
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr., 22 March 2024
Sec. Nutritional Epidemiology
Volume 11 - 2024 | https://doi.org/10.3389/fnut.2024.1363574
This article is part of the Research TopicEating Behavior and Chronic Diseases: Research Evidence from Population StudiesView all 16 articles
 Chuang Sun1†
Chuang Sun1† Jie Li2†Zeyuan Zhao1Shupeng Ren1Yue Guan1Miaoan Zhang1Tianfeng Li1Linglin Tan1
Jie Li2†Zeyuan Zhao1Shupeng Ren1Yue Guan1Miaoan Zhang1Tianfeng Li1Linglin Tan1 Qiying Yao3*
Qiying Yao3* Liang Chen1*
Liang Chen1*Objective: Extensive research has consistently shown the beneficial impact of fruit consumption on overall health. While some studies have proposed a potential association between fruit consumption and hypertension management, the influence of fruit consumption on mortality rates among hypertensive individuals remains uncertain. Consequently, aim of this study is to evaluate whether fruit consumption is associated with all-cause mortality among hypertensive patients.
Methods: Data were obtained from the National Health and Nutrition Examination Survey (NHANES), conducted between 2003 and 2006. Ten-year follow-up data from the National Death Index (NDI) were used to assess all-cause mortality. Cox proportional hazard model was utilized to explore the impact of fruit intake on all-cause mortality among hypertensive individuals.
Results: The study included a cohort of 2,480 patients diagnosed with hypertension, and during the follow-up period, a total of 658 deaths from various causes were recorded. The COX regression analysis demonstrated that hypertensive patients who consumed apples three to six times per week exhibited a significantly reduced risk of all-cause mortality (HR = 0.60, 95%CI: 0.45–0.78, p < 0.001) in comparison to those who consumed apples less than once per month. Likewise, consuming bananas three to six times per week also led to a comparable outcome (HR = 0.76, 95%CI: 0.59–0.97, p = 0.027). Moreover, Combined consumption of bananas and apples three to six times per week exhibited a noteworthy decrease in all-cause mortality (HR = 0.57, 95%CI: 0.39–0.84, p = 0.005) when compared to individuals who consumed these fruits less frequently. Conversely, no significant association was found between the consumption of other fruits, including pears, pineapples, and grapes, and all-cause mortality.
Conclusion: The study discovered that moderate consumption of apples and bananas was associated with a reduced risk of all-cause mortality in patients with hypertension.
Fruits play a pivotal role in promoting a nourishing diet on a global scale (1). The Dietary Guidelines for Americans 2015–2020 advocate for the inclusion of fruits in dietary patterns, with a particular emphasis on the consumption of whole fruits (2). Extensive research has consistently demonstrated a significant inverse association between the intake of substantial quantities of fruit and the risk of developing cardiovascular disease, obesity, diabetes, cancer, and stroke (3–7). Moreover, studies have indicated that fruit consumption can effectively mitigate the risk of all-cause mortality in individuals with diabetes and specific types of cancer (8, 9).
Hypertension is a widely prevalent cardiovascular disorder. The World Health Organization’s global report on Hypertension reveals that approximately one third of the global population experiences this condition, resulting in over 10 million deaths annually attributed to elevated systolic blood pressure, with a substantial annual mortality rate (10). Hypertension remains the most significant modifiable risk factor for global all-cause mortality (11). The reportprimarily emphasizes the mitigation of hypertension through lifestyle modifications, with particular attention given to the impact of dietary patterns on blood pressure (10). Both the Dietary Approaches to Stop Hypertension and Mediterranean diets are recognized in the scientific community as effective dietary patterns for reducing high blood pressure (12–16). Both diets emphasize the consumption of fruits in their recommended meal plan (12–16).
Fruit-based diets, particularly those including apples, bananas, pears, and grapes, can have a positive impact on human health due to their high nutrient content. These fruits are rich in antioxidants, vitamins, and potassium (17). These nutrients can reduce blood pressure by improving endothelial function, modulating stress reflex sensitivity, and increasing antioxidant activity (18). Additionally, antioxidants can hinder the generation of reactive oxygen species, these species can scavenge excess and harmful free radicals that are produced during normal metabolism, prevent DNA damage, and ultimately reduce all-cause mortality (19). Nevertheless, a consensus regarding the optimal quantity of fruit intake has yet to be reached. Discrepancies in nutritional guidelines for fruit consumption persist across different nations. The World Health Organization advocates for the consumption of five fruit servings, the U.S. Dietary Guideline suggests at least 2 servings, whereas the Chinese Dietary Guideline suggests consuming 2.5–4.5 servings (20–22). Additionally, limited research has been conducted on the association between fruits intake and mortality rates among individuals with hypertension. Thus, the objective of this study is to assess the relationship between fruit consumption and all-cause mortality within a cohort of hypertensive patients.
Source of study population was from the National Health and Nutrition Examination Survey (NHANES), a public database that monitors human health conditions and nutrition across ethnic groups in the United States through continuous updates. NHANES obtained resident samples of all races in the United States through multi-stage stratified sampling, including people of all ages from all regions of the country. Therefore, NHANES data is a representative reflection of the health status of United States residents. Researchers can obtain NHANES data for free from the official website (Supplementary Table S1). The Ethics Review Board of the National Center for Health Statistics had approved the NHANES study. All participants provided written informed consent, allowing researchers to use the data as long as the data source is identified in the findings. The NHANES database included 11,183 adult participants from diverse ethnic and geographic backgrounds, between 2003 and 2006. Hypertension was identified through a computer-assisted personal interview system and a questionnaire. 3,390 participants were identified as having hypertension, while 908 participants were excluded due to not completing the Food Frequency Questionnaire (FFQ). Two participants lacked sufficient information to link to the National Death Index (NDI) data, resulting in missing follow-up survival status results and their exclusion from the study. Ultimately, 2,480 participants were enrolled in the study, as illustrated in Figure 1.
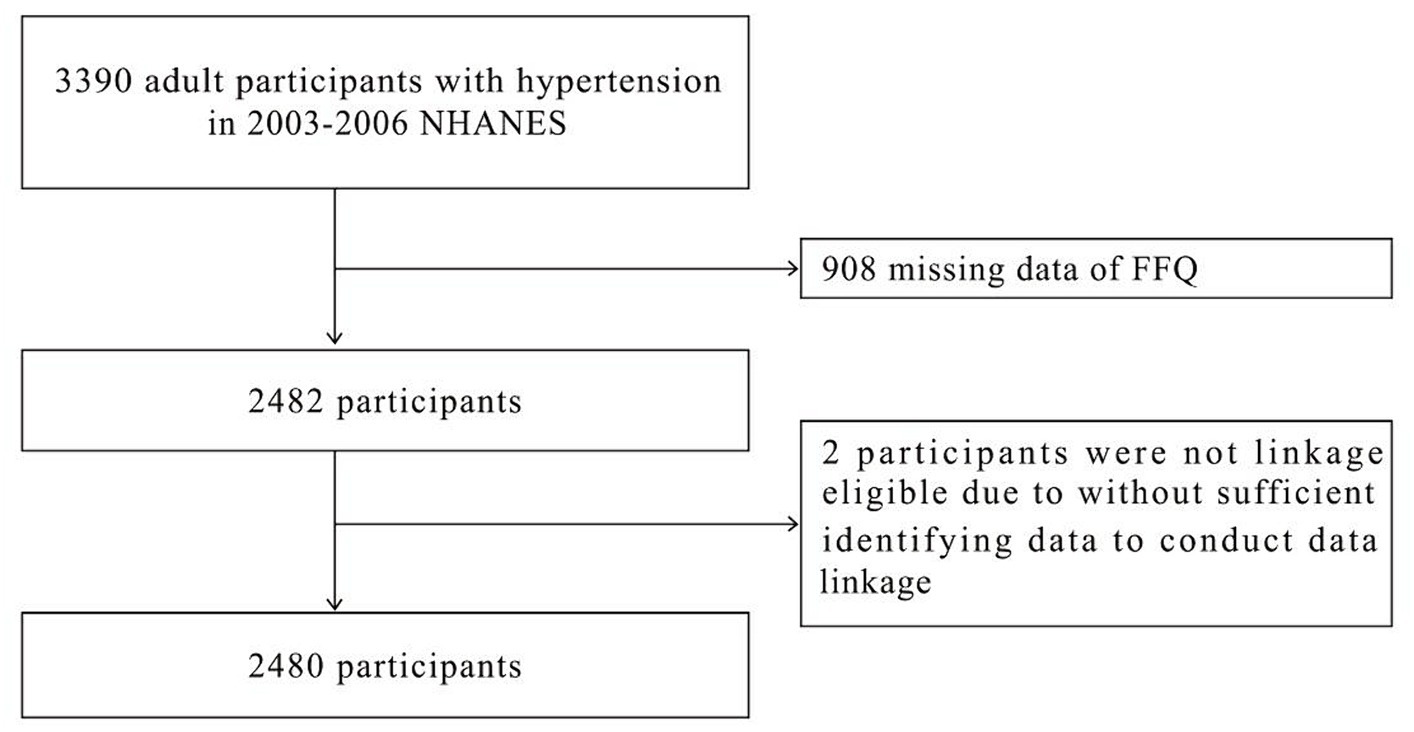
Figure 1. Flowchart of participant selection.
The Food Frequency Questionnaire (FFQ) is a tool used to collect information about food intake frequency in the past 12 months, including fruit consumption habits. Participants in this study were asked about their average intake of apples over the last year by responding to the prompt: “How often did you eat apples/ bananas/ pears/pineapples/grapes?” Their eating habits were then analyzed. Fruit consumption data was obtained via an FFQ, which categorized intake levels as follows: unknow, less than once /month, 1–3 times/month, 1–2 times/ week, three to six times/ week, or once or more /day for apples, pears, bananas, pineapples, and grapes.
All-cause mortality was examined using data from the National Death Index (NDI), which recorded death information for study participants from the survey’s commencement through December 31, 2019. The NDI, published by the National Center for Health Statistics, a United States government agency, connects NHANES data with mortality records. Data perturbation techniques were utilized in the NDI to reduce the risk of participant re-identification and maintain patient confidentiality. Study period concludes 10 years after enrollment. For deceased patients, the follow-up duration since their interview was computed based on the quarter and year of their passing. For living patients, follow-up duration was determined using the end of the follow-up period. All NDI data used in this study were obtained from publicly released documents on the website (Supplementary Table S1).
The collection of baseline patient data was facilitated by a computer-assisted personal interview system and a questionnaire survey. This comprehensive dataset encompassed various demographic factors such as gender, age, race, education level, ratio of family income to poverty, as well as health-related information including smoking and alcohol consumption, presence of hypercholesterolemia, diabetes, cardiovascular disease, stroke, lung disease, liver disease, and failing kidneys. Ethnicity was determined by categorizing patients as Mexican Americans, non-Hispanic Blacks, non-Hispanic whites, other Hispanics, or others. A smoking history of at least 100 cigarettes smoked throughout one’s lifetime was used as the criterion for identifying individuals as smokers. A drinker was operationally defined as an individual who had consumed a minimum of 12 cups alcoholic beverages within the preceding 12-month period. The presence of hypertension, hypercholesterolemia, diabetes, stroke, liver disease, and renal failure was ascertained based on prior diagnoses made by the participant’s healthcare provider. Participants who responded affirmatively to any of the following inquiries were categorized as having cardiovascular disease: “Have you ever been diagnosed with congestive heart failure, coronary heart disease, angina pectoris, or a heart attack by a healthcare professional?”
The median (first quartile, third quartile) was employed for continuous variables that did not adhere to a normal distribution. Categorical variables were expressed as numbers (percentages). The comparison of non-normally distributed continuous variables between two groups was conducted using the rank sum test. Furthermore, Chi-square tests were utilized to compare categorical variables between two groups. Cox proportional hazard model was utilized to examine the impact of fruit intake on all-cause mortality. Model 1 did not adjust any covariates. Model 2 made adjustments for gender, age, race, education level, and ratio of family income to poverty rate. In Model 3, covariates were selected based on the principle of covariate screening: confounding factors were compared before and after adding them to the regression model, and those resulting in a change in p value greater than 10% were included. Adjusting factors in the final Model 3 included sex, age, race, education level, ratio of family income to poverty rate, smoking history, history of hypercholesterolemia, diabetes, history of cardiovascular disease, stroke, lung disease, and history of failing kidneys. Before COX regression, collinearity screening was carried out for all covariates. The results indicated that the Variance Inflation Factor (VIF) for all covariates was less than 5. Splines smoothing plots were utilized to examine the linear or nonlinear correlation between the frequency of consuming different kinds of fruits and all-cause mortality. Additionally, stratified analyses were performed to confirm the consistency of the outcomes in the presence of different diseases. In addition, further elucidating the relationship between fruit intake and mortality was done by using a three-dimensional histogram and a time-mortality curve. The analysis of data was conducted using the R language package and EmPower software.1 p-values less than 0.05 are considered statistically significant.
A total of 2,480 participants met the study’s exclusion criteria and were included (Figure 1). The baseline characteristics of each participant are presented in Table 1. During the follow-up period, there were 1822 individuals who survived and 658 who died. The survivor group consisted of 44.5% males and 55.5% females. 15.8% of the population identified as Mexican American, 1.9% as other Hispanic, 53.4% as non-Hispanic white, 25% as non-Hispanic black, and 3.8% as belonging to other race. In regards to educational attainment, 45.4% of the population had education beyond high school. Concerning income, 40.3% of households had an income to poverty ratio greater than 3. Of the participants in survival group, 62.1% reported consuming alcohol, 48.9% smoked cigarettes, 47.3% had hypercholesterolemia, 17.8% suffered from diabetes, 14.2% from cardiovascular disease, 5.3% from stroke, 18.6% from lung disease, 4.1% from liver disease, and 3.3% from failing kidneys. In the group that experienced death, 55.5% were male and 44.5% were female. By race, 12.3% identified as Mexican American, 1.1% as other Hispanic, 65.5% as non-Hispanic white, 19.3% as non-Hispanic black, and 1.8% as other race. In terms of educational attainment, 34.2% possessed a high school education or higher. Regarding income, 24.8% had a ratio of family income to poverty exceeding 3. Of all participants in all-cause death group, 59.7% reported alcohol consumption, 62.8% reported smoking, 52.4% had hypercholesterolemia, 28.4% had diabetes, 37.8% had cardiovascular disease, 18.1% had a history of stroke, 26.1% suffered from lung disease, 4% experienced liver disease, and 10.9% had failing kidneys.
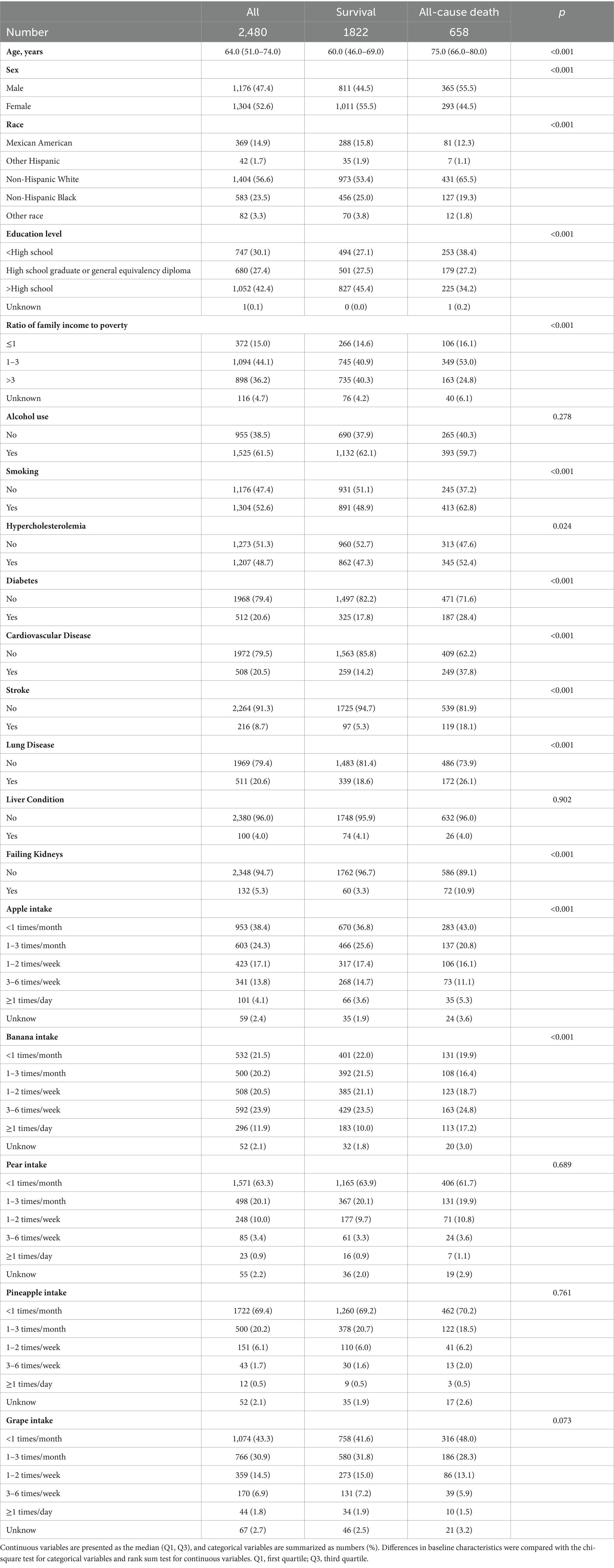
Table 1. Baseline characteristics of participants.
The study examined the association between fruit consumption and all-cause mortality. The findings from splines smoothing plots analysis, as depicted in Figure 2, illustrated a decreasing trend in the risk of all-cause mortality when consuming apples and bananas three to six times per week. However, no significant changes in the risk of all-cause mortality were observed for other fruits, regardless of the intake levels.
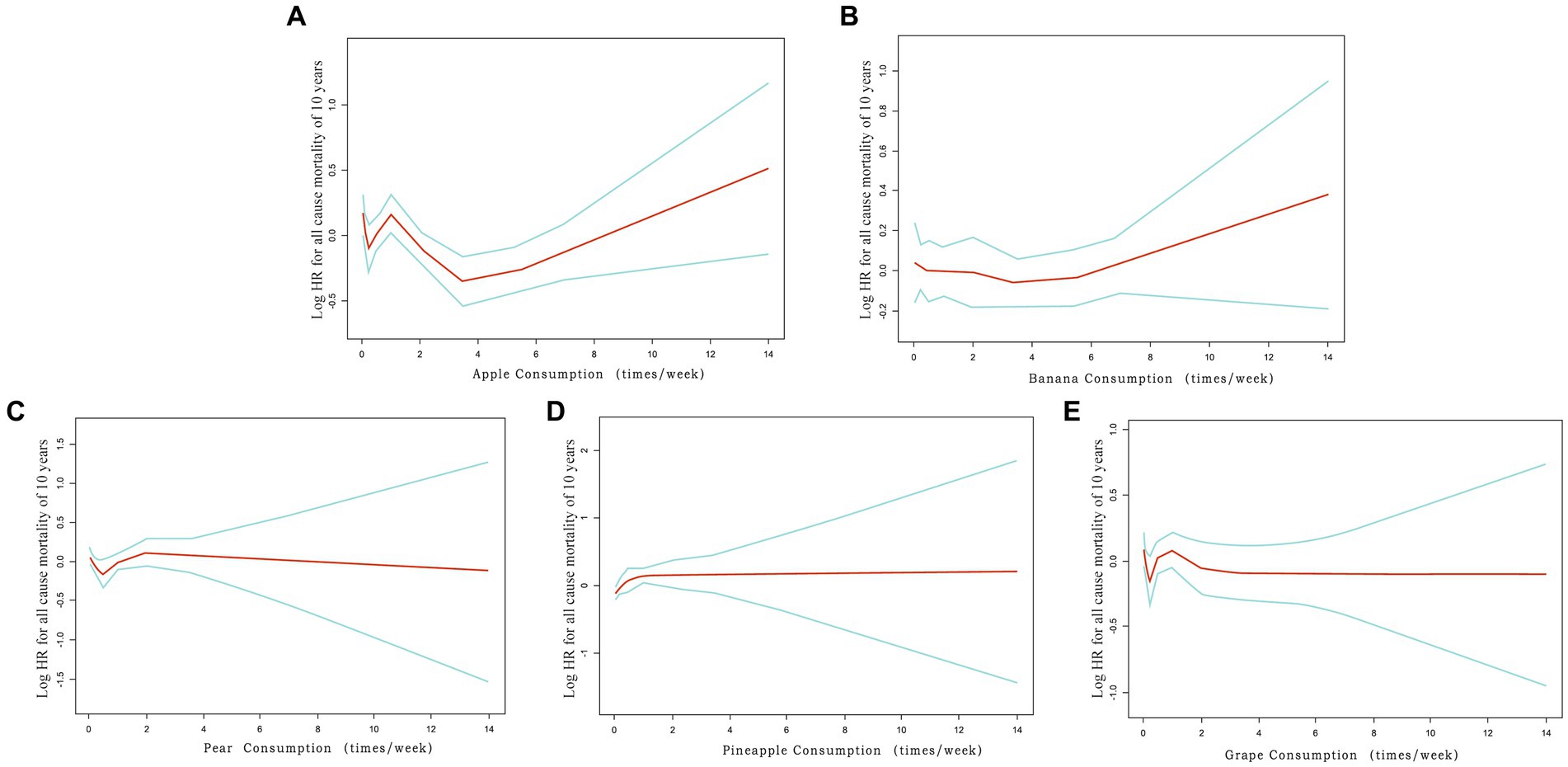
Figure 2. Splines smoothing plots of relationship between fruit consumption and all-cause mortality. (A) Splines smoothing plots of relationship between apple intake and all-cause mortality in patients with hypertension. (B) Banana intake. (C) Pear intake. (D) Pineapple intake. (E) Grape intake. HR has been fully adjusted for gender, age, race, education level, ratio of family income to poverty rate, smoking, hypercholesterolemia, diabetes, cardiovascular disease, stroke, lung disease, failing kidneys. HR, hazard ratio.
The findings from the multivariable adjusted Model 3 reveal that individuals who consume apples or bananas three to six times per week have a reduced risk of all-cause mortality by 40% (HR = 0.60, 95% CI: 0.45–0.78, p < 0.001) and 24% (HR = 0.76, 95% CI: 0.59–0.97, p = 0.027), respectively, compared to those who consume them less than once per month (Table 2). However, no statistically significant correlation was found between other frequency of consumption of apples and bananas and the risk of all-cause mortality. Furthermore, it is worth noting that no significant association is identified between the consumption of other fruits (including pears, pineapples, and grapes) and all-cause mortality.
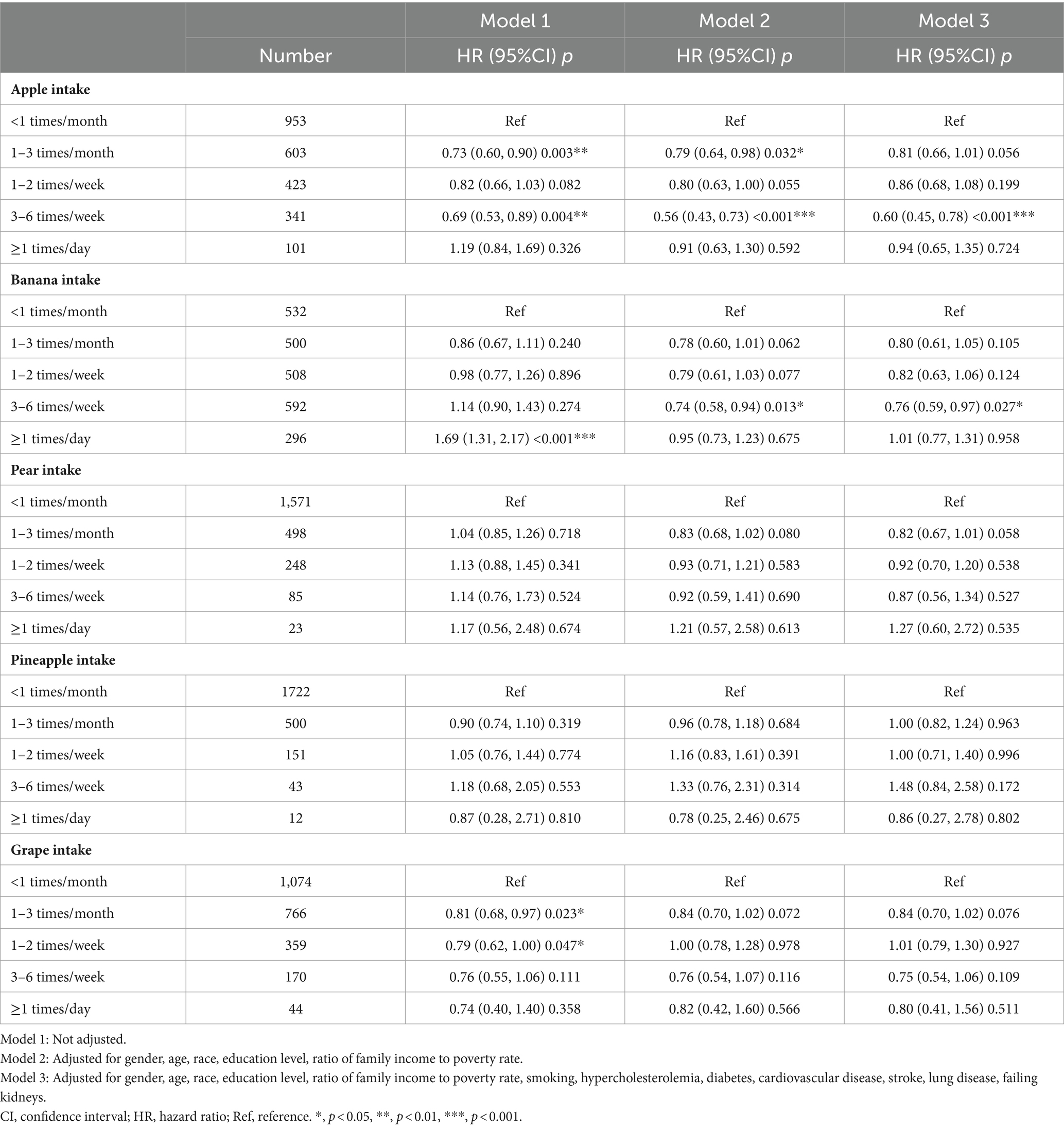
Table 2. Hazard ratios and confidence intervals of all-cause mortality for fruit consumption.
Subgroup analyses revealed that the association between apple consumption and all-cause mortality among individuals with hypertension remained unaffected by the presence or absence of comorbidities (all p values for the interaction were > 0.05) (refer to Table 3). Over the course of a 10-year follow-up period, our findings demonstrated that hypertensive individuals who consumed apples three to six times per week had a significantly lower risk of mortality compared to those who consumed them less than once a month. This observation is substantiated by the risk ratio results for all-cause mortality derived from the fully adjusted model, as illustrated in Figure 3 (log-rank test p < 0.05).
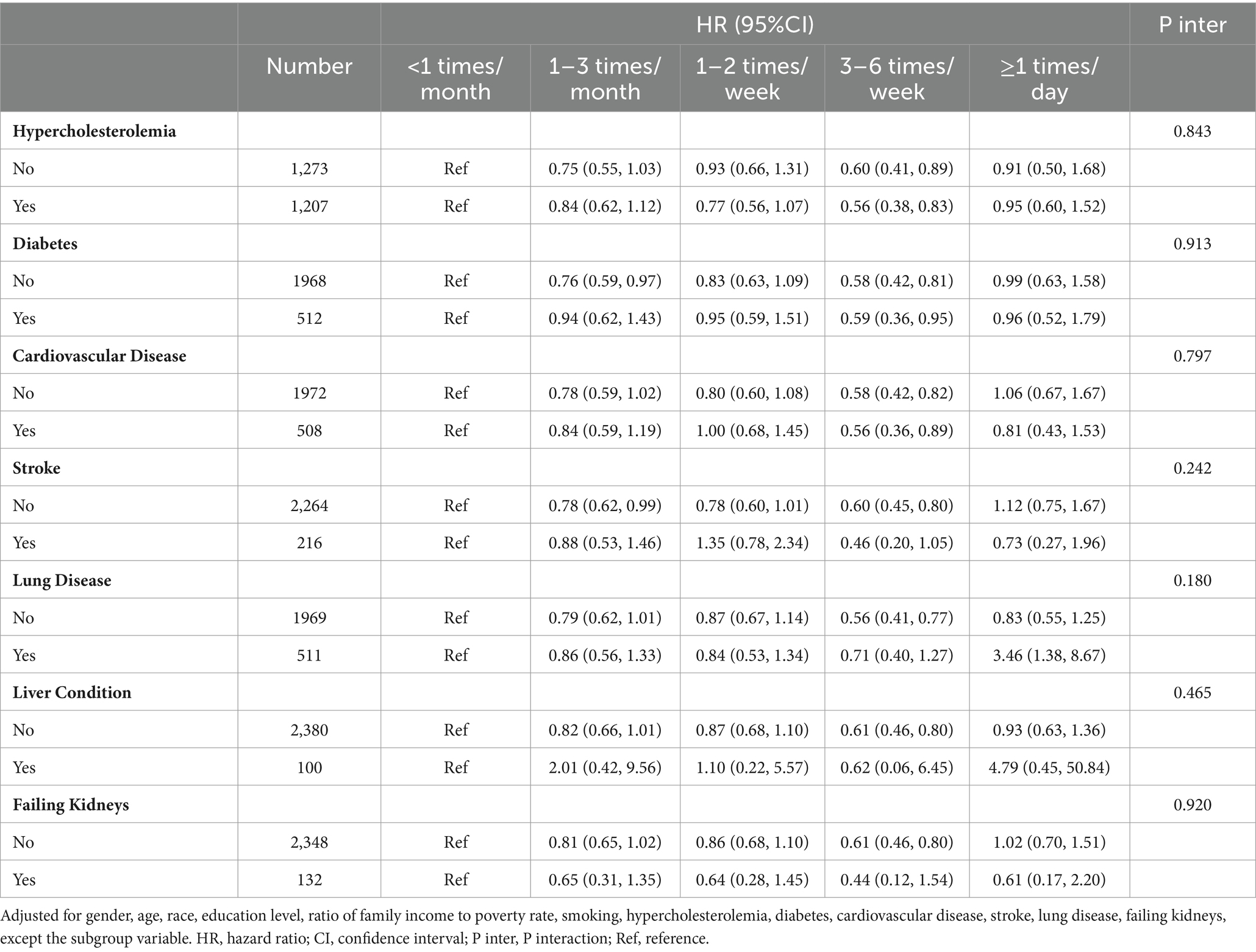
Table 3. Stratified analysis of relationship between apple intake and all-cause mortality.
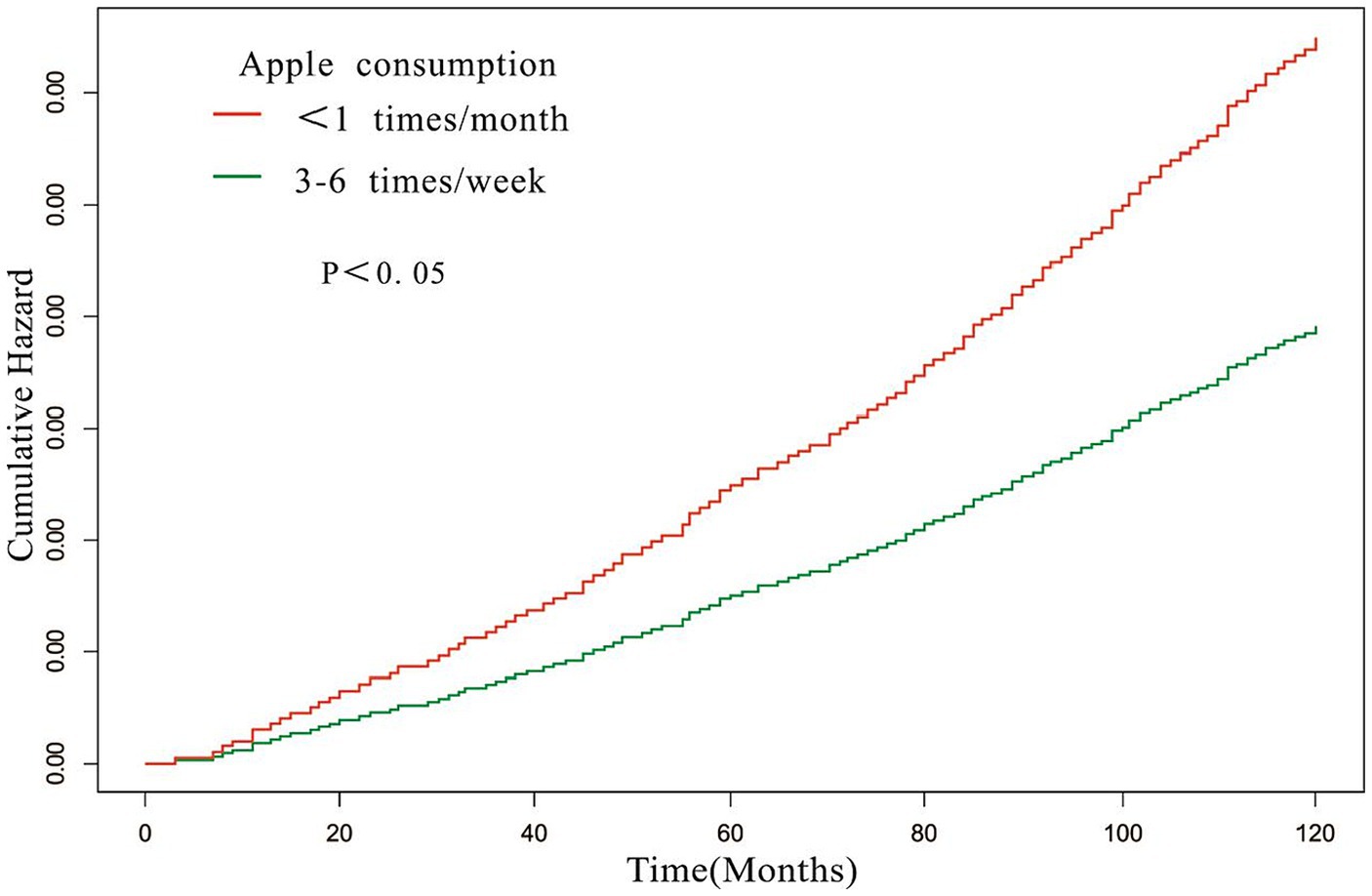
Figure 3. Time-mortality curve of the relationship between apple consumption and all-cause mortality. Adjusted for gender, age, race, education level, ratio of family income to poverty rate, smoking, hypercholesterolemia, diabetes, cardiovascular disease, stroke, lung disease, failing kidneys.
In a subgroup analysis, it was observed that the association between banana consumption and all-cause mortality among individuals with hypertension remained unaffected by the presence or absence of comorbidities (all p values for the interaction were > 0.05) (refer to Table 4). By employing COX regression analyses and accounting for confounding factors, the risk ratio for all-cause mortality was calculated. The results demonstrated that hypertensive individuals who consumed bananas three to six times per week had a significantly lower risk of mortality compared to those who consumed bananas less than once per month. The results are shown in Figure 4 (log-rank test p < 0.05).
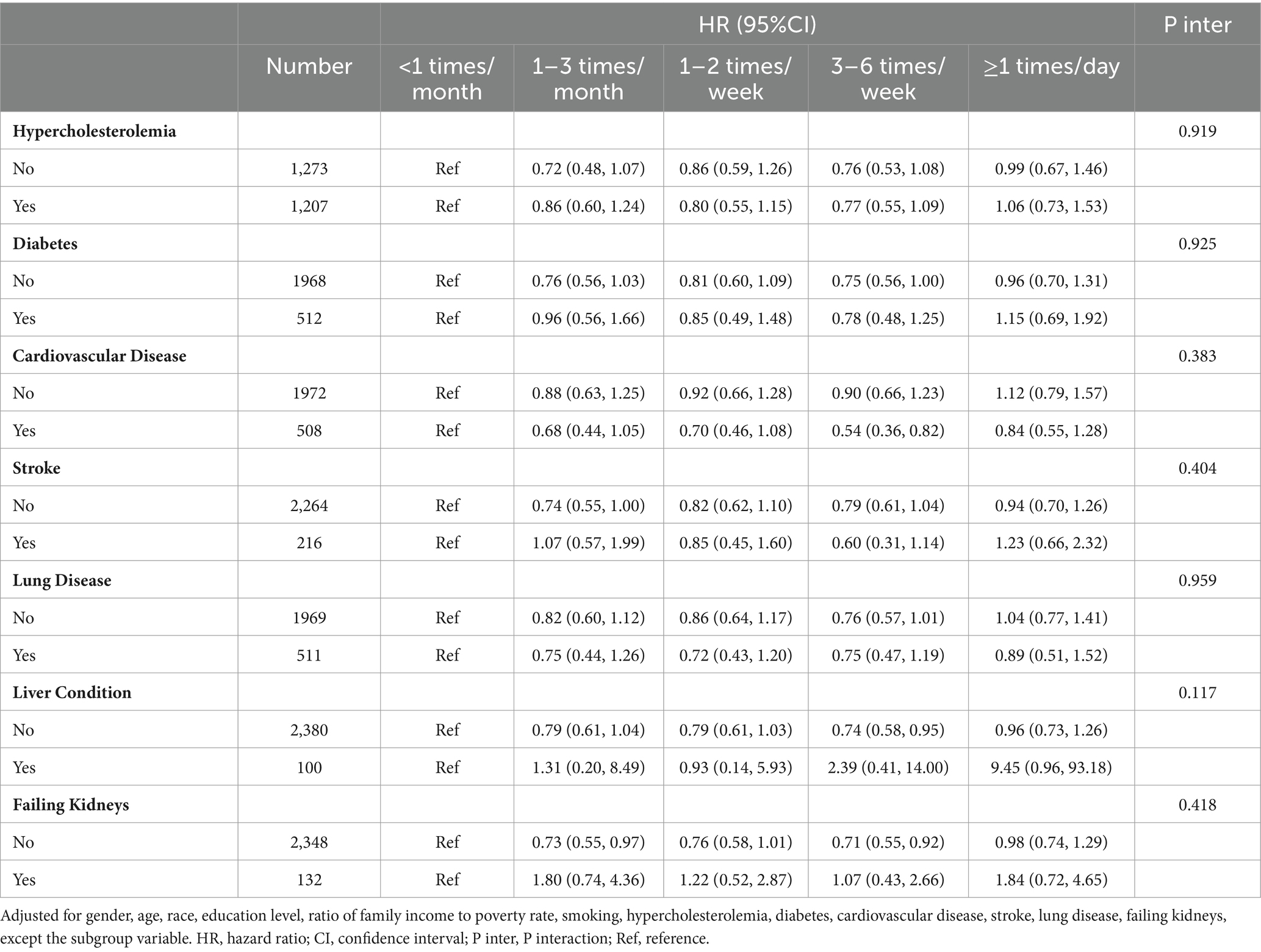
Table 4. Stratified analysis of relationship between banana intake and all-cause mortality.
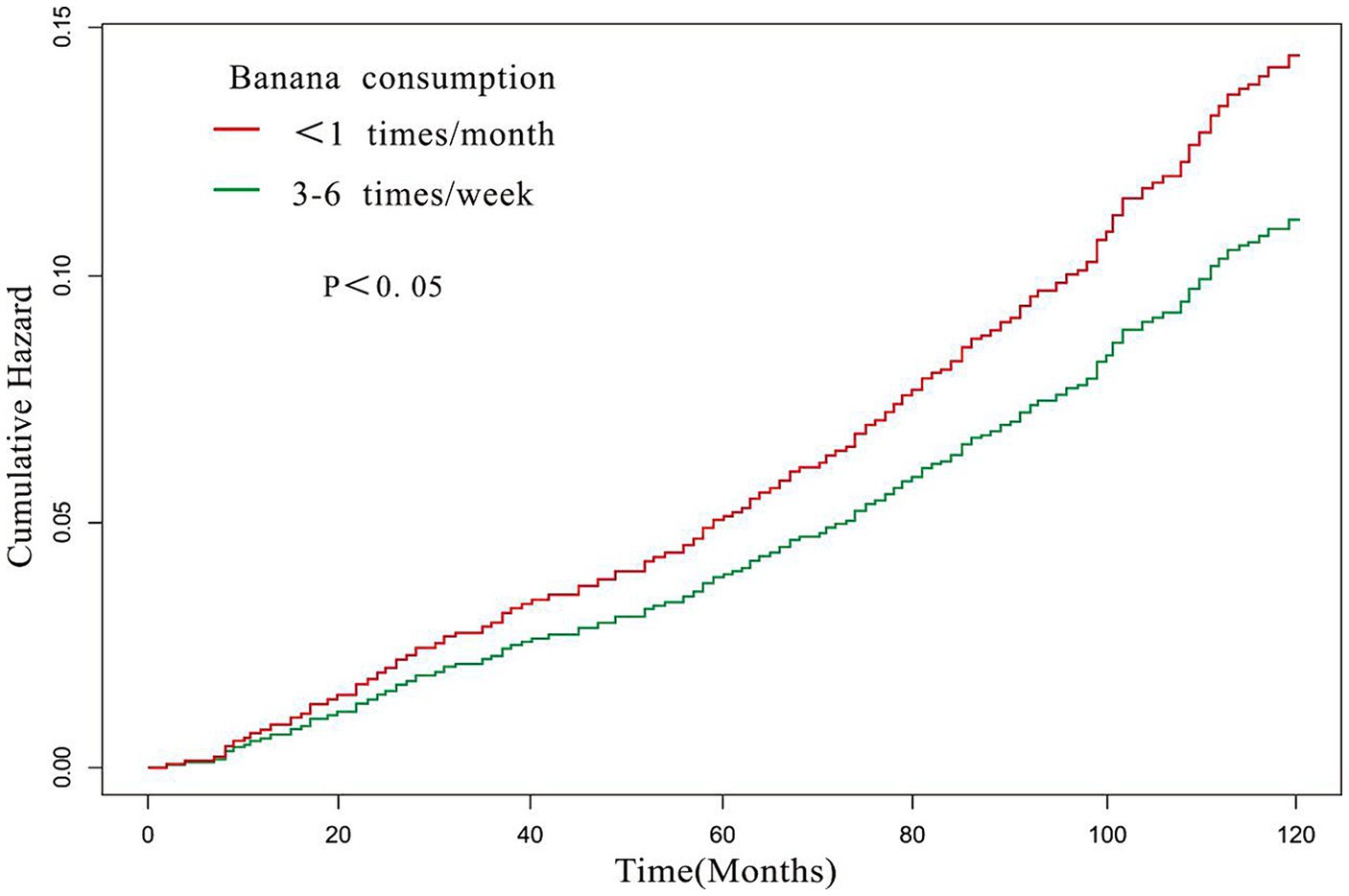
Figure 4. Time-mortality curve of the relationship between banana consumption and all-cause mortality. Adjusted for gender, age, race, education level, ratio of family income to poverty rate, smoking, hypercholesterolemia, diabetes, cardiovascular disease, stroke, lung disease, failing kidneys.
Further research was conducted to investigate the relationship between the consumption of a combination of apples and bananas and all-cause mortality rates. Participants were categorized into nine groups based on their frequency of consuming apples and bananas. Weekly consumption of apples and bananas was recorded as either three to six times, greater than three to six times, or less than three to six times. The Cox proportional hazard model was used to assess the risk of all-cause mortality. The findings (Figure 5; Supplementary Table S2) suggest that consuming apples and bananas three to six times per week significantly reduces the risk of all-cause mortality compared to consuming them less than three to six times per week (HR = 0.57, 95%CI: 0.39–0.84, p = 0.005). However, other consumption frequencies did not show a significant reduction in the risk of all-cause mortality.
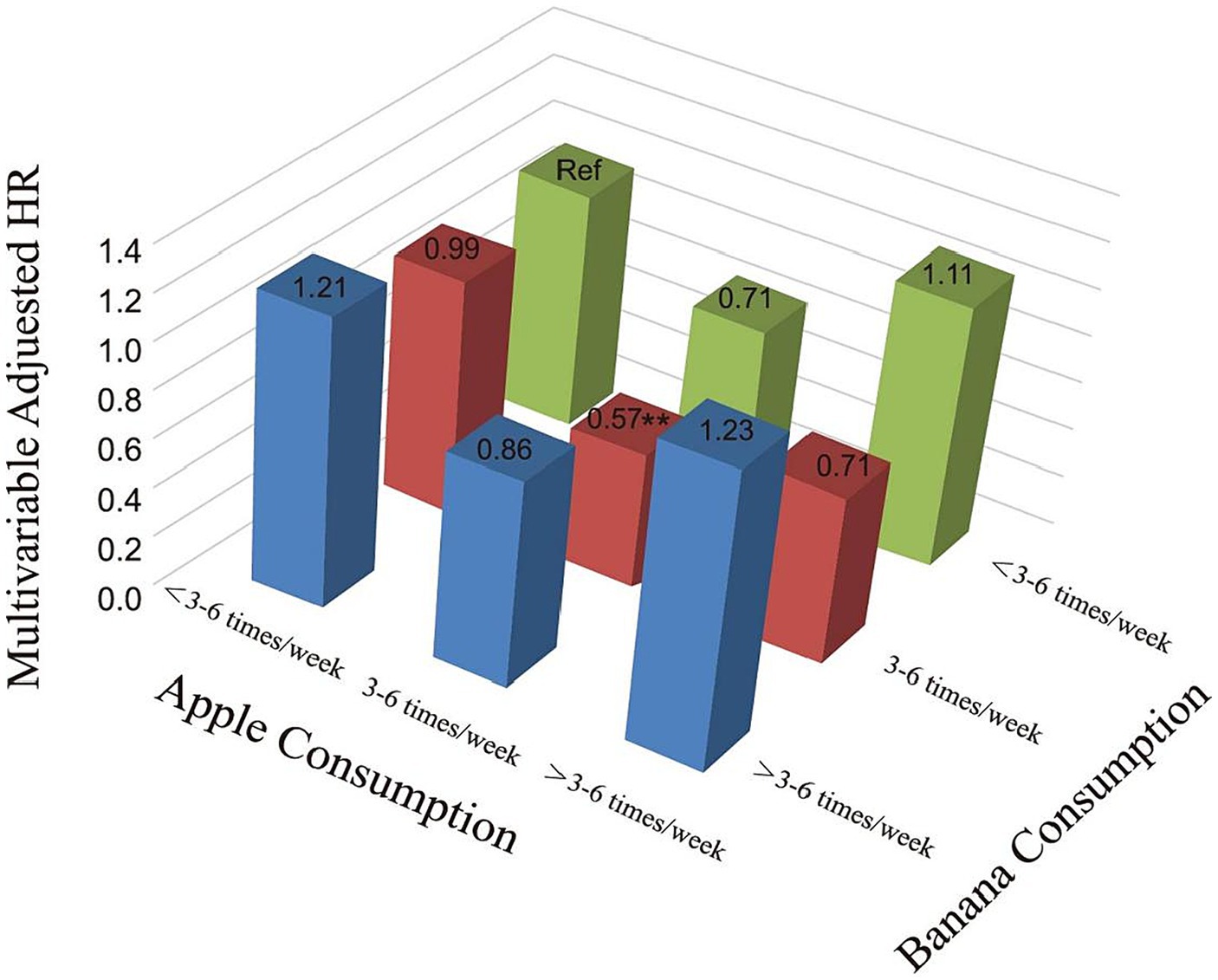
Figure 5. Three-dimensional histogram of relationship of combined consumption of apple and banana with the risk of all-cause mortality. Adjusted for gender, age, race, education level, ratio of family income to poverty rate, smoking, hypercholesterolemia, diabetes, cardiovascular disease, stroke, lung disease, failing kidneys, except the subgroup variable. HR, hazard ratio; Ref, reference. **, p < 0.01.
The study findings demonstrate that consuming apples or bananas three to six times per week is correlated with reduced all-cause mortality among individuals with hypertension, whereas no significant correlation was observed between the consumption of pears, pineapples, and grapes and lower all-cause mortality risks. Additionally, consuming a combination of apples and bananas three to six times per week may be associated with the greatest reduction in the risk of all-cause mortality. According to our knowledge, this is the first study to investigate the association between fruit consumption and all-cause mortality among individuals with hypertension.
Prior studies have demonstrated a connection between the intake of fruits and a decrease in mortality rates among populations afflicted with particular ailments. Chen et al. (8) sought to examine the association between fruit consumption and the dose–response relationship in relation to all-cause mortality in individuals diagnosed with type 2 diabetes in their study. The findings unveiled that a daily fruit consumption exceeding 42.9 g was associated with a 24% reduction in the risk of all-cause mortality (HR = 0.76; 95% CI 0.64–0.88) when compared to those who did not consume fruits. In a retrospective cohort study conducted by Martina et al. (9), it was observed that prostate cancer patients who consumed above-median quantities of fruits and vegetables exhibited a significantly higher likelihood of overall survival at 15 years in comparison to those with lower intake (71% versus 58%, p = 0.04; HR = 0.66, 95% CI: 0.47–0.93). These findings indicate a potential association between fruit and vegetable consumption and long-term survival among individuals diagnosed with prostate cancer. Similar to the aforementioned conditions, hypertension is a noteworthy health issue that affects a considerable portion of the population. Numerous studies have provided evidence that the consumption of fruit can reduce blood pressure levels in individuals with hypertension. However, the potential influence of fruit consumption on mortality rates among hypertensive populations has yet to be established. Our findings indicate that a moderate intake of apples and bananas is associated with a reduction in all-cause mortality among patients with hypertension, implying that fruit consumption may also confer survival benefits to hypertensive individuals.
Numerous studies have elucidated the positive impact of fruit consumption on health (23, 24). A meta-analysis has revealed that increased consumption of vegetables and fruits is associated with reduced all-cause mortality rates (24). The consumption of five servings of vegetables and fruits per day reached a point at which all-cause mortality no longer decreased. Our research suggests that consuming apples and bananas three to six times per week is associated with a decrease in mortality rates. However, increasing consumption beyond this range did not provide additional advantages. Further investigation into the relationship between fruit consumption and health is necessary to develop updated guidelines for optimal fruit intake.
Previous studies have primarily focused on the association between overall fruit consumption and mortality rates, with limited examination of the effects of specific types of fruit. Jonathan et al. found that increased apple consumption was associated with reduced all-cause mortality in elderly women (25). Our own research further supports this notion, demonstrating that the proper consumption of apples can effectively mitigate the risk of mortality. Jonathan’s study demonstrates that there is no significant correlation between heightened banana consumption and all-cause mortality. Conversely, our study has identified a notable association between appropriate intake of bananas and all-cause mortality. Discrepancies in findings may be ascribed to multiple factors observed across various studies, including disparities in the study population, methods of measuring fruit consumption, adjustments for confounding variables, duration of follow-up, and characteristics of the cohort.
There is a lack of literature describing individual fruits, which makes it difficult to understand the mechanisms involved. Both apples and pears belong to the Rosaceae family and are excellent sources of dietary fiber and phenolic compounds (26, 27). Dietary fiber has been shown to have a positive impact on cholesterol levels, blood sugar, and blood pressure, as well as promoting a healthy intestinal flora (28, 29). Phenolic compounds possess antioxidant, anti-inflammatory, anti-cancer, anti-aging, antiviral (30, 31). The study found no significant difference in dietary fiber content between apples and pears. However, apple skin had the highest concentration of polyphenolic compounds. In terms of inhibiting DPPH free radicals, the apple peel extract was the strongest while the pear pulp extract was the weakest (32). A study found that apples are the primary source of phenolic compounds and antioxidants in Northern Europe and the United States (33). The potential health benefits of apple polyphenols may exceed those of pear polyphenols. The antioxidant effects of pear polyphenols have only been demonstrated in vitro, as they have received less attention in research (26). In addition to this, apples can alleviate the symptoms of chronic diseases and reduce the risk of cardiovascular disease and cancer, due in large part to apple polyphenols (27, 34). As one of the most commonly consumed fruits, grapes are rich in antioxidants such as polyphenols and flavonoids. These antioxidants can reduce atherosclerosis by inhibiting the oxidation of low-density lipoproteins and activating novel proteins that prevent cellular senescence. Additionally, they can help prevent cardiovascular disease (35, 36). However, compared to apples, grapes may contain less dietary fiber. Dietary fiber has a blood pressure-lowering effect, which may be one of the reasons why apples can help alleviate chronic diseases (28, 29). Pineapple contains polyphenols, dietary fiber, and minerals. Studies have shown that pineapple exhibits anti-inflammatory and antioxidant activity (37). The polyphenol content in pineapple is lower than in apples. Although some studies have shown that pineapple skin contains more bioactives, it is not edible. Therefore, it is recommended to consume processed pineapple products and extracts (38). As a highly popular fruit worldwide, bananas possess a diverse range of nutrients, including phenolic compounds, vitamins C and E, carotenoids, as well as potassium ions (39). Many of these compounds exhibit antioxidant activity that protects the body against oxidative stresses, potentially decreasing mortality rates (40). Vitamin E, vitamin C, and carotenoids react with free radicals, specifically peroxyl radicals, and monolinear molecular oxygen to achieve antioxidant effects (19). Vitamin E helps prevent the oxidation of unsaturated fatty acids to peroxides, while carotenoids possess the ability to scavenge single-linear oxygen. Vitamin C plays a role in the regeneration of vitamin E and the elimination of free radicals within the cytoplasm (19). Furthermore, vitamin E has the potential to decrease platelet aggregation by inhibiting the proliferation of smooth muscle cells and reducing platelet adhesion to collagen (41). When comparing the potassium content of commonly consumed fruits, bananas contain more potassium than pears, and green grapes (17). Studies have shown that the consumption of potassium from dietary sources can lead to a decrease in blood pressure and a reduction in overall mortality (42–45). These mechanisms may help explain the correlation between bananas and apples intake and all-cause mortality, but not other fruits, with lowered all-cause mortality in our results for hypertensive patients. However, it is important to note that the conclusions of this study are specific to a particular population and cohort. Therefore, they should not be used to dismiss the health benefits of other fruits.
An important strength of this study is that it examines the association between fruit consumption and all-cause mortality within a hypertensive population, thereby providing a unique contribution to existing literature that has primarily focused on the general population. Moreover, our study boasts a substantial and diverse sample size, encompassing participants from different regions of the United States, varying ethnic backgrounds, and diverse socioeconomic statuses. The selection of the NHANHS database was based on its reputation for providing high-quality data and its recognition within the field. However, the scope of our study is constrained as it solely focused on examining the effects of apple and banana consumption on all-cause mortality, without considering the associations with specific causes of mortality such as cardiovascular disease, cancer, or chronic conditions. The researchers assessed the fruit intake of participants, which may introduce random measurement errors due to variations in individual diets over time. Additionally, observational studies may be subject to bias. In our study, we adjusted for covariates such as education level, poverty rate, and smoking to account for potential confounding factors. Although we made diligent attempts to account for all potential confounding variables and mitigate the impact of covariates in our analysis, it is plausible that unidentified or unmeasured factors could have influenced our findings.
In summary, our study has revealed that the consumption of a suitable quantity of apples or bananas can effectively lower mortality rates among individuals diagnosed with hypertension. Furthermore, the synergistic effect of consuming both fruits may yield even more advantageous outcomes. These findings may contribute novel evidence to the existing body of knowledge on dietetics for hypertensive populations.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding authors.
The studies involving humans were approved by the Ethics Review Board of the National Center for Health Statistics. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
CS: Data curation, Formal analysis, Methodology, Writing – original draft. JL: Data curation, Formal analysis, Methodology, Writing – original draft. ZZ: Methodology, Writing – original draft. SR: Validation, Writing – original draft. YG: Writing – original draft. MZ: Validation, Writing – original draft. TL: Validation, Writing – original draft. LT: Validation, Writing – original draft. QY: Project administration, Supervision, Writing – review & editing. LC: Conceptualization, Project administration, Supervision, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2024.1363574/full#supplementary-material
1. Di Renzo, L, Gualtieri, P, and De Lorenzo, A. Diet, nutrition and chronic degenerative diseases. Nutrients. (2021) 13:1372. doi: 10.3390/nu13041372
2. Wallace, TC, Bailey, RL, Blumberg, JB, Burton-Freeman, B, Chen, CO, Crowe-White, KM, et al. Fruits, vegetables, and health: a comprehensive narrative, umbrella review of the science and recommendations for enhanced public policy to improve intake. Crit Rev Food Sci Nutr. (2020) 60:2174–211. doi: 10.1080/10408398.2019.1632258
3. Zhan, J, Liu, YJ, Cai, LB, Xu, FR, Xie, T, and He, QQ. Fruit and vegetable consumption and risk of cardiovascular disease: a meta-analysis of prospective cohort studies. Crit Rev Food Sci Nutr. (2017) 57:1650–63. doi: 10.1080/10408398.2015.1008980
4. Hebden, L, O'Leary, F, Rangan, A, Singgih Lie, E, Hirani, V, and Allman-Farinelli, M. Fruit consumption and adiposity status in adults: a systematic review of current evidence. Crit Rev Food Sci Nutr. (2017) 57:2526–40. doi: 10.1080/10408398.2015.1012290
5. Du, H, Li, L, Bennett, D, Guo, Y, Turnbull, I, Yang, L, et al. Fresh fruit consumption in relation to incident diabetes and diabetic vascular complications: a 7-y prospective study of 0.5 million Chinese adults. PLoS Med. (2017) 14:e1002279. doi: 10.1371/journal.pmed.1002279
6. Aune, D, Giovannucci, E, Boffetta, P, Fadnes, LT, Keum, N, Norat, T, et al. Fruit and vegetable intake and the risk of cardiovascular disease, total cancer and all-cause mortality-a systematic review and dose-response meta-analysis of prospective studies. Int J Epidemiol. (2017) 46:1029–56. doi: 10.1093/ije/dyw319
7. Hu, D, Huang, J, Wang, Y, Zhang, D, and Qu, Y. Fruits and vegetables consumption and risk of stroke: a meta-analysis of prospective cohort studies. Stroke. (2014) 45:1613–9. doi: 10.1161/STROKEAHA.114.004836
8. Chen, Y, Su, J, Qin, Y, Luo, P, Shen, C, Pan, E, et al. Fresh fruit consumption, physical activity, and five-year risk of mortality among patients with type 2 diabetes: a prospective follow-up study. Nutr Metab Cardiovasc Dis. (2022) 32:878–88. doi: 10.1016/j.numecd.2021.10.024
9. Taborelli, M, Polesel, J, Parpinel, M, Stocco, C, Birri, S, Serraino, D, et al. Fruit and vegetables consumption is directly associated to survival after prostate cancer. Mol Nutr Food Res. (2017) 61:1600816. doi: 10.1002/mnfr.201600816
10. Al-Makki, A, DiPette, D, Whelton, PK, Murad, MH, Mustafa, RA, Acharya, S, et al. Hypertension pharmacological treatment in adults: a World Health Organization guideline executive summary. Hypertension. (2022) 79:293–301. doi: 10.1161/HYPERTENSIONAHA.121.18192
11. Charchar, FJ, Prestes, PR, Mills, C, Ching, SM, Neupane, D, Marques, FZ, et al. Lifestyle management of hypertension: International Society of Hypertension position paper endorsed by the world hypertension league and European Society of Hypertension. J Hypertens. (2024) 42:23–49. doi: 10.1097/HJH.0000000000003563
12. Filippou, CD, Tsioufis, CP, Thomopoulos, CG, Mihas, CC, Dimitriadis, KS, Sotiropoulou, LI, et al. Dietary approaches to stop hypertension (DASH) diet and blood pressure reduction in adults with and without hypertension: a systematic review and Meta-analysis of randomized controlled trials. Adv Nutr. (2020) 11:1150–60. doi: 10.1093/advances/nmaa041
13. Juraschek, SP, Miller, ER 3rd, Weaver, CM, and Appel, LJ. Effects of sodium reduction and the DASH diet in relation to baseline blood pressure. J Am Coll Cardiol. (2017) 70:2841–8. doi: 10.1016/j.jacc.2017.10.011
14. Filippou, CD, Thomopoulos, CG, Kouremeti, MM, Sotiropoulou, LI, Nihoyannopoulos, PI, Tousoulis, DM, et al. Mediterranean diet and blood pressure reduction in adults with and without hypertension: a systematic review and meta-analysis of randomized controlled trials. Clin Nutr. (2021) 40:3191–200. doi: 10.1016/j.clnu.2021.01.030
15. Guasch-Ferré, M, and Willett, WC. The Mediterranean diet and health: a comprehensive overview. J Intern Med. (2021) 290:549–66. doi: 10.1111/joim.13333
16. Slomski, A. Mediterranean diet vs low-fat diet for patients with heart disease. JAMA. (2022) 327:2386. doi: 10.1001/jama.2022.9509
17. Slavin, JL, and Lloyd, B. Health benefits of fruits and vegetables. Adv Nutr. (2012) 3:506–16. doi: 10.3945/an.112.002154
18. Li, B, Li, F, Wang, L, and Zhang, D. Fruit and vegetables consumption and risk of hypertension: a Meta-analysis. J Clin Hypertens (Greenwich). (2016) 18:468–76. doi: 10.1111/jch.12777
19. Sies, H, Stahl, W, and Sundquist, AR. Antioxidant functions of vitamins. Vitamins E and C, beta-carotene, and other carotenoids. Ann N Y Acad Sci. (1992) 669:7–20. doi: 10.1111/j.1749-6632.1992.tb17085.x
20. Margetts, B. FAO/WHO launch expert report on diet, nutrition and prevention of chronic diseases. Public Health Nutr. (2003) 6:323–5. doi: 10.1079/PHN2003481
21. McGuire, S. Scientific report of the 2015 dietary guidelines advisory committee. Washington, DC: US Departments of agriculture and health and human services, 2015. Adv Nutr. (2016) 7:202–4. doi: 10.3945/an.115.011684
22. Yang, YX, Wang, XL, Leong, PM, Zhang, HM, Yang, XG, Kong, LZ, et al. New Chinese dietary guidelines: healthy eating patterns and food-based dietary recommendations. Asia Pac J Clin Nutr. (2018) 27:908–13. doi: 10.6133/apjcn.072018.03
23. Miller, V, Mente, A, Dehghan, M, Rangarajan, S, Zhang, X, Swaminathan, S, et al. Fruit, vegetable, and legume intake, and cardiovascular disease and deaths in 18 countries (PURE): a prospective cohort study. Lancet. (2017) 390:2037–49. doi: 10.1016/S0140-6736(17)32253-5
24. Wang, X, Ouyang, Y, Liu, J, Zhu, M, Zhao, G, Bao, W, et al. Fruit and vegetable consumption and mortality from all causes, cardiovascular disease, and cancer: systematic review and dose-response meta-analysis of prospective cohort studies. BMJ. (2014) 349:g4490. doi: 10.1136/bmj.g4490
25. Hodgson, JM, Prince, RL, Woodman, RJ, Bondonno, CP, Ivey, KL, Bondonno, N, et al. Apple intake is inversely associated with all-cause and disease-specific mortality in elderly women. Br J Nutr. (2016) 115:860–7. doi: 10.1017/S0007114515005231
26. Reiland, H, and Slavin, J. Systematic review of pears and health. Nutr Today. (2015) 50:301–5. doi: 10.1097/NT.0000000000000112
27. Zhang, Y, Zeng, M, Zhang, X, Yu, Q, Zeng, W, Yu, B, et al. Does an apple a day keep away diseases? Evidence and mechanism of action. Food Sci Nutr. (2023) 11:4926–47. doi: 10.1002/fsn3.3487
28. Veronese, N, Solmi, M, Caruso, MG, Giannelli, G, Osella, AR, Evangelou, E, et al. Dietary fiber and health outcomes: an umbrella review of systematic reviews and meta-analyses. Am J Clin Nutr. (2018) 107:436–44. doi: 10.1093/ajcn/nqx082
29. Reynolds, AN, Akerman, A, Kumar, S, Diep Pham, HT, Coffey, S, and Mann, J. Dietary fibre in hypertension and cardiovascular disease management: systematic review and meta-analyses. BMC Med. (2022) 20:139. doi: 10.1186/s12916-022-02328-x
30. Stevenson, DE, and Hurst, RD. Polyphenolic phytochemicals – just antioxidants or much more? Cell Mol Life Sci. (2007) 64:2900–16. doi: 10.1007/s00018-007-7237-1
31. Rahman, MM, Rahaman, MS, Islam, MR, Rahman, F, Mithi, FM, Alqahtani, T, et al. Role of phenolic compounds in human disease: current knowledge and future prospects. Molecules. (2021) 27:233. doi: 10.3390/molecules27010233
32. Leontowicz, M, Gorinstein, S, Leontowicz, H, Krzeminski, R, Lojek, A, Katrich, E, et al. Apple and pear peel and pulp and their influence on plasma lipids and antioxidant potentials in rats fed cholesterol-containing diets. J Agric Food Chem. (2003) 51:5780–5. doi: 10.1021/jf030137j
33. Commisso, M, Bianconi, M, Poletti, S, Negri, S, Munari, F, Ceoldo, S, et al. Metabolomic profiling and antioxidant activity of fruits representing diverse apple and pear cultivars. Biology (Basel). (2021) 10:380. doi: 10.3390/biology10050380
34. Knekt, P, Kumpulainen, J, Järvinen, R, Rissanen, H, Heliövaara, M, Reunanen, A, et al. Flavonoid intake and risk of chronic diseases. Am J Clin Nutr. (2002) 76:560–8. doi: 10.1093/ajcn/76.3.560
35. Dohadwala, MM, and Vita, JA. Grapes and cardiovascular disease. J Nutr. (2009) 139:1788s–93s. doi: 10.3945/jn.109.107474
36. Ruf, JC. Wine and polyphenols related to platelet aggregation and atherothrombosis. Drugs Exp Clin Res. (1999) 25:125–31.
37. Mohd Ali, M, Hashim, N, Abd Aziz, S, and Lasekan, O. Pineapple (Ananas comosus): a comprehensive review of nutritional values, volatile compounds, health benefits, and potential food products. Food Res Int. (2020) 137:109675. doi: 10.1016/j.foodres.2020.109675
38. Zhao, Q, Ge, Q, Shang, Y, Zheng, M, Sun, X, Bao, S, et al. Eating with peel or not: investigation of the peel consumption situation and its nutrition, risk analysis, and dietary advice in China. Food Res Int. (2023) 170:112972. doi: 10.1016/j.foodres.2023.112972
39. Singh, B, Singh, JP, Kaur, A, and Singh, N. Bioactive compounds in banana and their associated health benefits – a review. Food Chem. (2016) 206:1–11. doi: 10.1016/j.foodchem.2016.03.033
40. Aune, D, Keum, N, Giovannucci, E, Fadnes, LT, Boffetta, P, Greenwood, DC, et al. Dietary intake and blood concentrations of antioxidants and the risk of cardiovascular disease, total cancer, and all-cause mortality: a systematic review and dose-response meta-analysis of prospective studies. Am J Clin Nutr. (2018) 108:1069–91. doi: 10.1093/ajcn/nqy097
41. Eichholzer, M, Lüthy, J, Gutzwiller, F, and Stähelin, HB. The role of folate, antioxidant vitamins and other constituents in fruit and vegetables in the prevention of cardiovascular disease: the epidemiological evidence. Int J Vitam Nutr Res. (2001) 71:5–17. doi: 10.1024/0300-9831.71.1.5
42. Whelton, PK, He, J, Cutler, JA, Brancati, FL, Appel, LJ, Follmann, D, et al. Effects of oral potassium on blood pressure. Meta-analysis of randomized controlled clinical trials. JAMA. (1997) 277:1624–32. doi: 10.1001/jama.1997.03540440058033
43. Dickinson, HO, Nicolson, DJ, Campbell, F, Cook, JV, Beyer, FR, Ford, GA, et al. Magnesium supplementation for the management of essential hypertension in adults. Cochrane Database Syst Rev. (2006) 3:Cd004640. doi: 10.1002/14651858.CD004640.pub2
44. Kwon, YJ, Lee, HS, Park, G, and Lee, JW. Association between dietary sodium, potassium, and the sodium-to-potassium ratio and mortality: a 10-year analysis. Front Nutr. (2022) 9:1053585. doi: 10.3389/fnut.2022.1053585
45. Bagheri, A, Naghshi, S, Sadeghi, O, Larijani, B, and Esmaillzadeh, A. Total, dietary, and supplemental magnesium intakes and risk of all-cause, cardiovascular, and Cancer mortality: a systematic review and dose-response Meta-analysis of prospective cohort studies. Adv Nutr. (2021) 12:1196–210. doi: 10.1093/advances/nmab001
Keywords: fruit consumption, apple consumption, banana consumption, hypertension, all-cause mortality
Citation: Sun C, Li J, Zhao Z, Ren S, Guan Y, Zhang M, Li T, Tan L, Yao Q and Chen L (2024) The correlation between fruit intake and all-cause mortality in hypertensive patients: a 10-year follow-up study. Front. Nutr. 11:1363574. doi: 10.3389/fnut.2024.1363574
Edited by:
Xiaoyue Xu, University of New South Wales, AustraliaReviewed by:
Mohammad Altamimi, An-Najah National University, PalestineCopyright © 2024 Sun, Li, Zhao, Ren, Guan, Zhang, Li, Tan, Yao and Chen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Qiying Yao, eWFvcXlAZG11LmVkdS5jbg==; Liang Chen, ZHlleWFycmh5dGhtaWFAMTYzLmNvbQ==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.