 Jonas Böcker
Jonas Böcker Marie-Therese Schmitz1,2
Marie-Therese Schmitz1,2 Uwe Mittag
Uwe Mittag Jens Jordan
Jens Jordan Jörn Rittweger
Jörn Rittweger- 1Department of Muscle and Bone Metabolism, German Aerospace Center, Institute of Aerospace Medicine, Cologne, Germany
- 2Institute of Medical Biometry, Informatics and Epidemiology (IMBIE), University Hospital Bonn, Bonn, Germany
- 3Chair of Aerospace Medicine, University of Cologne, Cologne, Germany
- 4German Aerospace Center, Head of Institute of Aerospace Medicine, Cologne, Germany
- 5Department of Pediatrics and Adolescent Medicine, University Hospital of Cologne, Cologne, Germany
To improve quantification of individual responses to bed rest interventions, we analyzed peripheral quantitative computer tomography (pQCT) datasets of the lower leg of 76 participants, who took part in eight different bed rest studies. A newly developed statistical approach differentiated measurement uncertainty UMeas from between-subject-variation (BSV) and within-subject variation (WSV). The results showed that UMeas decreased 59.3% to 80% over the two decades of bed rest studies (p < 0.01), and that it was higher for muscles than for bones. The reduction of UMeas could be explained by improved measurement procedures as well as a higher standardization. The majority (59.1%) of the individual responses pci exceeded the 95% confidence interval defined by UMeas, indicating significant and substantial BSV, which was greater for bones than for muscles, especially at the diaphyseal measurement sites. Non-significant to small positive inter-site correlations between bone sites, but very large positive inter-site correlation between muscle sites suggests that substantial WSV exists in the tibia bone, but much less so in the calf musculature. Furthermore, endocortical circumference, an indicator of the individual’s bone geometry could partly explain WSV and BSV. These results demonstrate the existence of substantial bone BSV, and that it is partly driven by WSV, and likely also by physical activity and dietary habits prior to bed rest. In addition, genetic and epigenetic variation could potentially explain BSV, but not WSV. As to the latter, differences of bone characteristics and the bone resorption process could offer an explanation for its existence. The study has also demonstrated the importance of duplicate baseline measurements. Finally, we provide here a rationale for worst case scenarios with partly effective countermeasures in long-term space missions.
Introduction
Microgravity exposure is associated with profound adaptations of the human body, including muscle atrophy and bone loss, both of are usually interpreted as a result of unloading and the lack of mechanical forces (Vico et al., 2000; LeBlanc et al., 2007; Fitts et al., 2010; Rittweger et al., 2018). Especially, the lower limb is affected by these adaptations resulting in muscle wasting of 6 and 24% of the baseline volume after 8 days and 6 month of microgravity exposure, respectively (LeBlanc et al., 1997; Narici and de Boer, 2011). Bone losses amount to an average loss rate of 1–1.5% bone mineral content (BMC) per month (Pavy-Le Traon et al., 2007), which, however, is subject to substantial between-subject variation (BSV). Furthermore, besides BSV there is a within-subject variation (WSV) shown by differences in bone loss at different body sites after bed rest (Rittweger et al., 2005), the latter being a suitable analog of microgravity exposure on earth. The −6° head down tilt (HDT) bed rest induces an unloading of muscles and bones of the lower extremities and the spine evoking adaptations that are comparable to those from space-related adaptations. Bed rest studies unanimously show loss of muscle volume, of muscle strength and of BMC (Hargens and Vico, 2016). The loss of the muscle volume is exponential and in a comparable manner followed by losses in muscle power and muscle strength (Narici and de Boer, 2011). After 7–14 days of unloading, there are moderate effects, larger effects occur within 35 days of bed rest (Winnard et al., 2019). Furthermore, there is a correlation between reduction in muscle cross-sectional area (CSA) and strength loss. Because of that, CSA is a good approximation for muscle strength (Maughan et al., 1983; Rittweger et al., 2000; Fukunaga et al., 2001). Mitigating these profound adaptations and maintaining a sufficient physiological status is the aim of suitable countermeasures (Winnard et al., 2019). Yet, different training effort using such countermeasures can lead to variations in the musculoskeletal response (Timmons, 2011; Rittweger et al., 2018), however, in contrast, comparable training effort can also lead to BSV in muscle loss (English et al., 2015) or bone loss (Sibonga et al., 2015). The variation may be explained by the fact that there are responders and non-responders toward a training intervention (Mann et al., 2014; Hecksteden et al., 2015; Ahtiainen et al., 2016) resulting in a BSV (McPhee et al., 2010; Ross et al., 2019).
Until now, there are few approaches for quantifying BSV and WSV in response to bed rest (Narici and de Boer, 2011; Debevec et al., 2018; Scott et al., 2021). Thus, previous approaches have compared the standard deviation (SD) of changes between intervention and control group (Atkinson and Batterham, 2015; Hopkins, 2015). But so far, most researchers do not perform such analysis getting information about individual differences (Atkinson and Batterham, 2015). Moreover, systematic attempt to separate BSV and WSV from measurement-related uncertainty are rare except Swinton et al. (2018). Following Scott et al. (2021), bed rest is a good possibility to quantify “true” and “false” individual differences, because due to the conditions of such a study, several influencing parameters like nutrition or daily activities are controlled. Atkinson et al. (2019) explained that there is an additional factor, which cannot be controlled. There is a random WSV due to the period of time between the baseline data collection (BDC) and the follow up measurements, mostly influenced by non-standardized behavior of the participants. Understanding BSV and WSV is of general interest. Thus, large BSV in the presence of small WSV would favor genetic and epigenetic mechanisms, whilst large BSV in combination with large WSV would require more complicated explanation models. Moreover, detailed information about BSV and WSV is highly relevant in practical terms when the health and well-being of single individuals is at stake. Therefore, the aim of the present work was to explore variation in musculoskeletal responses to bed rest, and to separate BSV, WSV and measurement-related uncertainty.
Materials and Methods
Selected Studies
We selected data sets of eight bed rest studies (AGBRESA, BBR, LTBR, MEP, NUC, Planhab, RSL, Valdoltra), which took place in France, Slovenia, and Germany, respectively, from 2001 till 2019 to explore the variation in musculoskeletal responses after bed rest. The studies varied in bed rest duration as well as bed rest condition (horizontal bed rest or head down tilt bed rest). The full study names, the year, the location, and the characteristics, which were important for this manuscript, are presented in Table 1. Additionally, Table 1 includes references, which explain the exact study details.
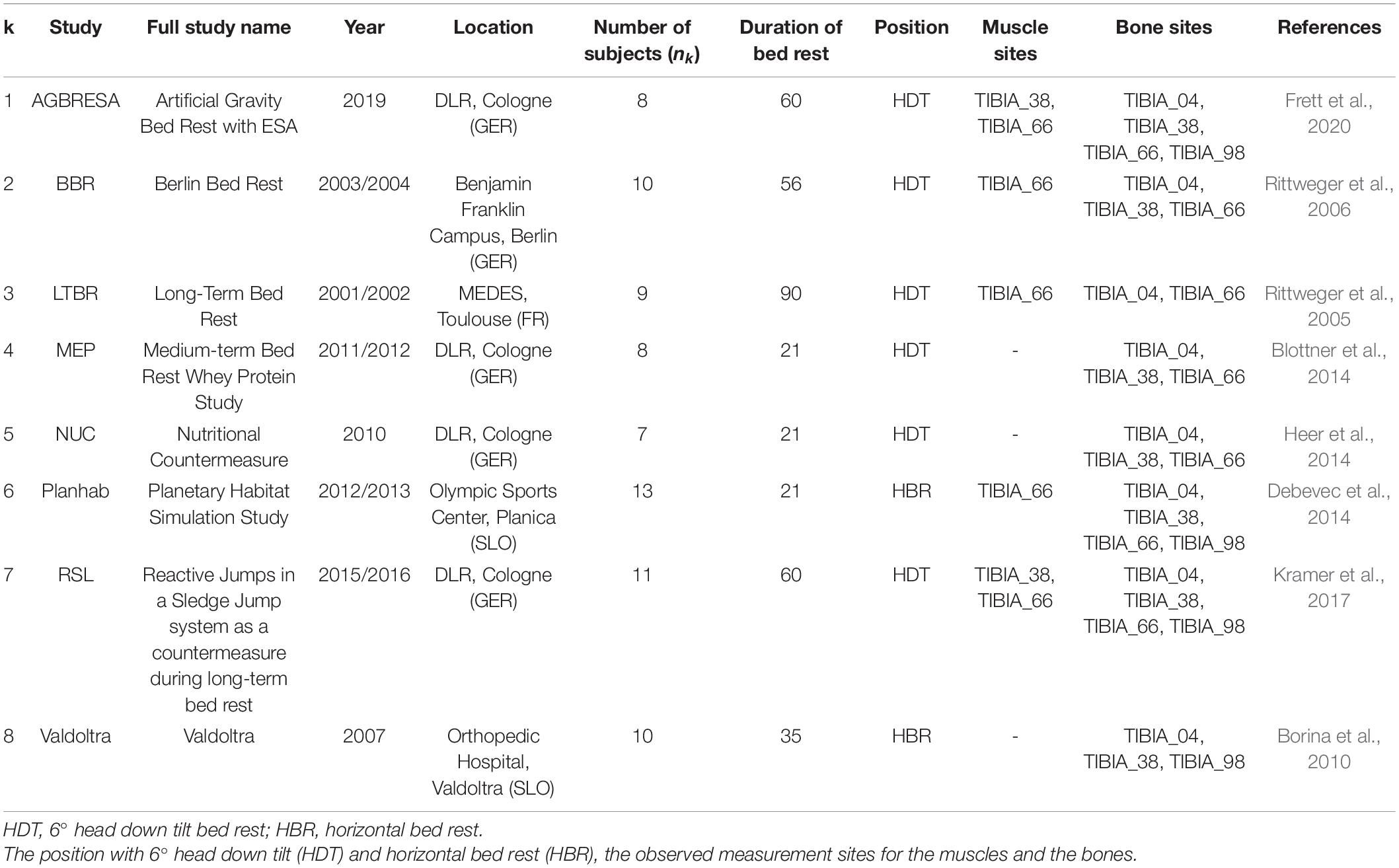
Table 1. Overview about the included studies with information about the year, the location, the number of subjects, the duration of bed rest, bed rest position, and measurement sites.
Three out of the eight studies (LTBR, RSL, and Valdoltra) included two baseline measurements of the peripheral quantitative computed tomography (explained later on). This enabled a calculation of the measurement uncertainty, because the time between the two measurements was short and no intervention took place. As it is very consistent in literature, the bone losses, but not muscle wasting, continue for another 10–20 days following re-ambulation (Rittweger et al., 2005, 2010; Hargens and Vico, 2016), muscle losses were quantified at the last day of bedrest and bone losses at 14 days of follow-up after re-ambulation. Due to comparable durations of bed rest, BBR was presented as AGBRESA and RSL with 60 days of bed rest in the results section.
Participants
In total, we analyzed datasets of 76 participants, who took part in the described eight different bed rest studies. For the purpose of this manuscript only the data of the control groups, which experienced no intervention excluding bed rest, were analyzed. Only for calculation of the measurement uncertainty of LTBR, RSL and Valdoltra we used the data sets of control and intervention group getting more precise values. Additionally, from 11 subjects of the LTBR study (control and intervention group), both legs were measured and were also used for analysis of the measurement uncertainty.
Peripheral Quantitative Computed Tomography Measurements
The tibia is composed of (1) distal and proximal epiphysis, which are both rich in trabecular bone and devoid of thick compact bone, (2) distal and proximal metaphysis, which are composed both of compact and trabecular bone, and (3) the diaphysis (shaft), which is mainly composed of thick compact bone and almost devoid of trabecular bone (Capozza et al., 2010), whereas at the proximal epiphysis the cortical shell consisting of compact bone is often not thicker than trabeculi. At diaphyseal sites, pQCT also allows segmentation of muscle from skin and bone tissues, thereby yielding the anatomical muscle cross-sectional area (CSA), albeit without distinction of individual muscle groups (Figure 1). All selected studies included a pQCT measurement with either a XCT2000 or a XCT3000 device (Stratec Medizintechnik, Pforzheim, Germany) (Table 2). The measurement process for pQCT has been described in detail elsewhere (Rittweger et al., 2010). In brief, the XCT devices use single-beam rotation-translation CT technology, and distal and proximal tibial sites are identified from tibio-talar and femoro-tibial scout views, respectively, whilst sites at the diaphysis are either found manually or via a scout view (Figure 1). Over the two decades that the studies have been performed, the procedures have been slightly modified to maximize repeatability of the measurements. Moreover, whilst earlier studies had solely focused on the distal tibia, the proximal tibia has also been studied since 2007, initially using femoro-tibial scout views in the frontal plane, and with sagittal scout views since 2016 (Table 2). As bed rest induces minimal to no changes in the metaphysis and in the forearms, the present manuscript focusses on epiphyseal and diaphyseal bone sites including two muscles sites at the diaphysis, thereby allowing WSV assessment in addition to BSV.
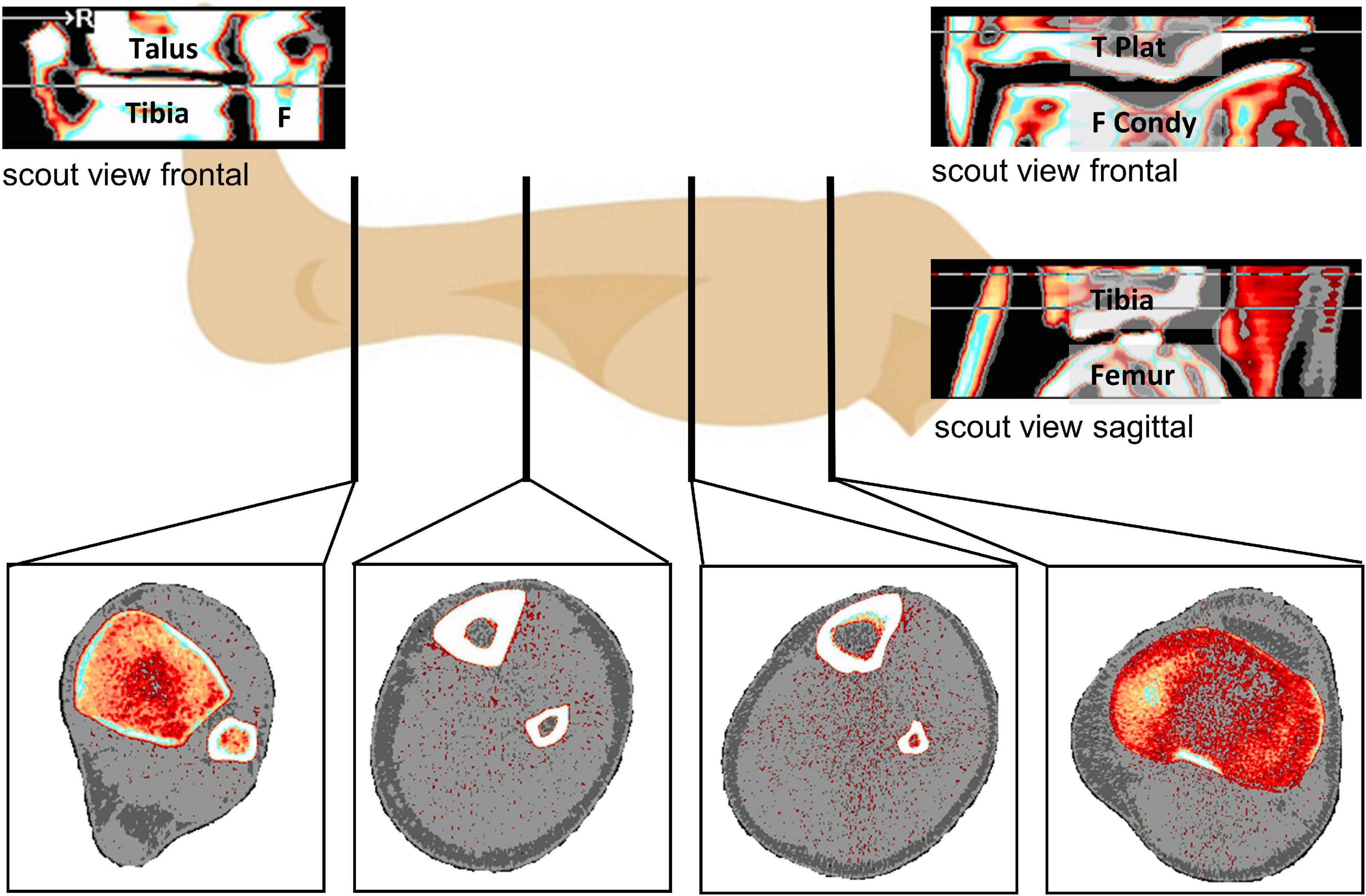
Figure 1. Overview about the analyzed measurement sites (at the bottom) from left to right with TIBIA_04 (Epiphysis at the ankle), TIBIA_38 and TIBIA_66 at the diaphysis and TIBIA_98 (Epiphysis at the knee joint). 04, 38, 66, and 98 represent the relative position regarding the tibia length from ankle joint to knee joint. Top left is the distal frontal scout view (Tibia, Talus, F: Fibula), top right the frontal proximal scout view (F Condy: Femur Condyles, T Plat: Tibia Plateau), below that the sagittal proximal scout view.
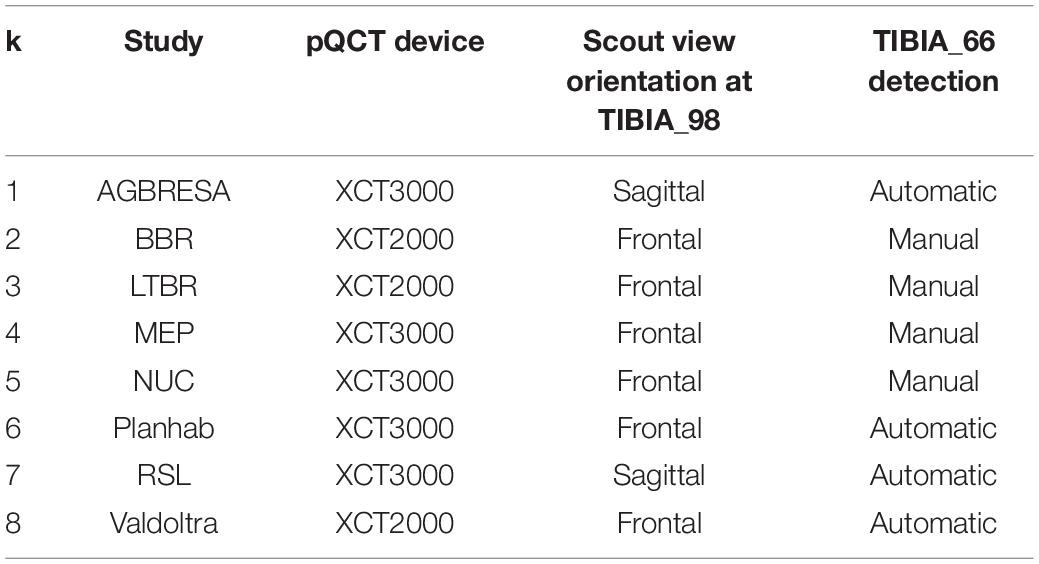
Table 2. Overview about the way of the determination of the measurement site of TIBIA_98 and TIBIA_66.
Image Analysis and Data Processing
All image analysis was performed with the integrated XCT software Stratec XCT Console in its version 6.20 in accordance with the manufacturer’s instructions. The operator marked the regions of interest (ROI) in each picture (tibia, fibula, muscle including tibia and fibula at 38 and 66% of tibia length) and defined the segmentation threshold for the outer bone or muscle contour. The threshold differed between measurement sites, studies, and could even differ between subjects, respectively. The threshold was chosen yielding a satisfactory contour of the ROI and was kept for each subject throughout the study. To differentiate between compact and trabecular bone tissue at the epiphyseal measurement sites, we run a second analysis with a segmentation threshold at 650 mg/cmł, which enabled quantifying the compact bone at these sites (Rittweger et al., 2010). After analyzing all pQCT scans, an analysis was performed by the XCT software that encompassed all CT numbers included in the present analysis. The resulting data base was further processed with custom-made R-scripts (Version 3.6.01), using the RStudio environment (Version 1.2.1335, Boston, MA, United States). Thus, BMC was identified as the product of the XCT-variables “TOT_DEN” and “TOT_A” divided by 1,000. The endocortical circumference (ENDO) was identified from “ENDO_C”. Muscle CSA was calculated as the differences between “TOT_A” of the ROI of the muscle and “TOT_A” of tibia and fibula.
Statistical Computation
We assumed that measurement uncertainty (UMeas) was variable across measurement sites and studies, but invariant within a given study and measurement site. Moreover, we assumed that UMeas and the individual response to the bed rest intervention (UIR) depict normal distribution. It follows then from the principle of linear superposition that the observed response’s uncertainty UObs can be conceptualized as the sum of these two parameters.
We defined the observed individual loss of bone or muscle of subject i (i = 1, …, nk with nk as the total number of subjects of study k, k = 1, …, 8) after bed rest intervention as the percent change pci:
pcik is defined as the difference either BMC or CSA between the individual result after the intervention (xIR,ik) and the result of the first baseline measurement (xBDC,ik) divided by the baseline result (xBDC,ik). This result is multiplied by 100 getting the percent change pcik. The mean among all subjects of a study is denoted by pck and is calculated for each measurement site of each of the eight included studies.
Empirically, the observed uncertainty Obs,k (k indicating the study) could be assessed as the variance of the individual percent change pcik of each participant of each study’s control group, nk is indicating the number of participants in the control group of study k, and the mean percent change of these participants:
Meas denote measurement uncertainties, which are usually assessed during baseline through repetition of measurements. Typically, we use two baseline measurements (ni = 2) to compute the variance within each participant. The mean of these variances of all participants of one study and measurement site represents . As we compared individual’s response toward the measurement uncertainty, the calculation of the variance was more practical resulting in absolute values compared to the coefficient of variation. For calculation of we used the baseline measurements of all subjects of study k, irrespective of the group (control or intervention group) to get more precise values. ni represents the number of baseline measurements, xBDC,mk the value of each baseline measurement (BMC or CSA), and the mean of all baseline measurements of the specific participant.
Solving Equation 1 for IR and replacing the parameters yields
This variable has been obtained for each study and measurement site. As only LTBR, RSL and Valdoltra included two baseline measurements, it was impossible to calculate for all study and measurement sites. So, for studies with only one baseline measurement, we used the result of the study with the most similar measurement condition (Table 2). If this was not possible due to missing data (e.g., Valdoltra provided no data about MUSCLE_66, which is needed for Planhab MUSCLE_66 calculations), we used the higher of the other studies (in the case of the example, we used of LTBR).
Additionally, to compare results of studies with different durations of bed rest, we introduced the adjusted between subject deviation (ABD) for each study k. ABDk is defined as the square root of the uncertainty of individual response divided by the mean of the percent change of each study and measurement site. This result is divided by each study’s duration in weeks. By using the mean percent change and the study duration, we normalized the uncertainty to bed rest duration and bed rest conditions as well as other factors like age or sex of the participants:
Besides these analyses of variances, we calculated the absolute bone loss (BL) as difference of BMC of the first baseline measurement and the post bed rest value:
Between-Subject Variation and Within-Subject Variation
The main focus of this manuscript is on the between-subject variation (BSV) and the within-subject variation (WSV) separated from the measurement uncertainty. For computation of the BSV, we calculated the mean percent change of each measurement site and study. Furthermore, we defined a 95%-confidence interval by using the term 1.96 ⋅ UMeas (measurement uncertainty of the specific measurement site and study or the most similar condition as described earlier). Thus, the interval was defined as the range between mean percent change added up and subtracted by the term based on the measurement uncertainty. If the individual percent change of a participant exceeded this interval, there was a BSV.
We defined WSV in this manuscript that there was no correlation between loss of muscle volume and/or BMC within one subject along the measurement sites. For this purpose, we used the Pearson’s correlation coefficient between the different measurement sites for each study. As there are differences regarding the bone tissue content between the bone sites, we additionally analyzed the loss of compact and trabecular bone loss and its relationships toward the other measurement sites.
Statistics
All computations and statistics were performed with RStudio (Version 1.2.1335, Boston, MA, United States) based on the R-environment (Version 3.6.0,see text footnote 1). Firstly, a mean value of the baseline BMC of the studies with two baseline measurements was calculated followed by calculation of the difference from the mean to the first baseline data collection (BDC1) and was checked for normal distribution. To assess changes of BMC and CSA after the bed rest intervention to BDC1, a paired sample t-test was performed separately for each measurement site and study. An ANOVA was used to evaluate differences in UMeas (studies with two baseline measurements: LTBR, RSL, Valdoltra). The mean of UObs and UIR for each measurement site was compared by an ANOVA. In case of a significant result for the F-test of the ANOVA, a post-hoc Tukey Honest Significant Differences test was performed to further analyze differences between the studies and measurement. BSV is shown by exceeding the 95%-confidence interval, which was calculated based on UMeas (as described before). The correlations of the percent changes for muscles and bones were analyzed by the Pearson correlation coefficient and scored as defined by Hinkle et al. (2009). Based on these results of the Pearson’s correlation coefficient we could do statements about WSV. The relationship between ENDO and BL was analyzed by a linear regression analysis for each study and all studies combined. This approach was performed based on the results of Rittweger et al. (2009) and adapted that we did not use the compact bone loss, but the total BMC loss. Finally, we fitted a linear mixed model (LMM) for analyzing the outcome variables BMC and CSA with fixed effects of measurement site, study days, amount of bed rest and ENDO (only for BMC), respectively, and random intercepts for study and subjects within a study allowing different variances for each measurement site (in case of heteroscedasticity of the within-group errors).
Results
Differences between values of baseline data collection 1 (BDC1) and the within-subject means of the two baseline measurements were near-normally distributed without any substantial deviation, thereby justifying the approach outlined in the equations above. The difference between BDC1 and post bed rest was significant for MUSCLE_38 (AGBRESA: p = 0.003 and RSL: p = 0.002) and MUSCLE_66 for AGBRESA (p = 0.01), BBR (p < 0.001), LTBR (p < 0.001) and RSL (p < 0.001), but not for the 21-day Planhab study (p = 0.07) (Supplementary Table 1). Figure 2 shows the study’s percent change at each measurement site.
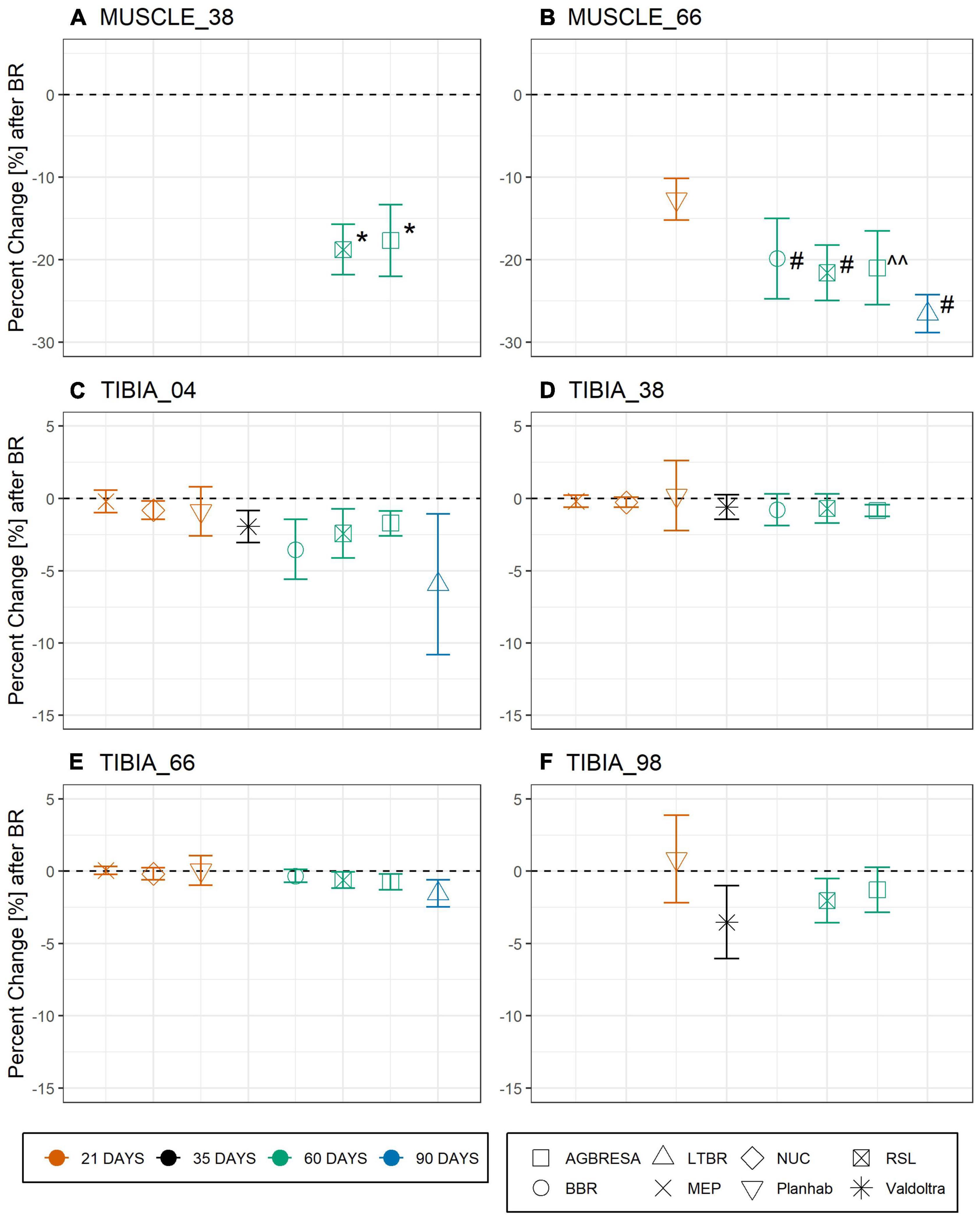
Figure 2. Percent change pck as response toward bed rest intervention on the basis of muscle cross section area (CSA) for (A) MUSCLE_38 (RSL: p = 0.0018; AGBRESA p = 0.0033) and (B) MUSCLE_66 (BBR: p = 6.58-04; RSL: p = 0.0002; AGBRESA: p < 0.05; LTBR: p = 3.35–07) and bone mineral content (BMC) for (C) TIBIA_04, (D) TIBIA_38, (E) TIBIA_66, and (F) TIBIA_98, respectively. Numbers indicate the relative measurement position regarding the entire tibia length from distal to proximal. The average response is shown, error bars represent standard deviation. The color indicates the bed rest duration and the shape represents the study. ^^ denotes significant changes with p < 0.05; * denotes significant changes with p < 0.01; # denotes significant changes with p < 0.001.
For computation of the measurement uncertainty UMeas, we used the results of the studies with two baseline measurements, meaning LTBR, RSL, and Valdoltra, respectively. ANOVA indicated a significant difference of UMeas between RSL and LTBR at TIBIA_66 (p = 0.005) (Table 3). As can be seen from Figure 3, the majority (59.1%) of the observed individual percent change pci exceeds the confidence intervals, indicating significant and substantial BSV. However, the BSV was greater for bone (65.9%) than for muscle (34.8%), and the BSV was greater for the diaphysis (71.0%) than for the epiphyseal measurement sites (60.2%). By subtracting the calculated UMeas from UObs, UIR was calculated (Table 4).
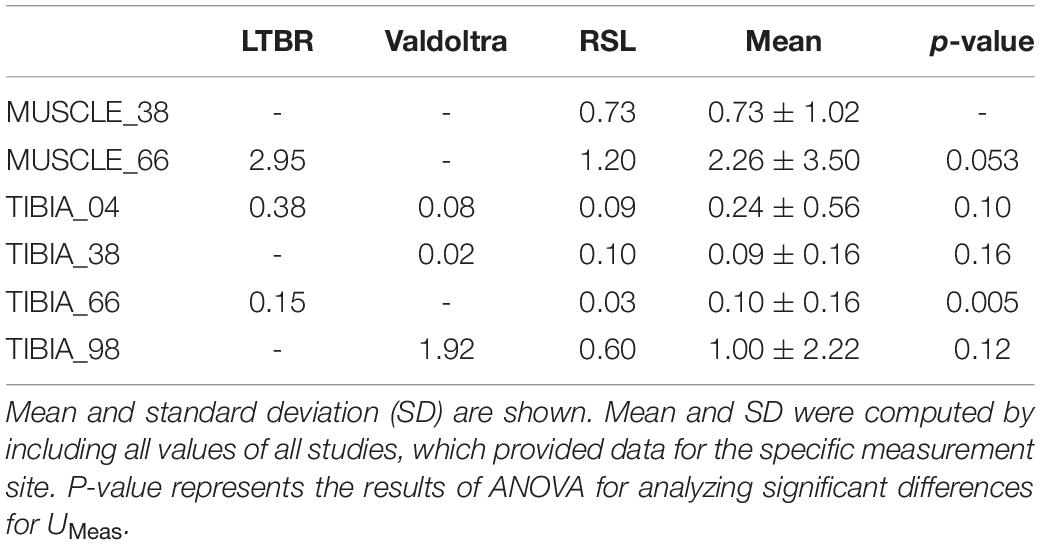
Table 3. Measurement Uncertainty UMeas [%2] of studies with two baseline measurements per body site.
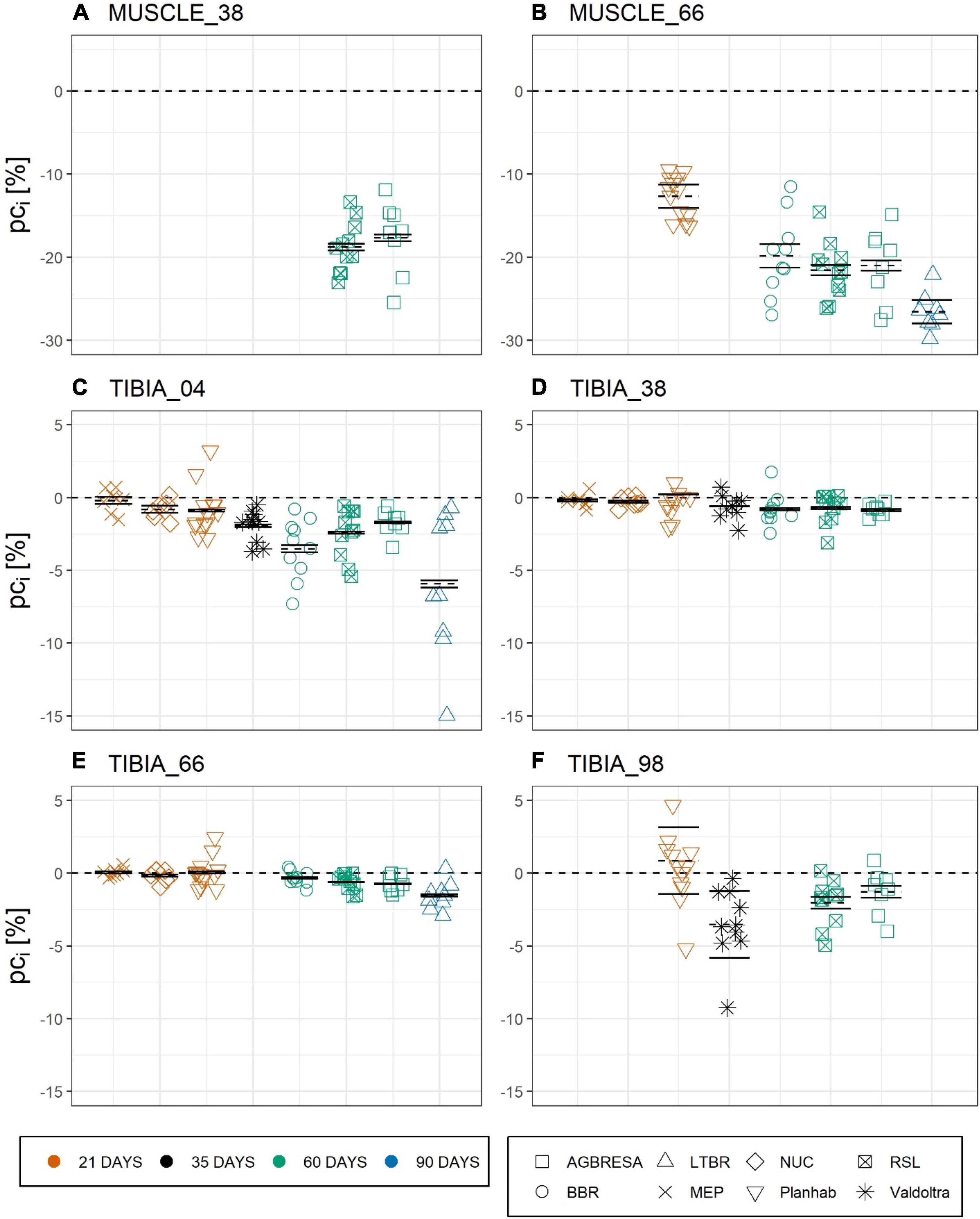
Figure 3. Chart of the individual percent change (pci) by measurement sites with (A) CSA at MUSCLE_38, (B) CSA at MUSCLE_66, (C) BMC at TIBIA_04, (D) BMC at TIBIA_38, (E) BMC at TIBIA_66, and (F) BMC at TIBIA_98, where the numbers indicate the relative measurement position regarding the entire tibia length from distal to proximal. The color indicates the bed rest duration and the shape represents the study. Each chart is separated by the studies that performed measurements at the measurement site. Mean of the pc as dashed line, upper and lower limit of the 95%-confidence interval based on measurement uncertainty UMeas as solid lines. Most pci exceed the confidence interval, indicating significant between-subject variation.
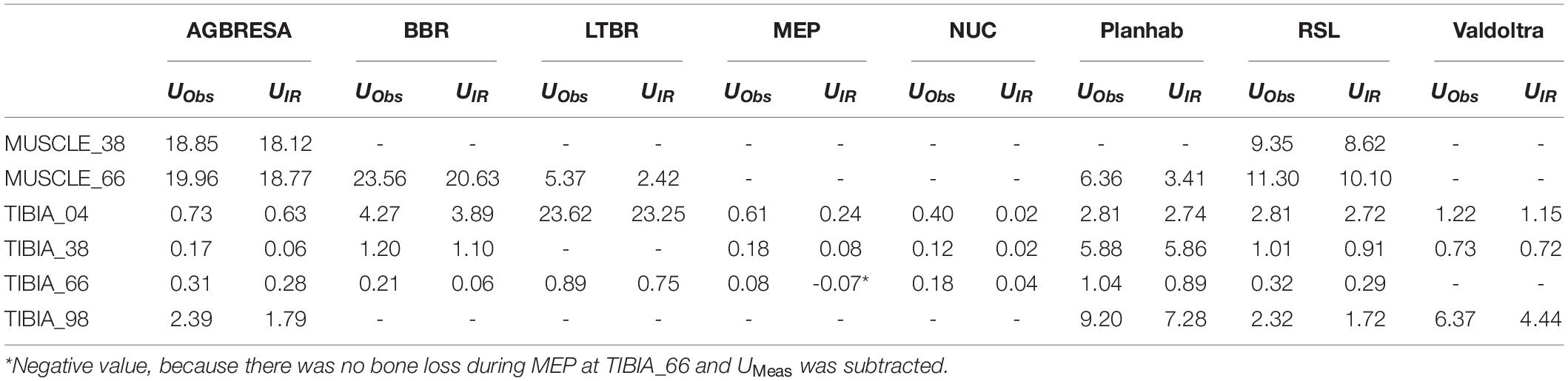
Table 4. Overview about Observed Uncertainty UObs [%2] and Uncertainty of individual response UIR [%2] by studies and body sites.
UObs and UIR were significantly greater for MUSCLE_66 compared to TIBIA_38 (p = 0.009 and p = 0.04) and TIBIA_66 (p = 0.005 and p = 0.02), as well as for MUSCLE_38 compared to TIBIA_66 (p = 0.03) (Supplementary Table 2). Generally, it could be seen a trend that both UObs and UIR were greater for the muscle measurement sites than for the bone measurement sites, except for LTBR, where UObs and UIR were greater for TIBIA_04 than for MUSCLE_66.
As shown in Figure 4, the adjusted between-subject deviation ABDk for the Planhab study depicts three outliers, namely for TIBIA_04 and TIBIA_66. In the absence of any bone loss for TIBIA_66 in the MEP study, ABD4 could not be computed. Figure 5 shows the results of the inter-site correlation analyses. A very high positive correlation of pci between MUSCLE_38 and MUSCLE_66 was observed (r = 0.90, p < 0.001). For BMC, there was no correlation seen between TIBIA_38 and TIBIA_98 (r = 0.29, p = 0.07), whereas the correlation ranged from 0.34 (TIBIA_04 and TIBIA_38; p = 0.006; low positive correlation) to 0.52 (TIBIA_38 and TIBIA_66; p < 0.001; moderate positive correlation) between the remaining bone site pairs. When differentiating compact and trabecular bone tissue at the epiphyseal bone sites, there were significant correlations between TIBIA_04_Comp and TIBIA_38 (r = 0.51; p < 0.001), and TIBIA_66 (r = 0.39; p = 0.002), respectively, but no correlation to TIBIA_98_Comp (r = 0.29; p = 0.19). Additionally, TIBIA_98_Comp showed no correlation to either TIBIA_38 (r = 0.12, p = 0.54) or TIBIA_66 (r = 0.10, p = 0.62). The loss of trabecular bone within the epiphyseal sites showed no correlation (r = −0.12, p = 0.36). With regards to muscle-bone inter-relationships, there was a moderate positive correlation between MUSCLE_38 and TIBIA_98 (r = 0.68, p = 0.001), MUSCLE_66 and TIBIA_66 (r = 0.56, p < 0.001) and MUSCLE_66 and TIBIA_98 (r = 0.56, p < 0.001), and a low positive correlation between MUSCLE_66 and TIBIA_04 (r = 0.47, p < 0.001) and MUSCLE_66 and TIBIA_38 (r = 0.34, p = 0.03; Table 5).
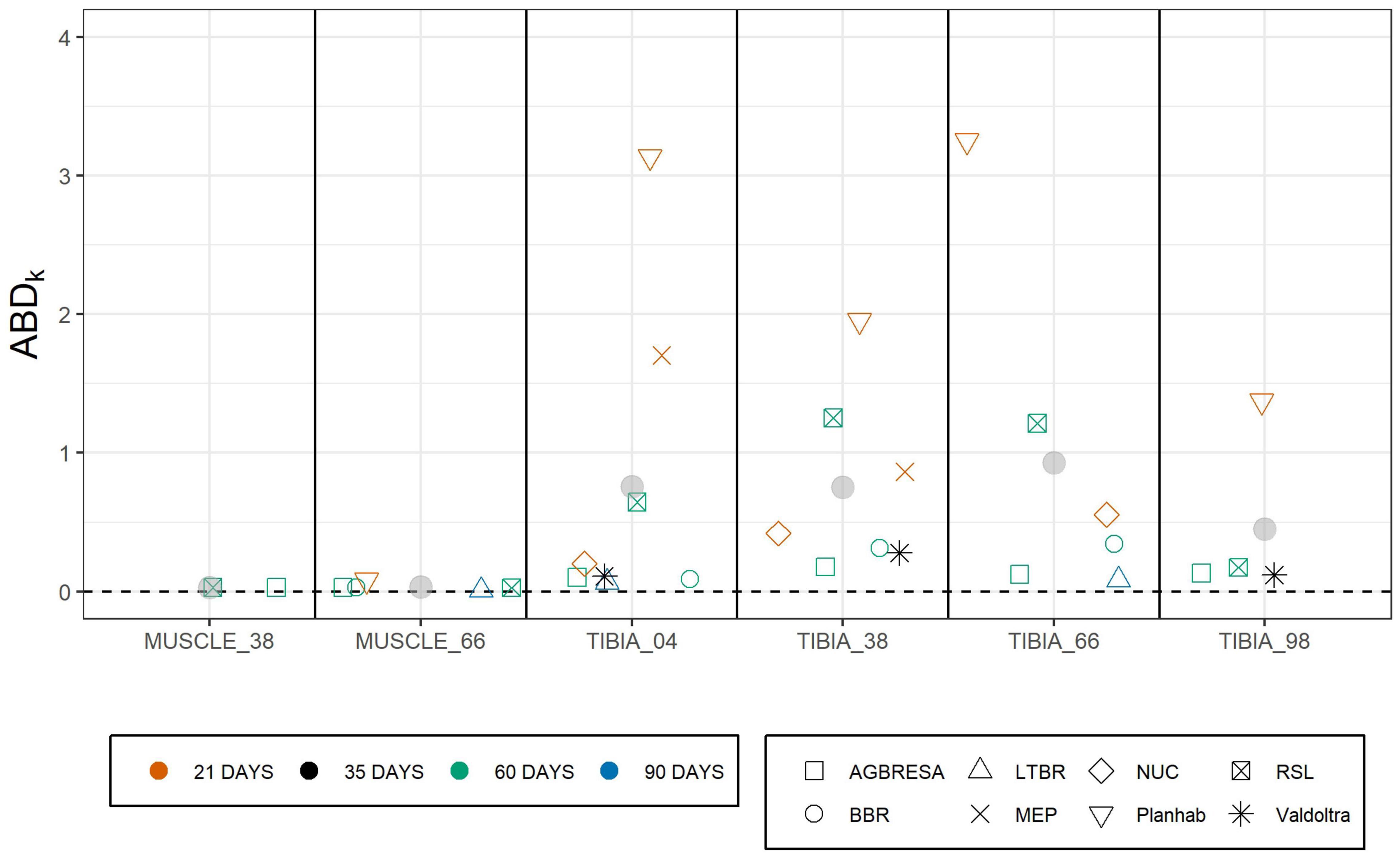
Figure 4. Adjusted between subject deviation (ABDk) of all studies separated by measurement sites. ABDk represented the square root of uncertainty of individual response UIR divided by pck enabling the comparison of several studies with different bed rest durations. The color indicates the bed rest duration and the shape represents the study. The data of MEP for TIBIA_66 are missing due to negative values of the uncertainty of individual response UIR. Gray points represent the mean value of the specific measurement site.
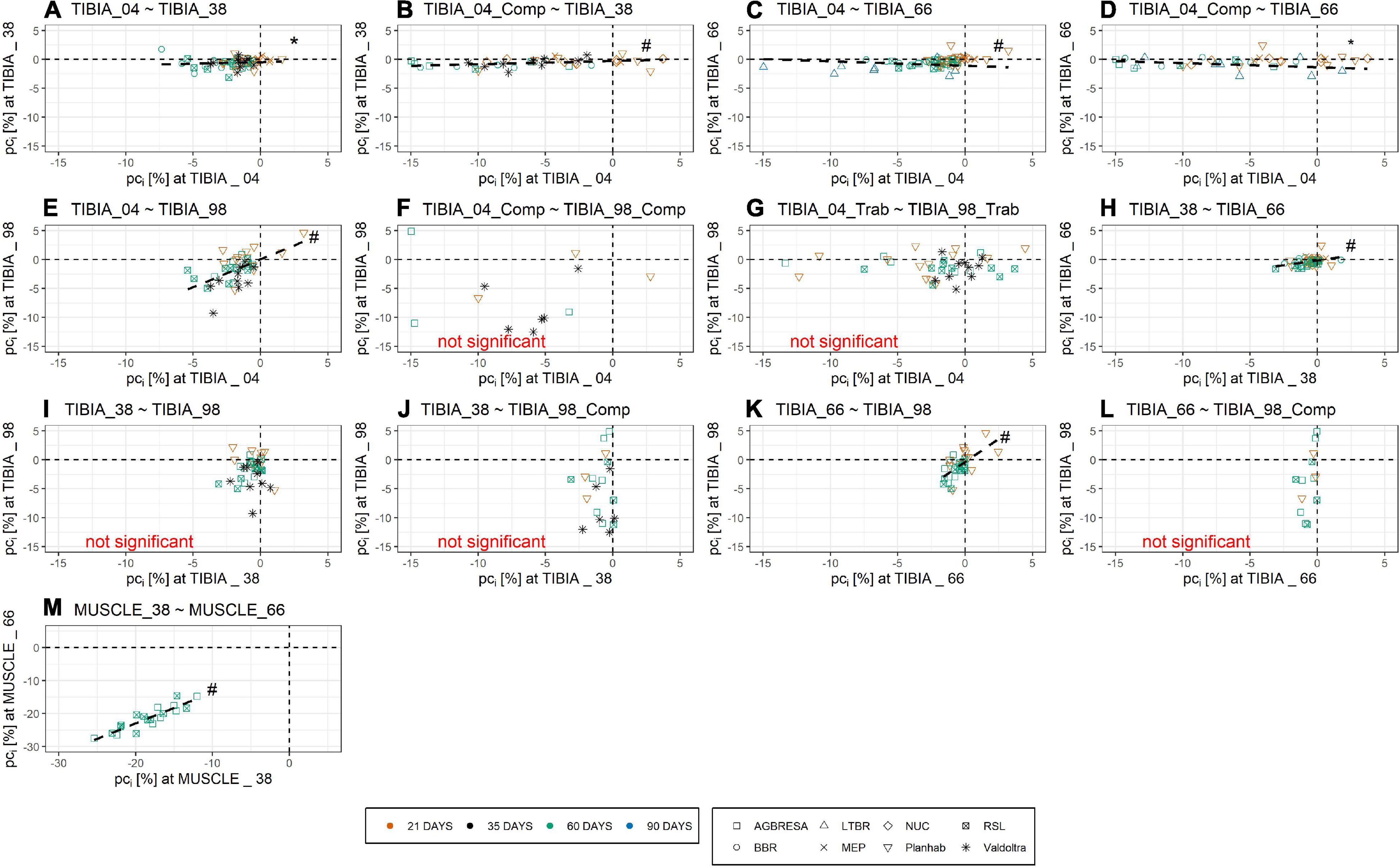
Figure 5. Pearson Correlation of pci of (A) TIBIA_04 and TIBIA_38, (B) TIBIA_04_Comp and TIBIA_38, (C) TIBIA_04 and TIBIA_66, (D) TIBIA_04_Comp and TIBIA_66, (E) TIBIA_04 and TIBIA_98, (F) TIBIA_04_Comp and TIBIA_98_Comp, (G) TIBIA_04_Trab and TIBIA_98_Trab, (H) TIBIA_38 and TIBIA_66, (I) TIBIA_38 and TIBIA_98, (J) TIBIA_38 and TIBIA_98_Comp, (K) TIBIA_66 and TIBIA_98, (L) TIBIA_66 and TIBIA_98_Comp, and (M) MUSCLE_38 and MUSCLE_66. Numbers indicate the relative measurement position regarding the entire tibia length from distal to proximal. Comp and Trab indicate compact and trabecular loss, respectively. The color indicates the bed rest duration and the shape represents the study. Several outliers are not shown in the figure due to graphical reasons, but are included in the linear regression analysis. Within the muscle sites, there was a strong positive correlation. The inter-site correlation of the bone sites ranged from no correlation to low positive correlation and moderate positive correlation. Strong positive correlation indicates no within-subject variation for the muscles, no correlation or low correlation indicates within-subject variation. Dashed line represents significant correlation. * denotes significant correlation with p < 0.01; # denotes significant correlation with p < 0.001.
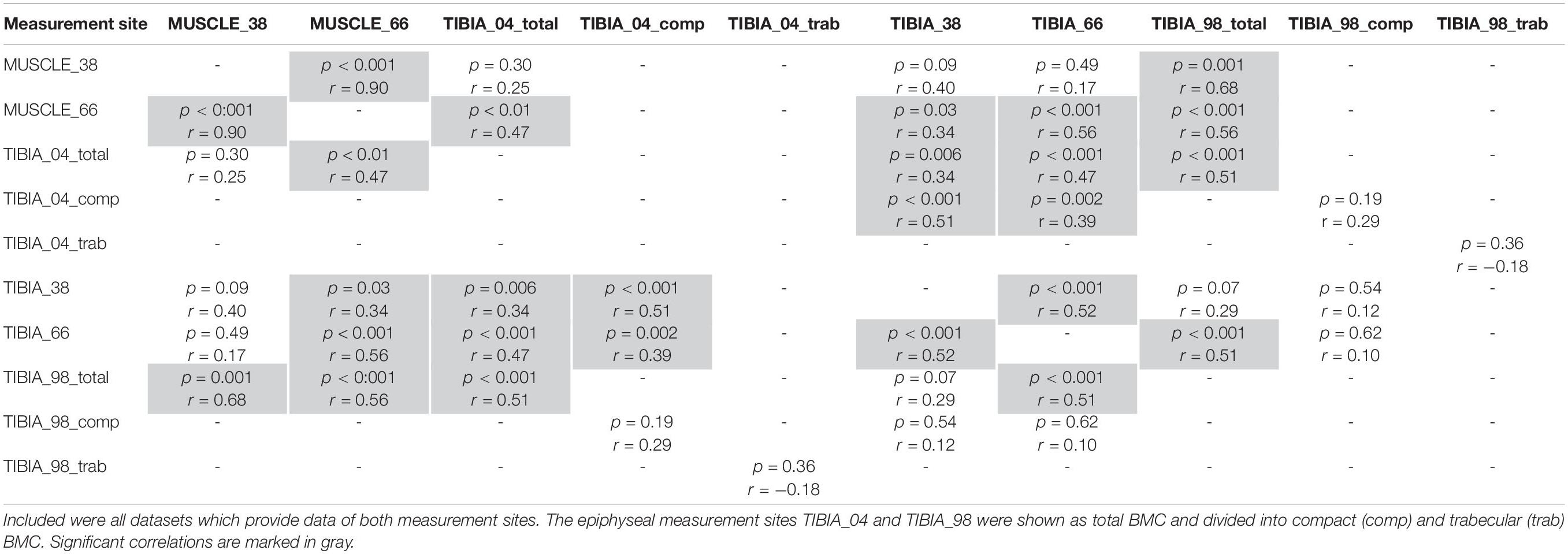
Table 5. Correlation (p-value and r) of percent change pck for CSA and BMC.
Figure 6 shows the relationship between ENDO and BL for all studies that provided BMC data for three or more bone sites. Linear regression analysis showed significant associations between ENDO and BL across the different studies (Supplementary Table 3) except for BBR (p = 0.93) and MEP (p = 0.07). However, these associations disappeared completely, when percent bone losses were plotted against the ratio of endocortical circumference to BMC, a maker of surface-to-volume ratio (Figure 7 and Supplementary Table 4).
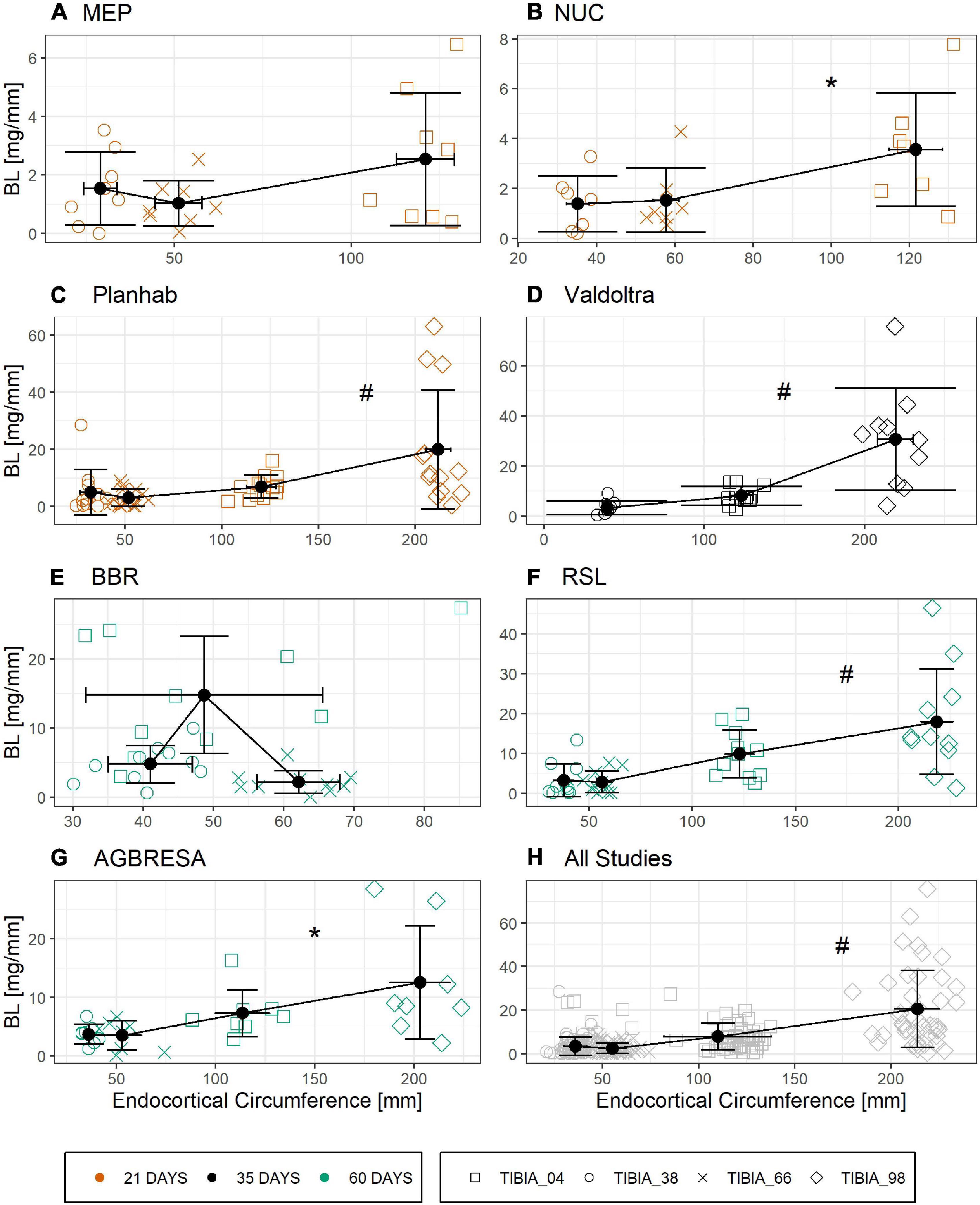
Figure 6. Linear relationship of Bone Loss BL in [mg/mm] and endocortical circumference ENDO [mm] divided by study with (A) MEP, (B) NUC, (C) Planhab, (D) Valdoltra, (E) BBR, (F) RSL, (G) AGBRESA, and (H) all studies. The color indicates the bed rest duration and the shape represents the measurement site. Numbers in the measurement site names indicate the relative measurement position regarding the entire tibia length from distal to proximal. Presented are studies with at least three out of four bone sites. Black points are the mean value of each measurement site with error bars of BL and ENDO. Linear regression analysis showed significant associations across the different studies except for BBR and MEP. * denotes significant relationship with p < 0.01; # denotes significant relationship with p < 0.001.
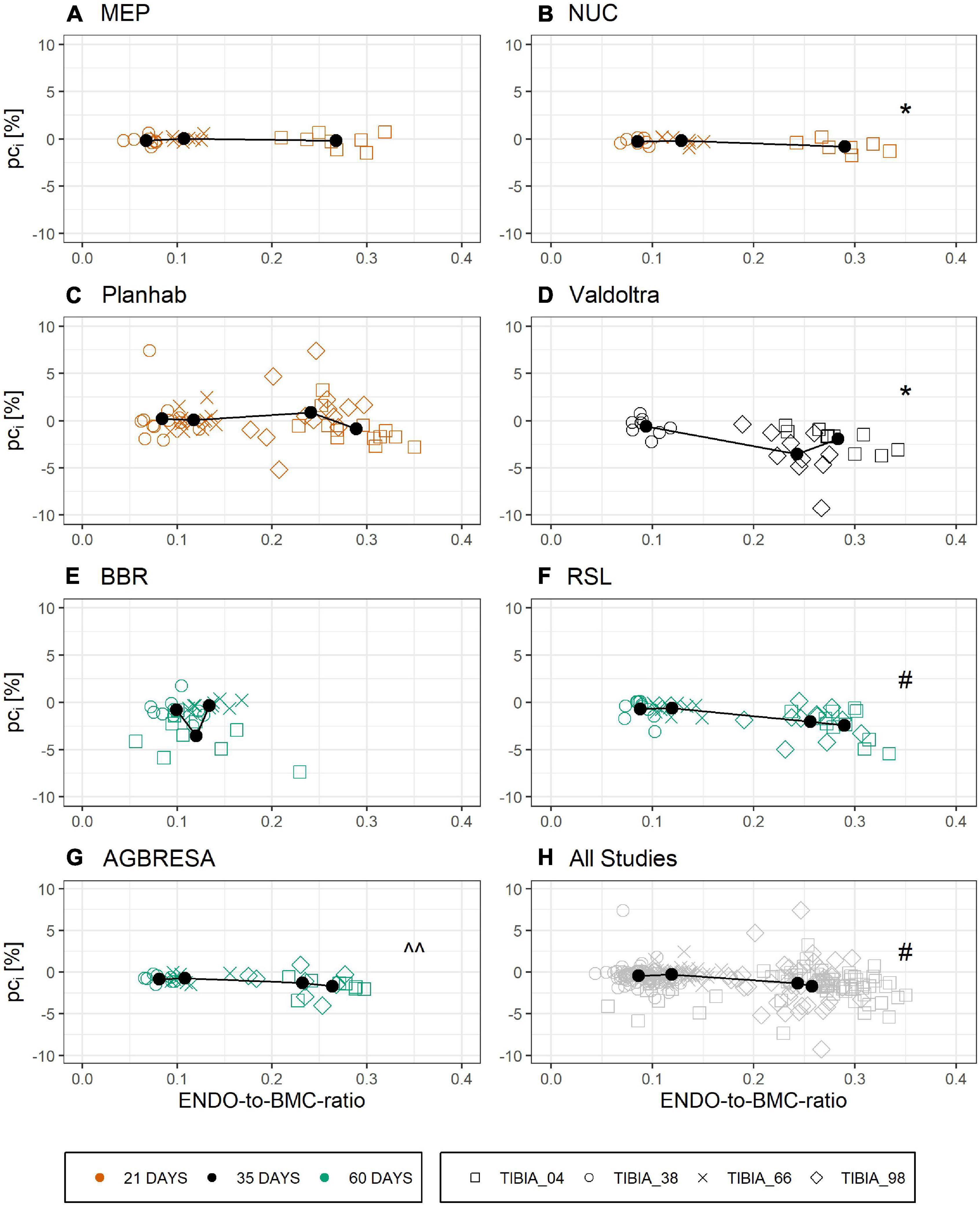
Figure 7. Linear relationship of ENDO-to-BMC-ratio at baseline and the individual pci by study with (A) MEP, (B) NUC, (C) Planhab, (D) Valdoltra, (E) BBR, (F) RSL, (G) AGBRESA, and (H) all studies. The color indicates the bed rest duration and the shape represents the measurement site. Numbers in the measurement site names indicate the relative measurement position regarding the entire tibia length from distal to proximal. Presented are studies with at least three out of four bone sites. Black points are the mean value of each measurement site. Linear regression analysis showed significant associations across the different studies except for BBR, MEP, and Planhab. ^^ denotes significant relationship with p < 0.05; * denotes significant relationship with p < 0.01; # denotes significant relationship with p < 0.001.
Analyses of BMC (mg/mm) of all bone sites with LMM showed that the variability among subjects (SD 47.1 mg/mm) was greater than the variability among studies (SD 4.9 mg/mm), and also greater than residuals (SD 37.7 mg/mm). The residual variability in BMC differed with measurement site: it was about 2.6 times greater for TIBIA_98 than for TIBIA_04, but lower for TIBIA_38 (by the factor 0.5) and TIBIA_66 (by the factor 0.07). For muscle (CSA in mm2), the variability among studies (SD 3.0 mm2) and subjects (8.9 mm2) were similar. Measurement site and study day were significantly associated with BMC and there was no association of ENDO or bed rest duration and BMC. Similar results were observed for CSA (Supplementary Tables 5, 6).
Discussion
This paper has separated within-subject variation, between-subject variation and measurement uncertainty in a set of control groups from previously bed rest studies, applying a statistical framework for quantifying these aspects. As previously published, bone loss and muscle wasting were generally observed across all studies, underlining the view of Hargens and Vico (2016). The main result of the present paper is that measurement uncertainty of the pQCT was small, and that it cannot explain the large variation of the adaptations after bed rest. In addition, results also demonstrate prominent within-subject variation for bone losses, but not for muscle wasting. Moreover, although some differences were found between studies, the general outcome was relatively homogeneous across studies.
Measurement Uncertainty
Over the almost two decades during which these studies were performed, we generally note a trend for an improvement in measurement precision, e.g., the difference from 2001/2002 during LTBR till 2015/2016 during RSL. The phenomenon is explained by the steady methodological improvements, especially in the scout view procedures. For example, during LTBR TIBIA_66 positioning was performed manually without scout views, due to the short z-range of the specific XCT2000 device used in that study, which did not allow using distal scout views. Moreover, a proximal scout view was not available at that time. A proximal scout view had become available in the Valdoltra study, albeit in the frontal plane only (Table 2 and Figure 1). These frontal plane knee scout views are often difficult to interpret and definition of a landmark on either of the two knee condyles or on the tibia plateau is inherently difficult. Therefore, introduction of sagittal scout viewing in the RSL study constituted further improvements as such sagittal scouts are much easier to interpret than frontal scout view.
In general, the measurement uncertainty was smaller for bone than for muscle sites. The observation may be explained by the fact that segmentation of muscle cross sections is somewhat more difficult than segmentation of bones. Moreover, orthostasis affects muscle volume. Although all leg muscle measurements were obtained after at least 60 min in the supine position, it is possible that these supine periods prior to pQCT sessions varied across studies, as well as prescription of fluid intake. As fluid redistribution is unlikely to affect BMC, inhomogeneity of fluid redistribution could have contributed to relative large measurement uncertainty for muscle sites. Possibly, different pQCT devices (Table 2) (LTBR: XCT2000 with short z-range; after LTBR XCT-devices with long z-range) are associated with different measurement error, but these are small (0.37% for XCT3000).
Finally, operator experience and skills also have a strong bearing on measurement precision when using pQCT. Therefore, it is recommendable to assess the measurement uncertainty in all bed rest studies, e.g., by performing two baseline measurements. The approach serves to differentiate measurement uncertainty from biological variation between subjects (Swinton et al., 2018) and also provides better estimates of baseline values, thus, increasing the statistical power of the experiment.
Between-Subject Variation
In general, the responses toward bed rest were homogenous across studies (Figure 2). Turning to between-subject variation, Figure 3 and Table 4 clearly demonstrate that it exists, both for bone loss as well as for muscle wasting, and that between-subject variation was greater for muscle than for bone than for muscle measures. In Figure 3, measurement uncertainty values were remarkably small for TIBIA_04, TIBIA_38 and TIBIA_66, and substantially larger for TIBIA_98 and the muscle sites. Regardless of the confidence interval width, the majority (59.1%) of the individual changes exceeded the interval. Notably, some individual participants showed positive values. The finding implies gains in CSA or BMC in the face of bed rest immobilization. However, such paradoxical gains were observed in the Planhab study only. The Planhab study involved only 21-day of bed rest, and average losses were therefore smaller than in studies with longer bed rest phases. In addition, there was only one baseline measurement in the Planhab study, which led to a less reliable baseline estimate and consequently also to a compromised reliability of the percent change. We therefore speculate that gains in bone mass and muscle CSA measurements may have been produced by a combination of small true changes in the study groups and limited reliability of individual percent changes. However, given the substantial between-subject variation observed in this study, by Scott et al. (2021) and the repeated observation of responders and non-responders to training interventions (McPhee et al., 2010; Mann et al., 2014; Hecksteden et al., 2015; Ahtiainen et al., 2016; Ross et al., 2019), blunted or even paradoxical responses to bed rest cannot be ruled out. We suggest that future bed rest studies should make further attempts at improving and unifying standard operating procedures for pQCT. In particular, two separate baseline measurements should be included whenever possible.
Figure 4 shows that the adjusted between-subject deviation (i.e., uncertainty of individual response relative to the averaged change per week for each study group) was greater for bone than for muscle. The observation is also confirmed by statistical analysis with linear mixed model, which has shown smaller adjusted between-subject deviation for muscle than for bone sites. Due to the fact that this manuscript referred to the data sets of the control groups only, it was impossible to use the already established approach of Hopkins (2015) and Atkinson and Batterham (2015), who compared the standard deviation of control and intervention group.
Within-Subject Variation
In addition to between-subject variation, the present study has also explored variation within subjects. A previous publication from the LTBR study reported significant correlation of bone losses at Tibia 66% with the other bone sites, but no such correlation among these other sites (Rittweger et al., 2005). In the present analysis of a much larger data base, these findings are replicated in that TIBIA_66 losses were correlated with losses at all other bone sites, even with the loss of compact bone tissue at TIBIA_04, but not at TIBIA_98. Yet, the present work did find correlations among the other bone sites, except between TIBIA_38 and TIBIA_98 (Figure 5 and Table 5). These significant correlations are consistent with individual traits in the bed rest responses of bone and muscle. However, all inter-bone site correlations (r between 0.34 and 0.52) were substantially weaker than the inter-muscle site correlation (r = 0.90). Looking at figures in Table 5, one might recognize a pattern of stronger correlations among diaphyseal sites (TIBIA_38 and TIBIA_66, r = 0.52), and of weaker correlations between epiphyseal and diaphyseal sites (r-values ranging between 0.29 and 0.51). Additionally, differentiating into compact and trabecular bone tissue at the epiphyseal bone sites showed that there were significant correlations between TIBIA_04_Cort and the diaphyseal sites, but no correlation to TIBIA_98_Cort, which could be explained by the fact that the compact bone tissue is often not thicker than the trabeculi at TIBIA_98. The comparison of the trabecular bone loss of the epiphyseal sites did not show any correlation, too. Overall, there seems to be little variability in the bed rest response within an individual’s calf musculature, while the tibia’s response exhibits substantial within-subject variation, even after dividing the epiphyseal measurement sites into compact and trabecular bone tissue.
Finally, it was observed that there were significant correlations between bone losses and muscle wasting, which are large for TIBIA_98 vs. either muscle sites (Table 5), but only moderate at best for the diaphyseal bone sites and for TIBIA_04. Bones adapt their structure to their mechanical environment (Frost, 1987; Rubin and Lanyon, 1987), and the greatest forces that bones are exposed to originate from regional muscle contractions (Rittweger, 2007). Consequently, bone strength measures typically depict large correlations with measures of muscle strength (Schiessl et al., 1998; Rittweger et al., 2000). Accordingly, previous studies had hypothesized to find correlations between individual muscle wasting and bone losses. However, such correlations never substantiated (Rittweger et al., 2005, 2010), at least at the diaphyseal and distal epiphyseal tibia sites and it had been proposed that bed rest is permissive, rather than inductive of bone loss (Rittweger et al., 2005). Large and highly significant correlations for the proximal epiphysis, which were observed in the present paper, are therefore unexpected. The question in how far the distal and proximal epiphysis differ deserves further study beyond the differences presented in this manuscript regarding adaptation of compact and trabecular bone tissue. However, the present study has much greater sample size than the aforementioned papers. Finding of a joint muscle-bone response also resonates with a recent report that habitual physical activity predicts space-flight induced bone losses (Gabel et al., 2021).
Origins of Variability
Muscles and bones fulfill mechanical roles for our organism and bed rest is foremost a model for the withdrawal of mechanical challenges. This withdrawal encompasses not only any habitual locomotor activities, but also participation in exercise and sports and it is also associated with metabolic derailments such as insulin resistance (Biensø et al., 2012). Given that there likely was substantial between-subject variation in exercise participation prior to participating in the bed rest studies, one could hypothesize that reductions in mechanical challenges varied between subjects, and that this variable reduction constitutes one origin of variability in bed rest response. Bed rest as well as spaceflight data support the idea (Rittweger et al., 2005; Gabel et al., 2021). Similarly, pre-study dietary habits may have varied between subjects, while the diet that is typically provided in ESA or NASA-funded bed rest studies is highly standardized. In many cases that diet will considerably deviate from the habitual intake patterns with expected effects on metabolism and adaptive processes. In addition, the well-established view of individual responsiveness to exercise interventions (McPhee et al., 2010; Mann et al., 2014; Hecksteden et al., 2015; Ahtiainen et al., 2016; Ross et al., 2019) also needs to be considered. This variable responsiveness may result from genetic and epigenetic pre-dispositions, which has been demonstrated, e.g., for the ACE ii/dd polymorphism (Montgomery et al., 1999; Valdivieso et al., 2017). Quite as much as in responses to increased mechanical and metabolic challenges, as in exercise training, genetic predispositions could also modulate the response to bed rest.
Finally, sizable variation in bone losses was observed between different tibia sites and bone tissues, but not between muscle sites. As a conclusion, changes in lifestyle like exercising and nutrition as well as genetic predisposition may largely explain variation in muscle wasting. But obviously, there may be additional factors causing the different inter-site bone losses. Possibly, the differences between muscle and bone variation could be explained by their participation in metabolic processes. For bone, the metabolic involvement is primarily in calcium and phosphate. Of the 1,000 g calcium in the human body, only 1 g is located outside bone. Moreover, rapid calcium transients cause electrophysiological disruptions that are potentially lethal. Accordingly, serum calcium levels have to be kept within bands that are extremely narrow when considering that the bone reservoir is 1,000 times larger than the extra-osseous pool. Moreover, bone surfaces are covered by bone lining cells, which constitute a relatively small amount of biomass in relation to the huge bone mass, and whose function it is to separate the ionic milieu in bone from the other fluid spaces (Rubinacci et al., 2002; Marenzana et al., 2005). High calcium-phosphate levels in the body fluids are known to foster extra-osseous calcifications, and, sub-clinical renal calculus formation can occur in spaceflight and bed rest alike, highlighting possible limitations in phospho-calcic excretion capability (Watanabe et al., 2004). Naturally, between-subject variation can be pertinent to that capability as well. This all results in the adaptive responses in bone being relatively slow, potentially with a variable degree of individual traits. Hence, extra-osseous factors involved in the handling end excretion of calcium could constitute another important source of between-subject variation in spaceflight- and immobilized bone losses.
Another important peculiarity of bone is the cellular mechanism by which it is degraded. When active, multi-nucleated osteoclasts resorb bone in a specific space, contrasting with skeletal muscle, where protein degradation likely occurs more uniformly in all cells. Moreover, different bone turnover rates strongly differ between tissue compartments as shown for the iliac crest by Balena et al. (1992), which is not direct transferable to the tibia, but could be a clue for osseous within-subject variation. These compartment-specific differences in the bone’s remodeling activity are likely the origin of the correlation between endocortical perimeter and BMC losses in Figure 6, thus confirming a previous finding. However, when using the ratio of endocortical perimeter to BMC as a marker of surface-to-volume ratio, all correlations with percent bone losses disappeared, indicating that bone “geometry” indicators do not predict individual losses (Figure 7). In addition, the linear mixed model showed that there was no association between endocortical circumference and BMC (Supplementary Table 5).
Preventing Worst Case Scenarios
Bed rest studies have so far focused on decrements in bone mass, muscle size etc., that were averaged within groups, and that were compared between control and countermeasure groups. This approach is straightforward to treat population means, but it could be problematic for single individuals. Provided the average bone loss in a long-term space mission at a given site is 1% per month and the between-subject SD of that loss is also 1% per month, the expected average loss is 12% during a 12-month mission. In addition, Gaussian distribution would predict that the largest bone loss in a 6-person crew will amount to 12% + 12% ⋅ 0.967 = 23.6%, with 0.967 being the upper tail quantile for 1/6 of the normal distribution. Therefore, when the aim is to safeguard the strongest responder to microgravity exposure of the crew members, a better understanding of between-subject variation becomes as important as averaged effectiveness of countermeasures.
Consequences of Variability
These above findings have important implications for the design and interpretation of bed rest studies. With regards to sample size estimation, if the scientists are interested in mean effects, one way to enhance study power is to increase the number of participants. Alternatively, one might try to diminish the influence of individual variations in study endpoints by better controlling for habitual physical activity and dietary habits. These covariates are highly controlled during, but not prior to the bed rest studies. However, subject recruitment for bed rest studies is already quite a challenge and expanding the list of inclusion and exclusion criteria would certainly hamper the feasibility of such studies. Moreover, even if it was possible to fully homogenize the response to the bed rest between subjects, the same homogenization would probably not be feasible for space missions. Therefore, it might be best to monitor, rather than to control putative pre-bed rest covariates in the future. At least, the habitual daily diet and physical activity need to be assessed by a detailed questionnaire. Definitely, these aspects should be transferred to future Astronaut recruitment, increased by analysis of the genetic predisposition and hormone analysis to make full use of the current available possibilities of individual response predictions. Especially the manned missions to Moon and Mars, which lasts clearly longer than the current missions and will have a greater demand on physical health, make an intense analysis of the predisposition regarding greater individual variations in bone loss and muscle wasting imperative.
Limitations
The assessment of measurement uncertainty was limited as only three out of eight studies provided two baseline measurements and the evaluated measurement sites differed among studies. To overcome this, the authors summarized results using the most similar condition. Enhanced estimation of measurement uncertainty could be achieved by increasing the baseline measurements of the same subjects on different days without any intervention. The analyses focused only on individual data of the control groups, thus the results of this paper are just valid for participants without any additional intervention besides bed rest. A further investigation of the intervention groups is needed. The intervention groups were excluded, because the aim of the paper was to do a first exploration of the relationship of measurement uncertainty, between-subject variation and within-subject variation, thus, additional intervention next to bed rest would complicate this approach. It needs to be mentioned that some of the included data sets are from cross-over design studies (Planhab, MEP, NUC), where participants underwent additional intervention, but there were well-dosed wash-out phases between interventions. The present evidence base comprises only two lower leg muscle sites and four tibia bone sites. However, obtaining data from more diverging bone and muscle sites would demand substantially greater subject time budgets, and also probably different technology such as full-size computed tomography or magnetic resonance imaging. By contrast, the strength of our data base is that it is used one single technology. Therefore, we trust that the principles of within-subject and between-subject variation in bone and muscle responses to bed rest, which have been firstly laid out here, may also apply to other anatomical sites. Yet, past studies have already shown that there is no bone loss in the upper extremity after bed rest (Hargens and Vico, 2016). Lastly, there may be additional factors affecting individual response that have not been captured.
Conclusion
Variation in muscle and bone responses to bed rest primarily results from between-subject and within-subject variation rather than measurement uncertainty. Nevertheless, measurement uncertainty should be considered in each data analysis, regardless of variation. It was observed that between-subject variation and within-subject variation were both lower for muscle than for bone sites. Training status, diet, and genetic predisposition may have contributed to the variation. The substantial variation in bone and muscle responses to deconditioning, be it in bed rest or during space missions, provides an impetus for a more individualized approach to countermeasure prescription.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Ethics Statement
The studies involving human participants were reviewed and approved by the local ethics committees. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
JB and JR created the idea of the manuscript. JB, M-TS, UM, and JR worked on the statistical approach. JR and UM provided the data of the measurements. JB analyzed the data and wrote the manuscript. JB, JR, M-TS, UM, and JJ edited and revised the manuscript. All authors contributed to the article and approved the submitted version.
Funding
The writing of this manuscript was funded by internal funding (Cost unit 2475030). However, the bed rest studies were funded as follows: AGBRESA by DLR, ESA (Contract No. 4000113871/15/NL/PG), and NASA (Contract No. 80JSC018P0078); BBR by ESA (Contract No. 14431/02/NL/SH2); participation at LTBR was funded by DLR (50 WB 0156); MEP by ESA and DLR (50WB1121); NUC by Microgravity Application Program of ESA and Space Directorate of the German Aerospace Center (DLR); Planhab by European Union Programme FP7 (Grant No. 284438), ESA (Contract No. 40001043721/11/NL/KML), and the Slovene Research Agency (Contract No. L3-3654); RSL by ESA (contract number 4000113871-15-NL); and Valdoltra by the Italian Space Agency (ASI), the Slovene Ministry of Defence, and the Gosta Fraenckel foundation for medical research.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We would like to thank all operators for conducting the measurements, which are the basis of this manuscript. Furthermore, we thank all participants, who took part in the several studies.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphys.2021.743876/full#supplementary-material
Footnotes
References
Ahtiainen, J. P., Walker, S., Peltonen, H., Holviala, J., Sillanpaa, E., Karavirta, L., et al. (2016). Heterogeneity in resistance training-induced muscle strength and mass responses in men and women of different ages. Age (Dordr.) 38:10. doi: 10.1007/s11357-015-9870-1
Atkinson, G., and Batterham, A. M. (2015). True and false interindividual differences in the physiological response to an intervention. Exp. Physiol. 100, 577–588. doi: 10.1113/EP085070
Atkinson, G., Williamson, P., and Batterham, A. M. (2019). Issues in the determination of ‘responders’ and ‘non-responders’ in physiological research. Exp. Physiol. 104, 1215–1225. doi: 10.1113/EP087712
Balena, R., Shih, M. S., and Parfitt, A. M. (1992). Bone resorption and formation on the periosteal envelope of the ilium: a histomorphometric study in healthy women. J. Bone Miner. Res. 7, 1475–1482. doi: 10.1002/jbmr.5650071216
Biensø, R. S., Ringholm, S., Kiilerich, K., Aachmann-Andersen, N. J., Krogh-Madsen, R., Guerra, B., et al. (2012). GLUT4 and glycogen synthase are key players in bed rest-induced insulin resistance. Diabetes 61, 1090–1099.
Blottner, D., Bosutti, A., Degens, H., Schiffl, G., Gutsmann, M., Buehlmeier, J., et al. (2014). Whey protein plus bicarbonate supplement has little effects on structural atrophy and proteolysis marker immunopatterns in skeletal muscle disuse during 21 days of bed rest. J. Musculoskelet. Neuronal Interact. 14, 432–444.
Borina, E., Pellegrino, M. A., D’Antona, G., and Bottinelli, R. (2010). Myosin and actin content of human skeletal muscle fibers following 35 days bed rest. Scand. J. Med. Sci. Sports 20, 65–73.
Capozza, R. F., Feldman, S., Mortarino, P., Reina, P. S., Schiessl, H., Rittweger, J., et al. (2010). Structural analysis of the human tibia by tomographic (pQCT) serial scans. J. Anat. 216, 470–481.
Debevec, T., Bali, T. C., Simpson, E. J., Macdonald, I. A., Eiken, O., and Mekjavic, I. B. (2014). Separate and combined effects of 21-day bed rest and hypoxic confinement on body composition. Eur. J. Appl. Physiol. 114, 2411–2425. doi: 10.1007/s00421-014-2963-1
Debevec, T., Ganse, B., Mittag, U., Eiken, O., Mekjavic, I. B., and Rittweger, J. (2018). Hypoxia aggravates inactivity-related muscle wasting. Front. Physiol. 9:494. doi: 10.3389/fphys.2018.00494
English, K. L., Lee, S. M. C., Loehr, J. A., Ploutz-Snyder, R. J., and Ploutz-Snyder, L. L. (2015). Isokinetic strength changes following long-duration spaceflight on the ISS. Aerosp. Med. Hum. Perform. 86(12 Suppl.), A68–A77. doi: 10.3357/AMHP.EC09.2015
Fitts, R. H., Trappe, S. W., Costill, D. L., Gallagher, P. M., Creer, A. C., Colloton, P. A., et al. (2010). Prolonged space flight-induced alterations in the structure and function of human skeletal muscle fibres. J. Physiol. 588(Pt. 18), 3567–3592.
Frett, T., Green, D. A., Mulder, E., Noppe, A., Arz, M., Pustowalow, W., et al. (2020). Tolerability of daily intermittent or continuous short-arm centrifugation during 60-day 6o head down bed rest (AGBRESA study). PLoS One 15:e0239228. doi: 10.1371/journal.pone.0239228
Fukunaga, T., Miyatani, M., Tachi, M., Kouzaki, M., Kawakami, Y., and Kanehisa, H. (2001). Muscle volume is a major determinant of joint torque in humans. Acta Physiol. Scand. 172, 249–255. doi: 10.1046/j.1365-201x.2001.00867.x
Gabel, L., Liphardt, A. M., Hulme, P. A., Heer, M., Zwart, S. R., Sibonga, J. D., et al. (2021). Pre-flight exercise and bone metabolism predict unloading-induced bone loss due to spaceflight. Br. J. Sports Med. 1–9. doi: 10.1136/bjsports-2020-103602
Hargens, A. R., and Vico, L. (2016). Long-duration bed rest as an analog to microgravity. J. Appl. Physiol. (1985) 120, 891–903. doi: 10.1152/japplphysiol.00935.2015
Hecksteden, A., Kraushaar, J., Scharhag-Rosenberger, F., Theisen, D., Senn, S., and Meyer, T. (2015). Individual response to exercise training – a statistical perspective. J. Appl. Physiol. (1985) 118, 1450–1459. doi: 10.1152/japplphysiol.00714.2014
Heer, M., Baecker, N., Wnendt, S., Fischer, A., Biolo, G., and Frings-Meuthen, P. (2014). How fast is recovery of impaired glucose tolerance after 21-day bed rest (NUC study) in healthy adults? Sci. World J. 2014:803083. doi: 10.1155/2014/803083
Hinkle, D., Wiersma, W., and Jurs, S. (2009). Applied Statistics for the Behavioral Sciences, 5th Edn. Boston: Cengage Learning Emea.
Hopkins, W. G. (2015). Individual responses made easy. J. Appl. Physiol. (1985) 118, 1444–1446. doi: 10.1152/japplphysiol.00098.2015
Kramer, A., Kummel, J., Mulder, E., Gollhofer, A., Frings-Meuthen, P., and Gruber, M. (2017). High-Intensity jump training is tolerated during 60 days of bed rest and is very effective in preserving leg power and lean body mass: an overview of the cologne RSL study. PLoS One 12:e0169793. doi: 10.1371/journal.pone.0169793
LeBlanc, A. D., Spector, E. R., Evans, H. J., and Sibonga, J. D. (2007). Skeletal responses to space flight and the bed rest analog: a review. J. Musculoskelet. Neuronal Interact. 7, 33–47.
LeBlanc, A., Rowe, R., Evans, H., West, S., Shackelford, L., and Schneider, V. (1997). Muscle atrophy during long duration bed rest. Int. J. Sports Med. 18(Suppl. 4), S283–S285.
Mann, T. N., Lamberts, R. P., and Lambert, M. I. (2014). High responders and low responders: factors associated with individual variation in response to standardized training. Sports Med. 44, 1113–1124. doi: 10.1007/s40279-014-0197-3
Marenzana, M., Shipley, A. M., Squitiero, P., Kunkel, J. G., and Rubinacci, A. (2005). Bone as an ion exchange organ: evidence for instantaneous cell-dependent calcium efflux from bone not due to resorption. Bone 37, 545–554. doi: 10.1016/j.bone.2005.04.036
Maughan, R. J., Watson, J. S., and Weir, J. (1983). Strength and cross-sectional area of human skeletal muscle. J. Physiol. 338, 37–49. doi: 10.1113/jphysiol.1983.sp014658
McPhee, J. S., Williams, A. G., Degens, H., and Jones, D. A. (2010). Inter-individual variability in adaptation of the leg muscles following a standardised endurance training programme in young women. Eur. J. Appl. Physiol. 109, 1111–1118. doi: 10.1007/s00421-010-1454-2
Montgomery, H., Clarkson, P., Barnard, M., Bell, J., Brynes, A., Dollery, C., et al. (1999). Angiotensin-converting-enzyme gene insertion/deletion polymorphism and response to physical training. Lancet 353, 541–545. doi: 10.1016/S0140-6736(98)07131-1
Narici, M. V., and de Boer, M. D. (2011). Disuse of the musculo-skeletal system in space and on earth. Eur. J. Appl. Physiol. 111, 403–420.
Pavy-Le Traon, A., Heer, M., Narici, M. V., Rittweger, J., and Vernikos, J. (2007). From space to Earth: advances in human physiology from 20 years of bed rest studies (1986-2006). Eur. J. Appl. Physiol. 101, 143–194.
Rittweger, J. (2007). “Physiological targets of artificial gravity: adaptive processes in bone,” in Artificial Gravity. The Space Technology Library, Vol. 20, eds G. Clément and A. Bukley (New York, NY: Springer), 191–231.
Rittweger, J., Albracht, K., Fluck, M., Ruoss, S., Brocca, L., Longa, E., et al. (2018). Sarcolab pilot study into skeletal muscle’s adaptation to long-term spaceflight. NPJ Microgravity 4:18. doi: 10.1038/s41526-018-0052-1
Rittweger, J., Belavy, D., Hunek, P., Gast, U., Boerst, H., Feilcke, B., et al. (2006). Highly demanding resistive vibration exercise program is tolerated during 56 days of strict bed-rest. Int. J. Sports Med. 27, 553–559.
Rittweger, J., Beller, G., Armbrecht, G., Mulder, E., Buehring, B., Gast, U., et al. (2010). Prevention of bone loss during 56 days of strict bed rest by side-alternating resistive vibration exercise. Bone 46, 137–147.
Rittweger, J., Beller, G., Ehrig, J., Jung, C., Koch, U., Ramolla, J., et al. (2000). Bone-muscle strength indices for the human lower leg. Bone 27, 319–326. doi: 10.1016/s8756-3282(00)00327-6
Rittweger, J., Frost, H. M., Schiessl, H., Ohshima, H., Alkner, B., Tesch, P., et al. (2005). Muscle atrophy and bone loss after 90 days’ bed rest and the effects of flywheel resistive exercise and pamidronate: results from the LTBR study. Bone 36, 1019–1029.
Rittweger, J., Simunic, B., Bilancio, G., De Santo, N. G., Cirillo, M., Biolo, G., et al. (2009). Bone loss in the lower leg during 35 days of bed rest is predominantly from the cortical compartment. Bone 44, 612–618.
Ross, R., Goodpaster, B. H., Koch, L. G., Sarzynski, M. A., Kohrt, W. M., Johannsen, N. M., et al. (2019). Precision exercise medicine: understanding exercise response variability. Br. J. Sports Med. 53, 1141–1153. doi: 10.1136/bjsports-2018-100328
Rubin, C. T., and Lanyon, L. E. (1987). Kappa Delta Award paper. Osteoregulatory nature of mechanical stimuli: function as a determinant for adaptive remodeling in bone. J. Orthop. Res. 5, 300–310. doi: 10.1002/jor.1100050217
Rubinacci, A., Covini, M., Bisogni, C., Villa, I., Galli, M., Palumbo, C., et al. (2002). Bone as an ion exchange system: evidence for a link between mechanotransduction and metabolic needs. Am. J. Physiol. Endocrinol. Metab. 282, E851–E864. doi: 10.1152/ajpendo.00367.2001
Schiessl, H., Frost, H. M., and Jee, W. S. (1998). Estrogen and bone-muscle strength and mass relationships. Bone 22, 1–6. doi: 10.1016/s8756-3282(97)00223-8
Scott, J. P. R., Kramer, A., Petersen, N., and Green, D. A. (2021). The role of long-term head-down bed rest in understanding inter-individual variation in response to the spaceflight environment: a perspective review. Front. Physiol. 12:614619. doi: 10.3389/fphys.2021.614619
Sibonga, J. D., Spector, E. R., Johnston, S. L., and Tarver, W. J. (2015). Evaluating bone loss in ISS astronauts. Aerosp. Med. Hum. Perform. 86(12 Suppl.), A38–A44. doi: 10.3357/AMHP.EC06.2015
Swinton, P. A., Hemingway, B. S., Saunders, B., Gualano, B., and Dolan, E. (2018). A statistical framework to interpret individual response to intervention: paving the way for personalized nutrition and exercise prescription. Front. Nutr. 5:41. doi: 10.3389/fnut.2018.00041
Timmons, J. A. (2011). Variability in training-induced skeletal muscle adaptation. J. Appl. Physiol. (1985) 110, 846–853. doi: 10.1152/japplphysiol.00934.2010
Valdivieso, P., Vaughan, D., Laczko, E., Brogioli, M., Waldron, S., Rittweger, J., et al. (2017). The metabolic response of skeletal muscle to endurance exercise is modified by the ACE-I/D gene polymorphism and training state. Front. Physiol. 8:993. doi: 10.3389/fphys.2017.00993
Vico, L., Collet, P., Guignandon, A., Lafage-Proust, M. H., Thomas, T., Rehaillia, M., et al. (2000). Effects of long-term microgravity exposure on cancellous and cortical weight-bearing bones of cosmonauts. Lancet 355, 1607–1611. doi: 10.1016/s0140-6736(00)02217-0
Watanabe, Y., Ohshima, H., Mizuno, K., Sekiguchi, C., Fukunaga, M., Kohri, K., et al. (2004). Intravenous pamidronate prevents femoral bone loss and renal stone formation during 90-day bed rest. J. Bone Miner. Res. 19, 1771–1778. doi: 10.1359/JBMR.040811
Keywords: between-subject variation, within-subject variation, measurement uncertainty, bed rest, muscle atrophy, bone loss
Citation: Böcker J, Schmitz M-T, Mittag U, Jordan J and Rittweger J (2022) Between-Subject and Within-Subject Variation of Muscle Atrophy and Bone Loss in Response to Experimental Bed Rest. Front. Physiol. 12:743876. doi: 10.3389/fphys.2021.743876
Received: 19 July 2021; Accepted: 30 December 2021;
Published: 22 February 2022.
Edited by:
Jonathan Paul Richard Scott, Medes, FranceReviewed by:
Susan Ann Bloomfield, Texas A&M University, United StatesOlga Vinogradova, Institute of Biomedical Problems, Russian Academy of Sciences (RAS), Russia
Copyright © 2022 Böcker, Schmitz, Mittag, Jordan and Rittweger. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jonas Böcker, Sm9uYXMuQm9lY2tlckBkbHIuZGU=