
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr. , 15 May 2024
Sec. Nutrition, Psychology and Brain Health
Volume 11 - 2024 | https://doi.org/10.3389/fnut.2024.1335979
This article is part of the Research Topic Nutrition and Neurobehaviors View all 18 articles
 Angel Gabriel Garrido-Dzib1,2
Angel Gabriel Garrido-Dzib1,2 Berenice Palacios-González3*
Berenice Palacios-González3* María Luisa Ávila-Escalante2Erandi Bravo-Armenta1
María Luisa Ávila-Escalante2Erandi Bravo-Armenta1 Azalia Avila-Nava1
Azalia Avila-Nava1 Ana Ligia Gutiérrez-Solis1*
Ana Ligia Gutiérrez-Solis1*Background: Some dietary patterns and dietary components have an important role in preventing and helping to improve patients’ quality of life of individuals with Mild Cognitive Impairment (MCI) and dementia. In Mexico, it is unknown what the dietary patterns are among older adults with MCI and dementia. We aimed to identify the dietary patterns of older adults with MCI and dementia living in Yucatan, Mexico.
Methods: A cross-sectional study was carried out among 39 patients as controls and 34 individuals as cases (MCI and dementia). A food frequency questionnaire collected diet information, anthropometric and clinical parameters, and lifestyle characteristics. The dietary patterns were evaluated through Partial Least-Squares Discriminant Analysis (PLS-DA).
Results: The food groups that showed discrimination between groups and were classified into the dietary patterns of MCI and dementia individuals were “pastries and cookies,” “soups,” and “legumes.” The dietary pattern of older adults without cognitive impairment was characterized by “nuts and seeds,” “candies,” “vegetables,” “coffee and tea,” and “water.” The consumption of “pastries and cookies” showed an increasing correlation with serum insulin levels (r = 0.36, p = 0.01), and “soups” showed an inverse correlation with total cholesterol levels (r = −0.36, p = 0.02) in patients with MCI and dementia. In controls, there is a positive correlation between the consumption of “nuts and seeds” (r = 0.333, p = 0.01) and “vegetables” (r = 0.32, p = 0.02) with levels of urea; “coffee and tea” showed a positive association with levels of insulin (r = 0.378, p = 0.05).
Conclusion: The dietary pattern of individuals with MCI and dementia has some nutritional deficiencies. Including an adequate intake of vegetables, fruits, and protein could improve the quality of life of subjects living with these conditions in Yucatan, Mexico.
The 2022 census shows that around 15 million older adults live in Mexico. Currently, 14% of the Mexican population is 60 or older (1). Older age remains one of the main risk factors associated with mild cognitive impairment (MCI) and dementia (2, 3). The Study on Aging and Dementia in Mexico (SADEM) reported a prevalence of 7.8% of older adults with Alzheimer’s Disease (AD) living in Mexico; this is the most common type of dementia among older people (4). MCI is a neurocognitive state between normal cognitive aging and dementia and can be detected in younger adults around 55 years old (5). Both conditions are characterized by a deterioration of cognitive function that prevents daily activities and reduces the quality of life (6).
Even though the physiopathology of dementia is still under research, some well-established lifestyle factors, such as physical activity, reducing alcohol consumption, and having an adequate nutritional status, have been associated with reducing the risk of MCI and dementia (7–9). Some dietary and nutritional components have been linked to the deterioration or improvement of cognitive function (10).
A recently published meta-analysis found that the diet of individuals with MCI and dementia living in Latin American Countries is characterized by a lower intake of fruits and vegetables and high consumption of simple carbohydrates and animal protein (11). As mentioned above, the importance of diet in delaying the intrinsic causes of pathologies and diseases associated with aging has been recognized for a long time. Over the last decades, evidence has accumulated on the protective role of bioactive compounds on the risk of chronic non-communicable diseases and even longevity and aging. However, understanding the net impact of diet on health is more complex than studying isolated components or foods. Humans do not consume individual foods but mixed food combinations that form a dietary pattern. Therefore, from a physiological point of view, analyzing eating habits considering the interactions between different foods and their components is of primary interest (12). As a result, it’s crucial to evaluate the diet as a whole. The principal components analysis (PCA) considers complex diets and multiple food groups instead of individual nutrients, specific foods, or food groups for pattern classification. Besides, dietary patterns can reflect an individual’s food preferences; therefore, dietary pattern analysis may add more information to reflect the complexity of dietary intake and provide new insights into the whole foods diet (13).
More recently, it has been suggested that dietary patterns and some dietary components have an important role in preventing these conditions and in helping to improve patients’ quality of life during the disease at different stages (12, 14). Many healthy dietary patterns have been associated with improved cognitive function, and these dietary patterns have several components in common: a high consumption of fruits, vegetables, and whole grains, along with a low consumption of red meat and sweets. However, it is unknown what the dietary patterns are among older adults with MCI and dementia in Mexico; therefore, this study aimed to identify the dietary patterns of older adults with MCI and dementia living in Yucatan, Mexico.
The present cross-sectional study was carried out between February 2022 and January 2023. The group of cases included individuals who attended the outpatient specialty unit of neurology and geriatrics at the Regional High Speciality Hospital, IMSS-Bienestar in Merida, Yucatan, Mexico, with diagnoses of MCI and dementia. For controls, individuals without MCI or dementia were included. Patients under medical treatment for specific diseases in the cardiology, endocrinology, respiratory, urology, and oncology units and individuals with implanted medical devices such as pacemakers or prostheses were excluded from the study. To ensure the representativeness of the population, a sample size was calculated using an unmatched case–control formula for an unknown population with a 95% two-sided confidence level, 90% power, 50% of controls exposed, and a 0.06 odds ratio (15). From this calculation, the minimum required sample size was 24 individuals in each group. Finally, a sample of 39 patients as controls and 34 individuals as cases (MCI and dementia) were selected for this study.
The study was approved by the Ethics Committee of the Regional High Speciality Hospital, IMSS-Bienestar (no. CONBIOETICA-31-CEI-002-20170731) in connection with a research project (identification code: 2021–012), following the guidelines for human experiments as laid down in the Helsinki Declaration. The participants signed the informed consent form before the start of the study.
Participants had a previously established diagnosis of dementia or MCI by a neurologist or geriatrician. Diagnoses were made following internationally accepted criteria for dementia. The diagnostic and statistical manual of mental disorders-V (DSM-V), ICD-10, and MCI Petersen criteria were used (16, 17). Additionally, subjects with dementia were evaluated using the mini-mental state examination (MMSE) and MCI individuals by the Montreal Cognitive Assessment (MoCA) (18, 19).
The habitual diet was assessed using a semi-quantitative food frequency questionnaire (SFFQ) previously validated in the Mexican population and administered by a trained dietician (20, 21); if the participant could not respond, the information was provided by the primary caregiver. The SFFQ contained 140 items grouped into previously pre-validated food groups by Gaona et al. (22) (Supplementary Table S1). For the analysis, only those food groups that reported 70% or more of consumption were included; 19 food groups were obtained. The SFFQ data were then converted to grams or milliliters per week consumption by multiplying the standard serving size. Foods were recorded in grams (g), and drinks and broths in milliliters (mL). However, to have similar units of measurement among foods and beverages, the milliliters per week were converted to cup units by dividing between 240 mL, resulting in cups per week.
Waist circumference (WC) (cm) was measured from individuals to the nearest 0.1 cm using an anthropometric tape measure (Lufkin, United States) at the midpoint between the lower costal margin and the superior of the iliac crest. Weight and height were measured using a calibrated scale. Body mass index (BMI) was calculated as weight divided by the square of height (kg/m2). Blood pressure (BP) (systolic and diastolic, SBP and DBP, respectively) was estimated after 15 min of rest in the sitting position using an automatic electronic sphygmomanometer (Omron, Japan). A pre-validated questionnaire was used to collect a brief clinical history of the participants, such as pre-existing diseases and lifestyle.
Following standard procedure, a trained researcher collected a blood sample after 12 h of overnight fasting. Clinical biochemistry tests were done following standard protocol to estimate levels of triglycerides (TG) (mg/dL), high-density lipoprotein cholesterol (HDL-C) (mg/dL), total cholesterol (mg/dL), fasting plasma glucose (FPG) (mg/dL), insulin (μIU/mL), glycated hemoglobin (HbA1c) (%), urea (mg/dL), creatinine (mg/dL), and uric acid (mg/dL). A pre-validated equipment (autoanalyzer COBAS® Integra 400 Plus, Roche Diagnostics) was used for the clinical biochemistry tests.
The statistical packages Jamovi (version 2.25, Sydney, Australia) and SPSS version 15.00 (IBM Corp, Armonk, New York, United States) were used to analyze the data. Descriptive statistics were calculated for the control and cases (MCI and dementia) groups. The Shapiro–Wilk test was used to check the normality. Clinical and serum biomarkers characteristics were presented as means ± standard deviation (SD) or medians and interquartile range (IQR). Proportions and corresponding percentages (%) were reported for comorbidities and lifestyles and tested by Pearson’s chi-squared test. Continuous variables between groups were compared using the independent t-test or the Mann–Whitney U test. A Spearman correlation analysis assessed the relationship between group foods and serum biomarkers. For all analyses, statistical significance was set at p < 0.05.
The web-based platform Metaboanalyst 5.0 was used to identify discrimination among food groups through partial least-squares discriminant analysis (PLS-DA) (23). For dietary patterns, the selected methods were: Row-wise; normalization: Normalization to constant sum; Data transformation: Cubic Root Transformation; and Data scaling: Autoscaling. Permutation testing was conducted to minimize the possibility that the observed separation on PLS-DA was by chance. Additionally, for cross-validation (R2, Q2, and accuracy), model validation was performed using a 2000 times permutation test. A loading scatter plot was constructed to determine the variables discriminating between the groups. The variable importance in the projection (VIP) plot was performed based on their significance in discerning studies from both groups. VIP cutoff >1.0 was designated since the number of variables in this study was less than 100 (24).
Seventy-three participants were analyzed, including 39 controls and 34 cases (17 individuals with MCI and 17 with dementia). Overall, cases (73.4 ± 10.10) were older than controls (67.2 ± 6.52) (p = 0.002), had a higher frequency of women (68.4%, p = 0.097), hypertension (50%, p = 0.056), and metabolic syndrome (MetS) (70%, p = 0.913). Besides, taking medication was significantly higher among participants with MCI and dementia (91%, p < 0.0001) (Table 1).
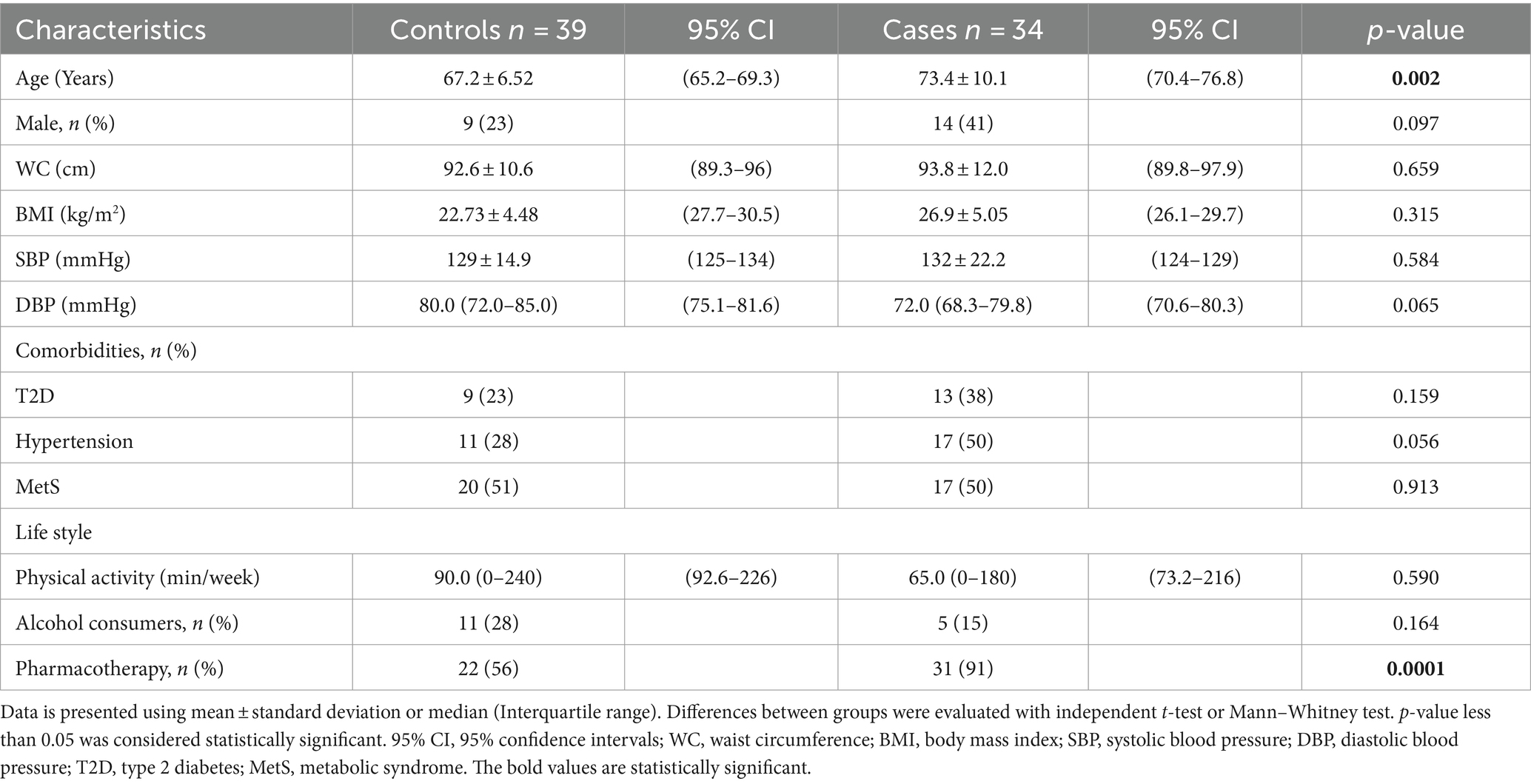
Table 1. General characteristics among controls and cases.
Levels of urea (39.1 (29.1–44.5) vs. 31.8 (23.3–34) mg/dL, p = 0.013), creatinine (0.94 (0.80–1.06) vs. 0.73 (0.64–0.88) mg/dL, p < 0.001), and percentage of HbA1c (5.96 (5.64–6.51) vs. 5.61 (5.30–6.03) %, p = 0.033) were significantly higher among cases than controls. Overall levels of other parameters such as triglycerides, cholesterol, FPG, insulin, and UA increased in the case group (Table 2).
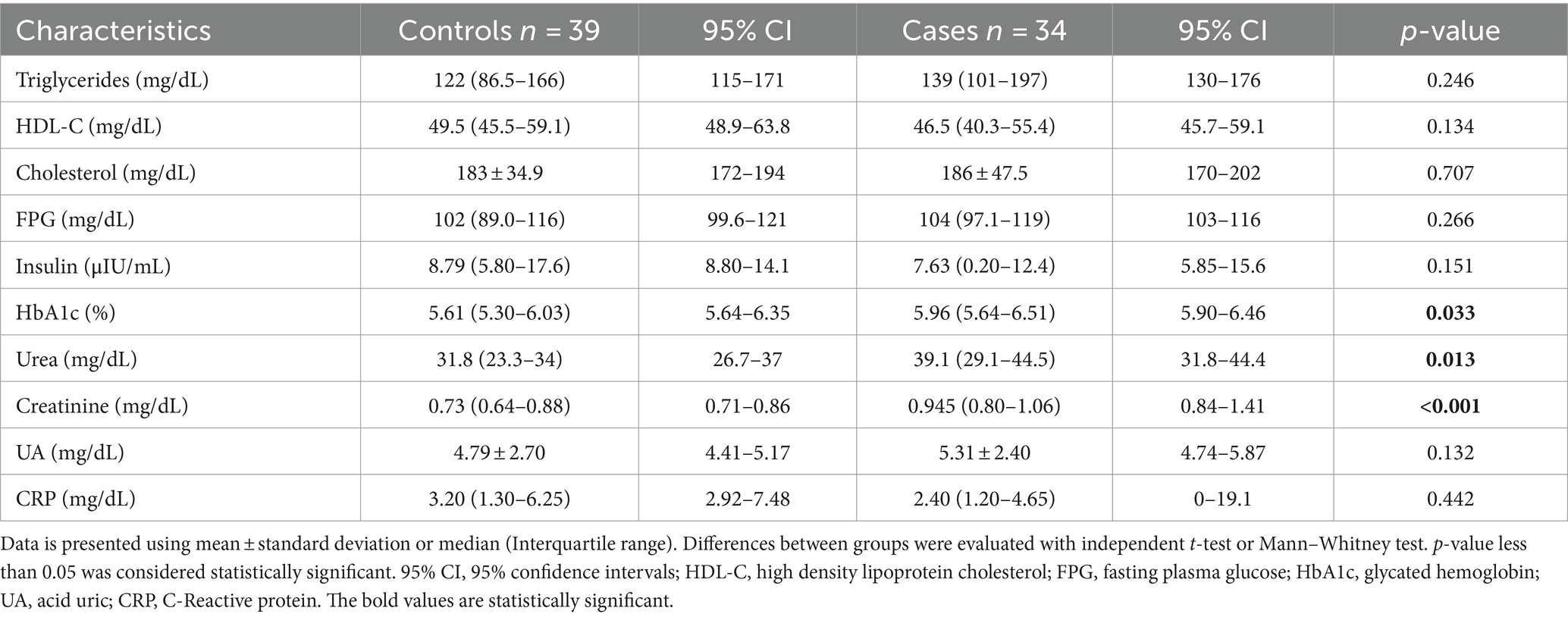
Table 2. Biochemical parameters among controls and cases.
The PLS-DA score plots presented slight evidence of separation according to having MCI and dementia vs. older adults without neurocognitive disease (Figures 1A,B). This difference between groups showed an accuracy of 0.69, R2: 0.354, Q2: 0.108, and permutation p value <0.005. The VIP plot revealed that “pastries and cookies,” “soups,” and “legumes” are responsible for discrimination among patients with MCI and dementia (Figure 1C). “Nuts and seeds,” “candies,” “vegetables,” “coffee and tea,” and “water” were the food groups that were found to be in charge of differentiation in the control group.
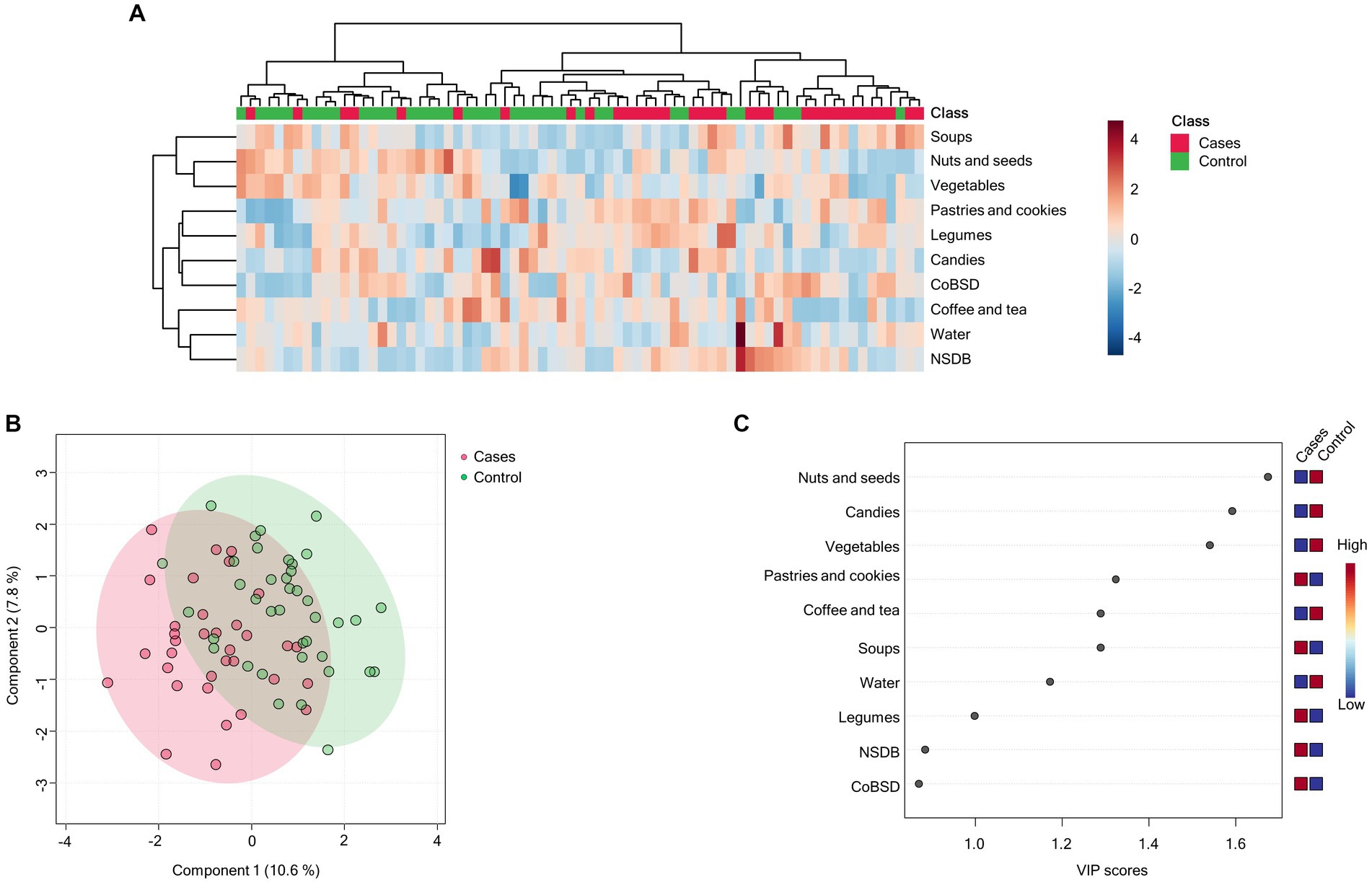
Figure 1. Dietary patterns are profiled according to the group of cases (MCI and dementia) and control. (A) Hierarchical heatmap for dietary patterns: control (green) and cases (red); red and blue show increasing and decreasing food group consumption, respectively. (B) The PLS-DA plot shows separation between cases (red) and controls (green). The explained variances are shown in brackets (accuracy: 0.69; R2: 0.354; Q2: 0.108; permutation p value <0.005). (C) The VIP analysis represents the relative contribution of food groups to the variance among groups. A high VIP score indicates a greater contribution of the food group to the dietary pattern. Red and blue boxes on the right indicate whether food group consumption is increased (red) or decreased (blue).
The consumption of “pastries and cookies” showed an increasing correlation with serum insulin levels (r = 0.36, p = 0.018), and the consumption of “soups” showed an inverse correlation with total cholesterol levels (r = −0.36, p = 0.02) in patients with MCI and dementia (Figures 2A,B; Supplementary Table S2). In controls, there is a positive correlation between the consumption of “nuts and seeds” (r = 0.333, p = 0.018) and “vegetables” (r = 0.32, p = 0.023) with levels of urea, meaning levels of urea significantly increase as the consumption of nuts and seeds and vegetables increases (Figures 3A,B). Additionally, the consumption of “coffee and tea” showed a positive association with levels of insulin (r = 0.38, p = 0.009) (Figure 3C; Supplementary Table S3).
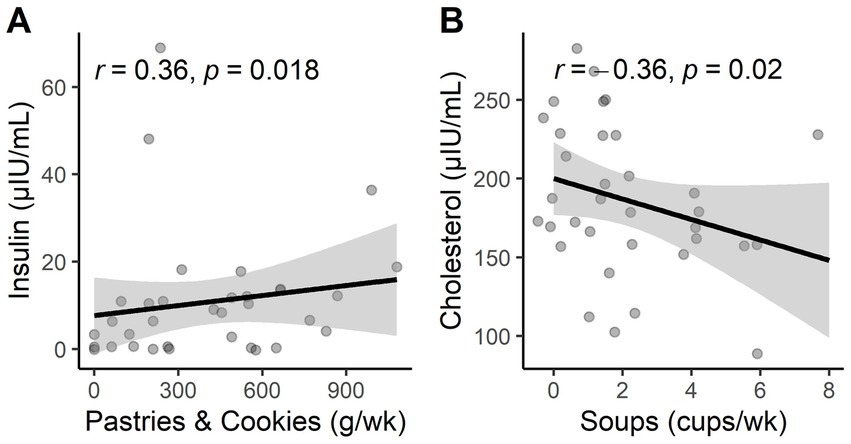
Figure 2. (A) Statistical correlations of pastries and cookie consumption with insulin levels in cases. (B) Statistical correlations of soup consumption with cholesterol levels in cases.
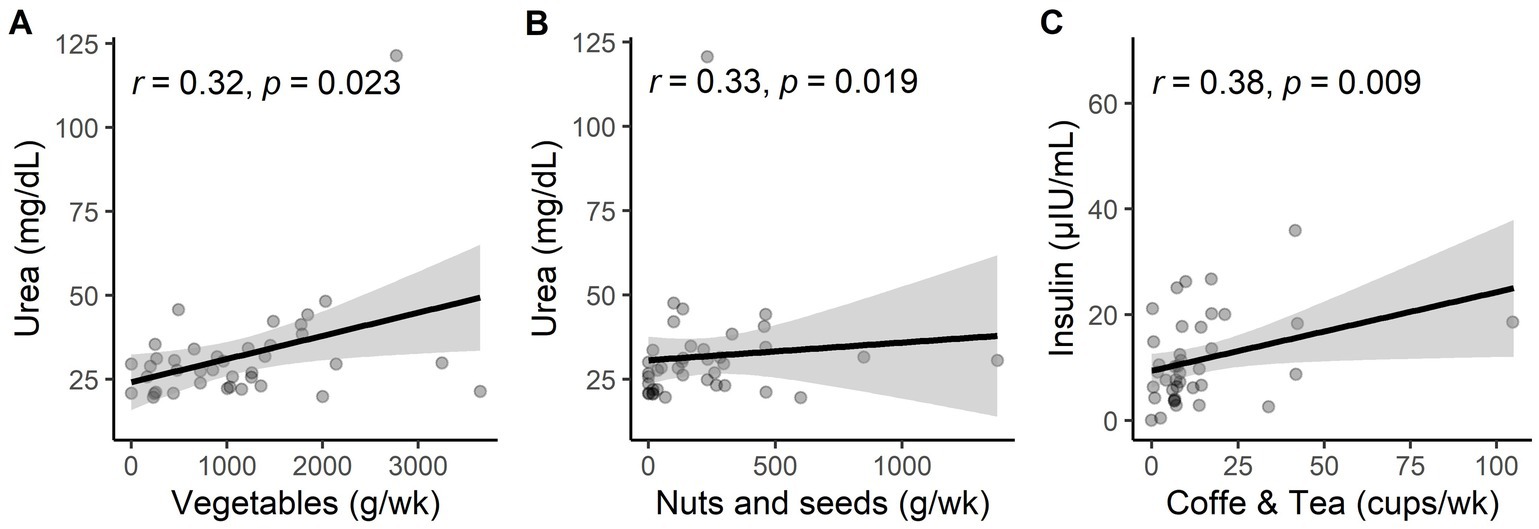
Figure 3. (A) Statistical correlations of vegetable consumption with urea levels in the control group. (B) Statistical correlations of nuts and seeds consumption with urea levels in the control group. (C) Statistical correlations of coffee and tea consumption with insulin levels in the control group.
The correlation between serum biomarkers and food groups, adjusting sex and age, was performed through a linear regression analysis using a rank transformation of variables. In the case group, the interaction of insulin and “pastries and cookies” was strong and significant (β = 0.391, p = 0.026); however, the correlation between “soups” and cholesterol levels was no longer significant after adjusting (β = −0.35, p = 0.052). In the control group, the interaction between insulin levels and “coffee and tea” (β = 0.33, p = 0.033), urea with “nuts and seeds” (β = 0.37, p = 0.021), and urea and “vegetables” (β = 0.35, p = 0.025) stayed significant and stronger after adjusting for sex and age.
This study identified two dietary patterns in the Mexican older adult population. The food groups that showed discrimination between groups and were classified into the dietary patterns of MCI and dementia individuals were “pastries and cookies,” “soups,” and “legumes.” The dietary pattern of older adults without cognitive impairment was characterized by the following food groups: “nuts and seeds,” “candies,” “vegetables,” “coffee and tea,” and “water.”
The focus of scientific nutrition research has shifted from examining the impact of individual foods and nutrients on health to examining dietary patterns that represent the combined intake of several meals and nutrients (13, 25). However, it is important to consider that dietary patterns might differ based on factors like age, culture, way of life, socioeconomic situation, and state of health (26).
In our study, the MCI and dementia dietary pattern included both “healthy” and “unhealthy” food groups, which are characterized by high consumption of “pastries and cookies,” “soups,” and “legumes,” this was also found among Korean and Chinese adults with MCI (27, 28). The food group “pastries and cookies” has been distinguished by its high content of added sugars, saturated and trans fats, salt, and additives that have been associated with cognitive impairment in prior research (29). The consumption of these products has been linked to intestinal dysbiosis, the promotion of proinflammatory cytokines, and metabolic alterations, which generate alterations in various organs, including brain damage (30–32). On the other hand, the food group “legumes” was primarily characterized by the consumption of beans, which have conflicting findings regarding their impact on health. Since ancient times, eating beans has been a staple of the Mexican diet (33). Flavonoids are the principal compounds of beans and have been associated with a lower risk of AD (34); however, there is still a gap in our knowledge of the underlying mechanisms and their association with brain health. Moreover, there is no daily intake recommendation for flavonoids in the diet.
Mixed vegetables and chicken soup were the types of food that were more frequent in the food group “soups.” Poultry and vegetables (especially leafy green vegetables) are two foods recommended in the diet to lower or prevent dementia (21). However, there is not sufficient literature that examines the benefits of the consumption of mixed vegetables and chicken soup on individuals with dementia. Mixed vegetables and chicken soup comprise several ingredients that could work synergistically at multiple targets on a neurocognitive level (35, 36).
The dietary pattern in the control group of older adults included healthier food groups in comparison to the MCI and dementia dietary patterns. Food groups such as “nuts and seeds,” “vegetables,” “coffee and tea,” and “water” were reported. Only “candies” could be identified as an unhealthy food group.
The reported more frequent vegetables among the study population included tomatoes and onions. One of the main bioactive compounds of the tomato is lycopene (37). Lycopene is a natural neuroprotective agent. This carotenoid seems to contribute to cognitive longevity and treat several neuronal diseases, including cerebral ischemia, Parkinson’s disease (PD), AD, and depression (38). Quercetin is a bioactive compound of the onion and another type of flavonoid (39). Its cognitive function was examined in a randomized, double-blind, placebo-controlled, parallel-group comparative clinical trial that evaluated the consumption of quercetin-rich onion for 24 weeks compared to quercetin-free onion as a placebo. Quercetin-rich onions reduce age-related cognitive decline, possibly by improving emotional conditions in healthy older adults from Japan (40). The pretreatment with quercetin significantly enhanced the expression levels of endogenous antioxidant enzymes such as Cu/Zn superoxide dismutase (Cu/Zn, SOD), manganese SOD (Mn/SOD), catalase (CAT), and GSH peroxidase in the hippocampal CA1 pyramidal neurons of animals suffering from ischemic injury. Thus, quercetin may be a neuroprotective agent for transient ischemia (41).
Caffeine is an alkaloid found in coffee, tea, and soft drinks (42). Consumption has been reported to decrease the risk of dementia (43). Vincenzo et al. found that people who regularly drank one to two cups of coffee daily had a reduced incidence of MCI than those who did not drink coffee (44). However, some other studies have shown that caffeine intake does not help improve neurocognitive abilities in men, only in women (45).
A high frequency of sugar consumption is associated with several conditions in older adults, such as type 2 diabetes, stroke, cancer, and dementia. Excessive sugar consumption has been linked to neurocognitive dysfunction. Also, it was found in animal models using rats that high sugar consumption may cause neuroinflammation in the hippocampal region (46).
Although the number of participants was fewer than the variables, PLS-DA has been reported to be able to use small sample sizes (47). In our analysis, the model fit (R2: 0.354) was moderate, and consistency (Q2: 0.108) showed that the results obtained had an accuracy of 0.69. Additionally, the permutation (10/2000) was reported to be statistically significant (p value <0.005). These results suggest that the obtained dietary patterns were relatively consistent and reliable; however, a larger sample could result in a stronger association with more power.
Some associations were found between serum biomarkers, food groups, and dietary patterns. Among the dietary patterns in cases (MCI and dementia individuals) where the consumption of “pastries and cookies” was positively associated with insulin levels, eating sugar-filled pastries or candies can cause blood glucose levels to rise, leading the pancreas to produce the hormone insulin (48). High levels of insulin and glucose will cause damage to the blood vessels of the brain, leading to a decline in mental capacity (49). Another food group that showed a significant association with cholesterol levels was “soups.” A negative relationship was found between “soups” and cholesterol, meaning that levels of cholesterol decrease with increasing consumption of “soup,” this could be explained by the addition of vegetables to soup, which increases the consumption of healthy foods such as fiber (50) and phytosterols (51) in the diet, both of which can help lower cholesterol levels.
In the dietary pattern of the control group, it was reported that there was a positive association between increased levels of urea and the consumption of “nuts and seeds” and “vegetables. “It has been reported that intake of these food groups could reduce urea levels in adults. However, these contradictory findings could be explained by the addition of salt to both food groups. Typically, the preparation and consumption of these food groups in this region of Mexico are accompanied by high amounts of salt (52). Lastly, insulin levels were positively associated with the consumption of coffee and tea; this association could be explained by the fact that 59% of older adults from this study reported sweetening their coffee and tea. In particular, the contribution of each source of salt and sugar consumption can vary according to culture, age groups, habits, and dietary practices.
Moreover, the dietary assessment tools need to allow for precise measurement. Further studies may focus on identifying dietary patterns and the intake of micro and macronutrients among MCI and dementia populations. These days, “Omics” technologies have advanced our understanding of individual and population health at the systems level. Specifically, metabolomics has enabled the identification of “metabotypes,” easily measured in urine or blood. Therefore, this method could result in objective biomarkers of foods, nutrients, and dietary patterns in individuals with MCI and dementia.
The absence of information on the participants’ type of dementia is a limitation of the current work; this will be crucial to investigate because Yucatán has been reported to have high rates of obesity, overweight, and other comorbidities linked to MCI and dementia. The results, however, provide the first information about the type of dietary pattern in older Mexican adults with these conditions. The implementation of long-term studies will help to identify and comprehend the association and underlying mechanisms of dietary patterns and serum biomarkers.
We found that the MCI and dementia dietary patterns have some nutritional deficiencies. They were characterized by high consumption of “pastries and cookies,” “soups,” and “legumes.” An adequate intake of vegetables, fruits, and protein could improve the quality of life of subjects living with these conditions in Yucatan.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding authors.
The studies involving humans were approved by Comité de Investigación & Comité de Ética en Investigación del Hospital Regional de Alta Especialidad. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
AG-D: Data curation, Investigation, Methodology, Project administration, Validation, Writing – review & editing, Visualization. BP-G: Investigation, Methodology, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing, Software. MÁ-E: Investigation, Resources, Supervision, Validation, Writing – review & editing. EB-A: Investigation, Resources, Supervision, Writing – review & editing. AA-N: Investigation, Resources, Supervision, Validation, Visualization, Writing – review & editing. AG-S: Conceptualization, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. Monetary sponsorship for the publication of this article was received from the Laboratorio de Envejecimiento Saludable del Instituto Nacional de Medicina Genómica (INMEGEN).
The authors are very grateful to the participants. We also thank Julio Vega for helping with data analysis and Valeria Magallón and Geovanni Chávez for additional technical support. AG-D received a scholarship from CONAHCyT (CVU 1142884). The present work was carried out under the framework of the Secretaría de Educación, Ciencia, Tecnología e Innovación de la Ciudad de México (SECTEI/227/2021).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2024.1335979/full#supplementary-material
1. Instituto Nacional de Estadística y Geografía (INEGI). Estadísticas a Propósito del Día Internacional de las Personas de Edad Datos Nacionales. (2022). https://inegi.org.mx/contenidos/saladeprensa/aproposito/2022/EAP_ADULMAY2022.pdf
2. Xu, Z, Zhang, D, Sit, RWS, Wong, C, Tiu, JYS, Chan, DCC, et al. Incidence of and risk factors for mild cognitive impairment in Chinese older adults with multimorbidity in Hong Kong. Sci Rep. (2020) 10:4137. doi: 10.1038/s41598-020-60901-x
3. Prince, MJ, Wu, F, Guo, Y, Robledo, LMG, O'Donnell, M, Sullivan, R, et al. The burden of disease in older people and implications for health policy and practice. Lancet. (2015) 385:549–62. doi: 10.1016/S0140-6736(14)61347-7
4. Juarez-Cedillo, T, Gonzelez-Figueroa, E, Gutierez-Gutierez, L, Aguilar-Navarro, SG, Garcia-Cruz, JC, Escobedo de la Peña, J, et al. Prevalence of dementia and Main subtypes in Mexico: the study on aging and dementia in Mexico (SADEM). J Alzheimers Dis. (2022) 89:931–41. doi: 10.3233/jad-220012
5. Petersen, RC, Caracciolo, B, Brayne, C, Gauthier, S, Jelic, V, and Fratiglioni, L. Mild cognitive impairment: a concept in evolution. J Intern Med. (2014) 275:214–28. doi: 10.1111/joim.12190
6. Jongsiriyanyong, S, and Limpawattana, P. Mild cognitive impairment in clinical practice: a review article. Am J Alzheimers Dis Other Dement. (2018) 33:500–7. doi: 10.1177/1533317518791401
7. Ranson, JM, Rittman, T, Hayat, S, Brayne, C, Jessen, F, Blennow, K, et al. Modifiable risk factors for dementia and dementia risk profiling. A user manual for brain health services—part 2 of 6. Alzheimers Res Ther. (2021) 13:169. doi: 10.1186/s13195-021-00895-4
8. Jia, L, Du, Y, Chu, L, Zhang, Z, Li, F, Lyu, D, et al. Prevalence, risk factors, and management of dementia and mild cognitive impairment in adults aged 60 years or older in China: a cross-sectional study. Lancet Public Health. (2020) 5:e661–71. doi: 10.1016/s2468-2667(20)30185-7
9. Livingston, G, Huntley, J, Sommerlad, A, Ames, D, Ballard, C, Banerjee, S, et al. Dementia prevention, intervention, and care: 2020 report of the lancet commission. Lancet. (2020) 396:413–46. doi: 10.1016/s0140-6736(20)30367-6
10. Dominguez, LJ, Veronese, N, Vernuccio, L, Catanese, G, Inzerillo, F, Salemi, G, et al. Nutrition, physical activity, and other lifestyle factors in the prevention of cognitive decline and dementia. Nutrients. (2021) 13:4080. doi: 10.3390/nu13114080
11. Garrido-Dzib, AG, Chávez-Loría, G, Magallón-Zertuche, V, Avila-Nava, A, Palacios-González, B, and Gutiérrez-Solis, AL. Micro-and macronutrient intake and food group frequency consumed by subjects with cognitive impairment and dementia in Latin America: a systematic review. J Alzheimers Dis. (2023) 94:425–39. doi: 10.3233/jad-230231
12. U.S Department of Agriculture and U.S Department of Health and Human Services. Dietary guidelines for Americans, 2020–2025. 9th ed (2020). Available at: https://www.dietaryguidelines.gov/sites/default/files/2020-12/Dietary_Guidelines_for_Americans_2020-2025.pdf
13. Allès, B, Samieri, C, Féart, C, Jutand, MA, Laurin, D, and Barberger-Gateau, P. Dietary patterns: a novel approach to examine the link between nutrition and cognitive function in older individuals. Nutr Res Rev. (2012) 25:207–22. doi: 10.1017/s0954422412000133
14. Cao, L, Tan, L, Wang, HF, Jiang, T, Zhu, XC, Lu, H, et al. Dietary patterns and risk of dementia: a systematic review and Meta-analysis of cohort studies. Mol Neurobiol. (2016) 53:6144–54. doi: 10.1007/s12035-015-9516-4
15. Shin, D, Lee, KW, Kim, MH, Kim, HJ, An, YS, and Chung, HK. Identifying dietary patterns associated with mild cognitive impairment in older Korean adults using reduced rank regression. Int J Environ Res Public Health. (2018) 15:100. doi: 10.3390/ijerph15010100
16. APA, Associación Psiquiátrica Americana. Diagnostic and statistical manual of mental disorders The American Psychiatric Association (2013).
17. Petersen, RC, Smith, GE, Waring, SC, Ivnik, RJ, Tangalos, EG, and Kokmen, E. Mild cognitive impairment: clinical characterization and outcome. Arch Neurol. (1999) 56:303–8. doi: 10.1001/archneur.56.3.303
18. Su, Y, Dong, J, Sun, J, Zhang, Y, Ma, S, Li, M, et al. Cognitive function assessed by Mini-mental state examination and risk of all-cause mortality: a community-based prospective cohort study. BMC Geriatr. (2021) 21:524. doi: 10.1186/s12877-021-02471-9
19. Aguilar Navarro, SG, Mimenza Alvarado, AJ, Palacios García, AA, Samudio Cruz, A, Gutiérrez Gutiérrez, LA, and Ávila Funes, JA. Validez y confiabilidad del MoCA (Montreal Cognitive Assessment) para el tamizaje del deterioro cognoscitivo en México. Rev Colomb Psiquiatr. (2018) 47:237–43. doi: 10.1016/j.rcp.2017.05.003
20. Instituto Nacional de Salud Pública, Instituto Nacional de Estadística y Geografía. Base de datos y cuestionario para ENSANUT 2018. (2019). Available at: https://ensanut.insp.mx/encuestas/ensanut2018/doctos/informes/ensanut_2018_informe_final.pdf
21. Hernández-Avila, M, Romieu, I, Parra, S, Hernández-Avila, J, Madrigal, H, and Willett, W. Validity and reproducibility of a food frequency questionnaire to assess dietary intake of women living in Mexico City. Salud Publica Mex. (1998) 40:133–40. doi: 10.1590/s0036-36341998000200005
22. Gaona-Pineda, EB, Martinez-Tapia, B, Rodríguez-Ramírez, S, Guerrero-Zúñiga, S, Perez-Padilla, R, and Shamah-Levy, T. Dietary patterns and sleep disorders in Mexican adults from a National Health and nutrition survey. J Nutr Sci. (2021) 10:e34. doi: 10.1017/jns.2021.24
23. Ruiz-Perez, D, Guan, H, Madhivanan, P, Mathee, K, and Narasimhan, G. So you think you can PLS-DA? BMC Bioinformatics. (2020) 21:2. doi: 10.1186/s12859-019-3310-7
24. Akarachantachote, N, Chadcham, S, and Saithanu, K. Cutoff threshold of variable importance in projection for variable selection. Int J Pure Appl Math. (2014) 94:307–22. doi: 10.12732/ijpam.v94i3.2
25. Tapsell, LC, Neale, EP, Satija, A, and Hu, FB. Foods, nutrients, and dietary patterns: interconnections and implications for dietary guidelines. Adv Nutr. (2016) 7:445–54. doi: 10.3945/an.115.011718
26. Gherasim, A, Arhire, LI, Niță, O, Popa, AD, Graur, M, and Mihalache, L. The relationship between lifestyle components and dietary patterns. Proc Nutr Soc. (2020) 79:311–23. doi: 10.1017/s0029665120006898
27. Kim, KY, and Yun, JM. Dietary patterns and mild cognitive impairment risk in Korean adults over 50 years old. Prev Nutr Food Sci. (2021) 26:132–45. doi: 10.3746/pnf.2021.26.2.132
28. Chan, R, Chan, D, and Woo, J. A cross sectional study to examine the association between dietary patterns and cognitive impairment in older Chinese people in Hong Kong. J Nutr Health Aging. (2013) 17:757–65. doi: 10.1007/s12603-013-0348-5
29. Marrón-Ponce, JA, Tolentino-Mayo, L, Hernández, FM, and Batis, C. Trends in ultra-processed food purchases from 1984 to 2016 in Mexican households. Nutrients. (2018) 11:45. doi: 10.3390/nu11010045
30. Martínez Leo, EE, and Segura Campos, MR. Effect of ultra-processed diet on gut microbiota and thus its role in neurodegenerative diseases. Nutrition. (2020) 71:110609. doi: 10.1016/j.nut.2019.110609
31. Jacques, A, Chaaya, N, Beecher, K, Ali, SA, Belmer, A, and Bartlett, S. The impact of sugar consumption on stress driven, emotional and addictive behaviors. Neurosci Biobehav Rev. (2019) 103:178–99. doi: 10.1016/j.neubiorev.2019.05.021
32. Dalile, B, Kim, C, Challinor, A, Geurts, L, Gibney, ER, Galdos, MV, et al. The EAT-lancet reference diet and cognitive function across the life course. Lancet Planet Health. (2022) 6:e749–59. doi: 10.1016/s2542-5196(22)00123-1
33. Chávez-Mendoza, C, and Sánchez, E. Bioactive compounds from Mexican varieties of the common bean (Phaseolus vulgaris): implications for health. Molecules. (2017) 22:1360. doi: 10.3390/molecules22081360
34. Holland, TM, Agarwal, P, Wang, Y, Leurgans, SE, Bennett, DA, Booth, SL, et al. Dietary flavonols and risk of Alzheimer dementia. Neurology. (2020) 94:e1749–56. doi: 10.1212/wnl.0000000000008981
35. Rennard, BO, Ertl, RF, Gossman, GL, Robbins, RA, and Rennard, SI. Chicken soup inhibits neutrophil chemotaxis in vitro. Chest. (2000) 118:1150–7. doi: 10.1378/chest.118.4.1150
36. Thuy, NM, Hang, L, Triep, TL, Tân, ND, and Tai, NV. Development and nutritional analysis of healthy chicken soup supplemented with vegetables in Viet Nam. Food Res. (2019) 4:113–20. doi: 10.26656/fr.2017.4(1).248
37. Crowe-White, KM, Phillips, TA, and Ellis, AC. Lycopene and cognitive function. J Nutr Sci. (2019) 8:e20. doi: 10.1017/jns.2019.16
38. Imran, M, Ghorat, F, Ul-Haq, I, Ur-Rehman, H, Aslam, F, Heydari, M, et al. Lycopene as a natural antioxidant used to prevent human health disorders. Antioxidants (Basel). (2020) 9:706. doi: 10.3390/antiox9080706
39. Anand David, AV, Arulmoli, R, and Parasuraman, S. Overviews of biological importance of quercetin: a bioactive flavonoid. Pharmacogn Rev. (2016) 10:84–9. doi: 10.4103/0973-7847.194044
40. Nishihira, J, Nishimura, M, Kurimoto, M, Kagami-Katsuyama, H, Hattori, H, Nakagawa, T, et al. The effect of 24-week continuous intake of quercetin-rich onion on age-related cognitive decline in healthy elderly people: a randomized, double-blind, placebo-controlled, parallel-group comparative clinical trial. J Clin Biochem Nutr. (2021) 69:203–15. doi: 10.3164/jcbn.21-17
41. Xu, D, Hu, MJ, Wang, YQ, and Cui, YL. Antioxidant activities of quercetin and its complexes for medicinal application. Molecules. (2019) 24:1123. doi: 10.3390/molecules24061123
42. Heckman, MA, Weil, J, and Gonzalez de Mejia, E. Caffeine (1, 3, 7-trimethylxanthine) in foods: a comprehensive review on consumption, functionality, safety, and regulatory matters. J Food Sci. (2010) 75:R77–87. doi: 10.1111/j.1750-3841.2010.01561.x
43. Zhang, Y, Yang, H, Li, S, Li, WD, and Wang, Y. Consumption of coffee and tea and risk of developing stroke, dementia, and poststroke dementia: a cohort study in the UK biobank. PLoS Med. (2021) 18:e1003830. doi: 10.1371/journal.pmed.1003830
44. Solfrizzi, V, Panza, F, Imbimbo, BP, D'Introno, A, Galluzzo, L, Gandin, C, et al. Coffee consumption habits and the risk of mild cognitive impairment: the Italian longitudinal study on aging. J Alzheimers Dis. (2015) 47:889–99. doi: 10.3233/jad-150333
45. van Gelder, BM, Buijsse, B, Tijhuis, M, Kalmijn, S, Giampaoli, S, Nissinen, A, et al. Coffee consumption is inversely associated with cognitive decline in elderly European men: the FINE study. Eur J Clin Nutr. (2007) 61:226–32. doi: 10.1038/sj.ejcn.1602495
46. Beilharz, JE, Maniam, J, and Morris, MJ. Short-term exposure to a diet high in fat and sugar, or liquid sugar, selectively impairs hippocampal-dependent memory, with differential impacts on inflammation. Behav Brain Res. (2016) 306:1–7. doi: 10.1016/j.bbr.2016.03.018
47. Sharma, A, and Paliwal, KK. Linear discriminant analysis for the small sample size problem: an overview. Int J Mach Learn Cybern. (2015) 6:443–54. doi: 10.1007/s13042-013-0226-9
48. Cetinkalp, S, Simsir, IY, and Ertek, S. Insulin resistance in brain and possible therapeutic approaches. Curr Vasc Pharmacol. (2014) 12:553–64. doi: 10.2174/1570161112999140206130426
49. Sędzikowska, A, and Szablewski, L. Insulin and insulin resistance in Alzheimer's disease. Int J Mol Sci. (2021) 22:9987. doi: 10.3390/ijms22189987
50. Brown, L, Rosner, B, Willett, WW, and Sacks, FM. Cholesterol-lowering effects of dietary fiber: a meta-analysis. Am J Clin Nutr. (1999) 69:30–42. doi: 10.1093/ajcn/69.1.30
51. Cabral, CE, and Klein, M. Phytosterols in the treatment of hypercholesterolemia and prevention of cardiovascular diseases. Arq Bras Cardiol. (2017) 109:475–82. doi: 10.5935/abc.20170158
Keywords: dementia, mild cognitive impairment, older adults, nutrition, dietary pattern, Mexico
Citation: Garrido-Dzib AG, Palacios-González B, Ávila-Escalante ML, Bravo-Armenta E, Avila-Nava A and Gutiérrez-Solis AL (2024) Dietary patterns in mild cognitive impairment and dementia in older adults from Yucatan, Mexico. Front. Nutr. 11:1335979. doi: 10.3389/fnut.2024.1335979
Edited by:
Lina Begdache, Binghamton University, United StatesReviewed by:
Kristin Rene Krueger, Rush University Medical Center, United StatesCopyright © 2024 Garrido-Dzib, Palacios-González, Ávila-Escalante, Bravo-Armenta, Avila-Nava and Gutiérrez-Solis. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Berenice Palacios-González, YnBhbGFjaW9zQGlubWVnZW4uZ29iLm14; Ana Ligia Gutiérrez-Solis, Z2FuYWxpZ2lhQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.