 Carla Rognoni1*
Carla Rognoni1* Maria Rosa Barcellona2Irene Bargellini3Maria Grazia Bavetta2Marilena Bellò4
Maria Rosa Barcellona2Irene Bargellini3Maria Grazia Bavetta2Marilena Bellò4 Maurizia Brunetto3Patrizia Carucci4Roberto Cioni3Laura Crocetti3Fabio D’Amato2
Maurizia Brunetto3Patrizia Carucci4Roberto Cioni3Laura Crocetti3Fabio D’Amato2 Mario D’Amico2Simona Deagostini4
Mario D’Amico2Simona Deagostini4 Désirée Deandreis4Paolo De Simone3Andrea Doriguzzi4Monica Finessi4
Désirée Deandreis4Paolo De Simone3Andrea Doriguzzi4Monica Finessi4 Paolo Fonio4
Paolo Fonio4 Serena Grimaldi4Salvatore Ialuna2Fabio Lagattuta2Gianluca Masi3Antonio Moreci2Daniele Scalisi2Roberto Virdone2
Serena Grimaldi4Salvatore Ialuna2Fabio Lagattuta2Gianluca Masi3Antonio Moreci2Daniele Scalisi2Roberto Virdone2 Rosanna Tarricone1,5
Rosanna Tarricone1,5- 1Centre for Research on Health and Social Care Management (CERGAS), SDA Bocconi School of Management, Bocconi University, Milan, Italy
- 2Azienda Ospedaliera Ospedali Riuniti Villa Sofia Cervello, Palermo, Italy
- 3Azienda Ospedaliero Universitaria Pisana, Pisa, Italy
- 4Azienda Ospedaliero Universitaria Città della Salute e della Scienza, Torino, Italy
- 5Department of Policy Analysis and Public Management, Bocconi University, Milan, Italy
Aims: To perform a cost-effectiveness analysis (CEA) comparing personalised dosimetry with standard dosimetry in the context of selective internal radiation therapy (SIRT) with TheraSphere for the management of adult patients with locally advanced hepatocellular carcinoma (HCC) from the Italian Healthcare Service perspective.
Materials and methods: A partition survival model was developed to project costs and the quality-adjusted life years (QALYs) over a lifetime horizon. Clinical inputs were retrieved from a published randomised controlled trial. Health resource utilisation inputs were extracted from the questionnaires administered to clinicians in three oncology centres in Italy, respectively. Cost parameters were based on Italian official tariffs.
Results: Over a lifetime horizon, the model estimated the average QALYs of 1.292 and 0.578, respectively, for patients undergoing personalised and standard dosimetry approaches. The estimated mean costs per patient were €23,487 and €19,877, respectively. The incremental cost-utility ratio (ICUR) of personalised versus standard dosimetry approaches was €5,056/QALY.
Conclusions: Personalised dosimetry may be considered a cost-effective option compared to standard dosimetry for patients undergoing SIRT for HCC in Italy. These findings provide evidence for clinicians and payers on the value of personalised dosimetry as a treatment option for patients with HCC.
Introduction
Globally, there are about 840,000 new cases of liver cancer each year (1). Primary liver cancer is the second leading cause of cancer death worldwide (2). Seventy-five percent of liver cancers are hepatocellular carcinoma (HCC) resulting from cirrhosis. Patients are typically diagnosed late in the disease, with a relatively small percentage eligible for curative treatments. Despite the addition of several new therapies for advanced HCC, the 5-year survival rate is 18% (3). Interventional techniques, like radiation-based approaches, are of interest because they are known to be cytocidal in adequate doses and are independent of other chemical or energy-based treatment techniques. While a delivery of more than 70 Gray (Gy) is considered necessary to achieve necrosis of a solid tumour (4), the tolerance of healthy liver tissue is about 30 Gy (5). These conditions were the basis of the development of liver-directed selective internal radiation therapy (SIRT) or brachytherapy, also referred to as transarterial radioembolisation (TARE) therapy. SIRT or TARE requires an infusion of radioactive microspheres, loaded with yttrium-90 (Y90) or, more recently, holmium-166 (Ho166).
In this context, TheraSphere is approved for the treatment of hepatic malignancies in Europe (CE mark indication). TheraSphere is made up of glass microspheres in which the Y90 radioactive isotope is imbedded. These microspheres are infused by an interventional radiologist and nuclear medicine physicians into the hepatic artery via a catheter and become lodged in capillaries within the tumour vasculature. With a penetration range of 2.5 mm, the emitted radiation destroys the cancer cells over a period of approximately 2 weeks. The aim of the treatment, with the standard dosimetric approach, is to deliver an absorbed dose of 120 ± 20 Gy to the treated hepatic volume.
Recent retrospective studies have shown that a personalised and optimised dosimetric approach, which takes into account the dose absorbed by the tumour, is technically possible and could lead to higher response rates (6, 7). The recently published DOSISPHERE-01 trial (8) is a randomised, multicentre, open-label phase 2 trial done at four healthcare centres in France with the aim to compare personalised to standard dosimetry. Dosimetry was evaluated by medical physicists and nuclear medicine physicians using a local software [volumetric analysis (Syngo Workstation, Siemens, Malvern, PA, USA) and PLANET Dose (DOSIsoft, Paris, France)]. The target in the personalised dosimetry approach was to deliver at least 205 Gy to the tumour, arriving at more than 250 Gy, if possible. The results of the study showed that, compared with standard dosimetry, personalised dosimetry significantly improved the overall survival and the objective response rate in patients with locally advanced hepatocellular carcinoma. Moreover, personalised dosimetry is likely to improve patient outcomes in clinical practice.
The aim of this study is to support stakeholders in the evaluation of the treatment choices in patients with HCC. Specifically, this study evaluated the cost-effectiveness of personalised dosimetry to standard dosimetry in the context of SIRT with TheraSphere from the National Healthcare Service (NHS) perspective in Italy.
Materials and methods
Medical devices have distinctive features compared to drugs, such as incremental innovation, dynamic pricing, a learning curve, and organisational impact (e.g., the need to create adequate operating rooms), that need consideration when evaluated (9). The study followed the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) reporting guideline (10), supplemented by the distinct features of medical devices (11). The checklist is highlighted in Appendix 1.
The model
A partition survival model with “stable disease,” “progression,” and “death” health states has been developed to estimate life years (LYs), quality-adjusted life years (QALYs), and the costs associated with personalised dosimetry and standard dosimetry in the context of SIRT with TheraSphere. The model considers the same population analysed by Garin and colleagues (8): adult population with a mean age of 64 years (91.5% men) with locally advanced hepatocellular carcinoma not amenable to surgery or local ablative treatment, BCLC (Barcelona Clinic Liver Cancer) B (intermediate stage) and C (advanced stage) (mainly C). This population reflects the indications of national (12) (Italy) and international guidelines (13, 14) for the management of hepatocellular carcinomas through SIRT.
All patients start in the “stable disease” health state. In cases of disease progression, patients move to the “progression” state. Once patients have progressed their disease, they cannot return to their previous health status. Once patients transition into the state of “death,” they remain in that state until the end of the process (Figure 1). The model considers a cycle length of 1 month and applies a “half-cycle” correction for costs and benefits. The partition survival model, which is now used in a significant proportion of appraisals (15, 16), may be seen as a relatively straightforward and intuitive approach because state occupancy can be estimated directly from trial-based estimates of survival. Indeed, patients’ distribution over time among the different health states has been derived from overall survival (OS) and progression-free survival (PFS) data available from the randomised controlled trial (RCT) DOSISPHERE-01 by Garin and colleagues (8). The model applies a time horizon of 45 years; given the median age of 64 years of the population considered, 45 years was considered long enough to cover the lifetime of every patient. In order to estimate clinical and economic outcomes over a lifetime horizon, clinical trial data were extrapolated through curve fittings. For standard dosimetry, for each clinical outcome (OS, PFS), the parameters were “fitted” with different functions, and the most plausible models were selected by statistical methods (see Appendix 2 for details). Specific hazard ratios (personalised dosimetry vs. standard dosimetry, HROS = 0.421, HRPFS = 0.71) reported in (8) were applied to both OS and PFS curves of standard dosimetry to obtain the curves for personalised treatment.
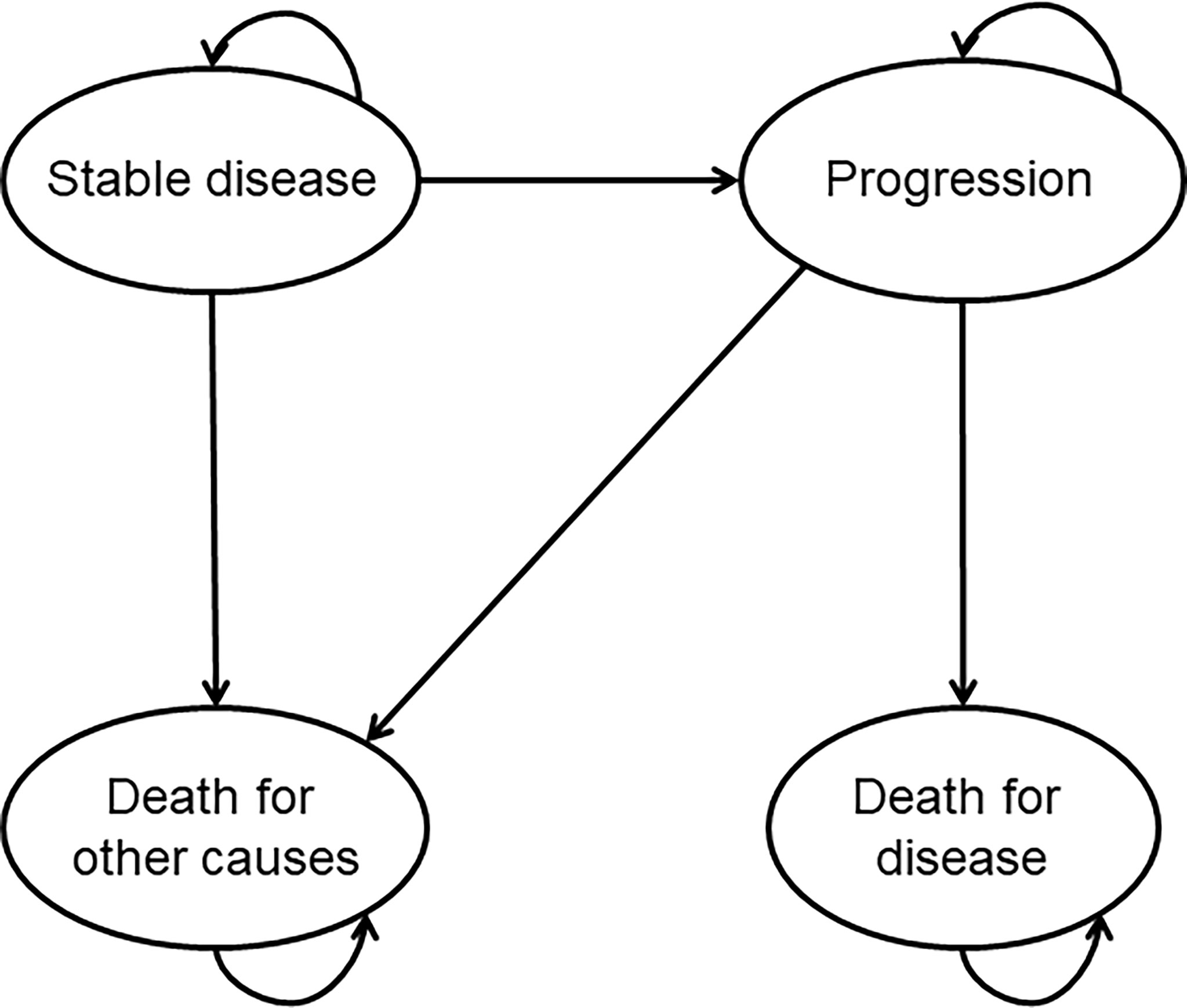
Figure 1 Representation of the implemented model.
Mortality rates were further adjusted for age and gender according to the Italian mortality tables (ISTAT) to consider deaths caused by other comorbidities (“Death for other causes” state). A discount rate of 3% was applied to health outcomes and costs (17).
Healthcare resource utilisation and costs
Table 1 reports the unit cost of the resources used for treatment with TheraSphere with personalised or standard dosimetry (€, 2021). The frequency of use was elicited through the administration of a questionnaire to clinicians from departments (oncology, interventional radiology, nuclear medicine, physics, and gastroenterology) in three clinical centres that are geographically distributed in Italy and perform a high volume of SIRT procedures annually (Azienda Ospedaliero Universitaria Pisana, Pisa; Azienda Ospedaliera Ospedali Riuniti Villa Sofia Cervello, Palermo; Azienda Ospedaliero Universitaria Città della Salute e della Scienza, Torino). Clinicians in each clinical centre completed the questionnaire in a collaborative way reporting data according to their clinical practice (12). The mean value for healthcare resource utilisation was calculated from the completed questionnaires. The model considers different healthcare services that are used in the peri-procedural period (in the first month, exams/visits performed before and after SIRT), together with other healthcare services used in the follow-up (stable disease or progression).
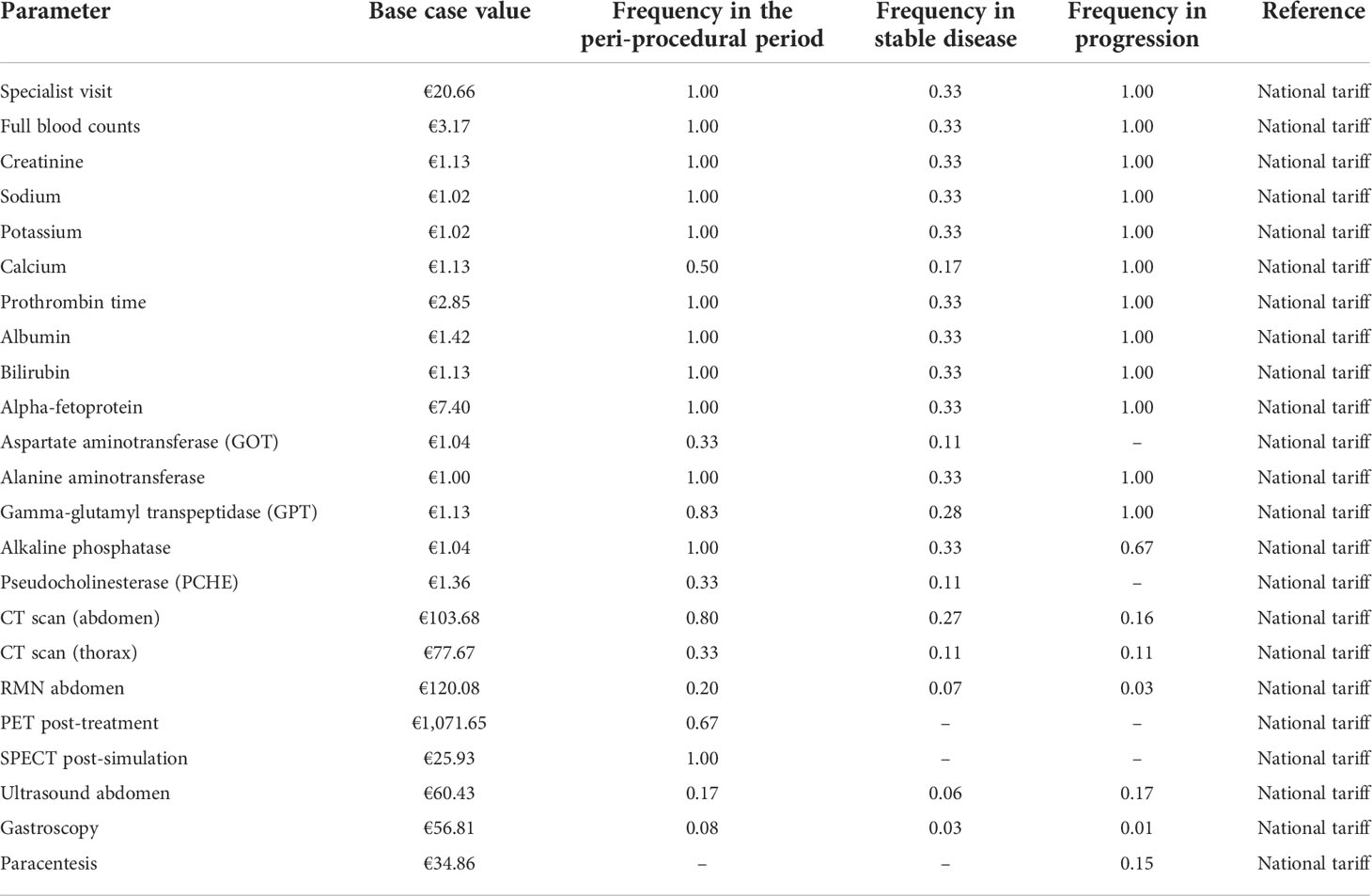
Table 1 Input parameters: healthcare resource utilisation and related unit costs.
Concerning SIRT treatment, a simulation and the treatment were considered for each patient. The simulation was used to evaluate the anatomy of the arterial supply to the liver, optimise the condition of the arteries to convey the treatment, and avoid side effects. The simulation referred to the diagnosis-related group (DRG) 203 (€4,085, national tariff), while the treatment referred to different reimbursement rates in the different Italian regions by their specific tariff and/or extra tariff DRGs (DRG 203 “Malignancy of hepatobiliary system or pancreas,” DRG 191 “Pancreas, liver & shunt procedures w cc,” DRG 192 “Pancreas, liver & shunt procedures w/o cc,” DRG 409 “Radiotherapy”). As such, reimbursement ranged between €1,279.77 and €22,364.35 (patients with comorbidities). In this analysis, we used the mean reimbursement rate from the four DRGs (national tariff), being the same reimbursement value considered for both strategies (SIRT with personalised or standard dosimetry). This meant that the choice of the tariff did not influence the results from the cost-effectiveness analysis (CEA). For personalised dosimetry, a cost of €150 for each SIRT procedure was applied for the software license. Based on the self-reported data collected from the questionnaires, the model accounting for 13% of the HCC cases required a coil embolisation to perform SIRT (DRG 203, national tariff €4,085).
Data collected from clinicians were used to detail the pharmacological treatments administered to patients following the procedure or in the progression phase. The former was mainly composed of antibiotic and anti-inflammatory therapy (3.5 g of ceftriaxone, 42% of patients; 875 cc of physiologic solution, 42% of patients; betamethasone 40 mg, 33% of patients; ursodeoxycholic acid 300 mg/day for 3 months, 33% of patients; potassium perchlorate 400 mg, 33% of patients) for a mean cost per patient of €11.20. The latter consisted of antibiotics (10 g of ceftriaxone, 24 g of piperacillin/tazobactam, 2% of patients), diuretics (75 mg of furosemide, 300 mg of potassium canrenoate, 2% of patients), and albumin (375 ml, 2% of patients) for a mean cost of €3.88 per patient.
Subsequent treatments were identified from the available literature (8) and incorporated into the model. They were liver resections (DRG 192, national tariff €9,558) performed in 36% and 4% of patients for personalised and standard dosimetry, respectively. It was assumed that subsequent treatments were performed after objective response evaluation (3 months after the SIRT) (8).
Current guidelines do not report recommendations about the specific case of progression management after SIRT treatment. In general, a systemic treatment may be performed in patients with advanced stage of disease (13, 14). Recently, lenvatinib showed non-inferiority efficacy compared with sorafenib, which was the established standard systemic therapy for HCC according to all international guidelines following the results reported a decade ago (18). We therefore conducted a scenario analysis by considering the cost of treatment with lenvatinib for patients progressing after SIRT. According to the data presented in (18), we considered a mean dose per day of 9.47 mg and a median duration of treatment of 5.7 months. Regarding the cost of lenvatinib, we referred to published Italian official tariffs (cost of €14.10 per mg) (19).
For terminal care, the model considered the cost of best supportive care reported in the literature for the Italian setting (€4,142—year 2012 corresponding to €4,374—year 2021) (20).
Quality-of-life estimates
Utility coefficients (0.51 for stable disease and 0.35 for progression) related to the health states were obtained from a published study (21), which estimated them from an analysis of studies in the Cost-Effectiveness Analysis Registry (22). Since the utility values of health states are not specific to the dosimetric approach used, we applied disutilities related to adverse events to capture the difference in the quality of life (QOL) between the two treatment options. Disutilities were retrieved from the cited registry. Since more than one study reported disutilities data, a mean value was estimated which took into account the highest quality degree [studies were classified on a quality scale from 1 (low) to 7 (high)]. For the duration of the adverse events, the threshold values in days for the different DRGs were considered (according to Italian Ministerial Decree 18/12/2008). Table 2 shows a summary of data related to the modelling of adverse events.
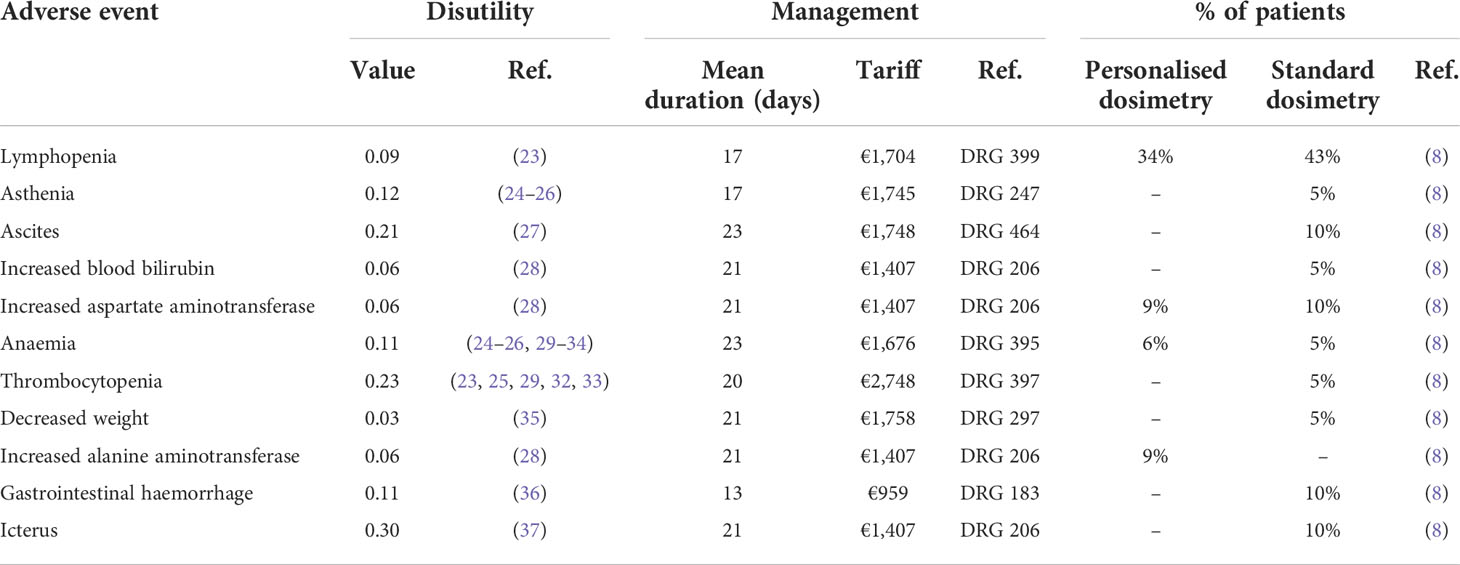
Table 2 Disutilities, frequencies, durations, and costs of adverse events used in the model.
Cost-effectiveness analysis
The incremental cost-effectiveness ratio (ICER) was calculated as the difference in the mean expected costs (i.e., incremental cost, ΔC) between personalised and standard dosimetry divided by the difference in the mean expected outcomes (i.e., incremental life years, ΔE) between these strategies (ICER = ΔC/ΔE). We referred to the incremental cost-utility ratio (ICUR) when effectiveness is expressed in QALYs.
As the long-term curve extrapolations may influence the results of the analyses, shorter horizons of 5 and 10 years have been also considered.
Deterministic and probabilistic sensitivity analyses (PSA) were performed to test the robustness of the model. The PSA was performed by assigning distributions to model parameters (beta for utilities, log-normal for hazard ratios, gamma for costs, and frequencies of events). In case the studies referencing the parameters reported 95% confidence intervals, these were applied to estimate parameter variations; otherwise, a standard deviation of 20% of the baseline value was used. For the PSA, 1,000 Monte Carlo simulations were performed by randomly sampling all the parameters from their assigned distributions. Results have been presented graphically as scatterplots in the cost-effectiveness plane. Results of the univariate analysis are reported as a tornado diagram for the ICUR. Supplementary Table 1 shows the details regarding the parameters used in the analyses.
Results
Cost-effectiveness analysis
Considering a lifetime horizon, the model estimated the average QALYs of 1.292 and 0.578, respectively, for patients undergoing personalised and standard dosimetry approaches. The estimated mean costs per patient were €23,487 and €19,877 for personalised and standard options, respectively. The model results for the two scenarios are summarised in Table 3. The ICUR of personalised versus standard dosimetry approaches was €5,056/QALY, highlighting the cost-effectiveness of the tailored procedure (ICUR < €50,000). The cost-effectiveness of personalised versus standard dosimetry was confirmed also considering the shorter time horizons of 5 and 10 years for the analyses (Table 3).
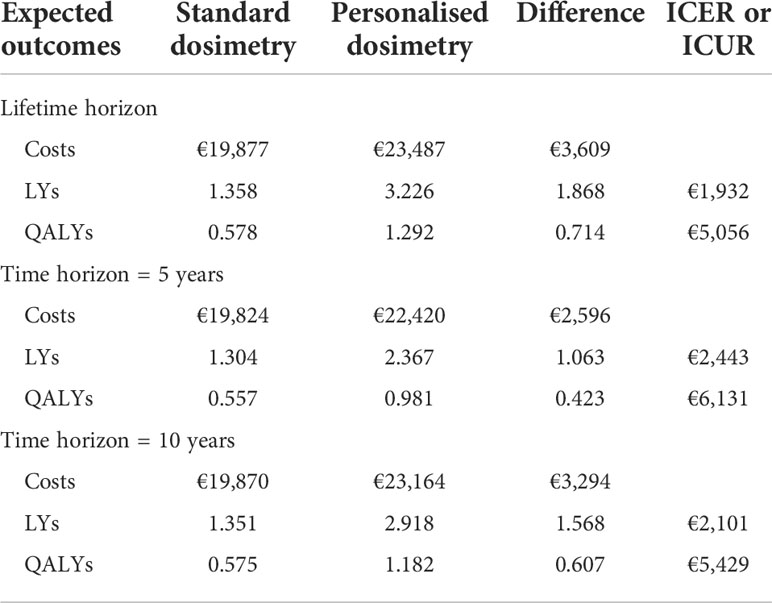
Table 3 Model results according to different time horizons.
Table 4 shows the detailed costs for each treatment strategy and by health states considered in the model. Personalised treatment, compared to standard dosimetry, led to lower costs for the management of adverse events and higher costs for second-line treatments like liver resections. The difference in subsequent treatment cost was due to the higher effectiveness of personalised dosimetry in improving patients’ outcomes, allowing patients to undergo curative liver resection. Terminal care costs are lower for the personalised dosimetry approach due to the lower number of patients dying from the disease.
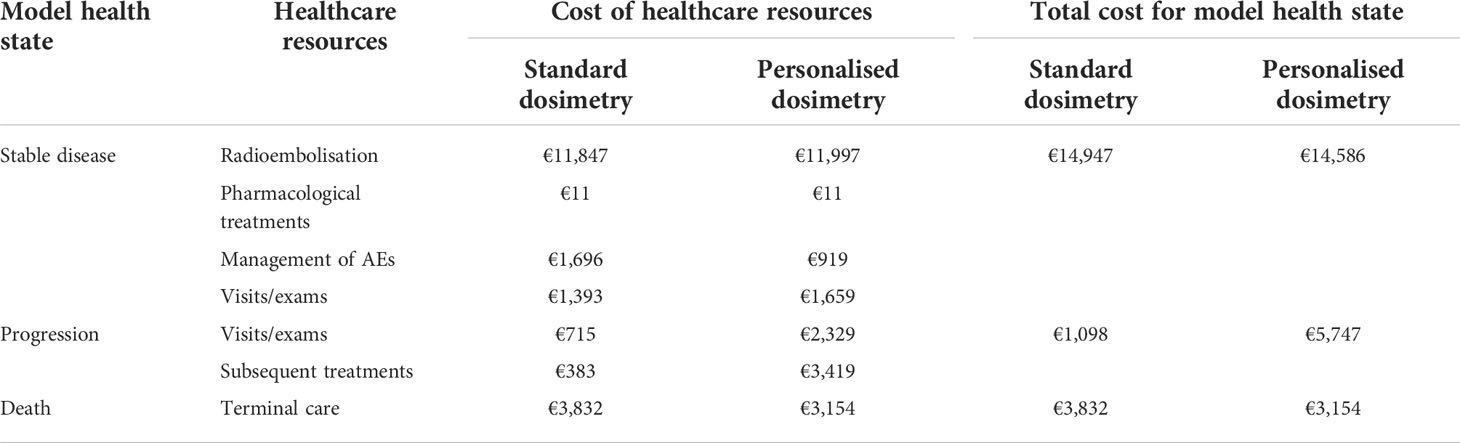
Table 4 Cost details.
The scenario analysis considering the cost of systemic chemotherapy for progressive patients led to mean costs per patient of €44,078 and €41,292 for personalised and standard dosimetry, respectively, showing a lower ICUR (€3,903/QALY) compared to the base case analysis.
Tornado diagrams reporting a one-way sensitivity analysis for the ICUR are reported in Figure 2. The most impactful parameters reporting greater variations on the ICUR were the hazard ratios for OS and PFS, the utility value for progression, and the cost for liver resection as subsequent treatment.
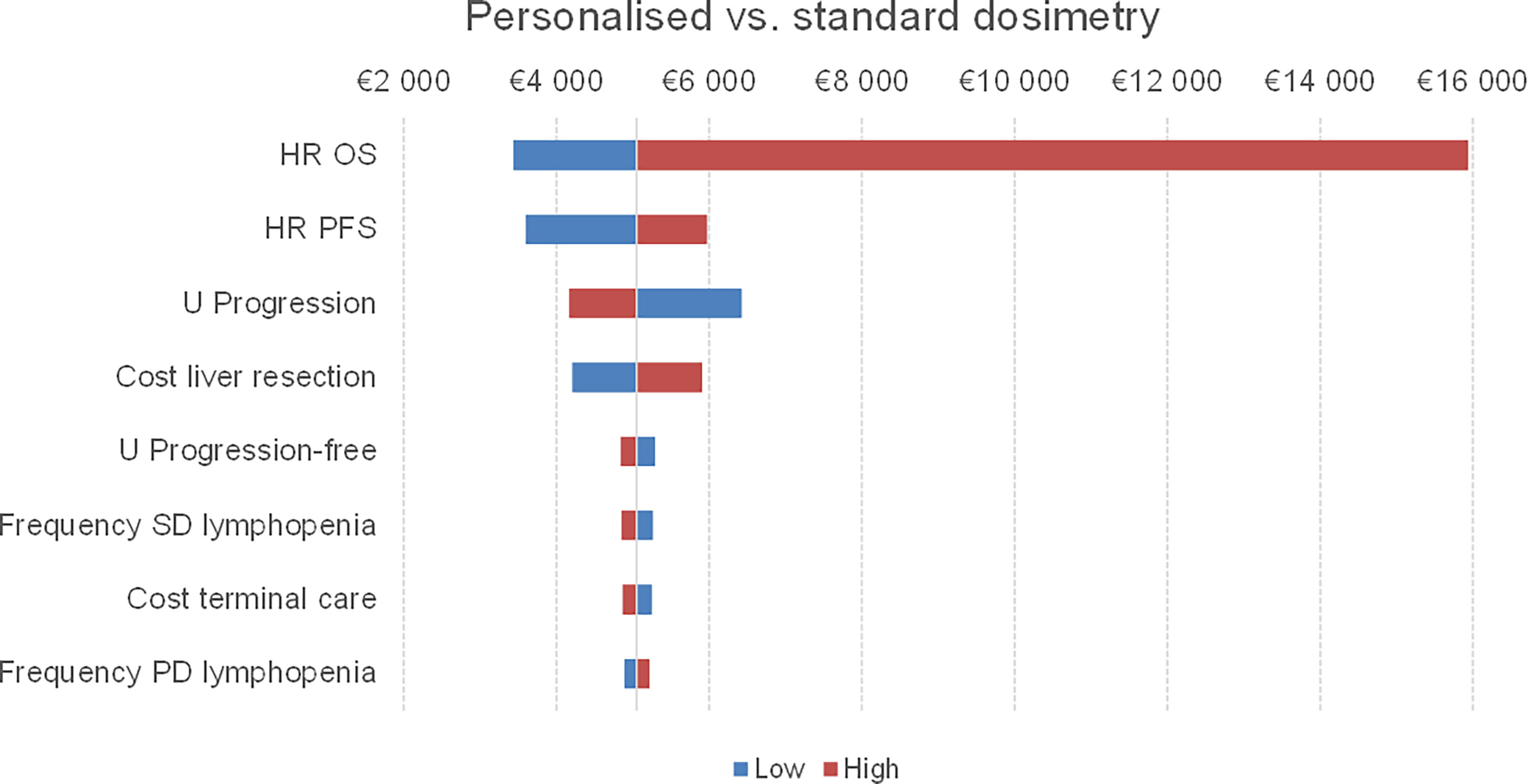
Figure 2 Tornado diagram of one-way sensitivity analysis of personalised and standard dosimetry for the ICUR. The vertical line represents the incremental value between the two strategies using the base case value for each parameter. As the parameters deviate from their base case values, the ICUR changes. The red bar represents the variation of the ICUR when the parameter ranges from the base case to the high uncertainty value. Conversely, the blue bar shows the ICUR variation when the parameter ranges from the low uncertainty value to the base case value. SD, standard dosimetry; PD, personalised dosimetry.
Concerning the PSA, the plot of incremental costs versus incremental QALYs obtained from the Monte Carlo simulations is shown in Figure 3A. The dotted line represents a theoretical cost-effectiveness willingness-to-pay threshold of €50,000/QALY. Nearly all the simulations (96.7%) were below this line. Figure 3B reports the acceptability curve.
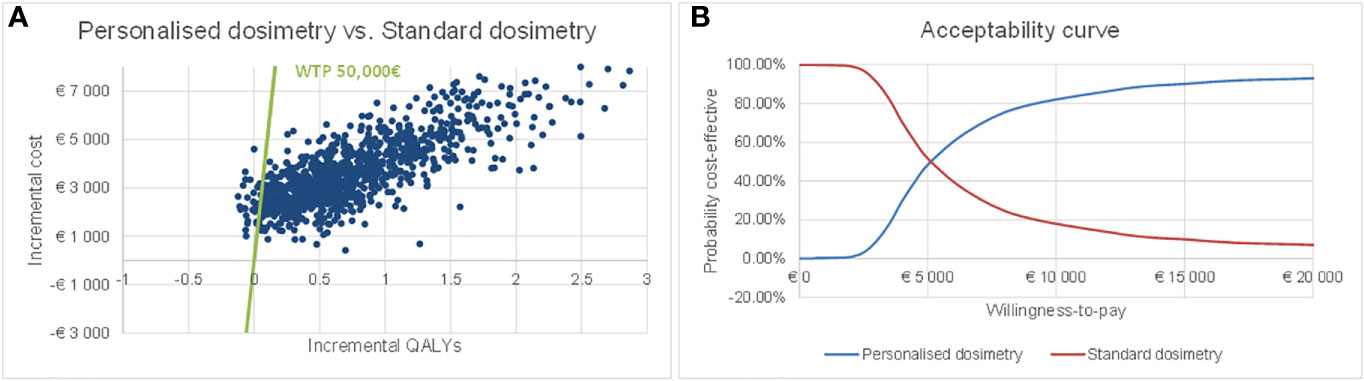
Figure 3 Probabilistic sensitivity analysis results: scatterplot in the cost-effectiveness plane (A) and acceptability curve (B).
Discussion
The first approach to medicine was “disease-based,” meaning that patients were treated only after disease manifestation. In this case, the diagnosis was mainly based on the signs and symptoms, and treatment was prescribed according to the experience of the physician. The current approach is described as “evidence-based” because the diagnostic–therapeutic pathway is conducted according to the outcome of clinical studies and clinical practice guidelines, developed based on clinical research. With this approach, it is possible to know the mechanisms of diseases and to implement the most appropriate therapy. The newer “personalised” approach tailors medical treatment to the individual characteristics of each patient (e.g., lifestyle parameters, genome, microbiome). As such, the ability to predict which medical treatments will be safe and effective for each patient is improved and the costs are contained (38). In this context, personalised dosimetry for SIRT with TheraSphere in patients with HCC improved the treatment workflow leading to better patient outcomes (8). SIRT with personalised dosimetry allowed for the improvement of patient outcomes enough to consent to curative resection surgery of the liver (liver resection was possible in 36% of the patients that previously had SIRT with personalised dosimetry compared to 4% of the patients who underwent SIRT with standard dosimetry). Moreover, the best clinical outcome of personalised dosimetry (i.e., improved overall survival) is obtained with a limited increase in costs (€150) for the procedure preparation. Regarding this aspect, dosimetry could also be performed without any commercial software but through the imaging workstation with the use of a datasheet, and this setting would allow to remove also this low additional fee (39).
Several studies comparing treatments for HCC exist, but to our knowledge, this study is the first to evaluate the cost-effectiveness of different types of dosimetry modalities. Although in Italy there is no official threshold to be considered in cost-effectiveness studies, the Italian Association of Health Economics suggests a threshold between €25,000 and €40,000 per QALY (40), while a published study (41) defined a cost-effective treatment whose maximum value per month of life gained is less than €5,000 (i.e., €60,000 per year gained). Considering an intermediate willingness-to-pay threshold of €50,000, this study showed that TheraSphere (SIRT) with personalised dosimetry for the treatment of patients with HCC may be a cost-effective option in comparison to the standard dosimetry approach. The clinical effectiveness of personalised and standard dosimetry was derived from a recently published RCT. The results from the RCT were robust and evaluated through one-way and probabilistic sensitivity analyses. The results showed that personalised dosimetry reduced the burden of adverse events, which is a non-negligible aspect that may affect from 4% to 17% of patients (42–46).
SIRT may be performed with different types of microspheres such as glass or resin. The ideal radiation therapy is to deliver lethal doses of radiation as high as possible to the tumour while protecting the surrounding normal liver parenchyma. In this analysis, we referred to glass microspheres as they were considered in the reference study (8). Preliminary data, investigating the dose of radiation delivered through glass versus resin-based Y90 SIRT in patients with intrahepatic cholangiocarcinoma, showed a significantly higher ratio of Y90 dose delivered to the tumour versus normal liver in the glass group compared to the resin group (4.9 ± 0.7 vs. 2.4 ± 0.3, respectively, p < 0.001) (47). The conclusions of this analyses are valid for glass microspheres, and we recommend that future studies should replicate this research to other types of microspheres.
Our study has some limitations. First, medical devices show particular challenges for health technology assessments caused by rapid innovation, outcomes influenced by training, the competence of the final users, and dynamic pricing (9). The reference study (8) did not report data on the technical success of the SIRT procedure. In patients with complications, the management cost may increase, potentially compromising the results of this study. This concept is related also to the experience of the operators who perform the interventions. It has been demonstrated that clinical outcomes and resource consumption related to patients managed with new technologies, such as SIRT, may be strongly influenced by the underlying learning curve of the operators (11). Also, centres performing a higher volume of procedures may obtain better performance of the device, yield better health outcomes, and lower procedure costs (11). Continuous data collection and monitoring could provide more robust data for the evaluation of these aspects.
Second, the model was populated according to clinical outcomes reported in a single RCT with a limited number of enrolled patients, and the generalisability of the model results to a broader real-world population, for example to patients with small lesions (i.e., <3 cm), should be performed with caution. Another point relates to the impact of disease severity or risk factors on the cost-effectiveness of personalised dosimetry. The good safety profile of the tailored approach is probably the result of accurate patient selection, with the inclusion of patients with good liver function and a hepatic reserve of at least 30% after selective internal radiation therapy (8); on the other side, baseline liver function abnormalities, prior to radioembolisation, have shown to be predictors of post-treatment toxicities (48). Also, the amount of activity administered to target the liver volume can be considered a risk factor of experiencing SIRT-related side effects (49). In this context, it is likely that patients treated in a real-world setting with personalised dosimetry experience the worst side effects, thus resulting in lower quality of life and higher management costs, leading to a possible worsening of the cost-effectiveness profile versus standard dosimetry.
Third, our model did not include systemic treatments (chemotherapy for progressed patients) performed after SIRT but focused on treatments like liver resections. Nevertheless, these results may be considered conservative because costs are likely to be higher for standard dosimetry, with a higher progression rate compared to personalised treatment. This result was also confirmed by the scenario analysis conducted considering treatment with systemic chemotherapy (lenvatinib) for progressive patients. With the limited availability of RCT data, comparative observational studies, patient registries, or claims databases may be suitable options for the generation of real-world evidence on the effectiveness and safety of medical devices to support health technology assessments (50–52).
Fourth, this model did not take into consideration the organisational impact of the constitution of the interventional radiology and nuclear medicine unit together with a medical physicist in a clinical centre (11, 53). However, it may be used for different purposes, as it entails substantial investments (e.g., adequate spaces, equipment, dedicated personnel, creation of multidisciplinary teams) to implement the diagnostic–therapeutic pathway for the treatment of patients with radiation therapy. Although the investment is initial and this aspect should not influence the comparison between the two treatment options considered, for personalised dosimetry, the cost of a training plan for nuclear physicians and medical physicists may be envisaged. Finally, data on patients’ QOL were derived from published literature, and the transferability of the retrieved utility values to an Italian context was not considered.
Our findings showed that personalised dosimetry for the management of SIRT in patients with HCC may be a cost-effective choice compared to standard dosimetry. These findings provide evidence for clinicians and payers on the value of personalised dosimetry as a treatment option for patients with HCC. An innovative treatment option is now available to clinicians who may offer an appropriate and customised management plan to improve clinical outcomes in patients. For now, decision-makers may use these preliminary results to support a tailored approach in defining and treating the targeted patient populations. Future studies comparing the personalised approach to the standard approach are recommended to increase the clinical evidence to confirm or reject the validity of this preliminary evaluation.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Author contributions
CR and RT contributed to the conception and design of the study. CR performed the cost-effectiveness analysis. CR wrote the first draft of the manuscript. RT supervised the manuscript preparation. MRB, IB, MGB, MBe, MBr, PC, RC, LC, FD’A, MD’A, SD, DD, PS, AD, MF, PF, SG, SI, FL, GM, AM, DS, and RV provided data on healthcare resource consumption. All authors contributed to manuscript revision and read and approved the submitted version.
Funding
This study was funded by Confindustria Dispositivi Medici Servizi Srl through an unrestricted grant to CERGAS, SDA Bocconi School of Management, via Sarfatti 10, 20136 Milan, Italy.
Conflict of interest
The authors declare that this study received funding from Confindustria Dispositivi Medici Servizi Srl. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2022.920073/full#supplementary-material
References
1. Worldwide cancer data. (2022) London: World Cancer Research Fund International. Available at: https://www.wcrf.org/dietandcancer/worldwide-cancer-data/.
2. Lafaro KJ, Demirjian AN, Pawlik TM. Epidemiology of hepatocellular carcinoma. Surg Oncol Clin N Am (2015) 24(1):1–17. doi: 10.1016/j.soc.2014.09.001
3. Hepatocellular carcinoma: Considerations for managed care professionals. Available at: https://www.ajmc.com/view/hepatocellular-carcinoma-considerations-for-managed-care-professionals.
4. Dawson LA, McGinn CJ, Normolle D, Ten Haken RK, Walker S, Ensminger W, et al. Escalated focal liver radiation and concurrent hepatic artery fluorodeoxyuridine for unresectable intrahepatic malignancies. J Clin Oncol Off J Am Soc Clin Oncol (2000) 18(11):2210–8. doi: 10.1200/JCO.2000.18.11.2210
5. Dawson LA, Normolle D, Balter JM, McGinn CJ, Lawrence TS, Ten Haken RK. Analysis of radiation-induced liver disease using the Lyman NTCP model. Int J Radiat Oncol Biol Phys (2002) 53(4):810–21. doi: 10.1016/S0360-3016(02)02846-8
6. Garin E, Rolland Y, Edeline J, Icard N, Lenoir L, Laffont S, et al. Personalized dosimetry with intensification using 90Y-loaded glass microsphere radioembolization induces prolonged overall survival in hepatocellular carcinoma patients with portal vein thrombosis. J Nucl Med Off Publ Soc Nucl Med (2015) 56(3):339–46. doi: 10.2967/jnumed.114.145177
7. Garin E, Lenoir L, Rolland Y, Edeline J, Mesbah H, Laffont S, et al. Dosimetry based on 99mTc-macroaggregated albumin SPECT/CT accurately predicts tumor response and survival in hepatocellular carcinoma patients treated with 90Y-loaded glass microspheres: preliminary results. J Nucl Med Off Publ Soc Nucl Med (2012) 53(2):255–63. doi: 10.2967/jnumed.111.094235
8. Garin E, Tselikas L, Guiu B, Chalaye J, Edeline J, de Baere T, et al. Personalised versus standard dosimetry approach of selective internal radiation therapy in patients with locally advanced hepatocellular carcinoma (DOSISPHERE-01): a randomised, multicentre, open-label phase 2 trial. Lancet Gastroenterol Hepatol (2021) 6(1):17–29. doi: 10.1016/S2468-1253(20)30290-9
9. Tarricone R, Amatucci F, Armeni P, Banks H, Borsoi L, Callea G, et al. Establishing a national HTA program for medical devices in Italy: Overhauling a fragmented system to ensure value and equal access to new medical technologies. Health Policy (2021) 125(5):602–8. doi: 10.1016/j.healthpol.2021.03.003
10. Husereau D, Drummond M, Petrou S, de Bekker-Grob E, Briggs AH, Carswell C, et al. Consolidated health economic evaluation reporting standards (CHEERS)–explanation and elaboration: a report of the ISPOR health economic evaluation publication guidelines good reporting practices task force. Value Health J Int Soc Pharmacoeconomics Outcomes Res (2013) 16(2):231–50. doi: 10.1016/j.jval.2013.02.002
11. Tarricone R, Callea G, Ogorevc M, Prevolnik Rupel V. Improving the methods for the economic evaluation of medical devices. Health Econ (2017) 26 Suppl:1, 70–92. doi: 10.1002/hec.3471
12. Linee guida 2020 epatocarcinoma, Vol. 154 (2020). AIOM (Associazione Italiana di Oncologia Medica), Italy
13. Vogel A, Cervantes A, Chau I, Daniele B, Llovet JM, Meyer T, et al. Hepatocellular carcinoma: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol 29 iv238–iv255 (2018). doi: 10.1093/annonc/mdy308
14. EASL–EORTC clinical practice guidelines: Management of hepatocellular carcinoma. Eur J Cancer (2012) 48(5):599–641.
15. Woods BS, Sideris E, Palmer S, Latimer N, Soares M. Partitioned survival and state transition models for healthcare decision making in oncology: Where are we now? Value Health (2020) 23(12):1613–21. doi: 10.1016/j.jval.2020.08.2094
16. Partitioned survival analysis TSD – NICE decision support unit. Available at: http://nicedsu.org.uk/technical-support-documents/partitioned-survival-analysis-tsd/.
17. PE Guidelines around the world: Italy. Available at: https://tools.ispor.org/PEguidelines/countrydet.asp?c=13&t=4.
18. Kudo M, Finn RS, Qin S, Han KH, Ikeda K, Piscaglia F, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non-inferiority trial. Lancet (2018) 391(10126):1163–73. doi: 10.1016/S0140-6736(18)30207-1
19. Gazzetta ufficiale. Available at: https://www.gazzettaufficiale.it/eli/id/2019/11/12/19A06972/sg.
20. Cammà C, Cabibbo G, Petta S, Enea M, Iavarone M, Grieco A, et al. Cost-effectiveness of sorafenib treatment in field practice for patients with hepatocellular carcinoma. Hepatol Baltim Md (2013) 57(3):1046–54. doi: 10.1002/hep.26221
21. Rognoni C, Ciani O, Sommariva S, Tarricone R. Real-world data for the evaluation of transarterial radioembolization versus sorafenib in hepatocellular carcinoma: A cost-effectiveness analysis. Value Health J Int Soc Pharmacoeconomics Outcomes Res (2017) 20(3):336–44. doi: 10.1016/j.jval.2016.09.2397
22. Search the CEA registry. Available at: http://healtheconomics.tuftsmedicalcenter.org/cear2n/search/search.aspx.
23. Bullement A, Nathan P, Willis A, Amin A, Lilley C, Stapelkamp C, et al. Cost effectiveness of avelumab for metastatic merkel cell carcinoma. PharmacoEconomics - Open (2019) 3(3):377–90. doi: 10.1007/s41669-018-0115-y
24. Holleman MS, Al MJ, Zaim R, Groen HJM, Uyl-de Groot CA. Cost-effectiveness analysis of the first-line EGFR-TKIs in patients with non-small cell lung cancer harbouring EGFR mutations. Eur J Health Econ HEPAC Health Econ Prev Care (2020) 21(1):153–64. doi: 10.1007/s10198-019-01117-3
25. Guan H, Liu G, Xie F, Sheng Y, Shi L. Cost-effectiveness of osimertinib as a second-line treatment in patients with EGFR-mutated advanced non-small cell lung cancer in China. Clin Ther (2019) 41(11):2308–2320.e11. doi: 10.1016/j.clinthera.2019.09.008
26. Zargar M, McFarlane T, Chan KKW, Wong WWL. Cost-effectiveness of nivolumab in recurrent metastatic head and neck squamous cell carcinoma. Oncologist (2018) 23(2):225–33. doi: 10.1634/theoncologist.2017-0277
27. Shen NT, Schneider Y, Congly SE, Rosenblatt RE, Namn Y, Fortune BE, et al. Cost effectiveness of early insertion of transjugular intrahepatic portosystemic shunts for recurrent ascites. Clin Gastroenterol Hepatol Off Clin Pract J Am Gastroenterol Assoc (2018) 16(9):1503–1510.e3. doi: 10.1016/j.cgh.2018.03.027
28. Sivignon M, Monnier R, Tehard B, Roze S. Cost-effectiveness of alectinib compared to crizotinib for the treatment of first-line ALK+ advanced non-small-cell lung cancer in France. PloS One (2020) 15(1):e0226196. doi: 10.1371/journal.pone.0226196
29. Park S, Kim A-Y, Cho H, Baik D, Lee H, Cho S, et al. Cost-utility analysis of pralatrexate for relapsed or refractory peripheral T-cell lymphoma based on a case-matched historical control study along with single arm clinical trial. BMC Cancer (2020) 20(1):1157. doi: 10.1186/s12885-020-07629-z
30. Li J, Zhang T, Xu Y, Lu P, Zhu J, Liang W, et al. Cost-effectiveness analysis of nivolumab plus ipilimumab versus chemotherapy as first-line treatment in advanced NSCLC. Immunotherapy (2020) 12(14):1067–75. doi: 10.2217/imt-2020-0112
31. Bregman B, Teitsson S, Orsini I, Cotté FE, Amadi A, Moshyk A, et al. Cost-utility analysis of nivolumab in adjuvant treatment of melanoma in France. Dermatol Ther (2020) 10(6):1331–43. doi: 10.1007/s13555-020-00446-z
32. Ding D, Hu H, Liao M, Shi Y, She L, Yao L, et al. Cost-effectiveness analysis of atezolizumab plus chemotherapy in the first-line treatment of metastatic non-squamous non-small cell lung cancer. Adv Ther (2020) 37(5):2116–26. doi: 10.1007/s12325-020-01292-3
33. Sarkar RR, Gloude NJ, Schiff D, Murphy JD. Cost-effectiveness of chimeric antigen receptor T-cell therapy in pediatric Relapsed/Refractory b-cell acute lymphoblastic leukemia. J Natl Cancer Inst (2019) 111(7):719–26. doi: 10.1093/jnci/djy193
34. Mistry R, May JR, Suri G, Young K, Brixner D, Oderda G, et al. Cost-effectiveness of ribociclib plus letrozole versus palbociclib plus letrozole and letrozole monotherapy in the first-line treatment of postmenopausal women with HR+/HER2- advanced or metastatic breast cancer: A U.S. payer perspective. J Manage Care Spec Pharm (2018) 24(6):514–23. doi: 10.18553/jmcp.2018.24.6.514
35. Rajan N, Boye KS, Gibbs M, Lee YJ, Davey P, Ball M, et al. Utilities for type 2 diabetes treatment-related attributes in a south Korean and Taiwanese population. Value Health Reg Issues (2016) 9:67–71. doi: 10.1016/j.vhri.2015.11.006
36. Lekuona I, Anguita M, Zamorano JL, Rodríguez JM, Barja de Soroa P, Pérez-Alcántara F. Would the use of edoxaban be cost-effective for the prevention of stroke and systemic embolism in patients with nonvalvular atrial fibrillation in Spain? Rev Espanola Cardiol Engl Ed (2019) 72(5):398–406. doi: 10.1016/j.rec.2018.03.024
37. Chen PY, Finkelstein EA, Ng MJ, Yap F, Yeo GS, Rajadurai VS, et al. Incremental cost-effectiveness analysis of gestational diabetes mellitus screening strategies in Singapore. Asia Pac J Public Health (2016) 28(1):15–25. doi: 10.1177/1010539515612908
38. Nardini C, Osmani V, Cormio PG, Frosini A, Turrini M, Lionis C, et al. The evolution of personalized healthcare and the pivotal role of European regions in its implementation. Per Med (2021) 18(3):283–94. doi: 10.2217/pme-2020-0115.
39. Chiesa C, Sjogreen-Gleisner K, Walrand S, Strigari L, Flux G, Gear J, et al. EANM dosimetry committee series on standard operational procedures: a unified methodology for 99mTc-MAA pre- and 90Y peri-therapy dosimetry in liver radioembolization with 90Y microspheres. EJNMMI Phys (2021) 8:77. doi: 10.1186/s40658-021-00394-3
40. Fattore G. Proposta di linee guida per la valutazione economica degli interventi sanitari in Italia. Pharmacoeconomics-Ital-Res-Articles (2009) 11:83–93. doi: 10.1007/BF03320660
41. Messori A, Santarlasci B, Trippoli S. Guadagno di sopravvivenza dei nuovi farmaci. PharmacoEconomics Ital Res Artic (2004) 6(2):95–104. doi: 10.1007/BF03320627
42. Jha AK, Larizgoitia I, Audera-Lopez C, Prasopa-Plaizier N, Waters H, Bates DW. The global burden of unsafe medical care: analytic modelling of observational studies. BMJ Qual Saf (2013) 22(10):809–15. doi: 10.1136/bmjqs-2012-001748
43. Allué N, Chiarello P, Bernal Delgado E, Castells X, Giraldo P, Martínez N, et al. [Assessing the economic impact of adverse events in Spanish hospitals by using administrative data]. Gac Sanit (2014) 28(1):48–54. doi: 10.1016/j.gaceta.2013.06.004
44. de Vries EN, Ramrattan MA, Smorenburg SM, Gouma DJ, Boermeester MA. The incidence and nature of in-hospital adverse events: a systematic review. Qual Saf Health Care (2008) 17(3):216–23. doi: 10.1136/qshc.2007.023622
45. Johnston SS, Juday T, Esker S, Espindle D, Chu BC, Hebden T, et al. Comparative incidence and health care costs of medically attended adverse effects among U.S. Medicaid HIV patients on atazanavir- or darunavir-based antiretroviral therapy. Value Health J Int Soc Pharmacoeconomics Outcomes Res (2013) 16(2):418–25. doi: 10.1016/j.jval.2012.10.021
46. Vincent C, Neale G, Woloshynowych M. Adverse events in British hospitals: preliminary retrospective record review. BMJ (2001) 322(7285):517–9. doi: 10.1136/bmj.322.7285.517
47. Nezami N, Kokabi N, Camacho JC, Schuster DM, Xing M, Kim HS. 90Y radioembolization dosimetry using a simple semi-quantitative method in intrahepatic cholangiocarcinoma: Glass versus resin microspheres. Nucl Med Biol (2018) 59:22–8. doi: 10.1016/j.nucmedbio.2018.01.001
48. Brown D, Krebs H, Brower J, O'Hara R, Wang E, Vaheesan K, et al. Incidence and risk factors for sustained hepatic function toxicity 6 months after radioembolization: analysis of the radiation-emitting sir-spheres in non-resectable liver tumor (RESIN) registry. J Gastrointest Oncol (2021) 12(2):639–65. doi: 10.21037/jgo-20-346
49. Sangro B, Gil-Alzugaray B, Rodriguez J, Sola I, Martinez-Cuesta A, Viudez A, et al. Liver disease induced by radioembolization of liver tumors. Cancer (2008) 112(7):1538–46. doi: 10.1002/cncr.23339
50. Tarricone R, Boscolo PR, Armeni P. What type of clinical evidence is needed to assess medical devices? Eur Respir Rev Off J Eur Respir Soc (2016) 25(141):259–65. doi: 10.1183/16000617.0016-2016
51. Daubner-Bendes R, Kovács S, Niewada M, Huic M, Drummond M, Ciani O, et al. Quo vadis HTA for medical devices in central and Eastern Europe? recommendations to address methodological challenges. Front Public Health (2020) 8:612410. doi: 10.3389/fpubh.2020.612410
52. Pongiglione B, Torbica A, Blommestein H, de Groot S, Ciani O, Walker S, et al. Do existing real-world data sources generate suitable evidence for the HTA of medical devices in Europe? mapping and critical appraisal. Int J Technol Assess Health Care (2021) 37(1):e62. doi: 10.1017/S0266462321000301
Keywords: trans-arterial radioembolisation, cost-effectiveness, cost-utility, personalised dosimetry, tailored treatment
Citation: Rognoni C, Barcellona MR, Bargellini I, Bavetta MG, Bellò M, Brunetto M, Carucci P, Cioni R, Crocetti L, D’Amato F, D’Amico M, Deagostini S, Deandreis D, De Simone P, Doriguzzi A, Finessi M, Fonio P, Grimaldi S, Ialuna S, Lagattuta F, Masi G, Moreci A, Scalisi D, Virdone R and Tarricone R (2022) Cost-effectiveness analysis of personalised versus standard dosimetry for selective internal radiation therapy with TheraSphere in patients with hepatocellular carcinoma. Front. Oncol. 12:920073. doi: 10.3389/fonc.2022.920073
Received: 14 April 2022; Accepted: 28 July 2022;
Published: 29 August 2022.
Edited by:
Silvia Cammelli, University of Bologna, ItalyReviewed by:
Cinzia Pettinato, Ca ‘Granda Foundation Maggiore Policlinico Hospital (IRCCS), ItalyJackie Yao, The Chinese University of Hong Kong, Hong Kong SAR, China
Copyright © 2022 Rognoni, Barcellona, Bargellini, Bavetta, Bellò, Brunetto, Carucci, Cioni, Crocetti, D’Amato, D’Amico, Deagostini, Deandreis, De Simone, Doriguzzi, Finessi, Fonio, Grimaldi, Ialuna, Lagattuta, Masi, Moreci, Scalisi, Virdone and Tarricone. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Carla Rognoni, Y2FybGEucm9nbm9uaUB1bmlib2Njb25pLml0