted from this signal showed the same expected pattern, reducing during the stress exposure and recovering afterward (Pisanski et al., 2018).
The variations of electrodermal activity (EDA) in our sample may correspond only to central nervous system modulation related to emotional and cognitive states of the individuals, once the environmental temperature interference can be discarded as the skin temperature did not vary over time (Sarchiapone et al., 2018). The phasic component of the EDA revealed differences after the intervention. This component, which corresponds to faster-changing activity, increased at baseline measurement, which indicates an augmented sympathetic arousal, on the contrary to what was expected after the intervention (Greco et al., 2021). We hypothesize that the participants anticipated their stress responses once they knew the elicitation tasks they were going to perform (i.e., Stroop test, arithmetic task, and description of feelings). Even so, it is important to highlight that both parameters extracted from the phasic component and the EDASymp were capable of distinguishing between the stressor of basal and recovery measurements. On the other hand, the tonic component of EDA showed an awaited pattern, increasing during the stress task, and a slower recovery time, seeming to accelerate slightly after the intervention, but still differing significantly from the baseline stage. During the stress exposure and recovery stages, the tonic level reduced significantly after intervention, which suggests an improvement in psychophysiological state and autonomic regulation (Marzi et al., 2021).
To summarize, the multiparametric chronic stress model comprises information of a combination of the most relevant physiological variables altogether, and their scores were in accordance with psychometric gold standards, therefore demonstrating to be a simple and objective tool to assess the effectiveness of a specific therapy. This procedure can be especially useful and easily applied in clinical practices, thus allowing to plan and properly combine different types of interventions for a more assertive treatment.
In the current study, the HCWs’ adherence was satisfactory, and they reported feeling motivated throughout the biofeedback protocol, which reinforces the feasibility of the intervention in this context and the importance of implementation by the health facilities as a preventive program. Moreover, HRV-BF is a proactive intervention that easily allows a multimodal measurement of electrophysiological parameters, ensuring the feasibility of the chronic stress model to assess its effectiveness and, more extensively, of other stress-reducing interventions.
Further research could replicate the proposed method in case-control studies and other interventions to confirm its efficacy for particular applications. To make the procedure even easier and unobtrusive, a remote wearable device may be used to monitor the mental status in real-time and to assess the effectiveness of interventions more extensively. A remote monitoring device would allow a longer follow-up and could be helpful in investigating other sources of stress and identifying protective and risk factors.
One limitation of this study is that the recruited sample comprises only women; therefore, it is not possible to extrapolate our findings related to the effectiveness of HRV-BF for men. Second, the relatively small sample size (n = 21) is analyzed, which could be reflected in statistically nonsignificant results and thus increasing the risk of type II error (i.e., false negatives).
The PRE–POST experimental design does not prevent us from bias and limit the interpretation of the results. For this reason, we could not generalize the effectiveness of the applied intervention, which would be feasible in a case-control study, although, as an advantage, the present study design with paired comparisons avoids the influence of interpersonal variations of the electrophysiological variables. In order to use the multiparametric chronic stress model (ESBSm) proposed by Aguiló Mir et al. (2021), we assumed that the variability and severity of samples in both studies were similar and applied our standardized data to calculate the chronic stress level. The necessary corrections were also made in EDA parameters due to calibration problems related to the measuring device.
There was no follow-up to observe if the effects remained long-term after withdrawal of biofeedback. Further studies should be considered to assess the durability of the effects.
Our study demonstrates that a 5-session HRV-BF protocol is an effective intervention to reduce stress, the risk of post-traumatic stress disorder, and symptoms of anxiety and depression among our group of frontline HCWs who worked during the COVID-19 pandemic. Our findings support that the chronic multiparametric model based on electrophysiological variables provides relevant information about the current mental health status, being a reliable objective tool to assess the effectiveness of HRV-BF and may be useful for other stress-reduction interventions and contexts of burden in mental health. The variance increase in the model’s scores after the intervention indicates that the effectiveness of the intervention depends on each individual; therefore, a systematic measurement should be crucial for follow-up and treatment decisions. Further research should examine the robustness of these findings controlling possible confounders and, in addition, could investigate the reliability of wearables in providing feedback and monitoring physiological responses, which would constitute a more unobtrusive and easier-to-use instrument to reproduce the proposed procedure.
The raw data supporting the conclusion of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Ethical Committee of the Hospital Clínic of Barcelona. The patients/participants provided their written informed consent to participate in this study.
The concept and design of the study were conducted by TCR, SA, EGP and JA. TCR, PSS and SA recruited the volunteers, carried out the experiments, and collected the data. Critical revision and contribution of scientific knowledge contribution were provided by BL-B, SA and JA. The relevant data analysis and statistical analysis were performed by TCR, PSS and LB. TCR wrote the manuscript with contributions from SA, EGP, PSS and JA. All authors contributed to the article and approved the submitted version.
This work was supported by the Fondo Supera COVID, funded by the Santander Bank, Conference of Rectors of Spanish Universities (CRUE) and Spanish National Research Council (CSIC).
We would like to thank healthcare workers all over the world for tirelessly fighting the coronavirus on the frontline, and especially those from the Hospital Clínic of Barcelona and Hospital del Mar for collaborating with the scientific study carried out.
Since 16th June 2022, the co-author PSS has been employed by Frontiers Media SA. PSS declared his/her affiliation with Frontiers, and the handling Editor states that the process nevertheless met the standards of a fair and objective review.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphys.2023.1147260/full#supplementary-material
Aguiló Mir, S., García Pagès, E., López Barbeito, B., Castro Ribeiro, T., Garzón-Rey, J. M., and Aguiló, J. (2021). Design and validation of an electrophysiological based tool to assess chronic stress. Case study: Burnout syndrome in caregivers. Stress 24 (4), 384–393. doi:10.1080/10253890.2020.1807512
Ahmed, A., Ali, N., Anna, G., Abd-alrazaq, A. A., Aziz, S., and Househ, M. (2021). Mobile applications for mental health self-care: A scoping review. Comput. Methods Programs Biomed. Update 1, 100041. doi:10.1016/j.cmpbup.2021.100041
Ahmed, T., Qassem, M., and Kyriacou, P. A. (2022). Physiological monitoring of stress and major depression: A review of the current monitoring techniques and considerations for the future. Biomed. Signal Process. Control 75, 103591. doi:10.1016/j.bspc.2022.103591
Aristizabal, J. P., Navegantes, R., Melo, E., and Pereira, A. (2020). Use of heart rate variability biofeedback to reduce the psychological burden of frontline healthcare professionals against COVID-19. Front. Psychol. 11, 572191. doi:10.3389/fpsyg.2020.572191
Armañac, P., Kontaxis, S., Lazaro, J., Laguna, P., Bailón, R., and Gil, E. (2019). Cardiovascular changes induced by acute emotional stress estimated from the pulse transit time difference” in 2019 computing in cardiology conference (CinC), Comput. Cardiol. 46, 1. doi:10.22489/CinC.2019.383
Arza, A., Mario Garzón-Rey, J, Lázaro, J, Gil, E, Lopez-Anton, R, de la Camara, C, et al. 2018. “Measuring acute stress response through physiological signals: Towards a quantitative assessment of stress.” Med. Biol. Eng. Comput., 57, 271. doi:10.1007/s11517-018-1879-z
Billman, G. E. (2013). The LF/HF ratio does not accurately measure cardiac sympatho-vagal balance. Front. Physiology. Billman 4, 26. doi:10.3389/fphys.2013.00026
Blevins, C.A., Weathers, F. W., Davis, M. T., Witte, T. K., and Domino, J. L. (2015). The posttraumatic stress disorder checklist for DSM-5 (PCL-5): Development and initial psychometric evaluation. J. Trauma. Stress 28 (6), 489–498. doi:10.1002/jts.22059
Cairns, P., Aitken, G., Pope, L. M., Cecil, J. E., Cunningham, K. B., Ferguson, J., et al. (2021). Interventions for the well-being of healthcare workers during a pandemic or other crisis: Scoping review. BMJ Open 11 (8), e047498. doi:10.1136/bmjopen-2020-047498
Diez-Quevedo, C., Rangil, T., Sanchez-Planell, L., Kurt, K., and RobertSpitzer, L. (2001). Validation and utility of the patient health questionnaire in diagnosing mental disorders in 1003 general hospital Spanish inpatients. Psychosom. Med. 63 (4), 679–686. doi:10.1097/00006842-200107000-00021
Di Nota, P. M., Bahji, A., and Groll, D. (2021). Proactive psychological programs designed to mitigate posttraumatic stress injuries among at-risk workers: A systematic review and meta-analysis. Syst. Rev. 10 (1), 126. doi:10.1186/s13643-021-01677-7
Flores, E. C., Fuhr, D. C., Bayer, A. M., Lescano, A. G., Thorogood, N., and Victoria, S. (2018). Mental health impact of social capital interventions: A systematic review. Soc. Psychiatry Psychiatric Epidemiol. 53 (2), 107–119. doi:10.1007/s00127-017-1469-7
García Pagès, E., Arza, A., Lazaro, J., Puig, C., Castro, T., Ottaviano, M., et al. (2023). Psychosomatic response to acute emotional stress in healthy students. Front. Physiology 13, 2605. doi:10.3389/FPHYS.2022.960118
Garzón-Rey, J. M., Lázaro, J., Milagro, J., Gil, E., Aguiló, J., and Bailón, R. (2017). Respiration-guided analysis of pulse and heart rate variabilities for acute emotional stress assessment. Comput. Cardiol. 44, 5–8. doi:10.22489/CinC.2017.318-093
Garzón-Rey, J. M. (2017). Psychosomatic approach to stress measurement” TDX (tesis doctorals en xarxa), Barcelona: Universitat Autònoma de Barcelona.
Gil, E., Mendez, M., Jose Maria Vergara, , Cerutti, S., Bianchi, A. M., and Laguna, P. (2009). Discrimination of sleep-apnea-related decreases in the amplitude fluctuations of PPG signal in children by HRV analysis. IEEE Trans. Biomed. Eng. 56 (4), 1005–1014. doi:10.1109/TBME.2008.2009340
Giorgi, G., Isaia Lecca, L., Alessio, F., Bondanini, G., Ginevra Lulli, L., Arcangeli, G., et al. (2020). COVID-19-Related mental health effects in the workplace: A narrative review. Int. J. Environ. Res. Public Health 17 (21), 7857–7922. doi:10.3390/ijerph17217857
Greco, A., Valenza, G., Lanata, A., and Luca, C. (2016). CvxEDA: A convex optimization approach to electrodermal activity processing. IEEE Trans. Biomed. Eng. 63 (4), 797–804. doi:10.1109/TBME.2015.2474131
Greco, A., Valenza, G., Lazaro, J., Mario Garzon-Rey, J., Aguilo, J., De-la-Camara, C., et al. (2021). Acute stress state classification based on electrodermal activity modeling. IEEE Trans. Affect. Comput. 1, 788–799. doi:10.1109/TAFFC.2021.3055294
Gross, M. J., Shearer, D. A., Bringer, J. D., Hall, R., Cook, C. J., and Kilduff, L. P. (2016). Abbreviated resonant frequency training to augment heart rate variability and enhance on-demand emotional regulation in elite sport support staff. Appl. Psychophysiol. Biofeedback 41 (3), 263–274. doi:10.1007/s10484-015-9330-9
Hasuo, H., Kanbara, K., and Fukunaga, M. (2020). Effect of heart rate variability biofeedback sessions with resonant frequency breathing on sleep: A pilot study among family caregivers of patients with cancer. Front. Med. 7, 61. doi:10.3389/fmed.2020.00061
Hayano, J., and Yuda, E. (2019). Pitfalls of assessment of autonomic function by heart rate variability. J. Physiological Anthropol. 38 (1), 3–8. doi:10.1186/s40101-019-0193-2
Heiss, S., Vaschillo, B., Vaschillo, E. G., Alix Timko, C., and Hormes, J. M. (2021). Heart rate variability as a biobehavioral marker of diverse psychopathologies: A review and argument for an ‘ideal range. Neurosci. Biobehav. Rev. 121, 144–155. doi:10.1016/j.neubiorev.2020.12.004
Hernando, A., Lázaro, J., Gil, E., Arza, A., Garzón, J. M., López-Antón, R., et al. (2016). Inclusion of respiratory frequency information in heart rate variability analysis for stress assessment. IEEE J. Biomed. Health Inf. 20 (4), 1016–1025. doi:10.1109/JBHI.2016.2553578
Kennedy, L., and Parker, S. H. (2019). Biofeedback as a stress management tool: A systematic review. Cognition, Technol. Work 21 (2), 161–190. doi:10.1007/s10111-018-0487-x
Kim, H. G., Cheon, E. J., DaiBai, S., YoungLee, H., and Koo, B. H. (2018). Stress and heart rate variability: A meta-analysis and review of the literature. Psychiatry Investig. 15, 235–245. doi:10.30773/pi.2017.08.17
Kirschbaum, C., Pirke, K-M., and DirkHellhammer, H. (1993). The ‘trier social stress test’ – a tool for investigating psychobiological stress responses in a laboratory setting. Neuropsychobiology 28 (1–2), 76–81. doi:10.1159/000119004
Kroenke, K., Spitzer, R. L., and Williams, J. B. W. (2001). The PHQ-9 validity of a brief depression severity measure. J. General Intern. Med. 16 (9), 606–613. doi:10.1046/j.1525-1497.2001.016009606.x
Lázaro, J., Alcaine, A., Romero, D., Gil, E., Laguna, P., Pueyo, E., et al. (2014). Electrocardiogram derived respiratory rate from QRS slopes and R-wave angle. Ann. Biomed. Eng. 42 (10), 2072–2083. doi:10.1007/s10439-014-1073-x
Lazaro, J., Gil, E., Jose Maria, V, and Laguna, P. (2014). Pulse rate variability analysis for discrimination of sleep-apnea-related decreases in the amplitude fluctuations of pulse photoplethysmographic signal in children. IEEE J. Biomed. Health Inf. 18 (1), 240–246. doi:10.1109/JBHI.2013.2267096
Lehrer, P. (2013). How does heart rate variability biofeedback work? Resonance, the baroreflex, and other mechanisms. Biofeedback 41 (1), 26–31. doi:10.5298/1081-5937-41.1.02
Lehrer, P., Kaur, K., Sharma, A., Shah, K., Huseby, R., Bhavsar, Jay, et al. (2020). Heart rate variability biofeedback improves emotional and physical health and performance: A systematic review and meta analysis. Appl. Psychophysiol. Biofeedback 45 (3), 109–129. doi:10.1007/s10484-020-09466-z
Lehrer, P., Vaschillo, B., Zucker, T., Graves, J., Katsamanis, M., Aviles, M., et al. (2013). Protocol for heart rate variability biofeedback training. Biofeedback 41 (3), 98–109. doi:10.5298/1081-5937-41.3.08
Lesage, F.- X., Berjot, S., and Deschamps, F. (2012). Clinical stress assessment using a visual Analogue scale. Occup. Med. 62 (8), 600–605. doi:10.1093/occmed/kqs140
Leyro, Teresa M., VersellaMin-Jeong, Y., Mark, V, Hannah, R. B., Hoyt, D. L., and Paul, L. (2021). Respiratory therapy for the treatment of anxiety: Meta-analytic review and regression. Clin. Psychol. Rev. 84, 101980. doi:10.1016/j.cpr.2021.101980
Limmer, A., Laser, M., and Schütz, A. (2021). Mobile heart rate variability biofeedback as a complementary intervention after myocardial infarction: A randomized controlled study. Int. J. Behav. Med. 3, 230–239. doi:10.1007/s12529-021-10000-6
LinMei, I., Fan, S. Y., Yen, C. F., Yeh, Y. C., Tang, T C., Huang, M. F., et al. (2019). Heart rate variability biofeedback increased autonomic activation and improved symptoms of depression and insomnia among patients with major depression disorder. Clin. Psychopharmacol. Neurosci. 17 (2), 222–232. doi:10.9758/cpn.2019.17.2.222
Martínez, J. P., Almeida, R., Olmos, S., Rocha, A. P., and Laguna, P. (2004). A wavelet-based ECG delineator: Evaluation on standard databases. IEEE Trans. Biomed. Eng. 51 (4), 570–581. doi:10.1109/TBME.2003.821031
Marzi, C., Greco, A., and Vanello, N. (2021). Towards a model of arousal change after affective word pronunciation based on electrodermal activity and speech analysis. Biomed. Signal Process. Control 67, 102517. doi:10.1016/j.bspc.2021.102517
Mateo, J., and Laguna, P. (2003). Analysis of heart rate variability in the presence of ectopic beats using the heart timing signal. IEEE Trans. Biomed. Eng. 50 (3), 334–343. doi:10.1109/TBME.2003.808831
McCraty, R., and Shaffer, F. (2015). Heart rate variability: New perspectives on physiological mechanisms, assessment of self-regulatory capacity, and health risk. Glob. Adv. Health Med. 4 (1), 46–61. doi:10.7453/gahmj.2014.073
Moss, D., and Shaffer, F. (2017). The application of heart rate variability biofeedback to medical and mental health disorders. Biofeedback 45 (1), 2–8. doi:10.5298/1081-5937-45.1.03
O’Rourke, N., and Hatcher, L. (2013). A step-by-step approach to using SAS for factor analysis and structural equation modeling. Cary, NC: SAS Institute Inc., 412. doi:10.5555/2530480
Pappa, S., Ntella, V., Giannakas, T., Giannakoulis, V. G., Papoutsi, E., and Katsaounou, P. (2020). Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav Immun 88, 901–907. doi:10.1016/j.bbi.2020.05.026
Pedrozo-Pupo, T., Carlos, J., and Campo-Arias, A. (2020). Depression, perceived stress related to COVID, post-traumatic stress, and insomnia among asthma and COPD patients during the COVID-19 pandemic. Chronic Respir. Dis. 17, 147997312096280. doi:10.1177/1479973120962800
Pisanski, K., Kobylarek, A., Jakubowska, L., Nowak, J., Walter, A., Błaszczyński, K., et al. (2018). Multimodal stress detection: Testing for covariation in vocal, hormonal and physiological responses to trier social stress test. Hormones Behav. 106, 52–61. doi:10.1016/j.yhbeh.2018.08.014
Pizzoli, S. F. M., Marzorati, C., Gatti, D., Monzani, D., Mazzocco, K., and Pravettoni, G. (2021). A meta-analysis on heart rate variability biofeedback and depressive symptoms. Sci. Rep. 11 (1), 6650–6710. doi:10.1038/s41598-021-86149-7
Posada-Quintero, G., Hugo, F., Florian, J. P., Orjuela-Cañón, Á. D., and Chon, K. H. (2016). Highly sensitive index of sympathetic activity based on time-frequency spectral analysis of electrodermal activity. Am. J. Physiology - Regul. Integr. Comp. Physiology 311 (3), R582–R591. doi:10.1152/ajpregu.00180.2016
Purtle, J., Nelson, K. L., Counts, N. Z., and Yudell, M. (2020). Population-based approaches to mental health: History, strategies, and evidence. Annu. Rev. Public Health 41 (1), 201–221. doi:10.1146/annurev-publhealth-040119-094247
Remor, E. (2006). Psychometric properties of a European Spanish version of the perceived stress scale (PSS). Span. J. Psychol. 9 (1), 86–93. doi:10.1017/S1138741600006004
Sarchiapone, M., Gramaglia, C., Iosue, M., Carli, V.r, Mandelli, L., Serretti, A., et al. (2018). The association between electrodermal activity (EDA), depression and suicidal behaviour: A systematic review and narrative synthesis. BMC Psychiatry 18 (1), 22–27. doi:10.1186/s12888-017-1551-4
Scavone, A., Kadziolka, M. J., and CarlinMiller, J. (2020). State and trait mindfulness as predictors of skin conductance response to stress. Appl. Psychophysiol. Biofeedback 1, 221–228. doi:10.1007/s10484-020-09467-y
Schuman, D. L., and Killian, M. O. (2019). Pilot study of a single session heart rate variability biofeedback intervention on veterans’ posttraumatic stress symptoms. Appl. Psychophysiol. Biofeedback 44 (1), 9–20. doi:10.1007/s10484-018-9415-3
Shaffer, F., and Ginsberg, J. P. (2017). An overview of heart rate variability metrics and norms. Front. Public Health 5, 258. doi:10.3389/fpubh.2017.00258
Shaffer, F., and Meehan, Z. M. (2020). A practical guide to resonance frequency assessment for heart rate variability biofeedback. Front. Neurosci. 14, 570400. doi:10.3389/fnins.2020.570400
Sobregrau Sangrà, P., Aguiló Mir, S., Aguiló Mir, , Castro Ribeiro, T., Esteban-Sepúlveda, S., García Pagès, E., et al. (2022). Mental health assessment of spanish healthcare workers during the SARS-CoV-2 pandemic. A cross-sectional study. Comprehensive psychiatry 112 (January) : 152278. doi:10.1016/j.comppsych.2021.152278
Spielberger, C. D., Gorsuch, R. L., Lushene, R. E., Vagg, P. R., and Jacobs, G. A. (1983). Manual for the state-trait anxiety inventory. Palo Alto, CA: Consulting Psychologists Press.
Stroop, J. R. (1935). Studies of interference in serial verbal reactions. J. Exp. Psychol. 18 (6), 643–662. doi:10.1037/h0054651
Tipton, M. J., Abbi Harper, J. F. R. P., Costello, J. T., and Costello, J. T. (2017). The human ventilatory response to stress: Rate or depth? J. Physiology 595 (17), 5729–5752. doi:10.1113/JP274596
Tonhajzerova, I., Ondrejka, I., Turianikova, Z., Javorka, K., Calkovska, A., and Javork, M. (2012). Heart rate variability: An index of the brain-heart interaction. Tachycardia. InTech. doi:10.5772/25763
World Health Organization (2022). World mental health report: Transforming mental health for all. Geneva, Switzerland: World Health Organization.
Yasuma, F., and Ichiro Hayano, J. (2004). Respiratory sinus arrhythmia: Why does the heartbeat synchronize with respiratory rhythm?” Chest. Elsevier 125 (2), 683–690. doi:10.1378/chest.125.2.683
Keywords: stress objective assessment, effectiveness of interventions, electrophysiological model, heart rate variability biofeedback, healthcare workers, mental health, stress
Citation: Castro Ribeiro T, Sobregrau Sangrà P, García Pagès E, Badiella L, López-Barbeito B, Aguiló S and Aguiló J (2023) Assessing effectiveness of heart rate variability biofeedback to mitigate mental health symptoms: a pilot study. Front. Physiol. 14:1147260. doi: 10.3389/fphys.2023.1147260
Received: 18 January 2023; Accepted: 24 April 2023;
Published: 10 May 2023.
Edited by:
Rui Min, Beijing Normal University, ChinaReviewed by:
Richard Gevirtz, Alliant International University, United StatesCopyright © 2023 Castro Ribeiro, Sobregrau Sangrà, García Pagès, Badiella, López-Barbeito, Aguiló and Aguiló. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Thais Castro Ribeiro, dGhhaXMuY2FzdHJvQHVhYi5jYXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.