
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr., 11 February 2025
Sec. Clinical Nutrition
Volume 12 - 2025 | https://doi.org/10.3389/fnut.2025.1474039
 Blanca Cecilia Díaz Chavarro1,2†
Blanca Cecilia Díaz Chavarro1,2† Manuel Romero-Saldaña3,4*†
Manuel Romero-Saldaña3,4*† Jorge Karim Assis Reveiz5†
Jorge Karim Assis Reveiz5† Guillermo Molina-Recio3,4†
Guillermo Molina-Recio3,4†Background: Nutritional assessment is a fundamental part of the treatment of patients hospitalized in the ICU, allowing the implementation of interventions appropriate to the identified requirements. Since the risk of malnutrition is a modifiable factor, its correct management can positively influence hospital evolution. This study aims to test the impact of the incorporation of nutritional screening and assessment on mortality and length of stay in patients hospitalized in an Intensive Care Unit in Cali, Colombia, during the years 2019 and 2021–2022.
Methods: This is a historical cohort epidemiological study where one cohort consisted of 114 patients who received a standard nutritional screening (interpretation of body mass index and its clinical impression). The other cohort of 630 patients was those exposed to screening with the Malnutrition Universal Screening Tool (MUST) scale. Hematological, clinical, and nutritional variables were considered and their relationship with adverse events, length of hospital stay, and discharge status.
Results: There were significant differences between the two cohorts (p < 0.001), with increased mortality and length of hospital stay in patients who received standard nutritional screening without MUST. Furthermore, there was a greater presence of enteral support, diarrhea, anemia, leukocytosis, and lymphopenia in this cohort.
Conclusion: Implementing the MUST screening method and specific nutritional interventions resulted in a significant improvement in patient mortality figures. In addition, the predictive mortality model revealed that emesis and leukopenia increased the probability of death.
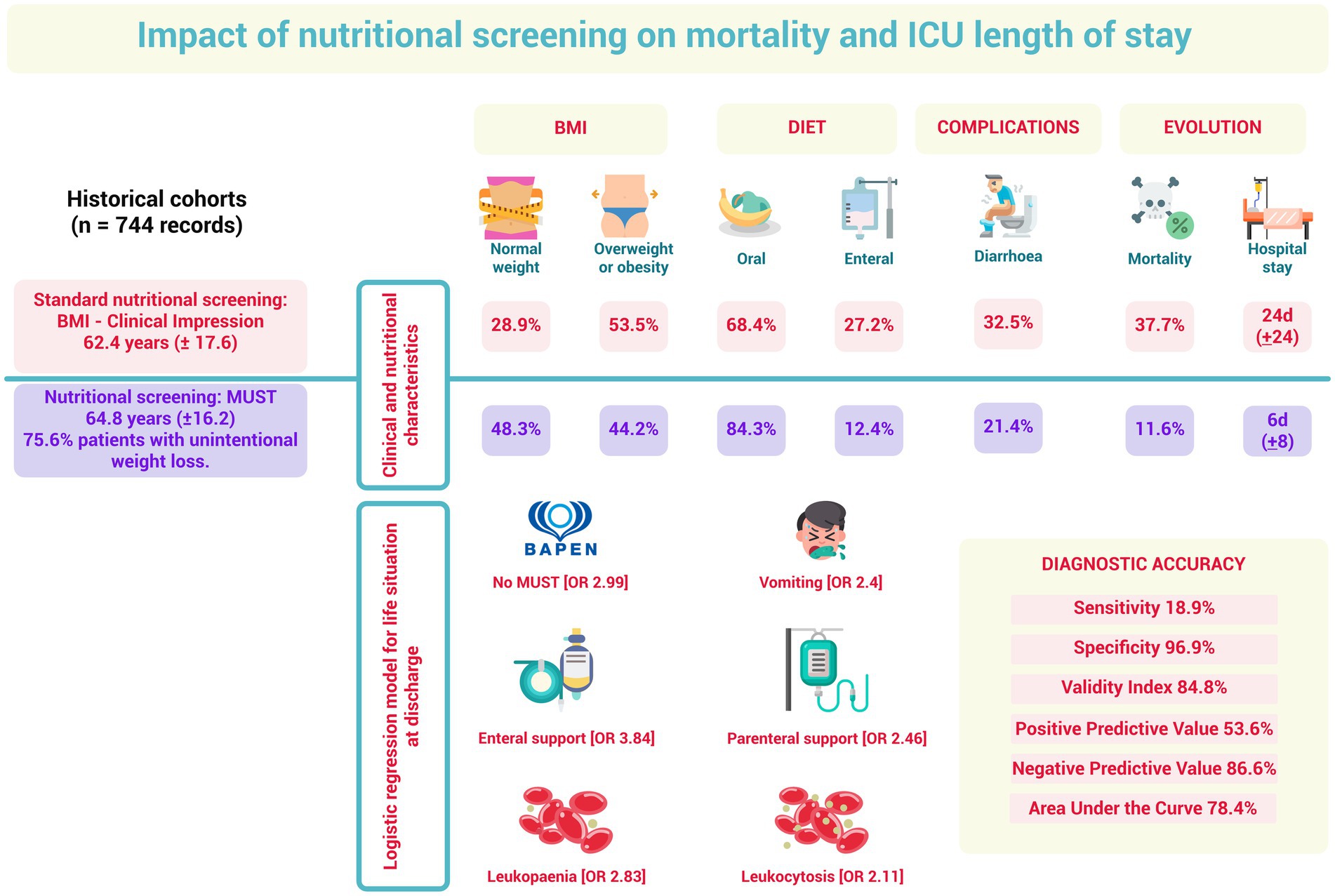
Graphical Abstract.
Disease-related malnutrition (DRE) is a complex syndrome resulting from inadequate nutrient intake (1) and the presence of a disease-related systemic inflammatory response (2), including insulin resistance, proinflammatory cytokine activity, and increased release of corticosteroids and catecholamines. This response, coupled with prolonged bed rest, results in a rapid depletion of the body’s energy and nutrient reserves (3). Other factors that may be associated with DRE syndrome include obstruction of the gastrointestinal system, malabsorption of nutrients, misassessment of the patient’s nutritional status, and inadequate administration of nutritional support (4).
From the epidemiological point of view, DRE is of great relevance, both in-hospital and in the community (5). Worldwide, it has been reported that between 30 and 55% of patients admitted to intensive care services are at risk of suffering from malnutrition. However, the percentage varies depending on the population and the criteria used for diagnosis (6). This modifiable risk generates suboptimal results, affecting the hospital course, recovery, and long-term consequences in patients (7), with longer admission time in intensive care units (ICUs) and increased mortality (8).
Therefore, nutritional assessment should be integrated as a fundamental part of the care of hospitalized patients in ICUs and as a general therapeutic strategy during their care (9). The Latin American Federation of Clinical Nutrition and Metabolic Nutritional Therapy, in a study conducted in 2012 in 47 hospitals, highlighted the need for nutritional assessment or screening to be part of the medical records and fulfilled during the first 24–48 h of care. It was reported that only 38% of records had a reference to the nutritional status of hospitalized patients, both in medical and surgical areas and in the ICU, showing a significant underreporting, which leads to a late diagnosis of nutritional risk (10).
A review of the data in Colombia reveals that only 46% of healthcare institutions providing nutrition to patients have an organized nutritional and metabolic support group. Additionally, fewer than 50% of nutritional support groups have the necessary professionals to deliver comprehensive care (11). This shortage is considered a contributing factor to malnutrition, as there is a lack of training and awareness among healthcare professionals and institutions responsible for patient care. Shortages of equipment and supplies and inadequate organizational structures further hinder the provision of care. Consequently, it is crucial to establish systems that facilitate the early identification of malnutrition, address its root causes, monitor nutritional risks, and provide timely and tailored nutritional support for each patient (12).
Moreover, an individualized assessment must be performed for nutritional therapy to be effective, which is not feasible to apply to all patients. Therefore, screening is the starting point to ensure that those who can benefit from nutritional support are identified (13) and, in this way, prevent poor prognosis and mortality associated with malnutrition (14). To carry out these activities, there must be a definition of tasks and responsibilities related to the nutritional care of patients, optimizing communication between the different professionals and hospital levels, and promoting education and continuous training in nutritional knowledge at all levels of care (13). These interventions include the application of objective variables to assess the patient’s condition and body composition, as they allow for the implementation of appropriate strategies to improve the quality of care (15).
At the clinic in Cali, Colombia, where the current investigation took place, it was found that, historically, the ICU did not use a validated scale to identify the risk of malnutrition in its patients. However, starting in 2021, the Malnutrition Universal Screening Tool (MUST) was standardized within the nutritional care protocol. This tool is valid for efficiently identifying nutritional risk in a specific patient population, is easy to use, and contains direct and objective questions, which facilitates its use in time-limited settings (16). Thus, it was possible to classify the level of nutritional risk, the type of nutritional support required for each patient and follow-up, the frequency of reassessment, and the specialist in charge of follow-up. Therefore, this study aimed to test the impact of incorporating nutritional screening and assessment of mortality and length of stay in patients hospitalized in an Intensive Care Unit in Cali, Colombia, during 2019 and 2021–2022.
A historical cohort epidemiological study was carried out. One cohort consisted of patients seen in the ICU during 2019 who received standard nutritional screening performed by the nutrition and dietetics team through the interpretation of body mass index (BMI) and their clinical impression. The other cohort of patients were those exposed to nutritional screening with the MUST scale, seen in the ICU from 2021 to 2022.
The total number of patients admitted to the adult ICU service during the study period was 4,324. The epidemiological statistical package Epidat version 4.2 was used to calculate the sample size. With a risk of DRE of 80% for patients receiving routine health care (17–19) vs. a 29.6% probability of DRE in patients undergoing nutritional screening (19), a ratio between groups equal to 1, a loss rate of 10%, a safety of 95%, a power of 90%, and applying a Yates continuity correction, a total sample of 52 patients was obtained, 26 patients per group. In any case, to ensure homogeneity in the sample, data were collected from 114 patients seen during 2019 (usual nutritional care) and from 630 patients seen during the second half of 2021 and the first half of 2022 (MUST nutritional screening), which allowed for a comparative analysis between the two cohorts, with a total of 744 patient records (Figure 1).
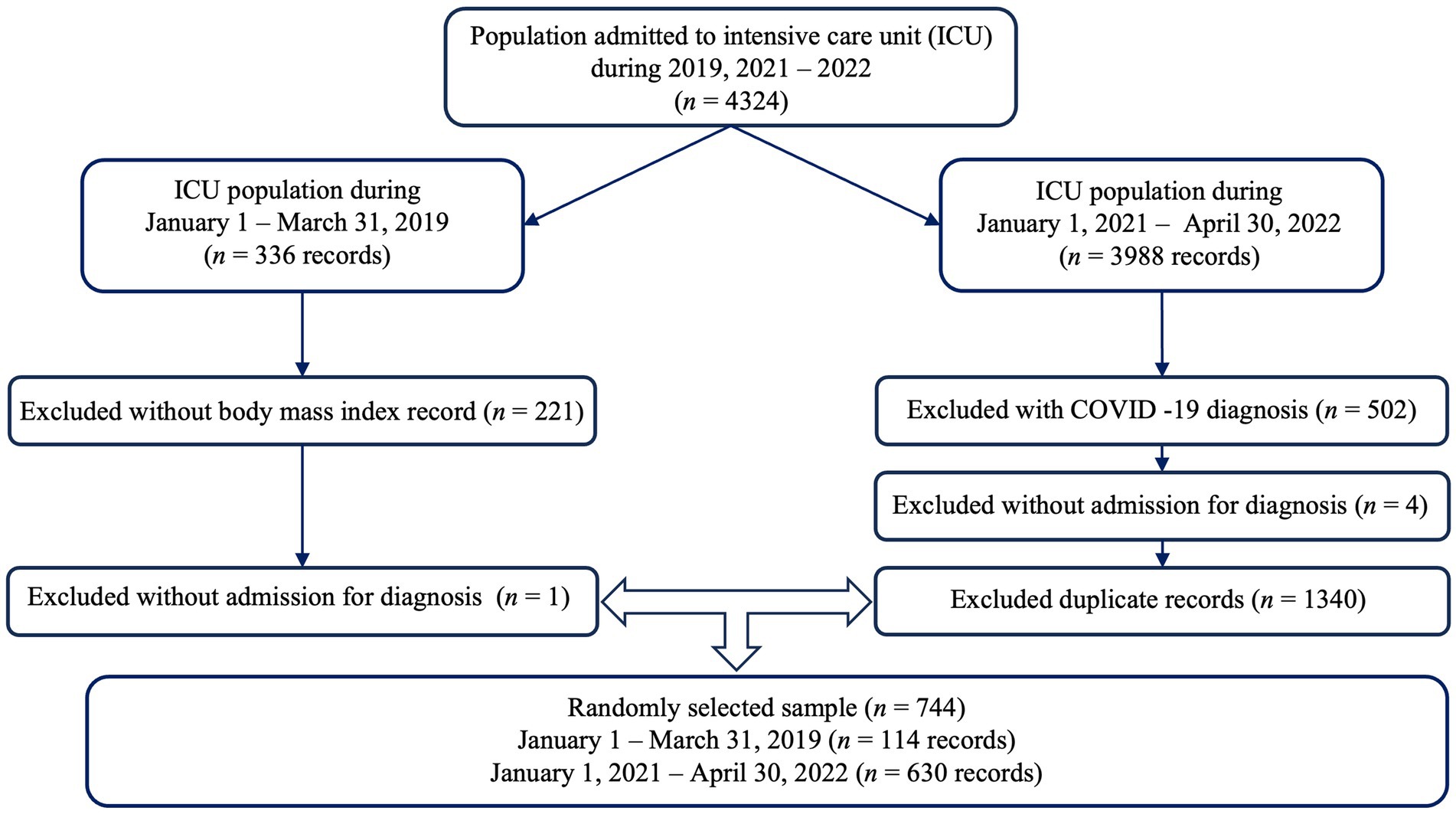
Figure 1. Diagram of sample selection.
The study’s inclusion criteria were as follows: patients seen within the ICU during 2019 to whom the MUST scale was not applied; patients admitted to the adult ICU service during the second semester of 2021 and the first semester of 2022 to whom the MUST scale was applied; and patients ˃18 years.
Patients hospitalized for COVID-19 were excluded. In addition, data from patients hospitalized during the year 2020 were omitted since a significant percentage of admissions was caused by this same pathology. This decision was made because, in this type of patient, there are some differentiating factors (reduced food intake, catabolism related to inflammation, decreased appetite, diarrhea, longer length of hospital stay, etc.) (20), which could bias the comparative results.
The following sociodemographic variables were taken into account: sex, age, and life course classification according to Resolution No. 3280 of Colombia, which identifies young people between 18 and 28 years, adults between 29 and 59 years, and older adults, those aged ≥60 years (21), and the disease of entry according to the International Classification of Diseases 11. Hematologic variables included hemoglobin levels, hematocrit percentage, leukocytes, and lymphocytes. Within the clinical variables, the presence of gastrointestinal symptoms such as hyporexia, bloating, abdominal pain, diarrhea, dysphagia, and emesis was included. Finally, nutritional variables were considered, such as the type of support received (oral feeding, enteral support, parenteral support, or mixed support) and the nutritional assessment according to MUST, which identified patients with low, medium, and high nutritional risk.
The following were considered as outcome variables: days of hospitalization, adverse events such as skin lesions associated with care dependency and healthcare-related infections (surgical site infection, urinary tract infection, pneumonia), and patient discharge status (alive or deceased).
The BMI, calculated as kg/m2, and the subjective clinical impression of nutritional status (carried out by the hospital nutrition team) were taken into account, classifying patients with a BMI <18.5 kg/m2 as underweight patients, BMI 18.5–24.9 kg/m2 as normal weight, BMI 25.0–29.9 kg/m2 as overweight, and BMI ≥30.0 kg/m2 as obese (22).
The MUST scale takes into account the analysis of three scores: (a) BMI, which is scored ≥20 kg/m2 = 0; 18.5–20 kg/m2 = 1; and ≤ 18.5 kg/m2 = 2; (b) unintentional weight loss during the past 3–6 months, calculated as a percentage and coded as follows: ≤5% = 0; 5–10% = 1; and ≥ 10% = 2; and (c) the effect of acute illness, where 2 points are assigned when there has been or is likely to be no nutritional intake for >5 days. The cumulative value of these three scores classified patients into three risk levels: 0 points = low risk; 1 point = medium risk; and ≥ 2 points = high risk (23, 24).
Those responsible for the evaluation of the nutritional status of the patients were the nutritionists of the health institution in response to the request of the ICU medical team. The frequency of the assessment depended on the level of risk identified in each patient. For low-risk patients, it was determined that the assigned physician would establish the dietary guidelines, and the screening was repeated weekly. For medium-risk patients, dietary intake was monitored for three consecutive days, and if sufficient, rescreening was performed weekly. For patients at high nutritional risk, follow-up was performed by the nutrition and dietetics unit, which established a treatment protocol and evaluation of the nutritional care plan.
Gastrointestinal symptoms were assessed by both the medical staff and the nutrition and dietetics team during the patient’s admission. This information was obtained through anamnesis with verbal reference from the patient (if the patient’s clinical condition permitted) or through information provided by the patient’s primary caregiver. This information was complemented with data from the physical assessment performed by the physician responsible for the patient in the ICU. In the case of hyporexia, it was documented from the verbal reference of the patient’s decreased appetite and oral intake.
The nutritional support collected in the study corresponds to that indicated in the patient’s clinical history, at the time of consultation with the nutrition and dietetics team. In this study, changes in the type of nutritional support were not recorded, considering that only the data from the first nutritional screening were collected, together with the results of the paraclinical tests on admission; analyzing the patient’s condition at a single moment of hospitalization, so that all the data would be related to the nutritional risk identified.
This research adhered to the international postulates for health-related research on human subjects, created by the Council for International Organizations of Medical Sciences in collaboration with the World Health Organization and the Declaration of Helsinki for the participation of human subjects in research. Approval was received from the Ethics and Bioethics Committee of the Department of Health of the University Santiago de Cali-Colombia—"CEB-USC,” in the session held on June 26, 2020, according to Minutes N° 01 and by the Scientific Technical Committee of the participating clinic, under registration IYECDO-1358 of February 11, 2021.
Statistical analysis was performed with SPSS software version 28.0. The characterization of sociodemographic factors such as life course, sex, and clinical factors such as the pathology causing hospitalization of the patients admitted to the ICU was performed by means of absolute and relative frequency tables. In addition, weight loss, global risk of malnutrition, and percentage of weight loss were determined, according to data reported in patients with MUST scale assessment.
Absolute and relative frequency analyses were performed on the nutritional factors and the interpretation of the patients’ paraclinical results, comparing the standard nutritional care cohort (2019) vs. the one seen after the implementation of the MUST scale (2021–2022), evaluating their association by means of Pearson’s chi-square test, with their respective corrections, when necessary. For the paraclinical data analyzed, the Kolmogorov–Smirnov test with Lilliefors correction was applied, finding that there was no normal distribution, so the comparison of means was performed through the Mann–Whitney U test.
A binary logistic regression model was performed for the mortality outcome, determining the adjusted OR values and the Hosmer and Lemeshow test for the goodness-of-fit of the model, as well as the Wald statistic and the Cox and Snell and Nagelkerke R2 coefficients of determination. In all cases, a statistical significance level of p < 0.05 was considered.
The sample of 744 admissions to the Intensive Care Unit in Cali, Colombia, was divided into two cohorts. The first corresponds to a standard nutritional program equivalent to 15.3% of care provided during 2019, while the rest corresponds to a nutritional program that included the MUST scale in patients seen between June 2021 and June 2022.
The diagnosis of circulatory and respiratory system pathologies was the most prevalent in both cohorts, but there were statistically significant differences (p < 0.001) related to a higher percentage of these pathologies during the 2021–2022 cohort (50% vs. 37.3%) and a higher percentage of neoplasms in patients seen during 2019 (29.8% vs. 17%). Significant associations or differences (p < 0.001) were also identified, with a mortality of 37.72% in patients seen during 2019 vs. a mortality of 11.6% in patients seen during 2021–2022 and a higher average number of days of hospital stay in patients who did not have MUST scale assessment performed within their nutritional care (24 vs. 6 days) (Table 1).
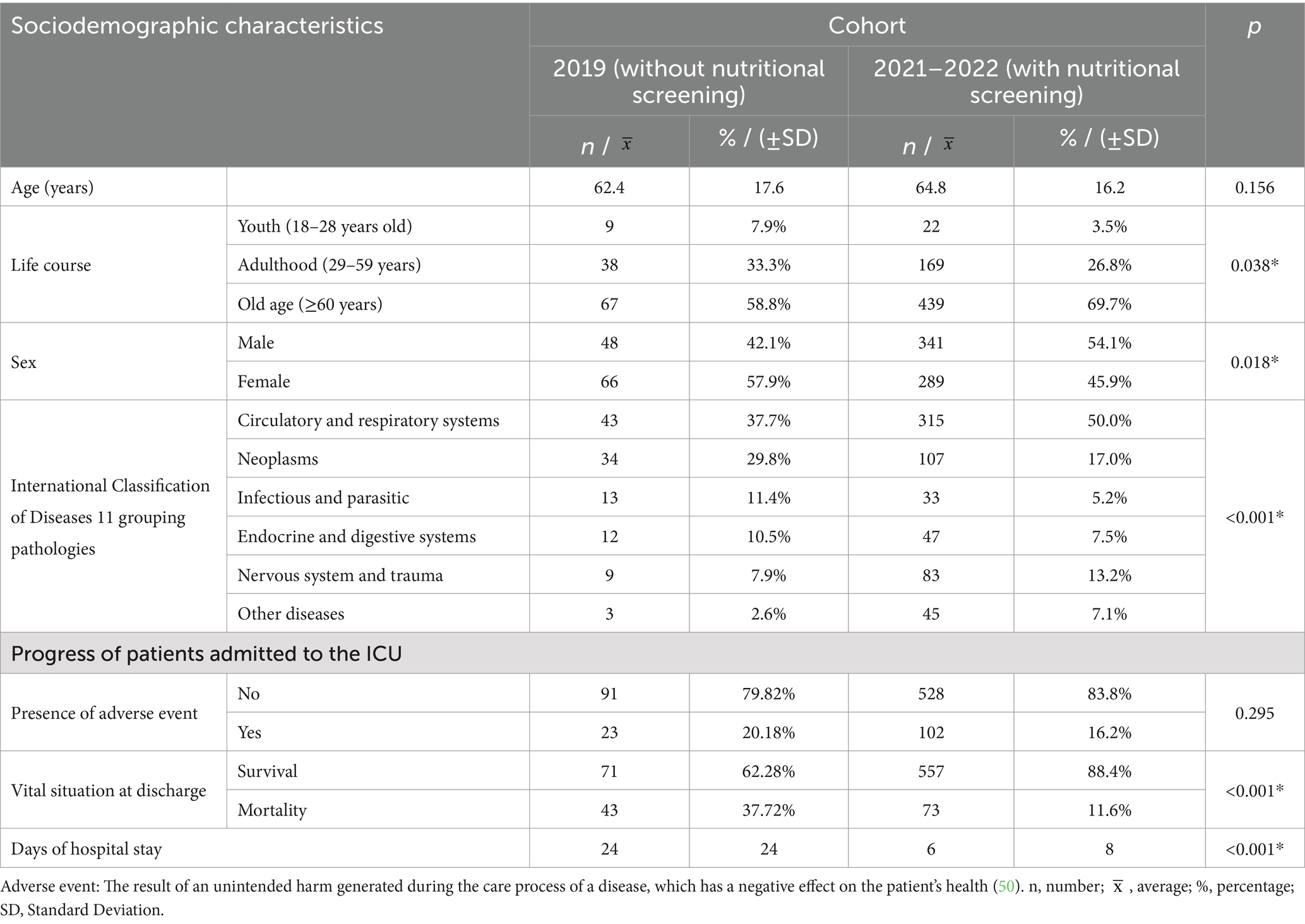
Table 1. Sociodemographic characteristics and progress of patients admitted to the intensive care unit (ICU) of the Cali, Colombia clinic during 2019 vs. 2021–2022.
The incidence rate (IR) of mortality in the 2019 cohort was 15.7 deaths per 1,000 ICU patients/day, while the IR of adverse events was 8.4 cases per 1,000 ICU patients/day. For the 2021–2022 cohort, the mortality IR was 19.1 deaths per 1,000 ICU patients/day, and the adverse event IR was 26.7 cases per 1,000 ICU patients/day.
In the cohort seen between 2021 and 2022, it was found that 3 out of 4 patients had reported unintentional weight loss during the last 6 months, with an average loss of 4.85% of body weight (standard deviation [SD] 6.20%). In determining nutritional risk according to the MUST scale, a high risk of malnutrition was reported in 28.4% (Table 2).
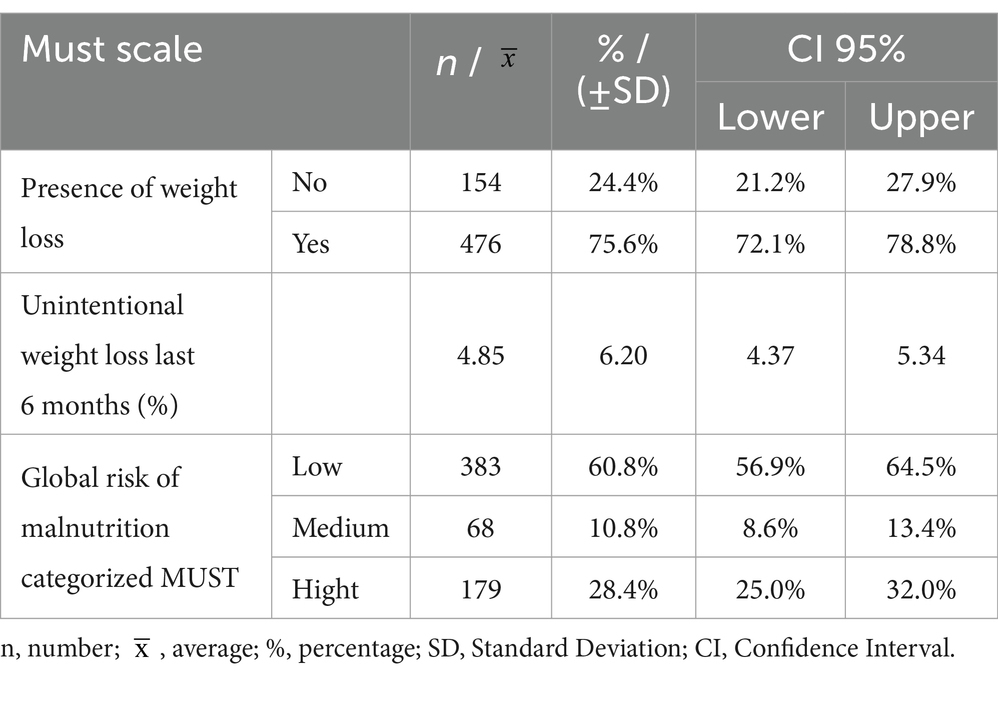
Table 2. Malnutrition universal screening tool (MUST) scale characteristics of patients admitted to the intensive care unit of the Cali, Colombia clinic during 2021–2022.
When analyzing BMI, there were statistically significant differences (p < 0.001) showing a higher percentage of patients with normal BMI in the 2021–2022 cohort (48.3% vs. 28.9%). Regarding diet, a higher use of enteral support was found in the 2019 cohort and a higher use of the oral route in patients seen between 2021 and 2022. When looking at the results related to nutritional supplementation through the addition of protein modules in the diet of patients, there were no significant statistical differences between cohorts.
For gastrointestinal symptoms, a greater presence of diarrhea was identified in the 2019 cohort, with a decrease of 11% of patients with this symptom during 2021–2022 admissions (p = 0.010). Within the alterations presented in the hematological parameters of the two cohorts, anemia was more prevalent in patients hospitalized during 2019 (74.6% vs. 62.1%; p = 0.024), and the same occurred with leukocytosis (47.4% vs. 27.9%; p < 0.001) and with lymphopenia (64.9% vs. 49.8%; p = 0.012; Table 3).
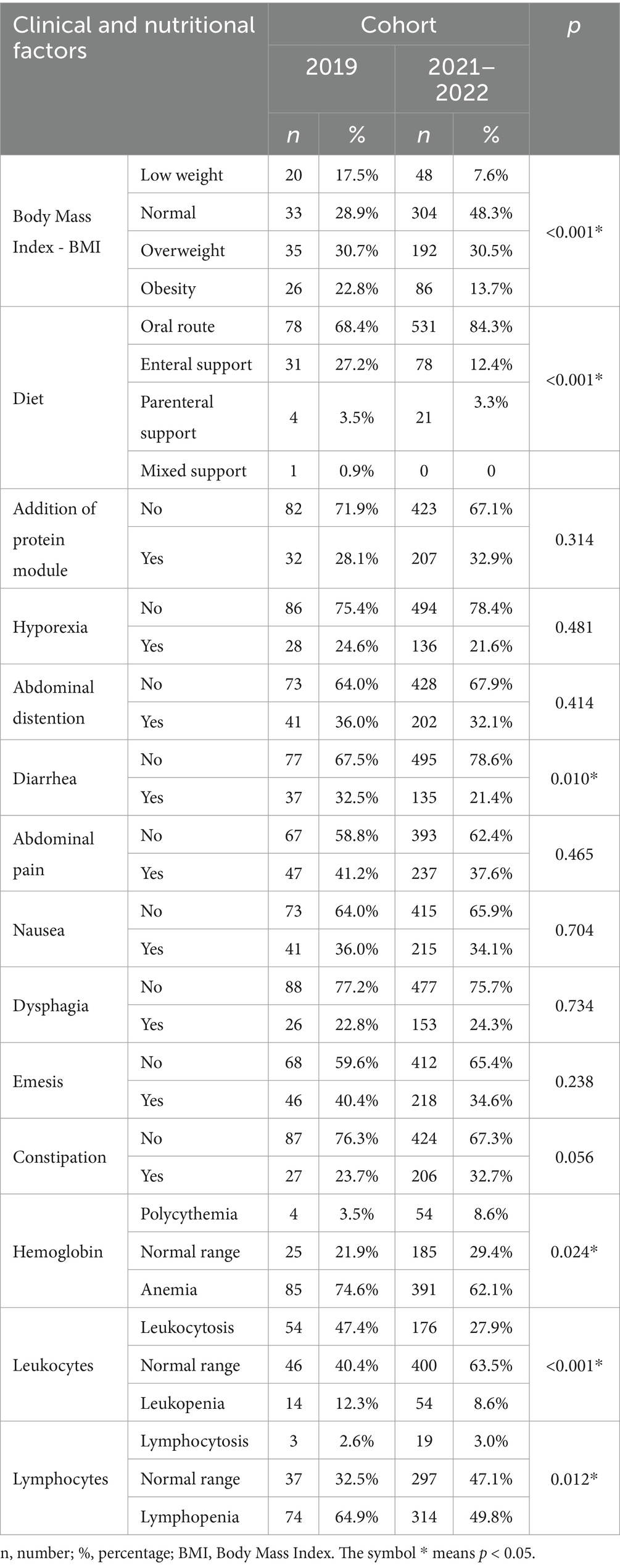
Table 3. Clinical, nutritional, and hematological characteristics of patients admitted to the intensive care unit (ICU) of the Cali, Colombia clinic during 2019 vs. 2021–2022.
In the logistic regression model for the variable “vital status at discharge,” the following predictor variables were significant: the cohort in which the patients were admitted, the type of nutritional support received, the presence of emesis, and the leukocyte levels.
In patients admitted during the 2019 period (without application of MUST screening), a nearly 3-fold increased risk for mortality was found, while in those who required parenteral nutritional support, this risk increased 2.46-fold vs. those who received oral feeding. Similarly, emesis during hospitalization and leukopenia were associated with an increased likelihood of death (2.40 [1.528–3.769] and 2.83 [1.434–5.570], respectively; Table 4).
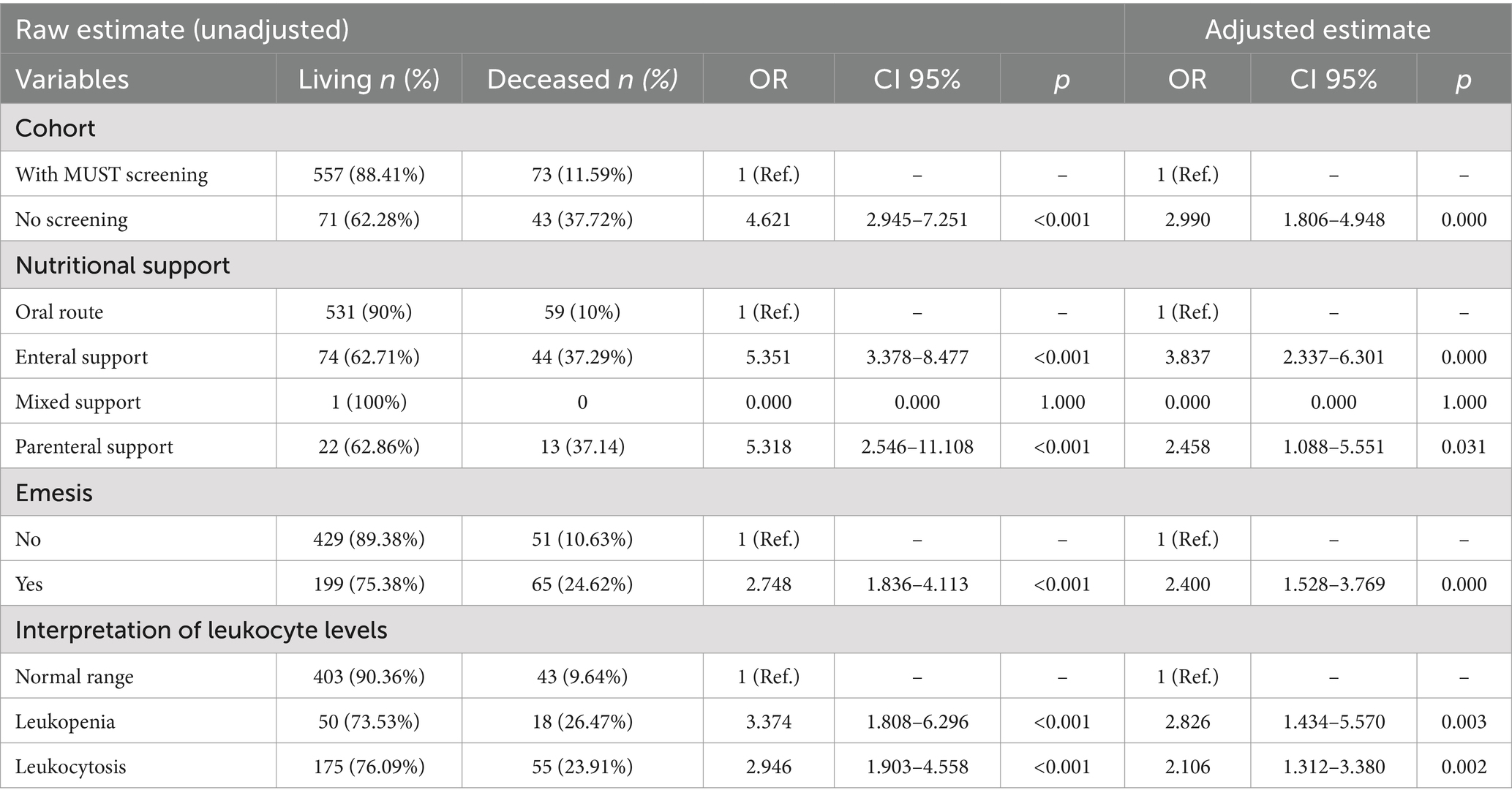
Table 4. Multivariate logistic regression model for vital status at discharge according to cohort.
When constructing an explanatory model of mortality with the final variables that remained after the adjusted estimation of the odds ratios (ORs), the omnibus test was significant (p < 0.001), and a goodness-of-fit of 0.957 was obtained, with a high specificity of 96.97%, an area under the curve (AUC) of 78.4%, and a validity index of 84.81% (Table 5).
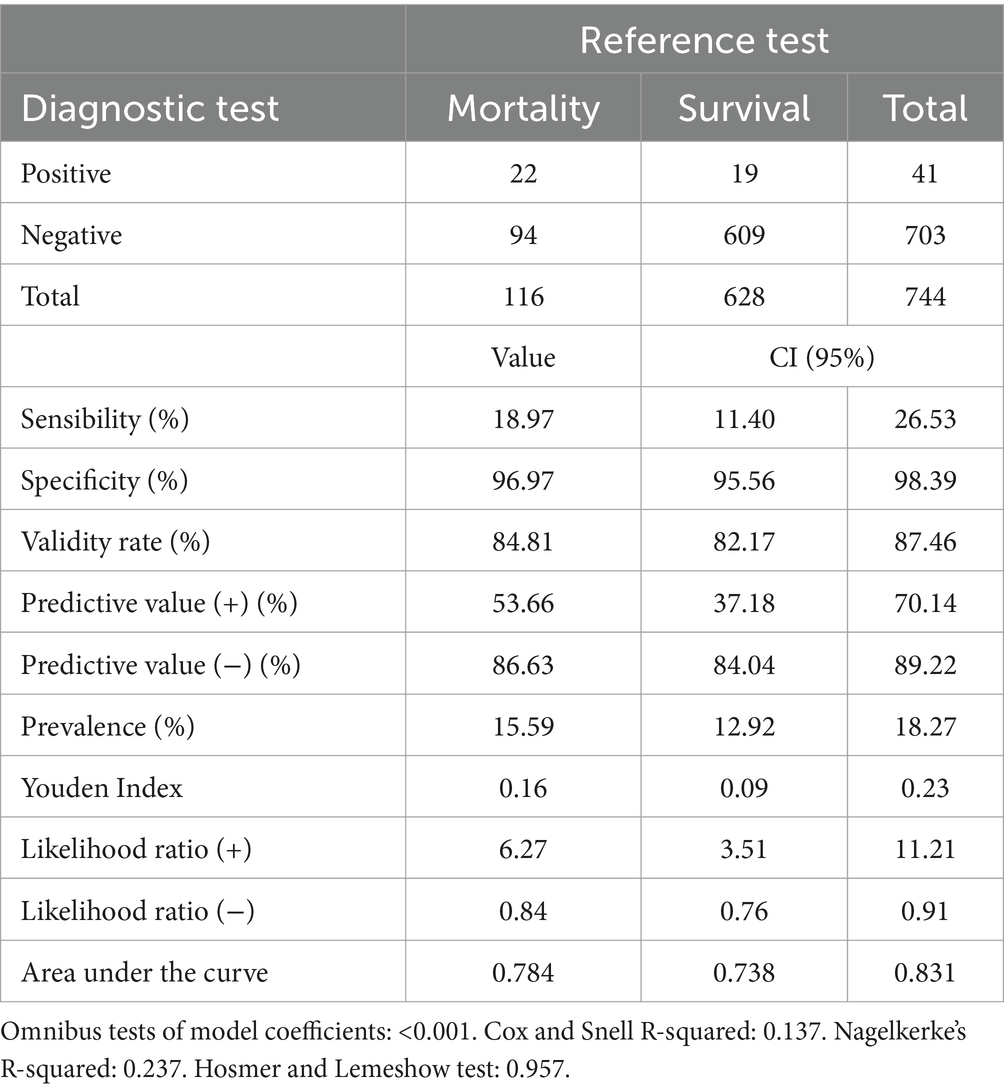
Table 5. Diagnostic accuracy for vital status at discharge.
Data from 744 patients hospitalized in the ICU of a clinic in Cali were analyzed and divided into two cohorts according to the method of nutritional assessment used: BMI or application of the MUST scale.
Regarding the sociodemographic characterization, it was determined that the group of older adults (>60 years) had a greater proportion in the 2021–2022 cohort. In view of this data, the literature indicates that there is limited information regarding the clinical outcomes of older adults admitted to the ICU. This occurs even though their admissions have increased worldwide (25), generally due to causes related to the presence of chronic diseases (26), such as circulatory pathologies and neoplasms, which increase their incidence with increasing age (27). This aspect was evidenced in the results of our study, where these were the most frequent pathologies in both cohorts.
Regarding the progress of people admitted to the ICU, a study with data from Korean patients seen from 2009 to 2014 found that the average length of hospital stay was 4 days, and the overall mortality was 13.8 (28). However, in data from ICUs from 45 countries, a mortality of 17.12% (confidence interval: 16.93–17.32) was found in patients without healthcare-associated infections, with an average length of stay in the ICU of 8.07 (8.01–8.10) days (29).
These data reflect that there is an important variation in the progress of patients hospitalized in the ICU, which can be affected by variables such as pathologies causing the admission, the inflammatory state manifested during hospitalization, the presence of adverse events such as infections associated with health care, the immunological response, and the nutritional status of patients. It is important to highlight here the role of nutritional risk screening performed with the population of patients seen during 2021–2022 in Cali, which allowed for rapid identification and prioritization of clinical interventions, which in the literature has been shown to have a positive impact on aspects such as length of stay in the ICU, morbidity, and mortality (30). This fact was also demonstrated in the results of this research.
When reviewing international data on the use of the MUST scale, results were found from a hospital in Australia with patients admitted to the ICU, where 20% of patients were identified as having a high nutritional risk, and 15% presented a medium risk (31). Similar proportions were observed in the cohort seen in the Cali ICU between 2021 and 2022, where 28.4% of patients had a high risk of malnutrition and 10.8% presented a medium risk.
Furthermore, in this same cohort of patients, it was found that three out of four had experienced unintentional weight loss during the last 6 months, with an average of 4.85% of their body weight (SD: 6.20%). This variable is part of the data collected in the application of the MUST scale (32), as weight loss greater than 5% in a short period has been associated with a deterioration in nutritional status (33). Therefore, some healthcare centers have used this data to evaluate their patients. A multivariate analysis performed on patient data from two hospitals in Toronto, Canada found that subjective global assessment ratings of nutritional status were significantly affected by weight loss (34).
A study conducted in Australia evaluated the information collected by dietitians from subjects admitted to the ICU, including the type of nutritional support received and the symptoms that affected the patients’ nutrition. The study found that oral feeding was the most common form of nutritional support, with 80% of patients receiving it (35). This finding is similar to that obtained with the data from the 2021–2022 cohort in Cali, where 84.3% of patients received oral feeding. In contrast, the 2019 cohort had a higher utilization of enteral support.
Differences in the type of nutritional support provided could be influenced by the presence of gastrointestinal symptoms. However, in our study, no statistically significant differences were observed between the two cohorts that could account for this variation. Both cohorts exhibited a high frequency of abdominal pain, followed by emesis and, to a lesser extent, hyporexia. It is important to consider that several relevant factors determine the route of nutritional support, including the patient’s ability to eat safely and adequately, the nutritional goals, the risk of aspiration, the functional status of the gastrointestinal tract, cognitive function and skills, availability of enteral and/or vascular access, and the results of tests and invasive procedures performed in the ICU (36).
The 2019 patient cohort exhibited a higher inflammatory status, evidenced by a greater prevalence of anemia and leukocytosis, likely related to the underlying disease prompting ICU admission. This higher inflammatory status may have resulted in increased utilization of alternative nutritional support routes, thereby overcoming barriers to oral intake and adhering to general recommendations for adjusting nutritional therapy based on the patient’s clinical condition regarding safety and efficacy (36).
Moreover, the hematological status of the patients also allowed us to identify a high frequency of lymphopenia in the 2019 population, this being a characteristic of immunosuppression, which is usually present on admission to the ICU (37, 38), regardless of whether or not there is a diagnosis of sepsis, thus being able to generate a poor prognosis. Other studies have supported its relevance as a predictive biomarker and possible therapeutic target in intensive care medicine (39). The high presence of lymphopenia in this cohort could have had an impact on patient discharge outcomes. However, the lack of follow-up data on these patients when transferred to other hospital services prevents us from confirming this fact (39).
Regarding supplementation with protein modules for Cali ICU patients, a higher percentage of this type of dietary therapeutic intervention was identified in the 2021–2022 cohort, although without presenting statistically significant differences with the 2019 cohort. In the study by Amon et al., it was observed that a diet high in energy and protein was the most common code assigned, with a mean cumulative nutritional adequacy of 47% (30–74%) for protein, presenting a high percentage of supplementation of this nutrient. This type of intervention has been associated with better clinical outcomes (40). In our study, introducing MUST screening in the care protocol could have been beneficial because it could have led to more precise interventions according to the risk identified in the population served during 2021–2022.
Estimating nutritional risk is often not considered in clinical practice (41), even though it has been shown that such detection and early treatment of malnutrition reduce morbidity and mortality and improve patient outcomes (42). In the case of the cohort admitted to the Cali ICU during the 2019 period (without application of the MUST scale), this aspect was evidenced, identifying a risk increased by almost 3 times for mortality during hospitalization. For these reasons, the need for adequate nutritional screening and assessment tools is evident, as they will help to identify effective strategies to reduce the negative impact of malnutrition (30).
Conversely, in our study, it was observed that patients who received enteral and parenteral nutritional support presented a higher risk of mortality compared to those who were fed orally. This type of support is recommended for critically ill patients with malnutrition who are unable to feed themselves due to their clinical conditions. It is possible that the greater severity of their condition, requiring the use of enteral or parenteral nutrition, contributes to the higher mortality rate in these patients. The literature is inconclusive regarding the comparison between tube feeding and oral diet with intravenous dextrose (standard care) vs. parenteral nutrition. Some studies suggest that tube feeding and standard care are associated with a lower infection risk than parenteral nutrition. However, mortality and risk of infection appear to be higher with standard care in malnourished populations (43).
It is important to mention that, according to the 2019 European Society for Clinical Nutrition and Metabolism recommendations, to avoid overfeeding patients, enteral and parenteral nutrition should be prescribed gradually between 3 and 7 days, avoiding excessive nutrient intake at the beginning of hospitalization. In addition, it is recommended that parenteral support be indicated only when all strategies to promote tolerance to enteral nutrition have been maximized, and this goal has not been achieved (44).
Food intolerance may present with gastrointestinal symptoms, such as emesis, high gastric residual volume, absence of gastrointestinal peristalsis, abdominal distension, and diarrhea (45). These symptoms have also been associated with an increased risk of mortality, generating an OR of up to 5.24 in surgical ICU patients (46). In our study, we observed that emesis increased the risk of mortality 2.4-fold. Therefore, it is essential to perform a thorough evaluation to identify food intolerance and provide an adequate approach to the patient, focusing on recovery of health status and reducing complications.
Regarding the changes in the levels of white blood cells present in our Cali patients and their relationship with the increase in mortality, it has been shown that these data are clinically significant and valuable for diagnosing and controlling the condition of hospitalized people (47). These findings coincide with a meta-analysis, demonstrating a clinically significant relationship between high white blood cell count and mortality in various study populations (47, 48).
Finally, an investigation in Greece with critically ill patients found that the Acute Physiology and Chronic Health Evaluation II classification system scale correlated well with in-hospital mortality, showing an AUC of 0.6684. This result suggests moderate discrimination in a mixed ICU population (49), similar to that of the population in our study. However, this research developed a predictive model for mortality with a higher AUC (0.784), which underlines the importance of working on the factors identified to counteract them and focus care on controlling these risks.
Regarding the limitations of the study, it is important to highlight that although the predictive model for mortality managed to obtain a high percentage of specificity, its sensitivity was relatively low. Therefore, it is crucial to continue adjusting this model, incorporating other variables that may improve its predictive capacity. Furthermore, it would be beneficial to apply the model in a multicenter sample to evaluate its performance in different clinical settings since the differences observed between the two cohorts could have affected the generalizability of the results. However, despite these limitations, the model proved to be a valid method to identify patients with a lower risk of mortality.
Admission to the ICU is frequently associated with chronic noncommunicable pathologies, such as circulatory diseases, respiratory diseases, and cancer, as well as with a higher proportion of older adult patients, whose functional deterioration due to aging and the increasing prevalence of chronic diseases may contribute to this phenomenon. Furthermore, a high percentage of overweight and obese patients was observed in both cohorts.
Our study has the statistical capacity to detect clinically relevant differences in the mortality of patients in our ICU in Cali, independently of the pathologies that motivated their admission. The assessment of nutritional status was carried out by nutrition and dietetics professionals of the hospital and complemented with laboratory data that provided valuable information on the clinical, hematological, and immunological status of the patients upon admission to the ICU.
The development of a predictive mortality model revealed that implementing the MUST screening method and specific nutritional interventions resulted in a significant improvement in the mortality figures of ICU patients. These results highlight the importance of using standardized and validated tools to assess nutritional risk, which can lead to a tangible improvement in the overall health status of patients and a reduction in complications during their ICU stay. This improvement in nutritional care can, in turn, promote faster recovery and better outcomes at hospital discharge.
The data analyzed in this study is subject to the following licenses/restrictions: the data are not publicly available, due to ethical reasons indicated by the research committee of the health institution, regarding the handling and privacy of patient data. Requests to access these datasets should be directed to Blanca Cecilia Díaz Chavarro, YmxhbmNhLmRpYXowMEB1c2MuZWR1LmNv.
The studies involving humans were approved by Ethics and Bioethics Committee of the Department of Health of the University Santiago de Cali-Colombia—"CEB-USC,” and Scientific Technical Committee of the participating clinic. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
BC: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. MR-S: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing, Resources. JR: Conceptualization, Data curation, Investigation, Methodology, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. GM-R: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This research has been funded by the Dirección General de Investigaciones of Universidad Santiago de Cali under call No. 01 – 2025.
The preprint of this article, Impact of Nutritional Screening on Mortality and Intensive Care Unit Length of Stay, is available on SSRN: https://ssrn.com/abstract=4892316 or http://dx.doi.org/10.2139/ssrn.4892316. This research has been funded by Dirección General de Investigaciones of Universidad Santiago de Cali under call No. 01-2025.
JR was employed by Clínica de Occidente SA.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2025.1474039/full#supplementary-material
1. Alencar, ES, LSDS, M, JLG, H, BDD, O, MCF, C, AMM, L, et al. Enteral nutritional support for patients hospitalized with COVID-19: results from the first wave in a public hospital. Nutrition. (2022) 94:111512. doi: 10.1016/j.nut.2021.111512
2. Schuetz, P, Seres, D, Gomes, F, Kaegi-Braun, N, and Stanga, Z. Management of disease-related malnutrition for patients being treated in hospital. Lancet. (2021) 398:1927–38. doi: 10.1016/S0140-6736(21)01451-3
3. Cederholm, T, Barazzoni, R, Austin, P, Ballmer, P, Biolo, G, and Singer, P. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin Nutr. (2017) 36:49–64. doi: 10.1016/j.clnu.2016.09.004
4. Domínguez-Berrueta, H. Analysis of the nutritional parameters and adjustment of the requirements of the initial parenteral nutrition in post-surgical critically ill patients. Nutr Hosp. (2014) 29:402–10. doi: 10.3305/nh.2014.29.2.7034
5. Ballesteros-Pomar, MD, Cortés, GB, Romero, FB, García, JMF, Gutiérrez, FP, Arroyo, VR, et al. Continuity of care in disease-related malnutrition and nutritional medical treatment. Endocrinología, Diabetes y Nutrición (English ed). (2022) 69:897–909. doi: 10.1016/j.endien.2022.11.013
6. Barker, L, Gout, B, and Crowe, T. Hospital malnutrition: prevalence, identification and impact on patients and the healthcare system. Int J Environ Res Public Health. (2011) 8:514–27. doi: 10.3390/ijerph8020514
7. Canales, C, Elsayes, A, Belcher, D, and Nakayama, A. Nutrition risk in critically ill versus the nutritional risk screening 2002: are they comparable for assessing risk of malnutrition in critically ill patients? J Parenter Enter Nutr. (2019) 43:81–7. doi: 10.1002/jpen.1181
8. Krager, K, Berens, M, Ponce, J, Timmerman, M, Hanson, C, and Jackson, M. Early enteral nutrition support and malnutrition status in patients on vasopressors in the ICU. J Acad Nutr Diet. (2023) 123:A27. doi: 10.1016/j.jand.2023.06.084
9. Thibault, R, Bear, DE, Fischer, A, Hiesmayr, M, and Tamási, P. Implementation of the ESPEN guideline on clinical nutrition in the intensive care unit (ICU): it is time to move forward!: a position paper from the nutrition in the ICU, ESPEN special interest group. Clin Nutrit ESPEN. (2023) 57:318–30. doi: 10.1016/j.clnesp.2023.06.033
10. Castillo, J, Gómez, A, Velasco, N, Díaz-Pizarro, J, Matos, A, and Miján de la Torre, A. Nutritional assessment of hospitalized patients in Latin America: association with prognostic variables. The ENHOLA study. Nutr Hosp. (2016) 33:655–62. doi: 10.20960/nh.275
11. Bermúdez, C, Sanabria, Á, and Vega, V. Soporte nutricional del paciente adulto. Resultados de la reunión de consenso de la Asociación Colombiana de Nutrición Clínica. Revista Colombiana de Cirugía. (2013) 28:101–16. doi: 10.30944/20117582.263
12. Hernández, JÁ, Pomar, MDB, and Fuster, GO. Desnutrición relacionada con la enfermedad y su tratamiento: relaciones coste-beneficio In: Tratado de nutrición : Editorial Médica Panamericana (2017). 75–92. Available at: https://dialnet.uniroja.es/servlet/articulo?codigo=7130934
13. Álvarez, J, Montejo, J, and García, A. Plan de Eficiencia Nutricional. Cuaderno no1. Herramientas de cribado nutricional para Hospitales, Residencias y Comunidad. Más nutridos – Mayores y enfermos. (2018). Available at: https://www.alianzamasnutridos.es/uploads/cuadernos/pdf/eadb6d997e5e3e77931bc9e25744ca22.pdf (Accessed on 2023 Dec 15)
14. Ballesteros-Pomar, MD, and González-Arnáiz, E. Why should we all be concerned about sarcopenia and disease-related malnutrition? Endocrinologia, Diabetes y Nutricion. (2021) 68:599–601. doi: 10.1016/j.endien.2021.11.029
15. Pereira, FJ, Barbosa, J, Munera, N, Yepez, M, Londoño, M, Cañas, D, et al. Thigh ultrasound findings, calf circumference and clinical outcomes during nutrition day-ICU at Clínica las Américas-Auna, Medellín (Colombia). Clin Nutrit ESPEN. (2023) 58:696. doi: 10.1016/j.clnesp.2023.09.787
16. Poulia, KA, Klek, S, Doundoulakis, I, Bouras, E, Karayiannis, D, Baschali, A, et al. The two most popular malnutrition screening tools in the light of the new ESPEN consensus definition of the diagnostic criteria for malnutrition. Clin Nutr. (2017) 36:1130–5. doi: 10.1016/j.clnu.2016.07.014
17. Valero, M, Díez, L, and El Kadaoui, N, Jiménez A.E, Rodríguez, H, and León, M. ¿Son las herramientas recomendadas por la ASPEN y la ESPEN equiparables en la valoración del estado nutricional?. Nutr Hosp, 20. (2005): 259–267. Available at: https//scielo.isciii.es/pdf/nh/v20n4/05HerramientasAspen.pdf
18. Löser, C. Malnutrition in hospital: the clinical and economic implications. Dtsch Arztebl Int. (2010) 107:911–7. doi: 10.3238/arztebl.2010.0911
19. Montoya, S, and Múnera, NE. Efecto de la intervención nutricional temprana en el resultado clínico de pacientes en riesgo nutricional. Nutr Hosp. (2014) 29:427–36. doi: 10.3305/nh.2014.29.2.7060
20. Pourmahmoudi, A, Nicolau, J, Veronese, N, Roustaei, N, and Hosseinikia, M. The importance of nutritional status on clinical outcomes among both ICU and non-ICU patients with COVID-19. Clin Nutrit ESPEN. (2022) 49:225–31. doi: 10.1016/j.clnesp.2022.04.016
21. Colombia. Ministerio de Salud y Protección Social. Resolución Número 3280 del 2018, Política Integral de Atención en Salud. (2018). Available at: https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/DE/DIJ/resolucion-3280-de-2018.pdf (consultado el 20 de marzo de 2024).
22. World Health Organization (WHO). Body Mass Index (BMI). (2025). Available at: https://www.who.int/data/gho/data/themes/topics/topic-details/GHO/body-mass-index (Consultado el 06 de mayo de 2024)
23. Anesi, G, Savarimuthu, S, Invernizzi, J, Hyman, R, Ramkillawan, A, Eddey, C, et al. ICU mortality across Prepandemic and pandemic cohorts in a resource-limited setting: a critical care resiliency analysis from South Africa. CHEST Critical Care. (2023) 1:100005. doi: 10.1016/j.chstcc.2023.100005
24. Parent, B, Seaton, M, and O’Keefe, GE. Biochemical markers of nutrition support in critically ill trauma victims. J Parenter Enter Nutr. (2018) 42:335–42. doi: 10.1177/0148607116671768
25. Boumendil, A, and Guidet, B. Elderly patients and intensive care medicine. Intensive Care Med. (2006) 32:965–7. doi: 10.1007/s00134-006-0172-z
26. Rodríguez-García, R, González-Lamuño, L, Santullano, M, and Martín-Carro, B. Clinical features and disease progression of elderly patients at the ICU setting. Med Int. (2024) 48:254–62. doi: 10.1016/j.medine.2024.02.009
27. Petitto, G, Goloubeva, OG, Masur, J, Childress, J, Iqbal, T, An, M, et al. Clinical outcomes of patients with acute myeloid leukemia and cardiovascular disease. Leuk Res. (2024) 138:107456. doi: 10.1016/j.leukres.2024.107456
28. Park, J, Jeon, K, Chung, CR, Yang, JH, Cho, YH, and Cho, J. A nationwide analysis of intensive care unit admissions, 2009–2014–the Korean ICU National Data (KIND) study. J Crit Care. (2018) 44:24–30. doi: 10.1016/j.jcrc.2017.09.017
29. Rosenthal, VD, Duszynska, W, Ider, BE, Gurskis, V, Al-Ruzzieh, MA, Myatra, SN, et al. International nosocomial infection control consortium (INICC) report, data summary of 45 countries for 2013-2018, adult and pediatric units, device-associated module. Am J Infect Control. (2021) 49:1267–74. doi: 10.1016/j.ajic.2021.04.077
30. Lew, CCH, Yandell, R, Fraser, RJ, Chua, AP, Chong, MFF, and Miller, M. Association between malnutrition and clinical outcomes in the intensive care unit: a systematic review. J Parenter Enter Nutr. (2017) 41:744–58. doi: 10.1177/0148607115625638
31. Egan, T, Chapple, LA, Morgan, H, Rassias, G, and Yandell, R. Nutritional risk screening in noninvasively mechanically ventilated critically ill adult patients: a feasibility trial. Aust Crit Care. (2022) 35:153–8. doi: 10.1016/j.aucc.2021.03.004
32. British Association for Parenteral and Enteral Nutrition – BAPEN. Manual Explicativo “MUST”. (2003). Available at: https://www.bapen.org.uk/images/pdfs/must/spanish/must-exp-bk.pdf (Consultado del 6 de mayo de 2024)
33. Correia, MIT, Perman, MI, and Waitzberg, DL. Hospital malnutrition in Latin America: a systematic review. Clin Nutr. (2017) 36:958–67. doi: 10.1016/j.clnu.2016.06.025
34. Detsky, AS, McLaughlin, JR, Baker, JP, Johnston, NANCY, Whittaker, S, and Jeejeebhoy, KN. What is subjective global assessment of nutritional status? J Parenter Enter Nutr. (1987) 11:8–13. doi: 10.1177/014860718701100108
35. Amon, JN, Tatucu-Babet, OA, Hodgson, CL, Nyulasi, I, Paul, E, Jackson, S, et al. Nutrition care processes from intensive care unit admission to inpatient rehabilitation: a retrospective observational study. Nutrition. (2023) 113:112061. doi: 10.1016/j.nut.2023.112061
36. Ukleja, A, Gilbert, K, Walker, R, and Ybarra, J. Task force on standards for nutrition support: adult hospitalized patients, the American Society for Parenteral and Enteral Nutrition. Standards for nutrition support: adult hospitalized patients. Nutr Clin Pract. (2018) 33:906–20. doi: 10.1002/ncp.10204
37. Moins-Teisserenc, H, Audigier, V, Ressaire, Q, Benyamina, M, Lambert, J, and Legrand, M. Severe altered immune status after burn injury is associated with bacterial infection and septic shock. Front Immunol. (2021) 12:586195. doi: 10.3389/fimmu.2021.586195
38. Rico-Feijoó, J, Bermejo, JF, Pérez-González, A, Martín-Alfonso, S, and Aldecoa, C. Influence of lymphopenia on long-term mortality in septic shock, a retrospective observational study. Revista Española de Anestesiología y Reanimación (English Edition). (2024) 71:368–78. doi: 10.1016/j.redare.2024.02.014
39. Hohlstein, P, Gussen, H, Bartneck, M, Roderburg, C, Buendgens, L, and Tacke, F. Prognostic relevance of altered lymphocyte subpopulations in critical illness and sepsis. J Clin Med. (2019) 8:353. doi: 10.3390/jcm8030353
40. Mogensen, KM, Robinson, MK, Casey, JD, Gunasekera, NS, Moromizato, T, Rawn, JD, et al. Nutritional status and mortality in the critically ill. Crit Care Med. (2015) 43:2605–15. doi: 10.1097/CCM.0000000000001306
41. Kahveci, F, Demirkan, K, Doganay, M, Gomceli, I, Gundogan, K, Topeli, A, et al. Parenteral nutrition consensus report from KEPAN. Nutrition. (2024) 123:112424. doi: 10.1016/j.nut.2024.112424
42. Tufan, A, Bahat, G, Ozkaya, H, Taşcıoğlu, D, Tufan, F, and Saka, B. Low skeletal muscle mass index is associated with function and nutritional status in residents in a Turkish nursing home. Aging Male. (2016) 19:182–6. doi: 10.1080/13685538.2016.1188069
43. Braunschweig, CL, Levy, P, Sheean, PM, and Wang, X. Enteral compared with parenteral nutrition: a meta-analysis. Am J Clin Nutr. (2001) 74:534–42. doi: 10.1093/ajcn/74.4.534
44. Xu, E, Tejada, S, Solé-Lleonart, C, Campogiani, L, Valenzuela-Sanchez, F, Koulenti, D, et al. Evaluation of the quality of evidence supporting guideline recommendations for the nutritional management of critically ill adults. Clinl nutrit ESPEN. (2020) 39:144–9. doi: 10.1016/j.clnesp.2020.07.004
45. Li, J, Wang, L, Zhang, H, Zou, T, Kang, Y, He, W, et al. Different definitions of feeding intolerance and their associations with outcomes of critically ill adults receiving enteral nutrition: a systematic review and meta-analysis. J Intensive Care. (2023) 11:29. doi: 10.1186/s40560-023-00674-3
46. Guan, X, Chen, D, and Xu, Y. Clinical practice guidelines for nutritional assessment and monitoring of adult ICU patients in China. J Intensive Med. (2024) 4:137–59. doi: 10.1016/j.jointm.2023.12.002
47. Park, C, Yoo, K, Lee, S, Kim, H, Son, E, and Lee, D. The prognostic significance of leukocyte count on all-cause and cardiovascular disease mortality: a systematic review and Meta-analysis. Am J Cardiol. (2023) 203:226–33. doi: 10.1016/j.amjcard.2023.06.119
49. Papadimitriou-Olivgeris, M, Panteli, E, Koutsileou, K, Boulovana, M, Zotou, A, Marangos, M, et al. Predictors of mortality of trauma patients admitted to the ICU: a retrospective observational study. Brazilian J Anesthesiol. (2021) 71:23–30. doi: 10.1016/j.bjane.2020.12.006
Keywords: nutritional screening, critical care, malnutrition, mortality, intensive care unit
Citation: Díaz Chavarro BC, Romero-Saldaña M, Assis Reveiz JK and Molina-Recio G (2025) Impact of nutritional screening on mortality and intensive care unit length of stay. Front. Nutr. 12:1474039. doi: 10.3389/fnut.2025.1474039
Edited by:
Renying Xu, Shanghai Jiao Tong University, ChinaReviewed by:
Cesar Ivan Aviles Gonzalez, Popular University of Cesar, ColombiaCopyright © 2025 Díaz Chavarro, Romero-Saldaña, Assis Reveiz and Molina-Recio. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Manuel Romero-Saldaña, ejkycm9zYW1AdWNvLmVz
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.