 Jialiang Gao
Jialiang Gao Guang Chen
Guang Chen Haoqiang He
Haoqiang He Chao Liu
Chao Liu Xingjiang Xiong
Xingjiang Xiong Jun Li1
Jun Li1 Jie Wang
Jie Wang
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Pharmacol., 23 May 2017
Sec. Ethnopharmacology
Volume 8 - 2017 | https://doi.org/10.3389/fphar.2017.00289
Breviscapine is a crude extract of several flavonoids of Erigeron breviscapus (Vant.) Hand.-Mazz., containing more than 85% of scutellarin, which has been traditionally used in China as an activating blood circulation medicine to improve cerebral blood supply. Accumulating evidence from various in vivo and in vitro studies has shown that breviscapine exerts a broad range of cardiovascular pharmacological effects, including vasodilation, protection against ischaemia/reperfusion (I/R), anti-inflammation, anticoagulation, antithrombosis, endothelial protection, myocardial protection, reduction of smooth muscle cell migration and proliferation, anticardiac remodeling, antiarrhythmia, blood lipid reduction, and improvement of erectile dysfunction. In addition, several clinical studies have reported that breviscapine could be used in conjunction with Western medicine for cardiovascular diseases (CVDs) including coronary heart disease, myocardial infarction, hypertension, atrial fibrillation, hyperlipidaemia, viral myocarditis, chronic heart failure, and pulmonary heart disease. However, the protective effects of breviscapine on CVDs based on experimental studies along with its underlying mechanisms have not been reviewed systematically. This paper reviewed the underlying pharmacological mechanisms in the cardioprotective effects of breviscapine and elucidated its clinical applications.
Erigeron breviscapus (Erigeron breviscapus (Vant.) Hand.-Mazz.), also known as Herba Erigerontis or Lamp Chrysanthemum, is a traditional Chinese herb that has been in use for more than 600 years, found in Yunnan, Sichuan, Guizhou, and other southwest provinces of China. It belongs to the daisy family, which is a perennial, clump-forming herb that can grow up to 50 cm (20 inches) tall, though in some cases it can be less than 1 cm (0.4 inches) tall. In addition, its flower heads have blue, purple, or white ray florets surrounding yellow disk florets (as shown in Figure 1). The dried whole plant of Erigeron breviscapus has been used in folk medicine for the treatment of paralysis, rheumatism, gastritis, toothache, and fever (Yunnan Institute of Materia Medica, 1976).

FIGURE 1. Erigeron breviscapus (A) flower; (B) whole plant.
Breviscapine is a crude extract of several flavonoids of Erigeron breviscapus (Vant.) Hand.-Mazz. (Zhang et al., 1988) that can be prepared into various forms including injection, granules, ordinary tablets, dispersible tablets, capsules, mixture, drop pills (Tian et al., 2014). To the best of our knowledge, the main active ingredient of breviscapine is scutellarin (Zhang et al., 1988). The use of breviscapine for the treatment of hypertension, cerebral embolism, and paralysis due to cerebrovascular accident dates back to the 1970s (Yunnan Institute of Materia Medica, 1976). Recent studies have suggested that breviscapine can be used to treat cerebral infarction and diabetic nephropathy. A meta-analysis of randomized and quasi-randomized controlled trials compared breviscapine plus routine therapy with routine therapy alone and showed a statistically significant benefit of using breviscapine for patient outcomes, with a marked neurologic improvement (Yang et al., 2012). Meanwhile, another meta-analysis of therapy combining breviscapine with mecobalamin for diabetic peripheral neuropathy suggested that the therapeutic efficacy of the combination was superior to mecobalamin alone (Liu et al., 2016). Another meta-analysis of the effect of breviscapine injection on the clinical parameters of diabetic nephropathy (Zheng et al., 2015) found significant renal protective effects (reduction in urine protein, serum creatinine and blood urea nitrogen) and adjustment for dyslipidaemia (effect on the levels of cholesterol, triglycerides (TG), and high-density lipoproteins).
Currently, because of its cardiovascular pharmacological effects (Tables 1, 2) and clinical benefits (Table 3), breviscapine has been extensively used in conjunction with Western medicine for the treatment of ischaemic cardiovascular disorders, such as angina pectoris and myocardial infarction (MI), in China (Cao et al., 2008; He et al., 2012). A meta-analysis to evaluate the efficacy and safety of breviscapine as an adjuvant therapy for patients with angina pectoris suggested that compared with the control group, the treatment group was superior in benefiting the patients with angina pectoris (Nie et al., 2012). In addition, breviscapine has been reported to have a broad range of cardiovascular pharmacological effects, including vasodilation, anti-thrombotic action, and platelet aggregation, anti-coagulation, scavenging of free radicals, and improvement in microcirculation, through various in vivo and in vitro experiments. Breviscapine has a series of pharmacological properties and is a kind of mixture of several flavonoids that can be used in clinical practice, but its underlying mechanism is still unclear.
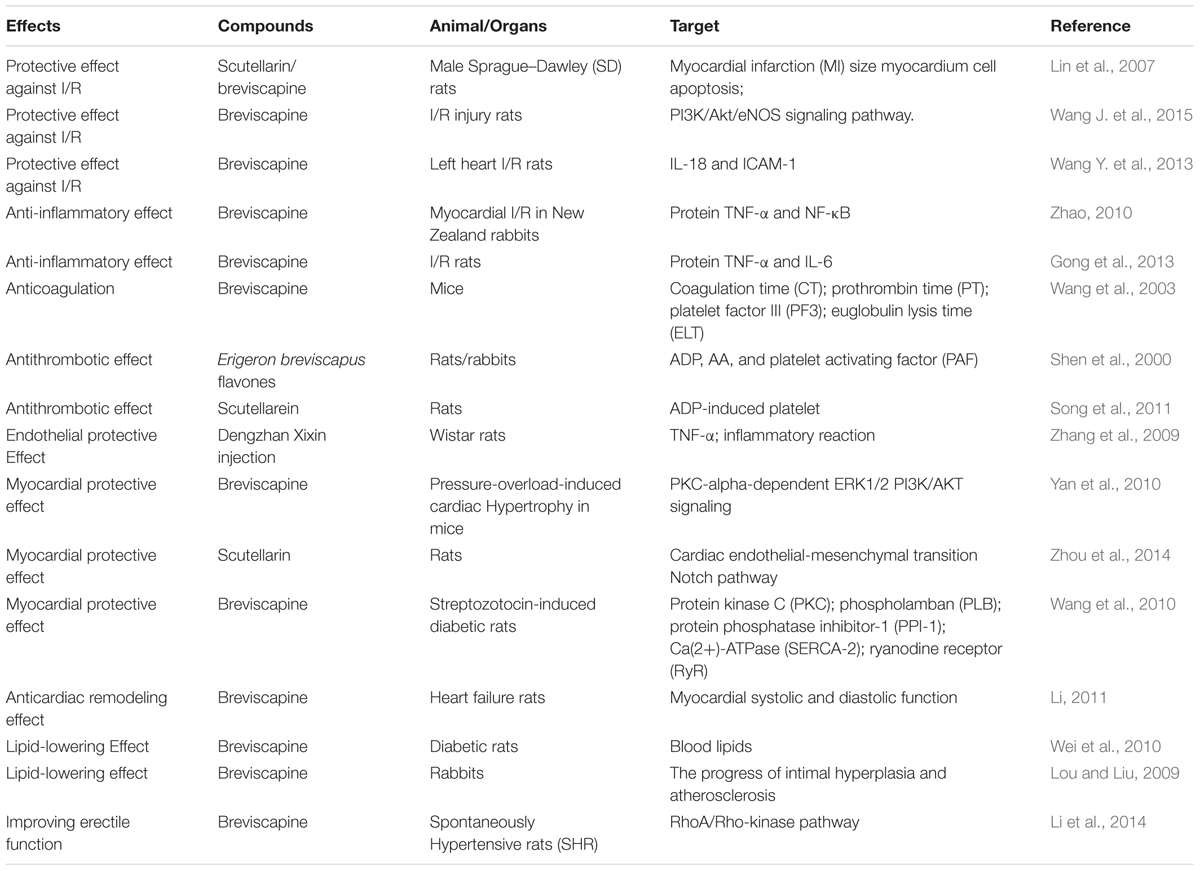
TABLE 1. In vivo cardiovascular effects of breviscapine and scutellarin.
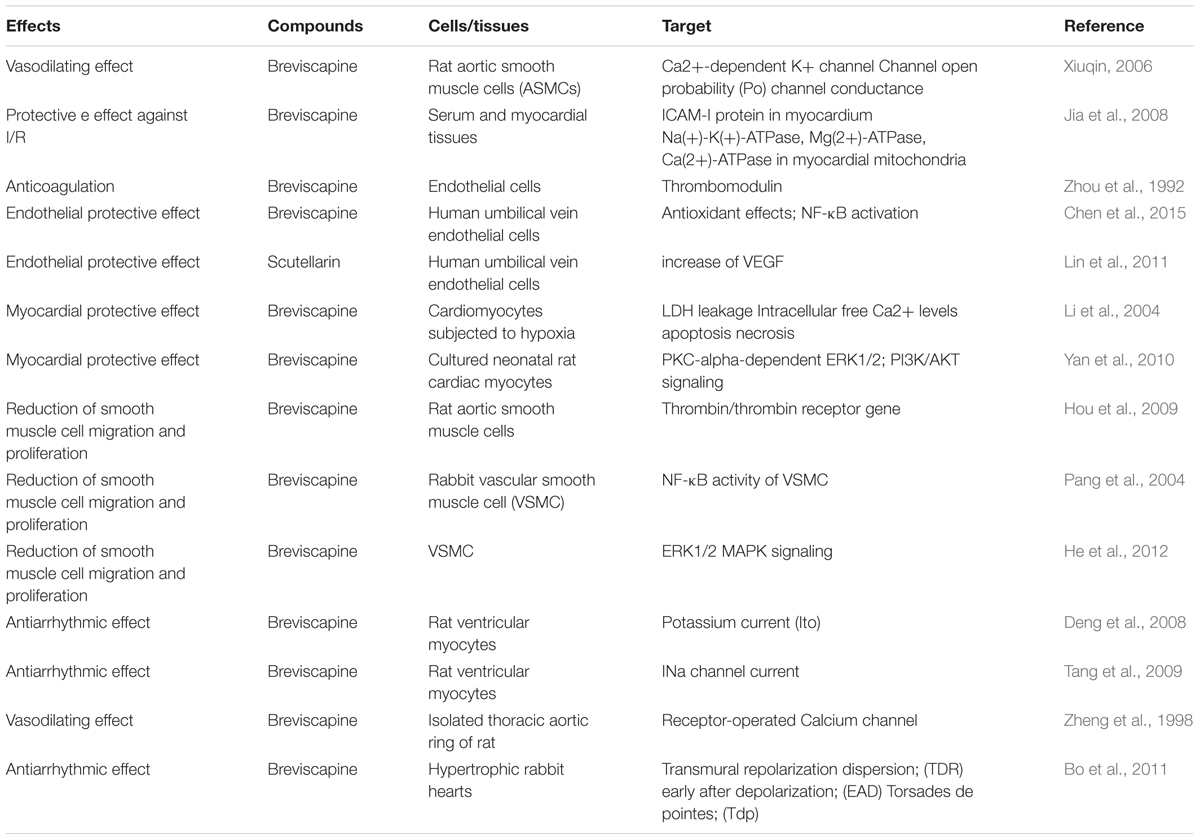
TABLE 2. In vitro cardiovascular effects of breviscapine and scutellarin.
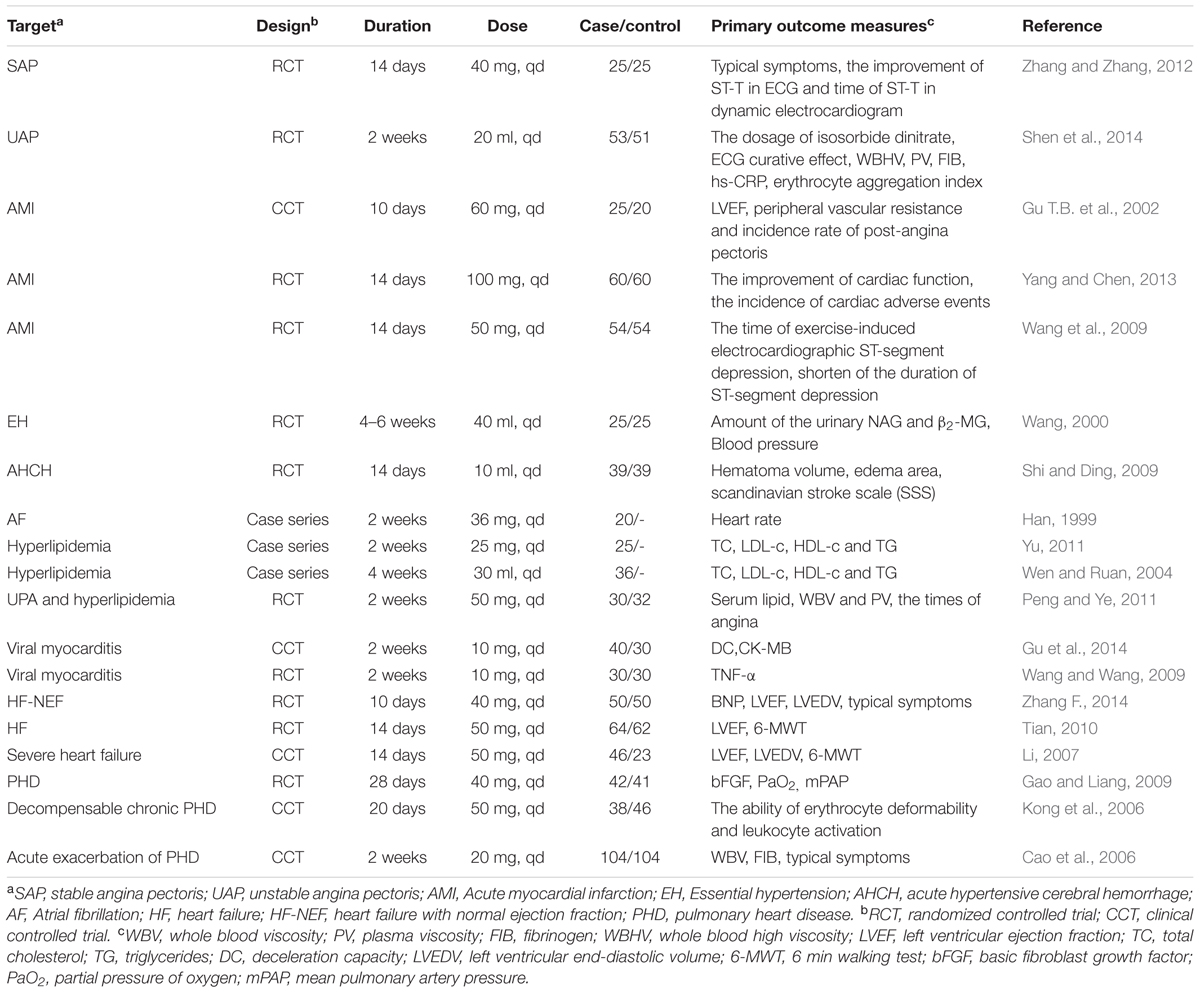
TABLE 3. Included trials of breviscapine for cardiovascular diseases.
The PubMed and SinoMed database were searched with the terms “Breviscapine” or “Erigeron breviscapus” or “Herba Erigerontis” or “Lamp Chrysanthemum” or “scutellarin” or “apigenin-7-O-glucuronide” or “dengzhanxixin” as “Title/Abstract” or the MeSH terms “Breviscapine” or “scutellarin-7-O-glucuronide”. Articles related to therapeutic effects in cardiovascular diseases (CVDs) were picked out manually. All articles with abstract were included and we applied no language restrictions.
Breviscapine mainly contains scutellarin (4′,5,6,7-tetrahydroxyflavone-7-O-glucuronide) and apigenin-7-O-glucuronide. Scutellarin is the primary active ingredient. Its molecular formula is C21H18O12, and its relative molecular mass is 462.35. Its chemical structure is shown in Figure 2. However, scutellarin has low aqueous solubility, poor chemical stability, short biological half-life and rapid elimination rate from the plasma (Hao et al., 2005; Lu et al., 2010). The chemical structure of apigenin-7-O-glucuronide is shown in Figure 3; its molecular formula is C21H18O11 and the relative molecular mass is 446 (Wu, 2011).
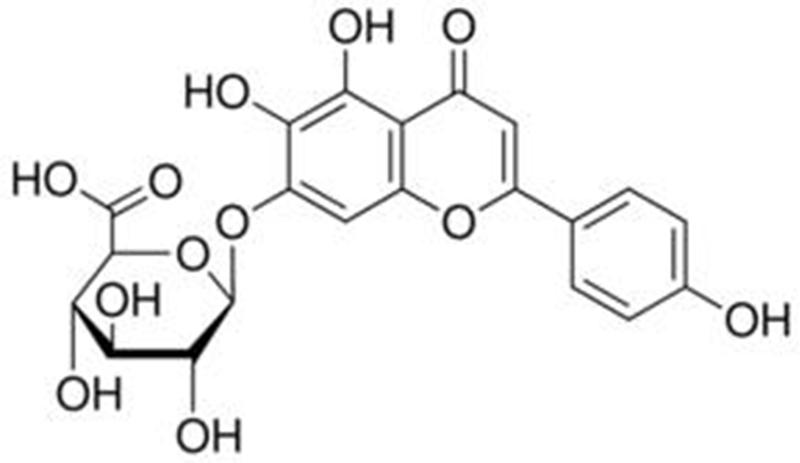
FIGURE 2. Structure of scutellarin.
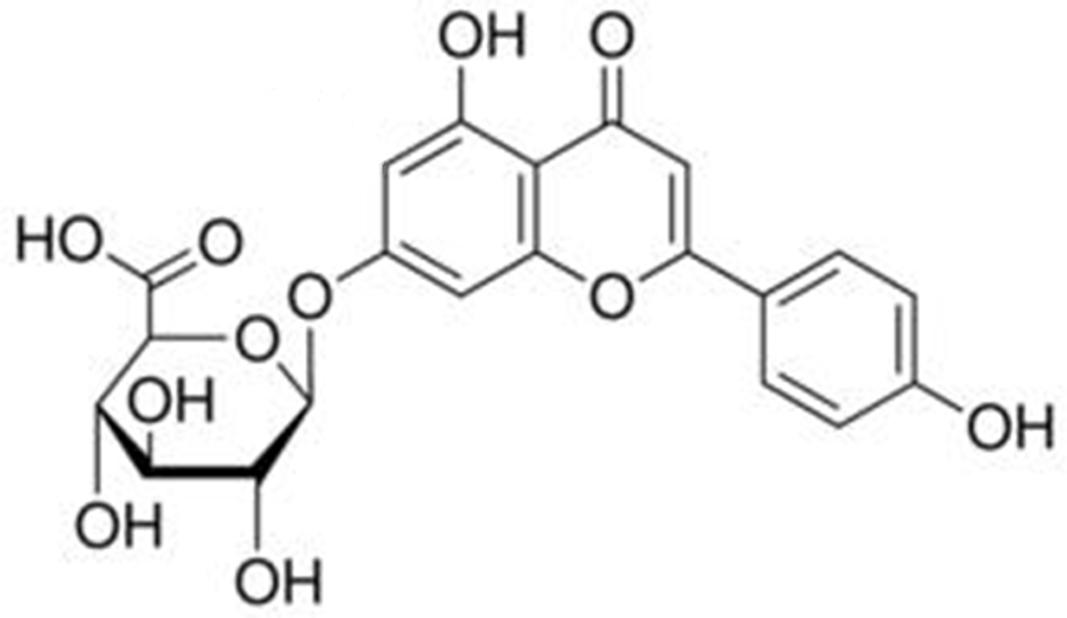
FIGURE 3. Structure of apigenin-7-O-glucuronide.
Vasculatures performing the function of maintaining vascular homeostasis play a vital role in both maintaining the blood pressure and providing the appropriate haemoperfusion according to dynamic physical conditions. As one of its regulatory mechanisms, the relaxation of vascular smooth muscles (VSM) can be triggered by the release of a series of endothelium-dependent and non-endothelium-dependent factors and has been demonstrated to be related to α-receptor, β-receptor, Ca2+ channel, and Ca2+-dependent K+ channel on the cell membrane (Furchgott, 1983; Rapoport et al., 1983; Tare et al., 1990; Bolotina et al., 1994). Based on in vitro studies, it has been concluded that breviscapine can relax norepinephrine-induced vasoconstriction in a concentration-dependent manner without influencing the function of the endothelium and without adjusting the α-receptors and β-receptors, even though it has been suggested that its vasodilation effect might be associated with the inhibition of the receptor-operated calcium channel (Zheng et al., 1998). There is another in vivo study showing that calcium activated potassium channels (KCa) can be activated by the application of breviscapine in rat aortic smooth muscle cells (ASMCs) via promoting the open probability (Po) of the channel and enhancing channel conductance (Xiuqin, 2006).
I/R injury often manifests as an aggravated endothelial impairment, leading to accelerated cardiomyocyte apoptosis or death, which can be measured by the size of MI (Kong et al., 2016; Yu et al., 2016). Studies have demonstrated that the protective effects of scutellarin alone on cardiovascular ischaemia are better than breviscapine with regards to the size of MI and myocardium cell apoptosis in MI rats, and its effects are dependent on the dose (Lin et al., 2007). The development of myocardial I/R injury has been shown to involve multiple mechanisms, including interference of specific pathways regulating the expression of some genes and activating relevant ATPase. One study suggested that breviscapine could provide significant protective effect against MI I/R injury, with the mechanism potentially involving the suppression of apoptosis of cardiomyocytes through the activation of the PI3K/Akt/eNOS signaling pathway (Wang J. et al., 2015). Moreover, as suggested by another study, breviscapine could inhibit the expression of IL-18 and ICAM-1 in protecting the lungs from inflammatory cascades (Wang Y. et al., 2013). In addition, the protective effects of breviscapine has been closely linked to the scavenging of oxygen free radicals, decreasing the expressions of ICAM-I protein in the myocardium and increasing the activities of Na(+)-K(+)-ATPase, Mg(2+)-ATPase, Ca(2+)-ATPase in the myocardial mitochondria (Jia et al., 2008).
Inflammatory processes play an important role in the development of CVDs and their associated complications (Ruparelia et al., 2017). Atherosclerosis is considered as an inflammatory disease (Ross, 1999). Many biological factors such as inflammatory cytokines, enzymes, and other mediators have been shown to be related to the effects of atherosclerosis (Walsh, 2003). It has been demonstrated that breviscapine is able to treat coronary disease and reduce the associated inflammatory response. The observed anti-inflammatory effects of breviscapine were demonstrated by a study comparing ischemic preconditioning with breviscapine and ischemic preconditioning alone; the combination treatment had better effect on decreasing the expression of TNF-α and NF-κB and reducing the injury due to inflammation to achieve myocardial protection during myocardial I/R in New Zealand rabbits (Zhao, 2010). Similarly, it could also decrease the expression of TNF-α and IL-6 to reduce the injury of I/R in rats (Gong et al., 2013).
The coagulation system and the anticoagulation and fibrinolytic systems interact dynamically, playing a major role in physiological haemostasis. On the other hand, this interaction might also be a common thread in a wide range of diseases, i.e., it might contribute to the pathology of various diseases, especially heart disease, cancer and inflammation (Marx, 1982). There is evidence that breviscapine can simulate fibrinolysis and anticoagulation of endothelial cells as indicated by the induction of thrombomodulin (TM) production and the downregulation of the expression of TM on the surface of the cells as well as the inhibition of TM release from the cells (Zhou et al., 1992). In addition, another study showed that the breviscapine extract influenced anticoagulation by significantly delaying the coagulation time (CT) and prothrombin time (PT), inhibiting the activity of platelet factor III (PF3) and decreasing the euglobulin lysis time (ELT); additionally, it could enhance the activity of fibrinolysis (Wang et al., 2003).
Pathogenic thrombi are responsible for acute clinical atherothrombotic diseases, such as acute coronary syndromes and ischaemic stroke. The activated platelets play a crucial role in the formation of pathogenic thrombi. During the process of platelet activation, specific agonists including thromboxane A2 (TxA2), adenosine diphosphate (ADP) and thrombin are associated with their corresponding receptors on the surface of platelets. Patients who suffered from atherothrombosis benefitted from the use of oral antiplatelet agents targeting the TxA2 (aspirin) and ADP (P2Y12 inhibitors such as clopidogrel, ticlopidine) platelet activation pathways (Fintel, 2012). One research showed that the Erigeron breviscapus flavones could significantly inhibit ADP, arachidonic acid (AA) and platelet activating factor (PAF) from forming into a thrombus (Shen et al., 2000). Meanwhile, another study suggested that scutellarin could prevent thrombosis and platelet aggregation and improve the characteristics of haemorheology by restricting the ADP-induced platelet aggregation rate in rats in a dose-dependent manner (Song et al., 2011).
Vascular endothelial cells (VECs) are important for the endocrine system and target organs (Salles et al., 2016). Damage to VECs can cause various vascular dysfunctions, frequently accompanied by endothelial cell injury, production of oxygen free radicals and release of inflammatory cytokines. One study showed that Dengzhan Xixin injection (the main ingredient is breviscapine) could reduce the damage of TNF-α to cardiac micro VECs by inhibiting the inflammatory reaction (Zhang et al., 2009). Meanwhile, breviscapine was shown to have a protective role in ox-LDL-induced endothelial cell injury, which may be related to its antioxidant effects and inhibition of NF-κB activation (Chen et al., 2015). Vascular Endothelial Growth Factors (VEGFs), the most potent angiogenic factors in both physiological and pathological angiogenesis, play a crucial step in the process of repair after injuries. Similarly, another study suggested that scutellarin had a protective effect on VECs after ischaemia-reperfusion injury, and the mechanism may be related to the early increase of VEGF (Lin et al., 2011).
When myocardial cells become injured by pathological factors such as cardiac surgery, ischaemia-reperfusion injury, diabetic injury, hypoxia injury, the pathological process may evolve from the initial cellular edema, degeneration, and necrosis into cardiac hypertrophy and myocardial fibrosis. There are several studies elucidating the potential myocardial protective effect of breviscapine and its mechanism. One study indicated that breviscapine favored myocardial protection by significantly reducing the LDH leakage, intracellular free Ca2+ levels, apoptosis and necrosis in cardiomyocytes subjected to hypoxia (Li et al., 2004). In case of diabetic injury, breviscapine may have a protective effect on diabetic cardiomyopathy by decreasing the expression of protein kinase C (PKC) and phospholamban (PLB), as well as increasing the expression of protein phosphatase inhibitor-1 (PPI-1), Ca(2+)-ATPase (SERCA-2), and ryanodine receptor (RyR) (Wang et al., 2010). In conditions of cardiac hypertrophy induced by angiotensin II (Ang II), it was demonstrated that breviscapine may still have a protective potential against cardiac hypertrophy by disrupting PKC-alpha-dependent ERK1/2 and PI3K/AKT signaling both in cardiac myocytes in vitro and mice in vivo (Yan et al., 2010). Another study also suggested that scutellarin could prevent isoprenaline-induced myocardial fibrosis by the inhibition of cardiac endothelial-mesenchymal transition, which may be associated with the Notch pathway (Zhou et al., 2014).
Vascular smooth muscle cell (VSMC) migration and proliferation is a major pathophysiological step in the development of atherosclerosis. In addition, modulation VSMC proliferation might have therapeutic effects for vascular diseases (Ross, 1993). Thrombin has been shown to induce VSMC proliferation. Thrombin receptor is present in all the cell types that respond to thrombin, including platelets, endothelial cells and VSMC. In addition, thrombin receptor antagonists could be used as therapeutic agents that might have value by specific inhibition of cellular proliferation (Pakala et al., 2001). There was a research suggesting that breviscapine could significantly inhibit the proliferation of rat aortic smooth muscle cells to induce thrombin. And the possible mechanism is blocking the expression of thrombin receptor gene (Hou et al., 2009). In addition, breviscapine could obviously inhibit the proliferation of VSMC and may prevent atherosclerosis, and the mechanism may be realized partly by regulating NF-κB activity of VSMC (Pang et al., 2004). Furthermore, breviscapine could ameliorate high glucose-induced proliferation and migration of VSMCs via inhibiting ERK1/2 MAPK signaling (He et al., 2012).
Ventricular remodeling is the process of pathological repair, ventricular compensation and a secondary pathophysiological response that is accompanied by a series of ventricular myocardial injury-associated changes in parameters including size, shape, wall thickness and tissue structure. One study suggested that breviscapine could regulate ventricular remodeling in heart failure animal by improving the myocardial systolic and diastolic function (Li, 2011).
Breviscapine has been shown to advance certain kinds of specific antiarrhythmic effects on the rabbit heart and rat ventricular myocytes, even though the underlying mechanism behind the effects remains unclear, and is still under research. One study showed that breviscapine could diminish the transmural repolarization dispersion (TDR) and reduced the incidence of early after depolarization (EAD) and torsades de pointes (Tdp), which decreased the incidence of ventricular arrhythmias in hypertrophic rabbit hearts (Bo et al., 2011). It has been demonstrated that cardiac electrical activities depend on the ion channels on membranes of cardiac cells for their physiological function. Then, concerns have been raised about affecting the potassium and sodium currents in ventricular myocytes. It has been observed that breviscapine could inhibit potassium current (Ito) in a concentration- and voltage-dependent manner (Deng et al., 2008) and INa channel current in a concentration-dependent manner (Tang et al., 2009), which might be an important mechanism in its antiarrhythmic effect.
Lipid-lowering is a routine treatment in CVDs. Some clinical studies have shown that breviscapine can reduce blood lipids. However, there have been different results in animal experiments. One study has shown that breviscapine could reduce blood lipid levels in diabetic rats (Wei et al., 2010). Another study suggested that it could inhibit the progress of intimal hyperplasia and atherosclerosis but could not reduce serum cholesterol levels (Lou and Liu, 2009). Additionally, there is no research explaining its mechanism of its lipid-lowering effect.
Impaired erectile response is one of the potential complications of essential hypertension. As mentioned in the 2013 ESH/ESC guidelines for the management of arterial hypertension (ESH/ESC Task Force for the Management of Arterial Hypertension, 2013), erectile dysfunction can be considered as an independent cardiovascular risk factor and an early diagnostic indicator for clinical organ damage. Therefore, efforts have been focused on finding out whether breviscapine could reverse hypertension-induced erectile dysfunction. It has been concluded that the impaired erectile response in spontaneously hypertensive rats (SHR) may be caused by the increased signaling by RhoA/Rho-kinase and decreased signaling by nitric oxide (NO). One study showed that breviscapine could improve erectile function by downregulating the RhoA/Rho-kinase pathway (Li et al., 2014).
Cardiovascular diseases are still the leading cause of death worldwide. Of the 57 million global deaths in 2008, more than 17.3 million (30%) were due to CVDs. Although the cardiovascular mortality rate has declined in many high-income countries in the past 2 decades, it has rapidly increased in low- and middle-income countries due to the lack of population-wide primary prevention and individual healthcare intervention (Mendis et al., 2011). Breviscapine is widely used in CVD prevention in China because of its effects on vasodilation, myocardial protection, anti-arrhythmia, decreasing arterial blood pressure, etc. Numerous studies have provided evidence to support these favorable effects; however, several studies have also reported adverse reactions, such as skin rashes, allergic shock, atrial fibrillation (AF), and diarrhea, occurring in CVDs (Liu and Bai, 2012; Zhang et al., 2016). This paper critically examines the scientific literature which reported the effects of breviscapine on cardiovascular diseases [coronary heart disease (CHD), MI, hypertension, arrhythmia, etc.]. Based on the methodology to perform this review, 19 trials were included in this review, among which there were 2 trials in CHD, 3 trials in MI, 2 trials in hypertension, 1 trial in arrhythmia, 3 trials in hyperlipidaemia, 2 trials in viral myocarditis (VMC), 3 trials in chronic heart failure (CHF), and 3 trials in pulmonary heart disease (PHD) (shown in Table 2).
Coronary heart disease is the most common type of CVD and one of the fatal diseases. The latest data showed that CHD led to 8.14 million deaths, which accounted for 16.8% of all deaths globally in 2013 (GBD 2013 Mortality and Causes of Death Collaborators, 2015). Currently, by changing lifestyle, such as exercising, having a healthy diet, treating hypertension, and medications, including anti-platelet drugs such as aspirin, nitro-glycerine, beta-blockers and statins, the morbidity of CHD has been reduced to some extent. However, these drugs also have some inevitable adverse effects. Breviscapine is a complementary medicine that has been used in combination with conventional medicine to prevent and treat CHD for decades in China. It provides many benefits; for example, it improves the therapeutic effectiveness compared to conventional treatment alone, and it helps to decrease the dosage of several drugs that may cause adverse effects (Wang C. et al., 2015). A large number of randomized, controlled trials have been carried out to explore the effects of breviscapine on CHD.
In one randomized controlled trial, 50 patients with stable angina pectoris were randomly allocated into two groups that received breviscapine (40 mg/250 ml 0.9% sodium chloride, iv drip, qd) combined with standard medication (n = 25) or standard medication alone (n = 25) for 14 days. The outcome showed that the symptoms of angina, the change of ST-T in ECG and the change time of ST-T in dynamic electrocardiogram improved more in the test group than in the control group. Additionally, the improvements in haemorheology, such as whole blood viscosity (WBV), plasma viscosity (PV), fibrinogen (FIB), and serum lipids in the test group were more remarkable than the control group (Zhang and Zhang, 2012). Similarly, another RCT was conducted to test the efficacy of breviscapine in patients with unstable angina pectoris, who were randomly assigned to receive 20 ml breviscapine daily in addition to conventional Western medicine (n = 53) or the conventional Western medicine alone (n = 51) for 2 weeks. The results demonstrated that the dosage of isosorbide dinitrate in the test group was lower than that in the control group and the curative effect on the ECG was better in the test group. In addition, the whole blood high viscosity (WBHV), PV, erythrocyte aggregation index, FIB and hs-CRP in the test group were also lower than that in the control group. Nevertheless, the researchers had not found a significant difference in the whole blood low shear viscosity and erythrocyte rigidity index between the two groups. In addition, this study reported 4 cases of nausea and 1 case of palpitation in the control group and 3 cases of nausea and 2 cases of abdominal distension in the test group (Shen et al., 2014).
MI, also known as acute myocardial infarction (AMI), is a heart attack caused by the blockage of blood flow to the heart due to a thrombus of a ruptured atherosclerotic plaque (Mendis et al., 2011). A study reported that the rate of MI has decreased globally between 1990 and 2010 (GBD 2013 Mortality and Causes of Death Collaborators, 2015). Although the morbidity and mortality of MI have been controlled to a large extent with early and effective preventive measures and interventions, there are still some problems in secondary prevention and rehabilitation of patients with MI. Chinese medicine (CM) shows some advantages in these aspects, such as improving the quality of life (QOL) and decreasing the rate of adverse events (Xu-Feng et al., 2010; Duan et al., 2012; Zhang Y.H., 2014). Several clinical studies with breviscapine have reported its effects on MI. A controlled clinical trial was designed to observe the efficacy of breviscapine in AMI patients who received either breviscapine (60 mg/d) with routine treatments (n = 25) or the routine treatments alone (n = 20) for a period of 10 days. The outcomes of left ventricular ejection fraction (LVEF), peripheral vascular resistance and incidence rate of post-angina pectoris were significantly different in the patients in the combination group compared to the patients in control group (Gu T.B. et al., 2002). Similarly, another RCT was conducted on 60 patients after percutaneous coronary intervention (PCI) who were treated with conventional medicine and breviscapine injection. The results showed that the proportion of cardiac function class ≤NYHA functional class II in the test group (88.3%) was higher than that in the control group (61.7%). In addition, the incidence of cardiac adverse events (MI, arrhythmia, death) was lower in test group (6.7%) compared to the control group (21.7%) (Yang and Chen, 2013). Another RCT was carried out to observe the effects of breviscapine on exercise tolerance in patients with AMI who have received a successful intravenous thrombolytic treatment. Ninety-eight patients were randomly assigned to receive breviscapine with conventional treatment or the conventional treatment alone for 14 days. The results of the treadmill exercise test showed a significant prolongation of the time of exercise-induced electrocardiographic ST-segment depression (≥0.1 mV) and shortening of the duration of ST-segment depression in the combination group than the control group on the 36th day. However, there was no significant difference on the 14th day. This implied that breviscapine might have sustained effects (Wang et al., 2009).
Hypertension results in 7.8 million deaths annually, accounting for 12.8% of the total deaths worldwide. The size of the population with uncontrolled blood pressure has grown from 6 million to nearly one billion between 1980 and 2008 (Mendis et al., 2011). Uncontrolled blood pressure is the major contributor not only to CHD and stroke but also to heart failure, chronic kidney disease, among others (Poulter et al., 2015). Herbal medicine combined with anti-hypertensive drugs are being increasingly used as an integrative therapy to control blood pressure and associated complications in both Eastern and Western countries (Ernst, 2005; Wang et al., 2012). A clinical trial studied the effects of erigeron injection on the renal function of elderly patients with essential hypertension. The result demonstrated that erigeron injection (the main ingredient is breviscapine) (40 ml, qd) had similar anti-hypertensive effect as enalapril (20 mg, qd). In addition, urinary NAG and β2-MG significantly decreased in the breviscapine group, which indicated that breviscapine might improve the tubular function of these patients (Wang, 2000). Another RCT aimed to investigate the efficacy of breviscapine in acute hypertensive cerebral hemorrhage patients. The patients were treated either with breviscapine plus routine Western medicine (n = 39) or routine Western medicine alone (n = 39) for 2 weeks. Outcomes of the haematoma volume, edema area and Scandinavian stroke scale (SSS) in breviscapine group were statistically better than those in control group (Shi and Ding, 2009).
In the clinical practice, most of the therapies for arrhythmia are medically indicated. However, AF, a serious type of arrhythmia (Munger et al., 2014), is still not easy to address. AF is a major cause of sudden cardiac death, which accounts for half of the death due to CVDs worldwide (Mehra, 2007). Although the anti-arrhythmic effect of breviscapine has been investigated in several animal studies, there are a few clinical trials. One case series of 30 elderly patients with persistent AF who received erigeron injection (36 mg, iv drip, qd) for 2 weeks reported that the heart rate in the patients decreased from 115.4 ± 8.2 to 83.3 ± 7.6 after the treatment. The reported adverse events included three cases of dizziness, which were spontaneously resolved (Han, 1999).
Hyperlipidaemia is abnormal increase of lipids in the blood, usually referred to the elevation of serum cholesterol and TG. High amount of cholesterol and TGs would increase the risk of CVDs. Data show that the prevalence of heart disease will decrease by 50% in 40-year-old men within five years if the serum cholesterol was reduced by 10% (Mendis et al., 2011). Thus, it is necessary to control the level of serum cholesterol and TGs. Animal studies have found that breviscapine can help lower elevated serum lipids. A clinical study was also carried out to observe its effects on patients with hyperlipidaemia. The results showed that the level of total cholesterol (TC), LDL-c, and TG decreased after a daily treatment with 25 mg breviscapine for 2 weeks. In contrast, the level of HDL-c increased (Yu, 2011). Another trial studied 36 elderly patients with hyperlipidaemia who received erigeron injection (30 mg, qd) for 2 weeks. A similar result was obtained (Wen and Ruan, 2004). Another RCT was designed to investigate the effect of breviscapine in patients with unstable angina pectoris with hyperlipidaemia. Neither the test group nor the control group received statins. The outcome of the serum lipid, WBV and PV showed statistically significant differences in the test group. Moreover, the duration of angina also decreased in the test group (Peng and Ye, 2011).
Viral myocarditis is an inflammation in the cardiac muscle due to a viral infection. It contributes to the development of heart failure. Currently, symptomatic treatment is the major treatment of VMC and other therapies, such as intravenous immunoglobulin (IVIG) or herbal medicine have not shown any evidence-based benefits (Robinson et al., 2005; Liu et al., 2012). Several studies have demonstrated the effects of breviscapine on VMC. A randomized controlled trial was designed to study the effect of breviscapine injection on the deceleration capacity (DC, a technique to quantitatively detect autonomic nerve tension) of the heart rate in children with VMC with daily administration of 10 mg breviscapine (n = 30) or 100 U coenzyme A (CoA) and 40 mg adenosine triphosphate (ATP) (n = 30) for 2 week. The results showed that there was a significant elevation of the DC in the breviscapine group compared to the control group. The investigators also found a more marked decrease in CK-MB in the test group than in the control group (Gu et al., 2014). Another study reported similar results; the investigators demonstrated the TNF-α, a cytokine that can reflect the degree of inflammation in the myocardium (Lenzo et al., 2001), noticeably dropped in the breviscapine group (Wang and Wang, 2009).
Chronic heart failure often occurs at the terminal stage of most CVDs. Epidemiological survey shows that the prevalence of CHF in adults in the developed countries is approximately 2%, and in China, it is 0.9% (Gu et al., 2002; Mcmurray and Pfeffer, 2005). Although 30–40% of the patients die within a year of CVD diagnosis, the mortality is less than 10% annually. The key problem that needs to be solved is the impact on the QOL, such as mood disorder (National Clinical Guideline Centre, 2010). In a randomized controlled trial, 100 stage NYHA III∼IV patients with heart failure with normal ejection fraction (HF-NEF) were instructed to take 40 mg/d breviscapine plus routine medication or the routine medication alone for 10 days. The outcome parameters demonstrated that the B-type natriuretic peptide (BNP) decreased more in the test group. However, there was no difference in the LVEF and left ventricular end-diastolic volume (LVEDV) between the test and control groups. In addition, the typical symptoms such as shortness of breath, chest tightness, fatigue, and weakness improved a lot in the test group than in the control group (Zhang F., 2014). One RCT was conducted in 126 stage NYHA II∼III patients who were randomly given breviscapine (50 mg, qd) with conventional medicine or the conventional medicine alone for 2 weeks. The results showed that the LVEF and 6-minute walk test (6 MWT) in the combination group was markedly better compared to the control group (Tian, 2010). Another clinical trial studied 46 stage NYHA III∼IV patients with severe heart failure and obtained similar results (Li, 2007).
Pulmonary heart disease leads to heart failure and/or respiratory failure. The pressure afterload is an initial step of the disease (Voelkel et al., 2013). At present, antibiotics, oxygen therapy, anticoagulants and vasodilators are the major treatments for PHD. Several studies have indicated the safety and effectiveness of Chinese medicine (Shenmai injection) combined with conventional treatment in this disease (Shi et al., 2015). There have also been some studies reporting the effects of breviscapine on PHD. A randomized controlled trial investigated the effects of breviscapine on 83 patients with PHD who were treated with conventional medicine plus 40 mg/d breviscapine or the conventional medicine alone for 28 days. The results demonstrated that the basic fibroblast growth factor (bFGF, a polypeptide that can induce vascular endothelial growth factor), partial pressure of oxygen (PaO2) and the mean pulmonary artery pressure (mPAP) noticeably improved in the breviscapine group (Gao and Liang, 2009). Another trial also observed the effects of breviscapine on PHD patients; the outcome of the erythrocyte deformability and leukocyte activation showed a significant difference between the breviscapine group and the control group. It has been suggested that breviscapine may prevent the progression of PHD by improving the erythrocyte deformability and leukocyte activation, which can affect the serum hypercoagulation state of patients with decompensated chronic PHD (Kong et al., 2006). One clinical trial investigated the effects of breviscapine on patients with acute exacerbation of PHD. The results showed that symptoms such as dyspnoea, cough, edema and cyanosis improved more in the test group than in the control group. In addition, there was an obvious decrease in some of the indexes such as WBV and FIB in the test group, which demonstrated the improvement in blood viscosity (Cao et al., 2006).
Breviscapine is widely used in clinics in the form of injection and oral administration. The recommended dosages of injection range from 5 to 20 mg per day at one time, and the dosages of oral administration range from 120 to 240 mg per day divided into three times. Due to its poor water solubility and low bioavailability in vivo, many new delivery methods have been designed and developed, including dispersion tablet, drop pill, liposome, nanoparticle, nanoemulsion, and lipid emulsion (Zhong et al., 2005; Patel et al., 2012; Ma et al., 2015). The adverse reaction of breviscapine mostly occurs during injection. One meta-analysis of the adverse reactions of breviscapine included 33 clinical studies of 1761 patients. Overall, 72 adverse reactions were reported, with an incidence rate of 4.09%. The adverse reactions included allergies, skin itching, rash, facial flushing, chest tightness, palpitation, dizziness/vertigo, headache, and gastrointestinal complaints. However, in this study, the investigators also found that there were no significant differences on the adverse reactions of the breviscapine injection compared with the counterpart medications, especially within 15 days (Feng et al., 2016). With regard to drug interactions, breviscapine could inhibit phenacetin metabolism mediated by CYP1A2 during short-term in vitro experiments (Qin et al., 2012) and inhibit the activity of CYP3A4 in vivo. Breviscapine also significantly increased the plasma concentration of dapsone in rats (Liu et al., 2013). The clinical safety and reasonable application of breviscapine injection clearly states that breviscapine is incompatible with the following drugs: ampicillin sodium, gentamicin sulfate, chloramphenicol, ciprofloxacin lactate, magnesium sulfate, procaine hydrochloride, cefradine, low molecular weight dextran, furosemide, and acetic acid hydrogenated prednisone (Zhao et al., 2008).
Traditional Chinese medicines (TCMs) continue to play an important role in the prevention and treatment of cardiovascular diseases in China. Unlike Western medicine, the holistic, and synergistic nature of TCMs arise from their herbal components, which contain hundreds of compounds and exert their effects on diseases via the binding of multiple compounds to multiple different targets to improve their performance on the systemic intervention of complex diseases. However, the mechanism of TCMs remains unclear, which makes it difficult for the rest of the world to understand how they work and prevent their global applications. Therefore, studies at the level of herbs might be a good way to provide comprehensive understanding of TCMs. Previously, one of the main strategies to study a compound prescription in TCMs has been to study its mechanism. Due to the presence of multiple compounds, it is always unclear which of the ingredients are producing real effects. The monomer component of Chinese herbal medicine (CHM), also known as the natural pure compound drug, has recently attracted much attention. The natural extract artemisinin and its derivatives are good examples of monomer components of CHM that can treat diseases through various activities, and can be a good starting point to uncover the mechanism of TCMs.
Similarly, a large number of monomer components of CHM with cardiovascular actions have been studied over the last few decades. For example, several systematic reviews have been conducted pertaining to salvianolic acid B (Wang J. et al., 2013), tetramethylpyrazine (Ming et al., 2016), Panax notoginseng saponins (Yang et al., 2014), etc. Among them, scutellarin, the principal component of breviscapine, is a type of monomer component of CHM and breviscapine has significant effects on vasodilation (improving erectile function); protection against I/R; anticoagulation and antithrombosis; reduction of smooth muscle cell migration and proliferation; anticardiac remodeling; antiarrhythmia, and reduction of blood lipids. Breviscapine also has a protective effects on myocardial and endothelial structures because of its anti-inflammatory effects. In addition, by reviewing the clinical studies, we believe that the most remarkable feature of breviscapine is its ability to perform multiple functions in regulating blood vessels, which are associated with cardiovascular diseases, stroke, and diabetes.
Though breviscapine has a wide range of cardiovascular effects on the prevention and treatment of CVDs, there are also a few problems that we need to consider. First, the above experimental studies that we reviewed focused on one aspect of the mechanism of breviscapine and very few studies could draw a definitive conclusion due to the low methodological quality, and none of the studies validated the findings both in vitro and in vivo. There were more studies investigating its properties of vasodilation, I/R and anticoagulation and antithrombotic effect than the other mechanisms. However, the results on its lipid-lowering effect in animal experiments were different in two studies. In addition, there was no study investigating its relevant mechanism. Second, since the studies were mainly published in China, the strength of the evidence was limited by the lack of controls or placebos, non-randomization, non-blinded design, and/or small samples of patients. Therefore, multicentred, large samples, and randomized controlled trials need to be done to evaluate the efficacy and safety of breviscapine for CVDs. Third, the side effects of breviscapine mostly occurred when it was injected, suggesting that suitable forms of delivery should be considered. In addition, patients with acute cerebral hemorrhage or bleeding tendency were excluded. Overall, it is very important to investigate the use of breviscapine for the treatment of CVDs. Nevertheless, all these pressing problems should be addressed in future studies.
JG and GC designed the work of review; JG, GC, HH, and CL reviewed the literature available on this topic and wrote the paper; XX and JL contributed in the scientific writing of the manuscript; JG, GC, and JW revised the manuscript. All authors approved the paper for publication. JG, GC, HH, and CL contributed equally to this work.
This paper was supported by The Innovative Funding for Ph.D. Students at China Academy of Chinese Medical Science, 2016CX003.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Bo, L. I., Zhao, G. A., Yin, G. T., Sun, H. Y., Gao-Ling, G. U., and Yang, X. L. (2011). Effect of breviscapine tablets on ventricular arrhythmias in hypertrophic myocardium of rabbit heart. J. Xinxiang Med. Coll. 2, 154–156.
Bolotina, V. M., Najibi, S., Palacino, J. J., Pagano, P. J., and Cohen, R. A. (1994). Nitric oxide directly activates calcium-dependent potassium channels in vascular smooth muscle. Nature 368, 850–853. doi: 10.1038/368850a0
Cao, R. B., Li-Hua, H. E., and Xiu-Zhen, H. E. (2006). Curative effects of eriseron breviscapus injection upon acutely aggravating stage of cor pulmonale. China J. Mod. Med. 16, 1560–1563.
Cao, W., Liu, W., Wu, T., Zhong, D., and Liu, G. (2008). Dengzhanhua preparations for acute cerebral infarction. Cochrane Database Syst. Rev. 63:CD005568. doi: 10.1002/14651858.CD005568.pub2
Chen, J. P., Ren, X. S., Sun, Z. H., and Guo, Z. Y. (2015). Protective effects and mechanisms of breviscapine on endothelial cells. J. Chin. Pharm. Univ. 5, 610–616.
Deng, C. Y., Tang, C. J., Kuang, S. J., Qian, W. M., Zi-Cheng, L. I., Wu, S. L., et al. (2008). Effect of breviscapin on I_(to) and I_(k1) channel current in isolated ventricular myocytes of rats. Chin. J. Pathophysiol. 24, 84–88.
Duan, W. H., Lu, F., Li, L. Z., Wang, C. L., Liu, J. G., and Yang, W. H. (2012). Clinical efficacy of traditional chinese medicine on acute myocardial infarction: a prospective cohort study. Chin. J. Integr. Med. 18, 807–812. doi: 10.1007/s11655-012-1116-9
Ernst, E. (2005). Complementary/alternative medicine for hypertension: a mini-review. Wien. Med. Wochenschr. 155, 386–391. doi: 10.1007/s10354-005-0205-1
ESH/ESC Task Force for the Management of Arterial Hypertension (2013). 2013 Practice guidelines for the management of arterial hypertension of the European Society of Hypertension (ESH) and the European Society of Cardiology (ESC): ESH/ESC Task Force for the Management of Arterial Hypertension. J. Hypertens. 31, 1925–1938. doi: 10.1097/HJH.0b013e328364ca4c
Feng, Y., Chen, H. Y., Yao, G. T., and Jin, N. M. (2016). Meta-analysis of clinical adverse reactions induced by breviscapine injection. J. Shanghai Univ. Tradit. Chin. Med. 4, 85–91.
Fintel, D. J. (2012). Oral antiplatelet therapy for atherothrombotic disease: overview of current and emerging treatment options. Vasc. Health Risk Manag. 8, 77–89. doi: 10.2147/VHRM.S26030
Furchgott, R. F. (1983). Role of endothelium in responses of vascular smooth muscle. Circ. Res. 53:557. doi: 10.1161/01.RES.53.5.557
Gao, X., and Liang, Q. (2009). Observe the curative effect of breviscapine in the treatment of chronic pulmonary heart disease. Inf. Tradit. Chin. Med. 26, 41–42.
GBD 2013 Mortality and Causes of Death Collaborators (2015). Global, regional, and national age–sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the global burden of disease study 2013. Lancet 385, 117–171. doi: 10.1016/S0140-6736(14)61682-2
Gong, M. Y., Du, C., and Yuan, B. Y. (2013). The effect of breviscapine on myocardial ischemia reperfusion in rats serum TNF- and IL-6. Lishizhen Med. Mater. Med. Res. 24, 1615–1616.
Gu, D., Huang, G., and He, J. (2002). Investigation of prevalence and distributing feature of chronic heart failure in Chinese adult population. Chin. J. Cardiol. 31, 3–6.
Gu, J., Bao, Q., Zhang, S., and Lei, S. (2014). Effects of dengzhanhuasu injection on deceleration capacity of heart rate in children with viral myocarditis. J. Pediatr. Pharm. 3, 23–25.
Gu, T. B., Shang, C. L., and Wang, W. X. (2002). Observation on acute myocardiac infarction treated by fleabane injection. J. Pract. Tradit. Chin. Med. 18, 8–9.
Han, F. (1999). Clinical observation on the treatment of Erigeron breviscapus injection for 30 cases of persistent atrial fibrillation. Med. J. Chin. Peoples Health 4, 57–58.
Hao, X., Cheng, G., Sun, J., Zou, M., Yu, J., Zang, S., et al. (2005). Validation of an hplc method for the determination of scutellarin in rat plasma and its pharmacokinetics. J. Pharm. Biomed. Anal. 38, 360–363. doi: 10.1016/j.jpba.2005.01.004
He, M., Xue, Z., Li, J., and Zhou, B. (2012). Breviscapine inhibits high glucose-induced proliferation and migration of cultured vascular smooth muscle cells of rats via suppressing the erk1/2 mapk signaling pathway. Acta Pharmacol. Sin. 33, 606–614. doi: 10.1038/aps.2012.6
Hou, S. S., Zhang, Q. H., and Zhang, Y. Q. (2009). The effect of breviscapine and thrombin receptor oligo-deoxy-nucleotides on thrombin induced proliferation of rat aortic smooth muscle cells. Tianjin Pharm. 19, 6–9.
Jia, J. H., Chen, K. P., Chen, S. X., Liu, K. Z., Fan, T. L., and Chen, Y. C. (2008). Breviscapine, a traditional Chinese medicine, alleviates myocardial ischaemia reperfusion injury in diabetic rats. Acta Cardiol. 63, 757–762. doi: 10.2143/AC.63.6.2033394
Kong, Q., Dai, L., Wang, Y., Zhang, X., Li, C., Jiang, S., et al. (2016). Hspa12b attenuated acute myocardial ischemia/reperfusion injury via maintaining endothelial integrity in a pi3k/akt/mtor-dependent mechanism. Sci. Rep. 6:33636. doi: 10.1038/srep33636
Kong, Q. F., Wei-Guo, L. I., Liu, F., Shen, Y. M., and Feng-Lan, L. I. (2006). Effect of breviscapine injection on the erythrocyte deformability, leukocyte activation and adhesive molecule cd11b expression in patients with decompensable chronic cor pulmonale. Int. J. Tradit. Chin. Med. 28, 278–281.
Lenzo, J. C., Fairweather, D. L., Shellam, G. R., and Lawson, C. M. (2001). Immunomodulation of murine cytomegalovirus-induced myocarditis in mice treated with lipopolysaccharide and tumor necrosis factor. Cell. Immunol. 213, 52–61. doi: 10.1006/cimm.2001.1859
Li, C. (2007). The effects of dengzhanhuasu injection on cardiac function and exercise capacity in patients with severe congestive heart failure. Chin. J. Mod. Drug Appl. 1, 4–6.
Li, X. L., Li, Y. Q., Yan, W. M., Li, H. Y., Xu, H., Zheng, X. X., et al. (2004). A study of the cardioprotective effect of breviscapine during hypoxia of cardiomyocytes. Planta Med. 70, 1039–1044. doi: 10.1055/s-2004-832644
Li, Y., Jiang, J., He, Y., Jiang, R., Liu, J., Fan, Z., et al. (2014). Icariin combined with breviscapine improves the erectile function of spontaneously hypertensive rats. J. Sex. Med. 11, 2143–2152. doi: 10.1111/jsm.12614
Li, Z. Z. (2011). The effect of breviscapine on hemodynamics in CHF rats. Harbing Med. J. 31, 426–427.
Lin, L., Hua, L., Cai, H. Y., and Yang, W. M. (2011). Effects of scutellarin on vascular endothelial growth factor and protein kinase c𝜀 expression in human umbilical vein endothelial cells after ischemia-reperfusion injury. J. Clin. Rehabil. Tissue Eng. Res. 20, 3723–3727.
Lin, L., Liu, A. J., Yu, X., Qin, L., and Su, D. (2007). Protective effects of scutellarin and breviscapine on brain and heart ischemia in rats. J. Cardiovasc. Pharmacol. 50, 327–332. doi: 10.1097/FJC.0b013e3180cbd0e7
Liu, X., Yao, L., Sun, D., Zhu, X., Liu, Q., Xu, T., et al. (2016). Effect of breviscapine injection on clinical parameters in diabetic nephropathy: a meta-analysis of randomized controlled trials. Exp. Ther. Med. 12, 1383–1397. doi: 10.3892/etm.2016.3483
Liu, Y., Li, X., Yang, C., Tai, S., Zhang, X., and Liu, G. (2013). Uplc-MS-MS method for simultaneous determination of caffeine, tolbutamide, metoprolol, and dapsone in rat plasma and its application to cytochrome p450 activity study in rats. J. Chromatogr. Sci. 51, 26–32. doi: 10.1093/chromsci/bms100
Liu, Y. P., and Bai, S. Q. (2012). Analysis of 12 cases of adverse reactions of breviscapine. Nei Mongol J. Tradit. Chin. Med. 31, 49–50.
Liu, Z. L., Liu, Z. J., Liu, J. P., Yang, M., and Kwong, J. (2012). Herbal medicines for viral myocarditis. Cochrane Database Syst. Rev. 11:CD003711. doi: 10.1002/14651858.CD003711.pub5
Lou, L., and Liu, H. (2009). Study on the mechanism of breviscapine to renal hypertrophy in type 2 diabetic rats. Lishizhen Med. Mater. Med. Res. 20, 86–87.
Lu, J., Cheng, C., Zhao, X., Liu, Q., Yang, P., Wang, Y., et al. (2010). PEG-scutellarin prodrugs: synthesis, water solubility and protective effect on cerebral ischemia/reperfusion injury. Eur. J. Med. Chem. 45, 1731–1738. doi: 10.1016/j.ejmech.2010.01.006
Ma, Y., Li, H., and Guan, S. (2015). Enhancement of the oral bioavailability of breviscapine by nanoemulsions drug delivery system. Drug Dev. Ind. Pharm. 41, 177–182. doi: 10.3109/03639045.2014.947510
Marx, J. L. (1982). Coagulation as a common thread in disease. Science 218, 145–146. doi: 10.1126/science.7123225
Mcmurray, J. J., and Pfeffer, M. A. (2005). Heart failure. Lancet 365, 1877–1889. doi: 10.1016/S0140-6736(05)66621-4
Mehra, R. (2007). Global public health problem of sudden cardiac death. J. Electrocardiol. 40, S118–S122. doi: 10.1016/j.jelectrocard.2007.06.023
Mendis, S., Puska, P., Norrving, B., Mendis, S., Puska, P., and Norrving, B. (2011). Global Atlas on Cardiovascular Disease Prevention and Control. Geneva: World Health Organization.
Ming, G., Yue, L., and Shi, D. (2016). Cardiovascular actions and therapeutic potential of tetramethylpyrazine (active component isolated from Rhizoma Chuanxiong): roles and mechanisms. Biomed. Res. Int. 2016:2430329. doi: 10.1155/2016/2430329
National Clinical Guideline Centre (2010). Chronic Heart Failure: National Clinical Guideline for Diagnosis and Management in Primary and Secondary Care: Partial Update. London: Royal College of Physicians.
Nie, X. L., Shen, H., Xie, Y. M., Hu, J., Zhang, Y. L., and Li, Y. Y. (2012). Meta-analysis of dengzhanxixin injection treatment for unstable angina pectoris. China J. Chin. Mater.Med. 37, 2768–2773.
Pakala, R., Liang, C. T., and Benedict, C. R. (2001). A peptide analogue of thrombin receptor-activating peptide inhibits thrombin and thrombin-receptor-activating peptide-induced vascular smooth muscle cell proliferation. J. Cardiovasc. Pharmacol. 37, 619–629. doi: 10.1097/00005344-200105000-00013
Pang, R. Q., Pan, X. H., Long, P. R., Qin, M., and Ya-Lin, W. U. (2004). Effect of breviscapine on the proliferation of rabbit vascular smooth muscle cells. Chin. J. Arterial Lerosis 12, 395–398.
Patel, T., Zhou, J., Piepmeier, J. M., and Saltzman, W. M. (2012). Polymeric nanoparticles for drug delivery to the central nervous system. Adv. Drug Deliv. Rev. 64, 701–705. doi: 10.1016/j.addr.2011.12.006
Peng, D., and Ye, G. U. (2011). Clinical observation on breviscapine injection on unstable angina pectoris combined with hyperlipidemia. J. Hubei Univ. Chin. Med. 13, 15–17.
Poulter, N. R., Prabhakaran, D., and Caulfield, M. (2015). Hypertension. Lancet 386, 801–812. doi: 10.1016/S0140-6736(14)61468-9
Qin, M., Liu, R., Liu, G., and Dong, F. (2012). Effects of breviscapines injections on cyp activities in rat liver microsomes in vitro. China Pharm. 15, 147–150.
Rapoport, R. M., Draznin, M. B., and Murad, F. (1983). Endothelium-dependent relaxation in rat aorta may be mediated through cyclic GMP-dependent protein phosphorylation. Nature 306, 174–176. doi: 10.1038/306174a0
Robinson, J., Hartling, L., Vandermeer, B., Crumley, E., and Klassen, T. P. (2005). Intravenous immunoglobulin for presumed viral myocarditis in children and adults. Cochrane Database Syst. Rev. 5:CD004370. doi: 10.1002/14651858.CD004370.pub2
Ross, R. (1993). The pathogenesis of atherosclerosis: a perspective for the 1990s. Nature 362, 801–809. doi: 10.1038/362801a0
Ross, R. (1999). Atherosclerosis – an inflammatory disease. N. Engl. J. Med. 340, 115–126. doi: 10.1056/NEJM199901143400207
Ruparelia, N., Chai, J. T., Fisher, E. A., and Choudhury, R. P. (2017). Inflammatory processes in cardiovascular disease: a route to targeted therapies. Nature Reviews Cardiology 14, 133–144. doi: 10.1038/nrcardio.2017.33
Salles, J. I., Duarte, M. E., Guimarães, J. M., Lopes, L. R., Vilarinho, C. J., Aguiar, D. P., et al. (2016). Vascular endothelial growth factor receptor-2 polymorphisms have protective effect against the development of tendinopathy in volleyball athletes. PLoS ONE 11:e0167717. doi: 10.1371/journal.pone.0167717
Shen, C. Q., Liu, Z. F., Ya-Ying, W. U., Yao, X. I., and Qian, Y. M. (2014). Clinical study of breviscapine injection on the treatment of unstable angina pectoris patients with coronary heart disease. Yunnan J. Tradit. Chin. Med. Mater. Med. 35, 23–26.
Shen, Z., Lei, W., Li, D., and Chen, Z. (2000). Inhibitory effects of Erigeron breviscapus flavones on platelet aggregation and thrombosis. Nat. Prod. Res. Dev. 12, 22–25.
Shi, L., Xie, Y., Liao, X., Chai, Y., and Luo, Y. (2015). Shenmai injection as an adjuvant treatment for chronic cor pulmonale heart failure: a systematic review and meta-analysis of randomized controlled trials. BMC Complement. Altern. Med. 15:418. doi: 10.1186/s12906-015-0953-4
Shi, Z. R., and Ding, J. B. (2009). Observe the curative effect of breviscapine in the treatment of 39 cases of hypertensive cerebral hemorrhage. Chin. J. Diffic. Complicat. Cases 8, 219–220.
Song, Y., Zhang, H. M., Ma, J. J., and Li, C. L. (2011). Effects of scutellarein on thrombosis and hemorheology in rats. Chin. J. New Drugs 20, 1446–1449.
Tang, C. J., Zi-Cheng, L. I., Deng, C. Y., Kuang, S. J., and Qian, W. M. (2009). Effect of breviscapin on I_(na) channel current in isolated rat ventricular myocytes. Chin. J. Pathophysiol. 25, 647–650.
Tare, M., Parkington, H. C., Coleman, H. A., Neild, T. O., and Dusting, G. J. (1990). Hyperpolarization and relaxation of arterial smooth muscle caused by nitric oxide derived from the endothelium. Nature 346, 69–71. doi: 10.1038/346069a0
Tian, L. H., Zhao, L. Z., Gu, J., Cai, J., and Yu, L. (2014). Breviscapine listed on progress of new varieties and dosage form research. China J. Chin. Mater. Med. 39, 3719–3722.
Tian, X. Z. (2010). Clinical observation of breviscapine in the treatment of chronic heart failure. Med. Innov. China 7, 54–55.
Voelkel, N. F., Gomezarroyo, J., Abbate, A., and Bogaard, H. J. (2013). Mechanisms of right heart failure—a work in progress and a plea for failure prevention. Pulm. Circ. 3, 137–143. doi: 10.4103/2045-8932.109957
Walsh, L. J. (2003). Mast cells and oral inflammation. Crit. Rev. Oral Biol. Med. 14, 188–198. doi: 10.1177/154411130301400304
Wang, C., Li, Y., Gao, S., Cheng, D., Zhao, S., and Liu, E. (2015). Breviscapine injection improves the therapeutic effect of western medicine on angina pectoris patients. PLoS ONE 10:e0129969. doi: 10.1371/journal.pone.0129969
Wang, H. B. (2000). Effect of Erigeron injection in renal early function of patients of primary hypertension in elderly. Mod. J. Integr. Tradit. Chin. West. Med. 18, 1744–1745.
Wang, J., Ji, S. Y., Liu, S. Z., Jing, R., and Lou, W. J. (2015). Cardioprotective effect of breviscapine: inhibition of apoptosis in h9c2 cardiomyocytes via the pi3k/akt/enos pathway following simulated ischemia/reperfusion injury. Pharmazie 70, 593–597.
Wang, J., Xiong, X., and Feng, B. (2013). Cardiovascular effects of salvianolic acid B. eCAM 2013:247948. doi: 10.1155/2013/247948
Wang, J., Yao, K., Yang, X., Liu, W., Feng, B., Ma, J., et al. (2012). Chinese patent medicine liu wei di huang wan combined with antihypertensive drugs, a new integrative medicine therapy, for the treatment of essential hypertension: a systematic review of randomized controlled trials. eCAM 2012:714805. doi: 10.1155/2012/714805
Wang, K. L., Huang, Y. H., and Zhang, Y. F. (2009). Observe the effects of breviscapine in exercise tolerance in patients with acute myocardial infarction after received a successful intravenous thrombolytic treatment. Proc. Clin. Med. 8, 1907–1909.
Wang, M., Zhang, W. B., Zhu, J. H., Fu, G. S., and Zhou, B. Q. (2010). Breviscapine ameliorates cardiac dysfunction and regulates the myocardial ca2+-cycling proteins in streptozotocin-induced diabetic rats. Acta Diabetol. 47, 209–218. doi: 10.1007/s00592-009-0164-x
Wang, S. M., and Wang, D. B. (2009). Breviscapine in the treatment of 30 children with viral myocarditis. Herald Med. 28, 599–600.
Wang, Y., Ji, M., Chen, L., Wu, X., and Wang, L. (2013). Breviscapine reduces acute lung injury induced by left heart ischemic reperfusion in rats by inhibiting the expression of icam-1 and il-18. Exp. Ther. Med. 6, 1322–1326. doi: 10.3892/etm.2013.1287
Wang, Y., Yang, X., Liu, H., and Tang, X. (2003). Study on effects of Erigeron breviscapus extract on anticoagulation. J. Chin. Med. Mater. 26, 656–658.
Wei, J. P., Li, J., Shi, Z., and Wang, Y. J. (2010). Inhibitory effect of Erigeron injection on the progression of atherosclerosis in rabbits. Lishizhen Med. Mater. Med. Res. 21, 750–751.
Wen, J. L., and Ruan, S. (2004). Clinical observation of 36 cases of Erigeron Injection in the treatment of elderly patients with hyperlipidemia. Guangdong Med. J. 25, 163.
Wu, T. (2011). The Total Synthesis of a Flavonoid Glyeoside Apigenin- 7-O-p-D-Glucuronid. Master’s thesis, Kunming University of Science and Technology, Kunming.
Xiuqin, L. I. (2006). Activation of breviscapine to calcium-activated potassium channels in rat aortic smooth muscle. J. Clin. Cardiol. 22, 351–353.
Xu-Feng, L. I., Liu, F., Jiang, T. L., Wang, Z. J., Han, Y. H., and Zhi-Hong, W. U. (2010). Efficacy of compound danshen drop pill in 42 patients with early acute myocardial infarction. Chin. J. New Drugs 18, 1699–1702.
Yan, L., Huang, H., Tang, Q. Z., Zhu, L. H., Wang, L., Liu, C., et al. (2010). Breviscapine protects against cardiac hypertrophy through blocking PKC-alpha-dependent signaling. J. Cell. Biochem. 109, 1158–1171. doi: 10.1002/jcb.22495
Yang, N. R., and Chen, Q. X. (2013). The effect observation of breviscapine for improving PCI curative myocardial function. Chin. J. Mod. Drug Appl. 7, 23–24.
Yang, W., Cheng, H., Xie, Y. M., Yang, H., and Zhuang, Y. (2012). Dengzhanxixin injection using character analysis in clinical based on real world his database. China J. Chin. Mater. Med. 37, 2718–2722.
Yang, X., Xiong, X., Wang, H., and Wang, J. (2014). Protective effects of panax notoginseng saponins on cardiovascular diseases: a comprehensive overview of experimental studies. Evid. Based Complement. Alternat. Med. 2014:204840. doi: 10.1155/2014/204840
Yu, H., Zhang, H., Zhao, W., Guo, L., Li, X., Li, Y., et al. (2016). Gypenoside protects against myocardial ischemia-reperfusion injury by inhibiting cardiomyocytes apoptosis via inhibition of chop pathway and activation of pi3k/akt pathway in vivo and in vitro. Cell. Physiol. Biochem. 39, 123–136. doi: 10.1159/000445611
Yu, X. P. (2011). Study on effect of breviscapine injection in the treatment of patients with hyperlipidemia and its mechanism. Pract. Clin. J. Integr. Tradit. Chin. West. Med. 11, 20–21.
Yunnan Institute of Materia Medica (1976). Study on the chemical constituents of Erigeron breviscapus. Chin. Tradit. Herbal Drugs 11, 11–14. Yunnan institute of materia medica as.
Zhang, F. (2014). The effect of breviscapine on heart failure patients with normal ejection fraction. Guangdong Med. J. 35, 3254–3256.
Zhang, H., Wang, X. Y., Liu, Y., Chai, L. J., Wang, H., Zhang, B. L., et al. (2009). Effects of dengzhan xixin injection on inflammatory cytokine production in rat cardiac microvascular cells induced by tumor necrosis factor. J. Chin. Pharm. Sci. 44, 1791–1795.
Zhang, Q. M., and Zhang, F. L. (2012). Clinical observation on the curative effect of breviscapine powder injection in treating heart stroke of coronary heart disease. Tianjin J. Tradit. Chin. Med. 29, 133–135.
Zhang, R. W., Zhang, Y. L., Wang, J. S., Lin, Y. Y., and Shang, B. (1988). Isolation and identification of flavonoids from shortscape fleabane (Erigeron breviscapus). Chin. Tradit. Herb Drugs 19:7.
Zhang, S., Liu, J. Y., Zhao, L., Lei, K., and Liu, Y. (2016). Analysis of 204 cases of adverse drug reactions caused by breviscapine injection. Chin. J. Hosp. Pharm. 36, 1585–1588.
Zhang, Y. H. (2014). Effect of Wenxin Granule combined with metoprolol on major cardiovascular acute myocardial infarction after PCI. Chin. J. Integr. Med. Cardiol. 12, 180–182.
Zhao, G. (2010). Experimental study of effect of combining breviscapine with ischemic/preconditioning on the expression of myocardial protein tumor necrosis factor-α, nuclear factor-kappa b during myocardial ischemia/reperfusion in rabbits. J. Clin. Cardiol. 8, 631–634.
Zhao, Z. G., Gao, H. C., and Wang, A. G. (2008). Clinical Safety and Rational Application of Injection. Beijing: Chemical Industry Press.
Zheng, C., Ou, W., Shen, H., Zhou, Z., and Wang, J. (2015). Combined therapy of diabetic peripheral neuropathy with breviscapine and mecobalamin: a systematic review and a meta-analysis of Chinese studies. Biomed. Res. Int. 2015:680756. doi: 10.1155/2015/680756
Zheng, G., Dong, Y., and Liang, Y. (1998). Effects of breviscapine on isolated rat thoracic aortic ring. Chin. Tradit. Herbal Drugs 10, 680–683.
Zhong, H., Deng, Y., Wang, X., and Yang, B. (2005). Multivesicular liposome formulation for the sustained delivery of breviscapine. Int. J. Pharm. 301, 15–24. doi: 10.1016/j.ijpharm.2005.04.001
Zhou, H., Chen, X., Chen, L., Zhou, X., Zheng, G., Zhang, H., et al. (2014). Anti-fibrosis effect of scutellarin via inhibition of endothelial-mesenchymal transition on isoprenaline-induced myocardial fibrosis in rats. Molecules 19, 15611–15623. doi: 10.3390/molecules191015611
Keywords: breviscapine, Chinese medicine, ethnopharmacology, herbal medicine, herbal active compounds
Citation: Gao J, Chen G, He H, Liu C, Xiong X, Li J and Wang J (2017) Therapeutic Effects of Breviscapine in Cardiovascular Diseases: A Review. Front. Pharmacol. 8:289. doi: 10.3389/fphar.2017.00289
Received: 10 January 2017; Accepted: 05 May 2017;
Published: 23 May 2017.
Edited by:
Adolfo Andrade-Cetto, National Autonomous University of Mexico, MexicoReviewed by:
Sevser Sahpaz, Lille 2 University, FranceCopyright © 2017 Gao, Chen, He, Liu, Xiong, Li and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jie Wang, d2FuZ2ppZTAxMDNAMTI2LmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.