 Xiaomei Fan
Xiaomei Fan Huixia Cui3*
Huixia Cui3*
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Nutr., 31 July 2024
Sec. Clinical Nutrition
Volume 11 - 2024 | https://doi.org/10.3389/fnut.2024.1413117
This article is part of the Research TopicNutrition and Metabolism in Cancer: Role in Prevention and PrognosisView all 30 articles
Objective: To evaluate and summarize the best evidence for nutritional support in patients receiving radiotherapy for nasopharyngeal carcinoma and to offer guidance for clinical practice.
Background: Patients with nasopharyngeal carcinoma undergoing radiotherapy often experience a high prevalence of malnutrition, and there is a lack of compiled guideline recommendations, which complicates the provision of a reference for clinical nursing.
Methods: A systematic literature search revealed the best evidence of nutritional support for nasopharyngeal carcinoma patients undergoing radiotherapy. Included in the review were various types of literature, such as clinical guidelines, expert consensus, systematic evaluations, meta-analyses, evidence summaries, and original studies. The evidence was graded according to the Australian Joanna Briggs Institute Centre for Evidence-Based Health Care Evidence Pre-Grading System (2016 version). Data were gathered from a range of sources, including BMJ Best Practice, the Scottish Intercollegiate Guidelines Network, the Cochrane Library, Embase, PubMed, Web of Science, CINAL, CNKI, the WanFang database, SinoMed, the Yi Maitong Guidelines Network, Dingxiangyuan, the Chinese Nutrition Society, the European Society for Clinical Nutrition and Metabolism website, and the American Society for Parenteral and Enteral Nutrition website. The search spanned from January 2013 to 2023.
Results: A comprehensive review identified a total of 3,207 articles, comprising six guidelines, eight expert consensus articles, four systematic evaluations, five randomized controlled trials, two cohort trials, and two observational studies. From these articles, we synthesized 63 pieces of evidence spanning six domains: nutritional risk screening and assessment, nutrient requirements, nutritional support, management of nutritional symptoms, functional exercise, and nutritional monitoring and follow-up.
Conclusion: A total of lines of evidence supporting nutritional support for nasopharyngeal carcinoma patients receiving radiotherapy were summarized. However, the evidence should be combined with the actual clinical situation, and it should be validated in the future by combining large-sample and multicenter studies to provide a more scientific and beneficial nutritional support program for nasopharyngeal carcinoma patients receiving radiotherapy.
Nasopharyngeal carcinoma, a malignant tumor arising in the mucosal epithelium of the nasopharynx, demonstrates a notable geographic variation in its occurrence (1). It is more prevalent in East Asia and Southeast Asia, with a higher incidence among males and a peak occurrence between the ages of 40 and 59 (2, 3). This cancer constitutes a common type of malignant head and neck tumor in China.
The primary treatment approach for nasopharyngeal carcinoma involves radiotherapy or a combination of therapies with radiotherapy as the cornerstone (4). Common side effects of radiotherapy for this type of cancer include acute radiation mucositis, radiation dermatitis, radiation-induced damage to salivary glands, and bone marrow suppression. These side effects often manifest as alterations in taste, oropharyngeal and throat pain, dry mouth, accumulation of mucus in the oropharynx and throat, difficulty in chewing or swallowing, and pain, which can impede the intake or absorption of nutrients (5, 6). Malnutrition is a frequent complication in patients undergoing radiotherapy for nasopharyngeal carcinoma, typically occurring early in treatment and worsening as treatment progresses (7, 8). Zhuang et al. (9) found that 69.0% of patients experienced malnutrition by the end of radiotherapy, while Wei et al. (10) reported a severe malnutrition incidence rate of 80.7% during radiotherapy. Hong et al. (11) observed that 20.19% of patients experienced more than a 10% weight loss by the end of radiotherapy. Additionally, a study (12) showed that the prevalence of malnutrition increased from 16.8% before treatment to 91.2% by the end of treatment. Nutritional support is crucial in the clinical management of nasopharyngeal carcinoma patients undergoing radiotherapy. Malnutrition can diminish sensitivity to radiochemotherapy, exacerbate side effects, reduce treatment tolerance, and impair patient quality of life (13–15).
With growing awareness of the nutritional challenges faced by patients undergoing radiotherapy for nasopharyngeal carcinoma, various nutritional support approaches are now accessible. Early nutritional intervention (16–18) is recognized as beneficial for enhancing patients’ nutritional status. Nutritional education combined with oral nutritional supplementation (ONS) has been shown to enhance patients’ nutritional intake (19–23), improve tolerance to radiotherapy (24), and decrease the occurrence of adverse reactions to radiotherapy in nasopharyngeal cancer patients through enteral nutrition (25, 26). In terms of nutritional intervention, there are a variety of intervention strategies available, such as personalized whole nutritional management (27–33), systematic nutritional management (34), the plan-do-check-act (PDCA) cycle model (35), intensive management mode (36, 37), and the multidisciplinary collaboration model (38, 39). These intervention methods are believed to enhance the nutritional status of nasopharyngeal cancer patients undergoing radiotherapy and improve their tolerance to the treatment. However, these intervention and management strategies have developed from other diseases and are built upon the framework of nutritional management for oncology patients. Yet, they lack the specificity and targeted guidance for nutritional support tailored to patients with nasopharyngeal carcinoma undergoing radiotherapy.
So far, there is only an expert consensus on nutritional support for nasopharyngeal cancer patients, with recommendations limited to nutritional risk screening and assessment, nutritional education, selection of nutritional treatment modalities, and nutrient requirements (7). Notably, there is a lack of guidance on nutritional monitoring and follow-up. Additionally, specific guidelines for treating nasopharyngeal carcinoma patients undergoing radiotherapy are absent, with simplified content devoid of specific recommendations. Consequently, nurses find it challenging to utilize this tool for guiding clinical practice. In this study, we systematically conducted a literature search on studies related to nutritional support for patients undergoing nasopharyngeal carcinoma radiotherapy. We then screened and integrated the available evidence with the aim of providing the best clinical practices for nutritional support in this patient population.
The PIPOST model, developed by the JBI Center for Evidence-Based Nursing at Fudan University in Shanghai, served as the framework for constructing evidence-based queries. P (population) identifies the specific target population: patients with nasopharyngeal carcinoma undergoing radiotherapy; I (intervention) denotes the nutritional support intervention; the second P (professional) refers to the professionals applying the evidence: clinical medical staff; O (outcome) focuses on the incidence of malnutrition and patients’ nutritional status; S (setting) specifies the location where the evidence is applied: radiology wards; T (type of evidence) outlines the variety of evidence types utilized, including guidelines, systematic evaluations, expert consensus, best clinical practice information booklets, evidence summaries, and original research.
This study searched the following databases and websites:
The following Chinese databases were used: China National Knowledge Infrastructure (CNKI), Wanfang Database, VIP Full Text Database, and China Biology Medicine (CBM).
The following English databases were used: PubMed, Embase, Web of Science, Cochrane Library, and CINAHL.
Guidelines networks: the Scottish Intercollegiate Guidelines Network (SIGN), BMJ Best Practice, National Guideline Clearinghouse (NGC), Ding Xiangyuan, Medlive.
Relevant nutrition society websites include the official websites of the European Society for Parenteral and Enteral Nutrition, the American Society for Parenteral and Enteral Nutrition, the American Academy of Nutrition and Dietetics (AND), and the Chinese Society for Nutrition.
Search strategy. The search terms included “Nasopharyngeal Carcinoma,” “Carcinoma, Nasopharyngeal,” “Head and Neck Neoplasms,” “Radiotherapy,” “Radiation Treatment,” “Targeted Radiotherapy,” “Nutritional Status,” “Nutrition Disorders,” “Diet, Food, and Nutrition,” “Enteral Nutrition,” and “Parenteral Nutrition,” with a search period from 2013 to 2023.
The inclusion criteria for the present study were patients who underwent radiotherapy for nasopharyngeal carcinoma; nutritional support for patients who underwent radiotherapy for nasopharyngeal carcinoma; guidelines, expert consensuses, summaries of evidence, systematic evaluations, and original research; and written in Chinese and English.
The exclusion criteria were as follows: guideline interpretations and plans; studies repeatedly published or updated; studies with incomplete information or unavailable full text; and studies with failed quality evaluation.
The literature was screened independently by two postgraduate students in the group who had received training in evidence-based nursing, and the screening steps were as follows: ① deduplication: Endnote software was used to de-adjust duplicates; ② initial screening: the titles and abstracts of the literature were read, and the literature that was not relevant to the topic was excluded; ③ rescreening: the remaining literature was read carefully, the eligible literature was screened, and the basic information of the literature was extracted. The screening results of the two researchers were cross-checked, and when the results were controversial, a third evidence-based care specialist was invited to determine the inclusion status.
For evaluating guidelines, we employed the Clinical Guidelines Research and Evaluation System (AGREE II), which assesses various aspects, including “scope and purpose,” “participants,” “rigor of development,” “clarity,” “applicability,” and “editorial independence.” This tool consists of 23 individual entries and two overall evaluation entries. Each entry is scored on a scale of 1–7, with higher scores indicating better compliance. The standardized percentage score for each item is calculated using the formula: (actual score – minimum possible score)/(maximum possible score – minimum possible score) × 100%. Items with standardized percentage scores ≥60% are categorized as Grade A, those with scores ≥30% but <60% as Grade B, and items with scores <30% as Grade C.
Systematic evaluations, meta-analyses, expert consensus, randomized controlled trials, cohort studies, and observational studies underwent assessment using the Australian JBI Centre for Evidence-Based Health Care’s Quality Assessment Criteria (2016) (40). Evaluators rendered judgments of “yes,” “no,” “unclear,” or “inapplicable” for each item based on the literature. Following group discussion, decisions were reached regarding inclusion, exclusion, or the need for further information for each item labeled as “no,” “unclear,” or “not applicable.”
The quality of the included studies was assessed separately by two researchers who had undergone evidence-based training. In cases of disagreement, the judges were assisted by deliberation or by a third evidence-based care specialist.
Two researchers with evidence-based training and more than a decade of clinical experience extracted and summarized evidence from the included literature. The grading of evidence followed the Australian Center for Evidence-Based Health Care’s Level of Evidence Recommendation System (2014 version). Any disagreements were resolved through consultation or with the aid of a third researcher. In instances of conflicting evidence conclusions, priority was given to high-quality and recently published evidence from peer-reviewed journals.
Initially, 3,207 articles were gathered, and after deduplication using ENDNOTE, 2,201 articles remained. Xiaomei Fan and Shasha Liu, both trained in evidence-based medicine, independently screened the titles and abstracts of these articles. They excluded 1,787 articles deemed irrelevant, leaving 414 articles for further review. Following a full-text assessment, eight articles were excluded due to unavailability, 290 for being off-topic, 2 for being updated guidelines, and 1 for being an interpretation of guidelines. This left 113 articles for careful scrutiny. Upon examination, 86 articles were further excluded due to either the inability to extract evidence or low evidence quality, resulting in the selection of 27 articles. These included six guidelines, eight expert consensuses, four systematic evaluations, five randomized controlled trials, two quasi-experiments, and two observational studies. The process of literature screening is outlined in Figure 1.
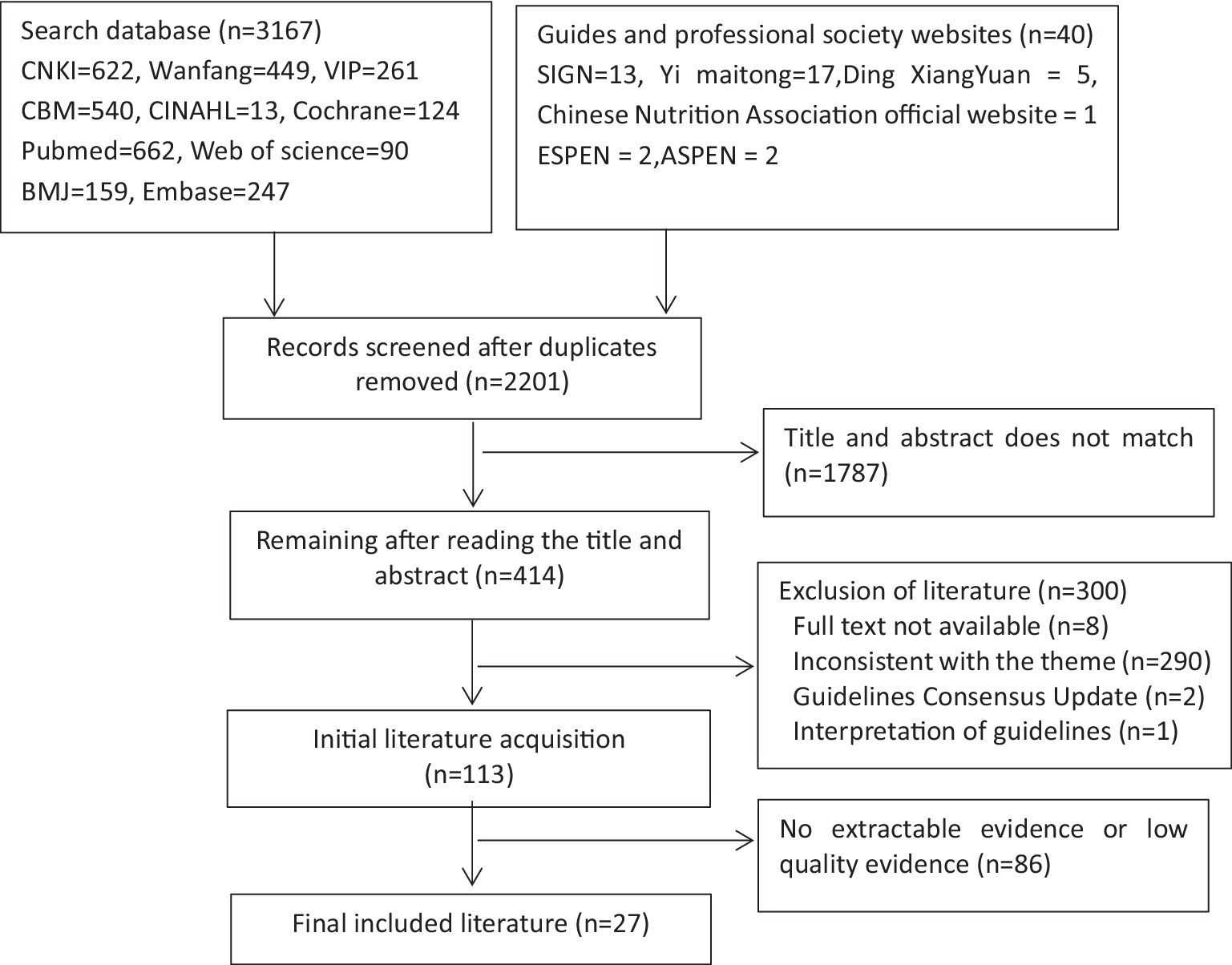
Figure 1. A flow chart of literature screening.
The general characteristics of the included studies are shown in Table 1.
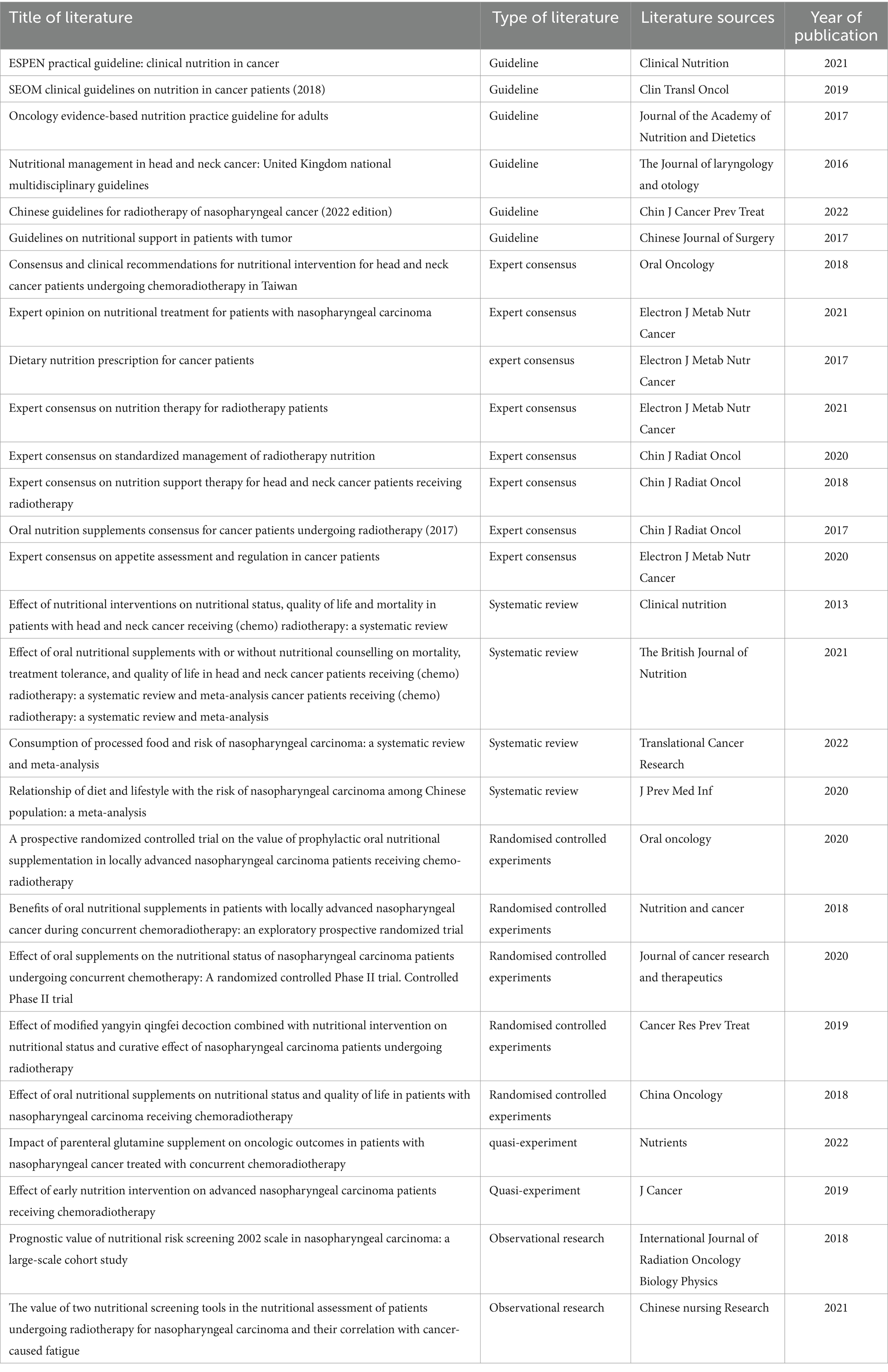
Table 1. The general characteristics of the included literature.
Six guidelines were included in the study, with their quality assessment results presented in Table 2. Two of these guidelines originated from China (5), The Chinese Society of Parenteral and Enteral Nutrition (45), offering recommendations for radiation therapy in nasopharyngeal carcinoma patients and nutrition management in cancer patients, respectively. One guideline was from the United States (43), focusing on nutrition support guidelines for cancer patients. Another guideline was from the UK, providing evidence-based nutritional practice guidelines for adults with cancer (44). Additionally, one guideline was from Spain (42), titled the SEOM clinical guidelines for cancer patient nutrition (2018), and one was from Europe, focusing on clinical nutrition guidelines (41). Except for Kang Min’s guideline (5), which specifically addressed nasopharyngeal carcinoma radiotherapy, the remaining guidelines pertained to nutrition. Among them, three articles received Grade A recommendations, while three received Grade B recommendations.
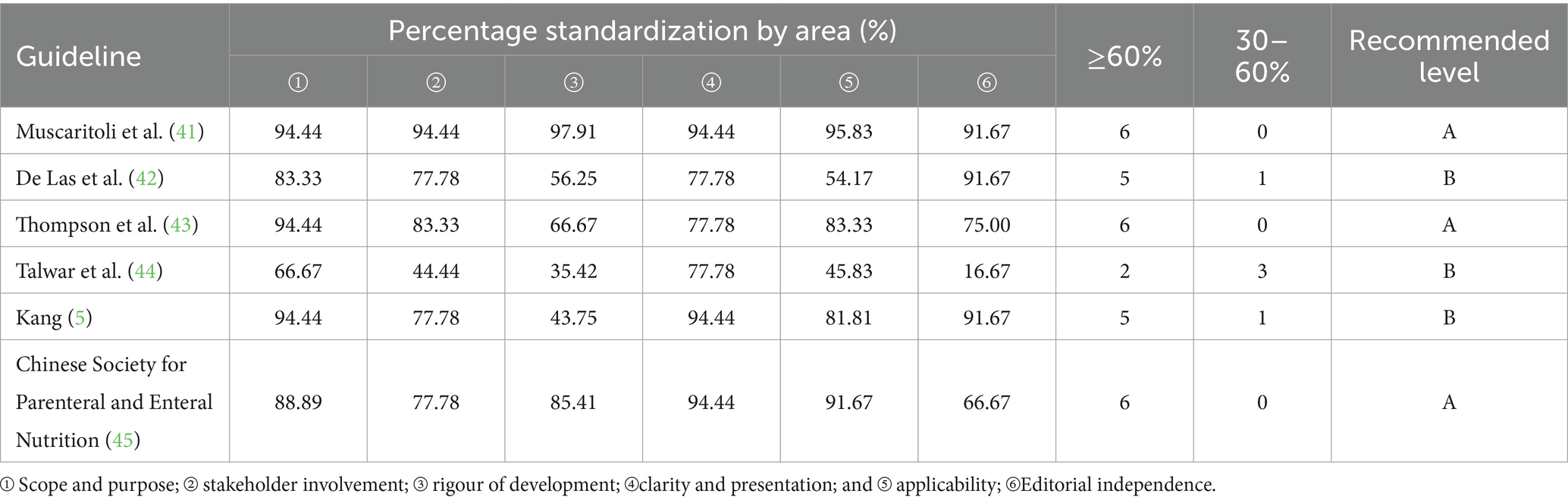
Table 2. Guide quality evaluation results.
Nine expert consensuses from China were included in the study. These were authored by Lin et al. (46), Li (7), Li et al. (47), Li et al. (13), Branch of Radiation Oncology of Chinese Medical Association (48), Cancer Radiotherapy Nutrition Group, Cancer Nutrition and Support Committee of China, China Anti-Cancer Association (49), China Society for Radiation Oncology (50), and Li et al. (51). Seven were written in Chinese, while one was in English. Among them, four articles discussed nutritional therapy (7, 13, 46, 48), one focused on ONS (50), one addressed diet nutrition (47), and one explored appetite regulation in cancer patients (51). The expert consensus was included in this study, and there was a high inter-rater agreement. All of the entries were yes, except for entry 6, “Is there any inconsistency between the proposed viewpoints and the previous literature?” The evaluation for each criterion is outlined, as detailed in Table 3.
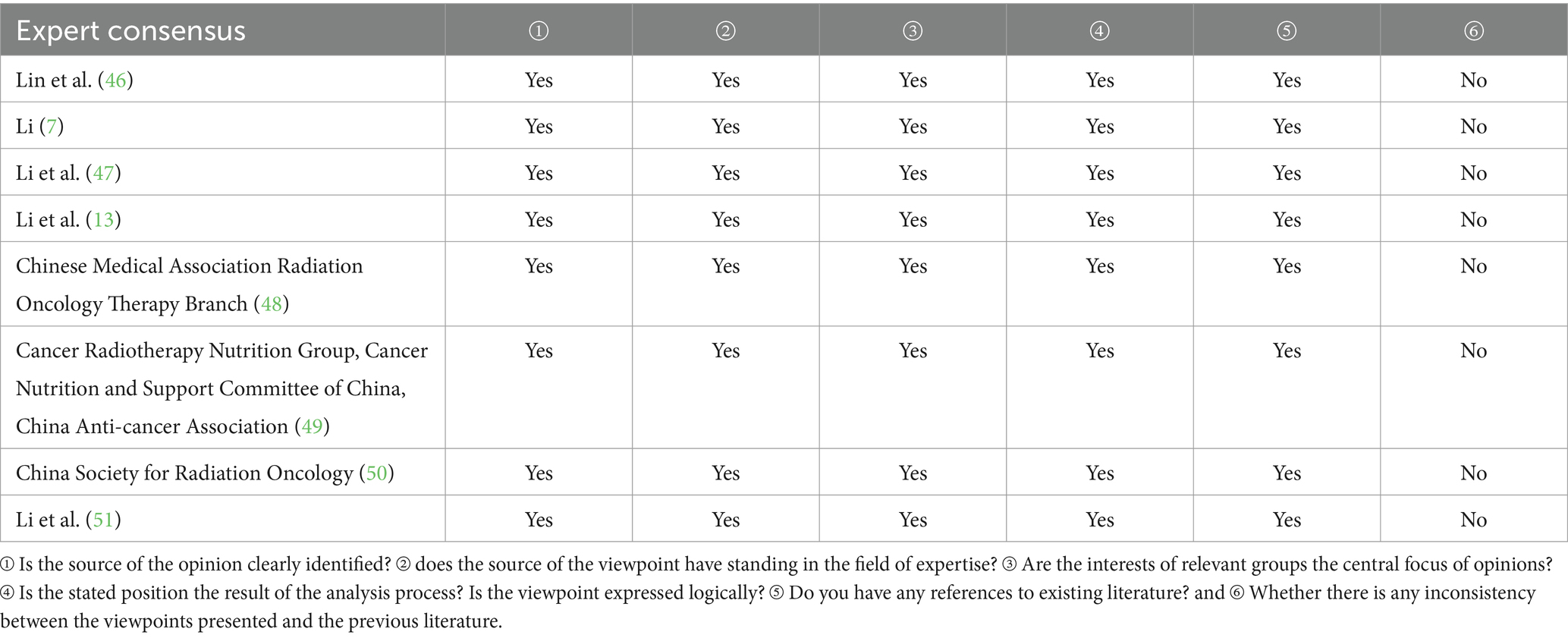
Table 3. Results of the evaluation of the quality of expert consensus.
Three systematic evaluations and one meta-analysis were included in the study: Langius et al. (52), Mello et al. (53), Feng et al. (54), and Chen et al. (55). Feng et al. (54) investigated the impact of processed foods on nasopharyngeal cancer patients, while Mello et al. (53) and Langius et al. (52) explored the effects of nutritional interventions on patients undergoing head and neck radiotherapy. Chen et al. (55) examined the correlation between lifestyle and dietary behaviors in a Chinese nasopharyngeal cancer population. The evaluation results can be found in Table 4.
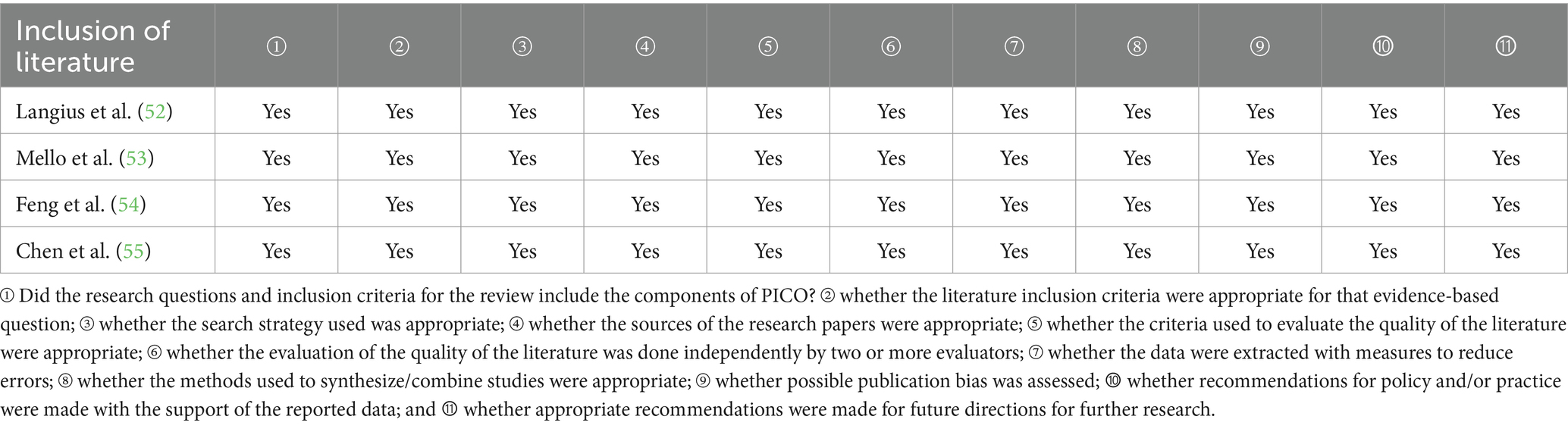
Table 4. Systematic evaluation or meta-analysis evaluation results.
Five randomized controlled trials were incorporated into the study: Huang et al. (24), Jiang et al. (23), Dou et al. (19), Huang et al. (51), and Ding et al. (15). Huang et al. (51) examined the utilization of traditional Chinese medicine decoctions in nutritional intervention for nasopharyngeal carcinoma patients. The remaining four articles explored oral nutritional supplementation in nasopharyngeal carcinoma patients. The evaluation results are provided in Table 5.
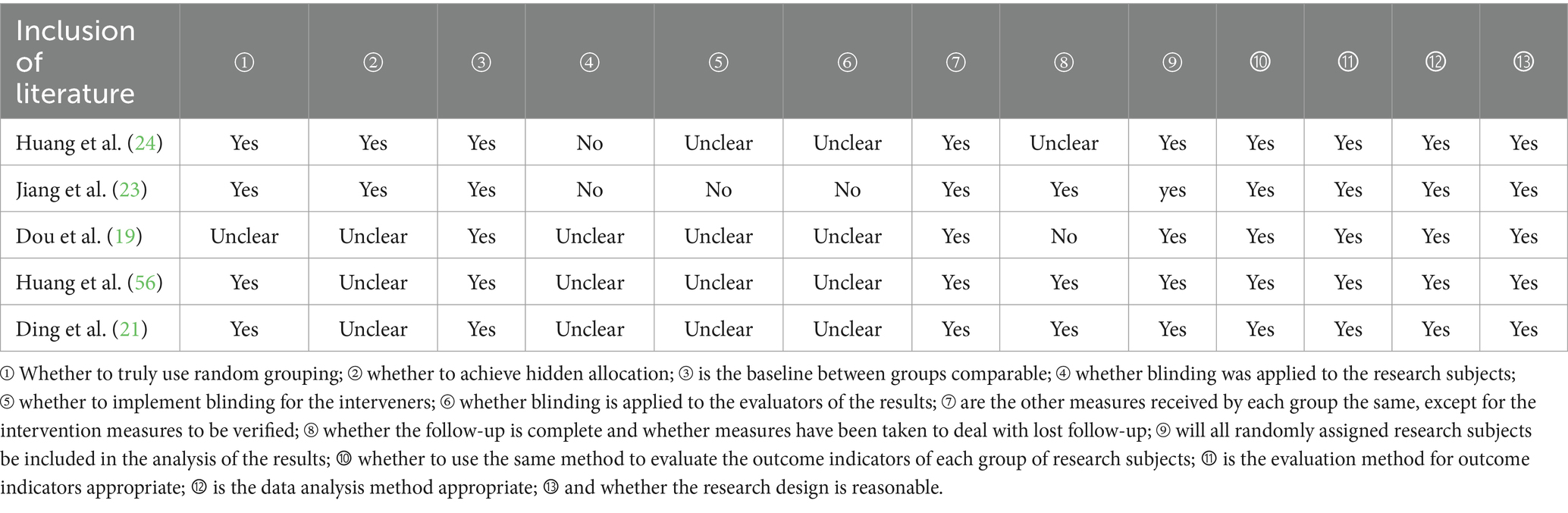
Table 5. Results of quality evaluation of randomized controlled trials.
Two quasi-experimental studies were included. Wang et al. (57) investigated the effects of parenteral glutamine supplementation on nasopharyngeal carcinoma patients undergoing concurrent radiotherapy, while Meng et al. (16) explored the effects of early nutritional intervention on nasopharyngeal cancer patients. Evaluation results are detailed in Table 6.
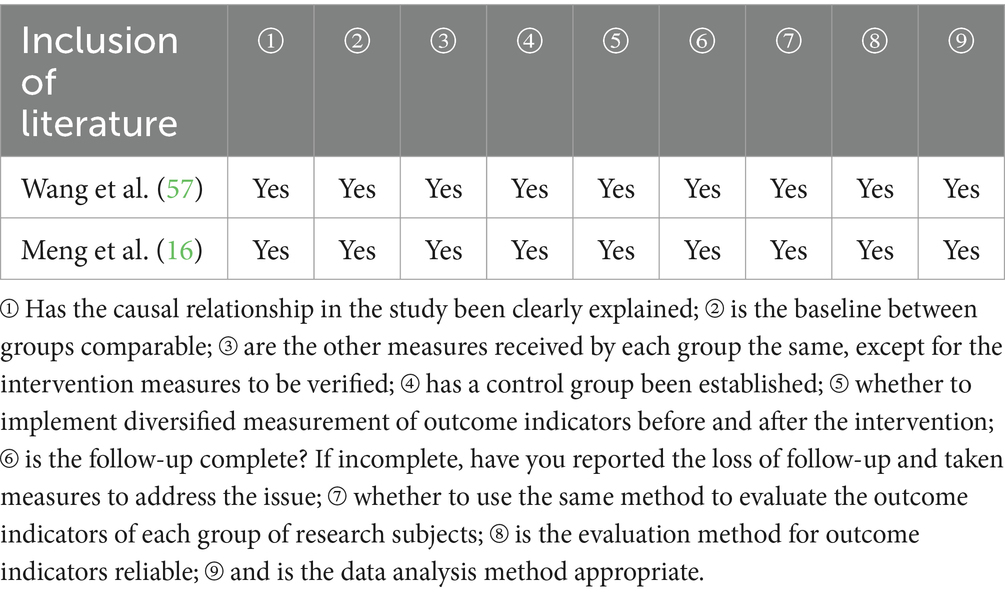
Table 6. Quality evaluation results of quasi-experiments.
Two observational studies were included. A study by Peng et al. (58) demonstrated the use of the NRS-2002 in the nutritional screening of nasopharyngeal cancer patients, and a study by Luo et al. (59) compared the value of the two nutritional screening tools in the nutritional assessment of nasopharyngeal cancer radiotherapy patients. The evaluation results are shown in Table 7.
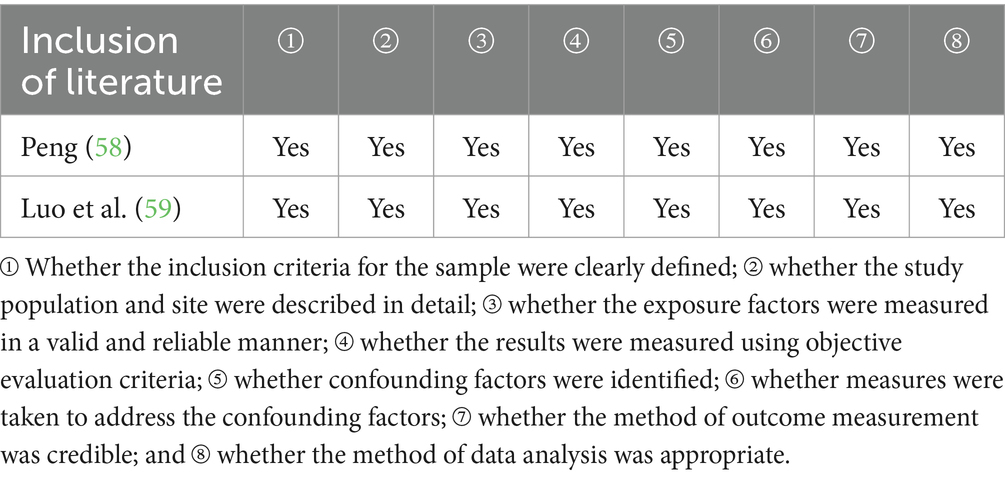
Table 7. Results of quality evaluation of observational studies.
We summarized the 60 pieces of best available evidence in 6 areas, namely, nutritional risk screening and assessment, nutrient requirements, nutritional support, nutritional symptom management, functional exercise, and nutritional monitoring and follow-up. The details are shown in Table 8.
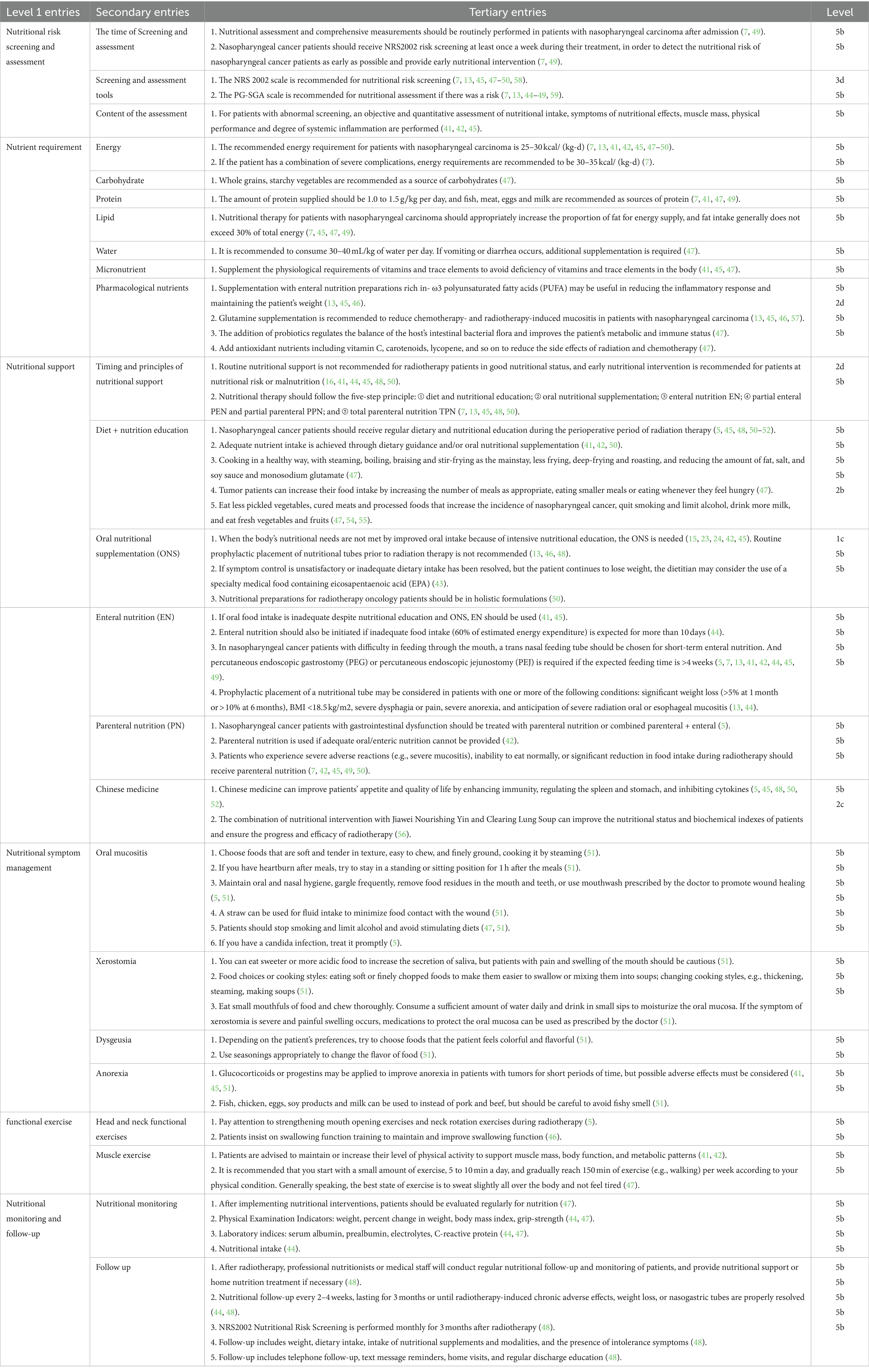
Table 8. Results of literature extraction and grading of evidence.
Nutritional risk screening and assessment involve three secondary entries and five tertiary entries. Both the consensus on nutritional support for nasopharyngeal carcinoma and the consensus on nutrition and supportive care for patients undergoing radiotherapy for head and neck tumors (7, 49) advocate for routine nutritional risk screening and assessment upon admission. The NRS2002 is recommended as a nutritional risk screening tool, while the PG-SGA is endorsed as an assessment tool. This recommendation is supported by multiple expert consensuses (7, 13, 47, 50) and guidelines (45). Furthermore, a large-scale cohort study (58) also suggested the use of NRS2002 as a nutritional risk screening tool for nasopharyngeal carcinoma patients. Patients with abnormalities should undergo timely, comprehensive assessments and early nutritional interventions (7, 49).
Nutrient requirements include seven secondary entries for energy, carbohydrates, proteins, fats, water, trace elements, and pharmacological nutrients, along with eleven tertiary entries. Nutrients serve as essential raw materials for sustaining organisms and are vital for ensuring proper nutrition. Several guidelines (41, 42, 45) and consensus documents (7, 13, 47–50) concur that the recommended energy intake for nasopharyngeal carcinoma patients ranges from 25 to 30 kcal/(kg·d). In cases of severe complications, the recommended energy intake increases to 30 to 35 kcal/(kg/d) (7). Additionally, recommendations for nutrient intake have been provided. Li et al. (47) outlined specific recommendations regarding food sources and cooking methods for proteins, carbohydrates, and other nutrients. Nutraceuticals such as glutamine and probiotics are also considered effective; Wang’s (57) findings suggest that parenteral supplementation of glutamine can mitigate side effects, thereby recommending it as a nutraceutical.
Nutritional support consists of six secondary entries and nineteen tertiary entries, covering topics like the timing and principles of nutritional support, diet and nutritional education, oral nutritional supplementation, enteral nutrition, parenteral nutrition, and traditional Chinese medicine. Patients undergoing radiation therapy for nasopharyngeal carcinoma should receive timely nutritional support if they are at risk of malnutrition (16, 41, 44, 45, 48, 50). An intervention study (16) demonstrated the beneficial effects of early nutritional intervention in maintaining patients’ nutritional status and improving treatment tolerance. Nutritional support follows a five-step treatment principle (7, 13, 45, 48, 50), including diet and nutritional education, oral nutritional supplements, enteral nutrition, and parenteral nutrition, as recommended by various guidelines and consensus documents. Diet and nutritional education are ongoing aspects of the nutritional support process, with regular provision of diet + nutritional education (5, 45, 48, 50–52). Oral intake is the simplest and most economical method. Emphasizing healthy cooking methods (47) and consuming small, frequent meals (47) is recommended for oral intake. Expert consensus (47) and two meta-analyses (54, 55) also suggest minimizing the consumption of pickled vegetables, cured meats, and processed foods. Oral nutritional supplements (ONS) are employed (23, 24, 42) when dietary intake and nutritional education are insufficient, supported by clinical evidence and guideline recommendations (42, 45). If ONS fails to meet nutritional needs, enteral nutrition (EN) is initiated, and if EN is inadequate, parenteral nutrition (PN) is considered. Additionally, in some studies, traditional Chinese medicine, an integral part of China’s medical heritage, has shown supportive effects in nutritional support for cancer patients (56).
Management of nutritional symptoms comprises four secondary symptoms: oral mucositis, dry mouth, taste disorders, and anorexia, along with twelve tertiary entries. Side effects induced by radiotherapy often disrupt patients’ nutritional intake, yet appropriate food choices and cooking methods can alleviate the impact of these symptoms. The expert consensus by Li et al. (51) offers detailed recommendations for preventing and treating nutritional symptoms.
Functional exercises include two secondary entries, head and neck functional exercises, and muscle exercises, along with four tertiary entries. Due to the potential stiffness of head and neck muscles induced by radiotherapy, patients are advised to incorporate exercises to strengthen neck-turning, mouth-opening (5), and swallowing (46). Furthermore, expert consensus (47) and guidelines (41, 42) suggest that encouraging patients to participate in suitable activities can improve bodily tolerance and facilitate nutrient absorption.
Nutritional monitoring and follow-up consist of two secondary entries and nine tertiary entries. Post-implementation of nutritional interventions, both guidelines (44) and consensus (47) advocate for regular monitoring of outcomes, including physical examination parameters, laboratory test results, and nutritional intake. Upon patient discharge, expert consensus (48) suggests follow-up by professional nutritionists or medical personnel every 2–4 weeks to assess the patient’s nutritional status. This can be achieved through various means, such as telephone follow-up, WeChat correspondence, or home visits.
Malnutrition is a prevalent issue among patients undergoing radiotherapy for nasopharyngeal carcinoma and is linked to adverse outcomes (54). Currently, there is a shortage of evidence-based strategies for providing nutritional support to these patients. To improve nutritional care for individuals undergoing radiotherapy for nasopharyngeal carcinoma, this study conducted an extensive literature review, evaluating the quality of available literature and summarizing evidence on six aspects of nutritional support programs: nutritional risk screening and assessment, nutrient requirements, nutritional support, nutritional symptom management, functional exercise, and nutritional monitoring and follow-up.
Patients diagnosed with nasopharyngeal carcinoma are at significant risk of malnutrition, with some already malnourished at the time of diagnosis. As treatment progresses, their nutritional status tends to worsen. Hence, early initiation of nutritional risk screening is crucial. Regular screenings not only detect high-risk individuals early but also enable timely nutritional support, reducing intolerance occurrences. This protocol outlines the timing, tools, and content for nutritional risk screening and assessment. Following guideline recommendations, we selected the NRS2002 (7, 13, 45, 47, 48, 50, 58, 60) for nutritional risk screening, scoring based on impaired nutritional status, disease severity, and age. For nutritional assessment, the PG-SGA is recommended (7, 13, 44–50, 59), comprising both patient-generated subjective global assessment and healthcare professionals’ evaluation (61). A meta-analysis comparing seven nutritional screening tools in cancer patients (62) revealed the PG-SGA’s superior sensitivity and predictive value, making it suitable for newly diagnosed cancer patients’ nutritional screening. Studies (63) have confirmed the NRS2002’s applicability for nutritional risk screening and the PG-SGA for nutritional assessment in nasopharyngeal carcinoma patients. While the NRS2002 and PG-SGA are widely used, other tools like MNA, MUST (64), and GLIM (12) can also serve for nutritional risk screening and assessment. As nutritional concerns gain prominence, body composition analyzers (65), CT, and metabolic carts are being employed for nutritional assessment, albeit at added costs. CT and MRI involve radiation, and operating metabolic carts could be complex. The NRS2002 and PG-SGA offer simplicity, high specificity, patient safety, and no added economic burden, making them suitable choices based on patients’ clinical circumstances.
Adequate nutritional substances are essential for patients undergoing radiotherapy for nasopharyngeal carcinoma, forming the foundation of nutritional support. This plan outlines the patient’s nutritional requirements and provides corresponding substance recommendations, including energy, carbohydrates, proteins, fats, water, trace nutrients, and pharmacologic nutrients. Proteins play a crucial role as the fundamental building blocks of life. Research (66) suggests that a diet rich in amino acids can delay the onset of sarcopenia in tumor patients undergoing radiotherapy and chemotherapy. Plant-derived fats, particularly unsaturated fatty acids, are preferred over saturated fatty acids. Two prospective cohort studies conducted in the United States (67) have demonstrated that substituting animal-sourced polyunsaturated fatty acids with plant-derived alternatives can reduce mortality rates. The addition of micronutrients such as glutamine, probiotics, and antioxidants is recommended to mitigate radiotherapy side effects. Studies indicate that parenteral glutamine supplementation can enhance energy intake in head and neck cancer patients (68) and decrease side effect incidence (40, 57, 69, 70). Probiotics have emerged as crucial players in tumor-patient immune regulation. A randomized controlled study indicated (71) that probiotics could lower Candida infections in head and neck cancer patients undergoing radiotherapy. Additionally, probiotics may reduce oral mucositis incidence by modulating immunity and gut microbiota (72–74). It has been indicated that probiotics and gut microbiota will likely become integral components of cancer prevention and treatment in the coming years (75). However, it is important to note that guidelines typically do not recommend routine pharmacologic nutrient supplementation. Clinical supplementation may be considered based on individual patient conditions.
The nutrition support section includes eight aspects: timing of nutritional support, principles of nutritional support, diet and nutrition education, ONS, TEN, PEN and PPN, TPN, and traditional Chinese medicine (TCM). Currently, our country’s focus on nutritional support is inadequate, leading to irregular applications of EN and PN. A nutritional support survey study involving 526 hospitalized cancer patients (76) revealed that among 245 patients scoring ≥3 on the NRS2002, the nutritional support rate was only 59.6%. Among them, 131 patients received PN, while only 15 patients were provided with EN, resulting in a parenteral to enteral nutrition ratio of 8.7:1. Hence, there is a pressing need to prioritize and standardize nutritional support. Early nutritional support should be promptly offered to patients at nutritional risk, while those without such risk may not require routine support. However, early support can help sustain the patient’s nutritional status and minimize side effects (16). Research also indicates that preemptive ONS can enhance tolerance to radiotherapy and chemotherapy (19). Therefore, whether to administer routine nutritional support to patients undergoing radiotherapy for nasopharyngeal carcinoma should be assessed based on individual circumstances and preferences. Tumor nutritional therapy adheres to the principle of frontline treatment, prioritizing diet, oral nutrition, nutrition education, and enteral nutrition, guided by a five-tier treatment approach (77). Additionally, TCM plays an active role in cancer adjuvant therapy (78), aiding in weight maintenance during radiotherapy (79), delaying oral mucositis onset (80), and enhancing quality of life (81). Studies (56) demonstrate that integrating Yangyin Qingfei Decoction with nutritional interventions can enhance patients’ nutritional status and biochemical indicators. Future endeavors should further advance TCM intervention research to explore the synergistic effects of TCM and Western medicine on cancer patients’ nutritional status.
In symptom management, guidelines and consensus offer recommendations for addressing conditions like oral mucositis, dry mouth, taste disturbances, and anorexia. Patients are advised to select suitable foods and employ appropriate cooking methods to alleviate symptoms. However, caution is advised when considering the use of glucocorticoids or progestogens to enhance appetite, given potential adverse reactions. Oral mucositis, closely linked to the patient’s nutritional status (8), has spurred considerable research into alleviation strategies. Honey (82–84), thalidomide (85), probiotics (72–74), and oral glutamine (70) have demonstrated efficacy in reducing oral mucositis. Taste disturbances, commonly reported post-radiation therapy, significantly impact patients’ quality of life (86). While options like radiation therapy mode, taste field dose distribution, and occlusal blocks may prove effective, current evidence remains inconclusive, necessitating further investigation.
As a result of radiotherapy’s adverse effects, patients often face challenges such as limited mouth opening and swallowing difficulties post-treatment. Hence, engaging in functional exercises becomes crucial. Alongside exercises targeting mouth and neck mobility to maintain oral and pharyngeal function, it is vital to gradually introduce whole-body muscle training to enhance overall physical health and resilience against illnesses. Studies suggest that multimodal exercise regimens can improve the physical well-being of nasopharyngeal cancer patients undergoing radiotherapy (87). Additionally, practices like the Eight-Section Brocade have shown promise in enhancing patients’ quality of life (88), while Tai Chi has demonstrated efficacy in alleviating tumor-related fatigue (89).
Following nutritional support, it is essential to conduct regular nutritional assessments, including physical examination indicators, laboratory parameters, and dietary intake. Based on the evaluation outcomes, adjustments to the nutritional support regimen can be made promptly. Upon discharge, dedicated professionals should conduct regular follow-ups with the patient. A customized follow-up strategy can be devised to address the patient’s specific nutritional concerns promptly and offer appropriate guidance.
This study aimed to consolidate the most reliable evidence on nutritional support for patients undergoing radiotherapy for nasopharyngeal carcinoma, intending to furnish a comprehensive blueprint for clinical nutritional intervention. However, since factors like hospital resources, patient preferences, financial capabilities, insurance coverage, and cultural beliefs can influence the implementation of such schemes, future endeavors should incorporate real-world clinical insights. Consulting expert opinions will be pivotal in refining nutritional support strategies for these patients. Furthermore, clinical validation of these interventions is imperative to enhance patient nutrition, improve treatment endurance, and diminish side effects.
Although this study provides evidence of nutritional support for patients with nasopharyngeal carcinoma undergoing radiotherapy, factors such as regional, ethnic, and cultural differences may affect the results. In addition, this study only searched for the literature in Chinese and English. Future updates should continuously update the data, explore the applicability and feasibility of the evidence, be combined with clinical updates, and promote the application of evidence in the clinic.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
XF: Conceptualization, Investigation, Methodology, Resources, Writing – original draft, Writing – review & editing. HC: Conceptualization, Funding acquisition, Methodology, Supervision, Validation, Writing – original draft, Writing – review & editing. SL: Data curation, Formal analysis, Supervision, Validation, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the Wannan Medical College under grant (number WYRCQD2023043).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Chen, YP, Chan, ATC, le, QT, Blanchard, P, Sun, Y, and Ma, J. Nasopharyngeal carcinoma. Lancet (London, England). (2019) 394:64–80. doi: 10.1016/s0140-6736(19)30956-0
2. Zhou, ZL, Li, KP, Li, NN, and Zhou, RZ. Age period cohort analysis of incidence and mortality trends of nasopharyngeal carcinoma in the Chinese population, 1994-2019. Chin J Dis Control Prev. (2023) 27:869–876+894. doi: 10.16462/j.cnki.zhjbkz.2023.08.001
3. Wang, L, Zhang, YX, Yang, L, Shen, WY, Liao, XZ, and Rang, WQ. Incidence and mortality of nasopharyngeal carcinoma in China's tumor registration areas,2005-2013. Pract Prev Med. (2020) 27:145–9.
4. Tang, LL, Chen, YP, Chen, CB, Chen, MY, Chen, NY, Chen, XZ, et al. The Chinese Society of Clinical Oncology (CSCO) clinical guidelines for the diagnosis and treatment of nasopharyngeal carcinoma. Cancer Commun. (2021) 41:1195–227. doi: 10.1002/cac2.12218
5. Kang, M . Chinese guidelines for radiotherapy of nasopharyngeal Cancer (2022 edition). Chin J Cancer Prev Treat. (2022) 29:611–22. doi: 10.16073/j.cnki.cjcpt.2022.09.01
6. Liu, T, and Liu, LP. Nutrition related symptoms and dietary interference in head and neck cancer patients on radiotherapy:a longitudinal study[J]. J Nurs Sci. (2022) 37:88–93.
7. Li, W . Expert opinion on nutritional treatment for patients with nasopharyngeal carcinoma. Electron J Metab Nutr Cancer. (2021) 8:600–4.
8. Shu, Z, Zeng, Z, Yu, B, Huang, S, Hua, Y, Jin, T, et al. Nutritional status and its association with radiation-induced Oral Mucositis in patients with nasopharyngeal carcinoma during radiotherapy: a prospective study. Front Oncol. (2020) 10:594687. doi: 10.3389/fonc.2020.594687
9. Zhuang, B, Zhang, LC, Wang, YJ, Zhang, T, Jin, SL, Gong, LQ, et al. Malnutrition and its relationship with nutrition impact symptoms and quality of life at the end of radiotherapy in patients with head and neck cancer. Chinese J Clin Nutr. (2020) 28:207–13. doi: 10.3760/cma.j.cn115822-20200723-00184
10. Wei, XY, Li, Y, and Hu, DS. Nutritional status and its influencing factors of nasopharyngeal carcinoma patients during Chemoradiotherapy. Cancer Res Prev Treat. (2020) 47:524–30. doi: 10.3971/j.issn.1000-8578.2020.20.0280
11. Hong, JS, Wu, LH, Su, L, Zhang, HR, Lv, WL, Zhang, WJ, et al. Effect of chemoradiotherapy on nutrition status of patients with nasopharyngeal cancer. Nutr Cancer. (2016) 68:63–9. doi: 10.1080/01635581.2016.1115099
12. Wan, M, Zhang, L, Chen, C, Zhao, D, Zheng, B, Xiao, S, et al. GLIM criteria-defined malnutrition informs on survival of nasopharyngeal carcinoma patients undergoing radiotherapy. Nutr Cancer. (2022) 74:2920–9. doi: 10.1080/01635581.2022.2044059
13. Li, T, Lv, JH, and Shi, HP. Expert consensus on nutrition therapy for radiotherapy patients. Electron J Metab Nutr Cancer. (2021) 8:29–34.
14. Wang, X, Yang, M, Ge, YZ, Tang, M, Rao, BQ, Chen, YB, et al. Association of systemic inflammation and malnutrition with survival in nasopharyngeal carcinoma undergoing Chemoradiotherapy: results from a multicenter cohort study. Front Oncol. (2021) 11:10. doi: 10.3389/fonc.2021.766398
15. Su, L, Lin, QJ, Li, R, Hua, YJL, Zhang, HR, Song, XR, et al. Prognostic value of nutritional impairment on treatment-related toxicity and survival in patients with nasopharyngeal carcinoma taking normal nutrition before radiotherapy. Head Neck. (2020) 42:3580–9. doi: 10.1002/hed.26426
16. Meng, L, Wei, J, Ji, R, Wang, B, Xu, X, Xin, Y, et al. Effect of early nutrition intervention on advanced nasopharyngeal carcinoma patients receiving Chemoradiotherapy. J Cancer. (2019) 10:3650–6. doi: 10.7150/jca.33475
17. Yi, HZ, and Chen, JJ. The influence of early full nutritional intervention on patients with locally advanced nasopharyngeal carcinoma with concurrent chemoradiotherapy. Modern Oncology. (2020) 28:2038–42. doi: 10.3969/j.issn.1672-4992.2020.12.009
18. Liao, TT, and Yang, L. Research progress on the effect of early nutrition intervention on prognosis of patients with nasopharyngeal carcinoma after radiochemotherapy. J Nurs Adm. (2019) 19:2020226430:48–52.
19. Dou, S, Ding, H, Jiang, W, Li, R, Qian, Y, Wu, S, et al. Effect of oral supplements on the nutritional status of nasopharyngeal carcinoma patients undergoing concurrent chemotherapy: a randomized controlled phase II trial. J Cancer Res Ther. (2020) 16:1678–85. doi: 10.4103/jcrt.JCRT_273_20
20. Chen, YY, Huang, S, Hu, QY, Hua, YH, Jiang, F, Cao, CN, et al. The impact of oral nutritional supplements in the local advanced nasopharyngeal carcinoma patients receiving chemoradiotherapy. Chin J Radiation Oncol. (2019) 8:575–9. doi: 10.3760/cma.j.issn.1004-4221.2019.08.004
21. Ding, HP, Dou, SJ, Wang, Q, Wu, Y, Qian, Y, Zhu, GP, et al. Effect of oral nutritional supplements on nutritional status and quality of life in patients with nasopharyngeal carcinoma receiving chemoradiotherapy. China Oncol. (2018) 28:62–8. doi: 10.19401/j.cnki.1007-3639.2018.01.009
22. Wang, D, and Hu, QC. Effects of oral nutrition support on nutritional status, immune function and radiation damage in patients with nasopharyngeal carcinoma radiotherapy. J Hainan Med Univ. (2018) 24:953–6. doi: 10.13210/j.cnki.jhmu.20180411.005
23. Jiang, W, Ding, H, Li, W, Ling, Y, Hu, C, and Shen, C. Benefits of Oral nutritional supplements in patients with locally advanced nasopharyngeal Cancer during concurrent Chemoradiotherapy: an exploratory prospective randomized trial. Nutr Cancer. (2018) 70:1299–307. doi: 10.1080/01635581.2018.1557222
24. Huang, S, Piao, Y, Cao, C, Chen, J, Sheng, W, Shu, Z, et al. A prospective randomized controlled trial on the value of prophylactic oral nutritional supplementation in locally advanced nasopharyngeal carcinoma patients receiving chemo-radiotherapy. Oral Oncol. (2020) 111:105025. doi: 10.1016/j.oraloncology.2020.105025
25. Li, X, Zhou, J, Chu, C, You, Q, Zhong, R, Rao, Z, et al. Home enteral nutrition may prevent myelosuppression of patients with nasopharyngeal carcinoma treated by concurrent chemoradiotherapy. Head Neck. (2019) 41:3525–34. doi: 10.1002/hed.25861
26. Blake, CL, Brown, TE, Pelecanos, A, Moroney, LB, Helios, J, Hughes, BGM, et al. Enteral nutrition support and treatment toxicities in patients with head and neck cancer receiving definitive or adjuvant helical intensity-modulated radiotherapy with concurrent chemotherapy. Head Neck. (2023) 45:417–30. doi: 10.1002/hed.27249
27. Ji, J, Zhu, H, Zhang, MX, Xu, XT, Jiang, DD, Xu, Z, et al. Individualized whole course nutrition Management for Nasopharyngeal Carcinoma Patients Undergoing Radiotherapy [article]. Clin Lab. (2022) 68:1120–30. doi: 10.7754/Clin.Lab.2021.210459
28. Lu, DS, Feng, YJ, Wang, WS, Mu, ZL, and Zhao, N. Influence of individualized nutrition intervention on quality of life and survival prognosis of patients with locally advanced nasopharyngeal carcinoma. China Oncol. (2021) 31:1202–8. doi: 10.19401/j.cnki.1007-3639.2021.12.008
29. Li, L, Liu, X, Chen, ZYY, and Han, XP. Application of individualized nutrition intervention to patients undergoing radiotherapy for head and neck malignant tumors. J North Sichuan Med College. (2021) 36:530–3. doi: 10.3969/j.issn.1005-3697.2021.03.029
30. Wang, L, Li, R, and Xiong, WJ. Effects of individualized nutritional support on nutritional related indicators in patients with nasopharyngeal carcinoma undergoing concurrent chemoradiotherapy: a Meta-analysis. Modern Prev Med. (2019) 46:1898–903.
31. Li, J, and Han, R. Nusing effect observation of whole course nutrition nursing management on nasopharyngeal carcinoma patients undergoing radiotherapy and its impact on quality of life. J North Sichuan Med Coll. (2020) 35:535–7. doi: 10.3969/j.issn.1005-3697.2020.03.046
32. Cao, YD, Sun, XC, and Tang, XY. Effect of whole course nutrition support on the acute radiation response and treatment compliance of nasopharyngeal carcinoma. Chin Clin Oncol. (2016) 21:349–52.
33. Wei, XY, Han, G, Li, Y, and Hu, DS. Effect of whole-course nutrition support on nutritional status of patients with locally advanced nasopharyngeal carcinoma. Cancer Res Prev Treat. (2020) 47:617–22. doi: 10.3971/j.issn.1000-8578.2020.20.0432
34. Huang, JF, Sun, RJ, Jiang, WJ, Wu, P, Zhang, L, Xu, MQ, et al. Systematic nutrition management for locally advanced nasopharyngeal carcinoma patients undergoing radiotherapy. Onco Targets Ther. (2019) 12:8379–86. doi: 10.2147/ott.S213789
35. Zeng, X, Huang, X, Wang, P, Liao, J, Wu, L, Liu, J, et al. The application of the PDCA cycle in the nutritional management of patients with nasopharyngeal carcinoma. Support Care Cancer. (2023) 31:251. doi: 10.1007/s00520-023-07724-4
36. Wei, YP, Chen, LY, Wu, QZ, and Du, J. Research on cluster Management in Nutritional Intervention for nasopharynx Cancer patients undergoing intensity modulated radiation therapy. West China Med J. (2016) 31:1258–61. doi: 10.7507/1002-0179.201600342
37. Qu, NN, and Yao, Y. The effect of bundled nursing intervention on the nutritional status and self-efficacy of nasopharyngeal carcinoma radiotherapy patients. J Shenyang Pharma Univ. (2021) 38:83.
38. Qiao, H, Chen, PJ, Wang, L, and Li, Q. Influence of ONScompliance and quality of life ofmulti-disciplinary mode on the patients with nasopharyngeal carcinoma. Parent Enteral Nutr. (2018) 25:337–41. doi: 10.16151/j.1007-810x.2018.11.004
39. Xia, LJ, Zhang, X, Liu, S, Shi, XQ, Ma, ZF, Min, J, et al. Nurse-led multidisciplinary nutritional support for patients with nasopharyngeal carcinoma undergoing concurrent radiochemotherapy. J Nurs Sci. (2021) 36:82–5. doi: 10.3870/j.issn.1001-4152.2021.04.082
40. Yuce Sari, S, Yazici, G, Yuce, D, Karabulut, E, Cengiz, M, and Ozyigit, G. The effect of glutamine and arginine-enriched nutritional support on quality of life in head and neck cancer patients treated with IMRT. Clin Nutr ESPEN. (2016) 16:30–5. doi: 10.1016/j.clnesp.2016.08.003
41. Muscaritoli, M, Arends, J, Bachmann, P, Baracos, V, Barthelemy, N, Bertz, H, et al. ESPEN practical guideline: Clinical nutrition in cancer. Clin Nutr. (2021) 40:2898–913. doi: 10.1016/j.clnu.2021.02.005
42. de Las, PR, Majem, M, Perez-Altozano, J, Virizuela, JA, Cancer, E, Diz, P, et al. SEOM clinical guidelines on nutrition in cancer patients (2018). Clin Transl Oncol. (2019) 21:87–93. doi: 10.1007/s12094-018-02009-3
43. Thompson, KL, Elliott, L, Fuchs-Tarlovsky, V, Levin, RM, Voss, AC, and Piemonte, T. Oncology evidence-based nutrition practice guideline for adults. J Acad Nutr Diet. (2017) 117:297–310 e47. doi: 10.1016/j.jand.2016.05.010
44. Talwar, B, Donnelly, R, Skelly, R, and Donaldson, M. Nutritional management in head and neck cancer: United Kingdom National Multidisciplinary Guidelines. J Laryngol Otol. (2016) 130:S32–40. doi: 10.1017/S0022215116000402
45. Chinese Society for Parenteral and Enteral Nutrition . Guidelines on nutritional support in patients with tumor. Chin J Surg. (2017) 55:801–29. doi: 10.3760/cma.j.issn.0529-5815.2017.11.001
46. Lin, MC, Shueng, PW, Chang, WK, Mu-Hsin Chang, P, Feng, HC, Yang, MH, et al. Consensus and clinical recommendations for nutritional intervention for head and neck cancer patients undergoing chemoradiotherapy in Taiwan. Oral Oncol. (2018) 81:16–21. doi: 10.1016/j.oraloncology.2018.03.016
47. Li, ZL, Chen, W, Qi, YM, Hu, W, Ge, S, Zhou, CL, et al. Dietary nutrition prescription for cancer patients. Electron J Metab Nutr Cancer. (2017) 4:397–408.
48. Branch of Radiation Oncology of Chinese Medical Association . Expert consensus on standardized management of radiotherapy nutrition. Chin J Radiat Oncol. (2020) 29:324–31. doi: 10.3760/cma.j.cn113030-20191212-00002
49. Cancer Radiotherapy Nutrition Group, Cancer Nutrition and Support Committee of China, China . Anti⁃cancer association. Expert consensus on nutrition support therapy for head and neck cancer patients receiving radiotherapy. Chin J Radiat Oncol. (2018) 27:1–6. doi: 10.3760/cma.j.issn.1004-4221.2018.01.001
50. China Society for Radiation Oncology . Oral nutrition supplements consensus for cancer patients undergoing radiotherapy (2017). Chin J Radiat Oncol. (2017) 26:1239–47. doi: 10.3760/cma.j.issn.1004-4221.2017.11.001
51. Li, ZL, Li, XL, Chen, W, Qi, YM, Hu, W, Ge, S, et al. Expert consensus on appetite assessment and regulation in cancer patients. Electron J Metab Nutr Cancer. (2020) 7:169–77. doi: 10.16689/j.cnki.cn11-9349/r.2020.02.007
52. Langius, JA, Zandbergen, MC, Eerenstein, SE, van Tulder, MW, Leemans, CR, Kramer, MH, et al. Effect of nutritional interventions on nutritional status, quality of life and mortality in patients with head and neck cancer receiving (chemo)radiotherapy: a systematic review. Clin Nutr. (2013) 32:671–8. doi: 10.1016/j.clnu.2013.06.012
53. Mello, AT, Borges, DS, de Lima, LP, Pessini, J, Kammer, PV, and Trindade, E. Effect of oral nutritional supplements with or without nutritional counselling on mortality, treatment tolerance and quality of life in head-and-neck cancer patients receiving (chemo)radiotherapy: a systematic review and meta-analysis. Br J Nutr. (2021) 125:530–47. doi: 10.1017/S0007114520002329
54. Feng, H, Zhou, Y, Wang, L, Wang, Y, Zhou, S, and Tian, F. Consumption of processed food and risk of nasopharyngeal carcinoma: a systematic review and meta-analysis. Transl Cancer Res. (2022) 11:872–9. doi: 10.21037/tcr-22-690
55. Chen, YY, Qiao, L, Li, B, Liu, XX, Zhao, YJ, Ma, Q, et al. Relationship of diet and lifestyle with the risk of nasopharyngeal carcinoma among Chinese population:a Meta-analysis. J Prev Med Inf. (2020) 36:399–405.
56. Huang, J, Shen, HM, and Wu, YL. Effect of modified Yangyin Qingfei decoction combined with nutritional intervention on nutritional status and curative effect of nasopharyngeal carcinoma patients undergoing radiotherapy. Cancer Res Prev Treat. (2019) 46:159–63. doi: 10.3971/j.issn.1000-8578.2019.18.0814
57. Wang, CC, Hwang, TZ, Yang, CC, Lien, CF, Wang, CC, Shih, YC, et al. Impact of parenteral glutamine supplement on oncologic outcomes in patients with nasopharyngeal Cancer treated with concurrent Chemoradiotherapy. Nutrients. (2022) 14:997. doi: 10.3390/nu14050997
58. Peng, H, Chen, BB, Tang, LL, Chen, L, Li, WF, Zhang, Y, et al. Prognostic value of nutritional risk screening 2002 scale in nasopharyngeal carcinoma: a large-scale cohort study [article]. Cancer Sci. (2018) 109:1909–19. doi: 10.1111/cas.13603
59. Luo, Q, Shen, M, and Chen, JF. The value of two nutritional screening tools in nutritional assessment of patients with nasopharyngeal carcinoma undergoing radiotherapy and their correlation with cancer related fatigue. Chin Nurs Res. (2021) 35:1751–6.
60. Kondrup, J, Allison, SP, Elia, M, Vellas, B, and Plauth, M. ESPEN guidelines for nutrition screening 2002. Clin Nutr. (2003) 22:415–21. doi: 10.1016/S0261-5614(03)00098-0
61. Ottery, FD . Rethinking nutritional support of the cancer patient: the new field of nutritional oncology. Semin Oncol. (1994) 21:770–8. doi: 10.1016/0167-8140(94)90364-6
62. Lin, LY, Xu, CL, Zhang, X, and Zhuang, PP. Huang YX.A network meta-analysis of 7 nutritional screening tools on accuracy of nutritional screening in cancer patients. J Nurs Sci. (2022) 37:92–6. doi: 10.3870/j.issn.1001-4152.2022.12.092
63. Pan, XX, Wang, CH, Li, R, Su, L, Zhang, MW, Cai, CS, et al. Applicability of the nutrition risk screening 2002 combined with a patient-generated subjective global assessment in patients with nasopharyngeal carcinoma. Cancer Manag Res. (2020) 12:8221–7. doi: 10.2147/cmar.S261945
64. Hsueh, SW, Lai, CC, Hung, CY, Lin, YC, Lu, CH, Yeh, KY, et al. A comparison of the MNA-SF, MUST, and NRS-2002 nutritional tools in predicting treatment incompletion of concurrent chemoradiotherapy in patients with head and neck cancer. Support Care Cancer. (2021) 29:5455–62. doi: 10.1007/s00520-021-06140-w
65. Xu, H, Zhou, JY, Ji, J, Qian, KY, and Yao, YM. Exploration of predicting the nutritional status of nasopharyngeal carcinoma patients during radiotherapy using human body composition and blood biochemical indicators. Chinese J Hemorheol. (2021) 31:370–3. doi: 10.3969/j.issn.1009-881X.2021.03.018
66. Ishikawa, T, Yasuda, T, Doi, T, Okayama, T, Sakamoto, N, Gen, Y, et al. The amino acid-rich elemental diet Elental® preserves lean body mass during chemo- or chemoradiotherapy for esophageal cancer. Oncol Rep. (2016) 36:1093–100. doi: 10.3892/or.2016.4877
67. Guasch-Ferré, M, Zong, G, Willett, WC, Zock, PL, Wanders, AJ, Hu, FB, et al. Associations of monounsaturated fatty acids from plant and animal sources with Total and cause-specific mortality in two US prospective cohort studies. Circ Res. (2019) 124:1266–75. doi: 10.1161/CIRCRESAHA.118.313996
68. Shono, H, Tsutsumi, R, Beppu, K, Matsushima, R, Watanabe, S, Fujimoto, C, et al. Dietary supplementation with monosodium glutamate suppresses chemotherapy-induced downregulation of the T1R3 taste receptor subunit in head and neck Cancer patients. Nutrients. (2021) 13:2921. doi: 10.3390/nu13092921
69. Vidal-Casariego, A, Calleja-Fernández, A, Ballesteros-Pomar, MD, and Cano-Rodríguez, I. Efficacy of glutamine in the prevention of oral mucositis and acute radiation-induced esophagitis: a retrospective study. Nutr Cancer. (2013) 65:424–9. doi: 10.1080/01635581.2013.765017
70. Pachón Ibáñez, J, Pereira Cunill, JL, Osorio Gómez, GF, Irles Rocamora, JA, Serrano Aguayo, P, Quintana Ángel, B, et al. Prevention of oral mucositis secondary to antineoplastic treatments in head and neck cancer by supplementation with oral glutamine. Nutricion Hospitalaria. (2018) 35:428–33. doi: 10.20960/nh.1467
71. Doppalapudi, R, Vundavalli, S, and Prabhat, MP. Effect of probiotic bacteria on oral Candida in head- and neck-radiotherapy patients: a randomized clinical trial. J Cancer Res Ther. (2020) 16:470–7. doi: 10.4103/jcrt.JCRT_334_18
72. Xia, C, Jiang, C, Li, W, Wei, J, Hong, H, Li, J, et al. A phase II randomized clinical trial and mechanistic studies using improved probiotics to prevent Oral Mucositis induced by concurrent radiotherapy and chemotherapy in nasopharyngeal carcinoma. Front Immunol. (2021) 12:618150. doi: 10.3389/fimmu.2021.618150
73. Das, M . Probiotics for chemoradiotherapy-induced oral mucositis. Lancet Oncol. (2019) 20:e14. doi: 10.1016/S1470-2045(18)30919-7
74. Jiang, C, Wang, H, Xia, C, Dong, Q, Chen, E, Qiu, Y, et al. A randomized, double-blind, placebo-controlled trial of probiotics to reduce the severity of oral mucositis induced by chemoradiotherapy for patients with nasopharyngeal carcinoma. Cancer. (2019) 125:1081–90. doi: 10.1002/cncr.31907
75. Górska, A, Przystupski, D, Niemczura, MJ, and Kulbacka, J. Probiotic Bacteria: a promising tool in Cancer prevention and therapy. Curr Microbiol. (2019) 76:939–49. doi: 10.1007/s00284-019-01679-8
76. Chang, Y, Zhang, Q, Fan, RX, and Huang, J. Research of nutritional risk, nutritional support and its relationship to clinical outcomes in patients with cancer. Parent Enteral Nutr. (2016) 23:71–73+77. doi: 10.16151/j.1007-810x.2016.02.002
77. Wang, L, Cong, MH, Cui, JW, Xu, HX, Chen, JQ, Li, T, et al. The basic principles of nutritional therapy for tumors. Electron J Metab Nutr Cancer. (2022) 9:727–34. doi: 10.16689/j.cnki.cn11-9349/r.2022.06.008
78. Zhang, X, Qiu, H, Li, C, Cai, P, and Qi, F. The positive role of traditional Chinese medicine as an adjunctive therapy for cancer. Biosci Trends. (2021) 15:283–98. eng. Epub 2021/08/24. doi: 10.5582/bst.2021.01318
79. Huang, YH, Chen, JL, Yang, SH, Liu, GH, Chang, KP, and Tsang, NM. Influence of Chinese medicine on weight loss and quality of life during radiotherapy in head and neck cancer. Integr Cancer Ther. (2013) 12:41–9. doi: 10.1177/1534735412443852
80. Wu, YF, and Fang, HB. Effect of Chinese comprehensive nursing on Oral Mucositis in patients undergoing radiotherapy for nasopharyngeal carcinoma. J New Chin Med. (2020) 52:147–50. doi: 10.13457/j.cnki.jncm.2020.11.042
81. Shao, JQ, Shen, HF, and Yu, P. Effect of integrated prevention and treatment in Chinese medicine on quality of life in patients undergoing radiotherapy for head and neck Cancer. J New Chin Med. (2020) 52:157–60. doi: 10.13457/j.cnki.jncm.2020.14.045
82. Charalambous, M, Raftopoulos, V, Paikousis, L, Katodritis, N, Lambrinou, E, Vomvas, D, et al. The effect of the use of thyme honey in minimizing radiation—induced oral mucositis in head and neck cancer patients: a randomized controlled trial. Europ J Oncol Nurs. (2018) 34:89–97. doi: 10.1016/j.ejon.2018.04.003
83. Jicman Stan, D, Sârbu, MI, Fotea, S, Nechifor, A, Bălan, G, Anghele, M, et al. Oral Mucositis induced by Chemoradiotherapy in head and neck Cancer-a short review about the therapeutic management and the benefits of bee honey. Medicina (Kaunas). (2022) 58:751. doi: 10.3390/medicina58060751
84. Hawley, P, Hovan, A, McGahan, CE, and Saunders, D. A randomized placebo-controlled trial of manuka honey for radiation-induced oral mucositis. Support Care Cancer. (2014) 22:751–61. doi: 10.1007/s00520-013-2031-0
85. Liang, L, Liu, Z, Zhu, H, Wang, H, Wei, Y, Ning, X, et al. Efficacy and safety of thalidomide in preventing oral mucositis in patients with nasopharyngeal carcinoma undergoing concurrent chemoradiotherapy: a multicenter, open-label, randomized controlled trial. Cancer. (2022) 128:1467–74. doi: 10.1002/cncr.34074.C
86. Gunn, L, Gilbert, J, Nenclares, P, Soliman, H, Newbold, K, Bhide, S, et al. Taste dysfunction following radiotherapy to the head and neck: a systematic review. Radiother Oncol. (2021) 157:130–40. doi: 10.1016/j.radonc.2021.01.021
87. Song, J, Wu, Z, Fang, Y, Li, R, Chuang, Y, Wang, W, et al. Effects of multimodal exercise on health-related physical fitness and quality of life in patients with nasopharyngeal carcinoma during radiotherapy. Pain Manag Nurs. (2023) 24:650–8. doi: 10.1016/j.pmn.2023.04.007
88. Wen, L, Chen, X, Cui, Y, Zhang, M, and Bai, X. Effects of Baduanjin exercise in nasopharyngeal carcinoma patients after chemoradiotherapy: a randomized controlled trial. Support Care Cancer. (2022) 31:79. doi: 10.1007/s00520-022-07548-8
Keywords: radiotherapy, nutritional support, evidence-based nursing, nasopharyngeal carcinoma, summary of evidence
Citation: Fan X, Cui H and Liu S (2024) Summary of the best evidence for nutritional support programs in nasopharyngeal carcinoma patients undergoing radiotherapy. Front. Nutr. 11:1413117. doi: 10.3389/fnut.2024.1413117
Edited by:
Antonio Moschetta, University of Bari Aldo Moro, ItalyReviewed by:
Radha Vaddavalli, The Ohio State University, United StatesCopyright © 2024 Fan, Cui and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence:Huixia Cui, MTMxOTQ0NzM2N0BxcS5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.