
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr., 12 February 2025
Sec. Neonatology
Volume 13 - 2025 | https://doi.org/10.3389/fped.2025.1498425
This article is part of the Research TopicThe Effects of Emerging and Commonly Used Medications on the Developing BrainView all 5 articles
 Henry Chen1,2,†,‡
Henry Chen1,2,†,‡ Adam L. Numis1,2,†,‡Renée A. Shellhaas3,‡John R. Mytinger4,‡
Adam L. Numis1,2,†,‡Renée A. Shellhaas3,‡John R. Mytinger4,‡ Debopam Samanta5,‡Rani K. Singh6,7,‡
Debopam Samanta5,‡Rani K. Singh6,7,‡ Shaun A. Hussain8,‡Danielle Takacs9,‡Kelly G. Knupp10,‡
Shaun A. Hussain8,‡Danielle Takacs9,‡Kelly G. Knupp10,‡ Li-Rong Shao11,‡
Li-Rong Shao11,‡ Carl E. Stafstrom11*‡
Carl E. Stafstrom11*‡
Background: Infantile Epileptic Spasms Syndrome (IESS) is the most common epilepsy syndrome in children with trisomy 21. First-line standard treatments for IESS include adrenocorticotropic hormone (ACTH), oral corticosteroids, and vigabatrin. Among children with trisomy 21 and IESS, treatment with ACTH or oral corticosteroids may yield higher response rates compared with vigabatrin. However, supporting data are largely from single-center, retrospective cohort studies.
Methods: Leveraging the multi-center, prospective National Infantile Spasms Consortium (NISC) database, we evaluated the efficacy of first-line (standard) treatments for IESS in children with trisomy 21. We assessed clinical spasms remission at two weeks, clinical spasms remission at three months, and improvement of EEG (resolution of hypsarrhythmia) three months after initiation of treatment.
Results: Thirty four of 644 (5.3%) children with IESS were diagnosed with trisomy 21. In all children with trisomy 21, epileptic spasms was their presenting seizure type. Twenty of 34 (59%) children were initially treated with ACTH, nine (26%) with oral corticosteroids, and five (15%) with vigabatrin. Baseline demographics did not vary among treatment groups. The overall clinical remission rate after two weeks of treatment was 53% including 13 of 20 (65%) receiving ACTH, three of nine (33%) receiving oral corticosteroids, and two of five (40%) receiving vigabatrin (p = 0.24). The continued clinical response rate at three months was 32% including 8 of 20 (40%) receiving ACTH, two of nine (22%) receiving oral corticosteroids, and one of five (20%) receiving vigabatrin. Thirty of the 34 (88%) children presented with hypsarrhythmia (88%). EEG improvement at three months was better for children treated with ACTH (74%) or oral corticosteroids (83%) than vigabatrin (20%; p = 0.048). Adjustment for time from epileptic spasms onset to treatment did not alter results.
Conclusions: In our cohort, epileptic spasms were the first presenting seizure type in all children with trisomy 21. Among first-line standard treatment options, ACTH may have superior efficacy for clinical and electrographic outcomes for IESS in children with trisomy 21.
• Epileptic spasms were the first recognized seizure type in all children with trisomy 21.
• Children with trisomy 21 who were treated with ACTH first had higher responder rates at 2 weeks and 3 months compared with oral corticosteroids and vigabatrin.
• Hypsarrhythmia resolution rate at 3 months was higher in children who received ACTH or oral corticosteroids than those who received vigabatrin.
Trisomy 21 (Down syndrome) is the most prevalent genetic disorder caused by a chromosomal abnormality and 5%–10% of affected children develop epilepsy (1, 2). Infantile Epileptic Spasms Syndrome (IESS) is the most common epilepsy syndrome in children with trisomy 21 with a lifetime prevalence estimate of 0.4%–12.8% (3–5). IESS typically presents as ictal flexor or extensor epileptic spasms with an electroencephalogram (EEG) that often exhibits the interictal pattern of hypsarrhythmia (6, 7). IESS can be associated with developmental stagnation or regression regardless of etiology (8). While children with trisomy 21 and IESS have been reported to respond favorably to treatment compared with spasms in the non-trisomy 21 population (3, 4, 9), epileptic spasms may exacerbate developmental deficits in children with Down syndrome. Therefore, early, effective treatment is critical to optimize neurodevelopmental outcomes (10, 11) and it is imperative to identify the most effective treatment strategy for this high-risk population (12).
Standard, first-line medications for the treatment of IESS include adrenocorticotrophic hormone (ACTH), oral corticosteroids (prednisone or prednisolone), and vigabatrin (13–18). Treatment choice and response rates can vary by etiology of IESS [i.e., children with IESS caused by tuberous sclerosis complex respond best to vigabatrin; (19, 20)]. However, the optimal choice of first-line therapy for IESS in children with trisomy 21 remains uncertain. Prior retrospective, single-center studies have reported trends toward higher response rates when treatment is initiated with hormonal therapies (ACTH or oral corticosteroids) compared with vigabatrin and nonstandard therapies (5, 21).
Here, we evaluate the efficacy of standard, first-line medications for the treatment of IESS in children with trisomy 21 using data from a multi-site, prospective database, the National Infantile Spasms Consortium (NISC). Using NISC, we examined early and sustained treatment responses by evaluating clinical remission of epileptic spasms (at 2 weeks and 3 months) and electrographic remission of hypsarrhythmia (at 3 months) (22). We hypothesized that treatment response trends in the trisomy 21 population would resemble the overall NISC population, with hormonal therapy being most efficacious for first-line treatment for children with IESS associated with trisomy 21.
We used a nested cohort design within the NISC dataset. NISC is a national 22-center prospective study developed by the Pediatric Epilepsy Research Consortium (PERC) to evaluate the efficacy of treatments in children with IESS from January 2012 to December 2018. Children presenting between the ages of two months and two years with new onset epileptic spasms were eligible for enrollment. Medication dosing recommendations for ACTH, oral corticosteroids, and vigabatrin were provided to all sites, but treatment decisions were made by the clinical team at each site. Detailed methods regarding data collection have been previously reported (22).
This study was approved by the Institutional Review Boards at all participating sites. Written informed consent was obtained from a parent or guardian of each enrolled child in accordance with site-specific institutional requirements. Data were collected through chart review entered in REDCap (REDCap Consortium; Nashville TN) (17, 22).
In this secondary analysis, we restricted the NISC cohort to children with a genetically confirmed diagnosis of trisomy 21. Baseline demographics were collected and the efficacy of first-line treatments for IESS was evaluated using clinical information collected 2 weeks and three months after treatment initiation. Given the low response rate to non-standard medications compared to standard medications (ACTH, corticosteroids, or vigabatrin) in the management of IESS, children who were initially treated with a non-standard first treatment were analyzed according to the first standard medication prescribed. Primary outcomes of IESS remission were measured at two time intervals: remission of clinical epileptic spasms at two weeks after initial standard treatment of IESS and continued remission of clinical epileptic spasms at three months after the initial standard treatment of IESS. Non-responders at three months included children with a lack of complete remission of spasms or relapse of clinical epileptic spasms.
We then evaluated the impact of treatment on hypsarrhythmia at three months (secondary outcome). In the NISC, hypsarrhythmia was defined as the presence of multifocal spikes, background disorganization, and background voltage >200 µV peak-to-peak in any epoch on a bipolar longitudinal montage, and was determined by the referring neurologist at each site (17). There was no consensus definition provided for modified hypsarrhythmia variants. With consideration of the low inter-rater reliability for hypsarrhythmia and modified hypsarrhythmia variants, we merged these two variables during analysis (23). An electroclinical response was defined as both resolved hypsarrhythmia on EEG and continued remission of spasms at three months.
To account for the potential impact of dosing variability on treatment response, we performed a sensitivity analysis on children receiving adequate doses of ACTH, oral corticosteroids, and vigabatrin. Within each treatment group, adequate dosing was defined as ACTH >140 U/m2, oral corticosteroids ≥40 mg/day, or vigabatrin ≥100 mg/kg/day (13, 24).
Between-group comparisons of continuous variables were accomplished with Student's t-tests, analysis of variance (ANOVA), or Kruskal–Wallis tests, as appropriate. Comparisons of categorical variables were carried out with chi-square tests. We evaluated the effect of lag-time from diagnosis of IESS to treatment initiation on 2-week and 3-month responder rates using a generalized linear model with log-link regression and robust standard errors. All analyses were conducted using Stata version® 17 (College Station, Texas, USA). Statistical significance was defined as p-value less than 0.05. Given the small sample size of this cohort, we highlight large effect sizes that are not statistically significant in our results.
In the NISC cohort, 34 of 644 (5.3%) children with IESS were diagnosed with trisomy 21, and this was the most common genetic diagnosis in the IESS cohort. Thirteen NISC sites provided at least one child included in the trisomy 21 cohort. Epileptic spasms were the presenting seizure type in all children with trisomy 21 (e.g., none had pre-existing epilepsy when they presented with their first epileptic spasm). There was no difference in the age of spasms onset among the children with trisomy 21 [6.88 months; interquartile range (IQR): 6.0, 7.8] vs. the overall NISC cohort (6.91 months; IQR: 6.8, 7.2) (p = 0.51).
Among the 34 children with trisomy 21 and IESS, twenty (59%) were initially treated with ACTH, nine (26%) with oral corticosteroids, and five (15%) with vigabatrin. One child had previously received zonisamide for 108 days for IESS and then due to inefficacy, was switched to ACTH. No other child received a non-standard medication as initial treatment of IESS.
We did not observe differences in demographics across treatment groups (Table 1). Due to limitations of our sample size, we were unable to adjust for demographic confounders. Thirty of 34 children (88%) had hypsarrhythmia on EEG and 14 children (56%) were diagnosed with developmental regression at the time of presentation. The median time from epileptic spasms onset to the administration of a standard IESS treatment was 27 days (IQR: 9, 64). Median lag-time from diagnosis of IESS to treatment initiation was longer in participants initially treated with ACTH (32 days) compared with patients treated with vigabatrin (16 days) or oral corticosteroids (21 days), though differences did not reach statistical significance (p = 0.47, Table 1).
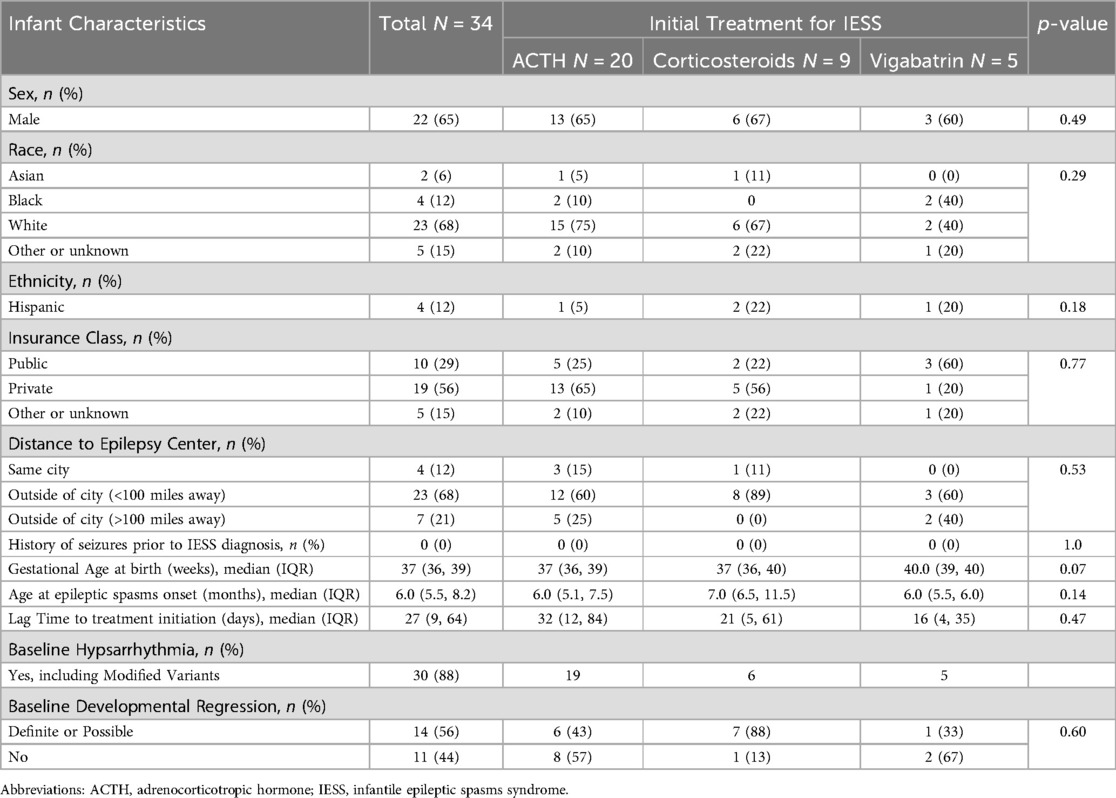
Table 1. Baseline characteristics of 34 children with trisomy 21 and infantile epileptic spasms syndrome.
On the participants for which brain magnetic resonance imaging (MRI) scans were obtained, findings were either normal or showed mild cortical, cerebellar, or brainstem hypoplasia, as previously shown for children with trisomy 21 (25). Vigabatrin-related gray matter diffusion restriction was not seen (26).
Side effects of ACTH, oral corticosteroids, and vigabatrin observed in our trisomy 21 patients were similar to those of the overall NISC cohort. Among those treated with ACTH or oral corticosteroids, weight gain, hypertension, and mild irritability were the most common adverse effects, and none were sufficiently severe to warrant medication discontinuation. Likewise, some children treated with vigabatrin showed mild irritability or sedation; there were no concerns about vision impairment during the brief follow up period.
Two weeks after initiation of a standard therapy, epileptic spasms resolved in 18 of 34 (53%) children. Responders at two weeks included 13 of 20 (65%) receiving ACTH, three of nine (33%) receiving oral corticosteroids, and two of five (40%) receiving vigabatrin (p = 0.24; Figure 1A, Table 2A). In children who responded to treatment at two weeks, relapse occurred in two of thirteen (15%) children who initially responded to ACTH, one of three children (33%) who initially responded to corticosteroids, and one of two children (50%) who initially responded to vigabatrin.
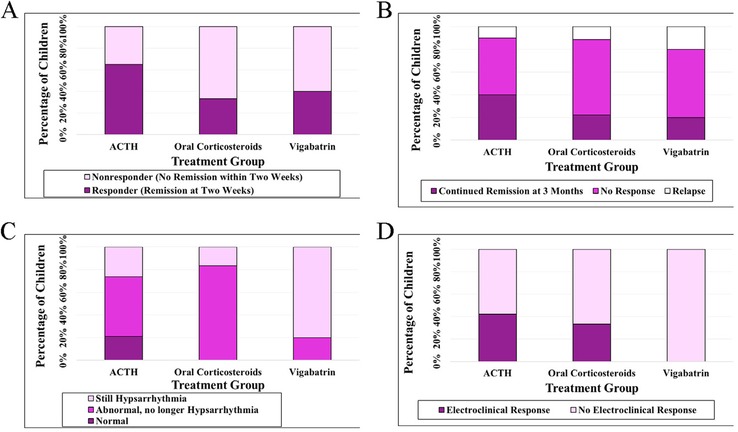
Figure 1. Treatment response at 2 weeks (A) and 3 months (B) for infantile epileptic spasms syndrome in children with trisomy 21, association with EEG improvement (C), and association with combined EEG improvement and clinical response at 3 months (D).

Table 2A. Clinical responses at 2 weeks and 3 months.
Of children with clinical remission at 2 weeks, there was continued remission of epileptic spasms in 9 of 18 (50%) children at 3 months, including seven of 13 (54%) receiving ACTH, one of three receiving oral corticosteroids (33%), and one of two (50%) receiving vigabatrin (not significant) (Table 2A). Irrespective of 2-week remission, clinical remission of epileptic spasms at three months was reported in 11 of 34 children (32%). These clinical responders at three months included 8 of 20 (40%) receiving ACTH, two of nine (22%) receiving oral corticosteroids, and one of five (20%) receiving vigabatrin (p = 0.52; Figure 1B; Table 2A). A similar non-significant result was seen if the ACTH cohort and the corticosteroid cohort were combined and compared with vigabatrin (p = 0.47).
Among the 30 children that presented with hypsarrhythmia at the time of IESS diagnosis, EEG improvement at three months was seen in 14 of 19 (74%) children receiving ACTH, five of six (83%) receiving oral corticosteroids, and one of five (20%) receiving vigabatrin (p = 0.03 comparing ACTH and oral corticosteroids with vigabatrin; Figure 1C; Table 2B). The EEG of four children (13%) with hypsarrhythmia at diagnosis of IESS normalized at three months; all of these children were treated with ACTH.

Table 2B. EEG improvement at 3 months in subjects presenting with hypsarrhythmia at time of diagnosis: n = 30.
When accounting for both EEG improvement and clinical remission at 3 months, an electroclinical response was observed in 10 of the 30 (33%) children who initially presented with hypsarrhythmia. Clinical remission without EEG improvement was observed in one child receiving vigabatrin. Electroclinical response was observed in a similar percentage of children receiving ACTH or oral corticosteroids: eight of 19 (42%) receiving ACTH and two of six (33%) receiving oral corticosteroids. Electroclinical response was not observed in any of the five children receiving vigabatrin (p = 0.14 comparing ACTH and oral corticosteroids to vigabatrin; Figure 1D). Adjustment for lag-time from diagnosis of IESS to treatment initiation by treatment group did not alter two-week or three-month results.
In a sensitivity analysis, we restricted our analysis to children who received adequate treatment doses. Adequate doses of initial standard treatments were given in 16 of 20 (80%) children receiving ACTH, eight of nine (89%) children receiving corticosteroids, and four of five (80%) children receiving vigabatrin. Results from this sensitivity analysis did not alter our other findings (Figure 2).
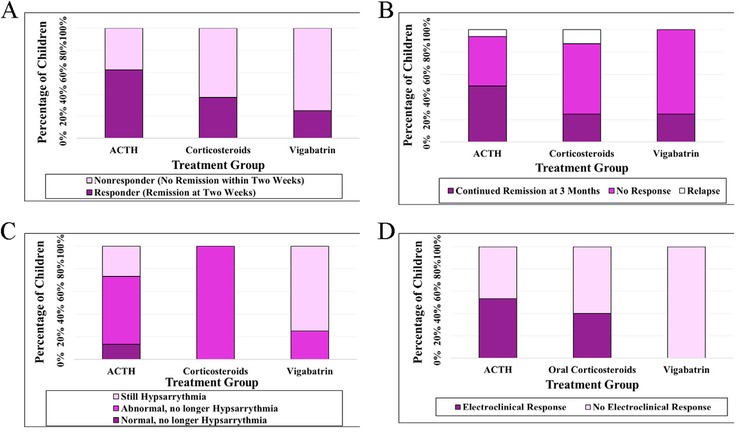
Figure 2. Treatment response at 2 weeks (A) and 3 months (B) for infantile epileptic spasms syndrome in children with trisomy 21 receiving adequate doses of first-line therapies, and association with EEG improvement (C), and association with combined EEG improvement and clinical response at 3 months (D).
In this multi-center prospective cohort study, we evaluated the outcomes of IESS treatments in children with trisomy 21. Our findings suggest that treatment with hormonal therapy (ACTH or oral corticosteroids) compared to vigabatrin result in an improved response at two weeks and three months after treatment initiation and improved resolution of hypsarrhythmia (at three months). The absence of electroclinical responders among children receiving vigabatrin may suggest that hormonal therapies are more effective than vigabatrin at improving clinical and electrographic outcomes, although the small sample size precludes precise estimates.
The 2-week and 3-month responder rates (53% and 32%) for children with trisomy 21 were similar to the overall NISC cohort responder rate (46%), and included both early and late responders. Likewise, the highest responder rates at two weeks were observed in children treated with ACTH, followed by oral corticosteroids and vigabatrin (22). Prior reports found ACTH and oral corticosteroids to have roughly similar effectiveness in IESS overall (17) and the lower response rates to oral steroids here was likely due to underpowering. Our findings on clinical and electrographic response to standard therapies corroborate the findings of several other groups that hormonal therapies are superior to vigabatrin for IESS among children with trisomy 21 (5, 21, 27–29).
Further support for that conclusion comes from a recent retrospective cohort study from Ireland of 54 children with IESS and trisomy 21, in which ACTH was underrepresented (only one of the 54 children was treated with ACTH) (26). A higher response rate was found among children treated with corticosteroids (60% had spasms cessation) relative to those treated with vigabatrin (28% had spasms cessation), though treatment with a combination of prednisolone and vigabatrin afforded an 83% spasms cessation rate. Despite some methodological differences between these studies, they reveal trends towards higher response rates to oral corticosteroids relative to vigabatrin, supporting the enlarging literature that hormonal therapy may be a more effective first-line therapy than vigabatrin for children with IESS in the setting of trisomy 21. Of note, a large retrospective review of treatments of infantile spasms across etiologies found a beneficial effect of vigabatrin or vigabatrin plus steroids (but only two of the 198 subjects had trisomy 21) (18). In the larger International Collaborative Infantile Spasms Study (ICISS) that included 37 children with infantile spasms and trisomy 21, those treated with prednisolone responded similarly to those treated with prednisolone plus vigabatrin, suggesting the lack of an additional benefit of vigabatrin (30).
Previous studies reported that diagnosis and treatment of IESS in children with trisomy 21 is often delayed compared to other children diagnosed with IESS (31). While the treatment lag-time (measured as the time from epileptic spasms onset to treatment initiation) in our cohort was shorter than that observed in previous studies in children with trisomy 21 and IESS, there remains a greater treatment lag-time relative to the general cohort in NISC [27 days (IQR: 9, 64) vs. 15 days (IQR: 6, 37)] (21, 31). Other studies have shown that shorter treatment lag-time may lead to improved IESS treatment efficacy (32, 33). Interestingly, in our study, children treated with ACTH had the longest lag times, yet maintained the highest responder rate across all standard therapies. Prompt diagnosis and efficient treatment initiation could provide opportunities for better outcomes (16).
Importantly, we observed that epileptic spasms were the presenting seizure type for all children with trisomy 21. That is, none of the children presented with focal seizures or other seizure types prior to infantile spasms, an observation that may be relevant to the mechanisms underlying predisposition to infantile spasms in children with trisomy 21 (34). In consideration of the challenges to prompt diagnosis and medical intervention for IESS in this population, our findings underscore the need for early epilepsy counseling of families of children with trisomy 21, at birth or soon thereafter (31, 35). IESS is a “never miss” diagnosis for pediatricians; our results emphasize the need for education of primary care providers about semiology of epileptic spasms and the urgency of diagnosis and treatment. Proactive counseling of families with infants at high risk for IESS (including children with trisomy 21) could include recommendations to record any suspicious events with a smartphone video and vigilant attention to any plateau or regression of developmental milestones (36, 37).
Historically, the low prevalence of children with both IESS and trisomy 21 has posed challenges to designing studies with adequate sample sizes and statistical power (5). In leveraging the multi-center prospective NISC cohort, we reduce the potential effect of site-specific treatment and selection bias inherent in single-center retrospective studies. Yet, despite enrolling from sites across the United States, NISC was still limited by a small sample size in this relatively rare disease combination. Collaboration between international consortia may be necessary to carry out multi-center prospective studies with larger sample sizes. Alternatively, use of a learning healthcare system model of research and quality improvement may offer an informative approach to case identification and research optimization for these children (38). Such efforts would provide further confidence in our results and strengthen understanding of the natural history of IESS in children with trisomy 21 and the relative efficacy of treatment options for this population.
We were also limited by our methodology for assessing electrographic changes on EEG. Neurologists at each NISC site classified EEGs as hypsarrhythmia or a modified variant of hypsarrhythmia. Since these data were collected, hypsarrhythmia assessments have been shown to demonstrate poor inter-rater reliability (39). To mitigate risks of EEG measurement validity, future studies could consider adopting the Burden of AmplitudeS and Epileptic Discharges (BASED) score, an EEG scoring system with demonstrated inter-rater validity or a centralized EEG review process to improve EEG assessment validity and accuracy (40, 41).
At this time, the optimal treatment choice for trisomy 21 children with IESS remains unclear. Our data support hormonal treatments but ACTH and corticosteroids are nonspecific with regard to mechanism and are also used as the first treatment choice for IESS of most other etiologies. MRI scan findings and potential side effects are not unique to the trisomy 21 population and MRI results did not alter the treatment approach in prior studies (25). Therefore, the choice of treatment can be informed by efficacy considerations.
In our cohort, epileptic spasms were the first presenting seizure type in all children with trisomy 21. Among first-line standard treatment options, hormonal therapies (and perhaps ACTH in particular) appear to have better efficacy than vigabatrin for clinical and electrographic outcomes of IESS in children with trisomy 21.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by University of California San Francisco Institutional Review Board, San Francisco, CA. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin.
HC: Data curation, Visualization, Writing – original draft, Conceptualization, Formal Analysis, Investigation, Methodology. AN: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Visualization, Writing – original draft, Project administration, Software, Supervision, Validation, Writing – review & editing. RS: Conceptualization, Formal Analysis, Investigation, Supervision, Writing – review & editing. JM: Conceptualization, Formal Analysis, Investigation, Supervision, Writing – review & editing, Data curation, Methodology. DS: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Writing – review & editing. RS: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Writing – review & editing. SH: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Writing – review & editing, Supervision. DT: Conceptualization, Formal Analysis, Investigation, Methodology, Writing – review & editing. KK: Conceptualization, Formal Analysis, Investigation, Methodology, Writing – review & editing, Data curation. LS: Formal Analysis, Methodology, Writing – review & editing, Visualization. CS: Visualization, Writing – review & editing, Data curation, Project administration, Supervision, Writing – original draft.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. Data were collected with research funds from Pediatric Epilepsy Research Foundation (PERF) and American Epilepsy Society (AES).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Stafstrom CE, Patxot OF, Gilmore HE, Wisniewski KE. Seizures in children with Down syndrome: etiology, characteristics and outcome. Dev Med Child Neurol. (1991) 33:191–200. doi: 10.1111/j.1469-8749.1991.tb05108.x
2. Silva ML, Cieuta C, Guerrini R, Plouin P, Livet MO, Dulac O. Early clinical and EEG features of infantile spasms in Down syndrome. Epilepsia. (1996) 37:977–82. doi: 10.1111/j.1528-1157.1996.tb00535.x
3. Stafstrom CE, Konkol RJ. Infantile spasms in children with Down syndrome. Dev Med Child Neurol. (1994) 36:576–85. doi: 10.1111/j.1469-8749.1994.tb11894.x
4. Arya R, Kabra M, Gulati S. Epilepsy in children with Down syndrome. Epileptic Disord. (2011) 13(1):1–7. doi: 10.1684/epd.2011.0415
5. Kats DJ, Roche KJ, Skotko BG. Epileptic spasms in individuals with Down syndrome: a review of the current literature. Epilepsia Open. (2020) 5(3):344–53. doi: 10.1002/epi4.12412
6. Shields WD. Infantile spasms: little seizures, BIG consequences. Epilepsy Curr. (2006) 6:63–9. doi: 10.1111/j.1535-7511.2006.00100.x
7. Zuberi SM, Wirrell E, Yozawitz E, Wilmshurst JM, Specchio N, Riney K, et al. ILAE classification and definition of epilepsy syndromes with onset in neonates and infants: position statement by the ILAE task force on nosology and definitions. Epilepsia. (2022) 63(6):1349–97. doi: 10.1111/epi.17239
8. Wirrell EC, Nabbout R, Scheffer IE, Alsaadi T, Bogacz A, French JA, et al. Methodology for classification and definition of epilepsy syndromes with list of syndromes: report of the ILAE task force on nosology and definitions. Epilepsia. (2022) 63(6):1333–48. doi: 10.1111/epi.17237
9. Beatty CW, Wrede JE, Blume HK. Diagnosis, treatment, and outcomes of infantile spasms in the trisomy 21 population. Seizure. (2017) 45:184–8. doi: 10.1016/j.seizure.2016.12.016
10. Barca D, Tarta-Arsene O, Dica A, Iliescu C, Budisteanu M, Motoescu C, et al. Intellectual disability and epielpsy in Down syndrome. Maedica. (2014) 9(4):344–50.25705303
11. Santoro JD, Pagarkar D, Chu DT, Rosso M, Paulsen KC, Levitt P, et al. Neurologic complications of Down syndrome: a systematic review. J Neurol. (2021) 268(12):4495–509. doi: 10.1007/s00415-020-10179-w
12. Tapp S, Anderson T, Visootsak J. Neurodevelopmental outcomes in children with Down syndrome and infantile spasms. J Pediatr Neurol. (2015) 13(2):74–7. doi: 10.1055/s-0035-1556768
13. Lux AL, Edwards SW, Hancock E, Johnson AL, Kennedy CR, Newton RW, et al. The United Kingdom infantile spasms study comparing vigabatrin with prednisolone or tetracosactide at 14 days: a multicentre, randomised controlled trial. Lancet. (2004) 364:1773–8. doi: 10.1016/S0140-6736(04)17400-X
14. Go CY, Mackay MT, Weiss SK, Stephens D, Adams-Webber T, Ashwal S, et al. Evidence-based guideline update: medical treatment of infantile spasms. Report of the guideline development subcommittee of the American Academy of Neurology and the practice committee of the Child Neurology Society. Neurology. (2012) 78(24):1974–80. doi: 10.1212/WNL.0b013e318259e2cf
15. Patel AD, Berg AT, Billinghurst L, Fain D, Fecske E, Feyma T, et al. Quality improvement in neurology: child neurology quality measure set: executive summary. Neurology. (2018) 90(2):67–73. doi: 10.1212/WNL.0000000000004806
16. O'Callaghan FJK, Edwards SW, Alber FD, Cortina Borja M, Hancock E, Johnson AL, et al. Vigabatrin with hormonal treatment versus hormonal treatment alone (ICISS) for infantile spasms: 18-month outcomes of an open-label, randomised controlled trial. Lancet Child Adolesc Health. (2018) 2(10):715–25. doi: 10.1016/S2352-4642(18)30244-X
17. Grinspan ZM, Knupp KG, Patel AD, Yozawitz EG, Wusthoff CJ, Wirrell EC, et al. Comparative effectiveness of initial treatment for infantile spasms in a contemporary US cohort. Neurology. (2021) 97(12):e1217–28. doi: 10.1212/WNL.0000000000012511
18. Kuchenbuch M, LoBarco T, Chemaly N, Chiron C, Nabbout R. Fifteen years of real-world data on the use of vigabatrin in individuals with infantile epileptic spasms syndrome. Epilepsia. (2024) 65(2):430–44. doi: 10.1111/epi.17808
19. Kotulska K, Kwiatkowski DJ, Curatolo P, Weschke B, Riney K, Jansen F, et al. Prevention of epilepsy in infants with tuberous sclerosis complex in the EPISTOP trial. Ann Neurol. (2021) 89(2):304–14. doi: 10.1002/ana.25956
20. Ramantani G, Bölsterli BK, Alber M, Klepper J, Korinthenberg R, Kurlemann G, et al. Treatment of infantile spasm syndrome: update from the interdisciplinary guideline committee coordinated by the German-speaking Society of Neuropediatrics. Neuropediatrics. (2022) 53(6):389–401. doi: 10.1055/a-1909-2977
21. Daniels D, Knupp K, Benke T, Wolter-Warmerdam K, Moran M, Hickey F. Infantile spasms in children with Down syndrome: identification and treatment response. Glob Pediatr Health. (2019) 6:2333794X18821939. doi: 10.1177/2333794X18821939
22. Knupp KG, Coryell J, Nickels KC, Ryan N, Leister E, Loddenkemper T, et al. Response to treatment in a prospective National Infantile Spasms Cohort. Ann Neurol. (2016) 79(3):475–84. doi: 10.1002/ana.24594
23. Demarest ST, Shellhaas RA, Gaillard WD, Keator C, Nickels KC, Hussain SA, et al. The impact of hypsarrhythmia on infantile spasms treatment response: observational cohort study from the National Infantile Spasms Consortium. Epilepsia. (2017) 58(12):2098–103. doi: 10.1111/epi.13937
24. O'Callaghan FJ, Edwards SW, Alber FD, Hancock E, Johnson AL, Kennedy CR, et al. Safety and effectiveness of hormonal treatment versus hormonal treatment with vigabatrin for infantile spasms (ICISS): a randomised, multicentre, open-label trial. Lancet Neurol. (2017) 16(1):33–42. doi: 10.1016/S1474-4422(16)30294-0
25. Trowbridge SK, Yuskaitis CJ, Baumer N, Libenson M, Prabhu SP, Harini C. Brain MRI abnormalities in patients with infantile spasms and Down syndrome. Epilepsy Behav. (2019) 92:57–60. doi: 10.1016/j.yebeh.2018.12.013
26. Harvey S, Allen NM, King MD, Lynch B, Lynch SA, O'Regan M, et al. Response to treatment and outcomes of infantile spasms in Down syndrome. Dev Med Child Neurol. (2022) 64(6):780–8. doi: 10.1111/dmcn.15153
27. Lujić L, Bosnjak VM, Delin S, Duranović V, Krakar G. Infantile spasms in children with Down syndrome. Coll Antropol. (2011) 35(Suppl 1):213–8.
28. Datta AN, Crawford J, Wong PKH. Infantile spasms and trisomy 21: unfavorable outcomes with first-line vigabatrin therapy. Can J Neurol Sci. (2021) 48(6):839–44. doi: 10.1017/cjn.2021.12s33472713
29. Glineur M, Toulas J, Vuillemin-Massie L, Camus M, Montagutelli S, Prioux E, et al. Infantile epileptic spasm syndrome and trisomy 21: treatment response and outcomes. Proc 5th Internat Conf Trisomy 21 Res Soc; June 5–8, 2024; Rome, Italy (2024).
30. Osborne JP, Edwards SW, Alber FD, Hancock E, Johnson AL, Kennedy CR, et al. The underlying etiology of infantile spasms (west syndrome): information from the International Collaborative Infantile Spasms Study (ICISS). Epilepsia. (2019) 60(9):1861–9. doi: 10.1111/epi.16305
31. Sanmaneechai O, Sogawa V, Silver W, Ballaban-Gil K, Moshé SL, Shinnar S. Treatment outcomes of West syndrome in infants with Down syndrome. Pediatr Neurol. (2013) 48(1):42–7. doi: 10.1016/j.pediatrneurol.2012.09.006
32. O'Callaghan FJ, Lux AL, Darke K, Edwards SW, Hancock E, Johnson AL, et al. The effect of lead time to treatment and of age of onset on developmental outcome at 4 years in infantile spasms: evidence from the United Kingdom Infantile Spasms Study. Epilepsia. (2011) 52(7):1359–64. doi: 10.1111/j.1528-1167.2011.03127.x
33. Nelson GR. Management of infantile spasms. Transl Pediatr. (2015) 4(4):260–70. doi: 10.3978/j.issn.2224-4336.2015.09.01
34. Janicot R, Shao LR, Stafstrom CE. Infantile spasms: an update on pre-clinical models and EEG mechanisms. Children (Basel). (2020) 7(1):5. doi: 10.3390/children7010005
35. Buterbaugh A, Visootsak J. Implications of delayed diagnosis of infantile spasm in a child with Down syndrome. J Pediatr Neurol. (2014) 12(2):105–7.25309120
36. Rao CK, Nordli DR III, Cousin JJ, Takacs DS, Sheth RD. The effect of smartphone video on lead time to diagnosis of infantile spasms. J Pediatr. (2023) 258:113387. doi: 10.1016/j.jpeds.2023.02.035
37. Wusthoff CJ, Shellhaas RA. Can a smartphone jump start care for infantile spasms? J Pediatr. (2023) 258:113442. doi: 10.1016/j.jpeds.2023.113442
38. Grinspan ZM, Patel AD, Shellhaas RA, Berg AT, Axeen ET, Clarke JBDF, et al. Design and implementation of electronic health record common data elements for pediatric epilepsy: foundations for a learning health care system. Epilepsia. (2021) 62(1):198–216. doi: 10.1111/epi.16733
39. Hussain SA, Kwong G, Millichap JJ, Mytinger JR, Ryan N, Matsumoto JH, et al. Hypsarrhythmia assessment exhibits poor interrater reliability: a threat to clinical trial validity. Epilepsia. (2015) 56(1):77–81. doi: 10.1111/epi.12861
40. Mytinger JR, Vidaurre J, Moore-Clingenpeel M, Stanek JR, Albert DVF. A reliable interictal EEG grading scale for children with infantile spasms—the 2021 BASED score. Epilepsy Res. (2021) 173:106631. doi: 10.1016/j.eplepsyres.2021.106631
Keywords: infantile spasms, infantile epileptic spasms syndrome, Down syndrome, trisomy 21, anti-seizure medications, hypsarrhythmia
Citation: Chen H, Numis AL, Shellhaas RA, Mytinger JR, Samanta D, Singh RK, Hussain SA, Takacs D, Knupp KG, Shao L-R and Stafstrom CE (2025) Treatment efficacy for infantile epileptic spasms syndrome in children with trisomy 21. Front. Pediatr. 13:1498425. doi: 10.3389/fped.2025.1498425
Received: 18 September 2024; Accepted: 23 January 2025;
Published: 12 February 2025.
Edited by:
Jennifer Burnsed, University of Virginia, United StatesReviewed by:
Gouri Rao Passi, Choithram Hospital and Research Centre, IndiaCopyright: © 2025 Chen, Numis, Shellhaas, Mytinger, Samanta, Singh, Hussain, Takacs, Knupp, Shao and Stafstrom. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Carl E. Stafstrom, Y3N0YWZzdDFAamhtaS5lZHU=
†These authors share first authorship
‡ORCID:
Henry Chen
orcid.org/0000-0001-7795-9541
Adam L. Numis
orcid.org/0000-0002-1594-9812
Renée A. Shellhaas
orcid.org/0000-0002-3175-3908
John R. Mytinger
orcid.org/0000-0001-7901-3960
Debopam Samanta
orcid.org/0000-0002-5154-8717
Rani K. Singh
orcid.org/0000-0001-9343-6070
Shaun A. Hussain
orcid.org/0000-0001-6947-8852
Danielle Takacs
orcid.org/0000-0001-6138-7200
Kelly G. Knupp
orcid.org/0000-0002-1967-0827
Li-Rong Shao
orcid.org/0000-0002-0624-7122
Carl E. Stafstrom
orcid.org/0000-0002-4432-2453
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.