
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr., 10 July 2024
Sec. Nutritional Epidemiology
Volume 11 - 2024 | https://doi.org/10.3389/fnut.2024.1339819
This article is part of the Research TopicNutrition and Sustainable Development Goal 3: Good Health and WellbeingView all 35 articles
 Zeritu Dewana Derbo1,2*
Zeritu Dewana Derbo1,2* Gurmesa Tura Debelew2
Gurmesa Tura Debelew2Background: A woman’s health and nutritional status has significant impact on her pregnancy situation. However, many pregnant women are undernourished. Moringa stenopetala is a plant consumed worldwide in various forms, and its consumption showed a reduction in the incidence of malnutrition. Although Moringa stenopetala is rich in essential macro- and micronutrients, there is little evidence on the proportion and determinants of fresh Moringa stenopetala leaf intake among pregnant women. The objective of this study was to fill this gap in the littérature and provide a baseline evidence for further research or intervention by investigation the proportion and determinants of fresh Moringa stenopetala leaf intake among pregnant women in the Gamo zone, south Ethiopian region.
Methods: A community-based cross-sectional study was conducted among 623 randomly selected pregnant women using a pre-tested and structured questionnaire via a face-to-face interview. The consumption pattern was assessed based on a self-reported dietary history over the last 30 days before data collection. Multivariable logistic regression model was fitted using STATA version 14. An adjusted odds ratio with a 95% confidence interval was reported to show an association between the dependent and independent variables with level of statistical significance at a p-value of <0.05.
Results: The proportion of fresh Moringa stenopetala leaves intake among pregnant women was 49.60% (95% CI: 45.67, 53.52%). The déterminants of fresh moringa leaf intake were being below 24 years old (AOR: 2.92; 95% CI: 1.51, 5.63), rural résidence (AOR: 1.97; 95% CI: 1.10, 3.50), antenatal care attendance (AOR: 2.08; 95% CI: 1.03, 4.21), history of contraceptive use (AOR: 1.88; 95% CI: 1.03, 3.55), and having a good knowledge about the importance of moringa Stenopetala (AOR: 9.76; 95% CI: 5.30, 17.95).
Conclusion: The study showed that almost half of the pregnant women consumed fresh Moringa stenopetala leaves. Women’s age, place of residence, prenatal care, history of contraceptive use, and knowledge of the benefits of Moringa Stenopetala were positively associated with the consumption of fresh Moringa Stenopetala leaves. Therefore, health authorities and stakeholders involved in maternal and child health need to target older women, and urban residents and promote the benefits of consumption by strengthening uptake of maternal health services and raising awareness about Moringa Stenopetela. Future studies involving large scale and longitudinal designs evidence are required to further validate the findings so that this nutritious diet can be promoted widely among pregnant women in the study area and Ethiopia at large.
Women have unique nutritional needs throughout their lifespan, especially during pre-pregnancy and pregnancy periods. Access to nutritious, safe, affordable, and sustainable food is crucial for women’s survival, health and well-being. Pregnancy also increases women’s need for protein, vitamins and minerals (1).
Despite this, 154 million (10%) and 520 million (33%) women worldwide were underweight and anemic, respectively, in 2020 (2). The overall pooled prevalence of malnutrition during pregnancy was 23.5% in Africa (3) and 29.07% in Ethiopia in 2021 (4). Inadequate nutritional intake is common among pregnant women due to food taboos, food insecurity, infectious diseases, and inadequate care (5–9). Malnutrition during pregnancy increases the incidence of low birth weight, preterm birth, poor APGAR (appearance, pulse, grimacing, activity, and respiration) scores, stillbirth, neonatal death, and postpartum hemorrhage, leading to poor pregnancy outcomes (10, 11). In contrast, better nutrition during pregnancy is essential to promote fetal health, survival, growth, and development. It is also a key strategy to reduce the burden of malnutrition, incidence of non - communicable diseases, and maternal and child mortality (12–18). However, most pregnant women in Ethiopia have poor and inadequate nutritional practices, with a total prevalence of 67.7% was malnourished (7, 19). Therefore, improving maternal nutritional status is an urgent priority.
Moringa Stenopetala (MS) is a fast-growing drought-resistant tropical tree that originated in India (20). This is commonly referred to as the “miracle tree,” (21) “never-dying tree,” (22) and “mother’s best friend” (23). It has different names in different localities, such as “Nébéday” in Senegal, “Yevu-ti” in Ghana and Togo, “Malunggay” in the Philippines (24), “Mlonge” in Kenya and Tanzania, “Zakalanda” in Zimbabwe, horseradish tree in the United States (24), horseradish or ben oil tree in the United Kingdom, “drumstick tree” in India (21, 22), and “Shiferaw” in Ethiopia (25). It also has different vernacular names in southern Ethiopia, such as “Aleko” or “Aluko” or “Haleko” in Gamo and Wolaita, “Kallanki” in Bena, “Telahu” in Tsemay, “Haleko” or “Shelchada” in Konso, and “Haleko” in Burje and Derashe (25).
Studies showed MS is safe for pregnant women and has a variety of nutritional and health benefits including reducing the risk of malnutrition, low birth weight, and anemia. Consuming MS during pregnancy may also help prevent DNA damage caused by stress and adverse pregnancy outcomes and improve breast milk supply. Additionally, MS has been shown to have anti-inflammatory and antioxidant effects that help fight diseases (26–33). Evidence also showed that MS leaves are rich in flavonoids, calcium, and antioxidants, making them suitable for consumption by pregnant women. In addition, MS leaf extract nanoparticles are reported to reduce anxiety levels among pregnant women with high blood pressure, and affected their blood pressure by increasing serotonin levels (34).
A country-wide study in Ethiopia found that 100 g of MS leaves contained 28.44% protein, 0.7% fat, 38.49% carbohydrate, 11.62% fiber, 54.85 mg iron, 1,918 mg calcium, 2.16 mg zinc, 2,094 mg potassium, 214.10 mg sodium, 28.49 mg vitamin C, 12.95 mg vitamin A, and other important nutrients (25). The finding indicate that MS species found in Ethiopia are rich in nutrients and their consumption helps in obtaining important macro- and micronutrients (25, 35–37). Current evidence in Ethiopia suggests that rising food prices will affect the intake of nutritious foods (38). MS leaves are a great way to fill this gap as they are rich in macro- and micronutrients and cheap as well.
Studies on consumption of MS species showed that it was widespread practice: 63% in India (39), 81% in Africa (39), 87.2% in Togo (40),and 90% in South Africa (41) but it has been underutilized (36%) in East Shoa Zones of Oromia,Ethiopia (42). Age, education level, marital status, occupation, household wealth status, awareness level, knowledge of plant biology, gender, and family size (43, 44) were factors associated with MS species consumption in the general population. However, such studies on the extent and determinants of MS use are lack among pregnant women. Although MS is widely cultivated in Ethiopia and has been indicated as having nutritional and health benefits for pregnant women, little is known about the level of consumption and factors affecting this during pregnancy. There are few studies on the nutritional, medicinal, and water purification properties of MS, and its effect on maternal hemoglobin levels, but there is little scientific evidence supporting MS consumption in pregnant women (25, 45). Therefore, this study aimed to investigate the level of consumption of fresh MS leaves, and factors associated with it among pregnant women in Gamo zone, southern Ethiopia.
The study was conducted in the Arba Minch Zuria and Chencha Districts, Gamo Zone, southern Ethiopia. It is located 434 Km and 443 km south of Addis Ababa (the capital city of Ethiopia) respectively (46). Based on projection made from the 2007 Ethiopian population and housing census the population residing in the two districts summed up to 353,019 in 2021/22, and the expected number of pregnant women was estimated to be 12,214. The area has two hospitals, nine health centers, sixty-three health posts, and a number of private health facilities at different levels of service standards that collectively provide curative, preventive, and rehabilitative services for the population (45).In the study area, fresh MS leaves are commonly prepared and consumed in the form of ‘Kurkufa’, and ‘Fosossie’ (through directly cooking a corn flour or its wraps with the leaves), and ‘Kita’(in the form ofa flat bread locally prepared from various cereals including corn, wheat, barley or ‘Teff’), and ‘Haleko’ (directly cooking the MS leaves in a separate dish like spinach and/or in the form of soup).
A community-based cross-sectional study was conducted from May 8th to June 20, 2022.
The source populations were all pregnant women living in Arba Minch Zuria and Chencha district, and the study populations were pregnant women in selected kebeles (smallest administrative unit in Ethiopia) in Arba Minch Zuria and Chencha district.
All pregnant women who were in between 20 and 26 weeks of gestation at the time of recruitment and permanently residing in Arba Minch Zuria and Chencha district were included in the study.
Women who did not give consent to participate in the study and who were seriously ill or unable to give information for the interview were excluded from the study. Women were considered as seriously ill when they had a health condition that made them unable to speak and carried a high risk of mortality and were more generally not able to perform activities and daily living and were excessively straining their care givers (47).
The sample size required to assess fresh MS consumption habits in pregnant women was estimated using the sample size estimation formula for single population proportions using Epiinfo version 7.2.3.1. As there are no previous studies on the proportion of fresh MS leaf consumption habits among pregnant women, we assumed a proportion of fresh MS leaf consumption during pregnancy (50%) (48, 49), and a confidence level of 95%, a margin of error of 5%. Considering the design effect of 1.5 for compensation of potential error due to the multistage cluster sampling and estimated non-response rate of 10%, the final sample size was 633.6(634).
A multistage cluster sampling method was used to recruit study participants into the study. From zone two districts were included in the survey. First, 10 kebeles from each of the districts were selected by lottery method. The list of pregnant women was taken from family folders available at the health posts, and samples were proportionally allocated to each of the selected kebeles based on the number of pregnant women with gestational age between 20 and 26 weeks. Finally, the required pregnant women were selected using simple random sampling technique from the sampling frame of pregnant women prepared for each kebele.
The dependent variable was consumption of fresh MS leaves and the independent variables were socio-economic and demographic factors (age of mother, Place of residence, Educational Status), health and obstetric related factors (Gravidity, Number of <5 children, Pre- Contraceptive use, ANC attendance), nutritional factors (Changed dietary intake, Dietary diversity, Food aversion,) and knowledge about MS.
MS consumers: women who consumed fresh moringa leaves at least once in the last 30 days (one month) before the data collection date regardless of amount or frequency were classified as consumers; otherwise they were regarded as non-consumers.
Knowledge about MS was assessed using questions consisting of 10-items, and women with knowledge scores equal to or above the mean score were classified as having good knowledge, and those who scored below the mean score were classified as having poor knowledge.
Women’s nutritional status was assessed using the mid-upper arm circumference (MUAC). This was measured using a flexible, non-stretchable standard tape at the mid-point between the tips of the ulna and the acromion and olecranon processes on the shoulder blade. The MUAC measurement was made on the right arm to the nearest 0.1 cm. Women with MUAC ≥23 centimeters were regarded as well nourished, and those with MUAC <23 centimeters were regarded as undernourished (7).
Minimum dietary diversity (MDD-W): Data were collected using a 24-h dietary recall method according to Food and Agriculture Organizations’ (FAO) 2016 guideline. For each of the 10 food groups, a woman was asked what they ate 24 h before the data collection time with a score of 1 for yes and 0 for no. Scores were calculated by counting the number of food groups. Finally, women with a score of 5 or more out of 10 were categorized as having adequate dietary diversity; otherwise they were regarded as having inadequate dietary diversity (50).
Pregnancy was determined based on women’s self-report of the first day of their last menstrual period (LMP), and gestational age was calculated based on the LMP and the date of data collection (51).
A pre-tested, interviewer-administered, and structured questionnaire, developed in English, and translated into the local language was used to collect data. Diet-related factors were assessed using a validated 24-h food frequency questionnaire (50). Household socioeconomic status was assessed by permanent household assets using a questionnaire adapted from the Ethiopian demographic and health survey household wealth index assessment tool (5).
Data were collected through face-to-face interview using a mobile phone-based application that allows filling of information electronically in both online and offline means and transfer of data to an online server created for this purpose (52). Ten nurses and two public health professionals were assigned to collect and supervise the data, respectively. Before data collection, the data collection teams were trained for 2 days on interview techniques and questionnaire content.
Data were checked daily online for completeness, consistency, and missing values. Once data collection was completed, the raw data were downloaded and exported to STATA statistical software version 14.0 for analysis. Principal component analysis (PCA) was conducted to determine participants’ wealth status and assess women’s knowledge on the importance of consuming fresh MS leaves. Three of the knowledge items [“Can consuming M prevent malnutrition?” “Is MS used as medicine?,” and “Does MS increase breast milk production?”] were removed because of commonalities less than 0.5 (0.49, 0.44, and 0.467, respectively). PCA revealed three factors explaining 85.3% of the total variance, and the factor score of the first factor explaining the maximum variance was used to classify women’s knowledge on the importance of consuming fresh MS leaves. Reliability analysis also showed acceptable internal consistency (Cronbach’s alpha = 0.85). Descriptive statistics including frequencies, percentages, means, and standard deviations were used to describe the characteristics of the study participants. For all explanatory variables, bivariate analysis was performed to assess the presence or absence of association with the outcome variable, and variables with p-values less than 0.25 in the bivariate analysis were included in the multivariable logistic regression analysis model. Adjusted odds ratio with its 95% CI and p-values < 0.05, respectively, were used to determine the degree of association and statistical significance. The results are presented in tables, figures, and texts.
Ethical approval and permission were granted by the Institutional Review Board of Jimma University Institute of Health (reference number: THRPG 1/469/2022). Written approval was obtained from the Gamo zone health department, and health offices of Arba Minch zuria and Chencha districts. Before participation, all participants provided written informed consent as approved by the ethics committee, and all procedures were performed in accordance with the relevant guidelines and regulations of the Declaration of Helsinki on ethical principles for medical research involving human subjects. Data collectors obtained written consent by reading the consent form to participants before the interview and proceeded to interview only after confirming that women were willing to participate in the study. We tried to reduce social desirability bias by conducting interviews with participants in a private place at their homes while at the same time ensuring protection of participants’ privacy, and confidentiality throughout the data collection process.
A total of 623 pregnant women participated in the study giving a response rate of 98.3%. The mean age the participants was 25 years (SD ± 0.17), 500 (80.26%) of the participants were formally unemployed women who were housewives. Over half (51.69%) and two-third (68.86%) respectively were from rural areas and had less than five family members (Table 1).
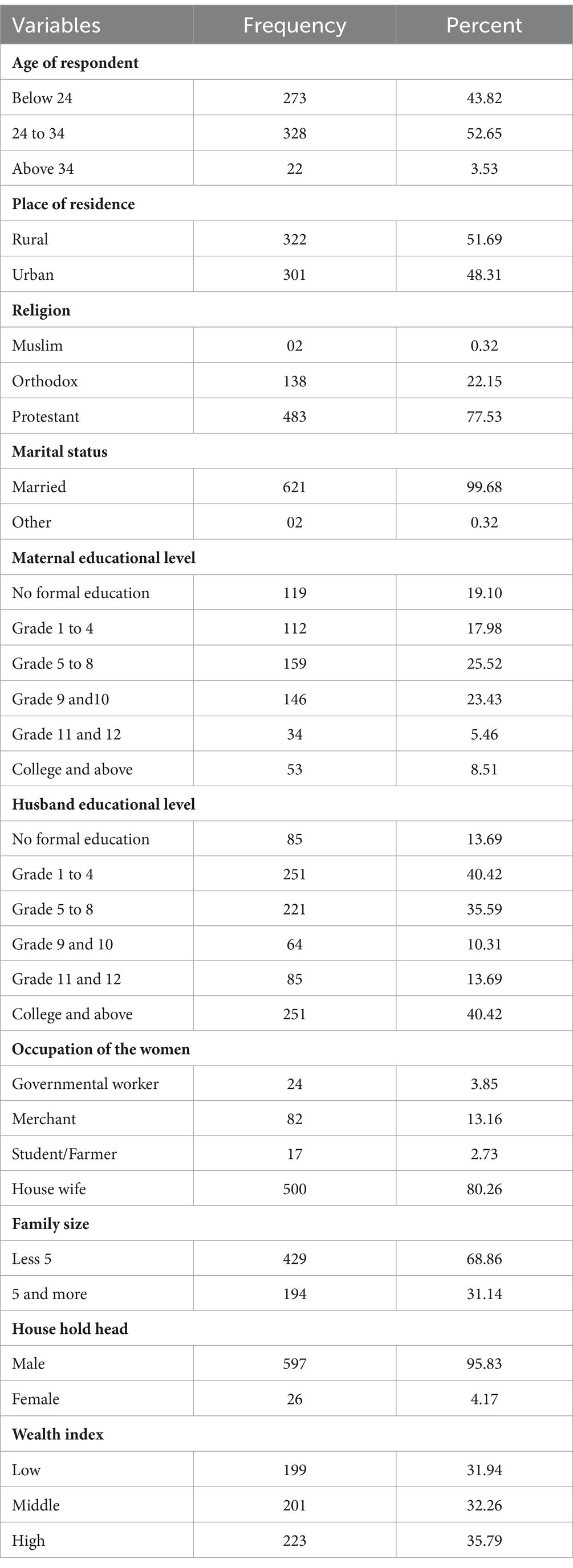
Table 1. Socio-demographic characteristics of pregnant women in Gamo zone, Southern Ethiopia, 2022.
Most of the study participants had less than five pregnancies (91.81%), and deliveries (93.54%).Nearly three-fourth of the participants (72.39%) had history of antenatal attendance (Table 2).

Table 2. Obstetrics and health-related characteristics of pregnant women in Gamo zone, southern Ethiopia, 2022.
Three hundred nine (49.60, 95% CI, 45.67, 53.52%) of the pregnant women consumed fresh MS leaves in the form of “Kurkufa,” ‘fossosie’, and ‘kita” along with ‘haleko’, a local dish made from fresh MS leaves. Nearly one-quarter of the pregnant women (23.27%) were malnourished, and nearly half (46.07%) did not eat the recommended number of meals during this pregnancy. Only 13 participants (2.09%) skipped meals during the current pregnancy (Table 3).
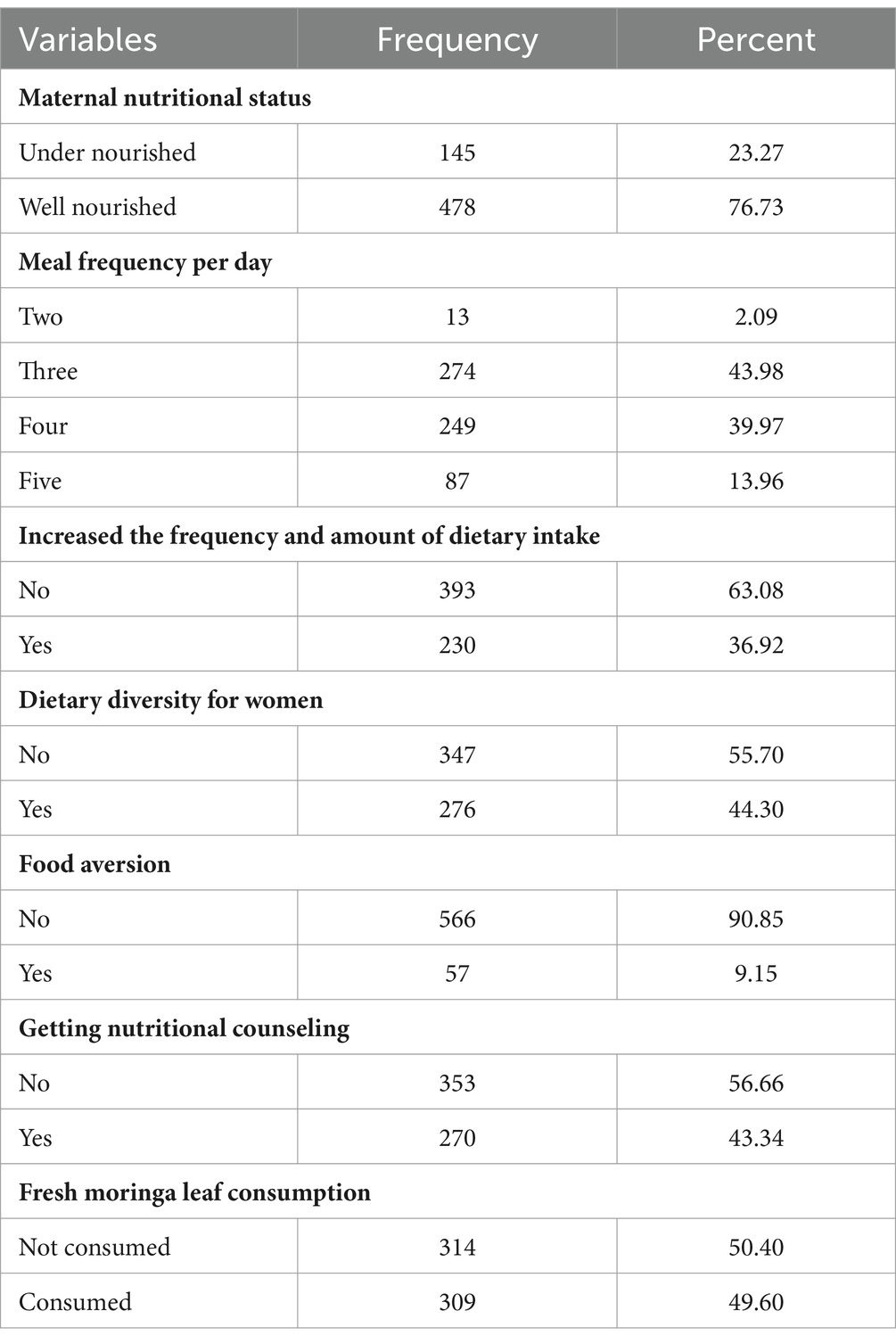
Table 3. Dietary related characteristics of pregnant women in Gamo zone, Southern Ethiopia, 2022.
Two hundred thirty-nine (38.36%) of the study participants had good knowledge about the importance of consuming fresh MS leaves. Participants were most likely to know about the edible parts of the MS tree (57.14%), followed by the importance of consuming MS for the pregnant mother and her fetus (55.22%). However, what they least knew was that MS can be consumed in powder form (1.12%), followed by its use in treating diabetes (11.08%) (Figure 1).

Figure 1. Knowledge of pregnant women on the importance of moringa in Gamo zone, Southern Ethiopia, 2022.
Approximately half of women who consumed fresh MS leaves (44.34%) consumed it three or more times a day, and 178 women (77.4%) used it as a food source (Figure 2).

Figure 2. Frequency of fresh moringa stenopetala leaves consumption among pregnant women in Gamo zone, Southern Ethiopia, 2022.
Of the 12 candidate variables for multivariable logistic regression analysis, seven associated with MS leaf intake during pregnancy. Age, place of residence, attendance to antenatal care, use of contraception before pregnancy, increased number of frequency, and amount of food intake, consumption of five or more food groups within the past 24 h, and women’s knowledge of the importance of consuming fresh MS leaves during pregnancy. The odds of fresh MS leaves intake was higher in women aged <24 years [AOR = 2.92, 95%CI (1.51, 5.63)], and in rural residents [AOR = 1.97, 95% CI (1.10, 3.50)] compared with their age and residence counterparts, respectively. Visited health care facility for ANC [AOR = 2.08, 95% CI (1.03, 4.21)], increased the frequency and quantity of food intake during pregnancy [AOR = 2.89, 95% CI (1.54, 5.41)], consumed five or more food groups in the last 24 h [AOR = 2.33, 95% CI (1.33, 4.08)], using contraceptives before pregnancy [AOR = 1.88, 95% CI (1.03, 3.55)], and had good knowledge on the importance of MS consumption [AOR = 9.76, 95% CI (5.30, 17.95)] were positively associated factors (Table 4).

Table 4. Factors associated with fresh moringa leaf consumption during pregnancy in Gamo zone, southern Ethiopia, 2022.
Pregnancy is a critical period during which significant physiological and biochemical changes occur in the mother and the developing fetus (53). Maternal diet before and during pregnancy is a key factor in the health of the mother as well as the child and can have a lasting impact on the child’s health and future development. MS is a nutritious plant grown in tropical regions of the developing world. All parts of the tree can be used in a variety of beneficial ways, but the leaves are a particularly good source of vitamins and other nutrients. Gram for gram, fresh moringa leaves have been reported to contain seven times more vitamin C than oranges, four times more vitamin A than carrots, three times more iron than spinach, four times more calcium than milk, and three times more vitamin D than cereals. They also contain more potassium than bananas and twice as much protein as yogurt (35). Micronutrient and vitamin intake is an important measure to promote maternal and child nutrition, health, and well-being, and should be continued throughout pregnancy, regardless of the nutritional status of the mother, especially in low- and middle-income countries. Moringa stenopetala leaves contain both micronutrients and vitamins, but consumption is still low in Ethiopia. In this study, we attempted to investigate the intake of fresh MS leaves and factors associated with the consumption among pregnant women in the Gamo zone of southern Ethiopia. The intake rate of fresh MS leaves among pregnant women was 49.60%. This is higher than previous studies in adults in central Ethiopia and Africa (39, 42), but lower than studies in Mauritius, Togo, and India (39, 40, 44). A possible explanation for this difference is probably the difference in culture, food habits, and awareness of the study participants. Pregnant women under 24 years of age were three times more likely to consume fresh MS leaves than those aged 24–34 years. This may be due to globalization, increased access to various media (54), and “education for all” (55) helping to improve dietary habits among young people. This contradicts a study conducted in Mauritius (44). This difference may be due to differences in age and food culture. Our study shows that rural residents are twice more likely to consume fresh MS leaves than urban residents. Similar results were reported in a study in Mauritius (44). A possible reason for this is the ease of growing and obtaining the crop in rural areas, increasing the likelihood of consuming fresh MS. Furthermore, rural residents are less likely to utilize modern healthcare due to lack of awareness and accessibility. Thus, they might rely on traditional medicine which promotes the consumption of MS leaves for its medicinal benefits (56). Pregnant women who visited health facilities for ANC were twice as likely to eat fresh MS leaves compared to non-visitors. The fact that ANC service is a good opportunity to provide pregnant women with advice on proper dietary habits (57) might increase their knowledge on healthy diet during pregnancy, which acts as a fuel for the intake of nutritious foods such as MS (58, 59).
Participants who increased their food intake during pregnancy were three times more likely to eat fresh MS leaves compared to participants who did not increase their food intake during pregnancy. Similarly, women who consumed five or more food groups were approximately twice as likely to consume fresh MS leaves compared to their counterparts. This can be explained by the fact that an increase in the frequency and amount of food intake can be used to increase the possibility of dietary diversity (58, 60). This could be because an increase in the frequency, amount, and food groups of meals could contribute to an increase in the consumption of more diverse foods including fresh MS leaves. Pregnant women with good knowledge about the importance of MS leaves were 10 times more likely to eat MS leaves compared to those with a lack of knowledge. This is in line with studies conducted in Mauritius (44) and Ethiopia (61) and could be because basic knowledge about nutrition can guide food choices (62). Women who used contraceptives before pregnancy were twice as likely to consume fresh MS leaves compared to those who did not. This may be because extended stays in health facilities promote health-promoting behaviors and the consumption of various food groups, increasing the likelihood of consuming fresh MS leaves (58). More than half of the pregnant women in the study area did not eat fresh MS leaves during pregnancy, and the majority of them did not have sufficient knowledge about the importance of MS leaves. The implication of these findings is that improved knowledge about the importance of fresh MS leaves consumption during pregnancy through increased utilization of health services, nutritional advice, and information dissemination could increase the consumption of fresh MS leaves, thereby allowing pregnant women to benefit from the nutritional content of MS.
The study was conducted at the community level in home gardens that provide an amenity to address a sensitive issue and is intended to be generalizable. There is a chance of recall bias on responses about dietary diversity and MS leaves consumption patterns particularly because of our participants background of education and culture. However, we have considered data from the most recent month before the survey period which is deemed to minimize recall bias regarding consumption habits. Added on this, the cross-sectional nature of the data might affect temporality and strength of the evidence reported from this study (63).
The study found that only half of the pregnant women consumed fresh MS leaves during pregnancy. Age, place of residence, utilization of health services (ANC visits and contraceptive use), knowledge about the importance of consuming MS leaves, higher frequency and amount of food intake, and consumption of more than five food groups were independently associated with consumption of fresh MS leaves. Therefore, the relevant authorities should promote the utilization of this wonderful gift to increase knowledge and consumption habits. Furthermore, the above factors associated with MS leaf consumption should be taken into consideration in the efforts. Policymakers should invest more and pay attention to the production of “high quality” food from plants like MS. Further research is needed to determine the amount of fresh MS leaves consumed per meal (per serving) and other relevant factors that may prevent this group from consuming this wonderful plant.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by the Institutional Review Board (of) Institute of Health, Jimma University, with reference number Ref. No. THRPG 1/469/2022. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
ZD: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. GD: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing.
The author(s) declare that financial support was received for the research data collection of this article. This project was financially supported by the Jimma University.
First of all, we would like to thank Jimma University and the Health Institute Postgraduate Coordination Office for giving us the opportunity to participate in research activities. We would like to thank the Gamo zone Health Office, Arba Minch Zuria and Chencha District Health Offices for providing background information. We are extremely grateful to the data collectors and supervisors, without their contribution this study would not have been possible. Furthermore, we would like to thank the study participants who generously sacrificed their time to participate in the interviews and provide us with the necessary information.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
ANC, Antenatal care; AOR, Adjusted odds ratio; APGAR score, Appearance, Pulse, Grimace, Activity, and Respiration; CI, Confidence interval; FAO, Food and Agriculture Organization of the United Nation; GA, Gestational age; MS, Moringa stenopetala; MUAC, Mid Upper Arm Circumference; NICU, Newborn intensive care unit; OR, Odds ratio; PCA, Principal components analysis.
1. UNICEF . UNICEF programming guidance. Prevention of malnutrition in women before and during pregnancy and while breastfeeding. New York: UNICEF (2021).
2. UNICEF . Nutrition, for every child: UNICEF nutrition strategy 2020–2030. New York: UNICEF (2020).
3. Desyibelew, HD, and Dadi, AF. Burden and determinants of malnutrition among pregnant women in Africa: a systematic review and meta-analysis. PLoS One. (2019) 14:e0221712. doi: 10.1371/journal.pone.0221712
4. Getaneh, T, Negesse, A, Dessie, G, Desta, M, Assemie, MA, and Tigabu, A. Predictors of malnutrition among pregnant women in Ethiopia: a systematic review and meta-analysis. Hum Nutr Metabol. (2021) 26:200131. doi: 10.1016/j.hnm.2021.200131
5. Central Statistical Agency/CSA/Ethiopia and ICF . Ethiopia demographic and health survey 2016. Addis Ababa, Ethiopia, and Rockville. Maryland, USA: CSA and ICF (2016).
6. Abraham, S, Miruts, G, and Shumye, A. Magnitude of chronic energy deficiency and its associated factors among women of reproductive age in the Kunama population, Tigray, Ethiopia, in 2014. BMC Nutr. (2015) 1:1–9. doi: 10.1186/s40795-015-0005-y
7. Gelebo, DG, Gebremichael, MA, Asale, GA, and Berbada, DA. Prevalence of undernutrition and its associated factors among pregnant women in Konso district, southern Ethiopia: a community-based cross-sectional study. BMC Nutr. (2021) 7:1–13. doi: 10.1186/s40795-021-00437-z
8. Ahmed, T, Hossain, M, and Sanin, KI. Global burden of maternal and child undernutrition and micronutrient deficiencies. Ann Nutr Metab. (2012) 61:8–17. doi: 10.1159/000345165
9. World Health Organization . Global nutrition targets 2025: Stunting policy brief. Geneva: World Health Organization (2014).
10. Kumar, K, Singh, S, Srivastava, RK, Jahan, S, and Nigam, S. Effect of maternal undernutrition on Foetal outcome. Int J Health Sci Res. (2018) 8:122–128.
11. Khalid, N, Aslam, Z, Kausar, F, Irshad, H, and Anwer, P. Maternal malnutrition and its kick on child growth: an alarming trim for Pakistan. J Food Nutr Popul Health. (2017) 1:24.
12. Jornayvaz, FR, Vollenweider, P, Bochud, M, Mooser, V, Waeber, G, and Marques-Vidal, P. Low birth weight leads to obesity, diabetes and increased leptin levels in adults: the CoLaus study. Cardiovasc Diabetol. (2016) 15:1–10. doi: 10.1186/s12933-016-0389-2
13. Fall, CHD . Nutrition in fetal life and childhood and its linkage with adult non-communicable disease: lessons from birth cohort studies in India. Proc Indian Natl Sci Acad. (2018) 84:881–9. doi: 10.16943/ptinsa/2018/49443
14. Koletzko, B, Godfrey, KM, Poston, L, Szajewska, H, van Goudoever, JB, de Waard, M, et al. Nutrition during pregnancy, lactation and early childhood and its implications for maternal and long-term child health: the early nutrition project recommendations. Ann Nutr Metab. (2019) 74:93–106. doi: 10.1159/000496471
15. Heidari-Beni, M . Early life nutrition and non communicable disease. Primordial Prevent Non Commun Dis. (2019) 1121:33–40. doi: 10.1007/978-3-030-10616-4_4
16. Luyckx, VA, Perico, N, Somaschini, M, Manfellotto, D, Valensise, H, Cetin, I, et al. A developmental approach to the prevention of hypertension and kidney disease: a report from the low birth weight and nephron number working group. Lancet. (2017) 390:424–8. doi: 10.1016/S0140-6736(17)30576-7
18. Meija, L., and Rezeberga, D., Proper maternal nutrition during pregnancy planning and pregnancy: A healthy start in life. Recommendations for health care specialists. Latvia: WHO. (2017). 1–31.
19. Bitew, ZW, Alemu, A, Ayele, EG, and Worku, T. Dietary diversity and practice of pregnant and lactating women in Ethiopia: a systematic review and meta-analysis. Food Sci Nutr. (2021) 9:2686–702. doi: 10.1002/fsn3.2228
21. Jain, N, Kumari, A, Sharma, R, Saini, V, and Jain, M. Drumstick tree–an explicable miracle. Emerg Life Sci Res. (2021) 7:49–55. doi: 10.31783/elsr.2021.714955
22. Morton, JF . The horseradish tree, Moringa pterygosperma (Moringaceae)—a boon to arid lands? Econ Bot. (1991) 45:318–33. doi: 10.1007/BF02887070
23. Mahmood, KT, Mugal, T, and Haq, IU. Moringa oleifera: a natural gift-a review. J Pharm Sci Res. (2010) 2:775.
25. Tekle, A, Belay, A, Kelem, K, Wodajo, B, and Tesfaye, Y. Nutritional profile of Moringa stenopetala species samples collected from different places in Ethiopia. European J. Nutr. Food Saf. (2015) 5:1100–1. doi: 10.9734/EJNFS/2015/21263,
26. Hadju, V, Dassir, M, Sadapotto, A, Putranto, A, Marks, G, and Arundhana, AI. Effects of Moringa Oleifera leaves and honey supplementation during pregnancy on mothers and newborns: a review of the current evidence. Open Access Maced J Med Sci. (2020) 8:208–14. doi: 10.3889/oamjms.2020.4670
27. Nurdin, MS, Imam, A, Thahir, A, and Hadju, V. Supplementations on pregnant women and the potential of Moringa oleifera supplement to prevent adverse pregnancy outcome. Int J Sci Healthc Res. (2018) 3:71–5.
28. Singh, A, and Chaturvedi, N. Medicinal value, herbal gold to combat malnutrition and health benefit of moringa leaf and multipurpose uses of all parts–a review. Plant Arch. (2021) 21:1327–32. doi: 10.51470/PLANTARCHIVES.2021.v21.no1.176
29. Muis, M, Hadju, V, Russeng, S, and Naiem, MF. Effect of moringa leaves extract on occupational stress and nutritional status of pregnant women informal sector workers. Int J Curr Res Acad Rev. (2014) 2:86–92.
30. Astuti, AD, and Rochmaedah, S. The effect of consumption of MORINGA leaves to pregnant WOMEN'S hemoglobin levels in the village of WAIMITAL, KAIRATU district, west SERAM region, MALUKU in 2019. Proceeding International Conference Syedza Saintika. (2020) 1.
31. Kundaryanti, R, and Novelia, S, The effect of Moringa Oleifera on hemoglobin level in pregnancy. (2021).
32. Nadimin, VH, Hadju, V, As'ad, S, Buchari, A, Haruna, I, and Hartono, R. Increasing of nutrition status of pregnant women after supplementation of Moringa leaf extract (Moringa oliefera) in the coastal area of Makassar, Indonesia. Indian J Public Health Res Dev. (2019) 10:521. doi: 10.5958/0976-5506.2019.00102.5
33. Mahmud, NU, Abdullah, T, and Arsunan, AA. The effect of Moringa Oleifera on the life outcome of pregnant and Breastfreeding mothers: Literature review. Medico-Legal Update. (2020) 20
34. Sulistyowati, D, Soejoenoes, A, Hadisaputro, S, and Sujianto, U. Effectiveness of Nano particles of Moringa Oleifera leaf extract on anxiety, serotonin levels in pregnant women with hypertension. NeuroQuantology. (2022) 20:1110. doi: 10.48047/NQ.2022.20.17.NQ880144
35. Haldar, R, and Kosankar, S. Moringa oleifera: the miracle tree. Int J Effect Dietary Supplementation Moringa oleifera Leaf Meal. (2017)
36. Abuye, C, Urga, K, Knapp, H, Selmar, D, Omwega, AM, Imungi, JK, et al. A compositional study of Moringa stenopetala leaves. East Afr Med J. (2003) 80:247–52. doi: 10.4314/eamj.v80i5.8695
37. EHNRI, F . Food composition table for use in Ethiopia part IV. Addis Ababa, Ethiopia: Ethiopian Health and Nutrition Research Institute (1998).
38. Bachewe, FN, and Minten, B. The rising costs of nutritious foods: The case of Ethiopia. Intl Food Policy Res Inst. (2019) 134.
39. Hedhili, A, Akinyemi, BE, Otunola, GA, Ashie-Nikoi, PA, Kulkarni, M, Husson, F, et al. Moringa oleifera lam.: a comparative survey on consumer knowledge, usage, attitude and belief in Africa and India. S Afr J Bot. (2022) 147:153–62. doi: 10.1016/j.sajb.2022.01.009
40. Mensah, TR, Eklou-Lawson, M, Gbeasor-Komlanvi, FA, Ekouevi, DK, Karou, DS, Ameyapoh, Y, et al. Assessment of knowledge and consumption patterns of soybean, Moringa oleifera, Aloe vera and other agro-resources: the case of the elderly and pregnant/nursing women in Lome, Togo. Eur Scient J. (2018) 14:179. doi: 10.19044/esj.2018.v14n3p179
41. Mashamaite, CV, Albien, AJ, Mothapo, PN, Pieterse, PJ, and Phiri, EE. Local knowledge, perceptions, and uses of the potentially conflict-generating plant species, Moringa oleifera lam.: a case study in Limpopo Province, South Africa. Hum Ecol. (2023) 51:979–94. doi: 10.1007/s10745-023-00438-5
42. Terfassa, G, and Negeyo, D. Pre-extension demonstration of Moringa preparation and utilization methods in east Shoa zones of Oromia, Ethiopia. J Biomat. (2020) 4:17–22. doi: 10.11648/j.jb.20200401.12
43. Gandji, K, Salako, VK, Fandohan, AB, Assogbadjo, AE, and Glèlè Kakaï, RL. Factors determining the use and cultivation of Moringa oleifera lam. In the Republic of Benin. Econ Bot. (2018) 72:332–45. doi: 10.1007/s12231-018-9424-4
44. Neergheen-Bhujun, V, Ruhomally, ZB, Dunneram, Y, Boojhawon, R, and Chan Sun, M. Consumption patterns, determinants and barriers of the underutilised Moringa oleifera lam in Mauritius. S Afr J Bot. (2020) 129:91–9. doi: 10.1016/j.sajb.2019.01.027
45. Derbo, ZD, and Debelew, GT. The effect of fresh Moringa leaf consumption during pregnancy on maternal hemoglobin level in southern Ethiopia: multilevel analysis of a comparative cross-sectional study. Int J Women's Health. (2023) 15:1125–37. doi: 10.2147/IJWH.S412241
46. Ethiopia. Office of the Population, and Housing Census Commission . Summary and statistical report of the 2007 population and housing census: Population size by age and sex Federal Democratic Republic of Ethiopia. Addis Ababa, Ethiopia: Population Census Commission (2008).
47. Kelley, AS, and Bollens-Lund, E. Identifying the population with serious illness: the “denominator” challenge. J Palliat Med. (2018) 21:S-7–S-16. doi: 10.1089/jpm.2017.0548
48. Daniel, WW, and Cross, CL. Biostatistics: A foundation for analysis in the health sciences. United States of America: Wiley (2018).
49. Macfarlane, SB . Conducting a descriptive survey: 2. Choosing a sampling strategy. Trop Dr. (1997) 27:14–21. doi: 10.1177/004947559702700108
51. Manca, DP, O’Beirne, M, Lightbody, T, Johnston, DW, Dymianiw, DL, Nastalska, K, et al. The most effective strategy for recruiting a pregnancy cohort: a tale of two cities. BMC Pregnancy Childbirth. (2013) 13:1–7. doi: 10.1186/1471-2393-13-75
52. Lakshminarasimhappa, M . Web-based and smart mobile app for data collection: kobo toolbox/kobo collect. J Ind Lib Assoc. (2022) 57:72–9.
53. Williamson, CS . Nutrition in pregnancy. Nutr. Bull. (2006) 31:28–59. doi: 10.1111/j.1467-3010.2006.00541.x
54. Sharifian, N, Kraal, AZ, Zaheed, AB, Sol, K, Morris, EP, and Zahodne, LB. Measurement invariance of social media use in younger and older adults and links to socioemotional health. Innov Aging. (2021) 5:igab009. doi: 10.1093/geroni/igab009
55. González García, E, Colomo Magaña, E, and Cívico Ariza, A. Quality education as a sustainable development goal in the context of 2030 agenda: bibliometric approach. Sustain For. (2020) 12:5884. doi: 10.3390/su12155884
56. Nwafor, I, Nwafor, C, and Manduna, I. Constraints to cultivation of medicinal plants by smallholder farmers in South Africa. Horticulturae. (2021) 7:531. doi: 10.3390/horticulturae7120531
57. Roba, AA, Tola, A, Dugassa, D, Tefera, M, Gure, T, Worku, T, et al. Antenatal care utilization and nutrition counseling are strongly associated with infant and young child feeding knowledge among rural/semi-urban women in Harari region, eastern Ethiopia. Front Pediatr. (2022) 10:1013051. doi: 10.3389/fped.2022.1013051
58. Dearden, KA, Bishwakarma, R, Crookston, BT, Masau, BT, and Mulokozi, GI. Health facility-based counselling and community outreach are associated with maternal dietary practices in a cross-sectional study from Tanzania. BMC Nutr. (2021) 7:1–11. doi: 10.1186/s40795-021-00447-x
59. Lincetto, O, Gomez, P, and Munjanja, S. Antenatal care In: Opportunities for Africa's newborns: Practical data, policy and programmatic support for newborn care in Africa (2006). 55–62.
60. Mekuria, G, Wubneh, Y, and Tewabe, T. Household dietary diversity and associated factors among residents of Finote Selam town, north West Ethiopia: a cross sectional study. BMC Nutr. (2017) 3:1–6. doi: 10.1186/s40795-017-0148-0
61. Melesse, MB, and van den Berg, M. Consumer nutrition knowledge and dietary behavior in urban Ethiopia: a comprehensive study. Ecol Food Nutr. (2021) 60:244–56. doi: 10.1080/03670244.2020.1835655
62. Spronk, I, Kullen, C, Burdon, C, and O'Connor, H. Relationship between nutrition knowledge and dietary intake. Br J Nutr. (2014) 111:1713–26. doi: 10.1017/S0007114514000087
Keywords: Moringa stenopetala, pregnant women, Gamo zone, southern Ethiopia, consumption
Citation: Derbo ZD and Debelew GT (2024) Fresh Moringa Stenopetala leaves consumption and its determinants among pregnant women in southern Ethiopia. Front. Nutr. 11:1339819. doi: 10.3389/fnut.2024.1339819
Edited by:
Mauro Serafini, University of Teramo, ItalyReviewed by:
Elisa Julianti, Universitas Sumatera Utara, IndonesiaCopyright © 2024 Derbo and Debelew. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zeritu Dewana Derbo, ZGV3YW5hemVyaXR1QGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.