 Dandan Yang
Dandan Yang Hongsheng Dai1†
Hongsheng Dai1† Jiayi Zhang
Jiayi Zhang Ming Shan
Ming Shan
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr. , 03 March 2025
Sec. Nutritional Epidemiology
Volume 12 - 2025 | https://doi.org/10.3389/fnut.2025.1557751
Background: Metabolic dysfunction-associated steatotic liver disease (MASLD) is one of the most widespread chronic liver diseases and a serious global public health problem. Further research to identify novel risk factors associated with MASLD is urgently needed. The non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR) was identified as a novel lipid marker. The objective of this research was to assess the association between NHHR and MASLD in adults.
Methods: This cross-sectional study utilized data from the 2017–2020 National Health and Nutrition Examination Survey (NHANES). MASLD was diagnosed in accordance with controlled attenuation parameter scores and a combination of cardiometabolic risk factors. Multivariate logistic regression analyses, in conjunction with the restricted cubic spline method, were employed to investigate the association between NHHR and MASLD risk. Furthermore, subgroup and interaction analyses were conducted.
Results: This study included 5,269 individuals, with 2,031 individuals diagnosed with MASLD and 3,238 without MASLD. Logistic regression analyses revealed a significant positive correlation between NHHR and MASLD. After the confounding factors were adjusted, each unit rise in NHHR was correlated with a 39% higher probability of MASLD (OR = 1.39, 95% CI: 1.13–1.69). Subgroup and interaction analyses revealed that the positive correlation between NHHR and MASLD held steady regardless of age, gender, race, poverty-to-income ratio, education level, physical activity, body mass index, diabetes, hypertension, dyslipidemia and smoking status (P for interaction >0.05). In addition, a non-linear relationship with an S-shaped manner between NHHR and MASLD was found, with an inflection point at 1.59.
Conclusion: Our findings imply that an increasing trend in NHHR is associated with a greater risk of MASLD development. NHHR has the potential to function as an indicator for estimating the likelihood of developing MASLD.
Metabolic dysfunction-associated steatotic liver disease (MASLD), once named non-alcoholic fatty liver disease (NAFLD), represents one of the most widespread chronic liver diseases and constitutes a significant global public health concern (1, 2). MASLD is predominantly distinguished by diffuse hepatocellular steatosis which is engendered by causes apart from alcohol and other identified liver injuries, and it is correlated with an elevated risk of liver-specific complications as well as a variety of extrahepatic diseases (3). Compared with NAFLD, MASLD is defined by more stringent criteria, including hepatic steatosis and at least one indicator of cardiometabolic dysfunction (4). Individuals meeting the diagnostic criteria for MASLD are older and at greater risk of death in contrast to those diagnosed with NAFLD, which may be attributed to cardiometabolic risk factors (4). Approximately 32% of adults in the U.S. are diagnosed with MASLD, indicating its significant prevalence (5). Owing to the epidemics of diabetes and obesity, its prevalence is expected to increase even more (6). Therefore, further research is needed to identify novel risk factors implicated in this disease. This might enable a more comprehensive understanding of the approaches for identifying high-risk individuals and formulating efficient prevention strategies.
Dyslipidemia has been found to be strongly associated with MASLD (7), with abnormal hepatic lipid alterations and dysfunctional lipoprotein metabolism being a predominant factor contributing to the elevated cardiovascular disease (CVD) risk among individuals with MASLD (8). Non-high-density lipoprotein cholesterol (non-HDL-c) encompasses all of the cholesterol that is potentially capable of inducing atherosclerosis and is contained within different types of lipoprotein particles like lipoprotein (a), low-density lipoprotein cholesterol (LDL-c), triglyceride-rich lipoproteins (TRLs), and TRL-remnants (9). Meanwhile, high-density lipoprotein cholesterol (HDL-c), present in the densest lipoprotein particles, protects against atherosclerosis (10). In individuals with MASLD, dyslipidemia typically manifests as heightened concentrations of triglyceride (TG) and LDL-c, along with diminished HDL-c levels, all of which are independently correlated with the incidence and/or mortality of CVD (7). In recent years, the non-HDL-c to HDL-c ratio (NHHR) has been progressively deemed as a novel index for assessing the risk of atherosclerosis and CVD (11, 12). It takes into account two aspects, non-HDL-c and HDL-c, and avoids the drawbacks of previous studies that were exclusive to lipids; moreover, its predictive ability has been shown to outperform that of conventional lipid indicators (13, 14). Studies have revealed that NHHR is not only efficient in evaluating the severity of atherosclerosis, but also shows a substantial correlation and predictive value for a wide variety of diseases. For example, a study carried out by Wang et al. (14) demonstrated that NHHR was significantly correlated with an elevated risk of developing hyperuricemia, accompanied by a U-shaped relationship between them. In addition, an investigation focusing on a sample characteristic of the U.S. adult population highlighted a positive correlation between NHHR and type 2 diabetes, with an 8% increase in the probability of contracting type 2 diabetes for every single-unit rise in NHHR (15). Additionally, emerging investigations have demonstrated that NHHR could be utilized as a predictive indicator for conditions like non-alcoholic steatohepatitis and metabolic syndrome, indicating that it may function as an effective and valuable tool in the prediction of diseases associated with metabolism (16, 17).
Subsequent to the introduction of the new naming system for NAFLD, the connection between the NHHR index and MASLD remains indistinct. Therefore, our study employed the National Health and Nutrition Examination Survey (NHANES) 2017–2020 dataset to conduct a cross-sectional study, aiming to explore the correlation between NHHR and MASLD by means of a more accurate and efficacious methodology.
This research capitalized on the data from the NHANES, which stands as a comprehensive database that sampling the non-institutionalized population across the U.S. biennially. This database extensively investigates the health conditions of U.S. population through questionnaires, laboratory tests, and physical examinations. The research protocol has garnered the endorsement of the Ethics Review Committee of the National Center for Health Statistics, and every subject provided informed consent.
The participants in the present research were selected from the NHANES database from 2017 to 2020, as from 2017, the NHANES first introduced vibration-controlled transient elastography to appraise liver steatosis through the measurement of controlled attenuation parameter (CAP). Initially, 15,560 candidates were included, and the exclusion criteria detailed below were implemented to determine the final study population: (a) age younger than 20 years; (b) insufficient data for the assessment of NHHR; (c) no liver elastography examination; (d) absent data on covariates covering gender, age, race, education level and poverty income ratio (PIR); (e) liver disease or heavy alcohol consumption or iron overload (ferritin ≥1,000 ng/mL); and (f) pregnant. After screening, 5,269 subjects were ultimately included in this research (Figure 1).
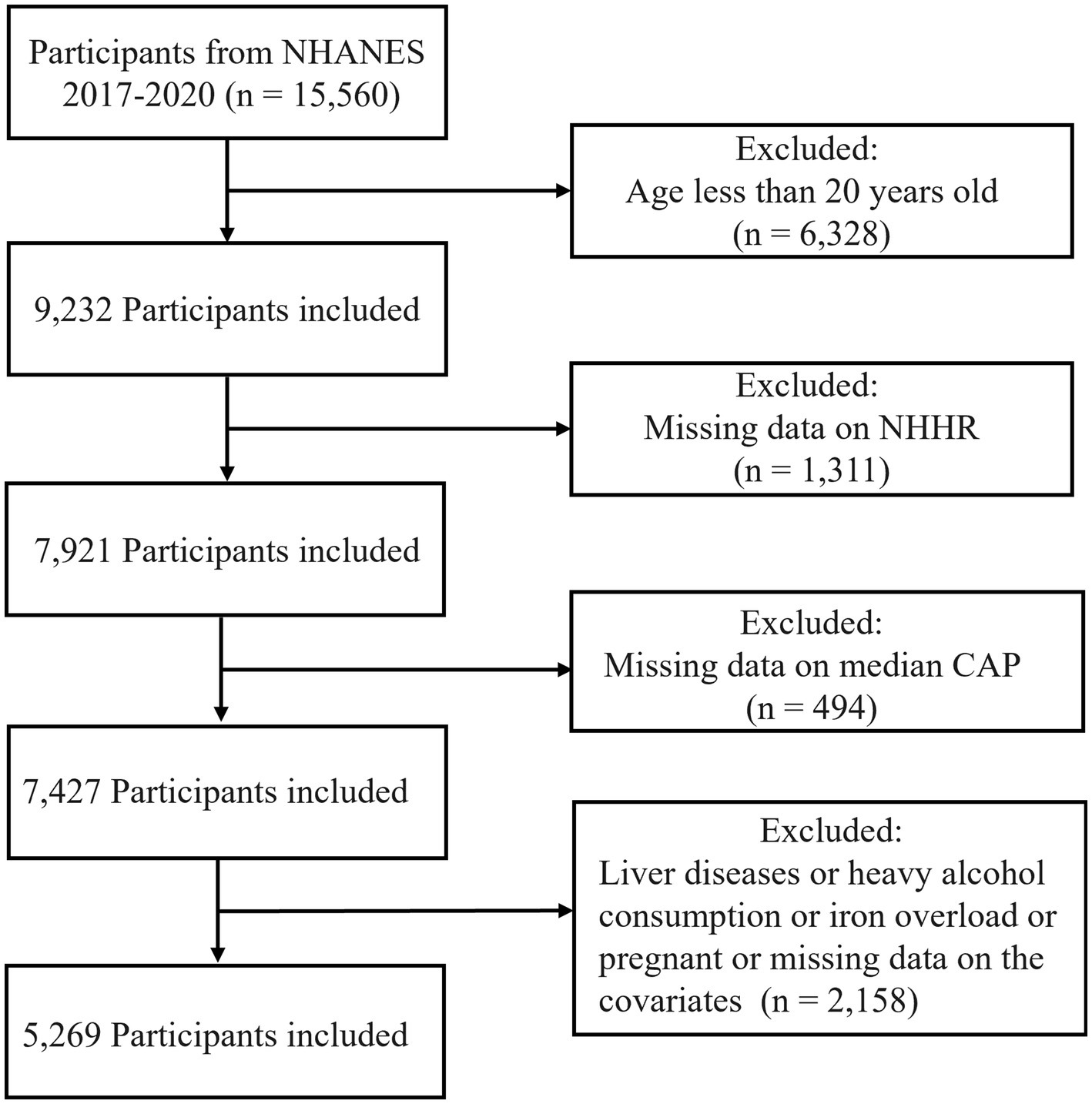
Figure 1. Flowchart of the subject screening process from NHANES 2017 to 2020.
In this research the NHHR calculated from the lipid levels of the fasting subjects was used as the exposure variable. As previously described in literature (15, 18), NHHR is the ratio of non-HDL-c to HDL-c. Non-HDL-c equals total cholesterol (TC) minus HDL-c. In the subsequent statistical analysis, the NHHR values of all participants in the sample were ranked in ascending order and divided into four groups based on quartile: Q1 (below 1.91), Q2 (between 1.91 and 2.59), Q3 (between 2.59 and 3.48), and Q4 (above 3.48) to facilitate more detailed analysis.
The diagnostic criteria for MASLD was a median CAP score ≥ 285 dB/m and a combination of at least one of the five cardiometabolic risk factors detailed below (19, 20): (a) body mass index (BMI) ≥ 25 kg/m2 or waist circumference ≥ 80 cm for females and >94 cm for males; (b) clinically diagnosed diabetes or current use of diabetes management medications or fasting glucose ≥100 mg/dL or 2-h postload glucose levels ≥140 mg/dL or hemoglobin A1c (HbA1c) ≥ 5.7%; (c) blood pressure ≥ 130/85 mmHg or in hypertensive management; (d) plasma TG ≥ 150 mg/dL or on lipid-lowering therapy; and (e) plasma HDL-c ≤ 50 mg/dL for females and ≤40 mg/dL for males.
To explore the correlation between NHHR and MASLD, we considered a variety of possible covariates, covering age, gender, race, education level, PIR, physical activity, BMI, smoking status, diabetes, hypertension and dyslipidemia. Information on demographic characteristics was collected through standardized household interviews. In accordance with previous literatures (21, 22), physical activity was categorized as no (no reported leisure-time activity), moderate (activities trigger a rise in heart rate or respiration lasting at least 10 min per week), or vigorous (individuals engaging in high-intensity exercise than described above). For smoking status, never smokers were defined as individuals whose cumulative cigarette consumption was under 100, current smokers referred to those with a smoking history exceeding 100 cigarettes and continued smoking, and former smokers were those who had quit smoking. Data on diabetes, hypertension and dyslipidemia status were obtained from self-report surveys.
The NHANES sample weights were incorporated into all analyses to address the intricacies of tiered cluster surveys. Initial normality assessment via the Kolmogorov–Smirnov test confirmed that all continuous variables exhibited non-normal distributions (Supplementary Figure S1). Therefore, continuous variables were presented as weighted medians (interquartile ranges, IQRs), and categorical variables were exhibited as sample sizes along with weighted percentages (%). The distinctions between the non-MASLD and MASLD cohorts were evaluated by chi-square test for categorical variables and Wilcoxon rank-sum test for continuous variables. The relationship between NHHR and MASLD was accessed utilizing multivariable logistic regression models. The variance inflation factor was subsequently used to identify multicollinearity in regression analyses. The NHHR was stratified into quartiles, and individuals in the lowest quartile were categorized into the reference group. In addition, a restricted cubic spline (RCS) regression model was utilized to explore the relationship between NHHR and the incidence of MASLD. Receiver operating characteristic (ROC) curve analysis was employed to evaluate the effectiveness of using TC, non-HDL-c, LDL-c, HDL-c, and NHHR in assessing the risk of MASLD development. Finally, we stratified the subjects according to various covariates and then performed interaction tests to explore whether there was a variation in the relationship between NHHR and MASLD among these subgroups. In this study, all the analytical procedures were carried out with the utilization of R software, and a p-value (two-sided) < 0.05 was recognized statistically significant.
As illustrated in Table 1, this research incorporated totally 5,269 participants with a median age of 48 years, which contained 52.0% female and 48.0% male. Among all participants, 2,031 were identified as MASLD-suspected cases with a median NHHR value of 3.11 (2.38, 3.95), and 3,238 lacked fulfillments of the diagnostic criteria for MASLD with a median NHHR value of 2.30 (1.71, 3.04). All the demographic and clinical traits of both the MASLD cohort and non-MASLD cohort are presented in Table 1. Compared with those in the non-MASLD cohort, individuals in the MASLD cohort tended to be older, male, have lower education levels, less physical activity, and a relatively greater occurrence rate of former smoking habits, and there were more people with diabetes, hypertension and dyslipidemia in the MASLD cohort. Additionally, individuals in the MASLD cohort exhibited increased BMI, CAP, TG, TC and non-HDL-c concentrations, and lower HDL-c levels.
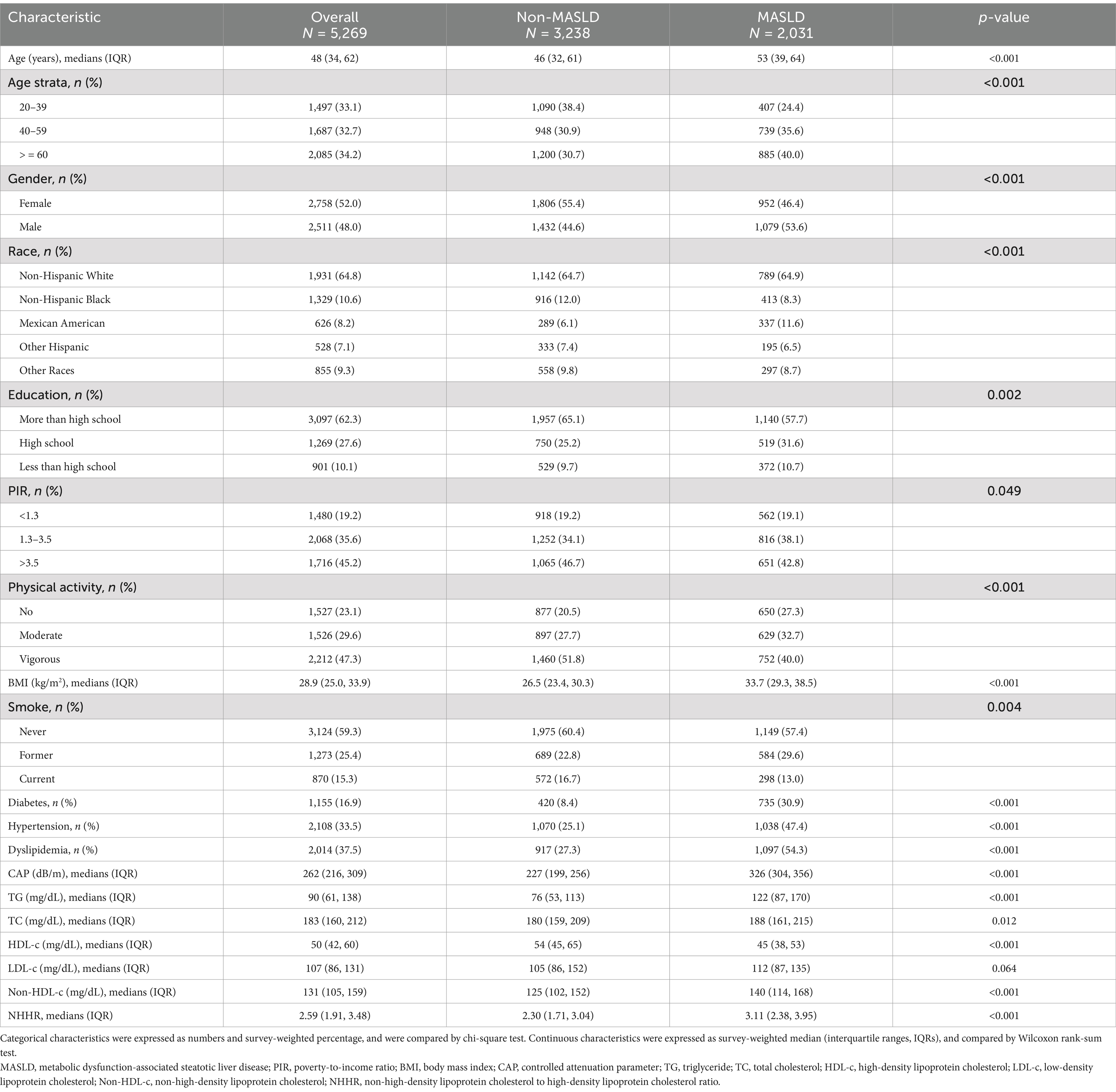
Table 1. Baseline characteristics of participants in the NHANES 2017–2020.
The correlation between NHHR and MASLD is shown in Table 2. When NHHR was regarded as a continuous variable, a positive association was found between it and the likelihood of developing MASLD. This correlative relationship held statistical significance across the logistic regression models without adjustment, with initial adjustment, and with full adjustment. Analysis with an unadjusted model indicated that for every single unit increase in NHHR, there was a corresponding 66% elevation in MASLD risk (OR = 1.66, 95% CI: 1.46–1.89, p < 0.001). After adjusting for covariates including age, gender, race, education level, PIR, physical activity, smoking status, BMI, diabetes, and hypertension, an increase of 39% in the prevalence of MASLD was found for each unitary increase in NHHR (OR = 1.39, 95% CI: 1.13–1.69, p = 0.006). In the comprehensively calibrated Model 3, in contrast to the subjects in the lowest quartile of NHHR, those in the third quartile (OR = 2.35, 95% CI: 1.55–3.54, p = 0.003) and the highest quartile (OR = 3.15, 95% CI: 2.07–4.80, p = 0.001) exhibited a notably higher risk of contracting MASLD. As shown in Figure 2, the results of the smoothed curve fitting demonstrate an S-shaped association between NHHR and the probability of contracting MASLD among the population (P for overall <0.001). Moreover, there was also evidence of non-linearity between NHHR and MASLD risk, as evidenced by a p-value for non-linearity less than 0.001. The correlation between NHHR and MASLD showed an inflection point when NHHR reached 1.59, and to the left of the inflection point, the likelihood of developing MASLD tended to decrease as NHHR increased. According to the results of the ROC curve analysis, the areas under the curve (AUCs) for NHHR, HDL-c, non-HDL-c, TC and LDL-c were 67.73, 66.56, 59.27, 52.61 and 52.12%, respectively (Figure 3).
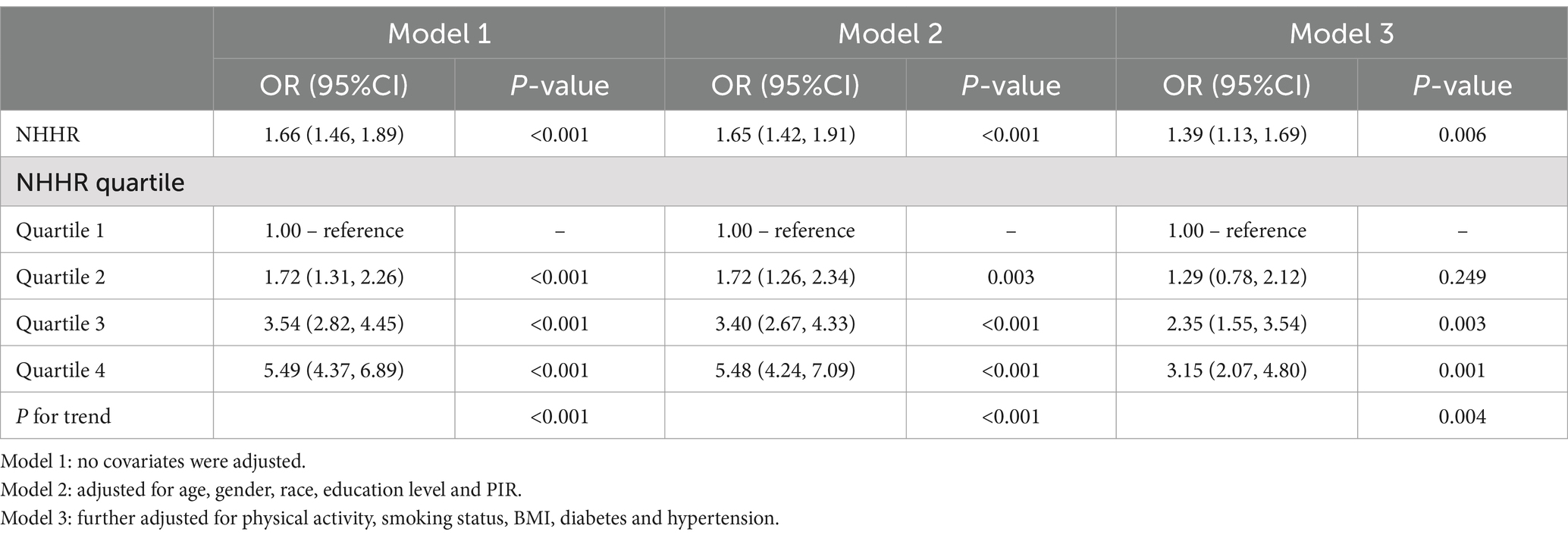
Table 2. The association between NHHR and MASLD (weighted).
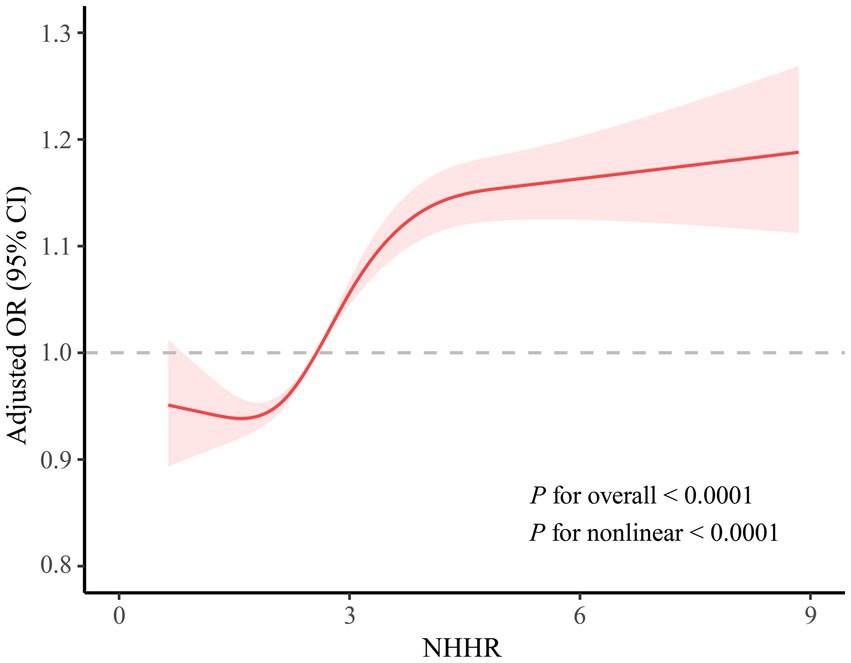
Figure 2. Non-linear relationships between NHHR and MASLD.
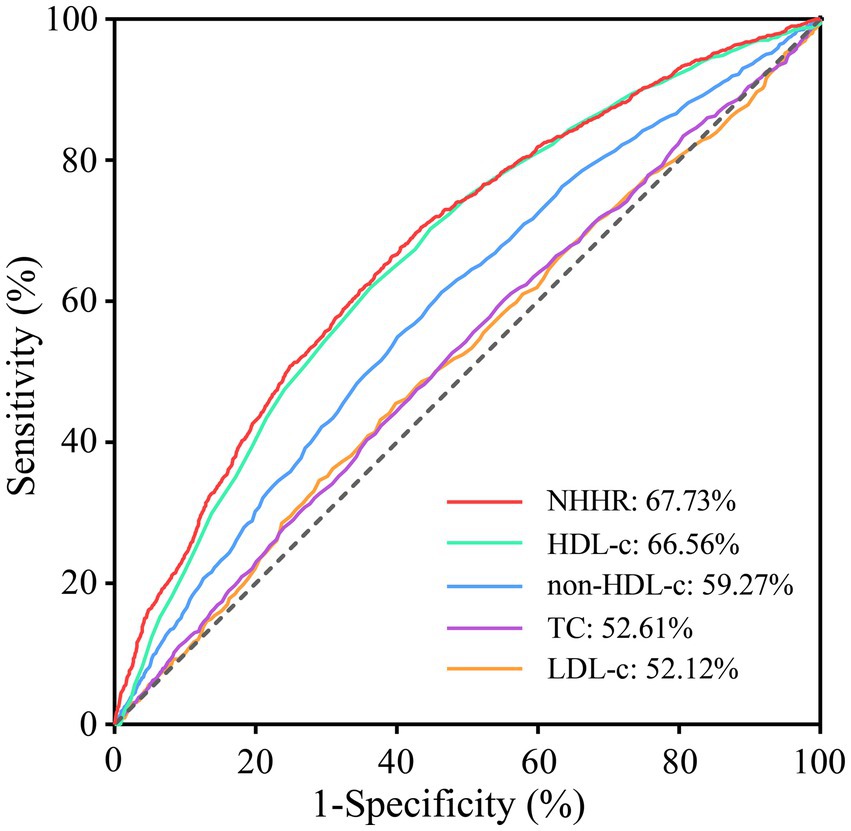
Figure 3. Receiver operating characteristic (ROC) curves for detecting MASLD.
Taking into account all factors, subgroup analyses were performed to assess the reliability of the relationship between NHHR and MASLD risk within diverse populations, and the results are illustrated in Figure 4. No significant interactions were detected among age, gender, race, PIR, education level, physical activity, BMI, smoking status, diabetes, hypertension and dyslipidemia, indicating that the positive correlation between NHHR and MASLD remained unaffected by these variables (P for interaction >0.05). Among these, strong association was identified in participants aged 40–59 years (OR = 1.44, 95% CI: 1.21–1.70) as well as those older than 60 years (OR = 1.52, 95% CI: 1.28–1.80). Notably significant correlations were also detected among Non-Hispanic Black individuals OR = 1.30, 95% CI: 1.14–1.49), Non-Hispanic White individuals (OR = 1.56, 95% CI: 1.37–1.78), and other races (OR = 1.63, 95% CI: 1.34–1.99). Individuals with lower-income (OR = 1.48, 95% CI: 1.27–1.71) and middle-income (OR = 1.49, 95% CI: 1.30–1.71) levels demonstrated meaningful correlations. Lifestyles of no daily activity (OR = 1.43, 95% CI: 1.17–1.75) and moderate physical activity (OR = 1.41, 95% CI: 1.16–1.73) also exhibited significant associations. In addition, significant correlations were also shown among those who had normal weight (OR = 1.84, 95% CI: 1.25–2.72), were overweight (OR = 1.35, 95% CI: 1.19–1.51), were currently smoking (OR = 1.37, 95% CI: 1.16–1.62), had a smoking history (OR = 1.68, 95% CI: 1.43–1.98), or had no dyslipidemia (OR = 1.52, 95% CI: 1.22–1.90), with p-values <0.05 for all associations.
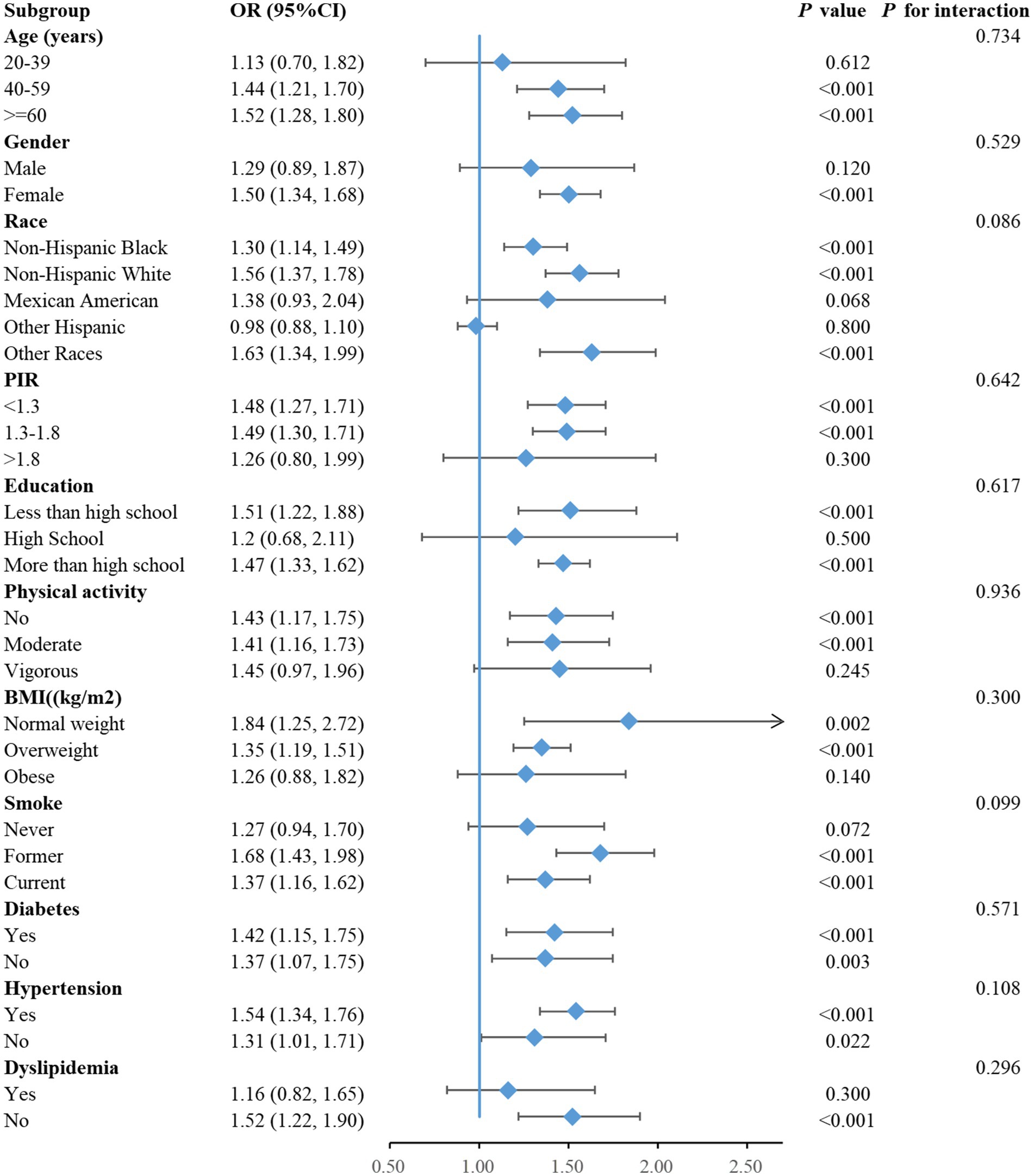
Figure 4. Forest plot of the associations of NHHR with MASLD.
The present study based on U.S. adult population investigated the association between NHHR and the probability of MASLD development. The present research demonstrated that individuals without MASLD possessed a considerably lower NHHR values than did those diagnosed with MASLD. Moreover, multivariable regression analysis revealed that elevated NHHR levels were strongly correlated with a higher risk of MASLD. Additionally, the relationship between NHHR and MASLD exhibited a non-linear and S-shaped profile, with an inflection point at 1.59.
The NAFLD is correlated with an increased risk of intra- and extra-hepatic malignancies and constitutes the primary etiological factor for liver-related mortality worldwide (23). Recently, MASLD has gradually supplanted NAFLD on account of the increasing prevalence of metabolic syndrome and obesity, emphasizing the importance of cardiometabolic risk factors (24). MASLD represents a multisystem disorder arising from systemic insulin resistance, dyslipidemia, and associated metabolic dysfunction (3). Patients diagnosed with MASLD manifest hepatic lipid metabolism imbalance characterized by increased lipolysis within adipose tissue, high hepatic de novo lipogenesis, impaired lipid oxidation and alterations in very-low-density lipoprotein secretion, which ultimately leads to hepatic lipid accumulation (25). The accumulation of lipids within hepatocytes generally induces lipotoxicity, subsequently resulting in chronic inflammation in hepatic tissue by mediating organelle dysfunction, endoplasmic reticulum stress, oxidative stress, ferroptosis, and the activation of proinflammatory factors, further aggravating insulin resistance (26, 27). In addition, the accumulation of toxic lipid metabolites triggers hepatocellular stress, damage and death, consequently leading to fibrogenesis and DNA mutations that eventually increase susceptibility to the progression of cirrhosis and hepatocarcinoma (28, 29).
In previous studies, LDL-c has been regarded as the central target of lipid metabolism disease management, whereas non-HDL-c, which encompasses the entirety of plasma lipoprotein particles apart from HDL-c, has been recognized as an independent risk factor and prognostic indicator of CVD (30–33). Notably, the association between dyslipidemia and liver diseases has been extensively explored (8, 34). A longitudinal cohort study conducted among Japanese adults demonstrated that LDL-c and non-HDL-c showed a significant positive correlation with the risk of developing NAFLD, while HDL-c was negatively associated with NAFLD risk (35). Furthermore, a prospective cohort study encompassing 147 individuals free of liver disease with a 7-year follow-up time revealed that non-HDL-c served as an independent prognostic indicator for the initial occurrence of NAFLD, and its predictive effect was stronger than that of other lipid components, such as TC, LDL-c and HDL-c (36). This association may result from the hepatotoxicity of non-HDL-c and account for the link between CVD and NAFLD. In addition, non-HDL-c has also been demonstrated to be associated with the severity of liver disease, and among subjects not taking lipid-lowering medications, the levels of non-HDL-c in patients with non-alcoholic steatohepatitis are markedly higher than those in patients with steatosis (37). In addition, serum remnant cholesterol, one of the constituents of non-HDL-c, was also verified to be positively correlated with the risk of NAFLD, and its predictive capacity for the progression of NAFLD surpassed that of traditional lipid components (38). This correlation was significant among individuals who exhibited normal levels of HDL-c, LDL-c, and triglycerides (38).
NHHR, a newly-emerged comprehensive marker of blood lipids proposed in recent years, encompasses all pertinent information regarding anti- and pro-atherosclerotic lipid particles, reflects the equilibrium among lipoproteins, and has progressively emerged as a potential marker for metabolic disorders (15, 39). A cross-sectional study encompassing 30,482 U.S. adults demonstrated that increased NHHR levels were significantly associated with a heightened gout prevalence. After accounting for various confounding factors, such as age, gender, race, education level, and so on, it was found that for every single unit increase in NHHR, the probability of gout incidence increased by 10% (40). Furthermore, a study including 12,578 U.S. adult subjects with prediabetes or diabetes disclosed that NHHR exhibited an L-shaped connection with cardiovascular mortality and a U-shaped correlation with all-cause mortality, with inflection points of 2.83 for cardiovascular mortality and 2.72 for all-cause mortality, respectively (41). Specifically, once baseline NHHR surpassed the inflection point, NHHR was positively associated with cardiovascular and all-cause mortality among patients with prediabetes or diabetes (41). However, studies on the correlation between NHHR and the risk of developing MASLD are currently limited, so it is unclear whether NHHR can be utilized as a valid marker to predict MASLD. The present study revealed that NHHR has a greater predictive value for MASLD with an AUC of 67.73% than traditional lipid related indicators, such as TC, non-HDL-c, LDL-c and HDL-c. Similar results were also reported in studies investigating the predictive effects of NHHR and conventional lipid parameters on hyperuricemia and diabetes. A study exploring the relationship between NHHR and the prevalence of hyperuricemia in US adults revealed that compared with non-HDL and HDL-c, NHHR had a better predictive effect on hyperuricemia, with an AUC of 61.76% (14). Similarly, compared to other conventional lipid parameters, NHHR is a more effective predictor of diabetes risk and an independent risk factor for new-onset diabetes mellitus in the general population (42).
After adjustment for potential confounders other than dyslipidemia, we found that each one-unit increase in NHHR was associated with a 39% increase in the risk of developing MASLD. A previous study exploring the relationship between lipid parameters and NAFLD risk, after adjusting for potential confounders other than BMI, reported that every single unit increase in TC was accompanied by a 17% increase in NAFLD risk, every single unit increment in LDL-c was corresponded to a 29% elevation in NAFLD risk, and every single unit rise in non-HDL-c was correlated with a 36% augmentation in NAFLD risk (35). In addition, RCS regression model in this study revealed a non-linear S-shaped relationship between NHHR and MASLD risk, which was consistent with prior research exploring the relationship between NHHR and the risk of diabetes development (42). This study bridges the gaps of prior research and expands the application of lipid ratios, indicating that NHHR could serve as a predictive indicator for MASLD. Notably, the correlation between NHHR and NAFLD has also been explored in previous studies. Huang et al. demonstrated increased NHHR levels are in close correlation with an augmented risk of CAP-defined NAFLD (43). However, Huang et al. (43) did not consider cardiometabolic risk factors, which served as potentially confounding factors and significant parts of defining MASLD. In the current research, MASLD was identified according to the existence of hepatic steatosis in combination with one or more of the five cardiometabolic risk factors, thus overcoming the limitations of the research conducted by Huang et al. (43).
This research has several strengths. First, this was a large sample size population-based study, providing evidence of the correlation between NHHR and MASLD. Second, the adjustment of covariates and subgroup analysis deepened the finding of the association between NHHR and MASLD. However, some limitations should be addressed in this study. First, we could not reveal cause-effect relationship between NHHR and MASLD in our study since it was a cross-sectional design. Second, liver biopsy is a better standard clinical test than CAP value from transient elastography we measured in this study for the diagnosis of liver steatosis. Third, the patients with MASLD enrolled in this research were all obtained from the U.S. population in NHANES database, and the extrapolation of the findings to other populations demands further exploration. Therefore, more prospective investigations are essential to further validate and explore the correlation between NHHR and MASLD.
Our findings imply that a heightened NHHR is significantly correlated with a greater propensity for developing MASLD in U.S. adults. This implies that lipid management and the possible influence of NHHR on MASLD should be considered during the prevention, evaluation, and treatment procedures for this disease. It is necessary to conduct more high-quality research in the future to validate our findings.
Publicly available datasets were analyzed in this study. This data can be found at: the NHANES repository (https://www.cdc.gov/nchs/nhanes/).
The studies involving humans were approved by The National Center for Health Statistics and Ethics Review Board. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. More information can be found on the CDC website at https://www.cdc.gov/nchs/nhanes/irba98.htm.
DY: Data curation, Funding acquisition, Methodology, Software, Writing – original draft. HD: Data curation, Formal analysis, Software, Visualization, Writing – review & editing. YW: Investigation, Writing – review & editing. JZ: Validation, Writing – review & editing. MW: Validation, Writing – review & editing. MS: Funding acquisition, Methodology, Supervision, Writing – original draft. XZ: Conceptualization, Funding acquisition, Methodology, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was supported by Shandong Province Medical and Health Science and Technology Project (202407020522 and 202002050423) and the Natural Science Foundation of Shandong Province of China (ZR2020QH286 and ZR2022LSW004).
We highly appreciate the work by participants in the NHANES project.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2025.1557751/full#supplementary-material
1. Miao, L, Targher, G, Byrne, CD, Cao, YY, and Zheng, MH. Current status and future trends of the global burden of Masld. Trends Endocrinol Metab. (2024) 35:697–707. doi: 10.1016/j.tem.2024.02.007
2. Rinella, ME, Lazarus, JV, Ratziu, V, Francque, SM, Sanyal, AJ, Kanwal, F, et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. J Hepatol. (2023) 79:1542–56. doi: 10.1016/j.jhep.2023.06.003
3. Targher, G, Byrne, CD, and Tilg, H. Masld: a systemic metabolic disorder with cardiovascular and malignant complications. Gut. (2024) 73:691–702. doi: 10.1136/gutjnl-2023-330595
4. Lu, Z, Shao, W, and Song, J. The transition from Nafld to Masld and its impact on clinical practice and outcomes. J Hepatol. (2024) 81:e155–6. doi: 10.1016/j.jhep.2024.02.021
5. Kalligeros, M, Vassilopoulos, A, Vassilopoulos, S, Victor, DW, Mylonakis, E, and Noureddin, M. Prevalence of Steatotic liver disease (Masld, Metald, and Ald) in the United States: Nhanes 2017-2020. Clin Gastroenterol Hepatol. (2024) 22:1330–2.e4. doi: 10.1016/j.cgh.2023.11.003
6. Tan, Z, Wu, Y, Meng, Y, Liu, C, Deng, B, Zhen, J, et al. Trends in oxidative balance score and prevalence of metabolic dysfunction-associated Steatotic liver disease in the United States: National Health and nutrition examination survey 2001 to 2018. Nutrients. (2023) 15:4931. doi: 10.3390/nu15234931
7. Katsiki, N, Mikhailidis, DP, and Mantzoros, CS. Non-alcoholic fatty liver disease and dyslipidemia: an update. Metabolism. (2016) 65:1109–23. doi: 10.1016/j.metabol.2016.05.003
8. Deprince, A, Haas, JT, and Staels, B. Dysregulated lipid metabolism links Nafld to cardiovascular disease. Mol Metab. (2020) 42:101092. doi: 10.1016/j.molmet.2020.101092
9. Hodkinson, A, Tsimpida, D, Kontopantelis, E, Rutter, MK, Mamas, MA, and Panagioti, M. Comparative effectiveness of statins on non-high density lipoprotein cholesterol in people with diabetes and at risk of cardiovascular disease: systematic review and network Meta-analysis. BMJ. (2022) 376:e067731. doi: 10.1136/bmj-2021-067731
10. Di Bartolo, BA, Cartland, SP, Genner, S, Manuneedhi Cholan, P, Vellozzi, M, Rye, KA, et al. Hdl improves cholesterol and glucose homeostasis and reduces atherosclerosis in diabetes-associated atherosclerosis. J Diabetes Res. (2021) 2021:6668506. doi: 10.1155/2021/6668506
11. Liu, L, Liu, S, Liao, Y, Zhang, X, Wang, M, Lin, L, et al. Association of Cumulative non-High-Density Lipoprotein Cholesterol to high-density lipoprotein cholesterol ratio with the risk of Cardiometabolic disease. Front Cardiovasc Med. (2024) 11:1500025. doi: 10.3389/fcvm.2024.1500025
12. Liu, C, Zhang, Z, Meng, T, Li, C, Wang, B, and Zhang, X. Cross-sectional analysis of non-Hdl/Hdl cholesterol ratio as a marker for cardiovascular disease risk in middle-aged and older adults: evidence from the Charls study. J Stroke Cerebrovasc Dis. (2024) 34:108168. doi: 10.1016/j.jstrokecerebrovasdis.2024.108168
13. Kouvari, M, Panagiotakos, DB, Chrysohoou, C, Georgousopoulou, EN, Tousoulis, D, and Pitsavos, AC. Sex-related differences of the effect of lipoproteins and apolipoproteins on 10-year cardiovascular disease risk; insights from the Attica study (2002-2012). Molecules. (2020) 25:1506. doi: 10.3390/molecules25071506
14. Wang, Z, Wu, M, Du, R, Tang, F, Xu, M, Gu, T, et al. The relationship between non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (Nhhr) and Hyperuricaemia. Lipids Health Dis. (2024) 23:187. doi: 10.1186/s12944-024-02171-4
15. Tan, MY, Weng, L, Yang, ZH, Zhu, SX, Wu, S, and Su, JH. The association between non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio with type 2 diabetes mellitus: recent findings from Nhanes 2007-2018. Lipids Health Dis. (2024) 23:151. doi: 10.1186/s12944-024-02143-8
16. Wang, D, Wang, L, Wang, Z, Chen, S, Ni, Y, and Jiang, D. Higher non-Hdl-cholesterol to Hdl-cholesterol ratio linked with increased nonalcoholic steatohepatitis. Lipids Health Dis. (2018) 17:67. doi: 10.1186/s12944-018-0720-x
17. Kim, SW, Jee, JH, Kim, HJ, Jin, SM, Suh, S, Bae, JC, et al. Non-Hdl-cholesterol/Hdl-cholesterol is a better predictor of metabolic syndrome and insulin resistance than apolipoprotein B/apolipoprotein A1. Int J Cardiol. (2013) 168:2678–83. doi: 10.1016/j.ijcard.2013.03.027
18. Qing, G, Deng, W, Zhou, Y, Zheng, L, Wang, Y, and Wei, B. The association between non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (Nhhr) and suicidal ideation in adults: a population-based study in the United States. Lipids Health Dis. (2024) 23:17. doi: 10.1186/s12944-024-02012-4
19. Siddiqui, MS, Vuppalanchi, R, Van Natta, ML, Hallinan, E, Kowdley, KV, Abdelmalek, M, et al. Vibration-controlled transient Elastography to assess fibrosis and steatosis in patients with nonalcoholic fatty liver disease. Clin Gastroenterol Hepatol. (2019) 17:156–63.e2. doi: 10.1016/j.cgh.2018.04.043
20. Rinella, ME, Lazarus, JV, Ratziu, V, Francque, SM, Sanyal, AJ, Kanwal, F, et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. Hepatology. (2023) 78:1966–86. doi: 10.1097/hep.0000000000000520
21. Thivel, D, Tremblay, A, Genin, PM, Panahi, S, Rivière, D, and Duclos, M. Physical activity, inactivity, and sedentary behaviors: definitions and implications in occupational health. Front Public Health. (2018) 6:288. doi: 10.3389/fpubh.2018.00288
22. Guo, B, Liu, X, Si, Q, Zhang, D, Li, M, Li, X, et al. Associations of Cbc-derived inflammatory indicators with sarcopenia and mortality in adults: evidence from Nhanes 1999 ∼ 2006. BMC Geriatr. (2024) 24:432. doi: 10.1186/s12877-024-05012-2
23. Friedman, SL, Neuschwander-Tetri, BA, Rinella, M, and Sanyal, AJ. Mechanisms of Nafld development and therapeutic strategies. Nat Med. (2018) 24:908–22. doi: 10.1038/s41591-018-0104-9
24. Chan, WK, Chuah, KH, Rajaram, RB, Lim, LL, Ratnasingam, J, and Vethakkan, SR. Metabolic dysfunction-associated Steatotic liver disease (Masld): a state-of-the-art review. J Obes Metab Syndr. (2023) 32:197–213. doi: 10.7570/jomes23052
25. Carli, F, Della Pepa, G, Sabatini, S, Vidal Puig, A, and Gastaldelli, A. Lipid metabolism in Masld and mash: from mechanism to the clinic. JHEP Rep. (2024) 6:101185. doi: 10.1016/j.jhepr.2024.101185
26. Yanai, H, Adachi, H, Hakoshima, M, Iida, S, and Katsuyama, H. Metabolic-dysfunction-associated Steatotic liver disease-its pathophysiology, association with atherosclerosis and cardiovascular disease, and treatments. Int J Mol Sci. (2023) 24:15473. doi: 10.3390/ijms242015473
27. Li, Y, Yang, P, Ye, J, Xu, Q, Wu, J, and Wang, Y. Updated mechanisms of Masld pathogenesis. Lipids Health Dis. (2024) 23:117. doi: 10.1186/s12944-024-02108-x
28. Takahashi, Y, Dungubat, E, Kusano, H, and Fukusato, T. Pathology and pathogenesis of metabolic dysfunction-associated Steatotic liver disease-associated hepatic tumors. Biomedicines. (2023) 11:2761. doi: 10.3390/biomedicines11102761
29. Wang, X, Zhang, L, and Dong, B. Molecular mechanisms in Masld/mash-related Hcc. Hepatology (2024). [Epubh ahead of preprint]. doi: 10.1097/hep.0000000000000786
30. Navarese, EP, Robinson, JG, Kowalewski, M, Kolodziejczak, M, Andreotti, F, Bliden, K, et al. Association between baseline Ldl-C level and Total and cardiovascular mortality after Ldl-C lowering: a systematic review and Meta-analysis. JAMA. (2018) 319:1566–79. doi: 10.1001/jama.2018.2525
31. Raja, V, Aguiar, C, Alsayed, N, Chibber, YS, ElBadawi, H, Ezhov, M, et al. Non-Hdl-cholesterol in dyslipidemia: review of the state-of-the-art literature and outlook. Atherosclerosis. (2023) 383:117312. doi: 10.1016/j.atherosclerosis.2023.117312
32. Duerden, M, O'Flynn, N, and Qureshi, N. Cardiovascular risk assessment and lipid modification: Nice guideline. Br J Gen Pract. (2015) 65:378–80. doi: 10.3399/bjgp15X685933
33. Ning, G, Fu, X, and Xu, T. Chinese guideline on the primary prevention of cardiovascular diseases: time to start better cardiovascular primary prevention. Cardiol Discov. (2021) 1:65–7. doi: 10.1097/cd9.0000000000000024,
34. Tutunchi, H, Naeini, F, Ebrahimi-Mameghani, M, Mobasseri, M, Naghshi, S, and Ostadrahimi, A. The Association of the Steatosis Severity, Nafld fibrosis score and Fib-4 index with Atherogenic Dyslipidaemia in adult patients with Nafld: a cross-sectional study. Int J Clin Pract. (2021) 75:e14131. doi: 10.1111/ijcp.14131
35. Lu, S, Xie, Q, Kuang, M, Hu, C, Li, X, Yang, H, et al. Lipid metabolism, Bmi and the risk of nonalcoholic fatty liver disease in the general population: evidence from a mediation analysis. J Transl Med. (2023) 21:192. doi: 10.1186/s12967-023-04047-0
36. Zelber-Sagi, S, Salomone, F, Yeshua, H, Lotan, R, Webb, M, Halpern, Z, et al. Non-high-density lipoprotein cholesterol independently predicts new onset of non-alcoholic fatty liver disease. Liver Int. (2014) 34:e128–35. doi: 10.1111/liv.12318
37. Corey, KE, Lai, M, Gelrud, LG, Misdraji, J, Barlow, LL, Zheng, H, et al. Non-high-density lipoprotein cholesterol as a biomarker for nonalcoholic steatohepatitis. Clin Gastroenterol Hepatol. (2012) 10:651–6. doi: 10.1016/j.cgh.2012.01.017
38. Huang, H, Xie, J, Zeng, Y, Liu, Z, Miao, M, Xu, L, et al. Remnant cholesterol independently predicts the development of nonalcoholic fatty liver disease. J Clin Endocrinol Metab. (2023) 108:2907–15. doi: 10.1210/clinem/dgad272
39. Wang, A, Li, Y, Zhou, L, Liu, K, Li, S, Zong, C, et al. Non-Hdl-C/Hdl-C ratio is associated with carotid plaque stability in general population: a cross-sectional study. Front Neurol. (2022) 13:875134. doi: 10.3389/fneur.2022.875134
40. Guo, X, Chu, H, Xu, H, Wang, S, He, J, and Wang, Y. Association of non-high-density lipoprotein cholesterol-to-high-density lipoprotein cholesterol ratio (Nhhr) with gout prevalence: a cross-sectional study. Front Nutr. (2024) 11:1480689. doi: 10.3389/fnut.2024.1480689
41. Yu, B, Li, M, Yu, Z, Zheng, T, Feng, X, Gao, A, et al. The non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (Nhhr) as a predictor of all-cause and cardiovascular mortality in us adults with diabetes or prediabetes: NHANES 1999-2018. BMC Med. (2024) 22:317. doi: 10.1186/s12916-024-03536-3
42. Sheng, G, Liu, D, Kuang, M, Zhong, Y, Zhang, S, and Zou, Y. Utility of non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio in evaluating incident diabetes risk. Diabetes Metab Syndr Obes. (2022) 15:1677–86. doi: 10.2147/dmso.S355980
43. Huang, X, Li, J, Zhang, L, Zhang, C, and Li, C. The association between the non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio and non-alcoholic fatty liver disease in us adults: a cross-sectional study. Sci Rep. (2024) 14:24847. doi: 10.1038/s41598-024-76002-y
Keywords: MASLD, NHHR, NHANES, dyslipidemia, cross-sectional study
Citation: Yang D, Dai H, Wang Y, Zhang J, Wei M, Shan M and Zhang X (2025) Association between the non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio and metabolic dysfunction-associated steatotic liver disease. Front. Nutr. 12:1557751. doi: 10.3389/fnut.2025.1557751
Edited by:
Rosa Casas Rodriguez, August Pi i Sunyer Biomedical Research Institute (IDIBAPS), SpainReviewed by:
Zongbiao Tan, Renmin Hospital of Wuhan University, ChinaCopyright © 2025 Yang, Dai, Wang, Zhang, Wei, Shan and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ming Shan, c2hhbm1pbmdAc2RzbXUuZWR1LmNu; Xiaoqian Zhang, MTM4NTM2OTczOTZAMTYzLmNvbQ==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.