 Motaz Hamed1*
Motaz Hamed1* Niklas Schäfer2Christian Bode3Valeri Borger1Anna-Laura Potthoff1
Niklas Schäfer2Christian Bode3Valeri Borger1Anna-Laura Potthoff1 Lars Eichhorn3Frank A. Giordano4
Lars Eichhorn3Frank A. Giordano4 Erdem Güresir1
Erdem Güresir1 Muriel Heimann1Yon-Dschun Ko5
Muriel Heimann1Yon-Dschun Ko5 Jennifer Landsberg6
Jennifer Landsberg6 Felix Lehmann3Alexander Radbruch7Elisa Scharnböck1Christina Schaub2Katjana S. Schwab8Johannes Weller2Ulrich Herrlinger2Hartmut Vatter1
Felix Lehmann3Alexander Radbruch7Elisa Scharnböck1Christina Schaub2Katjana S. Schwab8Johannes Weller2Ulrich Herrlinger2Hartmut Vatter1 Patrick Schuss1†
Patrick Schuss1† Matthias Schneider1†
Matthias Schneider1†- 1Department of Neurosurgery, Center of Integrated Oncology (CIO) Bonn, University Hospital Bonn, Bonn, Germany
- 2Division of Clinical Neuro-Oncology, Department of Neurology, Center of Integrated Oncology (CIO) Bonn, University Hospital Bonn, Bonn, Germany
- 3Department of Anesthesiology and Intensive Care, University Hospital Bonn, Bonn, Germany
- 4Department of Radiation Oncology, Center of Integrated Oncology (CIO) Bonn, University Hospital Bonn, Bonn, Germany
- 5Department of Oncology and Hematology, Center of Integrated Oncology (CIO) Bonn, Johanniter Hospital Bonn, Bonn, Germany
- 6Department of Dermatology and Allergy, Center of Integrated Oncology (CIO) Bonn, University Hospital Bonn, Bonn, Germany
- 7Department of Neuroradiology, Center of Integrated Oncology (CIO) Bonn, University Hospital Bonn, Bonn, Germany
- 8Department of Internal Medicine III, Center of Integrated Oncology (CIO) Bonn, University Hospital Bonn, Bonn, Germany
Object: Intra-tumoral hemorrhage is considered an imaging characteristic of advanced cancer disease. However, data on the influence of intra-tumoral hemorrhage in patients with brain metastases (BM) remains scarce. We aimed at investigating patients with BM who underwent neurosurgical resection of the metastatic lesion for a potential impact of preoperative hemorrhagic transformation on overall survival (OS).
Methods: Between 2013 and 2018, 357 patients with BM were surgically treated at the authors’ neuro-oncological center. Preoperative magnetic resonance imaging (MRI) examinations were assessed for the occurrence of malignant hemorrhagic transformation.
Results: 122 of 375 patients (34%) with BM revealed preoperative intra-tumoral hemorrhage. Patients with hemorrhagic transformed BM exhibited a median OS of 5 months compared to 12 months for patients without intra-tumoral hemorrhage. Multivariate analysis revealed preoperative hemorrhagic transformation as an independent and significant predictor for worsened OS.
Conclusions: The present study identifies preoperative intra-tumoral hemorrhage as an indicator variable for poor prognosis in patients with BM undergoing neurosurgical treatment.
Introduction
Hemorrhage in brain metastases (BM) is not rare, especially in the case of BM in melanoma patients (1, 2). The incidence of intracerebral/intra-tumoral hemorrhage caused by cerebral neoplasms may exceed 20% (2–5). With technical advances in imaging, microbleeds within tumors are becoming increasingly visualized even when they may have remained clinically inapparent (6, 7). On the other hand, acute hemorrhage may also trigger new neurologic symptoms or their aggravation in a considerable number of patients (2). This sudden event may lead to expedited access to diagnostic testing for BM, which may be associated with a more favorable disease course due to potentially earlier initiation. However, increased aggressiveness and pathological remodeling processes within the tumor tissue are also debated as potential mechanisms for hemorrhage (8). This notion is corroborated by reports on low tumor control rates after stereotactic radiotherapy (9, 10). The circumstance of inconsistent/different post-treatment modality may be a substantial contributor to a poorer outcome being reported in some cases (11). Nonetheless, important information on the influence of the observed hemorrhage on the prognosis of patients with BM remains scarce. In the present study, we reviewed and analyzed all patients who underwent surgical treatment for BM from extracranial primaries at our institution. By investigating the impact of this factor on survival before undergoing surgical resection, we hope to circumvent a possible surrogate effect that could result from radiation therapy alone to a hemorrhagic transformed lesion. Therefore, the primary study objective was to determine the influence of hemorrhagic transformation as an preoperatively easily collectable MRI-morphological parameter on overall survival for BM requiring surgery.
Methods
Patients
All patients with surgical management and subsequent histopathological evidence of BM in the authors’ institution were entered into a computerized database (SPSS, version 25, IBM Corp., Armonk, NY). Beforehand, this study had been approved by the institutional ethics committee. Institutional ethics committee approval was obtained for this study. Individual treatment decisions were determined at the first presentation of the patient and during subsequent follow-up through weekly institutional interdisciplinary tumor advisory board meetings for the central nervous system, as previously described (4).
Information, including patient characteristics, radiological features, preoperative laboratory values and functional neurological status at admission was collected and further analyzed. Hemorrhagic metastases were those that were either clearly identified on imaging by blood fluid levels, in cases where MRI sequencing on T1 pre-contrast sequences suggested the presence of blood products, or lesions suspicious for bleeding were identified on susceptibility weighted imaging (SWI). Tumor volumes were volumetrically assessed manually in T1 weighted MRI sequences using commercially available software (TumorTracking Tool, IntelliSpace Portal 5.0, Philips, Best, the Netherlands). The Karnofsky performance score (KPS) was used to evaluate patients according to their neurological functional status preoperatively. For further analysis, the results were dichotomized and thus a KPS ≥70 was defined as favorable outcome. Regarding the preoperative classification according to the American Society of Anesthesiologists (ASA), the included patients were divided into two groups: preoperative ASA 1 or 2 versus preoperative ASA ≥ 3. To estimate the preoperative comorbidity burden of surgically treated patients with BM, the Charlson Comorbidity Index (CCI) was assessed using the preoperative information. Here, patients were divided into two groups according to their burden: CCI ≤ 10 versus CCI > 10, as previously defined (4).
Overall survival (OS) was measured from the day of BM surgery until death or last observation. Patients in whom no further follow-up information was available due to further off-site treatment were excluded from further analysis. All parameters were compared in terms of OS.
Statistics
Data analysis was performed using the computer software package SPSS (version 25, IBM Corp., Armonk, NY). Unpaired categorical and binary variables were analyzed in contingency tables using the Fisher’s exact test. The Mann-Whitney U-test was chosen to compare continuous variables as the data were mostly not normally distributed. OS was analyzed by the Kaplan-Meier method. With reference to Heinze and Dunkler (12) preoperatively collectable parameters with known prognostic influence based on the literature as well as hemorrhagic transformation were entered in a multivariate analysis using the Cox proportional hazard model. Results with p<0.05 were considered statistically significant.
Results
Patient Characteristics
Between 2013 and 2018, a total of 382 patients with BM were surgically treated at the authors’ neuro-oncological center. 25 patients were excluded from further analysis after careful review of clinical records due to lack of further follow-up information. Therefore, 357 patients with surgically treated BM were included in further analysis. The median age was 65 years (range 20-91 years). At admission, patients presented with a median KPS score of 80. Median overall survival for patients with surgically treated BM was 10 months (95% CI 8.1-11.9).
26 out of 357 patients with surgically-resected BM (7%) were treated with adjuvant immuno- and/or chemotherapy only, 66 patients (18%) with adjuvant radiotherapy only and 233 patients (62%) with adjuvant combined chemo-, immuno- and radiotherapy. Patients with postoperative adjuvant oncological therapy exhibited a mOS of 12 months compared to 1 month for patients without postoperative adjuvant treatment (p<0.0001). 20 out of 244 patients with solitary BM (8%) received adjuvant immuno- and/or chemotherapy, 50 patients (20%) received adjuvant radiotherapy (among them 9 patients with whole brain radiation) and 146 patients (60%) were treated with a combination of adjuvant radio-, immuno- and chemotherapy. 28 patients (11%) received no adjuvant oncological therapy. 70 out of 133 patients (53%) with multiple BM received postoperative whole brain RT. See Table 1 for more patient-specific details.
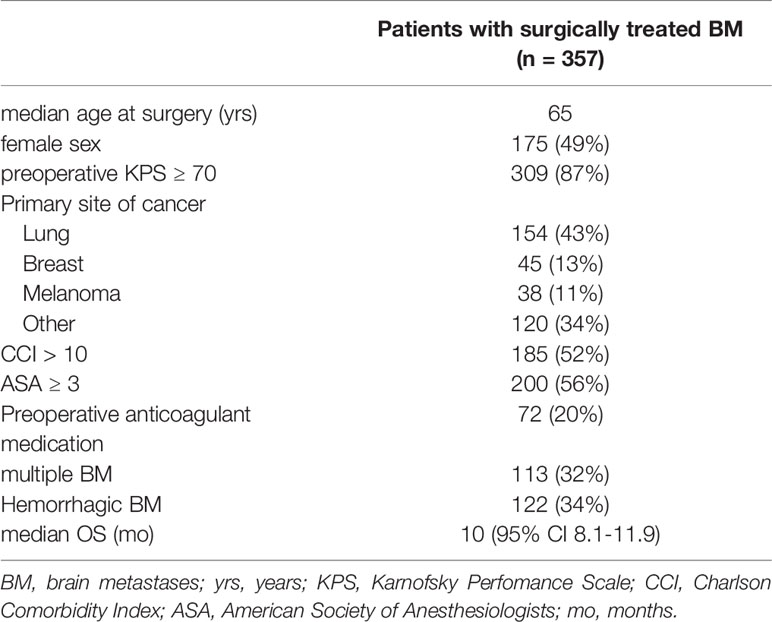
Table 1 Patient characteristics.
Influence of Intra-Tumoral Hemorrhagic Transformation/Hemorrhage
Overall, 122 patients (34%) suffered from preoperative hemorrhagic transformation of the surgically treated BM (Table 2). Patients with hemorrhagic BM were significantly older compared to patients without BM-associated hemorrhage at the time of surgery (p=0.003). Patients with intratumoral hemorrhage exhibited a median tumor volume of 24 ml (95% CI 18-30) compared to 14 ml (95% CI 10-17) for patients without preoperative intratumoral hemorrhage (p=0.002). Spearman correlation analysis could not find a strong correlation between tumor volume and OS (Spearman’s r = -0.12). Patients with hemorrhagic BM presented significantly more often with preoperative KPS < 70 compared to patients with non-hemorrhagic BM (p=0.02). Regarding the site of origin of the cancer, hemorrhagic transformed BM have been observed preoperatively significantly more often in patients with lung cancer (p=0.01) and patients with melanoma (p<0.0001). In contrast, patients with metastatic breast cancer presented less often with hemorrhagic transformed BM (p=0.04). Patients with higher preoperative comorbidity burden (CCI > 10) were more likely to suffer from preoperative bleeding into the BM to be resected than patients with lower burden of comorbid diseases (p=0.001). Patients with hemorrhagic BM received significantly more frequent preoperative administration of anticoagulant medication compared to patients without hemorrhagic BM (p=0.005). 26 out of 122 patients (21%) with preoperative intratumoral haemorrhage suffered from local recurrence of the metastatic lesion in the later course of cancer disease compared to 71 out of 253 patients (28%) without preoperative intratumoral haemorrhage (p=0.2).
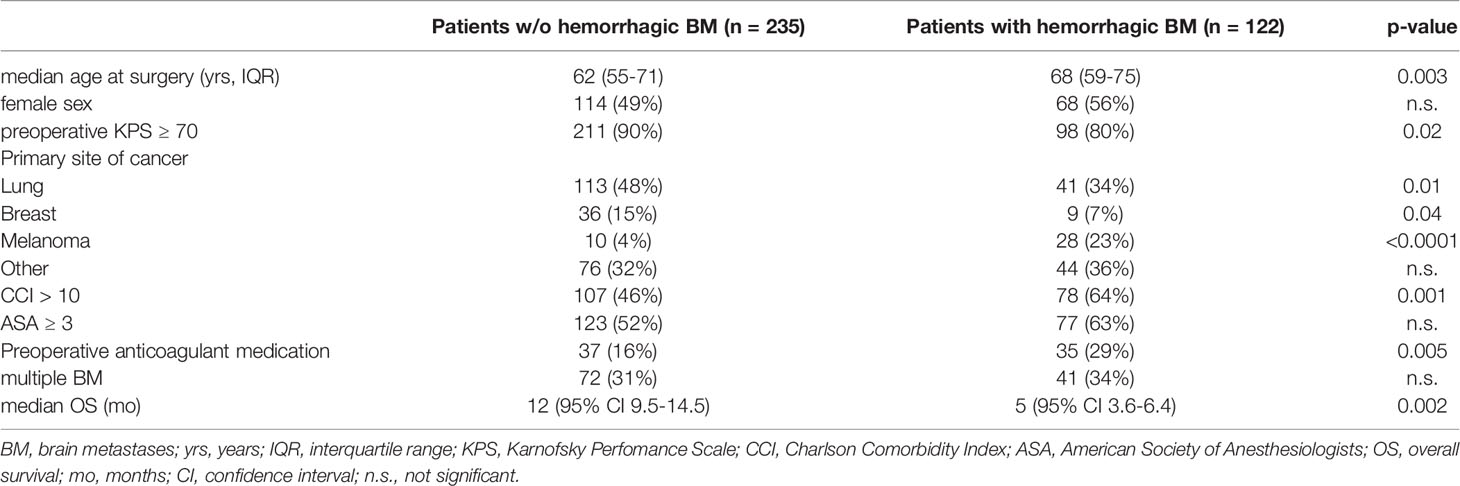
Table 2 Characteristics of hemorrhagic brain metastases.
Patients with a preoperative hemorrhagic transformed BM achieved a median OS of 5 months (95% CI 3.6-6.4), whereas patients with BM but without an apparent intra-tumoral hemorrhage achieved a median OS of 12 months (95% CI 9.5-14.5; p=0.002; Figure 1).
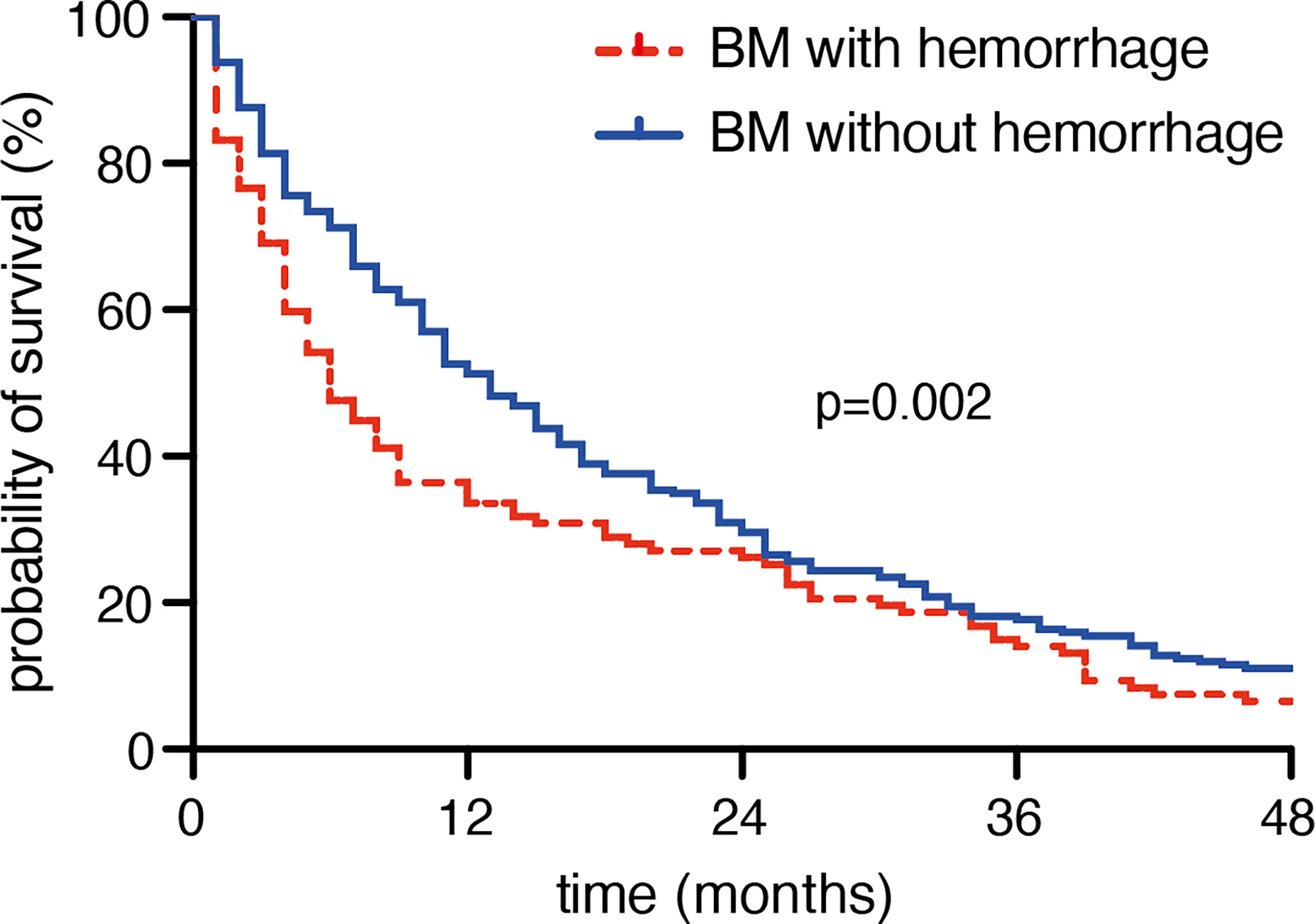
Figure 1 Preoperative hemorrhage is associated with poor survival in patients with brain metastases.
Multivariate Analysis
A Cox regression analysis was performed in order to identity factors influencing OS in patients with surgically treated BM. The multivariate analysis revealed “age > 65 years” (p=0.005, HR 1.4, 95% CI 1.1-1.8), “preoperative KPS < 70” (p=0.005, HR 1.6, 95% CI 1.2-2.3), “multiple BM” (p<0.0001, HR 1.7, 95% CI 1.3-2.2), as well as “preoperative hemorrhagic transformation of BM” (p=0.009, HR 1.4, 95% CI 1.1-1.8) as independent and significant predictors for dismal overall survival.
Discussion
Intra-tumoral hemorrhage in patients with metastatic intracranial lesions is a recognized characteristic that seems to occur in about 24% of all BM (2, 13). This number was found to be reproducible in the present study. Furthermore, in this selected patient collective of patients with surgically treated BM, preoperative intra-tumoral hemorrhage is shown to be a significant predictor of poor prognosis.
Various theories for the origin of intra-tumoral hemorrhage have been discussed. These include tumor-induced endothelial proliferation with vascular obliteration, vessel compression and/or distortion due to rapid aggressive tumor growth, as well as tumorous vessel wall invasion, and also elevated venous pressure in response to increased local intracranial pressure (2, 8). These histopathological interpretations seem to indicate an increased aggressiveness within the tumor lesion in patients with BM and intra-tumoral hemorrhage. This aspect seems to be reflected in the fact that patients with intra-tumoral hemorrhage had a worse prognosis in the present study.
Even in the case that surgical resection is not chosen as the method of first choice, intra-tumoral hemorrhage in BM seems to be associated with worse survival/outcome in other studies as well. Thus, a recent study by Bauer-Nilsen and colleagues has demonstrated that in cases of hemorrhagic BM, local control by radiotherapy is less likely to be achieved compared with BM without hemorrhagic transformation (14).
Nevertheless, the mere survival of patients with and without intra-tumoral hemorrhage has to be illuminated in more detail on the basis of the different characteristics. Patients with hemorrhagic transformation of BM are significantly older at the time of surgery compared to patients without such hemorrhage. Age itself seems to play an equally important role with regard to OS in patients with surgically treated BM, as shown by the present multivariate analysis. Apart from intra-tumoral hemorrhage, (older) age is an important prognostic factor for overall survival in patients with BM (15–17). Older age might also lead to an increased correlating burden of comorbidities. Again, a higher preoperative CCI value is evident in the present patient collective with intra-tumoral hemorrhage. An increased burden of comorbid concomitant diseases is also associated with a higher incidence of postoperative complications, which can significantly influence the further survival of the affected patient (4, 18). According to the definition of the CCI used here, existing diseases that require anticoagulant medication are also included (e.g., myocardial infarction, history of transient ischemic attacks) (19). Thus, it should come as no surprise that patients on anticoagulant medication are significantly more likely to present for surgical resection with intra-tumoral hemorrhage in the present series. On the other hand, cancer patients are more at risk for thromboembolic events. However, the rate of additional intra-tumoral hemorrhage does not seem to be influenced by the administration of low-molecular-weight heparin in patients with BM (20). Furthermore, indicated therapeutic anticoagulation in patients with BM does not appear to confer an increased risk of intracerebral hemorrhage/intra-tumoral hemorrhage based on the existing evidence (21). Moreover, the presence and severity of preoperative intratumoral hemorrhage might also depend on the entity of the underlying cancer disease. In line with the trend in the present series, melanoma has been reported to constitute a tumor entity with hemorrhagic transformation in the earlier course of disease (22). Further tumor entities like renal cell carcinoma are known to exhibit elevated levels of intratumoral hemorrhage (23) and might therefore not only lead to a correlation between tumor entity and survival, but also between the level of preoperative hemorrhage and survival. Further studies will be needed in order to more sufficiently address these potential prognostic MRI morphologic characteristics.
Nevertheless, in contrast to this possible causal linkage, the present multivariate cox analysis reveals a clear and independent influence of intra-tumoral hemorrhage on OS in patients with BM requiring surgical treatment. However, this fact should not discourage, but on the contrary: it should sensitize the perception regarding this seemingly elementary influence of intra-tumoral hemorrhage enabling a timely planning of the further therapy as well as a more precise information of patients/relatives about the eventual course of the disease as early as in the preoperative phase. In particular, due to a lower efficacy of radiosurgery of hemorrhagic BMs, potential improvement of neurological deterioration as well as reduction of tumor burden, surgical resection should remain as a treatment option if feasible (13, 14). However, because of the potential accompanying specific factors, an individual and in particular interdisciplinary evaluation of affected patients with BM indispensably remains an essential part of patient-centered management.
Limitations
Besides the inherent limitation of the retrospective design of this study, another relevant shortcoming is the assessment of hemorrhagic characteristics. These features were not centrally reviewed, leading to a potential interpreter bias. Despite a moderate sample size, further subgroup analyses are limited because of the then smaller number of hemorrhagic events.
Conclusions
In the present study, preoperative evidence of intra-tumoral hemorrhage was identified as indicators of poor prognosis in patients with BM undergoing neurosurgical treatment. In addition to improved counseling of affected patients, this finding also enables timely and individualized planning of further therapy in the context of interdisciplinary decision making in patients with BM.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethics Committee University Hospital Bonn. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
Conceptualization: MoH, PS and MS. Methodology: MuH, PS and MS. Validation: MoH, NS, UH, PS and MS. Formal analysis: MoH, NS, PS and MS. Writing – original draft preparation: MoH, PS and MS. Writing – review and editing: MoH, NS, CB, VB, LE, FG, EG, MoH, Y-DK, JL, FL, AR, ES, CS, KS, JW, UH, HV, PS and MS. Visualization: PS and MS. Supervision: UH, HV, PS and MS. Project administration: PS and MS. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Mandybur TI. Intracranial Hemorrhage Caused by Metastatic Tumors. Neurology (1977) 27(7):650–5. doi: 10.1212/wnl.27.7.650
2. Kondziolka D, Bernstein M, Resch L, Tator CH, Fleming JF, Vanderlinden RG, et al. Significance of Hemorrhage Into Brain Tumors: Clinicopathological Study. J Neurosurg (1987) 67(6):852–7. doi: 10.3171/jns.1987.67.6.0852
3. Schrader B, Barth H, Lang EW, Buhl R, Hugo HH, Biederer J, et al. Spontaneous Intracranial Haematomas Caused by Neoplasms. Acta Neurochirurgica (2000) 142(9):979–85. doi: 10.1007/s007010070052
4. Schneider M, Heimann M, Schaub C, Eichhorn L, Potthoff AL, Giordano FA, et al. Comorbidity Burden and Presence of Multiple Intracranial Lesions Are Associated With Adverse Events After Surgical Treatment of Patients With Brain Metastases. Cancers (2020) 12(11). doi: 10.3390/cancers12113209
5. Schneider M, Schäfer N, Bode C, Borger V, Eichhorn L, Giordano FA, et al. Prognostic Value of Preoperative Inflammatory Markers in Melanoma Patients With Brain Metastases. J Clin Med (2021) 10(4). doi: 10.3390/jcm10040634
6. Radbruch A, Bendszus M. Advanced MR Imaging in Neuro-Oncology. Clin Neuroradiol (2015) 25 Suppl 2:143–9. doi: 10.1007/s00062-015-0439-2
7. Franceschi AM, Moschos SJ, Anders CK, Glaubiger S, Collichio FA, Lee CB, et al. Use of Susceptibility-Weighted Imaging (SWI) in the Detection of Brain Hemorrhagic Metastases From Breast Cancer and Melanoma. J Comput Assisted Tomography (2016) 40(5):803–5. doi: 10.1097/RCT.0000000000000420
8. Jung S, Moon KS, Jung TY, Kim IY, Lee YH, Rhu HH, et al. Possible Pathophysiological Role of Vascular Endothelial Growth Factor (VEGF) and Matrix Metalloproteinases (MMPs) in Metastatic Brain Tumor-Associated Intracerebral Hemorrhage. J Neuro-Oncol (2006) 76(3):257–63. doi: 10.1007/s11060-005-6876-z
9. Redmond AJ, Diluna ML, Hebert R, Moliterno JA, Desai R, Knisely JP, et al. Gamma Knife Surgery for the Treatment of Melanoma Metastases: The Effect of Intratumoral Hemorrhage on Survival. J Neurosurg (2008) 109 Suppl:99–105. doi: 10.3171/JNS/2008/109/12/S16
10. Liew DN, Kano H, Kondziolka D, Mathieu D, Niranjan A, Flickinger JC, et al. Outcome Predictors of Gamma Knife Surgery for Melanoma Brain Metastases. Clin Article J Neurosurg (2011) 114(3):769–79. doi: 10.3171/2010.5.JNS1014
11. Lesueur P, Kao W, Leconte A, Geffrelot J, Lequesne J, Lacroix J, et al. Stereotactic Radiotherapy on Brain Metastases With Recent Hemorrhagic Signal: STEREO-HBM, a Two-Step Phase 2 Trial. BMC Cancer (2020) 20(1):147. doi: 10.1186/s12885-020-6569-1
12. Heinze G, Dunkler D. Five Myths About Variable Selection. Transplant Int Off J Eur Soc Organ Transplant (2017) 30(1):6–10. doi: 10.1111/tri.12895
13. Yoo H, Jung E, Gwak HS, Shin SH, Lee SH. Surgical Outcomes of Hemorrhagic Metastatic Brain Tumors. Cancer Res Treat (2011) 43(2):102–7. doi: 10.4143/crt.2011.43.2.102
14. Bauer-Nilsen K, Trifiletti DM, Chatrath A, Ruiz-Garcia H, Marchan E, Peterson J, et al. Stereotactic Radiosurgery for Brain Metastases From Malignant Melanoma and the Impact of Hemorrhagic Metastases. J Neuro-Oncol (2018) 140(1):83–8. doi: 10.1007/s11060-018-2933-2
15. Lagerwaard FJ, Levendag PC, Nowak PJ, Eijkenboom WM, Hanssens PE, Schmitz PI. Identification of Prognostic Factors in Patients With Brain Metastases: A Review of 1292 Patients. Int J Radiat Oncol Biol Phys (1999) 43(4):795–803. doi: 10.1016/s0360-3016(98)00442-8
16. Heimann M, Schäfer N, Bode C, Borger V, Eichhorn L, Giordano FA, et al. Outcome of Elderly Patients With Surgically Treated Brain Metastases. Front Oncol (2021) 11:713965. doi: 10.3389/fonc.2021.713965
17. Ilic I, Faron A, Heimann M, Potthoff AL, Schäfer N, Bode C, et al. Combined Assessment of Preoperative Frailty and Sarcopenia Allows the Prediction of Overall Survival in Patients With Lung Cancer (NSCLC) and Surgically Treated Brain Metastasis. Cancers (2021) 13(13). doi: 10.3390/cancers13133353
18. Schuss P, Schäfer N, Bode C, Borger V, Eichhorn L, Giordano FA, et al. The Impact of Prolonged Mechanical Ventilation on Overall Survival in Patients With Surgically Treated Brain Metastases. Front Oncol (2021) 11:658949. doi: 10.3389/fonc.2021.658949
19. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A New Method of Classifying Prognostic Comorbidity in Longitudinal Studies: Development and Validation. J Chronic Dis (1987) 40(5):373–83. doi: 10.1016/0021-9681(87)90171-8
20. Mantia C, Zwicker JI. Anticoagulation in the Setting of Primary and Metastatic Brain Tumors. Cancer Treat Res (2019) 179:179–89. doi: 10.1007/978-3-030-20315-3_12
21. Weinstock MJ, Uhlmann EJ, Zwicker JI. Intracranial Hemorrhage in Cancer Patients Treated With Anticoagulation. Thromb Res (2016) 140 Suppl 1:S60–65. doi: 10.1016/S0049-3848(16)30100-1
22. Reddy VU, Suneetha P, Shanthi V, Murali Mohan KV, Agrawal A. Intracranial Hemorrhagic Metastases as the First Manifestation of an Occult Melanoma. South Asian J Cancer (2015) 4(2):101–2. doi: 10.4103/2278-330X.155705
Keywords: hemorrhage, brain metastases, overall survival, hemorrhagic transformation, cranial surgery
Citation: Hamed M, Schäfer N, Bode C, Borger V, Potthoff A-L, Eichhorn L, Giordano FA, Güresir E, Heimann M, Ko Y-D, Landsberg J, Lehmann F, Radbruch A, Scharnböck E, Schaub C, Schwab KS, Weller J, Herrlinger U, Vatter H, Schuss P and Schneider M (2021) Preoperative Metastatic Brain Tumor-Associated Intracerebral Hemorrhage Is Associated With Dismal Prognosis. Front. Oncol. 11:699860. doi: 10.3389/fonc.2021.699860
Received: 09 June 2021; Accepted: 24 August 2021;
Published: 14 September 2021.
Edited by:
Christine Marosi, Medical University of Vienna, AustriaReviewed by:
Philippe Metellus, Hôpital privé Clairval, FranceYubo Wang, First Affiliated Hospital of Jilin University, China
Copyright © 2021 Hamed, Schäfer, Bode, Borger, Potthoff, Eichhorn, Giordano, Güresir, Heimann, Ko, Landsberg, Lehmann, Radbruch, Scharnböck, Schaub, Schwab, Weller, Herrlinger, Vatter, Schuss and Schneider. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Motaz Hamed, bW90YXouaGFtZWRAdWtib25uLmRl
†These authors have contributed equally to this work