 Hongquan Zhang
Hongquan Zhang Lizhuo Zhao3
Lizhuo Zhao3
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Nutr., 03 June 2024
Sec. Clinical Nutrition
Volume 11 - 2024 | https://doi.org/10.3389/fnut.2024.1370286
Nutritional support is crucial for the prognosis of children supported by extracorporeal membrane oxygenation (ECMO). This article discusses the latest research progress and guideline recommendations for nutritional support during ECMO. We summarize the nutritional status and evaluation of ECMO patients, nutritional support methods and timing, trace elements, the impact of continuous renal replacement therapy (CRRT), and energy requirements and algorithms. The article shows that malnutrition is high in ECMO patients compared to other critically ill patients, with nearly one-third of patients experiencing a decrease in nutritional indicators. The timing of the initiation of nutrition is very important for the nutritional status of the child. Early enteral nutrition can improve patient prognosis, which is the most commonly used, with parenteral nutrition as a supplement. However, the proportion of enteral nutrition is relatively low, and a stepwise nutrition algorithm can determine when to initiate early enteral nutrition and parenteral nutrition. Malnourishment during critical illness have been associated with increased morbidity as well as increased mortality. Nutritional status should be evaluated at admission by screening tools. In addition, changes in the levels of several metabolites in vivo, such as blood lipids, carnitine, and thiamine, can also reflect the degree of nutritional deficiency in critically ill children. This article provides a reference for the implementation of nutrition of pediatric ECMO patients and further research on nutritional support.
Extracorporeal membrane oxygenation (ECMO) is an advanced technology that is used to temporarily replace cardiac or pulmonary functions and buy time for the treatment of the underlying disease. The nutritional status of pediatric ECMO patients has a significant impact on prognosis. Proper nutritional support can influence treatment outcomes and prognosis of these children. Critically ill infants and children undergoing ECMO treatment are nutritionally vulnerable, and providing adequate nutrition is essential because it has a beneficial impact on outcomes. There is no clear consensus about the optimal approach to nutritional prescribing for these patients (1). We conducted a systematic review to mainly determine whether EN and PN is effective and its association with rates of complications and mortality in critically ill neonatal and pediatric populations supported by ECMO. In short, this article provides the existing evidence of the research progress on the nutritional status of pediatric ECMO patients during treatment, methods and timing of nutrition, complications, calculation of nutrition, as well as the indicators for nutritional metabolism. These findings can provide valuable insights for the nutritional management of pediatric ECMO patients.
The literature review was organized according to the Preferred Reporting Items for Systematic Review and Meta-Analysis 2020 guidelines (2) (Figure 1).

Figure 1. Preferred reporting items for systematic review and meta-analysis (PRISMA) flow diagram for review.
Studies that evaluated EN and PN in neonates and pediatric patients on ECMO were conducted. The studies also had to report either complications or mortality related to EN and PN.
The databases used in this literature review were MEDLINE, Web of Science (WOS), and the Cochrane Library database with the search terms ([Extracorporeal membrane oxygenation or ECMO or Extracorporeal Life Support or ECLS] AND [enteral nutrition or nasal feed* or tube feed* or gastric tube feed*] AND [parenteral nutrition] AND [pediatric or pediatric or child* or infant* or neonatal or newborn]) from inception to April 2024, with English language restrictions. The reference lists of reports that were potentially relevant were also searched to identify additional studies. After applying the exclusion criteria, there were a total of 10 studies that met the inclusion criteria (Table 1).
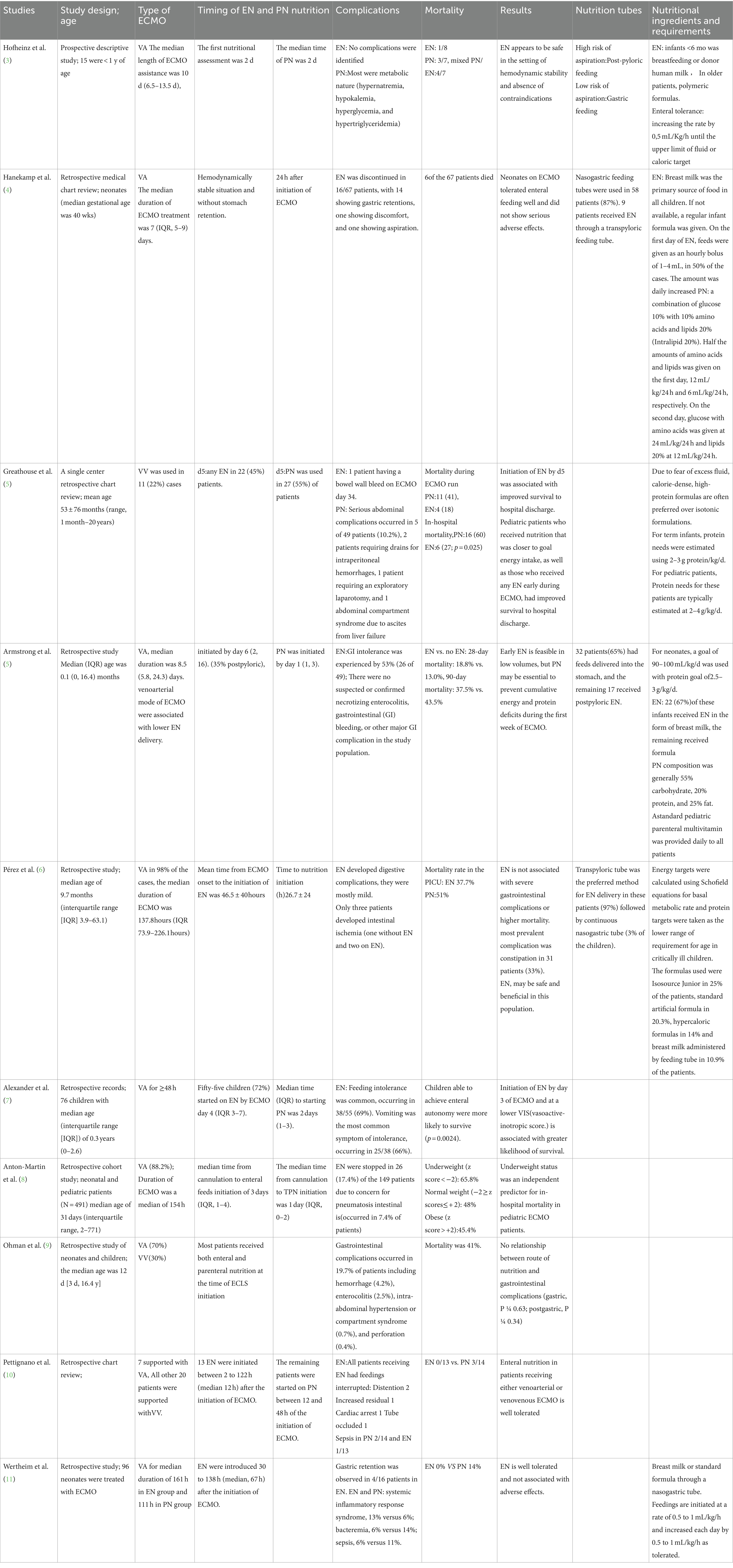
Table 1. Clinical characteristics, Nutrition management and results.
Children with ECMO have a higher risk of malnutrition (12), which is particularly prominent in children hospitalized in PICU. The study showed that nearly one-third of critically ill children had decreased nutritional indicators during their PICU stay. Retrospective studies have shown that the incidence of malnutrition in ECMO children is 33.3%, and the majority of them are under 2 years old (6). Anton-Martin (8) observed that 24% of 491 children with ECMO had a low body weight at the start of ECMO, low body weight was an independent risk factor for ECMO, and these children had a high in-hospital mortality. The stress response leads to muscle breakdown and amino acid release, exacerbating the problem of low body weight (13). Compared with adults, children have higher nutritional risks due to less nutritional energy reserves (14). The nutritional status of critically ill children is unstable and easy to deteriorate (15). pediatric ECMO patients show a trend of increased metabolism. Increased energy expenditure may lead to deterioration of the condition, resulting in prolonged mechanical ventilation and hospital stay. In addition, in vitro ECMO models have shown that the tubing itself may trigger pro-inflammatory and oxidative stress responses, increasing the risk of malnutrition in children (16).
Adequate feeding is typically defined as achieving 80–110% of the target value. The adequacy of nutrition provided for critically ill children during ECMO support is insufficient, particularly with regard to enteral nutrition (EN). EN may reduce gastrointestinal complications, but the proportion of calories and protein obtained through EN is lower, and the lower calories and protein from EN is because of the limited amount tolerated or provided (9). Additionally, a higher severity of illness score upon admission was found to be correlated with inadequate protein delivery (p = 0.040) (17). Study have shown (18) that when children have adequate energy intake (80% or more of predicted energy) and adequate protein intake (daily protein intake greater than or equal to 1.5 g/kg), their clinical outcomes are improved and the survival rate is higher. Moreover, protein adequacy may have a greater impact on children than energy intake, for example, more than 60% of predicted protein intake is associated with lower mortality in children with mechanical ventilation (19). In a multi-center study (20), the mortality rate was 9.3% in children receiving less than 20% of the predicted protein supply, 5.6% in those receiving 20 to 60, and 3.2% in those receiving more than 60%, indicating a positive correlation between survival and protein supply. Micronutrient and amino acid losses are marked during RRT in patients with AKI (21), To prevent a negative protein balance, enteral protein intake should be at least 1.5 g/kg/day, but currently there is insufficient evidence to support the need for additional supplementation of protein or amino acid intake during the acute phase. The nutritional status of ECMO children is closely related to clinical outcomes. Therefore, it is necessary to further study the nutritional adequacy of ECMO children and optimize the enteral nutrition strategy.
Various nutrition assessment parameters have been used to determine the presence and degree of malnutrition, including use of anthropometric measurements and laboratory values. Lipids are molecules involved in metabolism and inflammation. The plasma lipidome in critically ill children is very important to evaluate the nutritional status (22). Now, there are few studies on the relationship between lipids and nutrition metabolism in children with ECMO, but this provides a new perspective for further in-depth exploration. Carnitine is a key small molecule in the process of fatty acid oxidation and gluconeogenesis, and its deficiency can lead to significant complications in critically ill children. Study have shown (23) that the incidence of carnitine deficiency in ECMO children is higher than that in other hospitalized children, especially in children aged 1 week to 1 month. The level of carnitine is greatly influenced by nutritional support. About 75% of in vivo carnitine comes from dietary protein. The remaining carnitine can be synthesized endogenously in the liver, so older children are less prone to carnitine deficiency compared with neonates or premature infants (24). Evaluation of free carnitine levels may be appropriate for nutrition management, particularly if there are clinical concerns, such as unexpected hypoglycemia, cardiomyopathy, or chronic PN/dialysis use. Free carnitine <10 μM may reflect chronic deficiency and justify supplementation (25).
Currently, there is a lack of clarity on how to monitor and supplement carnitine, which points the way for future research. Thiamine is an essential coenzyme for aerobic glycolysis. Malnutrition may lead to thiamine deficiency, which in turn affects the symptoms of heart failure in children. Thiamine supplementation can significantly improve these symptoms (26). Thiamine supplementation is particularly important for high-risk children, especially those with malnutrition. In addition, in the case of thiamine deficiency, pyruvate is degraded by anaerobic metabolism, resulting in lactate formation and accumulation. Thiamine should be considered for treatment of children with unexplained lactic acidosis who are at risk for nutritional deficiencies. In hemodynamically stable children with elevated lactate, lactate levels can return to normal within 12 h after thiamine supplementation (27), allowing withdrawal of ECMO after 18 days. During ECMO treatment, more studies are needed to validate methods for blood lipids, carnitine, and thiamine measurements and the effects of their supplementation in critically ill children on the outcome deserve further investigations.
Body weight and basic nutritional status at admission are important for pediatric ECMO patients. Information on a child’s weight can be obtained by reviewing electronic medical records. Nutritional status should be evaluated within 24–48 h, which is not only helpful to monitor the changes in nutritional status of children, but also to assess the risk of nutritional deficiencies (28). The European Society for Pediatric and Neonatal Intensive Care (ESPNIC) recommends that the nutritional status of infants should be assessed regularly from the time of admission to the entire hospital stay (29). American Society for Parenteral and Enteral Nutrition (ASPEN) recommend that patients in the PICU undergo detailed nutritional assessment within 48 h of admission and that the nutritional status of patients be re-evaluated at least weekly throughout hospitalization (12). There are a variety of screening tools for nutritional status (such as the screening tool for risk on nutritional status and growth kids, STRONGkids) and screening tool for the assessment of malnutrition in pediatrics (STAMP). In the assesses, weight, height/length, mid-upper arm circumference and head circumference should also be included, and Z-score should be used to quantify it (29). The American Society for Parenteral and Enteral Nutrition (ASPEN) has developed an approach called nutrition-focused physical examination (NFPE), which focuses on nutrition and aims to detect fat and muscle loss early, thus reducing the severity of malnutrition. NFPE uses a head-to-toe approach to evaluate muscle mass, fat stores, fluid retention, micronutrient deficiencies, and functional capacity. However, its operation is relatively complex. A prospective cohort study (30) revealed that children who had lower nutritional complexity were more likely to complete the NFPE examination compared to those with higher nutritional risk. Moreover, older children were also more likely to complete the examination. Low complexity referred to patients needing basic nutrition education only, while high complexity referred to patients with chronic/complex diseases needing frequent reassessments or new enteral or parenteral nutrition interventions. The main challenges faced in completing NFPE were patient refusal and limited patient mobility/range of motion. Therefore, how to help children who need more time to complete NFPE due to mobility problems, nutritional complexity, and health related challenges and obtain their cooperation is the topic of future research.
EN has significant benefits for maintaining gastrointestinal structure and functions. These include integrity and peristalsis function of gastrointestinal, intestinal immunity and absorption function, which helps to reduce the risk of liver injury and sepsis-related complications. A number of studies have shown that children using EN as initial artificial nutrition support during ECMO has a lower incidence of complications and a higher survival rate (28, 29, 31). For children with ECMO, early initiation of EN (within 48 h after ECMO initiation or when clinically stable) is safe (3). Regarding the complications of EN, most studies have shown that gastrointestinal complications are relatively mild. A 5-year retrospective study reported 77 children treated with ECMO, 67 of whom were fed successfully without bilious vomiting, bloody stools, or abdominal distention (4). Another study (32) showed that EN did not increase the risk of infection or abdominal complications in 49 ECMO children, and the closer the nutritional intake was to the target value, the better the survival rate of children. It is important to note that the duration of ECMO support and low cardiac output are related factors for death in ECMO children. High VIS (vascular activity-muscle strength score) is associated with increased mortality in children (33). However, some studies have come to different conclusions, it has been suggested that early EN may be beneficial for ECMO children, but there does not appear to be a clear association between nutrient and protein adequacy and clinical outcomes. Most studies believe that early EN administration is beneficial to ECMO children and is well tolerated (34, 35).
There is no clear definition of the timing of early EN. Some studies have suggested (36) that EN performed within 24–72 h after ICU admission is early stage. Buckvold et al. (37) pointed out that it is safe to carry out EN within 24 to 36 h. ESPNIC recommends that EN should be performed as early as possible for full-term neonates, critically ill children and children after cardiac surgery who are hemodynamically stable with extracorporeal life support (ECLS) or dependent on drugs. In principle, EN should be started within 24 h after admission and gradually increased until the nutritional goal is reached. The American Society of Critical Care Medicine and ASPEN define early enteral nutrition as 6 to 48 h after admission. To sum up, it is recommended to start EN within 48 h of ECMO support or as soon as the patient’s condition is stable. A reasonable goal (18) is to achieve 2/3 of the EN nutritional target within the first week, and to avoid intolerance, EN is usually started at a sustained low volume rate (i.e., 10-20 mL /kg/d) and increased slowly (i.e., every 6–12 h). If intolerance occurs, such as aggravated abdominal distension, obvious gastric retention, gastrointestinal gas, effusion, etc., enteral feeding should be stopped immediately and replaced by parenteral nutrition.
The generally accepted nutritional mode is early EN combined with supplemental parenteral nutrition. Armstrong et al. (5) adopted a strategy of parenteral nutrition combined with early low-dose enteral nutrition for ECMO children. Early parenteral nutrition combined with low-dose enteral nutrition is beneficial to achieve nutritional goals and reduce mortality of children. Jimenez et al. (38) showed that the reasonable nutrition method for ECMO children is early and slow EN as the choice of nutritional support. If the goal of nutritional delivery cannot be achieved by EN alone, it is recommended that children with malnutrition or low birth weight should receive PN support within 3 to 5 days. In order to prevent energy and protein deficiency during the first week of ECMO, parenteral nutrition support was initiated within 5 to 7 days in well-nourished Pediatric patients. For children with hemodynamic instability, ESPNIC recommends stopping parenteral nutrition within the first week (39). For children who need to use parenteral nutrition for a long time, to avoid catheter-related infection, it is recommended to use a separate PN venous catheter for infusion (40). However, a study revealed that no significant difference was found in the proportion of patients who acquired a new infection while on ECMO support between those receiving any EN vs. PN alone. More studies are needed to investigate the relationship between parenteral nutrition and the risk of infection in children. In an in vitro experiment (41), lipid emulsions were laminated and coagulated in the circuit 30 min after infusion, 73% ECMO centers preferentially used separate venous channels for lipid infusion, and 18% ECMO centers used ECMO circuit infusion, which resulted in agglutination, membrane dysfunction, and thrombosis. At present, most ECMO centers set the initial lipid requirement at 0.5 g/ (kg/d), which can be gradually increased to 2–3 g/ (kg/d) under the premise of monitoring triglyceride. In the early years of ECMO, the use of lipids was associated with circuit complications (i.e., circuit clotting, lipid deposition, and oxygenator dysfunction and failure). With the development of technology, the change of oxygenator membranes from microporous polypropylene membranes to “true” nonporous, polymethylpentene membranes, more recent experience suggests that lipid infusions are not associated with oxygenator failure (28).
ECMO may lead to micronutrient deficiency. In the in vitro ECMO model, the essential amino acids isoleucine, vitamin A and vitamin E are lost from the pipeline (42). In animal models of acute lung injury induced by smoking, ECMO application is associated with selenium loss (43). The impact of these micronutrient deficiencies on ECMO treatment in children is important and requires further investigation. In children receiving ECMO and requiring dialysis, the loss of micronutrients is further aggravated, and continuous renal replacement therapy is associated with the loss of trace elements such as ionized calcium, inorganic phosphorus and selenium (44, 45). Calcium abnormalities frequently occurred in pediatric and neonatal patients undergoing ECMO support, and were found to be associated with a longer duration of ECMO and a longer length of ICU stay compared to patients who maintained normal calcium levels throughout ECMO therapy, with the underlying mechanism believed to be related to ECMO-induced disruption of normal calcium homeostasis (46). A 2014 American Society for Parenteral and Enteral Nutrition statement recommend an elemental calcium intake of 76 mg/kg and suggest a Ca:P ratio of 1.7:1 (mg:mg) or 1.3:1 (mmol:mmol) per day for short-term PN in neonates (47). Micronutrient loss in children with ECMO is an important area for future research.
CRRT can restore euvolemia in neonates receiving ECLS and improve outcomes without increasing long-term renal morbidity (48). The primary indication for renal replacement therapy (RRT) during ECMO therapy is for either active volume management or fluid overload prevention in nearly 60% of cases (49). CRRT is beneficial for children with ECMO and may improve their nutritional status. Enteral nutrition is well tolerated in children treated with CRRT (50). During the first 72 h of ECMO, children receiving early CRRT consumed a large amount of protein with no significant change in glucose infusion rate, fat emulsion, or total energy (48). Children with ECMO are at risk for fluid overload (FO), and fluid removal or FO prevention may improve survival (51). In a multicenter cohort study of ECMO in children, FO was very common, and FO was associated with prolonged ECMO support and increased mortality (52). The above suggests that intervening before FO occurs may be a potential clinical therapeutic target. In pediatric literature, fluid overload has been associated with mortality and prolonged ECMO duration, while a negative fluid balance leads to improved respiratory function and time to weaning ECMO. CRRT can be used to treat AKI to alleviate fluid overload, which should be considered to improve outcomes in cases of patients with unsuccessful ECMO treatment (53). However, the literature on the nutrition required for ECMO combined with CRRT therapy is limited. CRRT depletes certain intravenous nutrients, and lead to macro- and micronutrient loss, especially protein loss (54, 55). Other CRRT-mediated losses may occur, including the loss of trace minerals, key nutrients, and water-soluble vitamins. Low serum albumin (ALB) is associated with the prognosis of severe AKI patients receiving continuous renal replacement therapy. The higher the serum ALB before CRRT, the lower the mortality of critically ill patients with AKI and treated with CRRT, and the higher the clearance efficiency of serum phosphorus (56). So, increased protein provision is likely necessary for neonatal ECLS patients if CRRT is utilized. However, no such guidelines exist for neonates. Further studies are necessary so optimal outcomes can be achieved for these patients.
Energy requirements for pediatric ECMO patients are similar to those of other critically ill children and can be estimated using the same methods as for other critically ill Pediatric patients (31). During the acute phase, energy intake should not exceed resting energy expenditure. After the acute phase, energy intake should take into account basic energy needs, physical activity, rehabilitation, and growth. Methods for calculating energy include isotope tracing, indirect calorimetry (IC), and Schofield formula. IC is internationally recognized as the gold standard for measuring energy expenditure but is not widely used due to its high monitoring costs and instability factors (57, 58).
Indirect calorimetry involves a pipette added to the patient’s respiratory system to measure expired CO2 and oxygen consumption. However, in ECMO patients, the oxygenator membrane removes CO2, rendering indirect calorimetry measurements unreliable.
Both American Guidelines for Nutritional Support Therapy in Critically Ill Children and China’s Guidelines for Nutritional Assessment and Support Therapy in Critically Ill Children recommend using the Schofield equation to estimate resting energy expenditure when IC measurement is not feasible.
The Guidelines for Nutritional Assessment and Supportive Treatment of Critically Ill Children recommend a minimum protein intake of 1.5 g/kg/d. The protein supply of ECMO children should be at least 1.5 g/kg/ day or higher intakes to prevent negative protein balance (59), gradually increasing to 3 g/kg/ day depending on age and severity to meet the needs of the body. Children are in a high catabolic state during ECMO and up to 3 weeks after ECMO support, and it is critical to compensate for protein loss by providing adequate protein, research has found (60) that protein breakdown is 100% higher in ECMO newborns than in healthy newborns of the same age and needs to be provided. It takes 1.5 g/kg/d of protein to achieve a positive nitrogen balance. While ASPEN recommends receiving a neonatal protein supply of 3 g/Kg/ day from ECMO to offset catabolic losses, ESPNIC believes that there is currently insufficient evidence that intake of 1.5 g/kg/ day or higher protein/amino acids during the acute phase of disease is beneficial for clinical outcomes. Accurate assessment of energy and protein requirements in children with ECMO is also an important area for future research. Based on previous studies, the nutritional assessment procedures for ECMO children were as follows: Nutritional assessment was performed within 24 h, energy requirement was calculated using Schofield formula, protein was at least 1.5 g/Kg/ day, and hemodynamic stability assessment was performed within 24 to 48 h, and the following conditions were assessed as stable: (1). The dosage of vasoactive drugs was stable; (2). Liquid resuscitation has been completed; (3). Stable blood lactic acid. Contraindications for EN should be further excluded in stable children: (1). Unrepaired congenital diaphragmatic hernia(CDH); (2). Severe intestinal obstruction; (3). Other abdominal contraindications. Pediatric patients with stable hemodynamics and no contraindications were given EN, otherwise PN was considered. EN implementation generally starts at 10 m1/Kg/ day, every 6 to 12 h, and reaches 80% of the required energy within a week. If the EN target does not reach 50% on the third to fifth day, nutrition is increased through PN.
Current research suggests that nutritional support for children with ECMO should follow the critical illness nutrition guidelines and take into account the specific needs. Early administration of enteral nutrition (EN) is a relatively safe practice, but due to the limited number of studies, further prospective, randomized controlled studies are needed to establish the best nutritional practices. PN (PN) plays an important auxiliary role. There has been some research progress, but no consensus has been reached. The micronutrient needs should also be of concern to children treated with ECMO. Continuous renal replacement therapy (CRRT) cannot be ignored in the nutritional support of ECMO children, and the rational application of CRRT is conducive to the nutritional management of children. More studies are needed to provide higher quality evidence to guide nutritional support.
HZ: Conceptualization, Data Curation, Formal Analysis, Investigation, Writing – original draft, Writing – review & editing. LZ: Conceptualization, Data Curation, Formal Analysis, Investigation, Writing – review & editing. BJ: Data Curation, Formal Analysis, Investigation, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study is funded by Key Research Project in Henan Province Higher Education Institutions (Project No. 24B310012).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Toh, TSW, Ong, C, Mok, YH, Mallory, P, Cheifetz, IM, and Lee, JH. Nutrition in pediatric extracorporeal membrane oxygenation: a narrative review. Front Nutr. (2021) 8:666464. doi: 10.3389/fnut.2021.666464
2. Page, MJ, Mckenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. (2021) 10:89.
3. Hofheinz, SB, Núñez-Ramos, R, Germán-Díaz, M, Melgares, LO, Arroba, CMA, López-Fernández, E, et al. Which is the best route to achieve nutritional goals in pediatric ECMO patients? Nutrition. (2022) 93:111497. doi: 10.1016/j.nut.2021.111497
4. Hanekamp, MN, Spoel, M, Sharman-Koendjbiharie, I, Peters, JWB, Albers, MJIJ, and Tibboel, D. Routine enteral nutrition in neonates on extracorporeal membrane oxygenation. Pediatr Crit Care Med. (2005) 6:275–9. doi: 10.1097/01.PCC.0000161620.86647.72
5. Armstrong, LB, Ariagno, K, Smallwood, CD, Hong, C, Arbuthnot, M, and Mehta, NM. Nutrition delivery during pediatric extracorporeal membrane oxygenation therapy. JPEN J Parenter Enteral Nutr. (2018) 42:1133–8. doi: 10.1002/jpen.1154
6. Pérez, G, González, E, Zamora, L, Fernández, SN, Sánchez, A, Bellón, JM, et al. Early enteral nutrition and gastrointestinal complications in pediatric patients on extracorporeal membrane oxygenation. J Pediatr Gastroenterol Nutr. (2022) 74:110–5. doi: 10.1097/MPG.0000000000003317
7. Alexander, E, Absah, I, Steien, DB, Grothe, R, and Crow, S. Vasopressors and enteral nutrition in the survival rate of children during extracorporeal membrane oxygenation. J Pediatr Gastroenterol Nutr. (2022) 75:340–4. doi: 10.1097/MPG.0000000000003496
8. Anton-Martin, P, Papacostas, M, Lee, E, Nakonezny, PA, and Green, ML. Underweight status is an independent predictor of in-hospital mortality in pediatric patients on extracorporeal membrane oxygenation. JPEN J Parenter Enteral Nutr. (2018) 42:104–11. doi: 10.1177/0148607116673185
9. Ohman, K, Zhu, H, Maizlin, I, Williams, RF, Guner, YS, Russell, RT, et al. A multicenter study of nutritional adequacy in neonatal and pediatric extracorporeal life support. J Surg Res. (2020) 249:67–73. doi: 10.1016/j.jss.2019.11.018
10. Pettignano, R, Heard, M, Davis, RM, Labuz, M, and Hart, M. Total enteral nutrition versus total parenteral nutrition during pediatric extracorporeal membrane oxygenation. Crit Care Med. (1998) 26:358–63. doi: 10.1097/00003246-199802000-00041
11. Wertheim, HF, Albers, MJIJ, Piena-Spoel, M, and Tibboel, D. The incidence of septic complications in newborns on extracorporeal membrane oxygenation is not affected by feeding route. J Pediatr Surg. (2001) 36:1485–9. doi: 10.1053/jpsu.2001.27027
12. Mehta, NM, Skillman, HE, Irving, SY, Coss-Bu, JA, Vermilyea, S, Farrington, EA, et al. Guidelines for the provision and assessment of nutrition support therapy in the pediatric critically ill patient: Society of Critical Care Medicine and American Society for Parenteral and Enteral Nutrition. JPEN J Parenter Enteral Nutr. (2017) 41:706–42. doi: 10.1177/0148607117711387
13. Coss-Bu, JA, Hamilton-Reeves, J, Patel, JJ, Morris, CR, and Hurt, RT. Protein requirements of the critically ill pediatric patient. Nutr Clin Pract. (2017) 32:128S–41S. doi: 10.1177/0884533617693592
14. Joffe, A, Anton, N, Lequier, L, Vandermeer, B, Tjosvold, L, Larsen, B, et al. Nutritional support for critically ill children. Cochrane Database Syst Rev. (2016) 2016:CD005144. doi: 10.1002/14651858.CD005144.pub3
15. Green Corkins, K. Nutrition-focused physical examination in pediatric patients. Nutr Clin Pract. (2015) 30:203–9. doi: 10.1177/0884533615572654
16. Passmore, MR, Ki, KK, Chan, CHH, Lee, T, Bouquet, M, Wood, ES, et al. The effect of hyperoxia on inflammation and platelet responses in an ex vivo extracorporeal membrane oxygenation circuit. Artif Organs. (2020) 44:1276–85. doi: 10.1111/aor.13771
17. MacGowan, L, Smith, E, Elliott-Hammond, C, Sanderson, B, Ong, D, Daly, K, et al. Adequacy of nutrition support during extracorporeal membrane oxygenation. Clin Nutr. (2019) 38:324–31. doi: 10.1016/j.clnu.2018.01.012
18. Wong, JJ, Han, WM, Sultana, R, Loh, TF, and Lee, JH. Nutrition delivery affects outcomes in pediatric acute respiratory distress syndrome. JPEN J Parenter Enteral Nutr. (2017) 41:1007–13. doi: 10.1177/0148607116637937
19. Mehta, NM, Bechard, LJ, Zurakowski, D, Duggan, CP, and Heyland, DK. Adequate enteral protein intake is inversely associated with 60-d mortality in critically ill children: a multicenter, prospective, cohort study. Am J Clin Nutr. (2015) 102:199–206. doi: 10.3945/ajcn.114.104893
20. Ong, C, Mok, YH, Tan, ZH, Lim, CYS, Ang, B, Tan, TH, et al. Nutritional practices and adequacy in children supported on extracorporeal membrane oxygenation. Clin Nutr ESPEN. (2018) 26:21–6. doi: 10.1016/j.clnesp.2018.05.005
21. Oh, WC, Gardner, DS, and Devonald, MA. Micronutrient and amino acid losses in acute renal replacement therapy. Curr Opin Clin Nutr Metab Care. (2015) 18:593–8. doi: 10.1097/MCO.0000000000000220
22. Leimanis-Laurens, ML, Ferguson, K, Wolfrum, E, Boville, B, Sanfilippo, D, Lydic, TA, et al. Pediatric multi-organ dysfunction syndrome: analysis by an untargeted “shotgun” Lipidomic approach reveals low-abundance plasma phospholipids and dynamic recovery over 8-day period, a single-center observational study. Nutrients. (2021) 13:774. doi: 10.3390/nu13030774
23. Kelley, J, Sullivan, E, Norris, M, Sullivan, S, Parietti, J, Kellogg, K, et al. Carnitine deficiency among hospitalized pediatric patients: a retrospective study of critically ill patients receiving extracorporeal membrane oxygenation therapy. JPEN J Parenter Enteral Nutr. (2021) 45:1663–72. doi: 10.1002/jpen.2255
24. Flanagan, JL, Simmons, PA, Vehige, J, Willcox, MDP, and Garrett, Q. Role of carnitine in disease. Nutr Metab (Lond). (2010) 7:30. doi: 10.1186/1743-7075-7-30
25. Deswal, S, Bijarnia-Mahay, S, Manocha, V, Hara, K, Shigematsu, Y, Saxena, R, et al. Primary carnitine deficiency - a rare treatable cause of cardiomyopathy and massive hepatomegaly. Indian J Pediatr. (2017) 84:83–5. doi: 10.1007/s12098-016-2227-7
26. Vicinanza, A, de Laet, C, Rooze, S, Willems, A, Beretta-Piccoli, X, Vens, D, et al. Shoshin beriberi and severe accidental hypothermia as causes of heart failure in a 6-year-old child: a case report and brief review of literature. Front Pediatr. (2019) 7:119. doi: 10.3389/fped.2019.00119
27. Didisheim, C, Ballhausen, D, Choucair, ML, Longchamp, D, Natterer, J, Ferry, T, et al. Severe lactic acidosis in a critically ill child: think about thiamine! A case report. J Pediatr Intensive Care. (2021) 10:307–10. doi: 10.1055/s-0040-1713382
28. Lee, AE, Munoz, E, al Dabbous, T, Harris, E, O’Callaghan, M, and Raman, L. Extracorporeal life support organization guidelines for the provision and assessment of nutritional support in the neonatal and pediatric ECMO patient. ASAIO J. (2022) 68:875–80. doi: 10.1097/MAT.0000000000001767
29. Tume, LN, Valla, FV, Joosten, K, Jotterand Chaparro, C, Latten, L, Marino, LV, et al. Nutritional support for children during critical illness: European Society of Pediatric and Neonatal Intensive Care (ESPNIC) metabolism, endocrine and nutrition section position statement and clinical recommendations. Intensive Care Med. (2020) 46:411–25. doi: 10.1007/s00134-019-05922-5
30. Jimenez, EY, Lamers-Johnson, E, Long, JM, Mordarski, BA, Ma, X, and Steiber, A. Completion of a nutrition-focused physical exam with hospitalized adults and pediatric patients: secondary analysis of a prospective cohort study. Nutr Clin Pract. (2024) 1–15. doi: 10.1002/ncp.11137
31. Dennis, JL, Jordan, J, Rice, M, and Lee, AE. Enteral nutrition during extracorporeal membrane oxygenation in the neonatal and pediatric populations: a literature review. Pediatr Crit Care Med. (2023) 24:e382–9. doi: 10.1097/PCC.0000000000003239
32. Greathouse, KC, Sakellaris, KT, Tumin, D, Katsnelson, J, Tobias, JD, Hayes, D Jr, et al. Impact of early initiation of enteral nutrition on survival during pediatric extracorporeal membrane oxygenation. JPEN J Parenter Enteral Nutr. (2018) 42:205–11. doi: 10.1002/jpen.1032
33. Shukla, I, Hanson, SJ, Yan, K, and Zhang, J. Vasoactive-inotropic score and vasoactive-ventilation-renal score as outcome predictors for children on extracorporeal membrane oxygenation. Front Pediatr. (2021) 9:769932. doi: 10.3389/fped.2021.769932
34. Lu, MC, Yang, MD, Li, PC, Fang, HY, Huang, HY, Chan, YC, et al. Effects of nutritional intervention on the survival of patients with cardiopulmonary failure undergoing extracorporeal membrane oxygenation therapy. In Vivo. (2018) 32:829–34. doi: 10.21873/invivo.11315
35. Kim, S, Jeong, SK, Hwang, J, Kim, JH, Shin, JS, and Shin, HJ. Early enteral nutrition and factors related to in-hospital mortality in people on extracorporeal membrane oxygenation. Nutrition. (2021) 89:111222. doi: 10.1016/j.nut.2021.111222
36. Kim, H, Yang, JH, Cho, YH, Jun, TG, Sung, K, and Han, W. Outcomes of extracorporeal membrane oxygenation in children: an 11-year single-center experience in Korea. Korean J Thorac Cardiovasc Surg. (2017) 50:317–25. doi: 10.5090/kjtcs.2017.50.5.317
37. Buckvold, SM, and Kinsella, JP. Bleeding and thrombosis in pediatric extracorporeal membrane oxygenation. Can we improve anticoagulation strategies? Am J Respir Crit Care Med. (2017) 196:676–7. doi: 10.1164/rccm.201704-0723ED
38. Jimenez, L, Mehta, NM, and Duggan, CP. Timing of the initiation of parenteral nutrition in critically ill children. Curr Opin Clin Nutr Metab Care. (2017) 20:227–31. doi: 10.1097/MCO.0000000000000369
39. van Puffelen, E, Hulst, JM, Vanhorebeek, I, Dulfer, K, van den Berghe, G, Verbruggen, SCAT, et al. Outcomes of delaying parenteral nutrition for 1 week vs initiation within 24 hours among undernourished children in pediatric intensive care: a subanalysis of the PEPaNIC randomized clinical trial. JAMA Netw Open. (2018) 1:e182668. doi: 10.1001/jamanetworkopen.2018.2668
40. Buck, ML, Wooldridge, P, and Ksenich, RA. Comparison of methods for intravenous infusion of fat emulsion during extracorporeal membrane oxygenation. Pharmacotherapy. (2005) 25:1536–40. doi: 10.1592/phco.2005.25.11.1536
41. Hastings, SM, Ku, DN, Wagoner, S, Maher, KO, and Deshpande, S. Sources of circuit thrombosis in pediatric extracorporeal membrane oxygenation. ASAIO J. (2017) 63:86–92. doi: 10.1097/MAT.0000000000000444
42. Estensen, K, Shekar, K, Robins, E, McDonald, C, Barnett, AG, and Fraser, JF. Macro- and micronutrient disposition in an ex vivo model of extracorporeal membrane oxygenation. Intensive Care Med Exp. (2014) 2:29. doi: 10.1186/s40635-014-0029-7
43. McDonald, CI, Fung, YL, Shekar, K, Diab, SD, Dunster, KR, Passmore, MR, et al. The impact of acute lung injury, ECMO and transfusion on oxidative stress and plasma selenium levels in an ovine model. J Trace Elem Med Biol. (2015) 30:4–10. doi: 10.1016/j.jtemb.2015.01.004
44. Broman, M, Bryland, A, and Carlsson, O for the T‐Trace Acute Study Group. Trace elements in patients on continuous renal replacement therapy. Acta Anaesthesiol Scand. (2017) 61:650–9. doi: 10.1111/aas.12909
45. Datzmann, T, Träger, K, Reinelt, H, and von Freyberg, P. Elimination rates of electrolytes, vitamins, and trace elements during continuous renal replacement therapy with citrate continuous Veno-venous hemodialysis: influence of filter lifetime. Blood Purif. (2017) 44:210–6. doi: 10.1159/000477454
46. Kaplan, MC, and Heath, TS. Evaluation of calcium homeostasis and dietary supplementation for pediatric and neonatal patients receiving extracorporeal membrane oxygenation support. J Pediatric pharmacol therapeutics: JPPT: official J PPAG. (2019) 24:27–33. doi: 10.5863/1551-6776-24.1.27
47. Boullata, JI, Gilbert, K, Sacks, G, Labossiere, RJ, Crill, C, Goday, P, et al. A.S.P.E.N. Clinical guidelines: parenteral nutrition ordering, order review, compounding, labeling, and dispensing. JPEN J Parenter Enteral Nutr. (2014) 38:334–77. doi: 10.1177/0148607114521833
48. Murphy, HJ, Cahill, JB, Twombley, KE, Annibale, DJ, and Kiger, JR. Implementing a practice change: early initiation of continuous renal replacement therapy during neonatal extracorporeal life support standardizes care and improves short-term outcomes. J Artif Organs. (2018) 21:76–85. doi: 10.1007/s10047-017-1000-7
49. Dado, DN, Ainsworth, CR, Thomas, SB, Huang, B, Piper, LC, Sams, VG, et al. Outcomes among patients treated with renal replacement therapy during extracorporeal membrane oxygenation: a single-center retrospective study. Blood Purif. (2020) 49:341–7. doi: 10.1159/000504287
50. Santiago Lozano, MJ, Alonso Álvarez, C, Álvarez Heidbüchel, C, Fernández Lafever, S, Solana García, MJ, and López-Herce Cid, J. Nutrition in children with continuous renal replacement therapy. An Pediatr (Engl Ed). (2020) 92:208–14. doi: 10.1016/j.anpedi.2019.08.006
51. Constantinescu, AR, Adler, JL, Watkins, E, Negroni-Balasquide, XL, Laufenberg, D’A, Scholl, FG, et al. Aquapheresis (AQ) in tandem with extracorporeal membrane oxygenation (ECMO) in pediatric patients. J Extra Corpor Technol. (2019) 51:163–8. doi: 10.1051/ject/201951163
52. Gorga, SM, Sahay, RD, Askenazi, DJ, Bridges, BC, Cooper, DS, Paden, ML, et al. Fluid overload and fluid removal in pediatric patients on extracorporeal membrane oxygenation requiring continuous renal replacement therapy: a multicenter retrospective cohort study. Pediatr Nephrol. (2020) 35:871–82. doi: 10.1007/s00467-019-04468-4
53. Chung, KK, Coates, EC, Hickerson, WL, Arnold-Ross, AL, Caruso, DM, Albrecht, M, et al. Renal replacement therapy in severe burns: a multicenter observational study. J Burn Care Res. (2018) 39:1017–21. doi: 10.1093/jbcr/iry036
54. Jonckheer, J, Spapen, H, Malbrain, MLNG, Oschima, T, and de Waele, E. Energy expenditure and caloric targets during continuous renal replacement therapy under regional citrate anticoagulation. A viewpoint Clin Nutr. (2020) 39:353–7. doi: 10.1016/j.clnu.2019.02.034
55. Murphy, HJ, Finch, CW, and Taylor, SN. Neonatal extracorporeal life support: a review of nutrition considerations. Nutr Clin Pract. (2018) 33:625–32. doi: 10.1002/ncp.10111
56. Lv, J, Wang, H, Sun, B, Gao, Y, Zhang, Z, and Pei, H. Serum albumin before CRRT was associated with the 28- and 90-day mortality of critically ill patients with acute kidney injury and treated with continuous renal replacement therapy. Front Nutr. (2021) 8:717918. doi: 10.3389/fnut.2021.717918
57. Li, X, Yu, X, Cheypesh, A, and Li, J. Non-invasive measurements of energy expenditure and respiratory quotient by respiratory mass spectrometry in children on extracorporeal membrane oxygenation-a pilot study. Artif Organs. (2015) 39:815–9. doi: 10.1111/aor.12465
58. Wollersheim, T, Frank, S, Müller, MC, Skrypnikov, V, Carbon, NM, Pickerodt, PA, et al. Measuring energy expenditure in extracorporeal lung support patients (MEEP) - protocol, feasibility and pilot trial. Clin Nutr. (2018) 37:301–7. doi: 10.1016/j.clnu.2017.01.001
59. Jotterand Chaparro, C, Laure Depeyre, J, Longchamp, D, Perez, MH, Taffé, P, and Cotting, J. How much protein and energy are needed to equilibrate nitrogen and energy balances in ventilated critically ill children? Clin Nutr. (2016) 35:460–7. doi: 10.1016/j.clnu.2015.03.015
Keywords: extracorporeal membrane oxygen, children, nutritional support, enteral nutrition, parenteral nutrition
Citation: Zhang H, Zhao L and Jia B (2024) Research progress on nutritional support in the neonatal and pediatric populations receiving extracorporeal membrane oxygenation. Front. Nutr. 11:1370286. doi: 10.3389/fnut.2024.1370286
Edited by:
Maria Jose Santago, Gregorio Marañón Hospital, SpainReviewed by:
Gema Manrique Martin, Gregorio Marañón Hospital, SpainCopyright © 2024 Zhang, Zhao and Jia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Baohui Jia, emg4ODV4QDEyNi5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.